Embed Size (px)
Citation preview

NZHTA REPORT
August 2004
Volume 7 Number 6
Evidence Based Review
of Weight Loss Medicines:
A report commissioned by the New Zealand
Accident Compensation Corporation (ACC)
Pamela Smartt
New Zealand
Health Technology Assessment
Department of Public Health and General Practice Christchurch School of Medicine
Christchurch, NZ.
Division of Health Sciences, University of Otago

NEW ZEALAND HEALTH TECHNOLOGY ASSESSMENT (NZHTA)
Department of Public Health and General Practice Christchurch School of Medicine, Christchurch, New Zealand
Evidence Based Review of Weight Loss Medicines: A report commissioned by the New Zealand Accident Compensation Corporation (ACC)
Pamela Smartt
NZHTA REPORT August 2004 Volume 7 Number 6

This report should be referenced as follows: Smartt, P. Evidence based review of weight loss medicines: a report commissioned by the New Zealand Accident Compensation Corporation (ACC). NZHTA Report 2004; 7(6). 2004 New Zealand Health Technology Assessment (NZHTA) ISBN 1-877235-70-9 ISSN 1174-5142
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
i
Acknowledgements
This report was prepared by Dr Pamela Smartt (Principal Investigator) who conducted the critical appraisals and prepared the project report. Dr Ray Kirk (NZHTA Director until February 2005) also provided comment on various drafts and coordinated the overall project. Dr Robert Weir (NZHTA Acting Director from February 2005) coordinated the project from February 2005. Ms Margaret Paterson (NZHTA Information Specialist) developed and undertook the search strategy and coordinated retrieval of documents. Mrs Ally Reid (NZHTA Administrative Secretary) provided document formatting.
The Canterbury Medical Library assisted with the retrieval of articles.
NZHTA is a Research Unit of the University of Otago funded under contract to the Ministry of Health.
Disclaimer
New Zealand Health Technology Assessment (NZHTA) takes great care to ensure the information supplied within the project timeframe is accurate, but neither NZHTA, the University of Otago, nor the contributors involved can accept responsibility for any errors or omissions. The reader should always consult the original database from which each abstract is derived along with the original articles before making decisions based on a document or abstract. All responsibility for action based on any information in this report rests with the reader. NZHTA and the University of Otago accept no liability for any loss of whatever kind, or damage, arising from reliance in whole or part, by any person, corporate or natural, on the contents of this report. This document is not intended as personal health advice. People seeking individual medical advice are referred to their physician. The views expressed in this report are those of NZHTA and do not necessarily represent those of the University of Otago or the New Zealand Ministry of Health.
Copyright
Copyright © to Accident Compensation Corporation 2005. All rights reserved. No part of this report may be reproduced or distributed by any person without prior written permission and/or licence from the Accident Compensation Corporation. http://www.acc.co.nz/

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
ii
Contact details
New Zealand Health Technology Assessment (NZHTA) Department of Public Health and General Practice Christchurch School of Medicine and Health Sciences PO Box 4345 Christchurch New Zealand Tel: +64 3 364 3696 Fax: +64 3 364 3697 Email: [email protected] Web Site: http://nzhta.chmeds.ac.nz/

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
iii
Contents
Contents .................................................................................................................. iii
Executive Summary ............................................................................................... vii
Recommendations ................................................................................................ viii
Background...............................................................................................................1
Definition and measurement of obesity........................................................................1
The health consequences of obesity ..............................................................................1
Factors influencing body weight ....................................................................................2
Clinically significant weight reduction...........................................................................3
Obesity and Injury............................................................................................................3
Obesity trends in NZ.......................................................................................................3
The economic cost of obesity.........................................................................................4
Benefits associated with weight loss ..............................................................................4
Review questions ..................................................................................................... 7
Pharmacological treatments for obesity .................................................................. 9
Pharmacological interventions registered in New Zealand........................................9
Phentermine (DuromineTM, Umine Timedcaps) ..........................................................9 Diethylpropion hydrochloride (Tenuate Dospan) .....................................................10 Sibutramine hydrochloride (Reductil®, Meridia®) ......................................................11 Orlistat (Xenical®)...........................................................................................................12 Meal replacement plans..................................................................................................14
Methodology ........................................................................................................... 15
Systematic review............................................................................................................15
Search strategy and information sources ....................................................................16
Study selection criteria ...................................................................................................17
Methods of the review...................................................................................................17
Levels of evidence ..........................................................................................................18
Results..................................................................................................................... 19
Meal replacement plans: weight loss and co-morbidity risk reduction...................19
Phentermine hydrochloride: weight loss and co-morbidity risk reduction............20
Diethylpropion: weight loss and co-morbidity risk reduction.................................22
Orlistat: weight loss and co-morbidity risk reduction...............................................23
Sibutramine: weight loss and co-morbidity risk reduction.......................................28
Comparative drug studies..............................................................................................34
Combined drug studies..................................................................................................39
Safety/Side effects ..................................................................................................41
Safety and side effects of sibutramine therapy...........................................................41
Safety and side effects of orlistat therapy ...................................................................42
Safety and side effects of phentermine therapy .........................................................43

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
iv
Safety and side effects of diethylpropion therapy......................................................43
Summary of potential harms of pharmacotherapy intervention .............................44
Safety and side effects of meal replacement programs .............................................44
Practice recommendations and guidelines ............................................................47
National Institute of Health, USA...............................................................................47
The National Institute for Clinical Excellence (NICE), UK ...................................47
High profile clinical trials .......................................................................................49
Completed studies ..........................................................................................................49
Childhood obesity ..........................................................................................................49
Ongoing trials..................................................................................................................50
Other anti-obesity therapies ...................................................................................51
Horizon Scan ..........................................................................................................53
Economic considerations .......................................................................................55
The direct cost of medication.......................................................................................55
Economic analysis ..................................................................................................57
Economic evaluations of orlistat ..................................................................................57 Economic evaluations of sibutramine .........................................................................58 Economic evaluations of phentermine........................................................................63 Economic evaluations of diethylpropion ....................................................................63
Discussion...............................................................................................................65
Criteria for the evaluation of medication for the treatment of obesity ..................65
Expected weight loss and duration of weight loss.....................................................66 Potential barriers to use .................................................................................................66
Evidence Summary and Conclusions .....................................................................67
Clinical effectiveness and circumstances of use.........................................................67
Safety and side effects....................................................................................................72
Ethnic groups..................................................................................................................73
Economic considerations..............................................................................................73
Evidence Tables......................................................................................................75
Appendices............................................................................................................ 105
References............................................................................................................. 113
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
v
Tables
Table 1. Classification of body weight.............................................................................................. 1 Table 2. Obesity related co-morbidities and risk............................................................................. 2 Table 3. Inclusion and exclusion criteria for review studies........................................................17 Table 4. Scottish Intercollegiate Guidelines Network Evidence levels .....................................18 Table 5. Weight loss results at three months and one year for an unstratified and stratified study population .................................................................................................................19 Table 6a. Phentermine effectiveness studies ...................................................................................21 Table 6b. Phentermine vs. placebo post treatment outcomes, Haddock et al., 2002 ................21 Table 7. Diethylpropion effectiveness studies, Glazer et al., 2001.............................................22 Table 8. Diethylpropion vs. placebo post treatment outcomes, Haddock et al., 2002............23 Table 9. Summary of publications reporting the effectiveness of orlistat for weight loss in overweight and obese participants ...................................................................................24 Table 10. Meta-analysis of RCTs for Orlistat, long-term studies ≥ 1 year (NICE HTA, ............
Avenell, May 2004).............................................................................................................25 Table 11. Orlistat 120 mg/d weight loss in otherwise healthy obese populations .....................26 Table 12. Orlistat 30-120 mg/d weight loss in patients with hypercholesterolemia, results after one year........................................................................................................................27 Table 13. Weight loss with orlistat: results of 1 year clinical trials, European Medicine
Evaluation Agency..............................................................................................................27 Table 14. Orlistat 120 mg/d in diabetic patients or patients with glucose intolerance..............27 Table 15. Eligible studies reporting the effectiveness of sibutramine ..........................................28 Table 16. Meta-analysis of RCTs for Sibutramine, long-term studies ≥ 1 year (NICE HTA, Avenell May 2004)...............................................................................................................30 Table 17. Studies reporting the effectiveness of sibutramine in otherwise healthy overweight individuals ........................................................................................................32 Table 18. Studies reporting the effectiveness of sibutramine in individuals with type 2 diabetes .................................................................................................................................32 Table 19. Sibutramine dose ranging studies. Bray 1999 reported in Leung et al., 2003.............34 Table 20. Eligible studies comparing two or more review drugs ..................................................34 Table 21. Summary of the comparative effectiveness of orlistat, sibutramine and low fat diets that may include meal replacements........................................................................35 Table 22. Summary of short-term weight loss trials of sibutramine and orlistat not otherwise reported in systematic reviews and HTAs.....................................................35 Table 23. A comparison of the effectiveness of sibutramine, orlistat, phentermine and diethylpropion (Glazer et al., 2001) ..................................................................................37 Table 24. A comparative study of the effectiveness of sibutramine, orlistat, phentermine and diethylpropion (Haddock et al., 2002) ......................................................................37 Table 25. Weight loss drugs trade off between benefit and harm.................................................38 Table 26. The effect of sibutramine on blood pressure and heart rate; results from 20 studies (Nisoli and Carruba, 2003)....................................................................................41 Table 27. NZ Drug pricing according to MIMS, 2004 ...................................................................55 Table 28. The estimated cost of a course of anti-obesity treatment .............................................55 Table 29. Studies reporting on the cost or cost effectiveness of sibutramine, orlistat, phentermine and diethylpropion.......................................................................................57 Table 30. Sensitivity analysis around two base estimates of the cost effectiveness of sibutramine when different utilities are assigned to weight loss...................................59 Table 31. Economic evaluations of orlistat, sibutramine and phentermine.................................61

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
vi
Evidence Table 1. Meal replacement, Heymsfield, 2003 ............................................ 76 Evidence Table 2. Meal replacement, Allison et al., 2003........................................... 77 Evidence Table 3. Orlistat, Torgerson et al., 2004....................................................... 78 Evidence Table 4. Orlistat, Rissanen et al., 2001 ......................................................... 79 Evidence Table 5. Orlistat, Muls et al., 2001 ................................................................ 80 Evidence Table 6. Orlistat, Foxcroft et al., 2000 ......................................................... 81 Evidence Table 7. Orlistat, Derosa et al., 2003 ............................................................ 82 Evidence Table 8. Orlistat, Hanefield et al., 2002........................................................ 83 Evidence Table 9. Orlistat, Halpern et al., 2003........................................................... 84 Evidence Table 10. Orlistat, Leung et al., 2003.............................................................. 85 Evidence Table 11. Orlistat, Heymsfield et al., 2000..................................................... 86 Evidence Table 12. Orlistat, O’Meara et al., 2001.......................................................... 87 Evidence Table 13. Orlistat, Padwal et al., 2004 ............................................................ 89 Evidence Table 14. Sibutramine, O’Meara et al., 2002.................................................. 90 Evidence Table 15. Sibutramine,Tambascia et al., 2003 ............................................... 91 Evidence Table 16. Sibutramine, Padwal et al., 2004 .................................................... 92 Evidence Table 17. Sibutramine, Leung et al., 2003 ..................................................... 93 Evidence Table 18. Sibutramine, Nisoli and Carruba, 2003......................................... 94 Evidence Table 19. Sibutramine, Berkowtitz et al., 2003.............................................. 95 Evidence Table 20. Sibutramine, Hazenberg et al., 2000.............................................. 96 Evidence Table 21. Sibutramine, Gokcel et al., 2001 .................................................... 97 Evidence Table 22. Sibutramine, Kim et al., 2003 ......................................................... 98 Evidence Table 23. Sibutramine, Hauner et al., 2003.................................................... 99 Evidence Table 24. Sibutramine, McNulty et al., 2003 ............................................... 100 Evidence Table 25. Sibutramine, Wadden et al., 2000 ................................................ 101 Evidence Table 26. Comparative drug study, Poston et al., 2001 ............................. 102 Evidence Table 27. Comparative drug study, Haddock et al., 2002.......................... 103

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
vii
Executive Summary
Obesity is a chronic, relapsing disease which increases the risk of a number of other serious diseases including diabetes, heart disease, hypertension, stroke and some cancers. Even a modest weight loss in obese individuals may be associated with significant health benefits arising from improvements in blood pressure, blood glucose and cholesterol levels.
Anti-obesity drug treatment is perceived as an adjunct to other weight loss strategies in an overall program of supervised weight reduction, weight loss maintenance or management. Co-interventions are typically a calorie controlled diet, behavioural therapy and/or physical exercise.
Weight loss drugs currently available in New Zealand include phentermine, diethylpropion, orlistat and sibutramine. Meal replacement products are readily available and popular non-pharmacological weight loss adjuncts.
The evidence suggests that phentermine, diethylpropion, orlistat, sibutramine and specified meal replacement plans/products are all effective at achieving a moderate weight loss in obese individuals. On average, an additional weight loss of approximately 4.0 kilograms may be achieved when these products are used as part of an appropriate weight loss program. Clinically important weight loss is considered to be a loss of ≥ 5% of initial body weight; a substantial proportion of patients were reported to have achieved this goal with the aid of weight loss drugs.
In comparative studies, the newer weight loss drugs orlistat (Xenical®) and sibutramine (Reductil®) are reported to be safer, more acceptable and more effective weight loss agents than the earlier amphetamine related drugs, phentermine and diethylpropion. They can be prescribed for longer periods than the older drugs and both orlistat and sibutramine are currently being tested in adolescents. Sibutramine use has been cautioned in this age group outside a clinical trial while orlistat has recently been approved by the Food and Drug Administration (FDA) for use in adolescents.
Sibutramine may result in a higher weight loss than orlistat but with side effects that may limit its use in patients with hypertension or cardiovascular disease. For these patients, orlistat may provide a useful alternative although the accompanying gastrointestinal (GI) side effects may not be acceptable to all patients. Meal replacement plans may be useful for patients who cannot tolerate or do not respond to either of these medications.
Sibutramine is reported to be cost-effective under most scenarios, with a lower estimated cost per quality adjusted life year (QALY) gained in patient groups with significant obesity related co-morbidities such as diabetes. The cost per QALY gained with orlistat is reported to be high and for healthy obese patients orlistat may not be cost-effective. However, for patients with obesity related co-morbidities such as hypertension and/or hypercholesterolemia, orlistat may be considered to be good value for money.
It is not clear if phentermine, diethylpropion or meal replacement plans are cost-effective treatments for obesity as no economic analyses of these therapies were identified, however, the direct cost of a course of phentermine or diethylpropion is much lower than the cost of orlistat or sibutramine.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
viii
Recommendations
The weight loss drugs sibutramine and orlistat are effective adjuncts to an appropriate clinical program of weight loss for obese ACC claimants. Short-term treatment of up to six months should be considered for maximum weight loss. Longer-term treatment – i.e., up to two years should be considered if weight loss is to be maintained.
Patients with uncontrolled hypertension or cardiovascular disease may not be suitable candidates for sibutramine therapy; in these patients orlistat should be considered.
Meal replacement products should be considered for patients who are unable to tolerate these medications or who have not had an appropriate response. There is insufficient evidence to enable any specific product recommendations to be made.
Each of these interventions should be part of a medically monitored comprehensive regimen of weight reduction based on a calorie controlled diet, behaviour modification and where possible, physical exercise and lifestyle modifications.
Individuals with a body mass index (BMI) ≥ 30kg/m2 are generally considered to be obese and should be considered for weight loss therapy. Claimants who have a BMI of ≥ 27kg/m2 and obesity related co-morbidities including diabetes, hypertension and sleep apnoea may also benefit from medical assistance with weight loss and should be considered.
Consideration should also be given to the differing recommendations for obesity thresholds in non-Caucasian populations. The World Health Organisation (WHO) has defined a lower
obesity threshold (BMI ≥ 25kg/m2) for use in Asian populations and a higher threshold (BMI ≥ 32kg/m2) for Polynesians.


EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
1
Background
Definition and measurement of obesity
Obesity is a chronic, relapsing disease in which there is an abnormal accumulation of body fat. Definitions and measurement of obesity vary but most researchers currently use BMI 1 to classify individuals in terms of weight; individuals with a BMI of ≥ 30kg/m2 are generally considered to be obese, see Table 1.
Table 1. Classification of body weight
BMI (kg/m2)
Weight Class % Above
Ideal weight Caucasian Asian* PI*
Normal 0% 18.5-24.9 18.5-22.9 18.5-22.9 Overweight 20% 25.0-29.9 23.0-24.9 26.0-31.9
Class I (mild) 20-40% 30.0-34.9 25-29.9 ≥32.0 Class II (moderate) 400-100% 35.0-39.9 ≥30.0
Obesea Class III (severe- morbid) >100% ≥40.0 - - *Figures taken from WHO, The Asia-Pacific Perspective: Redefining Obesity and its treatment. PI= Pacific Islander. a person with a BMI over 30 is considered to be obese and this is an arbitrary value obtained from epidemiological studies showing that a relationship between mortality and BMI follows a J-shaped curve and that mortality increases by 50-100% at BMI value above 30kg/m.
Generally BMI correlates well with body fat, however, BMI is not a foolproof guide to morbid fat accumulation, as it does not take into account body frame size, proportion of lean mass, age, gender or ethnic differences. Misclassification can occur when a BMI =30kg/m2 threshold is used to define obesity in non-Caucasian populations. Polynesians tend to have a lower fat percentage than Caucasians for any given BMI and the threshold for obesity in Polynesians is BMI ≥ 32kg/m2. Asian populations, however, have more fat and co-morbidities for any given BMI than Caucasians and a lower obesity threshold of BMI=26kg/m2 has been suggested (Proietto and Baur 2004).
Other useful, but less commonly used, obesity indices include waist to hip ratio and waist circumference. These measures may provide additional useful information regarding risk factors associated with weight gain. In Caucasians, a WHR>1.02 for men and a WHR >0.88 for women is used to identify obesity and abdominal fat accumulation (NHANES III); this may be a better predictor of weight related cardiovascular risk than BMI.
Genetic disorders such as Alstrom’s syndrome and endocrine disorders such as hypothyroidism and Cushing’s disease must be ruled out before diagnosing obesity (Leung et al. 2003).
The health consequences of obesity
The 1997 New Zealand National Nutrition Survey (Wilson et al. 2001) estimated that the health risks associated with obesity were equivalent to a number of high-risk, chronic diseases including type 2 diabetes, heart disease, hypertension, stroke, gallstones and some cancers.
1 BMI= weight in kilograms divided by height in metres squared (kg/m2).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
2
The distribution of body fat is an important determinant of the type of associated health risk; abdominal or visceral fat (android obesity) is associated with increased risk of cardiovascular mortality, hypertension and non-insulin dependent diabetes.
Increased health risks for conditions associated with obesity vary from a substantial to moderately raised risk for diabetes, heart disease, hypertension and a number of other metabolic disturbances (Brown et al. 2000; Carey et al. 1997; Chan et al. 1994; Manson et al. 1990; Rimm et al. 1995) to a slightly raised risk for some cancers and lower back pain (Bergstrom et al. 2001a; Bergstrom et al. 2001b; Calle et al. 2003; Oliveria et al. 1999). There is also an increased risk of adverse events from anaesthesia in obese patients, see Table 2.
Table 2. Obesity related co-morbidities and risk
Substantial Risk Increase (RR>3) Moderate Risk Increase (RR=2-3) Slight Risk Increase (RR= 1-2)
Type II diabetes Coronary heart disease Breast, endometrial, colon cancers
Gall bladder Hypertension Reproductive hormone abnormalities
Dyslipidaemia Osteoarthritis of the knee and hips Polycystic ovary syndrome
Metabolic syndrome Hyperuricemia Impaired fertility
Sleep apnoea Gout Low back pain
Breathlessness Increased anaesthetic risk
Foetal defects (maternal obesity) RR= relative risk is the probability of an event in the treatment group divided by the probability of the event in the control group.
Psychological problems such as clinical depression are also associated with obesity. These problems may impact on quality of life and result in job discrimination and other employment difficulties.
Factors influencing body weight
A number of factors influence body weight and fat levels making some individuals more susceptible to obesity. Known contributors are:
• ethnicity
• gender
• age
• hormonal state
• genetic make-up.
People from southern Asia are at a greater risk of developing central obesity and their cardiovascular risk increases rapidly at lower levels of obesity relative to western standards. For this ethnic group increased cardiovascular risk starts at a BMI of 21-23kg/m2.. The WHO2 has proposed new obesity guidelines for Asian populations with an obesity threshold defined as a
BMI ≥25kg/m2. Individuals with certain learning disabilities such as Down’s syndrome are also at higher risk of obesity (NHS Centre for Reviews and Dissemination 1997).
2 WHO 2000, Redefining obesity and its treatment.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
3
Clinically significant weight reduction
Most obese individuals would need to shed 30% of their body weight to reach their “ideal weight”. Such goals are generally unrealistic. However, much smaller reductions in weight can be accompanied by substantial health gains. A clinically significant weight reduction can be achieved with a body weight loss of 5-10% within six months. Many obese people experience difficulty in achieving this amount of weight loss in the timeframe through diet and exercise alone (Derosa et al. 2003). These people may benefit from the pharmacological interventions reviewed here.
Obesity and Injury
Weight loss may be viewed as a modality to improve general health as well as an aid to treatment and recuperation from accident or injury. A number of obesity associated health problems may be present at the time of accident or injury, or acquired afterwards, as a result of mobility and lifestyle changes. Such problems may impede recovery and rehabilitation and impede or limit the effectiveness of treatment.
For individuals recovering from accidents and injury, obesity related problems may significantly interfere with treatment and recovery. Obese claimants may be refused surgical treatment because of increased risks associated with anaesthesia. Existing obesity or obesity arising from lack of mobility, activity and exercise after an accident or injury may interfere with a claimant’s return to independence or full employment. It may also substantially increase the claimant’s recuperation period. Personal care requirements may also increase, particularly in relation to attendant care and additional health interventions may be required for co-morbid conditions, which may be initiated or exacerbated as a consequence of obesity.
Obesity trends in NZ
A substantial proportion of the New Zealand population is obese. In 1997, the National Nutrition Survey reported that more than half of New Zealand adults were overweight with 17% classified as obese; it is estimated that by 2011 this will have risen to 29% (Wilson et al. 2001). Obesity rates in Maori and Pacific Islanders are higher than for the general New Zealand population with 27% of Maori men, 26% of Pacific men, 28 % of Maori women and 47% of Pacific woman reported as obese by the 1997 survey. Obesity in New Zealand children is also increasing and is of some concern.
Given these statistics it is highly likely that a significant number of ACC claimants will be obese or at risk of obesity at the time of accident or injury. Since some ethnic groups are more at risk of obesity than others, a correspondingly greater proportion of obese claimants, or claimants with recovery related obesity risk, may be expected in these susceptible groups. It is estimated that 75% of Pacific peoples in New Zealand are overweight; an immobilising accident or injury could put these claimants at risk of becoming obese while recovering from an accident or injury.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
4
The economic cost of obesity
The high prevalence of obesity in New Zealand and its associated co-morbidities suggests that obesity is likely to command a significant portion of the total health care costs incurred by any government agency.
Three component costs have been identified:
• the direct treatment cost to the individual and the service provider
• the opportunity costs to the individual and society arising from premature death or attributable morbidity
• the indirect costs to the individual and society of lost work production due to absenteeism from work and premature death.
An overall assessment of the economic cost of obesity by the WHO suggested that it accounts for between 2-7% of total health care costs in developed countries. As a significant proportion of ACC claimants are likely to be obese or overweight at the time of injury or accident, additional costs arising from obesity related complications may be expected. The additional cost may be expected to arise from the:
• direct cost of obesity treatment
• indirect costs associated with delays in returning the claimant to full employment as a result of obesity-related co-morbidities or treatment and rehabilitation problems arising from morbid obesity.
Benefits associated with weight loss
Even a modest weight loss of 5-10% has been associated with significant health benefits in the obese patients. These benefits arise from improvements in obesity related co-morbidities including blood pressure, blood glucose and cholesterol levels. It has been estimated that for every one kilogram reduction in body weight there is a:
• 0.05mmol/l decrease in total cholesterol
• 0.02mmol/l decrease in low density lipoprotein cholesterol (LDL-cholesterol)
• 0.015mmol/l decrease in triglycerides
• 0.007mmol/l increase in high density lipoprotein cholesterol (HDL-cholesterol).
Weight loss and dietary fat modification appear to have independent and additive effects on the reduction in serum lipids: the net favourable effect of weight loss seems to be greater than that of dietary fat modification as weight loss per se is only responsible for about 60% of the fall in LDL-cholesterol and 70% of the fall in triglycerides (Muls et al. 2001). Every 1% reduction in glycated haemaglobin (HbA1c) decreases cardiac complications from 9-40% depending upon the population and diabetes type (Gokcel et al. 2001).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
5
Higher weight losses have greater benefits (Jung 1997); a 10kg weight loss may be expected to incur:
• 10mmHg decrease in systolic blood pressure (SBP)
• 20mmHg decrease in diastolic blood pressure (DBP)
• 91% reduction in angina symptoms
• 33% raise in exercise tolerance
• 10% fall in total cholesterol
• 15% fall in LDL-cholesterol
• 30% fall in triglycerides
• 8% increase in HDL-cholesterol
• >50% reduction in the risk of developing diabetes
• 30-50% fall in fasting blood glucose
• 15% fall in HbA1c.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
6

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
7
Review questions
The following questions guided the current review:
• What are the most appropriate measures used to classify obesity and how is obesity defined across different ethnic and age groups – is the BMI of >35, as set out in ACC's 2001 guidance, still an appropriate definition of obesity for all claimants?
• What is the relative effectiveness of phentermine, diethylpropion, orlistat, sibutramine and meal replacement plans for claimants requiring treatment to aid weight loss and what degree of weight loss can be expected and maintained with each product?
• How long do the products take to achieve a clinically important weight loss and what are appropriate time limits for treatment with the various product regimes?
• What are the circumstances in which the various products should be used and what are the potential barriers to implementation?
• How do the specified products compare in terms of safety, contraindications and patient acceptability?
• What is the relative cost-effectiveness of specified products for claimants requiring treatment to aid weight loss?
• Do the effectiveness and cost-effectiveness of the various products vary according to patients’ ethnicity, and if so, how?

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
8

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
9
Pharmacological treatments for obesity
Pharmacological treatments for obesity are limited. Most have the potential to produce undesirable side effects, additionally, amphetamines administered for the purposes of weight loss may have euphoric actions and carry the potential for abuse (Silverstone 1992). Some previously available products have recently been withdrawn from the market in a number of countries, for example:
• phenylpropanolamine, an appetite suppressant, has been associated with increased haemorrhagic stroke in women and withdrawn in the USA
• fenfluramine and dexfenfluramine – two centrally acting appetite suppressants acting predominantly by releasing serotonin, were also withdrawn from the market recently because of an association with pulmonary hypertension and coronary valve damage (Gardin et al. 2000).
Pharmacological interventions registered in New Zealand
There are currently four generic drugs prescribed for the treatment of obesity in New Zealand:
• phentermine
• diethylpropion
• orlistat
• sibutramine.
Other non-pharmacological interventions include meal replacement products and plans and bariatric surgery. Surgery for obesity is not considered in this review.
Phentermine (DuromineTM, Umine Timedcaps3)
Phentermine has been available since the 1960s with a reported worldwide exposure of more than 50 million prescriptions (Glazer 2001). It is available in New Zealand as a resin under the brand name Duromine (15 or 30mg) or in a sustained release hydrochloride form under the brand name of Umine Timedcaps (30mg).
Phentermine is an appetite suppressant chemically related to amphetamine. It has its main effect on the dopaminergic and noradrenergic nervous systems and its actions include central nervous system (CNS) stimulation and blood pressure elevation. The resin complex (Duromine) is insoluble until it reacts with the GI fluids; phentermine is then released from the resin throughout the GI tract over a period of 10-14 hours. Phentermine HCL sustained release capsules (Umine) has peak concentrations at 2.4 hours after ingestion. There is almost complete absorption of the drug but eventually 70-80% of the oral dose is excreted unchanged in the urine with the remainder metabolised by the liver. The half-life of phentermine is about 25 hours.
3 Also marketed under the product names Ionamine, Fastin, Adipex in the USA.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
10
Phentermine use in children under 12 years, elderly patients and pregnant or breastfeeding women is not advised as safety and efficacy in these populations has not been established.
Dosage and administration: the starting dose is usually 30mg/d (milligrams per day), however, in light framed patients or those who have suffered side effects a dose of 15mg/d may be prescribed. Failure to achieve a weight reduction of 5% within 12 weeks of starting phentermine therapy is an indication for discontinuation of treatment. In order to reduce the risk of dependence, the maximum continuous period of treatment should not exceed 4-8 weeks.
Circumstances of use: phentermine may be used as a short-term adjunct in a medically monitored comprehensive regimen of weight reduction based on exercise, calorie controlled diet and behaviour modification in patients with a BMI ≥30kg/m2 who have not had an appropriate clinical response to an appropriate weight reduction program alone. Patients with obesity related co-morbidities such as sleep apnoea, insulin resistant diabetes mellitus, pre diabetes mellitus or impaired glucose tolerance (IGT) or high cardiovascular risk status, and have a BMI of less than 30kg/m2 may also be considered for treatment with phentermine.
Mode of action: phentermine is an amphetamine which operates by stimulating the release of noradrenaline and dopamine; it also inhibits monoamine oxidase (Lean 2001). Its central catecholamine mechanisms cause appetite suppression for 12-14 hours (Thearle and Aronne 2003).
Indications: phentermine 15mg and 30mg are indicated as a short-term adjunct in a medically monitored regime of weight reduction in obese patients that includes a calorie controlled diet, exercise and behaviour modification. It may also be appropriate to use phentermine in overweight patients with an increased risk of morbidity from other medical conditions including sleep apnoea, insulin resistant diabetes or IGT and cardiovascular disease.
Contraindications: patients with pulmonary artery hypertension, heart valve abnormalities or heart murmur, moderate to severe hypertension, cerebrovascular or cardiac disease, hypersensitivity to sympathomimetic drugs, hyperthyroidism, agitated states or psychiatric illness, depression, major eating disorder, glaucoma and patients with a history of substance abuse or dependence (Medsafe 2003).
Warning and precautions: serious cardiac valvular disease and primary pulmonary hypertension (PPH) has been reported in patients who have taken phentermine and fenfluramine or dexfenfluramine combinations (“phen-fen”) for weight loss. There have been no reported cases of valvular disease and only very rare cases of PPH in patients taking phentermine alone. There is also a theoretical risk of cardiac valvular disease if phentermine is combined with selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine and paroxetine, ergot derived drugs and clomipramine. Phentermine should not be administered with monoamine oxidase inhibitors and should be used with caution in patients with mild hypertension and patients under treatment with hypertensive agents as it may cause some loss of blood pressure control. The ability to perform activities requiring mental alertness such as driving and operating machinery may be impaired while taking phentermine (Medsafe 2003).
Diethylpropion hydrochloride (Tenuate Dospan)
Diethylpropion is an appetite suppressant or anorexiant. It is rapidly absorbed after oral administration with 75-100% of the dose excreted in the urine as diethylpropion hydrochloride or its metabolites. The half-life of diethylpropion in the plasma is about two hours and the excretory half-life of the drug and its metabolites is approximately 10 hours.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
11
The use of diethylpropion in children younger than 18 years and pregnant or breastfeeding women is not advised as safety and efficacy in these populations has not been established. Secondary organic causes of obesity should be excluded by diagnosis.
Dosage and administration: the recommended dose of sustained-release diethylpropion is 75mg once daily, one hour before meals. It is intended for short-term intermittent use only. Courses may be given over a period of up to 12 weeks with intervening period of at least one month without treatment. To limit unwanted exposure, treatment should be continued only if there is satisfactory weight loss within the first four weeks of treatment. Insulin requirements may need to be altered.
Circumstances of use: diethylpropion may be used as a short-term adjunct in a medically monitored comprehensive regimen of weight reduction based on exercise, calorie restriction and behaviour modification in obese patients with a BMI ≥ 30kg/m2 who have not had an adequate response to an appropriate weight loss program of diet and/or exercise alone. Patients with a BMI of less than 30kg/m2 with co-morbidities including sleep apnoea, insulin resistant diabetes mellitus, pre diabetes mellitus or IGT or high cardiovascular risk status, may require medical assistance with weight loss. Such patients may also be considered for treatment with diethylpropion.
Mode of action: diethylpropion is a sympathomimetic amine, it acts as a CNS stimulant, increasing the heart rate, raising blood pressure and decreasing the appetite.
Indications: diethylpropion is indicated as a short-term adjunct in a medically monitored comprehensive weight loss program based on calorie restricted diet, exercise and behaviour modification in obese patients who have not achieved an adequate weight reduction using diet and exercise alone. Overweight patients with sleep apnoea, insulin-resistant diabetes, IGT or with a high risk of cardiovascular disease may also be considered for treatment.
Contraindications: severe hypertension or pulmonary artery hypertension, advanced arteriosclerosis, hyperthyroidism, known hypersensitivity to sympathomimetic amines, glaucoma, agitated states and patients with a history of drug abuse. Failure to achieve a weight reduction of 5% in a period of 12 weeks is an indication for discontinuation of treatment. Use in conjunction with other anorectic agents is contraindicated (Medsafe 2004b).
Warning and precautions: diethylpropion should not be given during or within 14 days of monoamine oxidase inhibitors. It is not recommended for patients who have taken any anorectic agents within the prior year or for patients with a heart murmur or valvular heart disease. The use of anorexiants has been associated with PPH and an increased risk of PPH with repeated courses of therapy cannot be excluded. Epileptic patients should be carefully monitored. Diethylpropion should be used with caution in patients undergoing general anaesthesia (Medsafe 2003).
Sibutramine hydrochloride (Reductil®, Meridia®)
Sibutramine is an orally administered drug that promotes satiety after eating and stimulates energy expenditure (Lean 2001; Nisoli and Carruba 2003). It is the first product of its type to be used for the management of obesity (Medsafe, sibutramine data sheet). The drug is rapidly absorbed following ingestion with maximal plasma concentrations at one hour and an elimination half-life of about one hour. Most (77%) of the drug is absorbed from the GI tract and up to 85% of the oral dose is excreted in the urine and faeces.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
12
Sibutramine and its metabolites do not enhance dopamine release and have not been shown to have a potential for abuse (Schuh et al. 2000).
The long-term effects of sibutramine on the mortality and morbidity associated with obesity have not been established. Its use in obese children under 18 years, patients over 65 years and pregnant or breastfeeding women is not advised as safety and efficacy in these populations has not been established.
Dosage and administration: the recommended starting dose is 10mg once daily with or without food; in clinical trials sibutramine was given in the morning. If there is less than 2kg weight loss after four weeks and the 10mg dose is well tolerated the daily dose may be increased to 15mg. Patients usually achieve maximum weight loss – i.e., 5-10% of initial body weight, after six months of treatment. The European Union label states that patients responding well may be treated for up to a year, in the USA treatment may be maintained for up to two years (Astrup and Toubro 2001). The frequency of adverse events may be reduced if sibutramine is administered intermittently – i.e., alternating with placebo or drug free periods (Wirth and Krause 2001).
Circumstances of use: sibutramine may be used for the management of obesity including weight loss and weight maintenance in patients with a BMI ≥ 30kg/m2 or a BMI of ≥ 27kg/m2 in patients who have diabetes, dyslipidaemia or hypertension. It is intended for use when patients have not adequately responded to appropriate weight-reducing therapy such as hypocaloric diet and/or exercise alone – e.g., patients having difficulty in achieving or maintaining a 5% weight loss within three months.
Mode of action: sibutramine is a centrally acting monoamine reuptake inhibitor which blocks the pre-synaptic reuptake of serotonin and noradrenaline thereby potentiating the anorexic effect of these two neurotransmitters in the CNS.
Indications: sibutramine 10mg and 15mg is indicated as adjunctive treatment within a weight management program for patients between 18-65 years with a BMI of 30kg/m2 (i.e., obese) or patients with a BMI of 27kg/m2 (i.e., overweight) who also have type 2 diabetes or dyslipidemia. Patients must have failed to lose weight on diet and exercise in the past.
Contraindications: patients with severe hepatic or renal dysfunction, hypersensitivity to sibutramine, organic obesity or history of major eating disorders, patients with psychiatric illness, drug or alcohol abuse, inadequately controlled hypertension or history of cardiovascular disease, narrow angle glaucoma, hyperthyroidism, benign prostatic hyperplasia with urinary retention and phaeochromocytoma (Medsafe 2004a).
Warning and precautions: blood pressure and pulse rate should be monitored while patients are taking sibutramine. The ability to drive a vehicle or operate hazardous machinery may be impaired when taking sibutramine (Medsafe 2004a).
Orlistat (Xenical®4)
Orlistat is a novel anti-obesity agent that inhibits the digestion of fat. Undigested trigylcerides are excreted in the faeces 24 to 48 hours after administration resulting in a calorific deficit that has a positive effect on weight control.
4 Xenical®, Hoffman-Roche.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
13
Orlistat is minimally absorbed into the systemic circulation with approximately 97% of the administered dose excreted in the faeces, 83% is unchanged orlistat (Medsafe 2004c). The time to complete excretion is three to five days.
The long-term effects of orlistat on the mortality and morbidity associated with obesity have not been established. Its use in children, adolescents below the age of 18 years, patients over 65 years and pregnant or breastfeeding women is not advised as safety and efficacy in these populations has not been established.
Dosage, administration: the recommended dose of orlistat is 120mg three times a day (t.i.d.) with each main meal. Higher doses have not been shown to provide additional benefit. The greatest weight loss occurs within the first six months of treatment. In the USA, treatment may be maintained for up to two years (Astrup and Toubro 2001).
Circumstances of use: orlistat may be used for weight loss, weight maintenance and prevention of weight regain in adults with a BMI ≥ 30kg/m2. It should be used in conjunction with a low fat calorie controlled diet that is nutritionally balanced, rich in fruit and vegetables and contains approximately 30% of calories from fat distributed over three meals.
Mode of action: orlistat is a synthetic derivative of lipstatin a naturally occurring lipase inhibitor produced by Streptomyces toxytricini. It is a potent and specific irreversible inhibitor of pancreatic and gastric lipases that acts by bonding at the active site of lipases in the lumen of the GI tract. The inactivated enzyme is unable to hydrolyse ingested triglycerides into free fatty acids and monoglycerides for absorption. At the recommended dose and when diet contains approximately 30% of calorific intake from lipids, about 20g (180kcal) of fat is excreted in the daily stool. Orlistat may also influence dietary choices as high fat meals can lead to more severe GI adverse events.
Indications: orlistat is indicated as adjunctive treatment within a low fat calorie controlled program for obese patients between 18-65 years with a BMI of 30kg/m2. Patients must have demonstrated weight loss of 2.5kg one month before its use.
Contraindications: patients with chronic malabsorption syndrome, cholestasis, known hypersensitivity to orlistat or any of its components (Medsafe 2004c).
Warning and precautions: because of a possibility of a decreased absorption of fat soluble vitamins A, D, E, K and beta-carotene, the use of multivitamin supplements may be considered while patients are taking orlistat. High fat meals are likely to increase the possibility of GI events and patients should adhere to dietary fat intake guidelines. A reduction of plasma levels of cyclosporine5 is possible after orlistat administration; the effect of amiodarone may also be reduced. Coagulation parameters of patients on concomitant oral anticoagulants should be monitored. There is no information relating to effects on ability to drive and used machines (Medsafe, orlistat data sheet). The additive GI effects of concomitant use of orlistat and olestra, a non-absorbable dietary fat substitute commonly available in snack foods such as potato chips, has been reported (Heck et al. 2002).
5 Cyclosporine absorption may be reduced by approximately one third (Zhi et al., 2003).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
14
Meal replacement plans
Low calorie diets (LCDs) – i.e., diets in the range of 1200-1600kcal/day, are the cornerstone of modern weight control efforts. Meal replacement strategies and products are used by millions of consumers worldwide, however, there are no established definitions of meal replacement or partial meal replacement (PMR) plans, (Heymsfield et al. 2003).
The term ‘meal replacement’ is generally used in the scientific literature to cover beverages, pre-packaged shelf-stable and frozen entities and meal or snack bars. Most of these products are fortified with vitamins and minerals designed to be consumed in place of one or more regular meals. They may be an adjunct in a LCD. Eating, behaviour modification and physical exercise advice usually accompany commercial meal replacement programs.
Meal replacement nutritional supplements may be a useful weight loss therapy in obese individuals who:
• do not want to use weight loss drugs
• cannot tolerate the side effects of weight loss drugs
• cannot maintain eating habit change
• do not respond to weight loss drugs.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
15
Methodology
The main methodological tools for this review include a comprehensive literature search for published studies that fulfil pre-determined criteria, a systematic review of eligible studies and a synthesis of the evidence guided by specific review questions (see page 7).
Systematic review
A systematic review is a carefully defined process that involves systematically locating, appraising and synthesising evidence from scientific studies in order to obtain a reliable overview. The literature search is comprehensive involving as many relevant sources as possible being accessed; the study selection, data extraction and data pooling are performed according to pre-set criteria. The adherence to scientific principles sets the systematic review apart from traditional literature reviews making it less biased and more objective (O'Meara et al. 1998).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
16
Search strategy and information sources
Search strategy
A comprehensive literature search of major relevant bibliographic and review databases was undertaken together with additional searches for clinical trials, guidelines, government, and other evidence-based materials. A range of subject headings and keyword searches were used to search indexed databases (see Appendix II). The search was not restricted by date, but was restricted to English language articles. In addition, a methodology filter was used to identify systematic reviews, randomised controlled trials (RCTs), and economic studies. This comprehensive strategy identified 777 potentially relevant journal references. After screening the abstracts of these references, 211 full text articles from peer-reviewed journals were retrieved for analysis. All relevant health technology assessment (HTA) resources were also examined and five international HTA reports of pharmacological treatment of obesity were retrieved.
Principal sources of information
The following databases were searched using the search strategy outlined in Appendix II. The searches were carried out during June and July 2004.
Bibliographic databases
Medline
Cinahl
Embase
Web of Science
Current Contents
Toxnet
Cochrane Controlled Trials Register
Review databases
Cochrane Database of Systematic Reviews
Database of Abstracts of Reviews of Effects
Health Technology Assessment Database
NHS Economic Evaluation Database

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
17
Study selection criteria
The FDA guidelines for the clinical evaluation of weight-control drugs and the selection criteria set out in the recent HTAs of obesity treatment guided the determination of inclusion and exclusion criteria for this review. All studies of pharmacological agents included in the review were required to be randomised, placebo or active control double-blind studies with weight loss as the primary outcome and obese participants as the primary study population. Additionally, studies had to be written in English and published between 1996-2004.
Table 3. Inclusion and exclusion criteria for review studies
Inclusion Criteria
Study design Randomised placebo or active control, double-blind studies or HTAs or systematic reviews or meta-analyses of randomised, placebo-controlled, double-blind trials or RCTs, double blind, comparative drug trials, OR for meal replacement, a RCT against standard meal or diet plan.
Primary study purpose Weight loss Study size Unrestricted Study duration/ length of follow-up Any duration of treatment. Follow–up of at least 12 months for long-term benefits, any follow-
up length for short-term benefits. Participants Individuals with a BMI of at least 30kg/m2, no age restriction. Interventions Licensed drugs, sibutramine, orlistat, phentermine, diethylpropion or meal replacement
plans/products with or without co-interventions such as diet counselling, deficit diets, dietary advice sheets, education and encouragement to exercise if appropriate.
Outcome measures/endpoints Primary endpoints - actual weight loss, relative weight loss (% of body weight or % excess over ideal weight or change in BMI), changes in central obesity. Secondary endpoints - measurement of obesity related risk factors – e.g., lipids, blood pressure and glucose tolerance.
Health economics All economic and cost evaluations Language English language or English translation available Study dates/publication date Jan 1996-July 2004 Publication type Studies published in peer-reviewed journals or manufacturer’s unpublished material if
relevant and available.
Exclusion criteria
Pregnant or breastfeeding mothers Abstracts and case reports Animal studies Non-clinical studies Preliminary exclusion of overweight +co-morbidities Quasi randomised, open label and cross-over trials Studies recruiting patients with eating disorders such as anorexia or bulimia nervosa Single RCTs with a crossover design*
* Excluded because of (i) the possibility of carry over effects and (ii) because they are excluded from most meta-analyses because of their inadequacy in terms of estimating effect size (Kim et al. 2003).
Methods of the review
Studies were not limited in duration but in the analysis of results studies were considered in two groups to reflect the primary needs of ACC claimants:
• short-term studies – i.e., treatment duration < 6 months
• long-term studies – i.e., treatment durations ≥ 6 months.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
18
Further stratification by co-morbidity was carried out where feasible and obese patients with:
• type 2 diabetes
• hypercholesterolemia
• hypertension
were analysed separately to assess differences in need, weight loss goals and expectations that may be required by claimants with obesity related co-morbidities.
Levels of evidence
The evidence was graded using the Scottish Intercollegiate Guidelines Network (SIGN) instrument, see Table 4.
Table 4. Scottish Intercollegiate Guidelines Network Evidence levels
Level Type of evidence/study
Ia Evidence obtained from meta-analysis of randomised controlled trials Ib Evidence obtained from at least one randomised controlled trial IIa Evidence obtained from at least one well designed controlled study without randomisation IIb Evidence obtained from at least one other type of well-designed quasi-experimental study III Evidence obtained from well-designed non-experimental descriptive studies, such as comparative studies, correlation studies
and case control studies. IV Evidence obtained from expert committee reports or opinions and/or clinical experience of respected authorities.
However, only evidence from RCTs, systematic reviews, and meta-analysis of RCTs or HTAs including RCTs was considered in this review, limiting the evidence levels to Ia or Ib.
The main purpose of randomisation is to minimise bias, however, the quality of randomised studies can vary. Where the normal quality criteria are not met a number of biases may occur, these can be minimised in a number of ways:
• selection bias - full explanation of the method of randomisation, including concealment
• attrition bias - full reporting of the number and type of withdrawals and drop-outs
• intention to treat (ITT) analysis - preserves the baseline comparability between treatment groups achieved by randomisation
• detection bias - blinding of outcome assessor and blinding of participants.
The robustness and validity of the eligible studies was further determined from the degree of bias minimisation based on the four criteria above. The most useful and reliable study was considered to be a well designed and properly conducted randomised, placebo-controlled, double-blind clinical trial or a meta-analysis of such studies. Where blinding is not possible because of the nature of the intervention – e.g., meal replacements, a well designed and properly conducted RCT or meta-analysis was considered to be the most useful type of study for the purpose of this review.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
19
Results
Meal replacement plans: weight loss and co-morbidity risk reduction
Meal replacement eating plans have not been critically evaluated for safety and efficacy until very recently. The first meta-analysis evaluating RCTs of PMR plans and products was published in 2003 (Heymsfield et al. 2003). In this study a search of Medline, Embase and the Cochrane Clinical Trials Register between 1960 to January 2001 for clinical trials with meal replacements or meal plans, identified 276 potential publications of which 30 were meal replacement as defined in the protocol. Only six studies finally met the review criteria, 24 were excluded due to one or more of the following:
• lack of a control arm
• less than 12 weeks duration
• not meal intervention as defined in protocol
• inclusion of subjects <18 years
• inclusion of subjects BMI <25kg/m2
• use of the anorexic drug diethylpropion.
For the purpose of the Heymsfield meta-analysis, a PMR plan was defined as a program that:
“ includes one or more meals replaced by a commercially available, calorie-reduced product(s) that are fortified with vitamins and minerals and at least one daily meal consisting of regular foods. As a LCD, the plan’s calorie content should be >800<=1,600kcal/day.”
Primary data were available from the six eligible RCTs. These data were used in a meta-analysis and pooling analysis, see Table 5.
Table 5. Weight loss results at 3 months and one year for an unstratified and stratified study population
N=
ΛΛΛΛ (PMR-RCD)
kg(s.e.) 3 months
Significance of PMR-RCD difference
p=
N=
ΛΛΛΛ (PMR-RCD)
kg(s.e.) 12 months
Significance of PMR-RCD difference
p= Analysis of all participants - unstratified Meta-analysis Random effects 403 2.60(0.96) 0.006 219 2.43(1.65) 0.142 Meta analysis Fixed effects 403 3.01(0.33) <0.001 219 3.39(0. 72) <0.001 Pooled analysis of completers 403 2.54(0.37) <0.001 219 2.63(0.88) 0.003 Pooled analysis LOCF 485 2.39(0.35) <0.001 485 2.86(0.46) <0.001 Analysis - stratified by diabetic status Non-diabetic completers 305 2.79(0.37) <0.001 193 3.17(0.99) 0.002 Non-diabetic LOCF 367 2.67(0.35) <0.001 367 3.56(0.50) <0.001 Diabetic completers 98 2.46(1.84) 0.185 26 2.76(2.00) 0.183 Diabetic LOCF 118 2.62(1.89) 0.167 118 1.52(1.89) 0.424
Λ (PMR-RCD) = weight loss difference between the treatment (PMR) and the control (RCD) group measured from baseline body weight to body weight at the time of assessment. PMR = partial meal replacement, RCD = restricted calorie diet.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
20
For detailed results see Meal Replacement in Evidence Table 1, Heymsfield, 2003.
All methods of analysis indicated a significantly greater weight loss for individuals following the PMR plan than those following the conventional reduced calorie diet. On average, the PMR group lost 2.54 kilograms more than the control group after three months of treatment and 2.43 kilograms more after 12 months. The proportion of subjects losing ≥ 5% of initial body weight was 33% for the RCD group and 72% for the PMR group (p<0.001); at 12 months the proportions were 33% and 74% (p<0.001).
After stratification according to diabetic status, the non-diabetic completers lost on average 2.79 kilograms more than the control group after three months (p<0.001) and 3.17 kilograms more after 12 months (p=0.002). The much smaller diabetic completers lost on average 2.46 kilograms more than the control at three months and 2.76 kilograms more than the control at 12 months. Neither difference reached significance, however, the number of diabetic cases was small and the standard error for the group large.
All of the risk factors for obesity related co-morbidities showed improvement from their baseline values in both the treatment and control groups (p<0.001), however, there was no significant additional effect of PMR on risk factor improvement with the exception of plasma insulin (p<0.001). The authors concluded that the magnitude of the weight loss that could be achieved with PMR at 12 months was within the range observed for pharmacological agents and the range known to lower obesity related risk factors. They attributed the success of PMR to a general preference by participants for structured weight loss plans which promoted improved behavioural compliance, increased nutritional knowledge, more regular meals and less snacking. No reported adverse events were attributed to either the PMR plan or the control.
A comprehensive literature search for the current review carried out in July 2004 identified a further product and randomised trial that was eligible for inclusion. The randomised trial comprised a study of 100 overweight or obese participants (Allison et al. 2003) in which half were randomly assigned to a soy-meal replacement program and half to a 1200kcal exchange diet program. Both groups received dietary counselling and a pamphlet describing good weight loss practices. After 12 weeks, the treatment group lost significantly more weight from the baseline than the control group 7.00kg vs. 2.90kg (p<0.001, ITT analysis). Fat mass was also significantly lower in the treated group -4.3 vs -1.4 (p=0.003). Obesity related risk factors showed reductions in both groups but the magnitude of the effect was variable with large standard errors; LDL-cholesterol reductions were significantly greater at all time periods in the treatment group. Treatment was reported to be well tolerated with no serious side effects. For further details of results, see Meal Replacement in Evidence Table 2 (Allison et al. 2003).
Phentermine hydrochloride: weight loss and co-morbidity risk reduction
The efficacy and safety of phentermine has been assessed primarily in short-term studies of up to 12 weeks duration. The longest study was a randomised, double-blind, placebo-controlled study of 100 subjects undergoing phentermine therapy for 36 weeks (Munro et al. 1968) and reported in a recent systematic review by Glazer (2001). No large-scale, long-term studies of phentermine for weight loss have been performed (Thearle and Aronne 2003).
The systematic review of pharmacotherapy of obesity reported by Glazer in 2001 included a comparative analysis of all randomised, placebo-controlled, double-blind trials of nine months or more duration.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
21
Trials limited to diabetic patients were excluded from this comparative study. Four phentermine studies were reported (Munro 1979; Munro et al. 1968; Steel et al. 1973; Truant et al. 1972; Weintraub et al. 1984), see Table 6a.
Table 6a. Phentermine effectiveness studies
Study Year Dose Duration Weight Loss (kg)
P value†
Munro 1986 30mg 36 weeks 12.2 <0.001 4/4 36 weeks 13.0 <0.001 Weintraub 1984 20 weeks 11.3 <0.01 Truant 1972 16 weeks 8.8 <0.01 Steel 1973 36 weeks 12.0 -
4/4 =4 weeks of phentermine followed by 4 weeks not on phentermine therapy. † compared to placebo
Data from these early studies suggested that phentermine was well tolerated. Adverse events were reported as “minor” with between 3-8% of patients affected. Stimulant effects such as agitation and insomnia were noted. Overall, phentermine was reported as efficacious, with a significantly greater weight loss than the placebo group reported in each study. Weight loss relative to baseline body weight was not reported and the results of the studies were not pooled. When the percentage weight loss in excess of placebo was compared across all of the reported drugs, phentermine appeared to have a weight loss advantage (8.1% of baseline weight lost) over sibutramine (5.0% of baseline weight lost), orlistat (3.4% of baseline weight lost) and diethylpropion (-1.5% of baseline weight – i.e., weight gain). However, the high between-group variation in completion rates and other study variables make these comparisons of doubtful value.
In 2002, Haddock et al., in a meta-analysis of four decades of published randomised trials of pharmacotherapy for obesity, identified nine studies of phentermine published between 1969-1992. The resulting meta-analysis of six eligible randomised studies, comprising 386 participants with a mean follow-up of 13.2 weeks, reported a significantly greater weight loss for phentermine than the placebo (effect size <0.60). There was a mean weight loss of 2.8kg for the placebo group and 6.3kg for the group treated with phentermine. The overall difference in weight loss averaged 3.6 kilograms over the study period, see Table 6b. Most of the patients (>85%) in the reported trials were female.
Table 6b. Phentermine vs. placebo post treatment outcomes, Haddock et al., 2002
Number post test Mean Weight loss (kg) Drug
average dose
(dose range)
Studies
Subjects Duration
(Wks) Placebo
(range)
Phentermine
(range)
Placebo
(range)
Phentermine
(range)
D-P Kg
(range)
Phentermine 27.7mg/d
(15-30mg/d) 6 386 13.2 (2.24) 29.4 (12-74) 32(15-76) 2.8 (1.5-5.2) 6.3(3.6-8.8) 3.6(0.6-6.0)
When the treatment effect size for phentermine was compared to that obtained for other drugs in the study, the effect size for phentermine was second only to sibutramine and higher than either orlistat or diethylpropion. However, all confidence intervals overlapped and there were significant design differences between the studies.
There was no overall effect of treatment length for drugs evaluated in this study, suggesting an early treatment impact for most of the drugs. However, phentermine correlation results for this variable were large and it was suggested that treatment length may influence phentermine’s effect size.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
22
Follow-up outcome analysis, carried out after the formal study completion and treatment had stopped, reported a placebo subtracted weight losses of 2.43kg and 2.37kg for phentermine and sibutramine respectively with unweighted effect sizes of 0.81 and 1.05 respectively. These results were based on a very small number of studies. Overall, the size effect was modest (less than 0.80) and the placebo subtracted weight loss was also modest <4kg.
Phentermine combinations
In 1996, phentermine which was introduced into clinical practice more than 25 years ago, was administered with the newly introduced fenfluramine in the combination known as “Phen-Fen”. Following reports of cardio valvopathy associated with this combination fenfluramide was withdrawn from the market the following year (Rothman and Baumann 2000; Rothman et al. 2000). There was no evidence that phentermine was responsible for these serious adverse events (Hensrud et al. 2003). Studies that included this drug combination have not been included in this review.
In 1999, Bradley et al. examined the use of phentermine and bupropion in combination for weight loss. This randomised, double-blind, placebo-controlled trial recruited 44 obese (>30kg/m2) patients and ran for six months. Patients were randomly assigned in a double-blind fashion to receive either phentermine 30mg + placebo or phentermine 30mg + bupropion SR (sustained release), 150mg twice daily. Both groups followed a 1200-calorie diet which included liquid meal replacement products. After six months, both groups of patients had lost more than 12% of their initial body weight. There were no serious complications or adverse effects noted over the period. Although there was no weight loss advantage in adding bupropion to phentermine, the Beck Depression Index scores improved in the groups taking bupropion. The study investigators concluded that bupropion might be a useful adjunct to phentermine in obese patients subject to mood swings and/or sub-clinical depression.
Diethylpropion: weight loss and co-morbidity risk reduction
Diethylpropion is available as Tenuate 25mg t.i.d. and Tenuate Dospan 75mg extended release taken once a day. The longest eligible study was carried out by Silverstone in 1968 and reported in a systematic review of long-term pharmacotherapy of obesity by Glazer (2001). Two shorter trials were also reported in this comparative review, see Table 7.
Table 7. Diethylpropion effectiveness studies, Glazer et al., 2001
Weight loss kg Study Year
Follow-up
period Drug Placebo
D-P
Kg P value
Silverstone 1968 6 month 7.0 8.7 -1.7 NR 1 year 8.9 10.5 -1.5 NR Deramos 1964 6 months 7.8 1.9 5.9 >0.05 McKay 1973 6 months 11.7 2.5 9.2 <0.01
Data were reported in these trials for a total of 30 patients treated with diethylpropion for six months and five patients treated for 12 months. Results varied considerably for these small studies with one study reporting inferior weight loss for diethylpropion compared to the placebo, one reporting higher, but non-significant, weight loss for diethylpropion compared to the placebo and the other reporting significantly higher weight loss for the diethylpropion compared to the placebo (McKay 1973). Diethylpropion was reported to have few stimulant-related adverse events but weight loss beyond six months was not observed with these patients.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
23
Relatively rapid tolerance to the drug’s anorectic effects was reported. In a comparison of the efficacy of diethylpropion with phentermine, sibutramine and orlistat, diethylpropion was the only drug to record a weight gain. However, the between-study heterogeneity was high and the diethylpropion study comprised only five subjects making the validity of the comparison doubtful and its usefulness limited.
In 2002, Haddock et al., in an analysis of four decades of published randomised trials of pharmacotherapy for obesity, critically reviewed 13 studies of diethylpropion published between 1965-1983 (Haddock et al. 2002), see Comparative Studies in Evidence Table 27. Nine of these studies were employed in a meta-analysis, see Table 8 below.
The majority of patients were female (88%) and most studies used some form of life-style management program. Some of the studies included in the analysis had no weight loss or had weight gain against the placebo as evidenced by the negative values in the drug-placebo value range. Overall, however, diethylpropion produced a greater weight loss than the placebo with an effect size of approximately 0.6. The 95% confidence intervals for diethylpropion overlapped with sibutramine, which was the drug that produced the largest effect (i.e., > 0.80), suggesting that the effect size difference between the drugs was not significantly different.
Table 8. Diethylpropion vs. placebo post treatment outcomes, Haddock et al., 2002
Number post test Mean Weight loss (kg) Drug
(dose) Studies
Duration
(wks) Placebo DP Placebo DP
D-P
(kg)
Diethylpropion 9 17.6(6-52) 21.2(5-32) 18(4-29) 3.5 (-04-10.5) 6.5(1.9-13.1) +3.00
(-1.6-11.5)
DP=diethylpropion, D-P=drug minus placebo
When compared with 12 weeks of phentermine treatment (n=50), diethylpropion (n=49) patients lost 6.3kg against 8.3kg for phentermine (ns) with an effect size of 0.574. An analysis incorporating all drugs suggested that increasing length of treatment did not lead to more weight loss and overall, weight loss attributed to pharmacological intervention for obesity was considered to be modest – i.e., <4.0kg. No data were reported on the effect of diethylpropion of obesity related co-morbidities in this study.
Orlistat: weight loss and co-morbidity risk reduction
A comprehensive literature search for randomised, placebo controlled, double-blind trials or systematic reviews, meta-analyses or HTAs of such studies published between January 1996-July 2004 identified 10 systematic reviews (Arterburn and Hitchcock 2001; Avenell et al. 2004; Foxcroft and Milne 2000; Glazer 2001; Haddock et al. 2002; Hensrud et al. 2003; Heymsfield et al. 2000; Leung et al. 2003; O'Meara et al. 2001; Padwal et al. 2004) and seven additional trials not included in the systematic reviews (Derosa et al. 2003; Halpern et al. 2003; Hanefeld and Sachse 2002; Krempf et al. 2003; Muls et al. 2001; Rissanen et al. 2001; Torgerson et al. 2004), see Table 9 (overleaf). These studies are further summarised in Evidence Tables 3-13, 26 and 27.
There was a good deal of overlap between the systematic reviews and HTAs in terms of the studies reviewed. All limited their reviews to randomised, placebo-controlled, double-blind trials of obese or overweight and obese individuals. The trials comprised mixed risk populations including healthy obese, diabetic and hypertensive patients. Two of the reviews permitted studies of any duration to be included in the review (Hensrud et al. 2003; O'Meara et al. 2001).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
24
Table 9. Summary of publications reporting the effectiveness of orlistat for weight loss in overweight and obese participants
Study Size Study population Studies* Patients Study type Code Duration Health technology assessment, systematic reviews, Cochrane reviews, meta-analyses Avenell 2004 Obese Mixed 8 3885 HTA LT At least 1 year Padwal 2004 Obese Mixed 11 6021 CR LT At least 1 year Hensraud 2003 Obese Mixed 10 NR HTA MT Any Arterburn 2003 Obese mixed 6 1836 SR MT Any Leung 2003 Obese mixed 7 1830 SR MT More than 6 months Glazer 2001 Obese mixed 5 742 SR LT At least 9 months treatment Haddock 2001 Obese mixed 6 NR MA ST 48 weeks O’Meara 2001 Obese Mixed 11 5124 SR MT Any Foxcroft 2000 Obese mixed 3 551 SR LT More than 1 year Heymsfield 2000 Obese mixed 3 675 SR/MA LT 2 year follow-up Randomised, placebo-controlled, double-blind clinical trials Torgeson 2004 Obese diabetic 1 3305 RPCDBT LT 4 years Halpern 2003 Obese1 diabetic 1 365 RPCDBT ST 24 weeks Krempf 2003 Health obese 1 696 RPCDBT LT 10 months Dersosa 2003 Obese hypercholesterolemic 1 99 RPCDBT LT 1 year Rissanen 2001 Healthy obese 1 55 RBCDBT LT 1 year Hanefield 2002 Obese diabetic 1 492 RPCDBT ST 48 weeks Muls 2001 Obese hypercholesterolemic 1 441 RPCDBT ST 24 weeks + 24 weeks
* Published studies, LT=long-tern, ST=short-term, MT=mixed term, RPCDBT=randomised placebo-controlled, double-blind trial, CR=Cochrane review, SR=systematic review, MA=meta-analysis, HTA=health technology assessment.
Most of the reviews were interested in the long-term effects of orlistat in the treatment of obesity and therefore restricted their studies by duration of treatment or follow-up. Most required participants to be treated for at least one year.
The patient populations varied considerably between studies, as did the reporting of results. Most studies reported absolute weight loss or % change from baseline rather than the more clinically useful weighted mean difference between treatment and control and the proportion of patients with ≥ 5% and ≥ 10% weight loss. Later studies intended to report clinically useful endpoints more often than earlier studies. Study results were reported for three patients groups:
• otherwise healthy overweight/obese patients
• patients with type 2 diabetes/glucose intolerance
• patients with hypercholesterolemia.
One study was a Cochrane Review (Padwal et al. 2004) and one was a National Institute for Clinical Effectiveness (NICE) HTA (O'Meara et al. 2001). The three most recent reviews (Avenell et al. 2004; O'Meara et al. 2001; Padwal et al. 2004) assessed the evidence presented in a large number of randomised, placebo-controlled, double-blind trials with total populations of 3,885, 5,124 and 6,021 respectively.
Overall effectiveness of orlistat in obese patients (mixed risk)
The most recent meta-analysis of nine randomised placebo-controlled, double-blind studies of the effect of orlistat for the treatment of obesity was conducted by Avenell et al., (2004) for the NHS R&D HTAprogram in the UK. The results of the meta-analysis of these studies are summarised in Table 10 (overleaf).
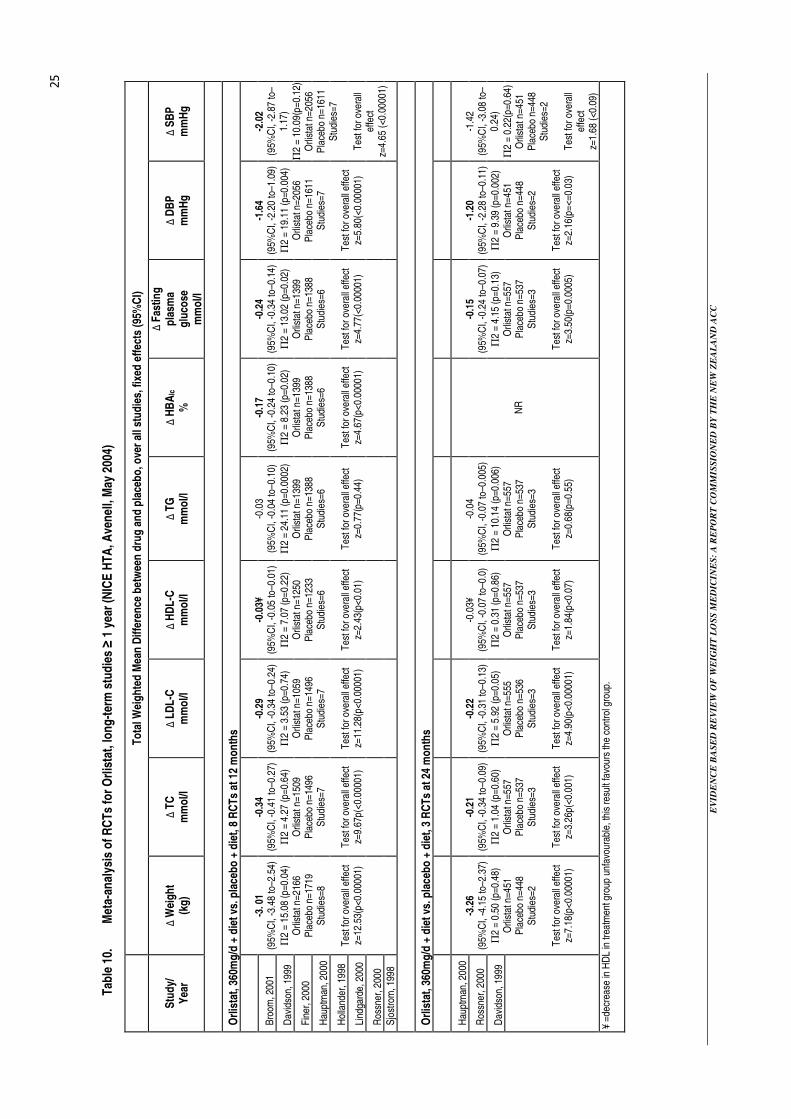
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
25
Tab
le 1
0.
Met
a-an
alys
is o
f R
CT
s fo
r O
rlis
tat,
lon
g-t
erm
stu
die
s ≥
1 y
ear
(NIC
E H
TA
, Ave
nel
l, M
ay 2
004)
T
ota
l Wei
gh
ted
Mea
n D
iffe
ren
ce b
etw
een
dru
g a
nd
pla
ceb
o, o
ver
all s
tud
ies,
fixe
d e
ffec
ts (
95%
CI)
Stu
dy/
Y
ear
∆ W
eig
ht
(kg
) ∆
TC
m
mo
l/l
∆ L
DL
-C
mm
ol/l
∆
HD
L-C
m
mo
l/l
∆ T
G
mm
ol/l
∆
HB
AIc
%
∆ F
astin
g
pla
sma
glu
cose
m
mo
l/l
∆ D
BP
m
mH
g
∆ S
BP
m
mH
g
Orl
ista
t, 3
60m
g/d
+ d
iet v
s. p
lace
bo
+ d
iet,
8 R
CT
s at
12
mo
nth
s
Bro
om, 2
001
Dav
idso
n, 1
999
Fin
er, 2
000
Hau
ptm
an, 2
000
Hol
land
er, 1
998
Lind
gard
e, 2
000
Ros
sner
, 200
0 S
jost
rom
, 199
8
-3
. 01
(95%
CI,
-3.4
8 to
–2.5
4)
Π2
= 15
.08
(p=0
.04)
O
rlist
at n
=216
6 P
lace
bo n
=171
9 S
tudi
es=8
Tes
t for
ove
rall
effe
ct
z=12
.53(
p<0.
0000
1)
-0
.34
(95%
CI,
-0.4
1 to
–0.2
7)
Π2
= 4.
27 (p
=0.6
4)
Orli
stat
n=1
509
Pla
cebo
n=1
496
Stu
dies
=7
T
est f
or o
vera
ll ef
fect
z=
9.67
p(<0
.000
01)
-0
.29
(95%
CI,
-0.3
4 to
–0.2
4)
Π2
= 3.
53 (p
=0.7
4)
Orli
stat
n=1
059
Pla
cebo
n=1
496
Stu
dies
=7
T
est f
or o
vera
ll ef
fect
z=
11.2
8(p<
0.00
001)
-0
.03¥
(9
5%C
I, -0
.05
to–0
.01)
Π
2 =
7.07
(p=0
.22)
O
rlist
at n
=125
0 P
lace
bo n
=123
3 S
tudi
es=6
Tes
t for
ove
rall
effe
ct
z=2.
43(p
<0.0
1)
-0
.03
(95%
CI,
-0.0
4 to
–0.1
0)
Π2
= 24
.11
(p=0
.000
2)
Orli
stat
n=1
399
Pla
cebo
n=1
388
Stu
dies
=6
T
est f
or o
vera
ll ef
fect
z=
0.77
(p=0
.44)
-0
.17
(95%
CI,
-0.2
4 to
–0.1
0)
Π2
= 8.
23 (p
=0.0
2)
Orli
stat
n=1
399
Pla
cebo
n=1
388
Stu
dies
=6
T
est f
or o
vera
ll ef
fect
z=
4.67
(p<0
.000
01)
-0
.24
(95%
CI,
-0.3
4 to
–0.1
4)
Π2
= 13
.02
(p=0
.02)
O
rlist
at n
=139
9 P
lace
bo n
=138
8 S
tudi
es=6
Tes
t for
ove
rall
effe
ct
z=4.
77(<
0.00
001)
-1
.64
(95%
CI,
-2.2
0 to
–1.0
9)
Π2
= 19
.11
(p=0
.004
) O
rlist
at n
=205
6 P
lace
bo n
=161
1 S
tudi
es=7
Tes
t for
ove
rall
effe
ct
z=5.
80(<
0.00
001)
-2
.02
(95%
CI,
-2.8
7 to
–1.
17)
Π2
= 10
.09(
p=0.
12)
Orli
stat
n=2
056
Pla
cebo
n=1
611
Stu
dies
=7
T
est f
or o
vera
ll ef
fect
z=
4.65
(<0.
0000
1)
Orl
ista
t, 3
60m
g/d
+ d
iet v
s. p
lace
bo
+ d
iet,
3 R
CT
s at
24
mo
nth
s
Hau
ptm
an, 2
000
Ros
sner
, 200
0
Dav
idso
n, 1
999
-3
.26
(95%
CI,
-4.1
5 to
–2.3
7)
Π2
= 0.
50 (p
=0.4
8)
Orli
stat
n=4
51
Pla
cebo
n=4
48
Stu
dies
=2
T
est f
or o
vera
ll ef
fect
z=
7.18
(p<0
.000
01)
-0
.21
(95%
CI,
-0.3
4 to
–0.0
9)
Π2
= 1.
04 (p
=0.6
0)
Orli
stat
n=5
57
Pla
cebo
n=5
37
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
3.26
p(<0
.001
)
-0
.22
(95%
CI,
-0.3
1 to
–0.1
3)
Π2
= 5.
92 (p
=0.0
5)
Orli
stat
n=5
55
Pla
cebo
n=5
36
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
4.90
(p<0
.000
01)
-0
.03¥
(9
5%C
I, -0
.07
to–0
.0)
Π2
= 0.
31 (p
=0.8
6)
Orli
stat
n=5
57
Pla
cebo
n=5
37
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
1.84
(p<0
.07)
-0
.04
(95%
CI,
-0.0
7 to
–0.0
05)
Π2
= 10
.14
(p=0
.006
) O
rlist
at n
=557
P
lace
bo n
=537
S
tudi
es=3
Tes
t for
ove
rall
effe
ct
z=0.
68(p
=0.5
5)
N
R
-0
.15
(95%
CI,
-0.2
4 to
–0.0
7)
Π2
= 4.
15 (p
=0.1
3)
Orli
stat
n=5
57
Pla
cebo
n=5
37
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
3.50
(p=0
.000
5)
-1
.20
(95%
CI,
-2.2
8 to
–0.1
1)
Π2
= 9.
39 (p
=0.0
02)
Orli
stat
n=4
51
Pla
cebo
n=4
48
Stu
dies
=2
T
est f
or o
vera
ll ef
fect
z=
2.16
(p=<
=0.0
3)
-1
.42
(95%
CI,
-3.0
8 to
–0.
24)
Π2
= 0.
22(p
=0.6
4)
Orli
stat
n=4
51
Pla
cebo
n=4
48
Stu
dies
=2
T
est f
or o
vera
ll ef
fect
z=
1.68
(<0.
09)
¥ =
decr
ease
in H
DL
in tr
eatm
ent g
roup
unf
avou
rabl
e, th
is re
sult
favo
urs
the
cont
rol g
roup
.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
26
Over a period of 12 months, obese patients treated with orlistat lost on average 3.01 kilograms more than the placebo group. The difference between the two groups increased slightly at 24 months with orlistat treated patients losing on average 3.26 kilograms more than the placebo group; at both time points the difference was significant.
At 12 months, there was also significant and favourable differences reported for the orlistat treated group in terms of total cholesterol, LDL-cholesterol, blood pressure, HbA1c and fasting plasma glucose. A non-significant decrease in triglycerides was reported in favour of the treatment group and an unfavourable decrease in HDL-cholesterol. This pattern was repeated in the assessments undertaken at 24 months with the exception that SBPreduction was less marked and did not reach significance. HbA1c was not reported at 24 months.
A chi squared test for between-study heterogeneity revealed significant heterogeneity in weight loss, triglyceride, HbA1c, fasting plasma glucose and DBP at the 12-month assessment. This heterogeneity persisted between a much smaller number of studies for triglycerides and DBP at 24 months. The high between-study heterogeneity is likely to have arisen as a consequence of the inclusion of some studies with diabetic and hypercholesterolemic participants as well as studies comprising only healthy obese participants. Where possible, these sub-groups have been reported separately in the current review.
Clinical-effectiveness of orlistat in otherwise healthy populations
Three studies (two RCTs and a meta-analysis of three RCTs) reported differences in weight loss between orlistat and the placebo in healthy obese populations. All of the studies reported the difference in mean weight loss or % weight lost from baseline between the treatment and placebo groups. In addition, two studies (Krempf et al. 2003; Torgerson 2004) reported the proportion of patients with clinically important weight loss – i.e., weight loss ≥ 5% and ≥ 10% of their original weight. The reported results are shown in Table 11.
Table 11. Orlistat 360mg/d weight loss in otherwise healthy obese populations
Study Year No of studies
No of subjects
Mean difference in % change
Mean Difference WL (kg)
% with WL≥5%
% with WL≥10%
-2.6* -2.9* NR NR Krempf (RCT) 2003 1 95 -3.5** -3.6** 58 NR
NR -4.4a 73a 41a Torgerson (RCT) 2004 1 3305 NR NR 53b 26b
Heymsfield (MA) 2000 3 675 -2.9* -2.5* NR NR * at one year, intention to treat (ITT) ** 18 months ITT, a difference at one year non-diabetic b difference at four years WL =weight loss
Reporting was variable across the three studies and no study reported all of the relevant weight loss parameters. Participants treated with orlistat lost a larger proportion of their original weight (2.6-2.9% at 12 months, 3.5% at 18 months) than those treated with the placebo, they also lost a greater amount of weight overall. Only two of the studies reported the proportion of patients who lost ≥ 5% of their original weight (Krempf et al. 2003; Torgerson et al. 2004). At one year, 58-73% of treated patients had lost 5% or more of their baseline weight this was a significantly higher proportion than the placebo treated group.
Clinical effectiveness of orlistat in patients with hypercholesterolemia
Two RCTs, not reported in the systematic reviews, examined the effectiveness of orlistat in reducing lipid and blood pressure parameters in patients with hypercholesterolemia, see Table 12 (overleaf).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
27
The approach to the reporting of the results and the number of parameters reported differed in the two studies with one reporting mean placebo minus drug differences, the other reporting differences for each group from the baseline value. However, both studies indicated a significant improvement in LDL-cholesterol, and total cholesterol. There was also evidence of a significant improvement in systolic and diastolic blood pressure. There was no evidence for improvement in the trigylceride and HDL-cholesterol profiles.
Table 12. Orlistat 360mg/d weight loss in patients with hypercholesterolemia, results after one year
Study Year No of
Studies (subjects)
Group Weight loss
LDL-C mg/dl
HDL-C mg/dl
Total-C mg/dl
TG mg/dl
SBP mmHg
DBP mmHg
LMS difference from placebo on % difference from baseline Muls RCT
2001 1 (411) P-O -3.03kg* -10.00 -7.56 -8.37 -0.63 NR NR
Mean % change from baseline for each group 1(23) Placebo -7.6kg** -10.8 +2.4 -12.1 -14.8 -3.0% -2.4%
Derosa RCT 2003
1(25) Orlistat -8.6kg** -19.0 +2.3 -15.0 26.5 -4.6% -4.7% Bold = significant difference from placebo *difference Placebo-Orlistat ** from baseline, LMS = least mean square
Patients with type 2 diabetes or impaired glucose intolerance
A European Medicine Evaluation Agency (EMEA) report of orlistat, comprised a meta-analysis of seven randomised, double blind, placebo-controlled trials of one to two years involving 4,188 diabetic and non-diabetic patients, see Table 13. A higher proportion of diabetic and non-diabetic patients receiving orlistat treatment experienced clinically significant weight loss (≥ 5% or ≥ 10% of baseline weight) than the placebo group. This difference was significant in all comparisons except for a weight loss of ≥ 10% for diabetic patients receiving orlistat vs. placebo. Overall, diabetic patients consistently lost less weight than their non-diabetic counterparts regardless of the treatment they received.
Table 13. Weight loss with orlistat: results of 1 year clinical trials, European Medicine Evaluation Agency.
Non-diabetic Type2 diabetes
Weight loss Orlistat* + diet
N=1561
Placebo+ diet
N=1119 P value
Orlistat* + diet
N=163
Placebo+ diet
N=159 P value
≥5% weight loss 45.3% 23.4% <0.001 30.2% 13.2% <0.001 ≥10% weight loss 20.2% 8.3% <0.001 9.3% 4.4% ns * 360mg/d
Weight loss in diabetic and non-diabetic participants was also reported in a systematic review by O'Meara et al. (2001). In a pooled analysis, non-diabetic participants who had taken orlistat 360mg/d had a mean weight loss difference (placebo minus drug) of 2.9kg compared to 1.8kg for the diabetic group; both groups lost significantly more weight than the placebo group.
A meta-analysis of studies examining glucose tolerance and changes in status from randomisation reported the weight loss achieved with orlistat 360mg/d (Heymsfield et al. 2000), see Table 14.
Table 14. Orlistat 360mg/d in diabetic patients or patients with glucose intolerance
Study Year Studies
(no subjects)
Glucose intolerant
Participants
WL - Change from baseline (kg)
% Progressing
% Improvement
IGT-NGT
Heymsfield Meta-analysis
2000 2 (675) Placebo group Orlistat group
3.79(±4.1) 6.27(±0.41)
7.6 3.0
49 72
WL=weight loss, IGT=impaired glucose tolerance, NGT=normal glucose tolerance, kg=kilogram

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
28
Both placebo and orlistat treated groups exhibited a significant change in weight from their baseline body weight. The treatment group, however, had a much higher total weight change, a higher proportion of patients improving their glucose tolerance and only half as many patients with IGT at baseline progressing to diabetic status.
Two short-term RCTs not otherwise reported in the systematic reviews, examined the effects of orlistat in obese diabetics (Halpern et al. 2003; Hanefeld and Sachse 2002), see Evidence Tables 8 and 9. In a 24-week study of 365 obese, non-insulin dependent diabetic patients (Halpern et al. 2003), the difference in weight loss between the orlistat and placebo group was 1.6kg (least squares mean difference, p=0.0003, ITT analysis) with 30% of orlistat and 17% of placebo patients losing ≥ 5% of their initial body weight (p=0.003). There were also significant differences (least square, mean difference, orlistat minus placebo) in total cholesterol (p=0.0001) and LDL-cholesterol (p=0.0002). HDL-cholesterol levels improved in the placebo group but not in the orlistat group (p=0.038). There was significant improvement in glycaemic control in the orlistat group with significant decreases in HbA1c (p=0.04), fasting plasma glucose (p=0.036) and post prandial glucose (p=0.05).
In a 48 week study of 492 overweight patients with type 2 diabetes treated with sulphonylurea therapy, Hanefeld et al., (2002) reported a weight loss of 4.6kg in the placebo group and 6.3kg in the orlistat group (p=0.07). Significantly more patients achieved a weight loss of ≥ 5% with orlistat than placebo (51.3% vs. 31.6% p=0.0001). There were also significantly higher improvements in HbA1c (p=0.001), fasting glucose (p=0.004), post prandial glucose (p=0.003) and LDL-cholesterol (p<0.05) in the patients treated with orlistat. There were no significant between-group differences in trigylcerides or a reduction in blood pressure. HDL-cholesterol did not change in the orlistat group, the placebo group showed an improvement over its baseline level (p=0.02).
Sibutramine: weight loss and co-morbidity risk reduction
A comprehensive literature search for randomised, placebo controlled, double-blind trials or systematic reviews, meta-analyses or HTAs of such studies, published between January 1996-July 2004 identified 10 systematic reviews (Avenell et al. 2004; Glazer 2001; Haddock et al. 2002; Hensrud 2004; Kim et al. 2003; Leung et al. 2003; McTigue et al. 2003; Nisoli and Carruba 2003; O'Meara et al. 2002; Padwal et al. 2004) and seven additional randomised trials not included in the systematic reviews (Berkowitz et al. 2003; Gokcel et al. 2001; Hauner et al. 2003; Hazenberg 2000; McNulty et al. 2003; Tambascia et al. 2003; Wadden et al. 2000), see Table 15 below. These studies are summarised in Evidence Tables 14-27.
Table 15. Eligible studies reporting the effectiveness of sibutramine
Study Size Study population Studies* Patients Study type Code Duration Health technology assessment, systematic reviews, Cochrane reviews, meta-analyses Avenell 2004 Obese Mixed 5 1455 HTA LT At least 1 year Padwal 2004 Healthy obese 3 929 CR LT At least 1 year Hensraud 2003 Obese Mixed 11 >1924 HTA MT Any Arterburn 2003 Obese mixed 6a 1975 SR MT Any Leung 2003 Obese mixed 10 3150 SR MT More than 6 months Glazer 2001 Obese mixed 1* 160 SR LT At least 9 months treatment Haddock 2001 Obese mixed 4 NR MA ST 8-26 weeks, mean=15.5 O’Meara 2002 Obese Mixed 11 2037 HTA MT Any McTigue 2003 Obese Mixed 7 2815 MA MT 6-12 months Nisoli 2003 Obese Mixed, safety 19 4039 SR MT 8-52 weeks** Kim 2003 Obese mixed 21(31a) 4528 MA MT 8-52 *in period and reported elsewhere, ** 1 study =5.5 hrs, a 21 published studies with 31 separately reported groups Randomised, placebo-controlled, double-blind clinical trials McNulty 2003 Obese diabetic 1 195 RPCDBT LT 12 months Gokcel 2001 Obese diabetic 1 60 RPCDBT ST 6 months Hazenberg 2000 Obese hypertensive 1 127 RPCDBT ST 12 weeks Berkowitz 2003 Healthy Obese adolescents 1 82 RPCDBT LT 12 months

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
29
Table 15. Eligible studies reporting the effectiveness of sibutramine (continued)
Study Size Study population Studies* Patients Study type Code Duration Randomised, placebo-controlled, double-blind clinical trials Tambascia 2003 Healthy obese 1 40 RPCDBT ST 24 weeks Hauner 2004 Healthy obese 1 389 RPCDBT LT 54 weeks Sibutramine and orlistat Wadden 2000 Obese mixed 1 34 RPCDBT ST 16 weeks
ST=short-term, LT=long-term, MT=mixed term, HTA = health technology assessment, CR = Cochrane review, SR = systematic review, MA = meta-analysis, RPCDBT = Randomised placebo controlled, double blind trial.
The patient populations varied considerably between trials as did the study size and duration. Study populations included healthy overweight and obese adults, mixed male and female participants, female only participants, healthy overweight adolescents, obese patients with poorly and well regulated type 2 diabetes, and obese hypertensive patients, patients with dyslipidemia. One study was carried out solely in a primary care setting.
Studies size varied between 34-389 for RCTs and 160-4,528 for systematic reviews, meta-analyses and HTAs. Reporting parameters also varied, some studies reported weight loss in kilograms and % weight loss from baseline weight for placebo and sibutramine, others reported the difference in weight change between the two. The reporting of clinically important weight loss – i.e., weight loss of ≥ 5% was variable.
One systematic review focussed attention on adverse events and side effects reported in 19 RCTs of sibutramine (Nisoli and Carruba 2003), two were NICE Health Technology Reviews (O'Meara et al. 2002) and one was a Cochrane Review (Padwal et al. 2004). The 2003 review of safety and side effects is reported separately in the section on safety and side effects of sibutramine therapy (see page 41). The most recent high quality HTA (Avenell et al. 2004) reported results obtained in a primary care setting.
There was considerable duplication of studies and reporting overlap between the systematic reviews, HTAs and MAs; this overlap and the heterogeneity of the reported parameters made it difficult to summarise and compare these studies.
The most recent HTA (Avenell et al. 2004) reported on five long-term studies including the Sibutramine Trial in Obesity Reduction and Maintenance (STORM), see Table 16 (overleaf). This was one of the most consistently reported studies with weighted mean differences between sibutramine reported for weight loss and risk factors. It was also a multi-therapy study which allowed direct comparison to be made between sibutramine and a number of other weight loss strategies including orlistat, see Table 17 and Table 21.
Over a period of 12 months, obese patients treated with sibutramine lost on average 4.12 kilograms more than the placebo group (p<0.00001). There was also a significant difference in favour of sibutramine treatment reported for HDL-cholesterol (p=0.0004) and triglyceride levels (p=0.004) together with non-significant differences favouring sibutramine for LDL-cholesterol, HbA1c and fasting glucose levels. There were overall differences in diastolic and SBP levels that favoured the placebo group; the difference was significant for DBP (p=0.0005). In both instances, blood pressure levels on average rose during the treatment period. There was no significant between-study heterogeneity at 12 months.
Results were reported for the STORM study at 18 months. Significant differences in favour of treatment were reported for weight loss (3.40kg, p<0.00001), triglycerides (p=0.02) and HDL-cholesterol (p=0.002). Differences in total cholesterol, LDL-cholesterol, HbA1c and fasting glucose levels also favoured treatment but the differences did not reach statistical significance. Blood pressure at 18 months was not reported.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
30
Tab
le 1
6.
Met
a-an
alys
is o
f R
CT
s fo
r S
ibut
ram
ine,
lon
g-t
erm
stu
die
s ≥
1 y
ear
(NIC
E H
TA
, Ave
nel
l May
200
4)
T
ota
l Wei
gh
ted
Mea
n D
iffe
ren
ce b
etw
een
dru
g a
nd
pla
ceb
o, o
ver
all s
tud
ies,
fix
ed e
ffec
ts (
95%
CI)
Stu
dy/
Y
ear
∆ W
eig
ht
(kg
) ∆
TC
m
mo
l/l
∆ L
DL
-C
mm
ol/l
∆
HD
L-C
m
mo
l/l
∆ T
G
mm
ol/l
∆
Hb
A1c
%
∆ F
astin
g
pla
sma
glu
cose
m
mo
l/l
∆ D
BP
m
mH
g
∆ S
BP
m
mH
g
Sib
utr
amin
e +
die
t vs
pla
ceb
o +
die
t, 4
RC
Ts
at 1
2 m
on
ths,
wei
gh
t red
uct
ion
FA
VO
UR
S
Sib
utr
amin
e P
lace
bo
S
ibu
tram
ine
Sib
utr
amin
e S
ibu
tram
ine
Sib
utr
amin
e S
ibu
tram
ine
Pla
ceb
o
Pla
ceb
o
Apf
elba
um, 1
999
McM
ahon
, 200
0
Sm
ith,2
001a
Sm
ith, 2
001b
-4.1
2 (9
5%C
I, -4
.97
to–
3.26
) Π
2 =
5.96
(p=0
.11)
Sib
utra
min
e n=
530
Pla
cebo
n=4
61
Stu
dies
=4
T
est f
or o
vera
ll ef
fect
z=
9.44
(p<0
.000
01)
0.01
(9
5%C
I, -0
.15
to 0
.18)
Π
2 =
0.03
(p=0
.98)
Sib
utra
min
e n=
378
Pla
cebo
n=2
87
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
0.16
(p=0
.87)
-0.0
8 (9
5%C
I, -0
.23
to–0
.07)
Π
2 =
1.36
(p=0
.24)
Sib
utra
min
e n=
212
Pla
cebo
n=1
36
Stu
dies
=2
T
est f
or o
vera
ll ef
fect
z=
1.09
(p=0
.28)
0.10
(9
5%C
I, 0.
04 to
0.1
5)
Π2
= 0.
27 (p
=0.6
0)
Sib
utra
min
e n=
214
Pla
cebo
n=1
37
Stu
dies
=2
T
est f
or o
vera
ll ef
fect
z=
3.57
(p=0
.000
4)
-0.1
6 (9
5%C
I, -0
.26
to–0
.05)
Π
2 =
1.10
(p=0
.78)
Sib
utra
min
e n=
459
Pla
cebo
n=3
65
Stu
dies
=4
T
est f
or o
vera
ll ef
fect
z=
2.87
(p=0
.004
)
-0.0
7†
(95%
CI,
-0.2
5 to
0.1
1)
Π2
= N
A
Sib
utra
min
e n=
265
Pla
cebo
n=7
7 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=0.
76 (p
=0.4
5)
-0.0
5 (9
5%C
I, -0
.26
to 0
.16)
Π
2 =
0.03
(p=0
.98)
Sib
utra
min
e n=
378
Pla
cebo
n=2
87
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
0.47
(p=0
.64)
2.04
‡ (9
5%C
I, 0.
89 to
3.20
) Π
2 =
2.99
(p=0
.22)
Sib
utra
min
e n=
445
Pla
cebo
n=3
75
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
3.47
(p=0
.000
5)
1.
16‡
(95%
CI,
0.60
to2.
39)
Π2
= 0.
12 (p
=0.9
4)
Sib
utra
min
e n=
445
Pla
cebo
n=3
75
Stu
dies
=3
T
est f
or o
vera
ll ef
fect
z=
1.29
(p=0
.20)
Sib
utr
amin
e +
die
t vs.
pla
ceb
o +
die
t, 1
RC
Ts
at 1
2 m
on
ths,
wei
gh
t mai
nte
nan
ce, h
yper
ten
sive
pat
ien
ts
ST
OR
M, 2
000
-3.9
0 (9
5%C
I, -5
.75
to–2
.05)
S
tud
ies=
1
0.04
(9
5%C
I, -0
.29
to0.
37)
Stu
die
s=1
0.08
(9
5%C
I, -0
.01t
o0.1
7)
Stu
die
s=1
0.02
(9
5%C
I,-0.
21to
0.25
) S
tud
ies=
1
-0.1
8 (9
5%C
I,-0.
47to
0.11
) S
tud
ies=
1 N
R
-0.0
8 (9
5%C
I, -0
.49
to 0
.33)
S
tud
ies=
1
3.30
(9
5%C
I, 0.
91-5
.69)
S
tud
ies=
1
1.20
(9
5%C
I, -2
.45
to 4
.85)
S
tud
ies=
1 †
Wei
ght m
aint
enan
ce S
TO
RM
200
0, ‡
incr
ease
d bl
ood
pres
sure
in tr
eatm
ent g
roup
unf
avou
rabl
e.
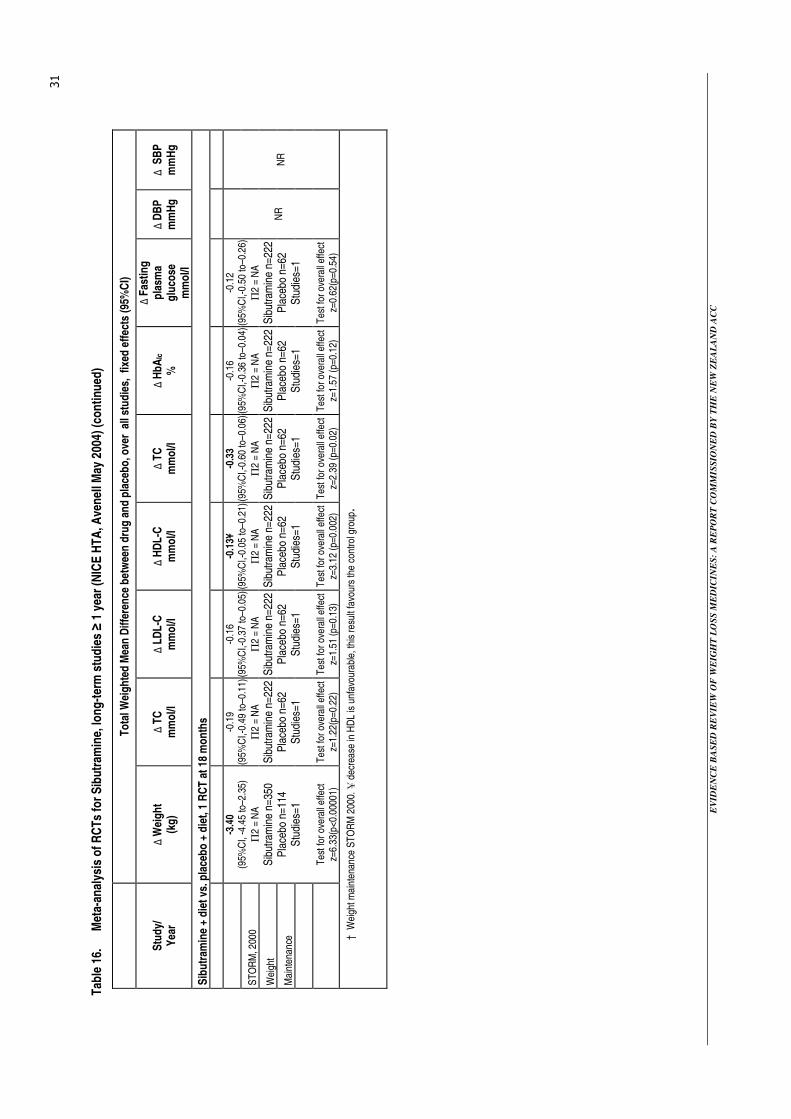
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
31
Tab
le 1
6.
Met
a-an
alys
is o
f R
CT
s fo
r S
ibut
ram
ine,
lon
g-t
erm
stu
die
s ≥
1 y
ear
(NIC
E H
TA
, Ave
nel
l May
200
4) (
con
tinu
ed)
T
ota
l Wei
gh
ted
Mea
n D
iffe
ren
ce b
etw
een
dru
g a
nd
pla
ceb
o, o
ver
all
stu
die
s, f
ixed
eff
ects
(95
%C
I)
Stu
dy/
Y
ear
∆ W
eig
ht
(kg
) ∆
TC
m
mo
l/l
∆ L
DL
-C
mm
ol/l
∆
HD
L-C
m
mo
l/l
∆ T
C
mm
ol/l
∆
Hb
AIc
%
∆ F
astin
g
pla
sma
glu
cose
m
mo
l/l
∆ D
BP
m
mH
g
∆ S
BP
m
mH
g
Sib
utr
amin
e +
die
t vs.
pla
ceb
o +
die
t, 1
RC
T a
t 18
mo
nth
s
ST
OR
M, 2
000
Wei
ght
Mai
nten
ance
-3.4
0 (9
5%C
I, -4
.45
to–2
.35)
Π
2 =
NA
Sib
utra
min
e n=
350
Pla
cebo
n=1
14
Stu
dies
=1
T
est f
or o
vera
ll ef
fect
z=
6.33
(p<0
.000
01)
-0.1
9 (9
5%C
I,-0.
49 to
–0.1
1)
Π2
= N
A
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=1.
22(p
=0.2
2)
-0.1
6 (9
5%C
I,-0.
37 to
–0.0
5)
Π2
= N
A
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=1.
51 (p
=0.1
3)
-0.1
3¥
(95%
CI,-
0.05
to–0
.21)
Π
2 =
NA
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=3.
12 (p
=0.0
02)
-0.3
3 (9
5%C
I,-0.
60 to
–0.0
6)
Π2
= N
A
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=2.
39 (p
=0.0
2)
-0.1
6 (9
5%C
I,-0.
36 to
–0.0
4)
Π2
= N
A
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=1.
57 (p
=0.1
2)
-0.1
2 (9
5%C
I,-0.
50 to
–0.2
6)
Π2
= N
A
Sib
utra
min
e n=
222
Pla
cebo
n=6
2 S
tudi
es=1
Tes
t for
ove
rall
effe
ct
z=0.
62(p
=0.5
4)
N
R
NR
† W
eigh
t mai
nten
ance
ST
OR
M 2
000.
¥ d
ecre
ase
in H
DL
is u
nfav
oura
ble,
this
resu
lt fa
vour
s th
e co
ntro
l gro
up.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
32
Sibutramine therapy for otherwise healthy overweight individuals
Three studies enabled an assessment of the effect of sibutramine in participants without significant obesity related co-morbidities, see Table 17. The mean difference in the percentage weight loss between sibutramine and placebo-treated patients was between 3% and 5% more in sibutramine treated patients (p=<0.05), a similar pattern was apparent for absolute weight loss.
Two of the three studies reported the proportion of patients with ≥ 5 % and ≥ 10% weight loss with difference between the treatment and placebo groups ranging from 21-34% for patients losing ≥ 5% and 15-21% losing ≥ 10% of their initial body weight. In both instances, the difference was significant. These results differ little from the overall picture obtained from the meta-analysis of trials with both low and high risk participants, see Table 17.
Table 17. Studies reporting the effectiveness of sibutramine in otherwise healthy overweight individuals
Study Year No of
studies (subjects)
Duration Dose Mg/d
Mean difference
in % change (s.d.)
Mean difference
Weight loss kg (s.d.)
% Difference WL ≥5%
(s.d.)
% Difference WL ≥10%
(s.d.) Padwal (SR) 2004 3(929) ≥1 years 15-20 4.6(3.8-5.4) a 4.3 (3.6-4.9) a 34(28-40) 15(4-27)
10 -6.1b -5.6b NR NR Tambascia (RCT) 2003 1(40) 24 weeks
- +1.1c +0.9c NR NR Hauner (RCT) 2003 1(389) 54 weeks 15 3.4 3.0(-1.4t o-4.6) a 21.2c 21.8a
a difference from placebo, b difference from baseline in sibutramine group, c difference from placebo. RCT=randomised controlled trial. WL=weight loss. Bold = a significant difference, s.d. = standard deviation.
Sibutramine therapy for patients with type 2 diabetes
Two RCTs reported the effects of sibutramine treatment on weight loss, metabolic control and blood pressure in patients with type 2 diabetes, see Table 18.
Table 18. Studies reporting the effectiveness of sibutramine in individuals with type 2 diabetes
Mean difference placebo-drug, bold = significant difference Study Year
Dose Mg/d
N= ≥5%
WL ≥10% WL
LDL-C mg/dl
HDL-C mg/dl
Total-C mg/dl
TG mg/dl
SBP mmHg
DBP mmHg
Pulse rate
15 46 14 0.0 0.1 0.0 -0.2 4.6 2.8 5.9 McNultya
(RCT) 2003
20 195
65 27 0.1 0.1 0.1 -0.3 -1.3 0.0 5.8 Gokcel 2001 10 60b NR NR 7.6 0.96 20.4 46.4 ns SR SR
a study patients were receiving metformin b females with poorly regulated diabetes. NR=not reported, SR=significant reduction no data reported.
Significantly more patients in the sibutramine group lost ≥ 5% and ≥ 10% of their initial body weight than the control group. Triglycerides were significantly reduced in the treatment group in one study (McNulty et al. 2003), differences between the groups in terms of cholesterol levels were not significant. Blood pressure and pulse rate increased significantly in the treatment group at a dose level of 15mg/d; in a few individuals blood pressure increases were particularly marked. The authors noted that blood pressure increase tended to be offset by weight loss; only 37% of patients who achieved a ≥ 10% weight loss showed a rise of ≥ 5mmHg in SBP.
A sibutramine dose-response effect was observed in one study (McNulty et al. 2003) with doses between 15-20mg/d eliciting increases in the proportion of participants losing 5% and 10% of their body weight.
In an earlier study, Gokcel et al. (2001) reported a 8.7kg greater weight loss for sibutramine after six months of treatment (drug-placebo, p<0.0001). All risk parameters, except SBP, significantly improved with treatment.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
33
A number of other eligible studies (Leung et al. 2003) reported stratification and sub-group analyses that included diabetic patients; all reported significant weight loss differences between sibutramine and placebo treated participants.
Sibutramine therapy for patients with hypertension
The effectiveness of sibutramine in a patient population of mild to moderately obese hypertensive patients was examined in one RCT (Hazenberg 2000). After 12 weeks of treatment with 10mg sibutramine, the treatment groups had lost 2.4% more of their baseline body weight than the placebo group (p=0.002). In addition, 44% of treated patients had lost more than 5% of their baseline body weight compared to 17% in the placebo group (p=0.01). Blood pressure reductions of 4-5mmHg were observed in both groups. Sibutramine patients showed a slightly lower mean improvement than the placebo group; differences between the groups were not significant.
A meta-analysis of 21 randomised, placebo-controlled, double-blind trials to determine the effect of >5mg/d sibutramine on weight loss and blood pressure was carried out by Kim et al., in 2003. The patient population was extremely heterogeneous and co-morbidities of diabetes, hypertension, hyperlipidemia were allowed. Sibutramine had a significant effect on weight loss with an effect size6 of -1.0 (range, -1.17 to -0.84) but increased blood pressure significantly. The net increase in blood pressure attributable to sibutramine was 1.6mmHg and 1.8mmHg for SBP and DBP respectively. Larger increases in blood pressure were observed in heavier and/or younger participants with an effect size of 0.16 (0.08-0.24) and 0.26 (0.18-0.33) respectively. The small increases in blood pressure observed were not considered to be important in normotensive patients or patients with well controlled hypertension being treated in a clinical setting. However, the increase was considered to be clinically important in patients who had borderline or high blood pressure.
Most other studies of sibutramine actually excluded patients with hypertension or cardiovascular disease, others only allowed well-controlled hypertension (Berkowitz et al. 2003; Gokcel et al. 2001; Hauner et al. 2003; McNulty et al. 2003; Padwal et al. 2004).
The use of sibutramine in adolescents
A recent dose ranging, randomised trial of sibutramine and behaviour therapy in obese adolescents aged 13-17 years reported an average weight loss of 7.8kg (s.d.=6.3kg) and 8.5% (s.d.=6.8 %) in an ITT analysis at six months (Berkowitz et al. 2003). The sibutramine treated children lost significantly more weight than the placebo treated group. Medication was reduced in 23 cases and discontinued in 10 cases to manage increases in blood pressure, pulse rate and other symptoms. The investigators concluded that medications for weight loss in children should only be employed in the context of a clinical trial until more extensive safety and efficacy data were available, see Evidence Table 19.
Sibutramine dose ranging studies
The dosage of sibutramine used in most of the studies included in this review varied between 5-30mg/d. In some cases a sub-group analysis was carried out for different dose levels, this was however uncommon. One dose ranging study (Bray et al. 1999), was identified in a systematic review of 10 RCTs by Leung et al., (2003).
6 Effect size = the standardised difference of changes in weight loss from baseline between the treatment and control group. An effect size of >0.80 in this context may be considered to be moderate, and effect size >1.0 may be considered to be large, however, interpretations of effect size importance may vary.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
34
Doses of sibutramine ranging from 1-30mg/d in 1047 obese patients produced a significant dose related weight loss at six months, see Table 19.
Table 19. Sibutramine dose ranging studies. Bray 1999 reported in Leung et al., 2003
% losing at least 5 or 10 % of base weight
Treatment group Dose mg/d
% Weight loss
5%
10%
Discontinuation due to
Adverse events %
SBP Change mmHg
DBP Change mmHg
Pulse Change bpm
Placebo - 1.2 19.5 0.0 8 -0.8 1.7 0.6 1 2.7 25.3 10.5 11 0.3 1.2 0.3 5 3.9 37.4 12.1 5 2.1 2.5 3.3 10 6.1 59.6 17.2 9 2.8 4.2 6.0 15 7.4 67.3 34.7 11 2.7 3.4 6.1 20 8.8 71.9 38.5 13 4.0 5.0 7.0
Sibutramine 24 weeks N=1047
30 9.4 77.2 45.5 18 3.3 4.1 5.3 Bold = significant difference from placebo
In this study, weight loss at four weeks was found to be predicative of weight loss at six months and the proportion of patients withdrawing from the trial because of adverse events increased with increasing sibutramine dose. Blood pressure and heart rate increased with increasing doses of sibutramine up to 20mg/d. This trend was not followed in the 30mg/d group, however, it is not clear if susceptible patients had withdrawn at this stage or if there was an ITT analysis. Treatment related adverse events that resulted in discontinuation were all more common in the 30mg/d group and included hypertension, palpitations, tachycardia, insomnia and dyspepsia.
Comparative drug studies
Seven systematic reviews of pharmacotherapy for obesity between 2001 and 2004 compared the effectiveness of two or more of the drugs being examined in the current review (Arterburn et al. 2004; Avenell et al. 2004; Glazer 2001; Haddock et al. 2002; Hensrud et al. 2003; McTigue et al. 2003; Padwal et al. 2004), see Table 20.
Table 20. Eligible studies comparing two or more review drugs
Study Phentermine Diethylpropion Orlistat Sibutramine Other weight loss therapies reported Avenell, 2004 (National Institute For Clinical Effectiveness) X X 3333 3333
Metformin Selective serotonin reuptake inhibitors (SSRIs) Acarbose VLCDs LCDs Protein sparing modified fast Diet, exercise, behaviour therapy
Hensraud, 2003 (ICSI Technology Assessment Committee)
3333 x 3333 3333
Ephedrine + Caffeine
Arterburn, 2003 McTique, 2004 (US Preventative Services Task Force)
3333 3333 3333 3333
Mazindol Metformin Fluoxetine
Haddock, 2002 (USA)
3333 3333 3333 3333
Dexamphetemine Benzocaine Benzphentermine Dexfenfluramine Fenfluramine Fluoxetine Mazindol Methamphetamine Phendimetrazine Phenylpropanolamine Sertaline
Glazer, 2001 (USA)
3333 3333 3333 3333 Mazindol Fluoxetine (SSRI) Sertaline (SSRI) Fenfluramine Dexfenfluramine
Padwal, 2004 (Cochrane Review, Canada)
X X 3333 3333 None

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
35
Avenell et al., May 2004. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
This extensive and well-reported review included a meta-analysis of all randomised, placebo-controlled, double-blind, efficacy trials of obesity therapy with a follow-up of at least one year. Pharmacological and non-pharmacological interventions were examined. The objective of the review was to identify therapies that achieved weight reduction, risk factor modification or improved clinical outcomes. A summary of the effects of sibutramine and orlistat resulting from a meta-analysis of eligible trials is shown in Table 21. Phentermine and diethylpropion were not included in this review, as they are no longer recommended for anti-obesity therapy in the UK. The reported results for low fat diets (LFDs) are also included as they can include meal replacement programs.
Table 21. Summary of the comparative effectiveness of orlistat, sibutramine and low fat diets that may include meal replacements
Therapy Assessed at Weight change from baseline
(kg)
95% Confidence
Interval Change in risk factors
Sibutramine + diet 18 months -3.40 -4.45 to –2.35 Beneficial except for DBP Orlistat + diet 24 months -3.26 -4.15 to –2.37 Beneficial Low Fat diets* 12 months -5.31 -5.86 to –4.77 Beneficial
* Can include meal replacement programs
Weight loss from baseline was greatest with LFD followed by sibutramine and orlistat. However, treatment duration varied between 12-24 months making it difficult to make a valid comparison of performance. A beneficial change in risk factors was reported for all three therapies with the exception of sibutramine and DBP. A weight loss of 10 kilograms was reported to be associated with a fall in total cholesterol of 0.25mmol/l and a fall in DBP of 3.6mmHg; a 10% weight loss was associated with a fall in SBP of 6.1mmHg.
Hensud, 2003. Pharmacological approaches to weight loss in adults. Institute for Clinical Systems Improvement, Technology Assessment Report, February 2003.
Most of the long-term trials reported in this HTA have been reported elsewhere in the current report. However, the inclusion of some short-term trials of orlistat and sibutramine not reported elsewhere and a comparative summary of changes associated with a wide range of obesity-related risk factors merits its inclusion here. The reported weight change from baseline and the proportions of patients losing clinically significant amounts of weight with the two drugs are shown in Table 22.
Table 22. Summary of short-term weight loss trials of sibutramine and orlistat not otherwise reported in systematic reviews and HTAs.
Therapy Assessed at Weight change from baseline
(kg)
% of participants with a loss of ≥5% of initial body weight
% of participants with a loss of ≥10% of initial body weight
Sibutramine + diet 12-52 weeks -2.4-to -16.6 27-88% 6-76% Orlistat + diet 12 months -3.9 to –10.3 33-69% 10-39% 24 months -5.0 to –7.4 NR NR
Overall, 5-25% of participants failed to complete the pre-randomisation run-in phase of the studies and 9-54% of those randomised failed to complete the study (orlistat, sibutramine and placebo groups). The greatest benefits were reported for patients with co-morbidities such as
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
36
diabetes, these participants experienced less weight loss but important physiological benefits based on Class A and M levels of evidence7.
The type of weight loss programs that led to high proportions of patients achieving clinically important levels of weight reduction (>50% of patients losing ≥ 5% of their initial body weight and >30% of patients losing ≥ 10% of their initial body weight) were examined for predictors of this outcome. High performing programs were characterised by a number of features notably:
• a placebo run-in period that identified individuals that were willing and able to make changes in their nutritional and activity patterns
• regular monitoring in a clinical setting
• exclusion of patients with serious disease, major depression or substance abuse
• information on behaviour modification
• changing nutritional choices
• increasing physical activity.
Padwal et al., August 2003. Long-term pharmacotherapy for obesity and overweight. Cochrane Review.
Eight anti-obesity agents were reviewed in this study but only orlistat and sibutramine studies met the review inclusion criteria. All of the studies included in this review were also reviewed elsewhere but not necessarily in the same review and not reported in the same way.
On average, orlistat treated patients lost 2.7kg (95% CI: 2.3 to 3.1kg) or 2.9% (95% CI: 2.3 to 3.4%) and sibutramine patients 4.3kg (95% CI: 3.6 to 4.9kg) or 4.6% (95% CI: 3.8 to 5.4%) more weight than the placebo group. The number of patients who achieved at least 10% weight loss was 12% (95% CI: 8 to 16%) higher with orlistat than placebo and 15 % (95% CI: 4 to 27%) higher with sibutramine than placebo. Orlistat and sibutramine were reported as being “modestly effective in promoting weight loss” but with “interpretation limited by high attrition rates”.
Glazer, 2001. Long-term pharmacotherapy of obesity, 2000.
This systematic review included a comparative analysis of all of the drugs examined in the current review – i.e., phentermine, diethylpropion, orlistat and sibutramine. In addition, it evaluated some early studies of phentermine and diethylpropion not included in other reviews. The studies identified for review were considered to be too few and too heterogeneous to warrant a meta-analysis of their findings and an average weight loss was reported for each of the drugs across the relevant studies. Trials lasted between 36 to 52 weeks. Three of the four drugs reviewed in the current report, sibutramine, orlistat and phentermine, were considered to have shown weight loss efficacy in long-term trials, see Table 23 (overleaf).
7 Class A = randomised controlled trial, Class M = meta-analysis or systematic review.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
37
Table 23. A comparison of the effectiveness of sibutramine, orlistat, phentermine and diethylpropion (Glazer et al., 2001)
Therapy
Weight loss attributable
to drugs
(kg)
Weight loss attributable
to druga (%)
Sibutramine 4.3 5.0 Orlistat 3.4 3.4 Phentermine 7.9 8.1 Diethylpropion -1.5 -1.5
a weight loss in excess of placebo
Patients receiving phentermine and sibutramine achieved a clinically important weight loss – i.e., weight loss of ≥ 5%, orlistat patients achieved a more modest weight loss while patients treated with diethylpropion on average gained weight. The magnitude of the weight loss was supported by Level I evidence8 for orlistat (2 studies) and sibutramine (1 study) and by Level I/II/III evidence9 for phentermine. With the exception of one short-term study, the level of evidence reported for phentermine was below the standard required for the present report. The authors concluded that while the weight loss achieved with the aid of medication was modest, it was associated with important health and psychological benefits.
Haddock et al., 2002. Pharmacotherapy for obesity: a quantitative analysis of four
decades of published randomised clinical trials
This review considered 15 FDA approved medicines used for weight loss in the USA that included phentermine, diethylpropion, orlistat and sibutramine. The results of the meta-analysis of studies reported between 1960 and 1999 are shown in Table 24.
Table 24. A comparative study of the effectiveness of sibutramine, orlistat, phentermine and diethylpropion (Haddock et al., 2002)
Therapy Dosage Per day
(mg)
Weeks of any treatment
(range)
Number at post-test
drug (range)
Number at post test placebo (range)
Weight loss attributable
to druga kg (range)
Mean effect sizec
Sibutramine 14.0 (10.0-20.0) 14.5(8-26) 27.3(15-52) 26.8(15-49) 3.5(2.4-5.1) 1.0 Orlistat 302.9 (190-360) 47.5(16-76) 236.9(46.7-657) 164.5(46-340) 2.08(0.30-4.2) 0.50 Phentermine 27.5 (15-30) 13.2 (2-24) 32(15-76) 29.4 (12-74) 3.6(0.6-6.0) 0.62 Diethylpropion 75 (75-75) 17.6(6-52) 21.2(5-32) 18(4-29) 3.0(-1.6 b -11.5) 0.60
a Drug-placebo b negative numbers for kilo changes indicate a weight gain. c reported in a figure and without consideration of study design differences, values in table approximate only. 0=no treatment effect.
Sibutramine produced the largest mean effect size in the meta-analysis with a significantly better weight loss than the other drugs. However, the 95% confidence intervals for the sibutramine estimate overlapped with diethylpropion and phentermine suggesting that there were no statistically significant differences between the effect sizes of these three drugs. Post treatment follow-up studies were reported for phentermine and sibutramine, patients treated with both drugs sustained a placebo subtracted weight loss of 2.43kg and 2.37kg and large effect sizes of 0.810 and 1.0510 respectively.
8 Level I evidence = randomised, double blind, placebo-controlled studies.
9 Level II/III evidence = double-blind, placebo-controlled study/blind comparison.
10 Effect sizes >0.80 produced by meta-analysis are considered to be in the “large” effects range.
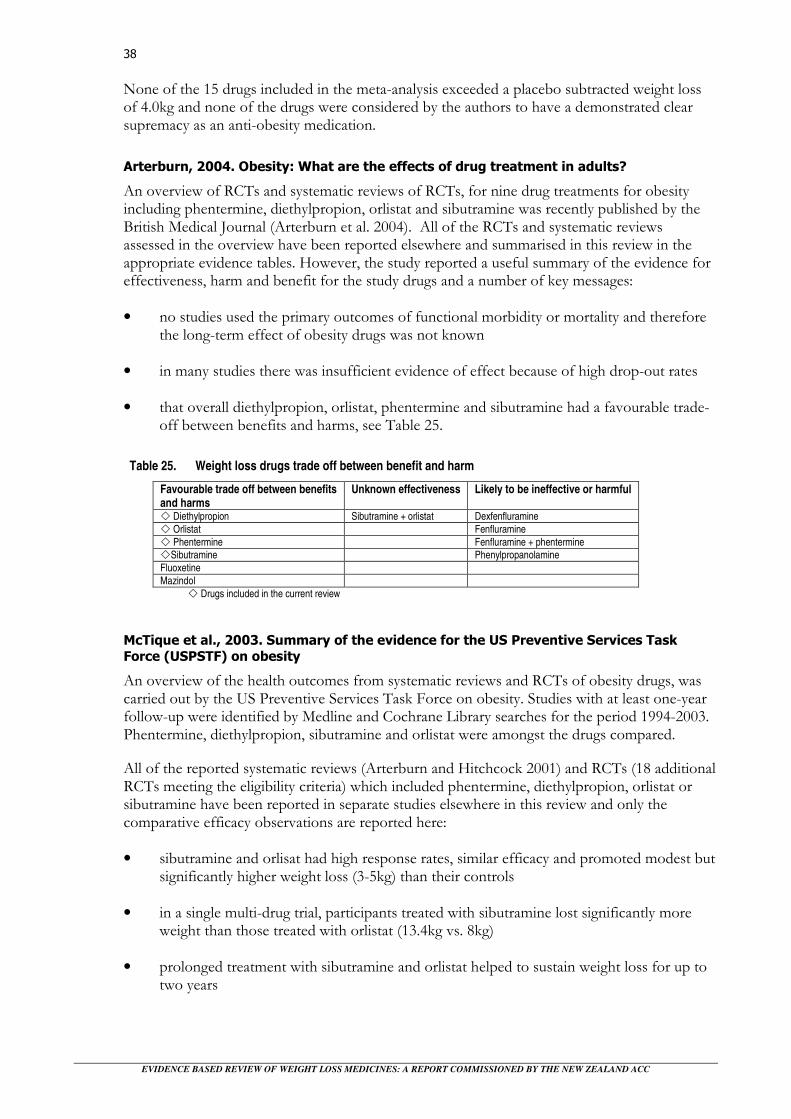
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
38
None of the 15 drugs included in the meta-analysis exceeded a placebo subtracted weight loss of 4.0kg and none of the drugs were considered by the authors to have a demonstrated clear supremacy as an anti-obesity medication.
Arterburn, 2004. Obesity: What are the effects of drug treatment in adults?
An overview of RCTs and systematic reviews of RCTs, for nine drug treatments for obesity including phentermine, diethylpropion, orlistat and sibutramine was recently published by the British Medical Journal (Arterburn et al. 2004). All of the RCTs and systematic reviews assessed in the overview have been reported elsewhere and summarised in this review in the appropriate evidence tables. However, the study reported a useful summary of the evidence for effectiveness, harm and benefit for the study drugs and a number of key messages:
• no studies used the primary outcomes of functional morbidity or mortality and therefore the long-term effect of obesity drugs was not known
• in many studies there was insufficient evidence of effect because of high drop-out rates
• that overall diethylpropion, orlistat, phentermine and sibutramine had a favourable trade-off between benefits and harms, see Table 25.
Table 25. Weight loss drugs trade off between benefit and harm
Favourable trade off between benefits and harms
Unknown effectiveness Likely to be ineffective or harmful
� Diethylpropion Sibutramine + orlistat Dexfenfluramine � Orlistat Fenfluramine � Phentermine Fenfluramine + phentermine �Sibutramine Phenylpropanolamine Fluoxetine Mazindol
� Drugs included in the current review
McTique et al., 2003. Summary of the evidence for the US Preventive Services Task
Force (USPSTF) on obesity
An overview of the health outcomes from systematic reviews and RCTs of obesity drugs, was carried out by the US Preventive Services Task Force on obesity. Studies with at least one-year follow-up were identified by Medline and Cochrane Library searches for the period 1994-2003. Phentermine, diethylpropion, sibutramine and orlistat were amongst the drugs compared.
All of the reported systematic reviews (Arterburn and Hitchcock 2001) and RCTs (18 additional RCTs meeting the eligibility criteria) which included phentermine, diethylpropion, orlistat or sibutramine have been reported in separate studies elsewhere in this review and only the comparative efficacy observations are reported here:
• sibutramine and orlisat had high response rates, similar efficacy and promoted modest but significantly higher weight loss (3-5kg) than their controls
• in a single multi-drug trial, participants treated with sibutramine lost significantly more weight than those treated with orlistat (13.4kg vs. 8kg)
• prolonged treatment with sibutramine and orlistat helped to sustain weight loss for up to two years

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
39
• phentermine had short-term efficacy – i.e., promoted modest weight loss, but was not approved for long-term use
• efficacy of diethylpropion was more limited and variable than the other reported drugs
• modest weight loss improved clinical outcomes
• a high number of patients can achieve a clinically significant (5%-10%) weight loss
• discontinuation of treatment may lead to rapid weight regain.
Combined drug studies
A single randomised trial examining the effectiveness of combined therapy with two weight loss drugs with different modes of action was identified (Wadden et al. 2000).
Wadden et al., 2000. Does adding orlistat to sibutramine induce further weight loss?
The effect of adding orlistat to weight loss therapy with sibutramine was examined in a trial of 34 obese, female volunteers. The participants had already lost weight on sibutramine therapy and were continuing to take the drug at a dosage of 10-15mg/d. At the end of a 16 week combined treatment period, body weight remained essentially unchanged in both the sibutramine + orlistat and the sibutramine + placebo group.
In a sub-group analysis, participants who had lost > 10% of their initial body weight in the previous period of sibutramine treatment gained weight in the extension study – regardless of whether they received orlistat or placebo. Patients who lost < 10 % of their initial body weight in the previous period of sibutramine treatment lost further amounts of weight when orlistat was added to their treatment. These participants lost more weight than those taking sibutramine alone; however, the difference did not reach a significance level of <0.05.
The authors suggested that most obese participants have a limit of 10-15% weight loss with further loss thwarted by a number of regulatory physiological processes including compensatory mechanisms that decrease energy expenditure.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
40

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
41
Safety/Side effects
Safety and side effects of sibutramine therapy
Sibutramine is currently being monitored by the New Zealand Intensive Medication Monitoring Program (IMMP)11.
A systematic review of the benefits and risks associated with the use of sibutramine in the management of obesity was carried out by Nisoli and Carruba (2003), see Table 26.
Table 26. The effect of sibutramine on blood pressure and heart rate; results from 20 studies (Nisoli and Carruba, 2003)
No Subjects
∆∆∆∆SBP (mmHg)
∆∆∆∆DBP (mmHg)
∆∆∆∆Heart rate (beats/min)
No Patients reporting
AEs
No of drop-outs Trial
Dose mg/d
Study Length
P S P S P S P S P S P S Obese subjects Apfelbaum 10 52wk 78 82 NR NR -1.9 +1.5 +1.0 +8.0§ 63 72 5a 2a
Fanghanel 10 24wk 54 55 -4.0 +1.7 -1.5 +0.3 -2.2 +0.1 23 31 10 15 Hanotin 10 12wk 114* 112 +0.6 +0.9 -0.1 +0.4 -0.9 +3.6 90 84 19 10 Cuellar 15 24wk 34 35 NR NR NR NR NR NR 16 23 25 13 Walsh 15 12 wk 9 10 NA NA NA NA NR NR NR NR NR NR Hanotin 5,10,15 12wk 59 177 NR NR NR NR -1.6 +3.2 42 126 12 29 Weintraub 5,20 8wk 20 40 NR NR NR NR NR NR NR NR 1 4 James 10,20 72wk 115 352 -2.4 +1.9 -.05 +3.4 +0.2 +4.6 5 48 58 148 McNulty 10,20 12wk 64 130 -0.2 +1.5 +0.5 +1.9 -0.8 +5.0 NR NR 18 32 Seagle 15,30 8wk 15 29 NR NR NR NR NR NR NR NR NR NR Hanson 30 5.5h 11 11 +5.0 +8.6 +1.4 -4.3 +2.8 +11.24 NA NA NA NA Patients with type 2 diabetes Knoll 10,20 52wk 163 332 -0.5 +0.7 -0.9 +0.8 +0.1 +2.7 NR NR 83 146 Knoll 15 NR 122 114 NR NR NR NR NR NR NR NR 12a 9a
Knoll 15,20 NR 64 131 NR NR NR NR NR NR NR NR 5A 14A
Bray 1.5-30 24wk 148 899 -0.8 +2.5 +1.7 +2.9 +0.6 +4.6 12 101 61 303 Fujioka 5,20 24wk 86 89 +2.4 +3.9 +1.4 +2.6 +0.7 +6.6 68 70 25 29 Gokcel 10 24wk 30 30 NR NR NR NR NR NR NR NR 5 1 Serrano-Rios
15 24wk 65 69 -1.1 +0.5 NR NR NR +2.4 34 42 8 16
Finer 15 12wk 44 47 NR NR NR NR +0.2 +7.5 45 42 4 4 Sibutramine use in children Berkowitz 5,10,15 24wk 39 43 +4.0 +0.1 +0.6 +1.8 2.0 +5.4 NR NR 5 3
a drop-out for adverse events, *comparison with dexfenfluramine § difference significant only at 6 months. P = Placebo, S = sibutramine
In general, the methodological quality of the reported trials was considered to be good. Double blinding, selection criteria and group comparability at baseline was reported for all trials. However, none of the trials included methods to determine if blinding had been successful and relatively few trials reported the use of a priori power calculation to estimate the required sample size.
All trials followed a similar protocol comprising a 1-3 week pre-randomisation run-in period, followed by a randomised assignment to sibutramine or placebo during a treatment period of between 8-52 weeks. In all trials adjunctive therapy comprising diet, exercise and behavioural modification advice was included in varying intensities.
11 IMMP is part of the NZ Pharmacological Vigilance Centre (formerly CARM), Department of Preventive and Social Medicine, Dunedin School of Medicine, University of Otago.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
42
Adverse events
The most commonly reported adverse events of sibutramine were headache, constipation and nausea. Certain adverse events associated with the nervous system including dizziness, dry mouth and insomnia were reported by >5% of patients.
The two most clinically important side effects reported for sibutramine were increased blood pressure and tachycardia; these were generally seen in the first eight weeks of treatment, see Table 26. Heart rate increases between 4-11 beats per min were reported for sibutramine against slightly decreased and increased rates (-2 to +3 beats per min) for the placebo. In a number of instances the difference was significant, however, overall heart rate did not change dramatically during the course of treatment. A similar trend could be discerned in sub-groups with type 2 diabetes with increased heart rates of 3-7 beats per minute for diabetic patients treated with sibutramine and +0.1 to +0.7 beats per minute for the placebo treated diabetic group.
Blood pressure changes
The effect of sibutramine on blood pressure is the consequence of a reducing effect due to its action on body weight and a stimulating effect based on noradrenaline reuptake inhibition. Therapeutic doses of sibutramine have been associated with increased blood pressure in a dose dependent manner (Weintraub et al. 1991), see Table 19.
SBP was higher in all studies in sibutramine patients (median +1.7mmHg, range +0.50 to +8.6) than those who had the placebo (median -0.5mmHg, range -4.00 to +5.00mmHg). Diastolic blood pressure followed the same pattern (sibutramine median =+1.5mmHg, range -4.3 to +3.4, placebo median =0.05mm Hg, range -1.9 to +1.7).
In a trial of obese hypertensive patients (Hazenberg 2000), the mean reduction in supine DBP was numerically but not statistically greater in the placebo group compared with the sibutramine group (5.7mmHg vs. 4.0mmHg; p=0.21). Similar reductions were reported in SBP.
In March 2002, the Italian Ministry of Health approached the EMEA for a reassessment of the benefit/risk ratio of sibutramine after 51 adverse events and two deaths were reported in a period of one year. Reporting incidence by number of fatal cases was calculated at 2.40-2.86 fatal events per 100,000 treatment years, which was lower than the estimated rate for the best available control population. EMEA reaffirmed a positive benefit risk profile for sibutramine based on these data.
Safety and side effects of orlistat therapy
No systematic review of the safety of orlistat and its side effects was identified. However, all of the studies reviewed reported on safety aspects of therapy and the adverse events associated with orlistat treatment.
The main adverse events reported by patients taking orlistat were GI in keeping with the local action of the drug. They included:
• fatty/oily stools
• liquid stools

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
43
• faecal urgency
• faecal incontinence
• flatulence
• lower serum levels of fat-soluble vitamins A, D, E and K1.
These adverse effects were generally mild to moderate and most events occurred early in the course of treatment. Although orlistat treated patients generally had significantly more adverse events than the control group, few serious adverse events were reported.
In the overview of systematic reviews and RCTs by McTigue (2003), it was noted that GI side effects were reported in 22-95% of orlistat users and that in addition to reduced vitamin absorption there was a reduced absorption of contraceptive pills (Arteburn, 2001). Reductions in plasma levels of warfarin and cyclosporine have been reported when co-administered with orlistat. There is insufficient evidence on weight regain and long-term safety for orlistat (Arterburn and Hitchcock 2001).
Safety and side effects of phentermine therapy
No systematic reviews of the safety and side effects of phentermine were identified. However, all efficacy studies reviewed reported on safety aspects of therapy and the adverse events associated with phentermine treatment. Most of the studies published between 1996-2004 were of short duration with small numbers of patients. There is little or no data on the effects of phentermine on obesity related co-morbidities reported in these studies. No serious adverse events were reported in earlier studies of phentermine reported by McTigue et al. (2003).
In 1996, phentermine was administered with the newly introduced fenfluramine in the combination known as “Phen-Fen”. Following reports of cardio valvopathy in patients treated with this combination fenfluramide was withdrawn from the market (Hensrud 2000; Rothman and Baumann 2000).
There was no evidence that phentermine was responsible for the valvopathy (Hensrud et al. 2003) and patients treated with phentermine alone had no reported adverse reaction of this type. Nonetheless, the Medicines Control Agency (MCA) warned that a link between phentermine and heart and lung problems could not be ruled out (Medicines Control Agency Committee on Safety in Medicines, 2004). Phentermine remains available for use in Europe, however, it is not recommended for use by the Royal College of Physicians (Wilding 2004).
Safety and side effects of diethylpropion therapy
No systematic reviews of the safety of diethylpropion and its side effects were identified. However, all of the studies reviewed reported on safety aspects of therapy and any adverse events associated with diethylpropion treatment. Data on the safety of diethylpropion is limited as published studies are generally of short duration (<3 months) in keeping with its conditions of use. Reported side effects include palpitations, tachycardia, elevated blood pressure and arrhythmia together with various adverse reactions associated with CNS stimulation – e.g., nervousness, restlessness, dizziness, euphoria and insomnia. As with amphetamine and other amphetamine derivatives, diethylpropion has a potential to induce dependence.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
44
Case reports of pulmonary hypertension have been reported and the European Medicines Control Agency warned that a link between diethylpropion and heart and lung problems could not be ruled out (Medicines Control Agency Committee on Safety in Medicines, 2004). Although diethylpropion still has a licence for use as an anti-obesity treatment in the UK, its use is no longer recommended for this purpose by the MCA or the Royal College of Physicians (Wilding 2004).
Summary of potential harms of pharmacotherapy intervention
Overall, pharmacotherapy for obesity when carried out as indicated, is reasonably safe. Clinically significant adverse events were reported for sibutramine and orlistat in studies of one to two years; however, the longer-term effects of these drugs is not known. Orlistat has predominantly GI side effects while sibutramine may cause clinically significant rises in blood pressure in some patient groups. Both of these drugs are reported to have clinically significant benefits in the treatment of obesity and its related co-morbidities and a positive trade off between benefits and harm.
Phentermine and diethylpropion are only indicated for short-term therapy. Their adverse events profile were somewhat sketchy in the studies reviewed, possibly because of the limits set on the publications dates for study inclusion for this review12. Phentermine in combination with fenfluramide (“Phen-Fen”) was reported to be responsible for a number of cases of cardio valvopathy and although no cases have been reported in patients taking phentermine alone, it is no longer recommended for use by the Royal College of Physicians in the UK. Diethylpropion has been linked in a number of case reports with pulmonary hypertension and the European MCA have noted that a link between the two cannot be ruled out. Diethylpropion is no longer recommended for the treatment of obesity by the MCA or the UK Royal College of Physicians.
Safety and side effects of meal replacement programs
Meal replacement programs have not been critically evaluated until recently and there are few reports of their safety. In the two studies evaluated in the current review (Allison et al. 2003; Heymsfield et al. 2003), there were few reported adverse events and their impact was limited.
A lack of adverse events reporting in any study patients, including PMR treated diabetics was noted by Heysfield et al., (2003) in a systematic review of six studies examining meal replacement strategies. On the other hand, an unblinded RCT of a novel soy-based meal replacement formula for weight loss in 100 obese volunteers (Allison et al. 2003) reported a large number of adverse events13 including:
• decreased appetite/anorexia
• constipation
• diarrhoea
12 Eligibility criteria limited studies to the period 1996-2004; most studies reporting on these drugs were published much earlier.
13 Assessed by the monitoring of side effects system (MOSES).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
45
• drooling/salivation
• gas/indigestion
• abnormal taste
• lethargy
• excessive sleep
• enuresis/nocturesis
• weight gain
• weight loss.
For five of the events (constipation, gas or indigestion, abnormal or metallic taste, lethargy and weight loss), there was a significantly higher incidence in the meal replacement group. Generally however, treatment was reported to be well tolerated and free of serious side effects by the study authors.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
46
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
47
Practice recommendations and guidelines
National Institute of Health, USA
General guidelines for incorporating weight loss medicines into the overall treatment plan for overweight and obese individuals were published by the National Institute of Health in 2000. It was recommended that:
1. Therapy should be initiated with lifestyle changes (diet and behaviour modification and exercise) and that if these failed to promote a 10% weight loss (or at least 0.5kg/wk) over six months that pharmacotherapy should be considered.
2. Only individuals with a BMI ≥ 30kg/m2 and no obesity related risk factors, or ≥ 27kg/m2 if the patient also has hypertension, dyslipidemia, coronary artery disease, type 2 diabetes or sleep apnoea, should be eligible for treatment.
3. If the patient does not lose at least 2kg in the first month of therapy, the likelihood of response to that medication is low and an adjusted dose, discontinuation of the drug or changing the medication is advised.
4. If significant weight loss occurs with the medication or the initial weight loss is maintained, medication may be continued as long as it remains effective and the side effects tolerable.
In addition, it was suggested that drugs that were limited by the FDA to a maximum period of administration of 12 weeks would be best administered in the setting of a clinical trial.
The National Institute for Clinical Excellence, UK
NICE published best practice guidelines for the use of orlistat and sibutramine in 2001.14
Orlistat
• Orlistat should only be prescribed for obese patients who fulfil the licensing criteria and have lost at least 2.5kg15 by dietary control and increased physical activity in the month prior to treatment.
• When treatment is offered trained practice nurses and dietitians should be available to offer advice, support and counselling on diet, physical exercise and behavioural strategies.
• Continuation of orlistat therapy beyond three months should be supported by evidence of at least 5% body weight loss since the start of treatment.
14 http://www.nice.org.uk.
15 The FDA guidelines do not require prior weight loss using diet and exercise alone and continuation of treatment beyond 3 and 6 months does not require weight loss of 5% and 10% respectively (Ballinger et al 2002).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
48
• Continuation of orlistat therapy beyond six months should be supported by evidence of at least 10% weight loss from the start of treatment.
• Treatment should not usually be continued beyond 12 months and never beyond 24 months16.
Sibutramine
• Sibutramine should be prescribed only as part of an overall treatment plan for the management of obesity for people aged 18-65 years.
• When people are prescribed sibutramine, they should also be offered advice, support and counselling on diet, exercise and behaviour changes.
• It should be prescribed for the management of obesity in people who have a BMI of 30kg/m2 or more, or who have a BMI of 27kg/m2 or more together with significant disease – e.g., type 2 diabetes, high cholesterol.
• Sibutramine should not be prescribed unless the person taking it is monitored for side effects.
• Treatment should only be continued for more than four weeks if patients have lost 2kg in weight and should only continue treatment beyond three months if they have lost at least 5% (5kg for each 100kg) of their body weight from the start of drug treatment.
• Sibutramine should be stopped if patients do not lose weight as described.
• Blood pressure should be checked regularly. Increases in blood pressure may be a reason to stop treatment.
• Sibutramine is not recommended for patients who already have high blood pressure – i.e., 145/90 or above.
• Treatment is not recommended beyond 12 months.17
• There is no evidence to show that prescribing sibutramine with other drugs used to treat obesity is beneficial.
16 The XENDOS trial of orlistat has recently reported on its safety and efficacy at four years.
17 This guidance is to be reviewed in September 2004.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
49
High profile clinical trials
Completed studies
Although there are a number of recently completed trials relating to the management of adult obesity (for a summary see Avenell et al., 2004, Appendix 9), most have little relevance to the ACC claimant population and/or do not involve any of the medications reviewed in the current report. Two high profile clinical trials of the newer weight loss drugs are notable exceptions. Their clinical outcomes have been reported in earlier sections of this review, they are examined individually here to describe the particular circumstances and goals of each trial and to highlight their contribution to this field of study.
STORM: STORM has been widely reported (Astrup and Toubro 2001; Hansen et al. 2001; James et al. 2000; James 2001) and its results incorporated in the recent systematic review by Avenell et al., (2004). This was a randomised double-blind, placebo-controlled, multi-centre European study of sibutramine for the induction and maintenance of weight loss in obese subjects. A total of 605 male and female obese patients were treated for 24 months with sibutramine 10mg/d and a 600kcal deficit diet. If weight regain occurred sibutramine was increased to 20mg/d. At the time of the study, the European Union licence only permitted continuous treatment with sibutramine for up to one year, the STORM study led the US FDA to extend its clearance of sibutramine therapy to two years.
XENDOS: this prospective trial built upon a number of earlier diabetes prevention studies in overweight subjects with IGT (e.g., the STOP-NIDDM, DPP, DPS and TRIPOD studies). Xendos was a randomised, double-blind, placebo-controlled, prospective, four year trial designed to determine the long-term diabetes-preventing and weight reducing effect of orlistat in combination with lifestyle changes in obese patients. Three thousand, three hundred and five obese patients were randomly assigned to orlistat 120mg t.i.d. or placebo. All patients had an energy-reduced diet (reduced by up to 800kcal/day) with 30% fat intake. Patients were instructed to walk 1km a day above their normal level of physical activity.
At four years the orlistat treated patients had lost 5.8kg compared with 3.0kg in the placebo groups (p=<0.001). In IGT patients, the values were 5.7kg and 3.0kg respectively. The cumulative incidence of diabetes over the period of the study was orlistat 6.2 vs. placebo 9.0 (p=0.003) – i.e., 37% reduction of risk of developing diabetes. The orlistat group also experienced significantly greater four year improvements in SBP and DBP, total-LDL and HDL-cholesterol and the LDL/HDL ratio as well as waist circumference, fibrinogen and plasminogen activator inhibitor-1 levels. It is not known if the effect would be greater if orlistat was combined with metformin and/or acarbose (Torgerson 2004; Torgerson et al. 2004).
Childhood obesity
A number of studies of the use of Xenical in children and adolescents are soon to be published – i.e., in the latter months of 2004.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
50
Ongoing trials
Although there are a large number of recently completed and new trials relating to the management of obesity (for a summary see Avenell et al., 2004, Appendix 9), most have little relevance to the ACC claimant population and/or do not involve any of the medications reviewed in the current study. Two ongoing studies are, however, worthy of mention as follows:
SCOUT: a large cardiac outcomes study of sibutramine has been planned in response to a request by the European Committee for Proprietary Medicinal Products (CPMP) for a post approval commitment (Nisoli and Carruba 2003). The Sibutramine Cardiovascular Outcome Trial (SCOUT) is a placebo-controlled, double-blind, global multi-centre study with the objective of comparing the effect of sibutramine and standard care for weight management to that of placebo on the incidence of a composite cardiovascular outcome. It is hoped that the trials will recruit 9,000 subjects ≥ 55 years with a BMI ≥ 27kg/m2 and < 45kg/m2 or BMI ≥ 25kg/m2 and <27kg/m with a waist circumference of ≥ 102cm in males or ≥ 88cm in females, at risk of a cardiovascular event.
The NICHD18 trial of Xenical in children and adolescents with obesity related diseases – this is a phase II clinical trial designed to determine the safety, tolerability and efficacy of orlistat in African American and Caucasian children aged 12-17 years with one or more obesity related co-morbidities (hypertension, hyperlipidemia, hepatic steatosis, insulin resistance, IGT, type II diabetes or sleep apnoea syndrome). The trial is expected to recruit 370 children19.
18 National Institute of Child Health and Human Development. http://clinicalstudies.info.nih.gov/cgi/detail.cgi?A_1998-CH-0111.html.
19 As this report was being written, the FDA announced that it had approved the use of Xenical in children.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
51
Other anti-obesity therapies
A number of additional anti-obesity therapies not considered in the current review have recently been reviewed by NICE (Avenell et al. 2004) and by the US Preventative Services Task Force (McTigue et al. 2003). The full list of therapies considered in each of these reviews is listed in Table 20.
Therapies that may be of particular interest to the ACC include:
• Acarbose
• Metformin
• Very low calorie diets (VLCD)
• LCDs other than those contained meal replacement products
• Mazindol (appetite suppressant)
• Fluoxetine (anti depressant, SSRI).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
52

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
53
Horizon Scan
There are a number of potential future therapies for obesity:
• Leptin: is a hormone released from adipocytes which signals energy availability to the brain. Its deficiency leads to severe obesity and most obese individuals have been found to have elevated leptin levels. However, like most diabetics most obese people are leptin resistant (Brower 2002). There have been a number of phase 2 trials of this agent with disappointing results to date (Thearle and Aronne 2003).
• Axokine: is recombinant human ciliary neurotrophic factor which has been observed to cause weight loss and, in rodents, does not lead to rebound weight gain upon cessation. Early phase trials have indicated that weight loss in excess of placebo is obtained and that weight loss is maintained after treatment has ceased (Brower 2002, Ettinger 2003).
• Topiramate: is an anti-epilepsy drug that has been evaluated for weight loss (Bray et al. 2003, McElroy et al. 2003). A recent dose ranging study has suggested that a clinically significant weight loss and improvement in obesity associated risk factors may be obtained with the therapy but longer and larger studies are required to fully assess its efficacy and safety (Thearle and Aronne 2003).
• Bupropion: is a peptide analogue of the fragment of human growth hormone that causes lipolysis.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
54

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
55
Economic considerations
The direct cost of medication
The cost of treating a single patient for a month at the recommended dose for each of the drugs considered in the current review is shown in Table 27.
Table 27. NZ Drug pricing according to MIMS, 2004†
Drug Proprietary Drug name
Pack
Manufacturer Price NZ$
(per tablet)
Patient Charge
NZ$
Cost per Tablet NZ$
Recommended Daily dosed
Cost‡ per patient per month
NZ$ Phentermine C5controlled drug
Durominea Umine
15mg [30] 30mg [30] 30mg[100]
21.52 24.58 35.90
37.12 42.40 61.93
1.24 1.41 0.62
15mg/d 30mg/d 30mg/d
37.82 43.01 18.91
Diethylpropion Tenuate Dospan b 75mg[100] 94.88 163.67 1.64 75mg/d 50.02 Sibutramine Reductil 10mg[30]
15mg[30] 103.35 119.10
178.28 205.45
5.94 6.83
10mg/d 15/mg/d
181.17 208.32
Orlistat Xenical 120mg[84] 112.00 193.20 2.30 360mg/d 210.45 † Propharma wholesalers may quote lower prices for these drugs. a = 3M New Zealand Ltd. b = Douglas Pharmaceutical Ltd.
d based on the manufacturer’s price. ‡ calculated using patient charges.
The estimated direct drugs costs of a course of treatment are shown in Table 28.
Table 28. The estimated cost of a course of anti-obesity treatment
Maximum permitted Prescribed period
Minimum period Maximum weight loss Drug
Proprietary Drug name
DailyDose
Time Period Cost Time Period Cost Phentermine C5controlled drug
Durominea Umine
15mg 30mg 30mg
3 months 3 months 3 months
$113.46 $129.03
$56.73
3 months† 3 months† 3 months†
$113.46 $129.03
$56.73 Diethylpropion Tenuate Dospan b 75mg 3 months $150.06 3 months† $150.06 Sibutramine Reductil 10mg
15mg
1 yr 2 yr 1 yr 2 yr
$2,174.04 $4,348.08 $2,499.84 $4,999.68
6 months
6 months
$1,087.02
$1,249.92
Orlistat Xenical 360mg 1 yr 2 yr
$2,525.40 $5,050.80
6 months $1,262.70
† not reported but assumed to be maximum continuous prescription period allowed.
The cost of monthly general practitioner (GP) and or nurse consultations, dietary modifications, ancillary monitoring of obesity related co-morbidities, laboratory tests and dietitians services have not been estimated.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
56

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
57
Economic analysis
Obesity is a major risk factor for a number of different health conditions and the economic implications of obesity are therefore significant. Cost of illness studies in the USA suggest that obesity accounts for 5.5-7.0% of national healthcare expenditure (Hensrud et al. 2003).
A comprehensive search of the literature for the present review identified five systematic reviews examining the economics of treating obesity with one or more of the review drugs. Upon inspection these reviews all drew upon data from a relatively small pool of studies20 (Foxcroft and Milne 2000; Lamotte et al. 2002), see Table 29.
Table 29. Studies reporting on the cost or cost effectiveness of sibutramine, orlistat, phentermine and diethylpropion
Systematic review/HTA Drug Reported data from Economic analysis
Avenell 2004 Sibutramine Orlistat
O’Meara 2001 O’Meara 2002 Foxcroft 1999 Foxcroft 2000 Lamotte 2002 BASF Pharma/Knoll 2000
Cost-effectiveness
Hensraud 2003 Orlistat Foxcroft 2000 (rapid review) Lamotte 2002 (HE model)
Cost-effectiveness
O’Meara 2002 Sibutramine BASF Pharma/Knoll 2000 Cost-effectiveness O’Meara 2001 Orlistat Foxcroft 2000 (rapid review) Cost-effectiveness
Glazer 2001 Phentermine Sibutramine Orlistat
Pharmacy chain average retail price Comparative cost
HE=health economics
A single new economic analysis of sibutramine (Warren et al. 2004) was identified in the comprehensive search carried out for this review.
Economic evaluations of orlistat
Two systematic reviews (Foxcroft and Milne 2000; O'Meara et al. 2001) used effectiveness from three RCTs (Davidson 1999; Hollander et al. 1998; Sjostrom et al. 1998) reporting on interventions with 120mg of orlistat three times a day in combination with a hypocaloric diet and compared to placebo plus diet to evaluate the cost-effectiveness of orlistat. The follow-up period was one to two years and outcomes were focussed on patients who lost ≥ 5% of their initial body weight.
The perspective adopted for the economic analyses was that of the health service provider and the cost estimates included:
• the initial consultation
• laboratory tests
20 BASF Pharma Knoll (2000). Unpublished study of economic analysis of Sibutramine reported in O'Meara (2002).

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
58
• outpatient consultations (4 per year)
• drug costs.
The incremental cost per QALY gained was estimated to be £45,888 (range £19,425-£55,391). It was noted that the trial data were not consistent with the EMEA prescription indication for orlistat21 and that the reported costs may differ from those obtained in clinical practice. It was not clear if the estimated cost of £45,888 was considered by the authors of the report to be cost-effective; however, an economic analysis conducted in 2004 (Warren 2004) suggested a cost-effectiveness threshold of approximately £20,000 for another anti-obesity drug. Using this threshold, orlistat would not be a cost-effective option in this group of patients.
A study by Lamotte et al., (2002) reported in European Euros (€) and funded by Roche Pharmaceuticals focussed on obese patients with type 2 diabetes. Using an economic modelling approach, the incremental cost-effectiveness of orlistat for two years in patients with diabetes but free of clinical events and without hypertension or hypercholesterolemia was estimated to be €19,986 22. This was just considered to be cost-effective against a threshold of approximately €20,000 per QALY but lacking robustness. The cost per life year saved decreased in patients with complications such as hypercholesterolemia and AHT, with the cost per life year saved reducing to €3,462 in patients with both hypercholesterolemia and AHT (see Table 30). Sensitivity analysis with inputs assuming that all weight is regained in 2.5 years rather than 5 years, increased the costs from €19,986 to €26,527 for event free patients and from €3,462 to €4,565 for patients with hypercholesterolemia. Treating only patients with hypertension and or hypercholesterolemia was considered to be good value for money, these results were robust under sensitivity analysis.
A study by Glazer (2001) reported only drug costs and direct costs per kg lost or 1% of base weight lost. However, these parameters were also reported for sibutramine and phentermine allowing a snapshot of comparative costs at a single point of time in the USA. The drug costs per kg weight loss were US$433, US$323 and US$91 for orlistat, sibutramine and phentermine respectively. The cost per 1% weight loss was US$433, US$268, US$89 for orlistat, sibutramine and phentermine respectively. These results suggest that orlistat and sibutramine will cost more than phentermine to reduce weight by a similar amount or by a similar proportion of initial body weight. The relative benefits and harms of therapy were not considered.
Economic evaluations of sibutramine
HTAs of sibutramine in 2002 and 2004 (Avenell et al. 2004; O'Meara et al. 2002) did not identify any published economic evaluations of sibutramine. A more recent comprehensive search for the present review (June/July 2004) identified one published economic analysis (Warren et al. 2004) and a simple comparative analysis of direct costs of a number of drugs including sibutramine by Glazer (2001). An unpublished cost utility analysis was submitted to NICE by the manufacturer BASF Pharma/Knoll (2000) and critiqued by O’Meara et al., (2002), see Table 29.
21 European Medicine’s agency prescription indication = loss of >2.5kg by diet in four weeks previous treatment and a loss of ≥ 5% body weight after 12 weeks of treatment.
22 Year 2000 Euros.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
59
A recent economic analysis by Warren et al., (2004) estimated the incremental cost-utility of 12 months of sibutramine therapy at a dose of 10mg/d combined with diet and lifestyle advice compared to diet and lifestyle advice alone in “healthy obese” individuals.
The clinical pathways modelled in this study were consistent with the European licensing for sibutramine23. The overall incremental cost per QALY was estimated at £4,780 based on the results of the sibutramine adiposity therapy (SAT) trial (central Estimate A, Table 29). The marginal gain for the cohort of 1,000 patients in this report was 48.15QALYs (0.048QALYs per patient). Sensitivity analyses showed that this value was sensitive to a number of parameters – particularly the utility associated with weight loss and the frequency of monitoring during and after treatment, see Table 30.
Table 30. Sensitivity analysis around two base estimates of the cost-effectiveness of sibutramine when different utilities are assigned to weight loss
Scenario‡
UK Cost per QALY Central Estimate A
SAT trial £4,780
UK Cost per QALY Central Estimate B SAMSA analysis†
£10,530 WL benefits only £6,341 £19,125 WL and CHD benefits only £5,403 £12,952 WL and diabetes benefits only £5,567 £14,664 Utility per kg WL = lower CI £14,072 £16,682 Utility per kg WL= upper CI £3,001 £5,965 Worst case £20,602 £34,260 Best case £2,950 £5,809 Compliance = 30% £8,605 £34,905 Compliance =50% £7,077 £21,482 Compliance =75% £5,738 £14,271 Adverse events not included £4,769 £10,505 Placebo=no monitoring costs £9,034 £19,899
Estimate A is based on the utility gain per kg of weight lost reported in the SAT trial.
Estimate B is based on the utility gain per kg of weight lost reported in the Samsa analysis.
† used in the NICE report ‡ Estimates for a cohort of 1,000 patients receiving 12 months treatment with
sibutramine.
The effect of differing assumptions and utilities on the estimated cost of sibutramine is also evident in the cost per QALY reported using the different utilities assumed in an economic analysis reported by Samsa et al., (2001), see Table 29. Sensitivity analyses on the central estimates of the cost per QALY for sibutramine vs. placebo based on the utilities reported in the two trials showed large variations in the estimated cost per QALY.
The basic model used in this analysis assumes coronary heart disease (CHD) and diabetes benefits in addition to weight loss and the effect of removing these effects from the model is shown for CHD and diabetes. They both appear to have effects of similar magnitude on the cost per QALY and when the effect of both is removed the cost rises from£4,780 to £6,341 for the estimates based on the SAT utilities and from £10,530 to £19,125 for estimates based on the Samsa utilities.
23 The European licensing for sibutramine only allows continued treatment for “responders” – i.e., patients who lose 2kg after one month and 5% of their initial weight after three months.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
60
Overall, cost was most sensitive to the utility24 attached to each kg of weight lost, however, even at the lower confidence interval of this variable, sibutramine was considered by the authors to be cost-effective by both analyses. Removing the effect of adverse events from the model makes very little difference to either estimate of the cost per QALY.
Only two obesity related co-morbidities, CHD and diabetes, were included in the analysis; however, the authors noted that if all co-morbidities were included in the model the cost per QALY of sibutramine would decrease.
It may be concluded from these analyses that the cost-effectiveness of sibutramine is dependent not only on the amount of weight lost but also on the effect the weight loss has on obesity related co-morbidities. Further calculations were carried out to identify the cost of treating sibutramine-induced side effects that would make treatment no longer a cost-effective option. For Estimate A, it was calculated that side effects that cost £900 per sibutramine patient would be required. Given the fact that sibutramine is well tolerated and that the most common side effects reported are constipation and dry mouth, it was considered unlikely that such a high cost would be incurred in the treatment of side effects.
A “comparative cost efficacy” of sibutramine, orlistat and phentermine reported by Glazer et al., (2001) estimated that the cost per kilogram of weight lost using sibutramine (US$323) was similar to that of orlistat (US$433) and higher than phentermine (US$91). The cost of each 1% weight loss with sibutramine was approximately 40% lower than a comparable weight loss with orlistat ($US268 vs. US$433) and again both of the newer drugs had higher costs than phentermine (US$89). An even weight loss over time was assumed in all calculations.
The BASF Pharma/Knoll model, Table 29, incorporated four weight loss scenarios:
• the effect of weight loss alone
• the effect of weight loss on cardiovascular risk reduction
• the effect of weight loss on diabetes risk reduction
• the combined effects of all three factors.
All weight lost was assumed to be regained after five years. There was some concern that the original estimates made by the company were based on unjustifiably high utility values resulting in an over-estimate of the likely gain in QALY per kg of weight lost.
24 Utilities are calculated from a relationship between weight loss and quality of life.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
61
Table 31. Economic evaluations of orlistat, sibutramine and phentermine
Study Type of study Type of analysis
Costs and assumptions Economic analysis
ORLISTAT Foxcroft 2000
Rapid review Cost-effectivenessd
Cost estimates Patient consultation + lab tests a£118 Monthly cost of orlistat 120mg tds =£45 GP consultation cost=£16 per visit Annual treatment costs=£7344 (1998) Estimated short run gain over a 2-year treatment period =0.016QALYs per year Assumptions Drop-outs treated on average for 3 months Drop-out rate 1yr=27%, 2yr 23% 4 outpatient appointments per year
Base case analysis Cost utility per QALY gained = £45,881 (range £19,452 - £55,391)
Glazer 2001
Systematic review of effectiveness which included a comparison of drug cost
Costs Cost of drug per month =US$119 Cost of drug per year=US$ 1,428 Cost per 1% weight lost=US$ 433 Cost per 1kg weight loss=US$433 Assumptions WMD Drug-placebo %=3.4, kg=3.4
No analysis
ORLISTAT Lamotte 2002
Primary research report Cost effectiveness Markov model
Drug cost
Per patients per year = €881 Incremental costs Drug-placebo
1.Event free diabetes = €1,608
2.Hypercholesterolemia= €1,514
3.AHT= €1,678
4. Hypercholesterolemia+ AHT= = €1,641 Life years gained
1.Event free diabetes = 0.08
2.Hypercholesterolemia= 0.204 3.AHT= 0.227
4. Hypercholesterolemia+ AHT= = 0.474 Assumptions Effectiveness data from Clark 1998 (1.=9.462, 2.=9.401,3.=8.93,4.=8.74) public health perspective Metformin base treatment = 119 euro per patient per year. 4.2% of patients could stop taking oral medication for diabetes and 10% could reduce their medication by approx 25%.
Cost per life year gained (LYG)
1. Event free diabetic=€19,986
2. Hypercholesterolemia =€7,407
3. AHT=€7,388
4. Hypercholesterolemia +AHT=€3.462 Cost-effectiveness Depending upon the risk profile (Lamotte)
1. Event free diabetes = €1,816
2. Hypercholesterolemia= €1,835
3. AHT= = €1,918
4. Hypercholesterolemia+ AHT= = €1,955
Maetzel 2003
Primary research paper Markov state transition model of obese individuals with type 2 diabetes
Cost estimates (2001 values: US$) ATG +Orlistat 120mg t.i.d. for 1 year =$US 19,987 ATG =$US 18,865 MI =$US 19,226 Stroke = $US 32,458 Microvascular disease =$US 1,248 Congestive heart failure= $US 4,842 Cateract =$US 2,163 Main Assumptions Orlistat treatment 120mg t.i.d. for one year All patients received standard type 2 diabetes treatment – i.e., sulphonylureas, metformin or insulin) No diabetes related complication at start of orlistat treatment Simulation continued for 11 years Male patients aged 52 years Reduction in HbA1c values directly translate to a reduction of diabetes related complications Perspective= US healthcare
Incremental cost-effectiveness ratio (CER) $US 8,327 per event free LYG Life expectancy increased by 0.13 years over an 11 year time frame by orlistat Sensitivity analysis for the base case Showed that 95% of CER fell under the threshold of cost effectiveness where the threshold was set at approximately $US 20,000 per event-free LYG. Conclusion Orlistat added to diabetes treatment is cost effective and that the CER is likely to be conservative as no account was taken of lipid parameter reductions or BP changes. CER for females was likely to be higher but still less than $US20,000 Note: shorter period of orlistat have less benefit
SIBUTRAMINE Glazer 2000
Systematic review of effectiveness which included a comparison of drug cost
Costs Cost per month =$116 Cost per year=$1,392 Cost per 1% weight lost=$268 Cost per 1kg weight loss=$323 Assumptions WMD Drug-placebo %=5.0, kg=4.3
No analysis

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
62
Table 31. Economic evaluations of orlistat, sibutramine and phentermine (continued)
Study Type of study Type of analysis
Costs and assumptions Economic analysis
SIBUTRAMINE O’Meara 2002
Systematic review Modellingc
cost utility analysis
BASF Pharma /Knoll UK British £
BASF Pharma /Knoll Cost per QALY through: 1.Weight loss alone=£14,700 2.CHD risk reduction = £32,000 3.Diabetes risk reduction= £58,260 Combined cost per QALY gained from the three influences=£7,860 Main Assumptions 1000 BMI>30kg/m free of co-morbities at the start of the modelling period. All weight is regained in 5 years
O’Meara recalculated the cost per QALY as 1.Weight loss alone=£19,000 2.CHD risk reduction = £42,000 3.Diabetes risk reduction= £77,000 Combined cost per QALY gained from the three influences = £10,500 (£5,700 - £35,200)
Warren 2004
Primary research publication Economic modelling based
Costs Sibutramine 10mg per month=£35, 15mg £39.09 GP visit £13 per month for 1 year Nurse practitioner £7.50 per month for 4 years Marginal costs of 1000 patients receiving sibutramine over placebo I= £305,314 (WL), £298,328 (WL + CHD), £288,776 (WL+ diabetes) Cost saving from avoided CHD events Non-fatal x1 =£2,577, fatal x1 =£2,160, ongoing yearly cost of non-fatal =£6,19. Cost saving from reduced diabetes incidence Annual per capita cost of treating diabetes=£780 Main Assumptions Both arms diet and lifestyle advice Participants =“healthy obese’ WL, CHD and diabetes benefits are assumed 25SAT marginal QALY gain over 1000 patients =48.15 SAMSAT marginal QALY gain over 1000 patients =26.76 SAMSAT analysis used a smaller utility than SAM analysis Cost effectiveness threshold = £20,000 Most common AEs constipation and dry mouth
Incremental cost per QALY Combined WL, CHD , diabetes SAM estimate =£4,780 SAMSAT estimate =£10,530 WL only SAM estimate =£6,341 SAMSAT estimate =£19,125 WL and CHD SAM estimate =£5,403 SAMSAT estimate =£12,952 WL and diabetes only SAM estimate =£5,567 SAMSAT estimate =£14,664
PHENTERMINE Glazer 2000
Costs Cost per month =$60 Cost per year=$720 Cost per 1% weight lost=$89 Cost per 1kg weight loss=$91 Assumptions WMD Drug-placebo %=8.1, kg=7.9
No analysis
a (NHS, Trust 1998) b Based of trials of efficacy by Sjostrom 1998, Davidson 1999, Hollander 1998. c Smith 1994, James 1999. d Sjostrom 1998, Davidson 1999, e Diethylpropion was not considered to be effective in the only long-term trial considered and was not included in the comparison
Aes = adverse events. ATG = adherence to diabetes guidelines for the duration of the model. AHT = arterial hypertension. BP = blood pressure. CER = cost effectiveness ration. CHD = coronary heart disease. LYG = life year gained. MI = myocardial infarction. QALY = quality adjusted life year. SAT= Sibutramine Adiposity Therapy Trial, SAMSAT= the Samsa review trials. WL = weight loss. WMD = weighted mean difference.
O’Meara et al., (2002) recalculated the cost effectiveness estimates. The recalculated estimates were 20-25% higher than the original values, see Table 30, and the combined effects cost per QALY for sibutramine reported as £10,500 with a best case to worst case scenario range between £5,700-£35,200 per QALY. The cost per QALY gained through CHD reduction alone was £42,000, though diabetes incidence reduction alone was£77,000 and from weight loss alone was £19,000. The cost per QALY was again very dependent on the starting utilities and a sensitivity analysis carried out with lower utility gains per kilogram (0.00048 for sibutramine and 0.00058 for placebo), resulted in a cost per QALY of £50,400. Assuming a hypothetical cost- effectiveness threshold of £20,000 (Warren 2004), careful evaluation of the likely utility gain per kilogram of weight lost is required for treatment to be cost-effectiveness.
25 Two estimates were made with one based on the SAT utilities and another on the SAMSAT utilities, sensitivity analyses were computed around both estimates.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
63
Economic evaluations of phentermine
No published economic analyses of phentermine were identified for the period (1996-2004). One study reported drug cost and cost per unit of weight lost comparisons between phentermine, orlistat and sibutramine (Glazer 2001). The estimated annual cost of phentermine was $720, and, on the assumption of a weighted mean difference between phentermine and placebo weight loss of 8.1% and 7.9kg, a cost per 1% weight loss of $89 and 1kg weight loss of $91. The drugs cost and direct cost 1% weight loss for phentermine was much lower than for orlistat or sibutramine.
Economic evaluations of diethylpropion
No published economic analyses or drug cost comparisons were identified over the period (1996-2004) for diethylpropion.
Economic evaluations of meal replacement plans
No published economic analyses or cost comparisons were identified over the period 1996-2004 for meal replacement products or plans.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
64

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
65
Discussion
Criteria for the evaluation of medication for the treatment of obesity
Obesity is the result of long-term mismatches in energy balance where daily intake exceeds daily energy expenditure. It has been suggested (Halpern and Mancini 2003) that a useful medication for obesity treatment should:
1. be effective for body weight reduction and result in improvement of overweight dependent conditions
2. provide evidence that side effects are tolerable and/or transitory
3. not be addictive
4. provide proof of long-term efficacy and safety
5. have a known mechanism of action
6. be reasonably affordable.
None of the weight loss strategies included in the current review fulfil all six requirements. However, all of the pharmacological therapies examined were effective to a greater or lesser degree for body weight reduction and the amelioration of obesity associated co-morbidities and had known mechanisms of action (criteria 1 and 5).
All of the drugs except phentermine and diethylpropion were reported to be unlikely to cause addiction (criterion 3); caution is advised in the administration of phentermine which is an amphetamine and diethylpropion which is an amphetamine derivative. However, all of the drugs except orlistat were reported to have a CNS stimulatory effect and were contraindicated for patients with a history of drug or substance abuse.
All of the pharmacological interventions reported side effects that for the majority of participants appeared to be tolerable and/or transient (criteria 2). All weight loss studies reported high drop-out rates and many reported withdrawals due to drug side effects; however, clinically significant side effects or serious adverse events were rare.
More recent weight loss medications such as orlistat and sibutramine were subject to more intensive reporting of safety and side effects than earlier drugs such as phentermine and diethylpropion. Sibutramine was recently subjected to a reassessment of its safety profile in Europe and a positive risk-benefit for the drug affirmed. Reported side effects for orlistat were generally mild to moderate although a number of serious adverse events possibly related to therapy were reported. Phentermine and diethylpropion are no longer recommended for use for the treatment of obesity by the Royal College of Physicians in the UK.
There was very limited evidence upon which to judge the affordability of treatment (criterion 6). The cost per patient per month was higher for the newer drugs – i.e., orlistat and sibutramine than for phentermine and diethylpropion.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
66
There were conflicting estimates of the cost-effectiveness of orlistat. There is some evidence to suggest that orlistat treatment in patients with a number of co-morbidities is likely to be better value for money than treating otherwise healthy obese patients. Orlistat treatment of patients with type 2 diabetes who were free of clinical events and without hypertension or cholesterolemia was considered to be on the margin of cost effectiveness in one study while in another study, the estimated incremental cost per QALY of orlistat treatment appeared to lie beyond the UK cost-effectiveness threshold.
In contrast the cost-effectiveness of sibutramine, as estimated in two separative evaluations with differing assumptions and utilities, appeared to be within the UK threshold. However, an assumption of lower utility gains per kilo of weight lost for sibutramine resulted in costs that exceeded the threshold for UK cost-effectiveness. If the same cost-effectiveness threshold is assumed for New Zealand and ACC claimants, the circumstances of use for orlistat needs careful assessment if the treatment is to be cost-effective. Sibutramine treatment is likely to be cost-effective for a much wider range of patients, although monitoring for side effects may impact on this assumption.
Expected weight loss and duration of weight loss
Most of the studies reviewed agree that weight loss achieved with pharmacotherapy is modest. For most purposes the mean difference between placebo and each of the drugs in the current review was under 4kg and maintenance of weight loss without continued treatment problematic. However, experience from clinical trials indicates that most weight loss occurs within the first six months of treatment with weight loss at four weeks reported to be predictive of weight loss at six months for sibutramine. Discontinuation of treatment of all of the drugs reviewed is advised if reasonable weight loss does not occur within 12 weeks of starting treatment.
Potential barriers to use
Weight loss targets set by obese people are frequently unrealistic. In most clinical trials, weight loss ranges from 500g – 1kg per week for about six months before stabilising spontaneously. Highly restrictive diets (< 800kcal/d) have not proven to be more effective in the long-term than more modest dietary interventions such as meal replacement. Reduction of 500-1000kcal per day is recommended. The potential barriers to use for phentermine, diethylpropion, orlistat and sibutramine have been reported in detail in an earlier sectionof the review (see drug descriptions pages 9-13). A summary is presented in Appendix I.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
67
Evidence Summary and Conclusions
More than half of the New Zealand adult population is overweight or obese. The problem is increasing in children and adults and is more prevalent in lower socio-economic groups and amongst Maori and Pacific peoples. Given the prevalence of obesity and overweight amongst New Zealanders, a significant proportion of ACC clients are likely to be obese at the time of accident or injury or overweight and in danger of becoming obese as a result of lifestyle changes that may result from injury or accident. There are a number potential consequences for ACC and its clients.
Obesity is associated with a number of co-morbidities including heart disease, diabetes, stroke, high blood pressure and certain cancers. There is also an increased risk of adverse events from anaesthesia in these clients and psychological problems such as clinical depression that may result in job discrimination and other employment difficulties.
Personal care requirements may increase, particularly in relation to attendant care and additional health interventions may be required for co-morbid conditions initiated or exacerbated as a consequence of obesity. These problems may impact on quality of life and significantly interfere with treatment, recovery and rehabilitation.
Overall, obese clients are likely to require additional treatment and/or health related resources compared to clients who are not obese. The potential cost implications of the additional health care and resources that may be associated with untreated obesity are likely to be significant.
Clinical effectiveness and circumstances of use
Weight loss
For all of the drugs examined, most weight loss was achieved within the first six months of treatment and weight loss was not generally maintained when medication was withdrawn. Pharmacologically aided weight loss was generally modest but clinically important because of concomitant reductions in risk levels for obesity-associated co-morbidities. For long-term maintenance of weight loss, the evidence to date suggests that obesity requires sustained therapy in much the same manner as other chronic diseases.
All of the drugs examined were used as adjuncts to diet and or behaviour therapy, physical exercise and lifestyle changes. In most studies, the weight loss drugs were added to a calorie controlled diet or a similar diet plan. There was great heterogeneity between the individual studies in terms of these accompanying non-drug interventions.
All of the appraised studies were evidence level 1a or 1b according to the SIGN criteria.
Phentermine hydrochloride 15mg and 30mg is indicated as a short-term adjunct in a medically monitored comprehensive regimen of weight reduction based on exercise, calorie controlled diet and behaviour modification in patients with a BMI ≥30kg/m2 who have not had a clinical response to an appropriate weight reduction program alone. Patients with obesity related co-morbidities such as sleep apnoea, insulin resistant diabetes mellitus, pre diabetes mellitus or IGT or high cardiovascular risk status, and have a BMI of less than 30kg/m2 may also be considered for treatment.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
68
Phentermine may be prescribed for up to 12 weeks when used as an adjunct in a medically monitored regimen of weight reduction. Failure to achieve a weight reduction of 5% within 12 weeks is an indication for discontinuation. Treatment may be continued beyond 12 weeks provided the patient is monitored for weight loss and medical conditions, and as long as weight loss is maintained.
The effectiveness of phentermine has been examined in a number of studies but most significantly in a comparative meta-analysis of four decades of published randomised trials of anti-obesity treatments. Patients who were prescribed phentermine lost on average 6.3 kilograms with a placebo subtracted average weight loss of 3.6 kilograms (mean follow-up 13.2 weeks). Weight loss was maintained for an unspecified period26 after the formal study completion at a placebo-subtracted average of 2.43 kilograms. When the effect size for phentermine was compared to other anti-obesity drugs, it was second to sibutramine and higher than either orlistat or diethylpropion. However, the confidence intervals for all four drugs overlapped suggesting that there was no significant difference in average weight loss between the medications.
Diethylpropion hydrochloride 75mg is an appetite suppressant with a recommended daily dose of 75mg taken once daily, mid-morning. It is indicated for short-term, intermittent use in a medically monitored regimen of weight reduction based on exercise, calorie restriction and behaviour modification in obese patients with a BMI ≥ 30kg/m2 who have not had an adequate response to an appropriate weight loss program of diet and/or exercise alone. Patients with a BMI of less than 30kg/m2 with co-morbidities including sleep apnoea, insulin resistant diabetes mellitus, pre diabetes mellitus or IGT or high cardiovascular risk status, may also require medical assistance with weight loss. These patients may also be considered for treatment with diethylpropion. It is not recommended for children under 18 years.
Diethylpropion may be prescribed for courses of up to 12 weeks, with intervening periods of one month without treatment. Failure to achieve a weight reduction of 5% within a period of 12 weeks is an indication for discontinuation of treatment.
The effectiveness of diethylpropion was reported in a number of small studies and a single meta-analysis of four decades of randomised trials of weight loss medication. The results varied considerably with both positive and negative placebo-subtracted weight loss – i.e., superior and inferior weight loss when compared to the placebo group. In the most rigorous study, comprising a meta-analysis of nine randomised trials of diethylpropion, effectiveness varied with some studies reporting a weight gain in comparison with the placebo group. Diethylpropion produced a 3.0-kilogram greater weight loss than the placebo with an effect size of 0.57. In a comparison of the effect sizes for diethylpropion, phentermine, orlistat and sibutramine, diethylpropion had a lower reported effectiveness than sibutramine and phentermine but a higher reported effectiveness than orlistat. The weight loss achieved by all of the drugs was similar and the confidence intervals for effect size overlapped.
Orlistat 120mg is indicated as a long-term treatment for obesity, weight-loss maintenance and prevention of weight regain in adults with a BMI ≥30kg/m2. It should be used in conjunction with a low fat calorie controlled diet that is nutritionally balanced and contains approximately 30% of calories from fat distributed over three meals. The diet should be rich in fruit and vegetables. The recommended daily dose is one 120mg capsule three times a day at mealtimes.
26 Mean follow-up assessment for all drugs studies = 17.3 weeks, median=6 weeks after the formal study completion.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
69
The efficacy of orlistat in children27 and adolescents below the age of 18 years has not been established. There are currently no safety and efficacy data beyond two years and the duration of treatment should not extend beyond this period.
As one of two relatively new anti obesity medications with a novel mode of action, orlistat has been subjected to close scrutiny. A large number of relevant studies were identified including 10 systematic reviews and seven additional eligible RCTs. One of the systematic reviews was a Cochrane Review and two were performed as part of an overall HTA commissioned by the NHS R&D HTA Program on behalf of NICE in the UK (Avenell et al. 2004; O'Meara et al. 2001). Some studies examined the effect of treatment with orlistat over a period of up to two years.
Patient populations varied considerably between the studies. For the purposes of this review the results have been summarised for four patient populations (a) all patients, mixed co-morbidity risk (b) healthy obese patients (c) diabetic or glucose intolerant patients and (d) hypercholesterolemic patients.
For all patients (mixed risk groups), the placebo subtracted weight loss was 3.01 kilograms after 12 months treatment and 3.26 kilograms after 24 months of treatment. In studies reporting otherwise healthy patients only the placebo subtracted weight loss was similar with a 2.5 - 2.9 kilogram loss after 12 months and 3.6 kilogram loss at 18 months. Clinically important weight loss – i.e., a weight loss of ≥ 5% was reported at one year for 58-78% of healthy obese patients.
For studies reporting on weight loss in diabetic or glucose intolerant patients, a clinically significant weight loss was reported in 30% of orlistat + diet treated patients against 13% of patients treated with placebo + diet. This was however, somewhat lower than that reported for the non-diabetic group where 45% of patients achieved a clinically important weight loss. In a pooled analysis of diabetic and non-diabetic patients, one HTA reported a placebo subtracted weight loss of 1.8 kilograms and 2.5 kilograms for diabetic and non-diabetic patients respectively.
A meta-analysis of diabetic only patients reported a greater proportion (72%) of patients improving their glucose tolerance with orlistat treatment than the placebo group (49%) and less than half as many patients (3.0% vs. 7.6%) with IGT progressed to diabetic status after treatment with orlistat.
Patients with hypercholesterolemia who had been treated with orlistat were reported to have lost up to 3kg more on average than those treated with placebo with significant improvements reported in LDL- cholesterol and total cholesterol; there was also evidence of a significant reduction in SBP and DBP.
Sibutramine hydrochloride 10mg and 15mg may be used as a long-term treatment and management of obesity including weight loss and weight maintenance in patients with an BMI ≥ 30kg/m2 or ≥ 27kg/m2 in patients who have diabetes, dyslipidaemia or hypertension. It is intended for use when patients have not adequately responded to appropriate weight-reducing therapy such as hypocaloric diet and/or exercise alone – e.g., patients having difficulty in achieving or maintaining ≥ 5% weight loss within three months. The recommended starting dose is 10mg once daily with or without food; in clinical trials sibutramine was given in the morning. If there is less than 2kg weight loss after four weeks, and the 10mg dose is well
27 As this report was being completed, the FDA announced that Xenical® had been approved for use in children.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
70
tolerated, the daily dose may be increased to 15mg. Sibutramine is not currently intended for general use in obese children under 18 years or in elderly patients over 65 years.
Patients who have demonstrated an adequate response – i.e., weight loss of ≥ 2kg within four weeks at a defined dose; usually achieve a maximum weight loss (5%-10% of initial body weight) after six months of continuous treatment with sibutramine. The current data sheet supports treatment for up to one year, however, the evidence of long-term safety and efficacy reported in the STORM study led to the US FDA to extend its clearance of sibutramine therapy to two years. Treatment must be discontinued in patients who have not had an adequate response – i.e., patients whose weight loss stabilises below 5% of initial body weight or whose weight loss within three months of starting treatment is less than 5% of their initial body weight. Treatment should not be continued in patients who regain 3kg or more after previous weight loss with sibutramine.
As one of two relatively new anti-obesity medications, sibutramine has been subjected to close scrutiny and a large number of relevant studies were identified including 10 systematic reviews and seven additional eligible RCTs. Patient populations varied considerably between the trials, as did the reporting of results. Study size varied considerably with RCTs varying between 34-389 participants and systematic reviews, HTAs and meta-analyses between 160-4,528 participants. There was considerable duplication and overlap between the studies and considerable heterogeneity in the reporting of results.
The most recent HTA reported a significant placebo subtracted average weight loss of 4.12 kilograms after 12 months of treatment. The STORM trial reported a placebo subtracted average weight loss of 3.4 kilograms after 18 months of treatment. For patients without significant obesity related co-morbidities a clinically significant weight loss – i.e., ≥ 5% of initial body weight was reported to be 21-34% higher for the sibutramine treated group than the placebo treated group, the placebo subtracted weight loss was between 3.0-4.3 kilograms.
For patients with type 2 diabetes, one study reported a clinically important weight loss difference between the treated groups and the placebo group of 45% at a dose of 15mg/d and 65% at a dose of 20mg/d. In another study, diabetic patients were reported to have lost 8.7 kilograms more weight than the placebo group (p<0.0001) after six months of treatment. In all other studies where stratification and sub-group analyses of diabetic patients were reported, a significant difference between the sibutramine treated diabetic group and the placebo treated diabetic groups was reported.
For patients with mild to moderate hypertension, 12 weeks of treatment with 10mg/d of sibutramine resulted in 44% of patients achieving a clinically important weight loss compared with 17% in the placebo group (p=0.01). In a meta-analysis of 21 RCTs, sibutramine showed a large effect size (-1.0, range –1.17 to -0.84) but increased blood pressure significantly. Most other studies of sibutramine actually excluded patients with hypertension or cardiovascular disease, others only allowed participants with well-controlled hypertension.
The effect of sibutramine varies with dose. The doses of sibutramine used in most studies in this review varied between 5-30mg/d. In some studies, a sub-group analysis was carried out for different dose levels, this was however uncommon. One study specifically designed to examine the effect of dose on treatment response was identified. It included a systematic review of 10 RCTs of 1,047 obese patients treated with doses of sibutramine ranging from 1-30mg/d. A significant dose response effect was reported after six months of treatment with the proportion of patients losing ≥ 5% of their initial rate varying from 25% at a dose of 1mg/d to 77% at a dose of 30mg/d. The proportion of placebo treated participants reporting a weight loss of ≥ 5% of initial body weight was 20%. The proportion of patients who withdrew because of adverse events, increased with increasing sibutramine dose levels. Treatment related adverse

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
71
events were more common in the 30mg/d group. Weight loss at four weeks was found to be predictive of weight loss at six months.
A recent dose ranging trial of sibutramine in obese adolescents between the ages of 13-17 years was also identified. A placebo subtracted average weight loss of 4.6 kilograms (95 % CI, 2.0-7.4, p=0.001) was reported in an ITT analysis after six months of treatment. Medication was reduced or discontinued in a significant number of sibutramine treated patients due to increases in blood pressure, pulse rate and other symptoms. Although sibutramine treatment was successful, the authors cautioned against the use of sibutramine in adolescents outside clinical trials until further efficacy and safety data were available.
Meal replacement plans
Meal replacement strategies are often included in LCDs (diets in the range of 1200-1600kcal/day), which are the cornerstone of modern weight control efforts. However, there are no established definitions of meal replacements plans. In the scientific literature, “meal replacement” is a term generally used to cover beverages, pre-packed, shelf-stable and frozen entities and meal or snack bars. Most of the products are fortified with vitamins and minerals and designed to be consumed in place of one or more regular meals.
Searches for specific meal replacement products such as Complan and Ensure did not identify any published scientific literature relating to these products between 1996-2004. A wider search for meal replacement plans revealed a similar paucity of information.
Meal replacement eating plans have only very recently been critically evaluated for safety and efficacy. The first meta-analysis evaluating RCTs of PMR plans was published in 2003. In this study of 276 potentially relevant publications, 30 were classified as meal replacement studies proper and only six of these studies met the review criteria. A meta-analysis of these studies estimated that the PMR group lost an average of 2.54 kilograms more than the control group after three months of treatment and 2.43 kilograms more than the control group after 12 months of treatment. The proportion of subjects losing ≥ 5% of initial body weight after three months was 33% for the control group and 72% for the PMR group (p<0.001).
After stratification according to diabetic status, non-diabetic completers lost on average 2.79 kilograms more than the control group after three months (p<0.001) and 3.17 kilograms more after 12 months (p=0.002). The diabetic group completers lost on average 2.46 kilograms more than the control at three months and 2.76 kilograms more than the control at 12 months; neither differences reached significance, however, the number of diabetic cases was small and the standard error for the group large.
A single additional product and RCT was identified by the comprehensive search strategy constructed for the current review. One hundred overweight or obese participants were randomly assigned to a novel soy-meal replacement program plus dietary counselling or 1200kcal exchange diet program plus dietary counselling. After 12 weeks, the treatment group lost significantly more weight than the control group (7.00kg vs. 2.90kg, p<0.001, ITT analysis). Fat mass was also significantly lower in the treated group -4.3 vs. -1.4 (p=0.003).
Obesity related risk factors
No data were reported on the effect of phentermine, diethylpropion or meal replacement therapy on obesity-related co-morbidities and their associated risk factors.
Orlistat induced weight loss was accompanied by significant and favourable changes in a number of CHD risk factors including total cholesterol, LDL-cholesterol, blood pressure and

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
72
glucose metabolism. When diabetic and glucose intolerant patients were treated with orlistat, a high proportion of diabetics improved their glucose tolerance and there was a reduction in the proportion of patients with IGT progressing to diabetic status.
Sibutramine treated patients also experienced significant and favourable changes in obesity related risk factors. Significant improvements were reported for HDL-cholesterol and triglyceride levels and non-significant improvements for LDL-Cholesterol, HbA1c and fasting glucose levels. However, blood pressure levels on average rose during treatment with sibutramine and in some instances there was a significant difference in favour of the control group. In patients with type 2 diabetes, blood pressure increases were reported to be offset by weight loss while in hypertensive patients blood pressure reductions were reported with sibutramine patients showing slightly lower mean improvements than the placebo group. Most studies of sibutramine excluded patients with hypertension or cardiovascular disease or only allowed well-controlled hypertension and further data may be required to determine more fully the effect of this drug on patients with raised blood pressure. In dose ranging studies, blood pressure and heart rate increased with increasing dose levels of sibutramine.
Safety and side effects
Overall, the therapies examined in this review were reported to be well tolerated and mostly without significant side effects or serious adverse events. However, safety and side effects have only been reported for highly selected patient populations in closely monitored clinical trials and the results obtained may not apply to typical clinical populations or the ACC claimant population.
Early studies of phentermine suggested that it was well tolerated with only minor adverse events reported for 3-8% of patients. Stimulant effects such as agitation and insomnia were reported. Concerns have been raised about the safety of phentermine and the drug is no longer recommended by the Royal College of Physicians in the UK.
Diethylpropion was reported to have few stimulant adverse events; rapid tolerance to the drugs anorectic effects was reported. Concerns have been raised about the safety of diethylpropion and the drug is no longer recommended by the Royal College of Physicians in the UK.
Orlistat is a locally acting drug and the main adverse events reported were gastrointestinal. Commonly reported side effects were fatty, oily or liquid stools, faecal urgency or incontinence and flatulence, reported in 22-95% of orlistat users. Most GI adverse events occurred early in the course of treatment and may be moderated by dietary adjustments, nevertheless, some of the GI side effects may be unacceptable to some groups of patients. Other undesirable effects attributed to orlistat were lower serum levels of fat-soluble vitamins and interference with the effectiveness of warfarin and cyclosporine treatment.
Sibutramine was generally well tolerated by the study populations at the recommended starting dose of 10mg/d. The most commonly reported side effects were headache, constipation and nausea. Adverse events associated with the CNS including dizziness, dry mouth and insomnia were reported by more than 5% of patients.
The two most clinically significant side effects were increased blood pressure and tachycardia. These symptoms were generally seen in the first eight weeks of treatment and although in some instances the increases reached statistical significance they were not generally considered to be clinically important in otherwise healthy obese patients. Sibutramine is contraindicated in patients with uncontrolled hypertension or cardiovascular disease.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
73
After a number of adverse events and two deaths the benefit/risk ratio of sibutramine was reassessed by the EMEA in 2002; a positive benefit-risk profile for the drug was reaffirmed by the agency after further investigation.
As significant safety and efficacy data for orlistat and sibutramine does not extend beyond two years there is no evidence of their long-term safety.
There are few reports on the safety and side effects of meal replacement plans. In the two studies evaluated in the current review, one (Heymsfield et al. 2003) reported a lack of adverse events in any study patients, including treated diabetics, while the other (Allison et al. 2003) reported a large number of adverse events. In the latter study, which was an unblinded RCT of a novel soy-based meal replacement formula for weight loss, constipation, gas or indigestion, abnormal or metallic taste, lethargy and weight loss were significantly higher in the meal replacement group. Generally however, treatment was reported to be well tolerated and free of serious side effects by the study authors.
Ethnic groups
Some ethnic groups are more at risk of obesity than others and BMI thresholds for obesity are known to vary with ethnicity, as are the co-morbidity risks. However, no studies of the efficacy of phentermine, diethylpropion, orlistat, sibutramine or meal replacement in different ethnic groups were identified. Most of the participants in the reported RCTs were white Caucasian females and the results obtained and the conclusions reached may not be applicable to other ethnic groups. A higher obesity threshold is advised for Polynesians and a lower threshold for Asians.
Economic considerations
Orlistat and sibutramine monthly drug costs are similar at $210.45 and $181.17-$208.32 (depending on dosage) respectively, the cost of phentermine and diethylpropion medication are much lower at $18.91 and $37.82-$43.01 respectively. Additional direct costs including GP visits and laboratory tests are likely to be the same for each of the drugs and are unlikely to exceed the monthly drug costs.
There were no published economic analyses of phentermine or diethylpropion, however, in one comparative study the estimated cost per kilogram of weight lost for phentermine, orlistat and sibutramine was US$91, US$433 and US$323 respectively. This is roughly in line with the differential daily NZ direct cost of the drugs.
Economic evaluations of orlistat from two systematic reviews suggested that the overall cost of orlistat therapy is high with the incremental cost per QALY gained estimated to be £45,888 (range £19,425 - £55,391) in one study and approximately £31,978 in another. Overall, treating healthy obese patients was much less cost-effective than treating patients with obesity related co-morbidities. Treating only patients with obesity related hypertension and/or hypercholesterolemia was considered to be good value for money and the results of the analysis robust under sensitivity analysis.
Only one published economic analysis of sibutramine was identified. Two central estimates of cost per QALY gained were reported arising from differing assumptions and utilities associated with weight loss.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
74
The costs per QALY arising from the two calculations were £4,780 and £10,530. However, the basic economic model used in both analyses assumed benefits additional to weight loss arising from associated improved risk profiles in patients with co-morbidities. The costs per QALY of weight loss alone were £6,341 and £19,125 and worst-case scenarios estimated at £20,602 and £34,260 respectively in the two models. Sibutramine was considered to be cost-effective even at the highest cost per QALY obtained in this analysis and it was noted that if all co-morbidities were included in the model, the cost per QALY would decrease.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
75
Evidence Tables

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
76
Evi
den
ce T
able
1.
Mea
l rep
lace
men
t, H
eym
sfie
ld, 2
003
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
ies
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
Wt-
loss
dif§
s.
e.
p v
alue
Val
idity
/App
licab
ility
S
afet
y C
oncl
usi
ons
C
omm
ents
Hey
msf
ield
, 20
03
Stu
dy d
esig
n
Met
a-an
alys
is o
f six
R
CT
s O
bje
ctiv
e T
o as
sess
the
safe
ty a
nd
effe
ctiv
enes
s of
m
eal r
epla
cem
ent
ther
apy
S
tud
ies
N=6
D
itchu
neit
et a
l.,
1999
**
Fle
tche
r-M
ors
et a
l.,
2000
**
Rot
hack
er 2
001
Yip
200
1 H
ensr
ud 2
001
Ash
ley
2001
A
hren
s 20
00
Par
ticip
ants
N=4
87
Mal
e= 2
5%
Fem
ale:
=75
%,
Mea
n ag
e 46
.1 y
ears
M
ean
BM
I at b
asel
ine
=31
Dia
betic
N=1
19 (2
4%)
Non
-dia
betic
N
=368
(76%
) In
clus
ion
R
ando
mis
ed tr
ial
com
parin
g P
MR
to a
tra
ditio
nal L
CD
S
tudy
dur
atio
n >
3mon
ths
Sub
ject
s >1
8 ye
ars
Exc
lusi
on
Stu
dies
with
sel
f re
porte
d da
ta.
Du
ratio
n
3-51
mon
ths,
med
ian
12
mon
ths
Loc
atio
n
US
A (n
=5)
Ger
man
y (n
=1)
No
te: 2
mea
ls a
day
w
ere
repl
aced
in th
e ex
posu
re d
urin
g th
e w
eigh
t los
s ph
ase,
one
m
eal a
day
dur
ing
the
wei
ght m
aint
enan
ce
phas
e.
Exp
osu
re (P
MR
) P
MR
– i.
e., o
ne o
r m
ore
mea
ls re
plac
ed
by a
com
mer
cial
ly
avai
labl
e, c
alor
ie-
redu
ced
prod
uct(s
) th
at a
re fo
rtifie
d w
ith
vita
min
s an
d m
iner
als
and
at le
ast o
ne d
aily
m
eal c
onsi
stin
g of
re
gula
r foo
ds, a
ctin
g as
a L
CD
and
pr
ovid
ing
>800
<=16
000k
cal/d
ay
Co
mp
aris
on (R
CD
) T
radi
tiona
l LC
D p
lan
(LC
D) w
ith th
e sa
me
calo
ric c
ompo
sitio
n as
th
e ex
posu
re.
Res
ults
at 3
mon
ths
Met
a-an
alys
is fi
xed
effe
cts
Met
a-an
alys
is ra
ndom
effe
cts
Poo
led
anal
ysis
of c
ompl
eter
s P
oole
d an
alys
is L
OC
F
Poo
led
anal
ysis
MI
>=5%
wei
ght l
oss
RC
D=3
4%,
PM
R=7
2%
Non
-dia
betic
P
oole
d an
alys
is o
f com
plet
ers
Poo
led
anal
ysis
LO
CF
P
oole
d an
alys
is M
I D
iabe
tic
Poo
led
anal
ysis
of c
ompl
eter
s P
oole
d an
alys
is L
OC
F
Poo
led
anal
ysis
MI
Res
ults
at 1
yea
r (R
CD
N=4
, PM
R
N=5
) M
eta-
anal
ysis
fixe
d ef
fect
s M
eta-
anal
ysis
rand
om e
ffect
s P
oole
d an
alys
is o
f com
plet
ers
Poo
led
anal
ysis
LO
CF
P
oole
d an
alys
is M
I >=
5% w
eigh
t los
s R
CD
=33%
P
MR
=74%
N
on-d
iabe
tic
Poo
led
anal
ysis
of c
ompl
eter
s P
oole
d an
alys
is L
OC
F
Poo
led
anal
ysis
MI
Dia
betic
P
oole
d an
alys
is o
f com
plet
ers
Poo
led
anal
ysis
LO
CF
P
oole
d an
alys
is M
I R
isk
fact
ors
⊥ ⊥⊥⊥
Glu
cose
(mg/
dl)
SB
P (m
mH
g)
DB
P (m
mH
g)
Insu
lin (Φ
U/m
l) C
hole
ster
ol (m
mol
/l)
HD
L (m
mol
/l)
LDL
(mm
ol/l)
T
G (m
mol
/l)
3.
01
2.60
2.
54
2.39
2.
23
2.79
2.
67
2.47
2.
46
2.62
1.
67
3.39
2.
43
2.63
2.
86
1.62
3.
17
3.56
2.
92
2.76
1.
52
2.86
3
moW
L p
= 0.
028
<0.0
01
ns
ns
ns
ns
0.03
9 0.
014
0.
33
0.96
0.
37
0.35
0.
35
0.37
0.
35
0.33
1.
84
1.89
1.
73
0.72
1.
65
0.88
0.
46
0.98
0.
99
0.50
0.
66
2.00
1.
89
2.53
6
moW
L p
= 0.
009
<0.0
01
ns
ns
<0.0
01
ns
0.00
1 0.
011
<0
.001
0.
006
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
ns
ns
ns
<0.0
01
0.14
2 0.
003
<0.0
01
0.11
9 <0
.001
0.
002
<0.0
01
<0.0
01
ns
ns
ns
PM
R-R
CD
p= ns
ns
ns
<0
.001
ns
ns
ns
ns
Bas
elin
e co
mpa
riso
n
PM
R a
nd R
CD
diff
ered
si
gnifi
cant
ly in
one
fact
or –
base
line
gluc
ose.
D
rop
-ou
t rat
e 3
mon
ths
(ns)
E
xpos
ure
= 16
%
Con
trol=
19%
1
year
(p<0
.001
) E
xpos
ure=
47%
C
ontro
l=64
%
Non
e of
the
drop
-out
repo
rted
prog
ram
or p
rodu
ct-r
elat
ed
adve
rse
even
ts.
Het
ero
gen
eity
E
stim
ates
of w
eigh
t los
s an
d ef
fect
iven
ess
of b
oth
grou
ps
from
the
indi
vidu
al s
tudi
es
wer
e he
tero
gene
ous
(p=<
0.00
1).
Qu
ality
T
he q
ualit
y of
all
stud
ies
as
asse
ssed
by
the
Jada
d cr
iteria
=
mod
erat
e.
Blin
ding
was
not
pos
sibl
e du
e to
the
natu
re o
f the
in
terv
entio
ns.
Blin
ding
of t
he o
utco
me
asse
ssor
was
not
des
crib
ed.
Ran
dom
isat
ions
des
crip
tion
was
incl
uded
in a
ll pr
otoc
ols
and
all s
tudi
es p
rovi
ded
deta
ils
of d
ropo
uts.
With
in th
e co
ntex
t of a
clin
ical
tri
al, P
MR
app
ears
to p
rom
ote
sign
ifica
ntly
gre
ater
wei
ght l
oss
than
a c
orre
spon
ding
RC
D p
lan.
T
he o
vera
ll m
agni
tude
of t
he
wei
ght l
oss
in a
poo
led
anal
ysis
at
1 ye
ar w
as in
the
rang
e re
porte
d in
som
e ph
arm
acol
ogic
al w
eigh
t co
ntro
l stu
dies
(Gla
ser 2
000)
and
is
at t
he le
vel k
now
n to
low
er
dise
ase
risk.
F
our s
tudi
es e
nrol
led
subj
ects
w
ith n
o co
-mor
bidi
ties,
the
othe
r 2
wer
e de
sign
ed fo
r pat
ient
s w
ith
type
2 d
iabe
tes.
A
ll si
x st
udie
s re
sulte
d in
si
gnifi
cant
wei
ght l
oss
from
ba
selin
e in
bot
h gr
oups
. P
MR
gro
ups
lost
sig
nific
antly
m
ore
wei
ght t
han
the
cont
rol
grou
p.
No
te: %
wei
ght l
oss
at 3
mon
ths
RC
D=4
%, P
MR
=7%
. % w
eigh
t lo
ss a
t 1 y
ear R
CD
. 3-7
%,
PM
R.7
-8%
T
he fi
rst s
yste
mat
ic e
valu
atio
n of
R
CT
s ev
alua
ting
PM
R p
lans
for
wei
ght m
anag
emen
t sug
gest
s th
at
they
can
saf
ely
and
effe
ctiv
ely
prod
uce
sign
ifica
nt w
eigh
t los
s.
The
re w
as n
o su
ppor
t for
pu
blic
atio
n bi
as.
*One
tria
l >=3
0 ye
ars
** s
ame
stud
y po
pula
tions
ns=
no
sign
ifica
nt d
iffer
ence
bet
wee
n gr
oups
§ P
MR
= p
artia
l mea
l rep
lace
men
t, R
CD
= re
duce
d ca
lorie
die
t. N
ote:
All
risk
fact
or v
alue
s fo
r bo
th g
roup
s w
ere
sign
ifica
ntly
diff
eren
t fro
m b
asel
ine
valu
es a
t 3 a
nd 6
mon
ths,
3m
oWL=
3 m
onth
wei
ght l
oss,
6m
oWL=
6 m
onth
wei
ght l
oss.
MI=
mul
tiple
impa
tatio
n, L
OC
F=l
ast o
bser
vatio
n ca
rrie
d fo
rwar
d.
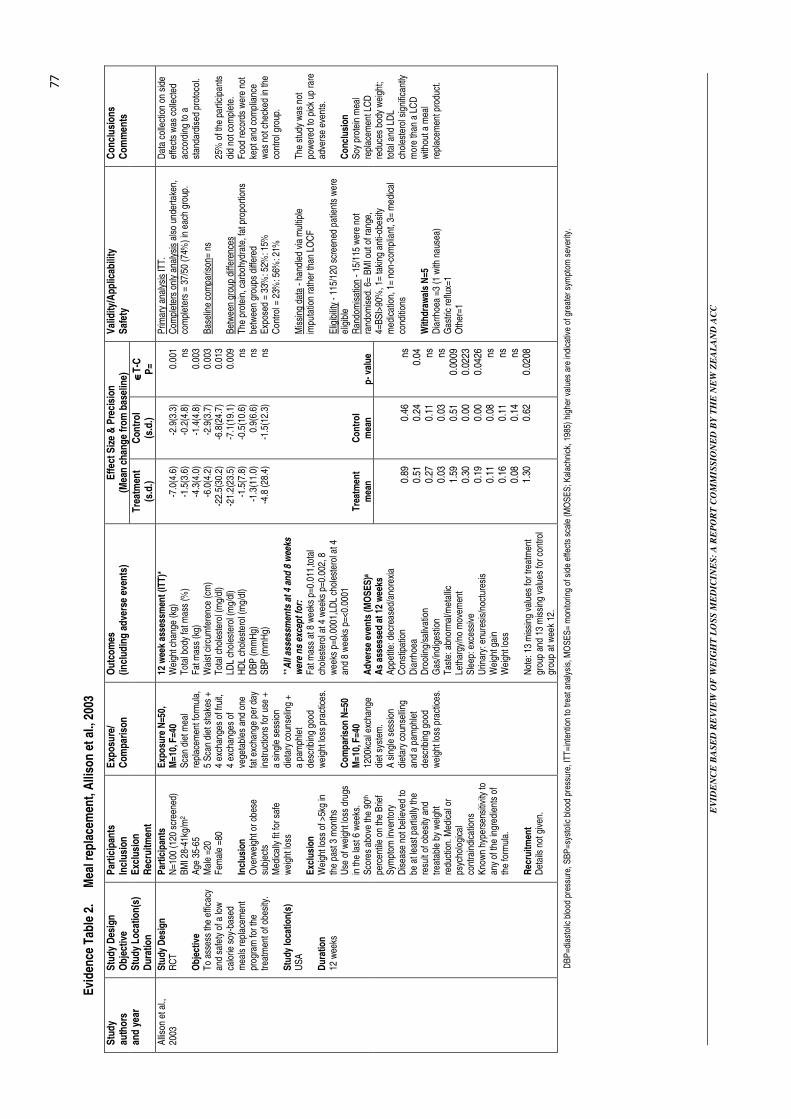
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
77
Evi
den
ce T
able
2.
Mea
l rep
lace
men
t, A
lliso
n e
t al
., 20
03
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y L
ocat
ion
(s)
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
R
ecru
itmen
t
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
)
Tre
atm
ent
(s.d
.) C
ontr
ol
(s.d
.) ∈ ∈∈∈
T-C
P
=
Val
idity
/App
licab
ility
S
afet
y C
oncl
usi
ons
C
omm
ents
-7
.0(4
.6)
-1.5
(3.6
) -4
.3(4
.0)
-6.0
(4.2
) -2
2.5(
30.2
) -2
1.2(
23.5
) -1
.5(7
.8)
-1.3
(11.
0)
-4.8
(28.
4)
Tre
atm
ent
mea
n
-2
.9(3
.3)
-0.2
(4.8
) -1
.4(4
.8)
-2.9
(3.7
) -6
.8(2
4.7)
-7
.1(1
9.1)
-0
.5(1
0.6)
0.
9(6.
6)
-1.5
(12.
3)
Co
ntr
ol
mea
n
0.
001 ns
0.
003
0.00
3 0.
013
0.00
9 ns
ns
ns
p
- val
ue
Alli
son
et a
l.,
2003
S
tudy
Des
ign
R
CT
O
bje
ctiv
e T
o as
sess
the
effic
acy
and
safe
ty o
f a lo
w
calo
rie s
oy-b
ased
m
eals
repl
acem
ent
prog
ram
for t
he
treat
men
t of o
besi
ty.
Stu
dy lo
catio
n(s
) U
SA
D
ura
tion
12
wee
ks
Par
ticip
ants
N
=100
(120
scr
eene
d)
BM
I 28-
41kg
/m2
Age
35-
65
Mal
e =2
0 F
emal
e =8
0 In
clus
ion
O
verw
eigh
t or o
bese
su
bjec
ts
Med
ical
ly fi
t for
saf
e w
eigh
t los
s E
xclu
sion
W
eigh
t los
s of
>5k
g in
th
e pa
st 3
mon
ths
Use
of w
eigh
t los
s dr
ugs
in th
e la
st 6
wee
ks.
Sco
res
abov
e th
e 90
th
perc
entil
e on
the
Brie
f S
ympt
om in
vent
ory
Dis
ease
not
bel
ieve
d to
be
at l
east
par
tially
the
resu
lt of
obe
sity
and
tre
atab
le b
y w
eigh
t re
duct
ion.
Med
ical
or
psyc
holo
gica
l co
ntra
indi
catio
ns
Kno
wn
hype
rsen
sitiv
ity to
an
y of
the
ingr
edie
nts
of
the
form
ula.
R
ecru
itmen
t D
etai
ls n
ot g
iven
.
Exp
osu
re N
=50,
M
=10,
F=4
0 S
can
diet
mea
l re
plac
emen
t for
mul
a,
5 S
can
diet
sha
kes
+ 4
exch
ange
s of
frui
t, 4
exch
ange
s of
ve
geta
bles
and
one
fa
t exc
hang
e pe
r day
in
stru
ctio
ns fo
r use
+
a si
ngle
ses
sion
di
etar
y co
unse
ling
+ a
pam
phle
t de
scrib
ing
good
w
eigh
t los
s pr
actic
es.
Co
mp
aris
on N
=50
M=1
0, F
=40
1200
kcal
exc
hang
e di
et s
yste
m.
A s
ingl
e se
ssio
n di
etar
y co
unse
lling
an
d a
pam
phle
t de
scrib
ing
good
w
eigh
t los
s pr
actic
es.
12 w
eek
asse
ssm
ent (
ITT
)*
Wei
ght c
hang
e (k
g)
Tot
al b
ody
fat m
ass
(%)
Fat
mas
s (k
g)
Wai
st c
ircum
fere
nce
(cm
) T
otal
cho
lest
erol
(mg/
dl)
LDL
chol
este
rol (
mg/
dl)
HD
L ch
oles
tero
l (m
g/dl
) D
BP
(mm
Hg)
S
BP
(mm
Hg)
**
All
asse
ssm
ents
at
4 an
d 8
wee
ks
wer
e n
s ex
cep
t fo
r:
Fat
mas
s at
8 w
eeks
p=0
.011
,tota
l ch
oles
tero
l at 4
wee
ks p
=0.0
02, 8
w
eeks
p=0
.000
1,LD
L ch
oles
tero
l at 4
an
d 8
wee
ks p
=<0.
0001
A
dve
rse
even
ts (M
OS
ES
)a A
s as
sess
ed a
t 12
wee
ks
App
etite
: dec
reas
ed/a
nore
xia
C
onst
ipat
ion
Dia
rrho
ea
Dro
olin
g/sa
livat
ion
Gas
/indi
gest
ion
Tas
te: a
bnor
mal
/met
allic
Le
thar
gy/n
o m
ovem
ent
Sle
ep: e
xces
sive
U
rinar
y: e
nure
sis/
noct
ures
is
Wei
ght g
ain
Wei
ght l
oss
Not
e: 1
3 m
issi
ng v
alue
s fo
r tre
atm
ent
grou
p an
d 13
mis
sing
val
ues
for c
ontro
l gr
oup
at w
eek
12.
0.
89
0.51
0.
27
0.03
1.
59
0.30
0.
19
0.11
0.
16
0.08
1.
30
0.
46
0.24
0.
11
0.03
0.
51
0.00
0.
00
0.08
0.
11
0.14
0.
62
ns
0.
04
ns
ns
0.00
09
0.02
23
0.04
26
ns
ns
ns
0.02
08
Prim
ary
anal
ysis
ITT
. C
ompl
eter
s on
ly a
naly
sis
also
und
erta
ken,
co
mpl
eter
s =
37/5
0 (7
4%) i
n ea
ch g
roup
. B
asel
ine
com
paris
on=
ns
Bet
wee
n gr
oup
diffe
renc
es
The
pro
tein
, car
bohy
drat
e, fa
t pro
porti
ons
betw
een
grou
ps d
iffer
ed
Exp
osed
= 3
3%: 5
2%: 1
5%
Con
trol =
23%
: 56%
: 21%
M
issi
ng d
ata
- han
dled
via
mul
tiple
im
puta
tion
rath
er th
an L
OC
F
Elig
ibili
ty -
115/
120
scre
ened
pat
ient
s w
ere
elig
ible
R
ando
mis
atio
n - 1
5/11
5 w
ere
not
rand
omis
ed. 6
= B
MI o
ut o
f ran
ge,
4=B
SI>
90%
, 1=
taki
ng a
nti-o
besi
ty
med
icat
ion,
1=
non-
com
plia
nt, 3
= m
edic
al
cond
ition
s W
ithd
raw
als
N=5
D
iarr
hoea
=3
(1 w
ith n
ause
a)
Gas
tric
reflu
x=1
Oth
er=1
Dat
a co
llect
ion
on s
ide
effe
cts
was
col
lect
ed
acco
rdin
g to
a
stan
dard
ised
pro
toco
l. 25
% o
f the
par
ticip
ants
di
d no
t com
plet
e.
Foo
d re
cord
s w
ere
not
kept
and
com
plia
nce
was
not
che
cked
in th
e co
ntro
l gro
up.
The
stu
dy w
as n
ot
pow
ered
to p
ick
up ra
re
adve
rse
even
ts.
Co
nclu
sion
S
oy p
rote
in m
eal
repl
acem
ent L
CD
re
duce
s bo
dy w
eigh
t; to
tal a
nd L
DL
chol
este
rol s
igni
fican
tly
mor
e th
an a
LC
D
with
out a
mea
l re
plac
emen
t pro
duct
.
DB
P=d
iast
olic
blo
od p
ress
ure,
SB
P=s
ysto
lic b
lood
pre
ssur
e, IT
T=i
nten
tion
to tr
eat a
naly
sis,
MO
SE
S=
mon
itorin
g of
sid
e ef
fect
s sc
ale
(MO
SE
S; K
alac
hnic
k, 1
985)
hig
her
valu
es a
re in
dica
tive
of g
reat
er s
ympt
om s
ever
ity.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
78
Evi
den
ce T
able
3.
Orl
ista
t, T
org
erso
n e
t al
., 20
04
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y L
ocat
ion
(s)
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
e
P
O
p=*
*
Val
idity
/App
licab
ility
S
afet
y C
oncl
usi
ons
C
omm
ents
Tor
gers
on e
t al.,
20
04
Stu
dy D
esig
n
Ran
dom
ised
, dou
ble
blin
d, p
lace
bo
cont
rolle
d m
ultic
entre
st
udy
Ob
ject
ive
To
dete
rmin
e th
e ef
fect
of
add
ing
orlis
tat t
o lif
esty
le c
hang
es o
n bo
dy w
eigh
t and
the
inci
denc
e of
type
2
diab
etes
. S
tudy
loca
tion
(s)
Sw
eden
D
ura
tion
F
our y
ears
Par
ticip
ants
N
=330
5 (p
lace
bo=1
637,
or
lista
t =16
40)
Mal
e=45
%
Fem
ale=
55%
M
ean
age
43.7
yea
rs
(pla
cebo
), 43
.0 y
ears
(orli
stat
). N
orm
al g
luco
se to
lera
nce
=79%
IG
T =
21%
In
clus
ion
A
ge 3
0-60
yea
rs
BM
I >=3
0kg/
m2
Non
-dia
betic
glu
cose
to
lera
nce
or IG
T (f
astin
g ve
nous
pla
sma
gluc
ose
<7.8
mm
o;/l
and
2 hr
pla
sma
gluc
ose
7.8-
11.1
mm
ol/l)
E
xclu
sion
D
iabe
tes
Ong
oing
/ act
ive
card
iova
scul
ar d
isea
se
Ong
oing
/act
ive
GI d
isea
se
Exp
osu
re
Orli
stat
120
mg
t.i.d
. +
redu
ced
calo
rie d
iet
(800
kcal
/day
def
icit)
. C
om
par
ison
P
lace
bo +
redu
ced
calo
rie d
iet
(800
kcal
/day
def
icit)
.
Wei
ght c
hang
e at
1 y
r (kg
) W
eigh
t cha
nge
at 4
yr (
kg)
Com
plet
ers
only
1 y
r (kg
) C
ompl
eter
s on
ly 4
yr (
kg)
>=5%
wei
ght l
oss
1 yr
(%)
>=5%
wei
ght l
oss
4 yr
(%)
>=10
% w
eigh
t los
s 1
yr (%
) >=
10%
wei
ght l
oss
4 yr
(%0
Car
dio
vasc
ula
r ri
sk fa
cto
rs (y
r 1)
D
BP
(mm
Hg)
S
BP
(mm
Hg)
T
otal
cho
lest
erol
(%)
LDL
chol
este
rol (
%)
HD
L ch
oles
tero
l (%
) LD
L-H
DL
ratio
T
rigly
cerid
es (%
) W
aist
circ
umfe
renc
e (c
m)
Fas
ting
who
le b
lood
* gl
ucos
e (m
mol
/l)
Fas
ting
seru
m in
sulin
(mm
ol/l)
F
ibrin
ogen
(µm
ol/l)
P
lasm
inog
en a
ctiv
ator
inhi
bito
r-1
(U/m
l) C
ard
iova
scu
lar
risk
fact
ors
(yr
4)
DB
P (m
mH
g)
SB
P (m
mH
g)
Tot
al c
hole
ster
ol (%
) LD
L ch
oles
tero
l (%
) H
DL
chol
este
rol (
%)
LDL-
HD
L ra
tio
Trig
lyce
rides
(%)
Wai
st c
ircum
fere
nce
(cm
) F
astin
g w
hole
blo
od*
gluc
ose
(mm
ol/l)
F
astin
g se
rum
insu
lin (p
mol
/l)
Fib
rinog
en (µ
mol
/l)
Pla
smin
ogen
act
ivat
or in
hibi
tor-
1 (U
/ml)
6.2
3.0
7.5
4.1
45.1
37
.3
20.8
15
.6
-2.6
-5
.2
-1.3
-1
.6
8.5
-0.3
-6
.3
-7.0
0.
2 -1
7.0
0.1
-3.0
-1
.9
-3.4
-2
.3
-5.1
9.
1 -0
.4
2.9
-4.4
0.
2 -2
0.6
-0.5
0.
1
10.6
5.
8 11
.4
6.9
72.8
52
.8
41.0
26
.2
-3.6
-7
.3
-8.8
-1
1.4
3.4
-0.5
-6
.2
-9.6
0.
1 -2
6.5
0.2
-7.1
-2
.6
-4.9
-7
.9
-12.
8 6.
5 -0
.6
2.4
-6.4
0.
1 -3
2.0
-0.4
-3
.0
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
1 <0
.01
<0.0
1 <0
.01
<0.0
1 <0
.01
<0.0
51
<0.0
1 <0
.012
<0.0
1 ns
<0.0
1 <0
.01
<0.0
1 <0
.01
<0.0
1 <0
.013
<0.0
1 ns
<0.0
1 <0
.014
<0.0
1 <0
.014
<0.0
1
Com
plia
nce
was
det
erm
ined
by
cou
ntin
g th
e nu
mbe
r of
caps
ules
retu
rned
. W
ithd
raw
als
Ref
usal
of t
reat
men
t, pl
aceb
o=20
%
orlis
tat=
14%
. With
draw
als
due
to in
suffi
cien
t the
rape
utic
re
spon
se, p
lace
bo=1
9%,
orlis
tat=
8%.
Com
plet
ers
and
non-
com
plet
ers
wer
e no
t si
gnifi
cant
ly d
iffer
ent.
Ad
here
nce
Pla
cebo
=92.
8 O
rlist
at=
93.3
%
Saf
ety
Orli
stat
was
wel
l tol
erat
ed
and
the
over
all i
ncid
ence
of
adve
rse
even
ts w
as th
e sa
me
in b
oth
grou
ps e
xcep
t fo
r GI e
vent
s. M
ost G
I eve
nts
wer
e m
ild to
mod
erat
e an
d oc
curr
ed d
urin
g th
e ea
rly
phas
e of
trea
tmen
t. O
ver t
he fo
ur-y
ear p
erio
d bo
th g
roup
s ha
d at
leas
t one
se
rious
adv
erse
eve
nt (1
3%
plac
ebo,
15%
orli
stat
). O
vera
ll 4%
of p
lace
bo a
nd
8% o
f orli
stat
pat
ient
s w
ithdr
ew b
ecau
se o
f adv
erse
ev
ents
prim
arily
GI e
vent
s.
The
re w
ere
sign
ifica
nt
decr
ease
s in
fat-s
olub
le
vita
min
s (A
, D, E
and
K1)
af
ter 4
yea
rs in
the
orlis
tat
grou
p.
Com
pare
d w
ith li
fest
yle
chan
ges
alon
e or
lista
t + li
fest
yle
chan
ges
resu
lted
in a
gre
ater
redu
ctio
n in
w
eigh
t and
a g
reat
er re
duct
ion
in
the
inci
denc
e of
type
2 d
iabe
tes
over
4 y
ears
. T
he b
enef
icia
l effe
ct o
f orli
stat
in
prev
entin
g di
abet
es w
as p
rimar
ily
due
to a
ben
efic
ial e
ffect
in IG
T
patie
nts.
T
he lo
ng-te
rm s
afet
y or
orli
stat
w
as d
emon
stra
ted.
D
urin
g 4
year
s of
trea
tmen
t or
lista
t + li
fest
yle
chan
ges
sign
ifica
ntly
dec
reas
ed th
e pr
ogre
ssio
n to
type
2 d
iabe
tes
com
pare
d w
ith p
lace
bo +
life
styl
e ch
ange
(log
-ran
k p=
0.00
32).
The
re w
as a
37.
3% d
ecre
ase
in
the
risk
of d
evel
opin
g di
abet
es
with
orli
stat
com
pare
d to
pla
cebo
. T
he d
iffer
ence
in w
eigh
t los
s w
as
the
sam
e w
heth
er a
sses
sed
by
LOC
F o
r BLC
F a
naly
sis.
O
nly
52%
of t
he tr
eatm
ent g
roup
an
d 34
% o
f the
pla
cebo
gro
up
wer
e re
tain
ed to
the
4th y
ear.
*ven
ous
bloo
d, L
OC
F =
last
obs
erva
tion
carr
ied
forw
ard,
BLC
F =
base
line
obse
rvat
ion
carr
ied
forw
ard,
ITT
=int
entio
n to
trea
t. **
Bet
wee
n tr
eatm
ent p
val
ues
for
anal
yses
, for
car
diov
ascu
lar
risk
fact
ors
anal
yses
by
LOC
F IT
T, B
LCF
ITT
and
obs
erve
d da
ta e
xcep
t whe
re in
dica
ted.
1 =
LOC
F a
nd o
bser
ved,
2 B
LCF
p<
0.05
3 LO
CF
and
BLC
F =
NS
, 4 B
CLF
=N
S.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
79
Evi
den
ce T
able
4.
Orl
ista
t, R
issa
nen
et
al.,
2001
Eff
ect S
ize
& P
reci
sion
(p
oole
d M
ean
ch
ange
fr
om
bas
elin
e at
1 y
ear)
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y L
ocat
ion
(s)
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
Cha
nge
(±se
m)
P
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Ris
sane
n et
al.,
20
01
Stu
dy d
esig
n
Ran
dom
ised
, pl
aceb
o co
ntro
lled,
do
uble
blin
d tri
al.
Ob
ject
ive
To
stud
y th
e ef
fect
of
wei
ght l
oss
on b
lood
co
agul
abili
ty a
nd
fibrin
olys
is in
hea
lth
obes
e w
omen
. L
ocat
ion
F
inla
nd
Du
ratio
n
12 m
onth
s
Par
ticip
ants
55
hea
lthy
obes
e w
omen
(5
1 co
mpl
eter
s)
Mea
n ag
e =4
4 ±
0.7
year
s M
ean
BM
I= 3
6±0.
5kg/
m2
Sm
oker
s =3
7 N
on-s
mok
ers=
14
Incl
usio
n
See
Sjo
stro
m
Exp
osu
re
Orli
stat
120
mg
t.i.d
.
+ hy
poen
erge
tic d
iet
Co
mp
aris
on
Pla
cebo
+
hypo
ener
getic
die
t H
ypo
calo
ric
die
t D
esig
ned
to c
ause
a
wei
ght l
oss
of 0
., 25
-0.
5kg/
wk
with
30%
fa
t, 50
%
carb
ohyd
rate
, and
20
% p
rote
in.
A m
axim
um o
f 30
0mg/
day
chol
este
rol w
as
dist
ribut
ed in
3 m
ain
mea
ls a
nd a
low
fat
snac
k. A
lcoh
ol
cons
umpt
ion
limite
d to
150
g pe
r wee
k.
Fur
ther
redu
ctio
n of
30
0kca
l/d a
fter 6
m
onth
s.
Wei
ght (
kg)
BM
I (kg
/m2 )
B
ody
fat (
kg)
Lean
bod
y m
ass
(kg)
D
BP
(mm
Hg)
S
BP
(mm
Hg)
S
- tot
al c
hole
ster
ol (m
mol
/l)
S-L
DL-
chol
este
rol (
mm
ol/l)
S
-HD
L-ch
oles
tero
l (m
mol
/l)
S-T
rigly
cerid
es (m
mol
/l)
S-in
sulin
(mU
/l)
Pla
cebo
vs.
orli
stat
wei
ght l
oss
at 1
2 m
onth
s (7
.2kg
vs.
13.
0kg)
was
not
si
gnifi
cant
and
the
resu
lts o
f orli
stat
and
pl
aceb
o w
ere
pool
ed.
-10.
0(1.
1)
-3.8
(0.4
) -6
.9(1
.0)
-3.1
(0.5
) -7
.1(1
.3)
-7.3
(1.9
) -0
.1(0
.1)
-0.2
(0.1
) -0
.0(0
.0)
-0.1
(0.1
) -3
.4(0
.8)
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
<0.0
01
ns
ns
ns
ns
<0.0
01
Wei
ght l
oss
was
no
t the
prim
ary
outc
ome,
dru
g an
d pl
aceb
o re
sults
poo
led.
The
re w
ere
bene
ficia
l cha
nges
in
fibrin
olys
is a
nd c
oagu
latio
n pe
rsis
ted
for o
ne y
ear i
f wei
ght l
oss
was
m
aint
aine
d.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
80
Evi
den
ce T
able
5.
Orl
ista
t, M
uls
et
al.,
2001
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e at
24
wee
ks±
s.d
., L
OC
F)
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y L
ocat
ion
(s)
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
e (in
clud
ing
ad
vers
e ev
ents
)
P
O
p=*
*
Val
idity
/App
licab
ility
S
afet
y C
oncl
usi
ons
C
omm
ents
Mul
s et
al.,
200
1 S
tudy
Des
ign
R
ando
mis
ed, p
lace
bo
cont
rolle
d, d
oubl
e bl
ind,
m
ultic
ente
r tria
l. O
bje
ctiv
e T
o as
sess
the
effe
ct o
f or
lista
t 120
mg
t.i.d
. ve
rsus
pla
cebo
on
wei
ght l
oss
and
seru
m
lipid
s in
obe
se
hype
rcho
lest
erol
emic
pa
tient
s.
Stu
dy lo
catio
n(s
) B
elgi
um
Du
ratio
n
24 w
eeks
follo
wed
by
an
optio
nal 2
4-w
eek
open
la
bel o
rlist
at e
xten
sion
ph
ase.
Par
ticip
ants
N
=441
recr
uite
d N
=294
rand
omis
ed
N=2
55 c
ompl
eter
s M
ale
19%
, Fem
ale
81%
M
ean
age
48(P
) and
50
(O) y
ears
In
clus
ion
B
MI 2
7-40
kg/m
2
Age
18-
70 y
ears
F
astin
g LD
L-C
4.1
to
6.7m
mol
/l an
d T
G<4
.5m
mol
/l (<
400m
g/dl
) E
xclu
sion
S
erio
us d
isea
se, d
iabe
tes
or u
ncon
trolle
d hy
perte
nsio
n W
omen
of c
hild
bear
ing
pote
ntia
l with
out
adeq
uate
con
trace
ptio
n P
revi
ous
baria
tric
surg
ery
Use
of a
ppet
ite
supp
ress
ants
or l
ipid
–lo
wer
ing
agen
ts
Evi
denc
e of
alc
ohol
or
subs
tanc
e ab
use.
Exp
osu
re
Orli
stat
120
mg
t.i.d
. +
diet
(-60
0kca
l/day
) with
<=3
0%
calo
ries
from
fat
Co
mp
aris
on
Pla
cebo
. + d
iet (
-600
kcal
/day
) with
<=
30%
cal
orie
s fro
m fa
t.
Wei
ght l
oss
(kg)
T
otal
cho
lest
erol
(mm
ol/l)
LD
L ch
oles
tero
l (m
mo;
/l)
HD
L ch
oles
tero
l (m
mo;
/l)
Trig
lyce
rides
(mm
ol/l)
LD
L-C
/HD
L-C
ratio
Lp
(a) (
mg/
l) D
ata
anal
ysis
A
naly
sis
was
bas
ed p
rimar
ily o
n th
e IT
T p
opul
atio
n fo
r who
m
follo
w-u
p w
as a
vaila
ble.
Las
t ob
serv
atio
n ca
rrie
d fo
rwar
d da
ta w
as in
clud
ed.
Ad
vers
e ev
ents
G
I eve
nts
Ove
rall
AE
s Li
quid
sto
ols
(%)
Incr
ease
d de
feca
tion
(%)
Loos
e st
ools
(%)
Dec
reas
ed d
efec
atio
n (%
) B
ronc
hitis
(%)
-1.8
8±4.
46
0.14
±0.
85
-0.0
9±0.
80
0.17
±0.
24
0.14
±9.
55
-0.4
6±0.
70
-6.5
0±26
38
67
8 5 3 12 6
-4.6
6±3.
77
0.42
±0.
75
-0.5
3±0.
65
0.07
±0.
22
0.08
±0.
72
-0.5
4±0.
67
3.00
±25
64
80
23
22
16
3 11
<0.0
01
<0.0
01
<0.0
01
<0.0
01
0.89
6 0.
294
0.22
5 0.
016
Pat
ient
s w
ere
stra
tifie
d by
st
udy
cent
re a
nd w
eigh
t los
s ca
tego
ry d
urin
g ru
n-in
(<
=2.0
0 vs
. >2.
0kg)
. A
2.6
% d
iffer
ence
bet
wee
n pl
aceb
o an
d tre
atm
ent g
roup
w
as ju
dged
to b
e cl
inic
ally
re
leva
nt. A
sam
ple
size
ca
lcul
atio
n de
term
ined
that
a
sam
ple
size
of 1
00 in
eac
h ar
m w
ould
be
requ
ired
for
ther
e to
be
an 8
0%
prob
abili
ty o
f sho
win
g a
2.6%
diff
eren
ce (e
ffect
siz
e of
0.4
) at t
he 5
% s
igni
fican
ce
leve
l. It
was
est
imat
ed th
at
30%
of p
atie
nts
wou
ld n
ot b
e fu
lly e
valu
able
and
that
ther
e w
ould
be
a 20
% w
ithdr
awal
ra
te in
the
plac
ebo
lead
-in
perio
d. T
he to
tal n
umbe
r re
quire
d to
be
rand
omis
ed
was
est
imat
ed to
be
284.
N
ote
: Li
mite
d re
porti
ng o
f wei
ght
loss
par
amet
ers
(BM
I, %
%
10%
not
repo
rted)
.
Co
nclu
sion
O
rlist
at a
s an
adj
unct
to
diet
ary
inte
rven
tion
prom
otes
cl
inic
ally
sig
nific
ant w
eigh
t los
s an
d LD
L-C
bey
ond
the
effe
ct
of w
eigh
t los
s in
ove
rwei
ght o
r ob
ese
patie
nts
with
co
ncom
itant
hy
perc
hole
ster
olem
ia.
Run
-in w
eigh
t los
s an
d w
eigh
t lo
ss d
urin
g th
e fir
st 4
wee
ks
wer
e pr
edic
tors
of l
onge
r-te
rm
wei
ght l
oss
at 2
4 w
eeks
.
LDL-
C =
low
den
sity
lipo
prot
ein
chol
este
rol,
P=p
lace
bo, O
=orli
stat
, **=
diffe
renc
e fr
om p
lace
bo. L
OC
F=l
ast o
bser
vatio
n ca
rrie
d fo
rwar
d.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
81
Evi
den
ce T
able
6.
Orl
ista
t, F
oxc
roft
et
al.,
2000
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) E
ffec
t Siz
e &
Pre
cisi
on
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Fox
crof
t et a
l.,
2000
S
tudy
des
ign
R
apid
sys
tem
atic
revi
ew
of R
CT
s.
Ob
ject
ive
To
clar
ify th
e po
tent
ial
bene
fits,
dis
bene
fits
and
cost
s of
orli
stat
in th
e tre
atm
ent o
f obe
sity
. S
tud
ies
incl
uded
S
jost
rom
et a
l., 1
998
Dav
idso
n et
al.,
199
9 H
olla
nder
et a
l., 1
998
Incl
usio
n
Sys
tem
atic
revi
ews
or R
CT
s of
orli
stat
in
the
treat
men
t of o
besi
ty
Effi
cacy
or c
ost e
ffect
iven
ess
Hum
an s
ubje
cts
only
. O
nly
phas
e III
clin
ical
tria
ls in
clud
ed.
Exc
lusi
on
Pha
se II
clin
ical
tria
ls
Not
sta
ted
but o
nly
3/10
9 st
udie
s or
pa
pers
wer
e in
clud
ed.
Exp
osu
re
Orli
stat
Out
com
es fo
r wei
ght l
oss
repo
rted
in
othe
r sys
tem
atic
revi
ews.
Qu
ality
of l
ife
Est
imat
ed Q
ALY
s ga
ined
in a
yea
r of
orli
stat
trea
tmen
t (ba
sed
on 1
00
pers
ons
star
ting
treat
men
t with
re
spon
ders
thos
e w
ho lo
st a
nd
mai
ntai
ned
>10%
of t
heir
initi
al b
ody
wei
ght o
ver 2
yea
rs).
Co
st d
ata
Pric
e of
a p
atie
nt c
onsu
ltatio
n (N
HS
19
98)
Mon
thly
cos
t of o
rlist
at 1
20 td
s.
Ave
rage
num
ber o
f con
sulta
tions
per
ye
ar.
GP
con
sulta
tion
cost
per
vis
it.
Dro
p-ou
t yea
r 1
Dro
p-ou
t yea
r 2
Ave
rage
cos
t per
yea
r for
100
pa
tient
s tre
ated
for 2
yea
rs.
The
cos
t /Q
ALY
of o
rlist
at tr
eatm
ent
(ext
rem
e va
lue
sens
itivi
ty a
naly
sis)
T
he c
ost/Q
ALY
in p
rimar
y ca
re
setti
ng (e
xtre
me
valu
e se
nsiti
vity
an
alys
is)
10kg
wei
ght r
educ
tion
over
2
year
s as
an
adju
nct t
o di
et
(NN
T=1
2 95
% C
I 7-3
7)
1.60
QA
LY p
er y
ear o
f orli
stat
tre
atm
ent
£118
.00
£45.
00
4 £16.
00
27%
23
%
£ 73
,436
£4
5,00
0 (1
3,54
1-13
1,91
8) p
er
QA
LY g
aine
d £2
6,63
5 (9
,779
–66
,505
)
Onl
y th
e “m
ost p
laus
ible
” re
sults
w
ere
used
for f
urth
er a
naly
sis.
E
ME
A p
resc
riptio
n in
dica
tions
for
orlis
tat d
o no
t coi
ncid
e w
ith th
e pu
blis
hed
trial
info
rmat
ion.
On
aver
age
orlis
tat r
esul
ts in
obe
se
peop
le lo
sing
an
addi
tiona
l 3-4
% o
f th
eir i
nitia
l bod
y w
eigh
t ove
r die
t al
one
over
a 2
-yea
r per
iod.
T
he e
stim
ated
cos
t util
ity o
f orli
stat
w
as £
46,0
00 p
er Q
ALY
gai
ned.
T
here
was
no
evid
ence
that
the
shor
t-te
rm w
eigh
t los
s w
ould
hav
e a
long
er-
term
impa
ct o
n m
orbi
dity
and
m
orta
lity.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
82
Evi
den
ce T
able
7.
Orl
ista
t, D
ero
sa e
t al
., 20
03
Eff
ect S
ize
& P
reci
sion
(%
cha
nge
fro
m b
asel
ine)
S
tud
y
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y D
ura
tion
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) P
N
=23
O
N=2
5 F
N
=24
OF
N
=24
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Der
osa
et a
l.,
2003
S
tudy
des
ign
R
ando
mis
ed, d
oubl
e bl
ind
plac
ebo-
cont
rolle
d O
bje
ctiv
e T
o as
sess
obe
se
patie
nts
with
hy
perc
hole
ster
olem
ia
who
wer
e pr
escr
ibed
a
stan
dard
ised
die
t, co
mpa
ring
the
actio
n of
or
lista
t, flu
vast
atin
, or
lista
t with
fluv
asta
tin
and
plac
ebo
on
anth
ropo
met
ric
mea
sure
men
ts, b
lood
pr
essu
re a
nd li
pid
prof
ile.
Du
ratio
n
One
yea
r
Par
ticip
ants
N
=99
Obe
se p
atie
nts
with
hy
perc
hole
ster
olem
ia
M=4
8 F
=51
Mea
n ag
e =5
1 ye
ars
(SD
=9)
Incl
usio
n
BM
I> 3
0kg/
m2
Age
>40
year
s T
otal
cho
lest
erol
>=
240m
g/dl
S
BP
>140
mg
Hg
DB
P<9
0mm
Hg
Exc
lusi
on
Sm
oker
s A
bnor
mal
thyr
oid
func
tion
Pat
ient
s ta
king
di
uret
ics
or b
eta
bloc
kers
Exp
osu
re/C
om
par
ison
O
rlist
at 1
20m
g t.i
.d.+
co
ntro
lled
ener
gy d
iet
Pla
cebo
+ c
ontro
lled
ener
gy d
iet
Flu
vast
atin
80m
g/d
+ co
ntro
lled
ener
gy d
iet
Orli
stat
120
mg
t.i.d
. +
Flu
vast
atin
80m
g/d
+ co
ntro
lled
ener
gy d
iet
All
parti
cipa
nts
unde
rtook
>=
30m
ins
aero
bic
activ
ity
4 da
ys a
wee
k D
iet:
150
0kca
l, 54
%
carb
ohyd
rate
, 24%
pr
otei
n, 2
2% fa
ts, 1
08m
g ch
oles
tero
l, 35
g fib
er
durin
g pl
aceb
o le
ad-in
pe
riod.
Foo
d di
arie
s w
ere
kept
. Die
t ins
truct
ion
ever
y 3
mon
ths.
At 6
mon
ths
BM
I (kg
/m2 )
W
CR
(cm
) B
WL
(kg)
A
t 1 y
ear
BM
I (kg
/m2 )
W
CR
(cm
) B
WL
(kg)
A
t 6 m
onth
s S
BP
(mm
Hg)
D
BP
(mm
Hg)
T
C
LDL-
C
HD
L-C
T
Gs
At 1
yea
r S
BP
(mm
Hg)
D
BP
(mm
Hg)
T
C
LDL-
C
HD
L-C
T
Gs
Saf
ety
Orli
stat
and
fluv
asta
tin w
ere
wel
l tol
erat
ed. 3
% o
f pat
ient
s ex
perie
nced
sid
e ef
fect
s.
The
re w
ere
no s
erio
us
adve
rse
even
ts.
N
S
NS
N
S
NS
P
<0.0
5 P
<0.0
5 N
S
NS
N
S
NS
N
S
NS
N
S
NS
P
<0.0
5 P
<0.0
5 N
S
NS
N
S
NS
N
S
P<0
.02
P<0
.0
P<0
.02
NS
N
S
NS
N
S
NS
N
S
P<0
.05
P<0
.05
P<0
.05
P<0
.05
NS
P
<0.0
2
N
S
NS
N
S
P<0
.05
P<0
.05
P<0
.05
NS
N
S
P<0
.05
P<0
.05
NS
N
S
P<0
.05
P<0
.05
P<0
.02
P<0
.02
P<0
.02
P<0
.05
p<
0.05
p
<0.0
5 p
<0.0
5 p<
0.01
p
<0.0
1 p
<0.0
1 N
S
NS
p<
0.02
p<
0.02
p
<0.0
2 p<
0.05
p<
0.01
p<
0.01
p<
0.05
p<
0.05
p
<0.0
5 p<
0.02
Bot
h gr
oups
com
para
ble
at b
asel
ine
Ran
dom
isat
ion
enve
lope
s us
ed
Com
plia
nce
asse
ssed
thro
ugh
tabl
et
coun
ting
96 (9
7%) c
ompl
eter
s, 3
sub
ject
s dr
oppe
d ou
t due
to a
dver
se re
actio
ns
(orli
stat
),
Vita
min
D le
vels
wer
e no
t mea
sure
d.
Sig
nific
ant d
ecre
ases
in
wei
ght,
BM
I and
wai
st
circ
umfe
renc
e w
as
foun
d on
ly in
the
orlis
tat+
fluva
stin
gro
up
at 6
mon
ths
and
in a
ll gr
oups
apa
rt fro
m B
MI
in th
e pl
aceb
o gr
oup
at
1 ye
ar. T
he c
ombi
ned
treat
men
t gro
ups
show
ed th
e gr
eate
st
redu
ctio
ns.
No
sign
ifica
nt c
hang
es
in B
P in
any
gro
up a
t 6
mon
ths,
but
ther
e w
as a
si
gnifi
cant
impr
ovem
ent
in th
e tre
atm
ent g
roup
s si
ngly
and
com
bine
d at
1
year
. The
gre
ates
t re
duct
ions
in B
P w
ere
in
the
com
bine
d tre
atm
ent
grou
ps.
Lipi
d pr
ofile
s w
ere
sign
ifica
ntly
bet
ter a
t 6
mon
ths
for a
ll pa
ram
eter
s in
the
com
bine
d tre
atm
ent
grou
p. A
ll gr
oups
sh
owed
sig
nific
ant
impr
ovem
ents
at 1
yea
r fo
r tot
al c
hole
ster
ol a
nd
low
-den
sity
lipo
prot
ein
chol
este
rol.
Aga
in th
e co
mbi
ned
treat
men
t gr
oup
had
the
grea
test
im
prov
emen
ts fo
r eac
h pa
ram
eter
at 6
mon
ths
and
1 ye
ar.
BM
I = b
ody
mas
s in
dex,
WC
R =
wai
st c
ircum
fere
nce
redu
ctio
n, B
WL=
bod
y w
eigh
t los
s, P
= pl
aceb
o gr
oup,
O=
orlis
tat 1
20m
g t.i
.d. g
roup
, F=f
luva
stat
in 8
0mg/
d gr
oup,
OF
= o
rlist
at 1
20 t.
i.d.+
fluva
stat
in 8
0mg/
d gr
oup.
TC
=to
tal c
hole
ster
ol, L
DL-
C=l
ow d
ensi
ty li
popr
otei
n ch
oles
tero
l, H
DL-
C+
high
-den
sity
lipo
prot
ein
chol
este
rol,
TG
s =
trig
lyce
rides
. Bo
ld =
rai
sed
valu
es, n
orm
al=d
ecre
ased
val
ues.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
83
Evi
den
ce T
able
8.
Orl
ista
t, H
anef
ield
et
al.,
2002
† =
Cha
nge
vs p
lace
bo, I
TT
= in
tent
ion
to tr
eat a
naly
sis,
LO
CF
= la
st o
bser
vatio
n ca
rrie
d fo
rwar
d, G
CP
=goo
d cl
inic
al p
ract
ice.
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy/
Yea
r L
ocat
ion
S
tud
y D
esig
n
Ob
ject
ive
Du
ratio
n
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
P
O
p=†
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Wei
gh
t los
s af
ter
1 yr
of t
reat
men
t B
ody
wei
ght (
kg)
Bod
y w
eigh
t (%
) W
eigh
t los
s >=
5%
Dia
bet
ic m
etab
olic
par
amet
ers
afte
r 48
wee
ks o
f tr
eatm
ent*
* H
bA1c
Fas
ting
gluc
ose
(mm
ol/l)
P
ost p
rand
ial g
luco
se(m
mol
/l)
Trig
lyce
rides
(mm
ol/l)
D
iab
etic
met
abo
lic p
aram
eter
s af
ter
1yr*
H
bA1c
Fas
ting
gluc
ose
(mm
ol/l)
P
ost p
rand
ial g
luco
se (m
mol
/l)
Lip
id p
rofil
e at
48
wee
ks
Tot
al c
hole
ster
ol
LDL-
chol
este
rol (
mm
ol/L
) H
DL-
chol
este
rol (
mm
ol/L
) L
ipid
pro
file
at 1
yr
Tot
al c
hole
ster
ol
LDL-
chol
este
rol (
mm
ol/L
) H
DL-
chol
este
rol (
mm
ol/L
) O
ther
CH
D r
isk
acto
rs
Trig
lyce
rides
(mm
ol/l)
S
BP
mm
Hg
DB
P m
mH
g A
nth
rop
omo
rph
ic in
dic
es
Wai
st c
ircum
fere
nce
(cm
)
3.
4±5.
3 3.
6±5.
7 31
.6%
-0.6
±1.
6 -0
.9±
2.8
-0.7
±4.
5 -0
.2±
3.8
-0.4
±1.
5%
-0.7
±3.
2 -0
.5±
4.6
0.
0±1.
4 +0
.01±
1.2
+0.0
7±0.
2
+1.8
±22
.0%
+5
.1±
34.3
%
+6.4
±24
.5%
NR
-4
.96
-4.7
8
-3.0
±5.
6
5.
3±5.
1 5.
4±5.
0 51
.3%
-0.9
±1.
1 -1
.7±
2.1
-1.4
±3.
5 -0
.1±
1.4
-0.9
+1.3
%
-1.6
±2.
5 -1
.8±
3.8
-0.2
±0.
9 -0
.09±
0.7
0.0±
0.2
-2
.3±
16.3
%
-2.0
±26
.7%
+0
.6±
20.0
%
NR
-4
.98
-4.8
0
-5.5
±5.
3
0.
006
0.00
6 0.
0001
0.47
0.
08
0.45
0.
12
0.00
03
0.00
4 0.
003
0.07
0.
12
0.02
<0.0
1 <0
.05
<0.0
1 ns
ns
ns
<0.0
1
Han
efie
ld e
t al
., 20
02
Loc
atio
n
Ger
man
y (P
rimar
y ca
re a
nd
outp
atie
nt
clin
ics)
Stu
dy D
esig
n
Ran
dom
ised
, pl
aceb
o co
ntro
lled,
do
uble
blin
d cl
inic
al
trial
. R
un
in p
erio
d
4 w
eek
plac
ebo
+ di
et ru
n in
per
iod.
O
bje
ctiv
e T
o as
sess
the
long
-te
rm e
ffect
of
orlis
tat o
n bo
dy
wei
ght,
glyc
aem
ic
cont
rol a
nd
card
iova
scul
ar ri
sk
fact
ors
in
over
wei
ght p
atie
nts
with
type
2
diab
etes
. T
reat
men
t D
ura
tion
48
wee
ks
Par
ticip
ants
N
= 49
2 en
rolle
d N
=383
rand
omis
ed
N=3
69 IT
T p
opul
atio
n M
ale
181,
Fem
ale=
188
A
vera
ge A
ge 5
6-57
A
vera
ge B
MI=
34k
g/m
2
Incl
usio
n
Age
18-
70 y
ears
B
MI>
=28k
g/M
2
HbA
1c =
6.5-
11%
D
iagn
osis
of t
ype
2 di
abet
es tr
eate
d w
ith s
ulph
onyl
urea
s fo
r at l
east
2
mon
ths
befo
re s
cree
ning
or w
ere
diag
nose
d w
ith d
iabe
tes
but n
ot y
et
treat
ed w
ith a
ntid
iabe
tic m
edic
atio
n.
Exc
lusi
on
Dia
betic
pat
ient
s tre
ated
with
an
tidia
betic
dru
gs o
ther
than
su
lpho
nylu
reas
P
atie
nts
treat
ed w
ith m
edic
atio
ns
know
n to
affe
ct b
ody
wei
ght,
seru
m
lipid
s or
vita
min
s.
Pat
ient
s w
ith p
rolif
erat
ive
retin
opat
hy, p
apill
oede
ma,
un
cont
rolle
d hy
perte
nsio
n (D
BP
>120
mm
Hg)
, hyp
o or
hy
perth
yroi
dism
, sec
onda
ry ty
pe 1
di
abet
es, c
ardi
ac in
suffi
cien
cy, o
r pr
esen
ce o
r his
tory
of c
ance
r or a
ny
sign
ifica
nt a
ppet
ite, r
enal
, hep
atic
, G
I, ps
ychi
atric
, im
mun
olog
ical
or
met
abol
ic d
isor
ders
. Fem
ale
patie
nts
wer
e ex
clud
ed if
they
wer
e pr
egna
nt, l
acta
ting
or fo
r ch
ildbe
arin
g po
tent
ial a
nd n
ot ta
king
ad
equa
te c
ontra
cept
ive
mea
sure
s.
Exp
osu
re
Orli
stat
120
mg
t.i.d
.+ a
60
0 ca
lorie
redu
ced
diet
(3
0% fa
t, 50
%
carb
ohyd
rate
, 20%
pr
otei
n, m
ax 3
00m
g/d
chol
este
rol)
Co
mp
aris
on
Pla
cebo
t.i.d
. + a
600
ca
lorie
redu
ced
diet
(3
0% fa
t, 50
%
carb
ohyd
rate
, 20%
pr
otei
n, m
ax 3
00m
g/d
chol
este
rol)
Rea
son
s fo
r d
isco
ntin
uatio
n
Pre
rand
omis
atio
n dr
op-o
ut =
109
Vio
latio
n of
sel
ectio
n cr
iteria
=59
Oth
er p
roto
col v
iola
tion=
16
Ref
used
trea
tmen
t =10
F
ailu
re to
retu
rn=1
0 D
id n
ot c
o-op
erat
e=8
Adv
erse
eve
nt=3
O
ther
=3
Pos
t ran
dom
isat
ion
drop
-out
=11
9 A
dver
se e
vent
s =2
8 (o
rlist
at =
16,
plac
ebo=
12)
With
draw
al o
f con
sent
=35
(orli
stat
=13
, pl
aceb
o=22
) Lo
st to
FU
=24
(orli
stat
=13,
pla
cebo
-11)
P
roto
col v
iola
tion=
14 (o
rlist
at=9
, pla
cebo
An
alys
is
Effi
cacy
ass
esse
d on
an
ITT
bas
is, I
TT a
naly
sis:
or
lista
t=18
9,
plac
ebo=
180
LOC
F m
odel
was
use
d fo
r mis
sing
dat
a =5
) E
xter
nal
val
idity
N
ote
s 1.
Stu
dy c
ondu
cted
ac
cord
ing
to G
CP
gu
idel
ines
2.
Com
plia
nce
asse
ssed
by
cap
sule
cou
nt
3.T
rain
ed m
onito
r ch
ecke
d pr
otoc
ol
adhe
renc
e 4.
Stu
dy a
udit
perfo
rmed
th
roug
hout
the
stud
y 5.
Stu
dy s
pons
ored
by
Hof
fman
n-La
-Roc
he
Stu
dy c
onc
lusi
ons
Orli
stat
+ d
iet r
esul
ted
in s
igni
fican
t wei
ght
loss
, im
prov
ed
glyc
aem
ic c
ontro
l and
ca
rdio
vasc
ular
risk
fa
ctor
pro
file
in
over
wei
ght p
atie
nts
with
type
2 d
iabe
tes.
C
om
men
ts
Effe
ct w
as c
alcu
late
d fro
m s
tart
of s
tudy
–
i.e.,
incl
udin
g ru
n in
pe
riod
and
from
ra
ndom
isat
ion.
T
he ru
n-in
per
iod
was
in
clud
ed in
the
repo
rted
conc
lusi
ons,
id
eally
the
resu
lts
durin
g th
e ra
ndom
isat
ion
perio
d sh
ould
hav
e be
en
repo
rted
Res
ults
wer
e re
porte
d fro
m th
e st
art o
f ra
ndom
isat
ion
(48
wee
ks) i
n th
e m
ain
tabl
e bu
t fro
m th
e st
art
of s
tudy
(1 y
ear)
in th
e su
mm
ary
and
conc
lusi
on.
A n
umbe
r of
sig
nific
ant
diffe
renc
es a
t 1 y
ear
wer
e ns
from
the
poin
t of
rand
omis
atio
n

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
84
Evi
den
ce T
able
9.
Orl
ista
t, H
alp
ern
et
al.,
2003
Eff
ect S
ize
& P
reci
sion
S
tud
y/Y
ear
Loc
atio
n
Stu
dy
Des
ign
O
bje
ctiv
e D
ura
tion
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
P
O
P=
Val
idity
/App
licab
ility
Con
clu
sio
ns
Com
men
ts
Hal
pern
et a
l.,
2003
L
ocat
ion
La
tin A
mer
ica:
B
razi
l, C
olum
bia,
C
osta
Ric
a M
exic
o
Stu
dy D
esig
n
Ran
dom
ised
, dou
ble
blin
d, p
lace
bo
cont
rolle
d m
ulti-
cent
re,
clin
ical
tria
l R
un
in p
erio
d
2-w
eek
open
, pla
cebo
pe
riod
prio
r to
rand
omis
atio
n O
bje
ctiv
e T
o de
term
ine
if no
n-in
sulin
dep
ende
nt
diab
etic
pat
ient
s lo
se
mor
e w
eigh
t whe
n tre
ated
for 2
4 w
eeks
w
ith o
rlist
at in
co
njun
ctio
n w
ith a
hy
poca
loric
die
t +
beha
viou
ral
coun
selli
ng th
an
plac
ebo
t.i.d
+
hypo
calo
ric d
iet +
be
havi
oura
l co
unse
lling
. D
ura
tion
24
wee
ks
Par
ticip
ants
N
=365
enr
olle
d N
=343
rand
omis
ed
N=2
80 c
ompl
eted
the
stud
y O
rlist
at N
= 16
4 P
lace
bo N
=174
M
ale=
104
Age
=51
year
s B
MI=
35
Cau
casi
an =
60%
In
clus
ion
A
ge 1
8-70
yea
rs
BM
I>27
kg/m
2
Dx
of N
IDD
M (W
HO
) H
bA1c
6.0
-11.
0%
Neg
ativ
e pr
egna
ncy
test
ad
equa
te c
ontra
cept
ion
in w
omen
of
child
bea
ring
pote
ntia
l E
xclu
sion
H
isto
ry o
f rec
ent M
I, un
cont
rolle
d hy
perte
nsio
n, s
igni
fican
t car
diac
, re
nal,
hepa
tic, G
I, re
spira
tory
, ne
urol
ogic
al, p
sych
iatri
c or
end
ocrin
e di
seas
e, G
I bar
iatri
c su
rger
y, p
ost
surg
ical
adh
esio
n, h
isto
ry o
f ca
rcin
oma,
bul
imia
, lax
ativ
e ab
use,
cl
inic
al s
ympt
oms
of fa
t-sol
uble
vi
tam
in d
efic
ienc
ies,
sub
stan
ce a
buse
, ap
petit
ive
supp
ress
ants
, ins
ulin
, re
tinoi
ds, s
yste
mic
ste
roid
s ot
her t
han
HR
T, a
carb
ose
(was
h-ou
t =2
mon
ths)
, pr
egna
nt la
ctat
ing
and
child
-bea
ring
pote
ntia
l wom
en n
ot ta
king
co
ntra
cept
ive
mea
sure
s.
Exp
osu
re
Orli
stat
120
mg
t.i.d
. +
hypo
calo
ric d
iet +
be
havi
oura
l co
unse
lling
C
om
par
ison
P
lace
bo t.
i.d. +
hy
poca
loric
die
t +
beha
viou
ral
coun
selli
ng
Wei
gh
t los
s IT
T p
op %
WL
Orli
stat
LM
S d
iff P
-O (k
g)
Com
plet
ers
pop
%W
L C
ompl
eter
s po
p W
L (k
g)
>=5%
WL
>=10
% W
L D
iab
etic
met
abo
lic p
aram
eter
s (D
MP
), 24
w
eeks
M
ean
decr
ease
in g
luco
se le
vels
F
astin
g pl
asm
a gl
ucos
e LS
M d
iff P
-O
ITT
pop
dec
reas
e H
bA1c
%
Com
plet
ers
pop
decr
ease
HbA
1c %
B
lood
pre
ssur
e at
24
wks
S
BP
D
BP
L
ipid
pro
file
at 2
4 w
eeks
T
otal
cho
lest
erol
(mm
ol/l)
LD
L-C
hole
ster
ol (m
mol
/l)
HD
L-ch
oles
tero
l (m
mol
/l)
Fas
ting
TG
s (m
mol
/l)
Pos
t pra
ndia
l TG
s (m
mol
/l)
An
thro
pom
orp
hic
ind
ices
H
igh
mea
n w
aist
circ
umfe
renc
e cm
A
dve
rse
even
ts
Ove
rall
adve
rse
even
ts(%
) S
erio
us a
dver
se e
vent
s P
atie
nts
with
draw
n fro
m s
tudy
bec
ause
of
GI
adve
rse
even
ts
Mo
st c
omm
on G
I eve
nts
O
vera
ll F
atty
/oily
sto
ol
Incr
ease
d de
feca
tion
Liqu
id s
tool
s O
ily e
vacu
atio
n F
latu
lanc
e w
ith d
isch
arge
A
bdom
inal
pai
n
3.
0± 1
.3%
N
R
-3.1
±1.
0%
2.58
±1.
4kg
17%
3%
0.
01±
0.30
0.
22∀
0.14
-0.
13∀
0.14
%va
lues
NR
va
lues
NR
-0
.03∀
0.11
+0
.03∀
0.09
+0
.02∀
0.02
-0
.10∀
0.12
-0
.11∀
0.13
-3
.5∀
5.4
60
.3 4
5(2)
65
(37.
0%)
18(1
0.4%
) 19
(11.
0%)
8(4.
6%)
0(0.
0%)
3(1.
7%)
6(3.
5%)
4.
7 ±
0.5%
1.
6kg
-4.9
±0.
7%
4.24
±0.
23
30%
7%
1.
0±0.
34
0.85
0.
61∀
0.15
-0
.64∀
0.16
va
lues
NR
va
lues
NR
-0
.40∀
0.08
-0
.31∀
0.08
-0
.02∀
0.02
-0
.18∀
0.09
-0
.03∀
0.13
-5
.3∀
5.3
74 5
8(7)
11
0(65
%)
77(4
5.6%
) 68
(40.
2%)
17(1
0.1%
) 17
(10.
1%)
13(7
.7%
) 13
(7.7
%)
N
R
0.00
03
NR
0.
0003
0.
003
0.07
2 N
R
0.03
6 0.
06
0.04
ns
ns
0.
0001
0.
0002
0.
038
0.21
7 0.
379
0.03
2
Ext
ern
al v
alid
ity
Hig
hly
sele
cted
pat
ient
s m
any
co-m
orbi
ditie
s ex
clud
ed.
Hig
h dr
op-o
ut ra
te
Dro
p-ou
t cau
ses
not
spec
ified
Stu
dy
con
clu
sio
ns
Orli
stat
is a
saf
e ad
junc
t to
diet
ary
inte
rven
tion
and
conv
entio
nal
antid
iabe
tic
phar
mac
othe
rapy
in
the
glob
al
treat
men
t of o
bese
di
abet
ic p
atie
nts.
It
prom
otes
a
clin
ical
ly
sign
ifica
nt w
eigh
t lo
ss a
nd im
prov
ed
glyc
aem
ic c
ontro
l an
d lip
id p
rofil
e.
Co
mm
ents
W
eigh
t los
s be
gan
to s
low
at b
etw
een
16-2
0 w
eeks
ITT
= in
tent
ion
to tr
eat,
LMS
=lea
st m
ean
squa
res,
WL=
wei
ght l
oss.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
85
Evi
den
ce T
able
10.
O
rlis
tat,
Leu
ng
et
al.,
2003
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
Eff
ect S
ize
& P
reci
sion
V
alid
ity/A
pplic
abili
ty
C
oncl
usi
ons
C
omm
ents
Leun
g et
al.,
20
03
Stu
dy ty
pe
Sys
tem
atic
revi
ew
Ob
ject
ive
To
desc
ribe
the
phar
mac
olog
ical
m
anag
emen
t of o
besi
ty
conc
entra
ting
on o
rlist
at
Incl
uded
stu
die
s O
rlist
at
Dav
idso
n, 1
999
Fin
er, 2
000
Hau
ptm
an, 2
000
Hill
, 199
9 H
olla
nder
, 199
8 R
ossn
er, 2
000
Sjo
stro
m, 1
998
Incl
usio
n
Stu
dies
bet
wee
n 19
66-
Feb
ruar
y 20
02
RC
Ts
of >
6 m
onth
s du
ratio
n re
porti
ng th
e ef
ficac
y of
or
lista
t
Exp
osu
re
Orli
stat
30-
120m
g t.i
.d.
Co
mp
aris
on
Pla
cebo
Wei
gh
t red
uct
ion
with
orli
stat
ass
ocia
ted
with
a s
igni
fican
t im
prov
emen
t in
cont
rol o
f car
diov
ascu
lar r
isk
fact
ors.
P
atie
nt w
ith h
yper
cho
lest
ero
lem
ia
Tot
al c
hole
ster
ol o
rlist
at v
s. p
lace
bo
LDL
chol
este
rol,
orlis
tat v
s. p
lace
bo
Pla
sma
insu
lin a
t the
end
of 2
yea
rs, o
rlist
at v
s. p
lace
bo (o
ne s
tudy
) S
ysto
lic b
lood
pre
ssur
e af
ter o
ne y
ear,
orlis
tat v
s. p
lace
bo
Dia
stol
ic b
lood
pre
ssur
e af
ter o
ne y
ear,
orlis
tat v
s. p
lace
bo.
Pat
ien
ts w
ith ty
pe
2 d
iab
etes
W
eigh
t los
s O
rlist
at +
hyp
ocal
oric
die
t vs.
pla
cebo
Im
prov
ed g
lyca
emic
con
trol o
rlist
at v
s. p
lace
bo
Pat
ien
ts w
ith IG
T
Nor
mal
isat
ion
of g
luco
se le
vels
, orli
stat
vs.
pla
cebo
. R
educ
tion
on ra
te o
f pro
gres
sion
to d
iabe
tes,
orli
stat
vs.
pla
cebo
A
dve
rse
even
ts
Mild
– m
oder
ate
GI e
ffect
s, o
rlist
at v
s. p
lace
bo
Low
pla
sma
leve
ls o
f fat
-sol
uble
vita
min
s an
d be
ta c
arot
ene
in th
e or
lista
t gro
up
Inte
ract
ions
repo
rted
with
cyc
losp
orin
e an
d w
arfa
rin
P<0
.05
11.9
% v
s. 4
.0%
, p<0
.001
17
.6%
vs.
7.6
%, p
<0.0
01
66.5
vs.
86.
3pm
ol/L
, p<0
.041
27m
m
Hg
vs. 1
29m
mH
g -=
0.00
1980
mm
H
g vs
. 82m
mH
g, p
=0.0
02
6.2
vs. 4
.3kg
p<0
.001
p<0.
001
71.6
% v
s. 4
9.1%
p=0,
04
3.0%
vs.
7.6
%p=
0.04
8-
27%
(yr 1
) 6-
22%
(yr2
) p<
0.05
With
draw
al ra
te n
ot
repo
rted
Orli
stat
and
si
butra
min
e de
mon
stra
ted
a fa
vour
able
effi
cacy
an
d sa
fety
pro
file
in
RC
Ts.
C
urre
nt e
vide
nce
supp
orts
thei
r use
as
adju
ncts
to li
fest
yle
mod
ifica
tions
in th
e tre
atm
ent o
f obe
sity
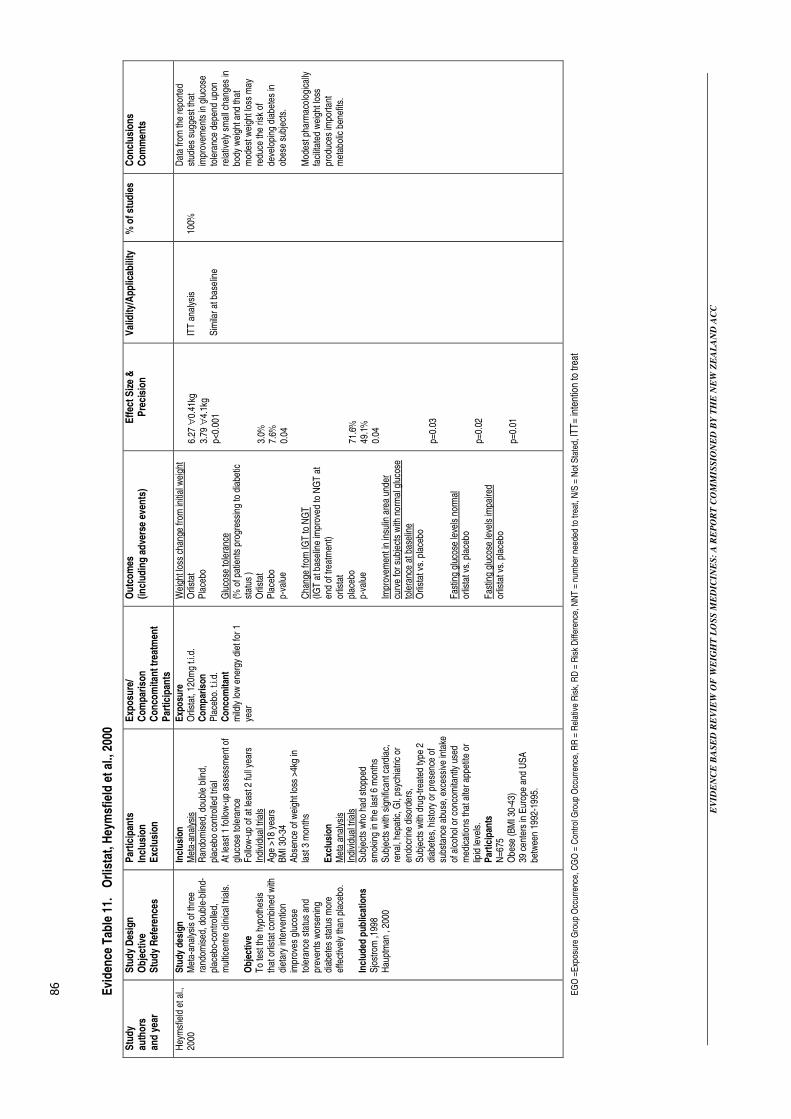
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
86
Evi
den
ce T
able
11.
O
rlis
tat,
Hey
msf
ield
et
al.,
2000
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
s
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
C
onco
mita
nt t
reat
men
t P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) E
ffec
t Siz
e &
P
reci
sion
V
alid
ity/A
pplic
abili
ty
% o
f stu
die
s C
oncl
usi
ons
C
omm
ents
Hey
msf
ield
et a
l.,
2000
S
tudy
des
ign
M
eta-
anal
ysis
of t
hree
ra
ndom
ised
, dou
ble-
blin
d-pl
aceb
o-co
ntro
lled,
m
ultic
entre
clin
ical
tria
ls.
Ob
ject
ive
To
test
the
hypo
thes
is
that
orli
stat
com
bine
d w
ith
diet
ary
inte
rven
tion
impr
oves
glu
cose
to
lera
nce
stat
us a
nd
prev
ents
wor
seni
ng
diab
etes
sta
tus
mor
e ef
fect
ivel
y th
an p
lace
bo.
Incl
uded
pub
licat
ion
s S
jost
rom
,199
8 H
aupt
man
, 20
00
Incl
usio
n
Met
a-an
alys
is
Ran
dom
ised
, dou
ble
blin
d,
plac
ebo
cont
rolle
d tri
al
At l
east
1 fo
llow
-up
asse
ssm
ent o
f gl
ucos
e to
lera
nce
Fol
low
-up
of a
t lea
st 2
full
year
s In
divi
dual
tria
ls
Age
>18
yea
rs
BM
I 30-
34
Abs
ence
of w
eigh
t los
s >4
kg in
la
st 3
mon
ths
Exc
lusi
on
Met
a an
alys
is
Indi
vidu
al tr
ials
S
ubje
cts
who
had
sto
pped
sm
okin
g in
the
last
6 m
onth
s S
ubje
cts
with
sig
nific
ant c
ardi
ac,
rena
l, he
patic
, GI,
psyc
hiat
ric o
r en
docr
ine
diso
rder
s,
Sub
ject
s w
ith d
rug-
treat
ed ty
pe 2
di
abet
es, h
isto
ry o
r pre
senc
e of
su
bsta
nce
abus
e, e
xces
sive
inta
ke
of a
lcoh
ol o
r con
com
itant
ly u
sed
med
icat
ions
that
alte
r app
etite
or
lipid
leve
ls.
Par
ticip
ants
N
=675
O
bese
(BM
I 30-
43)
39 c
ente
rs in
Eur
ope
and
US
A
betw
een
1992
-199
5.
Exp
osu
re
Orli
stat
, 120
mg
t.i.d
. C
om
par
ison
P
lace
bo. t
.i.d.
C
onc
om
itan
t m
ildly
low
ene
rgy
diet
for 1
ye
ar
Wei
ght l
oss
chan
ge fr
om in
itial
wei
ght
Orli
stat
P
lace
bo
Glu
cose
tole
ranc
e (%
of p
atie
nts
prog
ress
ing
to d
iabe
tic
stat
us )
Orli
stat
P
lace
bo
p-va
lue
Cha
nge
from
IGT
to N
GT
(IG
T a
t bas
elin
e im
prov
ed to
NG
T a
t en
d of
trea
tmen
t) or
lista
t pl
aceb
o p-
valu
e Im
prov
emen
t in
insu
lin a
rea
unde
r cu
rve
for s
ubje
cts
with
nor
mal
glu
cose
to
lera
nce
at b
asel
ine
Orli
stat
vs.
pla
cebo
F
astin
g gl
ucos
e le
vels
nor
mal
or
lista
t vs.
pla
cebo
F
astin
g gl
ucos
e le
vels
impa
ired
or
lista
t vs.
pla
cebo
6.27
∀0.
41kg
3.
79 ∀
4.1k
g p<
0.00
1 3.
0%
7.6%
0.
04
71.6
%
49.1
%
0.04
p=
0.03
p=
0.02
p=
0.01
ITT
ana
lysi
s S
imila
r at b
asel
ine
100%
Dat
a fro
m th
e re
porte
d st
udie
s su
gges
t tha
t im
prov
emen
ts in
glu
cose
to
lera
nce
depe
nd u
pon
rela
tivel
y sm
all c
hang
es in
bo
dy w
eigh
t and
that
m
odes
t wei
ght l
oss
may
re
duce
the
risk
of
deve
lopi
ng d
iabe
tes
in
obes
e su
bjec
ts.
Mod
est p
harm
acol
ogic
ally
fa
cilit
ated
wei
ght l
oss
prod
uces
impo
rtant
m
etab
olic
ben
efits
.
EG
O =
Exp
osur
e G
roup
Occ
urre
nce,
CG
O =
Con
trol
Gro
up O
ccur
renc
e, R
R =
Rel
ativ
e R
isk,
RD
= R
isk
Diff
eren
ce, N
NT
= n
umbe
r ne
eded
to tr
eat,
N/S
= N
ot S
tate
d, IT
T=
inte
ntio
n to
trea
t

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
87
Evi
den
ce T
able
12.
O
rlis
tat,
O’M
eara
et
al.,
2001
Eff
ect S
ize
& P
reci
sion
S
tud
y
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) W
eigh
ted
mea
n d
iffer
ence
†
Val
idity
/App
licab
ility
%
of
stud
ies
Com
men
ts
Con
clu
sio
ns
O’M
eara
et a
l.,
2001
S
tudy
type
O
bje
ctiv
e T
o sy
stem
atic
ally
ass
ess
the
evid
ence
for t
he
clin
ical
effe
ctiv
enes
s an
d co
st-e
ffect
iven
ess
of
orlis
tat i
n th
e m
anag
emen
t of o
besi
ty
Stu
die
s in
clud
ed
(N=1
1)
Dav
idso
n et
al.,
199
9 D
rent
& v
an d
er V
een,
19
93
Dre
nt e
t al.,
199
5 F
iner
et a
l., 2
000
Hau
ptm
an e
t al.,
200
0 H
ill e
t al.,
199
9 H
olla
nder
et a
l., 1
998
Mic
ic e
t al.,
199
9 R
ossn
er e
t al.,
200
0 S
jost
rom
et a
l., 1
998
Van
Gaa
l et a
l., 1
998
Incl
usio
n
RC
Ts
Any
dur
atio
n of
th
erap
y*
Any
leng
th o
f fo
llow
-up*
O
bese
or
over
wei
ght
patie
nts
or p
atie
nts
who
hav
e pr
evio
usly
bee
n
obes
e or
ov
erw
eigh
t wis
hing
to
mai
ntai
n w
eigh
t lo
ss.
Onl
y st
udie
s pu
blis
hed
in
Eng
lish,
Fre
nch,
D
utch
or G
erm
an
wer
e co
nsid
ered
fo
r inc
lusi
on.
Exc
lusi
on
Tria
ls re
crui
ting
peop
le w
ith e
atin
g di
sord
ers
such
as
anor
exia
ner
vosa
, an
d bu
limia
ne
rvos
a.
Orli
stat
Pri
mar
y o
utc
omes
W
eigh
t cha
nge
12 w
eeks
, 2 tr
ials
(50-
60m
g t.i
.d)
24 w
eeks
, 2 tr
ials
1-
and
2- y
ear e
ndpo
ints
(120
mg
t.i.d
) All
trial
s (n
=4)
Fro
m s
tart
of ru
n-in
per
iod
(n=2
) F
rom
dou
ble
blin
d ph
ase
(n=2
) A
t 1 y
ear (
n=2,
120
mg
t.i.d
.) A
t 2 y
ears
(n=2
, 120
mg
t.i.d
.) C
hang
e in
% o
f bod
y w
eigh
t at 2
yea
rs (n
=2,
120m
g t.i
.d.)
% w
eigh
t los
s re
lativ
e to
initi
al w
eigh
t at 2
4 w
eeks
30
mg
orlis
tat t
.i.d.
60
mg
orlis
tat t
.i.d.
12
0mg
orlis
tat t
.i.d.
24
0mg
orlis
tat t
.i.d.
P
lace
bo
% o
f pat
ient
s lo
sing
>10
% o
f bod
y w
eigh
t at
24 w
eeks
(n=2
), 30
mg
orlis
tat t
.i.d.
60
mg
orlis
tat t
.i.d.
12
0mg
orlis
tat t
.i.d.
24
0mg
orlis
tat t
.i.d.
P
lace
bo
Red
uctio
n in
wai
st c
ircum
fere
nce
at 2
4 w
eeks
(n=2
) 30
mg
orlis
tat t
.i.d.
60
mg
orlis
tat t
.i.d.
12
0mg
orlis
tat t
.i.d.
24
0mg
orlis
tat t
.i.d.
P
lace
bo
RR
of f
ailu
re to
ach
ieve
at l
east
5%
loss
of
initi
al w
eigh
t at 1
yea
r (or
lista
t, 12
0mg
t.i.d
, n=
4)
RR
of f
ailu
re to
ach
ieve
at l
east
10%
loss
of
initi
al w
eigh
t at 1
yea
r (or
lista
t, 12
0mg
t.i.d
, n=
5)
RR
of f
ailu
re to
ach
ieve
at l
east
10%
loss
of
initi
al w
eigh
t at 2
yea
r (or
lista
t, 12
0mg
t.i.d
, n=
3)
-1.2
4kg
(-2.
65 to
0.1
6), p
=0.0
8 -1
0.75
kg o
rlist
at, -
7.34
pla
cebo
-2
.9kg
(-3.
61 to
– 2
.19)
p=<
0.00
001
-2.4
kg(-
3.62
to –
1.47
), p<
0.00
001
-3.3
5kg(
-4.4
4 to
–2.
27),
p<0.
0000
1 -2
.38k
g (-
3.45
to –
1.31
) ,p<
0.00
001
-3.1
9kg(
-4.2
5 to
– 2
.12)
, p=0
.000
01
-3.2
3kg
(-4.
77 to
–1.
69),
p=0.
0000
1
8.5%
8.
8%
9.8%
9.3%
6.
6%
28%
28
%
37%
38
%
19%
3.
5cm
5.
1cm
5.
9cm
6.
3cm
6.
0cm
R
R=0
.72
(0.6
3-0.
82),
p<0.
0000
1
RR
=0.8
5 (0
.80-
0.91
), p<
0.00
001
RR
=0.8
6(0.
79-0
.93)
, p=0
.000
1
Ran
dom
ised
met
hod
desc
ribed
(n=1
1)
Con
ceal
ed ra
ndom
isat
ion
Sim
ilar a
t bas
elin
e,
Pat
ient
s bl
inde
d C
arer
s bl
inde
d B
lind
outc
ome
asse
ssm
ent
Inte
ntio
n to
trea
t ana
lysi
s P
atie
nt a
dher
ence
ass
esse
d W
ithdr
awal
s re
porte
d S
elec
tion
crite
ria
9%
100%
10
0%
100%
U
ncle
ar
9%, 9
1%
82%
91
%
100%
10
0%
In g
ener
al th
e m
etho
dolo
gica
l qua
lity
of
the
trial
s w
as m
oder
ate
to g
ood.
T
he o
ptim
um re
gim
en
was
120
mg
t.i.d
. M
ost t
rials
wer
e si
ngle
bl
ind,
pla
cebo
with
a ru
n-in
per
iod
prio
r to
doub
le
blin
d tri
al.
The
re is
a la
ck o
f in
form
atio
n on
the
effe
ctiv
enes
s an
d sa
fety
of
orli
stat
in o
lder
peo
ple.
F
or o
rlist
at tr
ials
that
m
atch
ed th
e pr
escr
ibin
g gu
idel
ines
mos
t rep
orte
d st
atis
tical
ly s
igni
fican
t re
sults
in fa
vour
of
orlis
tat f
or w
eigh
t los
s in
pa
rtici
pant
s w
ith a
nd
with
out d
iabe
tes.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
88
Evi
den
ce T
able
12.
Orl
ista
t, O
’Mea
ra e
t al
., 20
01 (
con
tin
ued
)
** m
anuf
actu
rer’s
tria
ls h
ad to
hav
e du
ratio
n of
at l
east
1 y
ear.
Eff
ect S
ize
& P
reci
sion
S
tud
y au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) W
eigh
ted
mea
n
diff
eren
ce†
N
NT
V
alid
ity/A
pplic
abili
ty
% o
f st
udie
s C
oncl
usi
ons
C
omm
ents
O’M
eara
et a
l.,
2001
(Con
t)
Ad
vers
e ev
ents
G
astro
inte
stin
al a
dver
se
even
ts: f
atty
sto
ols,
incr
ease
d de
feca
tion,
oily
spo
tting
. Lo
wer
ser
um le
vels
of f
at-
solu
ble
vita
min
s.
Eco
nom
ic e
valu
atio
n
Incr
emen
tal c
ost-u
tility
of
orlis
tat t
reat
men
t per
QA
LY
gain
ed fo
r WL
of 3
-4%
dur
ing
first
yea
r of t
reat
men
t.
Mor
e fre
quen
t in
orlis
tat g
roup
G
BP
45,
881
(19,
452-
55,3
91)

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
89
Evi
den
ce T
able
13.
O
rlis
tat,
Pad
wal
et
al.,
2004
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
/Typ
e O
bje
ctiv
e S
tud
y R
efer
ence
s
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) E
ffec
t Siz
e &
Pre
cisi
on
Val
idity
/App
licab
ility
%
of
stud
ies
Con
clu
sio
ns
Com
men
ts
Pad
wal
et a
l.,
2004
C
och
rane
Sys
tem
atic
R
evie
w
Ob
ject
ive
To
asse
ss/c
ompa
re th
e ef
fect
s an
d sa
fety
of
sing
le o
r com
bina
tion
anti-
obes
ity d
rug
ther
apy
in c
linic
al tr
ials
of a
t le
ast o
ne y
ear
11 tr
ials
6,
021
parti
cipa
nts
Incl
uded
stu
die
s H
olla
nder
et a
l., 1
998
Sjo
stro
m e
t al.,
199
8 D
avid
son
et a
l., 1
999
Fin
er e
t al.,
200
0 H
aupt
man
et a
l., 2
000
Lind
gard
e et
al.,
200
0 R
ossn
er e
t al.,
200
0 B
akris
et a
l., 2
002
Bro
om e
t al.,
200
2 K
elle
y et
al.,
200
2 M
iles
et a
l., 2
002
Incl
usio
n
BM
I ≥ 3
0kg/
m2
stud
y le
ngth
≥ 1
yr
rand
omis
ed
doub
le-b
lind
plac
ebo
or a
ctiv
e co
ntro
l S
ix tr
ials
requ
ired
a co
mpl
ianc
e ra
te o
f >7
5% in
the
run-
in
phas
e E
xclu
sion
O
besi
ty o
f end
ocrin
e or
igin
, di
abet
es m
ellit
us,
treat
men
t with
m
edic
atio
n th
at m
ay
alte
r bod
y w
eigh
t, un
cont
rolle
d hy
perte
nsio
n
Dru
g; O
rlist
at
Dos
e; 1
20m
g t.i
.d
Co
-inte
rven
tions
Lo
w fa
t hyp
ocal
oric
die
t (8
stud
ies)
D
ieta
ry c
ouns
ellin
g E
xerc
ise
coun
selli
ng
Foo
d in
take
dia
ries
Edu
catio
nal l
itera
ture
or
vide
os
Av
BM
I = 3
3.4k
g/m
2
Av
wei
ght =
96k
g A
v ag
e =
47 y
ears
80
% fe
mal
e 75
% C
auca
sian
H
igh
ris
k po
pula
tions
S
ix tr
ials
lim
ited
enro
llmen
t to
hig
her r
isk
patie
nts,
3
with
type
2 d
iabe
tes
on
stab
le d
oses
of o
ral
hypo
glyc
emic
age
nts
or
insu
lin, 3
with
at l
east
one
ad
ditio
nal C
VD
risk
fact
or
(hyp
erte
nsio
n,
dysl
ipid
emia
, typ
e 2
diab
etes
IGT
).
Pri
mar
y o
utc
omes
av
erag
e w
eigh
t los
s in
kg
av
erag
e w
eigh
t los
s as
% c
hang
e fro
m b
asel
ine
% w
ith w
eigh
t los
s >=
5%
%
with
wei
ght l
oss
>=10
%
tota
l pop
ulat
ion
high
risk
gro
up
low
risk
gro
up
Com
para
tive
BM
I red
uctio
n C
ompa
rativ
e w
aist
circ
umfe
renc
e re
duct
ion
for
Orli
stat
(5 tr
ials
, not
poo
led,
p<0
.05
in 4
of 5
st
udie
s)
Sec
ond
ary
outc
omes
(1
0 tri
als)
T
otal
cho
lest
erol
redu
ctio
n gr
eate
r in
orlis
tat
grou
p Lo
w-d
ensi
ty li
popr
otei
n re
duct
ion
grea
ter i
n or
lista
t gro
up (8
tria
ls)
HD
L re
duct
ion
high
er in
orli
stat
gro
up (
7 tri
als)
T
rigly
cerid
e le
vels
redu
ctio
n gr
eate
r in
orlis
tat
grou
p S
BP
net
dec
reas
e (9
tria
ls)
SB
P n
et in
crea
se (2
tria
ls)
DB
P n
et d
ecre
ase
(8 tr
ials
) F
astin
g pl
asm
a gl
ucos
e re
duct
ions
(9 tr
ials
, si
gnifi
cant
ly d
iffer
ent t
o pl
aceb
o in
5 tr
ials
) H
bA1c
redu
ctio
n (4
tria
ls, h
igh
risk
patie
nts)
A
dve
rse
even
ts
Incr
ease
d in
orli
stat
gro
up:
fatty
/oily
sto
ol a
nd o
ily s
potti
ng
faec
al u
rgen
cy (9
tria
ls)
Fae
cal i
ncon
tinen
ce in
crea
se
2.
7(2.
3-3.
1)
2.9(
2.3-
3.4)
21
(19-
24)
12(8
-16)
8(
5-10
) 17
(14-
21)
0.7-
3.4c
m
0.33
mm
ol/L
(0.2
8-0.
38)
0.27
mm
ol/L
(0.2
2-0.
31)
0.
02m
mol
/L (0
.01-
0.04
)
0.05
mm
ol/L
(0.0
7gai
n–0.
17
loss
) 1.
8mm
Hg
(0.9
-2.6
) 0.
4mm
Hg
(NS
) 1.
6mm
Hg
(0.7
-2.4
) 0.
1-1.
3 m
mol
/L
0.2%
(0.2
-0.3
)
16
-40%
6%
(5-8
%)
Ran
dom
ised
/allo
catio
n co
ncea
lmen
t met
hod
desc
ribed
S
imila
r at b
asel
ine
ITT
last
obs
erva
tion
carr
ied
forw
ard
Dou
ble
blin
d B
lind
outc
ome
asse
ssm
ent
Ave
rage
dro
p-ou
t rat
e
18%
55
%
0%*
100%
N
R
33%
(1
4-52
)
Bas
elin
e w
eigh
t was
ca
lcul
ated
from
the
star
t of t
he
run
in p
erio
d ra
ther
than
the
poin
t of r
ando
mis
atio
n –
infla
ting
the
abso
lute
cha
nge
in w
eigh
t. H
igh
attri
tion
rate
s w
ere
the
maj
or m
etho
dolo
gica
l lim
itatio
n.
Is th
e de
gree
of w
eigh
t los
s ac
hiev
ed o
f clin
ical
ben
efit?
It
may
be,
par
ticul
arly
for h
igh-
risk
grou
ps b
ut m
ore
defin
itive
da
ta a
re n
eede
d. W
eigh
t re
duct
ion
of 5
-10%
of b
ody
wei
ght i
s as
soci
ated
with
im
prov
emen
ts in
blo
od
pres
sure
, lip
id a
nd g
luco
se
para
met
ers
but d
ata
on th
e ef
fect
of m
orta
lity
and
card
iova
scul
ar e
vent
s ar
e la
ckin
g.
All
stud
ies
show
ed a
pos
itive
tre
atm
ent e
ffect
. How
ever
pu
blic
atio
n bi
as c
anno
t be
rule
d ou
t. T
he p
atie
nt p
opul
atio
n st
udie
s re
pres
ent a
hig
hly
sele
cted
gr
oup
of re
lativ
ely
heal
thy
obes
e pa
tient
s w
ho w
ere
able
to
com
ply
with
stu
dy d
iet a
nd
med
icat
ion
requ
irem
ent.
Mos
t of
the
patie
nts
wer
e fe
mal
e C
auca
sian
s. E
xtra
pola
tion
to
patie
nts
with
diff
eren
t de
mog
raph
ic p
rofil
e m
ust b
e m
ade
with
cau
tion.
N
ote
:
Leve
ls o
f fat
-sol
uble
vita
min
s A
, D, E
and
bet
a-ca
rote
ne
wer
e re
port
ed a
s lo
wer
ed in
th
e or
lista
t gro
up.
* al
l tria
ls h
ampe
red
by a
hig
h at
triti
on r
ate
of 1
4-52
%, a
vera
ge 3
3%

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
90
Evi
den
ce T
able
14.
S
ibu
tram
ine,
O’M
eara
et
al.,
2002
Eff
ect S
ize
& P
reci
sion
S
tud
y au
tho
rs
and
yea
r
Stu
dy
Des
ign
/Typ
e O
bje
ctiv
e S
tud
y R
efer
ence
s
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) W
eigh
ted
mea
n d
iffer
ence
, RR
Val
idity
/App
licab
ility
%
of
stud
ies
Con
clu
sio
ns
Com
men
ts
O’M
eara
et
al.,
2002
S
tudy
type
N
ICE
HD
L O
bje
ctiv
e T
o sy
stem
atic
ally
ass
ess
the
evid
ence
for t
he
clin
ical
effe
ctiv
enes
s an
d co
st-e
ffect
iven
ess
of
sibu
tram
ine
in th
e m
anag
emen
t of o
besi
ty
Stu
die
s in
clud
ed
(N=1
1)
Apf
elba
um e
t al.,
199
9 B
ray
et a
l., 1
999
Cue
llar e
t al.,
200
0 F
angh
anel
et a
l., 2
000
Fin
er e
t al.,
200
0 F
ujio
ka e
t al.,
200
0 H
anot
in e
t al.,
199
8 H
anse
n et
al.,
199
9 S
eagl
e et
al.,
199
8 W
alsh
et a
l., 1
999
Wei
ntra
ub e
t al.,
199
1 S
tud
ies
from
the
man
ufa
ctu
rer
(N=5
)*
Wirt
h et
al.,
199
8 S
mith
et a
l., 1
994
Jam
es e
t al.,
199
9 R
issa
n et
al.,
199
8 W
illia
ms
ey a
l., 1
999
* m
anuf
actu
rer’s
tria
ls
had
to h
ave
a du
ratio
n of
at
leas
t 1 y
ear
Incl
usio
n
RC
Ts
Any
dur
atio
n of
ther
apy
Any
leng
th o
f fol
low
-up
Obe
se o
r ove
rwei
ght p
atie
nts
or
patie
nts
who
hav
e pr
evio
usly
bee
n
obes
e or
ove
rwei
ght w
ishi
ng to
mai
ntai
n w
eigh
t los
s.
Onl
y st
udie
s pu
blis
hed
in E
nglis
h,
Fre
nch,
Dut
ch o
r Ger
man
wer
e co
nsid
ered
for i
nclu
sion
. E
xclu
sion
T
rials
recr
uitin
g pe
ople
with
eat
ing
diso
rder
s su
ch a
s an
orex
ia n
ervo
sa,
and
bulim
ia n
ervo
sa.
Sib
utra
min
e 5-
30m
g/d
Pri
mar
y o
utc
omes
W
eigh
t cha
nge
8 w
eeks
(3 tr
ials
, 10-
20m
g/d)
24
wee
ks (4
tria
ls, 1
0mg/
d)
1 ye
ar
RR
of f
ailu
re to
ach
ieve
a w
eigh
t lo
ss o
f at l
east
5%
of i
nitia
l bod
y w
eigh
t at 2
4 w
eeks
– 2
tria
ls
(10m
g/d)
. Not
e fo
r 15m
g/d
dose
si
gnifi
cant
het
erog
enei
ty w
as
obse
rved
. F
at c
onte
nt
Fat
-free
mas
s lo
ss a
t eig
ht w
eeks
(2
tria
ls, s
ibut
ram
ine)
F
at c
hang
e at
eig
ht w
eeks
(2
trial
s, s
ibut
ram
ine)
A
dve
rse
even
ts
Pul
se ra
te, b
lood
pre
ssur
e an
d he
art r
ate
H
eada
ches
, sle
ep d
iffic
ulty
, irr
itabi
lity
Man
ufa
ctu
rer’
s co
st u
tility
an
alys
is (B
MI<
30kg
/m2 ,
free
of
com
plic
atio
ns a
nd c
o-m
orbi
ditie
s,
no w
eigh
t los
s su
stai
ned
at 5
6 ye
ars,
cos
ts d
isco
unte
d at
6%
, be
nefit
s at
1.5
%))
Q
oL c
oeffi
cien
t for
sib
utra
min
e C
ost p
er Q
ALY
gai
ned
thro
ugh
CH
D re
duct
ion
Cos
t per
QA
LY g
aine
d th
roug
h di
abet
es in
cide
nce
Est
imat
ed c
ost p
er Q
ALY
B
est-w
orse
cas
e sc
enar
io
-3.4
kg (4
.22
to –
2.58
) p<0
.000
01
-4.0
to 9
.1kg
-4
.1 to
–4.
8kg
RR
=0.4
8 (0
.39-
0.60
), p<
0.00
001
-1.8
3kg(
-2.4
8 to
–1.
19)p
<0.0
0001
-1
.77k
g (-
2.58
-0.9
6) p
<0.0
0002
S
mal
l but
sig
nific
ant i
ncre
ase
with
si
butra
min
e, n
ot c
onsi
dere
d to
be
clin
ical
ly s
igni
fican
t. R
epor
ted
in o
ne s
mal
l tria
l. 0.
0018
5/kg
lost
£4
2,00
0 £7
7,00
0 £1
0,50
0 (£
5,70
00-£
35,0
00)
Ran
dom
ised
met
hod
desc
ribed
(n
=16)
C
once
aled
rand
omis
atio
n S
imila
r at b
asel
ine,
man
ufac
ture
rs
trial
s (n
=5),
othe
r tria
ls (N
=11)
P
atie
nts
blin
ded
Car
ers
blin
ded
Blin
d ou
tcom
e as
sess
men
t In
tent
ion
to tr
eat a
naly
sis
Pat
ient
adh
eren
ce a
sses
sed
With
draw
als
repo
rted
Sel
ectio
n cr
iteria
19%
10
0%
0%
100%
10
0%
uncl
ear
uncl
ear
69%
50
%
94%
10
0%
Man
y of
the
trial
s de
mon
stra
ted
a st
atis
tical
ly s
igni
fican
t di
ffere
nce
in fa
vour
of
sibu
tram
ine
in te
rms
of
(a) a
bsol
ute
wei
ght
loss
(b) %
of p
atie
nts
achi
evin
g at
leas
t 5%
or
10%
loss
of i
nitia
l bo
dy w
eigh
t. T
he d
iffer
ence
s w
ere
smal
l and
may
not
be
clin
ical
ly im
porta
nt.
Wei
ght l
oss
seem
s to
be
dos
e re
late
d w
ith
stat
istic
ally
sig
nific
ant
resu
lts re
porte
d fo
r 10-
20m
g do
ses
of
sibu
tram
ine.
B
etw
een
grou
p di
ffere
nce
in B
P, l
ipid
s le
vels
and
gly
caem
ic
cont
rol w
ere
inco
nsis
tent
.
EG
O =
Exp
osur
e G
roup
Occ
urre
nce,
CG
O =
Con
trol
Gro
up O
ccur
renc
e, R
R =
Rel
ativ
e R
isk,
RD
= R
isk
Diff
eren
ce, N
NT
= n
umbe
r ne
eded
to tr
eat,
N/S
= N
ot S
tate
d N
SD
no
sign
ifica
nt d
iffer
ence
, NS
= n
ot s
igni
fican
t ‡i
ndiv
idua
lly s
igni
fican
t dat
a no
t poo
led.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
91
Evi
den
ce T
able
15.
S
ibu
tram
ine,
Tam
bas
cia
et a
l., 2
003
Eff
ect S
ize
& P
reci
sion
S
tud
y/Y
ear
Loc
atio
n
Stu
dy
Des
ign
O
bje
ctiv
e D
ura
tion
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
P
S
Val
idity
/App
licab
iilty
C
oncl
usi
ons
C
omm
ents
Tam
basc
ia e
t al
., 2
003
Loc
atio
n
Bra
zil
Stu
dy D
esig
n
Ran
dom
ised
, P
lace
bo-c
ontro
lled,
dou
ble
blin
d cl
inic
al tr
ial
Ru
n in
per
iod
N
one
repo
rted
Ob
ject
ive
To
asse
ss th
e ef
fect
of
sibu
tram
ine
assi
sted
wei
ght
redu
ctio
n on
insu
lin s
ensi
tivity
an
d m
etab
olic
par
amet
ers
in
obes
e, n
orm
al g
luco
se
tole
rant
indi
vidu
als
over
a
perio
d of
24
wee
ks.
Du
ratio
n
24 w
eeks
Par
ticip
ants
N
=48
recr
uite
d N
=40
rand
omis
ed
N=3
1 co
mpl
eter
s H
ealth
y ob
ese,
fem
ale
volu
ntee
rs
Age
=41
.1±
9.9
year
s
Age
-ran
ge =
19-5
8 ye
ars
BM
I=34
.3±
2.9k
g/m
2 In
clus
ion
B
MI=
30-4
0kg/
m2
Exc
lusi
on
Psy
chia
tric
inst
abili
ty, h
isto
ry o
f an
ti-ob
esity
sur
gery
, rec
ent
chan
ge in
exe
rcis
e pa
ttern
, sm
okin
g ce
ssat
ion
with
in 6
m
onth
s, h
yper
tens
ion,
his
tory
of
CH
D, c
ardi
ac a
rrhy
thm
ia,
endo
crin
e di
sord
ers
incl
udin
g ty
pe 2
dia
bete
s an
d gl
ucos
e in
tole
ranc
e, h
isto
ry o
f dru
g or
al
coho
l abu
se, u
se o
f ant
i-de
pres
sant
age
nts,
mon
oam
ine
oxid
ase
inhi
bito
rs a
nd u
se o
f dr
ugs
that
affe
ct in
sulin
se
nsiti
vity
(cor
ticoi
ds, d
iure
tics,
in
sulin
sen
sitis
ers,
oes
troge
n re
plac
emen
t. F
emal
es w
ere
requ
ired
to h
ave
a ne
gativ
e se
rum
pre
gnan
cy te
st,
to b
e po
st m
enop
ausa
l, su
rgic
ally
ste
rilis
ed o
r usi
ng a
m
edic
ally
acc
epte
d co
ntra
cept
ive
met
hod.
Exp
osu
re
Sib
utra
min
e 10
mg/
d +
diet
ary
advi
ce fr
om o
bese
cl
inic
C
om
par
ison
P
lace
bo +
die
t adv
ice
from
ob
ese
clin
ic
Wei
gh
t los
s at
24
wee
ks
Wei
ght l
oss
(kg)
W
eigh
t los
s (%
) F
at m
ass
(%)
Dia
bet
ic m
etab
olic
par
amet
ers
at 2
4 w
eeks
G
luco
se (m
g/dl
) T
rigyl
cerid
es
Insu
lin (:
U/m
l) H
OM
A-IR
H
OM
A-≥
K
itt
Blo
od p
ress
ure
at 2
4 w
ks
SB
P m
mH
g D
BP
mm
Hg
Hea
rt ra
te (b
pm)
Lip
id p
rofil
e at
24
wee
ks
Tot
al c
hole
ster
ol
HD
L-ch
oles
tero
l LD
L-ch
oles
tero
l A
nth
rop
omo
rph
ic in
dic
es
Wai
st c
ircum
fere
nce
cm
Ad
vers
e ev
ents
S
ibut
ram
ine
= an
orex
ia, d
ry m
outh
and
na
usea
. S
erio
us
adve
rse
even
ts
Car
diac
arr
hyth
mia
=1
(sib
utra
min
e)
+0
.9
1.2
+0.4
0.
0 -8
.0
+4.6
+0
.8
+51
+0.1
9 +4
.0
+1.0
+2
.0
-8.0
-1
.0
-5.0
+1.0
-5
.6
-6.1
-1
.6
-2.0
-4
0.0
-9.3
-2
.2
-134
+1
.06
-5.0
-5
.0
+5.0
-8
.0
+2.0
-2
.0
-4.0
An
alys
is
Com
plia
nce
test
s –
pill
coun
ting
Com
plet
ers
anal
ysis
- an
alys
is p
er p
roto
col
Onl
y di
ffere
nce
from
ba
selin
e co
mpu
ted
for
each
trea
tmen
t se
para
tely
. P
ropo
rtion
of p
artic
ipan
ts
>=5%
and
10%
wei
ght
loss
not
repo
rted
Rea
son
s fo
r d
isco
ntin
uat
ion
A
dver
se e
vent
=1
Pre
gnan
cy=1
P
roto
col
devi
atio
n=3(
1S+2
P)
Lack
of e
ffica
cy=4
(1
S+3
P)
Ext
ern
al v
alid
ity
100%
fem
ale
very
larg
e nu
mbe
r of
excl
usio
n cr
iteria
Stu
dy c
onc
lusi
ons
The
aut
hors
con
clud
ed th
at
sibu
tram
ine
had
dem
onst
rate
d ef
ficac
y in
redu
cing
wei
ght i
n no
n-di
abet
ic fe
mal
es a
nd
amel
iora
ted
insu
lin s
ensi
tivity
pa
ram
eter
s an
d ot
her m
etab
olic
pa
ram
eter
s.
Co
mm
ents
W
eak
anal
ysis
Le
ss th
an 2
0 pe
r gro
up
No
form
al d
ieta
ry in
terv
entio
n or
be
havi
our m
odifi
catio
n pr
ogra
m
Sib
utra
min
e no
t adm
inis
tere
d as
pe
r lic
ence
.
HO
MA
-IR
, HO
MA
-≥ a
nd K
ittar
e in
sulin
sen
sitiv
ity te
sts,
BM
P =
bea
ts p
er m
inut
es, P
=pla
cebo
, S=s
ibut
ram
ine.
Bo
ld fi
gure
s =
sig
nific
ant d
iffer
ence
.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
92
Evi
den
ce T
able
16.
S
ibu
tram
ine,
Pad
wal
et
al.,
2004
Eff
ect S
ize
& P
reci
sion
S
tud
y au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) W
eigh
ted
mea
n
diff
eren
ce †
Val
idity
/App
licab
ility
%
of
stud
ies
Con
clu
sio
ns
Com
men
ts
Pad
wal
et a
l.,
2004
C
och
rane
S
yste
mat
ic R
evie
w
To
asse
ss/c
ompa
re
the
effe
cts
and
safe
ty
of s
ingl
e or
co
mbi
natio
n an
ti-ob
esity
dru
g th
erap
y in
clin
ical
tria
ls o
f at
leas
t one
yea
r M
cMah
on e
t al 2
000
Sm
ith e
t al 2
001
McM
ahon
et a
l 200
2
Incl
usio
n
BM
I ≥ ≥≥≥ 3
0kg
/m2
stud
y le
ngth
≥1
yr
rand
omis
ed
doub
le b
lind
plac
ebo
or a
ctiv
e co
ntro
l R
ando
mis
atio
n re
stric
ted
to
patie
nts
who
cou
ld fo
llow
di
etar
y ad
vice
or h
ad 7
5%
com
plia
nce
durin
g th
e ru
n-in
ph
ase.
E
xclu
sion
O
besi
ty o
f end
ocrin
e or
igin
, di
abet
es m
ellit
us, t
reat
men
t w
ith m
edic
atio
n th
at m
ay
alte
r bod
y w
eigh
t, un
cont
rolle
d hy
perte
nsio
n N
ote:
one
tria
l exc
lude
d be
caus
e 36
% o
f ran
dom
ised
pa
tient
s w
ere
not i
nclu
ded
in
the
anal
ysis
. D
uplic
ate
popu
latio
ns
Sib
utr
amin
e 15
-20m
g d
aily
C
o-in
terv
entio
ns =
3
trial
s (2
US
A, 1
UK
) 929
pa
rtici
pant
s A
v B
MI 3
3.4k
g/m
2
Av
wei
ght 9
6kg
Av
age
47 y
ears
80
% fe
mal
e 75
% C
auca
sian
2
trial
s lim
ited
enro
llmen
t to
obes
e hy
perte
nsiv
e pa
tient
s w
ith w
ell c
ontro
lled
BP
, in
the
rem
aini
ng tr
ial o
nly
*% h
ad a
tre
ated
car
diov
ascu
lar c
ondi
tion
Pri
mar
y o
utc
omes
av
erag
e w
eigh
t los
s in
kg
av
erag
e w
eigh
t los
s %
cha
nge
from
bas
elin
e %
of p
atie
nts
with
wei
ght l
oss
of le
ast 5
%
% o
f pat
ient
s w
ith w
eigh
t los
s of
at l
east
10%
C
ompa
rativ
e B
MI r
educ
tion
Wai
st c
ircum
fere
nce
redu
ctio
n S
econ
dar
y ou
tcom
es
Impr
oved
blo
od g
luco
se le
vels
(2 s
tudi
es)
sibu
tram
ine
treat
ed p
atie
nts
Trig
lyce
rides
leve
ls lo
wer
in s
ibut
ram
ine
arm
T
otal
cho
lest
erol
Lo
w-d
ensi
ty li
popr
otei
n H
DL
high
er in
sib
utra
min
e st
udie
s (n
=2)
Ad
vers
e E
ven
ts
(Sib
utra
min
e)
Sys
tolic
blo
od p
ress
ure
net i
ncre
ase
1.9m
mH
g (0
.2-3
.6)‡
.Dia
stol
ic b
lood
‡
pres
sure
1-4
mm
Hg
Pul
se ra
te in
crea
se 4
-6 b
eats
per
min
(p
=<0.
05)
Oth
er A
Es
mo
re c
om
mon
in s
ibu
tram
ine
arm
In
som
nia
Nau
sea
Dry
mou
th
Con
stip
atio
n
4.
3(3.
6-4.
9)
4.6(
3.8-
5.4)
34
(28-
40)
15(4
-27)
1.
5kg/
m2
(1.2
-1.8
) 4-
5cm
0.08
and
0.9
mm
ol/L
(NS
) 0.
18-0
.23
mm
ol/L
(p
<0.0
5)
NS
D
NS
D
0.08
-0.0
9mm
ol/L
(p
=<0.
05)
7-
20%
Ran
dom
ised
met
hod
desc
ribed
S
imila
r at b
asel
ine
Inte
ntio
n to
trea
t las
t obs
erva
tion
carr
ied
forw
ard
Dou
ble
blin
d B
lind
outc
ome
asse
ssm
ent
Com
plia
nce
D
rop-
outs
<20%
33
67
100
10
0 N
R
NR
Y
es (4
3%)
Het
erog
enei
ty in
pr
imar
y ou
tcom
es
cons
ider
ed to
be
of
negl
igib
le c
linic
al
rele
vanc
e. S
tratif
ying
in
to h
igh
and
low
risk
st
udy
popu
latio
ns
elim
inat
ed o
bser
ved
hete
roge
neity
.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
93
Evi
den
ce T
able
17.
S
ibu
tram
ine,
Leu
ng
et
al.,
2003
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
Eff
ect S
ize
& P
reci
sion
V
alid
ity/A
pplic
abili
ty
% o
f stu
die
s C
oncl
usi
ons
C
omm
ents
Leun
g et
al.,
20
03
Stu
dy ty
pe
Sys
tem
atic
revi
ew
Ob
ject
ive
To
desc
ribe
the
phar
mac
olog
ic
man
agem
ent o
f ob
esity
co
ncen
tratin
g on
si
butra
min
e In
clud
ed s
tud
ies
Sib
utra
min
e A
pfel
baum
, 199
9 C
uelle
r, 20
00
Duj
ovne
, 200
1 F
angh
anel
, 200
0 F
angh
anel
, 20
01
Fuj
ioka
, 200
0 Ja
mes
, 200
0 M
cMah
on, 2
000
Sm
ith, 2
001
Wirt
h, 2
001
Incl
usio
n
Stu
dies
bet
wee
n 19
66-F
ebru
ary
2002
R
CT
s of
> 6
m
onth
s du
ratio
n re
porti
ng th
e ef
ficac
y of
S
ibut
ram
ine
Exp
osu
re
Sib
utra
min
e 1-
30m
g t.i
.d.
Co
mp
aris
on
Pla
cebo
Do
se r
elat
ed w
eigh
t lo
ss a
t 6 m
onth
s S
ibut
ram
ine
1mg
5mg
10m
g 30
mg
Pla
cebo
M
eta
anal
ysis
of 4
long
-ter
m tr
ials
W
aist
circ
umfe
renc
e re
duce
d (s
ibut
ram
ine)
W
aist
hip
ratio
redu
ced
(sib
utra
min
e)
Wei
gh
t los
s g
reat
er in
trea
tmen
t gro
up
than
p
lace
bo
gro
up fo
r T
ype
2 di
abet
es m
ellit
us
Dys
lipid
emia
H
yper
tens
ion
Gre
ater
red
uctio
ns
with
sib
utr
amin
e vs
. pla
cebo
F
astin
g H
bA1c
and
glu
cose
leve
ls, s
erum
trig
lyce
rides
hi
gh d
ensi
ty li
popr
otei
n, c
hole
ster
ol, u
rate
, C-p
eptid
e In
sulin
A
dve
rse
even
ts
Dry
mou
th, a
nore
xia,
inso
mni
a, c
onst
ipat
ion,
hea
dach
e B
lood
pre
ssur
e, s
ibut
ram
ine
vs. p
lace
bo
Hea
rt ra
te, s
ibut
ram
ine
vs. p
lace
bo
2.
5%
3.9%
6.
1% p
<0.0
5 9.
4%
1.2%
p<0.
001
p<0.
02
p<
0.00
1 p<
0.05
p<
0.05
p<0
.05
p<
0.00
1 p<
0.00
1 1-
3mm
Hg
(mea
n in
crea
se)
4-5
beat
s/m
in (m
ean
incr
ease
)
Ove
rall
with
dra
wal
ra
tes
S
ibut
ram
ine
Pla
cebo
D
isco
ntin
uatio
n d
ue
to
hyp
erte
nsi
on
Sib
utra
min
e P
lace
bo
Dis
con
tinua
tion
du
e to
ta
chyc
ard
ia
Sib
utra
min
e P
lace
bo
No
qual
ity a
sses
smen
t w
as re
porte
d
9%
7%
0.4%
0.
4%
0.4%
0.
1%
Co
nclu
sion
O
rlist
at a
nd s
ibut
ram
ine
dem
onst
rate
d a
favo
urab
le e
ffica
cy
and
safe
ty p
rofil
e in
RC
Ts.
Cur
rent
ev
iden
ce s
uppo
rts th
eir u
se a
s ad
junc
ts to
life
styl
e m
odifi
catio
ns in
th
e tre
atm
ent o
f obe
sity
N
ote
: In
Mar
ch 2
002
the
Italia
n H
ealth
Min
istry
sus
pend
ed s
ales
of
sibu
tram
ine
for r
e-ev
alua
tion
of it
s sa
fety
pro
file
afte
r 2 d
eath
s an
d 50
ad
vers
e ev
ents
. Afte
r inv
estig
atio
n th
e E
AE
MP
(Jun
e 20
02) r
epor
ted
that
th
e ris
k-be
nefit
pro
file
of s
ibut
ram
ine
rem
aine
d po
sitiv
e.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
94
Evi
den
ce T
able
18.
S
ibu
tram
ine,
Nis
oli
and
Car
rub
a, 2
003
S
tud
y au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e In
clud
ed S
tud
ies
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
P
artic
ipan
ts
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
)
Adv
erse
Eve
nt
S
P
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Nis
oli a
nd
Car
ruba
, 200
3 S
tudy
des
ign
S
yste
mat
ic R
evie
w o
f all
trial
s of
sib
utra
min
e re
porti
ng u
nwan
ted
side
ef
fect
s of
sib
utra
min
e O
bje
ctiv
e A
ben
efit-
risk
asse
ssm
ent
of s
ibut
ram
ine
in th
e m
anag
emen
t of o
besi
ty
Incl
uded
stu
die
s H
anse
n et
al.,
199
8 W
alsh
et a
l., 1
999
Jam
es e
t al.,
200
0 A
pfel
baum
et a
l., 1
999
Kno
ll 20
00
Kno
ll200
0 K
noll
2000
M
cNul
ty e
t al.,
200
3 B
ray
et a
l., 1
999
Fan
ghan
el e
t al.,
200
0 C
uelle
r et a
l., 2
000
Fuj
ioka
et a
l., 2
000
Gok
cel e
t al.,
200
1 S
erra
no-R
ios
et a
l., 2
002
Han
otin
et a
l., 1
998
Fin
er e
t al.,
200
0 H
anot
in e
t al.,
199
8 W
eint
aub
et a
l., 1
991
Sea
gle
et a
l., 1
998
Incl
usio
n
All
clin
ical
tria
ls o
f sib
utra
min
e fo
r w
eigh
t man
agem
ent i
n ov
erw
eigh
t or
obes
e su
bjec
ts re
porti
ng u
nwan
ted
side
effe
cts
of s
ibut
ram
ine
Exp
osu
re
Sib
utra
min
e C
o-in
terv
entio
n
Low
cal
orie
die
t A
djun
ctiv
e th
erap
y in
the
form
of d
iet,
exer
cise
d an
d be
havi
or
mod
ifica
tion
advi
ce in
va
ryin
g in
tens
ities
.
Co
mm
on a
dve
rse
even
ts
asso
ciat
ed w
ith s
ibu
tram
ine
H
eada
che
Con
stip
atio
n N
ause
a N
ervo
us s
yste
m (>
5%)
Diz
zine
ss
Dry
mou
th
Inso
mni
a R
equ
irin
g r
egu
lar
mon
itori
ng
In
crea
sed
bloo
d pr
essu
re
Incr
ease
d he
art r
ate
ST
OR
M tr
ial
Dat
a re
latin
g to
blo
od li
pids
an
d ge
nera
l met
abol
ism
sh
owed
sub
stan
tial
impr
ovem
ents
in th
e si
butra
min
e gr
oup.
A
dver
se e
vent
s
Inso
mni
a N
ause
a In
c bl
ood
pres
sure
La
ssitu
de
Bac
k pa
in
With
draw
als
resu
lts fo
rm
adve
rse
even
ts
Sib
utra
min
e w
ithdr
awal
s as
a
resu
lt of
BP
8% v
s. 3
%
7% v
s. 1
%
8% v
s. 3
%
7% v
s. 1
1%
7% v
s. 9
%
14%
vs5%
0.
8%
All
tria
ls re
porte
d pa
rtici
pant
se
lect
ion
crite
ria a
nd c
ompa
rabi
lity
of g
roup
s at
bas
elin
e.
Rel
ativ
ely
few
tria
ls d
escr
ibed
the
use
of a
prio
ri po
wer
cal
cula
tion
to
estim
ate
requ
ired
sam
ple
size
. N
one
of th
e tri
als
incl
uded
m
etho
ds to
det
erm
ine
the
succ
ess
of b
lindi
ng o
f pat
ient
s, c
are
give
rs
or o
utco
mes
ass
esso
rs.
Rep
ortin
g of
num
bers
of
with
draw
als
per g
roup
with
re
ason
s w
as v
aria
ble.
A
few
tria
ls in
clud
ed a
n as
sess
men
t of p
atie
nt’s
adh
eren
ce
with
the
trial
regi
men
; usu
ally
ei
ther
cou
ntin
g re
turn
ed c
apsu
les
or s
elf-r
epor
ting
(bot
h ar
e po
tent
ially
unr
elia
ble)
.
The
aut
hors
co
nclu
ded
that
the
asse
ssm
ent-r
isk
prof
ile o
f si
butra
min
e w
as
posi
tive
alth
ough
th
e pr
oduc
t mus
t be
kep
t und
er
revi
ew a
nd B
P a
nd
hear
t rat
e m
onito
red
espe
cial
ly in
obe
se
hype
rtens
ive
patie
nts.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
95
Evi
den
ce T
able
19.
S
ibu
tram
ine,
Ber
kow
titz
et
al.,
2003
Eff
ect S
ize
& P
reci
sion
S
tud
y au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e L
eng
th o
f st
udy
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) P
lace
bo
(s
.d.)
Sib
utr
amin
e (s
.d.)
p
valu
e
Val
idity
/App
licab
ility
Co
ncl
usi
on
s C
om
men
ts
Ber
kow
titz
et
al.,
2003
S
tudy
des
ign
R
ando
mis
ed,
doub
le b
lind,
pl
aceb
o co
ntro
lled
trial
L
eng
th o
f st
udy
Inte
ntio
n to
trea
t an
alys
is a
t 6
mon
ths
Par
ticip
ants
N
=146
ado
lesc
ents
ev
alua
ted
at c
linic
, 82
rand
omis
ed, 6
4 ex
clud
ed
(psy
chia
tric
cond
ition
s (2
4), n
ot in
tere
sted
(21)
, un
able
to a
ttend
gro
up
mee
tings
(12)
, med
ical
co
nditi
ons
(2),
othe
r (7)
).
Mea
n ag
e =1
4.1
yrs
(SD
=1.2
) M
ean
wei
ght=
103.
6kg
(SD
=15.
4)
Mea
n B
MI=
37.8
(SD
=3.8
) M
ean
wai
st
circ
umfe
renc
e=11
0.8c
m
(SD
=10.
0)
Sex
= 55
F: 2
7M
Whi
te ra
ce=4
5 B
lack
race
=34
Incl
usio
n
adol
esce
nts
13
-17
year
s B
MI =
32-4
4.
Exc
lusi
on/
con
trai
nd
icat
ions
C
ardi
ovas
cula
r dis
ease
D
iabe
tes
(type
1 o
r 2)
Maj
or p
sych
iatri
c di
sord
ers
Use
of a
wei
ght l
oss
med
icat
ion
or w
eigh
t los
s of
5kg
or m
ore
in th
e pr
evio
us 6
mon
ths
Use
of m
edic
atio
ns
prom
otin
g w
eigh
t gai
n (e
.g.,
oral
ste
roid
s)
Use
of m
edic
ines
co
ntra
indi
cate
d w
ith u
se o
f si
butra
min
e C
igar
ette
sm
okin
g
Ph
ase
I, p
lace
bo
co
ntr
olle
d, 6
mon
ths
wei
ght l
oss
tria
l S
ibut
ram
ine
+ be
havi
or
ther
apy,
N=4
3 or
pla
cebo
+b
ehav
ior t
hera
py, n
=39
Med
icat
ion
pro
toco
l W
eek
one:
all
parti
cipa
nts
rece
ived
pla
cebo
. Wee
k tw
o:
eith
er 5
mg/
d si
butra
min
e or
pl
aceb
o. W
eek
thre
e:
10m
g/d
or p
lace
bo. W
eek
seve
n: 1
5mg/
d or
pla
cebo
D
ose
redu
ctio
n: in
sub
ject
s w
ith a
n in
crea
se in
SB
P o
r D
BP
of >
=10m
mH
g or
an
incr
ease
of p
ulse
rate
of
>=15
%, d
ose
redu
ced
in
5mg
until
des
ired
rate
s ac
hiev
ed. S
ibut
ram
ine
disc
ontin
ued
if B
P in
crea
sed
20m
m H
g or
mor
e.
Beh
avio
ura
l pro
toco
l W
eekl
y gr
oup
sess
ions
for
subj
ect a
nd s
epar
ate
grou
ps
sess
ions
for p
aren
ts. G
roup
s w
ere
led
by d
ietit
ians
, ps
ycho
logi
sts
or
psyc
hiat
rists
. D
iet
1200
-150
0kca
l/d 3
0% fa
t 15
% p
rote
in, 5
5%
carb
ohyd
rate
. E
xerc
ise
Eve
ntua
l goa
l of w
alki
ng o
r si
mila
r aer
obic
act
ivity
12
0min
s pe
r wee
k.
Oth
er
Dai
ly e
atin
g an
d ac
tivity
logs
Ph
ase
I M
ean
wei
ght l
oss
% c
hang
e in
BM
I W
aist
circ
umfe
renc
e B
MI r
educ
tion>
=5%
B
MI r
educ
tion>
=10%
B
MI r
educ
tion>
=15%
S
ysto
lic B
P (3
mo)
D
iast
olic
BP
(3m
o)
Sys
tolic
BP
(6m
o)
Dia
stol
ic (6
mo)
P
ulse
rate
(3m
o)
Pul
se ra
te (6
mo)
H
unge
r red
uctio
n 19
dro
pou
ts
Sys
tolic
BP
‡
Dia
stol
ic B
P‡
Pul
se ra
te
Ser
um c
hem
istr
y
3.
2kg
(6.1
) 4.
0%(5
.4)
-2.8
cm(5
.6)
14(3
6)
6(15
) 1(
3)
110.
7mm
Hg
55.7
mm
Hg
110.
3mm
Hg
55.3
mm
Hg
81.6
bea
ts/m
in
81.2
beat
s/m
in
No
betw
een
grou
p di
ffere
nces
7.
8kg
(6.3
) 8.
5% (6
.8)
-8.2
(6.9
) 27
(63)
17
(40)
8(
19)
114.
8mm
Hg
58.4
mm
Hg
112.
9mm
Hg
58.6
mm
Hg
85.6
beat
s/m
in
84.8
beat
s/m
in
grea
ter
+ 10
mm
Hg
+8.6
mm
Hg
+14.
3/m
in
0.
001
0.00
1 <0
.001
0.
02
0.02
0.
02
0.02
† 0.
23†
0.06
† 0.
11†
<0.0
01†
0.00
7†
0.00
2 <0
.001
<0
.001
<0
.001
Ph
ase
I C
ompl
eted
6 m
onth
as
sess
men
t P
lace
bo
Sib
utra
min
e T
aken
off
stud
y be
caus
e of
mar
ked
and
sust
aine
d B
P in
crea
se
with
sib
utra
min
e IT
T a
naly
sis
Stu
dy p
ower
ed to
de
tect
4%
diff
eren
ce in
ba
selin
e B
MI b
etw
een
treat
men
t gro
ups.
N
o si
gnifi
cant
di
ffere
nce
betw
een
grou
ps a
t bas
elin
e N
o si
gnifi
cant
di
ffere
nce
in
with
draw
als
betw
een
grou
ps
Ph
ase
II, m
ain
tena
nce
tria
ls 7
-12
mo
nth
s, a
ll su
bje
cts
rece
ive
sibu
tram
ine
Not
repo
rted
here
, en
dpoi
nts
not r
elev
ant.
34/3
9 (8
7%)
40/4
3 (9
3%)
5/43
(12%
)
Dur
ing
Pha
se I
19/4
3(44
%) p
artic
ipan
ts
had
dose
redu
ctio
ns o
r di
scon
tinue
d tre
atm
ent
with
sib
utra
min
e. B
P a
nd
HR
resu
lts re
flect
a
delib
erat
e at
tem
pt to
lim
it in
crea
ses
in B
P o
r HR
. C
om
men
t S
ibut
ram
ine
and
beha
viou
r the
rapy
re
sulte
d in
sig
nific
antly
gr
eate
r wei
ght l
oss
than
pl
aceb
o an
d be
havi
our
ther
apy.
B
ehav
iour
al a
nd
phar
mac
olog
ical
tre
atm
ents
app
eare
d to
ha
ve a
dditi
ve e
ffect
s th
at
max
imis
ed w
eigh
t los
s.
Sib
utra
min
e m
ust b
e ca
refu
lly m
onito
red
to
cont
rol i
ncre
ases
in B
P
and
puls
e ra
te.
† re
pres
ents
the
diffe
renc
e be
twee
n tr
eatm
ent c
ondi
tions
bet
wee
n ba
selin
e an
d m
onth
3, b
asel
ine
and
mon
th 6
. ‡ In
crea
se fr
om b
asel
ine
to ti
me
of d
ropo
ut
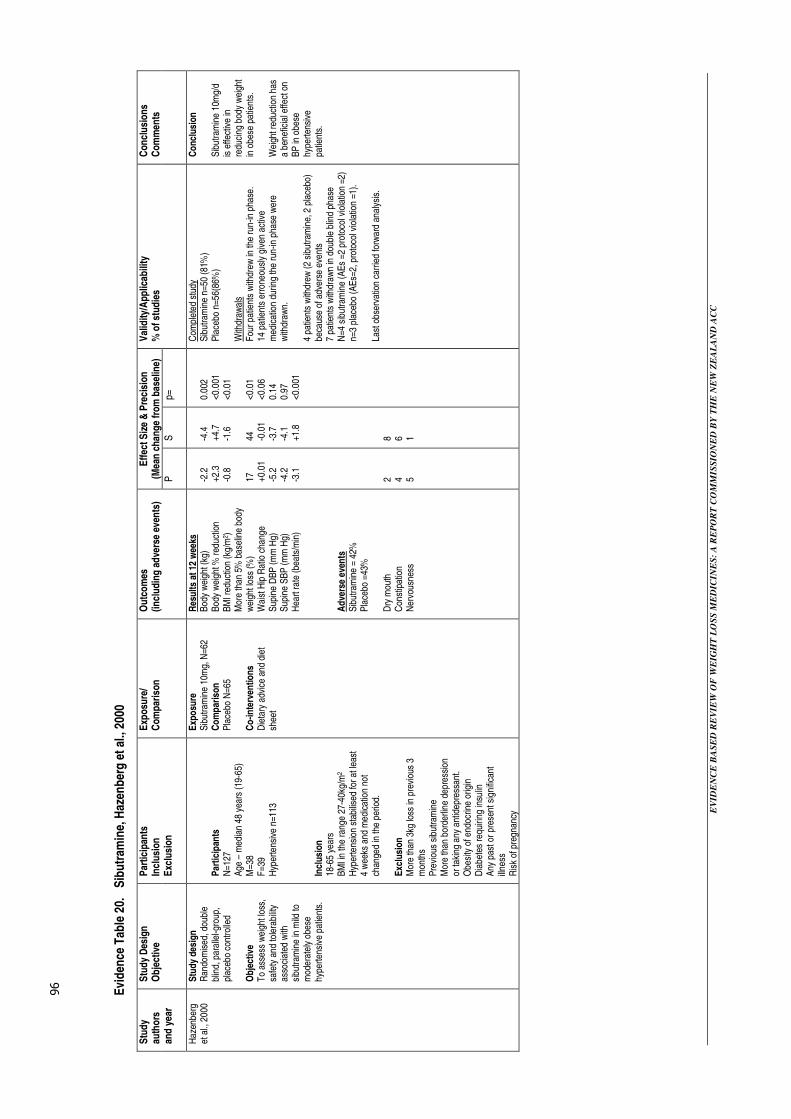
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
96
Evi
den
ce T
able
20.
S
ibu
tram
ine,
Haz
enb
erg
et
al.,
2000
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) P
S
p=
Val
idity
/App
licab
ility
%
of s
tud
ies
Con
clu
sio
ns
Com
men
ts
Haz
enbe
rg
et a
l., 2
000
Stu
dy d
esig
n
Ran
dom
ised
, dou
ble
blin
d, p
aral
lel-g
roup
, pl
aceb
o co
ntro
lled
Ob
ject
ive
To
asse
ss w
eigh
t los
s,
safe
ty a
nd to
lera
bilit
y as
soci
ated
with
si
butra
min
e in
mild
to
mod
erat
ely
obes
e hy
perte
nsiv
e pa
tient
s.
Par
ticip
ants
N
=127
A
ge –
med
ian
48 y
ears
(19-
65)
M=3
8 F
=39
Hyp
erte
nsiv
e n=
113
Incl
usio
n
18-6
5 ye
ars
BM
I in
the
rang
e 27
-40k
g/m
2 H
yper
tens
ion
stab
ilise
d fo
r at l
east
4
wee
ks a
nd m
edic
atio
n no
t ch
ange
d in
the
perio
d.
Exc
lusi
on
Mor
e th
an 3
kg lo
ss in
pre
viou
s 3
mon
ths
Pre
viou
s si
butra
min
e M
ore
than
bor
derli
ne d
epre
ssio
n or
taki
ng a
ny a
ntid
epre
ssan
t. O
besi
ty o
f end
ocrin
e or
igin
D
iabe
tes
requ
iring
insu
lin
Any
pas
t or p
rese
nt s
igni
fican
t ill
ness
R
isk
of p
regn
ancy
Exp
osu
re
Sib
utra
min
e 10
mg,
N=6
2 C
om
par
ison
P
lace
bo N
=65
Co
-inte
rven
tions
D
ieta
ry a
dvic
e an
d di
et
shee
t
Res
ults
at 1
2 w
eeks
B
ody
wei
ght (
kg)
Bod
y w
eigh
t % re
duct
ion
BM
I red
uctio
n (k
g/m
2 )
Mor
e th
an 5
% b
asel
ine
body
w
eigh
t los
s (%
) W
aist
Hip
Rat
io c
hang
e
Sup
ine
DB
P (m
m H
g)
Sup
ine
SB
P (m
m H
g)
Hea
rt ra
te (b
eats
/min
) A
dve
rse
even
ts
Sib
utra
min
e =
42%
P
lace
bo =
43%
D
ry m
outh
C
onst
ipat
ion
Ner
vous
ness
-2.2
+2
.3
-0.8
17
+0
.01
-5.2
-4
.2
-3.1
2 4 5
-4.4
+4
.7
-1.6
44
-0
.01
-3.7
-4
.1
+1.8
8 6 1
0.00
2 <0
.001
<0
.01
<0.0
1 <0
.06
0.14
0.
97
<0.0
01
Com
plet
ed s
tudy
S
ibut
ram
ine
n=50
(81%
) P
lace
bo n
=56(
86%
) W
ithdr
awal
s F
our p
atie
nts
with
drew
in th
e ru
n-in
pha
se.
14 p
atie
nts
erro
neou
sly
give
n ac
tive
med
icat
ion
durin
g th
e ru
n-in
pha
se w
ere
with
draw
n.
4 pa
tient
s w
ithdr
ew (2
sib
utra
min
e, 2
pla
cebo
) be
caus
e of
adv
erse
eve
nts
7 pa
tient
s w
ithdr
awn
in d
oubl
e bl
ind
phas
e N
=4 s
ibut
ram
ine
(AE
s =2
pro
toco
l vio
latio
n =2
) n=
3 pl
aceb
o (A
Es=
2, p
roto
col v
iola
tion
=1).
Last
obs
erva
tion
carr
ied
forw
ard
anal
ysis
.
Co
nclu
sion
S
ibut
ram
ine
10m
g/d
is e
ffect
ive
in
redu
cing
bod
y w
eigh
t in
obe
se p
atie
nts.
W
eigh
t red
uctio
n ha
s a
bene
ficia
l effe
ct o
n B
P in
obe
se
hype
rtens
ive
patie
nts.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
97
Evi
den
ce T
able
21.
S
ibu
tram
ine,
Go
kcel
et
al.,
2001
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) P
S
P
=
Val
idity
/App
licab
ility
%
of s
tud
ies
Con
clu
sio
ns
Com
men
ts
Gok
cel e
t al
., 2
001
Stu
dy d
esig
n
Ran
dom
ised
, dou
ble
blin
d,
plac
ebo
cont
rolle
d.
Ob
ject
ive
Eva
luat
ion
of th
e ef
ficac
y of
si
butra
min
e in
com
bina
tion
with
hyp
ogly
cem
ic d
rugs
in
obes
e fe
mal
es w
ith p
oorly
re
gula
ted
type
2 d
iabe
tes.
Par
ticip
ants
N
=60,
obe
se fe
mal
es
Incl
usio
n
HbA
1c >
8%
BM
I >30
kg/m
2 O
n m
axim
um d
osag
e of
m
etfo
rmin
(2,5
50m
g/d)
an
d su
lfony
lure
as
(glic
lazi
de, 3
20m
g/d
or
glip
izid
e, 2
0mg/
d).
Exc
lusi
on
Typ
e 1
diab
etes
O
besi
ty o
f end
ocrin
e or
igin
P
revi
ous
wei
ght l
oss
drug
s or
inte
nsiv
e w
eigh
t lo
ss p
rogr
am
Unc
ontro
lled
hype
rtens
ion,
S
BP
>160
mm
Hg
or D
BP
> 10
0mm
Hg.
G
lauc
oma
Pre
gnan
t wom
en
Pat
ient
s ta
king
bet
a-bl
ocke
rs, a
ntid
epre
ssan
ts,
mon
amin
e ox
idas
e in
hibi
tors
or a
ny d
rug
affe
ctin
g ap
petit
e or
w
eigh
t.
Exp
osu
re n
=29
Sib
utra
min
e 10
mg
t.i.d
. D
iet r
estri
ctio
n H
ypog
lyce
mic
dr
ugs
Co
mp
aris
on n
=25
Pla
cebo
D
iet r
estri
ctio
n H
ypog
lyca
emic
dr
ugs
Six
mon
ths
Wei
ght l
oss
(kg)
B
MI c
hang
e (k
g/m
2)
Wai
st c
ircum
fere
nce
(cm
) F
astin
g bl
ood
gluc
ose
(mg/
dl)
Pos
tpra
ndia
l blo
od g
luco
se (m
g/dl
) In
sulin
leve
l (:U
/ml)
HO
MA
IR
HbA
1c (
%)
Tot
al c
hole
ster
ol (m
g/dl
) H
DL
chol
este
rol (
mg/
dl)
LDL
chol
este
rol (
mg/
dl)
VLD
L ch
oles
tero
l (m
g/dl
) T
rigly
cerid
es (m
g/dl
) S
BP
– n
ot re
porte
d D
BP
& H
R s
igni
fican
t red
uctio
ns
repo
rted
but n
o da
ta g
iven
S
ide
effe
cts
(sib
utra
min
e)
Dry
mou
th, n
=11
Con
stip
atio
n, n
=16
H
yper
tens
ion,
n=1
(pat
ient
s w
ithdr
ew
from
stu
dy)
0.91
±0.
53
0.36
±0.
21
0.92
±0.
49
15.7
6±3.
89
32.8
8±6.
13
0.68
±0.
43
0.31
±0.
28
0.53
±0.
01
7.68
±5.
04
0.01
±1.
10
13.3
2±3.
94
0.01
±2.
58
0.36
±7.
26
-9.6
1±1.
37
-3.9
2±0.
54
-8.0
4±4.
43
124.
88±
8.58
10
2.24
±51
.99
5.66
±0.
97
7.09
±0.
81
2.73
±0.
01
28.0
8±4.
93
0.97
±1.
58
20.9
2±4.
66
8.68
±2.
58
46.7
6±13
.09
<0.0
001
<0.0
001
<0.0
001
<0.0
001
<0.0
001
<0.0
001
<0.0
001
<0.0
001
<0.0
08
>0.0
5 >0
.05
<0.0
2 <0
.08
With
draw
al -
one
subj
ect w
ithdr
ew
from
the
treat
men
t gro
up b
ecau
se
of h
yper
tens
ion.
E
xclu
sion
- fiv
e su
bjec
ts fr
om
plac
ebo
grou
p su
ffere
d lo
w
treat
men
t effi
cacy
and
wer
e ex
clud
ed a
nd s
witc
hed
to in
sulin
. C
ompa
rabl
e pa
tient
pop
ulat
ion
at
base
line
The
sig
nific
ant i
mpr
ovem
ent
in g
lyce
mic
con
trol i
n th
e si
butra
min
e gr
oup
was
at
tribu
ted
to w
eigh
t los
s.
The
re w
as a
lso
a si
gnifi
cant
po
sitiv
e ch
ange
in th
e lip
id
prof
ile o
f the
sib
utra
min
e pa
tient
s.
Co
nclu
sion
T
he a
dditi
on o
f sib
utra
min
e to
or
al h
ypog
lyca
emic
ther
apy
lead
s to
sig
nific
ant w
eigh
t los
s an
d im
prov
ed m
etab
olic
pa
ram
eter
s.
Sib
utra
min
e is
wel
l tol
erat
ed
and
safe
in th
is p
atie
nt
popu
latio
n.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
98
Evi
den
ce T
able
22.
S
ibu
tram
ine,
Kim
et
al.,
2003
DB
P=d
iast
olic
blo
od p
ress
ure,
SB
P=s
ysto
lic b
lood
pre
ssur
e
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
ies
Incl
ude
d
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) E
ffec
t Siz
e &
Pre
cisi
on
Sta
ndar
dise
d di
ffere
nce
of
chan
ges
from
bas
elin
e be
twee
n tre
atm
ent a
nd c
ontro
l§ (
95%
C
I)
Val
idity
/App
licab
ility
Con
clu
sio
ns
Com
men
ts
Kim
et a
l.,
2003
S
tudy
des
ign
M
eta-
anal
ysis
of
rand
omis
ed d
oubl
e bl
ind
plac
ebo
cont
rolle
d
trial
s.
Ob
ject
ive
A c
ompr
ehen
sive
met
a-an
alys
is o
f RC
Ts o
n th
e ef
fect
of s
ibut
ram
ine
on
wei
ght l
oss
and
bloo
d pr
essu
re.
Stu
die
s in
clud
ed, N
=21
Wei
ntra
ub e
t al.,
199
1 H
anot
in e
t al.,
199
8 S
eagl
e et
al.,
199
8 A
pfeb
aum
et a
l., 1
999
Bra
y et
al.,
199
9 H
anse
n et
al.,
199
9 C
uella
r et a
l., 2
000
Fan
ghan
el e
t al.,
200
0 F
iner
et a
l., 2
000
Fuj
ioka
et a
l., 2
000
Haz
enbe
rg e
t al.,
200
0 M
cMah
on e
t al.,
200
0 D
ujov
ne e
t al.,
200
1 G
okce
l et a
l., 2
001
Sm
ith e
t al.,
200
1 W
irth
et a
l., 2
001
Far
ia e
t al.,
200
2 M
cMah
on e
t al.,
200
2 S
erra
no-R
ios
et a
l.,
2002
S
ram
ek e
t al.,
200
2 Z
anna
d et
al.,
200
2
Incl
usio
n
Hum
an s
tudi
es
Dou
ble
blin
d ra
ndom
ised
, pla
cebo
co
ntro
lled
trial
s of
sib
utra
min
e E
nglis
h
Ful
l tex
t ava
ilabl
e O
bese
or o
verw
eigh
t par
ticip
ants
D
osag
e of
sib
utra
min
e >
5mg
Any
dur
atio
n C
o-m
orbi
ditie
s of
dia
bete
s,
hype
rtens
ion
or h
yper
lipid
emia
al
low
ed.
Exc
lusi
on
Stu
dies
of p
atie
nts
with
eat
ing
diso
rder
s C
ross
over
stu
dies
S
tudi
es th
at d
id n
ot p
rovi
de
info
rmat
ion
for e
stim
atin
g a
size
ef
fect
of w
eigh
t cha
nge.
S
tudi
es u
sing
dru
gs fo
r wei
ght
mai
nten
ance
S
tudi
es w
ith m
ultip
le tr
eatm
ent
grou
ps th
at d
id n
ot c
ompa
re e
ach
grou
p w
ith th
e co
ntro
l gro
up
inde
pend
ently
.
Exp
osu
re
Sib
utra
min
e >5
mg/
d C
om
par
ato
r P
lace
bo
Wei
gh
t cha
nge
O
vera
ll si
ze e
ffect
S
BP
O
vera
ll si
ze e
ffect
S
ize
effe
ct ra
nge
Net
incr
ease
d S
BP
attr
ibut
able
to
sib
utra
min
e D
BP
O
vera
ll si
ze e
ffect
S
ize
effe
ct ra
nge
Net
incr
ease
d D
BP
attr
ibut
able
to
sib
utra
min
e
-1.0
0 (-
1.17
to -0
.84)
0.
16 (0
.08
to 0
.24)
-0
.38
to 0
.45
1.6m
m H
g 0.
26 (0
.18
to 0
.33)
-0
.11
to 0
.73
1.8m
m H
g
All
stud
ies
wer
e ca
rrie
d ou
t in
Wes
tern
co
untri
es, w
hich
may
lim
it ap
plic
abili
ty.
Incl
usio
n cr
iteria
may
hav
e le
d to
und
er o
r ov
er-e
stim
atio
n of
the
effe
ct.
Bec
ause
onl
y pu
blis
hed
stud
ies
wer
e em
ploy
ed in
the
anal
ysis
ther
e is
a p
ossi
bilit
y of
pub
licat
ion
bias
, how
ever
Ros
enth
al’s
fail-
safe
N v
alue
s w
ere
appr
oxim
atel
y N
= 10
0 fo
r S
BP
and
N=
341
for D
BP
whi
ch m
akes
pu
blic
atio
n bi
as u
nlik
ely.
Sib
utra
min
e sh
owed
a
larg
e ef
fect
on
wei
ght b
ut
incr
ease
d bl
ood
pres
sure
si
gnifi
cant
ly, p
artic
ular
ly
in h
eavi
er a
nd/o
r you
nger
pa
rtici
pant
s. T
he s
ize
of
the
incr
ease
in b
lood
pr
essu
re w
as s
mal
l ho
wev
er, i
t was
co
nsid
ered
to b
e cl
inic
ally
im
porta
nt in
pat
ient
s w
ho
had
bord
erlin
e or
hig
h bl
ood
pres
sure
. A
gre
ater
incr
ease
in
SB
P w
as fo
und
in
subj
ects
<44
yea
rs o
f age
an
d in
the
larg
er tr
ials
(n
>=12
0).
Par
ticip
ants
with
a h
ighe
r w
eigh
t (>=
92kg
) ex
perie
nced
a h
ighe
r D
BP
and
SB
P.
The
ove
rall
effe
ct s
ize
was
sig
nific
antly
larg
er
whe
n th
e si
butra
min
e do
se w
as >
15m
g/d.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
99
Evi
den
ce T
able
23.
S
ibu
tram
ine,
Hau
ner
et
al.,
2003
Eff
ect S
ize
& P
reci
sion
C
hang
e in
wei
ght f
rom
bas
elin
e to
54
wee
ks
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
)
Pla
ceb
o
Sib
utr
amin
e P
-S
p=
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Hau
ner e
t al
., 2
003
Stu
dy d
esig
n
Ran
dom
ised
, dou
ble
blin
d, p
lace
bo c
ontro
lled
clin
ical
tria
l O
bje
ctiv
e T
o st
udy,
in a
prim
ary
heal
th c
are
setti
ng, t
he
effe
ct o
f a s
tand
ardi
sed
non-
phar
mac
olog
ical
pr
ogra
m a
nd 1
5mg
sibu
tram
ine
or p
lace
bo
on lo
ng-te
rm w
eigh
t re
duct
ion.
T
rial
du
ratio
n
54 w
eeks
Par
ticip
ants
N
=389
, IT
T p
opul
atio
n N
=348
C
onse
cutiv
e, G
P p
atie
nts
in th
e ar
ea o
f Col
ogne
-D
usse
ldor
f, G
erm
any.
M
ale=
89 (2
3%),
Fem
ale=
259(
67%
) M
ean
age
=42.
7 ±
11.
7 ye
ars
Incl
usio
n
Age
18-
65 y
ears
B
MI 3
0-40
kg/m
2 S
tabl
e w
eigh
t (±
2kg)
du
ring
the
prec
edin
g 3
mon
ths
Mot
ivat
ion
and
will
ingn
ess
to re
duce
wei
ght.
Exc
lusi
on
Ser
um c
reat
inin
e >2
mg/
dl
Hyp
erch
oles
tero
lem
ia
(tota
l cho
lest
erol
>3
20m
g/dl
) U
ncon
trolle
d hy
perte
nsio
n (>
160/
95m
mH
g, m
ean
of
3 in
depe
nden
t m
easu
rem
ents
) T
ype
2 di
abet
es m
ellit
us
Cor
onar
y he
art d
isea
se
Clin
ical
ly s
igni
fican
t dy
srhy
thm
ia
Psy
chia
tric
dise
ases
C
hild
bea
ring
pote
ntia
l w
ithou
t ade
quat
e co
ntra
cept
ion
Use
of m
edic
atio
n th
at
may
alte
r app
etite
.
Exp
osu
re N
=174
S
ibut
ram
ine
15m
g/da
y gi
ven
as a
n ad
junc
t to
a st
anda
rd n
on-
phar
mac
olog
ical
tre
atm
ent.
Co
mp
aris
on N
=174
P
lace
bo g
iven
as
an
adju
nct t
o a
stan
dard
non
-ph
arm
acol
ogic
al
treat
men
t. C
onc
om
itan
t non
-p
harm
aco
log
ical
ther
apy
Fou
r edu
catio
nal s
essi
ons
on fo
od c
hoic
e, p
hysi
cal
activ
ity, m
otiv
atio
n an
d be
havi
oral
mod
ifica
tion
and
diet
cou
nsel
ling.
S
ubje
cts
wer
e al
so
enco
urag
ed to
atte
nd 1
6 fu
rther
ses
sion
s.
A d
ietit
ian
mad
e in
divi
dual
di
etar
y co
unse
lling
and
en
ergy
requ
irem
ent
calc
ulat
ions
. Sub
ject
s w
ere
enco
urag
ed to
reco
rd
thei
r die
tary
inta
ke fo
r sel
f-co
ntro
l. S
ubje
cts
wer
e en
cour
aged
to
incr
ease
thei
r phy
sica
l ac
tivity
suc
h th
at e
xces
s en
ergy
exp
endi
ture
by
addi
tiona
l phy
sica
l act
ivity
sh
ould
exc
eed
1000
kcal
pe
r wee
k.
Wei
ght l
oss
(kg)
W
eigh
t los
s (%
) 5%
wei
ght r
educ
tion
(%)
10%
wei
ght r
educ
tion
(%)
WH
R
Wai
st c
ircum
fere
nce
(cm
) S
BP
(mm
Hg)
D
BP
(mm
Hg)
H
eart
rate
(bea
ts/m
in)
Tot
al c
hole
ster
ol (m
g/dl
) LD
L- c
hole
ster
ol (m
g/dl
) H
DL
- cho
lest
erol
(mg/
dl)
Trig
lyce
rides
(mg/
dl)
Ad
vers
e ev
ents
31
0/34
8 (8
5.6%
) pat
ient
s of
the
ITT
pop
ulat
ion
expe
rienc
ed
adve
rse
even
ts in
clud
ing:
B
ack
pain
B
ronc
hitis
S
inus
itis
Gas
tritis
Ill
def
ined
exp
erie
nce
Hea
dach
e In
fect
ion
Pha
ryng
itis
Acc
iden
tal i
njur
y E
nter
itis
Dry
mou
th
Sur
gery
F
lu s
yndr
ome
Fun
gal
der
mat
itis
Upp
er re
spira
tory
trac
t inf
ectio
n G
astro
inte
stin
al d
isor
der
Ecz
ema
Hyp
erte
nsio
n C
ons
tipat
ion
5.1(
-6.1
to –
4.1)
4.
9 (4
.0-5
.8)
41.4
19
.0
-0.0
19
(-0.
027
to –
0.01
2)
-6.0
(-7.
1 to
–5.
0)
-1.5
(-3.
9 to
0.0
9)
-1.3
(-2.
8 to
0.1
) -0
.9 (-
2.8
to 0
.8)
-1.4
(-7.
0 to
4.2
) -8
.7 (-
15.0
to –
2.3)
3.
9 (2
.2 to
5.5
) 17
.1 (-
15.3
to 4
9.6)
83
.5%
8.1(
-9.2
to –
6.9)
8.
3 (7
.1-9
.6)
62.6
40
.8
-0.0
24
(-0.
033
to –
0.01
4)
-8.5
cm (-
9.7
to –
7.2)
-2
.9 (-
5.1
to –
0.7)
-0
.3(-
1.8
to 1
.3)
1.9(
0.1
to 3
.8)
-2.5
(-7.
6 to
2.6
) -6
.1 (-
10.7
to –
1.5)
5.
6 (4
.1 to
7.1
) -9
.9(-
21.1
to 1
.3)
87.8
%
<0.0
1 ns
<0.0
01
<0.0
01
ns
ns
ns
ns
<0.0
5 ns
ns
ns
ns
ns
ns
ns
ns
ns
ns
ns
ns
ns
ns
0.00
1 ns
ns
0.02
2 ns
ns
ns
ns
0.00
2
The
pop
ulat
ions
wer
e si
mila
r at b
asel
ine
exce
pt
for a
sig
nific
antly
sm
alle
r nu
mbe
r of m
ales
in th
e si
butra
min
e gr
oup.
A
naly
sis
base
d on
ITT
and
at
leas
t one
follo
w-u
p vi
sits
w
ith w
eigh
t mea
sure
men
t. La
st o
bser
vatio
n ca
rrie
d fo
rwar
d (L
OC
F) w
as u
sed
for t
he fi
nal a
naly
sis.
T
here
wer
e a
sign
ifica
ntly
(p
<0.0
5) s
mal
ler n
umbe
r of
mal
es in
the
sibu
tram
ine
grou
p.
With
draw
als
Sib
utra
min
e =6
6 P
lace
bo=7
5 M
ain
reas
ons
for d
rop-
out
poor
com
plia
nce
and
disc
onte
nt w
ith w
eigh
t lo
ss, s
ibut
ram
ine
N=3
8,
plac
ebo
n=43
. A
dver
se e
vent
w
ithdr
awal
s, s
ibut
ram
ine
n=22
, pla
cebo
n=1
5.
Adj
unct
trea
tmen
t of o
bese
su
bjec
ts w
ith 1
5mg
sibu
tram
ine
daily
in
com
bina
tion
with
a
com
preh
ensi
ve n
on-
phar
mac
olog
ical
wei
ght
redu
ctio
n pr
ogra
m p
rodu
ces
addi
tiona
l; w
eigh
t los
s an
d ca
n be
read
ily im
plem
ente
d in
a p
rimar
y ca
re s
ettin
g.
Tre
atm
ent w
ith s
ibut
ram
ine
prov
ed to
be
safe
and
pa
rticu
larly
effe
ctiv
e in
thos
e ob
ese
subj
ects
who
wer
e le
ss s
ucce
ssfu
l with
the
non-
phar
mac
olog
ical
pro
gram
.
Out
com
e fig
ures
in b
old
are
sta
tistic
ally
sig
nific
ant

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
100
Evi
den
ce T
able
24.
S
ibu
tram
ine,
Mcn
ult
y et
al.,
200
3
Eff
ect S
ize
& P
reci
sion
(m
ean
diff
eren
ce s
ibu
tram
ine
–
pla
ceb
o ±
SE
or
med
ians
(ran
ge)
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e P
artic
ipan
ts
Incl
usio
n
Exc
lusi
on
Exp
osu
re/
Com
pari
son
O
utc
om
es
(incl
udin
g a
dve
rse
even
ts)
S15
mg
/d
95%
CI
S20
mg
/d
95%
CI
Val
idity
/App
licab
iilty
C
oncl
usi
ons
C
omm
ents
McN
ulty
et a
l.,
2003
S
tudy
des
ign
R
ando
mis
ed,
plac
ebo
cont
rolle
d,
doub
le b
lind,
m
ultic
entre
, and
m
ulti
natio
nal t
rial.
Ob
ject
ive
To
eval
uate
the
effe
cts
of
sibu
tram
ine
(15
and
20m
g/da
y) o
n w
eigh
t met
abol
ic
cont
rol a
nd b
lood
pr
essu
re in
m
etfo
rmin
obe
se
subj
ects
with
type
2
diab
etes
. R
ecru
itmen
t E
ligib
le p
atie
nts
from
cas
e no
tes
Par
ticip
ants
N
=195
M
ale=
45%
, Fem
ale=
55%
M
ean
Age
=48-
51ye
ars,
ra
nge
27-6
9yea
rs
Dur
atio
n=1
year
H
yper
tens
ive
=36%
with
29
% ta
king
ant
i- hy
perte
nsiv
e an
d 17
% li
pid
low
erin
g dr
ugs.
In
clus
ion
T
ype
2 di
abet
es >
6 m
o B
MI>
=27k
g/m
2
Met
form
in tr
eatm
ent 3
m
onth
s - 2
yea
rs
Age
25-
70 y
ears
F
astin
g se
rum
glu
cose
7-
15m
mol
/l E
xclu
sion
Is
chem
ic h
eart
dise
ase,
he
art f
ailu
re o
r stro
ke.
Sea
ted
puls
e ra
te
>100
BP
M,
DB
P>9
5mm
Hg
Fas
ting
seru
m
trigl
ycer
ides
>5.6
mm
ol/l
Fas
ting
seru
m c
hole
ster
ol
>7.8
mm
ol/l
Ser
um c
reat
inin
e >1
20µ
mol
/l S
erum
live
r enz
ymes
of
bilir
ubin
leve
ls x
2 up
per l
imit
of n
orm
al.
Wei
ght c
hang
e >3
kg in
pr
eced
ing
3 m
onth
s P
regn
ant o
r chi
ldbe
arin
g w
omen
or c
hild
bear
ing
pote
ntia
l not
taki
ng
adeq
uate
pre
caut
ions
aga
in
preg
nanc
y.
Exp
osu
re
Sib
utra
min
e 15
mg/
day
and
20m
g/da
y an
d st
anda
rd d
iet a
dvis
ed b
y a
diet
itian
. C
om
par
ison
P
lace
bo a
nd s
tand
ard
diet
adv
ised
by
a di
etiti
an.
Wei
ght c
hang
e (k
g)
BM
I (kg
/m2 )
W
aist
circ
umfe
renc
e (c
m)
Hip
W
aist
hip
ratio
>=
5% w
eigh
t los
s (%
) >=
10%
wei
ght l
oss
(%)
Met
abo
lic c
han
ges
Fas
ting
gluc
ose
(mm
ol/l)
H
bA1c
(%)
Fas
ting
insu
lin (p
mol
/l)
Cho
lest
erol
(mm
ol/l)
H
DL
LDL
Tot
al c
hole
ster
ol to
HD
L ch
oles
tero
l T
rigly
cerid
es (m
mol
/l)
Car
dio
vasc
ula
r ef
fect
s S
BP
(mm
Hg)
D
BP
(mm
Hg)
P
ulse
rate
(bea
ts p
er m
in)
Ad
vers
e ev
ents
S
ibut
ram
ine
Dry
mou
th
Con
stip
atio
n In
som
nia
-5.1
±0.
9 -1
.9-±
0.3
-4.9
±0.
9 -3
.0±
1.0
-1.4
±0.
9 46
14
-0.2
-0
.34±
0.33
-6
.0
0.0
0.1
0.0
-0.5
-0
.2
4.6±
2.2
2.8±
1.2
5.9
±1.
7
-7.0
to –
3.3
-2.6
tp-1
.2
-6.7
to-3
.0
-5.0
to-1
.0
-3.1
to 0
.3
-1.0
to 0
.7
-0.9
9 to
0.3
1 -2
4.0
to 1
2.0
-0.2
to 0
.3
0.0
to 0
.2
-0.2
to 0
.3
-0.9
to-0
.2
-0.6
to 0
.1
0.3
to 8
.8
0.4
to 5
.3
2.5
to 9
.4
-7.8
±1.
0 -2
.9±
0.3
-6.8
±1.
0 -6
.1±
1.0
-0
.9±
0.9 65
27
-0
.2
-0.1
0±0.
34
-18.
0 0.
1 0.
1 0.
1 -0
.2
-0.3
-1
.3 ±
2.2
0.0±
1.3
5.8±
1.8
-9.7
to-5
.9
-3.6
to-2
.2
-8.7
to-4
.9
-8.2
to-4
.1
-2.6
to 0
.8
-1.0
to 0
.5
-0.7
6 to
0.5
7 -3
0.0
to 0
.0
-0.1
to 0
.3
0.0
to 0
.1
-0.1
to 0
.3
-0.5
to 0
.1
-0.6
to 0
.0
-5.6
to 3
.1
-2.5
to 2
.4
2.3
to 9
.3
Rel
ativ
ely
youn
g pa
tient
po
pula
tion
Stri
ct in
clus
ion
crite
ria m
ay
limit
appl
icab
ility
.
Sib
utra
min
e w
as a
n ef
fect
ive
anti-
obes
ity
agen
t in
a su
bsta
ntia
l pr
opor
tion
of p
atie
nts
with
type
2 d
iabe
tes.
A
vera
ge w
eigh
t los
s at
on
e ye
ar w
as 5
.5kg
w
ith 1
5mg
sibu
tram
ine
and
8.0k
g w
ith 2
0mg
– pl
aceb
o pa
tient
s lo
st n
o w
eigh
t. In
fact
19%
ga
ined
mor
e th
an 2
kg
over
1 y
ear.
Wei
ght l
oss
of >
= 10
%
conf
erre
d m
etab
olic
an
d ca
rdio
vasc
ular
be
nefit
s. N
o pa
tient
s in
th
e pl
aceb
o gr
oup
lost
>=
10-%
bod
y w
eigh
t. P
oorly
con
trolle
d ob
ese
type
2 d
iabe
tic p
atie
nts
may
gai
n th
e m
ost f
rom
w
eigh
t los
s an
d an
ti-ob
esity
med
icat
ion.
Li
pid
chan
ges
wer
e m
odes
t in
this
stu
dy
and
low
er th
an o
ther
st
udie
s bu
t may
be
expl
aine
d by
the
fact
th
at s
tudy
par
ticip
ants
w
ere
rece
ivin
g m
etfo
rmin
whi
ch h
as
favo
rabl
e m
oder
atin
g ef
fect
on
lipid
s.
Sib
utra
min
e te
nded
to
incr
ease
blo
od
pres
sure
in m
ore
patie
nts
than
pla
cebo
an
d a
few
indi
vidu
als
show
ed m
arke
d ris
es.
Fig
ures
in b
old
= si
gnifi
cant
, S=s
ibut
ram
ine.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
101
Evi
den
ce T
able
25.
S
ibu
tram
ine,
Wad
den
et
al.,
2000
Eff
ect S
ize
& P
reci
sion
(M
ean
cha
nge
from
bas
elin
e)
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y L
ocat
ion
(s)
Par
ticip
ants
In
clus
ion
E
xclu
sion
R
ecru
itmen
t
Exp
osu
re/
Com
pari
son
Ou
tco
mes
S+P
S
+O
P=*
*
Val
idity
/App
licab
ility
S
afet
y
Con
clu
sio
ns
Com
men
ts
-0.7
±1.
2 -0
.5±
1.4
+0.1
±1.
8 +0
.5±
2.1
-0.7
±1.
3 -0
.3±
1.6
+0.2
±1.
9 +0
.8±
2.0
-0.7
±1.
8 -0
.7±
2.9
-0.4
±4.
2 +0
.1±
4.1
-0.9
±1.
9 -0
.7±
23.1
-0
.6±
4.4
+0.3
±4.
2
ns
ns
ns
ns
ns
ns
ns
ns
Wad
den
et a
l.,
2000
S
tudy
Des
ign
R
ando
mis
ed, d
oubl
e bl
ind,
pla
cebo
co
ntro
lled
clin
ical
tria
l. O
bje
ctiv
e T
o as
sess
if a
ddin
g or
lista
t to
sibu
tram
ine
indu
ces
furth
er w
eigh
t lo
ss o
r mai
ntai
ns
wei
ght l
ost i
n pa
tient
s w
ho h
ave
lost
wei
ght
taki
ng s
ibut
ram
ine
alon
e an
d co
ntin
ue
taki
ng s
ibut
ram
ine.
S
tudy
loca
tion
(s)
US
A
Du
ratio
n
16 w
eeks
afte
r 1 y
ear
of s
ibut
ram
ine
Par
ticip
ants
34
vol
unte
ers
M
ean
age
44.1
yea
rs
(±10
.4)
Fem
ale
=100
%
BM
I=33
.9±
4.9k
g/m
2 In
clus
ion
F
emal
es w
ho h
ad
com
plet
ed 1
yea
r tre
atm
ent w
ith
sibu
tram
ine
(10-
15m
g/d)
Exp
osu
re N
=17
Sib
utra
min
e (1
0-15
mg/
day)
and
orli
stat
+
pres
crib
ed d
iet +
a d
aily
m
ultiv
itam
in
Co
mp
aris
on n
=17
Sib
utra
min
e (1
0-15
mg/
d)
and
plac
ebo
+ pr
escr
ibed
di
et +
a d
aily
mul
tivita
min
. P
resc
rib
ed d
iet
1200
-160
0kca
l/day
re
pres
entin
g a
defic
it of
60
0-50
0kca
l/day
. Die
t to
com
pris
e 20
% c
alor
ies
from
pro
tein
, 50%
ca
rboh
ydra
te <
=30%
fat.
Hea
lthy
eatin
g ed
ucat
ion.
F
at in
take
lim
ited
to
60g/
d.
Exe
rcis
e/ac
tivity
M
onth
ly a
ctiv
ity g
oals
with
ev
entu
al g
oal o
f 5
sess
ions
of 3
0-40
min
s pe
r wee
k.
Ove
rall
– m
odes
t life
styl
e in
terv
entio
n.
Wei
ght c
hang
e in
16
wee
k co
ntin
uatio
n tri
al –
Last
obs
erva
tion
carr
ied
forw
ard
N=1
7 1
mon
th
2 m
onth
s 3
mon
ths
4 m
onth
s W
eigh
t cha
nge
in 1
6 w
eek
cont
inua
tion
trial
–E
nd p
oint
ana
lysi
s 1
mon
th (N
=16
S+P
, N=1
4 S
+O)
2 m
onth
s (N
=10
S+P
, N=
15 S
+O)
3 m
onth
s (N
=12
S+P
, N=1
5 S
+O)
4 m
onth
s (N
=10
S+P
, N=1
4 S
+O)
Ad
vers
e ev
ents
(% o
f pat
ien
ts)
Sof
t sto
ol
Incr
ease
d bo
wel
mov
emen
t F
aeca
l urg
ency
O
ily e
vacu
atio
n O
ily s
potti
ng
Fla
tus
with
dis
char
ge
Fat
ty o
ily s
tool
Li
quid
sto
ol
Sto
mac
h pa
in/u
pset
sto
mac
h F
aeca
l inc
ontin
ence
D
ecre
ased
bow
el m
ovem
ent
Pel
lets
/har
d st
ool
The
adv
erse
eve
nts
are
repo
rts fo
r the
la
st w
eek
of th
e tri
al.
Com
bini
ng th
e tre
atm
ents
did
not
app
ear
to re
sult
in a
ny u
nexp
ecte
d si
de e
ffect
s.
9.1
9.1
9.1
0 9.1
0 0 9.1
9.1
0 0 18.2
50
50
42.9
42
.9
28.6
28
.6
28.6
14
.3
14.3
7.
1 7.
1 7.
1
0.04
* 0.
04*
ns
0.02
* ns
ns
ns
ns
ns
ns
ns
ns
Sm
all s
tudy
S
hort
dura
tion
Die
t mod
ifica
tion
/life
styl
e th
erap
y no
t st
anda
rd.
Die
ts m
ay h
ave
been
ver
y lo
w fa
t. W
ithd
raw
als
Sib
utra
min
e +
orlis
tat,
n=3
(18%
) S
ibut
ram
ine,
n=5
(29%
) diff
eren
ce n
ot
sign
ifica
nt.
Com
plet
ers
(EP
A) a
nd la
st o
bser
vatio
n ca
rrie
d fo
rwar
d (L
OC
F) a
naly
ses
both
re
ache
d th
e sa
me
conc
lusi
ons.
N
ot c
lear
if IT
T a
naly
sis
was
car
ried
out b
ut a
chi
-squ
ared
test
on
the
drop
-ou
t sho
wed
no
sign
ifica
nt d
iffer
ence
. D
osa
ge
The
med
icat
ion
dosa
ge v
arie
d fo
r bot
h tre
atm
ents
, S
ibut
ram
ine
+ pl
aceb
o 10
mg/
d si
butra
min
e N
=7
15m
g/d
sibu
tram
ine
N=-
10
Sib
utra
min
e +
orlis
tat
10m
g/d
sibu
tram
ine
N=6
15
mg/
d si
butra
min
e N
=-11
O
rlist
at 1
20m
g t.i
.d.
Dos
e re
duct
ion
of s
ibut
ram
ine
had
been
mad
e in
the
prev
ious
1 y
ear
stud
y be
caus
e of
sid
e ef
fect
s no
tabl
y in
som
nia,
incr
ease
d bl
ood
pres
sure
an
d pu
lse.
B
lind
ing
84
.6%
of p
atie
nts
had
gues
sed
wha
t tre
atm
ent t
hey
wer
e on
.
Co
nclu
sion
B
ody
wei
ght r
emai
ned
esse
ntia
lly
unch
ange
d in
the
two
grou
ps o
ver
the
16-w
eek
stud
y pe
riod.
H
owev
er, t
hose
that
lost
>=1
0% o
f th
eir i
nitia
l wei
ght i
n th
e pr
evio
us 1
ye
ar g
aine
d w
eigh
t dur
ing
the
seco
nd s
tudy
rega
rdle
ss o
f m
edic
atio
n re
ceiv
ed. T
hose
that
ga
ined
<10
% in
the
initi
al s
tudy
lost
a
furth
er a
mou
nt o
f wei
ght i
n th
e se
cond
stu
dy w
ith th
ose
taki
ng
sibu
tram
ine
+ or
lista
t los
ing
mor
e w
eigh
t tha
n th
ose
taki
ng
sibu
tram
ine
alon
e (n
s).
Fur
ther
sub
-gro
up a
naly
ses
of
patie
nts
thou
ght m
ost l
ikel
y to
be
nefit
from
com
bina
tion
ther
apy
did
not i
ncre
ase
thei
r wei
ght l
oss.
T
he a
utho
rs s
ugge
st th
at m
ost
obes
e pa
tient
s ha
ve a
lim
it of
10-
15%
wei
ght l
oss.
Fur
ther
wei
ght
loss
app
ears
to b
e th
war
ted
by a
to
xic
envi
ronm
ent t
hat d
isco
urag
es
phys
ical
act
ivity
, enc
oura
ges
cons
umpt
ion
of h
igh
fat d
iet a
nd
com
pens
ator
y bi
olog
ical
m
echa
nism
that
dec
reas
e en
ergy
ex
pend
iture
.
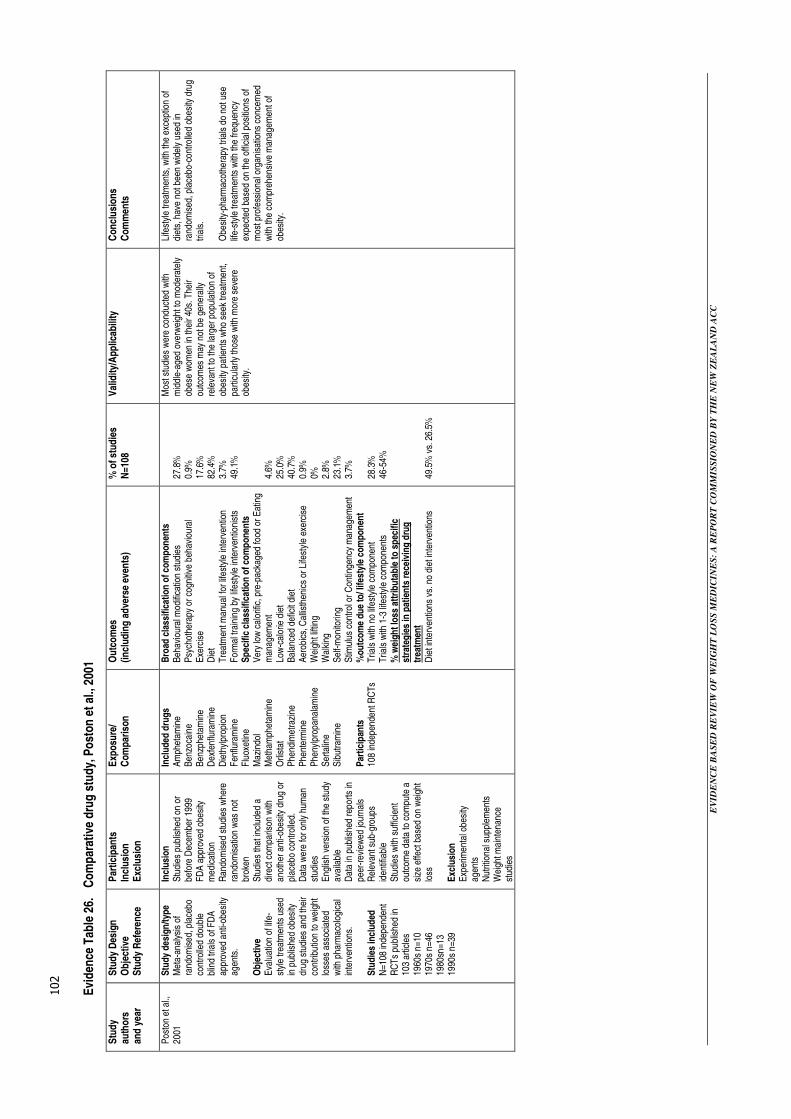
EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
102
Evi
den
ce T
able
26.
C
om
par
ativ
e d
rug
stu
dy,
Po
ston
et
al.,
2001
Stu
dy
auth
ors
an
d y
ear
Stu
dy
Des
ign
O
bje
ctiv
e S
tud
y R
efer
ence
Par
ticip
ants
In
clus
ion
E
xclu
sion
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) %
of s
tud
ies
N=1
08
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Pos
ton
et a
l.,
2001
Stu
dy d
esig
n/ty
pe
Met
a-an
alys
is o
f ra
ndom
ised
, pla
cebo
co
ntro
lled
doub
le
blin
d tri
als
of F
DA
ap
prov
ed a
nti-o
besi
ty
agen
ts.
Ob
ject
ive
Eva
luat
ion
of li
fe-
styl
e tre
atm
ents
use
d in
pub
lishe
d ob
esity
dr
ug s
tudi
es a
nd th
eir
cont
ribut
ion
to w
eigh
t lo
sses
ass
ocia
ted
with
pha
rmac
olog
ical
in
terv
entio
ns.
Stu
die
s in
clud
ed
N=1
08 in
depe
nden
t R
CT
s pu
blis
hed
in
103
artic
les
19
60s
n=10
19
70s
n=46
19
80sn
=13
1990
s n=
39
Incl
usio
n
Stu
dies
pub
lishe
d on
or
befo
re D
ecem
ber 1
999
FD
A a
ppro
ved
obes
ity
med
icat
ion
Ran
dom
ised
stu
dies
whe
re
rand
omis
atio
n w
as n
ot
brok
en
Stu
dies
that
incl
uded
a
dire
ct c
ompa
rison
with
an
othe
r ant
i-obe
sity
dru
g or
pl
aceb
o co
ntro
lled.
D
ata
wer
e fo
r onl
y hu
man
st
udie
s E
nglis
h ve
rsio
n of
the
stud
y av
aila
ble
Dat
a in
pub
lishe
d re
ports
in
peer
-rev
iew
ed jo
urna
ls
Rel
evan
t sub
-gro
ups
iden
tifia
ble
Stu
dies
with
suf
ficie
nt
outc
ome
data
to c
ompu
te a
si
ze e
ffect
bas
ed o
n w
eigh
t lo
ss
Exc
lusi
on
Exp
erim
enta
l obe
sity
ag
ents
N
utrit
iona
l sup
plem
ents
W
eigh
t mai
nten
ance
st
udie
s
Incl
uded
dru
gs
Am
phet
amin
e B
enzo
cain
e B
enzp
heta
min
e D
exfe
nflu
ram
ine
Die
thyl
prop
ion
Fen
flura
min
e F
luox
etin
e M
azin
dol
Met
ham
phet
amin
e O
rlist
at
Phe
ndim
etra
zine
P
hent
erm
ine
Phe
nylp
ropa
nala
min
e S
erta
line
Sib
utra
min
e P
artic
ipan
ts
108
inde
pend
ent R
CTs
Bro
ad c
lass
ifica
tion
of c
ompo
nen
ts
Beh
avio
ural
mod
ifica
tion
stud
ies
P
sych
othe
rapy
or c
ogni
tive
beha
viou
ral
Exe
rcis
e
Die
t
T
reat
men
t man
ual f
or li
fest
yle
inte
rven
tion
For
mal
trai
ning
by
lifes
tyle
inte
rven
tioni
sts
S
pec
ific
clas
sific
atio
n o
f co
mp
onen
ts
Ver
y lo
w c
alor
ific,
pre
-pac
kage
d fo
od o
r Eat
ing
man
agem
ent
Low
-cal
orie
die
t B
alan
ced
defic
it di
et
Aer
obic
s, C
allis
then
ics
or L
ifest
yle
exer
cise
W
eigh
t lift
ing
Wal
king
S
elf-m
onito
ring
Stim
ulus
con
trol o
r Con
tinge
ncy
man
agem
ent
%ou
tco
me
due
to/ l
ifest
yle
com
pon
ent
Tria
ls w
ith n
o lif
esty
le c
ompo
nent
T
rials
with
1-3
life
styl
e co
mpo
nent
s %
wei
ght l
oss
attr
ibu
tab
le to
sp
ecifi
c st
rate
gie
s in
pat
ien
ts r
ecei
ving
dru
g
trea
tmen
t D
iet i
nter
vent
ions
vs.
no
diet
inte
rven
tions
27.8
%
0.9%
17
.6%
82
.4%
3.
7%
49.1
%
4.6%
25
.0%
40
.7%
0.
9%
0%
2.8%
23
.1%
3.
7%
28.3
%
46-5
4%
49.5
% v
s. 2
6.5%
Mos
t stu
dies
wer
e co
nduc
ted
with
m
iddl
e-ag
ed o
verw
eigh
t to
mod
erat
ely
obes
e w
omen
in th
eir 4
0s. T
heir
outc
omes
may
not
be
gene
rally
re
leva
nt to
the
larg
er p
opul
atio
n of
ob
esity
pat
ient
s w
ho s
eek
treat
men
t, pa
rticu
larly
thos
e w
ith m
ore
seve
re
obes
ity.
Life
styl
e tre
atm
ents
, with
the
exce
ptio
n of
di
ets,
hav
e no
t bee
n w
idel
y us
ed in
ra
ndom
ised
, pla
cebo
-con
trolle
d ob
esity
dru
g tri
als.
O
besi
ty-p
harm
acot
hera
py tr
ials
do
not u
se
life-
styl
e tre
atm
ents
with
the
frequ
ency
ex
pect
ed b
ased
on
the
offic
ial p
ositi
ons
of
mos
t pro
fess
iona
l org
anis
atio
ns c
once
rned
w
ith th
e co
mpr
ehen
sive
man
agem
ent o
f ob
esity
.

EV
ID
EN
CE
BA
SE
D R
EV
IE
W O
F W
EIG
HT
LO
SS
ME
DIC
IN
ES
: A
RE
PO
RT
CO
MM
IS
SIO
NE
D B
Y T
HE
NE
W Z
EA
LA
ND
AC
C
103
Evi
den
ce T
able
27.
C
om
par
ativ
e d
rug
stu
dy,
Had
dock
et
al.,
2002
Stu
dy
au
tho
rs
and
yea
r
Stu
dy
Des
ign
O
bje
ctiv
e In
clud
ed M
edic
atio
ns
Incl
usio
n
Exc
lusi
on
Exp
osu
re/
Com
pari
son
Ou
tco
mes
(in
clud
ing
ad
vers
e ev
ents
) W
ks
Rx
Dos
e M
g/d
D
rug
min
us
pla
ceb
o (k
g)
Eff
ect s
ize
Val
idity
/App
licab
ility
C
oncl
usi
ons
C
omm
ents
Had
dock
et
al.,
2002
S
tudy
Des
ign
M
eta-
anal
ysis
of R
CTs
O
bje
ctiv
e A
com
preh
ensi
ve m
eta-
anal
ysis
of
RC
Ts
of m
edic
atio
ns fo
r ob
esity
. M
edic
atio
ns
Am
phet
amin
e (d
exam
phet
amin
e)
Ben
zoca
ine
Ben
zphe
tam
ine
Dex
fenf
lura
min
e†
Die
thyl
prop
ion*
F
enflu
ram
ine†
F
luox
etin
e M
azin
dol
Met
ham
phet
amin
e O
rlist
at*
Phe
ndim
etra
zine
P
hent
erm
ine
(HC
L an
d re
sin)
* P
heny
lpro
pano
lam
ine
(PP
A)
Ser
tralin
e S
ibut
ram
ine*
*
curr
ent r
evie
w m
edic
atio
ns
Incl
usio
n
FD
A a
ppro
ved
anti-
obes
ity d
rugs
P
resc
riptio
n or
OT
C o
r of
f lab
el
Stu
dies
pub
lishe
d in
pe
er re
view
ed jo
urna
ls
Pub
lishe
d be
fore
D
ecem
ber 1
999
Eng
lish
vers
ion
avai
labl
e H
uman
stu
dies
P
lace
bo o
r act
ive
com
para
tor
Ran
dom
ised
stu
dy
Out
com
e da
ta a
vaila
ble
Exc
lusi
on
Exp
erim
enta
l obe
sity
dr
ugs
Die
tary
sup
plem
ents
N
=108
clin
ical
tria
ls
incl
uded
Exp
osu
re
Orli
stat
S
ibut
ram
ine
Phe
nter
min
e D
ieth
ylpr
opio
n C
om
par
ison
P
lace
bo
Die
thyl
prop
ion
(9 s
tudi
es)
Orli
stat
(6 s
tudi
es)
Phe
nter
min
e (6
stu
dies
) S
ibut
ram
ine
(4 s
tudi
es)
18(6
-51)
48
(16-
76)
13(2
-24)
15
(8-2
6)
75
303(
190-
360)
28
(15-
30)
14(1
0-20
)
3.0(
-1.6
-11.
5)
2.08
(0.3
0-4.
2)
3.6(
0.6-
6.0)
3.
5(2.
4-5.
1)
<0.8
0 <0
.80
0.81
1.
05
Sta
ndar
dise
d m
ean
diffe
renc
e (d
) bas
ed o
n ch
ange
sco
res
(red
uctio
n in
wei
ght)
used
as
a m
easu
re o
f ef
fect
siz
e, w
here
: d 1
= (X
t i -X
c I)/
Si
Xt i
= m
ean
wei
ght l
oss
treat
men
t gro
up
Xc i
= m
ean
WL
cont
rol
grou
p S
i = p
oole
d S
D o
f ch
ange
for b
oth
Stu
dy w
eigh
ting
– in
vers
e fu
nctio
n of
sa
mpl
e va
rianc
e F
emal
e pr
epon
dera
nce
A la
rge
num
ber o
f st
udie
s di
d no
t pr
esen
t cod
able
da
ta.
Onl
y si
butra
min
e ha
d an
effe
ct s
ize
exce
edin
g 0.
90.
The
abs
olut
e pl
aceb
o-su
btra
cted
w
eigh
t los
s as
soci
ated
with
ant
i- ob
esity
dru
g us
e in
th
e M
A d
id n
ot
exce
ed 4
.0kg
(i.e
., m
odes
t).
Sib
utra
min
e, w
hich
w
as th
e dr
ug w
ith
the
larg
est e
ffect
si
ze, h
ad
over
lapp
ing
CIs
with
ph
ente
rmin
e.
Tre
atm
ent l
engt
h di
d no
t inf
luen
ce e
ffect
si
ze.
† w
ithdr
awn
1997
, NS
= n
ot s
igni
fican
t – i.
e., p
=<0
.05
* n
s if
Bon
ferr
oni’s
cor
rect
ion
for
mul
tiple
test
s is
use
d. O
TC
= o
ver t
he c
ount
er

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
104

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
105
Appendices

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
106
Appendix I. Summary of potential barriers to use of drugs included in the review
† For further details and information see
http://www.medsafe.govt.nz/profs/Datasheet/u/uminetimedcaps.htm http://www.medsafe.govt.nz/profs/Datasheet/d/durominecap.htm http://www.medsafe.govt.nz/profs/Datasheet/t/tenuate%20dospantab.htm http://www.medsafe.govt.nz/profs/Datasheet/r/Reductilcap.htm http://www.medsafe.govt.nz/profs/Datasheet/x/Xenicalcap.htm
Potential barriers to use† Medication
Contraindications Interactions Additional Cautions Phentermine
HCL
30mg Umine
Timedcaps
!5mg & 30mg DuromineTM
�Agitated patients �Alcoholics �Advanced arteriosclerosis �Symptomatic cardiovascular disease �Patients with a history of drug abuse �Glaucoma �Hypertension �Hyperthyroidism �Pregnant females �Valvular heart disease �Children and adolescents
# Hypotensive drugs # Thyroid hormones # MAO inhibitors # Chlorpromazine # Fenfluramine # SSRIs # Tricyclic antidepressants # Alcohol # Anaesthetics
! May impair ability to engage in potentially hazardous activities – e.g., operating machinery, driving a vehicle. ! Potential for abuse (amphetamine family of drugs) and dependence. ! Abrupt cessation after prolonged high doses may result in extreme fatigue, depression and sleep pattern changes. ! Insulin requirement in diabetics may change and strict monitoring of blood glucose is required.
Diethylpropion HCL
75mg
Tenutate Dospan
�Agitated patients �Advanced arteriosclerosis �Patients with a history of drug abuse �Glaucoma �Hypertension �Hyperthyroidism �Hypersensitivity or idiosyncrasy to the
sympthomimetic amine �Patients with pulmonary artery hypertension �Severe hypertension
# MAOI inhibitors # Other anorectic agents # General anaesthetics
! Altered anti-diabetic drug requirements
Sibutramine HCL
10mg & 15mg
Reductil®
�Hypersensitivity to sibutramine or its ingredients �Organic causes of obesity �History of major eating disorders �Psychiatric illness �Giulles de la Tourette’s syndrome �MAOI’s in the past 2 weeks �Other centrally acting drugs for the treatment of
psychiatric, weight reduction �Tryptophan for sleep disorders �History of coronary artery disease, congestive
heart failure, tachycardia, peripheral arterial occlusive disease, arrhythmia or cerebro-vascular disease.
�Inadequately controlled hypertension �Hyperthyroidism �Severe liver or renal impairment �Benign prostatic hyperplasia/urinary retention �Phaeochromocytoma �Narrow angle Glaucoma �Drug, medication or alcohol abuse �Pregnancy or breastfeeding women �Patients under 18 and over 65 years
# CNS active drugs # MAOI’s # Migraine therapy # Concomitant use of SSRI’s # Agents that may raise blood pressure or heart rate – e.g., decongestants, cough cold and allergy medications and anti-inflammatory agents # Drugs that affect cytochrome P450metabolism # Co-administrations of ketoconazole or erythromycin.Cimetidine # Alcohol excess
! Blood pressure and pulse rate should be monitored in all patients as sibutramine has caused clinically relevant increases in blood pressure in some patients. ! Caution is advised in patients taking concomitant medicines known to affect haemostasis or platelet function. ! Seizures have been reported in <0.1% of patients and sibutramine should be given with caution to patients with a history of seizures. ! Sibutramine should be given with caution to patients who have a history of motor or verbal ticks.
Orlistat 120mg
Xenical®
�Chronic malabsorption syndrome �Cholestasis �Known hypersensitivity to orlistat or any of its
components
# Warfarin and other anti-coagulants # Decreased absorption of fat-soluble vitamins D, E and beta-carotene when co-administered with orlistat. If a multivitamin is recommended it should be taken at least two hours after the administration of orlistat or at bedtime. A reduction in cyclosporine plasma levels has been observed with orlistat. Reduction in the exposure to amiodarone and des-ethylamiodarone has been recorded, but the clinical effects are unclear.
! When given with anticoagulants INR values should be monitored. ! Use of a multivitamin could be considered. ! Patients should be advised to use dietary guidelines and fat intake should be distributed over three main meals. ! Improved metabolic control in type 2 diabetes may allow dose reduction of oral hypo-glycaemic medication. ! Monitor cyclosporine levels more frequently when co-administered with orlistat ! Coagulation parameters should be monitored in patients treated with oral anticoagulants. ! There may be reduced therapeutic effects of patients on amiodarone

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
107
Appendix II. Search strategies
Medline strategy
1 exp Obesity/ (56799) 2 (obese or obesity).tw. (56362) 3 weight loss/ (8738) 4 appetite depressants/ (2734) 5 appetite/de (1343) 6 anti-obesity agents/ (628) 7 or/1-6 (82997) 8 exp Phentermine/ (819) 9 duromine.tw. (3) 10 umine.tw. (0) 11 Diethylpropion/ (224) 12 tenuate dospan.tw. (9) 13 sibutramine hydrochloride.tw. (27) 14 Cyclobutanes/ (845) 15 reductil.tw. (8) 16 orlistat.ti. (184) 17 lactones/ (7467) 18 xenical.tw. (30) 19 complan.tw. (9) 20 Food, Formulated/ (4095) 21 or/8-20 (13334) 22 7 and 21 (1214) 23 randomized controlled trials/ (33133) 24 randomized controlled trial.pt. (191180) 25 random allocation/ (51130) 26 double blind method/ (78837) 27 single blind method/ (8255) 28 clinical trial.pt. (386534) 29 exp clinical trials/ (156308) 30 (clinic$ adj trial$).tw. (79327) 31 ((singl$ or doubl$ or treb$ or tripl$) adj (blind$ or mask$)).tw. (75413) 32 placebos/ (23136) 33 placebo$.tw. (84981) 34 randomly allocated.tw. (7750) 35 (allocated adj2 random).tw. (607) 36 meta-analysis/ (5457) 37 (metaanaly$ or meta analy$).tw. (11523) 38 meta analysis.pt. (9354) 39 exp review, literature/ (2051) 40 (systematic adj (review$ or overview$)).tw. (5737) 41 or/23-40 (561105) 42 comment.pt. (253767) 43 letter.pt. (509370) 44 editorial.pt. (163392) 45 animal/ (3653674) 46 human/ (8547910) 47 45 not (45 and 46) (2808546)
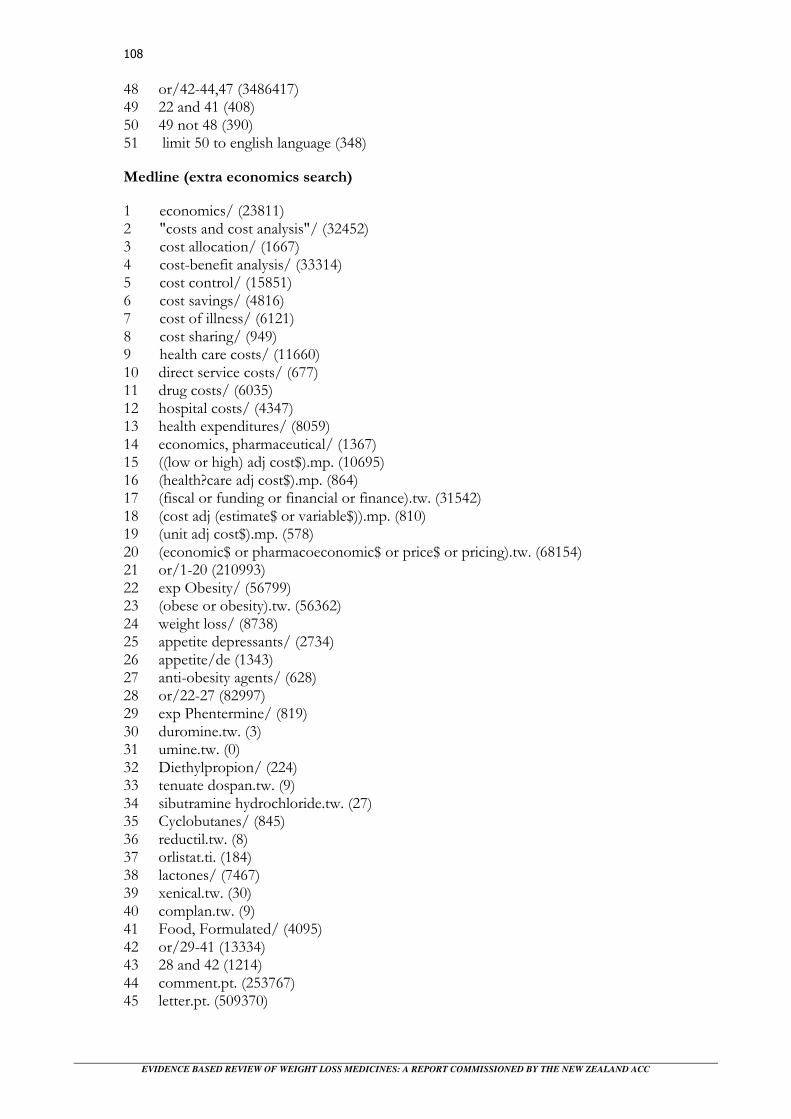
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
108
48 or/42-44,47 (3486417) 49 22 and 41 (408) 50 49 not 48 (390) 51 limit 50 to english language (348)
Medline (extra economics search)
1 economics/ (23811) 2 "costs and cost analysis"/ (32452) 3 cost allocation/ (1667) 4 cost-benefit analysis/ (33314) 5 cost control/ (15851) 6 cost savings/ (4816) 7 cost of illness/ (6121) 8 cost sharing/ (949) 9 health care costs/ (11660) 10 direct service costs/ (677) 11 drug costs/ (6035) 12 hospital costs/ (4347) 13 health expenditures/ (8059) 14 economics, pharmaceutical/ (1367) 15 ((low or high) adj cost$).mp. (10695) 16 (health?care adj cost$).mp. (864) 17 (fiscal or funding or financial or finance).tw. (31542) 18 (cost adj (estimate$ or variable$)).mp. (810) 19 (unit adj cost$).mp. (578) 20 (economic$ or pharmacoeconomic$ or price$ or pricing).tw. (68154) 21 or/1-20 (210993) 22 exp Obesity/ (56799) 23 (obese or obesity).tw. (56362) 24 weight loss/ (8738) 25 appetite depressants/ (2734) 26 appetite/de (1343) 27 anti-obesity agents/ (628) 28 or/22-27 (82997) 29 exp Phentermine/ (819) 30 duromine.tw. (3) 31 umine.tw. (0) 32 Diethylpropion/ (224) 33 tenuate dospan.tw. (9) 34 sibutramine hydrochloride.tw. (27) 35 Cyclobutanes/ (845) 36 reductil.tw. (8) 37 orlistat.ti. (184) 38 lactones/ (7467) 39 xenical.tw. (30) 40 complan.tw. (9) 41 Food, Formulated/ (4095) 42 or/29-41 (13334) 43 28 and 42 (1214) 44 comment.pt. (253767) 45 letter.pt. (509370)

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
109
46 editorial.pt. (163392) 47 animal/ (3653674) 48 human/ (8547910) 49 47 not (47 and 48) (2808546) 50 or/44-46,49 (3486417) 51 21 and 28 and 42 (28) 52 51 not 50 (24) 53 limit 52 to english language (21) Embase
1 Diabetic Obesity/ (437) 2 obesity/ or morbid obesity/ (40399) 3 weight reduction/ (18379) 4 (obese or obesity).tw. (36765) 5 or/1-4 (62130) 6 Phentermine/ (751) 7 duromine.tn,tw. (11) 8 umine.tn,tw. (0) 9 Amfepramone/ (375) 10 tenuate dospan.tn,tw. (22) 11 Sibutramine/ (882) 12 reductil.tn,tw. (110) 13 Tetrahydrolipstatin/ (1055) 14 xenical.tn,tw. (323) 15 complan.tn,tw. (1) 16 complan/ (1) 17 reductil/ (882) 18 tenuate dospan/ (375) 19 duromine/ (103) 20 umine/ (0) 21 ensure/ (48) 22 (meal adj3 replace$).tw. (73) 23 or/6-22 (2308) 24 5 and 23 (1436) 25 exp meta analysis/ (18397) 26 (metaanaly$ or meta analy$).tw. (10151) 27 (systematic$ adj (review$ or overview$)).mp. (5300) 28 randomized controlled trials/ (85380) 29 clinical trial/ (296906) 30 randomization/ (10898) 31 single blind procedure/ (4761) 32 double blind procedure/ (47475) 33 crossover procedure/ (14990) 34 placebo/ (44490) 35 randomi?ed controlled trial$.tw. (13528) 36 (clinic$ adj trial$).tw. (63823) 37 ((singl$ or doubl$ or tripl$ or trebl$) adj (blind$ or mask$)).tw. (55628) 38 placebo$.tw. (65892) 39 (random$ adj allocat$).tw. (6611) 40 prospective study/ (38007) 41 or/25-40 (421878)
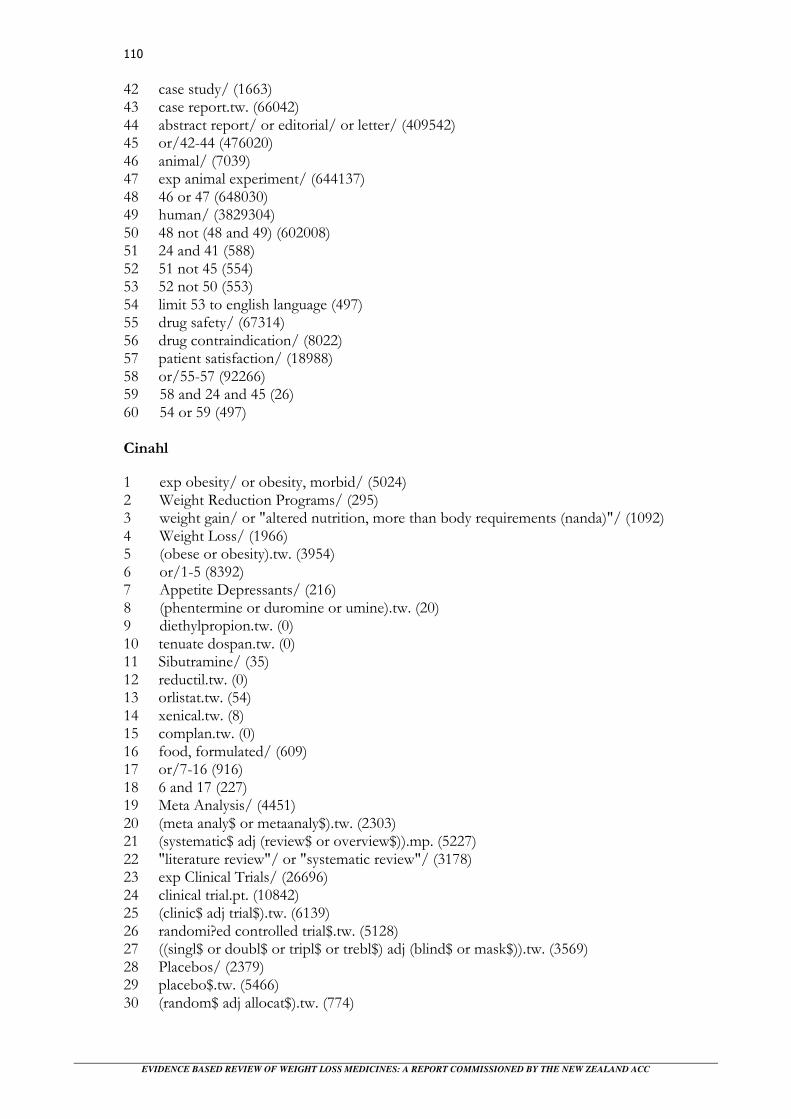
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
110
42 case study/ (1663) 43 case report.tw. (66042) 44 abstract report/ or editorial/ or letter/ (409542) 45 or/42-44 (476020) 46 animal/ (7039) 47 exp animal experiment/ (644137) 48 46 or 47 (648030) 49 human/ (3829304) 50 48 not (48 and 49) (602008) 51 24 and 41 (588) 52 51 not 45 (554) 53 52 not 50 (553) 54 limit 53 to english language (497) 55 drug safety/ (67314) 56 drug contraindication/ (8022) 57 patient satisfaction/ (18988) 58 or/55-57 (92266) 59 58 and 24 and 45 (26) 60 54 or 59 (497) Cinahl
1 exp obesity/ or obesity, morbid/ (5024) 2 Weight Reduction Programs/ (295) 3 weight gain/ or "altered nutrition, more than body requirements (nanda)"/ (1092) 4 Weight Loss/ (1966) 5 (obese or obesity).tw. (3954) 6 or/1-5 (8392) 7 Appetite Depressants/ (216) 8 (phentermine or duromine or umine).tw. (20) 9 diethylpropion.tw. (0) 10 tenuate dospan.tw. (0) 11 Sibutramine/ (35) 12 reductil.tw. (0) 13 orlistat.tw. (54) 14 xenical.tw. (8) 15 complan.tw. (0) 16 food, formulated/ (609) 17 or/7-16 (916) 18 6 and 17 (227) 19 Meta Analysis/ (4451) 20 (meta analy$ or metaanaly$).tw. (2303) 21 (systematic$ adj (review$ or overview$)).mp. (5227) 22 "literature review"/ or "systematic review"/ (3178) 23 exp Clinical Trials/ (26696) 24 clinical trial.pt. (10842) 25 (clinic$ adj trial$).tw. (6139) 26 randomi?ed controlled trial$.tw. (5128) 27 ((singl$ or doubl$ or tripl$ or trebl$) adj (blind$ or mask$)).tw. (3569) 28 Placebos/ (2379) 29 placebo$.tw. (5466) 30 (random$ adj allocat$).tw. (774)
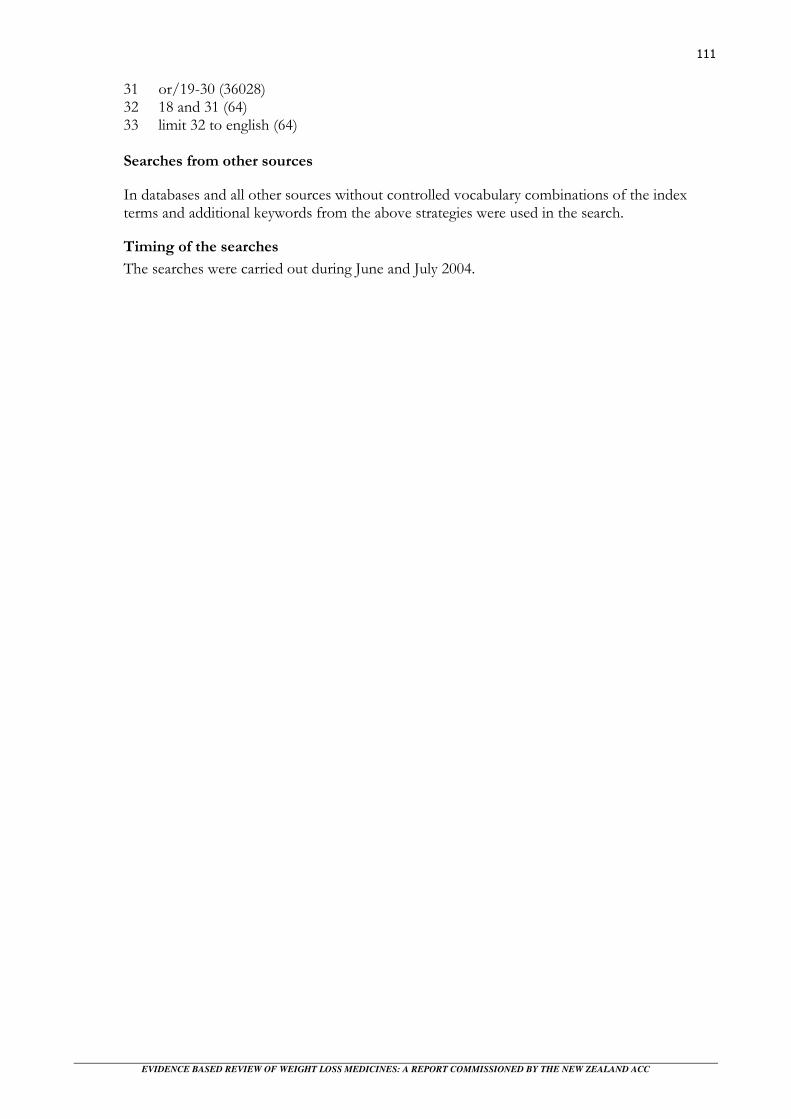
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
111
31 or/19-30 (36028) 32 18 and 31 (64) 33 limit 32 to english (64) Searches from other sources
In databases and all other sources without controlled vocabulary combinations of the index terms and additional keywords from the above strategies were used in the search.
Timing of the searches
The searches were carried out during June and July 2004.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
112

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
113
References
Allison, D. B., Gadbury, G., Schwartz, L. G., Murugesan, R., Kraker, J. L., Heshka, S., Fontaine, K. R., et al. (2003). A novel soy-based meal replacement formula for weight loss among obese individuals: a randomized controlled clinical trial. European Journal of Clinical Nutrition, 57, 514-522. Arterburn, D., & Hitchcock, N. P. (2001). Obesity. BMJ, 322, 1406-1409. Arterburn, D. E., Crane, P. K., & Veenstra, D. L. (2004). The efficacy and safety of sibutramine for weight loss: a systematic review. Archives of Internal Medicine, 164, 994-1003. Astrup, A., & Toubro, S. (2001). When, for whom and how to use sibutramine? International Journal of Obesity, 25, S2-S7. Avenell, A., Broom, I., Brown, T. J., Poobalan, A., Aucott, L., Stearns, S. C., Smith, W. C. S., et al. (2004). Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technology Assessment, 8. Bergstrom, A., Hsieh, C. C., Lindblad, P., Lu, C. M., Cook, N. R., & Wolk, A. (2001a). Obesity and renal cell cancer: a quantitative review. British Journal of Cancer, 85, 984-990. Bergstrom, A., Pisani, P., Tenet, V., Wolk, A., & Adami, H. O. (2001b). Overweight as an avoidable cause of cancer in Europe. International Journal of Cancer, 91, 421-430. Berkowitz, R. I., Wadden, R. A., Tershakovec, A. M., & Cronquist, J. L. (2003). Behavior therapy and sibutramine for the treatment of adolescent obesity: a randomized controlled trial. JAMA, 289, 1805-1812. Bradley, P. S., Maddox, R. R., & North, W. K. (1999). Bupropion sr with phentermine for weight reduction, 51st Institute on Psychiatric Services: 29th October-2nd November 1999, New Orleans. Bray, G. A., Blackburn, G. L., Ferguson, J. M., Greenway, F. L., Jain, A. K., Mendel, C. M., Mendels, J., et al. (1999). Sibutramine produces dose-related weight loss. Obesity Research, 7, 189-198. Bray, G. A., Hollander, P., Klein, S., Kushner, R., Levy, B., Fitchet, M., & Perry, B. H. (2003). A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obesity Research, 11, 722-733. Brower, V. (2002). Fighting fat. New drugs against obesity in the pipeline. EMBO Reports, 3, 601-603. Brown, C. D., Higgins, M., Donato, K. A., Rohde, F. C., Garrison, R., Obarzanek, E., Ernst, N. D., et al. (2000). Body mass index and the prevalence of hypertension and dyslipidemia. Obesity Research, 8, 605-619. Calle, E. E., Rodriguez, C., Walker-Thurmond, K., & Thun, M. J. (2003). Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. New England Journal of Medicine, 348, 1625-1638.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
114
Carey, V. J., Walters, E. E., Colditz, G. A., Solomon, C. G., Willett, W. C., Rosner, B. A., Speizer, F. E., et al. (1997). Body fat distribution and risk of non-insulin-dependent diabetes mellitus in women. The Nurses' Health Study. American Journal of Epidemiology, 145, 614-619. Chan, J. M., Rimm, E. B., Colditz, G. A., Stampfer, M. J., & Willett, W. C. (1994). Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care, 17, 961-969. Davidson, M. H. (1999). Weight control and risk factor reduction in obese subjects treated for 2 years with Orlistat: a randomized controlled trial. JAMA, 281, 1174-1174. Derosa, G., Mugellini, A., Ciccarelli, L., & Fogari, R. (2003). Randomized, double-blind, placebo-controlled comparison of the action of orlistat, fluvastatin, or both on anthropometric measurements, blood pressure, and lipid profile in obese patients with hypercholesterolemia prescribed a standardized diet. Clinical Therapeutics, 25, 1107-1122. Ettinger, M.P., Littlejohn, T.W., Schwartz, S.L., Weiss, S.R., McIlwain, H.H., Heymsfield, S.B. (2003). Recombinant variant of ciliary neurotrophic factor for weight loss in obese adults: a randomized, dose-ranging study. JAMA, 289, 1826-1832. Foxcroft, D. R., & Milne, R. (2000). Orlistat for the treatment of obesity: rapid review and cost-effectiveness model. Obesity Reviews, 1, 121-126. Gardin, J. M., Schumacher, D., Constantine, G., Davis, K. D., Leung, C., & Reid, C. L. (2000). Valvular abnormalities and cardiovascular status following exposure to dexfenfluramine or phentermine/fenfluramine. Journal of the American Medical Association, 283, 1703-1709. Glazer, G. (2001). Long-term pharmacotherapy of obesity 2000: a review of efficacy and safety. Archives of Internal Medicine, 161, 1814-1824. Gokcel, A., Karakose, H., Ertorer, E. M., Tanaci, N., Tutuncu, N. B., & Guvener, N. (2001). Effects of sibutramine in obese female subjects with type 2 diabetes and poor blood glucose control. Diabetes Care, 24, 1957-1960. Haddock, C. K., Poston, W. S. C., Dill, P. L., Foreyt, J. P., & Ericsson, M. (2002). Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. International Journal of Obesity, 26, 262-273. Halpern, A., & Mancini, M. C. (2003). Treatment of obesity: an update on anti-obesity medications. Obesity Reviews, 4, 25-42. Halpern, A., Mancini, M. C., Suplicy, H., Zanella, M. T., Repetto, G., Gross, J., Jadzinsky, M., et al. (2003). Latin-American trial or orlistat for weight loss and improvement in glycaemic profile in obese diabetic patients. Diabetes, Obesity & Metabolism, 5, 180-188. Hanefeld, M., & Sachse, G. (2002). The effects of orlistat on body weight and glycaemic control in overweight patients with type 2 diabetes: a randomized, placebo-controlled trial. Diabetes, Obesity & Metabolism, 4, 415-423. Hansen, D., Astrup, A., Toubro, S., Finer, N., Kopelman, P., Hilsted, J., Rossner, S., et al. (2001). Predictors of weight loss and maintenance during 2 years of treatment by sibutramine in obesity. Results from the European multi-centre STORM trial. Sibutramine Trial of Obesity

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
115
Reduction and Maintenance. International Journal of Obesity & Related Metabolic Disorders: Journal of the International Association for the Study of Obesity, 25, 496-501. Hauner, H., Meier, M., Jockel, K. H., Frey, U. H., & Siffert, W. (2003). Prediction of successful weight reduction under sibutramine therapy through genotyping of the G-protein beta3 subunit gene (GNB3) C825T polymorphism. Pharmacogenetics, 13, 453-459. Hazenberg, B. P. (2000). Randomized, double-blind, placebo-controlled, multicenter study of sibutramine in obese hypertensive patients. Cardiology, 94, 152-158. Heck, A. M., Calis, K. A., McDuffie, J. R., Carobene, S. E., & Yanovski, J. A. (2002). Additive gastrointestinal effects with concomitant use of olestra and orlistat. Annals of Pharmacotherapy, 36, 1003-1005. Hensrud, D. D. (2000). Pharmacotherapy for obesity. Medical Clinics of North America, 84, 463-476. Hensrud, D. D. (2004). Diet and obesity. Current Opinion in Gastroenterology, 20, 119-124. Hensrud, D. D., Billington, C., Blum, H. T., & Gonzales-Campoy, J. M. (2003). Pharmacological approaches to weight loss. Bloomington, M.N.: Institute for Clinical Systems Improvement (ICSI). Heymsfield, S. B., Segal, K. R., Hauptman, J., Lucas, C. P., Boldrin, M. N., Rissanen, A., Wilding, J. P., et al. (2000). Effects of weight loss with orlistat on glucose tolerance and progression to type 2 diabetes in obese adults. Archives of Internal Medicine, 160, 1321-1326. Heymsfield, S. B., Van Mierlo, C. A. J., Van Der Knaap, H. C. M., Heo, M., & Frier, H. I. (2003). Weight management using a meal replacement strategy: meta and pooling analysis from six studies. International Journal of Obesity, 27, 537-549. Hollander, P. A., Elbein, S. C., Hirsch, I. B., Kelley, D., McGill, J., Taylor, T., Weiss, S. R., et al. (1998). Role of orlistat in the treatment of obese patients with type 2 diabetes. A 1-year randomized double-blind study. Diabetes Care, 21, 1288-1294. James, W. P., Astrup, A., Finer, N., Hilsted, J., Kopelman, P., Rossner, S., Saris, W. H., et al. (2000). Effect of sibutramine on weight maintenance after weight loss: a randomised trial. STORM Study Group. Sibutramine Trial of Obesity Reduction and Maintenance. Lancet, 356, 2119-2125. James, W. P. T. (2001). A new drug to maintain weight loss. Hospital Practice, 36, 22-23. Jung, R.T. (1997). Obesity as a disease. British Medical Bulletin, 53, 307-321. Kim, S. H., Lee, Y. M., Jee, S. H., & Nam, C. M. (2003). Effect of sibutramine on weight loss and blood pressure: a meta-analysis of controlled trials. Obesity Research, 11, 1116-1123. Krempf, M., Louvet, J. P., Allanic, H., Miloradovich, T., Joubert, J. M., & Attali, J. R. (2003). Weight reduction and long-term maintenance after 18 months treatment with orlistat for obesity. International Journal of Obesity & Related Metabolic Disorders: Journal of the International Association for the Study of Obesity, 27, 591-597.
EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
116
Lamotte, M., Annemans, L., Lefever, A., Nechelput, M., & Masure, J. (2002). A health economic model to assess the long-term effects and cost-effectiveness of orlistat in obese type 2 diabetic patients. Diabetes Care, 25, 303-308. Lean, M. E. J. (2001). How does sibutramine work? International Journal of Obesity, 25, S8-S11. Leung, W. Y., Neil Thomas, G., Chan, J. C., & Tomlinson, B. (2003). Weight management and current options in pharmacotherapy: orlistat and sibutramine. Clinical Therapeutics, 25, 58-80. Manson, J. E., Colditz, G. A., Stampfer, M. J., Willett, W. C., Rosner, B., Monson, R. R., Speizer, F. E., et al. (1990). A prospective study of obesity and risk of coronary heart disease in women. New England Journal of Medicine, 322, 882-889. McElroy, S.L., Arnold, L.M., Shapira, N.A., Keck, P.E., Rosenthal, N.R., Karim, M.R. (2003). Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. American Journal of Psychiatry, 160, 255-261. McKay, R. H. (1973). Long-term use of diethylpropion in obesity. Current Medical Research & Opinion, 1, 489-493. McNulty, S. J., Ur, E., & Williams, G. (2003). A randomized trial of sibutramine in the management of obese type 2 diabetic patients treated with metformin. Diabetes Care, 26, 125-131. McTigue, K. M., Harris, R., Hemphill, B., Lux, L., Sutton, S., Bunton, A. J., & Lohr, K. N. (2003). Screening and interventions for obesity in adults: summary of the evidence for the U.S. Preventive Services Task Force. Annals of Internal Medicine, 139.
Medicines Control Agency Committtee on Safety in Medicines (2004). Important safety
message: European withdrawal of anorectic agents/appetite suppressants: new legal
developments, no new safety issues: Licences for phentermine and amfepramone being
withdrawn May 2001. Available from:
http://www.mca.gov.uk/ourwork/monitorsafequalmed/safetymessages/anorectic.htm Medsafe (2003). Duromine™: phentermine capsules 15mg and 30mg: data sheet. Wellington: NZ, Ministry of Health. Medsafe (2004a). REDUCTIL®: sibutramine hydrochloride: data sheet. Wellington: NZ, Ministry of Health. Medsafe (2004b). Tenuate dospan: diethylpropion hydrochloride 75 mg tablet: data sheet. Wellington: NZ, Ministry of Health. Medsafe (2004c). Xenical®: orlistat 120mg capsules: data sheet. Wellington: NZ, Ministry of Health. Muls, E., Kolanowski, J., Scheen, A., & Van Gaal, L. (2001). The effects of orlistat on weight and on serum lipids in obese patients with hypercholesterolemia: a randomized, double-blind, placebo-controlled, multicentre study. International Journal of Obesity, 25, 1713-1721. Munro, J. F. (1979). Clinical aspects of the treatment of obesity by drugs: a review. International Journal of Obesity, 3, 171-180.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
117
Munro, J. F., MacCusih, A. C., & Wilson, E. M. (1968). Comparison of continuous and intermittent anorectic therapy in obesity. BMJ, 1, 352-354. NHS Centre for Reviews and Dissemination (1997). The prevention and treatment of obesity. Effective Health Care, 3. Nisoli, E., & Carruba, M. O. (2003). A benefit-risk assessment of sibutramine in the management of obesity. Drug Safety, 26, 1027-1048. Oliveria, S. A., Felson, D. T., Cirillo, P. A., Reed, J. I., & Walker, A. M. (1999). Body weight, body mass index, and incident symptomatic osteoarthritis of the hand, hip, and knee. Epidemiology, 10, 161-166. O'Meara, S., Glenny, A. M., Sheldon, T., Melville, A., & Wilson, C. (1998). Systematic review of the effectiveness of interventions used in the management of obesity. Journal of Human Nutrition & Dietetics, 11, 203-206. O'Meara, S., Riemsma, R., Shirran, L., Mather, L., & ter Riet, G. (2001). A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity. Health Technology Assessment, 5, 1-81. O'Meara, S., Riemsma, R., Shirran, L., Mather, L., & ter Riet, G. (2002). The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment. Health Technology Assessment, 6, 1-97. Padwal, R., Li, S. K., & Lau, D. C. W. (2004). Long-term pharmacotherapy for obesity and overweight. Cochrane Database of Systematic Reviews. Poston, W. S. C., Haddock, C. K., Dill, P. L., Thayer, B., & Foreyt, J. P. (2001). Lifestyle treatments in randomized clinical trials of pharmacotherapies for obesity. Obesity Research, 9, 552-563. Proietto, J., & Baur, L. A. (2004). Management of obesity. Medical Journal of Australia, 180, 474-480. Rimm, E. B., Stampfer, M. J., Giovannucci, E., Ascherio, A., Spiegelman, D., Colditz, G. A., & Willett, W. C. (1995). Body size and fat distribution as predictors of coronary heart disease among middle-aged and older US men. American Journal of Epidemiology, 141, 1117-1127. Rissanen, P., Vahtera, E., Krusius, T., Uusitupa, M., & Rissanen, A. (2001). Weight change and blood coagulability and fibrinolysis in healthy obese women. International Journal of Obesity & Related Metabolic Disorders: Journal of the International Association for the Study of Obesity, 25, 212-218. Rothman, R. B., & Baumann, M. H. (2000). Neurochemical mechanisms of phentermine and fenfluramine: therapeutic and adverse effects. Drug Development Research, 51, 52-65. Rothman, R. B., Redmon, J. B., Raatz, S. K., Kwong, C. A., Swanson, J. E., & Bantle, J. P. (2000). Chronic treatment with phentermine combined with fenfluramine lowers plasma serotonin. American Journal of Cardiology, 85, 913-915. Schuh, L. M., Schuster, C. R., Hopper, J. A., & Mendel, C. M. (2000). Abuse liability assessment of sibutramine, a novel weight control agent. Psychopharmacology, 147, 339-346.

EVIDENCE BASED REVIEW OF WEIGHT LOSS MEDICINES: A REPORT COMMISSIONED BY THE NEW ZEALAND ACC
118
Silverstone, T. (1992). Appetite suppressants: a review. Drugs, 43, 820-836. Sjostrom, L., Rissanen, A., Andersen, T., Boldrin, M., Golay, A., Koppeschaar, H. P. F., & Krempf, M. (1998). Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. Lancet, 352, 167-172. Steel, J. M., Munro, J. F., & Duncan, L. J. (1973). A comparative trial of different regimens of fenfluramine and phentermine in obesity. Practitioner, 211, 232-236. Tambascia, M. A., Geloneze, B., Repetto, E. M., Geloneze, S. R., Picolo, M., & Magro, D. O. (2003). Sibutramine enhances insulin sensitivity ameliorating metabolic parameters in a double-blind, randomized, placebo-controlled trial. Diabetes, Obesity & Metabolism, 5, 338-344. Thearle, M., & Aronne, L. J. (2003). Obesity and pharmacologic therapy. Endocrinology & Metabolism Clinics of North America, 32, 1005-1024. Torgerson, J. S. (2004). Preventing diabetes in the obese: the XENDOS study and its context. British Journal of Diabetes & Vascular Disease, 4, 22-27. Torgerson, J. S., Hauptman, J., Boldrin, M. N., & Sjostrom, L. (2004). XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care, 27, 155-161. Truant, A. P., Olon, L. P., & Cobb, S. (1972). Phentermine resin as an adjunct in medical weight reduction: a controlled, randomized, double-blind prospective study. Current Therapeutic Research, Clinical & Experimental, 14, 726-738. Wadden, T. A., Berkowitz, R. I., Womble, L. G., Sarwer, D. B., Arnold, M. E., & Steinberg, C. M. (2000). Effects of sibutramine plus orlistat in obese women following 1 year of treatment by sibutramine alone: a placebo-controlled trial. Obesity Research, 8, 431-437. Warren, E., Brennan, A., & Akehurst, R. (2004). Cost-effectiveness of sibutramine in the treatment of obesity. Medical Decision Making, 24, 9-19. Weintraub, M., Hasday, J. D., Mushlin, A. I., & Lockwood, D. H. (1984). A double-blind clinical trial in weight control. Use of fenfluramine and phentermine alone and in combination. Archives of Internal Medicine, 144, 1143-1148. Weintraub, M., Rubio, A., Golik, A., Byrne, L., & Scheinbaum, M. L. (1991). Sibutramine in weight control: a dose-ranging, efficacy study. Clinical Pharmacology & Therapeutics, 50, 330-337. Wilding, J. (2004). Clinical evaluation of anti-obesity drugs. Current Drug Targets, 5, 325-332. Wilson, B. D., Wilson, N. C., & Russell, D. G. (2001). Obesity and body fat distribution in the New Zealand population. New Zealand Medical Journal, 114, 127-130. Wirth, A., & Krause, J. (2001). Long term weight loss with sibutramine: randomized controlled trial. JAMA, 286, 1331-1339.