Embed Size (px)
Citation preview
76 Health is Global
Using evidence and innovation to strengthen policy and practice
‘Stronger emphasis should be placed on translating knowledge into action to improve public health by bridging the gap between what is known and what is actually being done.’
WHO World Report on Knowledge for Better Health142
Knowledge derived from research and experience is of little value unless it is put into practice, and its success monitored and regularly evaluated. Closing the gap between what we know will work to improve health and what is put into practice around the world could save millions of lives over the coming decade.This requires a better understanding of how to promote the uptake and implementation of interventions and policies already shown to be effective.143
We will make sure that our research funding includes support for work in this area and will use the forums above to share best practice. We will continue to make independent advice from our scientific advisory committees publicly accessible, in line with the Code of Practice for Scientific Advisory Committees by the Government Office for Science.144
If policy makers are going to use the findings of research, they must be closely involved in owning the work from the onset. Following this principle, we will work with others to develop capability for policy makers to engage in this process effectively.WHO’s
Evidence Informed Policy Network (EVIPNet) is an example of an important initiative in this area (see Box 21).
Box 21:WHO Evidence Informed Policy Network
‘EVIPNet is an innovative initiative to promote the systematic use of health research evidence in policy making. Focusing on low- and middle-income countries, EVIPNet promotes partnerships at the country level between policy makers, researchers and civil society in order to facilitate both policy development and policy implementation through the use of the best scientific evidence available.
‘Low- and middle-income countries have scarce resources to address their health system challenges and need high-quality evidence to use those resources efficiently. Scientific evidence is a fundamental building block to improve the public health situation. If health sector managers and policy makers ignore evidence on the root causes of problems or what works best to address these problems, they risk wasting precious resources on inadequately designed programmes and policies.The direct consequence of ignoring this evidence is poor health for the population.’
WHO Evidence Informed Policy Network website (www.who.int/rpc/evipnet/en)
142 World Health Organization. World Report on Knowledge for Better Health. Geneva:WHO; 2004. 143 Sanders D and Haines A. Implementation research is needed to achieve international health goals. PLoS Med 2006;
3(6): e186. 144 The Code of Practice was published by the Government Office for Science in 2007 and is available at:
www.dius.gov.uk/publications/fi le42780.pdf.
Comment
1130 www.thelancet.com Vol 372 September 27, 2008
angiotensin-converting-enzyme inhibitors should remain the preferred renin-active agent to prevent vascular events in patients with or at high risk for cardiovascular disease.
*Toni L Ripley, Donald HarrisonUniversity of Oklahoma College of Pharmacy, Oklahoma City, OK 73190, [email protected]
We declare that we have no confl ict of interest.
1 Jorde UP, Ennezat PV, Lisker J, et al. Maximally recommended doses of angiotensin-converting-enzyme (ACE) inhibitors do not completely prevent ACE-mediated formation of angiotensin II in chronic heart failure. Circulation 2000; 101: 844–46.
2 McKelvie RS, Yusuf S, Pericak D, et al, for the RESOLVD Pilot Study Investigators. Comparison of candesartan, enalapril, and their combination in congestive heart failure: Randomized Evaluation of Strategies for Left Ventricular Dysfunction (RESOLVD) Pilot Study. Circulation 1999; 100: 1056–64.
3 The Heart Outcomes Prevention Evaluation Study Investigators. Eff ects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high risk patients. N Engl J Med 2000; 342: 145–53.
4 The Telmisartan Randomised AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease (TRANSCEND) Investigators. Eff ects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trial. Lancet 2008; published online Aug 31. DOI:10.1016/S0140-6736(08)61242-8.
EVIPNet Americas: informing policies with evidencePublic-health and health-system policies based on sound scientifi c evidence and best practices can improve health and equity, and the use of research results is essential for health and development.1–5 Yet accessing and incorporating research evidence to inform decision making does not occur systematically, but is especially critical in low-income and middle-income countries that face tremendous health challenges with insuffi cient resources. WHO is actively working to address this issue. Evidence-Informed Policy Network (EVIPNet) arose from the Ministerial Summit on Health Research in Mexico City in 2004 and a resolution adopted by the 58th World Health Assembly in 2005.6–8
The goal of EVIPNet is to improve public health and reduce inequities by increasing the systematic use of and access to high-quality applicable evidence that guides the development of policies, and helps to identify and prioritise knowledge gaps that need attention. EVIPNet addresses important issues as identifi ed by individual countries, such as maternal and child health, HIV and AIDS control, immunisation, and infectious diseases, as well as health-system challenges such as fi nancing, distri-bution of health workers, and governance. EVIPNet’s
framework is based on current evidence on eff ective strategies for knowledge dissemination that are adapted for local context.
EVIPNet has been set up in several regions. EVIPNet was started in Asia in 2005 (with teams in Laos, Malaysia, the Philippines, and Vietnam, and three teams in China), and in Africa in 2006 (with teams in Burkina Faso, Cameroon, Central African Republic, Ethiopia, Mozambique, Niger, and Zambia). Country teams are led by senior health offi cials from government, in partnership with representatives from national science and technology institutions and academia, among others.
The next wave of EVIPNet is being led by the Pan American Health Organization (PAHO) in the Americas. In 2007, PAHO, through its country offi ces, identifi ed countries that had requested technical cooperation for promoting evidence-informed decision making. Bolivia, Brazil, Chile, Costa Rica, Colombia, Mexico (both the national government and a Mexico–USA border offi ce), Puerto Rico, and Trinidad and Tobago were identifi ed as the fi rst round of EVIPNet participants. Local commitment, as well as the support of health authorities, was essential in planning and developing EVIPNet.
5 The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET) Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008; 358: 1547–59.
6 The EURopean trial On reduction of cardiac events with Perindopril in stable coronary Artery disease Investigators. Effi cacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet 2003; 362: 782–88.
7 The Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) Investigators. Angiotensin-converting-enzyme inhibition in stable coronary artery disease. N Engl J Med 2004; 351: 2058–68.
8 Granger CB, McMurray JJV, Yusuf S, et al, for the CHARM Investigators and Committees. Eff ects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet 2003; 362: 772–76.
9 Dahlöf, B, Devereux RB, Kjeldsen SE, et al, for the LIFE study group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359: 995–1003.
10 Kahn N, McAlister FA. Re-examining the effi cacy of β-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174: 1737–42.
11 Mochizuki S, Dahlöf B, Shimizu M, et al, for the Jikei Heart Study group. Valsartan in a Japanese population with hypertension and other cardiovascular disease (Jikei Heart Study): a randomised, open-label, blinded endpoint morbidity-mortality study. Lancet 2007; 369: 1431–39.

Comment
www.thelancet.com Vol 372 September 27, 2008 1131
In July, 2007, EVIPNet was introduced to country teams (fi gure). In addition, PAHO assembled a strong international resource group with expertise in knowledge transfer for policy making. This group provides technical support, participates in network activities, and has been responsible for reviewing country-work proposals. An evidence portal was launched in 2007 to provide access to reliable evidence sources, including the Cochrane Library (in English) and Cochrane Library Plus (in Spanish). The portal was developed jointly by PAHO’s Latin American and Caribbean Centre on Health Sciences Informa tion.9 A global EVIPNet website is under development and will serve as a knowledge-management tool for all EVIPNet teams, by providing them with a one-stop shop for retrieving evidence summaries and other relevant resources. Lastly, an evaluation protocol has been developed to measure the impact of EVIPNet worldwide. This eff ort is led by John Lavis at McMaster University.
Participating countries have shown tremendous interest and commitment to EVIPNet. What is lacking is ongoing funding dedicated to accessing and pro-moting research results. For many funding agencies, evidence-informed decision making falls between the cracks. Traditional research agencies see it as development work, and therefore not within their funding remit, while development agencies often consider it within the research realm, and therefore not part of their mandate. Fortunately, a few visionary organisations do recognise that ensuring that the results of research are actually used to inform policy and practice is as important as supporting the production of high-quality research. Other support networks have evolved, and research production and use are becoming components of the public-health agenda in the Americas.10,11
Successful implementation of EVIPNet in the Americas depends on several factors. Ministries of health need to live up to their commitment to EVIPNet by creating mechanisms and long-term strategies that encourage the use of evidence to shape policies, while stimulating a dialogue with the producers of research evidence. EVIPNet teams across Latin America (and around the world), need to work together to share experiences and strengthen their capacities in key areas such as interpreting systematic reviews or summarising existing evidence through the development of policy briefs that address a particular question. Moreover, wealthier countries need to work with those that have fewer
resources to stimulate this work. No single person or organisation can infl uence systematic change. However, if the collective commitment to EVIPNet’s goals currently displayed is any indication of potential future impact, we are on the right track toward ensuring that research evidence is systematically used to improve health.
EVIPNet Americas SecretariatPan American Health Organization/World Health Organization, Washington, DC 20037, [email protected]
Written on behalf of the EVIPNet Americas Secretariat by: Sonya Corkum, Luis Gabriel Cuervo, and Analía Porrás, from PAHO/WHO. We thank Fabio Zicker, Tomas Pantoja, and John Lavis from the EVIPNet Resource Group, and José Luis Di Fabio, and María Luisa Clark from PAHO/WHO, for constructive comments and guidance. We also thank the Swedish International Development Agency, the Alliance for Health Systems and Policy Research, European Commission Framework Programme 7, and Health Canada for fi nancial support and commitment to EVIPNet. We declare that we have no confl ict of interest.
1 Chalmers I. If evidence-informed policy works in practice, does it matter if it doesn’t work in theory? Evidence Policy 2005; 1: 227–42.
2 Lavis JN, Davies HTO, Oxman AD, Denis JL, Golden-Biddle K, Ferlie E. Towards systematic reviews that inform healthcare management and policymaking. J Health Serv Res Policy 2005; 10 (suppl 1): 35–48.
3 Lavis JN, Posada FB, Haines A, Osei E. Use of research to inform public policymaking. Lancet 2004; 364: 1615–21.
4 WHO. World report on knowledge for better health. 2004. http://www.who.int/rpc/meetings/wr2004/en/index13.html (accessed May 16, 2008).
5 Commission on Health Research for Development. Health research: essential link to equity in development. Oxford: Oxford University, 1990.
6 Hamid M, Bustamante-Manaog T, Dung TV, et al. EVIPNet: translating the spirit of Mexico. Lancet 2005; 366: 1758–60.
7 Ministerial Summit on Health Research. The Mexico Statement on Health Research. Knowledge for better health: strengthening health systems. Nov 16–20, 2004. http://www.who.int/rpc/summit/agenda/Mexico_Statement-English.pdf (accessed May 16, 2008).
8 World Health Assembly. Ministerial Summit on Health Research: WHA 58.34. May 25, 2005. http://www.who.int/gb/ebwha/pdf_f iles/WHA58/WHA58_34-en.pdf (accessed May 16, 2008).
9 Evidence Portal Virtual Health Library [Internet] BIREME Latin American & Caribbean Centre on Health Science Information. http://evidences.bvsalud.org/php/index.php?lang=en (cited June 13, 2008).
10 Pan American Health Organization. Proposed strategic plan 2008–2012 . October, 2007. http://www.paho.org/english/gov/csp/od328-full-e.pdf (accessed May 16, 2008).
11 Ministers of Health of the Americas. Health agenda for the Americas 2008–2012. June, 2007. http://www.paho.org/English/D/HAgenda_English.pdf (accessed May 16, 2008).
Figure: EVIPNET Americas introductory workshop, PAHO/WHO headquarters, Washington, DC, USA, 2007

Comment
It has been said that policymakers see research as theopposite of “action” rather than the opposite of “ignor-ance”. How can we overturn such sentiments so thatpolicymakers see research as a means of accessingknowledge and as the foundation for effective action?
In November, 2004, 20 ministers of health and seniorpolicymakers from 52 countries met in Mexico todiscuss how research can help them in their dauntingtask to develop and implement effective healthpolicies.1,2 Informed by the World Report on Knowledge forBetter Health,3 the outcomes of the ministerial summitmade their way into resolutions at the World HealthAssembly in May, 2005,4 with specific stepsrecommended on how knowledge can be used tostrengthen national health systems in the developingworld.
A year after Mexico, what progress has been madebeyond meetings, reports, and resolutions? How willthese ideas translate into reality and, at a practical level,how can ministers and other senior policymakers bebetter served by research?
EVIPNet (Evidence-informed Policy Network) hopesto provide the answer to these questions. The initiative,
launched by WHO in June, 2005, is an innovativeattempt to strengthen the links between research andpolicy in low-income and middle-income countries.Focusing on a bottom-up approach, countries wereinvited to form national teams and submit letters ofintent. A workshop was convened where country teamspresented their proposals and worked together toimprove them, with assistance from colleagues who hadexperience of similar initiatives. A final version of theseproposals was submitted and is currently undergoingexternal review for possible funding. Seven proposalswere received for the initial planning phase from Laos,Malaysia, Philippines, Vietnam, and China (Sichuan andShandong provinces, Beijing municipality) to befollowed, hopefully, by a longer-term implementationphase over 5 years with more substantial funding.
What is unique about EVIPNet? Country teams wereformed with the close involvement of ministries ofhealth, and had to consist of both researchers andpolicymakers. Although it was explained from theoutset that the process is a competitive one, weobserved strong camaraderie among participants and agenuine desire to help and learn from each other.EVIPNet also builds on similar, successful recentexperiences in the developing world—eg, in Africa5 andLatin America.6 The interaction between participants hasalready led to the establishment of a regional network,EVIPNet-Asia, and an ongoing electronic discussionplatform.7 We hope to extend the initiative to othercountries in the region and to other parts of the world.Following the lead set by the Ministries of Health forKenya, Tanzania, and Uganda for their Regional EastAfrican Community networking initiative (REACH-Policy), planning is already underway for the EVIPNet-Africa initiative to be launched in seven further countriesin Africa in early 2006.
Will it work? Policy formulation is a multidimensionaland complex process, and there is inadequate
EVIPNet: translating the spirit of Mexico
1758 www.thelancet.com Vol 366 November 19, 2005
WH
O
7 Grantham-McGregor SM, Powell CA, Walker SP, Himes JH. Nutritionalsupplementation, psychosocial stimulation, and mental development ofstunted children: the Jamaican study. Lancet 1991; 338: 1–5.
8 Walker SP, Grantham-McGregor SM, Powell CA, Chang SM. Effects ofgrowth restriction in early childhood on growth, IQ, and cognition at age11 to 12 years and the benefits of nutritional supplementation andpsychosocial stimulation. J Pediatr 2000; 137: 36–41.
9 Walker SP, Grantham-McGregor SM, Himes JH, Powell CA, Chang SM. Early
childhood supplementation does not benefit the long-term growth ofstunted children in Jamaica. J Nutr 1996; 126: 3017–24.
10 Pollitt E, Gorman KS, Engle PL, Martorell R, Rivera J. Early supplementaryfeeding and cognition: effects over two decades. Monogr Soc Res Child Dev1993; 58: 1–99.
11 Pollitt E, Watkins WE, Husaini MA. Three-month nutritionalsupplementation in Indonesian infants and toddlers benefits memoryfunction 8 y later. Am J Clin Nutr 1997; 66: 1357–63.

Comment
www.thelancet.com Vol 366 November 19, 2005 1759
knowledge about the crucial factors in strengtheninglinks between research and policy. Although much hasbeen written,8–10 information about what actually worksis limited, esp-ecially in the often challenging setting ofdeveloping countries. Questions abound, such as: whatconstitutes the best evidence and how relevant, feasible,and affordable is this evidence in a developing worldsetting,11 and what is the role, if any, of knowledgebrokers? Herein lies another unique feature andopportunity presented by EVIPNet. Faced with thisknowledge gap, together with the belief that theparticipating countries have valuable experiences oftheir own to contribute, we decided not to present thecountries with a fixed template, model, or framework ofbest practices developed by so-called experts in thedeveloped world. From the proposals we received it wasclear that each country faces a unique set of challengesand constraints, and that this diversity can actually beseized on as an unprecedented opportunity for furtherresearch based on a learning-by-doing approach. Thisresearch component will be built into the project fromthe start. Ultimately, EVIPNet will not only result inbetter policies and stronger health systems, but will alsohopefully help to push the boundaries of knowledge inthis under-researched area.3
The learning process has already begun as, on the basisof their experiences, participants themselves identifiedsome practical, commonly-shared “drivers” that theyfelt would enhance their chances of success. Strategicalliances between researchers and policymakers weredeemed crucial, and researchers should be involved inscale-up activities. Continuous dialogue was essential,as was the need to simplify and package research on thebasis of convincing and accurate evidence. Researchshould be embedded in implementation and a realisticlonger time-frame should be adopted for strengtheninglinks between researchers and policymakers. Access toevidence and information, and national capacity forsynthesising and presenting such evidence, weredeemed to be critically important, as was a one-stopshopping and rapid-response function to address keypolicy challenges related to hot topics for government.
The participants’ perceptions of important impedi-ments to success were equally valuable. These includedabsence of quality assurance in research, unavailabilityof timely data for policymaking, poor communication,poor understanding of the value of research, distortion
of evidence, and a shortage of post-policy research.Weak capacity in health-systems research and the abs-ence of an appropriate research agenda were also citedas obstacles.
By providing a bridge between research and policy,EVIPNet hopes to turn research into effective action andproblem solving to improve people’s health—arguablythe true spirit of the Mexico summit. When the nextministerial summit convenes in Africa in 2008, a reviewof the effects of this living laboratory will be the true testof its value.
Maimunah Hamid, Thiel Bustamante-Manaog, Truong Viet Dung, Kongsap Akkhavong, Hongpeng Fu,Yuanxin Ma, Xinqui Zhong, Reijo Salmela, Ulysses Panisset, *Tikki PangInstitute for Health Systems Research, Ministry of Health, Kuala Lumpur, Malaysia (MH); Health Policy Division, Departmentof Health, Manila, Philippines (TBM); Department of Science andTraining, Ministry of Health, Hanoi, Vietnam (TVD); NationalInstitute of Public Health, Ministry of Health, Vientiane, Laos (KA);Beijing Centres for Disease Prevention and Control, Beijing,China (HF); Shandong Provincial Health Bureau, Jinan, China (YM);Sichuan Provincial Health Bureau, Chengdu, China (XZ); WHOWestern Pacific Regional Office, Manila, Philippines (RS); andResearch Policy and Cooperation, World Health Organization, CH-1211 Geneva, Switzerland (UP, TP)[email protected]
We thank Sonya Corkum, Irving Gold, John Lavis, Soe Nyunt-U,Nelson Sewankanbo, Andy Oxman, Parminder Raina, Don de Savigny, Abu Bakar Suleiman, and Jimmy Volmink for their help in the development ofthis initiative, and Jonathan Lomas for the initial idea for the project. We alsothank the participants and team members from the countries: Dam Viet Cuong,Noormah Darus, Clemencia Rosa Gonzales, Jianlin Hou, Lailanor Hj Ibrahim,Baofa Jiang, Rusilawati Jaudin, Yuan Liu, Luu Ngoc Huat, Kalsom Maskon,Noorimi Morad, Nik Shamsidah, Nik Ibrahim, Merlita Opena,Kotsaythoune Phimmasone, Bounfeng Phoummalaysith, Lingzhong Xu,Haining Xue, and Xiaohua Zheng, from whom we learnt so much, and theSecretariat Staff at the Malaysian Institute for Health Systems Research for strongsupport. We acknowledge the sponsors of the initiative, including theNetherlands Research Organization, the Alliance for Health Policy and SystemsResearch, the Canadian Health Services Research Foundation, the CanadianInstitutes of Health Research, and the WHO Western Pacific Regional Office. Wedeclare that we have no conflict of interest.
1 The Lancet. Mexico, 2004: global health needs a new research agenda.Lancet 2004; 364: 1555–56.
2 The Lancet. The Mexico Statement: strengthening health systems.Lancet 2004; 364: 1911–12.
3 WHO. World report on knowledge for better health. Geneva: World Health Organization, 2004. http://www.who.int/rpc/wr2004 (accessedNov 1, 2005)
4 WHO. Ministerial summit on health research. Document WHA58/34. May 25, 2005. http://www.who.int/gb/ebwha/pdf_files/WHA58/WHA58_34-en.pdf (accessed Sept 19, 2005).
5 de Savigny D, Kasale H, Mouya C, Reid G. Fixing health systems. IDRCCanada and Ministry of Health Tanzania, 2004. http://www.idrc.ca/tehip(accessed Nov 1, 2005).
6 Frenk J, Sepulveda J, Gomez-Dantes O, Knaul F. Evidence-based healthpolicy: three generations of reform in Mexico. Lancet 2003; 362: 1667–71.
Comment
7 IBP Electronic Communication System. WPROep community.http://ibp.wa-research.ch/communities.aspx (accessed Nov 1, 2005).
8 Lavis JN, Becerra Posada F, Haines A, Osei E. Use of research to informpublic policymaking. Lancet 2004; 364: 1615–21.
9 Sheldon TA. Making evidence synthesis more useful for management andpolicy-making. J Health Serv Res Policy 2005; 10 (suppl 1): 1–5.
10 Haines A, Kuruvilla S, Borchert M. Bridging the implementation gap between knowledge and action for health. Bull World Health Organ 2004;82: 724–31.
11 Pablos-Mendez A, Chunharas, S, Lansang MA, Shademani R, Tugwell P.Knowledge translation in global health. Bull World Health Organ 2005;84: 723.
The 13th Cochrane Colloquium was held in Melbourneon Oct 22–26.1 The opening plenary session challengeddelegates, by asking “is evidence ever enough?” Anarticulate debate followed, informed by some of thegreatest advocates of evidence. Yet the conclusion wasthat compiling evidence alone is inadequate, and to fullyrealise the benefit of research, findings must be syn-thesised in a targeted manner and made readily availableat the point of need.
Rather than a downhearted response to this news,reviewers in the 700-strong gathering, or corroboree,appeared full of enthusiasm and imagination aboutways in which the Collaboration could shake off itsdowdy image and provide more helpful informationto consumers. One reason for optimism was the rapidresponse with text-light, tsunami-tailored evidenceearlier in the year, which showed both the value of this
unique database and the possibility of rewriting turgidreviews in a form that can be more easily understoodand acted on.2 With this impetus, there is now arefreshing interest in expanding the group’s work toinclude different research designs, complex inter-ventions, more focused outcomes, and wider partici-pation—particularly in the developing world. Cooperativeventures with other health and policy organisations,such as the Australian National Institute of ClinicalStudies, to achieve these aims seem likely.
The Cochrane Library has been justifiably criticised forits lack of accessibility, flexibility, and relevance. To beeffective, a change in emphasis from the product to itsusers will need to be more thorough than just re-branding, but must not compromise the rigour andquality for which their reviews are renowned. Much is atstake. If Cochrane fails to become an integral part ofdaily decision-making, health-care systems, providers,and consumers will continue to be deprived of safer,cheaper, and more effective interventions. However, if“new Cochrane” succeeds, not only will clinical carebenefit from the application of established evidence, butthe future research agenda will be challenged to provideevidence that focuses on the real needs of patients andthose who provide for them.
William SummerskillThe Lancet, London NW1 7BY, UK 1 Cochrane Collaboration. XIII Cochrane Colloquium, 2005.
http://www.colloquium.info (accessed Nov 11, 2005).2 Cochrane Collaboration. Evidence Aid: summaries relevant to natural
disasters and healthcare emergencies, 2005. http://www.cochrane.org/docs/tsunamiresponse/index.htm (accessed Nov 11, 2005).
Cochrane Collaboration and the evolution of evidence
1760 www.thelancet.com Vol 366 November 19, 2005
Robe
rt H
ardi
ng
Melbourne, Australia, host of the 2005 Cochrane corroboree
Rights were not granted to include this image in electronicmedia. Please refer to the printed journal

Search Search all BMJ Products
Advanced search
Search Search BMJ.com
Published 25 November 2008, doi:10.1136/bmj.a2733
Cite this as: BMJ 2008;337:a2733
Editorials
Global research for health
Should tackle health needs and inform policy
Last week delegations from 59 governments, international agencies, and researchers met in Bamako, Mali, to discuss the state of global
health research. It was an opportunity to review progress since their last meeting, four years earlier, in Mexico City, and to set an agenda for
the future.1 The meeting in Mexico is widely seen as a turning point, where the importance of research tackling the greatest health needs was
emphasised, and where a strategy for meeting these needs was proposed.
Arguably, in a world with scarce resources efforts should be focused on where they can do most good. To make this happen, those attending
the conference in Mexico advocated greater investment in research on health systems and policy, the development of national health
research policies, and the incorporation of evidence into health policy.
The consensus is that some progress has been made since Mexico. Funding for health systems and policy research has increased, and
some politicians now accept that evidence based policies are desirable.2 Yet we still have much to do. The births, lives, and deaths of many
of the world’s population remain unrecorded.3 Large scale programmes and healthcare reforms are still implemented without evaluation.4
The reasons why they succeed or fail are often unknown. And large parts of the world are effectively untouched by health research.
One purpose of a meeting like this is to facilitate dialogue among groups of people who might not otherwise meet. In this it succeeded.
Governmental delegations heard about the opportunities offered by health research and the obstacles to achieving them, in some cases
seemingly for the first time. Although good intentions often collide with financial and political realities at home, many remarks made by
ministers indicated that they had taken the messages on board. But what did the meeting achieve?
The most tangible outcome was a "call to action."5 In it, governments committed themselves to developing health research strategies and to
funding them adequately, allocating at least 2% of the budgets of their ministries of health. They also committed to creating research
infrastructure, including ethical review procedures, clinical trials registries, and open access to data, while promoting knowledge translation
as a means of developing evidence based policies. Finally, they accepted the need to build a critical mass of young researchers. Others must
also play a role. International development agencies are called on to devote at least 5% of their spending on health to development of
research capacity, while they and research funders should pursue innovative financing mechanisms and align their support with national
plans.
So what next? The call to action sets out an ambitious agenda, but so did the declaration at the Mexico City summit. An immediate need is to
establish a monitoring mechanism that can track progress against stated intentions, so that next time it will be possible to assess what has
been achieved and by whom. It is not obvious who should undertake this role, and that fact argues for a reassessment of the often confusing
roles of the different bodies that oversee global health research. Yet whoever does it, they should report regularly and publicly, so that
governments can be held to account by their populations.
The widespread view was that research funding must change. Short term project based funding should coexist with long term investment in
research capacity. Research portfolios should be balanced; they should include basic and applied research, as well as generalisable and
context specific studies. These last studies are often the ones that make the greatest difference. The importance of knowledge transfer was
stressed, and successes such as the Evidence-informed Policy Network were given as examples.6
Calls were also made for partnerships, in which researchers would work with governments, civil society, and more controversially, the drug
industry. The last of these stimulated the greatest debate. A few speakers highlighted past transgressions by the industry, seemingly implying
that the growth of clinical trials in developing countries was in itself a bad thing. But as Mark Walport, director of the Wellcome Trust, noted, it
is industry that makes the drugs that save lives, not academics. Another area of debate was the role of national research strategies. These
are clearly important but should not exclude innovative investigator led research.
Contact us - Privacy policy - Web site terms & conditions - Site map
HighWire Press - Feedback - Help - © 2008 BMJ Publishing Group Ltd.
The real challenge will be within countries. One of the most striking images was a map of the world, which showed research capacity.7 The
heaviest shading was, as expected, in the developed countries of Europe, North America, and East Asia. Large parts of the map were
completely empty, however, in west and central Africa, the Middle East, and the former Soviet Union.
The unresolved challenge is what we should do where there is virtually nothing to build on. Increasing global funding alone will not help.
External donors can help, if they are willing to invest strategically and recognise that the results of their funding may take a decade or more to
become apparent. However, governments must also act, by tackling the corruption and failures of governance that prevent not just the
development of health research but also the development of the basic institutions needed for anything to work.
Cite this as: BMJ 2008;337:a2733
Martin McKee, professor of European public health
1 London School of Hygiene and Tropical Medicine, London WC1E 7HT
Competing interests: MM attended the Bamako conference on behalf of the European Region of WHO. He is a member of WHO’s advisory
committee on health research and has recently completed a term as a member of the Wellcome Trust’s population and public health panel.
Provenance and peer review: Commissioned; not externally peer reviewed.
References
1. Ministerial Summit on Health Research. The Mexico statement on health research. Mexico City. 2004.
www.who.int/rpc/summit/agenda/en/mexico_statement_on_health_research.pdf. 2. Bennett S, Adam T, Zarowsky C, Tangcharoensathien V, Ranson K, Evans T, et al; Alliance STAC. From
Mexico to Mali: progress in health policy and systems research. Lancet 2008;372:1571-8.[Medline] 3. Mathers CD, Fat DM, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment
of the global status of cause of death data. Bull World Health Organ 2005;83:171-7.[ISI][Medline]
4. The state of health research worldwide. Lancet 2008;372:1519.[Medline] 5. The Global Ministerial Forum on Research for Health. The Bamako call to action on research for health.
Strengthening research for health, development, and equity. 2008.
www.bamako2008.org/dmdocuments/CTA_3.pdf.
6. WHO. Evidence-informed Policy Network. 2008. www.who.int/rpc/evipnet/en/. 7. Global Forum for Health Research. Global forum update on research for health. Vol 5. Fostering innovation for
global health. Geneva: GFHR, 2008.
CiteULike Complore Connotea Del.icio.us Digg Reddit Technorati What's this?
Relevant Article
Developing countries should have a greater say in local research agendas
Robert Walgate
BMJ 2008 337: a2713. [Extract] [Full Text]
Rapid Responses:
Read all Rapid Responses
Global research for Health
Harald M Lipman
bmj.com, 1 Dec 2008 [Full text]
146 Commonwealth Health Ministers’ Update 2009
Country Survey on Health and Climate Change
strengthen its capacity for evidence-based decision-making. The Ministry is also in the process of strengthening its National
Health Research and its Health Information Management System inorder to improve its health programmes and service delivery systems.
In addition, the Ministry of Health is in the process of planning andimplementing an Evidence Based Policy Network (EVIPNet). Theestablishment of such a network in Trinidad and Tobago will facilitatethe availability of timely and credible evidence for use in decision-making and policy development.
11. Have national resources been allocated to address climatechange and health in your country? If so, approximately howmuch has been allocated and for what issues?The national resources that have been allocated to address climatechange and health are incorporated in the overall health budget. Thismakes it difficult to quantify the funding that was specifically allocatedto the issue of climate change.
12. Is the Ministry of Health working together with otherministries (such as Ministries of Agriculture, Environment,Fisheries or Finance) to address health and climate change issues?The Ministry of Health currently works with the Ministry of LocalGovernment to address the issue of dengue and control of the vectoraedes aegypti mosquito.
Under the National Disaster Management System a National TaskForce was established. This is made up of 15 Task groups, with thespecific responsibility of planning for, mitigating against and respondingto disasters. The Ministry of Health chairs the Health Task Group.
The Ministry of Health also works with the Ministry of Agriculture inthe surveillance of yellow fever.
The Ministry of Health works indirectly with the Ministry of Works andTransport in the areas of clean up campaign and the prevention offlooding.
13. Has your country been involved in work to manage climatechange and health at the international level?Yes. Trinidad and Tobago is a signatory to the United Nations FrameworkConvention on Climate Change (UNFCCC). A working group has beenestablished that has oversight of the implementation of obligationsunder the United Nations Framework Convention on Climate Change(UNFCC).
14. How would you describe the capacity of your country toparticipate at the global level on climate change and health?There is moderate capacity. However, the Ministry of Health iscontinuing to work towards increasing its capacity.
! Homes were inspected and treated on a regular basis in areas whereaedes aegypti mosquitoes and larvae were present and where therewere increased activity such as dengue.
! Integrated biological and chemical control measures for themanagement of all vector species of mosquitoes (particularly, AedesAegypti) were implemented in certain localities for example the MtHope Medical Sciences Complex.
! Within the framework of the Emergency Services and DisasterPreparedness Coordinating Unit there is the establishment of anEmergency Operations Center (EOC) in each Regional HealthAuthority. The common functions of all EOCs are to collect, gatherand analyse data; make decisions that protect life and property,maintain continuity of the organisation, within the scope ofapplicable laws; and disseminate those decisions to all concernedagencies and individuals.
7. What are the current policy gaps in addressing climate changeand health?There is the need for an overarching policy to deal with climate changeand health.
8. How well equipped is your health system to cope with theimpacts of climate change?! We have established mechanisms for the early warning systems for
the diseases which are likely to proliferate due to the climaticchange such as malaria, cholera and Rift Valley fever.
! Rapid response teams have been trained and equipped ready for anysign of the outbreak of such diseases.
9. Have you made any changes to your health system in responseto increased risks resulting from climate change and if so, whatchanges have you made?The Ministry of Health has made changes to the health system inresponse to increased risks resulting from climate change in thefollowing areas:! The establishment of a focal point, the International Cooperation
Desk, to monitor the implementation of plans and programmes thatare required to fulfil Trinidad and Tobago’s obligations underInternational Agreements and Conventions, for example, the UnitedNations Framework Convention on Climate Change (UNFCCC).
! The establishment of an Emergency Services and DisasterPreparedness Coordinating Unit to deal with natural disasters.
! The decentralisation of services to the Regional Health Authorities. ! Improvement in the primary healthcare network.! Implementation of the safe hospital initiative to mitigate against the
loss of healthcare services in the event of a natural disaster.
Further changes will be made as the Ministry of Health continues theimplementation of its transformation plan.
10. What are the main constraints to addressing the healthimpacts of climate change in your country and how will these beaddressed?The main constraints that can be identified to addressing the healthimpacts of climate change are a lack of scientific evidence to guidepolicy, and also a lack of resources, both human and materials.
To address these areas the Ministry of Health, as stated before, iscurrently engaged in a transformation process which is geared to
145-146 Trinidad:2009 2/5/09 20:01 Page 146
Scaling up research and learning for health systems: now is the time 13
research. Their involvement in research will increase the likelihood that results are used to inform their decisions. Moreover, a greater sense of the utility of health systems research will help to foster greater de-mand for such research, which will lead to a virtuous cycle. For example the Malawi Emergency Human Resources Programme, which was based on research driven by the Government of Malawi, has resulted in significant improvements in training and retention of health workers within a space of five years (57 ).
Translation of research into policy and practice can be accelerated by support for appropriate networks and communities of practice. One example of these is the WHO Evidence-Informed Policy Network (EVIP-Net), which promotes the systematic use of health research evidence in policy-making (Box 5). Country teams, linked through regional networks in Africa, Asia and the Americas facilitate policy development and implementation through summarizing evidence, hosting policy dialogues and intensifying exchange between researcher and policy communities (58 ).
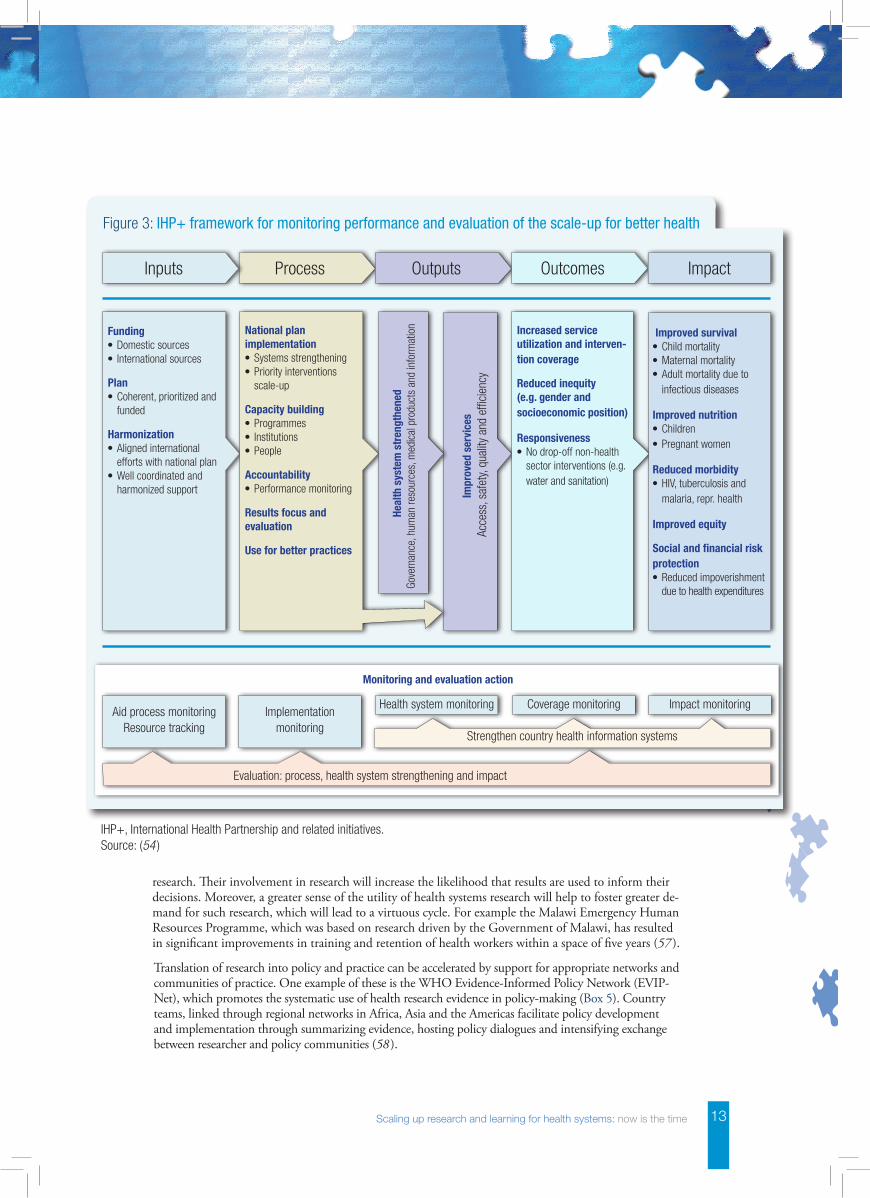
Figure 3: IHP+ framework for monitoring performance and evaluation of the scale-up for better health
Funding•Domestic sources• International sources
Plan•Coherent, prioritized and
funded
Harmonization•Aligned international
efforts with national plan•Well coordinated and
harmonized support
National plan implementation•Systems strengthening•Priority interventions
scale-up
Capacity building•Programmes• Institutions•People
Accountability•Performance monitoring
Results focus and evaluation
Use for better practices
Increased service utilization and interven-tion coverage
Reduced inequity (e.g. gender and socioeconomic position)
Responsiveness•No drop-off non-health
sector interventions (e.g. water and sanitation)
Heal
th s
yste
m s
tren
gthe
ned
Gove
rnan
ce, h
uman
reso
urce
s, m
edic
al p
rodu
cts
and
info
rmat
ion
Impr
oved
ser
vice
s A
cces
s, s
afet
y, qu
ality
and
effi
cien
cy
Improved survival•Child mortality•Maternal mortality•Adult mortality due to
infectious diseases
Improved nutrition•Children•Pregnant women
Reduced morbidity•HIV, tuberculosis and
malaria, repr. health
Improved equity
Social and financial risk protection•Reduced impoverishment
due to health expenditures
ProcessInputs Outputs Outcomes Impact
Aid process monitoringResource tracking
Implementationmonitoring
Health system monitoring Coverage monitoring Impact monitoring
Evaluation: process, health system strengthening and impact
Strengthen country health information systems
Monitoring and evaluation action
IHP+, International Health Partnership and related initiatives. Source: (54 )

14 Scaling up research and learning for health systems: now is the time
Policy-making is a complex process and research evidence is just one of the many factors that influence policy. For policy-makers, who may not be schooled in research, it can be chal-lenging to assess the quality of research. Furthermore, research results are often nuanced without clear evidence that a particular policy or strategy is effec-tive under all conditions. Accordingly, capacity development is necessary to enhance the skills of policy-maker to apply research evidence in the policy process, and this should be pursued as part of a broader capacity develop-ment strategy. Also related are dedi-cated knowledge brokering functions – supporting evidence-informed policy through encouraging connections that ease knowledge transfer – which are beginning to emerge in low- and middle-income countries, The Zambia Forum for Health Research being one example (59 ).
The Task Force recommends that:
2.1 mechanisms be developed at country level to ensure that key stakeholders (particularly policy-makers but also civil society) are engaged from identification of research priorities, through conception of studies, to interpretation of findings;
2.2 WHO further develop its knowledge brokering role at country level and also support the emerging knowledge brokering platforms;
2.3 mechanisms be developed that enable the research community and other stakeholders to access relevant research evidence in a succinct and easily understood format, when needed. To accelerate growth of the global knowledge-base on health systems, it is recommended that country, regional and global repositor-ies for evidence on health systems be established, similar to existing repositories for clinical evidence such as the Cochrane Collaborative.
3. Strengthen country capacity for health systems research backed up by effective regional and global support
Country capacitiesThere is strong global consensus that strengthening capacity for health systems research – particularly at country level – is the key to progress in the field. Few developing countries have the capacity to perform the analyses and syntheses needed to assist leaders and managers to address public health problems. Instead, they often depend on short-term consultants and advisers for analytical work on health systems. The growing trend in overseas development aid towards technical assistance, which now comprises more than 40% of the value of such aid, is indicative of this systematic bias in support to research capacity (14 ). This represents something of a substitution of efforts towards developing technical and research capacity on the ground.
There have been some small-scale attempts, such as the now defunct International Health Policy Program (60 ), to develop capacity in the health systems research field; however the scale of the investment has fallen
Box 5: WHO evidence-informed policy network
EVIPNet is an innovative initiative to promote the systematic use of health research evidence in policy-making. Focusing on low- and middle-income countries, EVIPNet promotes partnerships at the country level between policy-makers, researchers and civil society in order to facilitate both policy development and policy implementation through the use of the best scientific evidence available.
Low- and middle-income countries have scarce resources to address their health system challenges and need high-quality evidence to use those resources efficiently. Scien-tific evidence is a fundamental building block to improve the public health situation. If health sector managers and policy-makers ignore evidence on the root causes of prob-lems or what works best to address these problems, they risk wasting precious resources on inadequately designed programmes and policies. The direct consequence of ignor-ing this evidence is poor health for the population.
Source: (28 )
(EVIPNet)

October 2009, Volume 8, No. 7, Focus on Health
13
into policy decision-making is important. Knowledge generated through research and that is sys-tematically and transparently syn-thesized through systematic reviews provides a state-of-the-art view of a health problem and of policy op-tions to address it. Social actors gain the most comprehensive and best available evidence when it is drawn from both qualitative and quantita-tive approaches. Thus, questions of comparative effectiveness (whether one intervention is more effective than another), acceptability (wheth-er interventions fit in social and cultural norms and values), and the satisfaction of healthcare providers and patients are more likely to be addressed. Circulating in advance scientific evidence in a way that is “translated” to meet the needs of each social actor involved improves and facilitates the policy-making process.
What could governments in the Americas do to increase local re-search production and synthesis in ways that better inform policy-making? First, governments in the Americas must acknowledge the importance of health research to people’s health and to national de-velopment. According to various international recommendations, such as those from the Council on Health Research for Development (COHRED), progress in evidence-to-policy in the Americas may be enhanced if national health research policies are first developed and im-plemented.
The Bolivian government, for instance, lags behind this essential requisite, which is hindering health research priority setting, infrastruc-ture and human capacity building, and focused funding allocation pro-
cesses. Similarly, the governments of Peru and Ecuador could increase current health research expenditure from 0.10 per cent of their countries’ gross domestic product (GDP) to at least 0.54 per cent of the GDP, the Latin American average. Further-more, according to a Lancet article published by Anastasia Moloney in September 2009, the government of Colombia could increase the num-ber of postgraduate degrees and scholarships on offer, which would increase the current 1.8 per one mil-lion Colombian graduates with doc-torates annually to at least the Bra-zilian 50 per one million.
International research and de-velopment agencies could also help countries in the Latin American and Caribbean region to ensure they use five per cent of international aid for the health sector on research, as rec-ommended by the CORED in 1990. The largest Latin American econo-mies such as Brazil, Mexico, Chile, and Argentina could also enhance health research partnerships with neighboring countries, and with Canada and the United States.
Second, social actors should sup-port Knowledge Translation ini-tiatives aiming to improve policy and decision-making processes. Such initiatives are comprised of researchers “pushing” evidence to government, civil society and pri-vate groups; government, civil so-ciety and private groups “pulling” research evidence; and “exchange” among these social actors.
Bolivia, Mexico and Canada are examples of societies striving to fos-ter Knowledge Translation initiatives to varying extents. In 2007, Bolivia and Mexico joined the Evidence-Informed Policy Networks (EVIP-Net, www.evipnet.org), sponsored
by the World Health Organization. Canada has provided Knowledge Translation expertise and research and development funding to EVIP-Net and similar initiatives. The Ca-nadian Coalition for Global Health Research, with the support of the Pan American Health Organization, also organized in 2007 a workshop in Bolivia aiming at perfecting the proposal for research in health for Bolivia. Substantive government stewardship and investment remains essential to strengthen national re-search capacity in Bolivia.
Mexico’s Knowledge Translation experiences entail relative advance-ment and complexity. This came about partially due to the Mexi-can statement in the 2004 Ministe-rial Summit on Health Research, which called on establishing na-tional Knowledge Translation pro-grammes. Moreover, Mexico’s de-centralization of healthcare services increased the autonomy of munici-palities and states. Thus, building on close ties between the Mexican Ministry of Health and research in-stitutes, including the National In-stitute of Public Health, networks composed of researchers, govern-ment officials, and activists in civil society groups started to be trained through initiatives such as the Re-search Consortium for the Develop-ment of State Health Systems. This initiative included Mesoamerican countries and counted on Canadian collaboration. Despite Mexico’s at-tempts to implement such initia-tives, it faces challenges common to other Latin American countries: so-cio-economic inequalities, deficient Knowledge Translation-designated research funding, difficult access to high-quality scientific databases, and lack of expertise.
Getting information and evidence into policy-making and practice: strategies and mechanisms
163
disseminators, but also proactive actors in policy-mak-
ing. For example, regular (biennial) regional meetings
provide a forum for interactive discussion, sharing and
strategic planning.
More recently, with increasing global attention and
resource mobilization to address the health workforce
crisis in Africa, the Africa Health Workforce Observatory
(34) has evolved as part of the action agenda. With its
secretariat housed by the World Health Organization
(WHO), its mission is to “support actions that address
HRH challenges by promoting, developing and sustain-
ing a solid knowledge base for HRH information at all
levels: subnational, national, intercountry and regional”
(35) (Box 12.2, page 166).
Similarly, with support from WHO, the Eastern
Mediterranean Region Observatory on Human
Resources for Health grew out of an existing regional
observatory on health systems with the purpose “to
assist Member States in using a proactive approach
and sharing the best and most innovative options to
tackle HRH-related challenges” (36). Its outputs in the
public domain include updated profiles on the health
workforce situation within and across countries, analy-
ses of correlations between significant health workforce
Box 12.1 Evidence-Informed Policy Network: EVIPNet
In response to a call “to establish mechanisms to transfer knowledge in support of evidence-based public
health and health-care delivery systems, and evidence-based health-related policies”, in 2005 the World
Health Organization launched the collaborative Evidence-Informed Policy Network (EVIPNet) (26).
EVIPNet addresses the integration of two fundamental enabling factors in the process of evidence-
informed policy-making: best practices to promote interaction among stakeholders that generate and use
evidence; and capacity to implement research in a local context (27). Focusing on low- and middle-income
countries, EVIPNet promotes partnerships at the country level between policy-makers, researchers and
civil society in order to facilitate both policy development and policy implementation through the use of the
best scientific evidence available.
EVIPNet comprises a series of linked (but distinct) networks that bring together national teams, which are
coordinated at regional and global levels. Africa, Asia and the Americas each host regional networks,
which together work in some 25 countries. At the regional level, EVIPNet is supported by WHO regional
offices and by small secretariats responsible for promoting regional coordination. A global steering group
facilitates exchange between regions and supports international-level activities. The work is guided by a
group of international experts in the evidence-to-policy field, which provides strategic guidance, organizes
technical review of EVIPNet proposals, develops innovative methodologies and provides direct technical
support to country teams where necessary. A project priority is to identify best practices in developing
capacity of both policy-makers and researchers in working with scientific evidence-to-policy links, while
engaging citizens and advocacy groups to sustain demand for evidence-informed health policy.
Since its inception, EVIPNet has worked collaboratively with the Regional East African Community
Health Policy Initiative, an institutional mechanism whose mission is to access, synthesize, package
and communicate evidence required for health policy and practice and for influencing policy-relevant
research agendas for improved health equity (28). Similar initiatives are emerging in other countries,
focusing on supporting governments to use research evidence for health policy decisions – although the
specific scope of activities, nature of collaborative efforts and research evaluation methods are unique
across contexts. For example, country teams may organize workshops to build technical capacity; several
promote the inclusion of journalists as observers and advocates. Thus EVIPNet has contributed to creating
a supportive political environment for delivery of evidence-informed policies.
Recently, country teams have began to produce policy briefs based on systematic reviews of research,
offering policy options that include governance, delivery and financial arrangements adapted to specific
country or district contexts and the reality of existing resources. For instance, in February 2008, EVIPNet
Africa country teams produced policy briefs to address current policy challenges related to malaria
treatment services in their respective countries.
Getting information and evidence into policy-making and practice: strategies and mechanisms
169
12.4 Opportunities and directionsThe development and sustainability of long-term, com-
prehensive HRH policies and plans is a common
challenge for all countries to ensure the health work-
force is prepared to meet current and future health
system objectives and population health needs with
equitable and adequate coverage. In many coun-
tries, this entails strengthening institutional capacity for
defining appropriate policies and revising them period-
ically, which itself is dependent upon close cooperation
among a wide range of stakeholders in the policy dia-
logue from the inception stages. This includes not only
the ministry of health but also other sectors: finance
department, public service commission, educational
bodies, health professional regulatory bodies and
associations, programme managers (in the public,
parapublic and private sectors), development partners
and health services users’ groups. In order to achieve
balance across the different perspectives, and being
mindful that each country has specific challenges and
contexts for workforce development, a common frame-
work needs to be identified where collaborative efforts
can be focused. To this end, this chapter has exam-
ined various strategies and mechanisms to ground
HRH policies and strategies in scientific information
and evidence.
The sustainable provision of timely, reliable and relevant
data, information and evidence to improve HRH pol-
icies requires mechanisms to facilitate dissemination,
access and use in policy-making processes. Different
knowledge transfer platforms (such as EVIPNet) and
cooperative mechanisms (health workforce observato-
ries) can offer the opportunity for global and national
health institutions to take advantage of the latest inno-
vative and sound tools to support decision-making.
Their value lies in the forums they extend to facilitate
sharing of information and experiences and promotion
of collaborations at the national, regional and interna-
tional levels.
In particular, health workforce observatories can be a
good mechanism to facilitate the steering and nego-
tiating processes of cooperative partnerships. They
can contribute to the strengthening of working rela-
tions and development of joint agendas among
stakeholders. Their informational products help bring
new evidence on the health workforce situation to a
broader audience, often in a standardized way to fos-
ter better understanding and dialogue for comparisons
and benchmarking. Perhaps most crucially, they can
effectively raise the priority of HRH issues in the health
development agenda; for example, through its working
groups and mobilization efforts, the Observatories of
Human Resources for Health of the Americas network
has been credited as central in shaping the agenda for
long-term, intentional and coordinated efforts for HRH
development at the international, national, regional and
subregional levels (43).
A number of critical success factors in moving forward
with health workforce observatories and enhancing
their benefits have been identified (44). They include:
championing HRH issues in the country (including
high-level political commitment and leadership);
engaging all key stakeholders in joint planning and
nurturing joint work;
ensuring effective coordination;
building awareness and capacity in HRH issues;
developing approaches from different experiences;
harmonizing standards, definitions and indicators
for HRH profiling and analysis;
supporting networks of HRH researchers;
institutionalizing coordination mechanisms (man-
date and legitimacy);
creating a communication mechanism for tracing
the available information for public use (for exam-
ple a web site);
mobilizing resources (technical and financial).
In summary, health workforce observatories and other
knowledge transfer platforms present dynamic and
evolving networks, which can only stand to bene-
fit from increasing numbers of participating countries
and institutions. Securing the initial commitment is
often a challenge in establishing such mechanisms,
but maintaining interest and commitment (often while
coping with political changes and shifting donor prior-
ities) is another critical concern. This requires regular
dissemination of products that have proven to be use-
ful, active sharing and exchange of information and
knowledge, and continuous advocacy activities. The
last-mentioned should including a strong, actionable
communications strategy – aimed at policy-makers,
managers, researchers and other relevant stakeholders
inclusively – to advocate recognition of health workers
as the foundation of health systems and implemen-
tation of effective strategies to directly address HRH
bottlenecks, barriers and funding gaps at all levels.





























