Embed Size (px)
Citation preview

Ewen C. D. Todd Advertising, Public Relations
and RetailingMichigan State University
Train the Trainer Workshop at the International Food Safety Conference
Dubai, February 2009
What We Can Learn from the Role of the
Food Worker in Outbreaks

What Have We Learned What Have We Learned from Investigation of from Investigation of
Outbreaks Where Food Outbreaks Where Food Workers Were Implicated?Workers Were Implicated?

Impact of the Infected Food Impact of the Infected Food WorkerWorker
• CDC estimates 76 million cases of foodborne illness each year in the United States
• Estimated that between 18-20% of foodborne illness associated with an infected food worker in the US, and 7% of salmonellosis in the UK
• Thus, there may be up to 13-15 million cases in the US associated with an infected food worker (18-20% of 76 million)

Definition of Food WorkerDefinition of Food WorkerThe term food worker is used in this context to describe individuals, who harvest, process, prepare and serve food
It is broader in context than food handler although the two terms are used interchangeably in the literature and investigative reports

Purpose of Study of Infected Food Purpose of Study of Infected Food Workers Implicated in OutbreaksWorkers Implicated in Outbreaks
• Project of the Committee on Control of Foodborne Illness (CCFI) of the International Association for Food Protection (IAFP)
• Goal: to develop an understanding of the dynamics of transmission of infectious agents to and from the food worker in a variety of settings
• The CCFI approached the task with the premise that all foodborne illness is fundamentally preventable and that by influencing human behavior there will be fewer opportunities for spread of infectious disease agents by workers and others

Papers Prepared on Papers Prepared on Outbreaks Where Outbreaks Where Food Workers Have Been Implicated in the Food Workers Have Been Implicated in the Spread of Foodborne Disease in the Journal Spread of Foodborne Disease in the Journal
of Food Protection (2007-2009)of Food Protection (2007-2009)• Part 1: Description of the problem, methods and agents involved• Part 2: Description of outbreaks by size, severity, and settings • Part 3: Factors contributing to outbreaks and description of outbreak
categories • Part 4: Infective doses and pathogen carriage• Part 5: Sources of contamination and pathogen excretion from
infected persons • Part 6: Transmission and survival of pathogens in the food processing
and preparation environment• Part 7: Barriers and sanitizers in reducing contamination• Part 8: Hand hygiene


Outbreaks by Geographical Outbreaks by Geographical RegionRegion
Geographical Region
Number of Outbreaks (%)
Number of Cases
(%)
USA 647 (79.3) 54,888 (68.0)
Europe 63 (7.7) 7,694 (9.5)
Canada 62 (7.6) 3,320 (4.1)
Australia/Asia 27 (3.3) 4,680 (5.8)
Latin America/Caribbean
6 (0.7) 5,408 (6.7)
Africa 4 (0.5) 2,394 (3.0)
Middle East 3 (0.4) 400 (0.5)
Multiple Countries 2 (0.2) 1,843 (2.3)
Unknown 2 (0.2) 55 (0.1)
Totals 816 (100) 80,682 (100)

Summary of Data on Summary of Data on PathogePathogens
• 816 outbreak reports with 80,682 cases• Pathogens in order of frequency:
– norovirus/probable norovirus (338)– Salmonella enterica (151)– hepatitis A virus (84)– Staphylococcus aureus (53)– Shigella spp (33)– Streptococcus pyogenes Group A (17)– Parasites Cyclospora, Giardia, and
Cryptosporidium (23)

Outbreaks by Food CategoryOutbreaks by Food Category
0 100 200 300 400 500
Other
Multi-Ingredient Foods
Beverages
Produce
Breads and Bakery
Seafood
Dairy
Eggs
Poultry
Meats
Number of Outbreaks
Co
mm
od
ity

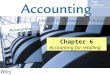
Foods Associated with Outbreaks Foods Associated with Outbreaks Where Food Workers Were Where Food Workers Were
ImplicatedImplicatedMultiple foods and multi-ingredient foods were noted most frequently– Salads, including potato, pasta and
coleslaw (92)– Sandwiches (74)– Chinese, Mexican type food, and pizza
(19)– Hors d’oeuvres and other RTE cold
snacks with sauces and glazes (8)

Outbreaks by SettingsOutbreaks by Settings
0 100 200 300 400 500
Unknown
Prison
Community Events
Commercial Travel
Armed Forces & Camps
Health Care
Schools
Home
Retail
Processing Plant & Bakeries
Catered Events
Food Service
Sett
ing
s
Number of Outbreaks* Mainly restaurants
*

Most Extreme OutbreaksMost Extreme Outbreaks
• Largest outbreak: – 6350 cases [1987, North Carolina: S.
sonnei]
• Largest number hospitalized: – 396 [1998, Brazil: S. aureus]
• Largest number of deaths: – 68 [1990, Mozambican refugees in
Malawi: V. cholerae]

2a, 4a, 4b, 5 Multiple workers cause outbreak at
the same location (2a), through contamination of food (4a), no clear no clear source source (4b), or workers may be the
victims (5)
1 Single worker causes an Single worker causes an
outbreak that affects outbreak that affects patronspatrons
3a, 3bFoods contaminated by infected Foods contaminated by infected worker are temperature abused worker are temperature abused
leading to outbreakleading to outbreak
7 Infected consumers (patrons, families,
institutional residents, etc) likely source of infectious
agent
2b Offsite food
worker(s) infects other workers at a different location
Ill Consumers (Patrons, Families, Institutional
Residents, etc)
6Food
contaminated by offsite workers
8Worker(s) are infected but deny illness and outbreaks not reported as caused by
infected worker(s)


Social Gathering and Social Gathering and Staphylococcus aureusStaphylococcus aureus
• 8,000 people gathered in a community to celebrate a Catholic priest’s ordination in 1998 in Brazil
• After eating food provided, 4,000 were acutely ill and 2,000 hospitalized, 16 died
• Eight food workers began preparing the chicken, roast beef, rice, and beans over 48 h on the Friday before the event, and stored in aluminum containers at room temperature until Sunday morning
• These food workers had positive fingernail swabs for Staphylococcus aureus, and five of them had the same strain isolated from their nasopharynxes
• Leftover food was also found to contain S. aureus at 2.0 x 108 CFU/g, which produced 6 µg of enterotoxin A/g

Social Gathering and Social Gathering and Staphylococcus aureusStaphylococcus aureus
• 8,000 people gathered in a community to celebrate a Catholic priest’s ordination in 1998 in Brazil
• After eating food provided, 4,000 were acutely ill and 2,000 hospitalized, 16 died
• Eight food workers began preparing the chicken, roast beef, rice, and beans over 48 h on the Friday before the event, and stored in aluminum containers at room temperature until Sunday morning
• These food workers had positive fingernail swabs for Staphylococcus aureus, and five of them had the same strain isolated from their nasopharynxes
• Leftover food was also found to contain S. aureus at 2.0 x 108 CFU/g, which produced 6 µg of enterotoxin A/g

Examples ofExamples of S. aureus S. aureus OutbreaksOutbreaks
• 2 handlers sores on hands, 5 handlers same strain in nose
• S. aureus isolated from infected cut on hand of person who baked cake
• 11 hospitalized S. aureus isolated from stool, vomitus, sandwich and infected finger of food handler, sandwiches stored 8-10 hours without refrigeration
• S. aureus in food and on food handler, inadequate storage temperature for 5 hours
• S. aureus phage 6 patients and 6 food handlers, infected cut on hand of one food worker who mixed food ingredients with bare hands
• Cook handled and cooked ham with open cuts, sores and finger lesion
• Contamination from hand of a symptomatic food worker, stored at inappropriate temperature

School Children and NorovirusSchool Children and Norovirus
• 3,236 (41.5%) of 7,801 schoolchildren and 117 (39.4%) of 297 teachers were ill in Japan in 1989 after eating catered food
• Food had been provided by a catering company to nine elementary schools
• Workers had bare-hand contact with the food, and a worker reported symptoms of gastrointestinal illness on the day the food was prepared

School Children and NorovirusSchool Children and Norovirus
• 3,236 (41.5%) of 7,801 schoolchildren and 117 (39.4%) of 297 teachers were ill in Japan in 1989 after eating catered food
• Food had been provided by a catering company to nine elementary schools
• Workers had bare-hand contact with the food, and a worker reported symptoms of gastrointestinal illness on the day the food was prepared

Frosted Cakes Leading to Frosted Cakes Leading to Norovirus InfectionsNorovirus Infections
• A bakery worker in Minnesota in 1982 prepared 76 litres of frosting using his arm up to the elbow to break sugar lumps and scrape the sides of the vat
• There were subsequently 3,000 cases of norovirus infection
• He had five episodes of diarrhea and two of vomiting during his 6-h shift when he frosted the cakes
• Also he had sick children at home

Frosted Cakes Leading to Frosted Cakes Leading to Norovirus InfectionsNorovirus Infections
• A bakery worker in Minnesota in 1982 prepared 76 litres of frosting using his arm up to the elbow to break sugar lumps and scrape the sides of the vat
• There were subsequently 3,000 cases of norovirus infection
• He had five episodes of diarrhea and two of vomiting during his 6-h shift when he frosted the cakes
• Also he had sick children at home

Giardiasis from SaladGiardiasis from Salad
• In 1990, a food worker in the cafeteria of a large Connecticut insurance company was infected with Giardia lamblia and used her bare hands while slicing raw vegetables, causing 27 cases of giardiasis
• She tested positive and had used gloves for most food preparation activities but not for salad bar items
• The investigators noted that the outbreak was probably only detected because the affected individuals were insurance company employees whose medical care was administered by a single health management team

Giardiasis from SGiardiasis from Salad
• In 1990, a food worker in the cafeteria of a large Connecticut insurance company was infected with Giardia lamblia and used her bare hands while slicing raw vegetables, causing 27 cases of giardiasis
• She tested positive and had used gloves for most food preparation activities but not for salad bar items
• The investigators noted that the outbreak was probably only detected because the affected individuals were insurance company employees whose medical care was administered by a single health management team

Hepatitis at a ResortHepatitis at a Resort• In 2004, a large outbreak with 351 hepatitis A cases occurred
involving tourists at a specific hotel in the Egyptian resort city of Hurghada
• Guests who developed HAV infection after their vacation were 2.6 times more likely to have ingested orange juice than were healthy controls
• None of the hotel staff in Egypt was positive • The juice was not pasteurized and came from a site where hygiene
problems were identified• Although an infected worker at the juice production company was
the most likely source, none of the company staff was IgM positive, but staff members often changed and were not available for testing

Hepatitis at a ResortHepatitis at a Resort• In 2004, a large outbreak with 351 hepatitis A cases occurred
involving tourists at a specific hotel in the Egyptian resort city of Hurghada
• Guests who developed HAV infection after their vacation were 2.6 times more likely to have ingested orange juice than were healthy controls
• None of the hotel staff in Egypt was positive • The juice was not pasteurized and came from a site where hygiene
problems were identified• Although an infected worker at the juice production company was
the most likely source, none of the company staff was IgM positive, but staff members often changed and were not available for testingbut staff members often changed and were not available for testing

Norovirus in a Restaurant (1)Norovirus in a Restaurant (1)• In Michigan in 2006, 364 restaurant patrons became ill with norovirus GI
illness after dining at a restaurant where employees had reported to work while ill
• On Jan 28, a line cook vomited at home before reporting to work at 11:00 a.m. and then vomited again into a waste bin beside the frontline workstation at approximately 2:00 p.m. while preparing antipasti platters, pizzas, and salads
• After vomiting, he remained on site (but off the cooking line) and left work at 4:15 p.m.
• This cook also reported to work on Jan 29 from 11:00 a.m. to 4:30 p.m. while still experiencing loose stools
• Because of the open physical layout of the restaurant, no barrier impeded airborne spread of the virus from the kitchen to the main dining area

Norovirus in a Restaurant (2)Norovirus in a Restaurant (2)• There was a significant association between the platter and the ill persons• Patron attack rates increased after the cook vomited and among
employees, particularly cooks vs. servers, who worked on Jan 28• The investigation revealed deficiencies in employee hand washing
practices, cleaning and sanitizing of food and nonfood contact surfaces, temperature monitoring and maintenance of potentially hazardous food, and maintenance of hand-sink stations for easy accessibility and proper use
• A quaternary ammonium based sanitizer normally used to clean the restaurant was ineffective against the norovirus
• Then, a bleach solution used to disinfect the restrooms and all surface areas within at least a 25-ft radius of the vomiting site was effective for preventing further illnesses

Norovirus in a Restaurant (1)Norovirus in a Restaurant (1)• In Michigan in 2006, 364 restaurant patrons became ill with norovirus GI
illness after dining at a restaurant where employees had reported to work while ill
• On Jan 28, a line cook vomited at home before reporting to work at 11:00 a.m. and then vomited again into a waste bin beside the frontline workstation at approximately 2:00 p.m. while preparing antipasti platters, pizzas, and salads
• After vomiting, he remained on site (but off the cooking line) and left work at 4:15 p.m.
• This cook also reported to work on Jan 29 from 11:00 a.m. to 4:30 p.m. while still experiencing loose stools
• Because of the open physical layout of the restaurant, no barrier impeded airborne spread of the virus from the kitchen to the main dining area

Norovirus in a Restaurant (2)Norovirus in a Restaurant (2)• There was a significant association between the platter and the ill persons• Patron attack rates increased after the cook vomited and among
employees, particularly cooks vs. servers, who worked on Jan 28• The investigation revealed deficiencies in employee hand washing
practices, cleaning and sanitizing of food and nonfood contact surfaces, temperature monitoring and maintenance of potentially hazardous food, and maintenance of hand-sink stations for easy accessibility and proper use
• A quaternary ammonium based sanitizer normally used to clean the restaurant was ineffective against the norovirus
• Then, a bleach solution used to disinfect the restrooms and all surface areas within at least a 25-ft radius of the vomiting site was effective for preventing further illnesses

Norovirus from SaladNorovirus from Salad• In 2000, a catered meal and distributed to 52 car dealerships in the US
as a reward for high car sales was responsible for multiple gastroenteritis outbreaks in 13 states, resulting in at least 333 cases
• Pasta salads from one caterer was strongly associated with illness
• Pasta was placed in large plastic bins, other ingredients were added, and food workers mixed the salad by immersing their ungloved arms up to the elbow
• Although the workers denied any history of illness in the preceding week, 2 of 15 employees had elevated IgA antibody titres to norovirus
• This caterer had been cited by health inspectors for multiple sanitary code violations and was temporarily closed pending sanitary improvements

Norovirus from SaladNorovirus from Salad• In 2000, a catered meal and distributed to 52 car dealerships in the US
as a reward for high car sales was responsible for multiple gastroenteritis outbreaks in 13 states, resulting in at least 333 cases
• Pasta salads from one caterer was strongly associated with illness
• Pasta was placed in large plastic bins, other ingredients were added, and food workers mixed the salad by immersing their ungloved arms up to the elbow
• Although the workers denied any history of illness in the preceding week, 2 of 15 employees had elevated IgA antibody titres to norovirus
• This caterer had been cited by health inspectors for multiple sanitary code violations and was temporarily closed pending sanitary improvements

Characteristics of PathogensCharacteristics of Pathogens

Infectivity of Pathogens Transmitted by Infectivity of Pathogens Transmitted by
Infected Food WorkersInfected Food Workers Agent Incubat
-ion PeriodIn Days(mean)
Carriage(C)
Rates Reported
(%)
Presymp-
tomaticSheddin
gTime
(days)
Sympto-
maticPeriod (Days)
Post-sympt
-omati
cShedd-ing
(days)
%Asymp-tomatic
OverallPeriod
of Infect-ivity
(days)
Source of
Infectious
Material Carriage
/Sheddin
g
Norovirus
0.6-3.2 GI : 1.1-1.5 Control 0.2
1.5? 1-11 2 weeks
32 May be >2 weeks
IT, F, RT, V
HAV 10-50 (28)
0.01 in population
10-14 7-14 21 (180)
8 (70 in elderly)
Up to 8 weeks
F, U
Salmon-ella
0.25-10 GI:0-16 Control: 0.1-1.6
X 7-10 4-22 weeks
0.23-1019 for FWs in DCs
Up to years
IT, F
Shigella 0.5-6 GI :0-0.8 X 4-7 60-150 55 - 75 Up to years
IT, F
S. aureus
2-6 hours
20-36 C C C 20 - 65 Years N, S, C
Giardia lamblia
3-25 (7) GI:0.4-16 X 7-60 Up to 35 (children)
Months IT, FIT = Intestinal Tract, RT = Respiratory Tract, F = Feces, N= Nasal Secretions, S = Skin/Skin Lesions, U = Urine, V = Vomitus

Foodborne Pathogens Transmitted by Foodborne Pathogens Transmitted by Infected Food Worker and Periods of Infected Food Worker and Periods of
InfectivityInfectivity0 50 100 150 200 250 300
Norovirus (SRSV/NLV)
Hepatitis A
Salmonella spp.
S. Typhi/Paratyphi
Shigella spp.
Staphylococcus aureus
Streptococcus pyogenes
Giardia lamblia
Campylobacter jejuni
Cryptosporidium parvum
Vibrio cholerae
E. coli O157:H7
Yersinia enterocolitica
Time After Exposure (Days)
Incubation Incubation/Pre-symptomatic
Pre-symptomatic Shedding Phase
ExtendedSymptomatic
SymptomaticPeriod
Post-symptomatic Phase ExtendedPost-symptomatic Phase
Carrier State

Levels of Pathogens in Body ExcretionsLevels of Pathogens in Body Excretions• Salmonella in feces
– Ill or early convalescence: 105-107 CFU/g– Late excretion (infants excrete longer): 100-103 CFU/g– 10-19 days after illness: 100-106 CFU/g– 69-102 days after illness: 100-104 CFU/g
• Sneeze with Streptococcus pyogenes– up to 106 CFU/sneeze– up to 500 CFU/154 cm2 1.5 – 9.5 feet from sneeze source
• HAV in feces just before hepatitis symptoms begin– 108 infectious particles/g
• Norovirus in feces while ill– 105 – 1010 copies/g
• Cryptosporidium in one bowel movement: 108 – 109 oocysts

Fecal Contamination of Hands During Fecal Contamination of Hands During Toilet Use With and Without Toilet Toilet Use With and Without Toilet
PaperPaper• Mean fecal weight/hand (g) after cleansing
– Without toilet paper 8.5 x 10-6 - 9.8 x 10-7
– With toilet paper 5.0 x 10-9
• Pathogens can be present in feces at levels of from 105 to 1011 per g. A tenth of a milligram of fecal material (10-4 g), an amount barely perceptible, might contain up to a million infectious bacterial cells or viral particles
• At 10-7 g fecal matter of contamination per hand and a pathogen that present at 1011 per g, if hands were washed and/or sanitized, a 2 to 3 log reduction (99%-99.9%) could still allow a worker to transmit a few cells
• Add to the fact that those ill may be more careless with fecal cleanliness (continual cleanup from diarrhea, fecal accidents, and not focused on the job and hygienic practices), and the risk increases greatly

Survival of Enteric Pathogens on Survival of Enteric Pathogens on
Hands and SurfacesHands and Surfaces Infective
AgentSurfaces Log, % Loss or
Half LifeSalmonella Enteritidis in egg white and yolk
Hands, inoculated eggs, formica surface, utensils
Survived well 24 hrs.
Shigella sonnei Fecally- contaminated hands
Survival for 3 hrs.
S. aureus Skin and clothing 1 log/5 hrs.
Campylobacter jejuni
Hands with peptone, chicken broth, and50% blood
3-7 log/ 2 min.6 log/ 15 min.6 log/ 45 min.
E. coli Skin 3 log/5 min.
E. coli in milk Fingertip 94% loss in 45 min.
Entamoeba histolytica
Hands (nails in feces) Survival for 45 min.

Survival of PathogensSurvival of Pathogens
• Norovirus survived in carpets and toilet facilities for more than one day after an individual vomited on seats and washroom; infected clean-up crew and subsequent concert hall attendees infected by aerosols
• Illnesses from carpet removers in a hospital ward 12 days after vomiting outbreak occurred
• Pathogens tend to survive longer on surfaces such as ceramic tile, steel, dust, glass and plastic than on hands

Levels of Pathogens in Raw Meat Levels of Pathogens in Raw Meat
and Poultryand Poultry
Infective Agent
Product Log 10 CFU
Campylobacter jejuni
Chicken juices, cecaChicken carcasses
103-109
<101-109
E. coli O157:H7 Ground beefCattle/sheep feces
5103-105
Salmonella Chicken juices, organ, carcassesChicken fillets
102-106
<10% with up to 103

Transfer of Organisms from HandsTransfer of Organisms from Hands
• The transfer efficiency between hands and lettuce was found to be 0.3% and from hands to spigots was 1%
• The transfer rate of HAV from fingerpads of adult volunteers to pieces of fresh lettuce was determined to be 9% of the infectious load on the fingers
• Lettuce touched by a washed hand may be contaminated with as many as 3.8 log10 CFU indicator bacteria
• A 10% transfer rate of bacteria from food to hands or bare hand to food; and by using gloves, this rate was reduced to 0.01%

Outbreaks Associated with Lack of Outbreaks Associated with Lack of
Adequate Hygienic FacilitiesAdequate Hygienic Facilities • Inadequate toilet facilities (Yersinia, Shigella,Vibrio,
Salmonella) • Non functional toilet (Shigella)• Lack of handwashing facilities (Shigella,Vibrio, HAV)• Inadequate handwash facilities (Shigella, norovirus)• Difficult to use faucets (HAV)• Lack of running water (Yersinia, Shigella,Vibrio)• Lack of fingernail brush (Giardia)• Lack of soap (Shigella,Vibrio, Giardia)• No paper towels for hand drying (Shigella,
Salmonella, norovirus)


Handwashing OccasionsHandwashing Occasions• Wash hands thoroughly with disinfectant
soap and water at appropriate times for the job description
• Also after the following:• handing raw foods• after going to the toilet• after contact with persons suffering from
acute GI symptoms• after being in contact with infants and
incontinent individuals

Minimize Hand ContactMinimize Hand Contact
Evaluate food handling procedures and modify to reduce or eliminate hand contact for RTE food:– Gloves– Utensils– Deli papers

Exclusion and Work Exclusion and Work RestrictionsRestrictions
• Exclude infected symptomatic persons (GI) from preparing and serving food during communicable periods of illness
• Exclude infected persons known to be asymptomatic carriers based on screening
• Restrict food workers from preparing or serving food• Infected skin lesions• Sore throat• Acute respiratory infections
• Food workers should be kept on sick leave for 48 h following disease cessation

Hygiene Education, Training and Hygiene Education, Training and SupervisionSupervision
• Train food workers and supervisors:– in proper food handling practices and procedures– to report personal and family illness
• Provide supervision of workers:– Surveillance of workers and correction of
handling errors– Screen food workers (nasal and stool):
• at start of employment• routine testing• upon return from travel in area having high endemic
disease rates
• Immunize workers when feasible (HAV, etc)

What Have Investigations of What Have Investigations of Outbreaks Where Food Workers Outbreaks Where Food Workers
Were Implicated Taught Us - Were Implicated Taught Us - Sources?Sources?
• There are many sources where food workers have become infected– Ill family members, homosexual partners or
diapering a sick child– Intravenous drug use– Eating contaminated food– Environmental sources, e.g., water, animals– Travel abroad– Contact with other infected workers

Spread in the Food Worker Spread in the Food Worker EnvironmentEnvironment
• Once a worker has brought an agent into a food operation, it can easily be transferred from person to person, person to food contact surfaces and to food
– Lack of adequate handwashing facilities and improper handwashing and drying
– Long and artificial nails are too difficult to clean effectively
– Lesions and wounds harboring pathogens are not properly covered
– Workers continuing to work when infected and ill (diarrhea and vomiting): management or worker decision
– Transmission between workers in food preparation area
– Lack of use of gloves/bare hand contact

Removal of Removal of ContaminantsContaminants
• Fecal contamination can be extensive even after washing – use of toilet paper doesn’t prevent all fecal organisms from going on finger tips and from there to contact surfaces
• Vomiting can spread viral particles over long distances despite any clean up afterwards and particles can persist for days or weeks
• Thorough and frequent handwashing and use of gloves keeps contamination in food environment to a minimum

Some Problems To Be Some Problems To Be ResolvedResolved
• Having incentives for workers to stay home when they are ill or diagnosed with a likely infection
• Identifying workers who are asymptomatic and need to be away from handling food and any physical contact with other workers
• Effective communication with low-paid workers, often speaking other languages than English, may not read well and will move on for a continual turnover, issues of trust and motivation
• Putting more resources into effective local investigation of outbreaks
• More priorities for handwashing in industry/home

AcknowledgementsAcknowledgements
• Bert Bartelson, Judy Greig, and Barry Michaels, members of the Committee for the Control of Foodborne Illness, International Association for Food Protection (IAFP), and IAFP Board

QUESTIONS?

Categorization of Outbreaks Where Food Workers Were
Implicated3. After food worker(s) contaminates food
via:3a) fecal contamination (e.g., by
Salmonella, Shigella, Yersinia) or 3b) through skin, nose and throat
contamination (e.g., Streptococcus pyogenes, Staphylococus aureus)
– Temperature abuse results in bacterial multiplication resulting in high enough numbers to cause illness

Categorization of Outbreaks Where Food Workers Were Implicated
4. Multiple food workers are: 4a) unequivocally the cause of the
outbreak though contamination of food or food contact surfaces, or
4b) linked to an outbreak but there is no clear initiating source
5. Food worker(s) becomes infected but uncertain whether they are victims or causes of outbreak

Categorization of Outbreaks Where Food Workers Were
Implicated6. Food contaminated with pathogens
by offsite workers and delivered to the location where the outbreak occurs by directly infecting consumers/patrons
– Details of the worker contribution to the contamination are usually not known

Categorization of Outbreaks Where Food Workers Were Implicated
7. Patrons (those being served), not workers, are the probable source of the infectious agent though contamination of food or food contact surfaces
8. Outbreaks where workers are implicated epidemiologically and likely are infected or colonized but deny illness

Category 1:Single Worker Causes an Outbreak
37 cases associated with cold salad bar items from the cafeteria of a Minnesota college, 2000
– Index case a symptomatic food worker– Called in sick but symptoms resolved later that day– Returned to work the next day and worked the
remainder of the week in salad bar section, with extensive bare-hand contact of salad items
– Noroviral agent based on epidemiological information – Call-in ill log useful to determine dates that
employees were ill and to ascertain the responsible employee

Category 2a:Multiple Workers Cause Outbreak
Multi-state outbreak of Salmonella Thompson: 78 cases at fast food restaurants and catered events– Full-time employee did not wear gloves and handled
every individual bread item at least twice– Worked with symptoms for 4 days until overnight
hospitalization– Resumed work after discharge and continued working
until termination of employment– She infected brother who also worked with dough and
bread– No formal training on safe food-handling practices– Many employees spoke only Spanish but had English
procedure manuals

Category 2b: Offsite Food Worker(s) Infects Workers at a
Different LocationHAV affected 40 university students, 11 employees of two restaurants, and 11 other residents in Arizona, 1973
– Two distinct epidemic waves at the 2 restaurants– Index case of first restaurant prepared salads– Index case of the second restaurant had eaten at
the first restaurant– Implicated vehicles at the second restaurant included
guacamole, green salad, spaghetti, and hamburger

Category 3a: Foods Fecally Contaminated by Infected Worker are
Temperature Abused Leading to Outbreak
July 1981 New York: Y. enterocolitica O:8 isolated from 37 persons including head cook and kitchen staff
– Five hospitalized for appendicitis – Powdered milk and dispenser contaminated when
food workers cleaned and repaired a broken spigot
– Same strain isolated from chow mein indicating multiple contamination scenarios
– Reconstituted milk held 24 hours under cool conditions but allowed growth of Yersinia

Category 3b:Foods Nasally Contaminated by Infected Worker are Temperature
Abused Leading to OutbreakConvention in Florida 1979: outbreak of pharyngitis, 72/231 ill, including waiters and cooks
• Streptococcus pyogenes Group G isolated from 10 of 16 with pharyngitis and 1 of 41 who did not
• Illness associated with chicken salad• Cook prepared chicken salad a day prior to her
symptoms• Cooked chicken refrigerated overnight in a deep
container • No indication she wore gloves or washed hands
frequently• Opportunity for growth of the Streptococcus

Category 3b: Foods Contaminated by Lesion of Infected Worker and are Temperature Abused Leading to
Outbreak: Commercial Travel• Flight attendant and 196 passengers rapidly
developed vomiting and diarrhea following ingestion of ham and cheese omelets served during a chartered flight for a tour group from Tokyo to Paris, stopping en route in Alaska and Denmark
• Cook who prepared ham had infected finger• Ham left at room temperature for six hours
• S. aureus isolated from food samples

Category 4a: Multiple Food Workers are Unequivocally the Cause of the
Outbreak 2000: multi-state outbreak, 333 cases, catered meal prepared in Ohio and distributed to 52 car dealerships nationwide
– Consumption of any of four side salads strongly associated with illness
– Ingredients were placed in large plastic bins and mixed by food workers who immersed ungloved arms
up to the elbow– 2 of 15 employees had elevated norovirus titers – Three food handlers were symptomatic before
outbreak

Category 4b: Multiple Food Workers are Linked to
Outbreak But There is No Clear Initiating Source
July 1992, 46 patrons at 21 restaurants in Michigan and one in Ohio infected with Shigella flexneri – Associated with consumption of pre-prepared
salads from a central commissary– 15 infected workers ill during the same time
period and four prepared salad during the outbreak period
– Salad was mixed with bare hands, bagged by machine, and employees added or subtracted from the bags to meet the weight standard
– Investigation failed to identify the infected employees

Category 5: Food Worker(s) Become Infected but Uncertain Whether They Are
Victims or Cause of Outbreak
Large outbreak of shigellosis associated with a mass gathering in a national forest area, North Carolina, 1987– Over 50% of 12,700 attendees infected – Transmission assumed to be by food and water,
followed by person-to-person contact– Food prepared in 47 communal kitchens with
limited sanitation– Food from at least one kitchen implicated and
unboiled water drunk by attendees

Category 6:Food Contaminated With Pathogens by Offsite Workers and Delivered to the Location Where the Outbreak Occurs
.Six norovirus outbreaks (1,143 cases) in institutions or commercial catering settings, June to Sept. 2005 in Denmark, linked to frozen raspberries imported from Poland– Unheated frozen raspberries served one day
before start of each outbreak– Estimated 400 elderly people affected and at
least 23 hospitalized– Three different norovirus serotypes isolated – Several independent contamination events
likely occurred – Infected workers in the harvesting or
processing of the raspberries in Poland were a likely but not proven source

Category 7: Patrons Are the Source of the Infectious Agent Though Contamination of
Food or Food Contact Surfaces
.Mediterranean-style restaurant in Melbourne, Australia, three successive norovirus outbreaks, May 1998 - June 1999
• Food served on platters and patrons ate with fingers, moving from table to table
• Different norovirus strains isolated in the three outbreaks indicating no reservoir but recurring contamination of food
• Demonstrates how norovirus can be transmitted where many people are in close contact and touch and eat food

Category 8: Outbreaks Where Workers Are Implicated but They
Deny Illness
Minnesota 2004: six relatives complained of GI illness after dining at a restaurant– 1 of 6 positive for norovirus– None of the workers were obviously
symptomatic – Most of the staff were Spanish speaking and the
manager acted as translator– Conclusion: outbreak could not be adequately
characterized even though the likely source of the norovirus was one or more employees

Examples of Streptococcus Outbreaks
• Military base: 3 food handlers of boiled egg salad were asymptomatic carriers of Streptococcus – hand contamination or sneezing
• Military base: an egg salad preparer tested positive, he shelled boiled eggs with bare hands for the salad
• School: food preparer had open hand lesion that came in direct contact with the macaroni and cheese
• Catered event: preparer of egg salad had extreme cellulitis on hands; he tasted the salad, workers coughed or sneezed

Examples of Hepatitis A Outbreaks
• Salads– Restaurant: two asymptomatic pantry workers
contaminating food by hand shredding lettuce and dipping fingers into dressing to taste them
– Caterer: “Salad boy” with apparent good hygiene hand-tore moist lettuce and soon developed fever and malaise
• Drinks– Employee, who was HAV positive but asymptomatic,
was a suspected IV drug user, and had helped prepare fountain drinks and sandwiches
– Bar tender had chronic diarrhea and contaminated the glasses when served beverages
– Asymptomatic carrier did not wash his hands after using the toilet and contaminated the punch at a catered event

Examples of Hepatitis A Outbreaks
• Fast food restaurant: food worker, who was a drug user and family described him as having poor hygiene, had diarrhea and tested positive for HAV
• Caterer: Asymptomatic sandwich maker had prior nausea and vomiting, most likely contamination through hand contact with foods
• Caterer: Pastry-cook had jaundice prior to preparing pastries by bare hand for meals
• Bakery: baker’s assistant with hepatitis was directly involved in handling and dipping cooked pastries

Examples of Shigella Outbreaks
• University: Shigella infections after eating shrimp deveined in India – contamination source uncertain but has to be human fecal
• Restaurant: employees ill with Shigella flexneri prepared tossed salad by reaching into chopped salad ingredients with bare hands
• Restaurant: worker infected with Shigella after a trip to Mexico washed lettuce with bare hands
• Restaurant: worker infected with Shigella flexneri in restaurant with hygiene violations, including a lack of hand washing between tasks and inadequate handwashing facilities

Examples of Salmonella Outbreaks
• Salmonella enteritidis on curly fried potatoes and ice handled bare-handed by employee who had onset of illness 1 day prior, no paper towels
• Prison: Inmate who deboned turkey had multiple excoriated lesions on both forearms that had a positive S. aureus culture, Salmonella infantis isolated from turkey eaters

Examples of Norovirus Oubreaks
• Salad: asymptomatic noroviral shedding by one or more of the workers who handled lettuce with bare hands
• RTE food: hand preparation by untrained staff and patients
• Catered function: food worker excreted the virus and touched RTE foods including melon
• Cruise ship: ice machine did not have proper air-gap device to prevent sewage backup, and the ice was contaminated by hands of those scooping it out
• Bakery: A cake decorator, ill with GI, was wearing long artificial nails with which she contaminated the icing
• Restaurant: bad management forced employee to work, who was sick and wanted to stay home, used bare hands on hamburgers

Examples of Outbreaks Associated with Bare Hand Contact
• Restaurants– Bare hands serving pineapple slices, not ill at the time,
but ill 3 hours after handling– Asymptomatic worker with no gloves sliced meats,
cheese and vegetables, no adequate washing area– Symptomatic worker prepared guacamole and salsa with
bare hands, good hand washing facilities– Employee excreting virus while using bare hands to
remove tissues from steamed bovine heads
• Bakeries– Soiled hands not washed due to painful skin lesions– Contaminated baked goods when applying sugar glaze
with bare hands
• Deli shop– 76 year old grandmother typhoid carrier handled
cannelloni without gloves after they were cooked once a week

Data SourcesOutbreak data from 1927 to 2004 from:
– Michigan (2000-2003): State line listings – Minnesota (1999-2004): State line listings and
outbreak reports – New York (1985-2000): State line listings – Washington (1990-2003): State line listings and
outbreak reports – Health Canada (1976-1996): Line listings from
annual reports of foodborne and waterborne disease outbreaks
– Outbreak reports from other countries– Published peer-reviewed literature including reviews

Large Gathering and Large Gathering and ShigellosisShigellosis
• For 2 weeks, food was prepared in 47 communal kitchens in a national forest area for a Rainbow gathering in North Carolina in 1987
• There were no toilets, hand washing facilities, safe drinking water sources, or refrigeration
• The outbreak began on July 4 1987, and rapidly spread throughout the gathering until it was closed on July 15 with a total of 6350 cases
• Transmission was assumed to be by food, water, and person-to-person contact.
• Secondary infections occurred after ill persons returned to home communities in other parts of the US

Cake and NorovirusCake and Norovirus
• A cake requiring direct hand contact during its preparation was associated with the majority of illnesses in an outbreak of 2700 persons in 2002 in Massachusetts
• At least two bakery employees experienced norovirus-compatible illness during the week preceding the weddings. Two wedding guests, a wedding hall employee, and one of the bakery employees were ill; identical sequence types were detected in the stool specimens submitted

Shigellosis from Hamburgers in Shigellosis from Hamburgers in a Resorta Resort
• A butcher who prepared hamburger patties at a resort in Haiti in 1984 had a Shigella flexneri infection and continued working while ill during the 3-week period in which 1,136 guests reported illness
• Illnesses were linked only to those who consumed raw or rare hamburger; this was followed by secondary person-to-person spread between roommates

Categorization of Outbreaks Where Food Workers Were Implicated
1. Single food worker causes an outbreak though contamination of food or food contact surfaces
2. Single food worker infects other workers (victims) who in turn infect consumers/patrons though contamination of food or food contact surfaces:
a) in the same establishment or b) in a separate location

Transfer of Organisms from HandsTransfer of Organisms from Hands
• Study using Nalidixic acid-resistant Enterobacter aerogenes as a surrogate for an enteric pathogen to follow cross-contamination demonstrated that after handling chicken, contaminated hands transferred 2.4 to 5.7 log10 of bacteria to a spigot used to wash hands; after washing 1.9 to 6.5 log10 still remained on hands (Chen et al. 2001)
• Perez et al. (2006) showed that there was a high risk with the use of the same gloves to handle contaminated chicken meat and then slice ham compared to the safer use of different gloves to handle each product

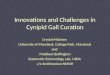
Listeria monocytogenes in Different Cross-contamination Scenarios (Perez et al., 2006)
• A series of cross contamination scenarios at retail were ranked according to their risk level
• The highest risk corresponded to the use of the same gloves to handle contaminated chicken meat and then sliced ham compared to the safer use of different gloves to handle each product
• The lowest risk corresponded to use of gloved hands but washed between handling the chicken and slicing the ham (only 250/100,000 slices would be contaminated)
• All scenarios were capable of ham reaching levels above 108 cfu/g after storage when growth can occur
• Lack of knowledge of transfer rates provided the model with an important uncertainty component

Simulated Distribution of L. monocytogenes at the Time of Consumption (N) for 3
Scenarios Perez et al., 2006)
Contaminated meat-bare hands-slice
Mean = -2,566866
X >-5,5595%
X >23.421%
0
0.05
0.1
0.15
0.2
0.25
-10 -8 -6 -4 -2 0 2 4 6 8 10
L. monocytogenes (log CFU/g)
Fre
qu
ency
Contaminated meat -gloved hands-gloved hands-slice
Mean = -6,145167
X >2.088%
X >-8,8395%
0
0.05
0.1
0.15
0.2
0.25
-15 -10 -5 0 5 10
L. monocytogenes (log CFU/g)
Fre
qu
ency
Contaminated meat-bare hands-washing-gloved hands -slice
Mean = -2,323807
X >-5,0795%
X >23.534%
0
0.05
0.1
0.15
0.2
0.25
-10 -8 -6 -4 -2 0 2 4 6 8 10
L. monocytogenes (log CFU/g)
Fre
qu
ency

Effective Handwashing • Wash, rinse, dry• Fingernail brush• Instant hand sanitizer• Frequent (Task appropriate)• Minimize cross-contamination-use
handsfree devices, e.g., turn on tap/faucet
• Paper towel dispensers/hot air drying/doorless entry or automatic doors
• Handwash process monitored, documented and verified (MDV)

Studies on Handwashing
• Thumbs, palms, spaces between fingers, and fingertips including the fingernail area, are areas in which contamination is most likely to remain. Hand drying may help make up for deficiencies in the washing process
• E. coli and Pseudomonas fluorescens mixed with ground beef and rubbed onto hands were 95% removed with a single handwashing using an E1 soap– a 75% reduction was subsequently shown with
a tap water wash only • Giardia was removed form the hands with soap
and handwashing. When 10,000 cysts were placed in the palm of the hand, handwashing eliminated 99% (100 cysts)

Studies on Handwashing
• Based on laboratory testing using artificial contaminants, the effectiveness of handwashing, including washing, rinsing and drying, ranged from 2 to 3 log10 reduction (99%-99.9%)
• Compliance rates for handwashing are estimated at 50% but no surveys have been done

Food Preparation and Environmental Control
• Follow proper cooking, hot holding, chilling and storage procedures
• Environmental controls:– Disinfect surfaces often– Clean change of work clothing

Airflight IllnessesAirflight Illnesses• 1. British Airways flights in 1984 with a total of 866 cases: 631
passengers, 135 aircrew, and 100 catering personnel and loaders, with 2 passenger deaths
• An ill chef prepared the aspic glaze, which was then left at ambient temperatures
• Also, it was reported that a party given by a senior catering manager at the catering center resulted in all guests becoming ill, with two hospitalized
• 2. Charter flights to and from Canary Islands to Finland in 1976 resulted in 1,800 salmonellosis cases
• Salmonella Typhimurium phage type 96 was isolated from passengers, mayonnaise, and one food worker in the Las Palmas catering establishment

Airflight IllnessesAirflight Illnesses• 1. British Airways flights in 1984 with a total of 866 cases: 631
passengers, 135 aircrew, and 100 catering personnel and loaders, with 2 passenger deaths
• An ill chef prepared the aspic glaze, which was then left at ambient temperatures
• Also, it was reported that a party given by a senior catering manager at the catering center resulted in all guests becoming ill, with two hospitalized
• 2. Charter flights to and from Canary Islands to Finland in 1976 resulted in 1,800 salmonellosis cases
• Salmonella Typhimurium phage type 96 was isolated from passengers, mayonnaise, and one food worker in the Las Palmas catering establishment