Embed Size (px)
Citation preview

Exams & Grading:
85% of the final grade:
Exam scores from each of the three Sections will represent one-third of a total of 85% of the final grade for the course. Two exams will be administered in Section I, while one exam each will be given in Sections II & III. Sectional exams will be based on Tuesday-Friday lectures and employ a mix of short answer & essay questions.
10% of the final grade: The Final Exam on the “Integrative Perspective on Diabetes” will comprise 10% of the final grade.
5% of the final grade: The average score for the written responses to pre-assigned topics for Monday Discussions will comprise a total of 5% of the final grade.
A traditional numerical scoring system will be used to generate a final letter grade - A= 90-100% B=80-89% C=70--79%, D=60-69%, and F= 59% or less.
FIS 2006

diabetes
• Type I– Autoimmune destruction of β-cells of
pancreas
• Type II– Insulin resistance coupled with deficient
release
hyperglycemia & hyperlipidemia leading to atherosclerosis, neuropathy & infection
FIS 2006 (Diabetes)Version date: Aug 03, 2006
Final Exam: Integrative Perspective on Diabetes - 10% Final Grade
Types of Questions:
Contrast the etiologies of Type I & Type II diabetes, and discuss the mechanisms for the metabolic derangements leading to hyperglycemia and hyperlipidemia.
Focus on a specific organ system (vascular, neural, host-defense)
subjected to long-standing hyperglycemia, hyperlipidemia and other abnormalities secondary to poorly controlled Type I or II diabetes:
- Discuss the mechanisms for pathology;- Discuss the mechanisms for pharmacological prophylaxis and/or
treatment of organ system dysfunction.

FIS Organization:
Exam #1- Basic Principles → diabetes
Exam #2- Neurobiology → diabetes
Exam #3- Endocrinology → diabetes
Exam #4- Immunology & Bacterial Pathogenesis → diabetes ↓
↓
(Exam #5: final)

FIS 2006 (Diabetes)
Lectures:
Sept 2 - Diabetes & PolyphagiaOct 06 - InsulinOct 10 - Counter Regulatory HormonesOct 18, 18 & 20 - Homeostasis & Responses to External EnvironmentNov 17 – Immunology of Diabetes
Monday Discussions: (student-driven lecture questions, student-driven journal clubs & faculty-driven discussion of relevance of lectures to diabetes).
Resource Text: Ellenberg & Rifkin’s DIABETES MELLITUS, sixth edition, Porte et al.,
Neurobiology
Sept 11 - Diabetes & Neuropathy Journal Club OrganizationSept 18 - Diabetes & Neuropathy Journal ClubSept 25 - Diabetes & Neuropathy Journal ClubOct 02 - Diabetes, Erectile Dysfunction & Viagra
Basic Principles & Endocrinology
Aug 28- Diabetes & AtherosclerosisOct 09 - Diabetes, Insulin Resistance & Metabolic SyndromeOct 16 – Pharmacological Management of DiabetesOct 23 - Diabetes, Insulin Resistance & Polycystic Ovary Syndrome
Immunology & Bacterial Pathogenesis:
Nov 27 - Immunology of DiabetesDec 04- Infections & Diabetes

FIS & Diabetes:
Type I Diabetes: Autoimmune destruction of β-cells of pancreas
Type II Diabetes: Insulin Resistance
Pathology of Diabetes:
Atherosclerosis
Neuropathy
Susceptibility to Infection
Pharmacological Prevention:
Type I- Insulin Replacement Regimens
Type II- Insulin Secretogogues - Insulin Sensitizers
Pharmacological Treatment:
examples: Viagra & Erectile DysfunctionAldose Reductase Inhibitors & NeuropathyInsulin Sensitizers & Polycystic Ovary Syndrome

Atherosclerosis: Abnormal vascular smooth muscle migration to sub-endothelial spaceand proliferation
Key abnormalities:- smooth muscle- lipid
Significance:-↓ perfusion- infarction
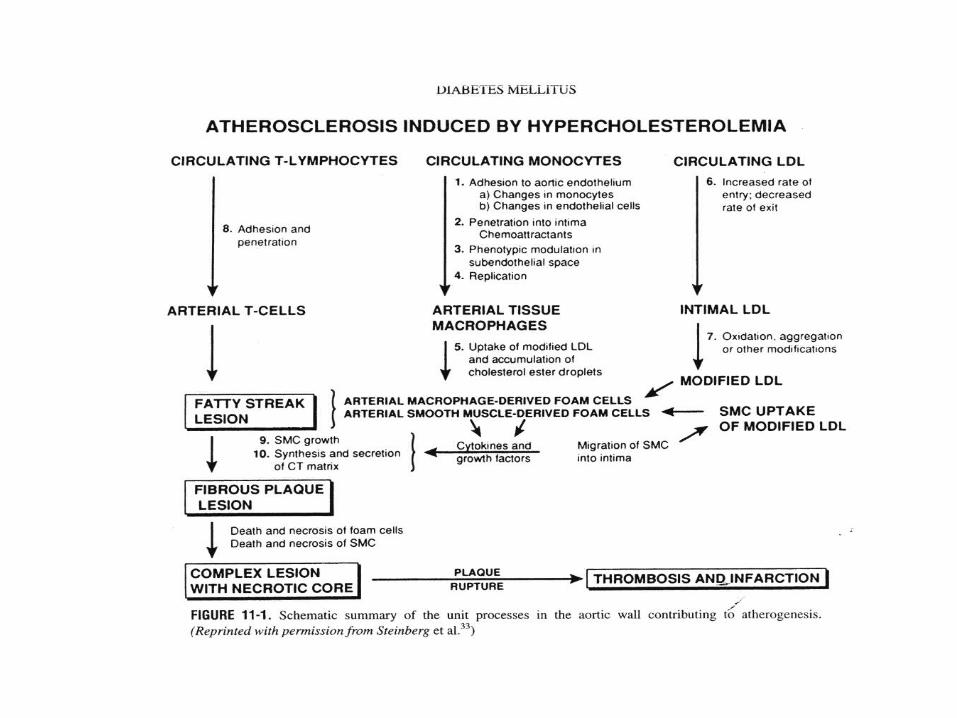

Atherosclerosis
Insult to Endothelium
potential mechanisms include non-enzymatic glycosylation
& lipid-induced macrophage growth factors
Consequence & Focus for FIS Discussion:- defective inhibitory proteoglycans of endothelial
extracellular matrix in contact with smooth muscle cells- deficient release of inhibitory NO to smooth muscle
cells- abnormal smooth muscle migration & proliferation

Diabetic Neuropathy

mechanism for diabetes-induced neurodegeneration
Sorbitol• glucose → sorbitol → fructose
– osmotic perturbations due to sorbitol (hydroxyated glucose),
» “trapped” intracellularly
» specific to neurons (aldose reductase)
» elevated intraneuronally in diabetes due to hyperglycemia & insulin-independent neuronal glucose uptake
– oxidative stress due to depletion in NADPH by aldose reductase
Diabetes & Neuropathy: 4 Journal Clubs
1) Descriptive changes:
Diabetes-induced changes in morphology & electrophysiology
2) Causal role of sorbitol:
Diabetes-induced intra-neuronal sorbitol, potentially leading to perturbations via osmotic distortion &/or oxidative stress
3) Abnormal protein phosphorylation of neuronal structure:
Diabetes-induced abnormal neurophilament phosphorylation, potentially leading to impaired structural/functional integrity and ultimately ↓ conduction & terminal degeneration.
4) Loss of neurotransmitter synthesis in nerve terminal:
Diabetes-induced degeneration of nitrergic neurons, specifically loss of NO synthesis, potentially leading to impaired vasodilation & erectile dysfuction
Diabetes & Immunology/Bacterial Pathogenesis
• Etiology of Type I diabetes:– Autoimmune destruction of β-cell
• Infections & diabetes– sensation (neural)– perfusion (vascular)– substrate for bacterial growth– host defense

Version date: 2006FIS Final Exam: Sample Questions
Q: Contrast the etiologies of Type I & Type II diabetes.
(Basis for Answer: Type I- Autoimmune & Type II- Insulin Resistance)
Q: Discuss the mechanisms for the potential pathological changes in a specific organ system, secondary to long-standing hyperglycemia and/or hyperlipidemia of Type II diabetes.
(Basis for Answer: Erectile Dysfunction due to both vascular occlusion (atherosclerosis) & deficient NO release from neurons responsible for vasodilation
Q: Review the pharmacological basis, including mechanism of action, for a prophylaxis and amelioration of this specific organ system disease - or its consequences.
(Basis for Answer: Prophylaxis- insulin sensitizing drugs; Treatment- Viagra, a cyclic GMP phosphodiesterase inhibitor)
















![[XLS]navy-training-transformation2.wikispaces.com · Web view0. 15 15. 85 85. 100 100. 5. 85. 100. 0.3 1 0.35 0.35 1. 85 85 85 85. 85 85 85 85. 85 85 85 85. 85 85 85 85. 85 85 85](https://img.pdfslide.net/doc/110x75/5b3ecf5e7f8b9a5e2c8b55c9/xlsnavy-training-web-view0-15-15-85-85-100-100-5-85-100-03-1-035.jpg)