Embed Size (px)
Citation preview

TEN YEAR PLAN FOR
THE BONG COUNTY
PREPARED IN SUAKOKO, BONG COUNTY
by
MEMBERS OF THE BONG COUNTY HEALTH TEAM:
Dr. Garfee T. Williams, CHOAlphonso W. Kofa, CHDD
Arthur Loryoun, County PharmacistAugustine Nyanplu, M&E Officer
Peter Tiah, Child Survival SupervisorGorma Cole, Reproductive Health Supervisor
Tokpa Wakpolo, TB/HIV SupervisorJoe E. Smith, Health Promotion Focal Person
Fatuma Jusu, Surveillance OfficerStephen B. Cooper, Clinical Supervisor
J. Lis Rowland, MDMRufus S. Domah, RBHS
Sarah Laywah, Save the ChildrenAnthony Yeakpalah, Africare
MOHSW TECHNICAL SUPPORT STAFF:
Dr. Saye Dahn Baawo, Director, Family Health DivisionJustine Korvayan, Director of Planning &Decentralization
DATE: 30 June, 2011

Executive Summary - Bong County Health Plan (2011-2021)
Bong is one of Liberia’s most populous counties with more almost 350,000 inhabitants. Its health infrastructure of 38 health facilities includes 3 hospitals; and 35 clinics. However, only 48% of the population lives within 5km (one hour walk) of a health facility. 23% of deliveries occur in health facilities with skilled assistance. While OPV3/Penta3 vaccination coverage for children under one year averages more than 90%, some districts have coverage of less than 60%.
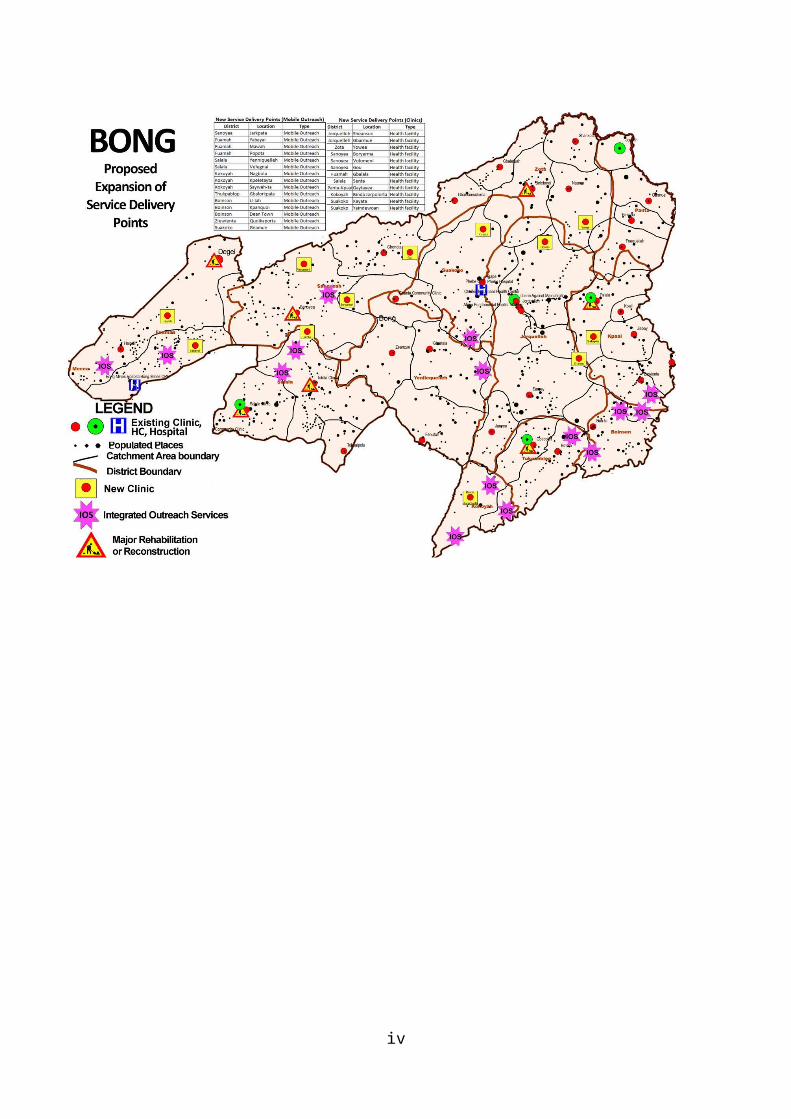
The Bong County Ten (10) Year Health Plan will improve access to the EPHS with the addition of 27 Service Delivery Points, including a combination of clinics, upgrading some clinics to health centers, building new health centers, outreach and community-based strategies (see map). The Plan will also reinforce systemic and community components to support services. Specific objectives, baselines (2010) and targets (2021) will strive to1: Increase the population living within 5 km of a health facility from 48% to 85%; Maintain children under 1 year who receive OBV3/Penta3 at 95% or more; Increase facility-based deliveries with a skilled birth attendant from 23% to 80%; Increase pregnant women provided with 2nd dose of IPT for malaria from 37% to 80%; Increase public facilities with a two star accreditation from 3% to 90%; Maintain timely, accurate and complete HIS reporting at more than 90%; and Increase facilities with no stock-out of tracer drugs to 95%.
1 Baselines and targets will be refined and adjusted as more reliable data become available.
ii

Table of Contents
Executive Summary.....................................................................................................................ii
Table of Contents........................................................................................................................iii
Foreword.....................................................................................................................................iv
Acknowledgements......................................................................................................................v
List of Acronyms........................................................................................................................vi
1. Introduction and Background .....................................................................................................1
2. Summary of Previous County Plan and Its Implementation........................................................5
3. Mission and Vision......................................................................................................................7
4. Service Provision.........................................................................................................................7
4.1 Main Existing Preventive Services.......................................................................................7
4.2 Main Existing Curative Services........................................................................................14
4.3 Main New Services.............................................................................................................23
5. System Components...................................................................................................................27
6. Sector Coordination Issues........................................................................................................31
7. Implementation, Monitoring & Evaluation................................................................................32
8. References..................................................................................................................................33
Figures and Tables:
Figure 1: Existing and Proposed Health Facilities, SDPs and PHC 1s
Figure 2: Organizational Chart Ministry of Internal Affairs
Figure 3: Organogram of Bong County Health and Social Welfare Team
Table 1: Bong County Implementation Plan
Table 2: Bong County Plan Monitoring Framework
ANNEXES
iii
Foreword
The development of a ten-year strategic plan and a two-year operational health plan for the county was a memorable working and learning experience for us! I can assure you that this is not a perfect plan, but it’s a wonderful representation of a realistic attempt by a county to set out its course aligned with the environment in which the system operates.
As we work towards achieving health for all and Universal Coverage in Liberia, our health systems have to be prepared to respond to the felt health needs of various communities in a way that the communities themselves participate in an empowering and meaningful way. This planning process involved a wide range of stakeholders reflecting both upstream and downstream accountability. We believe that the outcome of such an exercise will be the development of an environment where people are informed about the issues in delivering health services, and will also understand the need for ownership and interest in their own health.
The provision of health services across Bong County has been challenging, especially with the implementation of the BPHS based on the principle of equity, when there remains several inaccessible and hard-to-reach areas. The flexibility of this new plan is with the birth of what we call “service delivery points”, or SDPs. This ensures that services can be provided without a ‘clinic building’ as we know it. This new concept now challenges us to identify these under-served communities and develop intervention strategies to address their health needs.
We strongly believe that this plan will galvanize the kind of support that we need to implement EPHS with the expansion of old services, and the addition of new ones. This is our contribution to the National Roadmap for health care in Liberia and we are excited about facing the challenges that may accompany this journey.
Finally, the Bong County Health Team is committed to the underlying principles of the EPHS and will work to ensure a sustainable, equitable, and good quality health care for everyone who access health services in Bong County. The full implementation of the EPHS emphasizes both preventive and curative services at all levels of the Health system in a complementary way throughout the county.
Dr. Garfee T.WilliamsCounty Health & Social Welfare Officer,Bong County Health Team
iv
Acknowledgements
As we continue to mark progress along our journey to full Decentralization, we have made yet another milestone at the county level which is the drafting of two important county-specific documents; a ten-year strategic plan and a two-year operational plan. These documents will feed into the national health agenda and as such we will be held accountable as a county team, working closely together with our environment which includes all stakeholders, donors, and partners, to achieve our plans. We’ve had a lot of support throughout this process and for this we are extremely grateful.
On behalf of the Chairman and members of the Bong County Health & Social Welfare Board, I would like to express our profound thanks and appreciation to everyone who supported us during this exercise. Also to Dr. Saye Dahn Baawo and Mr. Justin Korkoyan, two Technical Assistants from MOH&SW central, for their guidance during the first draft of the plan. To all of the representatives from our partners who contributed to the planning process; Africare Liberia, MDM France, and SC-UK, please accept our thanks. Though there were some instances where full declaration from some partners was missing, we remain determine to pursue the ideals of the Paris Declaration and the Accra Agenda for Action which are international commitments around the issue of Aid effectiveness.
Finally to the Minister of Health & Social Welfare; the CMO, Program Heads, and staff of Health Services Department; the Deputy Minister and staff of the Department of Planning Research & Development; the Departments of Social Welfare and Administration, as well as all of the international consultants who helped to prepare us for these tasks.
v

List of Acronyms
AIDS Acquired Immune Deficiency Syndrome ANC Antenatal CareARV Anti Retro VirusBPHS Basic Package of Health ServicesCHO County Health OfficerCHVs Community Health VolunteersCHWs Community Health WorkersCM Certified MidwifeCHT County Health TeamCHSWT County Health & Social Welfare TeamCHDC County Health Development CommitteeCHSA County Health Service AdministratorCHDD County Health Department DirectorDHO District Health OfficerDHIS District Health Information SystemEHT Environmental Health TechnicianEPHS Essential Package of Health ServicesEPI Expanded Program on ImmunizationEmONC Emergency Obstetric Neonatal CareEPR Emergency Preparedness & ResponseFBO Faith Based OrganizationGoL Government of LiberiaHIV Human Immunodeficiency VirusHMIS Health Management Information SystemHR Human ResourcesHRH Human Resources for HealthIPT Intermittent Preventive TreatmentPRS Poverty Reduction StrategyPSI Population Services InternationalMERCI Medical Emergency & Relief Cooperative InternationalMCH Maternal and Child HealthM&E Monitoring and EvaluationMOE Ministry of EducationMOH Ministry of HealthMoH&SW Ministry of Health and Social WelfareNGO Non-Governmental OrganizationNHP National Health PolicyNCD Non Communicable DiseasePA Physician AssistantPHC Primary Health CarePMTCT Prevention of Mother to Child TransmissionQA Quality Assurance RBHS Rebuilding Basic Health ServicesSTIs Sexually Transmitted InfectionTB TuberculosisTT Tetanus Toxiod TTM Trained Traditional MidwifeUN United NationsUNMIL United Nations Mission in Liberia WHO World Health OrganizationWFP World Food Program
vi

1.0 INTRODUCTION AND BACKGROUND
1.1. Rationale for the Development of the Ten Year Plan
Since the first county health plan was developed in September 2007, a lot of changes have occurred in the health sector of the county. As indicated from the BPHS Assessment, access to BPHS services has increased as evidenced by an accreditation score of around 83%. (BPHS Assessment 2010). This year brings to an end the life span of the five year plan that was developed in 2007 and with the experience and lessons learned over the implementation period, it will serve to inform the county in the development of a new plan.
In 2007, the Bong County Health Team developed a five-year health plan which was generic and did not include any social welfare component. During the development of that plan, there were many shortcomings with limited or lack of information and data. These included the lack of health and demographic data, information on access to services, information on catchment population for health facilities and information on disease epidemiology and its burden. The county also set unrealistic targets which could not be achieved given the available resources and timeframe. The development and subsequent implementation of the Basic Package of Health Services in the county was based on the assumption that people will use them, coupled with inadequate funding for the plan which presented a lot of challenges.
Following four years of implementation, we have learned a lot of lessons and implementation experience. In addition, there are now data (health, demographics, HR, HF) to inform proper planning, to ensure the development of an evidence-based plan. Besides, the County situation has changed over the years with new partners in the health and non-health sectors. As the health system is being decentralized, the CHSWT will have increased responsibility to oversee the planning, management, implementation, monitoring and evaluation of health and social welfare services in the County. The MOHSW is also developing a ten year plan in which the CHSWT needs to fit in.
Based on the above and in order to contribute to the achievement of the overall national health targets set by the MOHSW in its Ten Year Health & Social Welfare Plan, it is expedient for the County Health & Social Welfare Team to properly plan if it is to succeed. A long term plan will assist the CHSWT develop annual operational plans which can be monitored and evaluated to assist the county to re-strategize and improve service delivery to the people of this county. Moreover, in the wake of limited resources, a plan of this nature will inform all stakeholders to mobilize additional resources to support the implementation of the plan over time. This plan will be informed by the following guiding principles: equity, efficiency, sustainability, accountability and transparency and the overall issue of health as a universal human right for the people of Bong County. This plan is also important to consider the new changes that have been made by the MOHSW in the area of service delivery with the development of an Essential Package of Health & Social Services with new services added to augment the current Basic Package of Health Services.
1.2. Bong County Geo-Demographic Information
Bong County, located in central Liberia, was created on July 26, 1964, as one of two counties formed out of the then Central Province. According to the latest census report by LISGIS the current population for the county is 328,919. Bong County is bounded in the northeast by Nimba, the southeast by Grand Bassa , the south by Margibi and the northwest by Lofa. The county also shares international border with the Republic of Guinea in the north. The St. Paul
- 1 -

River is on the southwest of Bong County and forms a boundary between Bong, Bomi & Gbarpolu counties while the St. John River forms the border between the county and Nimba.
Bong County is subdivided into 12 political districts and 2 townships. The districts are: Biosen, Fuamah, Jorquelleh, Kokoyah, Kpaii, Panta, Salala, Sanoyea, Suakoko, Tukpablee, Yellequelleh and Zota. Four of the districts (Boisen, Kpaii, Tukpablee, and Yellequelleh) are new districts created by legislative enactment in October 2003. There are two townships in the county, namely Boisville in Zota district and Yoloville in Boinsien district.
Figure 1: Existing and Proposed Health Facilities, SDPs and PHC 1s
There are Five major tribal groups in Bong County, namely: Kpelleh, Bassa, Mano, Lorma and Mandingo. Other tribal groups from around the country also reside in the county. Gbarnga is the capital and administrative seat of Bong County and has a population of 34,046.
Since 2005, the county has become a host of a number companies and institutions among which include, Central Agriculture Research Institute (CARI), Lee Group of Companies (rubber processing), AmLib (mineral exploration), BHP Billiton (mineral exploration), China Union (mineral exploration), GSM Companies (Lone Star, Cellcom, Comium, Libercell), and Kokoyah Millennium Village Project (KMVP).
Cuttington University (CU) and Gbarnga School of Theology (GST), are two higher learning institutions that are located in the county. Two other mid-level health training institutions also exist, namely Phebe School of Nursing and the African Fundamental Baptist Physician Assistant Training Program.
- 2 -

These companies and institutions serve as attraction for employment for many Liberians and foreign workers. The railroad track connecting Nimba with the seaport of Buchanan passes through Bong County. There are few banking institutions among which include Ecobank Liberia, LBDI and the Central Bank of Liberia. In addition to employment offered by these companies and institutions, the majority of the population are involved in the informal sector through cash crop production (rubber, palm, sugarcane, cocoa, coffee, peanuts, rice, cassava, etc) and small businesses (shops, petty trading, transportation, etc).
The county population is not evenly distributed. For example; Joequelleh district with a population of 79,000 is the most populous district, while Kokoyah district with a population of 3,702 is the least populous district. However, the sex ratio is almost 1:1 in distribution across all districts in the county. Based on estimates made from county population and HMIS data, about 34% of the population is above 15years of age with the age range of 15-39 years accounting for the bulk of the number. While the age range of 6-14 years constitute 45% of the total population. Majority of the residents in the county are employed in the informal sector; for example farming, petty trade, other small businesses, etc.
Within the various districts of the county there is a population density towards the urban areas. This urbanization can be attributed to the search for employment and academic advancement. Because of the poor income-generating power of the majority of the population there is a lower capacity of residents to purchase health care in the rural areas. On the other hand, in the urban settings there is some level of economic power and hence the utilization of services such as private-for-profit services and informal care-givers.
1.3 Administrative Structure of Bong County
The Superintendent of Bong County is the administrative head of the county and represents the Office of the President of Liberia in the county. The superintendent is assisted by an Assistant Superintendent for Development, who is responsible for coordination of development activities in the county, including the formulation of the county development agenda. There is a Superintendent Council of more than 50 members which draws its membership from local authorities, prominent citizens, and traditional leaders and is headed by the Superintendent and serves as an advisory body to the office of the superintendent. The County Steering Committee is the superintendent’s ministerial council and consists of heads of the various lines ministries.
Figure 2: Organizational Chart Ministry of Internal Affairs
- 3 -

1.4. The County Health and Social Welfare System
The Ministry of Health and Social Welfare is represented in the county by the County Health and Social Welfare Team which is the implementing arm for all health and social welfare services under the decentralization process. The role of the CHSWT is to provide leadership, to manage and improve the delivery of health services in the county, ensure effective system coordination, ensure access at all levels of services, reduce morbidity and mortality, improve coverage of health interventions, supervise and to support regulatory activities of the various Boards.
The CHSWT is headed by the County Health Officer who has oversight responsibility for the daily operation in the health and social welfare sector of the county.
Figure 3: Organogram of Bong County Health and Social Welfare Team
There exists a County Health and Social Welfare Board which is an advisory arm of the County Health and Social Welfare Team and is headed by the superintendent with the County Health Officer as its secretary. The composition of the board includes member from the following line ministries; Gender & Development, Public Work, Agriculture, Youth & Sports and Education. It also includes the county pharmacist, representatives of local drugstores owners, traditional leaders, the marketing association, all GSM companies, Cuttington University and all of the county’s international and local health partners.
There are two levels of service delivery, primary and secondary. At the primary level services are provided at the community and clinics while at the secondary levels services are provided in the hospitals. There are 38 clinics (3 private-for-profit, 1 private not for profit and 34 public) and 3 hospitals in the county. There are eight (8) health districts managed by eight District Health Officers (DHOs). Services are also provided through Community Health Volunteers which include gCHVs and TTMs. Community Health and Development Committees and Community Health Committees serve to oversee health delivery at the community level. Two facilities were not accredited because they were not providing the full BPHS; Joequelleh and Agape clinics.
- 4 -

1.5. The Bong County Planning Process
The Bong County planning process was initiated in 2010 at the central MOH&SW. it has four stages and steps;
Stage 1: Preparation; A roadmap workshop was conducted to map the policy and plan development process in September 2010, development of health sector situation analysis report in October 2010 and the adoption and launching of the roadmap by the president of Liberia in November 2010 at the Monrovia City Hall.
Stage 2: Policy Revision; The first draft of the revised National Health Policy was circulated in January 2011 to all partners. This was followed by county consultation process on the draft policy in February 2011 during which the Bong County Health & Social Welfare Team and other stakeholders set priorities for their county health plan. The county M&E Officer participated in the workshop in February 2011 at central MOH&SW to prepare for the county level consultation.
Stage 3: Plan Development; The CHSWT technical working group, with support from two central MOHSW staff worked for five days from April 11-15, 2011 to incorporate the ideas generated from the county consultation with stakeholders into the county first draft plan. Prior to this work, the CHSWT was sent data collection tools in February 2011 to be completed for the county plan development. The CHO also participated in the capacity building workshop on the data collection tools in March 2011.
Stage 4: Finalization; to follow after this process
2.0. SUMMARY OF PREVIOUS PLAN AND ITS IMPLEMENTATION
The Bong County Health & Social Welfare Team developed a five year county plan that was published in September 2007. The components of the plan were as follow:
Introduction and Background; County Health Planning Process; Situation and Gap analysis; County Health Facility Plan; Supervision, Monitoring & Evaluation; Implementation Challenges and solutions; and Annexes.
2.1. The County Health Facility and Service Delivery Plans
The county health facility and service delivery plan included: Construction of five new clinics and upgrading of five clinics to health center status; Minor rehabilitation of 14 clinics and major rehabilitation of seven clinics; Implementation of BPHS in 14 of its 33 functional health facilities; Recruitment of 1 medical doctor for the county hospital, 3 physician assistants, 18
CMs, 1 laboratory technician, and 2 environmental health technicians; and In-service training for all staff in the BPHS clinics.
- 5 -

2.2. Supervision, Monitoring & Evaluation Plan Develop one year M&E plan and establish HMIS/M&E Unit Develop standardized checklist for supervision and reporting form Strengthen CHWs to collect data at community level using standardized reporting
forms Conduct regular monitoring at all levels on a quarterly basis Bi-annual review of implementation activities to evaluate progress of program
activities Establish human resource unit at the county level Conduct bi-monthly supervision visit with partners
2.3. Implementation Progress
The Bong County Health plan, developed in September 2007 was based on a blueprint developed at the Central MOHSW and many targets were set with no evidence-based data or report. The plan set targets some of which were not realistic or achievable within the timeframe. For example, the following targets were set to be accomplished:
Increase ITN coverage from 0 to 80%; Increase IPT coverage from 0 to 75% for pregnant women; Increase access to EmONC services from 15 to 80%; Increase from 10 to 100% of staff to receive in-service training; Increase from 0 to 80% the number of CHVs to implement multi-purpose BPHS
activities; and Increase supervision from 48 to 100% at all health facilities.
Of the activities planned to be implemented the following were accomplished: Construction of three clinics (Kelebe, Yolota, Rockcrusher); None of the five planned upgrades to health center were achieved; Nine health facilities underwent minor rehabilitation; Three health facilities underwent major rehabilitation (CB Dunbar, Gbonota, and
Gbarnla); Recruitment of 1 MD, 4 PAs, 35 CMs, and 2 Laboratory technicians; BPHS was implemented in all health facilities with a 2010 accreditation score of
83%; In-service training was conducted for service providers in BLSS, FP, EPI, IMNCI,
Malaria, BPHS integrated curriculum, Nutrition, HR, and ENA; M&E unit was established at the county by central MOHSW; A total of 308 CHW (gCHVs) were recruited and trained. Bi-annual review of program activities implementation was not accomplished; A Human Resource office was established at the county level; and Conducted bi-monthly supervision visit with partners.
Some of the activities accomplished during the period of implementation were not included in the original plan. For example in Zeansue and Totota clinics, minor rehabilitation was planned to be carried out but major rehabilitation was done, while others were politically
- 6 -

motivated for example, one clinic was constructed in Boway and another constructed and opened in Kpaii. The delivery room in Bah-ta and the MCH wing of Foequelleh were also expanded and a MCH unit with a cold chain room was added to the Palala Clinic. At CB Dunbar and Gbonota, where major rehabilitation were planned to be carried out, construction of two new facilities were done.
2.4. Challenges and lessons learned Untimely budgetary allocation Political influence Bad road conditions Awarding of contract was done without the input of the CHSWT Staff turnover The plan was not evidence based Low community participation Strong influence from central MOH Slow decentralization process Less capacity at the county level in some areas Poor information sharing from central to county level
3.0. MISSION AND VISION Mission: To reform and manage the Bong County Health and Social Welfare sector to effectively and efficiently deliver comprehensive, quality health and social welfare services that are equitable, accessible, and sustainable for all residents of Bong County
Vision: A healthy population of Bong County with social protection for all its residents
4.0 SERVICE PROVISION
4.1 MAIN EXISTING PREVENTIVE SERVICES
A. CHILD HEALTHExpanded Program on Immunization Situation Analysis
1) 34 out of 38 health facilities are providing routine EPI servces2) Penta coverage of 75% (Bong County Excel Analysis 2010)3) Coverage for most vaccines are good – BCG 98%, Measles 86%, YF 86% and TT2
93% (MOHSW Annual Report 2010)4) Penta 3 coverage varies among health facilities in various districts. For example,
Gbalatuah and Belefani in Zota District have a coverage of 100% while in Sanoyea in Sonoyea District has 31% and Haindii in Fuamah has a coverage of 49%. This could be due to poor outreach, poor awareness from health workers to the mothers or caregivers, poor access to HFs and bad road conditions. Sanoyea has the worst coverage of penta 3. (BCHT Excel Analysis 2010)
5) Incorrect reporting from HF to CHT6) Some of the refrigerators in the health facilities are non-functioning (damaged
refrigerators, etc)
- 7 -

7) Outreach is being done once a week in most health facilities but not in a few.8) Logistics are available for outreach9) A central EPI depot at Phebe Hospital that supply all health facilities in the county
Target:Increase Penta3 and other vaccines coverage to at least 85% by 2021
Strategies1) To strengthen regular weekly outreach services in all catchment areas of existing
facilities2) To increase the number of vaccinators in HFs based on workload3) To improve logistics and other supplies for EPI services4) To strengthen supervision and surveillance at the HF and community level5) To intensify routine immunization services6) To improve vaccine storage at all levels7) To improve capacity building for service providers8) To improve IEC/BCC on EPI at the community level through community structures
Nutrition
Situation Analysis1) Prevalence of stunting 36% (CFSNS 2010 Report for Bong County)2) Prevalence of moderate acute malnutrition (MAM) 3.4% and severe acute
malnutrition (SAM) 0% (CFSNS 2010 Report for Bong County)3) Rate of exclusive breastfeeding 64.4% (CFSNS 2010 Report Bong County)4) Some components of growth monitoring are being carried out in 12 health facilities5) Four health professionals were trained as facilitators or trainers in ENA6) A total of 28 CMs and 240 gCHVs have been trained on ENA 7) Vitamin A is included in routine immunization and has a coverage of 72%. (BCHT
Report 2010)8) De-worming and Vitamin A supplementation are implemented bi-annually as part of
national EPI campaign9) Vitamin A is also provided to children under five during OPD consultations at some
HFs
GoalTo reduce the prevalence of stunting and acute malnutrition
Targets 90% of children 6-59 months of age receive Vitamin A supplementation 90% of children 12-59 months of age are de-wormed 80% of severely malnourished children are identified and referred 90% of infants <6 months are exclusively breastfed 80% of infants 6-12 months receive appropriate complementary feeding
- 8 -

Strategies1) To continue Vitamin A supplementation and de-worming activities in routine EPI
services, consultations and national campaigns2) To conduct IEC/BCC at the health facility and community level on ENA and IYCF 3) To build the capacity of service providers to conduct Growth Monitoring, Essential
Nutrition Actions (ENA) and Infant and Young Child Feeding (IYCF)4) To build the capacity of community health volunteers in growth monitoring and
nutrition education at the community level for timely referral5) To develop and strengthen additional community structures (household health
promoter) to improve information dissemination6) To integrate CMAM into all health facilities in the county and establish OTP and SFP
sites at 2 health facilities in each district7) To integrate CMAM into all health facilities and catchment communities in the
county
B. REPRODUCTIVE HEALTHFamily Planning
Situation Analysis1) Family Planning services are provided in the all majority health facilities2) All methods are not available in facilities and there are occasional stock-outs of FP
commodities especially implant and Depo because of stock out at the national level.3) Low FP uptake among women with children under 24 months – 20%. (CHT KPC -
2010) and adolescent. However, the survey did not capture reason for this, but our assumption is that women who have children at this age culturally believe that risk of preganacy is negligable. Also they delay having sexual intercourse until the child is above 24 months .
4) 18 CMs and OICs(6) from 8 HFs have been trained on implant 5) Those trained in the procedure of IUCD and implant insertion are not confident in
providing the services at their HFs because they need further supervision on the first occasion of insertion.
6) Capacity building has been provided in some areas of Family Planning for some service providers
7) Methods like IUD and implants are not used because of insufficient trained staff knowledgeable in the procedures
8) % of health facilities with at least 3 modern method of contraception at the time of survey – 85% (National EmONC NA Fact Sheet 2010)
9) CPR for the country is 11% and unmet need is 36% (LDHS 2007)10) The teenage pregnancy rate for the country is 32% (LMIS 2009)
GoalTo reduce maternal mortality from 994/100,000 to 497/100,000 by 2021
Targets By 2021, at least 80% of service providers are trained in family planning and youth
friendly services at all health facilities 70% of communities are provided family planning services through community-based
distribution
- 9 -

100% of health facilities have the 5 essential family planning commodities at any point in time
A stock out rate of <1% in all health facilities for all FP commodities Reduce teenage pregnancy rate from 32% to 25%
Strategies1) To integrate FP services into EPI and OPD consultations or services at the HF2) To conduct operational research on the uptake of different methods for clients to
inform service delivery3) To increase male involvement in the FP services4) To increase utilization of family planning services5) To improve the quality of and access to family planning services6) To build the capacity of service providers in all methods of family planning 7) To intensify IEC/BCC on family planning at the health facility and community levels8) To implement community-based distribution of family planning 9) To implement youth friendly services at all health facilities in the county10) To collaborate with youth centers and other partners to provide outreach services and
peer education on family planning for youth and young adults11) To integrate family planning education and counseling services in EPI outreach
activities and other consultations at the health facilities12) To improve and strengthen logistics for the delivery of FP services (commodities and
other supplies) in the county
Antenatal Care
Situational Analysis1) Antenatal care is provided in all health facilities, however, all the services are not
provided at all facilities2) Coverage for first ANC visit is 91%, while coverage for 4 th ANC is 71% (MOHSW
Annual Report 2010)3) First ANC visit is 56% and varies among health facilities in the county. For example,
Haindii Clinic in Fuamah District has 26% coverage with Fuamah District having a total of 36% while Panta/Kpaai District has an average ANC coverage of 73% with Yila and Garmue clinics having coverage of 100%. While first ANC visit is certainly always good, data shows that coverage for 4th ANC visit has always been low (26%). Many reasons can be attributed to the low coverage for ANC visits among which include poor geographic access, staff attitude, delay at the HFs, lack of awareness on importance of ANC and lack of incentives at the HFs for pregnant women (BCHT Excel Analysis 2010)
4) TT2+ coverage for pregnant women for Bong County is 25% (BCHT Report 2010)5) ITN distribution to pregnant women in the county was 4,200 in 2010 with a coverage
of 25% (CHT Report 2010)6) Percentage of facilities with TT vaccine at time of survey – 100% (EmONC NA
Factsheet 2011)7) 14 health facilities are implementing PMTCT and all service providers in these
facilities have been trained on PMTCT
- 10 -

8) Drugs for PMTCT are available but there are frequent stock-outs of test kits
Goal: To reduce maternal morbidity and mortality in the county Targets
80% of pregnant women attending ANC are fully examined and tested for HIV, syphilis and urine protein
70% of pregnant women attend 4th ANC visit 90% of ANC service provision sites provide PMTCT services Increase TT2 coverage to 80% Increase IPT2 coverage to 80% Increase ITN coverage among pregnant women to 80% 60% of HIV infected pregnant women who go through PMTCT are placed on ARV
Strategies1) To conduct outreach activities to communities to reach every pregnant woman2) To implement the “Reaching Every Pregnant Woman” strategy3) To build the capacity service providers on focused antenatal care and nutrition
counseling and integrate it with other essential services (FP)4) To ensure the availability of logistics for the delivery of ANC services (vaccines,
drugs, ITN, test kits, space, etc.)5) To conduct IEC/BCC at health facility and community levels on importance of ANC6) To strengthen regular monthly supervision and monitoring at all HFs7) To strengthen PMTCT services and follow-up for those found to be sero-positive8) To strengthen collaboration with TTMs to refer and accompany pregnant women to
complete their ANC visits9) To work through community structures (CHDCS, CHCs, CBOs, etc) and males to
improve service delivery and coverage of interventions
COMMUNICABLE DISEASE CONTROLMalaria
Situation Analysis1. ITN distribution took place in 2008 throughout the county in November2. Indoor Residual Spraying (IRS) is ongoing in 2 districts (Kokoya and Pantakpai) 3. Some awareness has been carried out in the county on the use of ITNs.4. IEC/BCC is being carried out at the health facility and community levels
GoalReduce the prevalence of malaria
Targets 100% of districts received IRS 100% gCHVs trained in health promotion activities on IRS& ITN Increase ITNs distribution to about 50% 100% Stock out prevention at all levels in the county
- 11 -
Strategies1. To continue IRS in the remaining districts2. To carry out extensive IEC/BCC in the communities on the importance of ITN and
IRS for the prevention of malaria3. To collaborate with other stakeholders on the war against malaria4. To continue ITN distribution to pregnant women and children under five at all health
facilities5. To ensure the availability of logistics and malaria products at all facilities
STIs and HIV/AIDS
Situation Analysis1. IEC/BCC is being carried out at all health facilities and communities and on the
county radio stations2. Condom distribution is being carried out at the health facility and community levels 3. There are no condom access points placed in health facilities or communities 4. The Lutheran Church in Liberia has fixed and mobile testing and counseling services
in the county5. There is one ART center at the county hospital6. Post-exposure Prophylaxis (PEP) is available at the county hospital and 10 MDM-
supported clinics
GoalTo reduce the incidence of STIs and HIV in the county
Strategies1. To strengthen IEC/BCC on how STIs and HIV are acquired and prevented2. To build the capacity of gCHVs on STI and HIV prevention 3. To involve communities in health promotion activities4. To improve access to HCT and PMTCT services5. To improve the availability of logistics for HIV and STI preventive services in all
health facilities and communities
Tuberculosis
Situation Analysis1) There is poor reporting on the disease in the county due to vertical operation of the
program2) There is limited capacity for the detection of sputum positive cases 3) There is poor follow-up and therefore increase drop out rate4) IEC/BCC is carried out on TB prevention at all health facilities5) There are four TB focal staff on CHSWT
Goal
To reduce the incidence of TB in the county
Targets
- 12 -

100% gCHVs trained in the module on TB prevention 85% of case detection at all Health facilities and communities level 85% cure rate at all health facilities and Communities level 100% of all health facilities should integrate TB services into PHC activities
Strategies
1) To strengthen IEC/BCC on how TB is acquired and prevented2) To build the capacity of gCHVs on TB prevention 3) To strengthen community participation in health promotion activities4) To improve the availability of logistics for TB preventive services in all health
facilities5) To improve case detection of TB at the health facility and community level6) To strengthen integration of TB services into other preventive services at the health
facility and community levels
Other Diseases with Epidemic Potential
Situation Analysis1) Active disease surveillance is in place for recommended diseases with epidemic
potential (lassa, polio, measles, rabies, etc)2) A total of 20 Lassa fever cases were reported in the county in 2010 with 5 deaths
(BCHT Report 2010)3) A Wild Polio Virus case was detected and confirmed from Charlie Town in Kokoya
District in March 20104) There were outbreaks of measles in three districts in 2010 and complications treated
at health facilities5) Three mini-campaigns for measles were implemented in the affected districts6) There were three deaths reported for rabies 7) There was an outbreak of whooping cough in two districts (Kokoya and Suakoko)8) A total of 129 cases of acute watery diarrhea without any death9) Five cases of neonatal tetanus without death
GoalTo reduce the prevalence/incidence of diseases with epidemic potential
TargetsTo ensure coverage for all vaccines to at least 80%
Strategies1) To strengthen disease surveillance2) Ensure timely reporting and regular supervision in all HFs and catchment
communities3) To strengthen outreach activities for immunization services4) To strengthen collaboration with partners to ensure immunization of pets in the
county5) To ensure the availability of logistics for control and management of diseases with
epidemic potential
- 13 -

6) To conduct IEC/BCC at the HFs and community levels on prevention and clinical manifestations of notifiable diseases
4.2 MAIN EXISTING CURATIVE SERVICES
Reproductive Health
Antenatal
Situation Analysis1) Antenatal care is provided at all health facilities, however some services are not
provided2) Coverage for first ANC visit is 56% for Bong County (Excel Spreadsheet Report
2010) 3) There is occasional stock out of drugs in most health facilities for malaria case
management in pregnancy 4) Syphilis testing and treatment are not routinely done in most health facilities5) Urine protein test is not done in the majority of health facilities6) Ferrous sulfate, folic acid and mebendazole are provided to pregnant women at most
HFs7) Magnesium sulfate is available at all most health facilities8) % of facilities with folic acid (65%) and ferrous supplement (74%) – (EmONC NA
Factsheet 2010)9) % of facilities with functional BP cuffs – 96% (EmONC NA Factsheet 2010)10) % of HFs with anticonvulsant at the time of survey – 63% (EmONC NA Factsheet
2010)11) % of HFs with folic acid at the time of survey – 96% (EmONC NA Factsheet 2010)12) % of facilities with rapid HIV test kits at the time of survey – 73% (EmONC NA
Factsheet 2010)
GoalTo reduce maternal morbidity and mortality in the county
Strategies1) To strengthen focused antenatal care2) To build the capacity of service providers on focused ANC services3) To improve the availability of logistics for curative maternal health services4) To build the capacity of TTMs and gCHVs in the recognition of danger signs of
pregnancy for prompt referral and treatment5) To strengthen feedback system from the health facility to the community level to
ensure completion of treatment for specific conditions in pregnancy
Labor & Delivery Care
Situation Analysis1) Thirty four (34) health facilities provide labor and delivery services2) All of these facilities have skilled birth attendants (CMs)
- 14 -

3) Fifty eight percent (58%) of deliveries take place under the care of skilled birth attendants (MOHSW Annual Report 2010)
4) Currently distribute baby kits in 22 health facilities on an irregular basis to improve institutional delivery
5) Majority of deliveries occur within the community under unskilled birth attendants and is done by TTMs in some health facilities
6) Referral of some pregnant women from the community to the health facility7) Percentage of health facilities with blank partograph was recently assessed at 89%
((EmONC NA Factsheet 2010)). Partograph is poorly use to monitor the progress of labor
8) Percentage of health facilities with availability of oxytocin was recently assessed at 100% (EmONC NA Factsheet 2010 Report)
9) Percentage of facilities with complete delivery set at time of survey – 93% (EmONC NA Factsheet 2010)
10) % of facilities with delivery tables with stirrups – 78% (EmONC NA Factsheet 2010)11) Percentage of facilities with midwives – 100% (EmONC NA Factsheet 2010)12) Monthly average number of deliveries per midwife among all facilities – 91 (EmONC
NA Factsheet 2010)13) Percentage of facilities with ARVs for mothers was 21% and newborns – 25% at the
time of survey (EmONC NA Factsheet 2010)14) Institutional delivery is low in the county with a coverage of 36% and variations
among the districts with the highest in Suakoko 66% and the lowest in Kokoyah District with 19%. The ANC 1st visit in Suakoko and Kokoyah districts are 60% and 53% respectively. This low coverage of institutional delivery can be alluded to the following: Health workers attitude, trust in the TTMs, refusal of TTMs to bring the patients to the HF for fear not receiving their compensation from the community, poor geographic access and occasional absence of skilled attendants at few HFs, etc. (Excel Spreadsheet Analysis 2010)
GoalTo reduce maternal and newborn mortality
Targets 80% of all deliveries attended by skilled birth attendant 100% of facilities with flexible staffing based on workload 100% of facilities with solar-powered base radios (vhf) 100% of facilities receive one joint supervisory visit every quarter 100% of our TTMs received incentives(Non- cash) for referring pregnant women to
the Health facilities. 100% of facilities with ARVs for mothers and newborns who require them
Strategies1) To increase institutional delivery under skilled attendants by providing innovative
methods of motivation for all staff2) To increase the number of skilled birth attendants at health facilities depending on
workload3) To strengthen and improve supplies and logistics for labor and delivery services
(drugs, supplies, equipment, lighting, communication for referral, monitoring forms)
- 15 -

4) To improve referral systems at all levels by providing vhf radios and supporting counter referrals
5) To strengthen regular supportive supervision at all levels6) To improve capacity building for service providers through in-service training,
workshops, and CPDs (continuous professional development)7) To provide IEC/BCC for communities on the importance of facility delivery8) To improve access to delivery services through effective, efficient and responsive
ambulance service 9) To improve infrastructures for labor and delivery services through the construction of
additional waiting homes 10) To strengthen the motivation for mothers who deliver within health facilities through
the provision of delivery kits, and other items 11) To provide motivation package for TTMs who refer pregnant women to health facility
for delivery
Emergency Obstetric & Newborn Care (EmONC)
Situation Analysis1) Two hospitals are providing Comprehensive EmONC in the county for the network of
primary health facilities while 34 clinics provide some components of BEmONC (BPHS Assessment 2009)
2) EmONC Needs Assessment has been completed in the county in sampled facilities and the findings are: ((EmONC NA Factsheet 2010))
3) % of facilities that performed removal of retained placenta in the last 3 months –22 %4) % of facilities that performed instrumental delivery with vacuum extractor in the last
3 months – 7%5) % of facilities that performed neonatal resuscitation in the last 3 months – 67%6) % of facilities that provided oxytocin in the last 3 months –100%7) % of facilities that provided parenteral anticonvulsants in the last 3 months – 63%8) % of facilities that provided parenteral antibiotics in the last 3 months – 100%9) % of facilities that performed C/section in the last 3 months – 4%10) % of facilities that performed blood transfusion in the last 3 months – 7%11) Met need for EmONC –64 %Direct obstetric case fatality rate among facilities that
treated direct complications – 4.2%12) % of facilities with functional MVA at the time of survey – 12%13) % of health facilities that provided Post abortion care services – 25%14) Maternal deaths is being reported on a weekly basis to Central MOHSW since August
201015) Obstetric fistula awareness has taken place in most communities and many cases have
been repaired by surgical outreach team that occasionally visits the Phebe Hospital16) Three functional ambulances are available at the hospital for 24/7 operation in the
county17) % of facilities with cell phone service – 100%18) There are 15 functional VHF radios in the county and two desk phones at 2 CEmONC
hospitals
- 16 -

19) There are five medical doctors (4 in Phebe and 1 in CB Dunbar) and 5 anesthetists ( 4 in Phebe and 1 in CB Dunbar)
20) There are 4 baby crib and 1 functional incubator at the Phebe Hospital with a separate neonatal room while at the CB Dunbar Hospital there is one neonatal room.
21) Some emergency obstetric cases brought to the hospital come in very late and in critical condition
22) All skilled birth attendants at the Phebe hospital are trained in the use of vacuum extractor and MVA
23) Awareness has been conducted in county on the scope of maternal deaths Goal:
To reduce maternal and newborn morbidity and mortality
Targets 100% of primary health facilities provide BEmONC services 2 motorcycle ambulances placed in each of the 8 districts Five additional ambulances to augment the existing ones The 3rd hospital is upgraded to provide CEmONC
Strategies:1) To ensure and improve the delivery of the full package of both basic and
comprehensive EmONC at the existing hospitals and clinics2) To provide and improve logistics, supplies, equipment, and drugs for the delivery of
EmONC services3) To build the capacity of service providers in the provision of EmONC services and
obstetric fistula repair4) To transform some health facilities to provide BEmONC and CEmONC services 5) To carryout IEC/BCC at the health facility and community level on complications of
pregnancy and the scope of maternal mortality in the county6) To improve reporting on maternal deaths from the health facility and community
levels and provide feedback7) To collaborate with traditional birth attendants to ensure facility-based delivery
Postpartum Care
Situation Analysis: 1) Postpartum visits by mothers to health facilities is estimated at less 30% 2) Midwives perform less post-partum checks for mothers who bring their newborns for
immunization 3) Postpartum hemorrhage is the commonest cause of maternal death in the county
(Maternal Death Weekly Report MOHSW 2010-2011)4) Percentage of facilities that provide PNC is 93% (EmONC NA Factsheet 2010)
Goal: To reduce maternal mortality Targets
75% of postpartum women make at least 3 postpartum visits
- 17 -

Strategies:1) To build the capacity of service providers on the active management of third stage of
labor and other care in the management of PPH2) To improve blood transfusion services in all CEmONC facilities3) To create awareness on voluntary donation of blood4) To carry IEC/BCC at HF and community levels on the importance of post-partum
visits for all mothers following delivery5) To strengthen and improve logistics and other supplies for the delivery of post-partum
care services at all health facilities6) To conduct operational research on the use of misoprostol (cycotec) in the
management of PPH7) To continue active surveillance on maternal and newborn deaths and provide
feedback to communities
Child Health: Integrated Management of Neonatal & Childhood Illness (IMNCI) Situation Analysis:
1) Malaria, pneumonia, malnutrition, anemia and diarrhea remain the major causes of morbidity and mortality in children under five in the county (MOHSW 2010 Report)
2) 46% of deaths in under five is caused by malaria (MOHSW 2010 Report)3) 19 HF have IMNCI-trained staff and are currently implementing the strategy4) Community case management is being implemented in 6 districts. Management of
ARI, diarrhea and pneumonia in 4 districts (Suakoko, Kokoyah, Sanoyea and Jorquelleh) and diarrhea management in 4 districts (Zota, Phantakpai, Kokoya and Jorquelleh)
5) Drugs and other logistics for the provision of IMNCI services are available, but there are occasional stock outs
6) Some health workers trained on IMNCI are not fully utilizing the IMNCI approach to manage children under five
Goal:
To reduce under five morbidity and mortality Target:
100% of primary health facilities implement IMNCI Strategies:
1) To build the capacity of service providers in IMNCI case management2) To build the capacity of gCHVs to provide community IMNCI case management in
hard-to-reach communities3) To improve the quality of care for the management of children under five through the
provision of supplies, drugs, equipment and other logistics 4) To strengthen supportive supervision at all levels5) To carry out IEC/BCC in communities on the importance of timely referral of
children with danger signs6) To integrate CMAM into IMNCI services
Nutrition
- 18 -
Situation Analysis:1) There is a separate ward at the Phebe Hospital for the in-patient management of
severe malnutrition (Specialized Nutrition Unit – SNU)2) Supplies for appropriate management of SAM are available but with occasional stock
outs 3) The staff on the malnutrition ward have been trained in management of SAM 4) There were 6 Supplementary Feeding Program (SFP) in the county supported by WFP
but are presently non functional
Goal:To reduce under five morbidity and mortality
Strategies:1) To improve the infrastructure, logistics, supplies, and equipment for the delivery of
SAM management (SNU) at the hospital2) To build the capacity of additional staff on SAM management 3) To integrate CMAM into all health facilities in the county 4) To establish SFP and OTP sites at 2 health facilities in each districts 5) To conduct IEC/BCC on the features of severe malnutrition at the health facility and
community levels for timely referral
COMMUNICABLE DISEASE CONTROL
Malaria:
Situation Analysis:1) Clinical case management is being provided at all health facilities2) All service providers have been trained in malaria case management and the protocols
are available at these facilities3) Occasional stock outs of malaria drugs especially quinine and diagnostic kits (RDT)4) Microscopic diagnostic services are available at 2 hospitals and one clinics while
RDT kits are available at all health facilities5) Malaria is the major cause of morbidity and mortality in children under five
Goal:To reduce the prevalence of malaria in the county
Target:Establish microscopic services at 15 health facilities with 2 in each district
Strategies:1) To strengthen regular monthly supportive supervision in order to prevent stock outs of
essential drugs and supplies2) To build the capacity of service providers in laboratory services3) To improve and strengthen existing infrastructures, logistics, drugs and supplies for
the management of malaria
STI and HIV/AIDS
- 19 -
Situation Analysis:1) There is one Care and Treatment center for HIV/AIDS in one district ( Phebe Hospital
in Suakoko District)2) STIs service is available in all health facilities and service providers at these facilities
have been trained on STI management3) HCT service is being provided at12 out of 38health facilities4) % of facilities with ARVs for mothers at the time of delivery – 78% (EmONC NA
Factsheet 2010)5) ARV drugs are available at the Phebe hospital for treatment but with occasional stock
outs of ARVs and other HIV supplies6) 13 service providers have been trained in HIV care and treatment7) A total 68 clients were under care and treatment with 34 of them on ART as of
December 20108) Nutritional support is provided for PLWA from NACP
Goal:1. To reduce the incidence of HIV infection2. To ensure care and treatment for those already infected
Target:Establish two additional care and treatment centers at the two hospitals
Strategies:1. To build the capacity of additional service providers in care/treatment of HIV 2. To improve nutritional support to those under care and treatment3. To strengthen defaulter tracing for those under care and treatment4. To improve infrastructures, logistics, supplies and drugs for STI and HIV care and
treatment program 5. To conduct IEC/BCC on the features of STI at the HF and community levels to
improve outcomes for treatment6. Same as for the previous; trying to separate curative from preventive with
focused/specific interventions/strategies. Tuberculosis
Situation Analysis:1. Six health facilities are currently implementing both TB microscopic diagnosis
and treatment while 6 facilities have microscope with inadequately trained staff who are not providing the service
2. Some HFs are providing only treatment for patients referred for microscopic diagnosis (total of 21 HF are implementing TB service)
3. There are reagents and drugs available at these health facilities with occasional stock outs
4. A total of 25 service providers have been trained on TB case diagnosis and management
5. TB detection rate is 42% (below target) and caseload is 164 patients6. Community DOTS program is being implemented in some districts
- 20 -
Goal:To ensure cure for all those diagnosed of TB
m Target:
100% of HF service providers are trained on TB case diagnosis and management
Strategies:1. To strengthen regular supportive supervision in order to prevent stock outs of TB
drugs and improve reporting2. To build the capacity of service providers in laboratory service and TB case
management3. To strengthen and improve existing infrastructures, logistics and supplies for the
management of tuberculosis4. To strengthen active case surveillance and defaulter tracing5. To scale-up community-based DOTS program
Other Diseases with Epidemic Potential
Situation Analysis:1) 20 suspected cases of lassa fever were admitted and managed in 2010 at the Phebe
Hospital with 5 deaths2) 18 cases of measles reported and all complicated measles cases are usually treated
at Phebe hospital3) In 2010 there were 2 suspected cases of yellow fever(1st in January and 2nd in
June) and 129 cases of acute watery diarrhea (throughout the year), but no case of cholera
4) Awareness is carried out at the health facility and community levels5) Twenty service providers have been trained in the case management of lassa fever
with 4 at the Phebe Hospital6) There is an isolation ward at the Phebe for suspected cases of lassa7) Specimens are usually sent to the Reference Lab at LIBR and treatment is
provided with Ribavarin in the hospitals Goal:
To ensure that those diagnosed with disease of epidemic potential have access to prompt treatment
Strategies:1) To improve the logistics, supplies, drugs and other supplies for the management of
lassa fever and other diseases with epidemic potential2) To build the capacity of service providers in lassa case management 3) To conduct IEC/BCC at the health facility and community levels for prompt referral
of suspected cases4) To strengthen the emergency response to outbreaks by development of an
Emergency Preparedness Plan which would capture logistics and training needs.
EMERGENCY CARE
- 21 -
Situation Analysis:1) Cases of RTA and other emergencies are received and managed at the health facilities2) 24/7 emergency service is available at the hospitals3) First aid for minor emergency cases is provided at the primary health facility and
referral done for major cases4) Supplies, drugs and equipment are in place for the management of minor and major
cases
Goal:To ensure that emergency cases are timely and properly managed
Strategies:1) To establish an active 24/7 communications link between the community and health
facility for reporting2) To improve the availability of logistics, supplies, drugs and equipment for the
management of emergencies at health facilities3) To build the capacity of service provider in the management of emergencies
MENTAL HEALTH
Situation Analysis1) Ten MDM-supported health facilities are providing mental health services2) All OICs and DHOs including county supervisors have been trained on mental
health counseling and case management 3) Drugs are available to provide treatment of minor psychiatric conditions4) There is a mental health focal person on the CHT
Goal To improve mental health services in the county
Strategies1) To scale up mental health services in other health facilities in the county2) To build the capacity of additional service providers on mental health case
management3) To integrate mental health services into existing primary health care services4) To provide needed logistics, drugs, supplies and other equipment for mental health
services5) To conduct IEC/BCC at the HF and community level to improve timely referral for
treatment6) To conduct operational research on mental health situation in the county7) To strengthen link with community structures that are providing informal mental
health services
4.3. MAIN NEW SERVICES
Phase One (1st 3 years)
Sexual and Gender-based Violence
- 22 -

Situation Analysis1) There is a focal person on SGBV on the CHT2) There exist a local coordinating body on SGBV3) Rape and domestic violence are common in the community, but under-reported at all
levels4) All OICs, CMs and county supervisors have been trained on clinical management of
rape5) Suspected rape cases are often carried to health facilities very late6) There is some level of awareness on SGBV
Goal1. To highlight SGBV cases as a medical and psychosocial problem2. To increase awareness on the extent of the problem in the county
Strategies1) To build the capacity of service providers in counseling and clinical management of
rape and other SGBV conditions2) To carry out IEC/BCC on SGBV at the health facility and community levels3) To ensure the availability of drugs,, supplies and other logistics for the management
of rape
Reproductive Tract Cancers
Situation analysis1) Cases of advanced cancer (cervical, prostate and bladder) have been seen at hospital2) No drugs are available for the treatment of cancers3) No awareness on cancer is done at health facility and community levels4) No data available on cancer in the county HMIS
GoalTo create awareness on cancer and the benefit for early detection and management
Strategies1) To build the capacity of service providers on surveillance, detection and referral of
cancer cases2) To conduct IEC/BCC on cancer at health facility and community levels3) To conduct operational research on cancer
Health Promotion
Situation analysis1) A health promotion focal person at county level is also responsible for social welfare 2) No training has been conducted for health facility staff on health promotion 3) Health education is carry out at all health facilities using the MOHSW flipcharts
Goal To improve health promotion activity at the level of the CHT and health facility
Strategies
- 23 -

1) To build the capacity of service providers on health promotion2) To ensure that HFs have standardized IEC/BCC materials for areas of intervention 3) To improve health promotion activities at the health facility and community levels
School Health
Situation analysis1) There are currently no school health services besides a clinic at Cuttington University2) There are few high schools and university health clubs for awareness
GoalTo create awareness on the importance of school health programs
Strategies1) To establish strong link with the various schools on the significance of school health
programs2) To build the capacity of nursing students to conduct screening in various schools for
vision and dental check
Environmental and Occupational Health
Situational analysis1) There are 6 EH technicians and one auxillary staff on the CHSWT 2) WATSAN activities are carried out in some districts by other partners3) Incinerators and placenta pits are in most health facilities for proper waste disposal
GoalTo improve ongoing EH program in the county
Strategies1) To strengthen on-going EH activities at the health facility and community levels2) To improve proper waste disposal at all health facilities and communities
Non-Communicable Disease (Hypertension, diabetes mellitus, sickle cell anemia, cancer, asthma )
Situation Analysis1) Cases of NCDs are being diagnosed and treated, but not reported in HMIS 2) NCDs (hypertension and diabetes) are serious medical problem in most communities3) Community awareness about most NCDs is very low
GoalTo create awareness on the consequences of NCDs
Strategies1) To build capacity of service providers to diagnose and manage common NCDs2) Conduct IEC/BCC on common NCDs, including prevention (facilities and communities) 3) To provide logistics, supplies and drugs for the diagnosis and management of
common NCDs4) To conduct operational research on NCDs
Neglected Tropical Disease (Leprosy, Onchocerciasis, Buruli ulcer, and soil helminthes/worms)
- 24 -

Situation Analysis1) Ongoing community-based ivermectin treatment for onchocerciasis2) Research and mapping have been done on filiariasis by the MOHSW3) Deworming exercise is carried out in health facility and during national EPI
campaigns4) There is no information on Buruli ulcer 5) There is rehabilitation facility for the care and management of leprosy6) Treatment is provided for schistosomiasis
GoalTo create awareness on the consequences of neglected tropical diseases
Strategies1) To build the capacity of service providers on the diagnosis and management of
neglected tropical diseases2) To conduct IEC/BCC at the health facility and community levels on NTDs3) To establish surveillance and case detection for NTDs4) To provide supplies, drugs and equipment for the diagnosis and management of NTDs
Pharmaceutical Services
Situation Analysis1) Stock outs of essential drugs and supplies are still a major challenge 2) One drug depot exists with limited storage capacity and limited power supply 3) Two pharmacists in the county, one drug depot assistant and drug depot focal person4) There is one supply chain vehicle 5) Quarterly supply of essential drugs and commodities received from MOHSW or from
NDS or local vendors and supplied to health facilities on a monthly basis6) Drugs procured by partners and supplied to some health facilities on monthly basis
GoalTo improve supply chain at all levels of the health system
Strategies1) To expand the drug depot and strengthen supply chain2) To build the capacity of existing depot staff on supply chain and drug management3) To build the capacity of service providers on rational use of drugs4) To reduce stock outs of essential drugs and commodities5) To ensure proper monitoring of drug utilization at all HFs6) To advocate for an increase in county budgetary allotment for the procurement of
drugs and medical supplies7) To conduct operational research on rational use of drugs
Facility Infection Prevention
Situation Analysis: The followings are findings from the EmONC NA Factsheet 20101) % of facilities with any source of water – 86%
- 25 -

2) % of facilities with heavy duty gloves – 50%3) % of facilities with container for decontamination – 96%4) % of facilities with bleach and powder for decontamination – 100%5) % of facilities with soap – 100%6) % of facilities with puncture proof containers for sharps disposal– 96%7) % of facilities with functional autoclaves and/or steam sterilizer– 81%8) % of facilities with incinerator– 56%
GoalTo ensure universal precautions at all health facilities in the county
Strategies1) To strengthen and improve on existing infection prevention practices at all HFs2) To ensure the distribution of SOPs for infection prevention at all HFs
Laboratory and Diagnostic Services
Situation Analysis1) Laboratory services are available at ten health facilities2) % of facilities with laboratory services – 19% (EmONC NA Factsheet 2010)3) One radiological diagnostic center at the Phebe4) Three HFs (Phebe, CB Dunbar and Bong Mines) provide ultrasound services 5) One radiographer and three assistants are available at the Phebe Hospital6) Fourteen laboratory technicians and eight laboratory aides are available in the county
GoalTo improve laboratory and diagnostic services
Strategies1) To upgrade the capacity of existing lab aides to become lab technicians2) To ensure that most health facilities provide laboratory services3) To improve on existing laboratory and diagnostic infrastructures and services4) To build the capacity of existing technicians and aides in laboratory diagnostic
procedures
Health Management Information System
Situation Analysis1) An HMIS Unit exist at the county level2) One M&E officer, one data manager , one County registrar, and 2 birth registration
clerks are on the CHT3) The DHIS software is being used for the collection and reporting of health facility
data.4) There are also other separate reporting forms (STI, HIV , TB, and malaria)5) Some equipment for birth registration are available but training has not been provided
for county registrars6) Training on new data collection tools has been completed for county trainers
- 26 -

Goal1. To roll out the new standardized data collection and reporting tools2. To improve the quality of data from all health facilities
Strategies1) To build the capacity of service providers and data collectors on the new standardized
data collection tools2) To strengthen monthly supervision at all health facilities3) To improve data quality (timeliness reporting, completeness and correctness) to
Central Ministry4) To analyze data at the health facility and county level to inform decision making on
improving services5) To provide needed logistics for data collection and reporting6) To implement birth registration program
5.0. SYSTEMIC COMPONENTS
5.1. NETWORK OF HEALTH FACILITIES TO PROVIDE THE SERVICES
Situation Analysis1) There are currently 33 clinics , 2 special clinics with targeted population, no health
center and 3 hospitals that provide health services in the county2) Distribution of HFs in the county – Fuamah District-3 , Zota District – 5, Salala
District -3, Sanoyea District – 2, Pantakpaii District -9, Kokoyah District – 3, Jorquelleh District – 7, Suakoko District – 6.
3) 16 HFs are supported by Africare, 10 by MDM, 6 SC, and 4 are privately owned4) 48% of the population of the county live within 5km of catchment facilities while
52% of the catchment population live more than 5-10km distance from HFs. Seven HFs have a catchment population within 5km distance, for example – Jorwah, Janyea and Gbalatuah, while most health facilities catchment population are more than 5-10km away. For example Fenutoli, Gbanla and Sanoyea have more than 80% of the catchment population more than 5-10km away (Bong County Analysis Report 2010)
5) 6 health facilities have a catchment population of <3,500 people, 17 HFs between 3,500-12,000 people, and 5 health facilities have catchment population >12,000 Bong County Analysis Report 2010)
6) Two hospitals serve as the referral points for all the network of primary health facilities in the county and one provide Comprehensive EmONC and other surgical services (Phebe Hospital), while the other provide on CEmONC service (CB Dunbar Maternity Hospital)
7) There is a referral form in place that is used by HFs to ensure referral of patients from primary health facilities to the hospitals. However, some patients come to the hospitals without referral forms from primary facilities 6554829
Goal: To ensure an equitable distribution and access to primary health services Targets:
Rehabilitate the Bong Mine Hospital to provide EmONC and other services
- 27 -
Construct 15 additional clinics – Fuamah 1, Salala 2, Panta-Kpai 1, Sanoyea 5, Jorquelleh 3, Suakoko 2, 0 Kokoyah , and Zota 1
Construct 9 MCH Level I Clinics in underserved areas – Fuamah 1, Salala 2, Panta-Kpai 1, Sanoyea 1, Jorquelleh 1, Suakoko 1, Kokoyah 1 and Zota 1.Establish 24 Service Delivery Points 3 in Fuamah, 2 in Zota, 1 in Pantakpai, 1 in Salala, 9 in Sanoyea, 1 in Suakoko, 6 in Kokoya, Joquelleh 1,
Upgrade 8 clinics to health center level, with one in each district Strategies:
1) To improve and strengthen existing HFs to improve the quality of care2) To provide needed logistics, drugs, supplies, equipment and others for service
delivery3) To improve the transportation and communication link from communities and
primary health facilities to the hospital for emergency cases4) To strengthen the referral link at all levels 5) To provide motivation package for service providers at primary level to ensure staff
retention (staff housing)6) To carry out minor and major rehabilitations/constructions of health facilities7) To provide needed logistics to ensure service delivery at SDPs and outreach sites8) To re-organize the workforce in order to serve on outreach and at SDPs9) To strengthen the referral hospitals to play its crucial role as the main county referral
centers in the delivery of EmONC services and other components of the EPHSS10) The establish and/or strengthen community structures to implement community-based
health services
5.2. Human Resources Management and Development
Situation Analysis:1) There are a total of 273 skilled professionals including the following categories of
health workers – Physicians –5 , PA -14 , RN -105 , CMs, 87- Pharmacist -2 , Lab Technicians-14 , EHT -6 , LPN-40;
2) The distribution of skilled health workers is not the same at the various HFs, however, most health facilities in all districts have at most 2 skilled staff while in some HFs (Salala and Palala) there are at least 3 skilled staff
3) The staff utilization rate varies among health facilities in the county. For example Zota and Pantakpaii districts have high staff utilization rates of 97% and 99%, respectively, while some have low staff utilization rates as evident in Jorquelleh with 27% and Fuamah with 51%. Facilities with less workload or utilization rate can be attributed to any of the following reasons: distance, health workers behavior, long waiting hours or the overall quality of care. (Bong County Excel Analysis Report 2010)
4) There are more unskilled staff (730) compared to skilled staff (273) most of whom are nurse aids (114) and dispenser (44)
5) Six professionals have benefited from graduate studies in public health, general surgery, dental nursing, etc
- 28 -

Goal:To improve access to quality health services at all primary and secondary health facilities
Strategies1) To reorganize skilled health professionals in HFs with low staff utilization rate to
serve in outreach and at SDPs 2) To build capacity of some existing unskilled staff (nurses aids and dispensers) to
professional level (nurses, midwives, lab technicians, x-ray technicians, environmental health technicians, etc.)
3) To institute quarterly performance evaluation for all staff based on their job descriptions
4) To continue in-service training in areas of need for professional staff5) To collaborate with other institutions (MPCHS, CU, AMD Medical College) to meet
the human resource needs of the county6) To build the capacity of the CHSWT to manage the decentralized heath system
5.3 Drug Distribution and Rational Use
Situation Analysis:1) Stock outs of essential drugs, commodities and supplies is still a major challenge 2) One drug depot exist with limited storage capacity and limited power supply 3) Two pharmacists in the county, one drug depot assistant and drug depot focal person4) There is one supply chain vehicle 5) Quarterly supply of essential drugs and commodities received from MOHSW or
procuredfrom NDS or local vendors and supplied to health facilities on a monthly basis
6) Drugs procured by partners and supplied to some health facilities on a monthly basis7) There is still problem with the rational use of drugs in some health facilities8) Twenty eight (28) health facilities have limited drug storage capacities 9) Monthly consumption report is submitted to CHT and to MOHSW
Target: To reduce stock out of essential drugs and supplies to <1%
Strategies1) To expand the drug depot and strengthen supply chain2) To build the capacity of existing depot staff on supply chain and drug management3) To build the capacity of service providers on rational use of drugs4) To reduce stock outs of essential drugs and commodities5) To ensure proper monitoring of drug utilization at all HFs6) To advocate for an increase in county budgetary allotment for the procurement of
drugs and medical supply 7) To improve drug consumption data quality 8) To strengthen logistics for the delivery of drugs and supplies
- 29 -

5.4. Financing
Situation Analysis:1) There is an accountant on the CHSWT2) There is an allotment from GOL Budget through the MOHSW to support the CHSW
system3) There is a separate GOL allotment to the Phebe Hospital and Bong Mines Hospital4) Africare, SC-UK and MDM support 32 health facilities with funding from USAID,
Pool Fund and EDF Grant5) Other funding comes indirectly to support health projects in the county from
UNICEF, GFATM, GAVI, UNFPA, UNDP, USAID, WHO, JICA,WB, WFP and County Development Funds.
6) The CHSWT has accounts with two banking institutions: LBDI and Ecobank7) There is delay of funds transfer from Central MOHSW but there is timely liquidation
of funds received from Central MOHSW8) Developed mini proposals and do annual plan with budget attached for the CHT
activities
Goal:To find additional sources of funding within and out of the county to support the county health sector
Strategies:1) To improve partnership and collaboration with companies, business community and
other stakeholders for resource mobilization2) To continue timely liquidation of GoL and other funds 3) To develop annual operational plans and funding mechanisms to support the health
sector4) To collaborate with partners in joint planning to support health activities in the county5) To improve the capacity of CHSWT in planning and budgeting for health programs
5.5. Supervision and Monitoring
Situation Analysis:1) Supportive supervision is not regularly done by CHSWT due to other competing
priorities2) Joint supervision is done with partners at the health facilities3) Standardized checklist from Central MOHSW is used4) There are logistical constraints to carry out regular supervision5) There are staff to do supervision and some level trainings have been conducted on
supportive supervision at the CHSWT
Goal:To improve the quality of care at all levels
Strategies:1) To build the capacity of supervisors, DHOs and OICs on supportive supervision
- 30 -

2) To improve and strengthen regular monthly supervision at all levels3) To strengthen logistics (vehicles, motorcycles) for the implementation of supervision4) To establish community level supervision through the use of one skilled health
professional (EHT)
5.6. Quality Improvement
Situation Analysis1) Supervision and mentoring is done at health facilities to ensure that personnel, drugs
and other supplies are available for service delivery2) Annual BPHS Assessment is implemented by Central MOHSW to assess the
implementation progress in the county3) No quality improvement tool is presently being used to assess quality from the
provider or client
Goala. To improve quality of care at all health facilities
Target100% of HFs providing quality care health services
Strategies1) To strengthen supportive supervision and monitoring activities to all health facilities2) To introduce Client Oriented Provider Efficient (COPE) or other quality assurance
tools to assess the quality of care on a quality basis3) To incorporate exit interviews as part of the supervision of facilities4) To continue the annual EPHSS assessment at all health facilities
6.0. SECTOR COORDINATION ISSUES
Situation Analysis:1) Regular monthly coordination meeting with partners is conducted2) There is no standard agreement on operation in the county between the CHT and
health partners3) Partners do not disclose operational budget to the CHSWT4) The CHSWT is not sometimes consulted for planning, discussion and implementation
of some activities carried out by partners ( e.g. training)5) Joint planning is not done for health service delivery at the county level6) The CHSW Board is strong as an advisory arm of the CHSWT
Goal: To improve and strengthen partnership and coordination with all stakeholders
Strategies:1) To continue the monthly coordination meetings with partners
- 31 -
2) To strengthen joint planning and coordination with partners in the health sector3) To develop exit strategies and plans with INGOs partners for the management of their
supported health facilities by CHSWT4) To strengthen, organize and revitalize the Community Health Committees in all
districts5) To advocate for the improvement of coordination between programs at Central
MOHSW and the CHSWT for the implementation of activities
7.0 IMPLEMENTATION AND MONITORING
7.1. Implementation Phase/Plan
Implementation of the plan will be done in two phases for each of the components indicated below. Phase one, which will be the first three years will cover the areas of service provision, systemic components and sector issues. The operational plan will detail out which components to be done in each phase. Phase 2 will be years 4 to 10.
Table 1: Bong County Implementation PlanArea Component Phase
Service Provision EPHSS Primary 1, 2EPHSS Hospital 1, 2
Systemic Components
Health FacilitiesHuman Resource
1, 2
Pharmaceutical 1, 2Financing 1, 2Supervision and Monitoring 1, 2Quality Improvement 1, 2
Sector Issues Coordination 1, 2Planning 1, 2
7.2. Monitoring and Evaluation
The progress on implementation of the plan will be assessed through a monitoring and evaluation mechanism to be established. Indicators for each component of the plan will be developed and monitor over the duration of the plan (see Table 2 below). Benchmarks and final targets will be set to be monitored and evaluated at mid-term and the end of the life of the plan. Monitoring and evaluation activities provide information that describes how the plan is operating and contributes to ways to improve it.
At the implementation stage, the questions addressed by monitoring and evaluation activities include: To what extent has the plan been implemented as designed? How much does implementation vary from district to district? How can the plan be improved? How can it become more efficient or effective? As a result of these activities, revisions may be made to staffing, materials, activities, and the organizational or administrative aspects of the plan. Sometimes, the information may be used to make decisions about the plan based on whether or not the plan's stakeholders think the activities occurring will probably be effective in achieving the goals.
The monitoring and evaluation plan should typically include the following components:1) assumptions regarding context, activities, and goals; 2) anticipated relationships between activities, targets, and outcomes;
- 32 -

3) well-specified measures and their operational definitions (indicators and metrics) and baseline values;
4) monitoring schedule, data sources, and M&E resource estimates; partnerships and collaborations required to achieve results; and a plan for data dissemination and use.
The following will be used to ensure monitoring and evaluation of the ten year plan to assess its progress and achievement of targets set:
Develop Indicators to monitor service provision, systemic components and sector issues
Standardized Supervision Checklist (Health Facility and Community Level) EPHSS Assessment Tool COPE tool (Health Facility and Community) Operational Research (Qualitative and Quantitative)
o Lot Quality Assurance Sampling (LQAS)o Rapid Health Service Provision Assessment (RHSPA)o Focus Group Discussions (FGD)
Table 2: Bong County Plan Monitoring Framework
Objective Indicator Base-line
Target 2021
Increased access and utilization of health services
% population living within 5 km from the nearest health facility
Service Provision
Maternal Health
[# and] % of deliveries that are facility-based with a skilled birth attendant
Family Planning
Couple-years protection with Family Planning Methods
Child Health/EPI
[# and] % of children under 1 year who received DPT3/pentavalent-3 vaccination
Service Consumption OPD consultations per inhabitant per year
Malaria [# and] % of pregnant women provided with 2nd dose of IPT for malaria
HIV/AIDSNumber of pregnant women testing HIV+ and receiving a complete course of ARV prophylaxis to reduce the risk of MTCT
Tuberculosis Number of smear positive TB cases notified per 100,000 population
Systemic compon-ents
Human Resources
Number of skilled birth attendants (physicians, nurses, midwives & physician assistants)/10,000 population
Drugs[# and] % of facilities with no stock-out of tracer drugs during the period (amoxicillin, cotrimoxazole, paracetamol, ORS, iron folate, ACT, FP commodity)
HMIS [# and] % of timely, accurate and complete HIS reports submitted to the MOH during the year
Financing % of execution of annual allocation of GoL budget for health
Quality# and % of facilities reaching two star level in accreditation survey including clinical standards (public network facilities)
- 33 -
8.0. REFERENCES
1. Bong County Health Plan, September 26, 2007
2. Ministry of Health & Social Welfare 2010 Annual Report, January 15, 2011
3. Comprehensive Food Security & Nutrition Report 2010, October 2010
4. Bong County Excel Spreadsheet 2010
5. Bong County Health & Social Welfare Team Report 2010
6. A Guide to Monitoring & Evaluating Child Health Program, Gage et al, September 2005
7. Road Map For Accelerating the Reduction of Maternal and Newborn Morbidity and Mortality in Liberia, March 2011
8. Liberia 2007 Demographic and Health Survey Key Findings
9. National EmONC Needs Assessment Factsheet 2010
10. BPHS Assessment January Report 2010, MOHSW
- 34 -





























