Embed Size (px)
Citation preview


Expanding Choosing Wisely® to the Medicare Population: Data analysis, audit & feedback to decrease low-value healthcare
Objectives
1. Understand the Choosing Wisely program
2. Discuss variation in practice in four metrics of potentially low-value healthcare in the Medicare population in Washington State
3. Describe advantages and limitations of audit-and-feedback as a provider-level intervention

Qualis Health
• A leading national population health management organization
• The Medicare Quality Innovation Network - Quality Improvement Organization (QIN-QIO) for Idaho and Washington
The QIO Program
• One of the largest federal programs dedicated to improving health quality at the local level

Thanks to Daniel Wolfson, MHSA
Executive VP, COO, ABIM Foundation
Presented at Choosing Wisely Summit
Seattle, Washington, 10/2015

Why Now? Stewardship
• Approximately 30% of healthcare costs (>$750B/yr) for wasted care American College of Physicians
• 53% of physicians say they would ultimately order an unnecessary test or procedure when presented with an insistent patient Unnecessary Tests and Procedures in the Health Care System: What Physicians Say about the Problem, the Causes, and the Solutions—Results from a National Survey of Physicians (Healthcare and The Commonwealth Fund [Internet]. 2009; Apr 27)
• Physician decisions account for 80% of all health care expenditures Crosson FJ. Change the microenvironment. Modern Healthcare and The Commonwealth Fund [Internet]. 2009; Apr 27
• “Some of the common medical tests routinely taken by Americans do more harm than good, waste billions of health care dollars annually and could endanger your health or even your life.” 10 Medical Tests to Avoid. Elizabeth Agnvall. AARP Bulletin, March 2014

Where is the Waste?
Source: Donald M. Berwick, MD, MPP; Andrew D. Hackbarth, Mphil, JAMA. 2012;307(14):1513-1516. doi:10.1001/jama.2012.362

The Choosing Wisely® Campaign
An initiative of the ABIM Foundation
• Help physicians and patients engage in conversations about the overuse of tests and procedures and support physician efforts to help patients make smart and effective care choices.

“Five Things” Lists
ABIM partnered with medical specialty societies to develop evidence-based recommendations of the “Five Things Physicians and Patients Should Question” because they’re ineffective, unnecessary, or harmful.
70+
Participating specialty societies
350+ Tests and procedures identified

“Five Things” Lists

Responsibility and ownership in creating lists
Specialty Controlled Frequently Used or Costly
Transparent Process Evidence-Based

What have we learned so far?
Power of • Professionalism
• Leadership and Partnerships
• Communications
• Culture as a change agent
• Responsibility and ownership
• Open platforms
• Choosing Wisely in system changes
• A brand

Professionalism
Fundamental Principles
• Primacy of patient welfare
• Patient autonomy
• Social justice
A Commitment to
• Professional competence
• Honesty with patients
• Patient confidentiality
• Maintaining appropriate relations with patients
• Improving quality of care
• Improving access to care
A just distribution of finite resources
• Scientific knowledge
• Maintaining trust by managing conflicts of interest
• Professional responsibilities

Leadership
• American Academy of Allergy, Asthma & Immunology • American Academy of Family Physicians • American College of Cardiology • American College of Physicians • American College of Radiology • American Gastroenterological Association • American Society of Clinical Oncology • American Society of Nephrology • American Society of Nuclear Cardiology • American Academy of Hospice and Palliative Medicine • American Academy of Neurology • American Academy of Ophthalmology • American Academy of Otolaryngology— Head and Neck Surgery • American Academy of Pediatrics • American College of Obstetricians and Gynecologists • American College of Rheumatology • American Geriatrics Society • American Society for Clinical Pathology • American Society of Echocardiography • American Urological Association • Society for Vascular Medicine • Society of Cardiovascular Computed Tomography • Society of Hospital Medicine • Society of Nuclear Medicine and Molecular Imaging • Society of Thoracic Surgeons • AMDA – Dedicated to Long Term Care Medicine • American Academy of Clinical Toxicology • American Academy of Dermatology • American Academy of Nursing • American Academy of Orthopaedic Surgeons • American Association for Pediatric Ophthalmology and Strabismus • The American Academy of Physical Medicine and Rehabilitation • American Academy of Sleep Medicine
• American Association for the Study of Liver Diseases • American Association of Blood Banks • American Association of Neurological Surgeons • American College of Chest Physicians • American College of Emergency Physicians • American College of Medical Genetics and Genomics • American College of Medical Toxicology • American College of Occupational and Environmental Medicine • American College of Preventive Medicine • American College of Surgeons • American Headache Society • American Medical Society for Sports Medicine • American Physical Therapy Association • American Psychiatric Association • American Society for Radiation Oncology • American Society for Reproductive Medicine • American Society of Anesthesiologists • American Society of Hematology • American Thoracic Society • Commission on Cancer • The Endocrine Society • Heart Rhythm Society • Infectious Diseases Society of America • North American Spine Society • Society for Cardiovascular Angiography and Interventions • Society for Cardiovascular Magnetic Resonance • Society for Healthcare Epidemiology of America • Society for Maternal-Fetal Medicine • Society of Critical Care Medicine • Society of General Internal Medicine • Society of Gynecologic Oncology

Partnerships
Founding Partners • AARP • Alliance Health Networks • Midwest Business Group on Health • National Business Coalition on Health • National Business Group on Health • National Center for Farmworker Health • National Partnership for Women & Families • Pacific Business Group on Health • SEIU • The Leapfrog Group • Wikipedia
National Partners and Specialty Societies
• Lamaze International • National Hospice and Palliative Care Organization • Union Plus
Regional Partners • The Alliance • Baby Boomers for Balanced Health Care • California Grower Foundation • Coalition for Compassionate Care of California • Connecticut Choosing Wisely Collaborative • Covered California • Detroit Regional Chamber • Greater Detroit Area Health Council • Health Policy Corporation of Iowa • Healthcare Collaborative of Greater Columbus • Los Angeles County Department of Public Health • Minnesota Health Action Group • Oregon Health Care Quality Corporation • Pittsburgh Regional Health Initiative • Rhode Island Business Group on Health • VNA Community Healthcare • Washington Health Alliance • Washington State Hospital Association • Washington State Medical Association • Qualis Health • WellOK • West Chester Library System • West Virginians for Affordable Health Care

Partnerships
Current Grantees • Greater Detroit Area Health Council
• Integrated Healthcare Association
• Maine Quality Counts
• North Carolina Healthcare Quality Alliance
• University of California, Los Angeles
• Washington Health Alliance
• Wisconsin Collaborative for Healthcare Quality
Specialty/State Medical Societies • American Academy of Hospice and Palliative
Medicine
• American Academy of Ophthalmology
• American College of Physicians
• American Society for Clinical Pathology
• American Society of Echocardiography
• American Society of Nuclear Cardiology and Massachusetts Medical Society
• Minnesota Medical Association
• Oregon Medical Association
• Society of Hospital Medicine
• Tennessee Medical Association
• Texas Medical Association
• Washington State Medical Association
Regional Collaboratives • Better Health Greater Cleveland
• HealthInsight Utah
• Institute for Clinical Systems Improvement and Minnesota Health Action Group
• Iowa Healthcare Collaborative
• Maine Quality Counts
• Massachusetts Health Quality Partners
• Michigan Health Information Alliance
• Washington Health Alliance
• Wisconsin Collaborative for Healthcare Quality

Culture as a Change Agent
Lessons learned from patient safety culture • Quick to go to quality improvement without clinician engagement
• Culture eats strategy for lunch….every time!

Open Platforms

Open Platform

Implementation

Medical Education in Training and Practice

Power of a Brand

What we need in the future
• Ownership and professionalism carried forward to implementation
• Development of measures for QI
• Continue to ramp up recommendations
• Continue implementation of recommendations through system changes beyond education
• Continue payment reform and delivery system redesign
• Evaluation/research of what works to de-implement a practice
• Support and recognition of practices that reduce waste
• Success of RWJF grantees

Choosing Wisely in Washington State

Sponsors and Community Partners
Co-Sponsors
• Washington State Medical Association (2012)
• Washington Health Alliance (2013)
• Washington State Hospital Association (2013)
Community Partners
• State specialty and professional societies (2014)
• Qualis Health (2015)
• Department of Health (2015)

Washington Task Force’s Overall Goals
Working together to advance Choosing Wisely across the state:
• Identify opportunities for improvement
• Accelerate implementation and integration
• Reduce the number of unnecessary tests and procedures
Members
• 22 physician leaders representing the largest healthcare organizations in Washington

Washington State Choosing Wisely Task Force
Health Systems • CHI Franciscan Health System
• Confluence Health
• Edmonds Family Medicine
• EvergreenHealth
• Group Health Cooperative
• Kadlec Health System
• PeaceHealth Health System
• Providence Regional Med Ctr Everett
• Signal Health
• Skagit Regional Health
• Swedish Medical Center
• UW Medicine
• Virginia Mason
Other Health
Partners • Fred Hutchinson Cancer Research
• Qualis Health
• WA Department of Health
Medical Groups • Northwest Physicians Network
• Rockwood Clinic
• The Everett Clinic
Health Plans • First Choice Health
• Group Health Cooperative
• Premera Blue Cross
• Regence Blue Shield

Overview of Washington Activities

Task Force’s Reports

Claims-Based Technical Specifications

Less waste. Less harm. Choosing Wisely in Washington state

Choosing Wisely recommendation
American Academy of Allergy, Asthma & Immunology: Don’t prescribe antibiotics for uncomplicated acute rhinosinusitis.
Commercial average: 43% Medicaid average: 28%

Choosing Wisely Action Manual
Kotter’s 8-Step Process for Leading Change to Integrate Choosing Wisely 1. Create a sense of urgency
2. Build a guiding coalition
3. Form a strategic vision and initiatives
4. Enlist a volunteer army
5. Enable action by removing barriers
6. Generate short-term wins
7. Sustain acceleration
8. Institute change ww.wsma.org/Choosing-Wisely
2016 and 2017 Activities/Achievements
• Awarded 3rd grant from ABIM Foundation • Goal: By 2018, reduce overuse on 3 measures by 20% across Group Health
and Swedish, and then spread throughout the state.
• Published 2nd statewide report on overuse, including Medicare data
• Published Consumer Engagement Toolkit
• Conduct third annual Choosing Wisely in Washington Summit – coming up October 27 in Seattle – join us!
Qualis Health SIP: Spread to Medicare Beneficiaries
• Qualis Health analyzed FFS Medicare claims to identify prevalence of selected “low-value” services among FFS Medicare beneficiaries
• Individual providers with higher than average rates of “low-value” services for Medicare beneficiaries

Targeted Low-Value Healthcare Services
• CT or MRI for simple syncope
• CT or MRI for uncomplicated headache
• Antibiotics for URI (supports 11th SoW Task C.3.10)
• Antipsychotic medications for behavioral and psychological symptoms of dementia (supports 11th SoW Task C.2)
All four measures showed significant variation in individual practice.
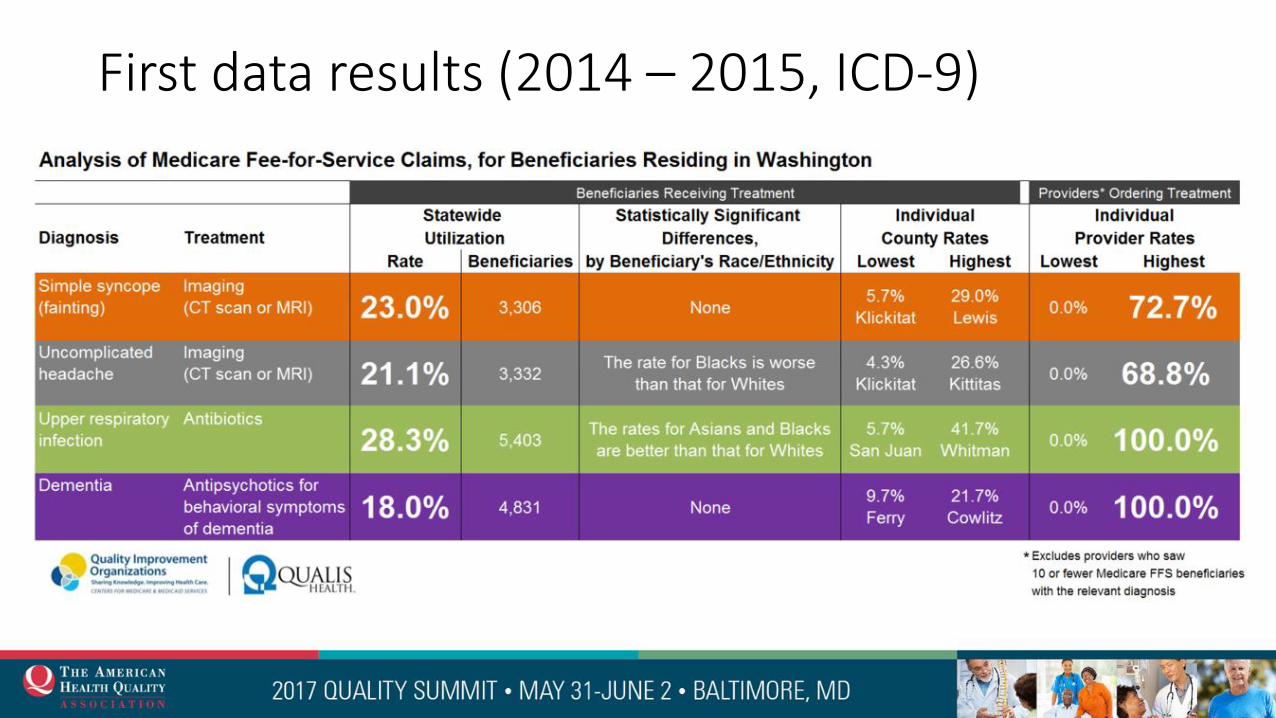
First data results (2014 – 2015, ICD-9)


Qualis Health Contributions to Reports: URI

Qualis Health Contributions to Reports: Imaging for H/A

Qualis Health Contributions to Reports: Imaging for Syncope
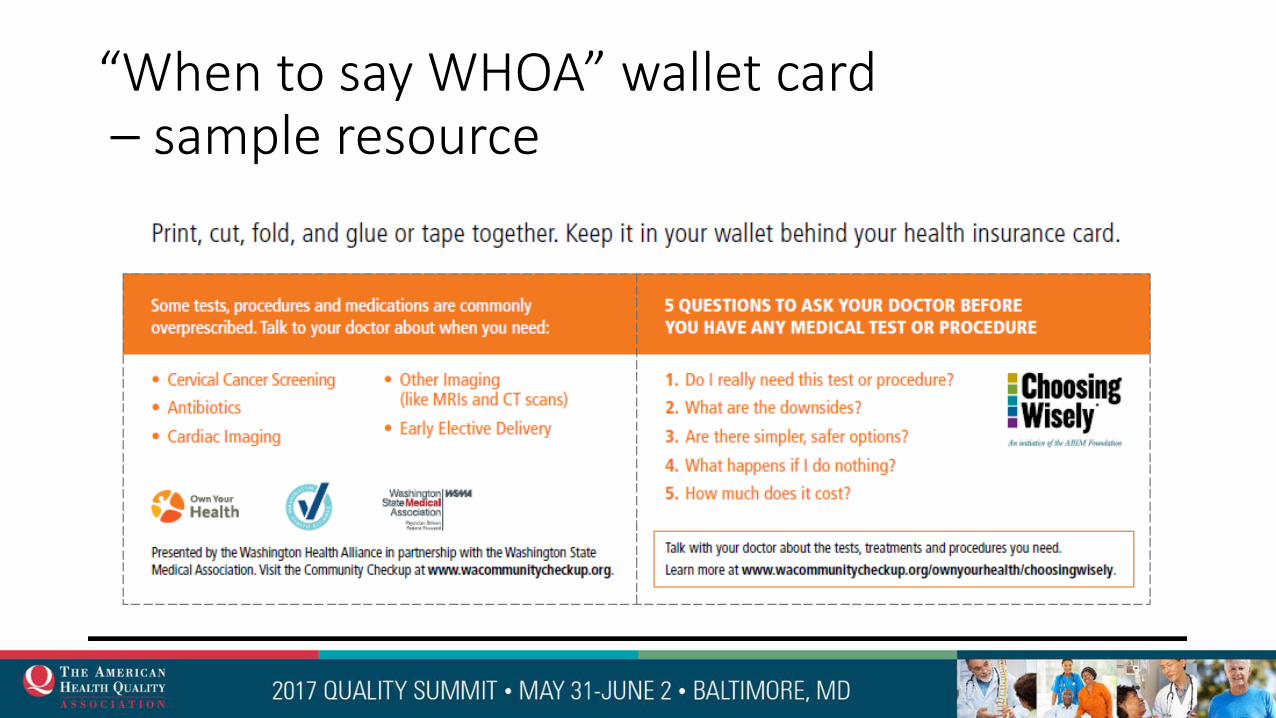
“When to say WHOA” wallet card – sample resource

Intervention
• Choosing Wisely for Medicare website www.Medicare.QualisHealth.org/ChoosingWisely
• Expanding upon local initiative
• Individual provider feedback
Individual Provider Feedback
• Confidential feedback to “high-utilizer” prescribers
• Compares individual prescriber’s rate to state average
• Introduces “high-utilizer” prescribers to Choosing Wisely initiative and resources, including clinical rationale and tools to support clinician-patient discussion


Provider Feedback
“…Two opposing forces make it difficult to balance proper use of imaging–clinically necessary use of imaging vs. patients demanding imaging and providing poor survey results if they do not get what they want…I was hoping you could comment on my concerns and provide guidance.”

Potential Cost Savings: Scenario Parameters • Number of beneficiaries who actually received low-value health
services from “high-utilizers”
• Number of avoided cases of low-value health services if “high-utilizers” had prescribed less low-value health services
• Attributable costs of avoided low-value services • Direct cost of low-value services
• Indirect cost of adverse outcomes related to low-value services

Intervention Effect Size Scenarios
Reducing the rate of low-value services among high-utilizers
• Large effect: 31-35 absolute percentage point reduction (reduce rate to the WA state average for selected low-value services)
• Small effect: 16 absolute percentage point reduction*
*JAMA. 2016;315(6):562-570 ; Cochrane Database of Systematic Reviews 2012, Issue 6. Art. No.: CD000259

Projected Avoided Low-Value Cases Using Large and Small Intervention Effect Sizes
0
100
200
300
400
500
600
700
800
syncope headache abx anti-psych
po
ten
tial
ly a
void
ed
cas
es
large effect small effect

Projected Annual Costs Avoided with Large and Small Effect Size Low Value Service Projected Costs Avoided / Effect Size
Large Small
CT/MRI for Headache $17,748 $9,022
CT/MRI for Syncope $123,326 $63,332
Antibiotics for URI $6,570 $3,469
Antipsychotics for dementia $2,331,083 $1,065,434
Totals $2,478,637 $1,141246

Basis of Direct Cost Estimates
• For imaging costs Sum of median Part B and Part A charges for all beneficiaries who received either CT or MRI for syncope or headache in the analysis year ($929 and $537 respectively)
• For antibiotics for URI Average Rx cost in the analysis year for all beneficiaries who received antibiotics for URI (7$)
• For antipsychotics Average yearly cost in the analysis year for all beneficiaries prescribed antipsychotics for behavioral symptoms of dementia ($3000)

Basis for Indirect Costs Estimates
For antibiotics:
• $13 dollars in societal costs for every ambulatory service antibiotic prescription inclusive of costs related to antibiotic-resistance attributable costs of hospitalization, second-line inpatient antibiotic use, second-line outpatient antibiotic use, and antibiotic stewardship.)3
• Not included in estimates, but related to potential cost savings, is the attributable cost of new and recurrent cases of Clostridium-difficile infection, $5,000-11,000 4,5
3Michaelidis et al. BMC Infectious Diseases (2016) 16:655
4Dubberke ER, et al. Clinical Infectious Diseases (2008) 46:497–504
5Duberke ER et al. Infect Control Hosp Epidemiol ((2014)35(11):1400-1407

Basis for Indirect Costs Estimates
For antipsychotics:
• Hospitalization cost for one stroke = $26,0006
• Hospitalization cost for one injury fall = $30,0007
• Using psychosocial treatment instead of antipsychotics results in 1 less stroke per 100 treated and one less injury fall per 1,000 treated8 • Large effect prevents 7 strokes, 1 injury fall
• Small effect prevents 3 strokes
6 Am Health Drug Benefits. (2014) Jun; 7(4): 200–209 7 Burns EB, Stevens JA, Lee RL. J Safety Res. (2016) Sep.58:99-103. 8 “An economic evaluation of alternatives to antipsychotic drugs for individuals living with dementia.” October 2011. NHS Institute for Innovation and Improvement.

Factors Thought to Improve Effectiveness of Audit and Feedback9
• Poor baseline performance
• Audit and Feedback via respected supervisor or colleague
• Repeated Audit and Feedback
• Feedback provided verbally and in writing
• Feedback provides clear target and action plan
9Cochrane Database of Systematic Reviews 2012, Issue 6. Art. No.:CD000259.

CY 2016 Preliminary Data Updates Metric Jan-Jun 2016 Jun-Dec 2016
Headache (no letters) 26.0% 25.5%
Headache (letters) 52.6% 53.2%
Syncope (no letters) 30.1% 29.3%
Syncope (letters) 49.4% 45.3%
URI (no letters) 31.0% 29.7%
URI (letters) 61.5% 45.2%
There was a statistically significant decrease for the people who received URI letters, but not for the headache or syncope letters. Many of the individual physicians fall out of the high outlier groups from previously due to small volumes rather than apparent change in practice. We are continuing to analyze the data – AP for dementia is pending.

Next Steps – Looking Forward

Questions?
Sharon Eloranta, MD Medical Director, Quality and Safety Initiatives [email protected] (206) 288-2474
For more information:
www.Medicare.QualisHealth.org/ChoosingWisely
This material was prepared by Qualis Health, the Medicare Quality Innovation Network - Quality Improvement Organization (QIN-QIO) for Idaho and Washington, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. WA-CW-QH-2944-05-17