Embed Size (px)
Citation preview
546
EXPANDING LESIONSOF THE TEMPORAL FOSSA
By LESLIE OLIVER, M.B.(Lond.), F.R.C.S., F.A.C.S.Neurosurgeon: Charing Cross Group of Hospitals, Royal Northern Hospital, West End Hospital for Neurology andNeurosurgery, The French Hospital, London; and Southend General Hospital, Southend-on-Sea. Senior Neurosurgeon:
North-East Regional Neurological and Neurosurgical Centre, Oldchurch Hospital, Romford, Essex
Brain-stem CompressionExpanding lesions in the temporal fossa readily
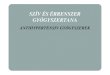
displace the brain-stem towards the opposite sidewhere it is forced against the edge of the tentorium.At the same time a wedge formed by the uncusand hippocampal gyrus is forced downward betweenthe midbrain and the edge of the tentorium on theside of the lesion (Fig. i). These two mechanismsproduce the various stages of midbrain com-pression. The downward herniation of the uncusand hippocampal gyrus also compresses the homo-lateral oculomotor nerve. Rarely the ncrve is atfirst stimulated and therefore the pupil is con-stricted, but as pressure on the nerve increasesparalysis ensues and the pupil becomes dilated.Usually, however, the pupil dilates as soon as thenerve is compressed. If the patient is conscious,ptosis and paralysis of the external ocular musclessupplied by the oculomotor nerve may be observed.The posterior cerebral artery prolapses throughthe tentorial notch with the herniated brain andoccasionally a contralateral homonymous hemi-anopia is produced by kinking of the artery or itscalcarine branch over the free edge of thetentorium.
Increased intracranial pressure is produced byexpansion of the lesion itself, pressure on the mid-brain and consequent obstruction of the aqueductof Sylvius, and often also by associated cerebraloedema. The increasing pressure, if not too rapid,may produce papilloedema. It also causes descentof the brain-stem through the tentorial openingsometimes resulting in sufficient traction on one orboth abducens nerves to cause unilateral orbilateral external rectus palsy. If descent of thebrain-stem continues, ' coning' of the cerebellartonsils occurs at the foramen magnum and com-pression of the medulla oblongata results.
Midbrain compression may be roughly classi-fied into the following stages:
Stage i. Clouding of consciousness, normalpupils or occasionally contraction of the pupil on
:ii.ii$iiliiiri;
:: I:. ::
iii.,iiiiiaiirl;illji.:;' .s.%.;.;.iig9l;;;"a.:·ii'::·:: :1;·::
:i I.sapr .e
:ig
::i:'
Y..i Lii:!:.ic?·i
:';l..ss.l:·ii··:;.T.Rs. 't...i.li;C
:" i'lP
::i:;:"'··'·'!l:CiiUi%ii
:siai:.l:·:i·iiiiiir:::lb
·ib,lSiiiiiiF.s.".8.i.g.j. ·:';i.ii..iiil!j.i.iii': il'.r"'e,·
:ti::
:::i:'S:iliii4LtiiiiiC1;;ilii:,ii i.ii i:;iiiiii.,ai:iiiii:!i:c.:··d:·*.·:1.::i
FIG. I.-Temporal lobe herniation. The groove madeby the free edge of the tentorium on the undersurface of the left temporal lobe is indicated byarrows. The enlargement of the temporal lobewas caused by a glioblastoma multiforme. (From'Basic Surgery' by kind permission of thepublishers, H. K. Lewis, London.)
the side of the lesion, and contralateral or homo-lateral hemiparesis with hypertonia, hyperreflexiaand a positive Babinski sign. (Homolateralpyramidal signs are caused by displacement of thebrain-stem away from the side of the lesion andresulting indentation of the contralateral cerebralpeduncle by the edge of the tentorium-theKernohan-Woltman phenomenon.) Occasionallycontralateral or homolateral Parkinsonian tremorand rigidity, presumably due to ischaemia of thesubstantia nigra or its efferent pathways.
Stage 2. Stupor, dilatation and paralysis of the
copyright. on 24 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.408.546 on 1 O
ctober 1959. Dow
nloaded from
OLIVER: Expanding Lesions of the Temporal Fossa
pupil on the side of the lesion (Hutchinson's pupil),and contralateral or homolateral hemiparesis,hypertonia, and hyperreflexia with unilateral orbilateral Babinski responses. Occasionally Parkin-sonian manifestations in the limbs. Increasingpulse rate (the classical slow pulse, although ofconsiderable diagnostic importance, is found lessoften than a fast one).
Stage 3. Coma, dilatation and paralysis of thepupil on the side of the lesion or on both sides,decerebrate rigidity with increased tendon jerksand bilateral Babinski responses. Cheyne-Stokesrespiration. Tachycardia (if cerebellar coningis causing compression of the medulla oblongata,the pulse may be slow and associated with in-creased blood pressure and slow respiration).
Stage 4. Absence of response to all externalsensory stimuli, dilatation and paralysis of bothpupils, flaccidity of all voluntary muscles, absenttendon reflexes, bilateral Babinski responses orabsent plantar reflexes. Rapid weak pulse.Shallow slow respirations.
Patients may pass from one stage to another ineither direction. Rapidly expanding lesions inthe temporal fossa may lead immediately to stages3 or 4. Thus there are often no lateralizing orlocalizing signs with acute lesions.
Visual Field DefectsThe optic radiation sweeps widely forward in
the upper posterior part of the temporal lobebefore passing backward to the occipital cortex.Thus lesions within the temporal lobe may invadethe optic radiation from below, and as light raysfrom above strike the lower part of the retina andlight rays from one side strike the opposite side ofthe retina, contralateral homonymous upperquadrantic field defects are produced. This is incontrast with lesions within the parietal lobe, forthey invade the optic radiation from above andcause contralateral homonymous lower quadranticfield defects. A lesion arising in either situationmay eventually cut across the whole of the opticradiation and produce a complete contralateralhomonymous hemianopia. Involvement of theoptic radiation usually, through not invariably,indicates a destructive lesion within the cerebrumrather than compression of its surface.
DysphasiaNominal dysphasia may occur with lesions of
the superior temporal convolution of the dominanthemisphere. Lesions which spread upwards andbackwards from the dominant temporal lobe mayeventually cause total aphasia by destroying thespeech centres of the parietal lobe.
Personality ChangesThe temporal cortex is concerned with the
reception, directly or indirectly, of association-fibre systems of the other areas of the cerebralcortex, and may therefore be expected to play animportant part in the total function of the cerebralcortex. Nevertheless, personality changes arerarely associated with expanding lesions of thetemporal fossa, but when they do occur they takethe form of anxiety, irritability and occasionallyagressiveness. This is in marked contrast withthe apathy often produced by expanding lesionsof the anterior fossa.
Temporal Lobe EpilepsyAbout a quarter of all cases of epilepsy have
their focus of discharge in one or other temporallobe. Although atrophy of part of the temporallobe is the most commonly occurring underlyingpathological process, tumours account for a sig-nificant proportion of cases of temporal lobeepilepsy. Often the discharge is confined to thetemporal lobe, giving rise to characteristicphenomena, but it may spread over the whole ofthe cerebral cortex to produce grand mal attacks.There are several modes of origin of temporal
epilepsy and each reflects one of the functions ofthe temporal lobe. The commonest is a sensa-tion in the abdomen, chest or throat (visceralaura) and is related to autonomic function. Theclassical attack as originally described byHughlings Jackson, begins with a sensation of abad smell or taste accompanied by smacking of thelips and a ' dreamy state'; the origin of suchattacks is in the uncus, hippocampus or amygdala,the location of olfactory and gustatory function.Other patients complain of unpleasant noises or adisturbance of equilibrium, sometimes so severethat the patient is thrown to the ground (gyratoryepilepsy); sounds may seem unduly loud or soft;these attacks are related to the auditory andequilibratory functions of the superior temporalconvolution. Some patients experience suddenfear, anger or pleasure. There may be a suddenfeeling of familiarity with the surroundings, or thepatient may feel that what is happening has takenplace before (deja vu phenomenon). Sometimesobjects seem small and receding (micropsia), orlarge and near (macropsia). A vivid recollectionof the past with its associated emotions may forceits way into consciousness. Patients may carryout complicated acts unrelated to present eventsbut sometimes related to the sensory phenomenaand tending to be aggressive (not to be confusedwith post-epileptic automatism). Depersonaliza-tion (a feeling of complete detachment from self),and sometimes the related phenomenon of auto-scopy (seeing an image of oneself in the external
October 1959 547
copyright. on 24 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.408.546 on 1 O
ctober 1959. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
environment), are sometimes experienced. Thesecurious effects are related to the highest functionallevels of the temporal lobe.
Neighbourhood EffectsExpansion of temporal lesions upward often
causes contralateral facial paresis due to involve-ment of the facial area of the frontal cortex or itsefferents. Expansion upwards and medially causescontralateral facial paresis and hemiparesis byinterference with the homolateral pyramidalfibres.
HaematomasExtradural HaematomaThe temporal fossa is the commonest site for this
type of haematoma. The haemorrhage arises fromdamage to the middle meningeal artery or itsbranches, severed diploic veins in the line offracture, or sometimes from a torn transverse orsuperior petrosal sinus. The haematoma isusually, but not always, associated with a fractureof the temporal bone and there is nearly always anoverlying visible scalp lesion.
Brain-stem compression (vide supra) rapidlydevelops, usually within 24 hours of the injury,and in about half the cases there is no improve-ment in the level of consciousness before the onsetof brain-stem compression. In childhood aninitial period of coma seldom occurs; more oftenchildren are momentarily dazed and later becomeunconscious from the effects of the expandinghaematoma. They sometimes have convulsions.Also, wide separation of the sutures or fracturelines sometimes allows much of the blood to escapeunder the elastic scalp producing some degree ofspontaneous decompression and delaying the onsetof compression of the brain. In infants, enoughblood may be lost from the circulation in theformation of an extradural haematoma to causesevere anaemia and shock.The mortality of extradural haematoma is still
about 50 per cent., for it is not sufficiently realizedthat it is one of the most rapidly lethal conditionsin surgery. Immediate diagnostic burr-holes areindicated in traumatic coma if (a) the level ofconsciousness does not rapidly improve, (b) thelevel of consciousness declines, or (c) any newabnormal neurological signs appear, e.g. hemi-paresis, pupillary dilatation.
Subdural HaematomaThere are three varieties of haematoma ocur-
ring between the dural and arachnoid membranes,acute, subacute and chronic. An acute subduralhaematoma is frequently found in head injuriesbut it is usually small and associated with severe
brain damage. Sometimes, however, an acutesubdural haematoma is large and clinically in-distinguishable from an extradural haematoma.Its bulk tends to be in the temporal fossa althoughit extends well beyond the temporal boundariesand may sometimes envelop the whole hemi-sphere. Acute subdural haematomas arise fromdamage to cortical vessels or venous sinuses.They have no capsule (cf. subacute and chronicsubdural haematomas).A subacute subdural haematoma reveals itself a
few weeks after a minor head injury although inmany cases no history of injury is obtained.This type of haematoma is thought to be causedby tearing of one of the veins which pass from thecerebral cortex to the venous sinuses. The bloodtends to gravitate to the temporal region but ex-tends well beyond its limits. A thin capsule formsaround the haematoma. In adults subacute hae-matomas are frequently bilateral; in early child-hood they are almost always bilateral. Thediagnosis is made when evidence of increasedintracranial pressure and perhaps contralateral,homolateral or bilateral pyramidal signs developa few weeks after a head injury. In the absence ofa history of trauma a clinical diagnosis of intra-cranial tumour is made and the haematoma re-vealed by subsequent investigations.A chronic subdural haematoma reveals itself
months or even years after a minor head injuryalthough again a history of trauma is often lacking.In most cases the clinical diagnosis is intracranialtumour. The capsule tends to be thick; oc-casionally the whole of the haematoma becomesreplaced by fibrous tissue and the presence of bloodpigment may be the only remaining evidence oftrauma.
In early childhood, birth trauma is thought tobe a common cause of subdural haematoma. Inthe majority of cases there is no characteristicclinical picture. Thus infants may show nothingmore than restlessness and bad temper or theremay be attacks of generalized convulsions, thecommonest manifestation of the condition in earlylife. Sometimes vomiting occurs. There ispyrexia in more than half the cases and bulgingof the fontanelle in somewhat less than half. Thecircumference of the head may be 2 to 3 in. morethan average. Retinal haemorrhages are quitecommon although papilloedema is rare owing tothe decompressive effect of separation of thesutures of the skull. The tendon reflexes may beexaggerated but paresis of the limbs occurs inonly a small proportion of cases. The mani-festations in early life are thus vague. Thereforea subacute or chronic subdural haematoma shouldbe one of the conditions considered when a childis not thriving.
548 October 1959copyright.
on 24 April 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.408.546 on 1 October 1959. D
ownloaded from
OLIVER: Expanding Lesions of the Temporal Fossa
Subdural Hygroma or HydromaSubdural collections of colourless or yellow
fluid of raised protein content may occur with orwithout a history of head injury. Some followmeningitis, especially that caused by H. influenzae.They are frequently bilateral and although thetemporal region is usually involved they tend to bewidespread. The clinical manifestations are thesame as those found with subdural haematomasand long-standing collections are surrounded by athin capsule.Intracerebral HaematomaThe temporal lobe is the commonest site for a
spontaneous intracerebral haematoma. Such ahaematoma may arise from rupture of an in-tracranial aneurysm or, less often, a vessel formingpart of a vascular malformation. In either casethere is commonly an associated subarachnoidhaemorrhage. Often there is no discoverablecause for the occurrence of a spontaneous in-tracerebral haematoma and in these cases sub-arachnoid haemorrhage is exceptional. Rarely anintracerebral haematoma develops in an area ofsoftening caused by a previous head injury (latepost-traumatic apoplexy). An expanding hae-matoma in the temporal lobe usually causes veryacute brain-stem compression.Arachnoid CystThe outer wall of an arachnoid cyst is formed by
arachnoid and the inner wall by pia. It is anexcessively rare type of congenital cyst which isusually found between the frontal and temporallobes in the Sylvian fissure. It contains clearyellow fluid of greatly raised protein content. Asthe cyst occupies part of the temporal fossa ittends to cause acute and sometimes fluctuatingbrain-stem compression. The importance ofarachnoid cysts is that their effects can be per-manently relieved by excision of the outerarachnoid wall.
Cerebral AbscessAbscesses occur more frequently in the temporal
lobe than elsewhere in the brain owing to theproximity of the middle ear and mastoid process.A temporal lobe abscess is more likely to arisefrom chronic infection of the middle ear than fromthe original acute infection. A metastatic abscess,usually from infection in the lungs, may developanywhere in the brain including the temporal lobe.A cerebral abscess may also be caused by a pene-trating head injury. Most cerebral abscessesmature in from one to two weeks and thereforethere is usually time for localizing and lateralizingsigns to be observed. A large abscess in thetemporal lobe may produce a contralateral
homonymous upper quadrantic field defect,contralateral facial paresis sometimes associatedwith hemiparesis, and, when the abscess is on thedominant side, nominal dysphasia or aphasia mayoccur. If untreated, the abscess with its ac-companying cerebral oedema causes progressivebrain-stem compression.GliomasThe commonest glioma encountered in the
temporal lobe is the glioblastoma multiforme. Itis a very malignant tumour which, because of itsrapid growth, its tendency to haemorrhagic in-farction and the surrounding cerebral oedema,commonly causes acute effects as the result ofmidbrain compression, and may be mistaken for astroke.
MeningiomasMedial sphenoid ridge meningiomas produce a
characteristic syndrome. Patients complain ofunilateral loss of vision and sometimes unilateralexophthalmos. There is homolateral opticatrophy, diminished visual acuity, and, in the earlystages, a central scotoma. There may be papil-loedema on the other side. (Optic atrophy withcentral scotoma on one side and papilloedemaon the other is known as the Foster-Kennedysyndrome.) When the optic tract is involvedinstead of the optic nerve, there is an homonymoushemianopia. Ophthalmoplegia is present in themajority of cases, and results from occlusion of theorbital fissure. The ophthalmic division of thetrigeminal nerve is affected in some cases; patientsthen complain of 'pins and needles' over theforehead where there is diminished or absentsensation. Temporal lobe epilepsy may occur,and is sometimes the presenting symptom. Thesedeeply placed tumours tend to envelop the internalcarotid artery and to adhere to the optic nerve.Middle sphenoid ridge meningiomas usually
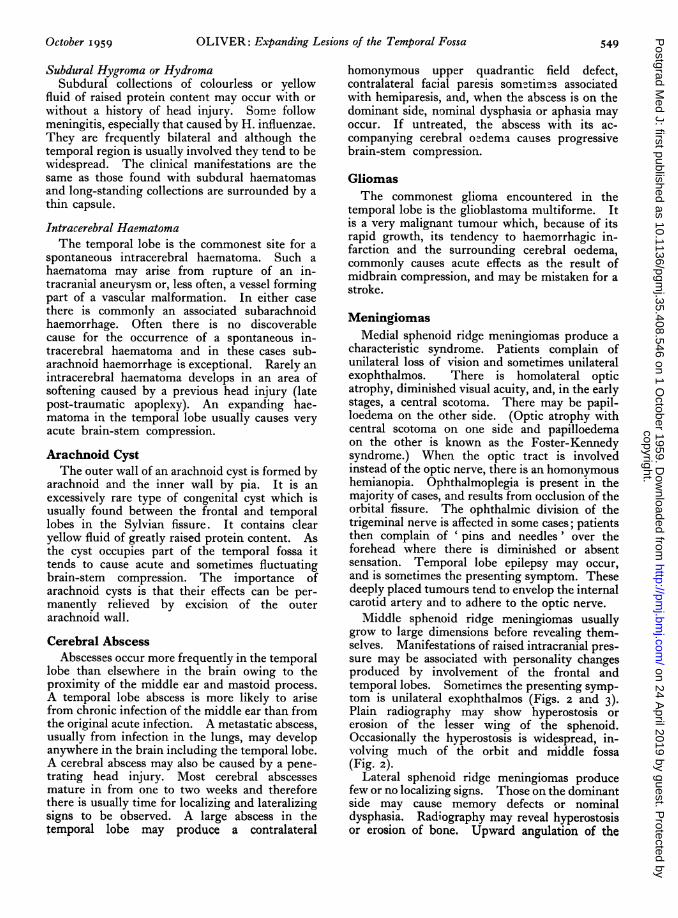
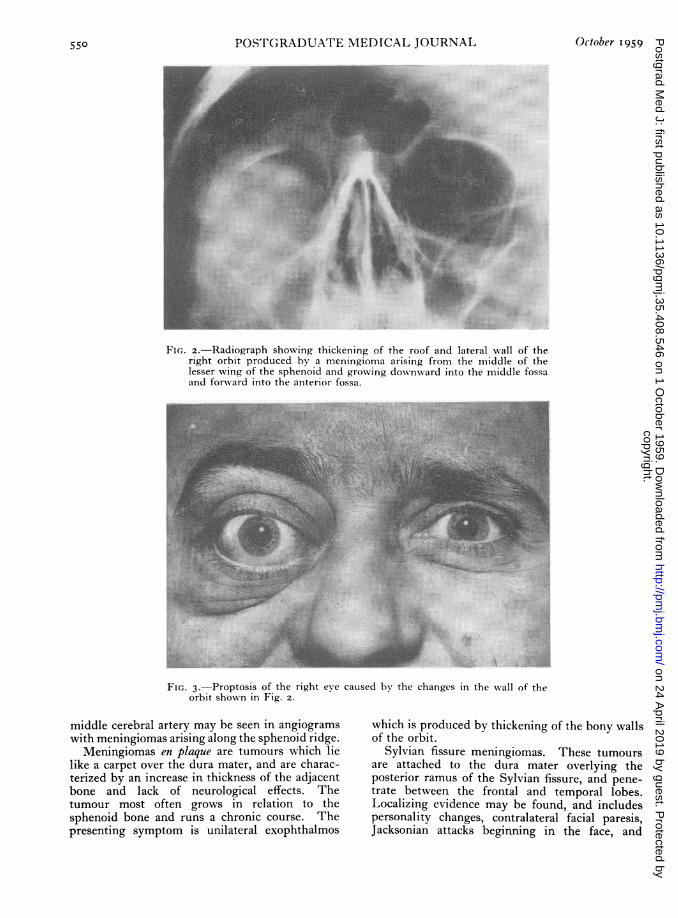
grow to large dimensions before revealing them-selves. Manifestations of raised intracranial pres-sure may be associated with personality changesproduced by involvement of the frontal andtemporal lobes. Sometimes the presenting symp-tom is unilateral exophthalmos (Figs. 2 and 3).Plain radiography may show hyperostosis orerosion of the lesser wing of the sphenoid.Occasionally the hyperostosis is widespread, in-volving much of the orbit and middle fossa(Fig. 2).
Lateral sphenoid ridge meningiomas producefew or no localizing signs. Those on the dominantside may cause memory defects or nominaldysphasia. Radiography may reveal hyperostosisor erosion of bone. Upward angulation of the
October 1959 549copyright.
on 24 April 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.408.546 on 1 October 1959. D
ownloaded from
550 POSTGRADUATE MEDICAL JOURNAL October I959
'iFs::.....
}e... t: :i. ::.. ii.,. ....'=.i: ~~~:i...:
*.:..
15 '.'.^. 2.
FIG. 2.-Radiograph showing thickening of the roof and lateral wall of theright orbit produced by a meningioma arising from the middle of thelesser wing of the sphenoid and growing downward into the middle fossaand forward into the anterior fossa.
~~~~i;i..!..!... ......z }..}--..~..........r'.::..::
.'....,.
' ,.fi ..' -
'··.i:r,
... '':i~"""LT""':`I::~ ;ll~lf.i...... ~.~.:l~:i,..,!.i ....ll
:i..:::·
D--in..'...
·:;
- E ... X - 2,. j :- - t -.;,.
-~~~~~js1-
FI,. 3.-Proptosis of the right eve caused by the changes in the wall of theorbit shown in Fig. 2.
middle cerebral artery may be seen in angiogramswith meningiomas arising along the sphenoid ridge.
Meningiomas en plaque are tumours which lielike a carpet over the dura mater, and are charac-terized by an increase in thickness of the adjacentbone and lack of neurological effects. Thetumour most often grows in relation to thesphenoid bone and runs a chronic course. Thepresenting symptom is unilateral exophthalmos
which is produced by thickening of the bony wallsof the orbit.
Sylvian fissure meningiomas. These tumoursare attached to the dura mater overlying theposterior ramus of the Sylvian fissure, and pene-trate between the frontal and temporal lobes.Localizing evidence may be found, and includespersonality changes, contralateral facial paresis,Jacksonian attacks beginning in the face, and
copyright. on 24 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.408.546 on 1 O
ctober 1959. Dow
nloaded from
October 1959 OLIVER: Expanding Lesions of t.'e Temporal Fossa 551nominal dysphasia with tumours on the dominantside.
InvestigationsLumbar Puncture
This procedure should not be carried out in thepresence of raised intracranial pressure due to anexpanding lesion, for it may precipitate or aggra-vate brain-stem compression, sometimes with afatal result. Furthermore, lumbar puncture isunlikely to yield worth-while information.
Plain RadiographyFractures may be confirmed or revealed. In
extradural haematoma, a fracture may be shownrunning across the markings of the middlemeningeal vessels, although some extraduralhaematomas occur without a fracture.
Bulging of the temporal fossa and/or elevationof the lesser wing of the sphenoid may be presentwith a long standing lesion, e.g. chronic subduralhaematoma, chronic subdural hygroma, arachnoidcyst.
If calcified, the pineal gland is usually seen to bedisplaced away from the side of a space-occupyinglesion.
In early childhood, the presence of raised in-tracranial pressure is revealed by separation of thesutures and exaggerated convolutional markings
Increased width and tortuosity of vascularchannels, occasionally with enlargement of theforamen spinosum, may be seen with meningiomas.Sometimes there are adventitious vascular channelsconverging towards the site of a meningioma.
Increase in thickness of the lesser and greaterwings of the sphenoid, the roof and lateral wall ofthe orbit, occurs with most meningiomas of thelesser wing of the sphenoid and meningiomas enplaque (Fig. 2). Rarefaction or total destructionof the posterior clinoid processes may be causedby long-standing raised intracranial pressure ordirectly by the growth of adjacent meningiomas.Increased size and density of one posteriorclinoid process may be seen with meningiomas ofthe medial end of the lesser wing of the sphenoid.
Calcification can be demonstrated radiologicallyin some meningiomas, some astrocytomas and mostoligodendrogliomas.Carotid AngiographyThis is the most valuable investigation for the
demonstration of space-occupying lesions in thetemporal fossa. It is preferable to ventriculo-graphy which dangerously increases intracranialpressure and aggravates or produces brain-stemcompression. Angiography is seldom indicated todemonstrate the presence of an extradural haema-toma, for the march of events is usually too rapidin this condition.
.. : t f i ::
*2.. .. .... ...........
Mi:
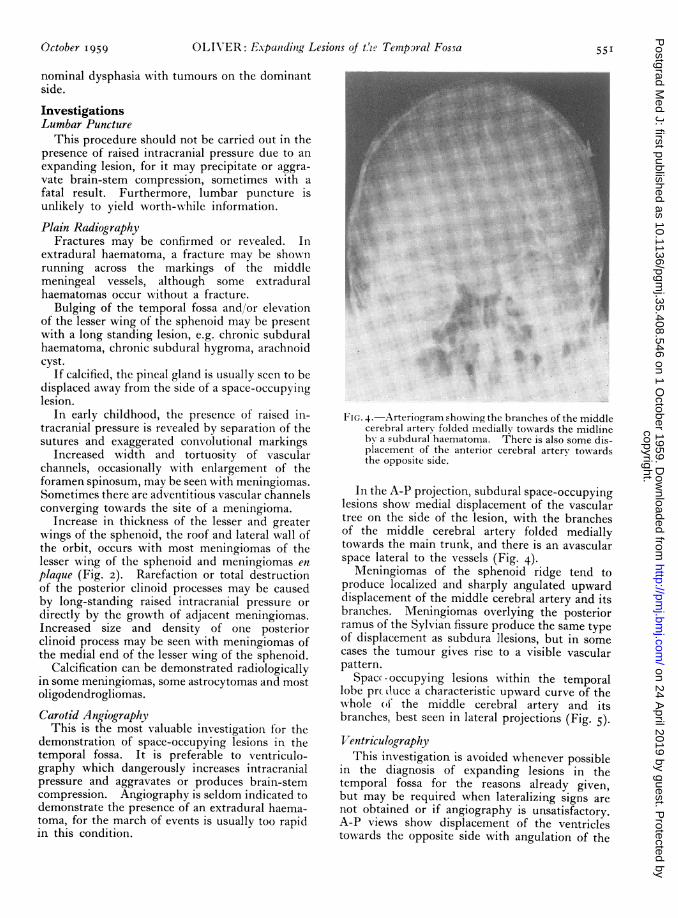
FIG. 4.-Arteriogram showing the branches of the middlecerebral artery folded medially towards the midlineby a subdural haematoma. There is also some dis-placement of the anterior cerebral artery towardsthe opposite side.
In the A-P projection, subdural space-occupyinglesions show medial displacement of the vasculartree on the side of the lesion, with the branchesof the middle cerebral artery folded mediallytowards the main trunk, and there is an avascularspace lateral to the vessels (Fig. 4).Meningiomas of the sphenoid ridge tend to
produce localized and sharply angulated upwarddisplacement of the middle cerebral artery and itsbranches. Meningiomas overlying the posteriorramus of the Sylvian fissure produce the same typeof displacement as subdura ]lesions, but in somecases the tumour gives rise to a visible vascularpattern.
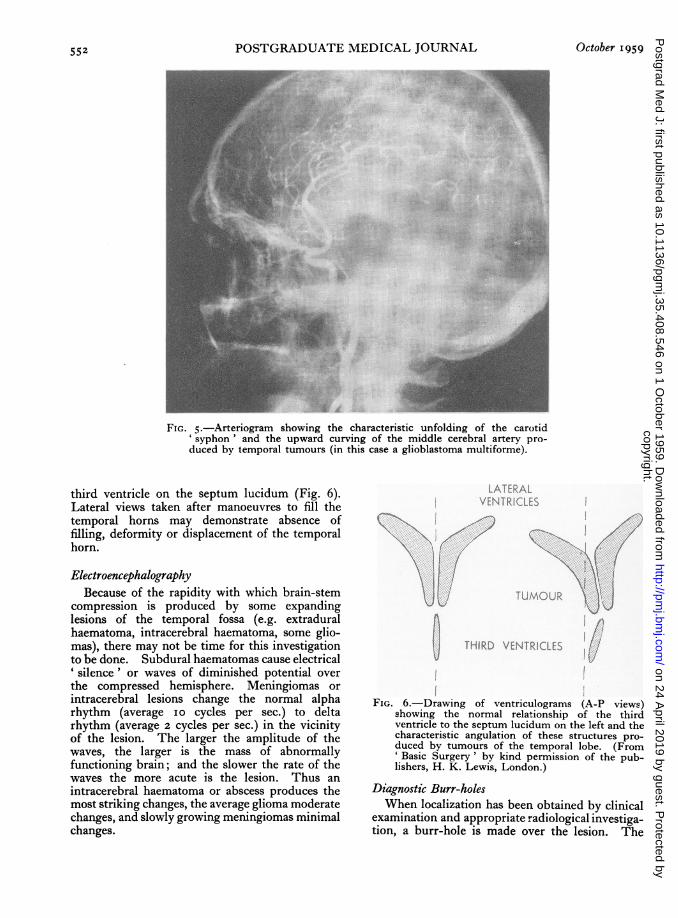
Space-occupying lesions within the temporallobe prtduce a characteristic upward curve of thewhole (o the middle cerebral artery and itsbranches, best seen in lateral projections (Fig. 5).VentriculographyThis investigation is avoided whenever possible
in the diagnosis of expanding lesions in thetemporal fossa for the reasons already given,but may be required when lateralizing signs arenot obtained or if angiography is unsatisfactory.A-P views show displacement of the ventriclestowards the opposite side with angulation of the
copyright. on 24 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.408.546 on 1 O
ctober 1959. Dow
nloaded from
552 POSTGRADUATE MEDICAL JOURNAL October 1959
···'· ::. ..:a. ::.
..",...'::::
..
*. :i?,:::. ::.:":
':;;' 6·".M's-.
.::,.... :: ::. .^.^3: ::.... .. ........
FIG. 5.-Arteriogram showing the characteristic unfolding of the carotid'syphon' and the upward curving of the middle cerebral artery pro-duced by temporal tumours (in this case a glioblastoma multiforme).
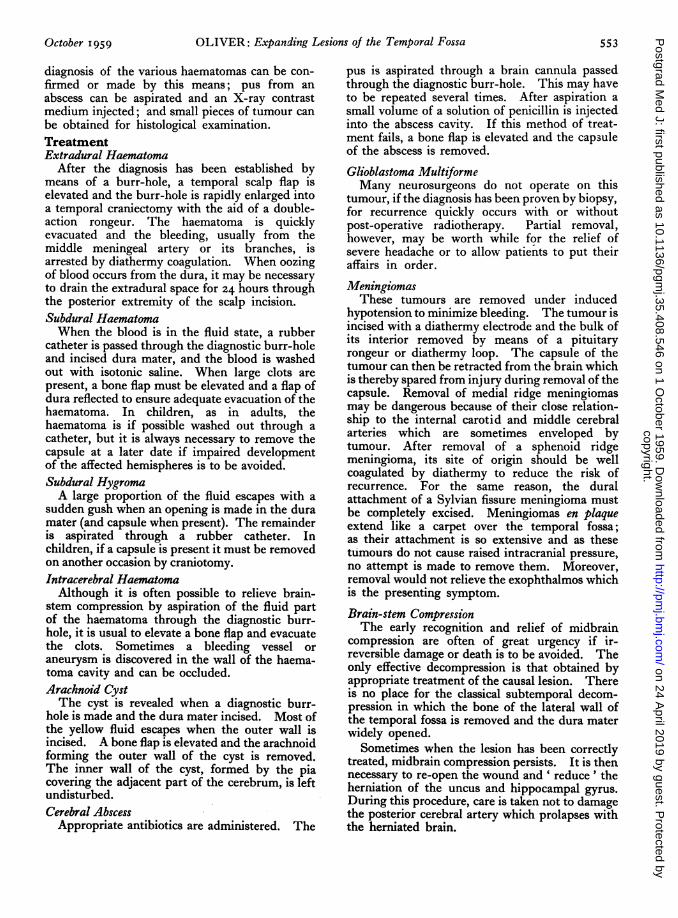
third ventricle on the septum lucidum (Fig. 6).Lateral views taken after manoeuvres to fill thetemporal horns may demonstrate absence offilling, deformity or displacement of the temporalhorn.
ElectroencephalographyBecause of the rapidity with which brain-stem
compression is produced by some expandinglesions of the temporal fossa (e.g. extraduralhaematoma, intracerebral haematoma, some glio-mas), there may not be time for this investigationto be done. Subdural haematomas cause electrical' silence' or waves of diminished potential overthe compressed hemisphere. Meningiomas orintracerebral lesions change the normal alpharhythm (average io cycles per sec.) to deltarhythm (average 2 cycles per sec.) in the vicinityof the lesion. The larger the amplitude of thewaves, the larger is the mass of abnormallyfunctioning brain; and the slower the rate of thewaves the more acute is the lesion. Thus anintracerebral haematoma or abscess produces themost striking changes, the average glioma moderatechanges, and slowly growing meningiomas minimalchanges.
LATERALVENTRICLES I
TUMOUR
THIRD VENTRICLES
I IFIG. 6.-Drawing of ventriculograms (A-P views)
showing the normal relationship of the thirdventricle to the septum lucidum on the left and thecharacteristic angulation of these structures pro-duced by tumours of the temporal lobe. (From'Basic Surgery' by kind permission of the pub-lishers, H. K. Lewis, London.)
Diagnostic Burr-holesWhen localization has been obtained by clinical
examination and appropriate radiological investiga-tion, a burr-hole is made over the lesion. The
copyright. on 24 A
pril 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.408.546 on 1 O
ctober 1959. Dow
nloaded from
OLIVER: Expanding Lesions of the Temporal Fossa
diagnosis of the various haematomas can be con-firmed or made by this means; pus from anabscess can be aspirated and an X-ray contrastmedium injected; and small pieces of tumour canbe obtained for histological examination.TreatmentExtradural Haematoma
After the diagnosis has been established bymeans of a burr-hole, a temporal scalp flap iselevated and the burr-hole is rapidly enlarged intoa temporal craniectomy with the aid of a double-action rongeur. The haematoma is quicklyevacuated and the bleeding, usually from themiddle meningeal artery or its branches, isarrested by diathermy coagulation. When oozingof blood occurs from the dura, it may be necessaryto drain the extradural space for 24 hours throughthe posterior extremity of the scalp incision.Subdural HaematomaWhen the blood is in the fluid state, a rubber
catheter is passed through the diagnostic burr-holeand incised dura mater, and the blood is washedout with isotonic saline. When large clots arepresent, a bone flap must be elevated and a flap ofdura reflected to ensure adequate evacuation of thehaematoma. In children, as in adults, thehaematoma is if possible washed out through acatheter, but it is always necessary to remove thecapsule at a later date if impaired developmentof the affected hemispheres is to be avoided.Subdural HygromaA large proportion of the fluid escapes with a
sudden gush when an opening is made in the duramater (and capsule when present). The remainderis aspirated through a rubber catheter. Inchildren, if a capsule is present it must be removedon another occasion by craniotomy.Intracerebral Haematoma
Although it is often possible to relieve brain-stem compression by aspiration of the fluid partof the haematoma through the diagnostic burr-hole, it is usual to elevate a bone flap and evacuatethe clots. Sometimes a bleeding vessel oraneurysm is discovered in the wall of the haema-toma cavity and can be occluded.Arachnoid CystThe cyst is revealed when a diagnostic burr-
hole is made and the dura mater incised. Most ofthe yellow fluid escapes when the outer wall isincised. A bone flap is elevated and the arachnoidforming the outer wall of the cyst is removed.The inner wall of the cyst, formed by the piacovering the adjacent part of the cerebrum, is leftundisturbed.Cerebral Abscess
Appropriate antibiotics are administered. The
pus is aspirated through a brain cannula passedthrough the diagnostic burr-hole. This may haveto be repeated several times. After aspiration asmall volume of a solution of penicillin is injectedinto the abscess cavity. If this method of treat-ment fails, a bone flap is elevated and the capsuleof the abscess is removed.
Glioblastoma MultiformeMany neurosurgeons do not operate on this
tumour, if the diagnosis has been proven by biopsy,for recurrence quickly occurs with or withoutpost-operative radiotherapy. Partial removal,however, may be worth while for the relief ofsevere headache or to allow patients to put theiraffairs in order.
MeningiomasThese tumours are removed under induced
hypotension to minimize bleeding. The tumour isincised with a diathermy electrode and the bulk ofits interior removed by means of a pituitaryrongeur or diathermy loop. The capsule of thetumour can then be retracted from the brain whichis thereby spared from injury during removal of thecapsule. Removal of medial ridge meningiomasmay be dangerous because of their close relation-ship to the internal carotid and middle cerebralarteries which are sometimes enveloped bytumour. After removal of a sphenoid ridgemeningioma, its site of origin should be wellcoagulated by diathermy to reduce the risk ofrecurrence. For the same reason, the duralattachment of a Sylvian fissure meningioma mustbe completely excised. Meningiomas en plaqueextend like a carpet over the temporal fossa;as their attachment is so extensive and as thesetumours do not cause raised intracranial pressure,no attempt is made to remove them. Moreover,removal would not relieve the exophthalmos whichis the presenting symptom.Brain-stem CompressionThe early recognition and relief of midbrain
compression are often of great urgency if ir-reversible damage or death is to be avoided. Theonly effective decompression is that obtained byappropriate treatment of the causal lesion. Thereis no place for the classical subtemporal decom-pression in which the bone of the lateral wall ofthe temporal fossa is removed and the dura materwidely opened.
Sometimes when the lesion has been correctlytreated, midbrain compression persists. It is thennecessary to re-open the wound and ' reduce' theherniation of the uncus and hippocampal gyrus.During this procedure, care is taken not to damagethe posterior cerebral artery which prolapses withthe herniated brain.
October I959 553copyright.
on 24 April 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.408.546 on 1 October 1959. D
ownloaded from