Embed Size (px)
Citation preview
69
Expert Review Examination of the Respiratory System Dr Fahd Mahmood1, Prof Robert J O Davies2 and Dr John M Wrightson3 ……………………………………………………………………………………………………………………………………..
The Journal of Clinical Examination 2011 (11): 69-89
Abstract This article describes a comprehensive method for performing an examination of the Respiratory System. The signs of common and important diseases that affect the respiratory system are discussed. It is based on a thorough review of the literature and is consistent with The Principles of Clinical Examination. We welcome responses to this article which provide evidence for improvements to the method described here but in the meantime we recommend this as a peer-reviewed and evidence-based method for the Examination of the Respiratory System. Word count: 8,708 (excluding abstract, figures, tables and references). Key words: physical examination, auscultation, palpation, percussion, respiratory. Address for correspondence: [email protected] Author affiliations: 1Foundation House Officer, Glasgow Royal Infirmary, NHS Greater Glasgow & Clyde. 2Professor of Respiratory Medicine, University of Oxford and Consultant Physician, Oxford Radcliffe Hospitals NHS Trust. 3NIHR Oxford BRC Clinical Research Fellow and Specialist Registrar, Oxford Radcliffe Hospitals NHS Trust. …………………………………………………………………………………………………………………………………….. Introduction The Principles of Examination of the Respiratory System Authors have proposed various methods for performing an examination of the respiratory system in medical literature. At best, most of the methods advocated can be described as ‘expert opinion’ rather than having a stronger evidence base; the best examination method is controversial. Where there is no good evidence we have taken a pragmatic approach guided by The Principles of Clinical Examination [1]. This article aims to synthesize evidence from medical literature together with descriptions advocated by major clinical medicine textbooks to produce a method suitable for medical school examinations, post-graduate examinations and routine clinical practice. The examination routine described here is designed to detect the signs of common and important respiratory diseases, together with multisystem disorders that also have respiratory sequelae, such as rheumatoid arthritis. An astute physician will always be vigilant for such multisystem disorders and use findings to guide further examination of non-respiratory systems.
This article describes a comprehensive and idealised version of the clinical examination of the respiratory system, which can be modified when a more focused examination is required in clinical practice. For acutely unwell patients, an ‘Airway, Breathing, Circulation, Disability, Exposure – ABCDE’ approach may be more appropriate. When the examination of the respiratory system is performed as part of medical school or post-graduate examinations it will be observed by at least one official examiner. In these circumstances it is not only necessary to perform a competent examination it is also necessary to be seen to be performing a complete examination. This includes communicating to the examiner when signs have been detected and justifying ad hoc decisions to modify the examination routine. An approach to dealing with these difficulties is beyond the scope of this article but where relevant we provide some suggestions for dealing with specific issues. Clinical examination is just one part of a comprehensive assessment of the patient which usually includes bedside investigations such as pulse oximetry and measurement of blood pressure. This account includes all the bedside tests relevant to the examination of the respiratory system. Formal investigations such as chest radiographs and full lung function testing do not form part of the

70
clinical examination and are therefore beyond the scope of this article. Anatomy and physiology Air enters through the oropharanx and nasopharanx passing through the larynx to the trachea which commences at the level of the cricoid cartilage in the neck (C6) and terminates at the carina into the left and right main bronchi (at the angle of Louis (T4/5)). The right bronchus is more vertical than the left; hence inhaled objects and chemical pneumonitis secondary to aspiration are more likely to be found on the right side. The main bronchi divide into lobar bronchi, which further subdivide into segmental bronchi. These segmental bronchi each feed into a bronchopulmonary segment of the lung. Alveoli within these segments allow gas exchange, the primary function of the lung, to occur. The lungs are surrounded by continuous membrane, the pleura, that is folded back on itself to create two layers: the visceral (inner) and parietal (outer) pleura. The visceral pleura is attached to the surface of the lung and the parietal pleura, which is innervated by the intercostal nerves, to the thoracic cavity. The space between these layers is referred to as the pleural cavity and contains a small amount (~10ml) of pleural fluid. Surface tension of the pleural fluid allows the lung to expand with inhalation, however in the case of pneumothorax, gas in the pleural cavity, this surface tension is lost and the lung cannot expand. Each lung is divided by fissures into lobes, the right lung has three lobes whilst the left has two (Figure 1). During normal inspiration, contraction of the intercostal muscles increases the transverse diameter of the thorax whilst contraction of the diaphragm increases the vertical length of the thorax. These changes increase the volume of the lungs, thereby decreasing intrapulmonary pressure relative to atmospheric pressure; allowing air into the lungs. In deep inspiration, the accessory muscles of respiration further maximise thoracic capacity. Overlying the lungs, the rib cage protects the lungs. In mid inspiration, the lungs’ lower borders cross the 6th rib in the mid clavicular line, the 8th in the mid axillary line and reach the 10th rib posteriorly. An appreciation of the anatomy and physiology of the lungs will allow accurate interpretation of any examination findings.
Figure 1a (top) and 1b (bottom). The surface anatomy of the lungs showing the right upper (RU), right middle (RM), right lower (RL), left upper (LU) and left lower (LL) lobes.
Figure 1c The cervical lymph nodes, including A) submental, B) submandibular, C) Jugular, D) pre-auricular, E) post-auricular F), occipital, G) posterior triangle and H) supraclavicular nodes. Common diseases Pulmonary pathology is varied and diverse in nature. Through your examination, you may elucidate signs relating to the following common conditions. Lung disease can be classified in different ways. See Table 1.

71
Obstructive Disease caused by obstruction of airways
Asthma Chronic Obstructive Pulmonary disease
Restrictive Disease caused by restricted lung expansion
Interstitial lung disease Asbestosis Pulmonary fibrosis Sarcoidosis
Infectious Due to infection of the lung
Pneumonia
Inflammatory Disease related to inflammatory response in the lung
Cystic fibrosis Acute respiratory distress syndrome
Vascular Pathology related to pulmonary vasculature
Pulmonary embolus Pulmonary oedema Haemorrhage (eg. Goodpasture’s syndrome)
Pleural cavity disease
Pathology affects pleural space
Pneumothorax Pleural plaques/mesothelioma
Table 1 Categories of lung disease Literature Review In developing this article, a literature review of publications related to respiratory examination was performed. The ‘diagnosis category’ of the PubMed Clinical Queries database was searched, using the ‘narrow, specific search’ filters with the following terms; (respiratory AND examination) (pleural AND (percussion OR auscultation)) (pneumonia AND (percussion OR auscultation)) (bronchiectasis AND (percussion OR auscultation)) (fibrosis AND (percussion OR auscultation)) (((lung OR bronchial) AND (cancer OR malignancy)) AND (percussion OR auscultation)) A further PubMed search was performed for clinical prediction rules, using the following strategy; (clinical prediction rule) AND (respiratory system)
(clinical prediction rule) AND (pulmonary OR respiratory) Retrieved articles from all search strategies were reviewed for relevance. Articles from the first strategy were also reviewed for the presence of clinical prediction rules. Review was limited to articles published in English, pertinent to humans. Only articles available through the University of Oxford or the National Health Service agreement were examined.
The Journal of the American Medical Association’s “Rational Clinical Examination” series [2] was reviewed, with all entries under ‘Pulmonary Diseases’ examined. The British Medical Journal’s Clinical Evidence series [3] was also examined. All reviews under ‘Respiratory disorders (acute)’ and ‘Respiratory disorders (chronic)’ were inspected. Evidence Based Medicine was also searched, with articles in Evidence Based Medicine collections relevant to ‘EBM Diagnosis’ and ‘EBM Clinical Prediction Guides’ fully reviewed.
The following textbooks of clinical examination were searched:
Clinical Examination: A Systematic Guide to Physical Diagnosis[4] Macleod’s Clinical Examination[5] Sapira’s Art and Science of Bedside Diagnosis[6] Evidence Based Physical Diagnosis[7] Preparation Clinical examination should ideally take place in a warm environment which is private and has good illumination. Make sure you have the necessary equipment available as listed in Table 2. The examiner should be appropriately dressed and a chaperone should be present if appropriate. Wash your hands, introduce yourself to the patient and obtain informed consent. Next confirm the patient’s identity (if this has not been done already), ensure he/she is positioned appropriately, lying on a bed or examination couch at an incline of approximately forty five degrees, and that there is adequate exposure. Ideal exposure is from the waist upwards but in practice less complete forms of exposure may be adequate and examiners should be pragmatic.
Stethoscope Peak expiratory flow meter Pulse oximeter Thermometer
Table 2 Equipment required for the respiratory examination

72
Finally check the patient is comfortable and does not have any pain. You must be sensitive and responsive to signs of pain at this stage and throughout the examination. If necessary ask the patient before you proceed with a maneuver if it is likely to cause any pain. Beginning the Examination Start from the end of the bed with an initial global inspection of the patient and their surroundings.
Figure 2 Initial global inspection with patient appropriately exposed Consider explaining what you are doing beforehand to avoid embarrassment. Note the environment in which the examination is taking place and look for walking aids, medical equipment and any other relevant items. Next look for signs of disease. Most signs are best detected during the detailed examination of individual anatomical areas but some signs such as cachexia, the use of accessory muscles of respiration (sternocleidomastoids, platysma and the strap muscles of the neck: sternothyroid, sternohyoid, thyrohyoid and omohyoid[8]) and the tripod position (sitting leaning forward with hands supported on the knees) which is frequently seen in patients in respiratory distress are best detected from the end of the bed. Any sign is potentially relevant and it is not possible to provide a full list here but the most important signs and their significance are described below. Look for equipment used to deliver oxygen therapy, inhalers and equipment for drug nebulisation. Look for a sputum pot and if a sample of sputum is available you should inspect it. Sputum is produced by the airways and should contain very little saliva. Note the colour and volume of the sputum and try to categorise. See Table 3. Whilst speaking to the patient note any abnormalities in the character of their voice, the ability to finish sentences in one breath and assess for the presence and character of any cough. See Table 4. A hoarse voice may be a sign of laryngitis, laryngeal cancer or recurrent laryngeal nerve palsy.
Recurrent laryngeal nerve palsy can be caused by invasion of the nerve by lung cancer [4]. The inability to finish sentences in one breath implies significant respiratory distress and has prognostic significance; for example in exacerbations of asthma. Next assess the rate, in breaths per minute, and the pattern of respiration. The rate can be affected if the patient is aware that it is being measured and many authors recommend doing it covertly later in the examination but it is justifiable to do it at this point. Suitable points for covert measurement are: whilst palpating the radial pulse, during close inspection of the chest, during palpation of the chest, during auscultation of the chest. The most time-efficient and accurate method is to count the number of breaths in a specific period, such as twenty seconds, and then calculate the number of breaths per minute. The time period should be defined using a watch or another timepiece. With experience it is possible to estimate the respiratory rate after listening for a brief undefined period but this is likely to be less accurate. The normal respiratory rate for an adult is 8-20 breaths per minute. Less than 8/min is bradypnoea and greater than 20/min is tachypnoea. Is the pattern of breathing normal or abnormal? Normally, inspiration is an active process being 75% diaphragmatic and 25% thoracic, whilst expiration occurs passively; the ratio of the length of inspiration to that of expiration is normally 1:2. Tachypnoea and bradypneoea can occur in a variety of situations as detailed in Table 5. Cheyne-Stokes ventilation describes a cyclical pattern of ventilation in which there is a periodic increasing rate and depth of ventilation followed by a decreased respiratory rate and effort, eventually reaching a state of temporary hypopnoea or apnoea. Cheyne-Stokes ventilation can be observed in patients with conditions that affect blood gas buffering such as congestive heart failure, carbon monoixide poisoning and toxic metabolic encephalopathy. It can also be present in conditions affecting the respiratory centres in the brainstem such as stroke, traumatic brain injury and brain tumours. Finally, it is also observed in palliative care patients and has also been reported as a normal finding during sleep in the elderly [10]. Kussmaul respiration describes deep sighing respirations, although patients may not feel subjectively yspnoeic; it is observed in metabolic acidosis[10]. d

73
Tachypnoea Bradypnoea Airway obstruction (Asthma, COPD)
Exhaustion in severe airway obstruction
Pneumonia Sedation Pulmonary Fibrosis Raised intracranial
pressure Pulmonary embolism Opiate overdose Pneumothorax Intoxication Pleural Effusion Cardiac Failure
Table 5 Causes of tachypnoea and bradypnoea
Assess if the patient is in respiratory distress; in which tachypnoea and increased respiratory effort (indicated by the use of accessory muscles, the tripod position and nasal flaring may be seen).
Look for pursing of the lips, where the lips are brought together on expiration, characteristic of patients with chronic obstructive pulmonary disease (EB1 and Clinical Prediction Rule 1). Lip pursing is thought to generate positive end-expiratory pressure, helping reduce dynamic airway collapse during expiration[7]. Listen for the presence of stridor, which is a harsh inspiratory noise, indicating upper airway obstruction, potentially secondary to a laryngeal tumour, bilateral vocal cord palsy or, more acutely, due to anaphylaxis. If you are unsure, ask the patient to cough, then take deep breaths with their mouth open[5]. Any stridor should always be investigated. Also listen for an audible expiratory wheeze, secondary to reduced lower airways calibre or for inspiratory ‘white noise’ - irregular, constantly varying in frequency and amplitude[17]. Both findings are present in patients with chronic obstructive pulmonary disease (EB1 and Clinical Prediction Rule 1) (COPD) or asthma (EB2). The Hands Move to the right-hand side of the patient [1] and examine the hands. Ask the patient to hold-out their hands and hold them gently with yours. Begin by looking at the fingers, especially the finger tips, and the nails. Examine for finger clubbing. See The JCE Expert Review: Examination for Finger Clubbing19 for a review of this examination. Other signs in the hand may include: nail changes (Table 6), tar staining indicative of recent smoking [5], wasting of the small muscles of the hand, especially at the thenar and hypothenar eminences,
seen when apical lung tumours (Pancoast’s tumour) impinge on the C8/T1 nerve roots, and changes seen in rheumatoid arthritis which may be associated with bronchiectasis and pulmonary fibrosis [7]. Peripheral cyanosis may also be detected in the hands [5] giving a blue colour to the tissues caused by the presence of deoxygenated haemoglobin. Note that, in the absence of central cyanosis, this is reflective of peripheral vasoconstriction and stasis of blood in the peripheries. Central cyanosis is seen in the tongue and lips due to desaturation of central arterial blood.
Figure 3 Examination of the hands for clubbing in A) non clubbed and B) clubbed fingers Ask the patient to hold their arms out in front of them, elbows extended, for about ten seconds and assess if they have a tremor. Then, maintaining this position, ask them to fully dorsiflex their wrists and hold that position for about thirty seconds whilst you closely observe for asterixis (Figure 4). It is best to give these instructions whilst demonstrating the position at the same time. Asterixis is manifest by sudden loss of dorsiflexion causing flexion movements towards the neutral position at the wrist and may be a sign of carbon dioxide retention (‘carbon dioxide flap’) or hepatic encephalopathy (‘liver flap’).
74
Nail abnormality
Definition Associated condition
Koilonychia Transverse and longitudinal concavity – giving a spoon shaped nail
Iron deficiency anaemia
Onycholysis Separation of nail plate from nail bed, leaving a white discolouration.
Sarcoidosis, ankylosing spondylitis
Yellow Nail Slow growing nail, with ‘heaped up’ appearance. The lunula disappears and the nail shows a yellow hue.
Pleural effusion, bronchiectasis
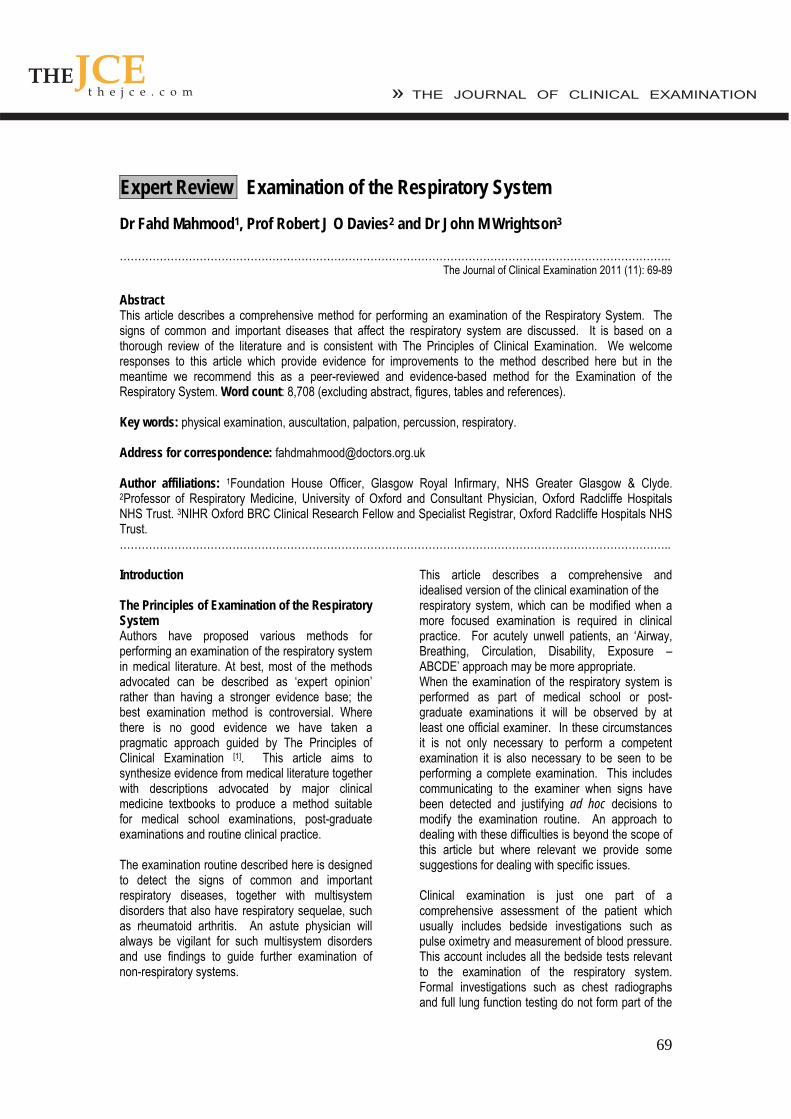
Table 6 Nail findings in respiratory disease
Figure 4 Examining for Asterixis. Radial Pulse Palpate the radial pulse and assess its rate, rhythm and character. For a fuller account of the cardiovascular examination and signs please the relevant Journal of Clinical Examination Review [20]. Pulsus paradoxus is a sign especially relevant to the respiratory examination, it is considered in EB3. The Face Begin by looking at the eyes. Assess pupil size and symmetry. Look at the eyelids, the normal upper lid lies 1.5mm below the superior corneal limbus. Ptosis refers to drooping of the upper eyelid, this can be partial or complete. Enophthalmos is a sign which refers to posterior displacement of the eye, a difference of 2mm between the eyes is usually evident on examination. Look at the facial skin for rashes and anhydrosis (loss of sweating). Ask the patient to open their
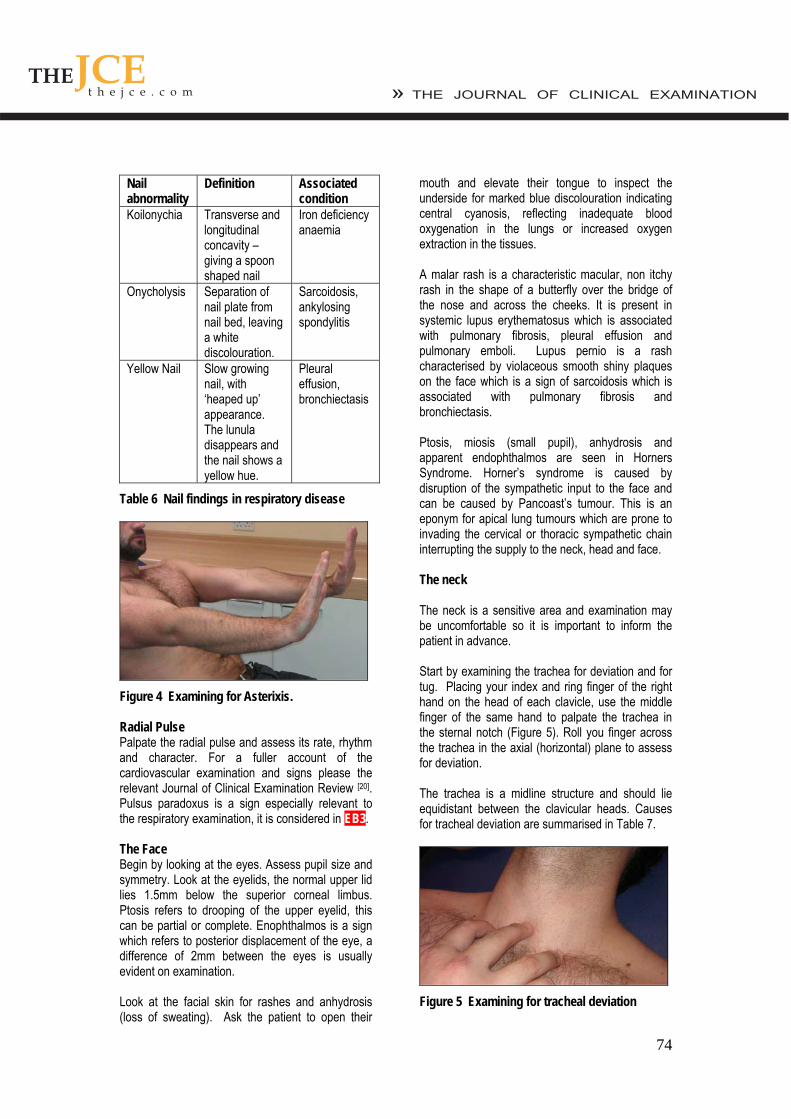
mouth and elevate their tongue to inspect the underside for marked blue discolouration indicating central cyanosis, reflecting inadequate blood oxygenation in the lungs or increased oxygen extraction in the tissues. A malar rash is a characteristic macular, non itchy rash in the shape of a butterfly over the bridge of the nose and across the cheeks. It is present in systemic lupus erythematosus which is associated with pulmonary fibrosis, pleural effusion and pulmonary emboli. Lupus pernio is a rash characterised by violaceous smooth shiny plaques on the face which is a sign of sarcoidosis which is associated with pulmonary fibrosis and bronchiectasis. Ptosis, miosis (small pupil), anhydrosis and apparent endophthalmos are seen in Horners Syndrome. Horner’s syndrome is caused by disruption of the sympathetic input to the face and can be caused by Pancoast’s tumour. This is an eponym for apical lung tumours which are prone to invading the cervical or thoracic sympathetic chain interrupting the supply to the neck, head and face. The neck The neck is a sensitive area and examination may be uncomfortable so it is important to inform the patient in advance. Start by examining the trachea for deviation and for tug. Placing your index and ring finger of the right hand on the head of each clavicle, use the middle finger of the same hand to palpate the trachea in the sternal notch (Figure 5). Roll you finger across the trachea in the axial (horizontal) plane to assess for deviation. The trachea is a midline structure and should lie equidistant between the clavicular heads. Causes for tracheal deviation are summarised in Table 7.
Figure 5 Examining for tracheal deviation
75
Table 7 Causes of tracheal displacement[9]
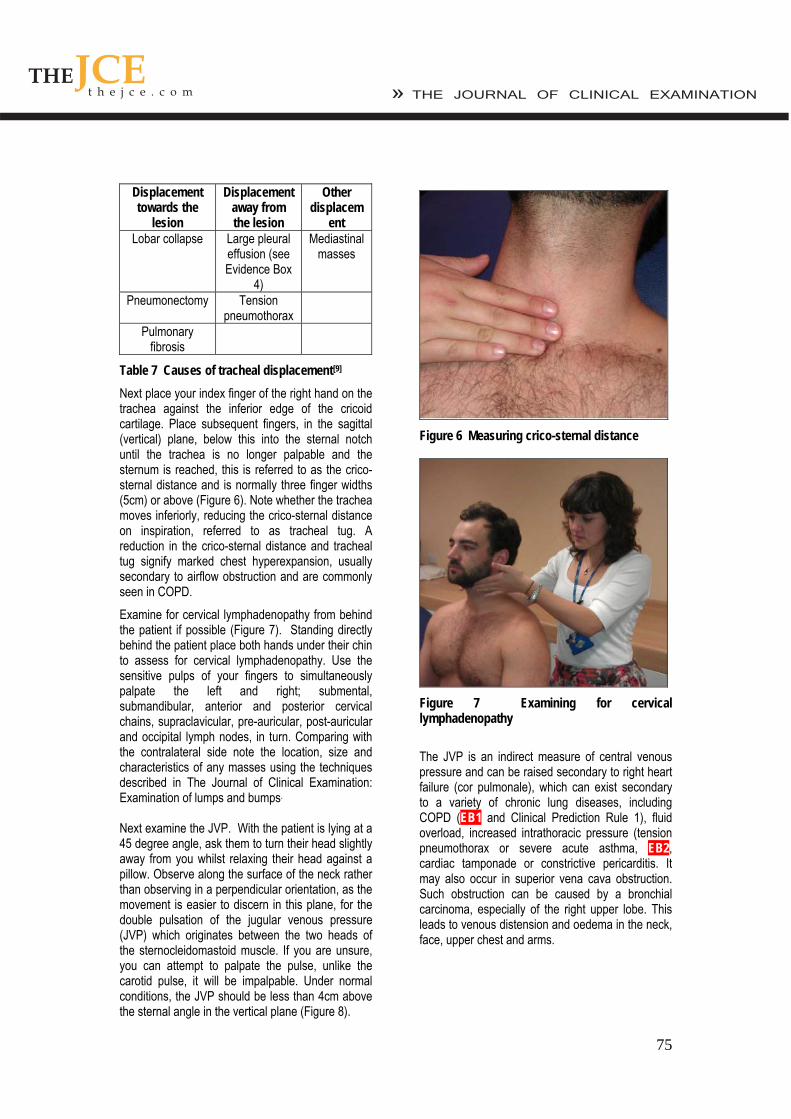
Next place your index finger of the right hand on the trachea against the inferior edge of the cricoid cartilage. Place subsequent fingers, in the sagittal (vertical) plane, below this into the sternal notch until the trachea is no longer palpable and the sternum is reached, this is referred to as the crico-sternal distance and is normally three finger widths (5cm) or above (Figure 6). Note whether the trachea moves inferiorly, reducing the crico-sternal distance on inspiration, referred to as tracheal tug. A reduction in the crico-sternal distance and tracheal tug signify marked chest hyperexpansion, usually secondary to airflow obstruction and are commonly seen in COPD.
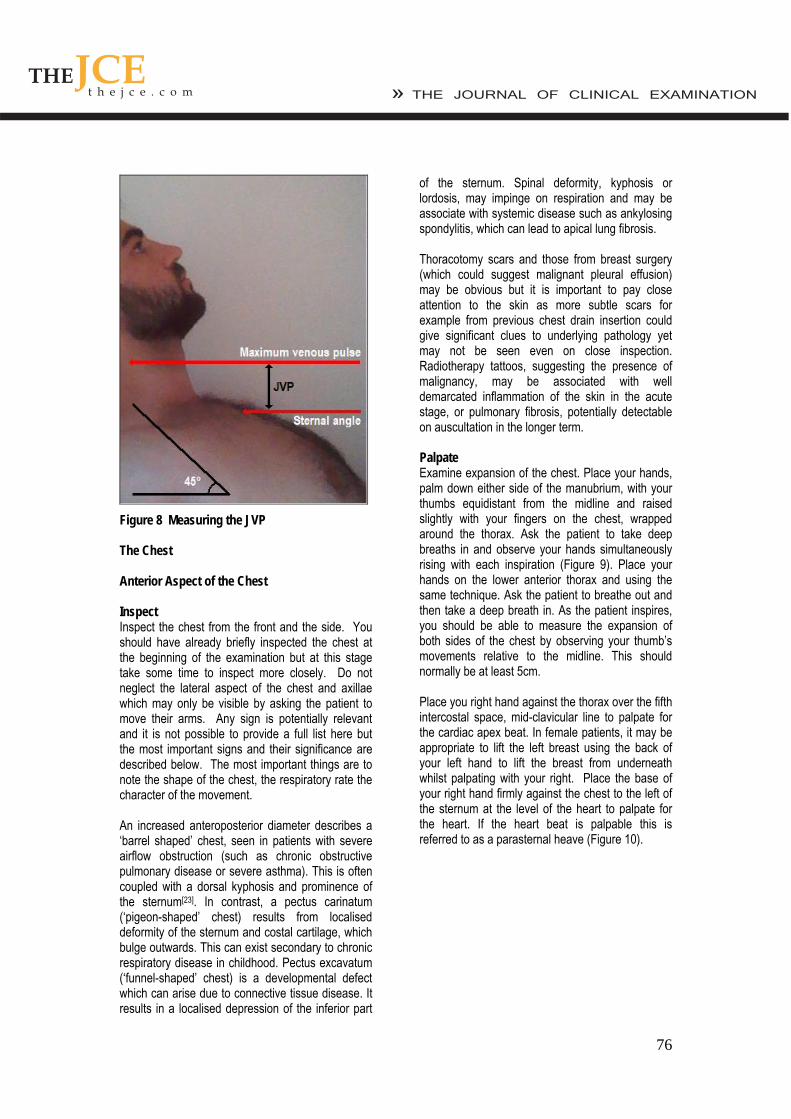
Examine for cervical lymphadenopathy from behind the patient if possible (Figure 7). Standing directly behind the patient place both hands under their chin to assess for cervical lymphadenopathy. Use the sensitive pulps of your fingers to simultaneously palpate the left and right; submental, submandibular, anterior and posterior cervical chains, supraclavicular, pre-auricular, post-auricular and occipital lymph nodes, in turn. Comparing with the contralateral side note the location, size and characteristics of any masses using the techniques described in The Journal of Clinical Examination: Examination of lumps and bumps. Next examine the JVP. With the patient is lying at a 45 degree angle, ask them to turn their head slightly away from you whilst relaxing their head against a pillow. Observe along the surface of the neck rather than observing in a perpendicular orientation, as the movement is easier to discern in this plane, for the double pulsation of the jugular venous pressure (JVP) which originates between the two heads of the sternocleidomastoid muscle. If you are unsure, you can attempt to palpate the pulse, unlike the carotid pulse, it will be impalpable. Under normal conditions, the JVP should be less than 4cm above the sternal angle in the vertical plane (Figure 8).
Figure 6 Measuring crico-sternal distance
Figure 7 Examining for cervical lymphadenopathy
The JVP is an indirect measure of central venous pressure and can be raised secondary to right heart failure (cor pulmonale), which can exist secondary to a variety of chronic lung diseases, including COPD (EB1 and Clinical Prediction Rule 1), fluid overload, increased intrathoracic pressure (tension pneumothorax or severe acute asthma, EB2, cardiac tamponade or constrictive pericarditis. It may also occur in superior vena cava obstruction. Such obstruction can be caused by a bronchial carcinoma, especially of the right upper lobe. This leads to venous distension and oedema in the neck, face, upper chest and arms.
Displacement towards the
lesion
Displacement away from the lesion
Other displacem
ent Lobar collapse Large pleural
effusion (see Evidence Box
4)
Mediastinal masses
Pneumonectomy Tension pneumothorax
Pulmonary fibrosis
76
Figure 8 Measuring the JVP The Chest Anterior Aspect of the Chest Inspect Inspect the chest from the front and the side. You should have already briefly inspected the chest at the beginning of the examination but at this stage take some time to inspect more closely. Do not neglect the lateral aspect of the chest and axillae which may only be visible by asking the patient to move their arms. Any sign is potentially relevant and it is not possible to provide a full list here but the most important signs and their significance are described below. The most important things are to note the shape of the chest, the respiratory rate the character of the movement. An increased anteroposterior diameter describes a ‘barrel shaped’ chest, seen in patients with severe airflow obstruction (such as chronic obstructive pulmonary disease or severe asthma). This is often coupled with a dorsal kyphosis and prominence of the sternum[23]. In contrast, a pectus carinatum (‘pigeon-shaped’ chest) results from localised deformity of the sternum and costal cartilage, which bulge outwards. This can exist secondary to chronic respiratory disease in childhood. Pectus excavatum (‘funnel-shaped’ chest) is a developmental defect which can arise due to connective tissue disease. It results in a localised depression of the inferior part
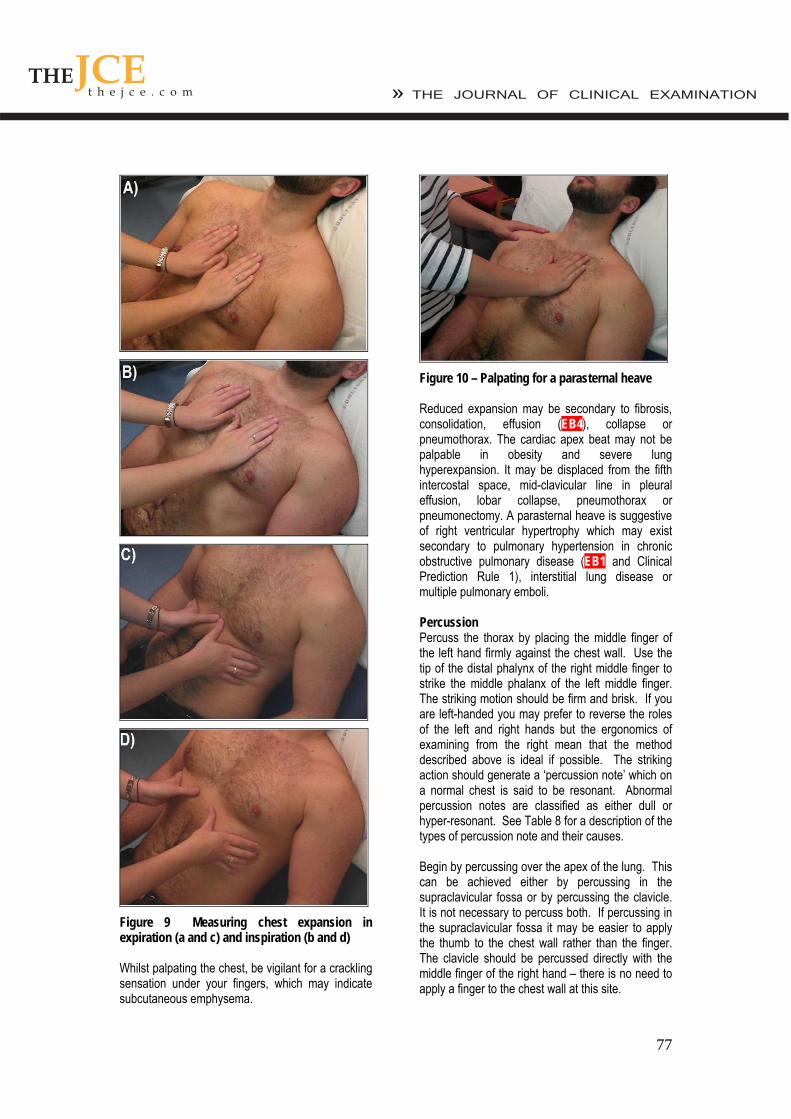
of the sternum. Spinal deformity, kyphosis or lordosis, may impinge on respiration and may be associate with systemic disease such as ankylosing spondylitis, which can lead to apical lung fibrosis. Thoracotomy scars and those from breast surgery (which could suggest malignant pleural effusion) may be obvious but it is important to pay close attention to the skin as more subtle scars for example from previous chest drain insertion could give significant clues to underlying pathology yet may not be seen even on close inspection. Radiotherapy tattoos, suggesting the presence of malignancy, may be associated with well demarcated inflammation of the skin in the acute stage, or pulmonary fibrosis, potentially detectable on auscultation in the longer term. Palpate Examine expansion of the chest. Place your hands, palm down either side of the manubrium, with your thumbs equidistant from the midline and raised slightly with your fingers on the chest, wrapped around the thorax. Ask the patient to take deep breaths in and observe your hands simultaneously rising with each inspiration (Figure 9). Place your hands on the lower anterior thorax and using the same technique. Ask the patient to breathe out and then take a deep breath in. As the patient inspires, you should be able to measure the expansion of both sides of the chest by observing your thumb’s movements relative to the midline. This should normally be at least 5cm. Place you right hand against the thorax over the fifth intercostal space, mid-clavicular line to palpate for the cardiac apex beat. In female patients, it may be appropriate to lift the left breast using the back of your left hand to lift the breast from underneath whilst palpating with your right. Place the base of your right hand firmly against the chest to the left of the sternum at the level of the heart to palpate for the heart. If the heart beat is palpable this is referred to as a parasternal heave (Figure 10).
77
Figure 9 Measuring chest expansion in expiration (a and c) and inspiration (b and d) Whilst palpating the chest, be vigilant for a crackling sensation under your fingers, which may indicate subcutaneous emphysema.
Figure 10 – Palpating for a parasternal heave Reduced expansion may be secondary to fibrosis, consolidation, effusion (EB4), collapse or pneumothorax. The cardiac apex beat may not be palpable in obesity and severe lung hyperexpansion. It may be displaced from the fifth intercostal space, mid-clavicular line in pleural effusion, lobar collapse, pneumothorax or pneumonectomy. A parasternal heave is suggestive of right ventricular hypertrophy which may exist secondary to pulmonary hypertension in chronic obstructive pulmonary disease (EB1 and Clinical Prediction Rule 1), interstitial lung disease or multiple pulmonary emboli. Percussion Percuss the thorax by placing the middle finger of the left hand firmly against the chest wall. Use the tip of the distal phalynx of the right middle finger to strike the middle phalanx of the left middle finger. The striking motion should be firm and brisk. If you are left-handed you may prefer to reverse the roles of the left and right hands but the ergonomics of examining from the right mean that the method described above is ideal if possible. The striking action should generate a ‘percussion note’ which on a normal chest is said to be resonant. Abnormal percussion notes are classified as either dull or hyper-resonant. See Table 8 for a description of the types of percussion note and their causes. Begin by percussing over the apex of the lung. This can be achieved either by percussing in the supraclavicular fossa or by percussing the clavicle. It is not necessary to percuss both. If percussing in the supraclavicular fossa it may be easier to apply the thumb to the chest wall rather than the finger. The clavicle should be percussed directly with the middle finger of the right hand – there is no need to apply a finger to the chest wall at this site.
78
Percussion Note
Common Causes
Dull * Pleural effusion (EB4), presence of hepatic tissue, consolidation, pleural thickening
Solid organ or fluid
Resonant
Normal lung Aerated lung tissue
Hyper-resonant
Pneumothorax, COPD (EB1 and Clinical Prediction Rule 1)
Hyperinflated lung tissue or air in the pleural space
* Some authors refer to stony-dull as a separate percussion note. We have not included this here. Table 8 Percussion Notes
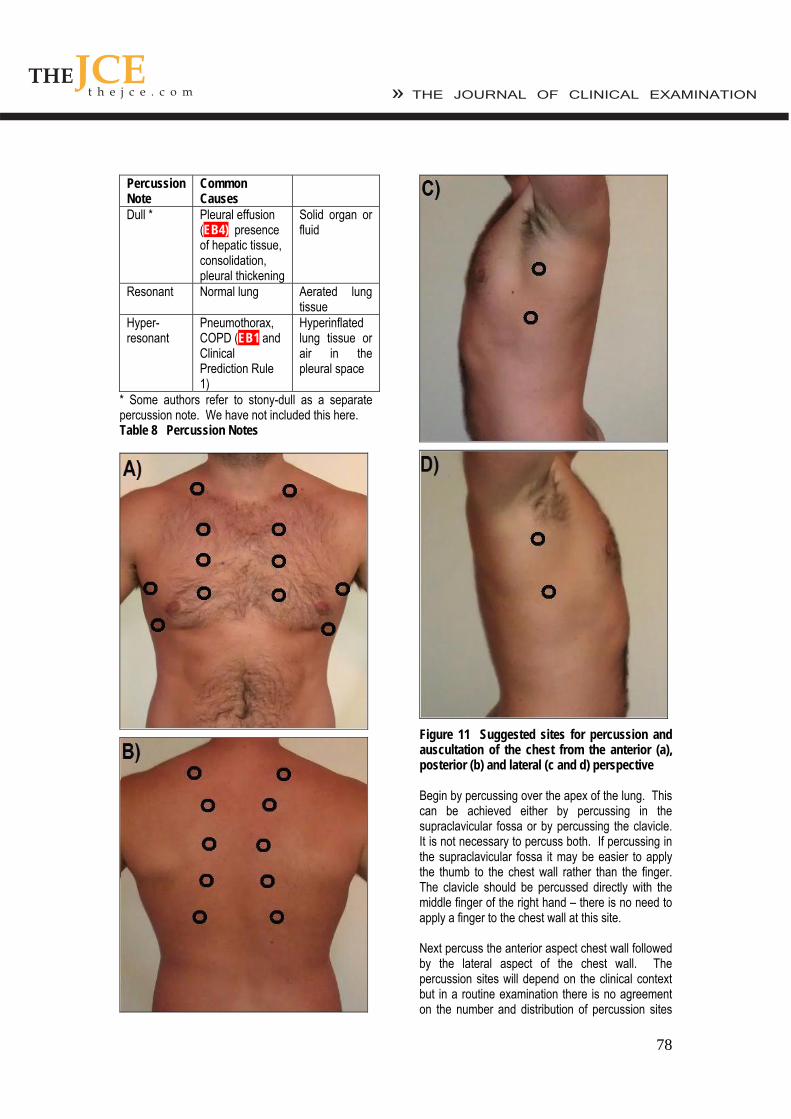
Figure 11 Suggested sites for percussion and auscultation of the chest from the anterior (a), posterior (b) and lateral (c and d) perspective Begin by percussing over the apex of the lung. This can be achieved either by percussing in the supraclavicular fossa or by percussing the clavicle. It is not necessary to percuss both. If percussing in the supraclavicular fossa it may be easier to apply the thumb to the chest wall rather than the finger. The clavicle should be percussed directly with the middle finger of the right hand – there is no need to apply a finger to the chest wall at this site. Next percuss the anterior aspect chest wall followed by the lateral aspect of the chest wall. The percussion sites will depend on the clinical context but in a routine examination there is no agreement on the number and distribution of percussion sites
79
that should be chosen. The conventional method is to choose three points on the anterior chest wall close to the midclavicular line and two points on the lateral chest wall close to the midaxillary line (Figure 11) – this allows a thorough assessment of each of the lobes of each lung. The exact site of percussion is not crucial but it is important to percuss the same site in each hemithorax one after the other to allow comparison. Auscultation Using the bell of the stethoscope auscultate the supraclavicular fossae in turn with the patient taking normal breaths through an open mouth. Next using the diaphragm auscultate the anterior and lateral chest in the same distribution as described for percussion comparing each hemithorax in turn - figure 11. In thin patients with prominent ribs the bell may need to be used to ensure good skin contact. Pay particular attention when auscultating the right axilla, right middle lobe pathology may only be demonstrated here. Repeat auscultation over the same areas, comparing each hemithorax in turn, whilst asking the patient to say ‘ninety-nine’ each time the stethoscope touches their chest to assess for vocal resonance. If consolidation is suspected, see below, auscultation can be further repeated with the patient whispering ninety-nine’ to assess for ‘whispering pectoriloquy’. Alternately instruct the patient to say the letter ‘E’ or the word ‘bee’ each time you auscultate as above to test for aegophony. If it is present you will hear ‘A’ (as in ate) rather than ‘E’, again suggesting consolidation. Be sure to remove your stethoscope for a second to verify the patient is still saying ‘E’! Whilst auscultating, listen for the quality of the breath sounds, the loudness of these sounds (EB5) and note any added sounds. See Table 9. Vocal resonance tests the lung’s ability to transmit sound. In an area of consolidation (EB6 and Clinical Prediction Rule 2), the patient’s voice becomes clearer, whilst if there is a pleural effusion (EB4), the sound will be damped and the patient’s voice becomes further muffled. If vocal resonance is increased to the point where a whisper can be heard clearly this is termed ‘whispering pectoriloquy.’ Aegophony is another test for areas of consolidation (EB6 and Clinical Prediction Rule 2). This phenomenon was originally described by Laennec[29], the term aegophony is thought to mean ‘goat sound,’ named as such because the sound
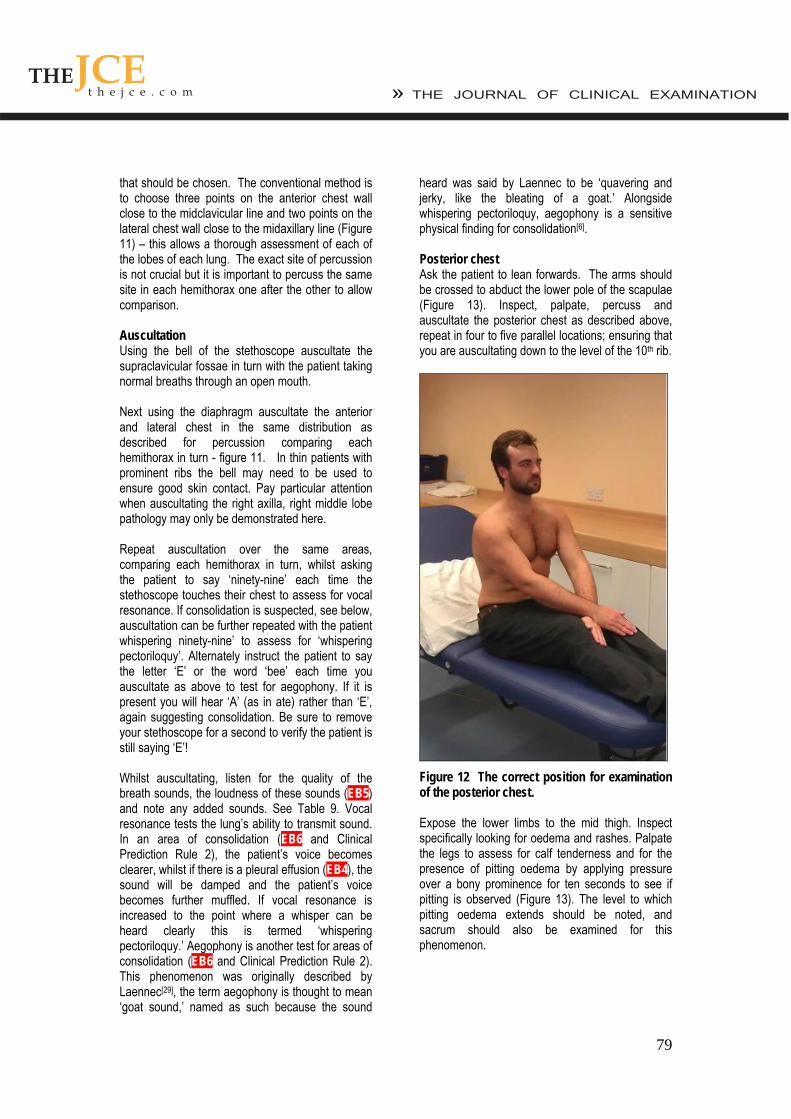
heard was said by Laennec to be ‘quavering and jerky, like the bleating of a goat.’ Alongside whispering pectoriloquy, aegophony is a sensitive physical finding for consolidation[6]. Posterior chest Ask the patient to lean forwards. The arms should be crossed to abduct the lower pole of the scapulae (Figure 13). Inspect, palpate, percuss and auscultate the posterior chest as described above, repeat in four to five parallel locations; ensuring that you are auscultating down to the level of the 10th rib.
Figure 12 The correct position for examination of the posterior chest. Expose the lower limbs to the mid thigh. Inspect specifically looking for oedema and rashes. Palpate the legs to assess for calf tenderness and for the presence of pitting oedema by applying pressure over a bony prominence for ten seconds to see if pitting is observed (Figure 13). The level to which pitting oedema extends should be noted, and sacrum should also be examined for this phenomenon.

80
Ascultate the left lower sternal edge for a pan systolic murmur loudest during inspiration as this is classically of tricuspid regurgitation, which can be secondary to right ventricle dilatation seen with pulmonary hypertension. Aucsultate the left upper sternal edge for a high pitched early diastolic murmur loudest during inspiration, a Graham Steell murmur, caused by high velocity regurgitant flow across the pulmonary valve typical of pulmonary hypertension.
Note the components of the heart sounds and listen for a right ventricular S4, giving a gallop rhythm. Note the cadence of the 3 heart sounds – S1, S2 and S4 which are said to resemble that of the word ‘Tennessee’ which are seen in pulmonary stenosis or pulmonary hypertension. Finally, note the volume of the components of the heart sounds for a loud P2 which will be evident in pulmonary hypertension.
Figure 13 Examining for peripheral pitting oedema Peripheral oedema may represent congestive cardiac failure or cor pulmonale secondary to pulmonary disease. A deep venous thrombosis may present with lower limb swelling or erythema. Erythema nodosum, a panniculitis which causes tender nodules; often on the shins may be observed. Erythema nodosum may be seen in respiratory disease such as streptococcal infection, tuberculosis and sarcoidosis.
Completing the examination To complete the examination you should perform pulse oximetry to measure oxygen saturations and measure the temperature. If obstructive airways disease is suspected then you should measure peak expiratory flow using a peak flow meter.
Auscultating the Heart A full examination of the cardiovascular examination is beyond the scope of this article but some cardiovascular signs are of direct relevance to the examination of the respiratory system and should be specifically sought-out. For a full account of how to perform the cardiovascular examination please see The Journal of Clinical Examination’s: Examination of the Cardiovascular System [34].
Finally, wash your hands, thank the patient and allow him/her redress in privacy. Conflict of interest None declared
81
References [1] Jopling H, The principles of Clinical Examination. The Journal Of Clinical Examination, 2006; 1: 3-6
[2] http://jama.amaassn.org/cgi/collection/rational_ clinical_exam
[3] http://clinicalevidence.bmj.com
[4] Clinical Examination: A Systematic Guide to Physical Diagnosis, Nicholas Talley and Simon O’Connor, Elsevier 2006
[5] Macleod’s Clinical Examination, Graham Douglas, Fiona Nicol and Colin Robertson, Elsevier 2005
[6] Sapira’s Art and Science of Bedside Diagnosis, Joseph Sapira and Jane Orient, Lippincott Williams & Wilkins 2005
[7] Evidence Based Physical Diagnosis, Steven McGee, Saunders 2001
[8] Breslin EH, The pattern of respiratory muscle recruitment during pursed-lip breathing. Chest. 1992; 101:75-78#
[9] Gaunt AC and Frang T, Examination of the Respiratory System. The Journal of Clinical Examination 2007; 4: 14-22
[10] Mared L, Cline C, Erhardt L, Berg S, Midgren B, Cheyne-Stokes respiration in patients hospitalised for heart failure. Resp Research 2004; 5: 14
[11] Straus SE, McAlister FA, Sackett DL, Deeks JJ, The accuracy of patient history, wheezing and laryngeal measurements in diagnosing obstructive airway disease. JAMA 2000; 283: 1853-1857
[12] Garcia-Pachon E, Paradoxical movement of the lateral rib margin (Hoover sign) for detecting obstructive airway disease. Chest. 2002; 122: 651-655
[13] Badgett RG, Tanaka DJ, Hunt DK et al, Can moderate chronic obstructive pulmonary disease be diagnosed by historical and physical findings alone? Am J Med, 1993; 94: 188-196
[14] Nath AR, Capel LH, Inspiratory crackles: Early and late. Thorax, 1974; 29: 223-227
[15] Celli et al, The Body-Mass Index, Airflow Obstruction, Dyspnoea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease, NEJM, 2004; 350: 1005-12
[16] Marin et a, Prediction of risk of COPD exacerbations by the BODE index. Resp Med 2009; 103. 373-378
[17] Forgacs P, The functional basis of pulmonary sounds, Chest. 1978; 73; 399-405
[18] British Thoracic Society Scottish Intercollegiate Guidelines Network, British Guideline on the Management of Asthma. Thorax (2008); 63 Supple 4:iv, 1-121
[19] Lynn SM, Kilbey, R, Examination for Finger Clubbing, J Clin Exam 2011; 11:13-21
[20] Dickson JM, Examination of the Cardiovascular System, J Clin Exam 2009; 9: 7
[20] Khasnis A, Lokhandwala Y. Clinical signs in medicine: pulsus paradoxus. J Postgrad Med. 2002 Jan-Mar; 48(1):46-9
[21] Gross NJ, Hamilton JD, Correlation between the physical signs of hypercapnia and the mixed venous pCO2. BMJ 1963; 2(5365): 1096-7
[22] Pierce JA, Ebert RV, The Barrel deformity of the chest, the senile lung and obstructive pulmonary emphysema. Am J Med. 1958; 25(1): 13-22
[23] Diacon et al, Accuracy of pleural puncture sites: a prospective comparison of clinical examination with ultrasound. Chest 2003: 123: 436-441
[24] Patterson LA, Costantine TG, Satz WA, Diagnosing pleural effusion: a prospective comparison of physical examination with bedside ultrasonography, Ann Emerg Med 2004; 44:5112
[25] Kalantri S, Joshi R, Lokhande T, Singh A, Morgan M, Colford JM, Pal M, Accuracy and reliability of physical signs in the diagnosis of pleural effusion
[26] Wong CL, Holroyd-Leduc J, Straus SE, Does this patient have a pleural effusion? JAMA 2009; 301(3): 309-17
[27] Yernault JC, Bohadana AE, Chest percussion, Eur Resp J, 1995; 8(10): 1755-60
[28] Jarcho S, Auenbrugger, Laennec, and John Keats. Some notes on the early history of percussion and auscultation. Med Hist. 1961; 5: 167-72
[29] Pardee NE, Martin CJ, Morgan EH. A test of the practical value of estimating breath sound intensity. Chest 1976; 70: 341-4

82
[30] Bohadana AB, Peslin R, Uffholtz H. Breath sounds in the clinical assessment of airflow obstruction. Thorax 1978; 33: 345-51
[31] Diehr P, Wood RW, Bushyhead J, Krueger L, Wolcott B, Tompkins RK, Prediction of pneumonia in outpatients with acute cough – a statistical approach. J Chronic Dis. 1984; 37(3): 215-225
[32] Heckerling PS, Tape TG, Wigton RS et al, Clinical prediction rule for pulmonary infiltrates. Ann Intern Med. 1990; 113: 664-670
[33] Tharmlaingham H and Dwight D, Examination of the Cardiovascular System, J Clin Exam 2010; 10: 26-40
[34] Lim et al, Defining community acquired pneumonia severity on presentation to hospital: an
international derivation and validation study. Thorax 2003; 58: 377-382
[35] British Thoracic Society Standards of Care Committee, BTS guidelines for the Management of Community Acquired Pneumonia in Adults. Thorax. 2001; 56 (Suppl 4): IV1-64
[36] Wells et al, Use of a clinical model for safe management of patients with suspected pulmonary embolism. Ann Intern Med, 1998; 129: 997-1005
[37] Wells et al, Derivation of a simple clinical model to categorise patients’ probability of pulmonary embolism: Increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000; 83: 416-420
83
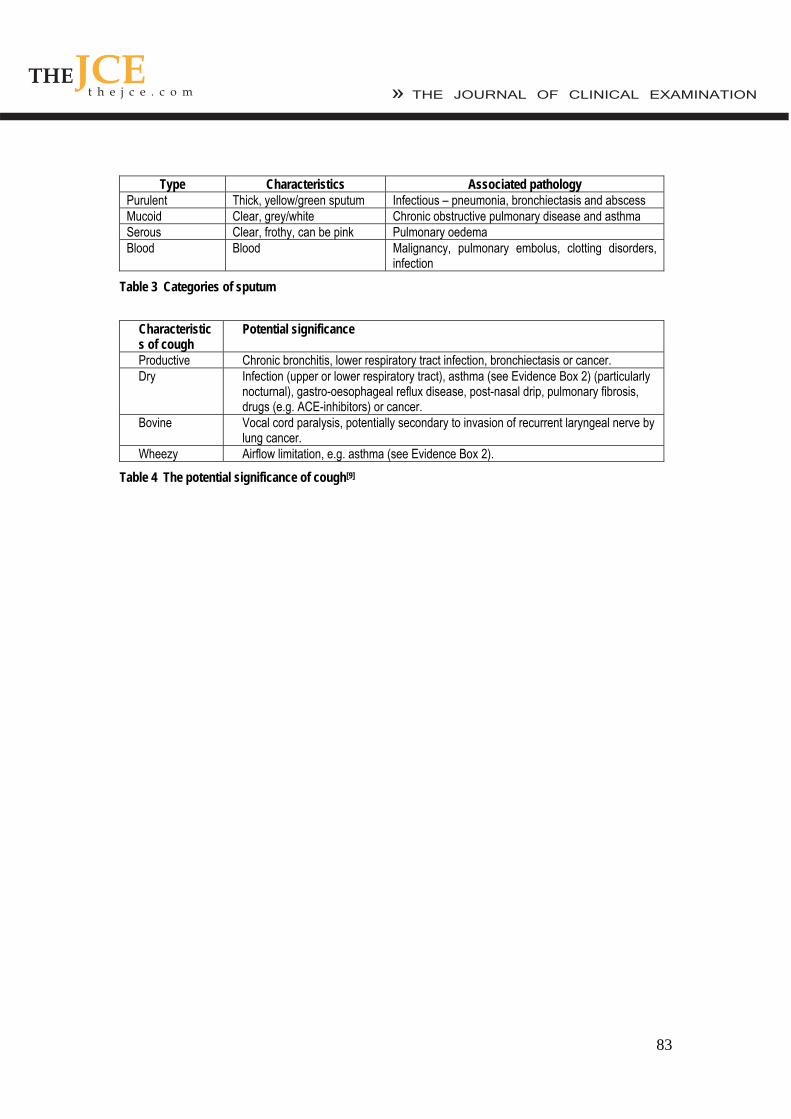
Type Characteristics Associated pathology Purulent Thick, yellow/green sputum Infectious – pneumonia, bronchiectasis and abscess Mucoid Clear, grey/white Chronic obstructive pulmonary disease and asthma Serous Clear, frothy, can be pink Pulmonary oedema Blood Blood Malignancy, pulmonary embolus, clotting disorders,
infection
Table 3 Categories of sputum
Characteristics of cough
Potential significance
Productive Chronic bronchitis, lower respiratory tract infection, bronchiectasis or cancer. Dry Infection (upper or lower respiratory tract), asthma (see Evidence Box 2) (particularly
nocturnal), gastro-oesophageal reflux disease, post-nasal drip, pulmonary fibrosis, drugs (e.g. ACE-inhibitors) or cancer.
Bovine Vocal cord paralysis, potentially secondary to invasion of recurrent laryngeal nerve by lung cancer.
Wheezy Airflow limitation, e.g. asthma (see Evidence Box 2).
Table 4 The potential significance of cough[9]
84
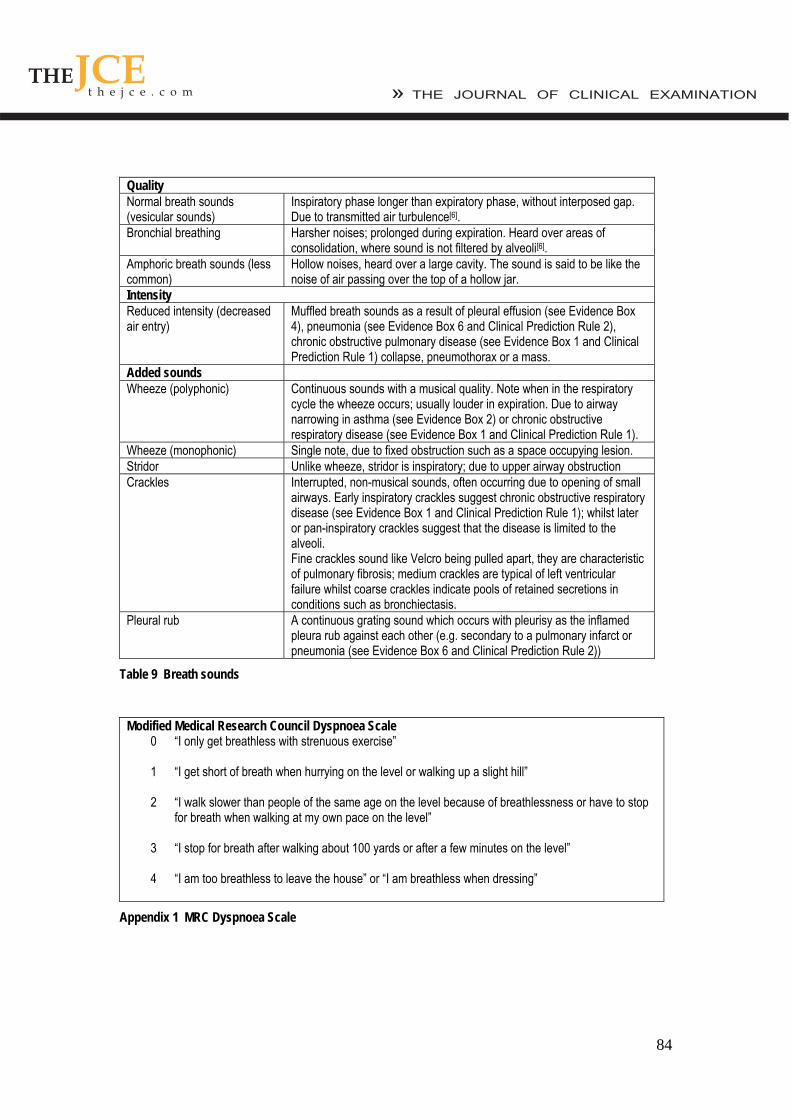
Quality Normal breath sounds (vesicular sounds)
Inspiratory phase longer than expiratory phase, without interposed gap. Due to transmitted air turbulence[6].
Bronchial breathing Harsher noises; prolonged during expiration. Heard over areas of consolidation, where sound is not filtered by alveoli[6].
Amphoric breath sounds (less common)
Hollow noises, heard over a large cavity. The sound is said to be like the noise of air passing over the top of a hollow jar.
Intensity Reduced intensity (decreased air entry)
Muffled breath sounds as a result of pleural effusion (see Evidence Box 4), pneumonia (see Evidence Box 6 and Clinical Prediction Rule 2), chronic obstructive pulmonary disease (see Evidence Box 1 and Clinical Prediction Rule 1) collapse, pneumothorax or a mass.
Added sounds Wheeze (polyphonic) Continuous sounds with a musical quality. Note when in the respiratory
cycle the wheeze occurs; usually louder in expiration. Due to airway narrowing in asthma (see Evidence Box 2) or chronic obstructive respiratory disease (see Evidence Box 1 and Clinical Prediction Rule 1).
Wheeze (monophonic) Single note, due to fixed obstruction such as a space occupying lesion. Stridor Unlike wheeze, stridor is inspiratory; due to upper airway obstruction Crackles Interrupted, non-musical sounds, often occurring due to opening of small
airways. Early inspiratory crackles suggest chronic obstructive respiratory disease (see Evidence Box 1 and Clinical Prediction Rule 1); whilst later or pan-inspiratory crackles suggest that the disease is limited to the alveoli. Fine crackles sound like Velcro being pulled apart, they are characteristic of pulmonary fibrosis; medium crackles are typical of left ventricular failure whilst coarse crackles indicate pools of retained secretions in conditions such as bronchiectasis.
Pleural rub A continuous grating sound which occurs with pleurisy as the inflamed pleura rub against each other (e.g. secondary to a pulmonary infarct or pneumonia (see Evidence Box 6 and Clinical Prediction Rule 2))
Table 9 Breath sounds
Modified Medical Research Council Dyspnoea Scale 0 “I only get breathless with strenuous exercise” 1 “I get short of breath when hurrying on the level or walking up a slight hill” 2 “I walk slower than people of the same age on the level because of breathlessness or have to stop
for breath when walking at my own pace on the level” 3 “I stop for breath after walking about 100 yards or after a few minutes on the level” 4 “I am too breathless to leave the house” or “I am breathless when dressing”
Appendix 1 MRC Dyspnoea Scale
85
Clinical signs in Chronic Obstructive Pulmonary Disease
Evidence Box 1 Chronic Obstructive Pulmonary Disease
COPD is an oft encountered pathology. A number of signs have been associated with COPD, these include: • Laryngeal height <4cm: The distance between the thyroid cartilage and suprasternal notch is
thought to be reduced as the clavicles and sternum are higher than normal. +LR – 3.6, -LR – 0.7[11].
• Hoover’s sign (costal paradox) – The examiner places one hand on each costal margin. Usually, the ribs move outwards whilst in a patient with chest hyperexpansion in COPD, the costal margins are instead pulled closer together. +LR – 4.2, -LR – 0.5[12].
• Hyper resonance of upper right anterior chest - +LR 5.1, -LR not significant[13]. • Absence of cardiac dullness on percussion – +LR 11.8, -LR not significant[13]. • Early inspiratory crackles - +LR 14.6, -LR – not significant[14].
British Thoracic Society guidelines for assessment of acute asthma The British Thoracic Society[18] has produced guidelines for the assessment of acute asthma in adults:
Moderate asthma Severe asthma Life threatening asthma
Peak expiratory flow > 50-75% best or predicted
Peak expiratory flow 33 – 50% best or predicted
Peak expiratory flow <33% best or predicted
SpO2 ≥92% SpO2 ≥92% SpO2 < 92% Speech normal Can’t complete sentences Silent chest, cyanosis or poor
respiratory effort
Respiration < 25 breaths/min Respiration ≥25 breaths/min Exhaustion, altered consciousness
Pulse <110 beats/min Pulse ≥ 110 beats/min Arrhythmia or hypotension
Guidelines for management are also included, for further information please review the full guidance at the British Thoracic Society website[18]
Evidence Box 2 Assessment of acute asthma
Pulsus paradoxus results in an exaggeration of the normal variation of the pulse with respiration – the pulse becomes weaker in inspiration, then stronger in expiration. This sign can be caused by a number of conditions; those relevant to the respiratory system include asthma (EB2), chronic obstructive pulmonary disease (EB1 and Clinical Prediction Rule 1) and tension pneumothorax. In these conditions, decreased blood return to the left heart during inspiration results in a decreased stroke volume, which in turn causes a lower systolic pressure. The lower pressure renders the pulse impalpable. The paradox lies in the fact that if one were to auscultate the chest whilst palpating for the radial pulse, beats would be heard but not felt. Pulsus paradoxus can be quantified by measuring the variation of blood pressure during respiration – a decrease of >10 mmHg in inspiration will be found if the sign is positive[21]. Carbon dioxide retention may result in a rapid, bounding pulse[22].
Evidence Box 3 Pulsus paradoxus
86
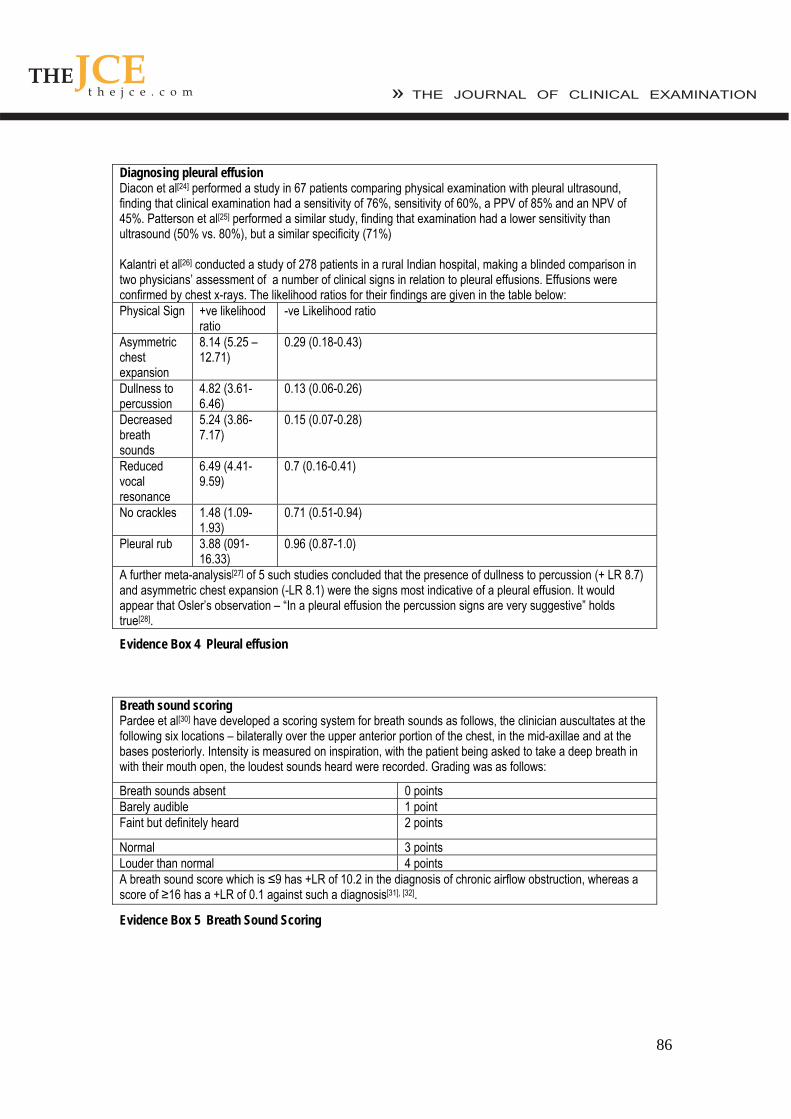
Diagnosing pleural effusion
Evidence Box 4 Pleural effusion
Diacon et al[24] performed a study in 67 patients comparing physical examination with pleural ultrasound, finding that clinical examination had a sensitivity of 76%, sensitivity of 60%, a PPV of 85% and an NPV of 45%. Patterson et al[25] performed a similar study, finding that examination had a lower sensitivity than ultrasound (50% vs. 80%), but a similar specificity (71%) Kalantri et al[26] conducted a study of 278 patients in a rural Indian hospital, making a blinded comparison in two physicians’ assessment of a number of clinical signs in relation to pleural effusions. Effusions were confirmed by chest x-rays. The likelihood ratios for their findings are given in the table below: Physical Sign +ve likelihood
ratio -ve Likelihood ratio
Asymmetric chest expansion
8.14 (5.25 – 12.71)
0.29 (0.18-0.43)
Dullness to percussion
4.82 (3.61-6.46)
0.13 (0.06-0.26)
Decreased breath sounds
5.24 (3.86-7.17)
0.15 (0.07-0.28)
Reduced vocal resonance
6.49 (4.41-9.59)
0.7 (0.16-0.41)
No crackles 1.48 (1.09-1.93)
0.71 (0.51-0.94)
Pleural rub 3.88 (091-16.33)
0.96 (0.87-1.0)
A further meta-analysis[27] of 5 such studies concluded that the presence of dullness to percussion (+ LR 8.7) and asymmetric chest expansion (-LR 8.1) were the signs most indicative of a pleural effusion. It would appear that Osler’s observation – “In a pleural effusion the percussion signs are very suggestive” holds true[28].
Breath sound scoring Pardee et al[30] have developed a scoring system for breath sounds as follows, the clinician auscultates at the following six locations – bilaterally over the upper anterior portion of the chest, in the mid-axillae and at the bases posteriorly. Intensity is measured on inspiration, with the patient being asked to take a deep breath in with their mouth open, the loudest sounds heard were recorded. Grading was as follows:
Breath sounds absent 0 points Barely audible 1 point Faint but definitely heard 2 points
Normal 3 points Louder than normal 4 points A breath sound score which is ≤9 has +LR of 10.2 in the diagnosis of chronic airflow obstruction, whereas a score of ≥16 has a +LR of 0.1 against such a diagnosis[31], [32].
Evidence Box 5 Breath Sound Scoring
87
Diagnosing Pneumonia A study of 1819 patients found cachexia had a +LR of 4.0 for pneumonia, with the –LR insignificant[32]. Percussion dullness was also found to have a +LR of 3.0, -LR insignificant[32]. Heckerling et al studied pneumonia in 464 patients, concluding that bronchial breathing had a +LR of 3.3, again the –LR was insignificant[33]. Vocal resonance was found to have a +LR of 4.1, with the –LR insignificant[32]. However, crackles have a +LR of only 1.8, with a –LR of 0.8; the evidence for wheezing is even poorer (+LR 0.8, -LR NS) [7].
Evidence Box 6 Pneumonia
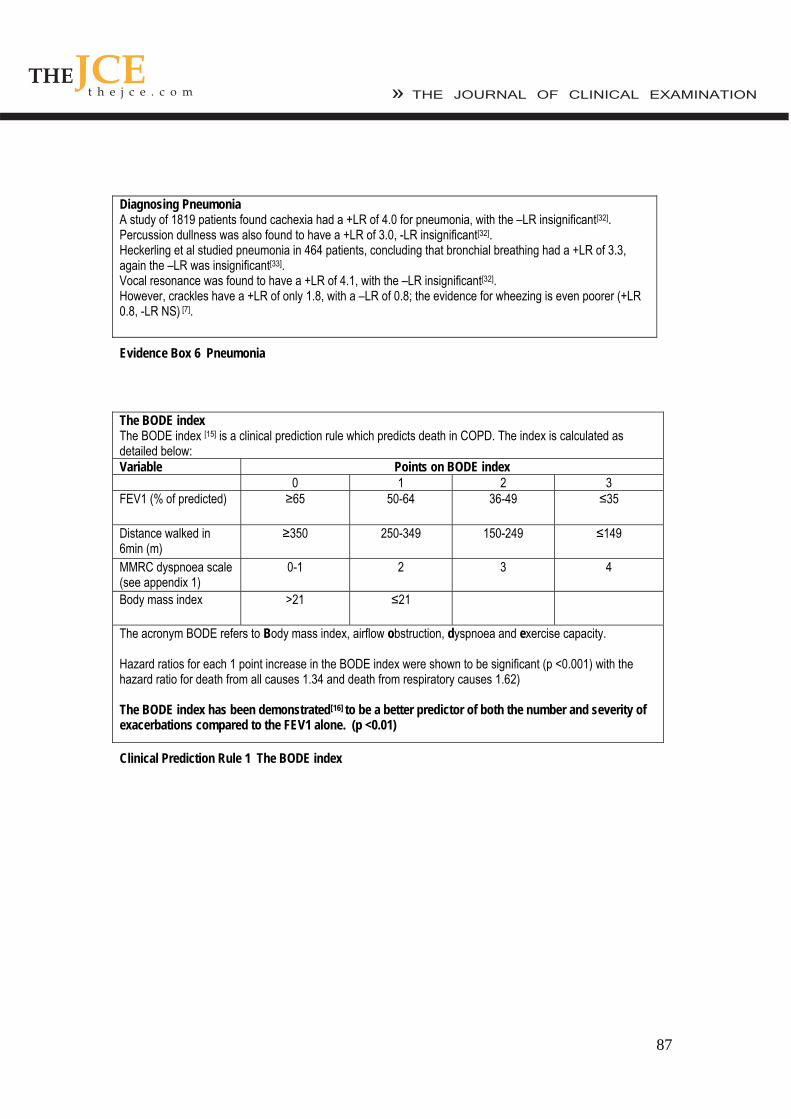
The BODE index The BODE index [15] is a clinical prediction rule which predicts death in COPD. The index is calculated as detailed below: Variable Points on BODE index 0 1 2 3 FEV1 (% of predicted) ≥65 50-64 36-49 ≤35
Distance walked in 6min (m)
≥350 250-349 150-249 ≤149
MMRC dyspnoea scale (see appendix 1)
0-1 2 3 4
Body mass index >21 ≤21
The acronym BODE refers to Body mass index, airflow obstruction, dyspnoea and exercise capacity. Hazard ratios for each 1 point increase in the BODE index were shown to be significant (p <0.001) with the hazard ratio for death from all causes 1.34 and death from respiratory causes 1.62) The BODE index has been demonstrated[16] to be a better predictor of both the number and severity of exacerbations compared to the FEV1 alone. (p <0.01)
Clinical Prediction Rule 1 The BODE index
88
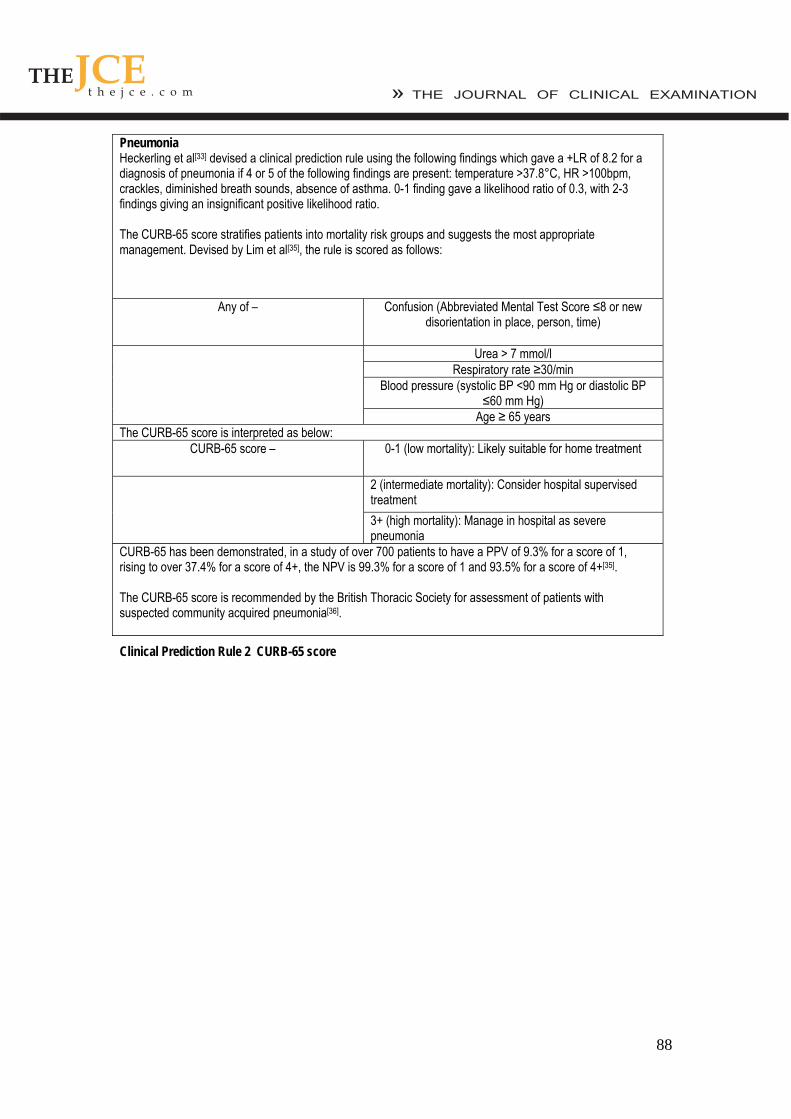
Heckerling et al[33] devised a clinical prediction rule using the following findings which gave a +LR of 8.2 for a diagnosis of pneumonia if 4 or 5 of the following findings are present: temperature >37.8°C, HR >100bpm, crackles, diminished breath sounds, absence of asthma. 0-1 finding gave a likelihood ratio of 0.3, with 2-3 findings giving an insignificant positive likelihood ratio.
Pneumonia
The CURB-65 score stratifies patients into mortality risk groups and suggests the most appropriate management. Devised by Lim et al[35], the rule is scored as follows:
Any of – Confusion (Abbreviated Mental Test Score ≤8 or new disorientation in place, person, time)
Urea > 7 mmol/l Respiratory rate ≥30/min
Blood pressure (systolic BP <90 mm Hg or diastolic BP ≤60 mm Hg)
Age ≥ 65 years The CURB-65 score is interpreted as below:
CURB-65 score – 0-1 (low mortality): Likely suitable for home treatment
2 (intermediate mortality): Consider hospital supervised treatment 3+ (high mortality): Manage in hospital as severe pneumonia
CURB-65 has been demonstrated, in a study of over 700 patients to have a PPV of 9.3% for a score of 1, rising to over 37.4% for a score of 4+, the NPV is 99.3% for a score of 1 and 93.5% for a score of 4+[35]. The CURB-65 score is recommended by the British Thoracic Society for assessment of patients with suspected community acquired pneumonia[36].
Clinical Prediction Rule 2 CURB-65 score
89
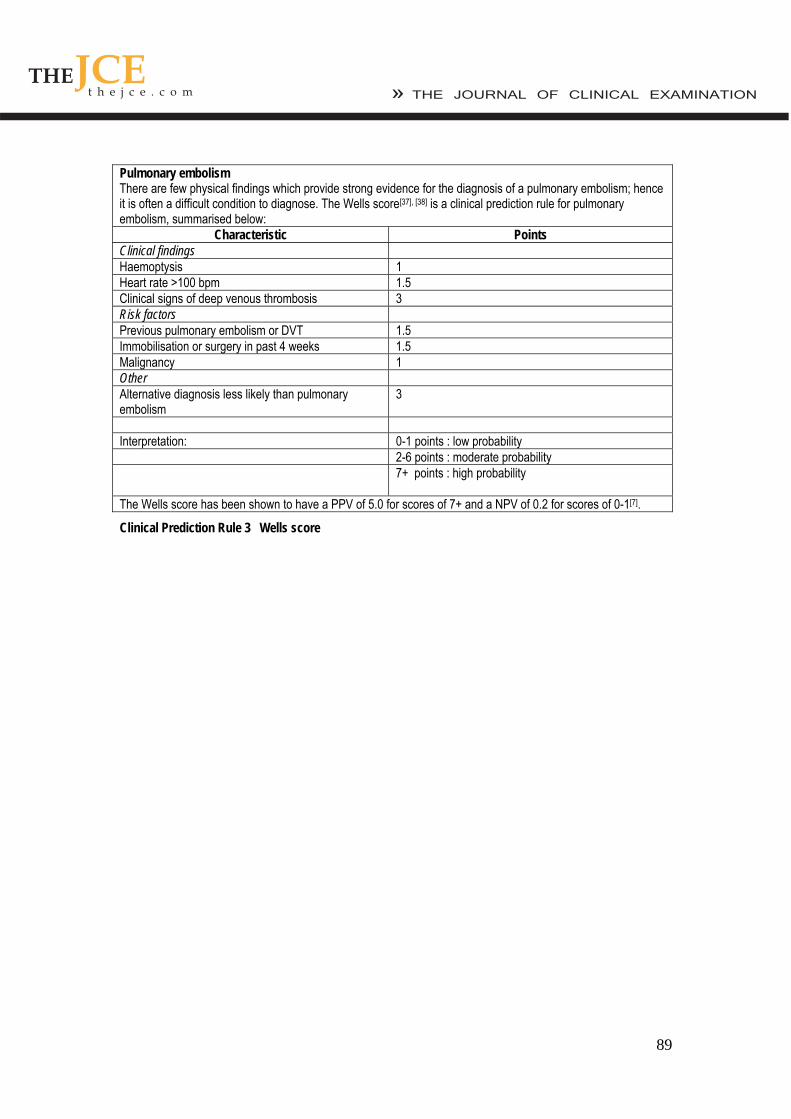
Pulmonary embolism
There are few physical findings which provide strong evidence for the diagnosis of a pulmonary embolism; hence it is often a difficult condition to diagnose. The Wells score[37], [38] is a clinical prediction rule for pulmonary embolism, summarised below:
Characteristic Points Clinical findings Haemoptysis 1 Heart rate >100 bpm 1.5 Clinical signs of deep venous thrombosis 3 Risk factors Previous pulmonary embolism or DVT 1.5 Immobilisation or surgery in past 4 weeks 1.5 Malignancy 1 Other Alternative diagnosis less likely than pulmonary embolism
3
Interpretation: 0-1 points : low probability 2-6 points : moderate probability 7+ points : high probability
The Wells score has been shown to have a PPV of 5.0 for scores of 7+ and a NPV of 0.2 for scores of 0-1[7].
Clinical Prediction Rule 3 Wells score




![Expert Consensus Meeting Management of Burns in Pre ... · situation (17) [IV]. Breathing Respiratory system support, in accordance with current British Thoracic Society “Guidelines](https://img.pdfslide.net/doc/110x75/5f04d1e67e708231d40fde56/expert-consensus-meeting-management-of-burns-in-pre-situation-17-iv-breathing.jpg)













![Infection Control for Ventilators Respiratory Support ...€¦ · Reference: [1] Expert Concensus of Mechanical Ventilation Infection Control for Novel Coronavirus,Chinese Journal](https://img.pdfslide.net/doc/110x75/5f630431b163d45920502ece/infection-control-for-ventilators-respiratory-support-reference-1-expert.jpg)