Embed Size (px)
Citation preview
Exploration of the Incidence of & Risk Factors for Postoperative Urinary Retention (POUR) in the Orthopaedic Total Joint Patient: A Pilot Study
Jan Bailey, MSN, RN, OCNS-CVallire Hooper, PhD, RN, CPAN, FAAN
Mission HospitalAsheville, NC
2
The Dilemma of Bladder Management for the Total Joint Arthroplasty (TJA) Surgery Patient
• Catheter Pros:– POUR incidence following TJA has been reported to be as high as
67%.– No evidence that catheter use increases incidence of catheter
associated urinary tract infection (CAUTI) when duration is less than 24 hours.
– May prevent bladder over-distension which can lead to permanent bladder dysfunction.
– Short-term use can decrease patient discomfort and nursing time (if intermittent catheter required).
– National Association of Orthopaedic Nurses (NAON) guidelines recommends use of indwelling catheter for first 24 hours following TJA.
Normal bladder function
• Adult bladder has capacity of 400-600 ml• Urge to void on average @ 150 ml• Sense of fullness on average @ 300 ml• Bladder volume > 500 ml increases risk for:
– Over-distension – Atony – Incomplete bladder emptying – UTI
Baldini, et al (2009)
4
Catheter Cons: Pressure to Eliminate Indwelling Catheter Use
Large body of evidence supports correlation between CAUTI and duration of catheter dwell time.
CDC published guidelines (2009) discouraging routine catheters during surgery & recommended removal in PACU with some exceptions that did not include total joint arthroplasty procedures.
Surgical Care Improvement Project (SCIP) calls for catheter removal on day 1 or 2 with day of surgery being day zero (2010).
Hospital reimbursement affected through Centers for Medicare and Medicaid Services (CMS) hospital-acquired condition program.
Prevention of CAUTI is a 2012 Joint Commission Patient Safety Goal.
MESSAGE RECEIVED: Do not use indwelling urinary catheters.
Our Problems
• Use of indwelling catheters for TJA patients had decreased dramatically.
• While post-operative orders include Q4 hour bladder scan with guidelines for catheterization if no void, this protocol was not initiated until arrival to the orthopaedic unit.
• Staff perception was that patients were arriving from PACU requiring immediate in & out catheterization and were requiring multiple intermittent catheterizations before resolution of urinary retention.
• Our in and out cath protocol was not being utilized in PACU.
6
Mission Intermittent Urinary Catheterization Protocol
If no void or voids < 250 ml within 4hours:• Perform bladder scan every 4 hours until spontaneous voiding
resumes.• If bladder volume ≥ 350 ml, perform straight cath.• If bladder volume <350, rescan in 2 hours if patient has not
voided; cath if volume > 350 ml.• If straight cath is required X 2, call MD for further orders• Call MD if urinary output < 250 ml over 8 hours• If bladder volume < 250 ml and pt voiding continue to monitor
I & O
Preliminary PI Project
• A team of orthopaedic nurses collected data for one week to see if an opportunity for improvement would be identified.
• Information was collected for 30 postoperative total knee replacment patients. .– 60% (N=18) did not have a foley placed during the perioperative period.
• Of patients without Foley:– Only 3 patients voided while in PACU.– No patients were scanned or catheterized in PACU.– 10 patients were able to void on arrival to unit.– 8 patients had to be catheterized on arrival.– 9 patients arrived to unit with bladder volume exceeding 500 ml (range
500-1000 ml) measured by bladder scan.• This information was shared at a joint meeting with PACU and a team
developed a plan for the research project.• The research was given exempt status by our community IRB.
8
Research Goal
• Explore the incidence of POUR in the total knee and hip replacement population in the Orthopaedic Units at Mission Hospital– POUR: The inability to empty the bladder, not withstanding it
being full, in the immediate to early postoperative period– The literature identified the following risk factors for POUR:
• Age over 50• Intraoperative fluid volume over 750 ml• Surgery duration over 2 hours• Spinal anesthesia• Bladder volume over 270 ml on admission to the PACU
Research Questions
• What is the mean bladder volume on first bladder scan in the PACU?
• What is the incidence of postoperative catheterization in the PACU?
• What is the incidence of postoperative urinary retention (POUR) in total hip and knee arthroplasty patients?
• What are risk factors for POUR in this population?
Study Design
• Prospective descriptive correlational design• Convenience sample (126 patients) of all adult
patients having total knee and/or hip replacements admitted to the orthopaedic unit.
• PACU nurse initiated data collection tool and it was completed by the orthopaedic unit nurse at the time of patient’s first void or catheterization after arrival to unit.
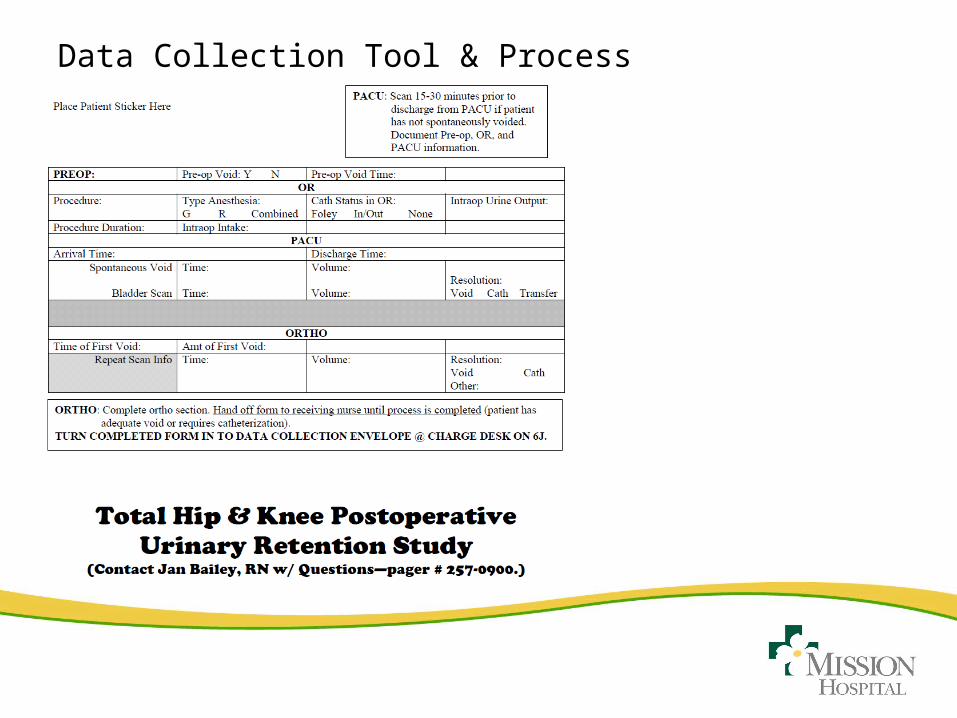
Data Collection Tool & Process
Results
• Mean age: 63.9 yrs (+10.18)• Gender
– 45.2% male– 54.8% female
• Type anesthesia– 63.2% general– 36.8% regional or
general/regional combo
• Surgical duration– Mean: 124.75 min (+ 38.7)
• Male: 133.42 min (+ 39.21)
• Female: 117.58 min (+ 37.0) (p < 0.022)
– Range: 60 to 310 min• Intraoperative volume
– 1590.78 ml (+ 482.49)– Range: 200-3300 ml
13
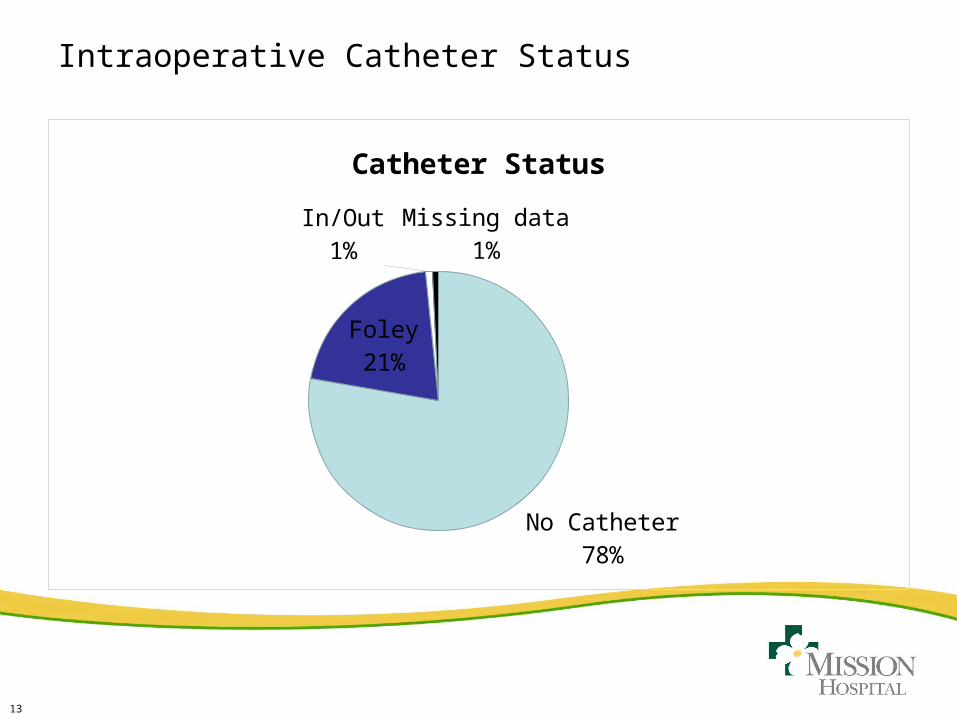
Intraoperative Catheter Status
No Catheter
78%
Foley21%
In/Out1%
Missing data1%
Catheter Status
14
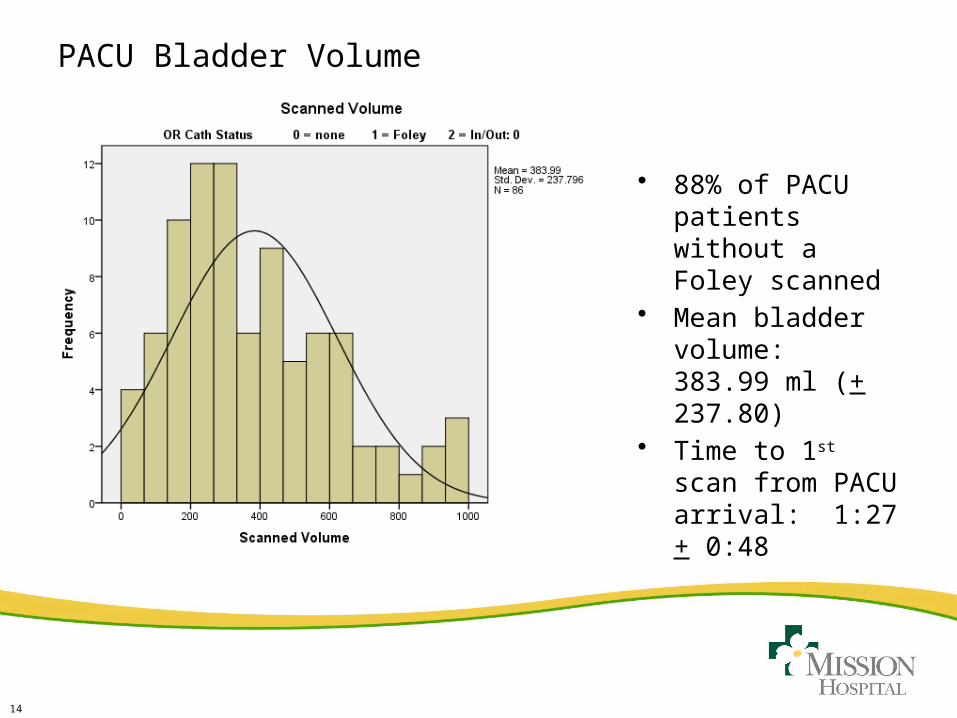
PACU Bladder Volume
• 88% of PACU patients without a Foley scanned
• Mean bladder volume: 383.99 ml (+ 237.80)
• Time to 1st scan from PACU arrival: 1:27 + 0:48
15
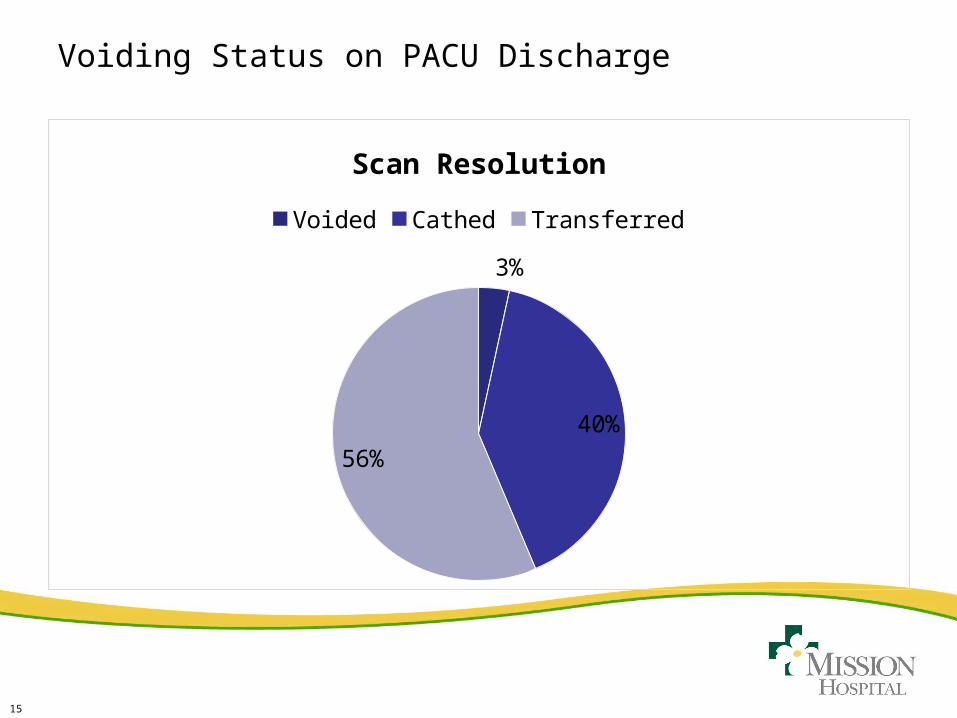
Voiding Status on PACU Discharge
3%
40%
56%
Scan Resolution
Voided Cathed Transferred
16
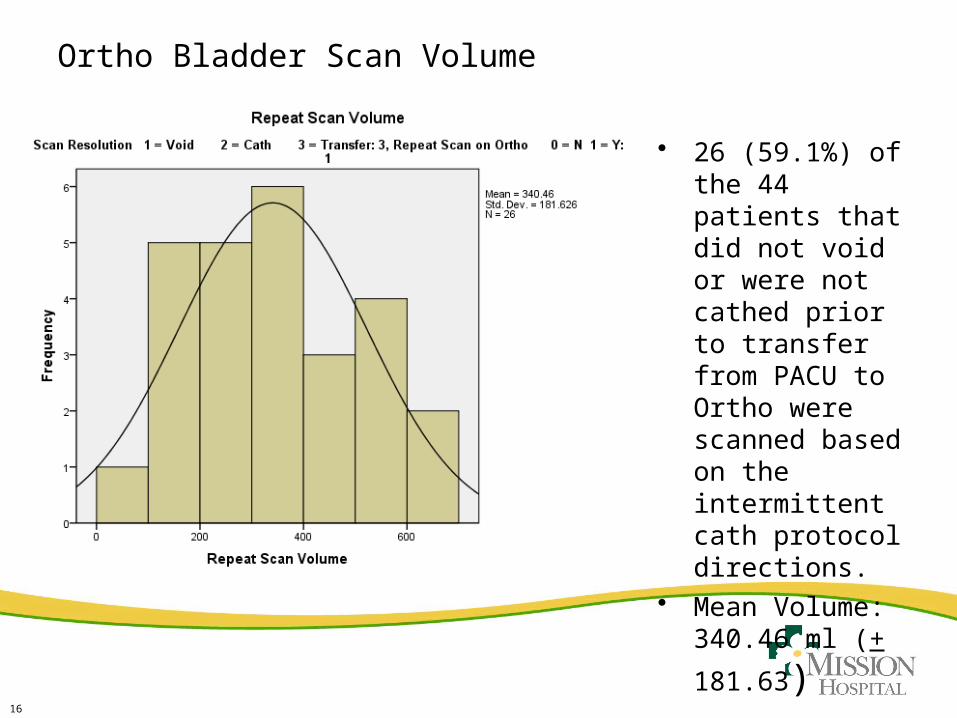
Ortho Bladder Scan Volume
• 26 (59.1%) of the 44 patients that did not void or were not cathed prior to transfer from PACU to Ortho were scanned based on the intermittent cath protocol directions.
• Mean Volume: 340.46 ml (+
181.63)
17
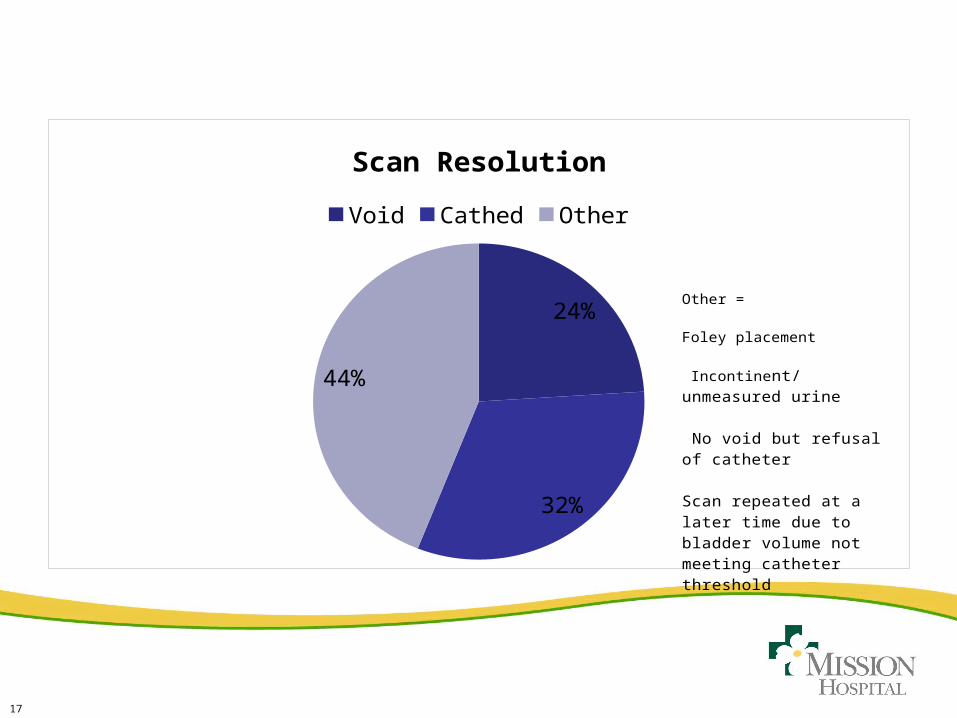
24%
32%
44%
Scan Resolution
Void Cathed Other
Other =
Foley placement
Incontinent/unmeasured urine
No void but refusal of catheter
Scan repeated at a later time due to bladder volume not meeting catheter threshold
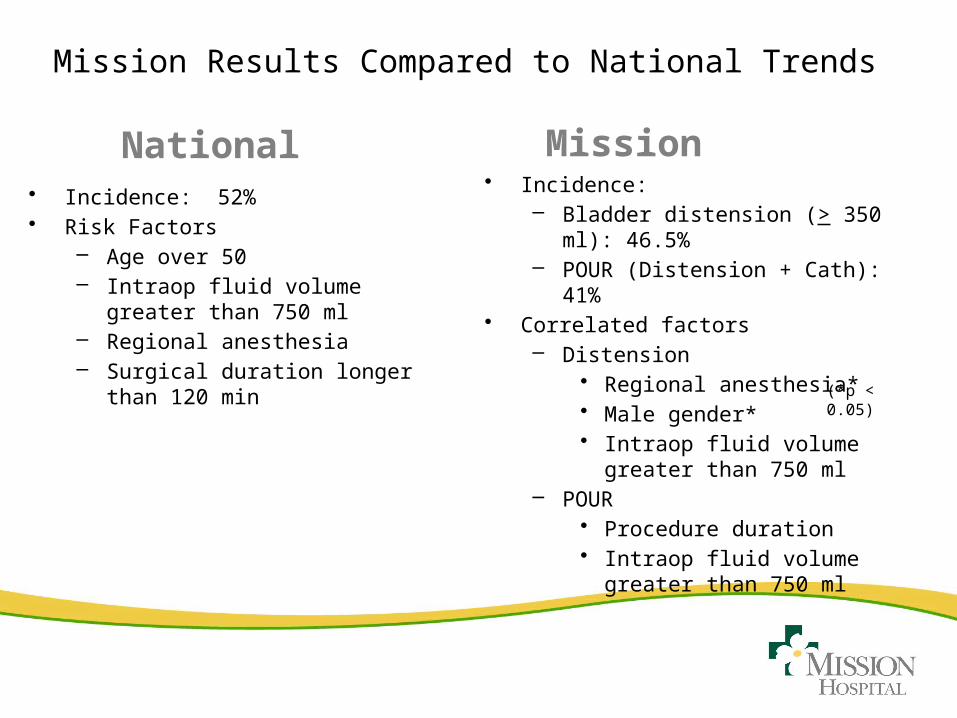
Mission Results Compared to National Trends
National Mission• Incidence: 52%• Risk Factors
– Age over 50– Intraop fluid volume greater than
750 ml– Regional anesthesia– Surgical duration longer than 120
min
• Incidence:– Bladder distension (> 350 ml):
46.5%– POUR (Distension + Cath): 41%
• Correlated factors– Distension
• Regional anesthesia*• Male gender*• Intraop fluid volume greater than
750 ml– POUR
• Procedure duration• Intraop fluid volume greater than
750 ml
(*p < 0.05)
Future Analysis/Future Research
– What is the average number of post-operative catheterizations for patients who develop urinary retention?
– What is the mean time to spontaneous void once cath is required?
– Can POUR incidence be reduced by use of indwelling catheter during surgery or until morning of post-operative day 1?
– Does the incidence of CAUTI differ among groups with intermittent catheterization, catheter during OR only, and indwelling catheter for 24 hours or less? Is there a cost difference?
– Does risk of CAUTI within first 24 hours post-op outweigh potential patient comfort, adverse outcomes, and costs associated with ultrasound use, intermittent cath supplies, and nursing time?
20
References
1. Baldini, G., Bagry, H., Aprikian, A., & Carli, F. (2009). Postoperative urinary retention: Anesthetic and perioperative considerations. Anesthesiology, 110(5), 1139-1157.
2. Brouwer, T. A., Eindhoven, B. G., Epema, A. H., & Henning, R. H. (1999). Validation of an ultrasound scanner for determing urinary volumes in surgical patients and volunteers. Journal of Clinical Monitoring & Computing, 15(6), 379-385.
3. Cabezon Gil, P., Lopez Yepes, L., Fernandez Perez, C., Barreales Tolosa, L., Montoya Gonzalez, P., & Lopez Timoneda, F. (2009). [Validity and reliability of bladder ultrasound imaging for noninvasive estimation of urine volume in a major outpatient surgery department]. [English Abstract
4. Validation Studies]. Revista Espanola de Anestesiologia y Reanimacion, 56(8), 479-484.
5. Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159.
6. Feliciano, T., Montero, J., McCarthy, M., & Priester, M. (2008). A restrospective, descriptive, exploratory study evaluating incidence of postoperative urinary retention after spinal anesthesia and its effect of PACU discharge. Journal of PeriAnesthesia Nursing, 23(6), 394-400.
7. Gallo, S., DuRand, J., & Pshon, N. (2008). A study of naloxone effect on urinary retention in the patient receiving morphine patient-controlled analgesia. [Randomized Controlled Trial]. Orthopaedic Nursing, 27(2), 111-115.
21
References
8. Hebl, J. R., Dilger, J. A., Byer, D. E., Kopp, S. L., Stevens, S. R., Pagnano, M. W., . . . Horlocker, T. T. (2008). A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. [Evaluation Studies
9. Research Support, Non-U.S. Gov't]. Regional Anesthesia & Pain Medicine, 33(6), 510-517.
10. Hughson, J., Newman, J., & Pendleton, R. C. (2011). Hip fracture management for the hospital-based clinician: a review of the evidence and best practices. [Review]. Hospital practice (1995) Hospital practice, 39(1), 52-61.
11. Keita, H., Diouf, E., Tubach, F., Brouwer, T., Dahmani, S., Mantz, J., & Desmonts, J. M. (2005). Predictive factors of early postoperative urinary retention in the postanesthesia care unit. Anesthesia & Analgesia, 101, 592-596.
12. Lamonerie, L., Marret, E., Deleuze, A., Lembert, N., Dupont, M., & Bonnet, F. (2004). Prevalence of postoperative bladder distension and urinary retention detected by ultrasound measurement. British Journal of Anaesthesia, 92(4), 544-546.
13. National Association of Orthopaedic Nurses. (2010). Practice Points: Postoperative Urinary Retention Retrieved July 16, 2012, from http://www.orthonurse.org/ResearchPractice/NAONPracticePoints/tabid/640/Default.aspx