Embed Size (px)
Citation preview
Kidney International, Vol. 44 (1993), pp. 1289—1297
Expression of glycolipid blood group antigens in single humankidneys: Change in antigen expression of rejected ABO
incompatible kidney graftsAM! ULFVIN, ANNIKA E. BACKER, HENRIK CLAUSEN, SEN-ITIR0H HAKOMORI,
LENNART RYDBERG, Bo E. SAMUELSSON, and MICHAEL E. BREIMER
Regional Blood Center and Department of Surgery, Sahlgren's University Hospital, and Department of Medical Biochemistry, University ofGoteborg, GOteborg, Sweden; Royal Dental Collage, Copenhagen, Denmark; and The Biomembrane Institute, University of Washington,
Seattle, Washington, USA
Expression of glycolipid blood group antigens in single human kidneys:Change in antigen expression of rejected ABO incompatible kidney grafts.Total neutral glycolipid fractions were separated into molecular specieson thin-layer chromatography plates and detected by immunostainingwith monoclonal anti-blood group antibodies. Blood group A antigensbased on type 1, 2, 3 and 4 carbohydrate core saccharides were presentin kidneys of A1 and A1B individuals. Blood group A2 individualsexpressed only small amounts of A antigen compared to A1 individualsespecially of the type 3 and 4 compounds. Kidneys from non-secretorindividuals contained less A antigen compared to secretor individuals,and in both groups a variation in the antigen expression between singleindividuals was noted. Blood group A type 2 and 3 (which is anextension of A type 2) antigens were present both as basic 6 and 9 sugarstructures as well as extended saccharide chains migrating in the 8 to IIsugar interval. In contrast, the type 1 chain based A and Lewis antigenswere only present as their basic 5 to 7 sugar chains, and no elongatedstructures were found. Four cases of A2 kidneys initially transplantedinto 0 recipients and removed after 5, 12, 21 days and 4 years,respectively, were also analyzed. Two of these kidneys, originatingfrom the same donor, showed a difference in A antigen expression. Thekidney functioning for four years (lost due to chronic rejection) com-pletely lacked X antigen with five sugar residues (present in all otherindividuals) and contained a large amount of A antigens. This showsthat the expression of antigens in an incompatible transplated organ canbe changed post-transplantation, and that the organ can function even iflarge amounts of incompatible antigens are present.
The chemical structures of the blood group ABH antigensand the structurally related Lewis and X/Y antigens wereinitially elucidated on milk oligosaccharides, ovarian cyst gly-coproteins and erythrocyte glycolipids [1—3]. The structuralcomplexity of these antigens has increased considerably and,for example, at least eleven different blood group A antigenshave been identified so far [4]. The expression of these antigensin tissues and cells is controlled by the ABO, H, Se, P, Le andX genes [2, 5, 6], but also other still unknown factors areinvolved, as exemplified by the difference in expression within
Received for publication May 10, 1993and in revised form July 14, 1993Accepted for publication July 15, 1993
© 1993 by the International Society of Nephrology
organs and cells of a single individual [5, 7—9]. The blood groupABH, Lewis and X/Y antigens therefore have an individual,tissue and cell specific distribution [8] and are present onvirtually every cell in the body. Phylogenetic studies haveshown that these antigens appear earlier in evolution in ecto-dermal or endodermal tissues and cells compared to mesenchy-mal hematopoietic cells [5], Therefore the term "histo-bloodgroup" antigens have been proposed for these carbohydrateantigens [6].
The ABH and related carbohydrate antigens are located onthe cell surface and are proposed to take part in cell-cellcommunication phenomena [10]. They are also targets forantibodies, which was shown in studies of ABO incompatibletransfusion [11] and organ transplantations [12] where bothantigen and individual specific antibody responses were pro-duced in the recipients challenged with incompatible bloodgroup A antigen. Transplantation of kidneys involving majorABO incompatibilities have been performed with good resultsusing an aggressive immunosupression regimen includingspleenectomy [13, 14], and kidneys from A2 donors can betransplanted to 0 recipients using standard immunosuppression[15]. We have described a difference in the expression of Aantigens in human kidney from single individuals using amonoclonal anti-A antibody reacting with all A determinants[15, 16]. In this paper the expression of structurally differentglycolipid based A, Lewis and X/Y antigens in several humankidneys from single individuals are analyzed by use of a panel ofspecific monoclonal antibodies. In addition, blood group A2kidneys transplanted into 0 recipients and later removed aftervarious time periods were also analyzed.
Methods
Kidney specimens
The kidney specimens were obtained from the transplanta-tion unit, Sahlgren's Hospital. The kidneys were discarded forlack of suitable recipients or for technical reasons. The kidneyswere perfused with kidney storage solution, kept cool andsterile. Blood group typing of the donors' erythrocytes wasperformed at the blood bank by standard procedures. Secretor
1289

1290 Ulfvin et a!: Human kidney blood group glycolipids
No A subtypingperformed
Kidney transplanted toa blood group 0recipient andremoved on day 21[15]
Kidney transplanted toa blood group 0recipient andremoved on day 5due to irreversiblevascular rejection,case 11:2 in [12]
Same donor as case13. Kidneytransplanted intoanother group 0recipient andremoved on day 12,case 11:1 in [12].
Kidney transplanted toblood group 0recipient. Removedafter 4 years due tochronic rejection.No Lewis typingperformed.
A Le(a—b+) individuals are regarded as secretors and Le (a+b—) asnon-secretors
b This donor was by printing error incorrectly assigned Le(a—b+) in[12]
status was deduced from the Lewis typing. In some cases bloodgroup A2 kidneys initially transplanted to blood group 0 recip-ients and removed after different time periods were obtainedand analyzed. The blood group types and relevant clinical datafor each kidney specimen are listed in Table 1.
Glycolipid preparationTotal neutral glycosphingolipid fractions were prepared from
the lyophilized kidney tissues as described in detail [171. Theaverage amount of total neutral glycolipid fractions isolatedfrom each non-transplanted kidney was 118 mg (range 61 to 195mg) corresponding to 5.5 mg per g dry tissue weight (range 4.7to 7.9 mg). The values for the transplanted and rejected kidneys
were 272 mg (188 to 334 mg) corresponding to 5.6 mg per g drytissue weight (3.7 to 9.4 mg).
Thin-layer chromatography and immunostaining of the plates
Thin-layer chromatography was performed on HPTLC-alu-minium-plates (Merck, Darmstadt, Germany) and developed inchloroform: methanol: water, 60:35:8 (vol :vol:vol). Detectionwas accomplished by a chemical reagent, anisaldehyde [171 orby autoradiography after incubating the plate with monoclonalanti-blood group antibodies, followed by '251-labeled secondaryantibody using a modification of the method by Magnani et al [8,12, 18].
Monoclonal antibodies and glycolipid reference samples
The mouse monoclonal antibodies, reference glycolipid sam-ples and glycolipid short hand nomenclature used are describedin Tables 2 and 3, respectively.
Results
The total non-acid glycolipid pattern of the human kidneyswere very similar when the plates were stained with a chemicalreagent [9, 15, 16] (not shown). The major components presenthad 1 to 4 sugar residues and small amounts of 5 sugarcomponents are also seen [9, 15, 16]. The amount of complexblood group type glycolipids was estimated to about 1% of thetotal glycolipid fraction [9], and were not seen on the plate usinga chemical reagent but were detected by immunostaining theplates with antibodies [15, 16], as shown in Figure 1. Thestaining of glycolipid antigens on thin-layer plates by biologicalreagents such as monoclonal antibodies, lectins, toxins andbacteria/virus is a qualitative and a "semiquantitative" tech-nique for antigen identification [11, 12, 29, 30]. Therefore, theresults were presented as autoradiograms (Fig. 1) and not asnumeric figures. The anti-A antibody used in Figure 1A recog-nized the terminal A trisaccharide and reacted with all struc-tural variants of A antigens [16]. This antibody revealed a verycomplex pattern of A structures in the kidneys of A1 individuals(lanes 1 to 9) while the A2 individuals stained very faintly (lane10) or not at all (lane 11). In addition to the componentsmigrating as the reference compounds with 6 to 9 sugar resi-dues, several slow moving components with about 10 to 12sugar residues were seen in some of the A1 individuals. The A2kidneys which had been transplanted into 0 recipients were allnegative or faintly stained (lanes 12 to 14), except for one case(lane 15). The antibodies AH-21 and HH-4 are specific for Amonofucosyl structures based on type 1 and 2 core chainstructures, respectively. The AH-21 antibody stained a 6 sugarcomponent present in all A1 kidneys and in some of the A2kidneys (Fig. 1B) while the HH-4 antibody stained componentsin the 8-9 sugar region in some of the A1 kidneys in addition tothe major staining present in the 6 sugar region of all A1individuals (Fig. lC). The A2 kidneys transplanted into 0recipients were all stained in various degrees with the A type 2antibody (Fig. 1C). The TH-1 antibody, specific for A type 3chain compounds (Fig. 1D) reacted with a 9 sugar structurepresent in the A1 kidneys but was absent in the A2 kidneysexcept for a very faint staining in one case (lane 10). The type3 chain compound in the kidneys migrated just below the A-9-3reference compound from human erythrocytes. This difference
Table 1. Blood group type and relevant clinical data for the kidneyspecimens analyzed in the immunostaining experiments
Clinical data andcomments
Lewis typing uncertaindue to old RBCsample
No Lewis typingperformed
Case(lanes inFig. 1)
23
4
5678
910
1112
13
14
15
Blood groupphenotype of
the donorerythrocytes
A1LC(a_b+)aA1Le(a—b+)A1Le(a—b+)
A1
A1Le(a—b+)A1Le(a+b—)A1(Le(a+b—)AB Le(a—b+)
A1B Le(a—b+)A2
A2Le(a+b—)A2Le(a—b—)
A2Le(a+b—)"
A2Le(a+b—)"
A2
No Lewis typingperformed

Ulfvin et a!: Human kidney blood group glycolipids 1291
Table 2. Antigen specificity of the mouse monoclonal antibodies used in the immunostaining experiments
Antibodya Fig. I Code no. Specificity Reference
Anti-A all variants A A581 Dakopatts Terminal A trisaccharide [16]Anti-A type 1 B AH-21 A type 1, monofucosyl [19]Anti-A type 2 C HH-4 A type 2, monofucosyl [4]Anti-A type 3 D TH-l A type 3 [20]Anti-A type 3 and 4 E HH-5 A type 3 and 4 [4]Anti.ALeb F HH-3 A type 1, difucosyl [21)AntiLea G XALA Chembiomed Lea terminalAntiLet H 9ALB Chembiomed Leb and H type I terminalsbAnti-X I SH-l X terminalscAnti-Y J AH-6 Y terminals [21]Anti-B — A582 Dakopatts Terminal B trisaccharide'
a The antibodies were culture supernatants containing 10 to 30 g Ig/mIb This antibody was shown to cross-react with the blood group H type I chain compounds
Singhal A., Nance S., Hakomori S., unpublished observationsd Reacts weakly with difucosylated structures
Table 3. Reference glycolipid samples used in the immunostaining experiments
Short handdesignationa Glycolipid structure Tissue source Reference
E Total non-acid glycolipid fraction Erythrocytes of a human [22]A1Le(a—b+) secretor individual
A-6-1 GalNAcal-3(Fucal-2)Gall3l-3GlcNAcI3l-3GalI3l-4Glcf3l-lCer Human meconium [23]A-6-2 GalNAcal-3(Fucal-2)Gal/3l-4GlcNAc/31-3Gall-4Glcfll-lCer Dog small intestine [24]A-7-l GalNAcal-3(Fucal-2)Gall-3(Fuca1-4)GlcNAcl-3Gal/31-4Glc/3l- ICer Human meconium [23]A-7-4 GalNAcal-3(Fucal-2)Galj3l-3GaINAc/3l-3Galal-4Gal/3l-4Glc/31-lCer Human kidney [25]A-9-3 GalNAcal-3(Fuca1-2)Galpl-3GalNAcal-3(Fucal-2)GalI31-4GlcNAcl-3 Human erythrocytes [4, 26]
Ga1131-4GlcI3l-lCerLea5 Gal/31-3(Fucal-4)GIcNAcI3I-3Gal/3l-4Glc/3l- ICer Human small intestineLeb6 Fucal-2GalI3l-3(Fucal-4)GlcNAc/31-3Galf3l-4GlcI3l- ICer Human small intestine
[27][7]
X-5 Galf3l-4(Fucal-3)GlcNAc/31-3Gal/3l-4Glc/3l-lCer Dog small intestine [28]Y-6 Fucal-2Gal/3l-4(Fucal-3)GlcNAcj3l-3Galf3l-4Glc/31-lCer Dog small intestine [28]
a For blood group glycolipids, the letter indicates blood group determinant, the first numeral the number of sugar residues, and the secondnumeral the type of carbohydrate chain
in mobility was most likely due to a more hydroxylated ceram-ide [31] than to a different carbohydrate structure. The HH-5antibody recognizing both type 3 and 4 chain A compoundsreacted with several bands in the A1 kidneys of which the A-7-4and A-9-3 were the dominating compounds (Fig. 1E). For theA2 kidneys a weaker and more variable staining was seen. Therelatively weak staining of A type 3 and 4 compounds in FigurelA compared to Figure IE was due to a weaker reactivity ofthese antigens with general anti-A antibodies recognizing theterminal A trisaccharide [20]. Blood group A difucosyl type Ichain (ALeb) compounds with 7 sugar residues were present inall A1 kidneys (Fig. iF) but the staining of A1Le(a+b—)individuals was weaker (lanes 6 and 7) and the A2 kidneys (lanes10 and 11) were negative while the transplanted kidneys (lanes12 to 15) showed a variable staining.
The anti-B antibody reacted only with the blood group ABkidneys (cases 8 and 9) as expected (not shown). The stainingwas present only in the 6 sugar region of the chromatogram, incontrast to blood group B kidneys obtained at autopsy [32]which also contained blood group B compounds in the 7-8 sugarinterval, most probably originating from erythi-ocytes trappedin the organ. The antiLea antibody stained a five sugar com-ponent present in variable amounts in all A1 kidneys and insome of the transplanted A2 kidneys (Fig. 1G). Leb antigenswith 6 sugar residues were present in a similar manner (Fig.
lH). In some cases (for example, 7) Leb antigens were found ina serological Leb negative individual, a phenomenon reportedbefore for human meconium [33] and small intestine [8].
The X antigens are the type 2 chain isomers of the Leaantigens, and these were detected by the SH-1 antibody react-ing with the terminal X trisaccharide determinant. This anti-body reacted with a 5 sugar component present in all kidneys(Fig. LI) except case 15. The X-5 glycolipid has been structur-ally identified as one of two components present in the 5 sugarband detected by the chemical staining of the plates [9, 321. Inthe transplanted kidneys several bands were stained (lanes 12 to15) migrating below the 5 sugar component. These are probablyelongated repetitive X structures originating from white bloodcells trapped in the rejected organs, since granulocytes havebeen shown to contain large amounts of these components [34].A similar distribution for the corresponding Y antigens (type 2chain isomers of Leb) was also found (Fig. U) with only traceamounts of a 6 sugar component in some of the nontransplantedkidneys, while several slow moving bands were seen in thetransplanted cases (lanes 12 to 15).
Discussion
The kidneys analyzed are a unique human tissue collectionobtained during a ten year period. Since the kidneys were

A A all types
V
S S S a S a — a a— r — — — —a
2345 6 7892E %::11o1112131415:E
B A type 1
ssA-6-1- 1 10 11 12 13 14 15
C A type 2
4-6-21 2 3 4 5 6 7 6 9A6-2E A-6-21 1011 121314 I5A-6-2E
P Atype3
a aa—I
A-9-3 1 2 3 4 5 6 7 6 9 A-9-3 E 1 10 11 12 13 14 15 E
1292 Ulfvin et at: Human kidney blood group glycolipids
A1-Kidneys A2-Kidneys

11
I n
I. M
pans
1*
4..
I: -l col 's
r 1
:1 1t
' I
-J a
* a C0
I. -'
r a
p.
Ulfvin et a!: Human kidney blood group glycolipids 1293
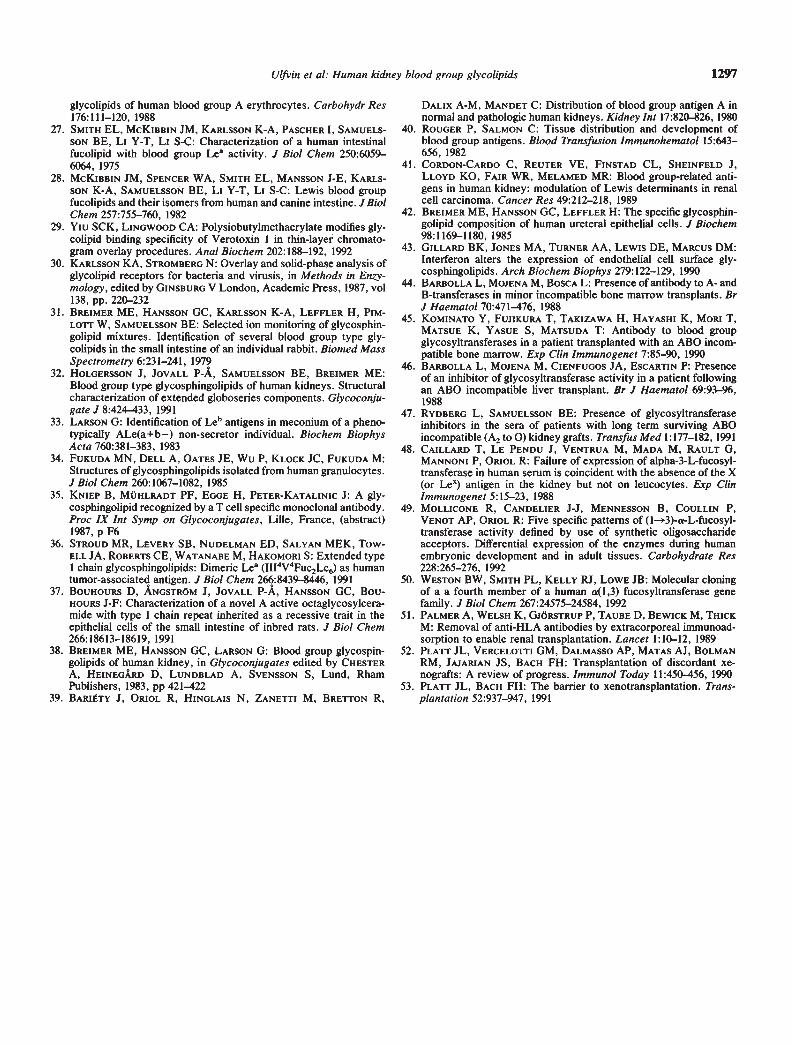
Fig. 1. Autoradiograms of thin-layer plates immunostained with different monoclonal anti-blood group antibodies. Total neutral glycosphin-golipid fractions isolated from single human kidneys (lanes ito 15), erythrocytes and appropriate pure reference glycolipids were applied on eachplate. Blood group status of the tissue donors, the structures and shorthand designation of the reference compounds are listed in Tables I and 3,respectively. The kidney fractions were subgrouped into blood group A1 (left column, lanes I to 9) and A2 (right column, lanes 10 to 15), of whichcases 12 to 15 were A2 kidneys transplanted to blood group 0 individuals and removed after various time periods (Table I). The monoclonalantibodies used were: A, A581; B, AH-21; C, HH-4; D, TH-I, E, HH-5; F, HH-3; G; XALA; H, 9ALB; I, SH-l; and J, AH-6. The specificity ofthe monoclonal antibodies is given in Table 2. The amount of glycolipid substance applied was about 40 jsg of the kidney fractions, 20 jig of theerythrocyte fraction and 0.2 jig of each pure reference compound. The chemical staining of plates (not shown) revealed no differences betweenthe individuals [15, 16], since the blood group components make up only about 1% of the glycolipis and are not detected by chemical staining [9].Arrows indicate sample origin.
E Atype3and4
A-7-1 1 2 3 4 5 6 7 8 9A-7-1 E A-7-1 1 10 11 12 13 14 15Fig. 1. Continued
intended for transplantation, they were perfused with saltsolution, removing plasma and blood cells, and thereafterstored sterile at low temperature. For most of the cases anextended blood group typing (A1/A2 and Lewis) of the donorerythrocytes was performed, but in some of the cases this wasnot possible due to lack of blood samples. From the Lewiserythrocyte phenotype, the secretor status was be concludedwhere Le(a+b—) individuals are regarded as non-secretors andLe(a—b+) as secretors.
The expression of A antigens in the kidneys is very complexwith both quantitative and qualitative differences between theindividuals. Comparing the A1, (Fig. lÀ through F, lanes I to 9)and A2 (lanes 10 to 11) kidneys, the A1 kidneys contain largeramounts and have a more complex expression of the A antigensthan the A2 kidneys. However, within the A1 group consider-able differences are seen of which some, but not all, can berelated to the secretor (lanes 1 to 5) and non-secretor (lanes 6 to7) status. The A type 2 and A type 3 (which is an extension of


Ulfvin et a!: Human kidney blood group glycolipids 1295
type 2; Table 3) antigens are present both as the basic A-6-2 andA-9-3 structures and with extended saccharide chains migratingin the 8 to 11 sugar interval (Fig. lC and E). In contrast, thetype 1 chain compounds are only present as their basic struc-tures with five (Lea5), six (A-6-1, Le'-6) and seven (A-7-1)sugar residues. The only extended type 1 chain core saccharideidentified so far in human tissues is a repetitive Lea structurewith eight sugar residues found in human meconium [35] andsmall intestine [36] (Holgersson J, Jovall p-A, Karisson K-A,Breimer ME, unpublished observations). A blood group Aoctaglycosylceramide with a repetitive type 1 chain core sac-charide has been found in rat small intestine [37]. For the type2 chain antigens X and Y, only 5 and 6 sugar compounds,respectively, were identified in the non-transplanted kidneys(Fig. 11 and J, lanes 1 to 11) but using another anti-X-antibodya 7 sugar component was seen in some of the cases analyzed atthat time (38].
Immunohistochemical studies have shown that the ABH,Lewis and related antigens are specifically distributed in thehuman kidney. The ABH antigens in the vascular epitheliumand the X antigens in the proximal convoluted tubules anddescending limb of the loop of Henle are expressed independentof the secretor gene, while the ABH and Lea/Leb antigens in thedistal tubules and collecting tubules are secretor dependent[39—41]. The expression of different blood group antigens incertain tissues and cells has also been correlated to the embry-ological origin of the tissues [5]. Blood group glycolipids arealso known to have a tissue and cell specific distribution [7—9]and a correlation between the number of hydroxyl groups in theceramide part and the distribution in different cells has beendocumented [7, 8, 42]. From the thin-layer mobility and massspectrometry analysis [9] (Holgersson, J, Jovall p-A, KarlssonK-A, Breimer ME, unpublished observations) the A type 2chain structures contain less hydroxylated ceramides comparedto the type 3 chain structure. This may indicate a differentcellular distribution of these compounds, that is, type 2 chaincompound in the vascular endothelium and type 3 structures inthe distal and collecting tubules. This also fits with the secretordependent expression of A antigens in the distal and collectingtubules since the amount of A type 3 chain structures are low innon-secretors (Fig. lD and E, lanes 6 and 7).
From the results presented here, it can be concluded that theexpression of the structurally different A antigens in the humankidney cannot be established from routine blood group typing ofthe donor erythrocytes, which is the major donor/recipientselection criterion in organ transplantation. The possibility tocross the ABO barriers in kidney transplantation has beenshown both by using immunologic modifications of the recipi-ents [13, 14] and using standard immunosuppression regimens[15]. In certain situations, the possibility to cross the ABObarriers may be necessary, and in these cases a more detailedknowledge of the antigen expression in the organ to be trans-planted would be of benefit to select a "low antigenic" organ,such as cases 6, 10 and 11 in Figure 1. The use of a panel ofmonoclonal anti-blood group antibodies for serological tests orimmunohistological studies of an organ biopsy may be thesolution for this problem.
An interesting finding is the difference in blood group glyco-lipid antigen expression in the two blood group A2 kidneysobtained from the same donor and transplanted into two differ-
ent blood group 0 recipients (cases 13 and 14 in Fig. 1corresponding to cases 11:1 and 11:2 in ref. 11). Kidney number13 was removed on day 5 post-transplantation and case 14 onday 12. Kidney 13 was probably not circulated for more thanone to two days. Several reasons for the low amounts of Aantigens present in case 14 seem possible. Destruction of theantigens by the immune system would result in less antigenexpression in the kidney lost after two weeks compared to theone removed after five days. Another possibility would be aninfluence on the expression by cytokines, for instance gammainterferon, which has been shown under experimental condi-tions to reduce the expression of neutral glycospingolipids, likegloboside, on endothelial cell surfaces [43]. Still another possi-bility could be the presence of glycosyltransferase inhibitors ofan antibody nature being produced in the recipient, influencingthe activity of the A-transferase and thus reducing the A antigenexpression. Such glycosyltransferase inhibitors have beenfound in ABO-incompatible bone marrow transplantations [44,45], in liver transplantation [46] and in renal transplantation[47]. The sera of patients 13 and 14 obtained four to five weeksafter transplantation were investigated for inhibitory activityagainst A-glycosyltransferase, but no such inhibitor was found(cases 9 and 10 in ref. 47). The reduced expression of antigensin case 14 compared to case 13 as investigated by thin-layerchromatography was compared with expression of A antigensin paraffin-embedded tissue sections by immunofluorescence.No major difference in expression could be detected by thistechnique (Rafael Oriol, personal communication). This doesnot, however, rule out a quantitative difference since the tissuesections only reveal the situation in a small areal of the organ.We have recently obtained two kidneys from one single donorof blood group A1Le(a—b+) and prepared the glycolipid frac-tions from each kidney separately. Immunostaining of theglycolipid fractions with anti-A antibodies revealed a bloodgroup pattern similar to cases 1 and 3, and no qualitative orquantitative difference between the two kidneys was found(data not shown). Therefore the change in glycolipid A antigenexpression in the transplanted pair of kidneys has occurredpost-transplantation. The large amount of extended X antigensfound in the transplanted kidneys (Fig. 11, lanes 12 to 15) mostprobably originates from white blood cells in the rejectedorgans since complex X glycolipid structures are major compo-nents in human granulocytes [34]. The origin of the extended Yantigens present in the transplanted kidneys (Fig. 1J, lanes 12 to15) may be explained in a similar way, but to our knowledge Yantigens have so far not been found in plasma or the variousblood cell components.
The complete absence of the X-5 compound in the A2 kidneytransplanted into an 0 recipient which functioned for four years(Fig. 1!, lane 15) is of particular interest. Since the X-5 antigenis present in all the non-transplanted kidneys (cases I to II) itoriginates from the kidney tissue itself. Immunofluorescencestudies have shown that the X antigen determinant is restrictedto the proximal convoluted tubules and some single granulo-cytes present in the interstitial compartment [48]. The absenceof the X-5 antigen in case 15 may be due to either lack of theantigen before transplantation or a change in the expressionoccurring post-transplantation as discussed above. Several dis-tinctly different a-3-fucosyltransferase activities have beenfound in human tissues [5, 49, 50]. No individual lacking the

1296 Ulfvin et a!: Human kidney blood group glycolipids
myeloid type of enzyme has been described so far, and only 11individuals lacking the plasma enzyme have been identified andall were found to be Lewis negative, Le(a—b—) [48, 49]. Thelow frequency of individuals lacking the a-3-fucosyltransferase,and the fact that the kidney of case 15 contains ALeb, Lea andLeb antigens (Fig. iF, G and H) makes it unlikely that the X-5antigen was absent in the kidney prior to transplantation. If theabsence of X-5 antigens is caused by a lack of enzyme activity,this is most probably due to a lack of the al-3 fucosyltrans-ferase since the presence of A-6-2 compounds (Fig. 1C, lane 15)shows that elongation of the type 2 chain precursor (neolac-totetra) is possible. However, it was not possible to test for thissince no fresh tissue from that case was available. The other A2kidneys transplanted into 0 recipients (cases 12 to 14) allcontain the X-5 compound, suggesting that the disappearance ofthis component occurred later in the post-transplantation pe-riod.
The problem with hyperacute rejection of allografts causedby anti-ABH or anti-HLA class I antibodies has been overcomeby removing the offending antibodies prior to the transplanta-tion, and thereafter maintaining antibody depletion for a finiteperiod [13, 51]. After this period the engrafted organ wouldcontinue to function despite the return of the antidonor anti-bodies and the presence of an intact complement system. Thisphenomenon has recently been referred to as "accomodation"[52, 53]. In our study, case 15 may be an example of thisphenomenon. This blood group A2 kidney transplanted into ano recipient functioned for four years and was lost due tochronic rejection. The removed kidney contained large amountsof blood group A antigens (Fig. 1A to C, and E, lane 15). At thetime of removal of this ABO incompatible kidney, the recipientanti-A agglutinin titer against A1 erythrocytes was 1:16 and theindirect antiglobulin titer 1:32. This shows that "accomoda-tion" can occur also when the incompatible antigens arepresent in the organ.
Acknowledgments
The work was supported by grants from the Swedish MedicalResearch Council (No. 6521 and 8452) and the authors are indebted toK.-A. Karlsson, 0. Larson and N. Stromberg for the gifts of A type I,2 and 3 glycolipids, and to R. Oriol for performing immunohistochem-istry on tissue sections from cases 13 and 14.
Reprint requests to Michael E. Breimer, M.D., Ph.D., Department ofSurgery, Sahlgrens Hospital, S-413 45 Goteborg, Sweden.
References
I. HAKOMORI 5, KOBATA A: Blood group antigens, in The Antigens,edited by SELA M, New York, Academic Press, 1974, vol 2, pp79—140
2. WATKINS WM: Genetics and biochemistry of some human bloodgroups. Proc R Soc Lond B 202:31—53, 1978
3. KABAT EA: Contributions of quantitative immunochemistry toknowledge of blood group A, B, H, Le, I and i antigens. Am J ClinPathol 78:28 1—292, 1982
4. CLAUSEN H, LEVERY SB, NUDELMAN E, BALDWIN M, HAKOMORI5: Further characterization of type 2 and type 3 chain blood groupA glycosphingolipids from human erythrocyte membranes. Bio-chemistry 25:7075—7085, 1986
5. 0iuo R, MOLLICONE R, COULLIN P, DALIC A-M, CANDELIER J-J:Genetic regulation of the expression of ABH and Lewis antigens intissues. Acta Pathol Microbiol Immuno! Scand 100 (Suppl 27):28—38, 1992
6. CLAUSEN H, HAK0M0RI S: ABH and related histo-blood groupantigens; Immunochemical differences in carrier isotypes and theirdistribution. Vox Sang 56:1—20, 1989
7. BREIMER ME: Tissue specificity of glycosphingolipids as expressedin pancreas and small intestine of blood group A and B humanindividuals. Arch Biochem Biophys 228:71—85, 1984
8. BJORK 5, BREIMER ME, HANSSON GC, KARLSSON K-A, LEFFLERH: Structures of blood group glycosphingolipids of human smallintestine. J Biol Chem 262:6758—6765, 1987
9. HOLGERSSON J, CLAUSEN H, HAKOMORI 5, SAMUELSSON BE,BREIMER ME: Blood group A glycolipidantigen expression inkidney, ureter, kidney artery, and kidney vein from a blood groupA1Le(a—b+) human individual. J Biol Chem 265:20790—2798, 1990
10. HAKOMORI 5: Glycosphingolipids in cellular interaction, differen-tiation and oncogenesis, in Sphingolipid Biochemistry, edited byKANFER iN, HAKOMORI S. New York, Plenum Press, 1983, pp.327—379
II. RYDBERG L, BREIMER ME, SAMUELSSON BE: Antibody responsein an ABO-incompatible blood transfusion. Transfusion 28:483—488, 1988
12. RYDBERG L, BREIMER ME, BRYNGER H, SAMUELSSON BE: ABOincompatible kidney transplantations (A2 to 0). Qualitative andsemiquantitative studies on the humoral immune response againstdifferent blood group A antigens. Transplantation 49:954—960, 1990
13. ALEXANDRE GPJ, LATINNE D, CARLIER M, MORIAN M, PIRs0N Y,GIANELLO P, SQUIFFLET JP: ABO-incompatibility and organ trans-plantation. Transplant Rev 5:230—241, 1991
14. OTA K, TAKAHASHI K, AGISHI T, SONDA T, OKA T, UEDA 5,AMEMIYA H, SHIRAMIZU T, OKAZAKI H, AKIYAMA N, HASEGAWAA, KAWAMURA T, TAKAGI H, UENO A: Multicentre trial ofABO-incompatible kidney transplantation. Transplant mt 5(Suppl1):540—543, 1992
15. RYDBERG L, BREIMER ME, SAMUELSSON BE, BRYNGER H: Bloodgroup ABO-incompatible (A2 toO) kidney transplantation in humansubjects: A clinical, serologic, and biochemical approach. Trans-plant Proc 19:4528—4537, 1987
16. BREIMER ME, SAMUELSSON BE: The specific distribution of gly-colipid based blood group A antigens in human kidney related toA1/A2, Lewis, and secretor status of single individuals. Transplan-tation 42:88—91, 1986
17, KARLSSON K-A: Preparation of total non-acid glycolipids for over-lay analysis of receptors for bacteria and viruses, in Methods inEnzymology, edited by GINSBURG V, London, Academic Press,1987, vol 138, pp 212—220
18. MAGNANI JL, SMITH DF, GINSBURG V: Detection of gangliosidesthat bind cholera toxin: Direct binding of 1251-labeled toxin tothin-layer chromatograms. Anal Biochem 109:399—402, 1981
19. ABE K, LEVERY SB, HAKOMORI 5: The antibody specific to type 1chain blood group A determinant. J Immunol 132:1951—1954, 1984
20. CLAUSEN H, LEvERY SB, NUDELMAN E, TSUCHIYA 5, HAKOMORI5: Repetitive A epitope (type 3 chain A) defined by blood group
A,-specific monoclonal antibody TH- I: Chemical basis of qualita-tive A1 and A2 distinction. Proc Nail Acad Sci USA 82:1199—1203,1985
21. CLAUSEN H, MCKIBBIN JM, HAKOMORI S: Monoclonal antibodiesdefining blood group A variants with difucosyi type 1 chain (ALeb)and difucosyl type 2 chain (ALe"). Biochemistry 24:6190—6194,1985
22. LE PENDU i, LAMBERT F, SAMuEL550N BE, BREIMER ME, SEITZRC, URDANIZ MP, SUESA N, RATCLIFFE M, FRANCOISEA, POSCHMANN A, VINAS J, ORIOL R: Monoclonal antibodiesspecific for type 3 and type 4 chain-based blood group determi-nants: Relationship to the Al and A2 subgroups. Glycoconjugate J3:255—271, 1986
23. KARL550N K-A, LARSON 0: Potential use of glycosphingolipids ofhuman meconium for blood group chemotyping of single individu-als. FEBS LetI 128:71—74, 1981
24. MCKIBBIN JM: Fucolipids. J Lipid Res 19:131—147, 197825. BREIMER ME, JOvALL P-A: Structural characterization of a blood
group A heptaglycosylceramide with globo-serier structure. FEBSLett 179: 165—171, 1985
26. BREIMER ME, KARLSSON H, KARLSSON K-A, NILs50N K, SAM-UELSSON BE, STROMBERG N: Structures of the eight- to nine-sugar
Ulfvin et a!: Human kidney blood group glycolipids 1297
glycolipids of human blood group A erythrocytes. Carbohydr Res176:111—120, 1988
27. SMITH EL, McKIBBIN JM, KARLSSON K-A, PASCHER I, SAMUELS-SON BE, Li Y-T, LI S-C: Characterization of a human intestinalfucolipid with blood group Lea activity. J Biol Chem 250:6059—6064, 1975
28. MCKIBBIN JM, SPENCER WA, SMITH EL, MANSSON J-E, KARLS-SON K-A, SAMUELSSON BE, LI Y-T, LI S-C: Lewis blood groupfucolipids and their isomers from human and canine intestine. JBiolChem 257:755—760, 1982
29. Ylu SCK, LINGWOOD CA: Polysiobutylmethacrylate modifies gly-colipid binding specificity of Verotoxin 1 in thin-layer chromato-gram overlay procedures. Anal Biochem 202:188—192, 1992
30. KARLSSON KA, STROMBERG N: Overlay and solid-phase analysis ofglycolipid receptors for bacteria and virusis, in Methods in Enzy-
mology, edited by GINSBURG V London, Academic Press, 1987, vol138, pp. 220—232
31. BREIMER ME, HANSSON GC, KARLSSON K-A, LEFFLER H, PIM-LOTT W, SAMUELSSON BE: Selected ion monitoring of glycosphin-golipid mixtures. Identification of several blood group type gly-colipids in the small intestine of an individual rabbit. Biomed MassSpectrometry 6:231—241, 1979
32. HOLGERSSON J, JOVALL p-A, SAMUELSSON BE, BREIMER ME:Blood group type glycosphingolipids of human kidneys. Structuralcharacterization of extended globoseries components. Glycoconju-gate J 8:424—433, 1991
33. LARSON G: Identification of Leb antigens in meconium of a pheno-typically ALe(a+b—) non-secretor individual. Biochem BiophysActa 760:381—383, 1983
34. FUKUDA MN, DELL A, OATES JE, Wu P, KLOCK JC, FUKUDA M:Structures of glycosphingolipids isolated from human granulocytes.JBiol Chem 260:1067—1082, 1985
35. KNIEP B, MUHLRADT PF, EGGE H, PETER-KATALINIC J: A gly-cosphingolipid recognized by a T cell specific monoclonal antibody.Proc IX mt Symp on Glycoconjugates, Lille, France, (abstract)1987, p F6
36. STROUD MR, LEVERY SB, NUDELMAN ED, SALYAN MEK, Tow-ELL JA, ROBERTS CE, WATANABE M, HAKOMORI 5: Extended type1 chain glycosphingolipids: Dimeric Lea (III4V4Fuc2Lc6) as humantumor-associated antigen. J Biol Chem 266:8439—84.46, 1991
37. BOUHOURS D, ANGSTROM J, JOVALL p-A, HANSSON GC, Bou-HOURS J-F: Characterization of a novel A active octaglycosylcera-mide with type 1 chain repeat inherited as a recessive trait in theepithelial cells of the small intestine of inbred rats. J Biol Chem266:18613—18619, 1991
38. BREIMER ME, HANSSON GC, LARSON G: Blood group glycospin-golipids of human kidney, in Glycoconjugates edited by CHESTERA, HEINEGARD D, LUNDBLAD A, SVENSSON S, Lund, RhamPublishers, 1983, pp 421—422
39. BARIETY J, Oiuoi. R, HINGLAI5 N, ZANETTI M, BRETTON R,
DALIX A-M, MANDET C: Distribution of blood group antigen A innormal and pathologic human kidneys. Kidney mt 17:820-826, 1980
40. ROUGER P. SALMON C: Tissue distribution and development ofblood group antigens. Blood Transfusion Immunohematol 15:643—
656, 198241. CORDON-CARDO C, REUTER VE, FINSTAD CL, SHEINFELD J,
LLOYD KO, FAIR WR, MELAMED MR: Blood group-related anti-gens in human kidney: modulation of Lewis determinants in renalcell carcinoma. Cancer Res 49:212—218, 1989
42. BREIMER ME, HANSSON GC, LEFFLER H: The specific glycosphin-golipid composition of human ureteral epithelial cells. J Biochem
98:1169—1180, 198543. GILLARD BK, JONES MA, TURNER AA, LEWIS DE, MARCUS DM:
Interferon alters the expression of endothelial cell surface gly-cosphingolipids. Arch Biochem Biophys 279:122—129, 1990
44. BARBOLLA L, MOJENA M, BOSCA L: Presence of antibody to A- andB-transferases in minor incompatible bone marrow transplants. BrJ Haematol 70:471—476, 1988
45. KOMINATO Y, FUJIKURA T, TAKIZAWA H, HAYASHI K, M0RI T,MATSUE K, YASUE 5, MATSUDA T: Antibody to blood groupglycosyltransferases in a patient transplanted with an ABO incom-patible bone marrow. Exp Clin Immunogenet 7:85—90, 1990
46. BARBOLLA L, MOJENA M, CIENFUGOS JA, ESCARTIN P: Presenceof an inhibitor of glycosyltransferase activity in a patient followingan ABO incompatible liver transplant. Br J Haemato! 69:93—96,
198847. RYDBERG L, SAMUELSSON BE: Presence of glycosyltransferase
inhibitors in the sera of patients with long term surviving ABOincompatible (A2 toO) kidney grafts. Tránsfus Med 1:177—182, 1991
48. CAILLARD T, LE PENDU J, VENTRUA M, MADA M; RAULT G,MANNONI P, ORIOL R: Failure of expression of alpha-3-L-fucosyl-transferase in human serum is coincident with the absence of the X(or Lex) antigen in the kidney but not on leucocytes. Exp ClinImmunogenet 5:15—23, 1988
49. MOLLICONE R, CANDELIER J-J, MENNESSON B, COULLIN P,VENOT AP, ORI0L R: Five specific patterns of (l—3)-a-L-fucosyl-transferase activity defined by use of synthetic oligosaccharideacceptors. Differential expression of the enzymes during humanembryonic development and in adult tissues. Carbohydrate Res228:265—276, 1992
50. WESTON BW, SMITH PL, KELLY RJ, LowE JB: Molecular cloningof a a fourth member of a human a(1,3) fucosyltransferase genefamily. J Biol Chem 267:24575—24584, 1992
51. PALMER A, WELSH K, GJORSTRUP P, TAUBE D, BEWICK M, THICKM: Removal of anti-HLA antibodies by extracorporeal immunoad-sorption to enable renal transplantation. Lancet 1:10-12, 1989
52. PLAn' JL, VERCELOTrI GM, DALMASSO AP, MATAS AJ, BOLMANRM, JAJARIAN JS, BACH FH: Transplantation of discordant Xe-nografts: A review of progress. Immunol Today 11:450-456, 1990
53. PLATT JL, BACH FH: The barrier to xenotransplantation. Trans-plantation 52:937—947, 1991