Embed Size (px)
Citation preview

S159Abstracts / Journal of Minimally Invasive Gynecology 20 (2013) S133–S181
Conclusion: Most obese women with endometrial cancer can be safelymanaged through laparoscopy with almost the same surgical and survivaloutcomes and hospitalization as women with normal BMIs.
531
Extraovarian Granulosa Cell Tumor of Fallopian Tube: A Case
Report
Barbosa LCR, Campos FSM, Archangelo SDCV, Francisco AMC.
Minimally Invasive Surgery Sector of Gynecology and Obstetrics,
Universidade do Vale do Sapuca�ı - UNIV �AS, Pouso Alegre, MG, Brazil
Study Objective: Report a case of tubal tumor.
Design: Clinical case description.
Setting: Minimally Invasive Surgery sector of Gynecology and ObstetricsService of Universidade do Vale do Sapucai - UNIVAS. Pouso Alegre -MG - Brazil.
Patients: A 62 years old patient, 1G1PN, menopausal for 11 years withoutHT use, presented with back pain. Sonography of the abdome showedcomplex cyst in the left ovarian.
On investigation, tumor markers (CA 125, CEA) were asked with negativeresults.
Intervention: She was submitted to laparoscopy and was evidenced a masswith about 6 cm, vascularized, originated from the distal portion of the leftfallopian tube. Performed resection of the mass, subjected to frozen biopsyshowing malignant neoplastic cells, performed complete staging of ovariantumor. All material was sent to anatomicopathological study.
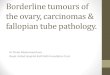
Measurements and Main Results: The result of immunohistochemicalstudy (picture A) showed tubal granulose cell tumor (GCT). Theexpression of alpha-inhibin (picture B) and calretinin (picture C),in thismorphological context, confirms GRANULOSA CELL TUMOR FROMTHE ADULT TYPE. Uterus, both ovaries and the opposite tube, with nosigns of malignancy.
GCTare themalignant sex cord-stromal tumors of the ovary. They constitute1-2% of all ovarian tumors. Rarely GCT can develop at an extraovarian site,but they can arise in locations other than the ovary and may be derived fromthe mesenchyme of the genital ridge. GCTs vary in their gross appearance.Most are partly cystic and partly solid.
Conclusion: The case is reported for its rarity and to describe its relevanceto the histologic origin and in clinical practice. Diagnosis is made bycharacteristic histologic features and by excluding previous GCT of ovary.Immunostains help to differentiate GCTs from other neoplasms.
532
Single Port Access (SPA) Robot-Assisted Laparoscopic Hepatic and
Diaphragmatic Resection in Patients with Advanced and Recurrent
Ovarian Cancer: Farghaly’s Technique
Farghaly SA. The Weill - Cornell Medical College, NYPH- Weill Cornell
University Medical Center, Cornell University, New York, New York
Study Objective: To evaluate the safety and efficacy of single port accessrobot assisted laparoscopic approach to hepatic and diaphragmatic resectionfor metastatic nodules in patients with advanced and recurrent ovariancancer.
Design: Patients with advanced and recurrent ovarian cancer undergoingdiaphragmatic and hepatic resection for tumor involvement of these organs.
Setting: In Patients.
Patients: All patients undergoe preoperative lab work, and contrast-enhanced multi-sliced CT, which is the fundamental imaging modality.All patients undergoe bowel preperation prior to surgery.
Intervention: Da Vinci surgical system is used. A 1.2-1.5-cm vertical intra-umbilical skin incision, and the Alexis wound 106 Advanced GynecologicEndoscopy retractor is inserted into the peritoneal cavity through theumbilicus, two 5-mm trocars and one 11-mm trocar are inserted. A rigid30-degree, 5-mm, endoscope 45 cm long is used. A V-care uterinemanipulator is placed. Da Vinci surgical system is used to perform, totalhysterectomy, bilateral salpingo-oophrectomy, bilateral pelvic adenectomy(including obturator, hypogastric, external iliac, and common iliac lymphnodes). Debulking to less than 0.5 cm in diameter is achieved. At the samesitting intraoperative sonography is performed to examine the liver anddiaphragm to reach for undedctable lesions and to obtain adequate surgicalresection margins. Hepatic resection is performed for metastatic nodules,and diaphragmatic muscle resection is performed to remove metastaticimplants. Then the robot is unlocked, and the skin incisions are sutured.
Measurements and Main Results: Operative time can be maintained in2.5 hours, mean blood loss of 200 ml. and, hospital stay for 4 days.
Conclusion: Farghaly’s Technique of single port access robot assistedlaparoscopic hepatic and diaphragmatic resection in patients withadvanced and recurrent ovarian cancer is safe, feasible, cost effective,with acceptable operative, pathological and short and long term clinicaloutcome. It retains the advantage of minimally invasive surgery. SPAsurgery offers, reduction of operative complications, less postoperativepain, and better cosmetic results.
533
Role of Video-Assisted Thoracoscopic Surgery (VATS) in Case of
Recurrent Ovarian Cancer with Distant Metastasis
Ki K-D,1 Lee J-M,1 Huh C-Y,1 Choi Y-J,1 Oh S-T.2 1Department of
Obstetrics and Gynecology, Kyung Hee University Hospital, Seoul, Korea;2Department of Obstetrics and Gynecology, Chonnam National University
Hospital, Gwangju, Korea
Study Objective: Although primary cytoreductive surgery for epithelialovarian cancer is well accepted as the cornerstone of initial management,the benefits of cytoreductive surgery for patients with recurrent ovariancancer remains unclear. Furthermore, no consensus has been reachedconcerning treatment strategies for recurrent epithelial ovarian cancer.
Design: Case report.
Patients: ; A 29-year-old woman was admitted to our hospital due tosuspicion of recurrent ovarian cancer. Four years previously, she was firstdiagnosed with an ovarian papillary serous adenocarcinoma stage IIIc.She underwent primary debulking surgery followed by six cycles ofadjuvant chemotherapy, which consisted of paclitaxel (175mg/m2) andcarboplatin (AUC=5). A physical examination revealed a palpableinguinal mass and multiple enlarged pelvic lymph nodes. In addition,a mediastinal mass with a well-defined margin was visualized by chest CT.
Intervention: Video-assisted thoracoscopic surgery (VATS) was utilizedfor the cytoreduction of the recurrent ovarian cancer with solitarymediastinal metastasis.
Measurements and Main Results: At the 20-month follow-up the patientwas without evidence of disease.