Embed Size (px)
Citation preview
FINAL CASE STUDY Case 2
Daniel Ma – California State University, Los AngelesDouglas Nguyen – California State University, Los Angeles
CASE SUMMARY• A newborn female has an infected cord stump at 4 weeks and
a high white blood cell count of 71,000/µL. Administration of IV antibiotics helped control the infection and brought the number of WBCs down to 20,000/µL.
• The patient had a brother who developed recurrent skin infections shortly after birth, had an infection in the large intestines, a high WBC count, and succumbed to pneumonia.
• Lab tests showed normal distribution of leukocytes, normal antibody levels, and normal complement levels.
• Rebuck skin window test showed no localization of leukocytes. B cells and NK cells were slightly elevated, and T cells had slight depressed response to mitogens
KEY INFORMATION POINTING TO DIAGNOSIS Marked leukocytosis –Elevated white blood cell count of
71,000/µL, but with normal serum Ig and complement levels.
Omphalitis with cultures from umbilical stump indicate the prescence of E. coli and S. aureus.
Failed Rebuck skin window test with no leukocytes found. Significant family history with a brother who had recurring
infections before dying of staphylococcal pneumonia at age one. Elevated WBC count was observed before death. His umbilical cord wasn’t infected but had delayed separation.

DIAGNOSIS
• From the key information, it is determined that the patient’s condition is due to leukocyte adhesion deficiency (LAD).
• There are three types of LAD. From the information given, the patient has LAD-1.– LAD-2 is associated with mental retardation and distinct
physical appearance– LAD-3 is associated with bleeding disorder
DIAGNOSTIC TESTS FOR LEUKOCYTE ADHESION DEFICIENCY
• Rebuck skin window test
• Flow cytometry using monoclonal antibodies (anti-CD18) to confirm diagnosis and determine if it is LAD-1 (low/absent LFA-1 and CD18) or LAD-2 (defective or no sialyl-LewisX)
• Absolute white blood cell count
• Review of family history and genetic testing of the parents– Sequence analysis to define the exact molecular defect
recommended.
THERAPY FOR DISEASE LEUKOCYTE ADHESION DEFICIENCY
• Aggressive intravenuous first-line antibiotic is needed to control infections.
• Bone marrow/hematopoeitic stem cell transplantation.
• Gene therapy studies have been done but without much success.– Other treatments include interferon gamma, granulocyte
transfusion
• Preimplantation genetic diagnosis (PGD) of leukocyte adhesion deficiency I
PROGNOSIS FOR DISEASE LEUKOCYTE ADHESION DEFICIENCY• Prognosis depends on the severity of the disease. • There are two forms of LAD-1: severe ( <2% expression of CD18)
and moderate (between 2% and 10% expression of CD18).• With the severe form, survival past infancy requires a bone marrow
transplant.– Bone marrow transplant has very high success rate, with 5 year survival rate
greater than 75%• Moderate form has fewer serious infections and can survive to
adulthood with antibiotic treatment during infections.– 50% of the cases survived into their mid-thirties
• Children making it past infancy will need antibiotics to treat recurrent periodontitis.
• Other care:– Oral hygiene– Treat bacterial infections with antibiotics aggressively– Vaccination
HOW WOULD YOU COMMUNICATE DIAGNOSIS AND DISEASE TO THE PARENTS• “Mr. and Mrs. Boleyn I have bad news. Your
daughter has leukocyte adhesion deficiency type 1. We will do more tests to determine the severity of the disease. In the severe case, a bone marrow transplant is necessary for her to survive past infancy. However, the success rate of the transplant is very high and the prognosis will be very good.”
THE THEORETICAL IMMUNOLOGICAL BASIS FOR DISEASE LEUKOCYTE ADHESION DEFICIENCY• LAD-1 is an autosomal recessive disorder with point mutation in the
CD18 gene. The gene is located on chromosome arm 21q22.3.
• Neutrophils are unable to make a tight adhesion to endothelial cells due to defects in the ITGB2 gene that encodes the β2 integrin (also known as CD18).
• This is needed to bind to CD11a to make LFA-1, which binds to ICAM-2 on endothelial cells.
• Peripheral leukocytosis is observed due to the inability of neutrophils to transmigrate to the site of infection.
– In LAD-2, neutrophils are unable to roll because sialyl-LewisX lacks fucose which weakly bind to E-selectins. However, this type of defect is very rare.
– In LAD-3, there is a defect in the β1, β2 , and β3 integrins.
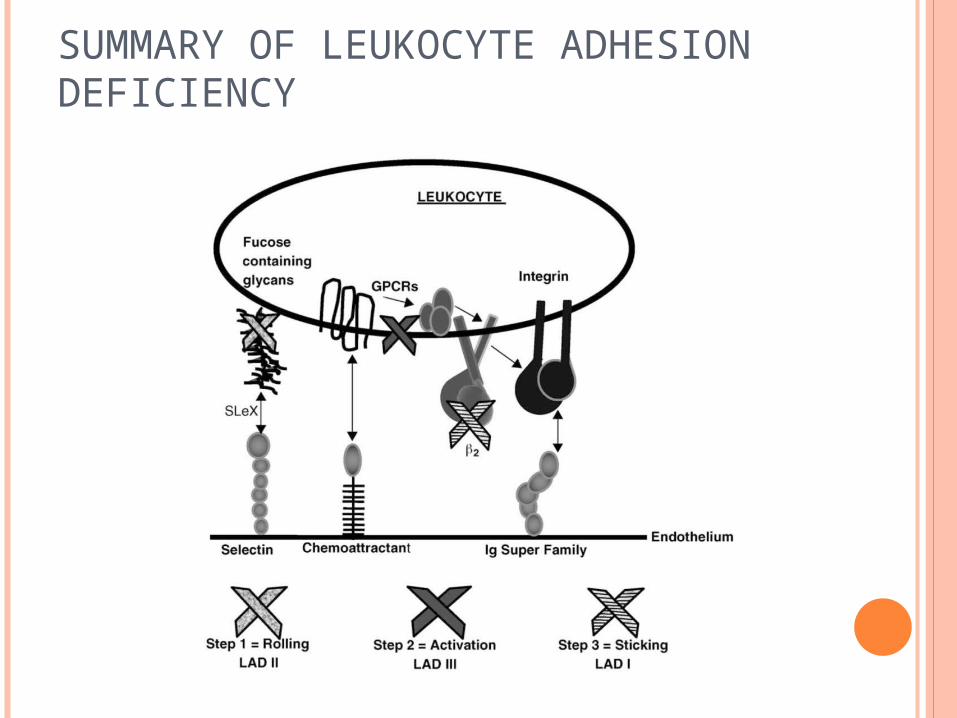
SUMMARY OF LEUKOCYTE ADHESION DEFICIENCY

NEUTROPHIL FUNCTION AND MOLECULAR ANALYSIS IN SEVERE LEUKOCYTE ADHESION DEFICIENCY TYPE I WITHOUT SEPARATION DELAY OF THE UMBILICAL CORD
• Tsai, Y.C., Lee, W.I, Huang J.L., Hung, I.J., Jaing T.H., Yao, T. C., Chen, M.T., Kuo, M.L. Pediatric Allergy Immunol 2008: 19:25-32
• Research objectives: • To investigate neutrophil adhesion moleculre CD11b/CD18, chemotaxis,
phagocytosis, and H202 production in one male infant with LAD-I
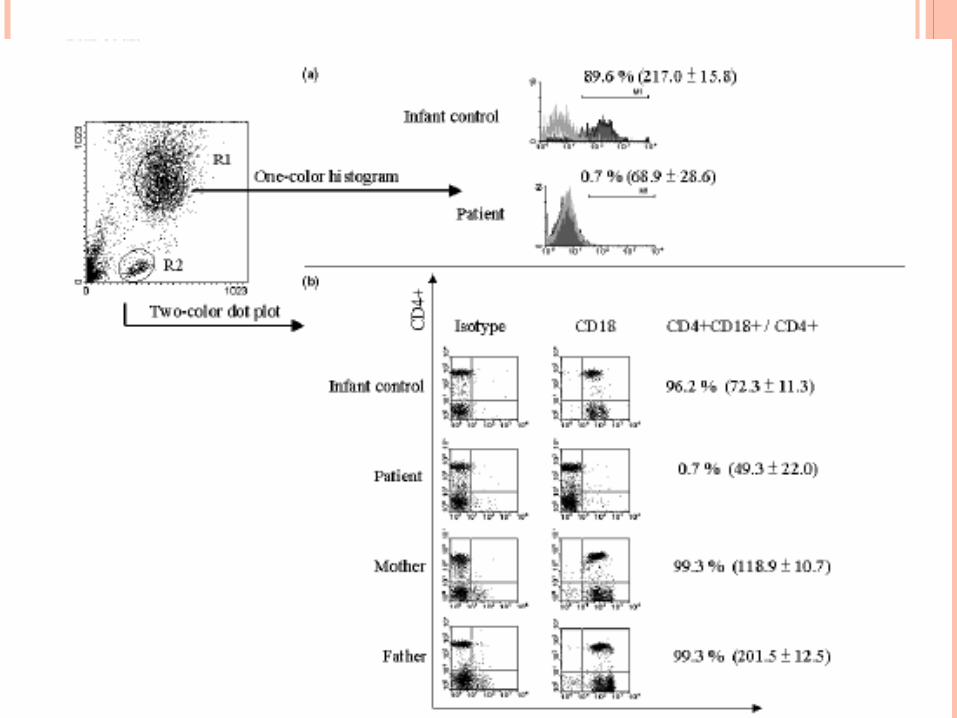
• Experimental set up:• Chemotaxis of PMNs via Boyden chamber using Met-Leu-Phe as the chemokine• Flow Cytometric analysis of expression of CD4, CD18, Mac-1• Phagocytosis Assay in the presence and absence of opsonins • Respiratory burse activity via dichlorodihydrofluorescein diacetate (DCFHDA)
which fluroresce to DCF and detected with spectrophotometer• RT-PCR of CD18 and gene sequencing
• Main Findings:• Migration of patient PMN cells decreased significantly• Phagocytosis of E. coli and S. aureus decreased significantly (27.6% and 53.7%,
respectively as compared to 90% and 70% found in control)• Respiratory burst activity was normal• CD18 were not expressed. LFA-1 (CD11a/CD18) and Mac-1 (CD11b/CD18) were
not expressed.• Parents are carriers, and patient had two truncated mutation that interrupted highly
conserved regions, losing cysteine rich transmembrane and cytoplasma domains
TAKE HOME MESSAGES• Leukocyte adhesion deficiency involves leukocytes of the immune system
being unable to move into tissue.
• Typical symptoms are recurrent infections since birth, periodontal disease, delayed umbilical cord separation, and slow wound healing.
• Diagnostics include Rebuck skin window test, flow cytometry, absolute white blood cell count, review of family history and genetic testing.
• Therapy is based on bone marrow transplantation.
• Prognosis depends if the patient has the moderate or severe form of LAD-1. The severe form will require a marrow transplant, while the moderate form will need antibiotic treatment during bacterial infections. Patients will have recurrent periodontitis if they make it past infancy.
REFERENCES
http://emedicine.medscape.com/article/887236-overview. accessed May 29th, 12:21PM
Murphy et al, Janeway’s Immunobiology. 7th edition, 2008, Garland Science
www.uptodate. Accessed May 29th, 12:35PM
Tsai, Y.C., Lee, W.I, Huang J.L., Hung, I.J., Jaing T.H., Yao, T. C., Chen, M.T., Kuo, M.L. Neutrophil function and molecular analysis in severe leukocyte adhesion deficiency type I without separation delay of the umbilical cord. Pediatric Allergy Immunol 2008: 19:25-32





























