Embed Size (px)
DESCRIPTION
Prevention of spinal ischemia during repair of descending (DTA) or thoracoabdominal aortic aneurysms (TAA). Fabien Koskas, Julien Gaudric CHU Pitié-Salpêtrière, Paris, France. PROTECTION MEDULLAIRE. Clampage médullaire. Hémodynamique. Ischémie médullaire. Hypoxie. Hyperpression LCR. - PowerPoint PPT Presentation
Citation preview

Prevention of spinal ischemia during repair of descending (DTA) or thoracoabdominal
aortic aneurysms (TAA)
Fabien Koskas, Julien Gaudric
CHU Pitié-Salpêtrière, Paris, France





Ischémie médullaire
Clampage médullaire
Hémodynamique
Hyperpression LCR
Hypoxie
PROTECTION MEDULLAIRE

Ischémie médullaire
Clampage médullaire
PROTECTION MEDULLAIRE
Identification groupes à risque
Clampage court <30mnIdentification et réimplantationde l’A. d’Adamkiewicz
Diminution métabolisme médullaireHypothermie profonde / péridurale
Perfusion aortique distaleCEC/shunts
Artifices techniques
Potentiels évoquéssomesthésiques/moteur
Pharmacologie (papavérine intrathécale etc…)

Contrôle tensionnel per op-clampage proximal-déclampage
CEC
Contrôle tensionnel post-opParaplégies 2aires
Contrôle pertes sanguinesCell saver, récupérateurs
Ischémie médullaire
Clampage médullaire
Hémodynamique
PROTECTION MEDULLAIRE

Oxygénateur/CECPaO2 post op
Ischémie médullaire
Clampage médullaire
Hémodynamique
Hypoxie
PROTECTION MEDULLAIRE
exclusion pulm G

Drainage per et post opératoire
Ischémie médullaire
Clampage médullaire
Hémodynamique
Hyperpression LCR
Hypoxie
PROTECTION MEDULLAIRE

Personal experienceOpen surgery of DTA-TAA
1990-2000 DTA % TAA I % TAA II % TAA III % TAA IV % Total %
Dissection 33 8 12 3 34 8 12 3 1 0 92 22
Atheroma 64 15 19 4 41 10 41 10 70 16 235 55
Other 47 11 5 1 19 4 17 4 11 3 99 23
Total 144 34 36 8 94 22 70 16 82 19 426 100
1990-2000 DTA % TAA I % TAA II % TAA III % TAA IV % Total %
Paraplegia 2 1 3 8 18 19 9 13 1 1 33 8
Paraparesis 8 6 3 8 12 13 5 7 1 1 29 7
Total 144 100 36 100 94 100 70 100 82 100 426 100

Mechanisms of postoperative paraplegia after T(EV)AR
• Reversible intraoperative spinal ischemia • Reperfusion injury
– Breakdown of cellular membranes : edema– Spinal compression injury
• Irreversible spinal ischemia– Permanent suppression of the spinal blood supply by the
aortic procedure– Thromboembolic events within the spinal blood supply
• Poor perioperative systemic hemodynamics

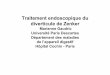
Vascularisation médullaire
ASP
ASA
ASP
Lazorthes G et al. Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-62
ADK: D8-L2=85%
Si ADK<D12: A radiculaire thor moy entre D7-D8
Kieffer E, in Techniques modernes en chirurgie vasculaire 2007

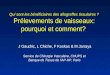
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
VA T3 T4 T5 T6 T7 T8 T9T10T11 T12
L1 L2 L3
Probability %
Adamkiewicz
MDA
SDA
480 personal cases using exhaustive spinal angiograpy
J Vasc Surg 2002;35:262-8.

Ann Vasc Surg 1989;3:34-46.
AK>
AK<
AK=
AK?

Risk of paraplegia/paresis after open surgical repair of TAA
Type % Class %
I 15 Ak> <10
II 15-40 Ak< <10
III 10 Ak= 5-50*
IV 10 Ak? 50*Depending upon spinal arterial reattachment
Ann Vasc Surg 1989;3:34-46.

Spinal angiography & Results
1990-2000 DTA % TAA I % TAA II % TAA III % TAA IV % Total %
Ak> 4 1 2 0 0 0 12 3 23 5 41 10
Ak< 26 6 3 1 0 0 0 0 0 0 29 7
Ak= 63 15 28 7 75 18 45 11 17 4 228 54
Ak? 6 1 1 0 13 3 6 1 5 1 31 7
Total done 99 23 34 8 88 21 63 15 45 11 329 77
1990-2000 DTA % TAA I % TAA II % TAA III % TAA IV % Total %
Paraplegia 2 1 3 8 18 19 9 13 1 1 33 8
Paraparesis 8 6 3 8 12 13 5 7 1 1 29 7
Total 144 100 36 100 94 100 70 100 82 100 426 100

Risk of paraplegia/paresis after endovascular repair
• Unknown• Probably globally lesser than after open surgery
– Selection bias – Better perioperative hemodynamics– Conservation of collateral pathways
• Very low, especially in the Ak> and Ak< groups• Not null, especially whenever Ak= or Ak?

Spinal angio versus spinal imaging
• Exhaustive spinal angio (ESA) is our gold standard, especially for open surgery of TAAs II
• ESA is technically demanding, time consuming, expensive and invasive
• EVAR might require a less exhaustive evaluation : selective spinal imaging (SSI)
• With modern CT technology, more and more cases can benefit from SSI without the need of another acquisition than that necessary to document the aortic lesion*
* Kawaharada et al. Eur J Cardiothorac Surg 2002;21:970-4.
* Yoshioka K et al. Radiographics 2003;23:1215-25


Principles of selective spinal imaging
• Explore all intercostal arteries to be covered by the stent-graft and adjacent
• With multislice CT (16 bit +), using the same acquisition as that taken for imaging the aortic lesion
• With sequential catheterization only in case of a failure
• Classify according to the result

Methods of spinal protection
• Spinal revascularization• Distal perfusion• Spinal or general hypothermia• Spinal drainage• Intrathecal or IV drugs
– Papaverin, steroïds , calcium blockers, radical scavengers, barbiturates, naloxone, PGEI, allopurinol, oxygen carriers etc…

Spinal revascularization
• Systematic and blind• Never• Selective
– Size, topography and backflow of intercostal arteries
– Intra-operative monitoring (evoked potentials)– Pre-operative spinal angiography

Distal perfusion
• Improves the hemodynamic tolerance to cross-clamping
• Reduces the duration of visceral and spinal ischemia

Methods of distal perfusion
• Passive shunt• Extra-anatomic bypass• Active shunt• Cardio-pulmonary bypass
– Better control of flow– Better oxygen transfer– Better control of temperature– But necessitates high doses of heparin

Hypothermic circulatory arrest
• Visceral (and spinal) protection• Avoids difficult or hazardous cross-clamping
– Dissection– Redo surgery– Inflammatory aneurysm
• Eases the anastomosis by the use of an open technique
• But – Bleeding– Sub-optimal myocardial protection through thoracotomy among
cardiac patients


Methods
1990-2000 DTA % TAA I % TAA II % TAA III % TAA IV % Total %
Xclamp 21 5 0 0 1 0 3 1 66 15 91 21
CBP 92 22 23 5 51 12 56 13 13 3 235 56
DHCA 31 7 13 3 42 10 11 3 0 0 97 23
Total 144 34 36 8 94 22 70 16 82 19 426 100

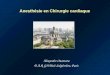
Syndrôme compartimental médullaire
PPerf Med ≈ PA(aortique distale) -P(LCR)
PA : lors du clampage proximalP(LCR) : à cause de l’oedeme médullaire
par phénomene de non réabsorption
Ne prend pas en compte les résistances artériolo capillaires P veineuse
Delayed onset of neurological deficit:signifiance and management.HuynhT et al.Sem in Vasc Surg 2000
Ischémie Ischémie-Reperfusion
PA
P(LCR)

CSF drainage does not target any other mechanism of postoperative paraplegia

CSF drainage is useful at reducing post-ischemic compression injury
27. Miyamoto K, Ueno A, Wada T, Kimoto S. A new and simple method of preventing spinal cord damage following temporary occlusion of the thoracic aorta by draining the cerebrospinal fluid. J Cardiovasc Surg (Torino) 1960;1:188-97.
28. Oka Y, Miyamoto T. Prevention of spinal cord injury after cross-clamping of the thoracic aorta. Jpn J Surg 1984;14:159-62.
29. McCullough JL, Hollier LH, Nugent M. Paraplegia after thoracic aortic occlusion: influence of cerebrospinal fluid drainage. Experimental and early clinical results. J Vasc Surg 1988;7:153-60.
30. Svensson LG, Grum DF, Bednarski M, et al. Appraisal of cerebrospinal fluid alterations during aortic surgery with intrathecal papaverine administration and cerebrospinal fluid drainage. J Vasc Surg 1990;11:423-9.
31. Crawford ES, Svensson LG, Hess KR, et al. A prospective randomized study of cerebrospinal fluid drainage to prevent paraplegia after high-risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991;13:36-45; discussion 45-6.
32. Woloszyn TT, Marini CP, Coons MS, et al. Cerebrospinal fluid drainage and steroids provide better spinal cord protection during aortic cross-clamping than does either treatment alone. Ann Thorac Surg 1990;49:78-82; discussion 83.
33. Safi HJ, Campbell MP, Ferreira ML, et al. Spinal cord protection in descending thoracic and thoracoabdominal aortic aneurysm repair. Semin Thorac Cardiovasc Surg 1998;10:41-4.
34. Bethel SA. Use of lumbar cerebrospinal fluid drainage in thoracoabdominal aortic aneurysm repairs. J Vasc Nurs 1999;17:53-8.
35. Coselli JS, LeMaire SA, Schmittling ZC, Koksoy C. Cerebrospinal fluid drainage in thoracoabdominal aortic surgery. Semin Vasc Surg 2000;13:308-14.
36. Safi HJ, Miller CC, 3rd, Huynh TT, et al. Distal aortic perfusion and cerebrospinal fluid drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ protection. Ann Surg 2003;238:372-80; discussion 380-1.
And at reversing it in some casesGarutti I, Fernandez C, Bardina A, et al. Reversal of paraplegia via cerebrospinal fluid drainage after abdominal aortic surgery. J Cardiothorac Vasc Anesth 2002;16:471-2.
And several unpublished personal cases

Etudes randomisées
Caractéristiques communesType d’études
Randomisation du drainage du LCR en chirurgie aortique thoracique.Chirurgie ouverte seulement (≠endovasculaire)
PatientsATA à haut risque (type I et II)
TechniqueDrainage LCR par ponction lombaire
Autres techniques de protection équivalentes dans les groupes cas et témoin :-CEC atriofémorale
-réimplantation de l’ADK
ObjectifMesure du taux de parésie/paraplégie postopératoire des membres inférieurs
-Crawford (JVS, 1991)
-Svensson (Annals of Thoracic Surg, 1998)
-Coselli (JVS, 2002)

Etude Drainage ContrôleLCR vol/pression
Drainage postop
Crawford 14/46 (30%) 17/52 (33%) 50ml Non
Svensson 2/17 (11,8%) 7/16 (43,8%) 7-10 cmH2O 48h
Coselli 2/82 (2,7%) 9/74 (12,2%) <10mmHg 48h
Etudes randomisées
-Résultats-

Indications du drainage
Indic drainage:-ATA I,II,III et IV si réimplantation ADK
Quel matériel:-Kit drainage externe du LCR. Sophysa(Tuohy 14G, KT multiperforé 60cm, poche de recueuil)

Indications
• SSI positive– Spinal artery(ies) arising from aortic segment to
be repaired– Adamkiewicz , MDA or SDA
• SSI negative– No spinal artery arising from aortic segment
• Surgical risk


SSI negative
• No CSF drainage• Endovascular or open repair in peace of
mind

SSI positive Good surgical risk
Ak / MDA or SDA with large territory• Open surgery with reattachment of critical
intercostal arteries using the best spinal protection methods available
MDA or SDA with small territory• Give objective information to patient• If EVAR preferred, CSF drainage, spinal
monitoring etc.• Retrievable stent-graft* ? • Ishimaru et al, J Thorac Cardiovasc Surg,
1998;115:811
• Midorikawa et al. Jpn J Thorac Cardiovasc Surg 2000;48:761-8

SSI positivePoor surgical risk
• Give information to patient• EVAR if feasible • CSF drainage• Careful monitoring of systemic blood
pressure• Retrievable stent-graft* under spinal
monitoring ?* Midorikawa et al. Jpn J Thorac Cardiovasc Surg 2000;48:761-8 & personal unpublished designs

Personal results with EVAR
• 1996-2003• Systematic ESA• Only 66 TEVAR cases (612 EVAR cases in the same period)• One paraparesis in one hybrid one-stepped
elephant trunk under hypothermic circulatory arrest
• No paraplegia

Conclusion
• Postoperative paraplegia remains a disaster for the patient and a medicolegal concern for surgeons and radiologists
• Given the low rates of paraplegia after DTA repair and the small number of patients in the series of TAA repair, efficiency of protective methods is difficult to demonstrate
• The availability of SSI using CT renders blind repair of DTA or TAA questionable