Embed Size (px)
Citation preview

Journal of Epidemiology and Community Health 1992; 46: 357-361
Factors influencing childhood immunisation in an
urban area of Brazil
Thalia Velho Barreto, Laura Cunha Rodrigues
AbstractStudy objective-The aim was to examine
the factors associated with incomplete vac-cination in an urban area in Sao Paulo,Brazil; and to explore whether differencesin vaccine coverage in the catchment area ofhealth centres remain after the demogra-phic constitution of the population in theseareas is controlled for.Design-The children were selected as
controls for a case-control study. 455 child-ren were selected at random (but agematched) from the health centre registries.Data was collected from the health centrerecords and from home interviews.Setting-All children were registered in
FAISA, a municipal health service compris-ing a large network of health centres andhospitals. FAISA's services are free at thepoint of delivery, and over 85% of the city'schildren are registered.Participants-Participants were selected
to represent, except in their age distribu-tion, all children registered in the municipalhealth service.Measurements and main results-In-
formation was collected on subjects' vaccinehistory, year of birth, sex, birth order andbirth weight, and health centre ofregistration; their mothers' age, education,and marital status; and the family's incomeper capita and history of migration. Analy-sis was undertaken to identify risk factorsfor vaccination and whether the differentialcoverage in health centres' catchment areasremained after demographic character-istics of the population were controlled for.The high coverage for DPT and polio vac-cines suggests that low overall coverage wasnot simply a result of mothers failing tobring children for vaccination. The variablethat best predicted vaccine coverage wasyear of birth. Children born to immigrantmothers or into large families had lowervaccine uptake. The characteristics ofchild-ren and their mothers did not account forthe variation in vaccination coverage incatchment areas of different health centres.Conclusions-It is likely that in this area
vaccination completeness was associatedmainly with the health centre's ability todeliver vaccination to the target population.J Epidemiol Community Health 1992; 46: 357-361
In 1974, The World Health Organization (WHO)launched the "Expanded Program on Immu-nization" (EPI) aiming at reducing the incidence
and mortality due to vaccine preventable diseaseby promoting the expansion of immunisationactivities around the world. According to thelatest estimate, however, 40% of children had notbeen reached by vaccination in 1986 in thedeveloping countries.1
Early studies exploring the reasons why somany children remain unvaccinated have focusedmainly on the demographic characteristics ofchildren and their families.2 Perception of diseaseseverity, and of the efficacy of vaccines in preven-ting disease-the "health belief' model-weresoon recognised as additional important factorsbehind the motivation of parents to seek vac-cination for their children.A0 Several investi-gators argued that beliefs about supernatural dis-ease causation and the efficacy of traditionalmedicine were obstacles to vaccination in deve-loping countries.9 11 Heggenhougen andClement"2 challenge this assumption in a recentreview, suggesting that "people are pragmatic"and use both traditional healers and allopathicservices. Friede et al'3 suggest that both knowl-edge and a positive attitude towards vaccinationresult from access to immunisation services andprevious experience with vaccination.
Studies of demographic characteristics andhealth beliefs have failed to show consistentresults, and recent studies have looked at the roleof the health services.'3 14 Studies carried out inMozambique,14 Ghana,'5 and Brazil'6 havereported low vaccination coverage associated withhealth system related factors, such as shortage ofvaccine at local level, the number of days vaccina-tion was performed, and distance to the nearestvaccination facility. Evidence from developed anddeveloping countries has also identified specificpractices within the health system that lead to lowvaccine coverage: professional health workersdoubting the efficacy of vaccines,'7 having exag-gerated concern about adverse reactions, andfollowing inappropriate contraindications. 17-19Health services personnel failing to make use ofopportunities for vaccination can account for asignificant proportion of the failures to vaccinatechildren.20 Sharp increases in coverage observedin some developing countries associated withmass immunisation campaigns have shown thatthe delivery system plays an important role invaccination uptake.2' 24
MethodsSTUDY POPULATIONAn analysis ofcross sectional data on 455 childrenwas performed to investigate factors associatedwith incomplete vaccination. The study site wasthe municipality of Santo Andre (population half
Faculdade de CienciasMedicas dePernambuco, BrazilT V BarretoLondon School ofHygiene and TropicalMedicine, KeppelStreet, London WC1E7HT, United KingdomL C Rodrigues
Correspondence to:Dr Rodrigues
Accepted for publicationOctober 1991
on 8 January 2019 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.46.4.357 on 1 A
ugust 1992. Dow
nloaded from

Thalia Velho Barreto, Laura Cunha Rodrigues
a million), part of the Greater Sao Paulo area, themost industrialised area of Brazil. A public healthsystem, The Fundacao de Assistencia a Saude deSanto Andre (FAI SA), based on 23 health centresand referral health facilities, provided free andaccessible well baby clinics, vaccination clinics,and paediatric care. About 85% of the childrenunder 12 years in Santo Andre were registered atFAISA during the period of study.The study population consisted of all children
born from 1971 to 1981 who were registered inFAISA. This analysis was restricted to childrenwho were selected as controls in a case-controlstudy on measles vaccine efficacy carried out atFAISA.25 As in the previous study a case basesampling scheme was applied; the sampled child-ren in that study represented not only thosewithout measles but they were also an agematched random sample ofthe children registeredat FAISA's health system. Hence the results ofthe present study can be extrapolated for allchildren of the same age in Santo Andre.26
DATA COLLECTIONData were collected through a review of medicalrecords of the children and a personal interviewwith their mothers. In FAISA, information onpersonal and family characteristics are recorded foreach child at the time of registration. Homeinterviews were conducted by trained interviewersusing a pretested standardised interview schedule.
Immunisation status was ascertained fromeither medical records or vaccination cards. InFAISA, information on vaccination is part of thechild's medical record and a copy of the vac-cination card is given to the mother. Informationwas collected on potential risk factors for incom-plete vaccine uptake. Data on child's birth order,birth weight, child's year of birth and sex, andmother's marital status and literacy were ascer-tained from the medical records. In addition,information on age of mother, family income percapita, and mother's length of residence in SantoAndre was obtained from home interviews.
METHODS OF DATA ANALYSISVaccination status was obtained for four vaccines;oral polio (poliomyelitis), DTP (diphtheria-per-
tussis-tetanus), BCG (tuberculosis), and measles.Children were defined as completely vaccinated ifthey had received the basic series of vaccinesrecommended by the state of Sao Paulo immunis-ation programme: three doses of DPT, threedoses of oral polio, and one dose of BCG, and formeasles, either one dose after 12 months, or onedose before 12 months followed by a booster.Since only 21 children had received no vac-cination at all, the children with incompletevaccination were grouped with those never vac-cinated. Vaccination coverage was derived forindividual vaccines and for the complete scheme.Income per capita was grouped in quartiles of
frequency. Mothers were classified into fivegroups according to time since migration. Thesewere later collapsed into recent migrants andothers (10 years since migration and natives).
Children were assigned to the health centre ofregistration. Health centres were classifiedaccording to the level of coverage of children fromtheir catchment area in either three groups: low(less than 400/ ), medium (40 to 60%,/), and high(over 600o), or two groups: low (less than 50tiO)and high (500o/ or more).The extent to which differences in coverage in
children living in particular health centrecatchment areas were explained by the children'sdemographic characteristics was determinedusing univariate analysis. The associationbetween each risk factor and level of coverage onthe catchment area defined as low or high wastested using Pearson's X2 test.The analysis of the association between demo-
graphic characteristics and vaccination inindividual children was conducted in two steps.Firstly, a univariate analysis was performed toassess the association between vaccination and theindependent variables. Odds ratios were calcu-lated using as the baseline the stratum with lowestrisk for incomplete vaccination. Test based (Miet-tinen's methods) 950h confidence limits for theodds ratio were produced on SAS.27 The associa-tion between each risk factor and vaccination wastested using Pearson's x2 test. Stratified x2 wasused to evaluate linear trends. Secondly, multiplelogistic regression was performed to assess theindependent effect of each variable, using thecomputer program EGRET.28 Those variables
-a
(0
100
80
60
40
20
10a)
8a,
6
4
2
Figure 1 Percentage ofchildren fully vaccinatedfor each type of vaccineby year of birth.
7 7
/
7
/
1972 73 74 75 76 77 78 79 80 81
Polio (complete basic series)
10
10
!0
0
1972 73 74 75 76 77 78 79 80 81
BCG
100 _
80
60
40-
1C
7;
HHU/ OI
U1 F-A V,,- -,,,,,,--,L- -
1972 73 74 75 76 77 78 79 80 81
DPT (complete basic series)
10
O _
1972 73 74 75 76 77 78 79 80 81
Measles
I
358
,1
on 8 January 2019 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.46.4.357 on 1 A
ugust 1992. Dow
nloaded from

Childhood immunisation in an urban area of Brazil
showing a statistically significant association at the5% level on the x2 test in the univariate analysiswere included in the multivariate analysis.
Finally, the health centres of registration wereaggregated into the model, in order to assess theindividual contribution of demographic char-acteristics and health centre practices.
ResultsOf the 455 children studied, 214 (47%) were fullyvaccinated and 241 (53%) had incomplete vacci-nation. The degree of compliance was high foreach specific vaccination, and only 21 (4 6%) ofthe children had not received at least one dose ofone of the four vaccines.An increase in vaccine coverage with time
during the whole period was evident. Figure 1shows the proportion of children vaccinated byyear of birth for the four types of vaccine. Therewas a linear trend with time in the proportion ofchildren fully vaccinated, presented in fig 2, from0% in 1971 birth cohort to 80% for those born in1981 (p<0-001).Figure 3 shows the percentage of children fully
vaccinated by each type of vaccine. As DPT andoral polio are usually given together, the per-centage of fully vaccinated children was similar forthe two vaccines. The percentage of children whohad received three doses of antipolio vaccine(87 7%) was markedly higher than that of thechildren who had only one (4 4%) or two doses(2 0%). The same was true for DPT vaccination:4-6% had received one dose and 5-3% two doses,compared to 84-0% who had completed the DPTprimary course (three doses). The percentage ofchildren adequately vaccinated withBCG (69 5%)and measles (63-8%)-which require a singel vac-cination each-was lower than we expected andshowed the most marked increase with time.
There was a wide variation in vaccinationcoverage according to the health centre to whichchildren were registered. Table I presents themean, standard deviation, and the range of cover-age for each specific vaccine and for completevaccination across the 23 health centres. Theproportion of completely immunised childrenvaried from 26-5% to 78-6% in different healthcentres. Themean value was 48-2% with standarddeviation of 15 5%.
In order to explore whether the difference invaccination coverage among health centres wasassociated with the demographic characteristics ofits users we looked at the proportion of single andilliterate mothers, and the frequency distributionof mother's age, income per capita, number ofyears mothers were living in Santo Andre, andchild's birth order in health centres with coveragebelow and above 50%. None of these weresignificantly different (table II) in the two groupsof centres.Table III shows unadjusted odds ratios and
95% confidence intervals (CI) for the associationbetween vaccination and demographic char-acteristics. Illiteracy and marital status ofmothers, birth weight and sex of children, andfamily income per capita did not influence vacci-nation uptake. High birth order and year of birthofthe child, mother's migration into Santo Andre,age of mothers, and health centre of registrationwere significantly associated with incompleteimmunisation (p < 0-05) and were included asregression terms in the multivariate analysis.Age of mothers lost its significance when
adjusted for the year of birth of the child. Onlymother's migration into Santo Andre, child'sbirth order, and year of birth remained statis-tically significant. The adjusted odds ratio ofbeing inadequately vaccinated, in a model that
Figure 2 Percentage ofchildren fully vaccinatedby year of birth. Test forlinear trend p < 0 001
Figure 3 percentage ofchildren with completescheme for each vaccine.
caD 100
= 80
- 60
40C- 20a)
0'lOO-
Ca)I. 80
to
.C
2 20
0400)
1972 73 74 75 76 77 78 79 80 81
les All
Table I Vaccine coverage in health centre catchment areas: mean, standarddeviation, minimum, and maximum.
Health centre coverageStandard
Mean deviation Lowest HighestDPT 82-9 9 0 600 96-7Polio 87-3 9-7 66-7 100 0BCG 70-8 14.1 448 92 3Measles 63-8 13 4 41 7 84-6All vaccines 48-2 15 5 26-5 78 6
Table II Demographic characteristics of childrenregistered in health centres with low and high coverage.
Vaccination coverage'Low High% (number) 0 (number)
Mother living in Santo Andre*Native 17-6 (41) 23-3 (27)1-2 years 5 6 (13) 2 6 (3)3-9 years 14-2 (33) 11-2 (13)10+years 62-7 (146) 62 9 (73)
Birth order*FirstSecondThird-fourthFifth
Mother's age (years)*<2525-2930-3435-3940+
Marital status*MarriedSingle
Mother's literacy*LiterateIlliterate
377 (100)19-2 (51)28-7 (76)14-3 (38)
8-6 (23)22-8 (61)31-0 (83)21-3 (57)16 4 (44)
40 4 (55)25-7 (35)17 6 (24)16 2 (22)
14 7 (21)25-9 (37)21-0 (30)20 3 (29)18 2 (26)
92-5 (135) 93-4 (256)7 5 (11) 6 6 (18)
918 (245) 92-9 (130)8-2 (22) 7-1 (10)
Incomeb*Less than 20$US 22-9 (55) 27 3 (38)21 to 38$US 25-4 (61) 31 7 (44)39 to 675US 22-9 (55) 23-7 (33)More than 685US 28-8 (69) 17-3 (24)
'Coverage low<50%; high> 50%bFamily income per capita per month.*No significant differences found/Pearson's x test: twotailed p value >0 05.
359
on 8 January 2019 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.46.4.357 on 1 A
ugust 1992. Dow
nloaded from
Thalia Velho Barreto, Laura Cunha Rodrigues
included year of birth2-75, p = 0022) for a tl240(95% CI = 1-29-4born to a migrant mo
If the variation in v
catchment area of he,these individual charano variation would rerrcharacterstics were coiexplore the effect of theexamined the associatiof registration (groupaccording to its level ofcontrolling for the effilength of time mothersbirth order. Adjustmelittle effect on the resttration remained an irn
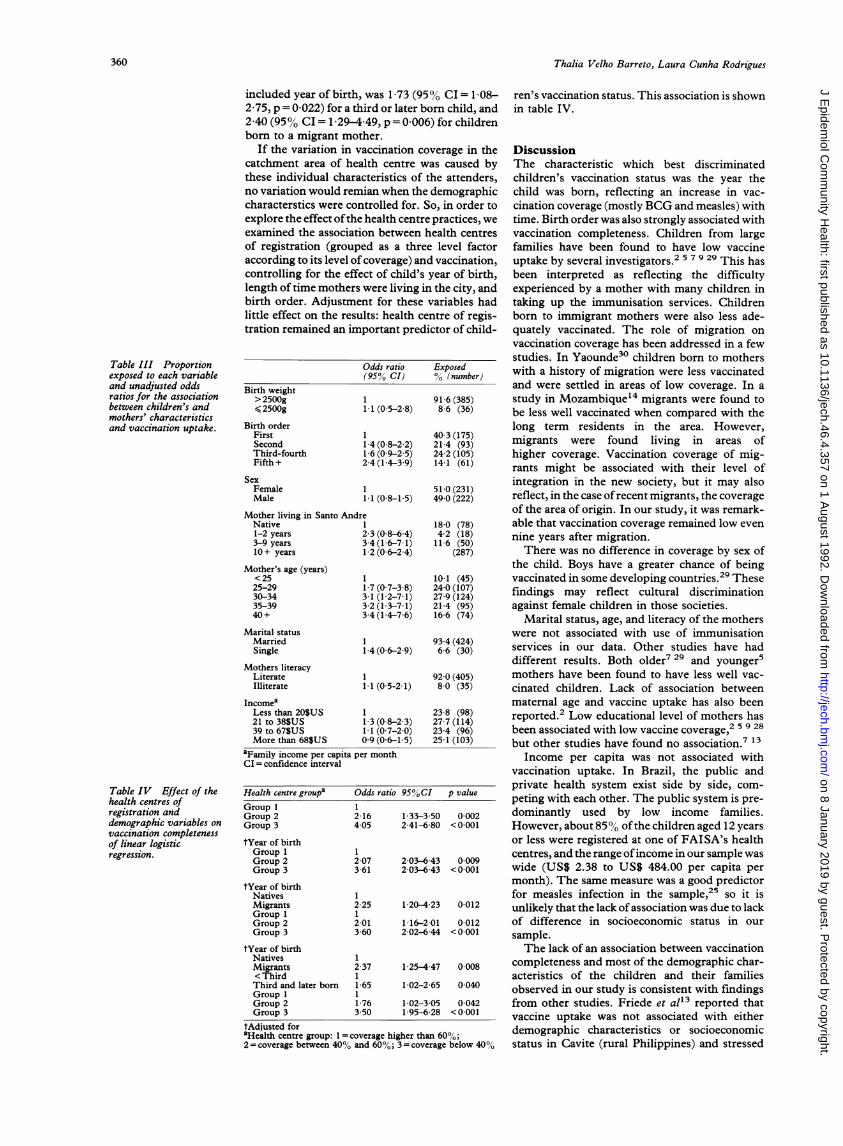
Table III Proportionexposed to each variableand unadjusted oddsratios for the associationbetween children's andmothers' characteristicsand vaccination uptake.
Birth weight>2500g2500g
Birth orderFirstSecondThird-fourthFifth +
SexFemaleMale
Mother living in Santo And:Native1-2 years3-9 years10+ years
Mother's age (years)<2525-2930-3435-3940+
Marital statusMarriedSingle
Mothers literacyLiterateIlliterate
IncomeaLess than 20$US21 to 38$US39 to 67$USMore than 68$US
aFamily income per capitaCI = confidence interval
Table IV Effect of thehealth centres ofregistration anddemographic variables onvaccination completenessof linear logisticregression.
p
Health centre group' C
Group 1 1Group 2 2Group 3 4
tYear of birthGroup 1 1Group 2 2Group 3 3
tYear of birthNatives 1Migrants 2Group 1 1Group 2 2Group 3 3
tYear of birthNatives 1Migrants 2< Third 1Third and later born 1Group 1 1Group 2 1Group 3 3
tAdjusted foraHealth centre group: 1 = co2= coverage between 40°h a:
,was 1 73 (950o CI= 108-hird or later born child, andL49, p = 0006) for children,ther.
ren's vaccination status. This association is shownin table IV.
raccination coverage in the Discussionalth centre was caused by The characteristic which best discriminatedLcteristics of the attenders, children's vaccination status was the year thenian when the demographic child was born, reflecting an increase in vac-ntrolled for. So, in order to cination coverage (mostly BCG and measles) withe health centre practices, we time. Birth order was also strongly associated withion between health centres vaccination completeness. Children from large)ed as a three level factor families have been found to have low vaccinef coverage) and vaccination, uptake by several investigators.2 5 7 9 29 This hasect of child's year of birth, been interpreted as reflecting the difficulty,were living in the city, and experienced by a mother with many children inMnt for these variables had taking up the immunisation services. Childrenalts: health centre of regis- born to immigrant mothers were also less ade-iportant predictor of child- quately vaccinated. The role of migration on
vaccination coverage has been addressed in a fewstudies. In Yaounde30 children born to mothers
Odds ratio Exposed with a history of migration were less vaccinatedand were settled in areas of low coverage. In a
91 6 (385) study in Mozambique'4 migrants were found to11 (0-5-2-8) 8 6 (36) be less well vaccinated when compared with the
long term residents in the area. However,1 40 3 (175) migrants were found living in areas of16 (09-25) 242 (105) higher coverage. Vaccination coverage of mig-2 4 (1 4-3 9) 14-1 (61) rants might be associated with their level of
1 51-0 (231) integration in the new society, but it may also1.1 (0 8-1 5) 49 0 (222) reflect, in the case of recent migrants, the coverage
,re of the area of origin. In our study, it was remark-1 18-0 (78) able that vaccination coverage remained low even23 (08-64) 42 (18) nine years after migration.3-4(1-6-7-1) 11-6 (50)1 2 (0 6-2 4) (287) There was no difference in coverage by sex of
the child. Boys have a greater chance of being1 10 1 (45) vaccinated in some developing countries.29 These1 7 (0-7-3-8) 24-0 (107) findings may reflect cultural discrimination3-1 (1-2-7-1) 27-9 (124)3 2 (1 3-7-1) 21 4 (95) against female children in those societies.3-4 (1-4-7-6) 16 6 (74) Marital status, age, and literacy of the mothers
were not associated with use of immunisation14 (06-29) 66 (30) services in our data. Other studies have had
different results. Both older7 29 and younger51 92 0 (405) mothers have been found to have less well vac-11 (05-21) 8-0 (35) cinated children. Lack of association between
maternal age and vaccine uptake has also been
1 (08-23) 277 (114) reported.2 Low educational level of mothers has1.1 (0 7-2 0) 23 4 (96) been associated with low vaccine coverage,2 5 9 280 9 (0-6-1 5) 25 1 (103) but other studies have found no association.713
)er month Income per capita was not associated withvaccination uptake. In Brazil, the public andprivate health system exist side by side, com-
)dds ratio 9500CI p value peting with each other. The public system is pre-'16 133-3 50 0002 dominantly used by low income families.05 2-41-6 80 < 0-001 However, about 85 ° of the children aged 12 years
or less were registered at one of FAISA's health
~-07 2-03--6-43 0-009 centres, and the range ofincome in our sample was,661 203-643 <0001 wide (US$ 2.38 to US$ 484.00 per capita per
month). The same measure was a good predictorfor measles infection in the sample,25 so it is
25 1 20-423 0 012 unlikely that the lack of association was due to lack'01 1 16-201 0012 of difference in socioeconomic status in our-60 2-02-6-44 < 0 001 sample.
The lack of an association between vaccination37 1-25-4-47 0 008 completeness and most of the demographic char-
acteristics of the children and their families*65 1*02-2 65 0-040 observed in our study is consistent with findings*76 1 02-3 05 0-042 from other studies. Friede et alt3 reported that50 1 95-6 28 <0 001 vaccine uptake was not associated with either
bverage higher than 600o; demographic characteristics or socioeconomicnd 60%; 3= coverage below 40%0 status in Cavite (rural Philippines) and stressed
360
on 8 January 2019 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.46.4.357 on 1 A
ugust 1992. Dow
nloaded from

Childhood immunisation in an urban area of Brazil
the influence of features of health services onvaccination. It is interesting that in societies asdifferent as Cavite and Santo Andre, when otherbarriers such as availability, distance, and directpayment of health services are removed, there isno differential use of vaccination services withwealth.The analysis of the immunisation pattems
suggests that an important role is played by healthservice practices in our study place. The propor-tion of fully vaccinated children increased sharplyover the study period. The speed of this increasesuggests that it was not caused by changes incultural attitudes and beliefs, which are normallyslow. It is likely that the creation of FAISAin 1967, which established a local regionalisedpublic health system, influenced the levels ofvaccination coverage in Santo Andre by facilitat-ing the access to vaccination services.
Fifty three percent of the children were inade-quately vaccinated, in spite of the fact that only4 -6% of all children had received no vaccination atall, showing that a large proportion of childrenwho started the course of immunisation did notcomplete it. The propotion of children fullyimmunised was consistently high during thewhole period under study for DPT and oral polio,which required at least three visits to the healthcentre for complete coverage, with a very low dropout rate between the first and the third doses. Inspite of the fact that full coverage of BCG andmeasles requires only one dose, coverage for thesevaccines was low and increased with time. Thisagain suggests that the overall increase in coveragein Santo Andre resulted from better performanceby health centres rather than from an improve-ment in mothers' compliance. Studies fromPakistan,22 India,24 and Mozambique'4 32identified missed opportunities and inappropriatecontraindications as important factors inhibitingbetter coverage. A study on measles vaccineuptake in Sao Paulo found that contraindicationto immunisation was responsible for 350% ofnon-vaccination.3'
In summary, the only demographic variableswhich had a statistically significant associationwith vaccine coverage were birth order and migra-tion. Our results support the hypothesis thatdifferences in practices across health centres had amajor impact on vaccine coverage. This is reas-suring news for health planners, as it suggests thatimproving health centre procedures and makingthe management of vaccination services respon-sive to the needs of large families and migrantscould increase vaccination coverage. Research oncauses of low vaccine uptake should also concen-trate on investigating features of the services,including application of contraindications, clinicstaff attitudes towards measles and BCG vacci-nation, provision of vaccines, and missed oppor-tunities.
We would like to thank the Fundacao de Assistencia aSaude de Santo Andre for generously allowing the use ofits records, CNPq (Conselho Nacional de Pesquisa,Brazil) and the Wellcome Foundation for their financialsupport, and Paul Fine, Fabio Zicker, and Steve Bennettfor their comments on an earlier version of this paper.
1 World Health Organization. Expanded program on
immunisation-update. Geneva; WH O, 1986.2 Marks JS, HalpinTJ, IrvinJJ, Johnson DA, Keller JR. Risk
factors associated with failure to receive vaccination.Pediatrics 1979; 64: 304-9.
3 RosenstockI, Derryberry M, Carriger B. Why people fail toseek poliomyelitis vaccination. Public Health Rep 1959; 74:98-103.
4 RosenstockIM. The health belief model and preventivehealth behaviour. Health Educ Monthly 1974; 2: 345-85.
5 Markland RE, Durand DE. An investigation of socio-psycological factors affecting infant immunization. Am JPublic Health 1976; 66: 168-70.
6 Hingson R, Lin N, Hingson RA. Achieving higherimmunization receptivity. Public Health Rev 1976; 6:93-117.
7 Selwyn BJ. An epidemiological approach to the study ofnon-users of child health services. AmJPublic Health 1978;68: 231-5.
8 RiddioughMA, Willems JS, Sanders CR, Kemp K. Factorsaffecting the use of vaccines: consideration for immuniz-ation program planners. Public Health Rep 1981; 96:528-35.
9 Halon P, Byass P, Yamuach M, Hayes R, BennettS, M'BogeBH. Factors infuencing vaccination compliance in peri-urban Gambian children. J Trop MedHyg 1988; 91: 29-33.
10 Streatifield K, Singarimbum M. Social factors affecting useof immunization in Indonesia. Soc Sci Med 1988; 27:1237-45.
11 Adekunlel L. Child immunization: what are theimpediments for reaching desired goals in a transitionalsociety? Soc Sci Med 1978; 12: 325-57.
12 Heggenhougen K, ClementJJ. Acceptability of childhoodimmunizations: social science perspectives. EPCpublication, No 14. London: London School of Hygieneand Tropical Medicine, 1987.
13 Friede AM, Watemaux C, Guyer B, de Jesus A, Pillip LC.An epidemiological assessment of immunization programparticipation in the Philippines.Int J Epidemiol 1985; 14:135-41.
14 Cutts FT, Rodrigues LC, ColomboS, Bennett S. Evaluationof factors influencing vaccine uptake in Mozambique. IntJtEpidemiol 1989; 18: 427-33.
15 Belcher DW, Nicholas DD, Ofosu-AmaahS, Wurapa FK. Amass immunization campaign in rural Ghana. Factorsaffecting participation.Int Health 1978; 93: 171-5.
16 Vasconcelos SR, Silva LMC. Cobertura vacinal em criancasmenores de 5 anos, residentes no interior do Estado daBahia no ano de 1981. Rev Bahiana Saude Publica 1983; 10:95-140.
17 Adjaye N. Measles immunizaion; some factors affectingnon-acceptance of vaccine. Public Health 1981; 95: 185-8.
18 World Health Stat Q 1985; 38 Ac 9. WHO/GEN.(?)19 Berkeley MIK. Measles-the effect of attitudes on
immunization. Health Bull 1983; 14: 141-6.20 Steinhoff MC, Cole P, Cole A, John JJ, Pereira EM.
Evaluation of the opportunities for the contraindications toimmunization in a tropical paediatric clinic. Bull WHO1985; 63: 915-18.
21 Dick B. Issues in immunization in developing countries-anoverview. EPC publication, No 7. London: London Schoolof Hygiene and Tropical Medicine.
22 Cruz RR. Cuba: mass polio vaccination program 1962-1982.Rev Infect Dis 1984; 6 (suppl 2): 408-12.
23 William PJ, Hull HF. Status of measles in the Gambia. RevInfect Dis 1983; 5: 391-4.
24 Risi JB. Nation-wide mass polio immunization in Brazil.Assignment Children 1984; 65: 137-57.
25 Rodrigues LC. A case-control study of measles efficacy.London: London School of Hygiene and TropicalMedicine, 1986. PhD Thesis.
26 Rodrigues LC, Kirkwood BR. Case-control designs in thestudy of common diseases: updates on the demise of the raredisease assumption and the choice of sampling scheme forcontrols. Int J Epidemiol 1990; 19: 205-13.
27 SAS supplemental user's guide. Cary NC: SAS Institute,1980.
28 EGRET; Epidemiological graphics, estimation and testingpackage, version 0-23-25; 1985. Statistics and Epidemi-ology Research Corporation.
29 Akesode FA. Factors affecting the use of primary health careclinics for children. J Epidemiol Community Health 1982;36: 310-14.
30 Brown J, Djogdom P, Murphy K, Kessenge E, Heymann D.Identifying the reason for low immunization coverage. Acase study of Yaounde (Cameroon). Rev Epidemiol SantePublique 1982; 30: 35-47.
31 Barbosa V, Iversson LB, Aquino Ac. Sarampo: inqueritosobre antecedentes vacinal e de doencas em criancas de 0 a14 anos atendidas nos centros de saude estaduais domunicipo de Sao Paulo, 1976. Rev Saude Publica 1977; 11:515-26.
32 Cutts F, Soares A, Jecque AV, Cliff J, Kontbeek S. ColomboS.The use of evaluation to improve the Expanded Programon Immunization in Mozambique. Bull WHO 1990; 68:199-208.
361
on 8 January 2019 by guest. Protected by copyright.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.46.4.357 on 1 A
ugust 1992. Dow
nloaded from











![[cover] Ghid pentru imunizările din copilărie pentru a ... Your Child is immunsied/A guide to childhood...A Guide to Childhood Immunisation Babies (Romanian) [cover] Ghid pentru](https://img.pdfslide.net/doc/110x75/5f0d00a57e708231d438313b/cover-ghid-pentru-imunizfrile-din-copilfrie-pentru-a-your-child-is-immunsieda.jpg)

















