Embed Size (px)
Citation preview
Family-Initiated Dialogue AboutMedications During Family-CenteredRoundsJessica M. Benjamin, PharmDa, Elizabeth D. Cox, MD, PhDa, Philip J. Trapskin, PharmDb, Victoria P. Rajamanickam, MSc,Roderick C. Jorgenson, BS Pharmb, Holly L. Weber, PharmDd, Rachel E. Pearson, PharmDd, Pascale Carayon, PhDe,Nikki L. Lubcke, PharmDb
abstract BACKGROUND AND OBJECTIVE: Experts suggest family engagement in care can improve safety for hospitalizedchildren. Family-centered rounds (FCRs) can offer families the opportunity to participate in errorrecovery related to children’s medications. The objective of this study was to describe family-initiateddialogue about medications and health care team responses to this dialogue during FCR to understandthe potential for FCR to foster safe medication use.
METHODS: FCR were video-recorded daily for 150 hospitalized children. Coders sorted family-initiatedmedication dialogue into mutually exclusive categories, reflecting place of administration, therapeutic class,topic, and health care team responses. Health care team responses were coded to reflect intent, actions takenby the team, and appropriateness of any changes.
RESULTS: Eighty-three (55%) of the 150 families raised 318 medication topics during 347 FCR. Most family-initiated dialogue focused on inpatient medications (65%), with home medications comprising 35%. Anti-infectives (31%), analgesics (14%), and corticosteroids (11%) were the most commonly discussedmedications. The most common medication topics raised by families were scheduling (24%) and adversedrug reactions (11%). Although most health care team responses were provision of information (74%),appropriate changes to the child’s medications occurred in response to 8% of family-initiated dialogue, withmost changes preventing or addressing adverse drug reactions or scheduling issues.
CONCLUSIONS:Most families initiated dialogue regarding medications during FCRs, including both inpatientand home medications. They raised topics that altered treatment and were important for medicationsafety, adherence, and satisfaction. Study findings suggest specific medication topics that health careteams can anticipate addressing during FCR.
WHAT’S KNOWN ON THIS SUBJECT: Familyengagement in the care of hospitalized childrenmay improve outcomes, including medicationsafety. Although family-centered rounds (FCRs)provide a venue for family engagement in care,how families use this venue to influencemedication-related topics is unknown.
WHAT THIS STUDY ADDS: Most families initiatedmedication-related dialogue during FCRs,discussing inpatient and home medications.Topics raised were important for medicationadherence and safety, even altering treatmentplans. Findings suggest specific medicationtopics that health care team members cananticipate addressing during FCR.
Departments of aPediatrics, and cBiostatistics and Medical Informatics, University of Wisconsin School ofMedicine and Public Health, Madison, Wisconsin; bUniversity of Wisconsin Hospital and Clinics, Madison,Wisconsin; dUniversity of Wisconsin-Madison School of Pharmacy, Madison, Wisconsin; and eCenter for Quality andProductivity Improvement, Department of Industrial and Systems Engineering, University of Wisconsin-Madison,Madison, Wisconsin
Dr Benjamin conceived and designed the study; oversaw all data collection, coding, and analyses;and drafted and revised the manuscript; Dr Cox secured funding, conceived and designed the study,oversaw all data collection and analyses, and revised the manuscript; Dr Trapskin, Mr Jorgenson,Dr Carayon, and Dr Lubcke assisted with development of the coding scheme and revised themanuscript; Ms Rajamanickam performed analyses and revised the manuscript; and Dr Weber andDr Pearson assisted with development of the coding scheme, coded the data, and revised themanuscript. All authors approved the final version for submission.
The content is solely the responsibility of the authors and does not necessarily represent the officialviews of the National Institutes of Health or other funders. The funders had no role in designing,conducting, or reporting the results of this study.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-3885
DOI: 10.1542/peds.2013-3885
Accepted for publication Sep 29, 2014
ARTICLE PEDIATRICS Volume 135, number 1, January 2015 by guest on June 28, 2018www.aappublications.org/newsDownloaded from

Pediatric patients are especiallysusceptible to medication safetyissues, including medication errors aswell as harm from use, nonuse, ormisuse of medications, due in part tochildren’s incomplete physiologicdevelopment and the complexities ofmedication delivery systems.1–4
Medication errors in the inpatientpediatric population occur at 3 timesthe rate of adult counterparts.5
Although preventing errors isa laudable goal, the fact that healthcare delivery requires theinvolvement of human providers andpatients suggests that preventing allerrors is not realistic.6,7 Therefore,a process that identifies errors beforethey reach a patient and remediateserrors to reduce harm is crucial.6
Error recovery describes this type ofprocess and includes 3 stages: (1)detection; (2) explanation; and (3)correction.8 Detection involvesidentifying the error and can bedone by the person committing theerror or by others familiar with thecare plan. Explanation involvesunderstanding how the error occurred.Correction involves the implementationof a new or modified care plan.Although error recovery can beperformed by a single health careteam member, the most robust errorrecovery strategies reside at the levelof the health care system and aredependent on the involvement ofother team members and patients.6,9–11
Families, who are experts on thehealth and care of their children,could contribute meaningfully to anyor all of these error recovery stages.
In the inpatient setting, the AmericanAcademy of Pediatrics recommendsfamily-centered rounds (FCRs) inwhich the medical team, family, andpatient are all present andencouraged to participate as standardof practice.12 FCRs represent anestablished venue in which several ofthe key features of successful errorrecovery are present.8,9,13 Specifically,FCRs often include monitoringmedication outcomes and review of
treatment plans under the watchfuleyes of those most knowledgeableabout the child’s care, such as attendingphysicians, nurses, pharmacists,and the family.14,15 The objective ofthe present study was to furtherunderstand the potential for FCRs tofoster pediatric medication safety. Tothat end, the study describes andquantifies medication-related topicsraised by families during FCR and howthis dialogue affects the children’streatment plans.
METHODS
Participants and Data Collection
Participants were enrolled fromOctober 2010 through May 2011 ata Midwestern, tertiary care, academicchildren’s hospital with 61 inpatientbeds. Patients admitted to the generalpediatric hospitalist, pulmonology,and hematology/oncology serviceswere eligible to participate. Patientswith sensitive reasons for admission(eg, child abuse, mental health issues)or without parents available toprovide consent were ineligible.
Our general pediatric hospitalistservice admits children with acuteconcerns while the other servicesadmit mostly children with ongoingillnesses (eg, cystic fibrosis, sicklecell disease, pediatric cancers). Theattending or fellow, senior resident,1 to 2 interns, 1 to 4 medicalstudents, and the patient’s nurseparticipate in FCRs, with other teammembers as needed (eg, a socialworker, pharmacist). The attendingon the pediatric hospitalist service isa hospitalist; the other services havesubspecialist attending physicians.FCRs routinely include the intern orstudent’s formal presentation of thechild’s case by using lay language,any status updates, and the plans forthe hospital day as well as dischargecriteria and plans. Upon admission,families receive 1 page of informationabout FCRs as part of a standard16-page packet of information. Thepurpose, who participates, what to
expect, and how families canprepare for FCRs are discussed.Recommendations for preparationinclude: (1) writing down questions;(2) making the team aware of anysensitive issues; and (3) having thechild’s medication schedule.
Of 233 parents of eligible admissions,194 agreed to learn about the studyfrom our research team; 172 (87%)agreed to participate. Participantsprovided written consent to havetheir FCRs video-recorded daily andcompleted surveys of demographicand hospitalization characteristics.Families were informed that the studywould help the hospital understandhow health care providers and familieswork together to provide care duringFCRs. Health care team membersalso consented to being video-recorded for this study. The Universityof Wisconsin–Madison Health Sciencesinstitutional review board approvedthis study.
Assessment of Family-InitiatedMedication Dialogue
From the FCR videos, trained codersassessed family-initiated medicationdialogue. Because we wanted tounderstand the medication topicsthat would arise from the perspectiveof the family, we evaluated onlyinstances of family-initiated medicationdialogue. We did not include familyresponses to medication topics initiatedby the health care team. To describefamily-initiated dialogue aboutmedications, our goal was tounderstand the following: (1) theplace of administration (inpatient orhome); (2) the medication’stherapeutic class; and (3) the specifictopic raised (eg, scheduling or routeof the drug). Inpatient medicationswere subdivided into current (patientis receiving the medication) or new(a new order for this medication isbeing considered). For health careteam responses to each instance offamily-initiated medication dialogue,we wished to describe: (1) the typeof response (eg, change to medicationtreatment plan, provision of
PEDIATRICS Volume 135, number 1, January 2015 95 by guest on June 28, 2018www.aappublications.org/newsDownloaded from
information); (2) how the family’sinitiation of this dialogue influencedthe child’s medication treatment plan(eg, initiating a new medication orchanging the route of a medication);and (3) whether the change inmedication was inappropriate, reflectingoveruse, underuse, or misuse.16
To develop the new coding schemerequired for this work, a team ofphysicians, pharmacists, anddoctorate of pharmacy studentsreviewed the literature on medicationsafety and pharmacist participationin rounds.17–20 From this literature,the team constructed a draft list ofcategories to describe each of thecoding scheme elements. Teammembers applied this coding schemeto FCR videos and iteratively revisedit to ensure an exhaustive set ofoptions to describe family-initiateddialogue and health care teamresponses. Supplemental Table 6provides descriptions of the fullcoding scheme, including codes anddefinitions. Revisions included addingdescriptors to capture topics notinitially recognized from theliterature (eg, family dialogue seekinga medication suggestion) and selectionof the 8 most common therapeuticclasses used in our population. Codersreceived 25 hours of training over 5weeks, using a training manual andpilot FCR videos.
Coding of Dialogue
A pair of trained coders reviewedeach FCR video and categorized allfamily-initiated medication dialogueand health care team responses intomutually exclusive categories, usingNoldus Observer.21 Discrepancieswere resolved by consensus.
Analyses
Analyses including percentages,means, and SDs were used to describeour participants, the family-initiatedmedication dialogue, and healthcare team responses. Generalizedestimating equations with the log linkand robust SEs were used to compareparent, child, and hospitalization
characteristics for families whoinitiated medication dialogue to thoseof all families who attended FCRs.
RESULTS
Prevalence of Family-InitiatedMedication Dialogue During FCR
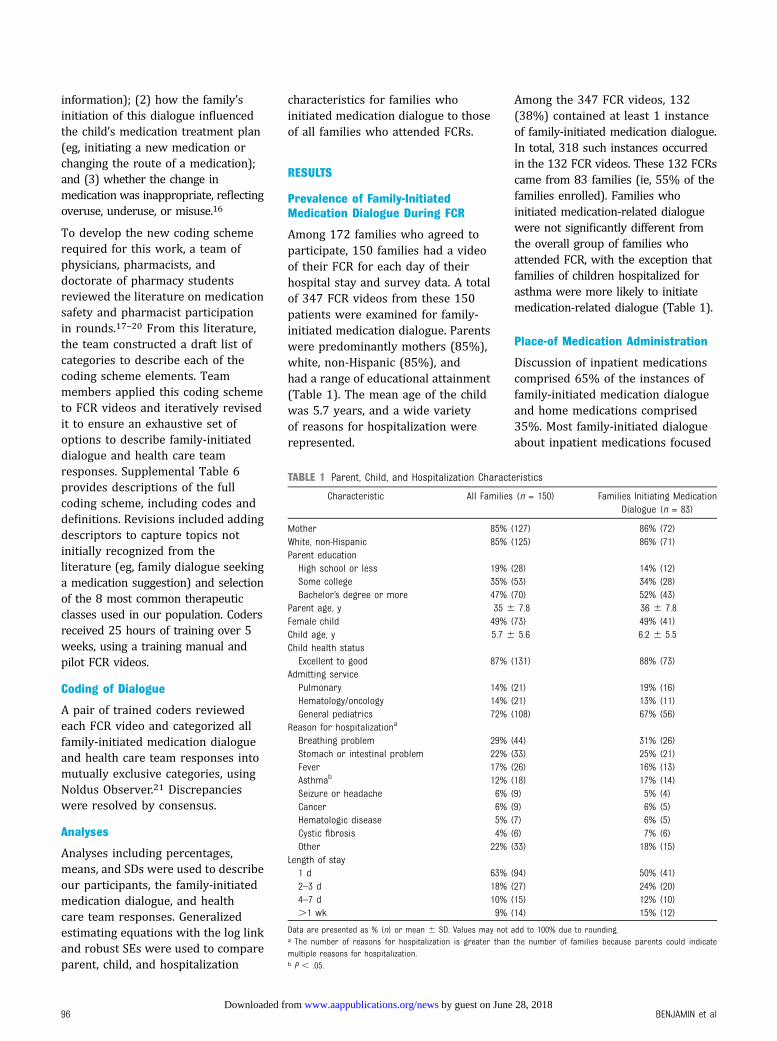
Among 172 families who agreed toparticipate, 150 families had a videoof their FCR for each day of theirhospital stay and survey data. A totalof 347 FCR videos from these 150patients were examined for family-initiated medication dialogue. Parentswere predominantly mothers (85%),white, non-Hispanic (85%), andhad a range of educational attainment(Table 1). The mean age of the childwas 5.7 years, and a wide varietyof reasons for hospitalization wererepresented.
Among the 347 FCR videos, 132(38%) contained at least 1 instanceof family-initiated medication dialogue.In total, 318 such instances occurredin the 132 FCR videos. These 132 FCRscame from 83 families (ie, 55% of thefamilies enrolled). Families whoinitiated medication-related dialoguewere not significantly different fromthe overall group of families whoattended FCR, with the exception thatfamilies of children hospitalized forasthma were more likely to initiatemedication-related dialogue (Table 1).
Place-of Medication Administration
Discussion of inpatient medicationscomprised 65% of the instances offamily-initiated medication dialogueand home medications comprised35%. Most family-initiated dialogueabout inpatient medications focused
TABLE 1 Parent, Child, and Hospitalization Characteristics
Characteristic All Families (n = 150) Families Initiating MedicationDialogue (n = 83)
Mother 85% (127) 86% (72)White, non-Hispanic 85% (125) 86% (71)Parent educationHigh school or less 19% (28) 14% (12)Some college 35% (53) 34% (28)Bachelor’s degree or more 47% (70) 52% (43)
Parent age, y 35 6 7.8 36 6 7.8Female child 49% (73) 49% (41)Child age, y 5.7 6 5.6 6.2 6 5.5Child health statusExcellent to good 87% (131) 88% (73)
Admitting servicePulmonary 14% (21) 19% (16)Hematology/oncology 14% (21) 13% (11)General pediatrics 72% (108) 67% (56)
Reason for hospitalizationa
Breathing problem 29% (44) 31% (26)Stomach or intestinal problem 22% (33) 25% (21)Fever 17% (26) 16% (13)Asthmab 12% (18) 17% (14)Seizure or headache 6% (9) 5% (4)Cancer 6% (9) 6% (5)Hematologic disease 5% (7) 6% (5)Cystic fibrosis 4% (6) 7% (6)Other 22% (33) 18% (15)
Length of stay1 d 63% (94) 50% (41)2–3 d 18% (27) 24% (20)4–7 d 10% (15) 12% (10).1 wk 9% (14) 15% (12)
Data are presented as % (n) or mean 6 SD. Values may not add to 100% due to rounding.a The number of reasons for hospitalization is greater than the number of families because parents could indicatemultiple reasons for hospitalization.b P , .05.
96 BENJAMIN et al by guest on June 28, 2018www.aappublications.org/newsDownloaded from

on current medications whileconsideration of new medicationscomprised only 15% of this dialogue.
Therapeutic Class of Medications AboutWhich Families Initiated Dialogue
Families most often initiatedmedication dialogue regarding anti-infectives (31%), analgesics (14%),and corticosteroids (11%)(Supplemental Table 7). Other commonmedications raised for discussionwere b-agonists (6%) and antiemeticagents (5%).
Medication Topics Raised by Families
The most common medication topicraised by families was scheduling(medication timing, frequency, orduration), comprising 77 (24%) ofthe 318 instances of family initiateddialogue (Table 2). Other commontopics included adverse drugreactions (ADRs; 11%), clarificationsabout the drug (10%), and drugindication (9%). Illustrative examplesof common topics in family-initiatedmedication dialogue are given inFigure 1.
Health Care Team MemberResponses to Family-InitiatedMedication Dialogue
The majority (74%) of health careteam responses to family-initiatedmedication dialogue involvedproviding information to the family(Table 3). In some instances, the
health care team simply acknowledgedthe dialogue (13%). Occasionally, thehealth care team deferred respondingto family-initiated medication dialogue(5%), often waiting for additionalinformation from other health careteam members. Only rarely did thehealth care team not respond tofamily-initiated medication dialogue(1% of instances).
Changes to Treatment ResultingFrom Family-Initiated MedicationDialogue
In response to 8% of instances inwhich families initiated medication-related dialogue, a change to the
medication treatment plan occurred(Table 3). Figure 2 contains examplesof family-initiated dialogue thatresulted in changes to the child’smedications. Of the 25 medicationtreatment plans that were changed,most were changed by adding amedication (44%) or throughscheduling changes (24%) (Table 4).Typical medication additions inresponse to family-initiated dialogueincluded prevention or treatment ofantibiotic-related diarrhea by addingprobiotics. Similarly, a test dose of oralantibiotic before discharge could beadded to ensure the child tolerated oralantibiotics at home. Medications werestopped in 12% of instances. Theremaining changes involved themedication’s dose or rate, route, orformulation. On review, none of thechanges was found to be inappropriate.
Family-Initiated Medication TopicsResulting in Changes to TreatmentPlan
Changes to the child’s medicationswere prompted by a variety of topics
TABLE 2 Family-Initiated MedicationDialogue Topics During FCRS(N = 318)
Dialogue Topic % N
Scheduling 24.2 77ADR 11.0 35Clarification 10.1 32Indication 9.4 30Dose or rate 8.2 26Route 7.9 25Suggestion 6.9 22Formulation 4.1 13Missing medication 3.8 12Contraindication or interaction 1.6 5Monitoring 1.3 4Duplication ,0.1 2Other 11.0 35
Values may not add to 100% due to rounding.
FIGURE 1Examples of common medication topics initiated by families.
TABLE 3 Health Care Team Responses toFamily-Initiated Medication-RelatedDialogue (N = 318)
Response % N
Inform 73.6 234Acknowledgment 12.6 40Change 7.9 25Defer 4.7 15No response 1.3 4
Values may not add to 100% due to rounding.
PEDIATRICS Volume 135, number 1, January 2015 97 by guest on June 28, 2018www.aappublications.org/newsDownloaded from
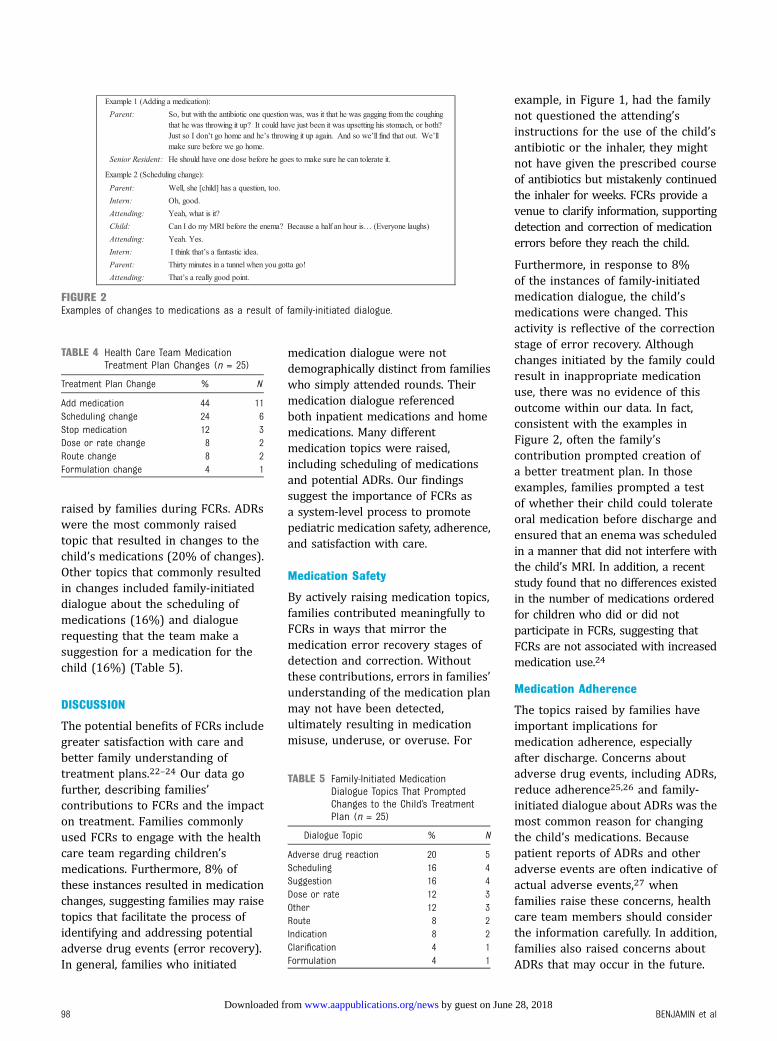
raised by families during FCRs. ADRswere the most commonly raisedtopic that resulted in changes to thechild’s medications (20% of changes).Other topics that commonly resultedin changes included family-initiateddialogue about the scheduling ofmedications (16%) and dialoguerequesting that the team make asuggestion for a medication for thechild (16%) (Table 5).
DISCUSSION
The potential benefits of FCRs includegreater satisfaction with care andbetter family understanding oftreatment plans.22–24 Our data gofurther, describing families’contributions to FCRs and the impacton treatment. Families commonlyused FCRs to engage with the healthcare team regarding children’smedications. Furthermore, 8% ofthese instances resulted in medicationchanges, suggesting families may raisetopics that facilitate the process ofidentifying and addressing potentialadverse drug events (error recovery).In general, families who initiated
medication dialogue were notdemographically distinct from familieswho simply attended rounds. Theirmedication dialogue referencedboth inpatient medications and homemedications. Many differentmedication topics were raised,including scheduling of medicationsand potential ADRs. Our findingssuggest the importance of FCRs asa system-level process to promotepediatric medication safety, adherence,and satisfaction with care.
Medication Safety
By actively raising medication topics,families contributed meaningfully toFCRs in ways that mirror themedication error recovery stages ofdetection and correction. Withoutthese contributions, errors in families’understanding of the medication planmay not have been detected,ultimately resulting in medicationmisuse, underuse, or overuse. For
example, in Figure 1, had the familynot questioned the attending’sinstructions for the use of the child’santibiotic or the inhaler, they mightnot have given the prescribed courseof antibiotics but mistakenly continuedthe inhaler for weeks. FCRs provide avenue to clarify information, supportingdetection and correction of medicationerrors before they reach the child.
Furthermore, in response to 8%of the instances of family-initiatedmedication dialogue, the child’smedications were changed. Thisactivity is reflective of the correctionstage of error recovery. Althoughchanges initiated by the family couldresult in inappropriate medicationuse, there was no evidence of thisoutcome within our data. In fact,consistent with the examples inFigure 2, often the family’scontribution prompted creation ofa better treatment plan. In thoseexamples, families prompted a testof whether their child could tolerateoral medication before discharge andensured that an enema was scheduledin a manner that did not interfere withthe child’s MRI. In addition, a recentstudy found that no differences existedin the number of medications orderedfor children who did or did notparticipate in FCRs, suggesting thatFCRs are not associated with increasedmedication use.24
Medication Adherence
The topics raised by families haveimportant implications formedication adherence, especiallyafter discharge. Concerns aboutadverse drug events, including ADRs,reduce adherence25,26 and family-initiated dialogue about ADRs was themost common reason for changingthe child’s medications. Becausepatient reports of ADRs and otheradverse events are often indicative ofactual adverse events,27 whenfamilies raise these concerns, healthcare team members should considerthe information carefully. In addition,families also raised concerns aboutADRs that may occur in the future.
FIGURE 2Examples of changes to medications as a result of family-initiated dialogue.
TABLE 4 Health Care Team MedicationTreatment Plan Changes (n = 25)
Treatment Plan Change % N
Add medication 44 11Scheduling change 24 6Stop medication 12 3Dose or rate change 8 2Route change 8 2Formulation change 4 1
TABLE 5 Family-Initiated MedicationDialogue Topics That PromptedChanges to the Child’s TreatmentPlan (n = 25)
Dialogue Topic % N
Adverse drug reaction 20 5Scheduling 16 4Suggestion 16 4Dose or rate 12 3Other 12 3Route 8 2Indication 8 2Clarification 4 1Formulation 4 1
98 BENJAMIN et al by guest on June 28, 2018www.aappublications.org/newsDownloaded from

For example, the family member inFigure 1 who expressed concernabout adverse effects of inhaledcorticosteroids created an opportunityto prevent a potential medication errorin the form of underuse of the inhaledcorticosteroids. Lack of adherence tothis medication could have evenresulted in future asthma exacerbationsand health care utilization.
Family-initiated medication dialoguealso promoted adherence by promptingchanges to medication schedules.Scheduling of home medications,especially ensuring medications do notconflict with activities such as school, iscritical to adherence.28–30 With muchof the family-initiated dialogueregarding medication schedulingrevolving around medications used afterdischarge, FCRs provide a structuredopportunity to close the communicationloop with families, with the goal ofreducing medication errors upontransition to the home environment.
Family and Patient Satisfaction
FCR provided a forum for betterinformation sharing, which can ultimatelyresult in increased satisfaction withcare.24,31,32 Specifically, in our secondexample in Figure 2, had the child notproactively raised concerns aboutscheduling an enema before her MRI,unanticipated harms could haveoccurred, such as emotional distressand delays in receiving diagnosticinformation. Furthermore, familiescommonly raised topics that reflectedtheir need for clarification regardingmedications. Previous literatureindicates that patients have increasedsatisfaction with their care whenthey are able to engage in a dialogueabout their medications.33 FCRspresent opportunities for thehealth care team to provide family-centered care by addressinginformation needs as identified by thefamily.12
Guidance for Health Care TeamMembers Performing FCRs
Several of our findings provide healthcare teams with guidance for
responding to family-initiatedmedication dialogue during FCRs.First, families who initiatedmedication-related dialogue were nodifferent demographically than thosewho did not; therefore, health careteam members cannot predict whichfamilies may initiate medicationtopics. However, because families ofchildren with asthma were morelikely to initiate this dialogue,healthcare teams can anticipate andprepare for a discussion of asthmamedications. These discussions havea multitude of potential benefits giventhe high readmission rate for asthmapatients often caused by nonadherence.34
Second, given the commonplacenature of family-initiated dialogueregarding home medications, havingan efficient process for addressingquestions about home medications iscrucial. After discharge, familiesbecome responsible for administeringand monitoring children’s medications.Adverse drug events, defined as harmresulting from use, nonuse, or misuseof medication, occur in 14% of pediatricoutpatient receiving a prescription.35
The majority of preventable adversedrug events (70%) occur duringparental administration rather than inearlier stages such as medicationordering. Thus, discussion about homemedications is crucial to partneringwith families regarding safe medicationuse. To facilitate this, our institutionprovides families with writtenmedication information ina patient/family-friendly format.36
For our population, which includedchildren hospitalized for acute andchronic illnesses, there may bespecific types of medications thathealth care team members cananticipate arising during FCRs. Notsurprisingly, families most ofteninitiated dialogue about medicationssuch as anti-infectives and analgesics.These medications are frequentlyused during pediatric hospitalizationsfor acute conditions and in ourstudy’s chronic disease populations,such as children with cystic fibrosisexacerbations or with chemotherapy-
associated fever and neutropenia.These medications are known tobe common sources of pediatricmedication errors.5,37 Furthermore,analgesics include narcotics, a commoncause of harm from medication useor misuse in children.38–40
For some medications such as inhaledsteroids, the frequency with whichfamilies raise these medications fordiscussion may be influenced byperceptions of potential adversereactions (eg, irritability or stuntedgrowth), by the multiple potentialadministration routes (eg, oral steroidsversus inhaled steroids), or by theircomplicated administration techniques(eg, nebulizers and dry powder ormetered-dose inhalers).25,41,42 Inaddition, confusion can occur regardingthe purpose of a rescue inhaler versusa maintenance inhaler, which canlead to misuse.43 These topics can beanticipated and responded to duringthe FCRs, allowing trainees topractice their responses to commonfamily-initiated medication-relatedtopics.
Limitations
Although we recruited patients frommultiple different services, ourdata arise from a single Midwesterninstitution and many participantswere admitted for acute disease;the findings may therefore not begeneralizable broadly to otherinstitutions or diverse populations.However, families who initiatedmedication-related dialogue did notdiffer on demographic characteristicsor health status from those whodid not initiate such a dialogue. Inaddition, while our recruitment ratewas high, families who did notparticipate may hold less favorableviews of FCRs, leading to potentialoverestimation of the amount offamily-initiated medication dialogue.Also, families were aware they werebeing video-recorded, but whetherthis awareness could increase ordecrease the initiation of medication-related dialogue is unknown; previousliterature has suggested, however,
PEDIATRICS Volume 135, number 1, January 2015 99 by guest on June 28, 2018www.aappublications.org/newsDownloaded from

that video-recorded interactions in thehealth care setting do not differ fromnonrecorded interactions.44,45
CONCLUSIONS
Most families initiated dialogueregarding medications during FCRs.
The families who initiated medicationdialogue did not differ in terms ofdemographic or health status fromthose who did not initiate medicationdialogue. Family-initiated medicationdialogue typically referenced bothinpatient medications and home
medications. Families’ contributionsresulted in appropriate changes totreatment plans. Our findings suggestthe importance of FCRs as asystem-level process to promotemedication safety, adherence, andsatisfaction with care.
Address correspondence to Elizabeth D. Cox, MD, PhD, University of Wisconsin School of Medicine and Public Health, 600 Highland Ave, H6/558 Clinical Science
Center, Madison WI, 53792. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: This work was funded through an Agency for Healthcare Research and Quality Health Services Research Dissemination and Demonstration grant (R18
HS018680) to Dr Cox. The project described was also supported by the Clinical and Translational Science Award program, previously through the National Center for
Research Resources (grant 1UL1RR025011) and now by the National Center for Advancing Translational Sciences (grant 9U54TR000021). Funded by the National
Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Ghaleb MA, Barber N, Franklin BD, WongICK. The incidence and nature ofprescribing and medication administrationerrors in paediatric inpatients. Arch DisChild. 2010;95(2):113–118
2. Stucky ER; American Academy ofPediatrics Committee on Drugs; AmericanAcademy of Pediatrics Committee onHospital Care. Prevention of medicationerrors in the pediatric inpatient setting.Pediatrics. 2003;112(2):431–436
3. Institute for Safe Medication Practices(ISMP) Canada. Definitions of terms.Available at: www.ismp-canada.org/definitions.htm. Accessed October 23,2014
4. Committee of Experts on Managementof Safety and Quality in Health Care(SP-SQS) Expert Group on Safe MedicationPractices. Glossary of terms related topatient and medication safety. Available at:www.bvs.org.ar/pdf/seguridadpaciente.pdf.Accessed October 23, 2014
5. Kaushal R, Bates DW, Landrigan C, et al.Medication errors and adverse drugevents in pediatric inpatients. JAMA.2001;285(16):2114–2120
6. Wetterneck TB. Error recovery in healthcare. In: Carayon P, ed. Handbook ofHuman Factors and Ergonomics in
Health Care and Patient Safety. 2nd ed.Boca Raton, FL: CRC Press; 2012:449–461
7. Alper SJ, Karsh BT. A systematic reviewof safety violations in industry. AccidAnal Prev. 2009;41(4):739–754
8. Kanse L, van der Schaaf TW, VrijlandND, van Mierlo H. Error recovery ina hospital pharmacy. Ergonomics.2006;49(5–6):503–516
9. Kontogiannis T, Embrey D. A user-centreddesign approach for introducingcomputer-based process informationsystems. Appl Ergon. 1997;28(2):109–119
10. Leplat J. Error analysis, instrument andobject of task-analysis. Ergonomics.1989;32(7):813–822
11. Weingart SN, Pagovich O, Sands DZ, et al.What can hospitalized patients tell usabout adverse events? Learning frompatient-reported incidents. J Gen InternMed. 2005;20(9):830–836
12. Committee on Hospital Care. AmericanAcademy of Pediatrics. Family-centeredcare and the pediatrician’s role.Pediatrics. 2003;112(3 pt 1):691–697
13. Sellen AJ. Detection of everyday errors.Appl Psychol. 1994;43(4):475–498
14. Kelly MM, Xie A, Carayon P, DuBenske LL,Ehlenbach ML, Cox ED. Strategies for
improving family engagement duringfamily-centered rounds. J Hosp Med.2013;8(4):201–207
15. Muething SE, Kotagal UR, Schoettker PJ,Gonzalez del Rey J, DeWitt TG. Family-centered bedside rounds: a newapproach to patient care and teaching.Pediatrics. 2007;119(4):829–832
16. Hepler CD, Strand LM. Opportunities andresponsibilities in pharmaceutical care.Am J Hosp Pharm. 1990;47(3):533–543
17. Rothschild JM, Churchill W, Erickson A,et al. Medication errors recovered byemergency department pharmacists.Ann Emerg Med. 2010;55(6):513–521
18. Leape LL, Cullen DJ, Clapp MD, et al.Pharmacist participation on physicianrounds and adverse drug events in theintensive care unit. JAMA. 1999;282(3):267–270
19. Kucukarslan SN, Peters M, Mlynarek M,Nafziger DA. Pharmacists on roundingteams reduce preventable adverse drugevents in hospital general medicine units.Arch Intern Med. 2003;163(17):2014–2018
20. Bond CA, Raehl CL. Clinical pharmacyservices, pharmacy staffing, and hospitalmortality rates. Pharmacotherapy. 2007;27(4):481–493
100 BENJAMIN et al by guest on June 28, 2018www.aappublications.org/newsDownloaded from

21. Noldus Information Technology. TheObserver Basic. Version 5.0 ed. Leesburg,VA: Noldus Information Technology; 2004
22. Mittal VS, Sigrest T, Ottolini MC, et al.Family-centered rounds on pediatricwards: a PRIS network survey of US andCanadian hospitalists. Pediatrics. 2010;126(1):37–43
23. Rappaport DI, Ketterer TA, Nilforoshan V,Sharif I. Family-centered rounds: viewsof families, nurses, trainees, andattending physicians. Clin Pediatr(Phila). 2012;51(3):260–266
24. Kuo DZ, Sisterhen LL, Sigrest TE, BiazoJM, Aitken ME, Smith CE. Familyexperiences and pediatric health servicesuse associated with family-centeredrounds. Pediatrics. 2012;130(2):299–305
25. Winnick S, Lucas DO, Hartman AL, Toll D.How do you improve compliance?Pediatrics. 2005;115(6) . Available at:www.pediatrics.org/cgi/content/full/115/6/e718
26. Wandstrat TL, Kaplan B. Pharmacoeconomicimpact of factors affecting compliance withantibiotic regimens in the treatment ofacute otitis media. Pediatr Infect Dis J. 1997;16(suppl 2):S27–S29
27. Zhu J, Stuver SO, Epstein AM, SchneiderEC, Weissman JS, Weingart SN. Can werely on patients’ reports of adverseevents? Med Care. 2011;49(10):948–955
28. Ho J, Taylor DM, Cabalag MS, Ugoni A,Yeoh M. Factors that impact onemergency department patientcompliance with antibiotic regimens.Emerg Med J. 2010;27(11):815–820
29. Fenerty SD, O’Neill JL, Gustafson CJ,Feldman SR. Maternal adherence factorsin the treatment of pediatric atopicdermatitis. JAMA Dermatol. 2013;149(2):229–231
30. Brown KK, Rehmus WE, Kimball AB.Determining the relative importance ofpatient motivations for nonadherence to
topical corticosteroid therapy inpsoriasis. J Am Acad Dermatol. 2006;55(4):607–613
31. Byczkowski TL, Fitzgerald M, KennebeckS, et al. A comprehensive view ofparental satisfaction with pediatricemergency department visits. AnnEmerg Med. 2013;62(4):340–350
32. Magaret ND, Clark TA, Warden CR,Magnusson AR, Hedges JR. Patientsatisfaction in the emergencydepartment—a survey of pediatricpatients and their parents. Acad EmergMed. 2002;9(12):1379–1388
33. Kassam R, Collins JB, Berkowitz J.Patient satisfaction with pharmaceuticalcare delivery in community pharmacies.Patient Prefer Adherence. 2012;6:337–348
34. Sadatsafavi M, FitzGerald M, Marra C,Lynd L. Costs and health outcomesassociated with primary vs secondarycare after an asthma-relatedhospitalization: a population-basedstudy. Chest. 2013;144(2):428–435
35. Zandieh SO, Goldmann DA, Keohane CA,Yoon C, Bates DW, Kaushal R. Risk factorsin preventable adverse drug events inpediatric outpatients. J Pediatr. 2008;152(2):225–231
36. Lexicomp. Patient Education. Databases& Modules. Available at: www.lexi.com/institutions/products/online/database-module-descriptions/patient-education/.Accessed October 23, 2014
37. Wang JK, Herzog NS, Kaushal R, Park C,Mochizuki C, Weingarten SR. Preventionof pediatric medication errors byhospital pharmacists and the potentialbenefit of computerized physician orderentry. Pediatrics. 2007;119(1). Availableat: www.pediatrics.org/cgi/content/full/119/1/e77
38. Ferranti J, Horvath MM, Cozart H,Whitehurst J, Eckstrand J. Reevaluatingthe safety profile of pediatrics:
a comparison of computerized adverse
drug event surveillance and voluntaryreporting in the pediatric environment.
Pediatrics. 2008;121(5). Available at:www.pediatrics.org/cgi/content/full/121/
5/e1201
39. Sharek PJ, McClead RE Jr, Taketomo C,
et al. An intervention to decreasenarcotic-related adverse drug events in
children’s hospitals. Pediatrics. 2008;122(4). Available at: www.pediatrics.org/
cgi/content/full/122/4/e861
40. Lee BH, Lehmann CU, Jackson EV, et al.
Assessing controlled substanceprescribing errors in a pediatric
teaching hospital: an analysis of thesafety of analgesic prescription practice
in the transition from the hospital tohome. J Pain. 2009;10(2):160–166
41. Bukstein DA, Luskin AT, Bernstein A.“Real-world” effectiveness of daily
controller medicine in children with mildpersistent asthma. Ann Allergy Asthma
Immunol. 2003;90(5):543–549
42. Kelloway JS, Wyatt RA, Adlis SA.
Comparison of patients’ compliance withprescribed oral and inhaled asthma
medications. Arch Intern Med. 1994;154(12):1349–1352
43. Partridge MR, van der Molen T, Myrseth
SE, Busse WW. Attitudes and actions ofasthma patients on regular maintenance
therapy: the INSPIRE study. BMC PulmMed. 2006;6:13
44. Penner LA, Orom H, Albrecht TL, et al.Camera-related behaviors during video
recorded medical interactions.J Nonverbal Behav. 2007;31(2):99–117
45. Pringle M, Stewart-Evans C. Doesawareness of being video recorded
affect doctors’ consultation behaviour?Br J Gen Pract. 1990;40(340):455–458
PEDIATRICS Volume 135, number 1, January 2015 101 by guest on June 28, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-3885 originally published online December 15, 2014; 2015;135;94Pediatrics
Nikki L. LubckeRoderick C. Jorgenson, Holly L. Weber, Rachel E. Pearson, Pascale Carayon and
Jessica M. Benjamin, Elizabeth D. Cox, Philip J. Trapskin, Victoria P. Rajamanickam,Family-Initiated Dialogue About Medications During Family-Centered Rounds
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/135/1/94including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/135/1/94#BIBLThis article cites 40 articles, 13 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 28, 2018www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2013-3885 originally published online December 15, 2014; 2015;135;94Pediatrics
Nikki L. LubckeRoderick C. Jorgenson, Holly L. Weber, Rachel E. Pearson, Pascale Carayon and
Jessica M. Benjamin, Elizabeth D. Cox, Philip J. Trapskin, Victoria P. Rajamanickam,Family-Initiated Dialogue About Medications During Family-Centered Rounds
http://pediatrics.aappublications.org/content/135/1/94located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2014/12/09/peds.2013-3885.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 28, 2018www.aappublications.org/newsDownloaded from





























