Embed Size (px)
Citation preview

REGULAR ARTICLE
Fathers’ involvement in Swedish child health care – the role of nurses’practices and attitudesPamela Massoudi ([email protected])1,2, Birgitta Wickberg3, C Philip Hwang1
1.Department of Psychology, University of Gothenburg, Gothenburg, Sweden2.Unit for Research and Development, Kronoberg County Council, Vaxjo, Sweden3.Research and Development Unit, South Bohuslan County Council, Molndal, Sweden
KeywordsAttitudes, Child health care, Fathers, Involvement,Nursing
CorrespondencePamela Massoudi, FoU-Kronoberg, Box 1223,S-351 12 Vaxjo, Sweden.Tel: +46 470 586387 |Fax +46 470 586455 |Email: [email protected]
Received23 July 2010; revised 27 September 2010;accepted 29 September 2010.
DOI:10.1111/j.1651-2227.2010.02047.x
ABSTRACTAim: To investigate how nurses in Swedish child health care perceived working with
fathers, and to what extent they offered support to, and included fathers in clinical encoun-
ters.Methods: A random sample of all nurses in Swedish child health care, 499 nurses,
were asked to complete a postal questionnaire. The response rate was 70%. Data were
analysed with content analysis, the chi-square test and logistic regression models.Results: Almost all of the nurses found working with fathers positive. Fathers’ partici-
pation in child health care was much lower than that of mothers’. Almost 90% of the
nurses estimated that it rarely came to their attention that a father was distressed, and less
than one of five nurses had offered supportive counselling to any distressed father in the
previous year. Nurses with regular supervision on mental health issues and nurses with a
paediatric specialization were more likely to offer supportive counselling to fathers. Approxi-
mately 50% of the nurses had an ambivalent attitude towards fathers’ caring capacity when
compared to that of mothers.
Conclusions: Fathers received less support from child health nurses, and many nurses wereambivalent about fathers’ caring abilities. Methods need to be developed to involve both parents inchild health care.
INTRODUCTIONPaternal involvement in childcare has been shown toenhance parental responsiveness and closeness in father–child relationships and also seems to predict differentaspects of adult adjustment (1). With changing culturalexpectations concerning men as fathers, and dual earnerfamilies gradually becoming the norm in most Western soci-eties, fathers have begun to take increasing responsibilityfor childcare. The importance of encouraging fathers’ earlyinvolvement in their children’s care in general as well as intheir children’s healthcare has been emphasized in severalstudies (1–3).
Living up to new expectations and demands is not alwayseasy. Literature reviews of fatherhood experience revealsthat fathers initially have positive expectations and inten-tions but during the first few weeks after the birth of theirnewborn they are confronted with the realities of adjustingto fatherhood, including experiences of distress, frustrationand inadequacy. Many fathers have stated that they graduallybond with their children and find a sense of satisfaction infathering but also that the absence of role models forces themto create their own roles for involved fatherhood (4,5).
Support for fathers’ involvement in childcare varies fromcountry to country. Many countries have little or no
paternity leave at all (6). Sweden was one of the first coun-tries to introduce paid parental leave for fathers in 1974.Sweden now has one of the world’s most generous parentaland paternity leave policies, entitling fathers to paid paternalleave for 10 days in conjunction with the birth of the childand another 60 days that can be used any time until thechild is 8 years old. In addition, fathers have full access tothe 360 days of parental leave that can be shared by bothparents. In 2008, 90% of all fathers took some parentalleave, and 22% of the total number of parental benefit dayswas paid to fathers (7). This can be compared with 1974when only 3% of fathers took any parental leave, with intotal 0.5% of the days (8). In Sweden, there is an ongoingdebate about how to increase fathers’ proportion of theparental leave. The parent with the lower salary tends to stayhome to care for the child and that tends to be the mother.
Sweden also has a long tradition of preventive childhealth care, free of charge. The degree of participation therevaries between fathers and mothers (9). The services includeimmunizations, regular health check-ups and screening aswell as support and advice to parents (10). During the pastdecade, screening new mothers for depression has graduallybeen implemented in the Swedish child health care services(11), and it has recently been recommended in the national
Acta Pædiatrica ISSN 0803–5253
396 ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401

guidelines for the treatment of depression and anxiety disor-ders (12).
Depression rates among new fathers vary depending onthe type of sample, measures used and time point chosenbut seem to be significantly lower than for women. A recentinternational meta-analysis estimated a prevalence rate ofapproximately 10%. When cases were defined using inter-view methods, a rate of 5% was estimated. The highest rateswere reported in US studies (13). A large UK study found a4% rate of depression symptoms in a community sample offathers with cases defined using self-rating scales (14). Cor-relation between paternal and maternal depressive symp-toms seems to be minimal during the antenatal period butincreases gradually over the first postpartum year(13,15,16). Antenatal mood, history of depression, partnerrelationship and partner’s mood have all been shown to bethe strongest predictors of paternal postnatal depression(13,14,17–19). There is some evidence that depression andanxiety in fathers may have adverse impacts on the child,independently of maternal psychiatric well-being. In somestudies, the risk of adverse outcome in the child differedsomewhat when fathers were distressed as compared withmothers, and sons seemed to be at more risk than daughters(14,18,19).
Against the backdrop of the Swedish parental leave pol-icy and child health care system stressing the importance ofboth parents, we wanted to investigate how nurses in Swed-ish child health care perceived working with fathers in gen-eral and to what extent they offered support to and includedfathers in clinical encounters. We were also interested inexploring nurses’ attitudes to fathers as carers of infants.
SUBJECTS AND METHODSSubjectsA random sample of 512 Swedish child health nurses,drawn from the total population of 2580 nurses at childhealth centres (CHC) in Sweden, were invited to take partin the study. Thirteen nurses were excluded from the samplefor reasons of retirement, moving or otherwise no longerworking at the centre, thus resulting in 499 valid question-naires being sent. After two reminders, 348 questionnaireswere returned, a response rate of 70%.
ProcedureNames and addresses of all nurses working at CHCs wereobtained from the child health coordinators in each county.All the names on the lists were numbered and a randomtable used to select the nurses who were invited to partici-pate in the study. A postal questionnaire, containing bothopen-ended and closed-ended questions and with an intro-ductory letter, was mailed to each nurse. Two reminderswere sent to non-respondents at 2- to 3-week intervals.
MeasuresA questionnaire was constructed for the study. Questionswere asked about the following variables (response alterna-tives are given in brackets):
Background factorsThe nurses were asked about their age, professional back-ground, years of experience at CHCs, whether they workedexclusively with child health at the primary health care unitor whether they had other assignments as well. They werealso asked whether they routinely screened mothers fordepression with the Edinburgh Postnatal Depression Scale(EPDS), whether they offered distressed mothers supportivevisits and whether they had regular supervision from a men-tal health specialist with whom they could discuss mentalhealth issues.
Working with fathers and fathers’ participation in CHCactivitiesThe nurses were asked to describe, in their own words, howthey perceived working with fathers in general. The nurseswere also asked how often fathers came to the CHC (atalmost all visits, at many visits, at around half of the visits,occasionally or almost never) and how many of the fathersvs. mothers attended the parental education groups (Almostall ⁄ all, many, around half, a few or almost none ⁄ none).
Nurses’ support to fathers with distressThe nurses were asked to estimate how often it came totheir attention that a father was distressed (in almost allcases, in many cases, in around half of all the cases, occa-sionally or almost never). The nurses were also askedwhether they had offered supportive counselling to anyfathers in the previous year (yes or no). If they had, theywere asked to specify to how many fathers and to give ashort description of the problems discussed and the type ofthe fathers’ distress. The nurses were asked whether theydid anything in particular to identify fathers with distress,and if so to describe what they did.
Nurses’ attitudes towards fathers as carers of infantsThe nurses were asked to reflect on four statements regard-ing attitudes to fathers as carers of infants and to chooseone alternative (agree ⁄ agree to some extent ⁄ disagree) thatbest matched their view.
1. Mothers are instinctively better at caring for infants thanfathers.
2. Fathers are as sensitive to infants’ needs as mothers.3. With the exception of breastfeeding, there is no differ-
ence between mothers’ and fathers’ abilities to relate toand care for infants.
4. Fathers have to learn what mothers know intuitively.
AnalysisAll quantitative data were recorded and analysed with theSPSS Statistics 17.0 software (SPSS Inc, Chicago, IL, USA).Chi-square and logistic regression analyses were carried outto see how fathers’ participation in child health care activi-ties, nurses’ attitudes towards fathers as carers of infantsand nurses’ support to distressed fathers were associatedwith a number of variables such as nurses’ access to
Massoudi et al. Fathers’ involvement in child health care
ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401 397

psychological supervision, screening mothers routinely withthe EPDS as well as factors such as the nurse’s age, years ofexperience in child health care, training and type of work-load. Ninety-five per cent confidence intervals (CI) werecalculated, and p-values <0.05 were considered statisticallysignificant. Content analysis (20) was used for the qualita-tive responses. All responses, in most cases fairly short state-ments, were listed and then condensed into categories closeto the text. Some responses consisted of more than oneaspect and could thus be placed in more than one category,resulting in the number of statements being larger than thenumber of responses.
EthicsThis study was performed in accordance with The SwedishResearch Council’s research ethics principles in humanis-tic-social scientific research (21).
RESULTSThe majority, 263 (76%) of the 348 registered nurses in thestudy, were district nurses (with primary health care train-ing), 44 (13%) were paediatric nurses and 40 (11%) hadboth qualifications. A few nurses (8) were also registeredmidwives. Almost 90% of the nurses worked in the publichealth care system, while 10% worked at private health cen-tres contracted by the counties. Forty-three per cent of thenurses worked exclusively in child health care with infants,preschool children and their parents, whereas the remain-ing 57% had other assignments as well, such as workingwith adult patients and the elderly in primary health care.Sixty-five per cent of the nurses (220 ⁄ 348) had regularsupervision, usually with a consultant perinatal and childpsychologist, at which questions concerning mental healthissues could be raised. The nurses’ years of experience inchild health care varied between 0.5 and 35 years, with amean of 13.3 years. The mean age was quite high, with over60% of the nurses being 50 or older and only 10% 39 oryounger.
How child health nurses perceived working with fathersand fathers’ participation in CHC activitiesWhen asked to describe how they perceived working withfathers, in an open question, 326 ⁄ 348 nurses replied with atotal of 485 statements condensed into four categories(Table 1). Practically all of the nurses seemed to be positivetowards working with fathers. Many statements (41%) wereshort but generally positive such as positive, nice, importantor important for the child or the whole family. Anothercategory reflected attitudes (22%), such as working withfathers being just as natural or important as working withmothers, and that fathers are capable. Others wereimpressed and ⁄ or found working with fathers different,enlightening or even touching. Some statements (8%)reflected the importance of the nurses’ own role in encour-aging fathers’ involvement in different ways, such as raisingissues on the role of the father when both parents were pres-ent and offering individual appointments and group
activities at times that made it possible for the father toattend as well. A few of the nurses were self-critical; somehad ideas of their own about how to approach fathers.
Issues concerning the frequency of fathers’ participationin the CHC programme were raised by over 40% of thenurses in 142 statements (29%). Some mentioned theirimpression that fathers’ involvement had increased over theyears, particularly younger fathers, while others were disap-pointed that fathers’ participation was still low and that theyrarely met some of the fathers. Several nurses described awide range of paternal involvement; on the one hand,fathers who were very actively involved in caring for thechild and regularly attended the CHC, and on the other,fathers they only met once or a few times during the earlydays after the birth when the fathers were on the 10-daypaternity leave. Financial ⁄ work-related factors as well asthe nurses’ own responsibility in making fathers feel wel-come and important were mentioned as factors that mightaffect fathers’ attendance at the CHC.
Almost all (94%) of the nurses stated that the parents intheir district (at some CHCs only first-time parents) wereoffered parental education groups and that mothers andfathers were usually invited to attend together. Nearly 80%of the nurses stated that almost all or all mothers attended agroup, while only 8% of the nurses said the same aboutfathers (Table 2). Approximately 20% of the nurses statedthat fathers were invited to attend groups exclusively for
Table 1 Main themes and categories describing how child health nurses per-
ceived working with fathers, and number of statements in each category. Four
hundred and eighty-five statements by 326 nurses
Main themes and categoriesNumber ofstatements (%)
Generally positive comments 199 (41)
Positive, nice, good, important for the child, for the
mother or for the whole family
Issues concerning the frequency and timing of fathers’
attendance
142 (29)
Fathers’ participation is too low, wish for more contact 43
Fathers’ participation has increased over the years,
young fathers participate more, some fathers come
more often when the child is older. The first home
visit ⁄ first weeks are important, participation declines
after that
99
Attitudes concerning fathers as parents and working with
fathers
107 (22)
Natural, just as important ⁄ natural as working with
mothers
31
Fathers are competent, many fathers are capable, nice
that fathers are involved in their children
34
Impressed by fathers’ competence, different,
stimulating, enlightening, rewarding, touching
42
The nurses’ role 37 (8)
One should do more for fathers, self-critical, too many
women at child health centres (CHC)
13
Important to encourage fathers’ involvement and ⁄ or
attendance at CHC, efforts to give attention to fathers
and raise father-oriented issues
24
Total 485
Fathers’ involvement in child health care Massoudi et al.
398 ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401
fathers, in some cases organized by a different organizationthan the CHC, such as the city council. Fathers’ attendanceat these groups was higher.
Support to distressed fathersAs many as 89% of the nurses (302 ⁄ 339) estimated that itonly occasionally or practically never came to their atten-tion that a father was distressed. Only 27% of the nursesstated that they attempted by different means to identifyfathers who were distressed. When asked to describe whatthey actually did, around one-fifth of these nurses men-tioned the first home visit as an important occasion to meetand talk to the father, as almost all fathers stay at home forthe 10-day paternity leave. Many added that they took thisopportunity to ask the father how he was feeling and howhe was adjusting and that they tried to give fathers the samekind of attention as mothers when the father actually cameto the CHC. No structured methods were used.
Sixty nurses (17.5%) stated that they had offered support-ive counselling to one or more fathers during the previousyear. They had given support to one, or ‘a few’ fathers.Almost one-third of these nurses mentioned problems in thecouples’ relationship, including separation and custodydisputes as the most common reason for the father needingsupport. Eight nurses mentioned the mother’s problems,such as depression, other mental or physical illness or sub-stance abuse as being a cause of the fathers’ distress. Otherreasons mentioned were the child being ill, or worryingabout the child possibly being ill, refugees with traumaticexperiences and ⁄ or difficulties adjusting such as insecurefathers in need of support, or difficulties adjusting to thenew role as a parent or to being the child’s primary care-giver. For some fathers in need of support, there were anumber of social, psychological and medical needs in thefamily. The odds of offering supportive counselling tofathers was three times as great (OR = 3.1 CI 1.2–7.9) fornurses who had regular supervision concerning mentalhealth issues and six times as great (OR = 6.6 CI 2.0–22.4)for nurses with a paediatric specialization (Table 3). In theinitial univariate analysis, working solely in child healthcare seemed to be associated with offering supportive coun-selling (OR = 2.4 CI 1.3–4.1), but this factor was no longersignificant in the further multivariate analysis. The nurses’age and years of experience in child health care was notassociated with giving support to fathers, nor using the
EPDS routinely with mothers or offering supportive coun-selling to mothers.
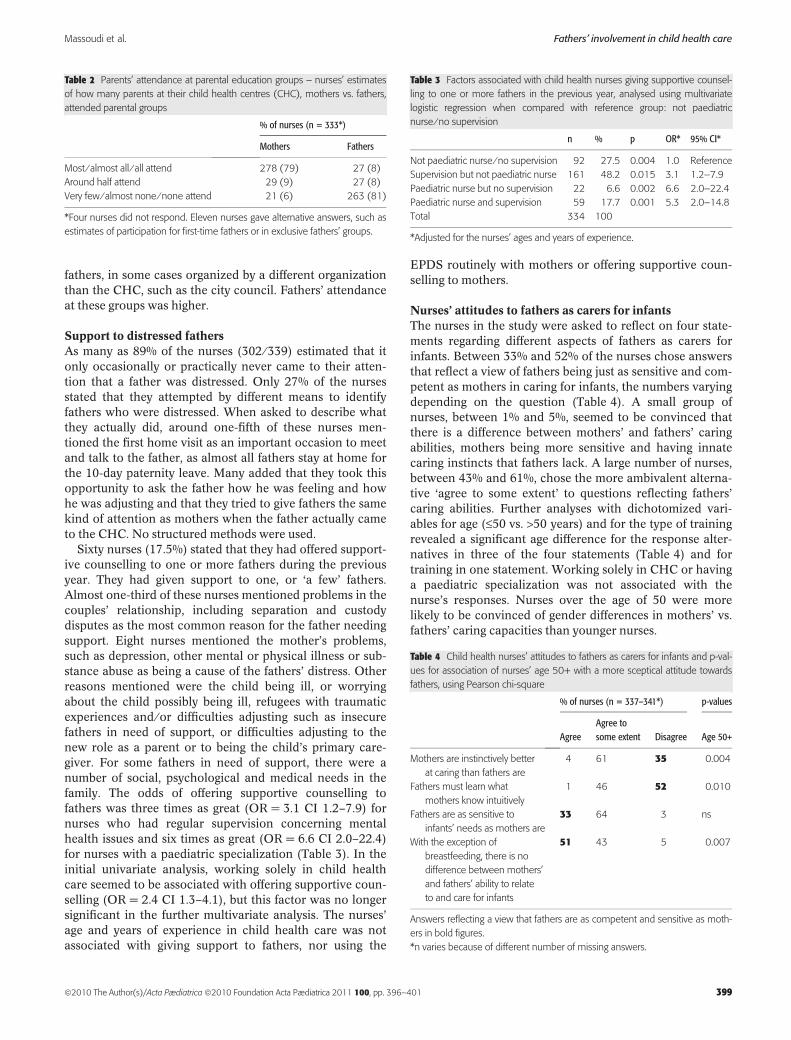
Nurses’ attitudes to fathers as carers for infantsThe nurses in the study were asked to reflect on four state-ments regarding different aspects of fathers as carers forinfants. Between 33% and 52% of the nurses chose answersthat reflect a view of fathers being just as sensitive and com-petent as mothers in caring for infants, the numbers varyingdepending on the question (Table 4). A small group ofnurses, between 1% and 5%, seemed to be convinced thatthere is a difference between mothers’ and fathers’ caringabilities, mothers being more sensitive and having innatecaring instincts that fathers lack. A large number of nurses,between 43% and 61%, chose the more ambivalent alterna-tive ‘agree to some extent’ to questions reflecting fathers’caring abilities. Further analyses with dichotomized vari-ables for age (£50 vs. >50 years) and for the type of trainingrevealed a significant age difference for the response alter-natives in three of the four statements (Table 4) and fortraining in one statement. Working solely in CHC or havinga paediatric specialization was not associated with thenurse’s responses. Nurses over the age of 50 were morelikely to be convinced of gender differences in mothers’ vs.fathers’ caring capacities than younger nurses.
Table 2 Parents’ attendance at parental education groups – nurses’ estimates
of how many parents at their child health centres (CHC), mothers vs. fathers,
attended parental groups
% of nurses (n = 333*)
Mothers Fathers
Most ⁄ almost all ⁄ all attend 278 (79) 27 (8)
Around half attend 29 (9) 27 (8)
Very few ⁄ almost none ⁄ none attend 21 (6) 263 (81)
*Four nurses did not respond. Eleven nurses gave alternative answers, such as
estimates of participation for first-time fathers or in exclusive fathers’ groups.
Table 3 Factors associated with child health nurses giving supportive counsel-
ling to one or more fathers in the previous year, analysed using multivariate
logistic regression when compared with reference group: not paediatric
nurse ⁄ no supervision
n % p OR* 95% CI*
Not paediatric nurse ⁄ no supervision 92 27.5 0.004 1.0 Reference
Supervision but not paediatric nurse 161 48.2 0.015 3.1 1.2–7.9
Paediatric nurse but no supervision 22 6.6 0.002 6.6 2.0–22.4
Paediatric nurse and supervision 59 17.7 0.001 5.3 2.0–14.8
Total 334 100
*Adjusted for the nurses’ ages and years of experience.
Table 4 Child health nurses’ attitudes to fathers as carers for infants and p-val-
ues for association of nurses’ age 50+ with a more sceptical attitude towards
fathers, using Pearson chi-square
% of nurses (n = 337–341*) p-values
AgreeAgree tosome extent Disagree Age 50+
Mothers are instinctively better
at caring than fathers are
4 61 35 0.004
Fathers must learn what
mothers know intuitively
1 46 52 0.010
Fathers are as sensitive to
infants’ needs as mothers are
33 64 3 ns
With the exception of
breastfeeding, there is no
difference between mothers’
and fathers’ ability to relate
to and care for infants
51 43 5 0.007
Answers reflecting a view that fathers are as competent and sensitive as moth-
ers in bold figures.
*n varies because of different number of missing answers.
Massoudi et al. Fathers’ involvement in child health care
ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401 399

Only one of three nurses fully agreed with the statementthat fathers are as sensitive to infants’ needs as mothers. Noassociation with the nurses’ age or training was found forthis statement. Two of three nurses agreed, completely or tosome extent, with the statement that mothers are instinc-tively better at caring for infants than fathers. Only 50% ofthe nurses disagreed with the statement that fathers have tolearn what mothers know instinctively. This was the onlystatement where type of training was found to be significant,paediatric nurses being somewhat less sceptical aboutfathers’ instinctive capacities.
DISCUSSIONSweden stands out internationally for its generous and gen-der-neutral parental leave policy as well as for its long tradi-tion of child health care services. The Swedish departmentof welfare has an ambition that support offered to parentsby the child health services, individually or in groups,should be designed so that both mothers and fathers feelequally welcome to participate (22). The results of thisnational study show that many child health nurses, to someextent, still favour mothers.
The present study has shown, in accordance with otherSwedish studies, that fathers’ participation in the activitiesat the CHC was much less than that of mothers (23,24). Arecent national report concluded that mothers’ participa-tion in group encounters at the CHC was at least five timesas great as fathers (22). When asked about how they per-ceived working with fathers, many nurses in our study wereconcerned with the frequency of fathers’ attendance at theCHC. The nurses clearly stressed the importance of theirencounters with fathers during the first few weeks after thebirth of the child, when most fathers are on paternity leave.Fathers’ attendance at the CHC usually declined after thisperiod. This pattern of attendance basically follows fathers’work patterns. CHC visits and group encounters are oftenscheduled during the daytime, making it more difficult forthe working parent to attend.
One consequence of fathers’ low attendance at the CHCseemed to be that they did not receive support to the sameextent as mothers did. Only one of four nurses in this studystated that they attempted to identify distressed fathers, ascompared with two of three nurses in our previous studyconcerning mothers (11). Methods mentioned by the nursesto identify distressed fathers were mainly asking fathershow they were feeling at the first home visit, when manyother topics and practical issues are addressed. No system-atic methods were used in detecting distressed fathers,which was to be expected, in view of the fact that this is nota recommendation in the programme for the child healthservices. The nurses themselves seemed to be aware of theirmethods being insufficient, as a vast majority estimated thatthey would only occasionally or practically never know if afather was distressed, and rarely offered support to dis-tressed fathers. Less than one of five nurses had offered sup-portive counselling to any father during the previous year.In our previous study concerning mothers, however, almost
nine of ten of these nurses stated that they offered distressedmothers supportive counselling (11). Nurses with regularsupervision (OR = 3.1, CI 1.2–7.9) as well as nurses with apaediatric specialization (OR = 6.6, CI 2.0–22.4) were morelikely to give extra support to fathers. The results indicatestrong associations although the confidence intervals arewide. A corresponding association with regular supervisionwas found in our previous study concerning support tomothers (11). The association between having a paediatricspecialization and giving support to fathers was notexplained by working solely in child healthcare, by thenurses’ age or by years of experience. Possible explanationsmay be related to differences in the nurses’ professionaltraining and experience. Paediatric nurses’ training mayhave a more family-oriented approach than district nurses’training. It is also possible that some paediatric nurses had abackground in paediatric hospital wards working with sickchildren and their families, where both parents are oftenactively involved.
One important issue to be addressed is how child healthnurses’ attitudes to fathers as carers for their infants mayinfluence fathers’ involvement in the CHC programme.Although subtle differences in parenting styles can beobserved in mothers and fathers, the evidence suggests thatsensitivity and responsiveness is not so much related to gen-der as to caretaking experience and other psychological fac-tors. Fathers seem to interact with newborn infants in amanner similar to mothers, even showing similar changes inhormonal levels (1). Despite positive intentions concerningworking with fathers, many nurses in our study seemed tohave traditional views on mothers’ vs. fathers’ instinctivecompetencies. This was particularly evident for nurses overthe age of 50. A recent qualitative study of district nurses’professional practices revealed that child health care wasstill assumed to be a mother-orientated working area wheremothers were regarded as primary givers of care and welfareand fathers’ absence was taken for granted. The nurses’ ten-dencies to fall back on ‘female competence’ in their contactswith parents and the very broad interdisciplinary content ofthe district nurses’ training were discussed (25). All of thenurses in our study were women. Could it be that they werebetter at recognizing distress in women than in men, andmore comfortable giving support to women? In a nationalreport by Sarkadi (26), an analysis of CHC waiting roomsfound 50% of CHC environments to be aimed at mothers.In another study by Fagerskiold, fathers were interviewedabout their expectations of the child health nurse. Thefathers stressed the importance of feeling welcomed andhaving a trusting relationship with the child health nurse.While some fathers expressed a desire for more communica-tion with and support from the nurse, others preferred sup-port from friends and colleagues (27). In other words,fathers’ needs and help-seeking behaviours vary, and atrustful relationship with the child health nurse may helpfathers express their specific needs.
In recent decades, there has been a major shift in focus inchild health care, from mainly focusing on the child’s physi-cal health to more focus on psychosocial issues (28). As
Fathers’ involvement in child health care Massoudi et al.
400 ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401

awareness of postnatal distress increased in this past dec-ade, the CHCs gradually started to include screening andsupport to distressed mothers in their programmes. It is,however, important to consider what signals are conveyedby nurses to fathers, as to their importance to the infant andparental role, if the routine includes assessing only newmothers’ emotional well-being. If the aim of the CHC is toinclude both parents, awareness of gender bias needs toincrease and methods must be developed for approachingfathers, too, about how they experience their fatherhood,how they are feeling and what type of support they expectfrom the child health nurse. Findings from a Norwegianstudy suggest that the information provided by nurses at thefirst home visit may have an impact on the frequency ofpostnatal depression in mothers (29). Considering thatfathers are often present at the first home visit, it may be asuitable occasion to present fathers with information onparenting from the fathers’ perspective, including aspectsconcerning the emotional health of fathers and support pro-vided by the health services.
ACKNOWLEDGEMENTSWe express our gratitude to all the nurses who took part inthe study. We also thank Professor Linda Haas for valuablecomments on the manuscript.
FUNDINGThis study was supported by the Kronoberg County Counciland the Clas Groschinsky Trust Fund.
References
1. Lewis C, Lamb ME. Fathers’ influences on children’s develop-ment: the evidence from two-parent families. Eur J PsycholEduc 2003; 18: 212.
2. Sarkadi A, Kristiansson R, Oberklaid F, Bremberg B. Fathers’involvement and children’s developmental outcomes: a system-atic review of longitudinal studies. Acta Paediatr 2008; 97:153–8.
3. Moore T, Kotelchuck M. Predictors of Urban fathers’involvement in their child’s health care. Pediatrics 2004; 113:574–80.
4. Nystrom K, Ohrling K. Parenthood experiences during thechild’s first year: literature review. J Adv Nurs 2004; 46: 319–30.
5. Goodman JH. Becoming an involved father of an infant.J Obstet Gynecol Neonatal Nurs 2005; 34: 190–200.
6. O’Brien M. Fathers, parental leave policies, and infant qualityof life: International perspectives and policy impact. Ann AmAcad Pol Soc Sci 2009; 624: 190–213.
7. Haas L, Cronholm A, Duvander A-Z, Hwang CP. Country Note– Sweden. In: Moss P, editor. International review of leavepolicies and related research. London: Department for BusinessEnterprise & Regulatory Reform, 2009: 326–36.
8. Forsakringskassan. 2008 [The Social Insurance Office. InSwedish.] Available from http://www.forsakringskassan.se/omfk/statistik_och_analys/barn_och_familj/foraldrapenning.
9. Socialstyrelsen. Stod i foraldraskapet: betankande. Stockholm:Report from Fritze, 1997 (In Swedish).
10. Sundelin C, Hakansson A. The importance of the Child HealthServices to the health of children: summary of the state-of-the-art document from the Sigtuna conference on Child Health Ser-vices with a view to the future. Acta Paediatr Suppl 2000; 89:76–9.
11. Massoudi P, Wickberg B, Hwang P. Screening for postnataldepression in Swedish child health care. Acta Paediatr 2007;96: 897–901.
12. Socialstyrelsen. Nationella riktlinjer for depressionssjukdomoch angestsyndrom: beslutsstod for prioriteringar. [Nationalguidelines for treatment of depression and anxiety disorders. InSwedish]. Stockholm: 2010.
13. Paulson JF, Bazemore SD. Prenatal and postpartum depressionin fathers and its association with maternal depression: a meta-analysis. JAMA 2010; 303: 1961–9.
14. Ramchandani P, Stein A, Evans J, O’Connor TG, ALSPACstudy team. Paternal depression in the postnatal period andchild development: a prospective population study. Lancet2005; 365: 2201–5.
15. Matthey S, Barnett B, Ungerer J, Waters B. Paternal andmaternal depressed mood during the transition to parenthood.J Affect Disord 2000; 60: 75–85.
16. Areias M, Kumar R, Barros H, Figueiredo E. Correlates ofpostnatal depression in mothers and fathers. Br J Psychiatry1996; 169: 36–41.
17. Goodman JH. Paternal postpartum depression, its relationshipto maternal postpartum depression, and implications for familyhealth. J Adv Nurs 2004; 45: 26–35.
18. Paulson JF, Dauber S, Leiferman JA. Individual and combinedeffects of postpartum depression in mothers and fathers onparenting behavior. Pediatrics 2006; 118: 659–68.
19. Ramchandani P, Psychogiou L. Paternal psychiatric disordersand children’s psychosocial development. Lancet 2009; 374:646.
20. Berg BL. Qualitative research methods for the social sciences.Boston: Pearson, 2004.
21. Swedish Research Council. The humanities and social sciences.CODEX – rules and guidelines for research. Available fromhttp://www.codex.vr.se/en/forskninghumsam.shtml.
22. SOU. Foraldrastod – en vinst for alla. [Parental support – goodfor all. In Swedish]. Stockholm: Government Official Report,2008.
23. Petersson C, Petersson K, Hakansson A. General parentaleducation in Sweden: participants and non-participants.Scand J Prim Health Care 2003; 21: 43–6.
24. Hallberg A-C. Parental support in a changing society. Malmo:Faculty of Medicine, Lund University, 2006.
25. Lindstrom A-C. Nagot som inte langre ar: distriktsskoterskorsyrkesutovning pa vardcentral ur ett genus perspektiv.[Something that is no longer – District nurses’ professional prac-tice at the primary health centre from a gender perspective. InSwedish]. Goteborg: Sahlgrenska Akademin vid GoteborgsUniversitet Institutionen for vardvetenskap och halsa, 2007.
26. Sarkadi A (ed). Foraldrastod i Sverige idag: var, nar och hur?[Parental support in Sweden today: where, when and how? InSwedish]. Kartlaggning och behovsinventering infor regerin-gens nationella strategi for 2009 ⁄ 2010 Underlagsrapport.Ostersund: Statens Folkhalsoinstitut, 2008.
27. Fagerskiold A. Support of fathers of infants by the child healthnurse. Scand J Caring Sci 2006; 20: 79–85.
28. Hallberg A-C, Lindbladh E, Petersson K, Rastam L, HakanssonA. Swedish child health care in a changing society. Scand JCaring Sci 2005; 19: 196–203.
29. Glavin K, Smith L, Sorum R. Prevalence of postpartumdepression in two municipalities in Norway. Scand J Caring Sci2009; 4: 705–10.
Massoudi et al. Fathers’ involvement in child health care
ª2010 The Author(s)/Acta Pædiatrica ª2010 Foundation Acta Pædiatrica 2011 100, pp. 396–401 401