Embed Size (px)
Citation preview

Faut-il traiter les Glomérulonéphrites extramembraneuses primitives ?
Gabriel Choukroun
Service de Néphrologie –Dialyse - Transplantation - CHU AmiensERI-12 INSERM - Amiens
IgG

Glomérulonéphrite Extramembraneuse
• Première cause de syndrome néphrotique de l’adulte
• Deuxième cause de GNC de l’adulte
• Rare chez l’enfant
• Plus fréquente après 60 ans
• H > F
• Environ 25 % de forme secondaire

Glomérulonéphrite ExtramembraneusePrésentation clinique
• Syndrome néphrotique impur (80 %)Hématurie microscopique (70 %)HTA et IRC
• Protéinurie modérée ± hématurie (20 %)
• Thrombose des veines rénales (< 1 %)Douleur lombaireHématurie macroscopiqueElévation des LDHIRA

Aspects histologiques des GEM
dépôts

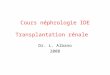
Aspects histologiques des GEMMicroscopie optique
Dépôts extra-membraneux pas toujours visiblesPas (ou peu) de prolifération cellulaire« Anomalies » de la MBG en regard des dépôts (coloration argentique)

Aspects histologiques des GEMIF : anti IgG
Dépôts extra-membraneux granuleux d'IgG (IgG1 et IgG4) dans tous les glomérules

Physiopathologie des GEM
RJ Glassock et al., N Engl J Med 2009

Principales causes de GEM secondaires
• GEM Primitives 75%
• GEM Secondaires 25%– Cancers : estomac, poumon, sein, colon, mélanome
– Hémopathies : LNH, Hodgkin
– LED, Sjögren, connectivite mixte
– Sarcoïdose, psoriasis, MICI, thyroïdite, drépanocytose
– Infections : hépatite B, paludisme, syphillis, filariose
– Médicaments : sels d’or, D pénicillamide, captopril, AINS, mercure

Glomérulonéphrites extramembraneuses
« Primitives » « Secondaires »
GEM
Cancers – HémopathiesMaladies « auto-immunes »InfectionsMédicaments et toxiquesAllo-immune (EPN)
Ac anti PLA2 type MAutres ?

Glomérulonéphrite extramembraneuse idiopathiqueUne maladie auto-immune
Idiopathic GEMHeymann Nephritis Allo-immune MN
MegalinAg M-type PLA2 Rc N endopeptidase

Identification du Rcp PLA2 de type M comme Ag cible dans les GEM idiopathiques
N = 37 patientsWB avec Broyats de glomérules normaux + sérum de patients ayant une « GEM idiopathiques »
LH Beck Jr et al., N Engl J Med 2009

Identification du Rcp PLA2 de type M comme Ag cible dans les GEM idiopathiques
LH Beck Jr et al., N Engl J Med 2009

Physiopathologie des GEM
Activation du Complément
production de MECDisruption du slip diaphragmeDétachement des podocytes
Disruption de :l’intégrité fonctionnelle de la MBG et la barrière de filtration des protéines
PodocytesC5b—9
ProtéinurieVoie alterne Complément
Atrophie tubulaireFibrose interstitielle
Cellules tubulaires
?

Faut-il traiter les GEM primitives ?
Risque de progression
Risque du traitement
Genre (M)Élévation de la créatinine
Pression artérielleProtéinurie (Débit et durée)
Élévation 2-microglobuline (> 0.5 µg/min)Lésions interstitielles et vasculaires

Cas clinique
Homme né en 1954
Hernie inguinaleTabac : 5 cigarettes/jour
Syndrome néphrotique (Pu > 5 g/j) impur (Hu + HTA)Scr : 94 µmol/l – eClcr : 85 ml/minGEM diagnostiqué en avril 2007

Cas clinique
Rx ThoraxFOGDColonoscopieTMD thoraco-abdominalCystoscopie
Tests immunologiquesPSA, CA 19/9, ACESérologies hépatites B et C

1. Rien, le pronostic est spontanément bon
2. IEC ± Diurétiques ± Statine ± AVK
3. Corticothérapie + Alkylant
4. Corticothérapie + MMF
5. Ciclosporine
6. Rituximab
Question 1 :Que faites-vous ?

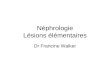
A Schieppati et al., N Engl J Med 1993
100 73 60 51 44 37 Nb de patients
n = 100 (68 H) 51 + 17 ansGEM histologiqueAucun traitement IS
A 5 ans : 65 % des patients sont en RC ou RP et 16 % en IRCTSi Sd N. Probabilité d’IRCT à 8 ans 25 %
Évolution spontanée des GEM primitives

Évolution spontanée des GEM primitives
Rémissionpartielle ou complète
ChronicitéSN persistant
Évolutionvers l’IRC T
Pronostic rénale
30 %Peu ou pas de
dégradation de la fonction rénale
40 % en 10 ansTraitement ?30 % en 2 ans
Bon pronostic

Traitement des GEM primitives

Traitement des GEM primitivesChez tous les patients
• Traitement du syndrome œdémateux
• Prévention du risque de thrombose veineuse
• Traitement de l’HTA : objectif PA < 130/80 mm Hg
• Traitement antiprotéinurique : IEC ± Diurétiques ±
ARAII
• Statine si syndrome néphrotique

Objectifs thérapeutiques
• Protéinurie• < 0,5 g/j Rémission complète• < 1 g/j ou < 3 g/j Rémission partielle
• Fonction rénale
• Prévention de la dégradation de la fonction rénale
• Réduction de la progression de l’IRC
• Décès

Traitement des GEM primitivesEn dehors du traitement symptomatique
•Corticothérapie
•Corticothérapie + Immunosuppresseur
•Ciclosporine ou Tacrolimus
•Mycophénolate mofétil
•Rituximab

Traitement des GEM primitivesCorticothérapie ou rien ?
DC Cattran et al., N Engl J Med 1989
Prospective randomized open label studyPrednisone 45 mg/m2 1 jour sur 2 pendant 6 mois vs pas de traitement
Control Group (N=77) Prednisone Group (N=81)
Age (median; range) 45 (16 – 83) 46 (18 – 77)
Sex (M/F) 44/33 61/20
Duration of disease (mo; mean ± SEM) 16.8 ± 1.0 15.2 ± 1.0
Creatinine (µmol/liter) Mean ± SEM (range)
103 ± 9 (53 – 574) 120 ± 10 (53 – 549)*
Creatinine Clearance (ml/sec/1.73m²) Mean ± SEM (range)
90 ± 4.8 (15 - 168) 78 ± 4.8 (15 – 156)
Protein excretion (g/24h) Mean ± SEM (range)
5.2 ± 0.9 (0.3 - 12.3) 6.9 ± 0.8 (0. 3- 26)*
Serum albumin (g/liter) Mean ± SEM (range)
30 ± 1 (17 – 47) 27 ± 1.3 (10 – 60)

Control
Prednisone
146 116 82 58 43 31 21 15
Months
Dec
lin
e in
Ren
al F
un
ctio
n
(Per
cen
t of
Pat
ien
ts)
0
20
40
60
80
100
0 12 24 36 48 60 72 84 96
Pas de différence entre les 2 groupes
Traitement des GEM primitivesCorticothérapie ou rien ?
DC Cattran et al., N Engl J Med 1989
p = 0.4

Changes in degree of Proteinuria in the Study Groups Changes in degree of Proteinuria in the Study Groups over 36 monthsover 36 months
Complete remission (%) Partiale remission (%)
Traitement des GEM primitivesCorticothérapie ou rien ?
DC Cattran et al., N Engl J Med 1989
Pas de différence entre les 2 groupes

MP 1 g IV x 3 MP 1 g IV x 3MP 1 g IV x 3
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
Study design
Traitement des GEM primitivesMP + chlorambucil

Traitement des GEM primitivesMP + Chlorambucil en ouvert
C Ponticelli et al., N Engl J Med 1989
p = 0.00001
Control Group (n = 39)
MP + CHL (n = 42)
* p < 0.01 versus basal value
**
* *
0
1
2
3
4
5
6
7
89
10
B 6 12 18 24
Months
Pro
tein
uri
a (g
/24
hr)

* p = 0.0002 versus Basal Value
p = 0.0041
Control Group
MP + CHL
Traitement des GEM primitivesMP + Chlorambucil en ouvert
C Ponticelli et al., N Engl J Med 1989
CChanges in the reciprocals of the plasma creatinine levels (Mean ±SD) in 30 treated and 25 control patients hanges in the reciprocals of the plasma creatinine levels (Mean ±SD) in 30 treated and 25 control patients followed for at least five yearsfollowed for at least five years

C Ponticelli et al., Kidney Int 1995
Slope of the mean reciprocal of plasma creatinine
n = 31 (Treated)
n = 25 (Controls)
° or * p < 0.05
°
°*
1.0
0.00
Time (months)
24 48 72 96 120
0.8
0.6
0.2
0.4
Pla
sma
crea
tin
ine
(mg/
dl)
Traitement des GEM primitivesMP + Chlorambucil

Cumulative probability of survival without dialysis
100
20
0
Time (months)24 48 72 96 120
80
60
40
60 %
92 %
Untreated
MP + CHLB
C Ponticelli et al., Kidney Int 1995
p = 0.0038
n = 81 GEM + SN – 10 years follow-up10 controls and 9 treated patients were lost to follow-up
Traitement des GEM primitivesMP + Chlorambucil

V Jha et al., J Am Soc Nephrol 2007
G 1 : Traitement symptomatiqueRestriction sodéeDiurétiqueAnti HTA
G2 : MP + CYP 6 months
Traitement des GEM primitivesMP + Cyclophosphamide

MP 1 g IV x 3 MP 1 g IV x 3MP 1 g IV x 3
MP 1 g IV x 3 MP 1 g IV x 3 MP 1 g IV x 3
R
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Cyclophosphamine2.5 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Cyclophosphamine2.5 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Cyclophosphamine2.5 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
Prednisone0.4 mg/kg 27 d
Chlorambucil0.2 mg/kg 30 d
C Ponticelli et al., J Am Soc Nephrol 1998
Study design
Traitement des GEM primitivesMP + chlorambucil vs MP + cyclophosphamide

Cumulative probability of obtaining partial or complete remission of the nephrotic syndrome
MP + ChlorambucilMP + Cyclosphosphamide
Cumulative probability of relapse of the nephrotic syndrome after complete or partial remission
C Ponticelli et al., J Am Soc Nephrol 1998
Traitement des GEM primitivesMP + chlorambucil vs MP + cyclophosphamide

D Cattran et al., Kidney Int 2001
Traitement des GEM primitivesCiclosporine + CS vs CS
n = 51 GEM avec syndrome néphrotique26 weeks treatmentAverage Follow-up 78 weeks
Time (weeks)
CyA + CS
CS
No difference in ScrHigh rate of relapse

A Perna et al., Am J Kidney Dis 2004
Traitement des GEM idiopathiquesRémission complète du syndrome néphrotique

A Perna et al., Am J Kidney Dis 2004
Traitement des GEM idiopathiquesRisque de décès ou de progression vers l’IRCT

Traitement des GEM primitivesPlace de l’acide mycophénolique
• Etude sur 16 patients avec SN résistant aux CS, aux IS ou à la CYC :- Traitement par MMF 0,5 à 2 g/j- Réduction de la protéinurie chez 6 patients (37%) après 6 mois de TTT
• Comparaison MMF + corticoïdes vs « Ponticelli modifié » :- Étude prospective randomisée sur 20 patients, traitement 6 mois- Effet similaire des 2 traitements sur la protéinurie (suivi 20 mois)
• Comparaison MMF vs CYC (+ corticoïdes) :- Groupe MMF (n = 32) vs groupe « historique» traité par CYC (n=32)- Durée de suivi courte : 23 (11 - 46) mois- Réduction de la protéinurie chez la majorité des patients- Mais meilleure réponse et moins de rechute dans le groupe CYC
Miller et al., Am J Kidney Dis 2000; Chan et al., Nephrology 2007; Branten et al., Am J Kidney 2007

B Dussol et al., Am J Kidney Dis 1998
Traitement des GEM primitivesPlace de l’acide mycophénolique
38 patients avec GEM et Syndrome néphrotiquePas de différence sur l’ensemble des critères de jugement
Essai prospectif, randomisé et contrôlé, MMF 2g/j vs Traitement symptomatique

Traitement des GEM primitivesPlace du Rituximab
G Remuzzi et al., Lancet 2002P Ruggenenti et al., J Am Soc Nephrol 2003
n = 8 (24 – 75 yrs)CrCl > 20 ml/minUPE > 3.5 g/24 h for > 6 months with ACE or ARAB
Rituximab 375 mg/m2 every weeks x 4No treatment before

Traitement des GEM primitivesPlace du Rituximab
FC Fervenza et al., Kidney Int 2008n = 15Crcl = 85 ± 28 ml/min
Open-label pilot studyRituximab 1 g every 2 weeks (2 infusions) ± 6 months later if CD 20 increase7 patients have been treated before with CS, CS + IS or Cyclo

• Les formes chroniques : Après 6 à 12 mois d’évolutionEn cas de protéinurie importante
• Traitement plus précoce : Syndrome néphrotique très sévère
Progression de l’insuffisance rénale
• En présence de facteurs de mauvais PronosticCréatinémie (> 150 µmol/l)Protéinurie élevée (> 8 g/j)HTALésions histologiques
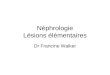
Quelles GEM primitives faut-il traiter ?

Membranous Nephropathy
Exclude or treat secondary causes
Idiopathic MN
Urine protein 3 - 8 g/d
Normal GFR Reduced GFR
Complete or partial remission
Regular follow up
Persistant protinuria > 4 g/d for 6 to 12 months
or
Loss of GFR
Disease-specific therapy
MP + CB or MP + CYP
CS + CyA
Rituximab
Urine protein < 3 g/d
Normal GFR
Urine protein > 8 g/d
Normal or reduced GFR
Proteinuria-reducing therapy
Lipid-lowering therapy
Blood pressure control

• OUI si facteurs de mauvais pronostic
• Au moment du diagnostic si syndrome néphrotique majeur ou si altération de la fonction rénale, après 6 à 12 mois si le syndrome néphrotique persiste sous traitement symptomatique
• Première intention Association CS + CB ou CYP
• Deuxième intention Rituximab ou Ciclo
Faut-il traiter les GEM idiopathiques ?