Embed Size (px)
Citation preview

1
Fidaxomicin
Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist – Infectious Diseases
MetroHealth Medical Center
Disclosure
! I have no conflicts of interest related to this presentation
Learning Objectives
! Describe mechanism of action, pharmacology and spectrum of activity of fidaxomicin
! List pros and cons of fidaxomicin therapy based upon recent clinical trial data and cost
Fidaxomicin
! Macrolide antibacterial
! FDA approved for treatment of Clostridium difficile-Associated Diarrhea
! Bactericidal against C. difficile in vitro, inhibiting RNA synthesis by RNA polymerases
Fidaxomicin (Dificid®) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
Pharmacology
! Minimal systemic absorption
! Distribution confined to GI tract
! Primarily transformed by hydrolysis at the isobutyryl ester to form the active metabolite, OP-1118
! Half-life of 1-3 hours
! Excreted mainly in feces Fidaxomicin (Dificid®) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
Spectrum of Activity
! Predominantly active against species of clostridia, including C. difficile
! More active in vitro (8x) than vancomycin1
! Changes in bacteroides group counts, reflecting changes in GI flora, where not observed with fidaxomicin, while reductions were seen with vancomycin2
1Louie TJ, et al. N Eng J Med 2011;364:422-31. 2Louie TJ, et al. Antimicrob Agents Chemother 2009;53:261-3.

2
Clinical Efficacy
! Pivotal trials – Louie TJ, et al. N Eng J Med 2011;364:422-31. – Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
! Pooled data – Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
! Phase 3, prospective, multicenter, double-blind, randomized, parallel-group, non-inferiority trial
! Site: United States and Canada
! Patients – 16 years of age and older with diagnosis of C. difficile
infection (CDI)
! Exclusions – Life-threatening CDI, toxic megacolon, previous exposure to
fidaxomicin, history of ulcerative colitis or Crohn’s disease, or > 1 occurrence of CDI within 3 months before study.
Louie TJ, et al. N Engl J Med 2011;364:422-31.
! Treatment – Fidaxomicin 200 mg PO Q 12 hours – Vancomycin 125 mg PO Q 6 hours – 10 day course; 28 day follow-up
! Outcomes – Primary: rate of clinical cure (non-inferiority margin -10%) – Secondary: recurrence of CDI during the 4 week period
after the end of the course of therapy and global cure. ! Recurrence
– Reappearance of >3 diarrheal stools per 24 hour period within 4 weeks after cessation of therapy
Methods
Louie TJ, et al. N Engl J Med 2011;364:422-31.
Results
Louie TJ, et al. N Engl J Med 2011;364:422-31.
629 patients enrolled and randomized
MITT Vancomycin
(n=309)
MITT Fidaxomicin
(n=287)
PP Vancomycin
(n=283)
PP Fidaxomicin
(n=265)
Patients (n=596)
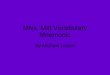
! Modified intent to treat population
– 59.4% inpatient
– 17.1% had previous episode of C. difficile infection
– 38.1% had NAP1/BI/027 strain
Louie TJ, et al. N Engl J Med 2011;364:422-31. Louie TJ, et al. N Engl J Med 2011;364:422-31.

3
NAP1/BI/027 strain
7.8
24.4 25.523.6
0%
5%
10%
15%
20%
25%
30%
NAP1 Non-NAP1
Fidaxomicin
Vancomycin
Rec
urre
nce
p=0.93 p<0.001
Louie TJ, et al. N Engl J Med 2011;364:422-31.
Recurrence Rate Previous C. difficile Episode
Rec
urre
nce
0%
5%
10%
15%
20%
25%
30%
35%
MITT PP
FidaxomicinVancomycin
Louie TJ, et al. N Engl J Med 2011;364:422-31.
21.4
31.2
16.7
31.6 p=0.30
p=0.14
Conclusions ! Rates of clinical cure with fidaxomicin were
noninferior to vancomycin ! Fidaxomicin was associated with a significantly
lower rate of recurrence of C. difficile infection associated with non-NAP1/BI/027 strains
Louie TJ, et al. N Engl J Med 2011;364:422-31.
! Phase 3, prospective, multicenter, double-blind, randomized, parallel-group, non-inferiority trial
! Site: Europe, Canada, United States
! Patients – 16 years of age and older with diagnosis of C. difficile
infection (CDI)
! Exclusions – Life-threatening CDI, toxic megacolon, previous exposure to
fidaxomicin, history of ulcerative colitis or Crohn’s disease, or > 1 occurrence of CDI within 3 months before study.
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
Methods ! Treatment
– Fidaxomicin 200 mg PO Q 12 hours – Vancomycin 125 mg PO Q 6 hours – 10 day course; 28 day follow-up
! Outcomes – Primary: rate of clinical cure (non-inferiority margin -10%) – Secondary: recurrence of CDI during the 4 week period
after the end of the course of therapy and global cure. ! Recurrence
– Reappearance of >3 diarrheal stools per 24 hour period within 4 weeks after cessation of therapy
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
Methods 535 patients enrolled and randomized
MITT Vancomycin
(n=252)
MITT Fidaxomicin
(n=257)
PP Vancomycin
(n=216)
PP Fidaxomicin
(n=235)
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.

4
Patients (n=509)
! Modified intent to treat population
– 68.2% inpatient
– 14.9% had previous episode of C. difficile infection
– 33.2% had NAP1/BI/027 strain
– 24.4% had severe infection
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
0%10%20%30%40%50%60%70%80%90%100%
MITT PP
MITT PP
MITT PP
FidaxomicinVancomycin
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
Clinical cure Recurrence Sustained
Patie
nts
Results
87.8
87
91.7
90
.6
12.7
26.9
12
.8 25
.3
76.6
63
.4 79
.6
65.5
*
* *
*
*=p<0.05
9.2
22.2
27.4
38
0%
5%
10%
15%
20%
25%
30%
35%
40%
NAP1 Non-NAP1
Fidaxomicin
Vancomycin
NAP1/BI/027 strain
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
Rec
urre
nce
p=0.079
p=0.0003
Recurrence Rates Previous C. difficile Episode
Rec
urre
nce
0%
5%
10%
15%
20%
25%
30%
35%
40%
MITT
FidaxomicinVancomycin
18.9
34.4 p=0.145
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
Clinical Cure Concomitant Antibiotics
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.
0%10%20%30%40%50%60%70%80%90%100%
MITT
FidaxomicinVancomycinPa
tient
s
90.2
73.3
p=0.031
Concomitant antibiotics received during treatment and/or follow up period, days 1-40
Conclusions ! Rates of clinical cure with fidaxomicin were
noninferior to vancomycin
! Fidaxomicin was associated with a significantly lower rate of recurrence of C. difficile infection associated with non-NAP1/BI/027 strains
! Exposure to concomitant antibiotics reduced clinical cure rate with vancomycin when compared to fidaxomicin
Cornely OA, et al. Lancet Infect Dis 2012;12:281-9.

5
! Pooled data from Phase 3 Louie TJ, et al. and Cornely OA, et al. trials
! Rates of cure, recurrence, and global cure were determined for subgroups of subjects defined by concomitant antibiotic (CA) use and treatment groups
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
Patients (n=999)
! Concomitant, non CDI, antibiotics were prescribed for 27.5% of subjects at some time during the study (days 1-40)
! 36.7% of subjects received >1 class of CA
! CA use was similar between fidaxomicin and vancomycin groups
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
Effect of CA on Outcomes
! CAs concurrent with CDI treatment was associated with: – Lower cure rate (84.4% vs. 92.6%, p<0.001)
– Extended time to resolution of diarrhea (97 vs. 54 hours, p<0.001)
! CA administration at any time was associated with a lower global cure rate (65.8% vs. 74.7%, p=0.005)
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
Effect of CA on CDI Treatment
70%
75%
80%
85%
90%
95%
CA No CA
FidaxomicinVancomycin
Clin
ical
Cur
e
CA = concomitant, non CDI, antibiotics at any time
90
79.4
92.3 92.8 p=0.04
p=0.80
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
Effect of CA on Recurrence
0%
5%
10%
15%
20%
25%
30%
35%
CA No CA
FidaxomicinVancomycin
Rec
urre
nce
CA = concomitant, non CDI, antibiotics at any time
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.
16.9
29.7
11.9
23.1
p=0.048
P<0.001
Conclusions
! Treatment with CAs compromised initial response to CDI therapy and durability of response.
! Fidaxomicin was significantly more effective than vancomycin in achieving clinical cure in presence of CA and in preventing recurrence regardless of CA use.
Mullane KM, et al. Clin Infect Dis 2011;53:440-7.

6
Warnings & Precautions
! Minimal systemic absorption
! Pregnancy category B
! Unknown if excreted in human milk
! Nausea (11%), vomiting (7%) and abdominal pain (6%) most common adverse effects
Fidaxomicin (Dificid®) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
Drug-Drug Interactions
! Substrate of P-glycoprotein, but no clinically significant drug-drug interactions
Fidaxomicin (Dificid®) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
Dosage & Storage
! Fidaxomicin 200 mg PO BID for 10 days
! May be taken with or without food
! No dosage adjustments for renal or hepatic dysfunction
! Supplied as 200 mg film-coated tablet
! Store at room temperature
Fidaxomicin (Dificid®) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
Cost Comparison Drug Dose AWP
LOT=10 days Fidaxomicin 200 mg PO BID $3360
Metronidazole 500 mg PO TID $21.45
Vancomycin PO 125-250 mg PO QID $625 - $1155* $40 - $80**
*Capsules **Compounded solution with AWP used for IV vancomycin AWP = Average wholesale price LOT = Length of therapy
SHEA/IDSA Guidelines for CDI
Cohen SH, et al. Infect Control Hosp Epidemiol 2010:31:431-55.
Type Data Treatment Initial episode, mild or moderate
WBC ≤15 SCr <1.5x pml
Metronidazole 500 mg PO TID x 10-14 days
A-I
Initial episode, severe
WBC ≥15 SCr ≥1.5x pml
Vancomycin 125 mg PO QID x 10-14 days
B-I
Initial episode, severe, complicated
Hypotension or shock, ileus, megacolon
Vancomycin 500 mg PO/NG QID + Metronidazole 500 mg IV Q 8h +/- Rectal vancomycin
C-III
1st Recurrence Same as initial episode A-II
2nd Recurrence Vancomycin in a tapered and/or pulsed regimen
B-III
SHEA=Society for Healthcare Epidemiology of America, IDSA = Infectious Diseases Society of America, pml = premorbid level
Conclusions
! Similar CDI cure rate compared to vancomycin
! Lower recurrence rate in non-NAP1 CDI compared to vancomycin
! More effective than vancomycin in achieving CDI clinical cure and preventing recurrence in presence of concomitant antibiotics
! Less deleterious effect on host GI flora

7
Place In Therapy ! Not for routine use
! Possible considerations: – Patients with allergies or intolerances to 1st line
agents – Patients on concomitant, non CDI, antibiotics – Guided therapy using C. difficile PCR to detect
non-NAP1 strains
Place in Therapy ! More data needed to determine:
– Who is at highest risk for recurrence ! Age >65 years2, DM1, hypoalbuminemia2, PPIs2,3, CAs4
– Utility in patients with multiple CDI recurrences – Use in severe disease – Cost effectiveness
! 2010 SHEA/IDSA CDI guideline update in progress
1Shakov R, et al. Am J Infect Control 2011;39:194-8., 2Kim JW, et al. World J Gastroenterol 2010;16:357-7., 3Linsky A, et al. Arch Intern Med 2010;170:772-8., 4Garey KW, et al. J Hosp Infect 2008;70:298-304.
Thank you for your time and attention
Question 1
! Fidaxomicin is bactericidal against C. difficile and has over 90% oral bioavailability A. True B. False
! Answer: B
Question 2
! In clinical trials, rates of C. difficile recurrence were significantly higher in patients with the BI/NAP1/027 epidemic strain when treated with fidaxomicin versus treatment with vancomycin A. True B. False
! Answer: B
Question 3 ! Which statement(s) about fidaxomicin is/are
true? A. Metabolized by cytochrome P450 enzymes B. A substrate of the efflux transporter, P-glycoprotein C. Systemic absorption D. Noninferior to vancomycin in the treatment of C. difficile
infection E. A and B F. B and D G. None of the above
! Answer: F