Embed Size (px)
DESCRIPTION
goajgidsjg
Citation preview

c o n s u l t a n t o n c a l l
Profile
DEFINITIONTick-borne diseases are caused by etiologicagents that are transmitted from ticks todogs; such agents include Ehrlichia,Anaplasma, Babesia, Rickettsia, hemotropicMycoplasma, Francisella, Hepatozoon amer-icanum, and Borrelia species.
SYSTEMS• Ticks cause multisystemic disease in
dogs.• Hematologic changes are common and
sometimes typical (e.g., thrombocytopenia)• Multiorgan dysfunction with associated
clinical signs and clinicopathologicchanges are common (Ehrlichia,Anaplasma, Rickettsia, H. americanum).
• Single organ dysfunction can occur(arthropathy in borreliosis).
INCIDENCE/PREVALENCE/GEOGRAPHIC DISTRIBUTION• Incidence and geographic distribution
are dependent on distribution of the tickvector throughout the United States(Table 1).
• Prevalence within a geographic region isusually dependent on season andecology of the tick vector (Table 1).
BREED PREDILECTION• All dogs are susceptible to tick-borne
disease.• Babesia gibsoni has shown an increased
incidence of infection in American
Staffordshire and American pit bullterriers; disease is believed to beacquired during fighting.
• German shepherds and Dobermanpinschers develop more chronic andsevere forms of rickettsial diseases.
RISK FACTORS• Major factor is exposure to ticks (young
hunting dogs with extensive outdooractivity).
• Exposure depends on ecology of the tick,including the season during which it ismost prevalent, infection rate of thedisease in the tick species, attachmentrequirements of tick to transmitdisease—American dog tick requiresattachment > 5 hours to transmit R.rickettsii; ticks of the Ixodes speciesrequire 24 hours of attachment totransmit Borrelia burgdorferi;Amblyomma maculatum requiresingestion to transmit H. americanum.
• Blood transfusion—receiving blood fromunscreened donors from enzootic regionsis a high risk factor.
• Splenectomy predisposes dogs to clinicaldisease with M. hemocanis; a milderform of E. canis infection also occurs insplenectomized dogs.
• Concomitant infection with tick-borne orother diseases or a weakened immunesystem (from age, immunosuppressivedrug therapy, or congenital defects)predisposes to more severe disease.
PATHOPHYSIOLOGY• Depends on the disease.
- Rickettsials—Vasculitis and immunemechanisms lead to endothelialdamage in multiple organs,thrombocytopenia, hyperglobulinemia,and eventual bone marrow depletionwith pancytopenia. Different organismsmanifest with different organinvolvement—for example, E. ewingiimainly centers on joints and the centralnervous system, A. platys mainlyaffects platelets, R. rickettsii mainlyaffects endothelial cells of smallarteries and venules. Incubation periodis 8 to 20 days.
- Babesia—Intravascular andextravascular hemolysis with anemia.Transplacental transmission occurs.
- Mycoplasma—Splenectomy,immunosuppression from concomitantinfectious diseases, or drug therapy canprecipitate anemia in which immunemechanisms are also involved.Transplacental transmission does notoccur.
- Francisella—Macrophages becomeinfected and spread the organism tolungs, spleen, liver, lymph nodes, andskin where microabscess formationoccurs.
- Borrelia—Few infected dogs developclinical signs; immune mechanismsagainst borrelial proteins and cytokineresponses are implicated in pathologicconditions of the joint. Transplacentaltransmission rare but can occur.
- Hepatozoon—Infected ticks areingested; sporozoites enter blood and
c o n t i n u e s
Practical Guide toTick-Borne DiseaseStephen C. Barr, BVSc, MVS, PhD, Diplomate ACVIM (Small Animal), Cornell University
P A R A S I T O L O G Y
consultant on ca l l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . N AV C c l in ic ian’s br ief. . . .may.2006. . . . .7

c o n s u l t a n t o n c a l l C O N T I N U E D
8. . .may.2006. . . . . N AV C c l in ic ian’s br ief . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . consultant on ca l l
Ticks of Pathogenic Importance in the United States
Tick
Rhipicephalus sanguineus(brown dog tick)
Dermacentor variabilis(American dog tick)
Dermacentor andersoni(wood tick)
Amblyomma americanum(Lone Star tick)
Amblyomma maculatum(Gulf Coast tick)
Ixodes scapularis(eastern black-legged tick)
Ixodes pacificus(western black-legged tick)
Etiologic Agent
B. canis vogeli, B. gibsoni,† E.canis, Mycoplasma hemocanis,E. ewingii,† A. platys†
E. canis, E. chaffeensis,Rickettsia rickettsii, Francisellatularensis, E. ewingii†
Rickettsia rickettsii, Francisellatularensis
E. ewingii, E. chaffeensis,Francisella tularensis
Hepatozoon americanum
A. phagocytophilum, Borreliaburgdorferi, Babesia species†
Geographic Area
Widely distributed throughoutUnited States
East from ND, SD, NE, KS, OK,and mid TX; coastal CA, south-western OR, southern WA, ID
Northwestern states (WY, ID, UT,NV, western MT and CO, easternWA and OR)
Southern, southeastern, andAtlantic coastal states; movingnorthward (OK, KS, KY)
Mainly southern states of TX,LA, MS, AL, GA, and FL butexpanding north into OK, KS,and KY
Most cases occur in NewEngland and Northeastern andAtlantic states; fewer casesoccur in Midwest (WI, MI, MN,IL, MS, IA) and on West Coast
Season
Throughout year but especiallyspring
Spring through early fall
Spring through early summer
Spring to late fall
Summer through early fall
Nymphs feed during the spring;adults in early fall
Table 1. Geographic and Seasonal Distribution of Tick Vectors in the United States*
*A = Anaplasma; B = Babesia; E = Ehrlichia †Suspected
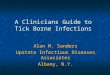
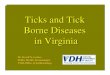
Unengorged female ofAmblyomma americanum
(bar = 1 mm)
Unengorged female ofAmblyomma maculatum
(bar = 2 mm)
Unengorged female ofDermacentor andersoni
(bar = 1 mm)
Unengorged female ofDermacentor variabilis
(bar = 1 mm)
Unengorged female of Ixodes scapularis
(bar = 1 mm)

lymphatics viastomach mucosathen targetlymphatic tissue,bone marrow, orother organs (liver,lungs, kidneys),causing hepatitis,pneumonitis, andglomerulonephritis.Transplacentaltransmission occurs.
SIGNS• There is no one clinical sign typical of
tick-borne diseases (Table 2).• Travel history should be carefully
considered (Table 1).• Many infections, such as those caused by
Borrelia, Babesia, Rickettsia, Anaplasma,and Mycoplasma, are asymptomatic, butmay manifest with clinical signs if theyoccur concomitantly with otherinfections or immunosuppression.
• Clinical signs usually indicate multi-systemic involvement, which shouldalways prompt the clinician to place tick-borne diseases high on the differentialdiagnosis list.
• Some tick-borne diseases do show morespecific signs, such as severe debilitation,intermittent antibiotic–nonresponsivefever, weight loss, muscle atrophy, andhyperesthesia; mucopurulent oculardischarge occurs in most dogs infectedwith H. americanum.
Diagnosis
• Identification of a tick removed from apatient with specific clinical signs canprovide direction in diagnosing thespecific pathogen (Table 1, Figures).
• Clinical signs should be correlated withinthe geographic area in which the patientresides or has traveled. For example, adog from New Jersey that presents withjoint pain (polyarthritis) is likely to have
borreliosis; a dog from Oklahoma withjoint pain probably has E. ewingiiinfection.
• Important and common clinical signs often associated with tick-borne diseasesinclude fever, chronic weight loss, pe-techiae/ecchymoses, and lymphadeno-pathy.
• Clinicopathologic findings (Table 2) inconjunction with clinical signs shouldprompt a more specific search (serologicevaluation) for certain pathogens.
• Important and common clinicopathologicfindings that should trigger the clinicianto think of tick-borne diseases includethrombocytopenia (rickettsial diseases,Babesia, Francisella), regenerativeanemia (Babesia, Mycoplasma),hyperglobulinemia (Ehrlichia, H.americanum), and profound leukocytosis(H. americanum).
• Many tick-borne diseases cause visibleintracellular inclusions that, althoughrare for some agents, are definitivelydiagnostic if found:- Ehrlichia—Morulae within leukocytes
(E. canis, E. chaffeensis, E. ewingii, A.phagocytophilum) or platelets (A.platys).
- Babesia—Large, often in doubles,piriform organisms (B. canis) or smaller,single organisms (B. gibsoni) within redblood cells.
- Mycoplasma—Chains of organisms onred blood cell surfaces.
- H. americanum—Gamonts withinneutrophils or monocytes.
• Tick-borne diseases can occurconcomitantly, so use serologic testingand other pathogen-specific assays tosearch widely; the finding of one diseaseshould prompt a search for otherstransmitted by the same tick species orothers that are enzootic to a specificgeographic area.
• Results of serologic tests need to beassessed in the context of prevalence,which affects the predictive value of atest.
• Cross-reaction with other pathogens isoften common, especially within therickettsial group (Table 3).
Treatment
• Most dogs can be treated as outpatients.• The sooner treatment is initiated, the
more favorable will be the prognosis.• Dogs with chronic tick-borne diseases
are rarely curable.• Supportive therapy with fluids for
dehydration (rickettsial diseases,Francisella), and blood transfusion(Babesia, Mycoplasma) may be indicatedbut will not appreciably increase plateletor leukocyte counts.
Medications
• Although there is a range of drugs forrickettsial agents, doxycycline is the mostcommonly used agent (Tx at a Glance).
• Imidocarb may be a first choice forrickettsial diseases as well at Babesiacanis if a definitive diagnosis has not yetbeen made.
• Whether dogs that are serologicallypositive for Borrelia but clinically normalshould be treated with doxycycline orother antibiotics is controversial.Because fewer than 5% of Borrelia-positive dogs ever develop clinical signsand treatment does not guaranteeremoval of the organism, there seems tobe little rationale for antibiotic treatmentin these dogs at this time.
• Early use of glucocorticoids in diseaseswith an immune-mediated component(rickettsial diseases, Babesia, Myco-plasma) may improve the outcome aslong as they are used in conjunctionwith appropriate antibiotic therapy.
• Glucocorticoids used for immuno-suppression in suspected cases ofimmune-mediated thrombocytopenia will
c o n t i n u e s
consultant on ca l l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . N AV C c l in ic ian’s br ief. . . .may.2006. . . . .9
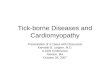
Unengorged female of Rhipicephalus sanguineus
(bar = 2 mm)

10. . .may.2006. . . . . N AV C c l in ic ian’s br ief . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . consultant on ca l l
Etiologic Agent
Ehrlichia ewingii
Ehrlichia canis
Ehrlichia chaffeensis
Anaplasma phagocytophilum
Babesia canis vogeli
Anaplasma platys
Babesia gibsoni
Mycoplasma hemocanis
Rickettsia rickettsii
Francisella tularensis
Hepatozoon americanum
Borrelia burgdorferi
Table 2. Clinical Signs Associated with Tick-Borne Diseases*
Main Clinical/Clinicopathologic Findings
Lameness (polyarthritis) Fever, neurologic abnormalities (ataxia, paresis, conscious proprioceptive deficits, anisocoria, vestibular dysfunction)Mild thrombocytopenia and anemia Neutrophils in joint fluid and CSF
Fever, anorexia, weight lossHemorrhagic diathesis, CNS signs, lymphadenopathyThrombocytopenia, leukopenia, anemiaHyperglobulinemia, proteinuria
Anterior uveitis, lymphadenopathy, vomiting, epistaxis, erythema multiformeThrombocytopenia, lymphocytic pleocytosis
Fever, anorexiaSplenomegaly, hepatomegaly, CNS signsLameness (polyarthritis)Thrombocytopenia, mild Ô serum albumin, Õ ALP, neutrophils in joint fluid and CSF
Often asymptomaticMild fever, uveitis, petechiaeThrombocytopenia
Often asymptomaticYoung animals: fever, lethargy, anemia, icterus, splenomegaly, lymphadenopathy, pigmenturiaAnemia (regenerative), thrombocytopenia, Õ bilirubinemia (if RBC lysis rapid), large piroplasms in RBC
Hemolytic regenerative anemia, weight loss, debilitationChronic form more common—lethargy, mild fever, anemia, splenomegaly, hepatomegaly, lymphadenopathyThrombocytopenia (variable), small single annular bodies in RBC
Asymptomatic (nonsplenectomized dogs)Splenectomized dogs—listless but normal appetites, pale mucous membranes, regenerative anemia, chains of
organisms on RBC surface
Fever, lethargy, weight loss, vomiting, diarrhea Edema/hyperemia: lips, scrotum, pinnae, prepuce, cutaneous necrosisPetechial hemorrhage: ocular, oral, genital; mucosal (epistaxis rarely)Ocular signs: scleral congestion, conjunctivitis, anterior uveitisLymphadenopathy, joint swelling, arthralgiaCNS signs: hyperesthesia, tetraparesis, ataxia, seizuresThrombocytopenia, leukocytosis + left shift, Ô serum albumin, Õ ALP, Õ coagulation times,
neutrophils in joint fluid and CSF
Anorexia, listlessness, low-grade feverSubcutaneous abscessesOcular signs: uveitis, conjunctivitisSudden death Thrombocytopenia, leukocytosis + left shift, Õ ALT, Õ serum bilirubin
Fever, anorexia, diarrhea, paraparesis, ataxiaBloody diarrhea (dogs in Tx)Generalized muscle atrophy, cervical/trunk rigidity (periosteal pain), chronic weight loss, hyperesthesia, stiffness,
neck guarding (radiographically apparent periosteal bone proliferation)Ocular: low tear production, focal retinal scarring, hyperpigmentation, papilledema, uveitisProlonged course: periods of remission interspersed with fever and painProfound leukocytosis (sometimes up to 200,000 cells/µl blood) + left shift; sometimes eosinophilia (up to 20%);
mild normocytic, normochromic regenerative anemiaThrombocytosisÔ serum albumin, Õ ALP, Õ globulin, Ô glucose (artifact due to high neutrophil counts), Õ urine protein-creatine
ratio (glomerulopathy)
Recurrent acute arthritis with lameness in 1 or more joints (3–4 days; responds well to antibiotic treatment)Fever, anorexia, depression, lymphadenopathy (superficial cervical and/or popliteal), complete heart block—rareCNS signs—rareGlomerulonephritis progressing to fatal renal failureJoint fluid: Õ neutrophils in multiple jointsRenal failure: uremia, proteinuria, Õ cholesterol and phosphate levels, Ô albumin
* ALP = alkaline phosphataseALT = alanine transaminaseCNS = central nervous systemCSF = cerebrospinal fluid RBC = red blood cellTx = treatment

consultant on ca l l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . N AV C c l in ic ian’s br ief. . . .may.2006. . . . .11
c o n s u l t a n t o n c a l l C O N T I N U E D
not negatively affect concurrenttreatment of rickettsial agents.
Follow-up
• Response to therapy during acute stagesof disease caused by rickettsial agents,Babesia, Mycoplasma, and Borreliashould occur within 24 to 48 hours.
• Most follow-up should consist ofphysical examination, CBC, biochemistrypanel (globulins, liver enzymes, renal
function), and urinalysis rather thanserologic testing.
• Platelet counts should return to normalwithin 5 to 8 days. If not, seek anothercause.
• Repeat platelet counts at the end oftherapy and again in 6 months.
• Serologic testing and blood polymerasechain reaction are not effective methodsof assessing the efficacy of therapy withehrlichial diseases; reinfection is possible.
• Long-term immunity does develop aftersuccessful treatment of R. rickettsii.
• Therapy is seldom effective in removingthe organism in most cases of tick-bornedisease, so lifelong monitoring for returnof clinical signs is essential. The excep-tion is that a single dose of imidocarb isbelieved to eliminate the carrier state ofB. canis.
PREVENTION• Vaccines are only available for Borrelia
and should only be used in enzootic areas.• Whole-cell vaccines and recombinant
c o n t i n u e s
Etiologic Agent
Ehrlichia ewingii
Ehrlichia canis
Ehrlichia chaffeensis
Anaplasma phagocytophilum
Anaplasma platys
Babesia canis vogeli
Babesia gibsoni
Mycoplasma hemocanis
Rickettsia rickettsii
Francisella tularensis
Hepatozoon americanum
Borrelia burgdorferi
Table 3. Preferred Serologic Tests for Tick-Borne Diseases*
Serologic Diagnostic Technique of Choice
Specific serology unavailable; IFA using other rickettsial antigens (e.g., E. canis, E. chaffeensis) that cross-react with E. ewingii
Western blot (rarely clinically available)—differentiates between E. canis and E. ewingii
Specific IFA; cross-reaction with E. chaffeensis, E. ewingii (not pathogenic Anaplasma species);titers reliable 3 wk postinfection (reliable in clinically affected dogs)
SNAP-3Dx (IDEXX; an in-house ELISA antibody test)—excellent specificity and good sensitivity
Specific IFA; cross-reaction with E. canis, E. ewingii (not pathogenic Anaplasma spp.); titers reliable 3 wk postinfection (reliable in clinically affected dogs)
Specific IFA; very low cross-reaction with E. canis, E. ewingii, and A. platys; titers reliable 3 wk postinfection (reliable in clinically affected dogs)
Specific IFA; very low cross-reaction with A. phagocytophilum; titers reliable 3 wk postinfection (reliable in clinically affected dogs)
Polymerase chain reaction
IFA; cross-reaction with other Babesia species Microscopic exam of stained (modified Wright’s stain) blood smear; capillary blood will Õ sensitivity
IFA; cross-reaction with other Babesia species Microscopic examination of blood smear stained with modified Wright’s stain; capillary blood may Õ sensitivity
Microscopic examination of blood smear stained with modified Wright’s stain; capillary blood may Õ sensitivityOrganisms usually present in clinically affected dogs
Micro-IFA most commonly used; may take 2–3 wk for IgG titers to increase; if first test negative in highly suspectcase, repeat in 3 wk
Microscopic agglutinationTiters of 1:140 to 1:160 = recent infection
Muscle biopsy (most definitive method) Gamonts in neutrophils or monocytes in blood smears (rare)ELISA is 93% as sensitive and 96% as specific as muscle biopsy
SNAP-3Dx (in house) or ELISA followed by Western blot to differentiate infected vsvaccinated
*ELISA = enzyme-linkedimmunosorbent assay IFA = indirect fluorescent anti-body assay

12. . .may.2006. . . . . N AV C c l in ic ian’s br ief . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . consultant on ca l l
c o n s u l t a n t o n c a l l C O N T I N U E D
OspA vaccines induce antiOspAantibodies to develop in the host; theseantibodies are passed to the tick whilefeeding and incapacitate the Borreliaorganisms within the tick, therebypreventing transmission.
• Vaccination of an already infected dog isnot indicated.
• Tick control is essential.• Effective products include fipronil
(Frontline—Merial), imidocloprid/permethrin combination (K9 Advantix—Bayer), and amitraz (Preventic—Virbac).Use of spot-on or oral flea controlproducts combined with pyrethrum-based collars is also effective.
• Daily body checks for attached ticks islikely to be effective in preventinginfection with tick-borne diseases,although it requires considerable effortfor the owner, who must wear glovesand use tweezers to remove the ticks.Ticks need to be disposed of carefully
at a glance
Etiologic Agent Treatment of Choice
Ehrlichia ewingii, E. canis, Doxycycline: 5 mg/kg PO Q 12 H × 28 daysE. chaffeensis, Anaplasma platys, A. phagocytophilum, Mycoplasma hemocanis
Rickettsia rickettsii Doxycycline: 10 mg/kg PO Q 12 H × 14 days
Borrelia burgdorferi Doxycycline: 10 mg/kg PO Q 12 H × 28 days
Babesia canis vogeli Imidocarb dipropionate: 6.6 mg/kg IM once; then repeat × 14 days
Babesia gibsoni Atovaquone: 13.3 mg/kg PO Q 8 H together withAzithromycin: 10 mg/kg PO Q 24 H × 10 days
Francisella tularensis Gentamicin: 5 mg/kg SC Q 24 H together withEnrofloxacin: 5 mg/kg PO Q 24 H × 10 days
Hepatozoon americanum TMS: 15 mg/kg PO Q 12 H together withClindamycin: 10 mg/kg PO Q 8 H and Pyrimethamine: 0.25 mg/kg PO Q 12 H × 2 weeks Maintain remission with decoquinate: 15 mg/kg PO Q 12 H for life
*TMS = trimethoprim-sulfadiazine
(incinerated) to prevent dogs fromeating them.
• Some have advocated the use oftetracycline (6.6 mg/kg, PO Q 24 H) aschemoprophylaxis against the rickettsialagents, Borrelia, and Mycoplasma, fordogs entering enzootic areas, althoughthis approach may not be practical.
• Screening of blood donors or blood usedfor transfusion and limiting fightingbehavior in pit bull terriers are important.
PROGNOSIS/FUTURE CONSIDERATIONS• It is often difficult to separate
recrudescence from reinfection in mosttick-borne diseases.
• Response to therapy for cases of defini-tively diagnosed rickettsial agents can beexpected to be approximately 70%.
• All Borrelia cases showing clinical signsof polyarthropathy should improvedramatically after 3 days of antibiotics—
failure to do so should prompt furtherinvestigation of the joints for othercauses, especially immune-mediated.
• Dogs treated for babesiosis clinicallyimprove within 24 hours but few drugseliminate the parasites. However, becauseof the balance between low parasitenumbers and host immune response,hemolytic crises during recurring infectionare rare.
• The long-term prognosis for dogs infectedwith H. americanum is good (Tx at aGlance). Relapses do occur, but a 2-yearsurvival rate of 84% can be expected.Some dogs live for more than 5 yearsafter diagnosis. Death usually results fromglomerulonephritis and amyloidosis.
• Few reports of diagnosed Francisella orsurvival of Francisella have beendocumented in dogs. ■
See Aids & Resources, back page, forreferences, contacts, and appendices.