Embed Size (px)
DESCRIPTION
Final Health Ministry Annual Report 2008-09
Citation preview
ANNUANNUANNUANNUANNUAL REPORTAL REPORTAL REPORTAL REPORTAL REPORT
2008-092008-092008-092008-092008-09
MMMMMinistry of Health & Family Winistry of Health & Family Winistry of Health & Family Winistry of Health & Family Winistry of Health & Family WelfareelfareelfareelfareelfareGovernment of IndiaGovernment of IndiaGovernment of IndiaGovernment of IndiaGovernment of India
New DelhiNew DelhiNew DelhiNew DelhiNew Delhi

CONTENTSCONTENTSCONTENTSCONTENTSCONTENTS
PPPPPARTARTARTARTART-I D-I D-I D-I D-I DEPEPEPEPEPARTMENTARTMENTARTMENTARTMENTARTMENT OFOFOFOFOF H H H H HEALEALEALEALEALTHTHTHTHTH & F & F & F & F & FAMILAMILAMILAMILAMILYYYYY W W W W WELFELFELFELFELFAREAREAREAREARE
Chapter Page No.
Introduction 1
1. Organization & Infrastructure 5
2. NRHM, Health & Population Policies 23
3. Funding for the Programme 51
4. Maternal Health Programme 61
5. Child Health Programme 69
6. National Programmes under NRHM 83
7. Information, Education and Communication 117
8. Partnership With Non-Government Organisations 123
9. Family Planning 127
10. Training Programme 137
11. Research 149
12. Other National Health Programmes 151
13. Medical Relief and Supplies 165
14. Quality Control In Food & Drugs Sector, Medical Stores 193
15. Medical Education, Training & Research 203
16. Facilities For Scheduled Castes and Scheduled Tribes 315
17. Use of Hindi in Official Work 319
18. International Co-Operation for Health & Family Welfare 321
19. Activities In North East Region 327
PPPPPARTARTARTARTART-II D-II D-II D-II D-II DEPEPEPEPEPARTMENTARTMENTARTMENTARTMENTARTMENT OFOFOFOFOF A A A A AYURVEDYURVEDYURVEDYURVEDYURVEDAAAAA, Y, Y, Y, Y, YOGAOGAOGAOGAOGA-N-N-N-N-NAAAAATUROPTUROPTUROPTUROPTUROPAAAAATHYTHYTHYTHYTHY, U, U, U, U, UNANINANINANINANINANI, S, S, S, S, SIDHAIDHAIDHAIDHAIDHA & & & & &HHHHHOMOEOPOMOEOPOMOEOPOMOEOPOMOEOPAAAAATHYTHYTHYTHYTHY (A (A (A (A (AYUSH)YUSH)YUSH)YUSH)YUSH)
Overview 349
1. Organization 353
2. National Policy 355
3. Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH) 359
4. Education 363
5. Research and Development 385
6. Increasing the Availability of Medicinal Plants for Raw Material 403
7. Standardization and Quality Control of ASU&H Drugs 411
8. AYUSH Pharmaceutical Industry 417
9. Information Education and Communication 419
10. International Cooperation 427
11. Mainstreaming of AYUSH in National Health Care 433
12. Information Technology 435
13. Gender Issues 437
PPPPPARTARTARTARTART-III D-III D-III D-III D-III DEPEPEPEPEPARTMENTARTMENTARTMENTARTMENTARTMENT OFOFOFOFOF H H H H HEALEALEALEALEALTHTHTHTHTH R R R R RESEARCHESEARCHESEARCHESEARCHESEARCH 439
PPPPPARTARTARTARTART-IV D-IV D-IV D-IV D-IV DEPEPEPEPEPARTMENTARTMENTARTMENTARTMENTARTMENT OFOFOFOFOF AIDS C AIDS C AIDS C AIDS C AIDS CONTROLONTROLONTROLONTROLONTROL 449
AAAAANNEXURENNEXURENNEXURENNEXURENNEXURE P P P P PARTARTARTARTART-I M-I M-I M-I M-I MINISTRYINISTRYINISTRYINISTRYINISTRY OFOFOFOFOF H H H H HEALEALEALEALEALTHTHTHTHTH & F & F & F & F & FAMILAMILAMILAMILAMILYYYYY W W W W WELFELFELFELFELFAREAREAREAREARE
� Organisation Chart of Department of Health and Family Welfare 486
� Organisation Chart of DGHS 498
� Organisation Chart of Department AYUSH 500
� Organisation Chart of Department of Health Research 502
� Organisation Chart of Department of AIDS Control 503
AAAAANNEXURESNNEXURESNNEXURESNNEXURESNNEXURES P P P P PARTARTARTARTART-II D-II D-II D-II D-II DEPEPEPEPEPARTMENTARTMENTARTMENTARTMENTARTMENT OFOFOFOFOF A A A A AYUSHYUSHYUSHYUSHYUSH
Annexure-I List of publications made by various organization under the 507Department of AYUSH during the last one year / distributed by AYUSH.
� Central Council for Research in Yoga and Naturopathy
� Central Council for Research in Homoeopathy, New Delhi
� Morarji Desai National Institute of Yoga
� Central Council for Research in Unani Medicine
Annexure-II Department of AYUSH Eleventh Plan Outlay 518
Annexure-III Scheme-wise Tenth Plan Outlay and Expenditure 519
Annexure-IV Summary of Infrastructure Facilities under AYUSH 521
Annexure-V State-wise Number of AYUSH Registered Practitioners as on 1.1.2008 522
Annexure-VI State-wise number of AYUSH Registered Practitioners per 523Lakh Population as on 1.1.2008
Annexure-VII State-wise/System-wise Number of Hospitals with their 524Bed Strength under AYUSH as on 1.4.2008
Annexure-VIII State-wise/System-wise number of 525Dispensaries under AYUSH as on 1.4.2008
Part - I
Department ofHealth & Family Welfare


1
ANNUAL REPORT 2008-09
India has made substantial progress in healthdeterminants over the past decades. The criticalindicators of health, including Infant Mortality Rate,Maternal Mortality ratio, Disease prevalence,morbidity as well as mortality rates have shownconsistent decline over the years. Theseachievements are the cumulative result of severalinterconnected changes. The improved coverageand efficiency of Public Health Delivery System aswell as expanding private health sector havecontributed in equal measures to ameliorating thesufferings associated with adverse health events.The over all economic upturn as well as improvementin collateral determinants of health has assistedthe country to achieve critical milestones likeelimination of Leprosy and reduction in the burdenof Tuberculosis.
India is in the midst of an epidemiological anddemographic transition largely on account of thesignificant progress in improving life expectancy atbirth, in reducing mortality due to Malaria, as well asin reducing infant and maternal mortality over thelast few decades. This adds to the already dauntingchallenge of reaching quality health care to everyhousehold in the country.
The National Rural Health Mission (NRHM) is amajor flag ship programme of the Ministry. Over thelast three years of implementation, the NHRM hasbrought about comprehensive rejuvenation of PublicHealth System in the country. This rejuvenation hasaddressed the fundamental issues encumbering thehealth system. The Central Government hassubstantially increased the financial support to thehealth sector. The funds are being utilised throughthe process of decentralised planning andimplementation to ensure the ownership of respectivestate Governments in the reform process. At the sametime, the community based monitoring and proactiveroles to Village Health & Sanitation Committees andRogi Kalyan Samitis has restored the confidence of
IntroductionIntroductionIntroductionIntroductionIntroduction
the community in the Public Health Systems. Throughthe process of decentralised Integrated Planning andinter-sectoral convergence, the states are able toaddress the expectations of the citizens and lead thecountry towards a healthier future.
In partnership with States and through state ledinnovations, NRHM is rapidly expanding accessible,affordable and accountable quality care to everyhousehold in the country. More than 6.28 lakh ASHAsand Link Workers are connecting households tohealth facilities. States across the country arereporting significantly higher utilization of outpatientservices, diagnostic facilities, institutional deliveriesand inpatient care. Large scale demand side financingunder the Janani Suraksha Yojana has brought poorhouseholds to public sector health facilities on a scalenever witnessed before. More than 2.97 lakh Villageand Sanitation Committees have been madefunctional to bring about community ownership andplanning in health sector. Rogi Kalyan Samitis set atvarious levels have been made the custodians ofthe untied funds and annual maintenance grant forhealth facilities. Untied funds at various levels haveintroduced functional flexibility in proper upkeep ofhealth institutions ensuring the availability of thequality services to the citizens. Detailed integratedDistrict Health Action Plans have been prepared inover 541 districts, and convergence of key healthand health related initiatives is being ensured throughthe District Health Missions and the State HealthMissions.
Quarterly reporting on flagship programmes as“Bharat Nirman Quarterly Reports”
The Ministry of Health & Family Welfare has launcheda web based Health MIS (HMIS) portal in March 2008to facilitate data capturing at the District level. Theportal captures physical and financial performanceunder the NRHM from the States. The Ministry hopesto fully operationalise the HMIS by the end of June2009.

2
ANNUAL REPORT 2008-09
Reproductive and Child Health Programme is amajor component of NRHM and aims at reductionof Infant Mortality Rate to 30/1000, Maternal MortalityRatio to 100/100000 live births and Total Fertility Rateto 2.1. These targets are to be achieved by 2010.Against these goals, IMR of 55/1000 live births, (SRS2007) MMR of 254/100000 live births (SRS 2006)and Total Fertility Rate of 2.8 (SRS 2006) have beenachieved.
Rapid urbanization has led to rapid increase in thenumber of urban poor, majority of whom live in slums.In order to improve the health status of the urbanpoor particularly the slum dwellers and otherdisadvantaged sections by facilitating equitableaccess to quality health care with the activeinvolvement of the Urban Local Bodies (ULBs) incities with population of one lakh and above and StateCapitals, the National Urban Health Mission(NUHM) has been planned. The NUHM would becovering 21.07 crore urban population with a specialfocus on 6.25 crore urban poor living in slums andbeyond, spread over 430 cities. The proposedfinancial outlay is Rs.6207.84 crore in the XIth Plan.
The Integrated Disease Surveillance Project(IDSP) launched in 2004 with the objective to detectand respond early to warning signals of diseaseoutbreaks, has established an IT network in 317 ofthe 400 sites with the help of NIC and ISROconnecting all States, District HQ and Governmentmedical colleges and certain national institutionsinvolved in disease surveillance and response. Inaddition, a 24x7 Call Centre set up in February 2008receives disease alerts from all over the country ontoll free number 1075 and a total of 34,459 calls havebeen received till March 2009.
Prevention and control of vector borne diseasessuch as Malaria, Filaria, Kala-azar, JapaneseEncephalitis, Dengue & Chikungunya has a directlink with economic & social development of thecommunity. The malaria incidence in the countrywas brought down from 6.4 million cases in 1976 to1.86 million cases in 2003. Since then it has beenkept below 2 million cases. However, malaria stillcontinues to be a major public health problem in manytribal areas as well as hilly and forested areas which
require focused attention for the country. Kala-azar& Lymphatic Filariasis have been targeted forelimination by 2010 & 2015 respectively and the goalof elimination must be achieved to make our countryfree from these diseases affecting the health of largepopulation.
HIV situation in the country is assessed andmonitored through regular annual sentinelsurveillance mechanism established since 1992. Thethird phase of National AIDS Control Programme(NACP) was launched in June 2007. The overall goalof NACP-III is to halt and reverse the epidemic inIndia over the next 5 years. Considering that morethan 99% of the population in the country is freefrom infection, NACP-III will place the highest priorityon preventive efforts while, at the same time, seekingto integrate prevention with care, support andtreatment. Building up of a strong StrategicInformation Management System and strengtheningthe Surveillance and Research components toprovide evidence for planning and implementationwill be given major thrust during NACP-III. NationalAIDS Control Programme is currently focusing on up-scaling of services to improve coverage and toimprove the quality of services provided.
Tuberculosis is a major public health problem inIndia. About 3.25 lakh persons are estimated to dieof TB every year in the country. The Revised NationalTB Control Programme (RNTCP), using DirectlyObserved Treatment Shortcourse (DOTS) strategy,with the objective of curing at least 85% of new sputumpatients put on treatment and detecting at least 70%of such patients is being implemented in the countryin a phased manner from 1997 and the entire countryhas been covered by March 2006.
As part of the continued efforts to achieve leprosyelimination in six States/UTs viz, Bihar, Chattisgarh,West Bengal, Jharkhand, Chandigarh and D&NHaveli as well as to provide support for DisabilityPrevention and Medical Rehabilitation for theseStates, and 29 States/UTs which have achievedleprosy elimination, support is being provided forReconstruction Surgery (RCS).
Cancer is a major public health concern in India andhas become one of the ten leading causes of death

3
ANNUAL REPORT 2008-09
in the country. With a total outlay of Rs. 2400.00 crore,the National Cancer Control Programme (NCCP) isproposed to be modified to meet the gap in availablecancer care facilities and trained manpower in thecountry. The Government has set up the " HealthMinister's Cancer Patient Fund "(CPF) to providefinancial assistance to Below Poverty Line (BPL)cancer patients for treatment of this chronic disease,which is highly expensive and prolonged.
Tobacco is the single most preventable cause of deathin the country. The Government of India is taking stepsto ensure effective implementation of the Cigarettesand other Tobacco Products (Prohibition ofAdvertisement and Regulation of Trade and Commerce,Production, Supply and Distribution) Act, 2003. TheMinistry of Health & FW has launched the NationalTobacco Control Programme in the 11th Five Year Planto build capacity of the States for the effectiveimplementation of the Tobacco Control Act and theFramework Convention on Tobacco Control (FCTC).As per Tobacco Control Legislation, 2003, the Rulesregarding pictorial warnings of Health Hazards ofSmoking has come into effect on 31st May, 2009.
To address major causes of mortality and morbidityin the country in a focused manner, the Governmenthas launched a number of new initiatives. Thepilot programme under the National Programmeon Prevention and Control of Diabetes,Cardiovascular diseases and Stroke last yearhas been expanded to 10 States and the Programmeaims at using health promotion and health education,advocacy, early detection of persons with high riskfactors (at the risk of developing disease) throughopportunistic screening and strengthening of healthsystems at all levels to tackle Non-CommunicableDiseases and improvement of quality of care. TheNational Programme on Prevention and Controlof Deafness (NPPCD) is addressing the secondmost cause of disease morbidity - hearing impairment/deafness - in the country and covers nearly 80districts in 2008-09.
Occurrence of cases of H1N1 infection (Swineflu) in the country
Recently, human cases of Swine flu (H1N1 virus
infection) have been reported in several countries,including India. In order to check the entry and spreadof this virus in our country, this Ministry has taken anumber of measures on war footing e.g. streng-thening of the laboratory facilities and casemanagement facilities, health screening ofpassengers coming from the affected countries,contact tracing and enhanced surveillance,stockpiling of essential drugs etc.
The Transplantation of Human Organs Act wasenacted in 1994 to curb commercial transactions inhuman organs. In the light of experience gatheredover the last decades, it is now proposed to amendthe law to facilitate genuine cases of organ donationand to prescribe harsh punishment for illegaltransactions. A programme to promote organdonation will also be launched shortly.
With the objectives of creating and expanding healthmanpower in old age care, promoting relevantresearch to provide for evidence based active andhealthy ageing and integrated, comprehensive andquality health care to older people at all levels - ininstitutions and community-the National Programmefor Healthcare of Elderly is proposed to be launchedin 2009.
In order to reduce the gaps in availability of tertiaryhealthcare across states, the Pradhan MantriSwasthya Suraksha Yojana (PMSSY) Phase I hasbeen launched. This programme envisages settingup of 6 new AIIMS like Institutions in the States ofBihar, Chattisgarh, Madhrya Pradesh, Orissa,Rajasthan and Uttranchal and upgradation of 13existing Government medical colleges. GOI has alsoapproved Phase II of PMSSY project to set up 2 AIIMSlike institutions one each in Uttar Pradesh and WestBengal and upgrade 6 existing Medical CollegeInstitutions.
Universal Immunization Programme was startedin 1985-86 to cover six vaccine preventable diseasesin phased manner covering all the districts in thecountry by 1989-90. Since 2006, two new vaccinesviz. Japanese Encephalitis (JE) and Hepatitis B havebeen introduced in select district and States. Thereis a plan to introduce a combination (pentavalent)
4
ANNUAL REPORT 2008-09
vaccine having five antigens DPT-Hepatitis B-Hibto immunize children against five vaccine preventablediseases of Diphtheria, Pertussis, Tetanus, HepatitisB and Hib disease in some States.
Revival of Vaccine producing units in the PublicSector -Vaccine producing units in the Public Sectorwill be revived to support the Immunisationprogramme. The action plan for revival of productionof DPT group of vaccines at CRI Kasauli is alreadybeing implemented
Nursing plays an important role in the health caredelivery system. In order to strengthen and expandNursing Services to provide Health Services to therural people, Government of India has taken Nursingas a priority programme in the 11th Plan. A newscheme namely Human Resource (Health) Serviceswhich inter alia include upgradation/strengtheningof Nursing Services at a cost of Rs. 200 crore duringthe 11th Plan period has been approved.
To meet shortage of doctors and specialists,comprehensive changes in four regulations ofMedical Council of India (MCI), relating to under-graduate/postgraduate medical education, startingof new medical colleges and minimum requirementqualification for teachers have been approved bythe Ministry and awaiting notification by MCI. A newcentrally sponsored scheme with 75%assistance from the Centre for strengtheningand up gradation of state government medicalcolleges for increasing seats in PG courses andstarting new PG courses has been formulated. Forthis purpose, an amount of Rs. 1350 crores has beenearmarked in the 11th five year plan.
National Council for Human Resources in Health -
In order to reform the current regulatory frame workand enhance the supply of skilled personnel, theGovernment of India has proposed to set up a
National Council for Human Resources in Health asan overarching regulatory body. To deliberate on theissue of setting up of the National Council, a TaskForce under the chairmanship of the Union Secretaryfor Health & Family Welfare has been constituted.The Task Force is expected to submit its report by31st July 2009.
During the year 2008-09, concerted efforts were madetowards the implementation of the newly enacted FoodSafety and Standards Act, 2006 which seeks tointegrate the various existing laws on food. In this regard,the Food Safety and Standards Authority of India(FSSAI) was established for effective implementationof the new Act.
Health relief activities in cyclone (AILA) affectedareas of West Bengal -The cyclonic storm (AILA)struck the State of West Bengal on 25th - 26th May2009 affecting about 39 lakh people from 19 districts.The Public Health Teams of the Ministry were deputedto the worst affected areas for rapid healthassessment. Medical teams were also mobilizedfrom Railways, ESIC and the Army, apart fromneighbouring States. These teams are monitoringthe situation.
Achieving an acceptable standard of health forgeneral population has been the objective over theplan era in the Health sector. In line with thisobjective, there has been a steady increase inallocations made for this Sector from very beginningof the Plan era. Allocation for Health & Family Welfareduring 10th Plan was of the order of Rs.37,153 crores.This has been substantially enhanced to Rs.1,40,136crores during the XIth plan. We hope that substantiallyenhanced funding along with rationalisation ofpolicies and systemic corrections initiated underNRHM would help establish a robust Public HealthSystem which would respond to the expectations ofthe citizens of India.
NARESH DAYAL
Secretary (H &FW)Ministry of Health & Family Welfare
Date : 11-07-2009
New Delhi
5
ANNUAL REPORT 2008-09
Chapter 1
1.1 Introduction
In view of the federal nature of the Constitution,areas of operation have been divided between UnionGovernment and State Governments. SeventhSchedule of Constitution describes three exhaustivelists of items, namely, Union list, State list andConcurrent list. Though some items like Public Health,hospitals, sanitation, etc. fall in the State list, the itemshaving wider ramification at the national level likepopulation control and family welfare, medicaleducation, prevention of food adulteration, qualitycontrol in manufacture of drugs etc. have beenincluded in the Concurrent list.
The Union Ministry of Health & Family Welfare isinstrumental and responsible for implementation ofvarious programmes on a national scale in the areasof Health & Family welfare, prevention and control ofmajor communicable diseases and promotion oftraditional and indigenous systems of medicines.Apart from these, the Ministry also assists states inpreventing and controlling the spread of seasonaldisease outbreaks and epidemics through technicalassistance.
Ministry of Health & Family Welfare incurs expenditureeither directly under Central Schemes through itstwo departments, including the attached offices ofDGHS and its various subordinate offices, or by wayof grants - in - aids to the autonomous/statutorybodies etc. and NGOs. In addition to the 100%centrally sponsored family welfare programme, theMinistry is implementing several World Bank assistedprogrammes for control of AIDS, Malaria, Leprosy,and Tuberculosis and Blindness in designated areas.Besides, State Health Systems Develoment Projectswith World Bank assistance are under implementationin various states. The projects are implemented by
Organization & InfrastructureOrganization & InfrastructureOrganization & InfrastructureOrganization & InfrastructureOrganization & Infrastructure
the respective State Governments and the Departmentof Health & Family Welfare only facilitates the Statesin availing of external assistance. All these schemesaim at fulfilling the national commitment to improveaccess to Primary health care facilities keeping inview the needs of rural areas and where the incidenceof disease is high.
The Union Ministry of Health & Family Welfarecomprises the following departments, each of whichis headed by a Secretary to the Government of India:-
� Department of Health & Family Welfare
� Department of AYUSH
� Department of AIDS Control (Created inDecember, 2008)
� Department of Health Research
Organograms of the above Departments of Health &Family Welfare ,Department of AYUSH , Departmentof AIDS Control and Department of Health Researchare at Annexure (Part-I) at the end of the AnnualReport.
Directorate General of Health Services (Dte.GHS) isan attached office of the Department of Health &Family Welfare and has subordinate offices spreadall over the country. The DGHS renders technicaladvice on all medical and public health matters andis involved in the implementation of various healthschemes.
1.2 Minister in Charge
The Ministry of Health and Family Welfare is headedby Union Minister of Health and Family Welfare, ShriGhulam Nabi Azad since 29th May, 2009. He isassisted by the Ministers of State for Health andFamily Welfare-Shri Dinesh Trivedi and Shri S.Gandhiselvan.
6
ANNUAL REPORT 2008-09
Union Minister of Health and
Family Welfare
Shri Ghulam Nabi Azad
Minister of State for Health
and Family Welfare
Shri Dinesh Trivedi
Minister of State for Health
and Family Welfare
Shri S. Gandhiselvan
1.3 Administration
In order to fulfill Government's commitment to providebetter health care facilities, the Department has takennew initiatives and steps to ensure that theGovernment policies and programmes areimplemented in a time-bound and efficient manner.It has enforced discipline and accountability amongstits officers and staff.
As part of responsive administration, Director(Administration) attends to service related grievancesof the staff in the Department of Health and FamilyWelfare. Secretary(Health and Family Welfare) alsogives personal hearing to staff grievances.
For quick and timely redressal of public grievances,Shri P A Sawant, Director (Welfare & PG) in theDepartment is functioning as nodal officer. UnderSecretary (welfare and PG) assists him in the matter.
1.4 Healthy Lifestyle Centre (YOGA &GYM)
A Healthy Lifestyle Centre (Yoga & Gym), funded byWHO has been functioning in the Ministry since 28th
November 2005. The officers and staff of the Ministryhave been availing this facility
1.5 Modernization of Office
The work relating to modernization of office premisescontinued in 2008-09, during which period, about10 rooms have been upgraded, creating more space
and improved working environment. Two conferencehalls have been modernized and one mini conferencehall has been newly built.
1.6 Central Health Service
The Central Health Service was restructured in 1982to provide medical manpower to various participatingunits like Directorate General of Health Services(DGHS), Central Government Health Service(CGHS), Government of National Capital Territory(GNCT) of Delhi, Ministry of Labour, Deptt. of Posts,Assam Rifles, etc. Since inception a number ofparticipating units like ESIC, NDMC, MCD, HimachalPradesh, Manipur, Tripura, Goa, etc. have formedtheir own cadres. The latest in the list of institutionswhich has gone out of CHS cadre is JIPMER,Pondicherry which has become an autonomous bodyw.e.f. 14th July, 2008. Recently, Ministry of Labour(Labour Welfare Organization) and Assam Rifleswhich is under the Ministry of Home Affairs have alsoopted out of CHS partially. At the same time unitslike CGHS have also expanded. The Central HealthService now consists of the following four sub cadresand the present strength of each sub-cadre is asunder:
i) General Duty Medical Officer sub-cadre - 3137
ii) Teaching Specialists sub-cadre - 778
iii) Non-Teaching Specialists sub-cadre - 784
iv) Public Health Specialists sub-cadre - 079
7
ANNUAL REPORT 2008-09
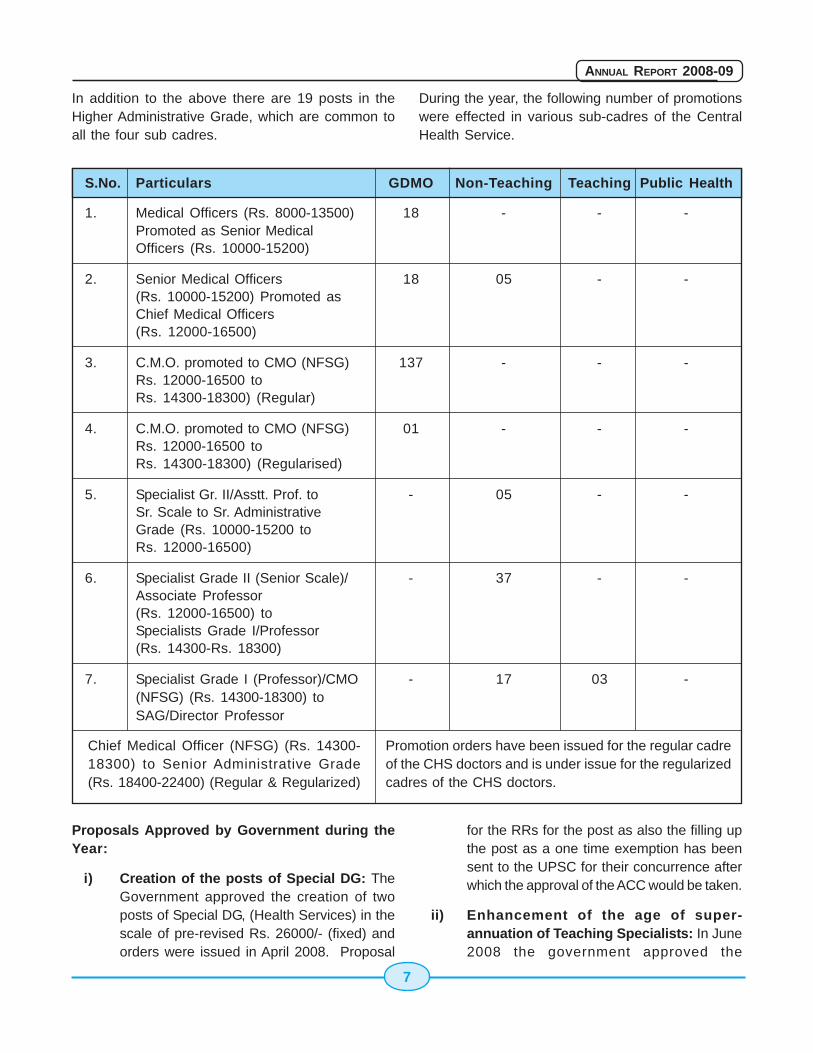
In addition to the above there are 19 posts in theHigher Administrative Grade, which are common toall the four sub cadres.
During the year, the following number of promotionswere effected in various sub-cadres of the CentralHealth Service.
S.No. Particulars GDMO Non-Teaching Teaching Public Health
1. Medical Officers (Rs. 8000-13500) 18 - - -Promoted as Senior MedicalOfficers (Rs. 10000-15200)
2. Senior Medical Officers 18 05 - -(Rs. 10000-15200) Promoted asChief Medical Officers(Rs. 12000-16500)
3. C.M.O. promoted to CMO (NFSG) 137 - - -Rs. 12000-16500 toRs. 14300-18300) (Regular)
4. C.M.O. promoted to CMO (NFSG) 01 - - -Rs. 12000-16500 toRs. 14300-18300) (Regularised)
5. Specialist Gr. II/Asstt. Prof. to - 05 - -Sr. Scale to Sr. AdministrativeGrade (Rs. 10000-15200 toRs. 12000-16500)
6. Specialist Grade II (Senior Scale)/ - 37 - -Associate Professor(Rs. 12000-16500) toSpecialists Grade I/Professor(Rs. 14300-Rs. 18300)
7. Specialist Grade I (Professor)/CMO - 17 03 -(NFSG) (Rs. 14300-18300) toSAG/Director Professor
Chief Medical Officer (NFSG) (Rs. 14300-18300) to Senior Administrative Grade(Rs. 18400-22400) (Regular & Regularized)
Promotion orders have been issued for the regular cadreof the CHS doctors and is under issue for the regularizedcadres of the CHS doctors.
Proposals Approved by Government during theYear:
i) Creation of the posts of Special DG: TheGovernment approved the creation of twoposts of Special DG, (Health Services) in thescale of pre-revised Rs. 26000/- (fixed) andorders were issued in April 2008. Proposal
for the RRs for the post as also the filling upthe post as a one time exemption has beensent to the UPSC for their concurrence afterwhich the approval of the ACC would be taken.
ii) Enhancement of the age of super-annuation of Teaching Specialists: In June2008 the government approved the
8
ANNUAL REPORT 2008-09
enhancement of age of superannuation ofMedical Teaching Specialists of the CentralHealth Service and other medical institutionsunder the Ministry of Health and FW from 62years to 65 years. This would be applicableto all the Teaching Specialists of the CentralHealth Service as also the Medical TeachingFaculty in AIIMS, New Delhi, PGIMER,Chandigarh, NIMHANS, Bangalore,NEIGRIHMS, Shillong, RIMS, Imphal, AIIH &PH, Kolkatta and LGBRIMH, Tezpur.
iii) Extension of DACP Scheme upto SAGlevel: Government approved the extensionof Dynamic Assured Career Progression(DACP) Scheme upto Senior AdministrativeGrade (SAG) in respect of all Medical andDental doctors including doctor of the CentralHealth Service under the Ministry of Healthand Family Welfare.
iv) Posting of doctors to Andaman & NicobarIslands: The Andaman & NicobarAdministration had formed their own serviceknown as Andaman Health Services.However, despite best efforts on their partthe vacancies of Specialists (Non-Teaching)Sub-Cadre could not be filled and thatAdministration has sought assistance fromthis Ministry to fill up the posts. Accordingly,from August 2008 onwards General DutyMedical Officers with requisite PGqualification are being deputed to the A & NIslands for a period of 90 days in Specialitiesof Medicine, Radiology, ENT, Skin andObstetrics & Gynaecology. By the end ofMarch 2009 it is expected that 21 officerswould have completed their tenure of 90 dayseach in the Islands. The Andaman andNicobar Administration has also been advisedto tie up with some of the well known hospitalslike Lifeline/Apollo Hospitals for better patientcare through the system of telemedicine. Inthe case of Lakshadweep Islands the systemof rotational transfer of Specialists for aperiod of 90 days is still continuing.
v) Contractual appointments of retiredGDMOs: The Government of India has
approved the appointment of retired GDMOsof CHS on contract basis in CGHSdispensaries subject to the following termsand conditions:
a) The contract will be for one yearextendable by another one year
b) Retired GDMOs will be engaged on aconsolidated amount of Rs. 25,000/- p.m.
c) All appointees shall be below the age of65 years.
vi) Increasing the remuneration ofcontractual employees: The contractualemployees appointed under the Governmentof India were in receipt of a lump sum amountof Rs. 26000/ p.m. However, havingconsideration to the fact these contractemployees supervise the work of the Juniorand Senior Residents and the pay of theseResident has been substantially increasedas a result of the recommendations of the6th CPC, it has been decided that the pay ofcontractual employees be raised to Rs.47500/- plus DA.
Other Service related matters
i) Special efforts for obtaining ACRs:One of the major component cadremanagement of CHS is to ensure timelysubmission of ACRs by all participatingunits in respect of CHS officers workingunder them. In order to catalyze thesystem of collecting of ACRs NodalOfficers had been appointed during 2006for three or four participating units in aparticular territory. These Nodal Officerswere required to coordinate withindividual units for collection andsubmission of ACR to the Ministry in time.It has been observed that the system hasborne fruits and there is a quantum jumpin timely submission of
ii) the ACRs by the participating units.Further, it was noticed that one of theparticipating units, namely GNCT Delhi
9
ANNUAL REPORT 2008-09
was found wanting in submission of ACRsin time. Accordingly, the matter was takenup at the highest level in GNCT byaddressing a suitable letter to the ChiefSecretary, GNCT, Delhi explaining thepoor position of submission of ACRs bythat Government. The response to thatletter has been very good andencouraging as hundreds of ACRs havebeen received in respect of CHS officersworking under GNCT, Delhi. It is in thefitness of thing that the letters arereceived from various hospitals underGNCT, Delhi intimating the submissionsof ACR to the Secretariat in Delhi forfurther follow up. In order to give fillip tothe on-going efforts, team of officers ofCHS Division have been constituted forvisit to various participating units of theCHS throughout the country.
iii) Formation of the Delhi Health Service:The formation of the Delhi health Servicewas going on since 2006. The UPSChave now approved the Delhi HealthService Allopathy Rules on 14thNovember 2008 and have requested theGNCT of Delhi to issue the Notificationwithin a period of ten weeks. Specialefforts had been taken by this Ministry toexpedite the formation of the Delhi HealthService in order to gauge the number ofdoctors that would be remaining in theCHS after the formation of the Delhi HealthService and JIPMER which has alreadybeen declared as an autonomousorganization in July 2008.
Tentative figures indicate that the strength of CentralHealth Service in each of the sub-cadres would beas follows:
Teaching Sub Cadre 241
Non-Teaching Sub Cadre 598
Public Health 75
GDMO 2175
(iii) RTI: The number of RTI cases receivedin this Division is 113.
(iv) Court Cases: There were 83 CAT/Courtcases pending in various CAT/Courts in thebeginning of financial year 2008-09. But dueto vigorous efforts by the CHS Division, 19cases have been disposed off by the courtsand only 64 cases are pending in courts.
(v) Deputation of GDMO with PGQualification: The CHS Rules provide for100 posts to be filled on deputation. It hasaccordingly been decided to allow GDMOSub-Cadre of CHS with PG qualification inany Specialty to apply to the posts ofSpecialists in any of the three Specialists SubCadre i.e. Teaching, Non Teaching and PublicHealth on deputation basis.
Non Medical Scientists
A proposal has been mooted to amend the ISP Rules,90 to incorporate provisions for inclusion of moreposts within its ambit as also to exclude some of theposts outside its purview.
Draft COS Note has also been circulated amongconcerned Departments calling for their commentson the proposal for amendment of UPSC(Exemptionfrom Consultation) Regulations, 1958 under Ministryof Health and Family Welfare with a view to do awaywith the requirement of consultation with the UPSCin the matter of in-situ promotion upto S.IV level.Action has also been taken to fill up three out of thesix vacant posts at S-V level.
Dental Posts:-
During the year 2008-09 six posts of Dental Surgeonsunder Ministry of Health and Family Welfare havebeen filled up on regular basis. Orders for promotionof three Dental Surgeons as Junior Staff Surgeonsand placement of two Dental Officers in the NFSGwere issued.
A proposal for giving the benefit of DACP to the DentalOfficers from a retrospective date i.e. the date fromwhich it was made applicable to CHS Officers, hasbeen submitted to the COS for its consideration.

10
ANNUAL REPORT 2008-09
The process has also been initiated to amend theDental Posts Recruitment Rules, 1997 to bring themin conformity with the changes that have since takenplace.
Seniority Lists
The grade-wise seniority lists of doctors belongingto the four sub-cadres of CHS have been posted onthe website of Ministry of Health & FW and is beingregularly updated.
1.7 E-Governance Initiatives of theMinistry of Health & FW
Health Informatics Division of National InformaticsCentre provides MIS and Computerization supportto Ministry of Health & Family Welfare. More than1200 PCs of the Ministry are connected to the LocalArea Network (LAN), which in turn, connected toNICNET through RF Link and leased line circuits.Salient features of the some of the projects handledby NIC are as follows:
Web Page of the Ministry of Health & FamilyWelfare :
The updation of Website of the Ministry of Health &Family Welfare http://mohfw.nic.in and various otherwebsites under the ministry is done on a regular basis,as and when the information is provided by the users.Critical information such as Bird Flu, notifications ofthe CGHS, Tenders under the Ministry, SanctionDetails of the Principal Accounts Office & PublicExpenditure Management, etc are such areas whereregular updation takes place.
Network Maintenance and email, internetusage
NIC provides new LAN connections; network basedAnti-virus solution in addition to maintaining existingnetwork users. At present over 1200 LAN nodes havebeen provided in the Department of Health & FamilyWelfare and about 100 LAN nodes are there at IRCSBuilding at Dept of AYUSH. The email and internetusage has grown significantly and officials preferemail communication over other means.
Computerization of Central Govt. HealthScheme (CGHS)
CGHS is high on the agenda of the Government withthe ultimate objective to provide effective, timely andhassle free healthcare to the CGHS beneficiary. Thecomputerized system is aimed at computerizing allfunctions of the dispensary such as Registration,Doctors' prescription, Pharmacy Counter, Stores,Laboratory & Indent. The system has beensuccessfully implemented in the CGHS dispensariesof Delhi/NCR a year before. Now the 102dispensaries outside Delhi in 6 locations namelyMumbai, Pune, Nagpur, Chennai, Hyderabad andChennai are under implementation.
The system requires robust internet connectivity inthe CGHS dispensaries to access the computerizedweb based system work. The broadband connectivitycurrently provided in the dispensaries is beingupgraded to the Managed Leased Data Network(MLDN) which will provide dual use of Leased Lineand Broadband connection and can be monitoredremotely, the implementation of which is undercompletion. The similar MLDN network is also underimplementation in 110 locations in CGHSdispensaries of NCR region and 6 aforesaidlocations outside Delhi/NCR.
The introduction of plastic cards for every individualCGHS beneficiary with the barcode number is underimplementation. Hence every beneficiary will haveto carry plastic card in place of the CGHS Index Card(which was the family card). The distribution of plasticcards has already started and is likely to completeby this year.
More modules have been introduced in thecomputerized system. The pilot implementation ofclaims processing of individual beneficiaries,diagnostic centers, permissions etc is underway. TheURL of the site is http://cghs.nic.in . .
FSSAI Web portal
Food Safety & Standards Authority of India (FSSAI)has been established under the Food Safety andStandards Act, 2006 as a statutory body for layingdown science based standards for articles of food

11
ANNUAL REPORT 2008-09
and regulating manufacturing, processing, distribution,sale and import of food so as to ensure safe andwholesome food for human consumption. The webportal of the FSSAI has been designed and launched.The complete System Requirements Study isunderway. The URL of the site is http://fssai.gov.in.
Intra-Health Portal for the Ministry:
NIC had initiated the development of a portal for theMinistry of Health and Family Welfare. The serviceslike Pay slips, user profile, Birthday Greetings, FileMovement System, Project Monitoring System, News,Events, Notices and Circulars, Photo of the week etchave been incorporated. File Movement system isbeing accessed by various sections of theDepartment of AYUSH & Department of Health &Family Welfare. The portal URL is http://intrahealth.nic.in. This portal can become an effectivetool for the users to communicate within the Ministryand share the files, documents, notifications, circularsetc.
Grant-In-Aid (GIA) and Utilization Certificates(UC) monitoring system
The web based system has been launched in theMinistry and all the Pay & Accounts Offices of theministry use it centrally. Now it's possible to track thestatus of GIA and UCs division wise, institution wise,state wise. It can become more useful when all thedivisions in the Ministry start using this system. TheURL is http://mohfw.nic.in/uc/super/login.asp.
PNDT Web Portal
Pre-Natal Diagnostic Techniques (PNDT) has beenestablished under the Pre-Conception and Pre-NatalDiagnostic Techniques (Prohibition of sex selection)Act, 1994. The Web portal was launched in April 2008during the launch of the Save the Girl ChildCampaign by the Hon'ble Prime Minster of India. Theportal provides all the necessary information aboutthe Act and its implementation. A web based MIS hasalso been developed through which all the hospitalsand diagnostics centers such as Ultra Sound Clinicsand Labs involved in pre-natal examinations arerequired to submit the online form F against eachcase reported with them. The monitoring and
regulation of these cases is carried out by the Stateand District Appropriate Authorities through the onlinesystem. The training has been successfullycompleted for State and District AppropriateAuthorities in most affected States where the ratio ofFemales to Males is alarmingly low. The training isunderway to cover all the States and UTs.
Computerisation of Medical Stores Organization(MSO) and General Medical Stores Depots(GMSDs)
The MSO is a premier organization of the MoHFW,which is involved in procurement and supply ofmedicines to the Central Govt. hospitals across India,CGHS, Para-military forces. MSO does it through its7 GMSDs located across India. Inventorymanagement is therefore very vital for the MSO sothat the medicines are supplied to the indenters intime after proper quality check.
The web based Inventory management system forthe MSO & GMSD has been implemented on a pilotbasis. The full cycle implementation is underway withvarious stack holders such as indenters, suppliers;Labs etc are to be provided with the connectivity tobe part of the online system.
Integrated Diseases Surveillance Project (IDSP)
Integrated Disease Surveillance Project (IDSP) is adecentralized, State based Surveillance Program ofMOHFW covering the whole country. It is intended todetect early warning signals of impending outbreaksand help initiate an effective response in a timelymanner.
NIC has been entrusted with the turn keyresponsibility of establishing the ICT infrastructureat around 800 sites including 604 Districts, 35 statecapitals, 147 Medical colleges, 12 ID hospitals andcentral offices in Delhi.
The ICT infrastructure has so far been madefunctional at around 85 % of the total locations. Thework is in progress in the states of Bihar, Jharkhandand UP which joined later in IDSP. This ICT networkenables enhanced Speedy Data Transfer, VideoConferencing, Discussions, Training e-learning for

12
ANNUAL REPORT 2008-09
outbreaks and program monitoring under IDSP. Videoconferencing is being used regularly for discussionsbetween states and Central Unit during outbreaksand for monitoring if IDSP implementation andTraining. A 24X7 call center with toll free telephoneno 1075 accessible from BSNL/MTNL telephone fromall states is in operation since February 2008. Thisreceives disease alerts from anywhere in the countryand shares the information with the respective State/District Surveillance Units for verification and initiatingappropriate actions wherever required. During thelast 10 months of operation, 29,548 calls werereceived at 1075 during last 10 months of which 68were Health Alerts resulting in 7 outbreak alerts.
Development of OncoNET India: a computernetwork of 125 Cancer Centers:
NIC is proposing to outsource the development ofOncoNET to a vendor and has developed a businessmodel for implementation of the project. The vendorwould set up the medical equipment (viz. DigitalMicroscope and X-Ray scanner) at the centres tofacilitate transmission of patients' EMR; in additionthe network would facilitate scheduling ofappointments, management/treatment and follow upvisits. The vendor would be using telemedicinesoftware indigenously developed by NIC. RFP for bidsfor the same would be released shortly.
Computerised Medical Seats Allotment System:
In compliance of the Hon'ble Supreme Court of India,Directorate General of Health Services allot 15%undergraduate medical/dental seats and 50%Postgraduate recognised/approved MD/MS degree/diploma seats and MDS seats. Towards this,Computerised Medical Seats Allotment System isimplemented by NIC and operational for the last 15years.
Earlier, the Post Graduate/Under Graduate Medical/Dental Seats Allotment was done only at New Delhi.From the academic year 2007-08, Undergraduatemedical/dental seats counselling was providedthrough Video conferencing based counselling in thecities of Puducherry and Kolkatta in addition to NewDelhi. Also, reservations for SC/ST category meritholders had also been implemented from theacademic year 2007-08.
From the academic year 2009-10 onwards, thecomputerized Seat Allotment will be done in the citiesof New Delhi, Mumbai, Chennai, Kolkatta and Shillongthrough VC based counselling. Also, reservationsfor OBC and PH merit holders in addition to SC/STcategory merit holders is being introduced from theacademic year 2009-10.
ehospital@NIC:
NIC had developed work flow based HospitalManagement Information System (HMIS) thro' TripuraState Unit. Presently, this software had beenimplemented and successfully running in G.B. PantHospital, Agartala. Various customized versions ofthis software are running in number of governmentHospitals, to name a few, ESIC Hospital, BasaiDarapur, Delhi, Bhagwan Das Memorial Hospital,Shillong, Indira Gandhi Medical College, Nagpur etc.This software had been demonstrated to the officialsof Ministry of Health & Family Welfare and Dr. RamManohar Lohia Hospital. The proposal pertaining tothe implementation of this software at Dr. RamManohar Lohia hospital had been approved by theMinistry.
Health Management Information System
The Ministry has recently launched a dedicatedHealth Management Information System (HMIS) portalfor all Public Health related information in October2008. The HMIS portal captures data to be collectedas per the revised HMIS formats on a web-basedsystem at the District level and also enablesinformation to be entered for each facility. Theapplication would facilitate timely and accuratecollection, capturing and dissemination of data. Theportal would help in converting the data locally intouseful information, management indicators, districtprofiles, trends which could be displayed graphicallyin reports.
The portal would be generating unique analyticalreports using Data Warehousing platform for finetuning policy initiatives. Information could be madeavailable quickly and regularly to decision makersand other users in the form of specific and tailoredmonthly, quarterly and annual reports.

13
ANNUAL REPORT 2008-09
1.8 Accounting Organisation
General Accounting Set up
As provided in Article 150 of the Constitution, theAccounts of the Union Government, shall be kept insuch form as the President of India, may on theadvise of Comptroller & Auditor General of Indiaprescribe. The Controller General of Accounts(CGA) in the M/o Finance shall be responsible toprepare and compile the Annual Accounts of theUnion Government to be laid in Parliament. The CGAperforms this function through the Accounts wing ineach Civil Ministry. The Officials of Indian CivilAccounts Organization are responsible formaintenance of Accounts in Civil Ministries. Theadministration of Accounts Officials in all CivilMinistries is under the control of the office of theCGA. However, the Railways, P&T and DefenceMinistries have independent Finance and Accountsservices and are submitting accounts to the CGAthrough the heads of their accounting organizations.
The Secretary of each Ministry/Department is the ChiefAccounting Authority. This responsibility is to bedischarged by him through and with the help of theChief Controller of Accounts (CCA) and on the adviseof the Financial Advisor of the Ministry. The Secretaryis responsible for certification of AppropriationAccounts and is answerable to Public AccountsCommittee and Standing parliamentary Committee onany observations of the accounts. The Chief Controllerof Accounts is submitting Internal audit observationsand matter related to financial discipline directly tothe Secretary in respect of each Department and itssubordinate organizations. The Annual Review Reportof the Internal Audit is also subject to scrutiny by theCGA and Ministry of Finance.
Accounting Set Up in the Ministry-
The Ministry of H&FW has two departments i.e.Department of Health & Family Welfare andDepartment of Ayush (Ayurveda, Yoga, Unani, Sidha& Homeopathy). There is a common Accounting Wingfor both the departments. The Accounting wing isfunctioning under the supervision of a ChiefController of Accounts supported by a Controller ofAccounts (CA), Dy. CA and eleven Pay & Accounts
Officers (PAOs) and 138 Drawing & DisbursingOfficers (DDOs) in the field.
In addition there are Fourteen encadred posts ofthe Accounts Officers located at various places.There is a common Internal Audit wing for bothDepartments, which carry out the inspection of allthe Cheque Drawing and Non-Cheque drawingDDO's, Pr. Accounts Office and all the PAOs. Thereare 5 Field Inspection Parties located at Delhi,Chandigarh, Mumbai, Kolkatta and Bangalore.
Accounting Functions in the Ministry-
The Accounting function of the Ministry comprises ofvarious kinds of daily payments and receipts,compiling of daily challans, vouchers, preparation ofdaily Expenditures Control register etc. Monthlyexpenditure accounts, monthly receipts and monthlynet cash flow statements are being prepared forsubmission to Ministry of Finance through the CGA'soffice. The Pr. Accounts Office prepares Annualfinance Accounts, Annual Appropriation Accounts,Statement of Central Transactions, Annual ReceiptsBudget, Actual Receipts and Recovery statementfor each grant of the Ministry. The head wiseappropriation accounts are submitted to theParliament by the CGA along with the C&AG's report.In addition, the Pr. Accounts office also issues ordersof placement of funds to other civil Ministries, issuedadvices to Reserve Bank of India (RBI) for releaseof loans/grants to State Governments and LOC tothe accredited Bank of the Ministry for placing fundswith DDOs.
Apart from General Accounting functions, theAccounts wing also gives technical advices of variousBudgetary, Financial and Accounting matters.
The Accounting wing also function as a coordinatingagency on all accounts matters between Ministry andOffice of the Controller General Accounts & theComptroller and Auditor General. Similarly itcoordinates on all budget matters between Ministryand the Budget Division of the Ministry of Finance.
1.9 Implementation of RTI Act, 2005
The Law Commission of India's 179th Report andReports of number of Committees and Councils
14
ANNUAL REPORT 2008-09
working on this subject sensitized the Governmentof India to enact a specific law on the right toinformation. Likewise in May 2005 the Right toInformation Act (22 of 2005) was passed by theParliament.
The Right to Information Act, 2005, enacted with aview to promote transparency and accountability inthe functioning of the Government by securing tothe citizens the right to access the information underthe control of public authorities, have already comeinto effect w.e.f. 12.10.2005.
Under the Right to information Act, 2005, 35 CentralPublic Information Officers( CPIOs) and 13 AppellateAuthorities( A/As) have been appointed in the Ministryof Health & Family Welfare(Department of Health &Family Welfare).
All CPIOs including autonomous organizations/PSUswere requested for placing all obligatory informationpertaining to their Division/programme, under Section4(i) of the RTI Act, 2005 in the Website of Ministryand the same has been done. Now RTI/Request/Appeal Management System (RRMS) is underimplementing stage. Under this system CPIOs andAppellate Authorities (including autonomousorganizations) would create computer Basedmanagement of RTI requests and appeal.
Applications under the Act for seeking informationfrom general public are accepted at FacilitationCentre, near Gate No.5, Nirman Bhavan & atCoordination-II ( CDN-II) Section, Room No. 215A,'D' Wing, Nirman Bhawan, New Delhi. Applicationsare also accepted by post through Receipt & Issue(R&I) Section. During 2008-09 1681 applicationsand 268 appeals have been received which werereplied to in time, Annual return for the year 2008-2009 has also been sent to CIC.
1.10 Vigilance
There is Vigilance machinery functioning for theDepartment of Health & Family Welfare under a JointSecretary working as Chief Vigilance Officer (CVO)on part-time basis. The CVO is assisted by aDirector/Deputy Secretary and an Under Secretary.A Vigilance Section with a Section Officer withsupporting staff functions as a part of this set-up.
Apart from dealing with disciplinary cases of theDepartment of Health & FW, the vigilance casesinvolving officials of Directorate General of HealthServices and CGHS are also dealt with by theVigilance Division. The machinery mainly handlesthe vigilance inquiries/ disciplinary proceedings inrespect of doctors and non-medical/technicalpersonnel borne on the Central Health Serviceworking in various hospitals, and CGHS/ P&TDispensaries and other Institutions like MedicalStores Organization, Port Health Organization,Labour Welfare Organization etc.
During 2008-09, 17 charge sheets for major penaltyand 3 charge sheets for minor penalty for allegedirregularities including unauthorized absence wereissued. Penalty was imposed in 5 cases and chargeswere dropped in 7 cases. 2 officials/ officers havebeen placed under suspension during the year. In 3cases, sanction for prosecution was issued.
Central Vigilance Commission's guidelines for usinginformation technology in vigilance administration arebeing implemented and major initiatives have alreadybeen taken to use information technology as a toolto usher in e-governance, minimizing the manualinterface etc. In the CGHS, the entire processstarting from registration of patients to maintenanceof personal records, patients' prescriptions,investigation advices, distribution of medicines andraising indent to local chemists has beencomputerized leaving little scope of corruption.Similarly, e-submissions, standard operatingprocedures have been introduced in the CentralDrugs Standard & Control Organization. An officialwebsite has been launched giving all importantinformation, including status of applications forlicenses etc. Initiatives of these nature are bringingin the much desired transparency in the functioningof the schemes/ organizations.
1.11 Activities of the ComplaintCommittee on Sexual Harassmentof Women Employees
In pursuance of the direction of Hon'ble SupermenCourt in their judgment in the case of Vishakha andother Vs. State of Rajasthan and Others, a Complaint
15
ANNUAL REPORT 2008-09
Committee has been constituted in the Departmentof health and Family Welfare to look into thecomplaints of sexual harassment of women employeesin the Department. The SHC is chaired by Mrs. GangaMurthy, Economic Adviser and has four members Smt.Aparna Sharma- Member, Mr. J.P. Pandey-member,Smt. Manorama Bawa-NGO Member and Mrs. RekahChauhan-Member Secretary.
Three complaints of sexual harassment werereferred to the Committee durin the year 2008. Thebrief of each case is given below:
1. Programme Division Incharge of NIB videletter dated 12.4.2007 referred to the SexualHarassment Committee(SHC) complaintsreceived from two Junior Scientist of NIB,namely Mrs. E. Madhu and Mrs. Ajanta Sarkarabout inappropriate and harassment metedout by Dr. V.K. Kashyap, Director, NIB.Subsequently, on 27.04.2007, the case of Dr.Achala Prasad, Scientist Grade III of NIB wasalso sent. The SHC deliberated on thecomplaints and held Eleven Meetings for thepurpose of deposition by the complainantsand the respondents. A report was submittedto Secretary (HFW) on 5.9.2008.
2. In another case, a complaint was receivedform Dr. Punita k. Sodhi working as assistantProfessor in Ophthalmology in Lady HardingMedical College against Dr. K. P. S. MalikHOD, Ophthalmology, Safdarjung Hospital. Inthis case the complainant was requested toapproach to SHC of Lady Harding MedicalCollege in connection with her complaint.
3. Complaint from the students namely Km Anju(M. Sc.-Microbiology) of IAMR, Ghaziabad,Kum. Payal Tyagi (M.SC.-Biotech) of ITS,Ghaziabad, Kum. Ekta Singh (M.Sc.-Biotech)of ITS, Ghaziabad and Kum. Monica Sharma(M.Sc.-Bilotech) of ITS, Ghaziabad wasreceived against Dr. G.N. Singh, Director CIPLand others. Notices were issued to thecomplainants for their deposition but theyneither attended the meeting nor gaveanything in writing to the committee.
Therefore the committee decided not topursue the case further in the absence ofsupport form the complainants.
As per directions, the Committee is also looking intothe matters relating to appropriate conditions i.e.Hygiene conditions that have an impact on health ofthe women employee of the department.
1.12 Public Grievance Cell
Public Grievance Redressal Mechanism isfunctioning in the Ministry of Health and FamilyWelfare as well as in the attached offices of theDirectorate of Health Services and the otherSubordinate Offices of CGHS ( both in Delhi andother Regions), Central Government Hospitals andPSUs falling under the Ministry for implementation ofthe various guidelines issued from time to time bythe Government of India through the Ministry ofPersonnel, Public Grievances and Pensions.
Ms. Shakuntala D. Gamlin, Joint secretary in theDepartment of Health has been designated as NodalOfficer for Public Grievances relating to theDepartment. Shri P.A. Sawant, Director in theDepartment of Health has been working as PublicGrievance Officer. Similarly other organizations underthe Ministry have also senior level officials functioningas Public Grievance Officers.
Director (A&V), Directorate General of Health Servicesand Director (EMR), Directorate General of HealthServices are functioning as Public/ Staff GrievanceOfficer of the Directorate general of Health services.
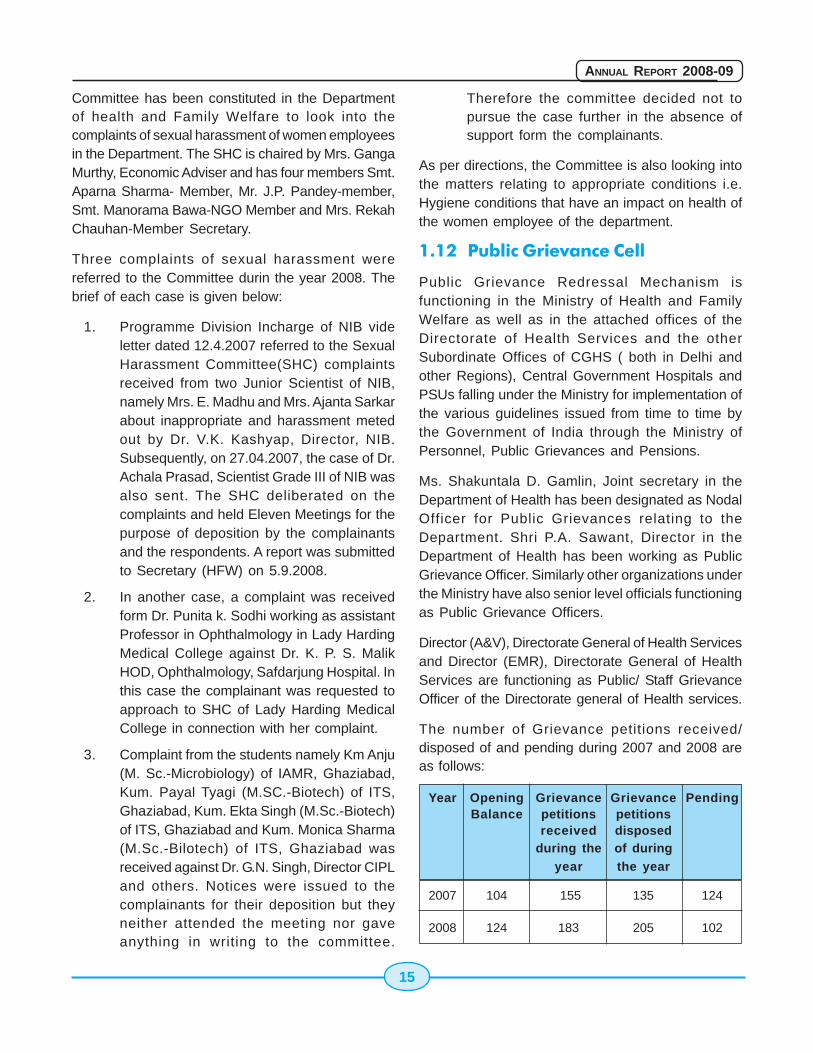
The number of Grievance petitions received/disposed of and pending during 2007 and 2008 areas follows:
Year Opening Grievance Grievance PendingBalance petitions petitions
received disposedduring the of during
year the year
2007 104 155 135 124
2008 124 183 205 102
16
ANNUAL REPORT 2008-09
1.13 Information & Facilitation Centre
To strengthen the Public Redressal Mechanism inthe Ministry of Health &Family Welfare an Information& Facilitation Centre is functioning adjacent to GateNo.5, Nirman Bhawan. The facilitation centerprovides the following information to public: -
1. Circulars/ Booklets/ Pamphlets/ Posters/ NGOGuidelines and forms for public use.
2. Receipt of Application under Right toInformation Act 2005
3. Information and Guidelines to avail the grantfrom Health Minister's Discretionary fund andRashtriya Arogya Nidhi.
4. Guidelines and instructions regarding issueof NOC to Indian Doctors to pursue highermedical studies abroad.
5. Petitions/ Complaint/ Suggestions on publicGrievances are received at the Centre.
6. Information and guidelines relating to CGHSand Query regarding work of Drugs ControllerGeneral (India) Office
7. Query regarding WHO's WHO in the Ministrypersonally and on Telephone
During the year 5,000(approximate) queries werereceived at the Information & Facilitation Centre,which were disposed of to the satisfaction of allconcerned.
1.14 National Urban Health Mission
Context:
Rapid urbanization has led to rapid increase innumber of urban poor population, majority of wholive in slums. The need for improving the delivery ofhealth care for the urban poor has been recognizedby the National Health Policy (2000), the NationalPopulation Policy (2002) and the Eleventh Five YearPlan.
However, policy prescriptions have not optimallytranslated into focused strategies for improving thehealth status of the urban poor. On the other hand
the challenges posed by rapid urbanization, degradedenvironmental conditions / poor health indicators ofurban poor population, inadequacy and sub optimalfunctioning of urban primary health infrastructure andovercrowding at secondary level, multiplicity ofservice providers with weak interdepartmentalcoordination, heterogeneity and need for differentstrategies to reach to different section of population;sub optimal utilization of the strengths of private andcharitable service providers, weak communitycapacity, clearly pronounce the need of different setof strategies for meeting the above challenges.
Aim:
The proposed National Urban Health Mission aimsto improve the health status of the urban poorparticularly the slum dwellers and otherdisadvantaged sections by facilitating equitableaccess to quality health care with the activeinvolvement of the Urban Local Bodies (ULBs) incities with population one lakh and above and StateCapitals. The NUHM would be covering 21.07 croreurban population with a special focus on 6.25 croreurban poor living in slums and beyond, spread over430 cities.
Core Strategies:
(i) Improving the efficiency of public healthsystem in the cities by strengthening,revamping and rationalizing urban primaryhealth structure
(ii) Partnership with non government providersfor filling up of the health delivery gaps
(iii) Promotion of access to improved health careat household level through community basedgroups (Mahila Arogya Samittees) and UrbanSocial Health Activist (USHA)
(iv) Strengthening public health throughpreventive and promotive action
(v) Increased access to health care through riskpooling
(vi) IT enabled services (ITES) and e-governance for improving access improvedsurveillance and monitoring
17
ANNUAL REPORT 2008-09
(vii) Capacity building of stakeholders
(viii) Prioritizing the most vulnerable amongst thepoor
(ix) Ensuring quality health care services.
Financial Allocation:
The proposed financial outlay of the National UrbanHealth Mission is Rs. 5249 Crores of which anestimated allocation of Rs.4495 crores would be fromthe Central Government for a period of 4 years (2008-2012) and State/ULB share would be Rs. 754 crores,to enable adequate focus on urban health. Thiswould be supplemented by remaining balance ofRs.958.84 crores i.e. outlay for the CentrallySponsored Scheme (CSS) - Urban Health Centres(UFWCs. and UHPs) which is through the Treasuryroute. Thus the total outlay for NUHM would be Rs.5249 crores and the remaining balance of Rs. 958.84crores.
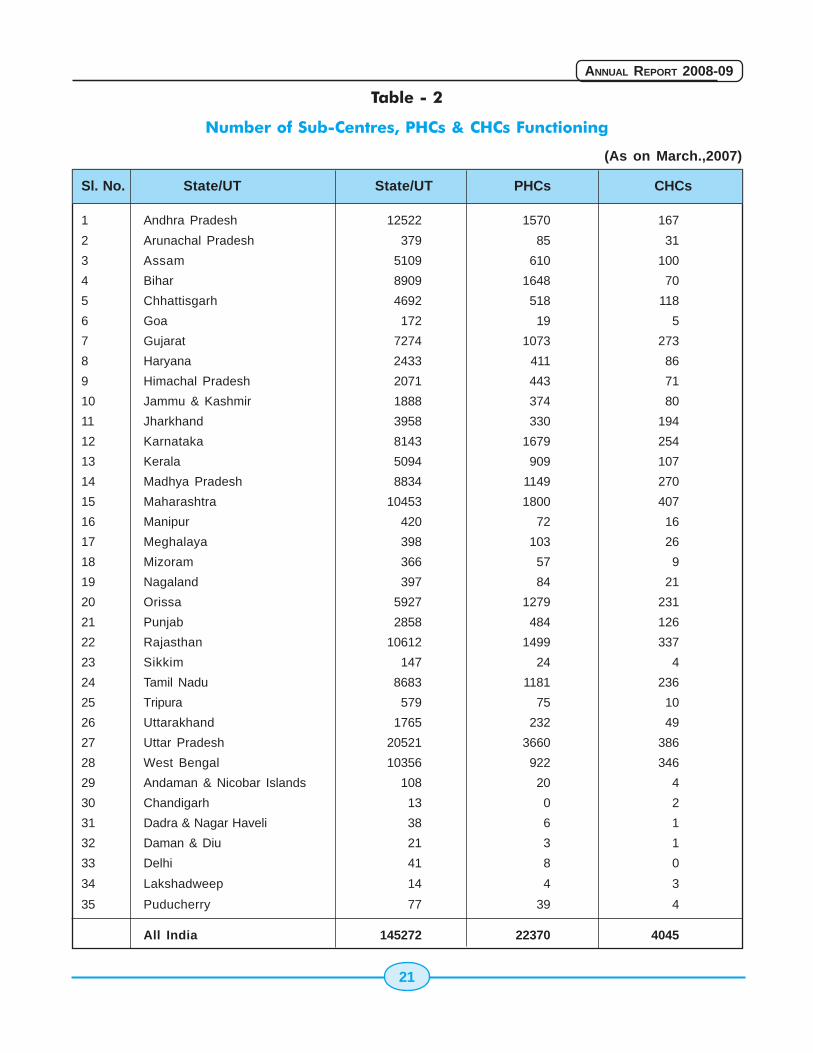
1.15 Rural Health Services
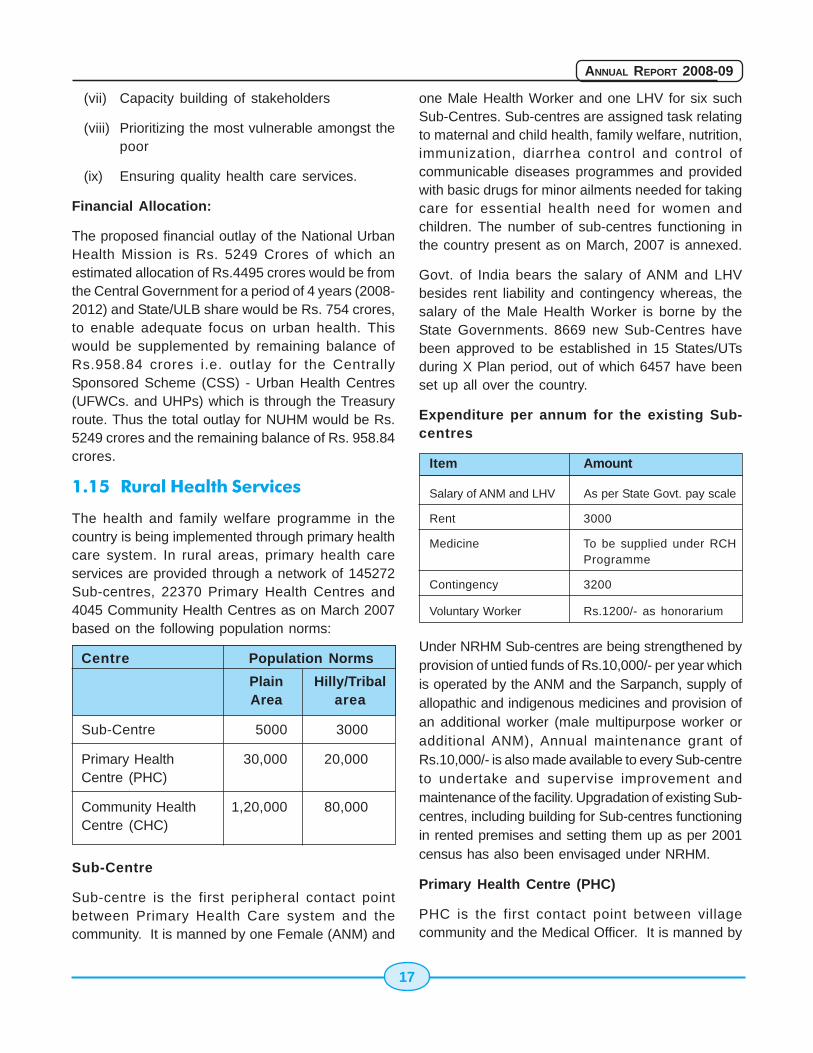
The health and family welfare programme in thecountry is being implemented through primary healthcare system. In rural areas, primary health careservices are provided through a network of 145272Sub-centres, 22370 Primary Health Centres and4045 Community Health Centres as on March 2007based on the following population norms:
Centre Population Norms
Plain Hilly/TribalArea area
Sub-Centre 5000 3000
Primary Health 30,000 20,000Centre (PHC)
Community Health 1,20,000 80,000Centre (CHC)
Sub-Centre
Sub-centre is the first peripheral contact pointbetween Primary Health Care system and thecommunity. It is manned by one Female (ANM) and
one Male Health Worker and one LHV for six suchSub-Centres. Sub-centres are assigned task relatingto maternal and child health, family welfare, nutrition,immunization, diarrhea control and control ofcommunicable diseases programmes and providedwith basic drugs for minor ailments needed for takingcare for essential health need for women andchildren. The number of sub-centres functioning inthe country present as on March, 2007 is annexed.
Govt. of India bears the salary of ANM and LHVbesides rent liability and contingency whereas, thesalary of the Male Health Worker is borne by theState Governments. 8669 new Sub-Centres havebeen approved to be established in 15 States/UTsduring X Plan period, out of which 6457 have beenset up all over the country.
Expenditure per annum for the existing Sub-centres
Item Amount
Salary of ANM and LHV As per State Govt. pay scale
Rent 3000
Medicine To be supplied under RCHProgramme
Contingency 3200
Voluntary Worker Rs.1200/- as honorarium
Under NRHM Sub-centres are being strengthened byprovision of untied funds of Rs.10,000/- per year whichis operated by the ANM and the Sarpanch, supply ofallopathic and indigenous medicines and provision ofan additional worker (male multipurpose worker oradditional ANM), Annual maintenance grant ofRs.10,000/- is also made available to every Sub-centreto undertake and supervise improvement andmaintenance of the facility. Upgradation of existing Sub-centres, including building for Sub-centres functioningin rented premises and setting them up as per 2001census has also been envisaged under NRHM.
Primary Health Centre (PHC)
PHC is the first contact point between villagecommunity and the Medical Officer. It is manned by

18
ANNUAL REPORT 2008-09
a Medical Officer and 14 other staff. It acts as areferral Unit for 6 Sub-Centres and has 4-6 beds forpatients. It performs curative, preventive, promotiveand Family Welfare services. There are 22370 PHCsfunctioning in the country.
The PHCs are being strengthened under NRHM toprovide a package of essential public healthprogrammes and support for outreach services toensure regular supplies of essential drugs andequipment, round the clock services in all PHCsacross the country, upgrading single doctor PHC to2 doctors PHC by posting AYUSH practitioners at PHClevel, provision of 3 Staff Nurses in a phased manner.The States/UTs have to incorporate their proposalsand requirement of funds in their Annual ProgrammeImplementation Plans under NRHM. Untied Grant ofRs.25,000/- per PHC for local health action andAnnual Maintenance Grant of Rs.50,000/- per PHCthrough PHC level Panchayat Committee/RogiKalyan Samiti to undertake and superviseimprovement and maintenance of physicalinfrastructure have been provided.
Community Health Centre (CHC)
CHC is established and maintained by the StateGovernments and as per standards it is supposedto be manned by four Medical specialists i.e.Surgeon, Physician, Gynecologist and Pediatriciansupported by 21 paramedical and other staff. It has30 in-door beds with one OT, X-ray, and Labour roomand Laboratory facilities and serves as a referralcentre for 4 PHCs. It provides facilities for emergencyobstaetrics care and specialist consultations. IndianPublic Health standards lays down that this CHC isto be manned by 6 Medical Specialists includingAnaesthetics and an eye surgeon (for 5 CHCs)supported by 24 paramedical and other staff withinclusion of two nurse midwives in the present systemof seven nurse midwives. At present 4045 CHCsare functioning in the country.
For Upgradation of CHCs as per the Indian PubicHealth Standards (IPHS). State/UTs have beenrequested to carry out the facility survey of all CHCsso as to gauge the exact requirement of funds interms of upgrdation of the facility as far as manpower,building, equipments etc. if concerned. Initial funds
@ Rs.20 lakh per CHC has already been providedunder the initiative and more funds are beingprovided every year as requested by the States intheir annual Programme Implementation Plan underNRHM.
Strengthening of the Sub-Divisional /Sub-District and District Hospitals
For upgradation of District Hospitals to IPHS, theStates/UTs other than NE Sttes have been releasedfunds @ Rs.20.00 lakhs as an initial amount for 498District Hospitals and @ Rs.one crores per DH in theNE States for 69 District Hospitals.
Indian Public Health Standards (IPHS)
Indian Public Health Standards (IPHS), which detailthe specifications of standards to which institutionsof primary health care would have to be raised to sothat the citizen is confident of getting public healthservices in the hospital that can be measured to beof acceptable standards. Indian Public HealthStandards (IPHS Sub-centres, PHCs, CHCs, Sub-divisional/Sub-district Hospitals and District Hospitalslay down Standards not only for personnel andphysical infrastructure, but also for delivery ofservices, and management. A system of performancebench marks will be introduced to concurrently assessthe adherence of public hospitals to IPHS, in atransparent manner.
Each Hospital would, as part of IPHS, be required toset up a Rogi Kalyan Samittee (RKS)/HospitalManagement Committee), which will bring incommunity control into the management of publichospitals. Guidelines for setting up of Rogi KalyanSamiti have been circulated to all State/UTs. Basedon the registration details of RKSs set up by variousStates/UTs, funds @ Rs. one lakh per PHC, CHC,Sub-divisional/Sub-district Hospitals and @ Rs.5.00lakhs per District Hospital have been released forRKSs to these States/UTs. The objective is to providesustainable quality care with accountability andpeoples participation alongwith total transparency.
Mobile Medical Units/Health Camps
With the objective to take health care to the doorstep of the public in the rural areas, especially in
19
ANNUAL REPORT 2008-09
under-served areas, Mobile Medical Units (MMUs),have been provided, one per district under NRHM.The States are however, expected to address thediversity and ensure the adoption of more suitableand sustainable model for the MMU to suit their localrequirements. They are also required to plan forlong-term sustainability of the intervention.
Two kinds of MMUs are envisaged, one withdiagnostic facility for the States other than North-East States, Himachal Pradesh and J&K. In addition,for the North- Eastern States, Himachal Pradesh andJ&K, specialized facilities and services such as X-ray, ECG and ultrasound are proposed to beprovided in MMUs due to their difficult hilly terrain,non-approachability by public transport, longdistances to be covered etc.
The States are needed to involve District HealthSociety/Rogi Kalyan Samiti/NGOs in deciding theappropriate modality for operationalization of theMMUs. The provision of staff will be considered onlyfor the States who will run the vehicles with supportof NGOs/RKSs and in case of States out-sourcingthe vehicles. States are needed to work out numbersof mobile dispensaries/health camps as a means ofmobilizing local communities of health action and forcreating demand
Tackling the problem of lack of manpower inRural Areas :
The Government is seized of the problem of lack ofskilled manpower in rural health infrastructure. Anumber of new and innovative steps have been takenby various State/UT Governments to bridge the gapbetween the available and required manpowerespecially for ensuring the availability of Doctors inrural areas. A Task Group constituted under theNational Rural Health Mission under the chairmanshipof Director General of Health Services hasrecommended the following measures to ensure theservices of doctors in rural areas :
- Increase in the age of retirement of doctorsto 65 years preferably with posting nearhometown;
- Decentralization of recruitment at districtlevel;
- Walk-in-interview and contractualappointment of doctors;
- Enhancing the salary for posting in ruralareas by one-third;
- Increasing the admission capacity in medicalcolleges for Anesthesia;
- Reviving the Diploma Course in Anesthesia;
- To start one year Certificate Course inAnesthesia for Medical Officers working inthe system at present to be given by NationalBoard of Examination.
- Recognition of five hundred bedded Hospitalsto provide the facility for conducting theabove course;
- Hiring of private practitioners on case-to-case basis.The above recommendation werecirculated to All the State /UT Governments.State/UT Governments have taken a numberof initiatives to ensure presence of doctorsin rural areas such as :
- Compulsory rural/difficult area posting foradmission to post-graduate courses and asa pre-requisite for promotion, foreignassignment or training abroad ;
- Compulsory rotation of doctors on completionof prescribed tenure as per classification oflocations;
- Contractual appointment of doctors;
- Option to forgo non practicing allowance andundertake practice without compromising onassigned duties, as per the service rules;offering incentive in form of allowance etc.
- Manning of PHCs by NGOs/ Non GovernmentStatkeholders
- Involvement of Medical colleges.
Apart from doctors, steps have been taken to deploycontractual manpower in all other cadres ie. ANM,MPWs, Pharmacists etc. The funds are beingreleased to all States/UTs under NRHM as per their
20
ANNUAL REPORT 2008-09
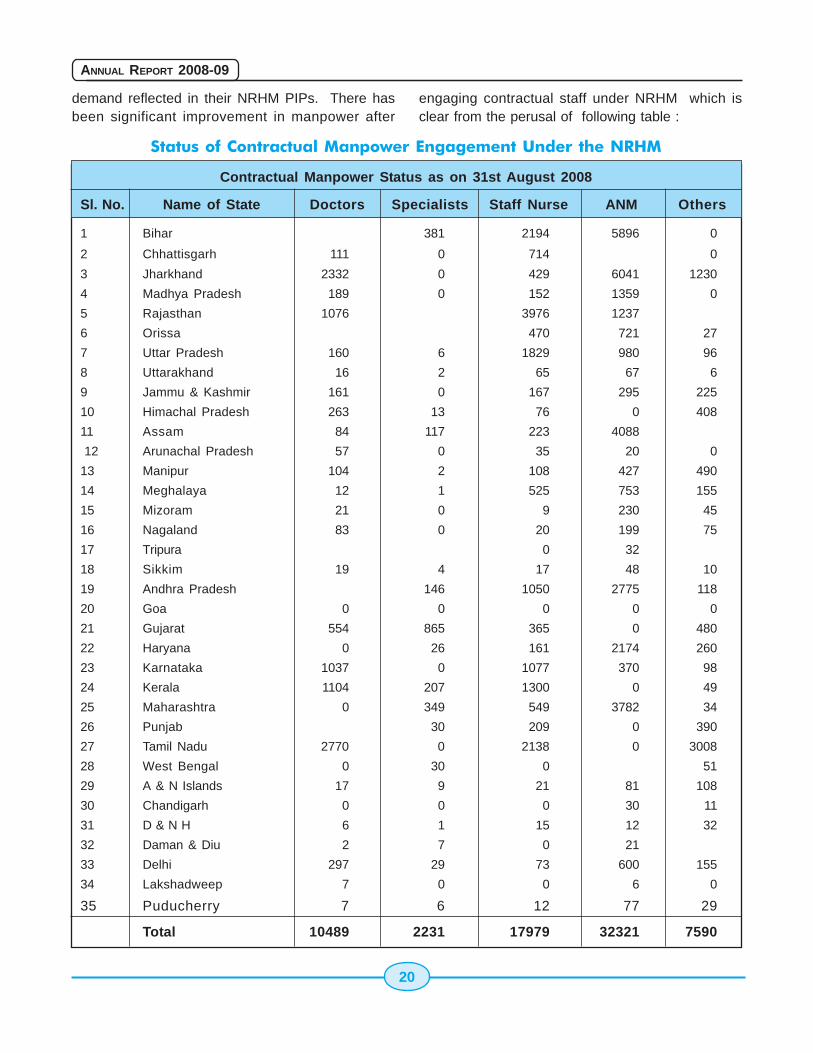
demand reflected in their NRHM PIPs. There hasbeen significant improvement in manpower after
engaging contractual staff under NRHM which isclear from the perusal of following table :
Status of Contractual Manpower Engagement Under the NRHM
Contractual Manpower Status as on 31st August 2008
Sl. No. Name of State Doctors Specialists Staff Nurse ANM Others
1 Bihar 381 2194 5896 0
2 Chhattisgarh 111 0 714 0
3 Jharkhand 2332 0 429 6041 1230
4 Madhya Pradesh 189 0 152 1359 0
5 Rajasthan 1076 3976 1237
6 Orissa 470 721 27
7 Uttar Pradesh 160 6 1829 980 96
8 Uttarakhand 16 2 65 67 6
9 Jammu & Kashmir 161 0 167 295 225
10 Himachal Pradesh 263 13 76 0 408
11 Assam 84 117 223 4088
12 Arunachal Pradesh 57 0 35 20 0
13 Manipur 104 2 108 427 490
14 Meghalaya 12 1 525 753 155
15 Mizoram 21 0 9 230 45
16 Nagaland 83 0 20 199 75
17 Tripura 0 32
18 Sikkim 19 4 17 48 10
19 Andhra Pradesh 146 1050 2775 118
20 Goa 0 0 0 0 0
21 Gujarat 554 865 365 0 480
22 Haryana 0 26 161 2174 260
23 Karnataka 1037 0 1077 370 98
24 Kerala 1104 207 1300 0 49
25 Maharashtra 0 349 549 3782 34
26 Punjab 30 209 0 390
27 Tamil Nadu 2770 0 2138 0 3008
28 West Bengal 0 30 0 51
29 A & N Islands 17 9 21 81 108
30 Chandigarh 0 0 0 30 11
31 D & N H 6 1 15 12 32
32 Daman & Diu 2 7 0 21
33 Delhi 297 29 73 600 155
34 Lakshadweep 7 0 0 6 0
35 Puducherry 7 6 12 77 29
Total 10489 2231 17979 32321 7590
21
ANNUAL REPORT 2008-09
Table - 2
Number of Sub-Centres, PHCs & CHCs Functioning
(As on March.,2007)
Sl. No. State/UT State/UT PHCs CHCs
1 Andhra Pradesh 12522 1570 167
2 Arunachal Pradesh 379 85 31
3 Assam 5109 610 100
4 Bihar 8909 1648 70
5 Chhattisgarh 4692 518 118
6 Goa 172 19 5
7 Gujarat 7274 1073 273
8 Haryana 2433 411 86
9 Himachal Pradesh 2071 443 71
10 Jammu & Kashmir 1888 374 80
11 Jharkhand 3958 330 194
12 Karnataka 8143 1679 254
13 Kerala 5094 909 107
14 Madhya Pradesh 8834 1149 270
15 Maharashtra 10453 1800 407
16 Manipur 420 72 16
17 Meghalaya 398 103 26
18 Mizoram 366 57 9
19 Nagaland 397 84 21
20 Orissa 5927 1279 231
21 Punjab 2858 484 126
22 Rajasthan 10612 1499 337
23 Sikkim 147 24 4
24 Tamil Nadu 8683 1181 236
25 Tripura 579 75 10
26 Uttarakhand 1765 232 49
27 Uttar Pradesh 20521 3660 386
28 West Bengal 10356 922 346
29 Andaman & Nicobar Islands 108 20 4
30 Chandigarh 13 0 2
31 Dadra & Nagar Haveli 38 6 1
32 Daman & Diu 21 3 1
33 Delhi 41 8 0
34 Lakshadweep 14 4 3
35 Puducherry 77 39 4
All India 145272 22370 4045

22
ANNUAL REPORT 2008-09
23
ANNUAL REPORT 2008-09
Chapter 2
2.1 National Rural Health Mission(NRHM)
The National Rural Health Mission (NRHM) launchedon 12.4.2004 by the Hon'ble Prime Minister of India,is being operationalised throughout the Country withspecial focus on 18 States which included 8Empowered Action Group States (Bihar, Jharkhand,Madhya Pradesh, Chhattisgarh, Uttar Pradesh,Uttaranchal, Orissa and Rajasthan, 8 NE States,Himachal Pradesh and Jammu and Kashmir.
ASHAs/ Link Worker
� Selection of 6, 48,516 ASHAs/Link workershave been done in the entire country, out ofwhich 5, 63,462 ASHAs were given orientationtraining and positioned in villages.
� 4.11 lakhs ASHAs have been provided withdrug kit as well.
Infrastructure
� 1.45 lakhs Subcentres in the country areprovided with untied funds of Rs. 10,000each. 3,02,200 Subcentres & VHSC haveoperational joint accounts of ANMs andPradhans for utilization of annual untiedfunds. 25,743 Subcentres are functional withsecond ANM.
� Out of 4045 Community Health Centres, 2788CHCs have been selected for upgradationto IPHS and facility survey has beencompleted in 2698 CHCs.
� 23,100 Rogi Kalyan Samitis have beenregistered at different level of facilities.
Manpower
� 10,948 Doctors and Specialist, 33,719 ANMs,
20,977 Staff Nurses, 8645 Paramedics havebeen appointed on contract by States to fillin critical gaps.
Management Support
� 1588 professionals (CA/MBA/MCA) havebeen appointed in the State and 576 Districtlevel Program Management Units (PMU) and3474 Block level Program Management Units(BPMU) have been established to supportNRHM.
Mobile Medical Units
� Funds for one Mobile Medical Unit (MMU) perdistrict released for 318 districts. The states,till date has operationalised 243 MobileMedical Units with their own funds.
Immunization
� Intense monitoring of Polio Progress -Services of ASHA useful.
� JE vaccination completed in 11 districts in 4states - 93 lakh children immunized during2006-07. JE vaccination is being implementedin 26 districts of 10 states in 2007. The 11districts of 4 states where JE vaccination wascarried out in 2006 have introduced JEvaccine in Routine Immunization to vaccinatenew cohort between 1-2 years of age withbooster dose of DPT.
� House tracking of polio cases and intensemonitoring.
� Neonatal Tetanus declared eliminated from7 states in the country.
� Full immunization coverage evaluated at43.5% at the national level.(NFHS-III)
NRHM, Health & Population PoliciesNRHM, Health & Population PoliciesNRHM, Health & Population PoliciesNRHM, Health & Population PoliciesNRHM, Health & Population Policies
24
ANNUAL REPORT 2008-09
� Accelerated Immunization Programme takenup for EAG and NE State.
Institutional Delivery
� Janani Suraksha Yojana (JSY) isoperationalised in all the States, 7.04 lakhwomen are benefited in the year 2005-06,29.31 lakh in 2006-07, 72.01 lakh in 2007-08 and 51.55 lakh in the year 2008-2009.
Neo Natal Care
� Integrated Management of Neonatal andChildhood Illnesses (IMNCI) started in 219districts this year.
� With the help of Neonatology Forum over90,401 health care personnel trained inNewborn Care in the country.
� Module for Home based new born caredeveloped in consultation with Dr. AbayBhang.
Convergence
� Over 37 lakhs in 2006-07, 49 lakhs in 2007-08 and 29 lakhs in 2008-2009 Monthly Healthand Nutrition Days being organized at theAnganwadi Centres in various States.
� The States have constituted 3,42,801 VillageHealth and Sanitation Committees. They arebeing involved in dealing with diseaseoutbreak.
� Convergence with ICDS/Drinking Water/Sanitation/NACO/PRIs ground workcompleted.
� School health programmes have beeninitiated in over 20 States
Health Action Plans
� State PIPs have been received from 31 statesduring 2006-07, 35 in the year 2007-08, and35 State PIPs received in the current year2008-09. Project Implementation Plan (PIPs)of the States under NRHM has beenappraised and funds being released for theyear 2008-09.
� The first cut of Integrated District Health ActionPlans (DHAP) has been finalized for 558districts.
Mainstreaming of AYUSH
� Mainstreaming of AYUSH has been taken upin the States. Total 7275 AYUSH facilities areavailable at District and below district levelhealth institutions. AYUSH person are part ofState Health Mission/Society/RKS/ASHAtraining as members.
Trainings
� Trainings in critical areas includingAnesthesia, Skilled Birth Attendance (SBA)taken up for MOs/ANMs. Integrated SkillDevelopment Training for ANMs/ LMV/MOs,Training on Emergency Obstetrics care andNo Scalpel Vasectomy (NSV) for MOs,Professional Development Programme forCMOs is on full swing.
� ANM Schools being upgraded in all States.
� New nursing schools taken up.
Mother NGOs
� 345 Mother NGOs appointed for 404 districtstill date are fully involved in ASHA training andother activities.
Health Resource Centres
� National Health Systems Resource Centre(NHSRC) set up at the National level.
� Regional Resource Centre set up for NE.
� State Resource Centre being set up byStates.
Monitoring and Evaluation
� Independent evaluation of ASHAs/JSY byUNFPA/UNICEF/GTZ in 8 States.
� Immunization coverage evaluated by UNICEF.
� Independent monitoring by identifiedinstitutions like Institute of Public Auditors ofIndia.
25
ANNUAL REPORT 2008-09
� Ground work for community monitoringcompleted. Phase I of community monitoringin 9 states namely Rajasthan, Orissa,Maharashtra, Madhya Pradesh, Tamilnadu,Chattisgarh, Jharkhand, Karnataka andAssam has been completed.
Surveys
� NFHS III and DLHS III completed.
Financial Management
� Financial Management Group set up underNRHM in the Ministry.
� During the FY 2005-06, out of total allocationof Rs. 6731.16 crore for the ministry, anamount of Rs. 5862.57 crore was releasedas part of NRHM.
� Against Rs. 9065 crore for NRHM activitiesduring 2006-07, Rs. 7361.08 crore released.
� During the FY 2007-08, out of total allocationof Rs. 11010 crore for the ministry, an amountof Rs. 10189.03 crore was released as partof NRHM.
� During the FY 2008-09, out of total allocationof Rs. 12050 crore for the ministry, anamount of Rs. 8242.95 crore (till February,2009) was released as part of NRHM.
2.2 Financial Management of NRHM
In order to ensure that enhanced allocations to theStates/UTs and other institutions under the NRHMare fully coordinated, managed, and utilized, a unifiedsystem was devised for release, monitoring andutilization of funds. The Empowered ProgrammeCommittee (EPC) of the NRHM decided to expandthe ambit of the existing Financial ManagementGroup (FMG) to FMG-NRHM. The following financialmanagement arrangements and funds flow processesunder NRHM were put in place w.e.f. 1.4.2007.
Organizational Set up
1. Director, RCH (Finance) has beenredesignated as Director, NRHM (Finance)to guide the financial management activitiesof the NRHM.
2. NRHM Finance Division stands created videorder dated 21.12.2006 with one UnderSecretary, two Accounts Officers, one SectionOfficer, one Assistant, one data entryoperator and one Group- D. All sanctionorders for allocation of funds under the RCHFlexible Pool and Mission Flexible Pool arebeing prepared and issued by this Division.The reorganized FMG-NRHM which will nowhave a revised strength of 16 personnel oncontract/deputation i.e four FinanceControllers, three Finance Analysts and nineFinance Assistants being recruited with theassistance of the Development Partners like,World Bank, UNFPA, DFID etc. is also a partof the NRHM Finance Division.
Objectives of FMG-NRHM
� Bring about integration in the finances of theNational Health Programmes subsumedunder the NRHM.
� Improve Financial Management Systems atthe Centre, State and District levels underthe NRHM.
� Maintain a sound system for funds flow,monitoring utilization, accounting and auditof all programmes subsumed under NRHM.
Functions of FMG-NRHM
� Fund release under RCH Flexible Pool andMission Flexible Pool under NRHM.
� Monitoring and compilation of FinancialMonitoring Reports (FMRs) on quarterlybasis.
� Claims for refund from Development Partnerslike World Bank, DFID etc.
� Audit arrangements and submission of auditreports to Development Partners.
� Providing Financial Management formats andMonitoring Financial performance indicators.
� Capacity building of finance and accountspersonnel of States/UTs.

26
ANNUAL REPORT 2008-09
� Obtaining UCs for the various programmesunder NRHM
� Generating MIS reports on the basis of FMRsreceived.
System of Funds Release
� Obtaining approval of National ProgrammeCoordination Committee (NPCC) andcommunicating the approved amounts to theStates/UTs
� Releases are however, restricted to BE/REenvelope approved by the Ministry of Financeand separately communicated to States.
� As per GFRs, up to 75% of the approvedBEs can be released to the States on receiptof provisional UCs for the previous year.
� Balance 25% is released after receipt ofsatisfactory audited accounts with final UCs.Concurrence of IF is invariably obtained.
� Centrally transfer the funds electronically tothe State Health Societies for all programmesunder NRHM and maintain a centralized database for all releases and utilization under allcomponents of NRHM viz. (a) RCH, (b)Additionalities under NRHM, (c) Immunizationand (d) National Disease ControlProgrammes.
Training & capacity building of Finance &AccountsPersonnel
The FMG-NRHM conducts training of finance andaccounts personnel of the State/District HealthSocieties. The State/District level functionaries of allhigh focus states have already been trained. ATraining Workshop for State Finance and AccountsManagers had been convened at LBSNAA,Mussoorie in May, 2007. A Consultation Meeting forfinance & accounts personnel of the eight north-eastern States was organized with the help ofRegional Resource Centre (RRC) at Guwahati inOctober, 2008. A National Workshop on FinancialManagement Under NRHM to discuss and finalize thenew Open Tender System for engagement of
Statutory Auditors for State & District Health Societiesfrom 2008-09, in consultation with Mission Directors,Finance & Accounts Managers of the States/UTs washeld at Kolkata from 4th to 6th February, 2009 inassociation with the development partner DFID. Inaddition to this, training and capacity building offinance & accounts personnel is also regularly takenup by the National Institute of Health & Family Welfare,an autonomous body under this Ministry.
An accounting system in Tally has also beendeveloped. Important guidelines on financialmanagement pertaining to NRHM are also availableon the Ministry's website mohfw.nic.in
Other arrangements
Multiple societies in the States have been mergedinto Integrated Health Societies, paving the way fora single window release of funds from the Centre.The post of Director (Finance & Accounts) sanctionedearlier will be the overall in-charge of all financial,accounting and audit processes of the State andDistrict Health Societies and will be the nodal pointfor interaction between the States and the Centre.
2.3 Health Policy
The National Health Policy-2002 (NHP-2002) givesprime importance to ensure a more equitable accessto health services across the social and geographicalexpanse of the country. The Policy outlines the needfor improvement in the health status of the peopleas one of the major thrust areas in the social sector.It focuses on the need for enhanced funding andorganizational restructuring of the public healthinitiatives at national level in order to facilitate moreequitable access to the health facilities. Anacceptable standard of good health amongst thegeneral population of the country is sought to beachieved by increasing access to the decentralizedpublic health system by establishing newinfrastructure in deficient areas ,and by upgradingthe infrastructure in existing institutions. Emphasishas been given to increase the aggregate publichealth investment through a substantially increasedcontribution by the Central Government. Prioritywould be given to preventive and curative initiatives

27
ANNUAL REPORT 2008-09
at the primary health level through increased sectoralshare of allocation.
In pursuance of the overall objectives of the HealthPolicy, several health initiatives have been underimplementation over the years to control/preventcommunicable diseases and non-communicablediseases. The major programmes include NationalVector Borne Disease Control Programme, RevisedTB control Programme, Leprosy Programme,Blindness Control Programme, Mental HealthProgramme, National Programme for the HIV/AIDSetc. One of the major initiatives taken by the Ministryhas been launching of National Rural Health Mission(NRHM) in April, 2005. The Mission acts as anoverarching umbrella to the existing vertical schemes/programmes of Health and Family Welfare includingRCH-II, Vector Borne Disease Control Programmes,T.B. Control Programme, Leprosy, Blindness andIodine Deficiency. The targets set under the NHP-2002 have been achieved in respect of eliminationof leprosy, setting up of integrated System of DiseaseSurveillance and putting in place the system ofNational Health Accounts.
Other important health programmes initiated duringrecent years are the following:-
National Urban Health Mission (NUHM):
With a view to address primary health needs ofpeople living in urban areas, the Ministry is launchingNUHM. Urban Poor families, slum dwellers, migrantworkers and extremely vulnerable population wouldbe identified by the Urban Local Body (ULB) andcovered under the scheme and shall be issued aphoto Family Health Card. There are 427 cities(including state capitals) in India having a populationof 1.00 lakh and above out of which 100 constitutehi-focus cities. This will complement the activitiesundertaken by NRHM in rural areas. The programmewill be on Public -Private Partnership mode.
Strengthening Tertiary Health Care Services(PMSSY)
In order to reduce the gaps in the availability oftertiary health care across States, the Governmenthas drawn up the Pradhan Mantri Swasthya Suraksha
Yojana (PMSSY), for setting up six AIIMS likeInstitutions and up gradation of 13 Medical Collegesin the country. The AIIMS-like institution are to be setup in each of the states of Bihar (Patna),Chhattisgarh(Rajpur), Madhya Pradesh(Bhopal),Orissa (Bhubaneswar), Rajasthan (Jodhpur) andUttarakhand (Rishikesh).
In the 2nd phase of PMSSY, it is proposed to set uptwo AIIMS like institutions at i) Lalganj, Rae Bareilly,UP,ii) Talganj, District Uttar Dinajpur, West Bengal. Itis also proposed to upgrade 5 medical collegeinstitutions-i) Govt. Medical College, Amritsar,Punjabii) Govt. Medical College Tanda, H.P. iii) Govt. MedicalCollege Madurai, TN iv) Govt. MedicalCollege,Nagpur, Maharashtra v) Jawaharlal NehruMedical College of Aligarh Muslim University,Aligarh(UP).
Tobacco control initiative:
Recognizing the fact that consumption of tobaccohas led to large scale health problems in the countryranging from cancer, diabetes, cardiovasculardiseases, deformities to passive smoking, the Ministryhas been taking a lot of measures to prevent peoplefrom using tobacco. A significant step in this directionis the recent ban on use of tobacco in public placeswith effect from October, 2008. It has initiated asmoke-free workplace policy and set up a TobaccoRegulatory Authority. Besides, it is in the process ofmaking a pictorial warning mandatory on tobaccoproducts. The District School Tobacco Programmealso focuses on creating awareness against theadverse impact of the use of tobacco and alcohol.Various awareness programs are conducted toeducate people on the ill effect of tobaccoconsumption and to affect self control on use of suchdangerous substances rather than imposingregulations.
Other initiatives
A number of initiatives such as establishment of theCentral Food Safety and Standards Authority of Indiafor bringing in global quality standard for food in India,the National programme on speech and hearing,National Emergency and Trauma Programme arebeing implemented. New initiatives such as National
28
ANNUAL REPORT 2008-09
Organ Transplant Programme, Oral Health,Prevention and Control of Fluorosis, Heath Care forElderly, Human Resources on Health, and NationalAdvisory Boards for standards, National Programmefor Blood and Blood Products etc. are being proposedto be taken up during the 11th Five Year Plan.
2.4 National Commission onPopulation
National Commission on Population was constitutedunder the Chairmanship of Hon'ble Prime Minister ofIndia vide Government of India Gazette Notificationdated 11th May 2000. The Commission startedfunctioning from its Secretariat at PlanningCommission, Yojana Bhavan and was fully functionalwhile located at Planning Commission, YojanaBhavan by exercising its financial and AdministrativePowers, with the supportive help of PAO, PlanningCommission. However, in February 2005, theCommission was re-constituted as per the decisionof Cabinet and its Secretariat was shifted fromPlanning Commission, Yojana Bhavan to Ministry ofHealth & FW. The Chairman of the re-constitutedCommission remained Hon'ble Prime Minister ofIndia, Deputy Chairman of the Planning Commissionand the Minister of Health & FW, the two ViceChairmen and Secretary, FW, as the Member-Secretary of the Commission.
The Terms of reference of the Commission are asfollows: -
� To review, monitor and give directions for theimplementation of the National PopulationPolicy with a view to meeting the goals setout in the policy.
� To promote synergy between demographic,educational, environmental anddevelopmental programmes so as to hastenpopulation stabilization.
� To promote inter-sectoral coordination inplanning and implementation acrossgovernment agencies of the Central andState Governments, to involve the civil societyand the private sector and to explore thepossibilities of international cooperation insupport of the goals set out in the Policy.
� To facilitate the development of a vigorouspeople's movement in support of this nationaleffort.
2. The first meeting of the reconstituted Nationalcommission on Population was held under thechairmanship of Hon'ble Prime Minister on 23rd July2005. The following decisions were taken in themeeting: -
� Conduct of an Annual Health Survey of alldistricts which could be published annuallyso that health indicators at district level areperiodically published, monitored andcompared against benchmarks
� Setting up of five groups of experts forstudying the population profile of the Statesof Bihar, Uttar Pradesh, Rajasthan, MadhyaPradesh and Orissa to identify weaknessesin the health delivery systems and to suggestmeasures that would be taken to improve thehealth and demographic status of the States.
3. In accordance with the above decision, thefollowing measures have been taken to implementthe decisions:-
i. Ministry of Health & Family Welfare had wideranging discussion with Office of RegistrarGeneral and Planning Commission forconducting Annual Health Survey (AHS) andOffice of Registrar General has beenidentified as the nodal organization forconducting the AHS. A Steering Committeehas been constituted on 6th September 2007under the Chairmanship of Mission Director(NRHM), Ministry of Health & Family Welfareto coordinate the content of the survey, itsmethodology and comparability with theexisting National level surveys. The firstmeeting of the Steering Committee was heldon 16th October 2007 under theChairmanship of Mission Director (NRHM). AnEFC Note for undertaking the Annual HealthSurvey through the Office of RGI had beendiscussed in a meeting of the ExpenditureFinance held on 4th September, 2008.
29
ANNUAL REPORT 2008-09
Process for providing HR support toundertake the Survey has been initiated.
ii. Five Experts Groups have been constitutedon 29th September 2005 for studying thepopulation profile of the States of Bihar, UttarPradesh, Rajasthan, Madhya Pradesh andOrissa in order to identify weaknesses in thehealth delivery systems and to suggestmeasures to improve the health anddemographic status of these States. TheseGroup of Experts have already deliberatedthe issue pertaining to Health Delivery Systemand Demographic Status of these. Thereports of these Groups of Experts have beenreceived and are being examined in thisMinistry.
The Commission has been providing policy supportto the population stabilization efforts under overallframework of implementation of NRHM by the states.The Commission has come out with a number ofpublications in collaboration with Registrar Generalof India and Institute of Economic Growth, whichprovides valuable inputs on future demographictrends, challenges and suggestive measures forachieving population stabilization as envisaged inNPP 2000 and NRHM goals.
2.5 State Population Commissions
State Population Commissions have been constitutedin 20 States/UTs. viz. Andhra Pradesh, ArunachalPradesh, Assam, Haryana, Himachal Pradesh, J&K,Kerala, Madhya Pradesh, Gujarat, Uttar Pradesh,Maharashtra, West Bengal, Meghalaya, Mizoram,Punjab, Rajasthan, Sikkim, Tamil Nadu, Andaman &Nicobar Island and Lakshadweep.
2.6 Janasankhya Sthirata Kosh
In the inaugural address of National Commission onPopulation held on 22nd July 2000, the Prime Ministerhad announced the constitution of the NationalPopulation Stabilization Fund (NPSF), which was setup under National Commission on Population.Subsequently, the NPSF was transferred to theDepartment of Family Welfare in April 2002. It wasrenamed and registered as Janasankhya Sthirata
Kosh (JSK) under the Societies Registration Act, 1860in June, 2003.
The objective of JSK is to facilitate the attainment ofthe goals of National Population Policy 2000 andsupport projects, schemes, initiatives and innovativeideas designed to help population stabilization bothin the Government and Voluntary sectors, andprovide a window for canalizing resources throughvoluntary contributions from individuals, industry,trade organizations and other legal entities infurtherance of the national cause of populationstabilization.
JSK has been reconstituted on 14-6-2005. Underthe new set up, the General Body of the JSK ischaired by the Minister for Health and Family Welfare,while the Governing Board is chaired by the Secretary(H&FW). The Executive Director, selected from thecivil society, is the Chief Executive Officer of the Kosh.Eight meeting of the Governing Board of JansankhyaSthirata Kosh was held on 11th August 2008 underthe Chairmanship of Secretary (H&FW) & Chairmanof the Governing Board (JSK).
The major strategies initiated by JSK are givenbelow: -
GIS Mapping
JSK has mapped 485 districts through a uniqueamalgamation of GIS Maps and Census Data whichgives a picture of each district, its sub-division andthe population of every village along with its basichealth infrastructure. Easily accessible on theinternet the maps highlight inequalities in coveragedown to every village of the country at the touch of abutton. JSK has won the award under the categoryof Best Government Initiative for mapping Healthamenities with the help of GIS maps for entire countryexcept North eastern states and Himachal Pradeshdue to the non availability of data. The award wasgiven in an event named "eINDIA 2008" held atPragati Maidan, New Delhi on 31st July 2008.
Call Centre
JSK has established a Call Centre to give authenticinformation on reproductive and infant health in
30
ANNUAL REPORT 2008-09
English and Hindi, using computer based software.The service is routed through a leading BPO providerCustomer and trained agents give advice toadolescents, newly married and about-to-be marriedcouples and others who seek guidance. The CallCentre number (011-66665555) is being accessedfrom different parts of the country and providesinformation anonymously in English or Hindi. Thesoftware has been developed by leading medicalcolleges and is a boon for people who seek authenticinformation in privacy.
The Call Centre number is being advertised in thedistricts of EAG states to open a new window ofinformation for underserved areas.
Website
JSK's website is accessed on an average 475 pagesper day with 89% Indian visits and 11% internationalvisits. Most sought after subjects are sexual health(in Hindi) and the district health facilities through GISmapping.
Prerna Strategy
JSK has introduce a "Responsible Parenthood"model called Prerna to reward couples in high focusdistricts who voluntarily delay the age of marriage,allow girls stay in school and to couples that plantheir family in the interest of the health of the motherand child. JSK gives rewards for couples if they satisfythe following conditions:
� Girl's marriage after 19 years of age. (Rewardof Rs.5000/-)
� Giving birth to the first child after the motherwas 21 years old. (Reward of Rs.7000/- if it'sa girl child & Rs 5000/- if it's a boy)
� Keeping a 36 month gap between first andsecond child, and one parent gettingsterilized after the second child isborn.(Reward of Rs.7000/- if it's a girl child &Rs 5000/- if it's a boy)
Coupled with:
� Registration of Marriage
� Registration of birth
JSK has introduced the Prerna strategy in MadhyaPradesh and Rajasthan. Couples from Dhaulpur andJodhpur have already received the awards at thehands of the Collector at a public function.
Santushti Strategy
This strategy provides an opportunity to privatesector gynaecologists / vasectomy surgeons toconduct operations in Public Private Partnershipmode and to receive payment according tocompensation rates notified by the Ministry of Healthand Family Welfare. Santushti is a fast-track strategywhich enables an accredited facility to get Rs.1.5lakhs for conducting 100 surgeries with a Rs.15,000start up advance. Rs. 500 more is also being givenper case provided an accredited nursing ho meconducts 30 or more cases in a day. This strategywas initiated in Madhya Pradesh and Rajasthan.
Involving Private O&G Practitioner for IUCD380 A
JSK has involved the private sector in promoting theintra-uterine contraceptive device called IUCD 380Awhich gives protection for 10 years. The improvedversion has not been picked up in large measure inthe private sector although it is a boon for womenwho want to have both long term protection frompregnancy keeping the option of having a babyaccording to preference. 4 workshops have beenheld with over 250 gynecologists who have beenencouraged to popularize the device within the privatesector.
Display Mindset Change Posters
In consultation with UNFPA, JSK prepared mindsetchange posters which address family members togive the girl a chance to be in good health beforeshe produces a child. The posters are available athttp://www.jsk.gov.in/jsk_strategies.asp for beingdownloaded by any organization and they can fix theirown logo and display them at places like post offices,rural banks, fertilizer depots, shops or any placeswhere congregates .
This is one way of promoting mindset changes byinvolving civil society. These posters have already
31
ANNUAL REPORT 2008-09
been displayed by Indian Railways using their ownLogo at Railway Stations in the Northern states as apart of Corporate Social Responsibility. PSU's in theMinistry of Power and Ministry of Petroleum andNatural Gas are also about to adopt this strategy.
2.7 Family Welfare Linked HealthInsurance Scheme.
As a measure to encourage people to adoptpermanent method of Family Planning, this Ministryhas been implementing a Centrally SponsoredScheme since 1981 to compensate the acceptors ofsterilization for the loss of wages for the day on whichhe/she attended the medical facility for undergoingsterilization.
Apart from providing for cash compensation to theacceptor of sterilisaion some States/UTs wereapportioning some amount for creating amiscellaneous purpose fund utilized for payment ofex-gratia to the acceptor of sterilisaion or his/hernominee in the unlikely event of his/her death orincapacitation or for treatment of post operativecomplications attributable to the procedure ofsterilization, as under:-
i) Rs. 50,000/- per case of death.
ii) Rs. 30,000/- per case of incapacitation.
iii) Rs. 20,000/- per case of cost of treatment ofserious post operation complication.
Any liability in excess of the above limit was to beborne by the State/UT/NGO/ Voluntary Organizationconcerned from their own resources.
The Hon'ble Supreme Court of India in its Order dated1.3.2005 in Civil Writ Petition No. 209/2003(Ramakant Rai V/s Union of India) has, inter alia,directed the Union of India and States/UTs forensuring enforcement of Union Government'sGuidelines for conducting sterilization proceduresand norms for bringing out uniformity with regard ofsterilization procedures by -
� Creation of panel of Doctors/health facilitiesfor conducting sterilization procedures andlaying down of criteria for empanelment of
doctors for conducting sterilizationprocedures.
� Laying down of checklist to be followed byevery doctor before carrying out sterilizationprocedure.
� Laying down of uniform proforma forobtaining of consent of person undergoingsterilization.
� Setting up of Quality Assurance Committeefor ensuring enforcement of pre andpostoperative guidelines regardingsterilization procedures.
� Bringing into effect an insurance policyuniformly in all States for acceptors ofsterilizations etc.
The above directions have all been taken intoconsideration and consolidated in the updatedmanuals on standards and quality assurance insterilization services available on the ministry'swebsite (www.mohfw.nic.in). The family planninginsurance scheme is also one of the initiativeslaunched under direction from the Hon'ble SupremeCourt.
Under the existing government scheme nocompensation was payable for failure of sterilization,and no indemnity cover was provided to Doctors/health facilities providing professional services forconducting sterilization procedures etc. With a viewto do away with the complicated process of paymentof ex-gratia to the acceptors of Sterilisation fortreatment of post operative complications,incapacitation or death attributable to the procedureof sterilization, the Family Planning InsuranceScheme was introduced w.e.f 29th November, 2005for a period of one year to take care of the cases offailure of Sterilisation, medical complications or deathresulting from Sterilisation, and also provide indemnitycover to the doctor / health facility performingSterilisation procedure, with Oriental Insurance Co.and was subsequently renewed for one more yearfrom 29.11.2006 to 31.12.2007 with OIC. The benefitsextended under the scheme are as follows:-
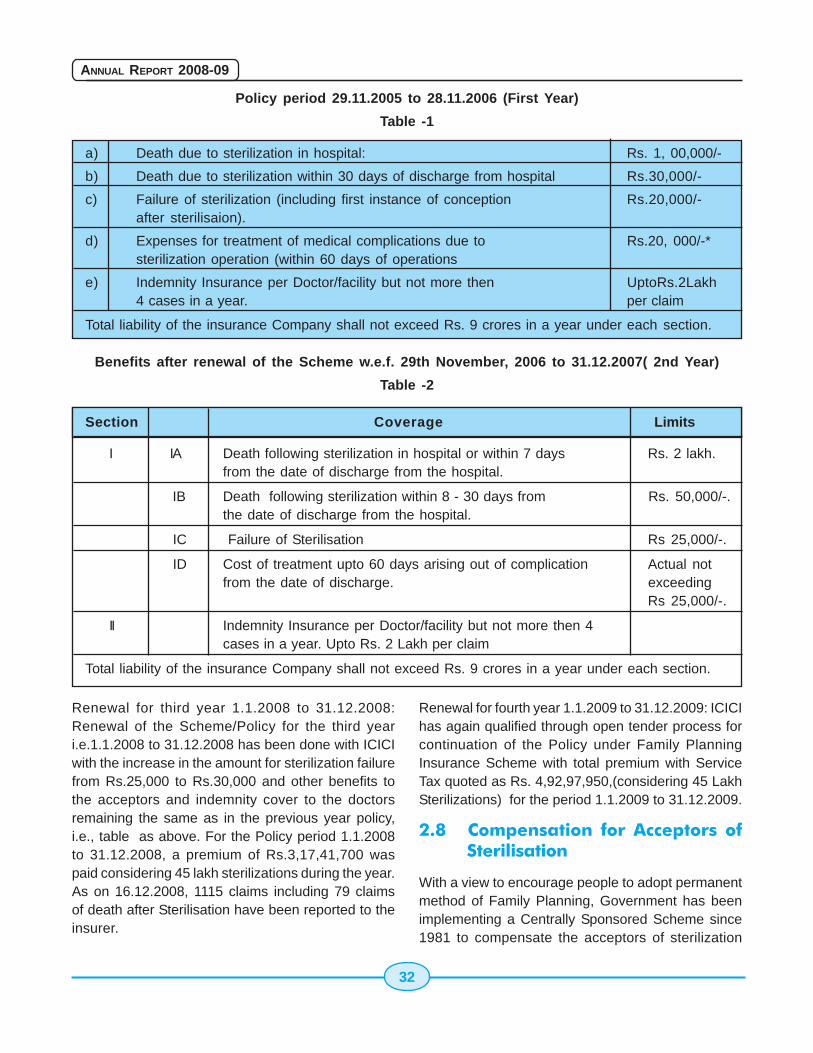
32
ANNUAL REPORT 2008-09
Policy period 29.11.2005 to 28.11.2006 (First Year)
Table -1
a) Death due to sterilization in hospital: Rs. 1, 00,000/-
b) Death due to sterilization within 30 days of discharge from hospital Rs.30,000/-
c) Failure of sterilization (including first instance of conception Rs.20,000/-after sterilisaion).
d) Expenses for treatment of medical complications due to Rs.20, 000/-*sterilization operation (within 60 days of operations
e) Indemnity Insurance per Doctor/facility but not more then UptoRs.2Lakh4 cases in a year. per claim
Total liability of the insurance Company shall not exceed Rs. 9 crores in a year under each section.
Benefits after renewal of the Scheme w.e.f. 29th November, 2006 to 31.12.2007( 2nd Year)
Table -2
Section Coverage Limits
I IA Death following sterilization in hospital or within 7 days Rs. 2 lakh.from the date of discharge from the hospital.
IB Death following sterilization within 8 - 30 days from Rs. 50,000/-.the date of discharge from the hospital.
IC Failure of Sterilisation Rs 25,000/-.
ID Cost of treatment upto 60 days arising out of complication Actual notfrom the date of discharge. exceeding
Rs 25,000/-.
II Indemnity Insurance per Doctor/facility but not more then 4cases in a year. Upto Rs. 2 Lakh per claim
Total liability of the insurance Company shall not exceed Rs. 9 crores in a year under each section.
Renewal for third year 1.1.2008 to 31.12.2008:Renewal of the Scheme/Policy for the third yeari.e.1.1.2008 to 31.12.2008 has been done with ICICIwith the increase in the amount for sterilization failurefrom Rs.25,000 to Rs.30,000 and other benefits tothe acceptors and indemnity cover to the doctorsremaining the same as in the previous year policy,i.e., table as above. For the Policy period 1.1.2008to 31.12.2008, a premium of Rs.3,17,41,700 waspaid considering 45 lakh sterilizations during the year.As on 16.12.2008, 1115 claims including 79 claimsof death after Sterilisation have been reported to theinsurer.
Renewal for fourth year 1.1.2009 to 31.12.2009: ICICIhas again qualified through open tender process forcontinuation of the Policy under Family PlanningInsurance Scheme with total premium with ServiceTax quoted as Rs. 4,92,97,950,(considering 45 LakhSterilizations) for the period 1.1.2009 to 31.12.2009.
2.8 Compensation for Acceptors ofSterilisation
With a view to encourage people to adopt permanentmethod of Family Planning, Government has beenimplementing a Centrally Sponsored Scheme since1981 to compensate the acceptors of sterilization
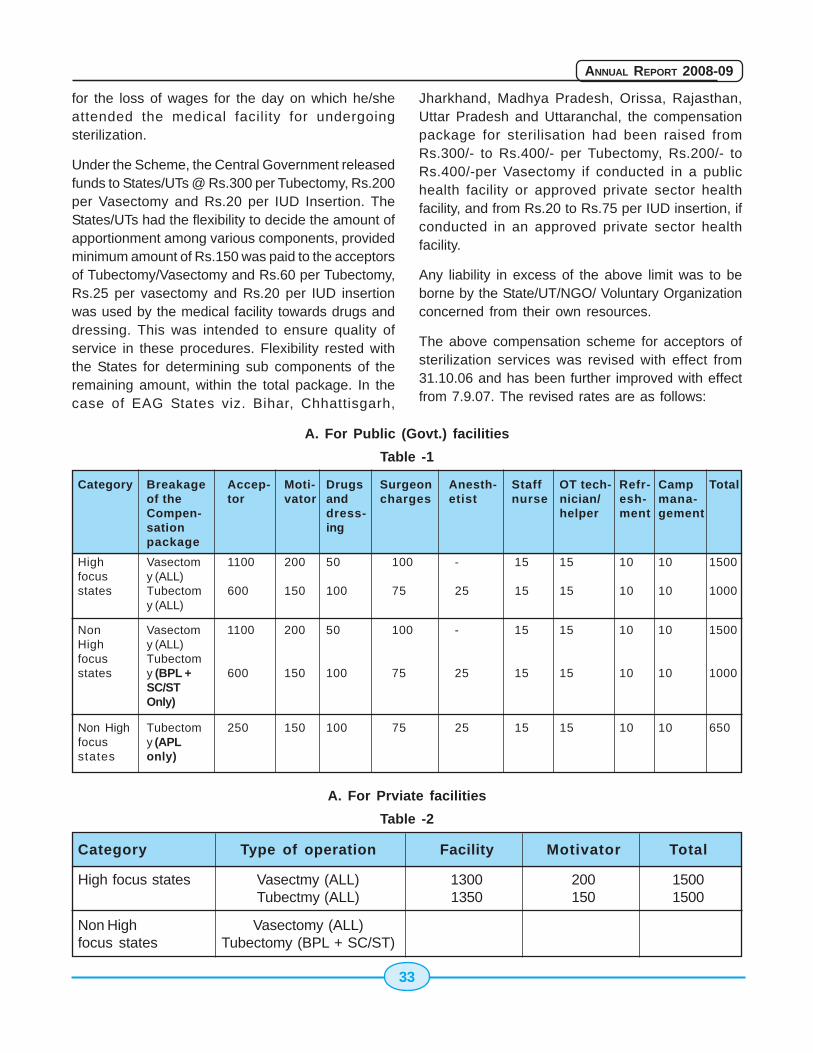
33
ANNUAL REPORT 2008-09
for the loss of wages for the day on which he/sheattended the medical facility for undergoingsterilization.
Under the Scheme, the Central Government releasedfunds to States/UTs @ Rs.300 per Tubectomy, Rs.200per Vasectomy and Rs.20 per IUD Insertion. TheStates/UTs had the flexibility to decide the amount ofapportionment among various components, providedminimum amount of Rs.150 was paid to the acceptorsof Tubectomy/Vasectomy and Rs.60 per Tubectomy,Rs.25 per vasectomy and Rs.20 per IUD insertionwas used by the medical facility towards drugs anddressing. This was intended to ensure quality ofservice in these procedures. Flexibility rested withthe States for determining sub components of theremaining amount, within the total package. In thecase of EAG States viz. Bihar, Chhattisgarh,
Jharkhand, Madhya Pradesh, Orissa, Rajasthan,Uttar Pradesh and Uttaranchal, the compensationpackage for sterilisation had been raised fromRs.300/- to Rs.400/- per Tubectomy, Rs.200/- toRs.400/-per Vasectomy if conducted in a publichealth facility or approved private sector healthfacility, and from Rs.20 to Rs.75 per IUD insertion, ifconducted in an approved private sector healthfacility.
Any liability in excess of the above limit was to beborne by the State/UT/NGO/ Voluntary Organizationconcerned from their own resources.
The above compensation scheme for acceptors ofsterilization services was revised with effect from31.10.06 and has been further improved with effectfrom 7.9.07. The revised rates are as follows:
Category Breakage Accep- Moti- Drugs Surgeon Anesth- Staff OT tech- Refr- Camp Totalof the tor vator and charges etist nurse nician/ esh- mana-Compen- dress- helper ment gementsation ingpackage
High Vasectom 1100 200 50 100 - 15 15 10 10 1500focus y (ALL)states Tubectom 600 150 100 75 25 15 15 10 10 1000
y (ALL)
Non Vasectom 1100 200 50 100 - 15 15 10 10 1500High y (ALL)focus Tubectomstates y (BPL + 600 150 100 75 25 15 15 10 10 1000
SC/STOnly)
Non High Tubectom 250 150 100 75 25 15 15 10 10 650focus y (APLstates only)
A. For Public (Govt.) facilities
Table -1
Category Type of operation Facility Motivator Total
High focus states Vasectmy (ALL) 1300 200 1500Tubectmy (ALL) 1350 150 1500
Non High Vasectomy (ALL)focus states Tubectomy (BPL + SC/ST)
A. For Prviate facilities
Table -2
34
ANNUAL REPORT 2008-09
No apportioning of the above amount is admissiblefor creating a miscellaneous purpose fund forpayment of compensation in case of deaths,complications and failures as these are alreadycovered under the National Family PlanningInsurance Scheme.
The performance in sterilization (national figures)which was 47.35 lakh in 2000-2001 has shown slightdownward trend in 2006-07 with 45.14 cases.
The Government has taken following steps to addressthe concerns of the service providers and acceptorsalike and the programme in general for giving a boostto the sterilization performance:
� National Family Planning InsuranceScheme since 29.11.05: which covers boththe clients as well as the providers againstany mishaps like deaths, complications andfailures and the ensuing litigations
� Orders dated 26th July 2007 of Hon'bleSupreme Court: The orders relating tocriteria of 5 years experience for performingsterilizations were waived off.
� The revision of Compensation packagein Sept.2007 to compensate for loss ofwages and also to provide compensation toproviders of services. It also provided forpartnerships with the non - governmentalsector.
� Promoting Acceptance of No ScalpelVasectomy to ensure male participation.Holding of workshops, seminars,advocacy meet and frequentinteractions with the states to orient themon the GOI's strategy
� Promoting IUD 380A intensively as aspacing method because of its longevity of10 years and advantages over other IUDs
� Increasing skills of IUD providers throughalternative training strategy in IUD insertionin 12 states to start with.
� Fixed day Fixed Place Family PlanningServices round the year - made possibleon account of growing number of 24X7 PHCsand better functioning CHCs and other healthfacilities under NRHM.
� Increasing the basket of choice bysystematically and carefully introducing newand effective contraceptives in theprogramme.
Improved performance of sterilization in 2007-08: Asa result of the above measures and the focusedstrategy at the Government of India level with closestate wise monitoring as also the opportunitiesafforded under NRHM in terms of plugging theloopholes and bolstering the demand side financingin the new revised compensation scheme, thesterilization has shown a healthy 9.4% increase over06 -07 in the country.
2.9 Health Insurance Scheme
The Ministry of Finance looks after the UniversalHealth Insurance Scheme, which was launched in2003. The National Common Minimum Programme[CMP] has made a commitment regarding HealthInsurance for the poor. Accordingly National RuralHealth Mission has also made commitment regardingeffective and viable risk pool and social healthinsurance to provide health security to the poor byensuring accessible, affordable, accountable andgood quality hospital care.
Under the National Rural Health Mission [NRHM], theMOHFW has set up a task force to explore new healthfinancing mechanisms. The terms of reference forthis task force include review of existing mechanismsto include health financing, human resourceimplications to manage health financing and riskpooling schemes, extent of subsidies required,ensuring equity and non-discrimination, feasibility invarious states, suggested design of pilots and sitesto launch community based health insurance models,and required modifications of existing structures tointroduce health financing schemes.
35
ANNUAL REPORT 2008-09
Based on the recommendations of the Task Force aFramework for developing health insuranceprogramme [some suggestions for the States] havebeen developed and this Ministry has advised theState/UT Governments to prepare Health Insurancemodels as per their local needs to be run on pilotbasis. Government of Andhra Pradesh, Rajasthan,Madhya Pradesh and Mizoram has sent proposalsfor funding the above pilot projects.
Andhra Pradesh:
Pilot project for implementation of Health InsuranceScheme from Andhra Pradesh for Anantapur,Mahboobnagar and Srikakulam Districts wasreceived with request for providing funds to the tuneof Rs.46.20 Crores. An amount of Rs.10 Crores wasagreed to as share of Union Government during theyear 2007-08. Government of Andhra Pradeshimplemented the Aarogyasri Community HealthInsurance Scheme in five more districts of Chittoor,East Goadavari, West Godavari, Nalgonda andRanga Reddy in Second Phase from 5th December2007. Proposal for extension of the Scheme to 15more districts during the year 2008-09 in threephases has been received from the StateGovernment.
The State Government has sought for Rs.10 Croresin the Programme Implementation Plan under NRHMfor the Health Insurance Scheme during the year2008-09 and the same has been approved by theMinistry.
Andhra Pradesh government felt a need in the stateto provide medical assistance to BPL families fortreatment of Critical Illness as Cancer, Kidney failure,Heart and Neuro etc requiring hospitalization.However, government facilities do not have requisitefacilities and specialist to meet the state widerequirement.
Many people approached the Government forfinancial assistance to meet the medical/surgicalexpenses. During the period from 14/05/04 to 26/
06/07, financial assistance to the tune of Rs 168.52crores were provided from CM's Relief fund for 55361cases to meet hospitalization expenses for suchpeople.
Based on this experience, Government of AndhraPradesh introduced a health Insurance scheme in 3districts w.e.f. 1/04/07 covering 25.27 lakhs BPLfamilies on pilot basis in Phase I for Heart, Cancer,Neuro Surgery, Renal diseases, Burns and PolyTrauma (not covered by MV Act) covering mostly 163surgical interventions through stand alone healthinsurance company with public private partnershipof health providers by paying premium @ Rs 330/-per family i.e. Rs 66 crores. Sum Insured is Rs. 1.50lakh with a buffer of Rs 50,000 per family.
Reviewing the scheme, the state has introduced thisscheme in Phase II by increasing the interventionsto 213 by open tender process in 5 districts w.e.f. 5/12/07 covering 48.23 lakhs BPL families through thesame insurer which quoted the lowest rate of Rs 220/- per family.
Encouraged with the responses, now state hasproposed to replicate the scheme in whole of thestate in phased manner i.e. Phase III - 34.86 lakhsBPL families in 5 districts from 5/04/08, Phase IV -35.46 lakhs BPL families in 5 districts from 05/07/08,Phase V - 40.92 lakhs BPL families in remaining 5districts from 05/10/ 08. Thereby state would becovering total 1.85 crores BPL families i.e. 6.55 croresBPL population.
The scheme is being implemented through a trustcalled "Aarogyasri Health Care Trust". BPL isidentified by biometric ration card issued by CivilSupplies department. Now trust is issuing the healthcard to all BPL families based on above data.
It is presumed that BPL families will avail benefitsunder the scheme and get cashless treatment in thenetwork hospital.
The Statistics of the scheme is given in next page:
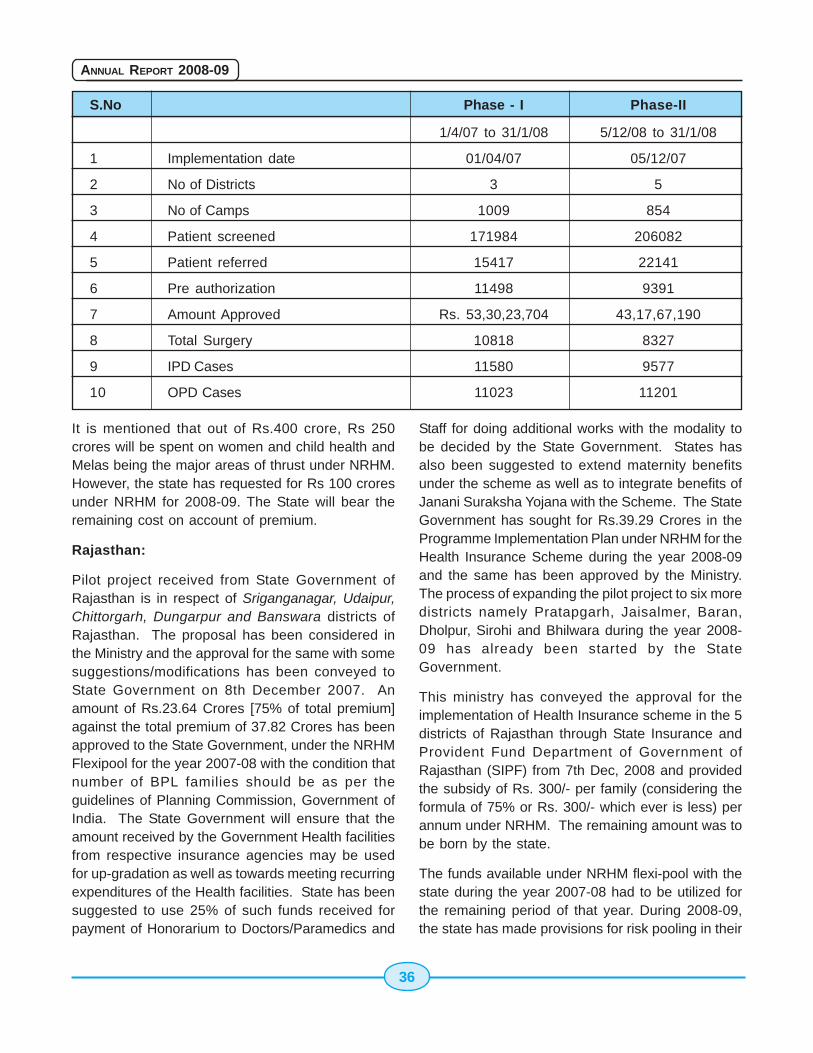
36
ANNUAL REPORT 2008-09
S.No Phase - I Phase-II
1/4/07 to 31/1/08 5/12/08 to 31/1/08
1 Implementation date 01/04/07 05/12/07
2 No of Districts 3 5
3 No of Camps 1009 854
4 Patient screened 171984 206082
5 Patient referred 15417 22141
6 Pre authorization 11498 9391
7 Amount Approved Rs. 53,30,23,704 43,17,67,190
8 Total Surgery 10818 8327
9 IPD Cases 11580 9577
10 OPD Cases 11023 11201
It is mentioned that out of Rs.400 crore, Rs 250crores will be spent on women and child health andMelas being the major areas of thrust under NRHM.However, the state has requested for Rs 100 croresunder NRHM for 2008-09. The State will bear theremaining cost on account of premium.
Rajasthan:
Pilot project received from State Government ofRajasthan is in respect of Sriganganagar, Udaipur,Chittorgarh, Dungarpur and Banswara districts ofRajasthan. The proposal has been considered inthe Ministry and the approval for the same with somesuggestions/modifications has been conveyed toState Government on 8th December 2007. Anamount of Rs.23.64 Crores [75% of total premium]against the total premium of 37.82 Crores has beenapproved to the State Government, under the NRHMFlexipool for the year 2007-08 with the condition thatnumber of BPL families should be as per theguidelines of Planning Commission, Government ofIndia. The State Government will ensure that theamount received by the Government Health facilitiesfrom respective insurance agencies may be usedfor up-gradation as well as towards meeting recurringexpenditures of the Health facilities. State has beensuggested to use 25% of such funds received forpayment of Honorarium to Doctors/Paramedics and
Staff for doing additional works with the modality tobe decided by the State Government. States hasalso been suggested to extend maternity benefitsunder the scheme as well as to integrate benefits ofJanani Suraksha Yojana with the Scheme. The StateGovernment has sought for Rs.39.29 Crores in theProgramme Implementation Plan under NRHM for theHealth Insurance Scheme during the year 2008-09and the same has been approved by the Ministry.The process of expanding the pilot project to six moredistricts namely Pratapgarh, Jaisalmer, Baran,Dholpur, Sirohi and Bhilwara during the year 2008-09 has already been started by the StateGovernment.
This ministry has conveyed the approval for theimplementation of Health Insurance scheme in the 5districts of Rajasthan through State Insurance andProvident Fund Department of Government ofRajasthan (SIPF) from 7th Dec, 2008 and providedthe subsidy of Rs. 300/- per family (considering theformula of 75% or Rs. 300/- which ever is less) perannum under NRHM. The remaining amount was tobe born by the state.
The funds available under NRHM flexi-pool with thestate during the year 2007-08 had to be utilized forthe remaining period of that year. During 2008-09,the state has made provisions for risk pooling in their

37
ANNUAL REPORT 2008-09
PIP for 2008-09 to the tune of Rs. 39.29 Crores andhas been approved for the 11 districts (5 earlier and6 new) under NRHM.
A total of 24452 claims were reported and an amountof Rs.10,16,67,517 was paid to government hospitalsup to August, 2008 against the premium of Rs.22,94,95,866 received by them in 4 installments upto August, 2008 including service tax.
SIPF has made an arrangement of risk sharing withICICI, Reliance and SIPF with the ratio of 45%: 45%;10% respectively from Dec, 07. The risk wastransferred based on the accepted share of 455:45% to ICICI and Reliance @ Rs. 375 per beneficiaryincluding service tax on 4 monthly installments @Rs.125 per installment. Two installment has beenpaid, the third installment has not been releasedwhich is due from August 08. In between State Govt.has invited the tenders for a health insurance schemeto be implemented in whole of the state and basedon the lowest quote received.
The SIPF has been paid @ Rs. 337 from July 2008including service tax. The scheme being implementedthrough SIPF will be merged with a scheme calledBhamashah Financial Improvement Scheme(BHIS) being introduced from 1st Oct, 08 by the Stateof Rajasthan in whole of the state. BhamashahFinancial Improvement Scheme (BHIS) is a schemeof financial inclusions based on banking services.Punjab National Bank and Bank of Baroda are thepartners of the scheme.
A tender for health insurance was invited for the entire33 district and contract has been awarded to ICICIbeing L-1. Rate quote is Rs. 337 including ST forproviding the health services on the lines of RSBYonly in 25 districts including the 11 districtsunder NRHM (5 old +6 new). It is also learnt thatMinistry of Labour, GOI has withdrawn theirscheme from the state as the implementationof Bhamashah Scheme is not in accordancewith the RSBY scheme. State is also in process ofoffering this scheme in the reaming 8 districts coveredunder RSBY.
In respect of contribution of NRHM, it was clarifiedthat the support will be 75% or Rs 300/- of the
premium which ever is the less for the remainingperiod of the policy in the year 2008-09, if formalapproval is given. A provision for the year 2009-10shall be required to be made in the PIP of 2009-10.
Madhya Pradesh:
A proposal was received from Government of MadhyaPradesh to introduce health insurance scheme forfamilies below poverty line in March 2007 to a groupcomprising of about 20 lakh BPL families from thetotal BPL population of about 43 lakhs in the ruralarea and about 13 lakhs in the urban areas on apilot basis. The Scheme was examined in this Ministryand Government of Madhya Pradesh was asked toprovide list of districts for operation of the schemeinitially should not be more than 4 to 5 districts withclearly stipulating contribution of the State forpayment of premium of the scheme. To begin with toreduce the cost of premium, State was suggested toavoid payment of transport expenses/out of pocketexpenses to the beneficiaries. Government ofMadhya Pradesh accordingly decided to introducethe Health Insurance Scheme on pilot basis in thefour districts of Ujjain, Gwalior, Indore, Jabalpur andhas requested this Ministry's formal approval for thesame. Since full details regarding the scheme asper framework suggested by the Ministry was notfurnished by the State Government, they wererequested to furnish the same and include theproposal in Programme Implementation Plan underNRHM for the year 2008-09.
The State Government has now proposed a SocialSecurity and Health Insurance Scheme viz. "DindayalAntyodaya Upchar Yojana" with 50% support andrequested for a support of Rs.1500 lakhs in theirProgramme Implementation Plan for the year 2008-09. NPCC in their meeting has approved an amountof Rs.1000 Lakhs for the scheme to be operatedthrough Rogi Kalyan Samities. No further details areavailable.
Mizoram:
Government of Mizoram has implemented "MizoramState Health Care Scheme" in the State from 1st April2008 for providing universal health insurance to allthe residents of Mizoram including APL population

38
ANNUAL REPORT 2008-09
but excluding Central, State and Public Sectoremployees. Government of Mizoram has requestedthis Ministry to provide grants to the tune of Rs.5.39Crores [Rs.4.90 Crores as premium @ Rs.700/- perfamily per year and Rs.0.49 Crores as administrativeexpenses]. The total population of the State hasbeen given as 1068953 with 202462 households outof which 69745 are BPL households with a populationof 384212. The proposal from Government ofMizoram has been examined in the Ministry andGovernment of Mizoram has been requested tofurnish certain clarifications before their request forgrant is considered by the Ministry.
Others States:
Proposal regarding taking up of pilot projects underthe Scheme were reflected in the ProgrammeImplementation Plans of NRHM for the year 2007-08by the States of Kerala, West Bengal, Assam,Haryana and Uttar Pradesh. These States havebeen reminded to submit their pilot projects for launchof Health Insurance Scheme for BPL families. Assam,Maharashtra, Madhya Pradesh, Rajasthan, AndhraPradesh, Jammu & Kashmir and Kerala Governmentshas included the Scheme in their ProgrammeImplementation Plan under NRHM for 2008-09 butdetails of the scheme have been sought fromrespective states.
Family Planning [Indemnity] Insurance Scheme:
The Government of India has launched FamilyPlanning Insurance Scheme w.e.f. 29.11.2005 toprovide compensation for failure of sterilization,medical complications arising out of sterilizationprocedure and in the most unlikely event of death.The insurance scheme also provides indemnity to thedoctors/health facilities in the Government and alsoaccredited NGO and private sector providers whoprovide sterilization facilities. This provision has beenmade because a number of doctors were facinglitigation on account of failure of sterilization etc.
The Indemnity Insurance Scheme provides forcompensation of Rs. Two lakh in case of death due tosterilization in hospital or within 7 days from the dateof discharge from the hospital, Rs. 50,000 for deathdue to sterilization within 8-30 days from the date of
discharge from the hospital, and Rs. 30,000 for failureof Sterilization (limited to the actual expenditure) formedical complications. The indemnity cover todoctors/health facilities is for a maximum amount ofRs.2 lakh per doctor/health facility per case up to amaximum of 4 cases in a year. The cover also includesthe legal costs and actual modality of defending theprosecuted doctor/health facility in court which wouldbe borne by the insurance scheme within limitsmentioned in the policy.
This scheme is applicable to all States/U.Ts.Government of India has paid entire premium for theinsurance policy to the Oriental Insurance Co Ltd.for the period November 2005- December 2006 andDecember 2006-December 2007. The Policy hasnow been renewed with ICICI Lombard for the periodup to 31.12.2008 States does not have to incur anyexpenditure under this scheme. The InsuranceCompany will make payment against the claims ofacceptors of sterilization directly to the acceptorswithout any hassle.
Rashtriya Swasthya Bima Yojana Scheme[RSBY]:
Recently a Health Insurance Scheme [RashtriyaSwasthya Bima Yojana Scheme] for the Workers ofUnorganized Sector has been introduced by Ministryof Labour and a Technical Cell is being set up forproviding assistance to the States for implementationof the Scheme.
Recently Ministry of Labour & Employment hasannounced the "Rashtriya Swasthya Bima Yojana(National Health Insurance Scheme)" for providinghealth insurance cover to Below Poverty Line workersin the unorganized sector and their families. Thescheme is on similar lines as that of Health InsuranceScheme on pilot basis being taken up in selecteddistricts of some states under NRHM. While givingour comments on this health insurance scheme, itwas mentioned that the pilot schemes under NRHMwould be continued to be funded. The details of the"Rashtriya Swasthya Bima Yojana" (copy enclosed)are as under:
� The sum insured under this scheme wouldbe Rs.30,000 per family per annum on a
39
ANNUAL REPORT 2008-09
floater basis, which would be available forhospitalization of most common illnesses withfew exceptions.
� Contribution by Government of India: 75% ofthe estimated annual premium of Rs.750/-,subject to a maximum of Rs.565/- per familyper annum.
� Contribution by the respective StateGovernments: 25% of the annual premium,as well as any additional premium in caseswhere the total premium exceeds Rs.750/-.
� The beneficiary would pay Rs.30/- per annumas registration/renewal fee.
� Any administrative and other related cost ofadministering the scheme in each State shallbe borne by the respective StateGovernments.
� The scheme would be implemented in aphased manner covering 20% districts ofcountry each year starting 2008-09 and thuscovering all districts in a period of five years.
� Each BPL family would be issued Smart Cardfor the purpose of identification as well asfor keeping details about the benefits availedand expenditure.
� After the approval of the project, the StateGovernments shall, from time to time, intimatethe Union Government about the payment ofthe premium to the Insurers. The UnionGovernment, on receipt of this information,shall release its share of premium.
This Ministry is supporting Ministry of Labour inprovision of technical support as well as throughparticipation in Advisory & Approval Committee of thatMinistry. The Scheme has been taken-up from thefinancial year 2008-09.
2.10 Health Minister's DiscretionaryGrant
Financial Assistance to the poor and indigent patientsis given from the Health Minister's Discretionary Grantto defray a part the expenditure on hospitalization/treatment in Govt. Hospital as these patients cannotbe considered for financial assistance under
Rashtiya Arogya Nidhi due to income of above povertyline, but less than Rs.50,000/- per annum. Duringthe year 2007-08, financial assistance totalingRs.39.23 lakh was given to 210 patients. A provisionof Rs.100.00 lakh has been made during the currentfinancial year i.e. 2008-09 and till October, 2008 asum of Rs. 13.67 lakh has been released to 72patients.
2.11 Rashtriya Arogya Nidhi
Rashtriya Arogya Nidhi was set up under Ministry ofHealth & Family Welfare in 1997 to provide financialassistance to patients, living below poverty line, whoare suffering from major life threatening diseases toreceive medical treatment in Government Hospitals.Under the scheme of Rashtriya Arogya Nidhi, grants-in-aid to also provided to State Governments forsetting up State Illness Assistance Funds. Such fundshave been set up by the Governments of AndhraPradesh, Bihar, Chhattisgarh, Goa, Gujarat, HimachalPradesh, Jammu & Kashmir, Karnataka, Kerala,Madhya Pradesh, Jharkhand, Maharashtra, Mizoram,Rajasthan, Sikkim, Tamil Nadu, Tripura, West Bengal,Uttrakhand, Haryana, Punjab NCT of Delhi andPondicherry. The Grants-in-aid released to thesefunds have been shown in the Annexure. OtherStates/Union Territories have been requested to setup the Fund, as soon as possible.
Applications for financial assistance up to Rs.1.5 lakhare to be processed and sanctioned by the respectiveState Illness Fund. Applications for assistancebeyond Rs.1.50 lakh and also of those where StateIllness Fund has not been set up are processed inthis Department for release from the RashtriyaArogya Nidhi.
In order to provide immediate financial assistance,to the extent of Rs.1,00,000/- per case, to criticallyill, poor patients who are living below poverty lineand undergoing treatment, the MedicalSuperintendents of Dr. RML Hospital, SafdarjungHospital, Smt.Sucheta Kriplani Hospital, All IndiaInstitute of Medical Sciences, New Delhi, PGIMER,Chandigarh, JIPMER, Pondicherry, MINHANS,Bangalore, CNCI, Kolkatta, Sanjay Gandhi PostGraduate Institute of Medical Sciences,Lucknow,RIMS, Imphal, NEIGRIHMS, Shillong and CIP,
40
ANNUAL REPORT 2008-09
Ranchi have been provided with a revolving fund ofRs.10-40 lakhs. The revolving fund is replenishedafter its utilization. For cases requiring financialassistance above the 1,00,000/- (Rs. one lakh only)per case the applications are processed in theDepartment of Health & Family Welfare through aTechnical Committee headed by Director General,DGHS before being considered for approval by aduly constituted Managing Committee with Hon'bleMinister for Health & Family Welfare as the Chairman.During the year 2007-08, financial assistance totalingRs.342.00 lakh was given directly to 212 patientsunder Rashtriya Arogya Nidhi (Central fund.).
2.12 Medical Tourism in India
Medical tourism has gained momentum in India overthe past few years with the emergence of new high-quality healthcare service providers. India is seeinga surge of patients from developed countries as wellas from countries in Africa and South and West Asia.The emergence of low-cost, high value specialistmedical care territories in India has been noteworthy.
Meetings between Union Ministers for Healthand Tourism:
The first high level meeting between the Minister ofHealth and Family Welfare and the Minister of Statefor Tourism was held on the 5th November 2004.Various decisions like accreditation of hospitals, spasand Ayurvedic Systems, price range within whichvarious treatments would be made availablemarketing of hospitals were taken in the meeting.
The second meeting was held on the 15th March2005. Some of the major decisions taken in themeeting are as under.
o Reputed institutions like CII, FICCI, IMA,FOGSIE etc. would bring out websitescontaining information on good hospitals,giving advice to exercise due diligence aboutthe cost and quality before seeking healthcare from any hospital/institution.
o Ministry of Tourism will bring out brochure,CDs etc. to promote Medical Tourism.
Introduction of M-Visa by Ministry of HomeAffairs:
A new category of "Medical Visa" [M-Visa] has beenintroduced, which can be given for specific purposesto foreign tourists coming to India for medicaltreatment. This type of visa is granted for seekingmedical attendance only in reputed/recognizedspecialized hospitals/treatment centers in thecountry.
Other Initiatives:
Ministry of Tourism, in close coordination with theMinistry of Health and Family Welfare has initiatedseveral measures to promote Medical Tourism.Some of the major initiatives are as under: -
� Indian Health Care Federation, a Non-Governmental Organization affiliated to theConfederation of Indian Industries, on adviceby Government, has prepared a guide onselected Indian Hospitals of the country forhealth tourism purposes.
� Brochures, CDs and other publicity materialsto promote Medical and Health tourism havebeen produced and have been widelycirculated for publicity in target markets.
� Guidelines for accreditation of Ayurvedic andPanchkarma Centres have been finalized andcirculated to all State Governments forimplementation.
� Medical and Health Tourism has beenspecifically promoted at various internationalplatforms such as World Travel Mart, London,ITB Berlin, Arabian Travel Mart.
� Yoga/Ayurveda/Wellness has been promotedover the last two years in the print, electronic,internet and outdoor medium under theMinistry's "Incredible India campaign".
� Brochure, CDs on Body, Mind and Soulcovering the traditional system of medicinehave been produced and circulatedextensively.
41
ANNUAL REPORT 2008-09
2.13 Pre-conception and Pre-NatalDiagnostic Techniques (Prohibi-tion of Sex Selection Act, 1994)
Sex ratio (number of females per thousand males) isone the most important indicator used for study ofpopulation characteristics. Declining trend in sexratio has been a matter of concern for all in thecountry. Sex ratio in India has declined over thecentury from 972 in 1901 to 927 in 1991. However,it was 933 in 2001.
In contrast the child sex ratio for the age group of 0-6 years in 2001 is 927 girls per thousand boysagainst 945 recorded in 1991 Census.
The Census 2001 figures further reveal that the childsex ratio is comparatively lower in the affluent regions,i.e., Punjab (798), Haryana (819), Chandigarh (845),Delhi (868), Gujarat (883) and Himachal Pradesh(896). State/UT wise Sex ratio and Child Sex ratio asper 1991 and 2001 Census is enclosed.
Some of the reasons commonly put forward to explainthe consistently low levels of sex ratio are sonpreference, neglect of the girl child resulting in highermortality at younger age, female infanticide, femalefoeticide, higher maternal mortality and male bias inenumeration of population. Easy availability of thesex determination tests and abortion services mayalso be proving to be catalyst in the process, whichmay be further stimulated by pre-conception sexselection facilities.
Sex determination techniques have been in use inIndia since 1975 primarily for the determination ofgenetic abnormalities. However, these techniqueswere widely misused to determine the sex of thefoetus and subsequent abortions if the foetus wasfound to be female.
In order to check female foeticide, the Pre-natalDiagnostic Techniques (Regulation and Preventionof Misuse) Act, 1994, was brought into operation from1st January, 1996. The Pre-natal DiagnosticTechniques (Regulation and Prevention of Misuse)Act, 1994 has since been amended to make it morecomprehensive. The amended Act and Rules cameinto force with effect from 14.2.2003 and the PNDT
Act has been renamed as "Pre-conception and Pre-Natal Diagnostic Techniques (Prohibition of SexSelection) Act, 1994" (PC & PNDT Act, 1994) tomake it more comprehensive.
The PC & PNDT Act, 1994 provides for:
� Prohibition of sex selection, before and afterconception (Sec 3A of the Act)
� Regulation of prenatal diagnostic techniques(e.g. amniocentesis and ultrasonography) fordetection of genetic abnormalities, byrestricting their use to registered institutions.The Act allows the use of these techniquesonly at a registered place for a specifiedpurpose and by a qualified person, registeredfor this purpose. (Sec 4 of the Act)
� Prevention of misuse of such techniques forsex selection before or after conception. (Sec6 of the Act)
� Prohibition of advertisement of any techniquefor sex selection as well as sex determination(Sec 22 of the Act)
� Prohibition on sale of ultrasound machinesto persons not registered under this Act (Rule3A, inserted vide GSR, 109 (e) dt 14-2-2003)
� Punishment for violation of provisions of theAct (Sec 23) as under:
o Imprisonment up to 3 years and fine upto Rs. 10,000.
o For any subsequent offences, he/shemay be imprisoned up to 5 yearsand fined up to Rs. 50,000 / 100,000.
o The name of the registered medicalpractitioner is reported by theAppropriate Authority to the State MedicalCouncil concerned for taking necessaryaction including suspension of theregistration if the charges are framed bythe court and till the case is disposed off.
Other salient features of the Act are:
� The Central Supervisory Board (CSB),
42
ANNUAL REPORT 2008-09
constituted under Section 7 of the (PC &PNDT Act, 1994), under the Chairmanshipof Minister for Health and Family Welfare hasbeen empowered for monitoring theimplementation of the Act.
� State level Supervisory Boards on the linesof CSB has been introduced for monitoringand reviewing the implementation of the Actin States/UTs.
� The State/UT level Appropriate Authority havebeen made a multi member body for betterimplementation and monitoring of the Act inthe States.
� Appropriate Authorities are empowered withthe powers of Civil Court for search, seizureand sealing the machines, equipments andrecords of the violators of law includingsealing of premises and commissioning ofwitnesses.
� It has been made mandatory for the GeneticClinics/Centres, etc., to maintain properrecords in respect of the use of ultrasoundmachines and other equipments capable ofdetection of sex of foetus and also in respectof tests and procedures that may lead to pre-conception selection of sex.
As per the reports received from the States and UTs35661 bodies using ultrasound, image scanners etc.have been registered under the Act. 367 ultrasoundmachines have been sealed and seized for violationof the law. As on 31.3.2009, there were 464 ongoingcases in the Courts/Police for various violations ofthe law. Though most of the cases are for non-registration of the centre/clinic and non-maintenanceof records, 99 cases relate to determination anddisclosure of the sex of the foetus in different theStates. 32 cases exist against people who havegiven advertisement about facilities of pre-conception/pre-natal sex selection. The concernedState governments are regularly requested to takeeffective measures for speedy disposal of theongoing cases.
Action taken for implementation of the Act:
� Constitution of National Inspection &Monitoring Committee (NIMC):
For taking stock of the ground realities byfield visits to the problem States. During2006-08, the Committee has visited the Stateof Delhi, Haryana, Maharashtra, UP,Rajasthan, Orissa, Karnataka, Kerala, H.P.and Punjab.
� Constitution of National Support andMonitoring Cell (NSMC) with fundingfrom UNFPA:
For effective implementation of the Act,including formulation of modules forapprehending by the Appropriate Authoritiesthe persons committing female foeticide/abetting female foeticide.
� Frequently Asked Questions (FAQs)
The Ministry of Health and Family Welfare,in collaboration with the United NationsPopulation Fund (UNFPA), have developed'Frequently Asked Questions' about the PNDTAct which will be useful to the lay persons,medical community and to the AppropriateAuthorities in understanding the provisionsof the Act for better implementation.
� The National Level Meeting on 'Save the GirlChild' held on 28.4.2008 at Vigyan Bhawan,New Delhi, was inaugurated by Dr.Manmohan Singh, hon'ble Prime Minister ofIndia, in the presence of the hon'ble UnionMinister of Health & F.W., hon'ble UnionMinister of State (I/C) for Women & ChildDevelopment, hon'ble Minister of State forHealth & F.W.. The large turnout of hon'bleHealth Ministers, Members of Parliament andsenior Health officers from the Central andState/UT Governments and representativesof various organisations active in the areaof Child welfare at the daylong fruitfuldeliberations of the National Meet lent thenecessary impetus to the 'Save the GirlChild' mission.
43
ANNUAL REPORT 2008-09
All the State/UT Governments have been requestedto replicate such a meeting in their respective States/UTs.
� Website on PC & PNDT:
In addition to the Union Health & F.W.Ministry's website, (www.mohfw.nic.in), anindependent website, 'pndt.gov.in' for PNDTDivision was launched by the hon'ble UnionMinister of Health & F.W. on 28.4.2008. Thiswebsite, in addition to containing all therelevant information relating to PNDT Act,Rules., Regulations and activities, enablesonline filing of data right down from Clinics(including submission of From-F' online bythe Clinics), in the field to the District andState level and their retrieval at the District,State and National levels. An exercise is onto impart training to the user groups on theuse of the website in a phased mannerbeginning with the focused states. TheAppropriate Authorities of UT of Chandigarh,NCT of Delhi, Himachal Pradesh, Gujarat,Rajasthan, Punjab, Haryana, Maharashtraand U.P. have so far been imparted training.This training programme is being conductedby the experts from National InformaticsCentre.
� Toll Free Telephone:
Along with the above said PNDT Website, a'Toll Free Telephone' was also launched bythe hon'ble Union Minister of Health & F.W.on 28.4.2008 to enable the public to seekgeneral information relating to PC & PNDTAct & the Rules framed thereunder and tolodge complaint against any violators of theAct. However, this service is temporarilysuspended pending resolution of certainoperational details.
� Awareness Generation:
Various activities have been undertaken tocreate awareness against the practice of pre-natal determination of sex and femalefoeticide through Radio, Television, and print
media units. Workshops and seminars arealso organized through VoluntaryOrganizations at State/regional/district/blocklevels to create awareness against this socialevil. Cooperation has also been sought fromreligious / spiritual leaders, as well as medicalfraternity to curb this practice. TheGovernment of India has launched 'Save theGirl Child Campaign' with a view to lessenson preference by highlighting achievementsof young girls. Shri Kapil Dev, former Captainof the Indian national Cricket Team, has beennominated as the Brand Ambassador for thecampaign.
� Gender Testing/Sex Determination Kits:
The Government is endeavouring to containthe adverse impact of the Gender Testing/Sex Determination Kits being advertised onthe internet and their purchase onlinethrough inter-ministerial consultations
2.14 Improvement in the Quality ofHealth Care
The improvement in the quality of health care overthe years is reflected in respect of some basicdemographic indicators (see Table I below). TheCrude Birth rate (CBR) declined from 40.8 births perthousand population in 1951 to 29.5 in 1991 andfurther to 23.1 in 2007. Similarly there was a sharpdecline in Crude Death Rate (CDR) which decreasedfrom 25.1 deaths per thousand population in 1951to 9.8 in 1991 and further to 7.4 in 2007. Also, theTotal Fertility Rate (Average number of children likelyto be born to a woman between 15-44 years of age)has decreased from 6.0 in 1951 to 2.8 in 2006 asper the estimates from the Sample RegistrationSystem (SRS) of Registrar General India (RGI),Ministry of Home Affairs.
The Maternal mortality Rate has also declined from437 per one lakh (100,000) live births in 1992-93 to254 in (2004-06) SRS, according to the Reportbrought out by RGI. Infant Mortality Rate, whichwas 110 in 1981, has declined to 55 per 1000 livebirths in 2007. Child Mortality Rate has alsodecreased from 57.3 in 1972 to 17.0 in 2006.
44
ANNUAL REPORT 2008-09
Table 1 : Achievement of Family Welfare Programme
Sl. No. Parameter 1951 1981 1991 Current level
1 Crude Birth Rate (Per 1000 Population) 40.8 33.9 29.5 23.1 / (2007)
2 Crude Death Rate (Per 1000 Population) 25.1 12.5 9.8 7.4 / (2007)
3 Total Fertility Rate (Per women) 6.0 4.5 3.6 2.8 / (2006)
4 Maternal Mortality Rate NA NA 437 (1992-93) 254(Per 100,000 live births) NFHS (2004-06) SRS
5 Infant Mortality Rate (Per 1000 live births) 146 110 80 55 (2007)(1951-61)
6 Child (0-4 years) Mortality 57.3 41.2 26.5 17.0 $(2006)Rate per 1000 children (1972)
7 Couple protection Rate (%) $ 10.4 22.8 44.1 46.7 $ (2006)(1971)
Source: (1) Office of Registrar General, Ministry of Home Affairs. India.
$ (2) Family Welfare Statistics-2006, Ministry of Health and Family Welfare.
Family Planning Methods. The total number ofacceptors of different Family Planning methodsenrolled in the country during the year 2007-08 was41.47 million. Table-2 below summarizes the position
in regard to family planning achievements during2007-08 and 2008-09 (up to Nov.2008) at All IndiaLevel.
Table 2 : Family Planning Acceptors by methods
(Figures in millions)Sl. Methods Achievement* Achievement*
No. April2007- 2008-09 2007-08March08 (April 2008- (April 2007-
Nov-2008) Nov-2007)
1 2 3 4 5
1. Sterilisation 5.01 2.32 2.14
2. IUD Insertions 6.07 3.9 3.72
3. Condom Users(Eq.) 20.67$ 18.30 18.06$
i. Under Free Distribution 10.81 9.82 9.74Scheme(Eq.)
ii. Under Commercial 9.85 8.48 8.31Distribution scheme(Eq.)
4. Oral Pill Users(Eq.) 9.72 8.21$ 8.45
i. Under Free distribution 5.33 4.82 4.84Scheme (Eq.)
ii. Under Commercial 4.39 3.38 3.62Distribution Scheme(Eq.)
Total 41.47 32.73 32.78
Eq. : Equivalent $ : May not tally with the total due to rounding off. * : Provisional figures
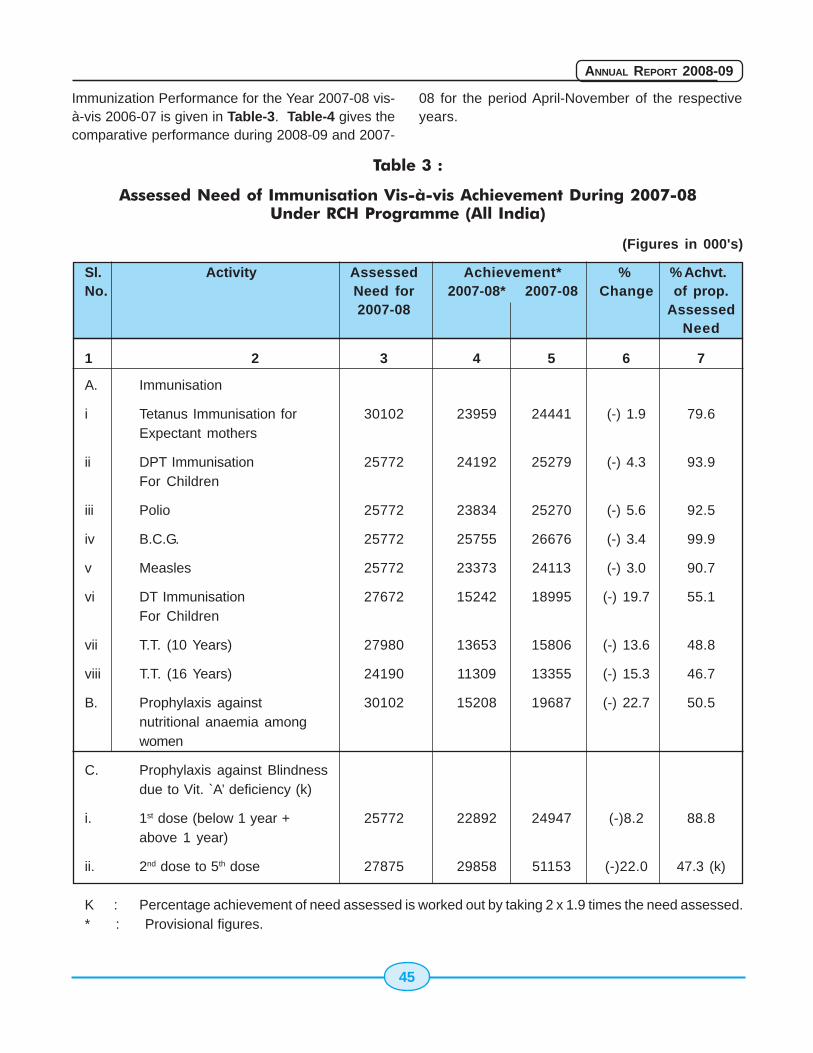
45
ANNUAL REPORT 2008-09
Immunization Performance for the Year 2007-08 vis-à-vis 2006-07 is given in Table-3. Table-4 gives thecomparative performance during 2008-09 and 2007-
08 for the period April-November of the respectiveyears.
Table 3 :
Assessed Need of Immunisation Vis-à-vis Achievement During 2007-08Under RCH Programme (All India)
(Figures in 000's)
Sl. Activity Assessed Achievement* % % Achvt.No. Need for 2007-08* 2007-08 Change of prop.
2007-08 AssessedNeed
1 2 3 4 5 6 7
A. Immunisation
i Tetanus Immunisation for 30102 23959 24441 (-) 1.9 79.6Expectant mothers
ii DPT Immunisation 25772 24192 25279 (-) 4.3 93.9For Children
iii Polio 25772 23834 25270 (-) 5.6 92.5
iv B.C.G. 25772 25755 26676 (-) 3.4 99.9
v Measles 25772 23373 24113 (-) 3.0 90.7
vi DT Immunisation 27672 15242 18995 (-) 19.7 55.1For Children
vii T.T. (10 Years) 27980 13653 15806 (-) 13.6 48.8
viii T.T. (16 Years) 24190 11309 13355 (-) 15.3 46.7
B. Prophylaxis against 30102 15208 19687 (-) 22.7 50.5nutritional anaemia amongwomen
C. Prophylaxis against Blindnessdue to Vit. `A’ deficiency (k)
i. 1st dose (below 1 year + 25772 22892 24947 (-)8.2 88.8above 1 year)
ii. 2nd dose to 5th dose 27875 29858 51153 (-)22.0 47.3 (k)
K : Percentage achievement of need assessed is worked out by taking 2 x 1.9 times the need assessed.* : Provisional figures.
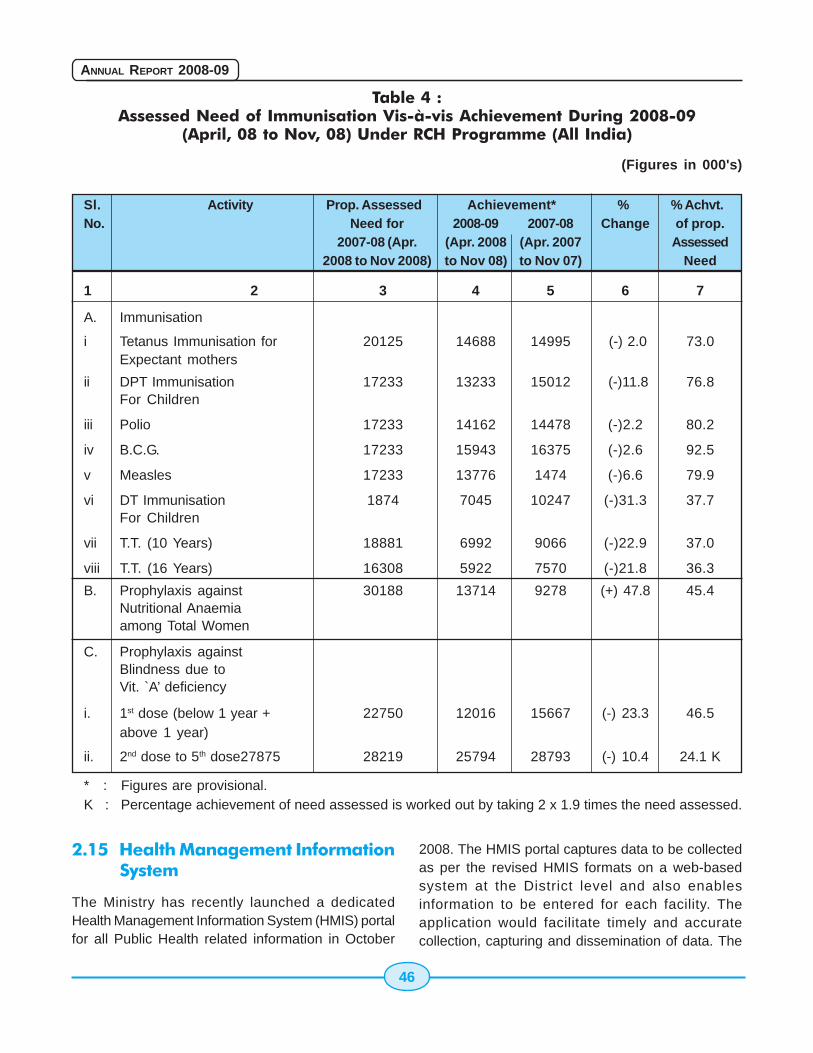
46
ANNUAL REPORT 2008-09
Table 4 :Assessed Need of Immunisation Vis-à-vis Achievement During 2008-09
(April, 08 to Nov, 08) Under RCH Programme (All India)
(Figures in 000's)
Sl. Activity Prop. Assessed Achievement* % % Achvt.No. Need for 2008-09 2007-08 Change of prop.
2007-08 (Apr. (Apr. 2008 (Apr. 2007 Assessed2008 to Nov 2008) to Nov 08) to Nov 07) Need
1 2 3 4 5 6 7
A. Immunisation
i Tetanus Immunisation for 20125 14688 14995 (-) 2.0 73.0Expectant mothers
ii DPT Immunisation 17233 13233 15012 (-)11.8 76.8For Children
iii Polio 17233 14162 14478 (-)2.2 80.2
iv B.C.G. 17233 15943 16375 (-)2.6 92.5
v Measles 17233 13776 1474 (-)6.6 79.9
vi DT Immunisation 1874 7045 10247 (-)31.3 37.7For Children
vii T.T. (10 Years) 18881 6992 9066 (-)22.9 37.0
viii T.T. (16 Years) 16308 5922 7570 (-)21.8 36.3
B. Prophylaxis against 30188 13714 9278 (+) 47.8 45.4Nutritional Anaemiaamong Total Women
C. Prophylaxis againstBlindness due toVit. `A’ deficiency
i. 1st dose (below 1 year + 22750 12016 15667 (-) 23.3 46.5above 1 year)
ii. 2nd dose to 5th dose27875 28219 25794 28793 (-) 10.4 24.1 K
* : Figures are provisional.K : Percentage achievement of need assessed is worked out by taking 2 x 1.9 times the need assessed.
2.15 Health Management InformationSystem
The Ministry has recently launched a dedicatedHealth Management Information System (HMIS) portalfor all Public Health related information in October
2008. The HMIS portal captures data to be collectedas per the revised HMIS formats on a web-basedsystem at the District level and also enablesinformation to be entered for each facility. Theapplication would facilitate timely and accuratecollection, capturing and dissemination of data. The

47
ANNUAL REPORT 2008-09
portal would help in converting the data locally intouseful information, management indicators, districtprofiles, trends which could be displayed graphicallyin reports.
The portal would be generating unique analyticalreports using Data Warehousing platform for finetuning policy initiatives. Information could be madeavailable quickly and regularly to decision makersand other users in the form of specific and tailoredmonthly, quarterly and annual reports.
2.16 District Level Household SurveyIII
The District Level Household Surveys (DLHS) wereinitiated in 1997 with a view to assess the utilizationof services provided by government health facilitiesand people's perception about the quality of services.The District Level household Survey (DLHS -3) isthe third in the series of the district surveys, precededby DLHS-1 in 1998-99 and DLHS 2 in 2002-04. DLHS3, like other two rounds, is designed to provideestimates on important indicators on maternal andchild health, family planning and other reproductivehealth services. In addition, DLHS 3 providesinformation on important interventions of NationalRural Health Mission (NRHM).
DLHS -3 interviewed ever-married women (age 15-49) and never married women (age 15-24).DLHS-3 adopts a multi-stage stratified samplingdesign and sampled households representing adistrict vary from 1000 to 1500.
The uniform bilingual questionnaires, both in Englishand in local language, were used in DLHS-3 viz.,Household, Ever Married Women (age 15-49),Unmarried Women (age 15-24), Village and Healthfacility questionnaires. In the householdquestionnaire, information on all members of thehousehold and the socio-economic characteristicsof the household, assets possessed, number ofmarriages and deaths in the household since January2004, etc. was collected. In case of female deaths,attempts were made to assess maternal death. Thehousehold questionnaire also collected informationon respondent's knowledge about messages relatedto various government health programmes being
spread through media and other sources. The evermarried women's questionnaire consisted of sectionson women's characteristics, maternal care,immunization and child care, contraception andfertility preferences, reproductive health includingknowledge about HIV/AIDS. The unmarried women'squestionnaire contained information on hercharacteristics, family life education and age atmarriage, reproductive health-knowledge andawareness about contraception, HIV / AIDS, etc. Thevillage questionnaire contained information onavailability of health, education and other facilities inthe village and whether the health facilities areaccessible throughout the year. For the first time,population-linked facility survey has been conductedin DLHS-3. In a district, all Community Health Centres(CHCs) and District Hospital (DH) were covered.Further, all Sub-centres (SC) and Primary HealthCentres (PHC) which were expected to serve thepopulation of the selected PSU were also covered.There were separate questionnaires for SC, PHC,CHC and DH. They broadly include questions oninfrastructure, human resources, supply of drugs &instruments, and performance.
The survey was conducted in two phases, startingfrom December, 2007 with field work of each phaselasting for about four months. The second phasestarted immediately after the first phase in May, 2008.The preliminary results for the key findings of the 27States have been released in Dec 2008 in the formof fact sheets.
2.17 Population Research Centres
The Ministry established 18 Population ResearchCentres (PRCs) in various institutions in the countrywith a view to carry our research on various topicspertaining to population stabilization, Demographicand other Health related programs. While 12 of thesePRCs are located in Universities, the remaining sixare located in institute of national repute. The Ministryof Health & Family Welfare provide 100% financialgrant-in-aid to all PRCs as on a year-to-year basistowards salaries of staff, books and journals, TA/DA,data processing / stationary/ contingency etc., andother infrastructure requirement.
48
ANNUAL REPORT 2008-09
Studies conducted by the Population ResearchCentres in the year 2007-08: During the year 2007-08 the studies completed by the PopulationResearch Centres (PRCs) on some of the importanttopics of research including the studies assigned bythe Ministry are given below.
List of studies undertaken by PRCs during 2007-08
1) Changing child population and Health careinfrastructure in Karnataka.
2) Role of NGOs in the Presentation of HIV/AIDS- a Study in Karnataka.
3) Awareness of HIV/ AIDS in Karnataka:Analysis of RCH- II Data
4) Determinants of Maternal and ChildHealth(MCH) care service use : ARegional analysis in Karnataka
5) Effects of Population on Environmentaldegradation with special reference to India.
6) Economic Growth and Public Health in India.
7) A study of Reproductive Health problemsamong men and women in urban slums withspecial reference to sexually transmittedinfections.
8) Maternal mortality in India : levels,differentials and causes
9) Reproductive and sexual health of youngunmarried women and men in urban slums
10) Assessment of access and quality of healthservices in relation to the district's RCH Statusin Gujarat.
11) Emerging causes and determinants ofMaternal mortality in India.
12) Current and Future Health scenario vis-a visDevelopment in Major States of India.
13) Incidence of Reproductive tract infection andsexually transmission diseases in India: levelsand differentials.
14) Evaluation Study on Impact of Existing IECActivities on Poor and Marginalised Groupson RCH Issues.
15) Monitoring of the District Level HouseholdSurvey (DLHS) - 3
16) Supporting the Elderly in India: Someevidence of gender disparity.
17) Women, Marriage and Mobility: Somepatterns , issues and perspectives inInternational out- migration from IndianPunjab.
18) National Family Health Survey-III Punjab; aPreliminary Welfare indicators.
19) National Family Health Survey-III Haryana; aPreliminary Welfare indicators.
20) Pre Project Survey of Border AreaDevelopment Programme in HimachalPradesh.
21) Health Care Services in Punjab: findings frompatient satisfaction survey.
22) Demographic Field Surveys RecentEvidence from Punjab and Haryana.
23) The Prevalence of Non-InstitutionalDeliveries in Rural Punjab: Why WomenPersist from Home Deliveries?
24) DSHS-RCH Round II Phase II
25) Unmet need for family planning in Bihar
26) National Family Health Survey
27) Gender, Environment and Collective Actionin India and Nepal
28) Is caring for Elder an Act of Altruism ? SomeEvidence based on a Household Survey inDelhi.
29) Unmet and Met needs for contraception inIndia
30) Women's Reproductive Morbidity andTreatment seeking behaviour in India
49
ANNUAL REPORT 2008-09
31) Demographic Transition in India
32) Challenges for the NRHM: A Study of recenttrends in Demographic and Health indicatorsin Selected states of India.
33) Missing issues in the Imbalance of Child SexRatio : A Study on Northwestern India
34) Immunization Coverage of Children in India
35) Health & Heights : Rural facilities in HimalayanIndia
36) Childhood Mortality and Health in India
37) Birth Rate Trends in India: A DecompositionAnalysis
38) World Population Growth during 1950-2000.
39) Assessing the patterns and Drivers ofmigration / mobility of Sex workers (Femalesand Hijras) and male migrant workers in themove and examining the links with HIV Risks.
40) Family Health International
41) General population survey of STS/ IDS inBelgaum and Bellary districts- Karnataka
42) A study on the role of Panchayat RajInstitution in Implementing RCH program inTamil Nadu.
43) A study on co-ordination between AnganwadiWorkers and Village Health Nurse indelivering Adolescent Reproductive HealthServices at village level in Tamil Nadu.
44) District level comparative study on householdamenities of North Eastern of India
45) Maternal and Child Health care in someselected districts of Assam: Evidence fromRCH-I and RCH-II
46) Evaluation of functioning of AIE Centres withfocus on Retention of Mainstream childrenin formal school in Assam.
47) Level of Deviation in the perform of Familyplanning program of Assam and some North
Eastern States from the well performingStates of India and also from NationalAverage.
48) Rural and Urban divide in utilization ofReproductive and Child Health Services inUttar Pradesh.
49) Fertility trends in Uttar Pradesh: An analysisbased on Census Data
50) Routine Immunization in Uttar Pradeshcoverage and differentials.
51) Evaluation of 24 hours Delivery ServicesScheme in Uttar Pradesh.
52) Demographic profile of Bihar
53) Poverty and demographic indicators in Bihar: An evidence from RCH Results
54) Population and Health in Bihar
55) Maharatna, Arup, Population, Economy andSociety in West Bengal since the 1970sJournal of Development Studies
56) Children's work activities in a PeasantHousehold: Epitome of Neo-classicalRationality or Else ?
57) Monitoring of District Level House HoldSurvey-3( Phase-I) on Reproductive andChild Health in Karnataka, Goa an MadhyaPradesh.
58) External Evaluation of Continuing EducationProgramme in Mysore Districts
59) Representation of Social Groups in HigherEducation: An Analysis of NSSO 55th Round.
60) Are Fertility differentials by Social Groupsconverging in Andhra Pradesh
61) Quality of Health Care in Public HealthProgrammes: A Review.
62) Workshop on "Census of India 2001: DataDissemination".
63) A follow Up study of Women Undergoing
50
ANNUAL REPORT 2008-09
Ultrasound Tests in two districts of Haryana:Panchkula and Ambala
64) Reproductive and Child Health : RapidCluster Survey in Haryana
65) Adolescent Fertility and Utilization of HealthFacilities in Haryana
66) Assessment of Janani Express Scheme inMadhya Pradesh.
67) Assessment of Janani Suraksha Yojana: Apilot study in Sagar District.
68) Factors influencing underutilization ofimmunization services in Madhya Pradesh
69) Estimation of Demographic indicators basedon Census 2001 data for Madhya Pradesh-Part1. Study on internal Migration in MadhyaPradesh.
70) Strategies for Strengthening Rural HealthCare PRIs and community involvement.
71) Population Dynamics in district Chamba inHimachal Pradesh
72) Reproductive Morbidity among women indistrict Chamba.
73) Rural Health infrastructure and its utilizationin district Chamba, Himachal Pradesh.
74) Evaluation of centrally sponsored scheme inJammu and Kashmir
75) Unintended pregnancies in Jammu andKashmir State : Levels and correlatesServices in Jammu and Kashmir.
76) Reproductive Health of women Labourers: Acase study of cashew workers in KollamDistrict
77) Interventions of Juniors Public Health Nurses(JPHNs) on Matters regarding Reproductiveand Child Health: A Beneficiary Perspective.
78) Reproductive Health problems of adolescentsand youth in selected districts of Kerala
79) Fertility and contraceptive use in MalappuramDistrict of Kerala
80) Migration and its impact on Child Health andstatus of women: Evidences from the Stateof Kerala
81) A study on Maternal Mortality in Kerala
82) Scenario of crimes against women in Indiaand Kerala.
83) Awareness about AIDS in slums dwellers ofUdaipur districts
84) Role of ASHA in promoting safe delivery inRajasthan
85) Problem of services providers in DeliveringRCH services in Rural Area of Rajasthan
86) Janani Suraksha Yojana : A study ofimplementation status in selected districts ofRajasthan
87) Study on the assessment of the functioningof ANM/ MPHW(F) Training schools fundedby State Government / Private Organizations.
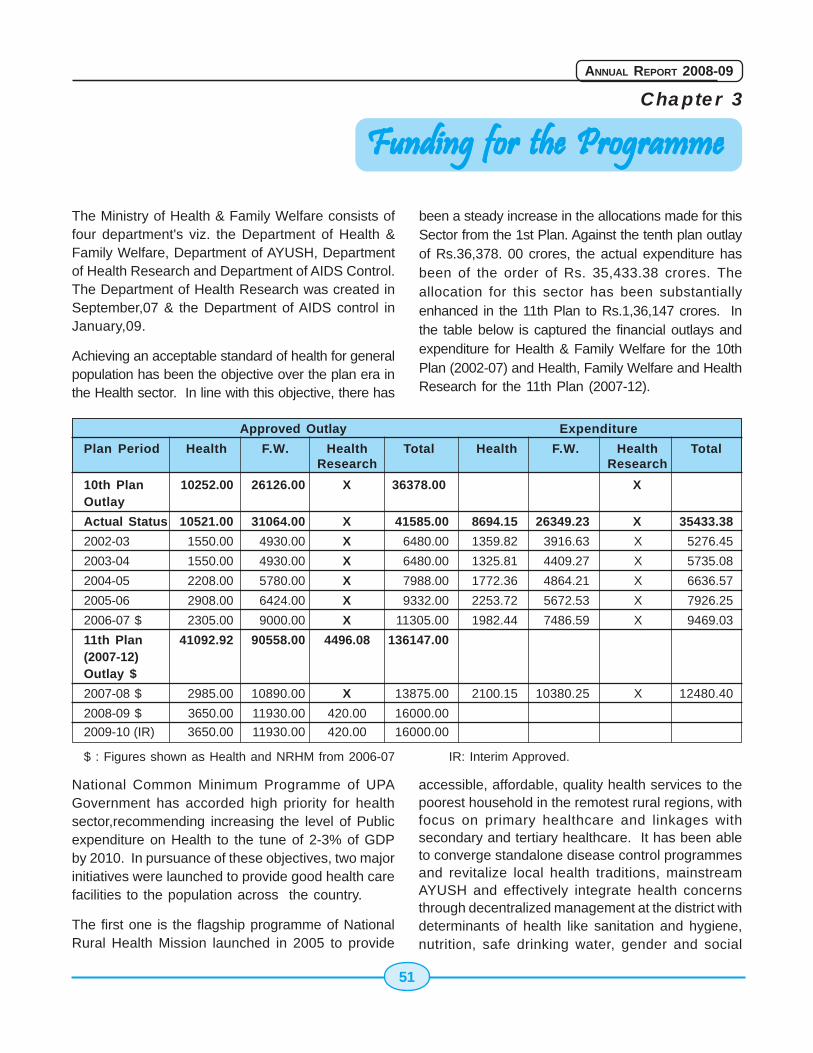
51
ANNUAL REPORT 2008-09
Chapter 3
The Ministry of Health & Family Welfare consists offour department's viz. the Department of Health &Family Welfare, Department of AYUSH, Departmentof Health Research and Department of AIDS Control.The Department of Health Research was created inSeptember,07 & the Department of AIDS control inJanuary,09.
Achieving an acceptable standard of health for generalpopulation has been the objective over the plan era inthe Health sector. In line with this objective, there has
Funding for the ProgrammeFunding for the ProgrammeFunding for the ProgrammeFunding for the ProgrammeFunding for the Programme
been a steady increase in the allocations made for thisSector from the 1st Plan. Against the tenth plan outlayof Rs.36,378. 00 crores, the actual expenditure hasbeen of the order of Rs. 35,433.38 crores. Theallocation for this sector has been substantiallyenhanced in the 11th Plan to Rs.1,36,147 crores. Inthe table below is captured the financial outlays andexpenditure for Health & Family Welfare for the 10thPlan (2002-07) and Health, Family Welfare and HealthResearch for the 11th Plan (2007-12).
National Common Minimum Programme of UPAGovernment has accorded high priority for healthsector,recommending increasing the level of Publicexpenditure on Health to the tune of 2-3% of GDPby 2010. In pursuance of these objectives, two majorinitiatives were launched to provide good health carefacilities to the population across the country.
The first one is the flagship programme of NationalRural Health Mission launched in 2005 to provide
accessible, affordable, quality health services to thepoorest household in the remotest rural regions, withfocus on primary healthcare and linkages withsecondary and tertiary healthcare. It has been ableto converge standalone disease control programmesand revitalize local health traditions, mainstreamAYUSH and effectively integrate health concernsthrough decentralized management at the district withdeterminants of health like sanitation and hygiene,nutrition, safe drinking water, gender and social
Approved Outlay Expenditure
Plan Period Health F.W. Health Total Health F.W. Health TotalResearch Research
10th Plan 10252.00 26126.00 X 36378.00 XOutlay
Actual Status 10521.00 31064.00 X 41585.00 8694.15 26349.23 X 35433.38
2002-03 1550.00 4930.00 X 6480.00 1359.82 3916.63 X 5276.45
2003-04 1550.00 4930.00 X 6480.00 1325.81 4409.27 X 5735.08
2004-05 2208.00 5780.00 X 7988.00 1772.36 4864.21 X 6636.57
2005-06 2908.00 6424.00 X 9332.00 2253.72 5672.53 X 7926.25
2006-07 $ 2305.00 9000.00 X 11305.00 1982.44 7486.59 X 9469.03
11th Plan 41092.92 90558.00 4496.08 136147.00(2007-12)Outlay $
2007-08 $ 2985.00 10890.00 X 13875.00 2100.15 10380.25 X 12480.40
2008-09 $ 3650.00 11930.00 420.00 16000.00
2009-10 (IR) 3650.00 11930.00 420.00 16000.00
$ : Figures shown as Health and NRHM from 2006-07 IR: Interim Approved.
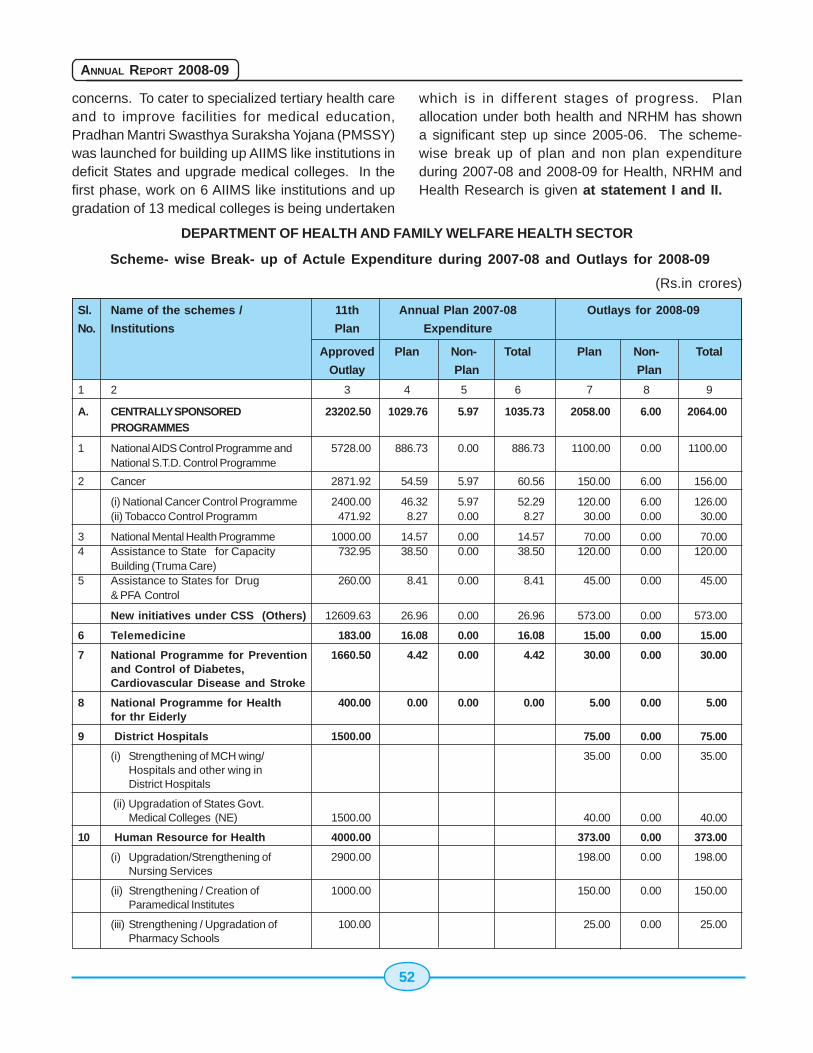
52
ANNUAL REPORT 2008-09
concerns. To cater to specialized tertiary health careand to improve facilities for medical education,Pradhan Mantri Swasthya Suraksha Yojana (PMSSY)was launched for building up AIIMS like institutions indeficit States and upgrade medical colleges. In thefirst phase, work on 6 AIIMS like institutions and upgradation of 13 medical colleges is being undertaken
which is in different stages of progress. Planallocation under both health and NRHM has showna significant step up since 2005-06. The scheme-wise break up of plan and non plan expenditureduring 2007-08 and 2008-09 for Health, NRHM andHealth Research is given at statement I and II.
DEPARTMENT OF HEALTH AND FAMILY WELFARE HEALTH SECTOR
Scheme- wise Break- up of Actule Expenditure during 2007-08 and Outlays for 2008-09
(Rs.in crores)
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
A. CENTRALLY SPONSORED 23202.50 1029.76 5.97 1035.73 2058.00 6.00 2064.00PROGRAMMES
1 National AIDS Control Programme and 5728.00 886.73 0.00 886.73 1100.00 0.00 1100.00National S.T.D. Control Programme
2 Cancer 2871.92 54.59 5.97 60.56 150.00 6.00 156.00
(i) National Cancer Control Programme 2400.00 46.32 5.97 52.29 120.00 6.00 126.00(ii) Tobacco Control Programm 471.92 8.27 0.00 8.27 30.00 0.00 30.00
3 National Mental Health Programme 1000.00 14.57 0.00 14.57 70.00 0.00 70.004 Assistance to State for Capacity 732.95 38.50 0.00 38.50 120.00 0.00 120.00
Building (Truma Care)5 Assistance to States for Drug 260.00 8.41 0.00 8.41 45.00 0.00 45.00
& PFA Control
New initiatives under CSS (Others) 12609.63 26.96 0.00 26.96 573.00 0.00 573.00
6 Telemedicine 183.00 16.08 0.00 16.08 15.00 0.00 15.00
7 National Programme for Prevention 1660.50 4.42 0.00 4.42 30.00 0.00 30.00and Control of Diabetes,Cardiovascular Disease and Stroke
8 National Programme for Health 400.00 0.00 0.00 0.00 5.00 0.00 5.00for thr Eiderly
9 District Hospitals 1500.00 75.00 0.00 75.00
(i) Strengthening of MCH wing/ 35.00 0.00 35.00Hospitals and other wing inDistrict Hospitals
(ii) Upgradation of States Govt.Medical Colleges (NE) 1500.00 40.00 0.00 40.00
10 Human Resource for Health 4000.00 373.00 0.00 373.00
(i) Upgradation/Strengthening of 2900.00 198.00 0.00 198.00Nursing Services
(ii) Strengthening / Creation of 1000.00 150.00 0.00 150.00Paramedical Institutes
(iii) Strengthening / Upgradation of 100.00 25.00 0.00 25.00Pharmacy Schools
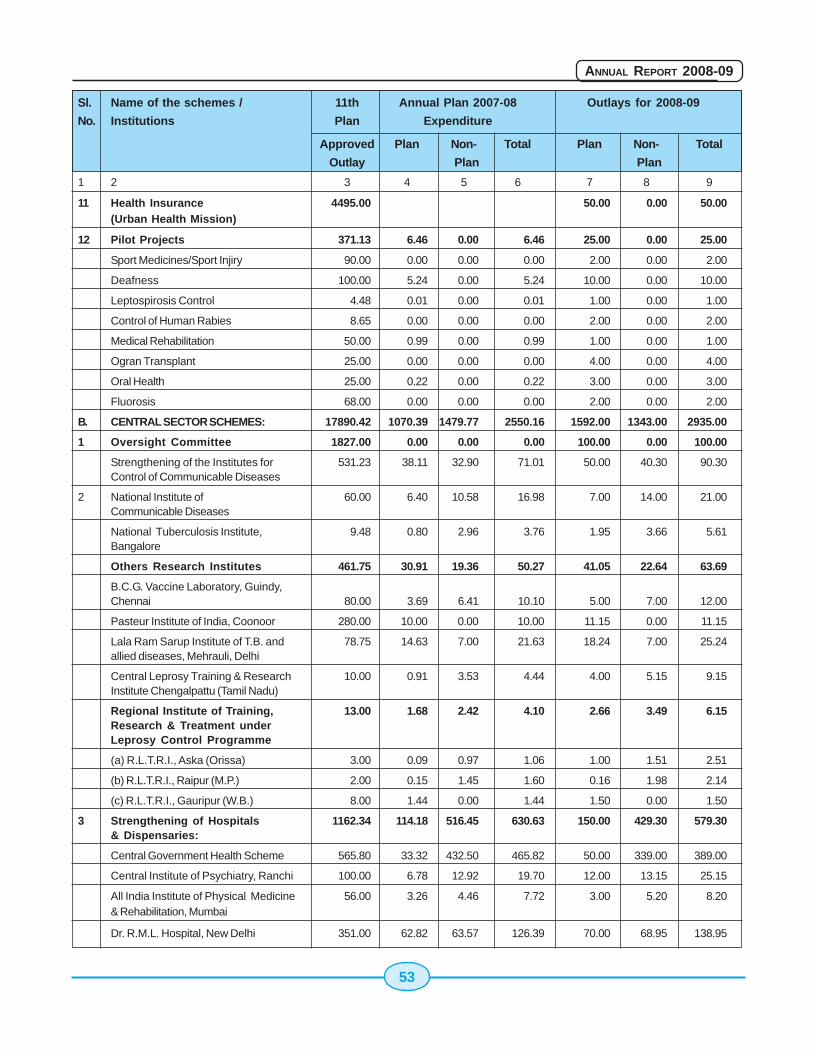
53
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
11 Health Insurance 4495.00 50.00 0.00 50.00(Urban Health Mission)
12 Pilot Projects 371.13 6.46 0.00 6.46 25.00 0.00 25.00
Sport Medicines/Sport Injiry 90.00 0.00 0.00 0.00 2.00 0.00 2.00
Deafness 100.00 5.24 0.00 5.24 10.00 0.00 10.00
Leptospirosis Control 4.48 0.01 0.00 0.01 1.00 0.00 1.00
Control of Human Rabies 8.65 0.00 0.00 0.00 2.00 0.00 2.00
Medical Rehabilitation 50.00 0.99 0.00 0.99 1.00 0.00 1.00
Ogran Transplant 25.00 0.00 0.00 0.00 4.00 0.00 4.00
Oral Health 25.00 0.22 0.00 0.22 3.00 0.00 3.00
Fluorosis 68.00 0.00 0.00 0.00 2.00 0.00 2.00
B. CENTRAL SECTOR SCHEMES: 17890.42 1070.39 1479.77 2550.16 1592.00 1343.00 2935.00
1 Oversight Committee 1827.00 0.00 0.00 0.00 100.00 0.00 100.00
Strengthening of the Institutes for 531.23 38.11 32.90 71.01 50.00 40.30 90.30Control of Communicable Diseases
2 National Institute of 60.00 6.40 10.58 16.98 7.00 14.00 21.00Communicable Diseases
National Tuberculosis Institute, 9.48 0.80 2.96 3.76 1.95 3.66 5.61Bangalore
Others Research Institutes 461.75 30.91 19.36 50.27 41.05 22.64 63.69
B.C.G. Vaccine Laboratory, Guindy,Chennai 80.00 3.69 6.41 10.10 5.00 7.00 12.00
Pasteur Institute of India, Coonoor 280.00 10.00 0.00 10.00 11.15 0.00 11.15
Lala Ram Sarup Institute of T.B. and 78.75 14.63 7.00 21.63 18.24 7.00 25.24allied diseases, Mehrauli, Delhi
Central Leprosy Training & Research 10.00 0.91 3.53 4.44 4.00 5.15 9.15Institute Chengalpattu (Tamil Nadu)
Regional Institute of Training, 13.00 1.68 2.42 4.10 2.66 3.49 6.15Research & Treatment underLeprosy Control Programme
(a) R.L.T.R.I., Aska (Orissa) 3.00 0.09 0.97 1.06 1.00 1.51 2.51
(b) R.L.T.R.I., Raipur (M.P.) 2.00 0.15 1.45 1.60 0.16 1.98 2.14
(c) R.L.T.R.I., Gauripur (W.B.) 8.00 1.44 0.00 1.44 1.50 0.00 1.50
3 Strengthening of Hospitals 1162.34 114.18 516.45 630.63 150.00 429.30 579.30& Dispensaries:
Central Government Health Scheme 565.80 33.32 432.50 465.82 50.00 339.00 389.00
Central Institute of Psychiatry, Ranchi 100.00 6.78 12.92 19.70 12.00 13.15 25.15
All India Institute of Physical Medicine 56.00 3.26 4.46 7.72 3.00 5.20 8.20& Rehabilitation, Mumbai
Dr. R.M.L. Hospital, New Delhi 351.00 62.82 63.57 126.39 70.00 68.95 138.95
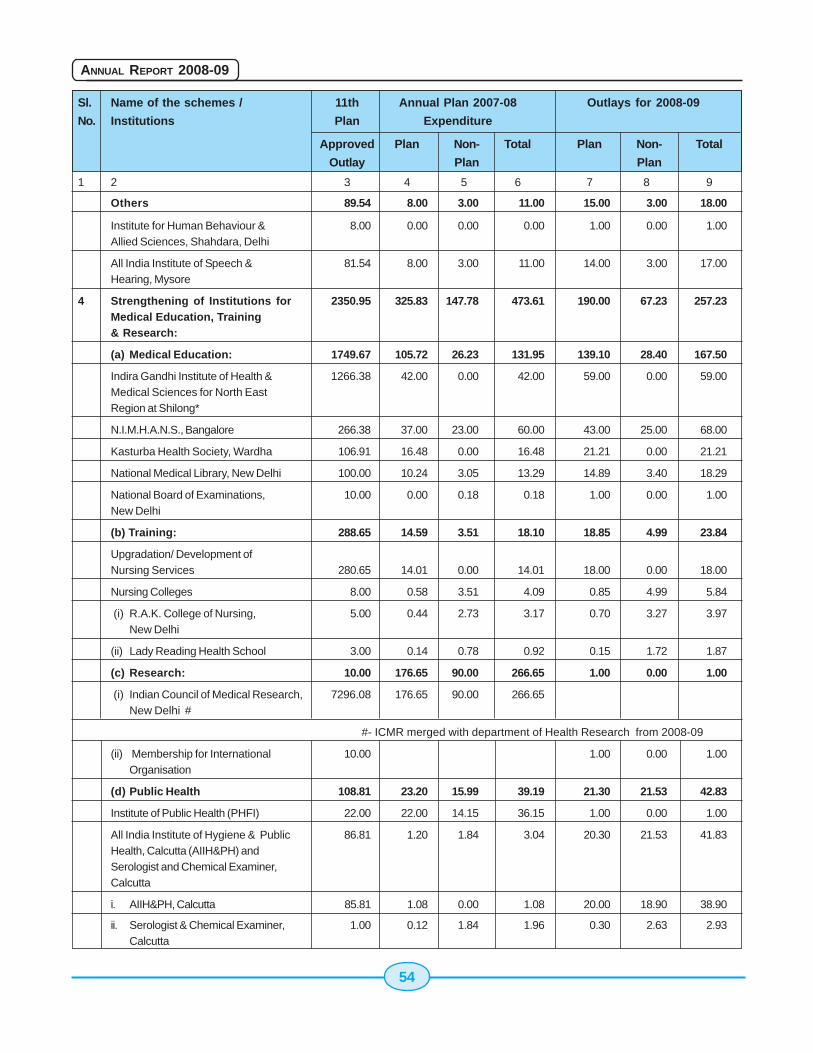
54
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
Others 89.54 8.00 3.00 11.00 15.00 3.00 18.00
Institute for Human Behaviour & 8.00 0.00 0.00 0.00 1.00 0.00 1.00Allied Sciences, Shahdara, Delhi
All India Institute of Speech & 81.54 8.00 3.00 11.00 14.00 3.00 17.00Hearing, Mysore
4 Strengthening of Institutions for 2350.95 325.83 147.78 473.61 190.00 67.23 257.23Medical Education, Training& Research:
(a) Medical Education: 1749.67 105.72 26.23 131.95 139.10 28.40 167.50
Indira Gandhi Institute of Health & 1266.38 42.00 0.00 42.00 59.00 0.00 59.00Medical Sciences for North EastRegion at Shilong*
N.I.M.H.A.N.S., Bangalore 266.38 37.00 23.00 60.00 43.00 25.00 68.00
Kasturba Health Society, Wardha 106.91 16.48 0.00 16.48 21.21 0.00 21.21
National Medical Library, New Delhi 100.00 10.24 3.05 13.29 14.89 3.40 18.29
National Board of Examinations, 10.00 0.00 0.18 0.18 1.00 0.00 1.00New Delhi
(b) Training: 288.65 14.59 3.51 18.10 18.85 4.99 23.84
Upgradation/ Development ofNursing Services 280.65 14.01 0.00 14.01 18.00 0.00 18.00
Nursing Colleges 8.00 0.58 3.51 4.09 0.85 4.99 5.84
(i) R.A.K. College of Nursing, 5.00 0.44 2.73 3.17 0.70 3.27 3.97New Delhi
(ii) Lady Reading Health School 3.00 0.14 0.78 0.92 0.15 1.72 1.87
(c) Research: 10.00 176.65 90.00 266.65 1.00 0.00 1.00
(i) Indian Council of Medical Research, 7296.08 176.65 90.00 266.65New Delhi #
#- ICMR merged with department of Health Research from 2008-09
(ii) Membership for International 10.00 1.00 0.00 1.00Organisation
(d) Public Health 108.81 23.20 15.99 39.19 21.30 21.53 42.83
Institute of Public Health (PHFI) 22.00 22.00 14.15 36.15 1.00 0.00 1.00
All India Institute of Hygiene & Public 86.81 1.20 1.84 3.04 20.30 21.53 41.83Health, Calcutta (AIIH&PH) andSerologist and Chemical Examiner,Calcutta
i. AIIH&PH, Calcutta 85.81 1.08 0.00 1.08 20.00 18.90 38.90
ii. Serologist & Chemical Examiner, 1.00 0.12 1.84 1.96 0.30 2.63 2.93Calcutta
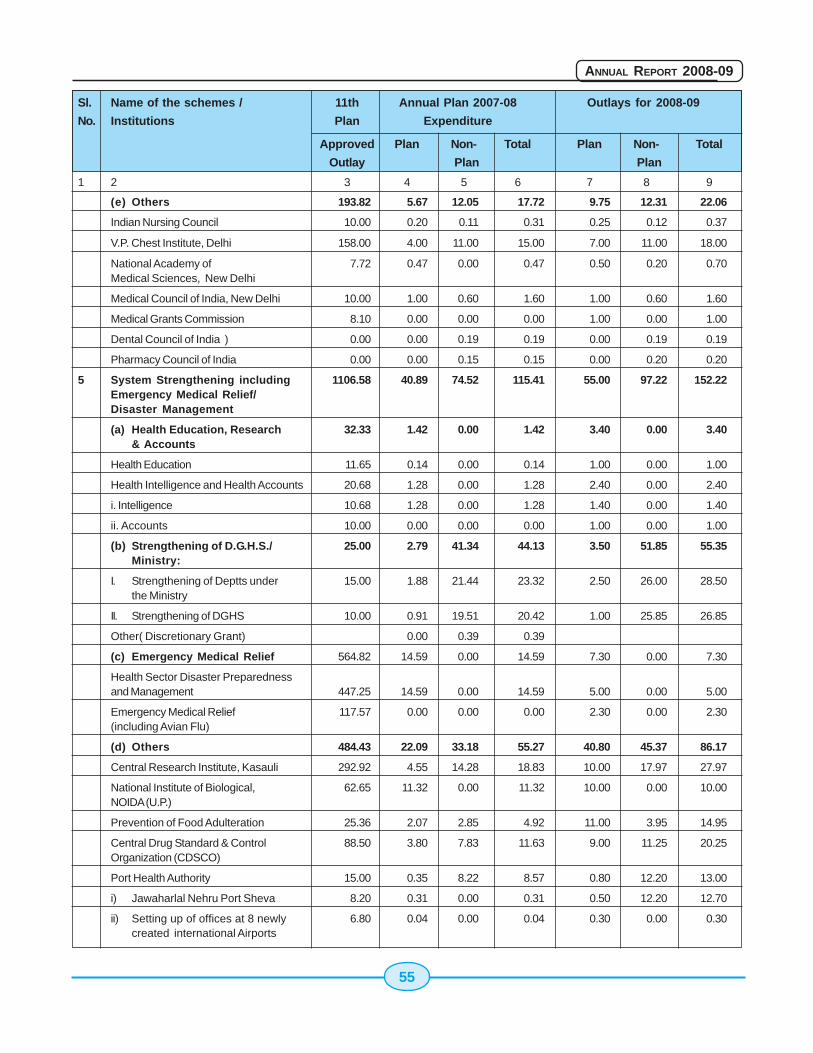
55
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
(e) Others 193.82 5.67 12.05 17.72 9.75 12.31 22.06
Indian Nursing Council 10.00 0.20 0.11 0.31 0.25 0.12 0.37
V.P. Chest Institute, Delhi 158.00 4.00 11.00 15.00 7.00 11.00 18.00
National Academy of 7.72 0.47 0.00 0.47 0.50 0.20 0.70Medical Sciences, New Delhi
Medical Council of India, New Delhi 10.00 1.00 0.60 1.60 1.00 0.60 1.60
Medical Grants Commission 8.10 0.00 0.00 0.00 1.00 0.00 1.00
Dental Council of India ) 0.00 0.00 0.19 0.19 0.00 0.19 0.19
Pharmacy Council of India 0.00 0.00 0.15 0.15 0.00 0.20 0.20
5 System Strengthening including 1106.58 40.89 74.52 115.41 55.00 97.22 152.22Emergency Medical Relief/Disaster Management
(a) Health Education, Research 32.33 1.42 0.00 1.42 3.40 0.00 3.40& Accounts
Health Education 11.65 0.14 0.00 0.14 1.00 0.00 1.00
Health Intelligence and Health Accounts 20.68 1.28 0.00 1.28 2.40 0.00 2.40
i. Intelligence 10.68 1.28 0.00 1.28 1.40 0.00 1.40
ii. Accounts 10.00 0.00 0.00 0.00 1.00 0.00 1.00
(b) Strengthening of D.G.H.S./ 25.00 2.79 41.34 44.13 3.50 51.85 55.35Ministry:
I. Strengthening of Deptts under 15.00 1.88 21.44 23.32 2.50 26.00 28.50the Ministry
II. Strengthening of DGHS 10.00 0.91 19.51 20.42 1.00 25.85 26.85
Other( Discretionary Grant) 0.00 0.39 0.39
(c) Emergency Medical Relief 564.82 14.59 0.00 14.59 7.30 0.00 7.30
Health Sector Disaster Preparednessand Management 447.25 14.59 0.00 14.59 5.00 0.00 5.00
Emergency Medical Relief 117.57 0.00 0.00 0.00 2.30 0.00 2.30(including Avian Flu)
(d) Others 484.43 22.09 33.18 55.27 40.80 45.37 86.17
Central Research Institute, Kasauli 292.92 4.55 14.28 18.83 10.00 17.97 27.97
National Institute of Biological, 62.65 11.32 0.00 11.32 10.00 0.00 10.00NOIDA (U.P.)
Prevention of Food Adulteration 25.36 2.07 2.85 4.92 11.00 3.95 14.95
Central Drug Standard & Control 88.50 3.80 7.83 11.63 9.00 11.25 20.25Organization (CDSCO)
Port Health Authority 15.00 0.35 8.22 8.57 0.80 12.20 13.00
i) Jawaharlal Nehru Port Sheva 8.20 0.31 0.00 0.31 0.50 12.20 12.70
ii) Setting up of offices at 8 newly 6.80 0.04 0.00 0.04 0.30 0.00 0.30created international Airports
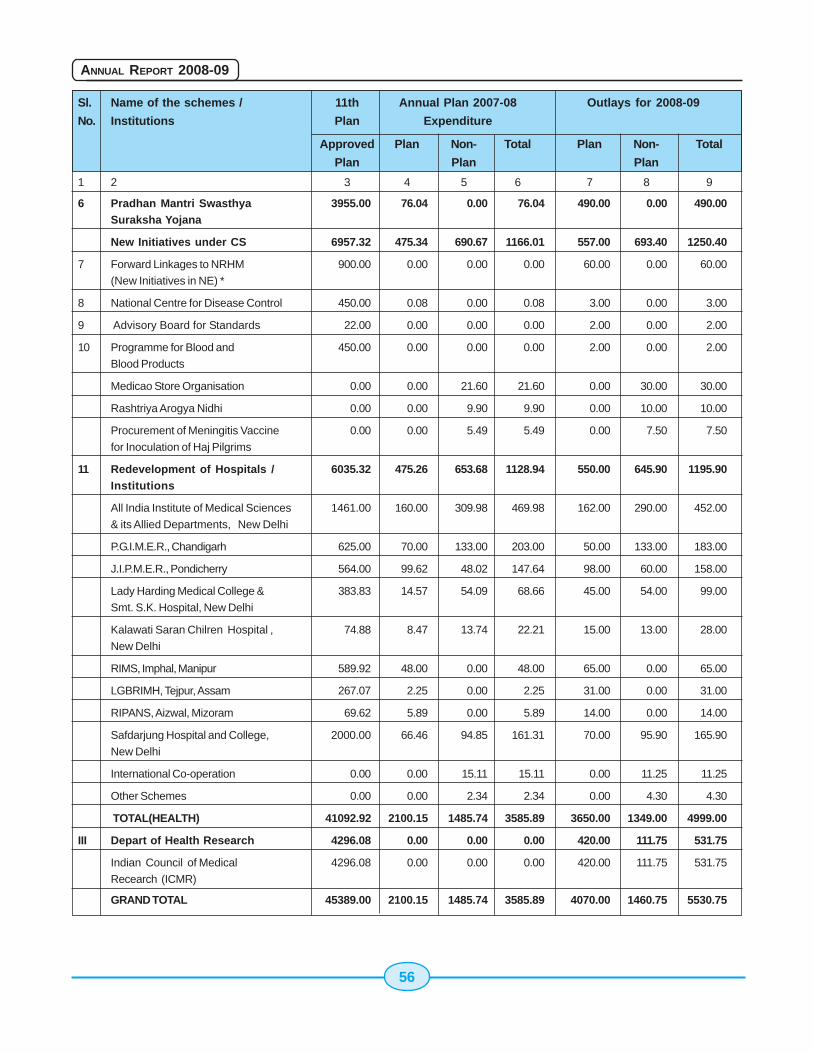
56
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Plan Plan Plan
1 2 3 4 5 6 7 8 9
6 Pradhan Mantri Swasthya 3955.00 76.04 0.00 76.04 490.00 0.00 490.00Suraksha Yojana
New Initiatives under CS 6957.32 475.34 690.67 1166.01 557.00 693.40 1250.40
7 Forward Linkages to NRHM 900.00 0.00 0.00 0.00 60.00 0.00 60.00
(New Initiatives in NE) *
8 National Centre for Disease Control 450.00 0.08 0.00 0.08 3.00 0.00 3.00
9 Advisory Board for Standards 22.00 0.00 0.00 0.00 2.00 0.00 2.00
10 Programme for Blood and 450.00 0.00 0.00 0.00 2.00 0.00 2.00
Blood Products
Medicao Store Organisation 0.00 0.00 21.60 21.60 0.00 30.00 30.00
Rashtriya Arogya Nidhi 0.00 0.00 9.90 9.90 0.00 10.00 10.00
Procurement of Meningitis Vaccine 0.00 0.00 5.49 5.49 0.00 7.50 7.50
for Inoculation of Haj Pilgrims
11 Redevelopment of Hospitals / 6035.32 475.26 653.68 1128.94 550.00 645.90 1195.90Institutions
All India Institute of Medical Sciences 1461.00 160.00 309.98 469.98 162.00 290.00 452.00
& its Allied Departments, New Delhi
P.G.I.M.E.R., Chandigarh 625.00 70.00 133.00 203.00 50.00 133.00 183.00
J.I.P.M.E.R., Pondicherry 564.00 99.62 48.02 147.64 98.00 60.00 158.00
Lady Harding Medical College & 383.83 14.57 54.09 68.66 45.00 54.00 99.00
Smt. S.K. Hospital, New Delhi
Kalawati Saran Chilren Hospital , 74.88 8.47 13.74 22.21 15.00 13.00 28.00
New Delhi
RIMS, Imphal, Manipur 589.92 48.00 0.00 48.00 65.00 0.00 65.00
LGBRIMH, Tejpur, Assam 267.07 2.25 0.00 2.25 31.00 0.00 31.00
RIPANS, Aizwal, Mizoram 69.62 5.89 0.00 5.89 14.00 0.00 14.00
Safdarjung Hospital and College, 2000.00 66.46 94.85 161.31 70.00 95.90 165.90
New Delhi
International Co-operation 0.00 0.00 15.11 15.11 0.00 11.25 11.25
Other Schemes 0.00 0.00 2.34 2.34 0.00 4.30 4.30
TOTAL(HEALTH) 41092.92 2100.15 1485.74 3585.89 3650.00 1349.00 4999.00
III Depart of Health Research 4296.08 0.00 0.00 0.00 420.00 111.75 531.75
Indian Council of Medical 4296.08 0.00 0.00 0.00 420.00 111.75 531.75
Recearch (ICMR)
GRAND TOTAL 45389.00 2100.15 1485.74 3585.89 4070.00 1460.75 5530.75
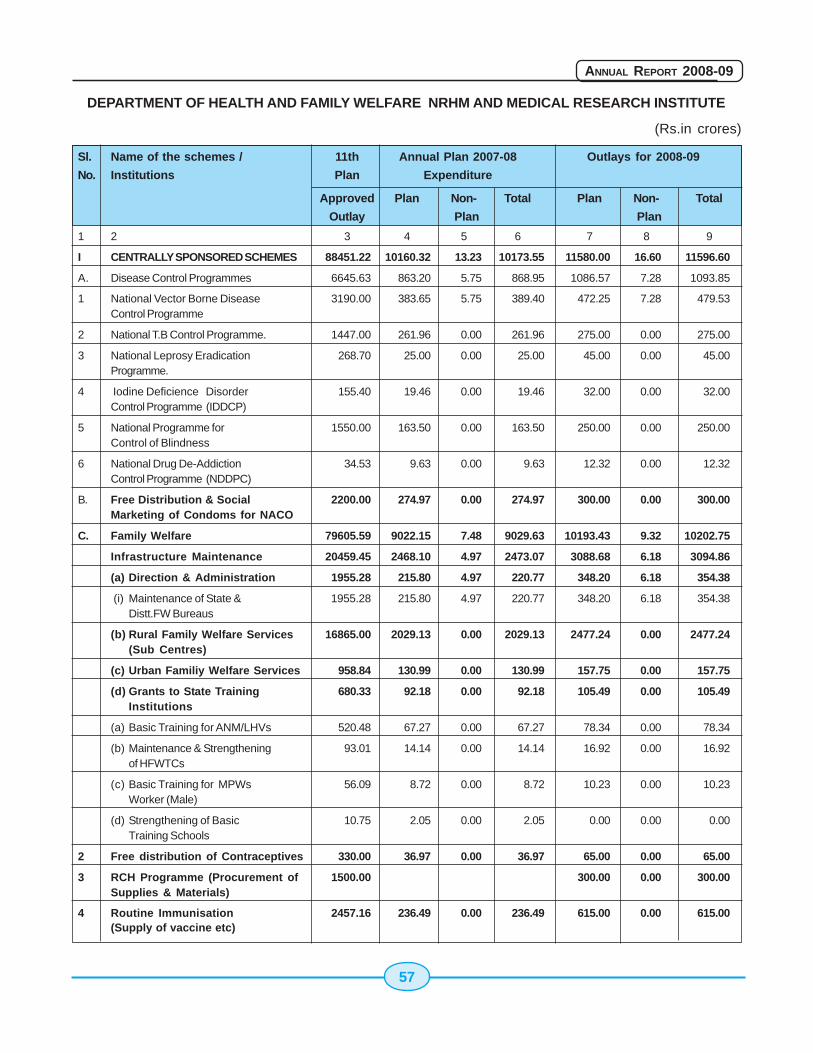
57
ANNUAL REPORT 2008-09
DEPARTMENT OF HEALTH AND FAMILY WELFARE NRHM AND MEDICAL RESEARCH INSTITUTE
(Rs.in crores)
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
I CENTRALLY SPONSORED SCHEMES 88451.22 10160.32 13.23 10173.55 11580.00 16.60 11596.60
A. Disease Control Programmes 6645.63 863.20 5.75 868.95 1086.57 7.28 1093.85
1 National Vector Borne Disease 3190.00 383.65 5.75 389.40 472.25 7.28 479.53Control Programme
2 National T.B Control Programme. 1447.00 261.96 0.00 261.96 275.00 0.00 275.00
3 National Leprosy Eradication 268.70 25.00 0.00 25.00 45.00 0.00 45.00Programme.
4 Iodine Deficience Disorder 155.40 19.46 0.00 19.46 32.00 0.00 32.00Control Programme (IDDCP)
5 National Programme for 1550.00 163.50 0.00 163.50 250.00 0.00 250.00Control of Blindness
6 National Drug De-Addiction 34.53 9.63 0.00 9.63 12.32 0.00 12.32Control Programme (NDDPC)
B. Free Distribution & Social 2200.00 274.97 0.00 274.97 300.00 0.00 300.00Marketing of Condoms for NACO
C. Family Welfare 79605.59 9022.15 7.48 9029.63 10193.43 9.32 10202.75
Infrastructure Maintenance 20459.45 2468.10 4.97 2473.07 3088.68 6.18 3094.86
(a) Direction & Administration 1955.28 215.80 4.97 220.77 348.20 6.18 354.38
(i) Maintenance of State & 1955.28 215.80 4.97 220.77 348.20 6.18 354.38Distt.FW Bureaus
(b) Rural Family Welfare Services 16865.00 2029.13 0.00 2029.13 2477.24 0.00 2477.24(Sub Centres)
(c) Urban Familiy Welfare Services 958.84 130.99 0.00 130.99 157.75 0.00 157.75
(d) Grants to State Training 680.33 92.18 0.00 92.18 105.49 0.00 105.49Institutions
(a) Basic Training for ANM/LHVs 520.48 67.27 0.00 67.27 78.34 0.00 78.34
(b) Maintenance & Strengthening 93.01 14.14 0.00 14.14 16.92 0.00 16.92of HFWTCs
(c) Basic Training for MPWs 56.09 8.72 0.00 8.72 10.23 0.00 10.23Worker (Male)
(d) Strengthening of Basic 10.75 2.05 0.00 2.05 0.00 0.00 0.00Training Schools
2 Free distribution of Contraceptives 330.00 36.97 0.00 36.97 65.00 0.00 65.00
3 RCH Programme (Procurement of 1500.00 300.00 0.00 300.00Supplies & Materials)
4 Routine Immunisation 2457.16 236.49 0.00 236.49 615.00 0.00 615.00(Supply of vaccine etc)
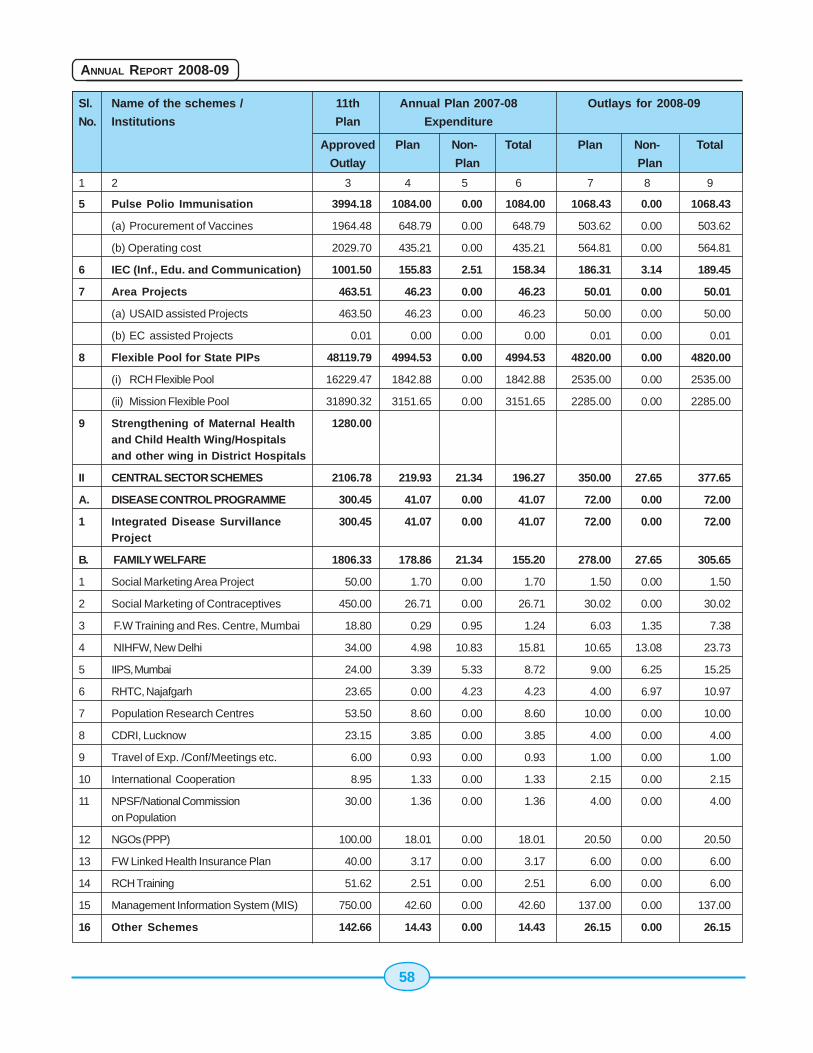
58
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
5 Pulse Polio Immunisation 3994.18 1084.00 0.00 1084.00 1068.43 0.00 1068.43
(a) Procurement of Vaccines 1964.48 648.79 0.00 648.79 503.62 0.00 503.62
(b) Operating cost 2029.70 435.21 0.00 435.21 564.81 0.00 564.81
6 IEC (Inf., Edu. and Communication) 1001.50 155.83 2.51 158.34 186.31 3.14 189.45
7 Area Projects 463.51 46.23 0.00 46.23 50.01 0.00 50.01
(a) USAID assisted Projects 463.50 46.23 0.00 46.23 50.00 0.00 50.00
(b) EC assisted Projects 0.01 0.00 0.00 0.00 0.01 0.00 0.01
8 Flexible Pool for State PIPs 48119.79 4994.53 0.00 4994.53 4820.00 0.00 4820.00
(i) RCH Flexible Pool 16229.47 1842.88 0.00 1842.88 2535.00 0.00 2535.00
(ii) Mission Flexible Pool 31890.32 3151.65 0.00 3151.65 2285.00 0.00 2285.00
9 Strengthening of Maternal Health 1280.00and Child Health Wing/Hospitalsand other wing in District Hospitals
II CENTRAL SECTOR SCHEMES 2106.78 219.93 21.34 196.27 350.00 27.65 377.65
A. DISEASE CONTROL PROGRAMME 300.45 41.07 0.00 41.07 72.00 0.00 72.00
1 Integrated Disease Survillance 300.45 41.07 0.00 41.07 72.00 0.00 72.00Project
B. FAMILY WELFARE 1806.33 178.86 21.34 155.20 278.00 27.65 305.65
1 Social Marketing Area Project 50.00 1.70 0.00 1.70 1.50 0.00 1.50
2 Social Marketing of Contraceptives 450.00 26.71 0.00 26.71 30.02 0.00 30.02
3 F.W Training and Res. Centre, Mumbai 18.80 0.29 0.95 1.24 6.03 1.35 7.38
4 NIHFW, New Delhi 34.00 4.98 10.83 15.81 10.65 13.08 23.73
5 IIPS, Mumbai 24.00 3.39 5.33 8.72 9.00 6.25 15.25
6 RHTC, Najafgarh 23.65 0.00 4.23 4.23 4.00 6.97 10.97
7 Population Research Centres 53.50 8.60 0.00 8.60 10.00 0.00 10.00
8 CDRI, Lucknow 23.15 3.85 0.00 3.85 4.00 0.00 4.00
9 Travel of Exp. /Conf/Meetings etc. 6.00 0.93 0.00 0.93 1.00 0.00 1.00
10 International Cooperation 8.95 1.33 0.00 1.33 2.15 0.00 2.15
11 NPSF/National Commission 30.00 1.36 0.00 1.36 4.00 0.00 4.00on Population
12 NGOs (PPP) 100.00 18.01 0.00 18.01 20.50 0.00 20.50
13 FW Linked Health Insurance Plan 40.00 3.17 0.00 3.17 6.00 0.00 6.00
14 RCH Training 51.62 2.51 0.00 2.51 6.00 0.00 6.00
15 Management Information System (MIS) 750.00 42.60 0.00 42.60 137.00 0.00 137.00
16 Other Schemes 142.66 14.43 0.00 14.43 26.15 0.00 26.15
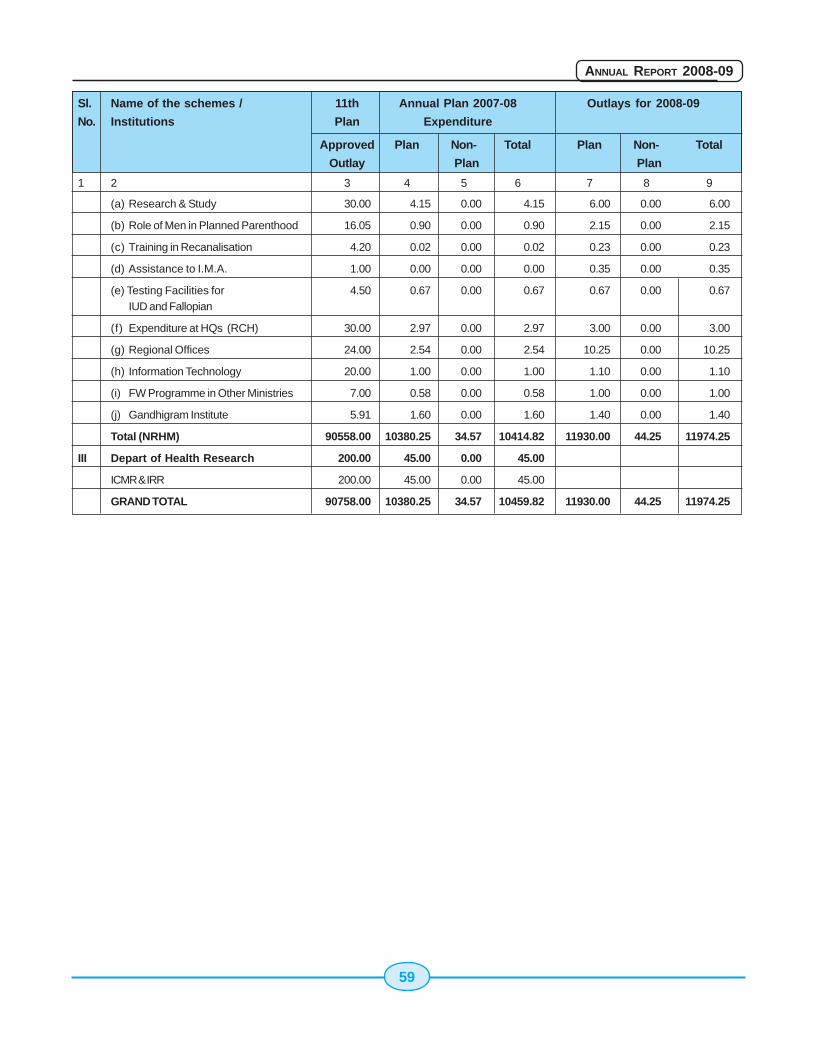
59
ANNUAL REPORT 2008-09
Sl. Name of the schemes / 11th Annual Plan 2007-08 Outlays for 2008-09
No. Institutions Plan Expenditure
Approved Plan Non- Total Plan Non- Total
Outlay Plan Plan
1 2 3 4 5 6 7 8 9
(a) Research & Study 30.00 4.15 0.00 4.15 6.00 0.00 6.00
(b) Role of Men in Planned Parenthood 16.05 0.90 0.00 0.90 2.15 0.00 2.15
(c) Training in Recanalisation 4.20 0.02 0.00 0.02 0.23 0.00 0.23
(d) Assistance to I.M.A. 1.00 0.00 0.00 0.00 0.35 0.00 0.35
(e) Testing Facilities for 4.50 0.67 0.00 0.67 0.67 0.00 0.67IUD and Fallopian
(f) Expenditure at HQs (RCH) 30.00 2.97 0.00 2.97 3.00 0.00 3.00
(g) Regional Offices 24.00 2.54 0.00 2.54 10.25 0.00 10.25
(h) Information Technology 20.00 1.00 0.00 1.00 1.10 0.00 1.10
(i) FW Programme in Other Ministries 7.00 0.58 0.00 0.58 1.00 0.00 1.00
(j) Gandhigram Institute 5.91 1.60 0.00 1.60 1.40 0.00 1.40
Total (NRHM) 90558.00 10380.25 34.57 10414.82 11930.00 44.25 11974.25
III Depart of Health Research 200.00 45.00 0.00 45.00
ICMR & IRR 200.00 45.00 0.00 45.00
GRAND TOTAL 90758.00 10380.25 34.57 10459.82 11930.00 44.25 11974.25

60
ANNUAL REPORT 2008-09
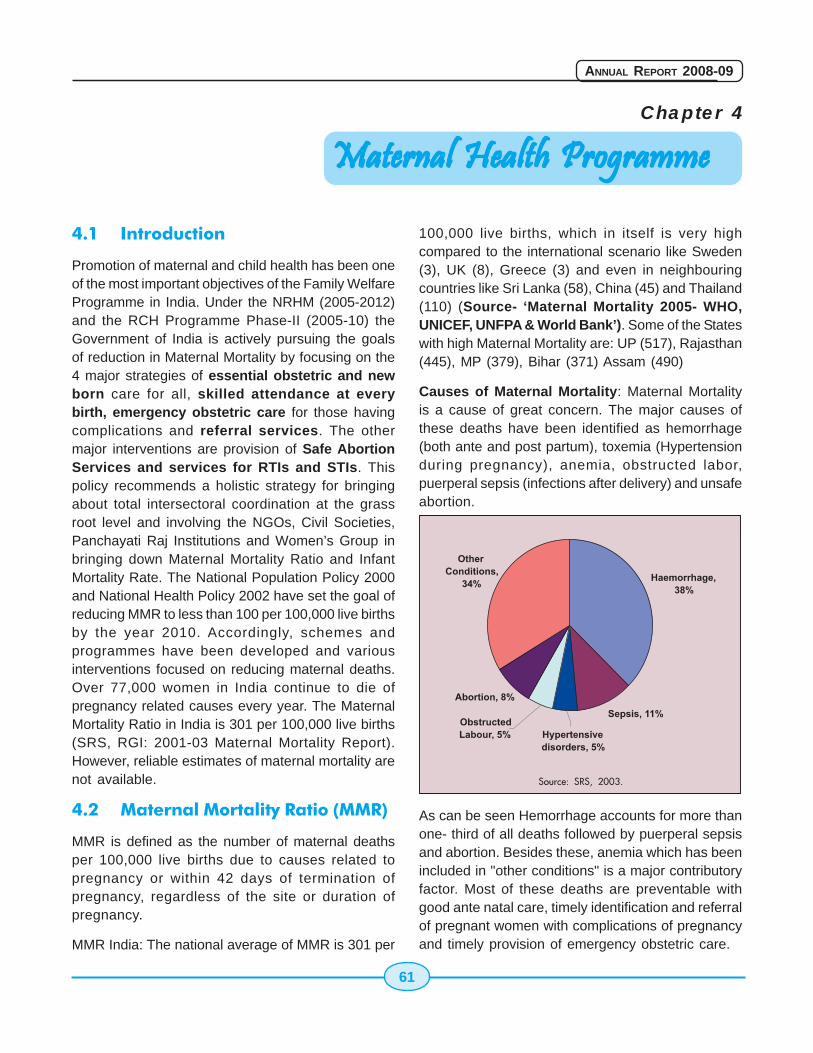
61
ANNUAL REPORT 2008-09
Chapter 4
4.1 Introduction
Promotion of maternal and child health has been oneof the most important objectives of the Family WelfareProgramme in India. Under the NRHM (2005-2012)and the RCH Programme Phase-II (2005-10) theGovernment of India is actively pursuing the goalsof reduction in Maternal Mortality by focusing on the4 major strategies of essential obstetric and newborn care for all, skilled attendance at everybirth, emergency obstetric care for those havingcomplications and referral services. The othermajor interventions are provision of Safe AbortionServices and services for RTIs and STIs. Thispolicy recommends a holistic strategy for bringingabout total intersectoral coordination at the grassroot level and involving the NGOs, Civil Societies,Panchayati Raj Institutions and Women’s Group inbringing down Maternal Mortality Ratio and InfantMortality Rate. The National Population Policy 2000and National Health Policy 2002 have set the goal ofreducing MMR to less than 100 per 100,000 live birthsby the year 2010. Accordingly, schemes andprogrammes have been developed and variousinterventions focused on reducing maternal deaths.Over 77,000 women in India continue to die ofpregnancy related causes every year. The MaternalMortality Ratio in India is 301 per 100,000 live births(SRS, RGI: 2001-03 Maternal Mortality Report).However, reliable estimates of maternal mortality arenot available.
4.2 Maternal Mortality Ratio (MMR)
MMR is defined as the number of maternal deathsper 100,000 live births due to causes related topregnancy or within 42 days of termination ofpregnancy, regardless of the site or duration ofpregnancy.
MMR India: The national average of MMR is 301 per
100,000 live births, which in itself is very highcompared to the international scenario like Sweden(3), UK (8), Greece (3) and even in neighbouringcountries like Sri Lanka (58), China (45) and Thailand(110) (Source- ‘Maternal Mortality 2005- WHO,UNICEF, UNFPA & World Bank’). Some of the Stateswith high Maternal Mortality are: UP (517), Rajasthan(445), MP (379), Bihar (371) Assam (490)
Causes of Maternal Mortality: Maternal Mortalityis a cause of great concern. The major causes ofthese deaths have been identified as hemorrhage(both ante and post partum), toxemia (Hypertensionduring pregnancy), anemia, obstructed labor,puerperal sepsis (infections after delivery) and unsafeabortion.
As can be seen Hemorrhage accounts for more thanone- third of all deaths followed by puerperal sepsisand abortion. Besides these, anemia which has beenincluded in "other conditions" is a major contributoryfactor. Most of these deaths are preventable withgood ante natal care, timely identification and referralof pregnant women with complications of pregnancyand timely provision of emergency obstetric care.
Maternal Health ProgrammeMaternal Health ProgrammeMaternal Health ProgrammeMaternal Health ProgrammeMaternal Health Programme
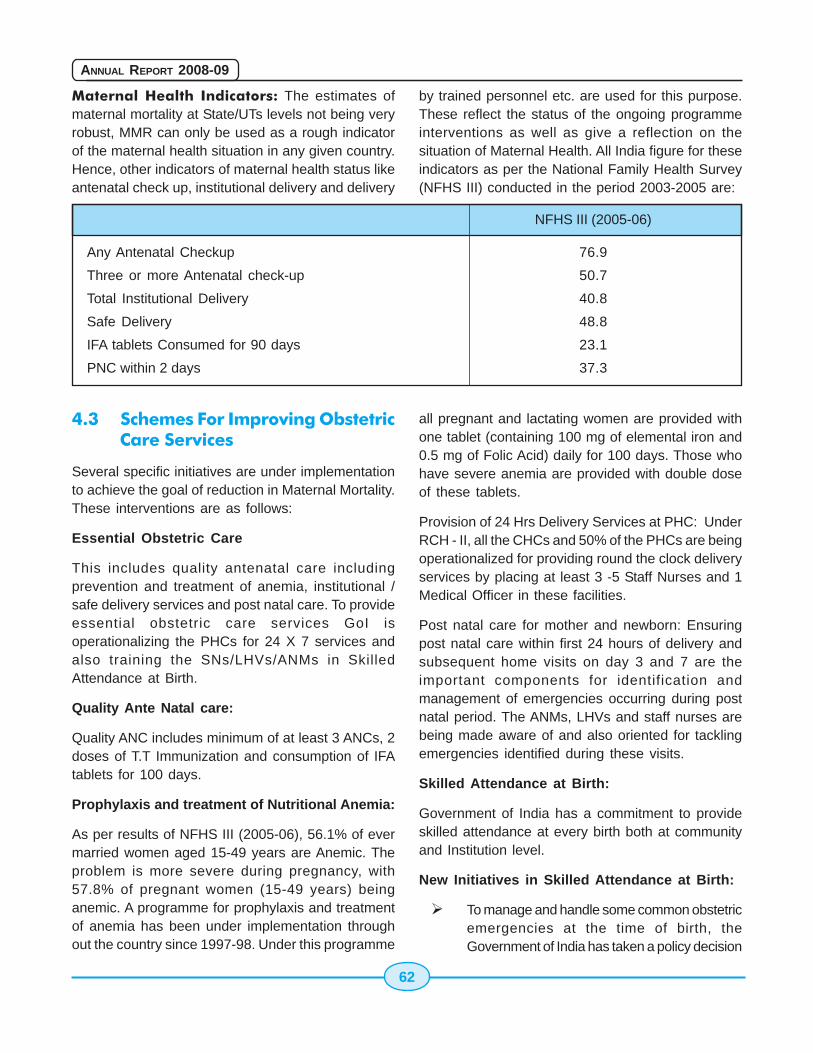
62
ANNUAL REPORT 2008-09
Maternal Health Indicators: The estimates ofmaternal mortality at State/UTs levels not being veryrobust, MMR can only be used as a rough indicatorof the maternal health situation in any given country.Hence, other indicators of maternal health status likeantenatal check up, institutional delivery and delivery
by trained personnel etc. are used for this purpose.These reflect the status of the ongoing programmeinterventions as well as give a reflection on thesituation of Maternal Health. All India figure for theseindicators as per the National Family Health Survey(NFHS III) conducted in the period 2003-2005 are:
NFHS III (2005-06)
Any Antenatal Checkup 76.9
Three or more Antenatal check-up 50.7
Total Institutional Delivery 40.8
Safe Delivery 48.8
IFA tablets Consumed for 90 days 23.1
PNC within 2 days 37.3
4.3 Schemes For Improving ObstetricCare Services
Several specific initiatives are under implementationto achieve the goal of reduction in Maternal Mortality.These interventions are as follows:
Essential Obstetric Care
This includes quality antenatal care includingprevention and treatment of anemia, institutional /safe delivery services and post natal care. To provideessential obstetric care services GoI isoperationalizing the PHCs for 24 X 7 services andalso training the SNs/LHVs/ANMs in SkilledAttendance at Birth.
Quality Ante Natal care:
Quality ANC includes minimum of at least 3 ANCs, 2doses of T.T Immunization and consumption of IFAtablets for 100 days.
Prophylaxis and treatment of Nutritional Anemia:
As per results of NFHS III (2005-06), 56.1% of evermarried women aged 15-49 years are Anemic. Theproblem is more severe during pregnancy, with57.8% of pregnant women (15-49 years) beinganemic. A programme for prophylaxis and treatmentof anemia has been under implementation throughout the country since 1997-98. Under this programme
all pregnant and lactating women are provided withone tablet (containing 100 mg of elemental iron and0.5 mg of Folic Acid) daily for 100 days. Those whohave severe anemia are provided with double doseof these tablets.
Provision of 24 Hrs Delivery Services at PHC: UnderRCH - II, all the CHCs and 50% of the PHCs are beingoperationalized for providing round the clock deliveryservices by placing at least 3 -5 Staff Nurses and 1Medical Officer in these facilities.
Post natal care for mother and newborn: Ensuringpost natal care within first 24 hours of delivery andsubsequent home visits on day 3 and 7 are theimportant components for identification andmanagement of emergencies occurring during postnatal period. The ANMs, LHVs and staff nurses arebeing made aware of and also oriented for tacklingemergencies identified during these visits.
Skilled Attendance at Birth:
Government of India has a commitment to provideskilled attendance at every birth both at communityand Institution level.
New Initiatives in Skilled Attendance at Birth:
� To manage and handle some common obstetricemergencies at the time of birth, theGovernment of India has taken a policy decision

63
ANNUAL REPORT 2008-09
to permit Staff Nurses (SNs) and ANMs to givecertain injections and also perform certaininterventions under specific emergencysituations to save the life of the mother.
� Training Strategy involves a 2-3 week trainingof SNs and 3-6 week training of ANMs/LHVsin Skilled Attendance at Birth. For thisCurriculum and Technical Guidelines havebeen developed and have already beendisseminated to the States.
Provision of Emergency Obstetric and NeonatalCare at FRUs:
Provision of Emergency Obstetric and Neonatal Careat FRUs has been done by operationalizing all FRUsin the country. While operationalization, the thrustshould be on the critical components such asmanpower, blood storage units and referral linkagesetc. Availability of trained manpower (Skill BasedTraining for MBBS doctors) should be linked withoperationalization of FRUs. The initiatives beingundertaken in this regard are:
Training of MBBS Doctors in Life SavingAnesthetics Skills for Emergency ObstetricCare:
Provision of adequate and timely EmergencyObstetric Care (EmOC) has been recognized globallyas the most important intervention for saving lives ofpregnant women who may develop complicationsduring pregnancy or childbirth. The operationalizationof First Referral Units, at sub- district i.e. CHC levelfor providing EmOC to pregnant women is a criticalstrategy of RCH-II, which needs focused attention. Ithas not been possible to operationalize these FRUstill now due to various factors most pertinent beingshortage of specialist manpower, i.e. gynecologistand Anesthetist, particularly at district and sub districtlevel.
In view of this, for effective and better managementof Emergency Obstetric needs at the grass root level,GOI has taken a policy decision and is implementing18 weeks programme for training of MBBS doctorsin anesthetic skills for Emergency Obstetric care atFRU.
The training shall be undertaken for only thatnumber of MBBS doctors who are required for theoperationalization of FRUs and CHCs and shall belimited to the requirement of tackling emergencyobstetric situations only. In no way, will it be areplacement of the specialist anesthetists who areworking after pursuing degree / diploma in thesubject. Guidelines for the training programme havebeen disseminated to the States for taking initiativesin identifying the medical colleges in the state wherethis training programme can be conducted.
Training in Obstetric Management Skills:
Government of India has also introduced training ofMBBS doctors in Obstetric Management Skills incollaboration with Federation of Obstetric andGynecological Society of India. A 16 weeks trainingprogramme in obstetric management skills includingCaesarian Section operation is being implementedat the level of Medical Colleges and District Hospitalsin the States.
Referral Services at both Community andInstitutional level:
Establishing referral linkages between the communityand First Referral Units is an essential componentfor utilization of services particularly duringEmergencies. Since emergencies during the processof birth can not be predicted, it is essential to placeeffective referral linkages which can be accessed byall pregnant women in case of emergency.
Other Major Interventions are:
Safe Abortion Services/ Medical termination ofPregnancy (MTP):
Abortion is a significant medical and social problemin India. An ICMR study (1989) documented that therates of safe (legal) and unsafe (Illegal) abortionswere 6.1 and 13.5 per 1000 pregnancies,respectively. It is evident that perhaps two-thirds ofall abortions take place outside the authorized healthservices by unauthorized, often unskilled providers.
The Medical Termination of Pregnancy Act waspassed by the Indian Parliament in 1971 and cameinto force from April 1. 1972. The aim of this Act wasto reduce maternal mortality and morbidity due to
64
ANNUAL REPORT 2008-09
unsafe abortions. The MTP Act, 1971 lays down theconditions under which a pregnancy can be terminatedand the place where such terminations can beperformed. A recent amendment to the Act (2003)includes decentralization of power for approval ofplaces, as MTP centers, from the states to the districtlevel with the aim of enlarging the network of safeMTP service providers. The amendment also providesfor specific punitive measures for performing MTPsby unqualified persons and in places not approvedby the government.
Whether spontaneous or induced, abortion has beena matter of concern over many decades now,particularly because of sepsis and other complicationsassociated with it. Eight percent of maternal deathsare attributed to complicated abortions. This is apreventable tragedy. This is also an indication of theunmet need for safe abortions. The National PopulationPolicy 2000 underlines the provision of safe abortionsas one of the important operational strategies. Provisionof MTP services at 24 X 7 PHCs, CHCs and FRUs arebeing strengthened by training of medical manpowerin techniques of MTP by the States.
� Strategies:
� Community level:
� Spread awareness regarding safe MTPin the community and the availability ofservices thereof.
� Enhance access to confidentialcounseling for safe MTP; train ANMs,AWWs and link workers/ASHAs to providesuch counseling.
� Promote post-abortion care throughANMs, link workers/ASHAs and AWWswhile maintaining confidentiality.
� Facility level:
� Provide quality MVA (Manual VacuumAspiration) facilities at all CHCs and atleast 50% of PHCs that are beingstrengthened for 24-hour deliveries.
� Provide comprehensive and high qualityMTP services at all FRUs.
� Encourage private and NGO sectors toestablish quality MTP services.
Guidelines for Manual Vacuum Aspiration (MVA) upto8 weeks of pregnancy for Medical Officers forperforming safe abortions at primary health carefacilities have been disseminated to the states forimplementation.
The ministry also proposes to developcomprehensive safe abortion guidelines includingmedical abortion and providing services for medicalabortion through the peripheral health careinfrastructure.
Provision of RTI/STI services at all FRUs, CHCsand at 24 X 7 PHCs is also being made underRCH II
Reproductive Tract Infections/Sexually TransmittedInfections (RTIs/STIs) Reproductive tract andsexually transmitted infections (RTI/ STIs) were notrecognized as a public health problem until recently.Research conducted in India to document themagnitude of reproductive morbidity, has made theincidence of these infections more visible andbrought them into the reproductive health agenda.Several studies conducted in India during the pastdecade suggest high prevalence of reproductivemorbidity among women. As per DLHS-II (2003-2004), about one-third of women reported somesymptoms of RTI/ STI, but only 32% sought treatment.The spread of HIV infection and the role that RTI/STIplays in the transmission of HIV have also broughturgency to the problem. The identification andmanagement of reproductive tract infections is animportant objective of the RCH Programme.
� Strategies under RCH II:
� The prevention, early detection andeffective management of common lowerreproductive tract infections have beenincluded as a component of essential carethrough the existing primary health careinfrastructure.
� Convergence with the National AIDSControl Programme (NACP) is envisagedin provision of these services, in terms of
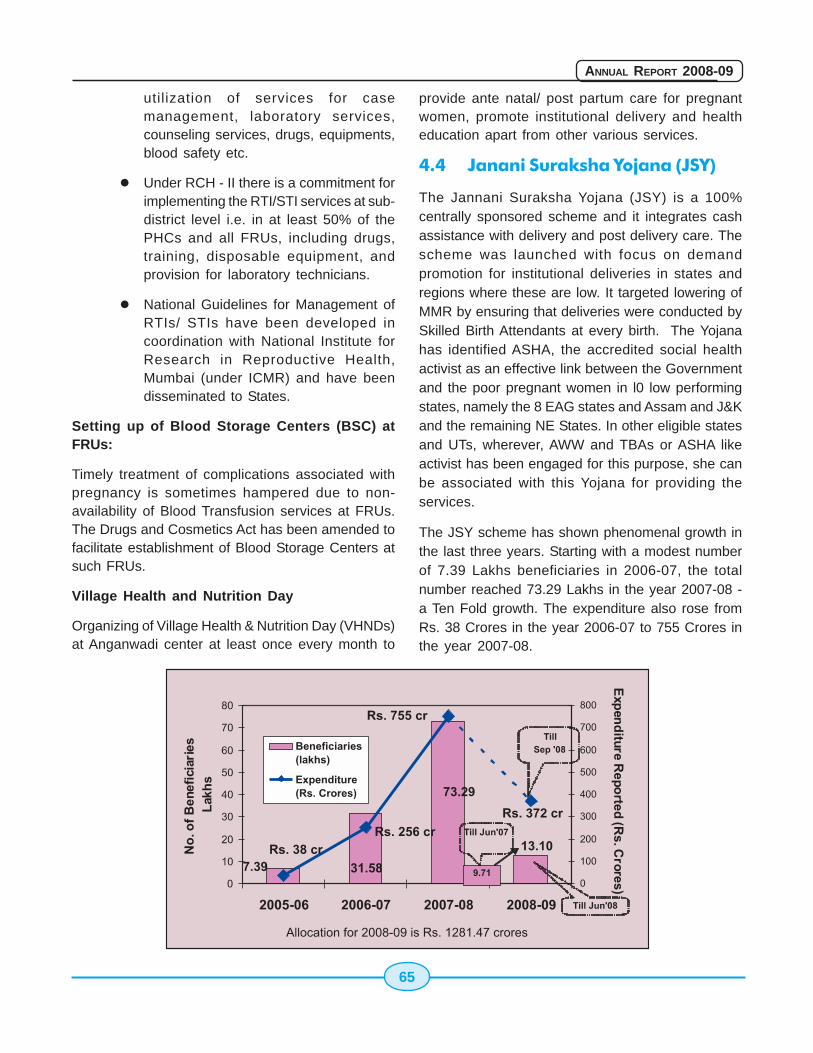
65
ANNUAL REPORT 2008-09
utilization of services for casemanagement, laboratory services,counseling services, drugs, equipments,blood safety etc.
� Under RCH - II there is a commitment forimplementing the RTI/STI services at sub-district level i.e. in at least 50% of thePHCs and all FRUs, including drugs,training, disposable equipment, andprovision for laboratory technicians.
� National Guidelines for Management ofRTIs/ STIs have been developed incoordination with National Institute forResearch in Reproductive Health,Mumbai (under ICMR) and have beendisseminated to States.
Setting up of Blood Storage Centers (BSC) atFRUs:
Timely treatment of complications associated withpregnancy is sometimes hampered due to non-availability of Blood Transfusion services at FRUs.The Drugs and Cosmetics Act has been amended tofacilitate establishment of Blood Storage Centers atsuch FRUs.
Village Health and Nutrition Day
Organizing of Village Health & Nutrition Day (VHNDs)at Anganwadi center at least once every month to
provide ante natal/ post partum care for pregnantwomen, promote institutional delivery and healtheducation apart from other various services.
4.4 Janani Suraksha Yojana (JSY)
The Jannani Suraksha Yojana (JSY) is a 100%centrally sponsored scheme and it integrates cashassistance with delivery and post delivery care. Thescheme was launched with focus on demandpromotion for institutional deliveries in states andregions where these are low. It targeted lowering ofMMR by ensuring that deliveries were conducted bySkilled Birth Attendants at every birth. The Yojanahas identified ASHA, the accredited social healthactivist as an effective link between the Governmentand the poor pregnant women in l0 low performingstates, namely the 8 EAG states and Assam and J&Kand the remaining NE States. In other eligible statesand UTs, wherever, AWW and TBAs or ASHA likeactivist has been engaged for this purpose, she canbe associated with this Yojana for providing theservices.
The JSY scheme has shown phenomenal growth inthe last three years. Starting with a modest numberof 7.39 Lakhs beneficiaries in 2006-07, the totalnumber reached 73.29 Lakhs in the year 2007-08 -a Ten Fold growth. The expenditure also rose fromRs. 38 Crores in the year 2006-07 to 755 Crores inthe year 2007-08.
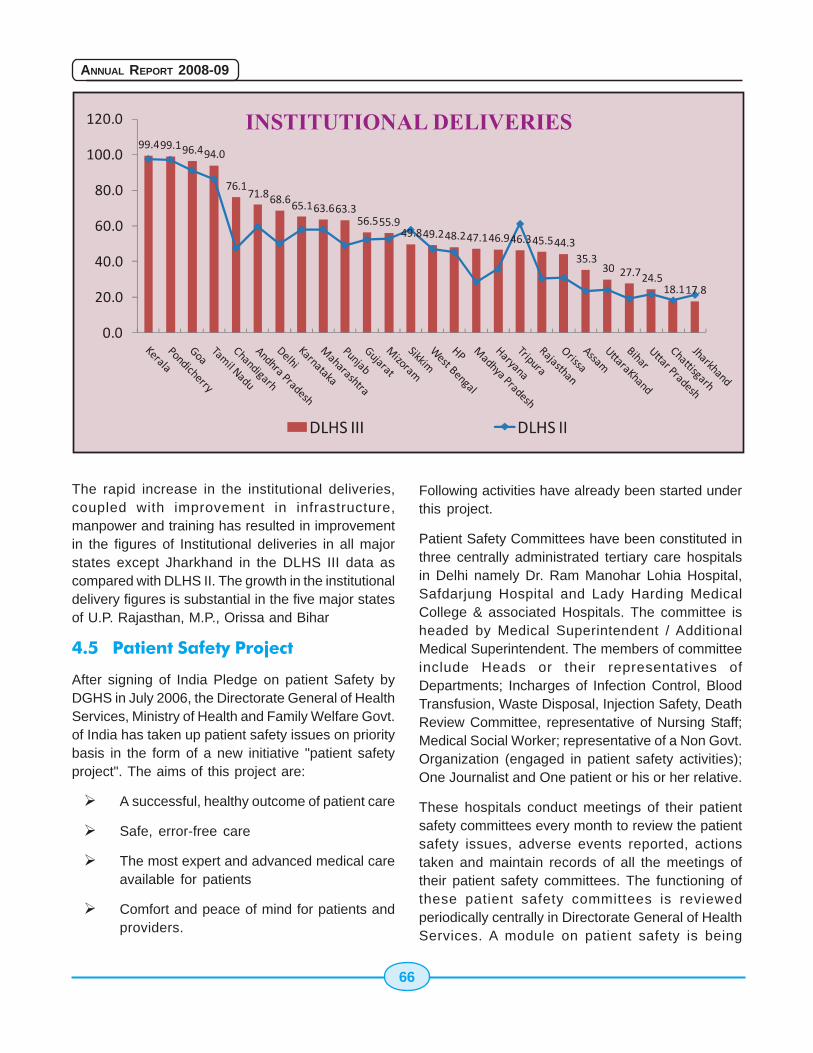
66
ANNUAL REPORT 2008-09
The rapid increase in the institutional deliveries,coupled with improvement in infrastructure,manpower and training has resulted in improvementin the figures of Institutional deliveries in all majorstates except Jharkhand in the DLHS III data ascompared with DLHS II. The growth in the institutionaldelivery figures is substantial in the five major statesof U.P. Rajasthan, M.P., Orissa and Bihar
4.5 Patient Safety Project
After signing of India Pledge on patient Safety byDGHS in July 2006, the Directorate General of HealthServices, Ministry of Health and Family Welfare Govt.of India has taken up patient safety issues on prioritybasis in the form of a new initiative "patient safetyproject". The aims of this project are:
� A successful, healthy outcome of patient care
� Safe, error-free care
� The most expert and advanced medical careavailable for patients
� Comfort and peace of mind for patients andproviders.
Following activities have already been started underthis project.
Patient Safety Committees have been constituted inthree centrally administrated tertiary care hospitalsin Delhi namely Dr. Ram Manohar Lohia Hospital,Safdarjung Hospital and Lady Harding MedicalCollege & associated Hospitals. The committee isheaded by Medical Superintendent / AdditionalMedical Superintendent. The members of committeeinclude Heads or their representatives ofDepartments; Incharges of Infection Control, BloodTransfusion, Waste Disposal, Injection Safety, DeathReview Committee, representative of Nursing Staff;Medical Social Worker; representative of a Non Govt.Organization (engaged in patient safety activities);One Journalist and One patient or his or her relative.
These hospitals conduct meetings of their patientsafety committees every month to review the patientsafety issues, adverse events reported, actionstaken and maintain records of all the meetings oftheir patient safety committees. The functioning ofthese patient safety committees is reviewedperiodically centrally in Directorate General of HealthServices. A module on patient safety is being
67
ANNUAL REPORT 2008-09
developed to upscale the skills of hospital staff inthe area of patient safety.
Following Performas have been introduced in the3 hospitals as mentioned above as part of patientsafety project.
i. Modified version of WHO Surgical Safetycheck list for use in Operation Theatre,to suit Indian requirements.
ii. Check list for safety of surgical patientsin the ward to be used by senior residentdoctors of Surgery & Anesthesia and Staffnurses.
iii. Patient safety evaluation Performa forobtaining feedback from patient or hisattendant at the time of discharge. The dataso obtained is analyzed for improvement ofservices from patient safety point of view.
iv. Adverse Event Reporting Performa:
Error reporting is encouraged through non-
punitive system. It is followed by Root Cause Analysisto find out why adverse event occurred and takingappropriate steps to avoid it in future.
Auto disabled syringes have been introduced forgiving injections in Centrally Administered Institutionswith effect from 1-4-09, to promote safe injectionpractices.Various other safety measures have beenintroduced like trainings in infection control and Bio-medical waste management for different levels ofHealth workers, implementation of WHO guidelineson Hand Hygiene in Health Care, both using soapand water and alcohol based formulation, devisingsafety norms for patients in vital areas of hospital,conducting regular death review meetings, trainingof senior resident doctors in giving D.C. shock,obtaining feedback from Grievance Cell,Implementation of Patient Safety Measures in OutPatient Departments in the form of Single WindowApproach, May I help you counter and proper signagesystem etc. Adequate emphasis is given to thesuggestions of patients and their attendants andaction taken to put them into practice.

68
ANNUAL REPORT 2008-09
69
ANNUAL REPORT 2008-09
Chapter 5
5.1 Introduction
In 1951, India was the first country in the world tolaunch a family planning programme. Since thenapproaches aimed at reducing population growthhave taken a variety of forms. The passive, clinic-based approach of the 1950s gave way to a moreproactive, extension approach in the early 1960s.The late 1960s saw the emergence of a "time-bound","target-oriented" approach with a massive effort topromote the use of IUDs and condoms. This wasfollowed by an even more forceful "camp approach"to promote male sterilization in the 1970s. Theexcesses of these campaigns lead to a backlash fromwhich it took years for the programme to recover.The 1980s saw the rebuilding of the programme withan emphasis on female sterilization, and maternaland child health. In the 1990s the InternationalConference on Population and Development, Cairoand the International Conference on Womenprompted a paradigm shift, with the advocacy of aclient-centred, need based, quality-orientedreproductive health approach. . The NationalPopulation Policy of 2000 and the National HealthPolicy 2002 took cognisance of this and accordinglybroadened the perspective of the National FamilyWelfare programme and renamed it theReproductive and Child Health programme and set2010 as the target date to achieve replacement-levelfertility.
Method-specific targets were removed, and theprogramme focused on the unmet needs of clients.RCH II continues with this approach Technologicallythe programme has attempted to keep pace with the
technological advances in the world of medicine byincorporating them in the programme as and whenthe planners felt that these advances fulfilled the feltneeds of the community. Hence over the yearsmethods like the lippes loop (incorporated into theprogramme during the third Five Year Plan) and theNational Health Policy 1983 envisionedsignificant reduction in IMR, NMR & CMR by2000. All the child health programmes aredirected towards achieving these goals.
India is a signatory to the Millenium DevelopmentGoals(MDGs).The fourth Millenium DevelopmentGoal is reduction of child mortality and the target forthis is to reduce by two thirds, between 1990-2015the mortality rate of children under five. This isreflected in the Tenth Five Year Plan (2002-07),which states that Infant Mortality Rate is to bereduced to 45/1000 by 2007 and 28/1000 live birthsby 2012.
5.2 Infant Mortality Rate
Status
Infant mortality, currently at 58 per 1000 livebirths(2005), has declined substantially(by 35%) overthe past 15 years. Manipur has the lowest IMR (13 /1000 live births) and Madhya Pradesh is the highestat 76 per 1000 live births. Infant mortality rates havedeclined in both urban(40/1000 live births) and ruralareas(64/1000 live births). Higher rates of ante-natal,delivery and post natal care are usually associatedwith lower infant mortality. Such an inverserelationship is observed with higher education statusof mothers and a higher standard of living index.
Child Health ProgrammeChild Health ProgrammeChild Health ProgrammeChild Health ProgrammeChild Health Programme
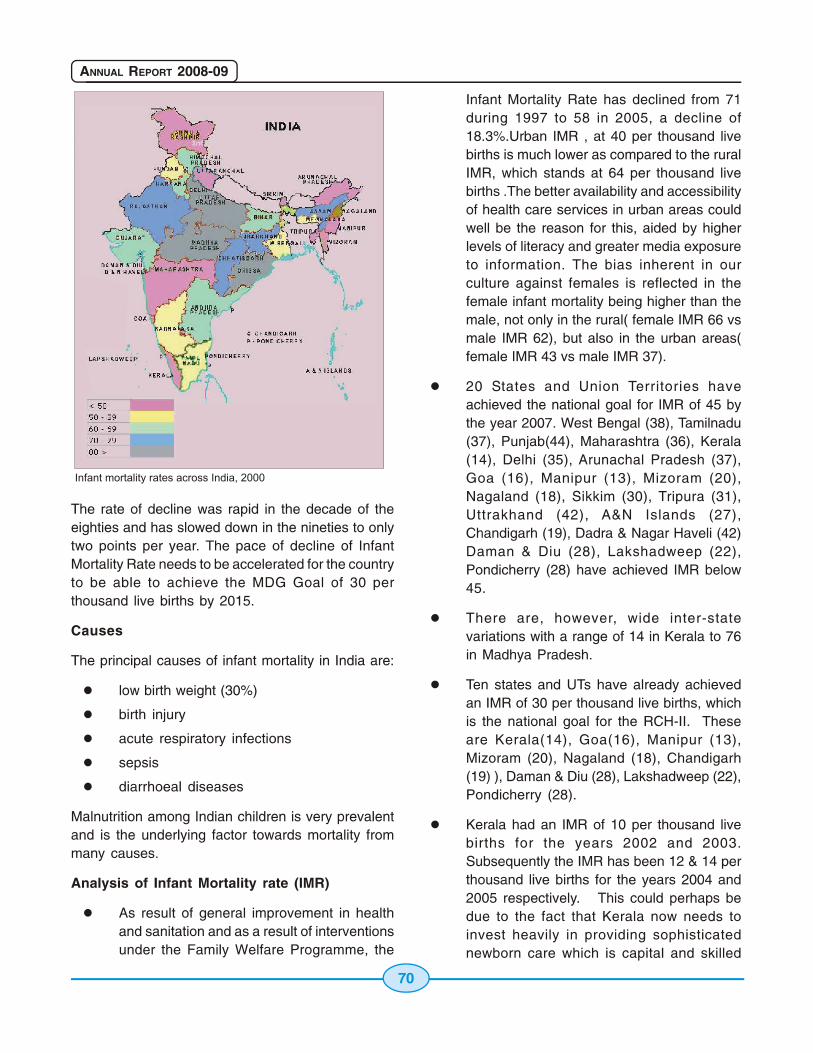
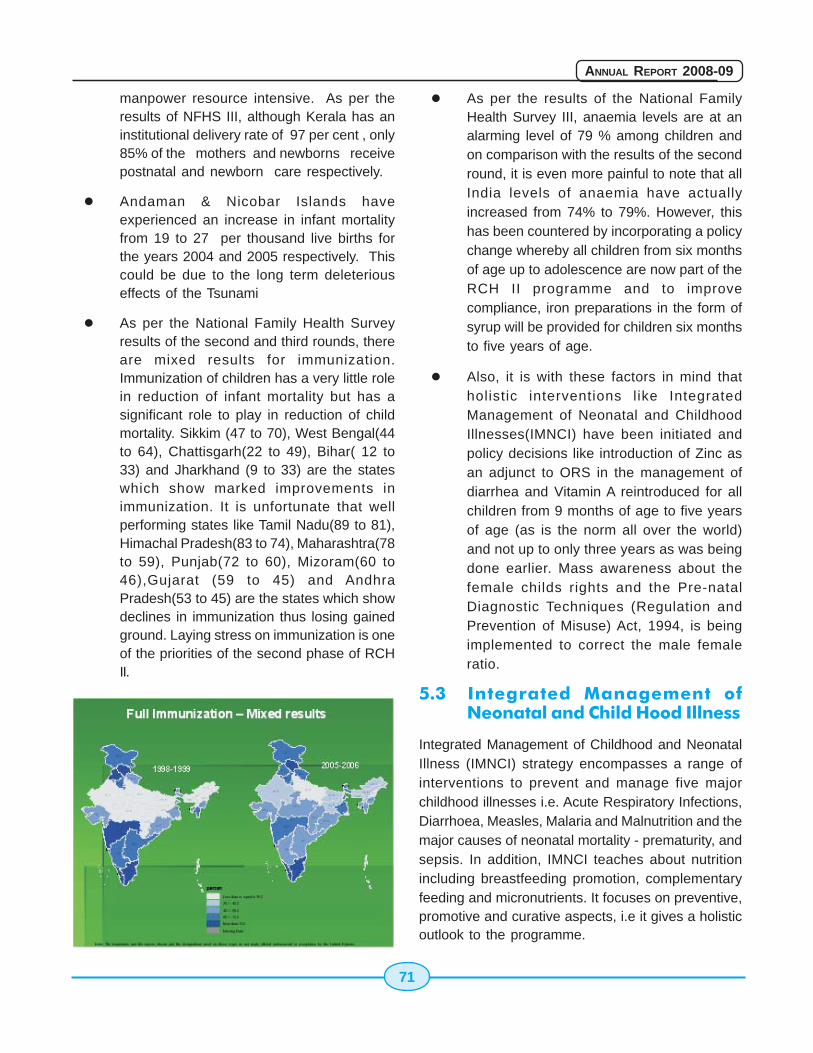
71
ANNUAL REPORT 2008-09
manpower resource intensive. As per theresults of NFHS III, although Kerala has aninstitutional delivery rate of 97 per cent , only85% of the mothers and newborns receivepostnatal and newborn care respectively.
� Andaman & Nicobar Islands haveexperienced an increase in infant mortalityfrom 19 to 27 per thousand live births forthe years 2004 and 2005 respectively. Thiscould be due to the long term deleteriouseffects of the Tsunami
� As per the National Family Health Surveyresults of the second and third rounds, thereare mixed results for immunization.Immunization of children has a very little rolein reduction of infant mortality but has asignificant role to play in reduction of childmortality. Sikkim (47 to 70), West Bengal(44to 64), Chattisgarh(22 to 49), Bihar( 12 to33) and Jharkhand (9 to 33) are the stateswhich show marked improvements inimmunization. It is unfortunate that wellperforming states like Tamil Nadu(89 to 81),Himachal Pradesh(83 to 74), Maharashtra(78to 59), Punjab(72 to 60), Mizoram(60 to46),Gujarat (59 to 45) and AndhraPradesh(53 to 45) are the states which showdeclines in immunization thus losing gainedground. Laying stress on immunization is oneof the priorities of the second phase of RCHII.
� As per the results of the National FamilyHealth Survey III, anaemia levels are at analarming level of 79 % among children andon comparison with the results of the secondround, it is even more painful to note that allIndia levels of anaemia have actuallyincreased from 74% to 79%. However, thishas been countered by incorporating a policychange whereby all children from six monthsof age up to adolescence are now part of theRCH II programme and to improvecompliance, iron preparations in the form ofsyrup will be provided for children six monthsto five years of age.
� Also, it is with these factors in mind thatholistic interventions like IntegratedManagement of Neonatal and ChildhoodIllnesses(IMNCI) have been initiated andpolicy decisions like introduction of Zinc asan adjunct to ORS in the management ofdiarrhea and Vitamin A reintroduced for allchildren from 9 months of age to five yearsof age (as is the norm all over the world)and not up to only three years as was beingdone earlier. Mass awareness about thefemale childs rights and the Pre-natalDiagnostic Techniques (Regulation andPrevention of Misuse) Act, 1994, is beingimplemented to correct the male femaleratio.
5.3 Integrated Management ofNeonatal and Child Hood Illness
Integrated Management of Childhood and NeonatalIllness (IMNCI) strategy encompasses a range ofinterventions to prevent and manage five majorchildhood illnesses i.e. Acute Respiratory Infections,Diarrhoea, Measles, Malaria and Malnutrition and themajor causes of neonatal mortality - prematurity, andsepsis. In addition, IMNCI teaches about nutritionincluding breastfeeding promotion, complementaryfeeding and micronutrients. It focuses on preventive,promotive and curative aspects, i.e it gives a holisticoutlook to the programme.
72
ANNUAL REPORT 2008-09
The major components of this strategy are:
� Strengthening the skills of the health careworkers
� Strengthening the health care infrastructure
� Involvement of the community
The first two components are the facility based IMNCIand the third is the community based IMNCI.
5.3.1 Goals
Current NRHM MDGstatus 2012 2015
IMR (Infant 58 30 27Mortality Rate) (SRS 2005)
NMR 37 < 20* < 19*(Neonatal (SRS 2004)Mortality Rate)
*Estimated
5.4 Home Based New Born Care
The Government of India has recently approved theimplementation of Home Based NewbornCare(HBNC) based on the Gadchirolli model , whereappreciable decline in Infant Mortality Rates has beendocumented on the basis of work done by SEARCH,a NGO. ASHAs will be trained in identified aspectsof newborn care during the second year of theirtraining. The modules have been finalized and statesensitization workshops have been held. In the fivehigh focus states to be covered under the IndoNorway Initiative , the HBNC shall be implementedby SEARCH with support from ICMR. Permission hasbeen accorded in 2 districts in each of these fivestates(- MP, UP, Orissa, Rajasthan and Bihar) forASHAs to use injectable antibiotics for neonatal sepsisand childhood pneumonia.
5.5 Facility Based New Born Care
The facility based newborn care programmeimplanted by the Government in 140 districts withtechnical assistance from the National NeonatologyForum(NNF) has been evaluated and based on this
feedback, a facility based newborn care programmeis being set up.
Level II sick newborn units have been proposed bythe states in their RCH II PIPs and are being set upthroughout the country in a phased manner, initiallyat district hospitals. Facilities have been establishedat Purulia, Birbhum, Cooch behar, Uttar Dinajpur andBankura, Udaipur, Jaipyr, Bhilwada, Tonk, Guna,Vaishali, Lalitpur, Guwahati, Nadia, Burdwan, Malda,North 24 Parganas (Barasat) and Darjeeling(Siliguri).
5.6 Vitamin - A
Objective
With the objective of decreasing the prevalence ofVitamin A deficiency to levels below 0.5%, the strategybeing implemented is:
Strategy
Infancy
� Health and nutrition education is being takenup to encourage colostrums feeding,exclusive breastfeeding for the first sixmonths and the introduction ofcomplementary feeding thereafter.
� 1,00,000 IU dose of Vitamin A is being givenat nine months
Childhood
� Health education efforts to ensure adequateintake of Vitamin A rich food throughoutchildhood
� Early detection and prompt treatment ofinfections
� Vitamin A dose of 1,00,000 IU at 9 monthsand 2,00,000 I.U thereafter at six monthlyintervals up to five years of age.
Sick children
� All children with xerophthalmia to be treatedat health facilities
� All children suffering from measles to be
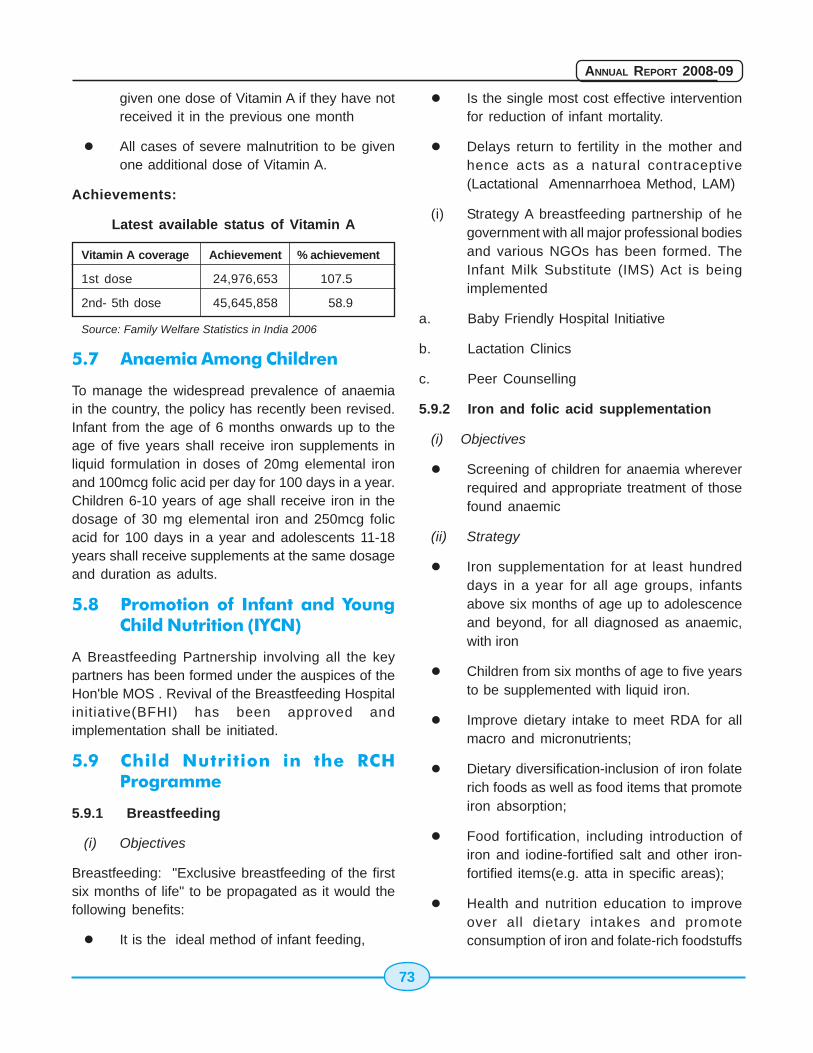
73
ANNUAL REPORT 2008-09
given one dose of Vitamin A if they have notreceived it in the previous one month
� All cases of severe malnutrition to be givenone additional dose of Vitamin A.
Achievements:
Latest available status of Vitamin A
Vitamin A coverage Achievement % achievement
1st dose 24,976,653 107.5
2nd- 5th dose 45,645,858 58.9
Source: Family Welfare Statistics in India 2006
5.7 Anaemia Among Children
To manage the widespread prevalence of anaemiain the country, the policy has recently been revised.Infant from the age of 6 months onwards up to theage of five years shall receive iron supplements inliquid formulation in doses of 20mg elemental ironand 100mcg folic acid per day for 100 days in a year.Children 6-10 years of age shall receive iron in thedosage of 30 mg elemental iron and 250mcg folicacid for 100 days in a year and adolescents 11-18years shall receive supplements at the same dosageand duration as adults.
5.8 Promotion of Infant and YoungChild Nutrition (IYCN)
A Breastfeeding Partnership involving all the keypartners has been formed under the auspices of theHon'ble MOS . Revival of the Breastfeeding Hospitalinitiative(BFHI) has been approved andimplementation shall be initiated.
5.9 Child Nutrition in the RCHProgramme
5.9.1 Breastfeeding
(i) Objectives
Breastfeeding: "Exclusive breastfeeding of the firstsix months of life" to be propagated as it would thefollowing benefits:
� It is the ideal method of infant feeding,
� Is the single most cost effective interventionfor reduction of infant mortality.
� Delays return to fertility in the mother andhence acts as a natural contraceptive(Lactational Amennarrhoea Method, LAM)
(i) Strategy A breastfeeding partnership of hegovernment with all major professional bodiesand various NGOs has been formed. TheInfant Milk Substitute (IMS) Act is beingimplemented
a. Baby Friendly Hospital Initiative
b. Lactation Clinics
c. Peer Counselling
5.9.2 Iron and folic acid supplementation
(i) Objectives
� Screening of children for anaemia whereverrequired and appropriate treatment of thosefound anaemic
(ii) Strategy
� Iron supplementation for at least hundreddays in a year for all age groups, infantsabove six months of age up to adolescenceand beyond, for all diagnosed as anaemic,with iron
� Children from six months of age to five yearsto be supplemented with liquid iron.
� Improve dietary intake to meet RDA for allmacro and micronutrients;
� Dietary diversification-inclusion of iron folaterich foods as well as food items that promoteiron absorption;
� Food fortification, including introduction ofiron and iodine-fortified salt and other iron-fortified items(e.g. atta in specific areas);
� Health and nutrition education to improveover all dietary intakes and promoteconsumption of iron and folate-rich foodstuffs
74
ANNUAL REPORT 2008-09
(iii) Infants:
� Exclusive breast feeding for six months, andintroduction of green leafy vegetables alongwith cereal/pulse/oilseed mix in the seventhmonth for the prevention of anaemia;
� Screening for anaemia in pre-term , low birthweight infants and those with growth falteringand repeated episodes of infection; and
� Appropriate treatment for anaemic infants.
(iv) Preschool Children
� advocacy with regard to dietary diversificationfor the prevention of anaemia;
� all growth retarded children and those withrepeated infections have to have HBestimation carried out and
� those found to be anaemic are provided withappropriate treatment.
In hookworm endemic areas, it is necessary toimprove:
� sanitation and educate people not to walkbarefoot;
� treat children with a history of passing wormswith broad spectrum antihelminthics;
� screen all anaemic children for hookworminfestation and treat them
The co-operation of the PRIs and womens' self helpgroups, where ever existent, may be sought topromote and monitor intake of IFA tablets in theircommunity.
(v) Coverage
� As per a survey carried out in 2002 by theNational Nutrition Monitoring Bureau, underthe ICMR, 67% of the preschool children wereanaemic.
� 2,84,729 kits are distributed throughout thecountry each year under the RCHprogramme, each kit containing 13,000tablets of paediatric IFA tablets.
(vi) Implementation
Through the health institutions under the governmentsector
5.10 Routine ImmunizationProgramme
Immunization programme is one of the keyinterventions for protection of children from lifethreatening conditions, which are preventable.Immunization Programme in India was introduced in1978 as Expanded Programme of Immunization. Thisgained momentum in 1985 as Universal ImmunizationProgramme (UIP) and implemented in phasedmanner to cover all districts in the country by 1989-90. UIP become a part of Child Survival and SafeMotherhood Programme in 1992. Since, 1997,immunization activities have been an importantcomponent of National Reproductive and Child HealthProgramme. Immunization is one of the key areasunder National Rural Health Mission (NRHM)launched in 2005.
Under the Immunization Programme Government ofIndia is providing vaccination to prevent six vaccinepreventable diseases i.e. Tuberculosis, Diphtheria,Pertussis, Tetanus, Polio, and Measles. Thevaccination schedule is as under:
� BCG (Bacillus Calmetter-Guèrin)- Birth
� DPT ( Diphtheria, Pertussis and TetanusToxoid )- 6,10,14 weeks and at 16-24 monthsof age
� OPV (Polio)- 6,10,14 weeks & 16-24 monthsof age and birth dose for institutional delivery
� Measles - 9-12 months of age
� DT (Diphtheria and Tetanus Toxoid) - 5 yearsof age
� TT (Tetanus Toxoid ) - 10 years and 16 yearsof age
� TT - for pregnant woman two doses or onedose if previously vaccinated within 3 years
The Immunization coverage of vaccines underRoutine Immunization as per NFHS-II and NFHS-III
75
ANNUAL REPORT 2008-09
data is enclosed. To improve the coverage in lowperforming NE States, Speical Immunization weeksare being observed in the NE States along with EAGStates from the year 2005-06 every year.
To further strengthen the Routine Immunization, withthe aim to improve the coverage, Government of Indiahas taken the following initiatives as part of NRHM:
� Introduction of AD syringes for allimmunization replacing the existing glasssyringe and needles.
� Downsizing the BCG vial from 20 dose to 10dose.
� Plans for alternate vaccine delivery from PHCto Sub centre and outreach sessions.
� Outsourcing immunization activities in urbanslums and under served areas.
� Strengthening supervision and monitoring.
� Mobility support to District Immunization officerfor supportive supervision and monitoring.
� Review meeting at the State level with thedistricts on 6 monthly basis.
� Mobilization of children to immunizationsession sites by Accredited Social HealthActivist. (ASHA), Link workers, Women SelfHelp Groups etc.
All the States/UTs are asked to prepare their ownState Programme Implementation Plan (PIP) forImmunization as part 'C' of NRHM PIP from the year2005-06 to address their specific needs.
5.10.1 Status of Routine Immunization
To strengthen Routine Immunization Government ofIndia under NRHM has launched newer initiatives aspart of the State Programme Implementation Plan(PIP), some initiatives are:
� To ensure injection safety, Auto Disable (AD)Syringe introduced throughout country.
� Support for alternate vaccine delivery fromPHC to Sub-Centres and Outreach Sessions.
� Provision for deploying additional manpowerto carryout Immunization activities in urbanslums and underserved areas where servicesare deficient.
� Mobility support to State Immunization Officer,District Immunization Officer and other Officeras per State Plan for monitoring andsupportive supervision.
� Review meeting at the State level with thedistricts on 6 monthly intervals.
� Training of ANM, Cold Chain Handlers, MidLevel Managers, Refrigerator Mechanics etc.
� Support for mobilization of children toimmunization session sites by AccreditedSocial Health Activist (ASHA), Women SelfHelp Groups etc.
� One Computer Assistant to State HeadQuarter and each District.
� Printing of Immunization Cards and othertools like tickler bag, tally sheet, monitoringchart, Cold Chain temperature monitoringchart, vaccine inventory charts etc.
� Implementation of Routine ImmunizationMonitoring System (RIMS) software.
� Support for other specific issues.
� In addition the central support of the followingwill continue under Immunization as suppliesto States -
� Strengthening of cold chain system in theState
� Cold Chain Maintenance
� Supply of vaccines
� Supply of vaccine van at the rate of one perdistrict
5.11 Introduction of Hepatitis - BVaccine
A pilot project for the introduction of Hepatitis-Bvaccine in the National Immunization Programme was

76
ANNUAL REPORT 2008-09
approved by the Government and launched byHon'ble Prime Minister on 10th June 2002. Underthe pilot project 33 districts and 15 metropolitan citiesimplemented Hepatitis B vaccination. The currentschedule includes birth dose along with earlier 3doses.
Vaccine and syringes are being made available byGlobal Alliance for Vaccine and Immunization (GAVI)for the expansion programme. Expenditure for IEC,training and monitoring budget is being incurredthrough the domestic funds.
5.11.1 The progress of Hepatitis-B project
After the success of pilot project, the Hepatitis Bprogramme has been expanded to 10 states viz.Andhra Pradesh, Himachal Pradesh, Jammu &Kashmir, Karnataka, Kerala, Madhya Pradesh,Maharashtra, Punjab, Tamil Nadu and West Bengalin phased manner. As on 2008, the overall coverageof infants in 11 districts and 6 cities, which have beencontinuing Hep-B vaccination since the pilot project,is 56.7%. The overall coverage of infants in the 10states is 39.0 %.
5.11.2 Introduction of Japanese Encephalitis(JE) Vaccine
JE Vaccination was started 2006 in 11 districts and 4states using SA-14-14-2, with 88% of the targeted10.5 million children in the 12 month to 15 years ageimmunized. In 2007, 27 districts in 10 states werecovered with 75% of the targeted 22.0 million childrenin the 12 month to 15 years age immunized. In 2008,24 more endemic districts have been added.
The JE vaccine is being integrated into routineimmunization in the districts where campaign hadalready been conducted to immunize theunimmunized cohort of children by vaccinating withsingle dose at 16-18 months
5.12 Pulse Polio Immunization
In pursuance to the World Health Assemblyresolution No. 1988/41.28 pulse Polio Immunization(PPI) Programme was started in India from 1995 toeradicate Polio from India. Following the successful
pilot undertaking in Delhi in 1994, Nation-wide PPIrounds was undertaking in 1995 covering childrenin the age group of 0-3 years from 1996-97 the agecohort for vaccination was started to cover 0-5 yearschildren. Till 1998-99 two rounds used to beorganized in the month of December and Januaryeach year. From 1999-2000 house to housevaccination of missed children was also introducedto vaccinate children missed during the fixed boothbased vaccination of children. This resulted inincreasing coverage of 2-3 crore additional children.
5.12.2 The annual strategy for polio eradication isdecided on the basis of the recommendations of theIndia Expert and International Experts from WorldHealth Organization (WHO), United Nation's ChildrenFund (UNICEF), and Centre for Disease Control(CDC) Atlanta. The IEAG reviews the Polioepidemiological situation two times a day andrecommend the suitable strategies for the country.The National Polio Surveillance Project( NPSP) ofWHO provides technical support for high qualityAcute Flaccid Paralysis(AFP) surveillance and assiststhe government in micro planning, training andmonitoring of polio immunization campaign.
5.12.3 Since the initiative to eradicate polio fromIndia started in 1995, significant success has beenachieved in reducing number of polio cases in thecountry and total cases decline gradually to only 66cases in 2005. Out of 35 States & UTs, 33 States &UTs were free from indigenous transmission of poliovirus since last three years. It is taking more times inUP and Bihar to achieve zero transmission due tofactors like high population density and poorsanitation.
5.12.4 In order to achieve the goal of zerotransmission at the earliest, the strategy in UP andBihar has been modified to have increased numberof polio immunization campaign with Monovalentvaccine type I (mOPV 1) as per the recommendationof India Expert Advisory Group on polio to target thePolio virus type 1 and polio virus type 3 sequentially.
5.12.5. As a result of this strategy, there has been asignificant decline in the number of cases caused by
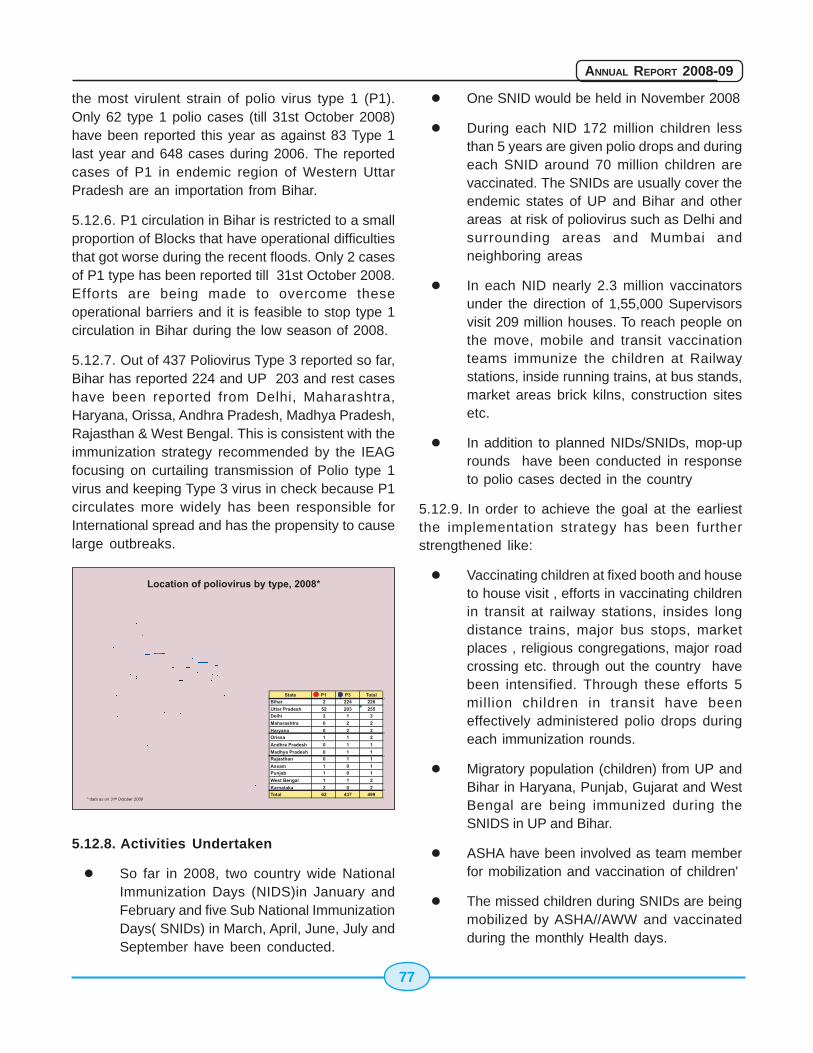
77
ANNUAL REPORT 2008-09
the most virulent strain of polio virus type 1 (P1).Only 62 type 1 polio cases (till 31st October 2008)have been reported this year as against 83 Type 1last year and 648 cases during 2006. The reportedcases of P1 in endemic region of Western UttarPradesh are an importation from Bihar.
5.12.6. P1 circulation in Bihar is restricted to a smallproportion of Blocks that have operational difficultiesthat got worse during the recent floods. Only 2 casesof P1 type has been reported till 31st October 2008.Efforts are being made to overcome theseoperational barriers and it is feasible to stop type 1circulation in Bihar during the low season of 2008.
5.12.7. Out of 437 Poliovirus Type 3 reported so far,Bihar has reported 224 and UP 203 and rest caseshave been reported from Delhi, Maharashtra,Haryana, Orissa, Andhra Pradesh, Madhya Pradesh,Rajasthan & West Bengal. This is consistent with theimmunization strategy recommended by the IEAGfocusing on curtailing transmission of Polio type 1virus and keeping Type 3 virus in check because P1circulates more widely has been responsible forInternational spread and has the propensity to causelarge outbreaks.
5.12.8. Activities Undertaken
� So far in 2008, two country wide NationalImmunization Days (NIDS)in January andFebruary and five Sub National ImmunizationDays( SNIDs) in March, April, June, July andSeptember have been conducted.
� One SNID would be held in November 2008
� During each NID 172 million children lessthan 5 years are given polio drops and duringeach SNID around 70 million children arevaccinated. The SNIDs are usually cover theendemic states of UP and Bihar and otherareas at risk of poliovirus such as Delhi andsurrounding areas and Mumbai andneighboring areas
� In each NID nearly 2.3 million vaccinatorsunder the direction of 1,55,000 Supervisorsvisit 209 million houses. To reach people onthe move, mobile and transit vaccinationteams immunize the children at Railwaystations, inside running trains, at bus stands,market areas brick kilns, construction sitesetc.
� In addition to planned NIDs/SNIDs, mop-uprounds have been conducted in responseto polio cases dected in the country
5.12.9. In order to achieve the goal at the earliestthe implementation strategy has been furtherstrengthened like:
� Vaccinating children at fixed booth and houseto house visit , efforts in vaccinating childrenin transit at railway stations, insides longdistance trains, major bus stops, marketplaces , religious congregations, major roadcrossing etc. through out the country havebeen intensified. Through these efforts 5million children in transit have beeneffectively administered polio drops duringeach immunization rounds.
� Migratory population (children) from UP andBihar in Haryana, Punjab, Gujarat and WestBengal are being immunized during theSNIDS in UP and Bihar.
� ASHA have been involved as team memberfor mobilization and vaccination of children'
� The missed children during SNIDs are beingmobilized by ASHA//AWW and vaccinatedduring the monthly Health days.
78
ANNUAL REPORT 2008-09
� Strategy to involve the leaders and opinionmakers of the underserved committee is beingadopted in Western U.P. districts to involvedthe community better in the programme
5.13 Cold Chain System VaccineStorage At PHC/CHC Level
The National Cold Chain Assessment has beenconducted in the country with support of UNICEF andWHO to assess the gaps and take necessary actionsto strengthen the cold chain. The cold chain systemconsists of a series of transportation & storagefacilities for vaccines from the manufacturers to thebeneficiaries at a recommended temperature. Morethan 72000 units consisting of the followingequipments have been supplied to the States forstoring the vaccines:
1. Walk-in-Coolers and Walk-in-FreezersRooms: These are supplied at State/Regional Level to maintain a vaccine stockrequired for 3 months in its catchment area.There are at present 161 walk in coolers and36 walk in freezers installed at variouslocations of the States in the country.
2. Ice Lined Refrigerators (Large) and DeepFreezers (Large) at the District Level:6300 numbers ILRs (L) and Deep Freezers(L) have been supplied. At the district storesDeep Freezers can be used for storing Poliovaccine at below (-)15 Centigrade.
3. A Twin set of ILR/Deep Freezer: Thesehave been supplied in pairs to all PHCs,where a stock of one month's requirement ofvaccines is maintained. 65700 such unitshave been supplied to different healthinstitutions.
5.14 Reproductive & Child Health- II(RCH II)
In order to effectively improve the health status ofwomen and children and fulfill the unmet need forFamily Welfare services in the country, especiallythe poor and under served by reducing infant childand maternal mortality and morbidity, Government
of India during 1997-98 launched the RCHProgramme for implementation during the 9th planperiod by integrating Child Survival and SafeMotherhood (CSSM) Programme with otherreproductive and child health (RCH) services. Inaddition, a new component for management ofReproductive Tract Infection (RTI) and SexuallyTransmitted Infection (STI) has also beenincorporated. The RCH Programme is partly fundedby World Bank, UNICEF, UNFPA and EuropeanCommission etc. Reproductive and Child HealthProgram is in 5th year of its operation and is currentlyoperational in entire country. The program follows adifferential strategy with inputs under the programlinked to the needs of the area coupled with thecapacity for implementation. The program wasreviewed extensively not only in context ofachievements during mid-term stage, but also incontext of National Population Policy.
Efforts were made to strengthen the routineimmunization as well as PPI by launching a projectfor Immunization Strengthening with the World Bankassistance. The ongoing activities were acceleratedand new schemes on Financial Envelop, Dais'Training, RCH Camps and RCH out reach serviceswere started to address felt gaps. The implementationof EC assisted Sector Investment Programme hasgeared up, especially State/District level activities andurban RCH component.
Under the Reproductive and Child Health Programme(RCH) being implemented in all States of the countryvarious interventions for reduction of infant mortalityrate are being implemented. These includeimmunization against fixed vaccine communicablediseases, control of death during diarrhea, controlof deaths due to acute respiratory infections;prophylaxis against vitamin A deficiency and irondeficiency anemia. Essential new born care andpromotion of exclusive breastfeeding andappropriate complementary feeding practices.Unequal access of pregnant women in rural areasand those in the lower socio economic bracket isrecognized as an important issue. Provision has beenkept under the National Rural Health Mission tostrengthen the services at village and sub-center level
79
ANNUAL REPORT 2008-09
and also for provision of transport facilities topregnant women needing emergency treatment.
Integrated Management of Neonatal and ChildhoodIllnesses(IMNCI) package will be implemented in aphased manner throughout the country in the secondphase of the RCH programme. It offers acomprehensive package for the management of themost common causes of childhood illnesses i.esepsis, measles, malaria, diarrhoea, pneumonia andmalnutrition. It is supported by appropriatestrengthening of the health care system andpromotion of positive health care practices of thecommunity.
Integrated Management of Childhood Illness (IMCI)strategy, which has already been implemented inmore than 100 countries all over the globe,encompasses a range of interventions to preventand manage five major childhood illnesses i.e. AcuteRespiratory Infections, Diarrhoea, Measles, Malariaand Malnutrition. It focuses on preventive, promotiveand curative aspects, i.e it gives a holistic outlook tothe programme.
Govt. of India recognized the need to strengthen childhealth activities in the country. In order to strengthenChild Health activities and introduce IMCI in thecountry, a Core Group was constituted which includedrepresentatives from Indian Academy of Pediatrics(IAP), National Neonatology Forum of India (NNF),National Anti Malaria Program (NAMP), Departmentof Women and Child Development (DWCD), Child-in-Need Institute (CINI), WHO, UNICEF, eminentPediatricians and Neonatologists, and the
representatives from Ministry of Health and FamilyWelfare Government of India. The Adaptation Groupdeveloped Indian version of IMCI guidelines andrenamed it as Integrated Management of Neonataland Childhood Illness (IMNCI).
The major components of this strategy are:
� Strengthening the skills of the health careworkers
� Strengthening the health care infrastructure
� Involvement of the community
The major highlights of Indian adaptation are:
� Incorporation of neonatal care as it nowconstitutes two thirds of infant mortality
� Inclusion of 0-7 days
� Incorporating National guidelines on Malaria,Anemia, Vitamin A supplementation andImmunization schedule
� Training schedule reduced from 11 to 8 days
� Training begins with sick young infant upto 2months
� Proportion of training time devoted to sickyoung infant and sick child is almost equal
The Government has initiated implementationof the IMNCI strategy in four districts each in nineselected states of Orissa, Rajasthan, MadhyaPradesh, Haryana, Delhi, Gujarat, Uttaranchal, TamilNadu and Rajasthan.
TAMIL NADU MATERNAL AND NEONATAL HEALTH PROJECT
Tamil Nadu, a South Indian state, has a MMR of 115/ 100,000 live births compared to thenational figures. The IMR in this state is just 37/1000 live births vis-à-vis a nationally reportedfigure of 58/1000. The main interventions responsible for this rapid progress were the growthof safe deliveries and provision of Emergency obstetric care.
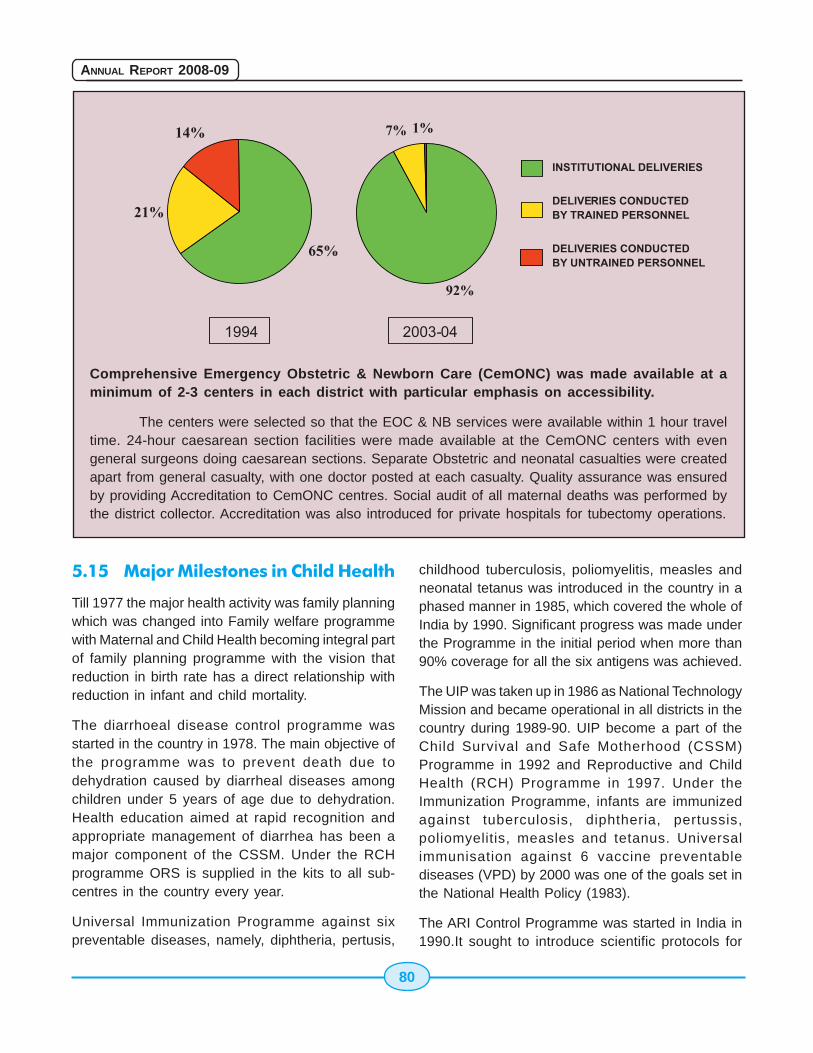
80
ANNUAL REPORT 2008-09
Comprehensive Emergency Obstetric & Newborn Care (CemONC) was made available at aminimum of 2-3 centers in each district with particular emphasis on accessibility.
The centers were selected so that the EOC & NB services were available within 1 hour traveltime. 24-hour caesarean section facilities were made available at the CemONC centers with evengeneral surgeons doing caesarean sections. Separate Obstetric and neonatal casualties were createdapart from general casualty, with one doctor posted at each casualty. Quality assurance was ensuredby providing Accreditation to CemONC centres. Social audit of all maternal deaths was performed bythe district collector. Accreditation was also introduced for private hospitals for tubectomy operations.
5.15 Major Milestones in Child Health
Till 1977 the major health activity was family planningwhich was changed into Family welfare programmewith Maternal and Child Health becoming integral partof family planning programme with the vision thatreduction in birth rate has a direct relationship withreduction in infant and child mortality.
The diarrhoeal disease control programme wasstarted in the country in 1978. The main objective ofthe programme was to prevent death due todehydration caused by diarrheal diseases amongchildren under 5 years of age due to dehydration.Health education aimed at rapid recognition andappropriate management of diarrhea has been amajor component of the CSSM. Under the RCHprogramme ORS is supplied in the kits to all sub-centres in the country every year.
Universal Immunization Programme against sixpreventable diseases, namely, diphtheria, pertusis,
childhood tuberculosis, poliomyelitis, measles andneonatal tetanus was introduced in the country in aphased manner in 1985, which covered the whole ofIndia by 1990. Significant progress was made underthe Programme in the initial period when more than90% coverage for all the six antigens was achieved.
The UIP was taken up in 1986 as National TechnologyMission and became operational in all districts in thecountry during 1989-90. UIP become a part of theChild Survival and Safe Motherhood (CSSM)Programme in 1992 and Reproductive and ChildHealth (RCH) Programme in 1997. Under theImmunization Programme, infants are immunizedagainst tuberculosis, diphtheria, pertussis,poliomyelitis, measles and tetanus. Universalimmunisation against 6 vaccine preventablediseases (VPD) by 2000 was one of the goals set inthe National Health Policy (1983).
The ARI Control Programme was started in India in1990.It sought to introduce scientific protocols for

81
ANNUAL REPORT 2008-09
case management of pneumonia with co-trimoxazole.Initially 14 pilot districts were selected and later onnew districts were included. A review of the healthfacility done in 1992 revealed that although 87% ofpersonnel were trained and the drug supply wasregular yet there were problems in correct caseclassification and treatment. Since 1992 theProgramme was implemented as part of CSSM andlater with RCH. Cotrimoxazole tablets are suppliedas part of drug kit for use by different category ofworkers for managing cases of Pneumonia. UnderRCH-II activities are proposed to be implemented inan integrated way with other child healthinterventions.
The Child Survival and Safe Motherhood Programmejointly funded by World Bank and UNICEF werestarted in 1992-93 for implementation up to 1997-98. The Child Survival and Safe MotherhoodProgramme were implemented in a phased mannercovering all the districts of the country by the year1996-97. The objectives of the programmes were toimprove the health status of infants, child and
maternal morbidity and mortality. The programmesseek to sustain high coverage levels achieved underthe Universal Immunisation Programme (UIP) in goodperformance areas and strengthen the immunisationservices of poor performing areas. The programmealso provides for augmenting various activities underthe Oral Rehydration Therapy (ORT) Programme,universalising prophylaxis schemes for control ofanemia in pregnant women & control of blindness inchildren and initiating a programme for control ofacute respiratory infection (ARI) in children. Underthe safe motherhood component, training oftraditional birth attendants (TBA), provision ofasceptic delivery kits and strengthening of firstreferral units to deal with high risk and obstetricemergencies were taken up. The approved outlayfor the CSSM Programme was Rs. 1125.58 croresfor the entire IDA credit facility of SDR period. TheProgramme yielded notable success in improving thehealth status of pregnant women, infants and children& also making a dent in IMR, MMR and incidence ofvaccine preventable diseases.

82
ANNUAL REPORT 2008-09
83
ANNUAL REPORT 2008-09
Chapter 6
6.1 Introduction
Several National Health Programmes such as theNational Vector Borne Diseases Control, LeprosyEradication, TB Control, Blindness Control and IodineDeficiency Disorder Control have now come underthe umbrella of National Rural Health Mission.
6.2 National Vector Borne DiseaseControl Programme (NVBDCP)
The National Vector Borne Disease ControlProgramme is a comprehensive programme forprevention and control of vector borne diseasesnamely Malaria, Filaria, Kala-azar, JapaneseEncephalitis (JE), Dengue and Chikungunya whichis covered under the overall umbrella of NRHM. TheStates are the implementing agency for prevention& control whereas the Directorate of NVBDCP, Delhiprovides technical assistance, policies and assistanceto the States in the form of cash & commodity, as perapproved pattern. Malaria, Filaria, JapaneseEncephalitis, Dengue and Chikungunya aretransmitted by mosquitoes whereas Kala-azar istransmitted by Sandflies. The transmission of vectorborne diseases in any area is dependent onfrequency of man-vector contact, which is furtherinfluenced by various factors including vector density,biting time, etc.
The general strategy for prevention and control ofvector borne diseases under NVBDCP is describedbelow:
(i) Disease Management including early casedetection and complete treatment,strengthening of referral services, epidemicpreparedness and rapid response.
(ii) Integrated Vector Management (forTransmission Risk Reduction) including
National Programmes under NRHMNational Programmes under NRHMNational Programmes under NRHMNational Programmes under NRHMNational Programmes under NRHM
Indoor Residual Spraying in selected high riskareas, use of Insecticide treated bed nets,use of Larvivorous fish, anti larval measuresin urban areas including bio-larvicides, minorenvironmental engineering.
(iii) Supportive Interventions includingBehaviour Change, Communication, PublicPrivate Partnership & Inter-sectoralconvergence, Human Resource Developmentthrough capacity building, Operationalresearch including studies on drug resistanceand insecticide susceptibility, Monitoring andevaluation through periodic reviews/fieldvisits and Management Information System.
6.3 Malaria
Malaria is acute parasitic illness caused byPlasmodium falciparum or Plasmodium vivax in India.Nine major species of anopheline mosquitoestransmit malaria in India. The main clinicalpresentation is fever with chills, however nausea andheadache can also occur. The diagnosis is confirmedby microscopic examination of a blood smear andRD Kits for Pf cases. Majority of the patients recoverfrom the acute episode within 7 to10 days. Malariacontinues to pose a serious public health threat indifferent parts of the country, particularly due toPlasmodium falciparum, as it is sometimes prone tocomplications, if not treated early.
The major vector mosquito for rural malaria viz.Anopheles culcifacies, is distributed all over theCountry and breeds in clean ground watercollections. Other important Anopheline speciesbreed in running channels, streams with clean water.Some of the vector species also breed in forestareas, mangroves, lagoons, etc, even in those withorganic pollutants.
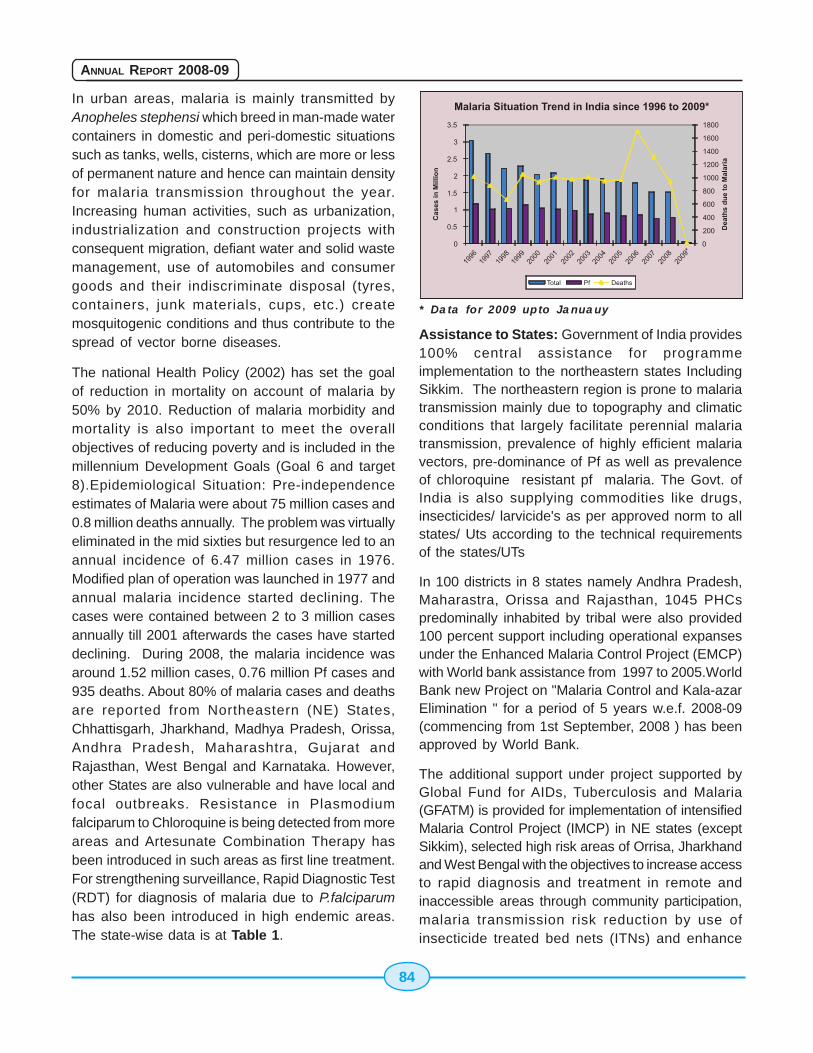
84
ANNUAL REPORT 2008-09
In urban areas, malaria is mainly transmitted byAnopheles stephensi which breed in man-made watercontainers in domestic and peri-domestic situationssuch as tanks, wells, cisterns, which are more or lessof permanent nature and hence can maintain densityfor malaria transmission throughout the year.Increasing human activities, such as urbanization,industrialization and construction projects withconsequent migration, defiant water and solid wastemanagement, use of automobiles and consumergoods and their indiscriminate disposal (tyres,containers, junk materials, cups, etc.) createmosquitogenic conditions and thus contribute to thespread of vector borne diseases.
The national Health Policy (2002) has set the goalof reduction in mortality on account of malaria by50% by 2010. Reduction of malaria morbidity andmortality is also important to meet the overallobjectives of reducing poverty and is included in themillennium Development Goals (Goal 6 and target8).Epidemiological Situation: Pre-independenceestimates of Malaria were about 75 million cases and0.8 million deaths annually. The problem was virtuallyeliminated in the mid sixties but resurgence led to anannual incidence of 6.47 million cases in 1976.Modified plan of operation was launched in 1977 andannual malaria incidence started declining. Thecases were contained between 2 to 3 million casesannually till 2001 afterwards the cases have starteddeclining. During 2008, the malaria incidence wasaround 1.52 million cases, 0.76 million Pf cases and935 deaths. About 80% of malaria cases and deathsare reported from Northeastern (NE) States,Chhattisgarh, Jharkhand, Madhya Pradesh, Orissa,Andhra Pradesh, Maharashtra, Gujarat andRajasthan, West Bengal and Karnataka. However,other States are also vulnerable and have local andfocal outbreaks. Resistance in Plasmodiumfalciparum to Chloroquine is being detected from moreareas and Artesunate Combination Therapy hasbeen introduced in such areas as first line treatment.For strengthening surveillance, Rapid Diagnostic Test(RDT) for diagnosis of malaria due to P.falciparumhas also been introduced in high endemic areas.The state-wise data is at Table 1.
* Data for 2009 upto Januauy
Assistance to States: Government of India provides100% central assistance for programmeimplementation to the northeastern states IncludingSikkim. The northeastern region is prone to malariatransmission mainly due to topography and climaticconditions that largely facilitate perennial malariatransmission, prevalence of highly efficient malariavectors, pre-dominance of Pf as well as prevalenceof chloroquine resistant pf malaria. The Govt. ofIndia is also supplying commodities like drugs,insecticides/ larvicide's as per approved norm to allstates/ Uts according to the technical requirementsof the states/UTs
In 100 districts in 8 states namely Andhra Pradesh,Maharastra, Orissa and Rajasthan, 1045 PHCspredominally inhabited by tribal were also provided100 percent support including operational expansesunder the Enhanced Malaria Control Project (EMCP)with World bank assistance from 1997 to 2005.WorldBank new Project on "Malaria Control and Kala-azarElimination " for a period of 5 years w.e.f. 2008-09(commencing from 1st September, 2008 ) has beenapproved by World Bank.
The additional support under project supported byGlobal Fund for AIDs, Tuberculosis and Malaria(GFATM) is provided for implementation of intensifiedMalaria Control Project (IMCP) in NE states (exceptSikkim), selected high risk areas of Orrisa, Jharkhandand West Bengal with the objectives to increase accessto rapid diagnosis and treatment in remote andinaccessible areas through community participation,malaria transmission risk reduction by use ofinsecticide treated bed nets (ITNs) and enhance
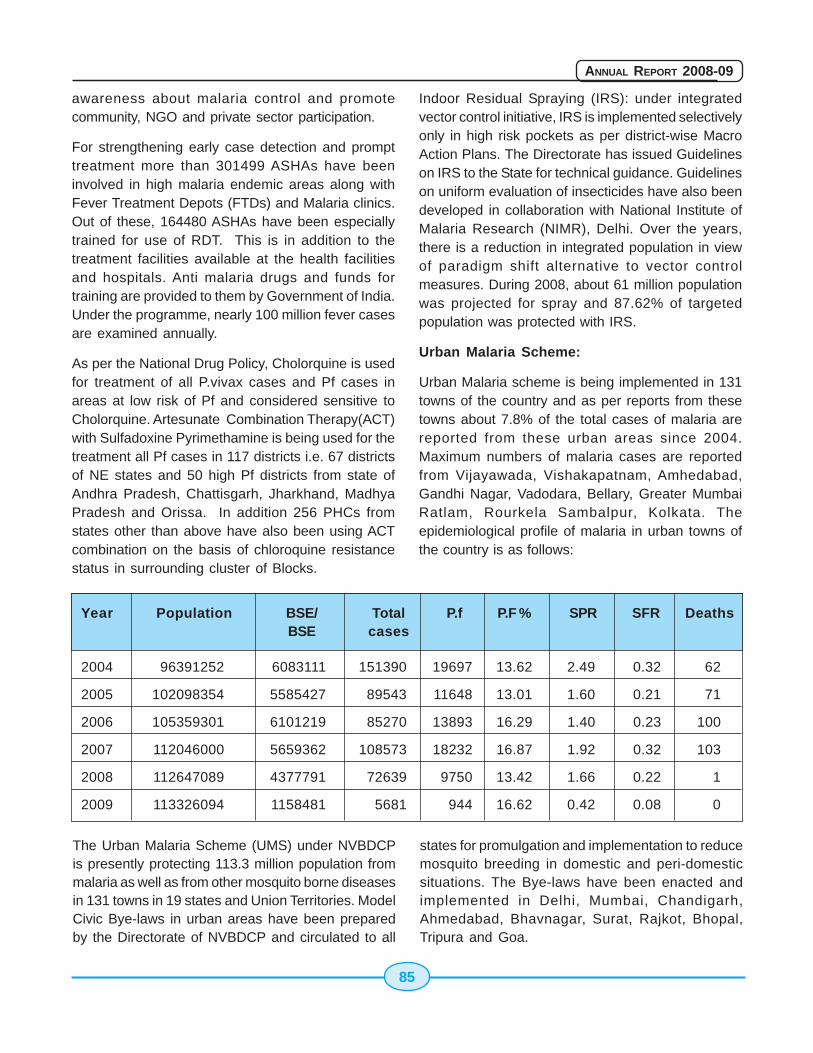
85
ANNUAL REPORT 2008-09
awareness about malaria control and promotecommunity, NGO and private sector participation.
For strengthening early case detection and prompttreatment more than 301499 ASHAs have beeninvolved in high malaria endemic areas along withFever Treatment Depots (FTDs) and Malaria clinics.Out of these, 164480 ASHAs have been especiallytrained for use of RDT. This is in addition to thetreatment facilities available at the health facilitiesand hospitals. Anti malaria drugs and funds fortraining are provided to them by Government of India.Under the programme, nearly 100 million fever casesare examined annually.
As per the National Drug Policy, Cholorquine is usedfor treatment of all P.vivax cases and Pf cases inareas at low risk of Pf and considered sensitive toCholorquine. Artesunate Combination Therapy(ACT)with Sulfadoxine Pyrimethamine is being used for thetreatment all Pf cases in 117 districts i.e. 67 districtsof NE states and 50 high Pf districts from state ofAndhra Pradesh, Chattisgarh, Jharkhand, MadhyaPradesh and Orissa. In addition 256 PHCs fromstates other than above have also been using ACTcombination on the basis of chloroquine resistancestatus in surrounding cluster of Blocks.
Indoor Residual Spraying (IRS): under integratedvector control initiative, IRS is implemented selectivelyonly in high risk pockets as per district-wise MacroAction Plans. The Directorate has issued Guidelineson IRS to the State for technical guidance. Guidelineson uniform evaluation of insecticides have also beendeveloped in collaboration with National Institute ofMalaria Research (NIMR), Delhi. Over the years,there is a reduction in integrated population in viewof paradigm shift alternative to vector controlmeasures. During 2008, about 61 million populationwas projected for spray and 87.62% of targetedpopulation was protected with IRS.
Urban Malaria Scheme:
Urban Malaria scheme is being implemented in 131towns of the country and as per reports from thesetowns about 7.8% of the total cases of malaria arereported from these urban areas since 2004.Maximum numbers of malaria cases are reportedfrom Vijayawada, Vishakapatnam, Amhedabad,Gandhi Nagar, Vadodara, Bellary, Greater MumbaiRatlam, Rourkela Sambalpur, Kolkata. Theepidemiological profile of malaria in urban towns ofthe country is as follows:
The Urban Malaria Scheme (UMS) under NVBDCPis presently protecting 113.3 million population frommalaria as well as from other mosquito borne diseasesin 131 towns in 19 states and Union Territories. ModelCivic Bye-laws in urban areas have been preparedby the Directorate of NVBDCP and circulated to all
states for promulgation and implementation to reducemosquito breeding in domestic and peri-domesticsituations. The Bye-laws have been enacted andimplemented in Delhi, Mumbai, Chandigarh,Ahmedabad, Bhavnagar, Surat, Rajkot, Bhopal,Tripura and Goa.
Year Population BSE/ Total P.f P.F % SPR SFR DeathsBSE cases
2004 96391252 6083111 151390 19697 13.62 2.49 0.32 62
2005 102098354 5585427 89543 11648 13.01 1.60 0.21 71
2006 105359301 6101219 85270 13893 16.29 1.40 0.23 100
2007 112046000 5659362 108573 18232 16.87 1.92 0.32 103
2008 112647089 4377791 72639 9750 13.42 1.66 0.22 1
2009 113326094 1158481 5681 944 16.62 0.42 0.08 0
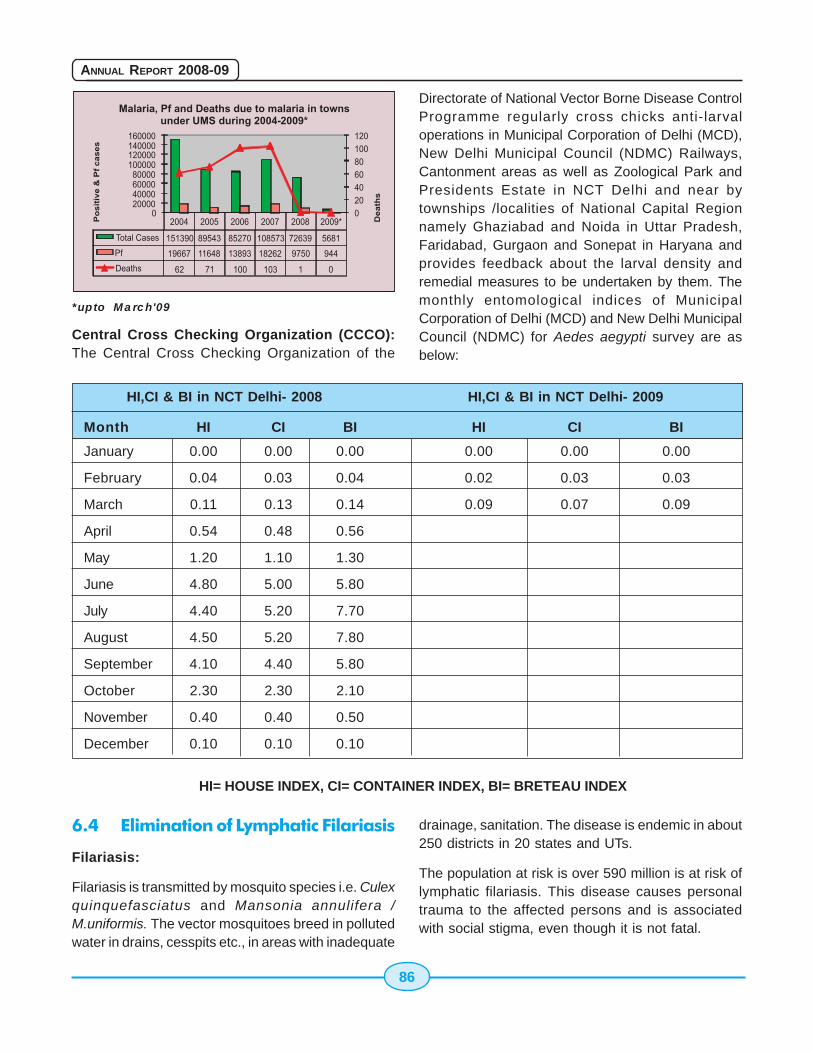
86
ANNUAL REPORT 2008-09
*upto March'09
Central Cross Checking Organization (CCCO):The Central Cross Checking Organization of the
Directorate of National Vector Borne Disease ControlProgramme regularly cross chicks anti-larvaloperations in Municipal Corporation of Delhi (MCD),New Delhi Municipal Council (NDMC) Railways,Cantonment areas as well as Zoological Park andPresidents Estate in NCT Delhi and near bytownships /localities of National Capital Regionnamely Ghaziabad and Noida in Uttar Pradesh,Faridabad, Gurgaon and Sonepat in Haryana andprovides feedback about the larval density andremedial measures to be undertaken by them. Themonthly entomological indices of MunicipalCorporation of Delhi (MCD) and New Delhi MunicipalCouncil (NDMC) for Aedes aegypti survey are asbelow:
6.4 Elimination of Lymphatic Filariasis
Filariasis:
Filariasis is transmitted by mosquito species i.e. Culexquinquefasciatus and Mansonia annulifera /M.uniformis. The vector mosquitoes breed in pollutedwater in drains, cesspits etc., in areas with inadequate
drainage, sanitation. The disease is endemic in about250 districts in 20 states and UTs.
The population at risk is over 590 million is at risk oflymphatic filariasis. This disease causes personaltrauma to the affected persons and is associatedwith social stigma, even though it is not fatal.
HI,CI & BI in NCT Delhi- 2008 HI,CI & BI in NCT Delhi- 2009
Month HI CI BI HI CI BI
January 0.00 0.00 0.00 0.00 0.00 0.00
February 0.04 0.03 0.04 0.02 0.03 0.03
March 0.11 0.13 0.14 0.09 0.07 0.09
April 0.54 0.48 0.56
May 1.20 1.10 1.30
June 4.80 5.00 5.80
July 4.40 5.20 7.70
August 4.50 5.20 7.80
September 4.10 4.40 5.80
October 2.30 2.30 2.10
November 0.40 0.40 0.50
December 0.10 0.10 0.10
HI= HOUSE INDEX, CI= CONTAINER INDEX, BI= BRETEAU INDEX
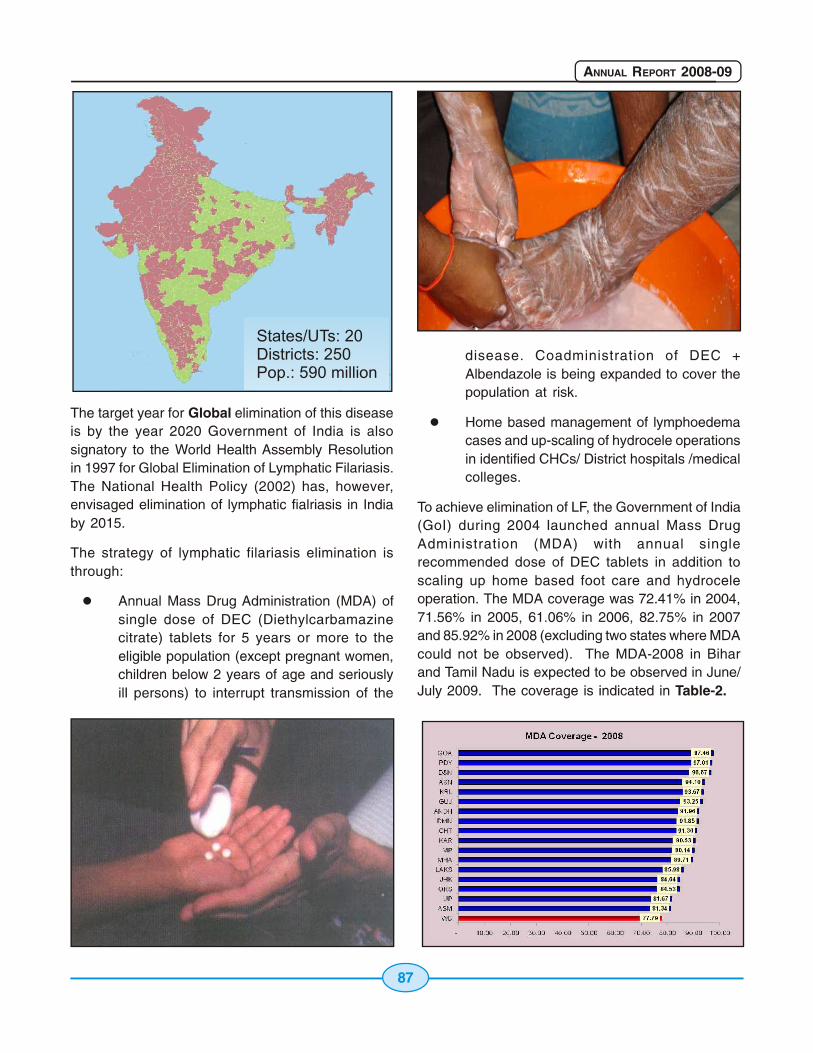
88
ANNUAL REPORT 2008-09
The Line listing of lymphoedema and Hydrocele caseswere initiated since 2004 by door to door survey inthese filaria endemic districts. The enlisted casesare regularly being updated by state healthauthorities and more cases are being recorded. Thisincrease is mainly due to incomplete surveys duringinitial years and reluctance on part of community toreveal their manifestations of lymphoedema andHydrocele. The updated figure till 2007 revealed that7.7 lakhs lymphoedema and 3.8 lakhs Hydrocelecases have been enlisted. The initiation have alsobeen taken to demonstrate the simple washing offoot to maintain hygiene for prevention of secondarybacterial & fungal infection in chronic lymphoedemacases so that the patients get relief from frequentacute attacks. The states have also been requestedto update the list and intensify the hydroceleoperations in their respective states.
The microfilaria survey in all the implementation units(districts) is being done through night blood surveybefore MDA. The survey is done in 4 sentinel and 4random sites as per the guidelines. The analysis ofoverall reports reveals that during 2007 (basedon the data of 2006), 180 districts have reportedmicrofilaria rate less than 1%. The data of pre MDAsurvey during 2008 is being analyzed. There is definiteevidence of microfilaria reduction in the MDA districts.However, the repeated survey for 3-4 consecutiveyears will reflect the trend of mf reduction.
6.5 Kala-Azar
Kala-azar is caused by a protozoan parasiteLeishmania donovani and spread by sandfly, whichbreeds in shady, damp and warm places, in cracksand crevices in the soft soil, in masonry and rubbleheaps, etc. Proper sanitation and hygiene are criticalto prevent sand fly breeding. The National HealthPolicy (2002) of Government of India has set thegoal for elimination of Kala-azar from the country by2010. In pursuance to achieve the elimination goal,case detection and treatment compliance has beenstrengthened and Rapid Diagnostic Test kit and oraldrug miltefosine have been introduced. World Bankis providing assistance in 46 districts in 3 statesnamely Bihar, Jharkhand and West Bengal.
Kala-azar, is endemic in 52 districts (31 in Bihar, 4 inJharkhand, 11 in West Bengal and 6 in UP). The
Kala-azar Control Programme was launched in 1990-91. The annual incidence of disease came down from77,099 cases in 1992 to 44533 cases in 2007 anddeaths from 1419 to 203 in 2007 respectively. Duringthe year 2008, 33234 cases and 146 deaths werereported whereas in 2009 till March, 2254 cases and5 deaths have been reported - Table- 3.
To realize the goal of elimination of Kala-azar, theGovt. of India is providing 100% support to endemicstates sincr 2003-04.
Initiatives undertaken for Kala-azar elimination:
Active Case Search: The frequency of casesearches has been increased, from a singleannual case search to quarterly casesearches. The active case searches arecarried out during a fortnight designated asthe 'Kala-azar Fortnight', during which theperipheral health workers and volunteers areengaged to make door-to-door searches andrefer cases conforming to case definition ofkala-azar and PKDL to the treatment centresfor definitive diagnosis and treatment.
Institutional Surveillance (passive casedetection): Majority of the kala-azar cases arereported from PHC's/district hospitals. Manyprivate practitioner, NGO, FBO's have been
89
ANNUAL REPORT 2008-09
advised to report cases to the district healthauthorities.
Treatment: To ensure complete treatmentcompliance, a Patient Coding Scheme hasbeen put in place in all the treatment cetnres.
Vector Control: Two rounds of DDT spray areundertaken in affected villages of theendemic district, at a dosage of 1g/m2.
A health education programme with personalcontacts as well as through mass media hasbeen initiated to create awareness of thedisease amongst the public, emphasizing theneed for early case detection, acceptanceof a full course of treatment and other controlmeasures.
Intensive training programme for all levels ofhealth staff has been undertaken includingone Inter-country training & one Inter-countrytraining on standard operation.
Introduction of rapid diagnosis and oral drugmiltefosine in 10 pilot district of 3 endemicstates.
The kala-azar activist/ Accredited SocialHealth Activist (ASHA) under the NationalRural Health Mission (NRHM) will be providedincentives to involve them in the variousactivities for control of kala-azar.
6.6 Japanese Encephalitis
Japanese Encephalitis is a zoonotic disease whichis transmitted by vector mosquito, mainly belongingto Culex vishnui group. The transmission cycle is
maintained in the nature by animal reservoirs of JEvirus like pigs and water birds. Man is the dead endhost, i.e. JE is not transmitted from one infectedperson to other. Outbreaks are common in thoseareas where there is close interaction betweenanimals/birds and human beings. The vectors of JEbreed in large water bodies such as paddy fields.Thepopulation at risk is about 300 million.
Epidemiological Situation: JE has been reported fromdifferent parts of the country. The disease is endemicin 14 states of which Assam, Bihar, Haryana, andUttar Pradesh have been reporting outbreaks. During2006, 2871 cases and 663 deaths due to AES/JEwere reported. During the year 2007, the reportedAES figures indicated 4110 cases and 995 deaths.In the year 2008, 3838 cases and 684 deaths werereported. State-wise JE cases and deaths are givenin Table - 4.

90
ANNUAL REPORT 2008-09
There is no specific cure for this disease, symptomaticand early case management is very important tominimize risk of death and complications. A killed mousebrain JE inactivated vaccine is manufactured at theCentral Research Institute (CRI), Kausauli andprocured directly by the states. However, theproduction of this vaccine is inadequate and does notmeet the state demand. There are operationalproblems in the delivery of three doses of this vaccineand booster dose after every three years. Consideringthese problems, during the year 2006, Govt. of Indialaunched JE vaccination programme as an integralcomponent of Universal Immunization Programme(UIP) with single dose live attenuated JE (SA- 14-14-2) in 11 endemic districts of 4 States namely UttarPradesh, Assam, West Bengal and Karnataka forchildren between 1 and 15 years of age and 88.39%coverage was achieved. During 2007, JE vaccinationwith SA-14-14-2 vaccine has been expanded to 28districts in 10 states (Assam, Karnataka, UttarPradesh, West Bengal, Haryana, Bihar, AndhraPradesh, Tamil Nadu, Maharashtra and Kerala) During2008 JE vaccination has seen carried out in 22 districts.In Uttar Pradesh all the 34 identified JE endemicdistricts have been covered under JE vaccination.
In addition, implementation of public health measuressuch as, Health Education through different media likeradio, TV including cable network miking, inter-personal communication, etc for disseminatingappropriate messages in the community is crucial. Theemphasis is given on keeping pigs away from humandwellings or in pigsties particularly during dusk to dawnwhich is the biting time of vector mosquitoes.Sensitization of the community regarding avoidanceof man-mosquito contact by using bet nets and fullycovering the body are also advocated. Since earlyreporting of cases is crucial to avoid any complicationand mortality, community is given full information aboutthe signs and symptoms as well as availability of healthservices at health centres/hospitals. Besides, the
states are advised fogging with malathion (Technical)as an outbreak control measure in the affected areas.
6.7 Denguefever / DengueHaemorrhagic Fever
Dengue Fever is an outbreak prone viral disease, alsotransmitted by Aedes aegypti mosquitoes. Aedesaegypti mosquitoes prefer to breed in man madecontainers, viz., cement tanks, overhead tanks,
underground tanks, tyres, desert coolers, pitchers,discarded containers, junk materials, etc, in which waterstagnates for more than a week. This is day bitingmosquito and prefers to rest in hard to find dark areasinside the houses. The risk of dengue has shown anincrease in recent years due to rapid urbanization, lifestyle changes and deficient water management includingimproper water storage practices in urban, peri-urbanand rural areas, leading to proliferation of mosquitobreeding sites. The disease tends to follow seasonalpattern i.e., the cases peaks after monsoon and it is notuniformly distributed. Dengue is a self limiting acutemosquito transmitted disease characterized by fever,headache, muscle, joint pains, rash, nausea and

91
ANNUAL REPORT 2008-09
vomiting. Some infections results in DengueHaemorrhagic Fever (DHF) and in its severe formDengue Shock Syndrome (DSS) can threaten thepatient's life primarily through increased vascularpermeability and shock. The case fatality rate which was3.3 % in 1996 had come down to 0.63 in 2008 becauseof better management of Dengue cases in the country.
Epidemiological Situation: Dengue is endemic in23 states/UTs. After 1996, outbreak with a totalnumber of 16517 cases (suspected) and 545 deathsagain upsurge of cases were recorded in 2003 with12754 cases and 215 deaths. Subsequently, in theyear 2005 again, 11985 cases along with 157 deathshad been reported respectively. In 2008 total 12561cases and 80 deaths have been reported. During2009, till March 665 cases and 3 deaths have beenreported (Table-5).
The States have been communicated to undertakewidespread campaigns for community awareness andmobilization through different media like mass media,miking, inter-personal communication, etc. Theemphasis is on elimination of mosquito breedingsources like avoidance of water collection in andaround houses, removal of all discarded anddisposed/junk materials, keeping all water containers/storage facilities tightly covered and cleaning thewater coolers at least once a week before re-filling.Since early reporting of cases is crucial to avoid anycomplication and mortality, the community is givenfull information about the signs and symptoms aswell as availability of health services at health centres/hospitals. Alerting the Hospitals for making adequatearrangements for management of Dengue/DengueHaemorrhagic Fever cases have also been advised.
The Directorate of National Vector Borne DiseaseControl has provided detailed guidelines for theprevention and control of dengue to the affectedstates. Intensive health education activities throughprint, electronic and inter-personnel media, outdoorpublicity as well as and inter-sectoral collaborationwith civil society organization (NGOs/CBOs/Self-HelpGroups), PRIs and Municipal bodies have beenemphasized. Regular supervision and monitoring isconducted by the Programme. The Government ofIndia in consultation withStates has identified 137sentinel surveillancehospitals with laboratorysupport for augmentation ofdiagnostic facilities in theendemic states. Further, foradvanced diagnosis andbackup support, 13 Apexinstitutions (Table-7) havebeen identified and linkedwith sentinel surveillancehospitals.
6.8 Chikungunya
Chikungunya is a debilitatingnon-fatal viral illness causedby Chikungunya virus hasre-emerged in the country
There is no specific anti-viral drug for dengue andmortality can only be minimized by early diagnosisand prompt symptomatic management of the cases.A strategic action plan has been developed forprevention and control of Dengue and issued to theendemic States for implementation. Guidelines forclinical management of dengue fever/ denguehaemorrhagic fever and dengue shock syndromehas been developed and sent to the states for widercirculation. Advisories have been sent to the endemicareas for effective vector control through inter-sectoral collaboration and active communityinvolvement, regular monitoring of fever, Denguecases as well as entomological parameters to forecastlikely outbreaks and take timely remedial measures.

92
ANNUAL REPORT 2008-09
after a quiescence of three decades. In India a majorepidemic of Chikungunya fever was reported duringthe last millennium viz.; 1963 (Kolkata), 1965(Pondicherry and Chennai in Tamil Nadu,Rajahmundry, Vishakapatnam and Kakinada inAndhra Pradesh; Sagar in Madhya Pradesh; andNagpur in Maharashtra) and 1973, (Barsi inMaharashtra). This disease is also transmitted byAedes mosquito. Both Ae. aegypti and Ae.albopictuscan transmit the disease. Humans are considered tobe the major source or reservoir of Chikungunyavirus. Therefore, the mosquitoes usually transmit thedisease by biting infected persons and then bitingothers. The infected person cannot spread theinfection directly to other person (i.e. it is notcontagious disease). Symptoms of Chikungunyafever are most often clinically indistinguishable fromthose observed in dengue fever. However, unlikedengue, hemorrhagic manifestations are rare andshock is not observed in Chikungunya virus infection.Chikungunya outbreaks typically result in largenumber of cases but deaths are rarely encountered.
During 2006, total 1.39 million clinically suspectedChikungunya cases reported in the country. Out of15961 samples tested 2001 (12.5%) were foundpositive for Chikungunya serologically. Out of 35States/UTs 16 were affected: Andhra Pradesh,Karnataka, Maharashtra, Tamil Nadu, MadhyaPradesh, Gujarat, Kerala, Andaman & NicobarIslands, GNCT of Delhi, Rajasthan, Pondicherry, Goa,Orissa, West Bengl, Lakshadweep and UttarPradesh. There are no reported deaths directlyrelated to Chikungunya. In 2007, total 14 states wereaffected and reported 59535 suspectedChikungunya fever cases with nil death. Out of 7850samples tested 1826 (23.26%) were confirmedpositive for Chikungunya virus. Subsequently in2008, 95091 suspected Chikungunya fever casesand nil deaths have been reported. Though 13states had reported Chikungunya fever cases,maximum cases were reported from Karnataka(48.91%) followed by Kerala (25.96%) and WestBengal (18.82%) (Table-6).
As already mentioned, Aedes mosquitoes bite duringthe day and breed in a wide variety of man-made
containers which are common around humandwellings. These containers such as discarded tyres,flower pots, old water drums, family water trough,water storage vessels and plastic food containerscollect rain water become the source of breeding ofAedes mosquitoes. Ae.aegypti played the major rolein transmitting the disease in all the states exceptKerala, where Ae. albopictus played the major role.Ae. albopictus breeding was detected in latexcollecting cups of rubber plantations, shoot-off leavesof areca palm, fruit shells, leaf axils, tree holes etc.There is neither any vaccine nor drugs are availableto cure the Chikungunya infection. Supportive
93
ANNUAL REPORT 2008-09
therapy that helps ease symptoms, such asadministration of non-steroidal anti-inflammatorydrugs, and getting plenty of rest are found tom bebeneficial.
Government of India is continuously monitoring thesituation & sending guidelines and advisories forprevention and control of Chikungunya fever to thestates. Support in the form of logistics and funds areprovided to the states. The central teams are deputedto the affected states for technical guidance of thestate health authorities. Since same vector isinvolved in the transmission of Dengue andChikungunya strategies for transmission riskreduction by vector control are also same. Acomprehensive Long Term Action Plan for prevention& control of Chikungunya and Dengue/DengueHaemorrhagic Fever has been prepared anddisseminated for guidance to the states. As mosttransmission occurs at home, therefore communityparticipation and co-operation is of paramountimportance for successful implementation ofprogramme strategies for prevention and control ofChikungunya. Therefore, considerable efforts havebeen made through advocacy and social mobilizationfor community education/awareness. For effectivecommunity participation, people are informed aboutChikungunya and the fact that major epidemics canbe prevented by taking effective preventivemeasures by community itself.
For carrying out proactive surveillance and
enhancing diagnostic facilities for Chikungunya/ the137 Sentinel Surveillance hospitals involved indengue in the affected states also carriesChikungunya tests. Both Dengue and ChikungunyaDiagnostic kits to these institutes are providedthrough National Institute of Virology, Pune and costis re-imbursed by GOI. Further, rapid response bythe concerned health authorities has been envisagedon report of any suspected case from the SentinelSurveillance Hospitals to prevent further spread ofthe disease.
The overall strategies for prevention and control aresame as in Dengue such as symptomaticmanagement of cases, reduction of breedingsources, personal protection and intensive IEC andcapacity building. Initiatives undertaken by Govt. ofIndia for prevention and control of Dengue/Chikungunya
Continuous monitoring of Chikungunya andDengue situation in states.
Circulation of guidelines and advisories forprevention and control of diseases toaffected states.
Launch of Intensive IEC and BehaviourChange Communication activities throughprint, electronic media, interpersonalcommunication, outdoor publicity as well asinter sectoral collaboration with civil societyorganizations (NGOs/CBOs/ Self HelpGroups), PRIs.
Provision of larvicides and adulticides toaffected states.
Identification and strengthening of ApexReferral Laboratories and sentinelsurveillance hospitals for diagnosis andregular surveillance.
NIV, Pune has been entrusted for supply oftest kits to the identified institutions and toupscale its test kit production capacity.
Contingency grant provided to the Apex ReferralLaboratories and sentinel surveillance hospitals tomeet the operational cost.
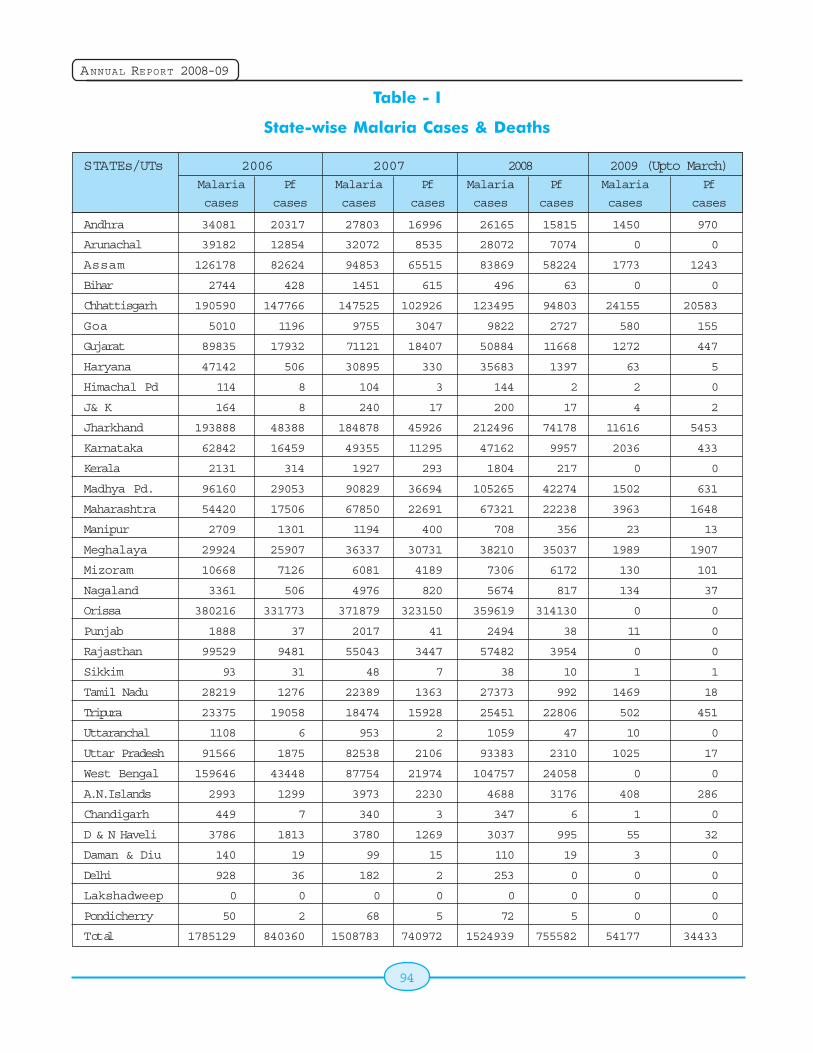
94
ANNUAL REPORT 2008-09
Table - I
State-wise Malaria Cases & Deaths
STATEs/UTs 2006 2007 2008 2009 (Upto March)Malaria Pf Malaria Pf Malaria Pf Malaria Pf
cases cases cases cases cases cases cases cases
Andhra 34081 20317 27803 16996 26165 15815 1450 970
Arunachal 39182 12854 32072 8535 28072 7074 0 0
Assam 126178 82624 94853 65515 83869 58224 1773 1243
Bihar 2744 428 1451 615 496 63 0 0
Chhattisgarh 190590 147766 147525 102926 123495 94803 24155 20583
Goa 5010 1196 9755 3047 9822 2727 580 155
Gujarat 89835 17932 71121 18407 50884 11668 1272 447
Haryana 47142 506 30895 330 35683 1397 63 5
Himachal Pd 114 8 104 3 144 2 2 0
J& K 164 8 240 17 200 17 4 2
Jharkhand 193888 48388 184878 45926 212496 74178 11616 5453
Karnataka 62842 16459 49355 11295 47162 9957 2036 433
Kerala 2131 314 1927 293 1804 217 0 0
Madhya Pd. 96160 29053 90829 36694 105265 42274 1502 631
Maharashtra 54420 17506 67850 22691 67321 22238 3963 1648
Manipur 2709 1301 1194 400 708 356 23 13
Meghalaya 29924 25907 36337 30731 38210 35037 1989 1907
Mizoram 10668 7126 6081 4189 7306 6172 130 101
Nagaland 3361 506 4976 820 5674 817 134 37
Orissa 380216 331773 371879 323150 359619 314130 0 0
Punjab 1888 37 2017 41 2494 38 11 0
Rajasthan 99529 9481 55043 3447 57482 3954 0 0
Sikkim 93 31 48 7 38 10 1 1
Tamil Nadu 28219 1276 22389 1363 27373 992 1469 18
Tripura 23375 19058 18474 15928 25451 22806 502 451
Uttaranchal 1108 6 953 2 1059 47 10 0
Uttar Pradesh 91566 1875 82538 2106 93383 2310 1025 17
West Bengal 159646 43448 87754 21974 104757 24058 0 0
A.N.Islands 2993 1299 3973 2230 4688 3176 408 286
Chandigarh 449 7 340 3 347 6 1 0
D & N Haveli 3786 1813 3780 1269 3037 995 55 32
Daman & Diu 140 19 99 15 110 19 3 0
Delhi 928 36 182 2 253 0 0 0
Lakshadweep 0 0 0 0 0 0 0 0
Pondicherry 50 2 68 5 72 5 0 0
Total 1785129 840360 1508783 740972 1524939 755582 54177 34433
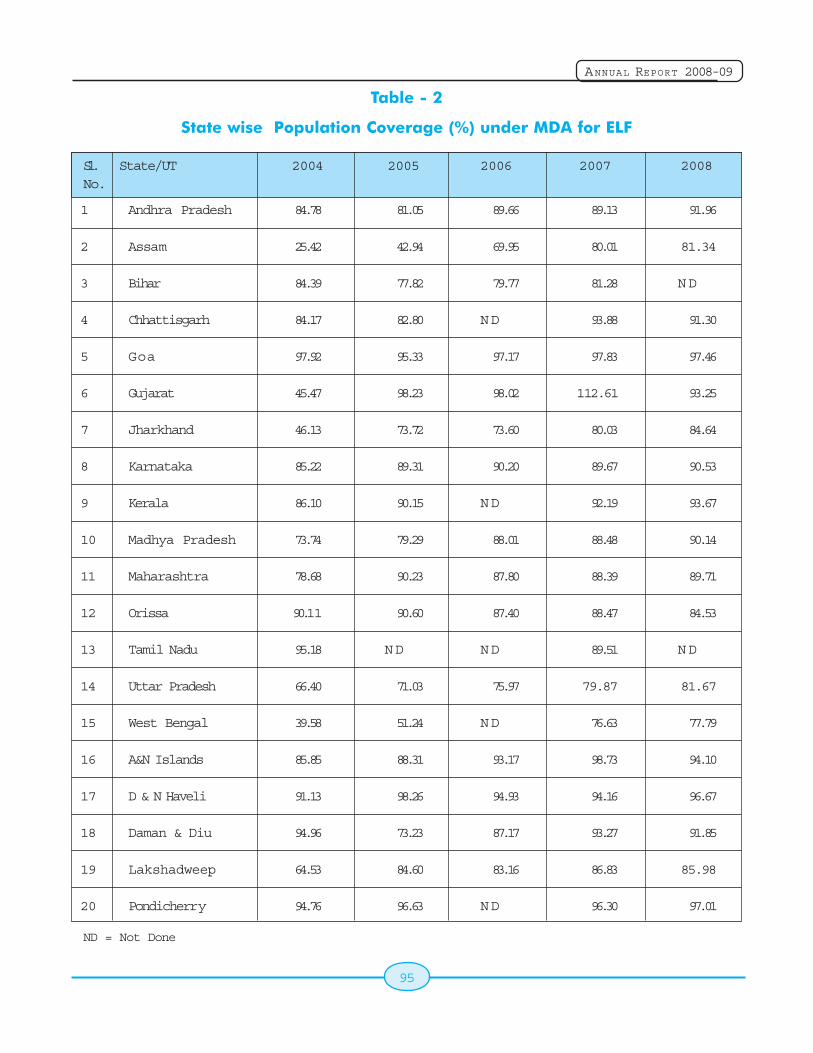
95
ANNUAL REPORT 2008-09
Table - 2
State wise Population Coverage (%) under MDA for ELF
Sl. State/UT 2004 2005 2006 2007 2008No.
1 Andhra Pradesh 84.78 81.05 89.66 89.13 91.96
2 Assam 25.42 42.94 69.95 80.01 81.34
3 Bihar 84.39 77.82 79.77 81.28 ND
4 Chhattisgarh 84.17 82.80 ND 93.88 91.30
5 Goa 97.92 95.33 97.17 97.83 97.46
6 Gujarat 45.47 98.23 98.02 112.61 93.25
7 Jharkhand 46.13 73.72 73.60 80.03 84.64
8 Karnataka 85.22 89.31 90.20 89.67 90.53
9 Kerala 86.10 90.15 ND 92.19 93.67
10 Madhya Pradesh 73.74 79.29 88.01 88.48 90.14
11 Maharashtra 78.68 90.23 87.80 88.39 89.71
12 Orissa 90.11 90.60 87.40 88.47 84.53
13 Tamil Nadu 95.18 ND ND 89.51 ND
14 Uttar Pradesh 66.40 71.03 75.97 79.87 81.67
15 West Bengal 39.58 51.24 ND 76.63 77.79
16 A&N Islands 85.85 88.31 93.17 98.73 94.10
17 D & N Haveli 91.13 98.26 94.93 94.16 96.67
18 Daman & Diu 94.96 73.23 87.17 93.27 91.85
19 Lakshadweep 64.53 84.60 83.16 86.83 85.98
20 Pondicherry 94.76 96.63 ND 96.30 97.01
ND = Not Done
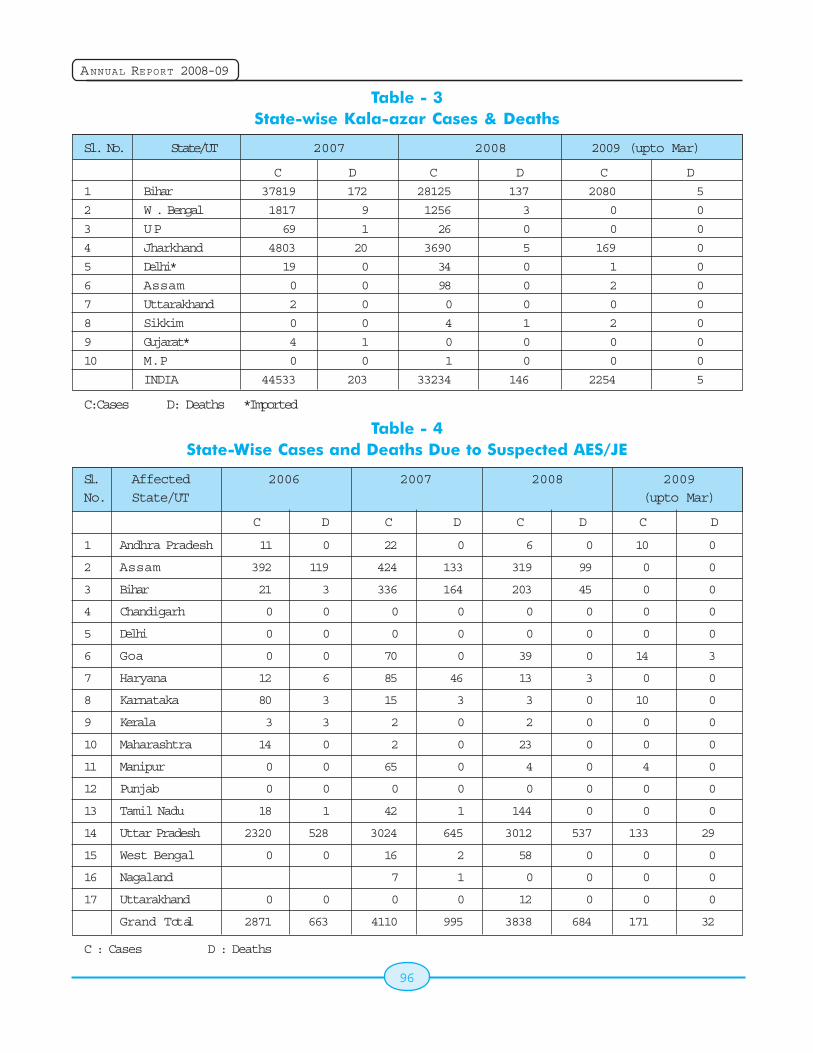
96
ANNUAL REPORT 2008-09
Table - 3State-wise Kala-azar Cases & Deaths
Sl. No. State/UT 2007 2008 2009 (upto Mar)
C D C D C D
1 Bihar 37819 172 28125 137 2080 5
2 W . Bengal 1817 9 1256 3 0 0
3 UP 69 1 26 0 0 0
4 Jharkhand 4803 20 3690 5 169 0
5 Delhi* 19 0 34 0 1 0
6 Assam 0 0 98 0 2 0
7 Uttarakhand 2 0 0 0 0 0
8 Sikkim 0 0 4 1 2 0
9 Gujarat* 4 1 0 0 0 0
10 M.P 0 0 1 0 0 0
INDIA 44533 203 33234 146 2254 5
C:Cases D: Deaths *Imported
Table - 4State-Wise Cases and Deaths Due to Suspected AES/JE
Sl. Affected 2006 2007 2008 2009No. State/UT (upto Mar)
C D C D C D C D
1 Andhra Pradesh 11 0 22 0 6 0 10 0
2 Assam 392 119 424 133 319 99 0 0
3 Bihar 21 3 336 164 203 45 0 0
4 Chandigarh 0 0 0 0 0 0 0 0
5 Delhi 0 0 0 0 0 0 0 0
6 Goa 0 0 70 0 39 0 14 3
7 Haryana 12 6 85 46 13 3 0 0
8 Karnataka 80 3 15 3 3 0 10 0
9 Kerala 3 3 2 0 2 0 0 0
10 Maharashtra 14 0 2 0 23 0 0 0
11 Manipur 0 0 65 0 4 0 4 0
12 Punjab 0 0 0 0 0 0 0 0
13 Tamil Nadu 18 1 42 1 144 0 0 0
14 Uttar Pradesh 2320 528 3024 645 3012 537 133 29
15 West Bengal 0 0 16 2 58 0 0 0
16 Nagaland 7 1 0 0 0 0
17 Uttarakhand 0 0 0 0 12 0 0 0
Grand Total 2871 663 4110 995 3838 684 171 32
C : Cases D : Deaths
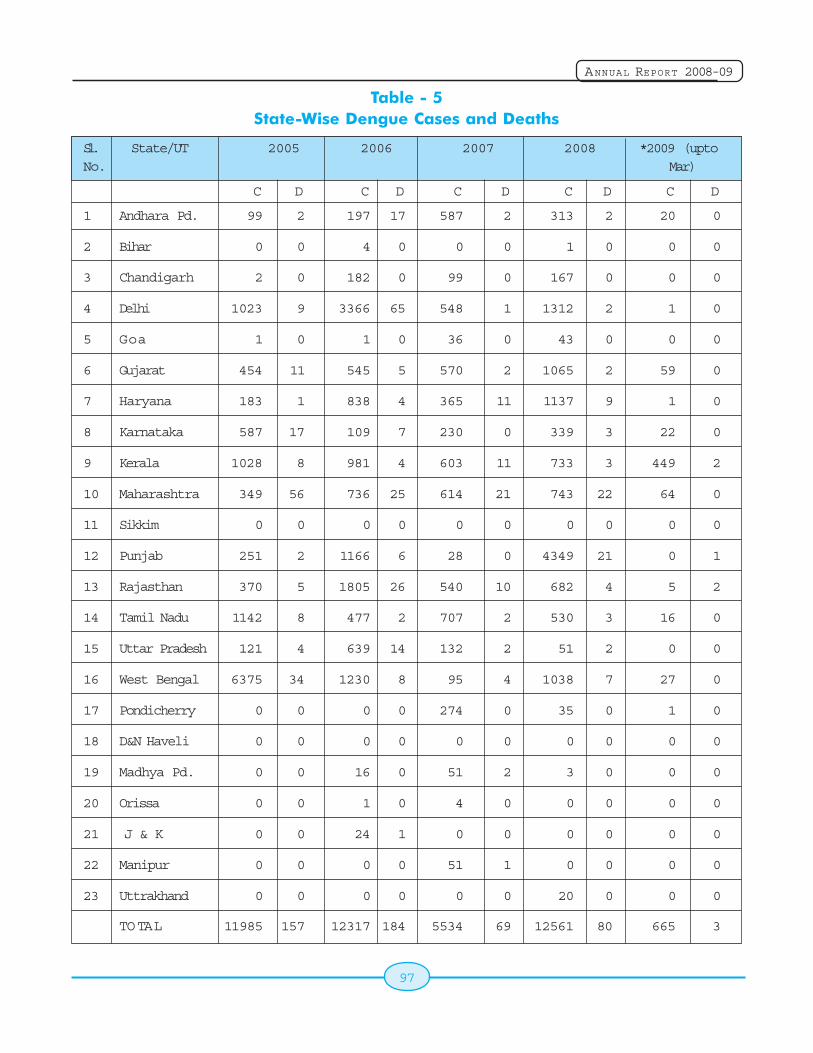
97
ANNUAL REPORT 2008-09
Table - 5State-Wise Dengue Cases and Deaths
Sl. State/UT 2005 2006 2007 2008 *2009 (uptoNo. Mar)
C D C D C D C D C D
1 Andhara Pd. 99 2 197 17 587 2 313 2 20 0
2 Bihar 0 0 4 0 0 0 1 0 0 0
3 Chandigarh 2 0 182 0 99 0 167 0 0 0
4 Delhi 1023 9 3366 65 548 1 1312 2 1 0
5 Goa 1 0 1 0 36 0 43 0 0 0
6 Gujarat 454 11 545 5 570 2 1065 2 59 0
7 Haryana 183 1 838 4 365 11 1137 9 1 0
8 Karnataka 587 17 109 7 230 0 339 3 22 0
9 Kerala 1028 8 981 4 603 11 733 3 449 2
10 Maharashtra 349 56 736 25 614 21 743 22 64 0
11 Sikkim 0 0 0 0 0 0 0 0 0 0
12 Punjab 251 2 1166 6 28 0 4349 21 0 1
13 Rajasthan 370 5 1805 26 540 10 682 4 5 2
14 Tamil Nadu 1142 8 477 2 707 2 530 3 16 0
15 Uttar Pradesh 121 4 639 14 132 2 51 2 0 0
16 West Bengal 6375 34 1230 8 95 4 1038 7 27 0
17 Pondicherry 0 0 0 0 274 0 35 0 1 0
18 D&N Haveli 0 0 0 0 0 0 0 0 0 0
19 Madhya Pd. 0 0 16 0 51 2 3 0 0 0
20 Orissa 0 0 1 0 4 0 0 0 0 0
21 J & K 0 0 24 1 0 0 0 0 0 0
22 Manipur 0 0 0 0 51 1 0 0 0 0
23 Uttrakhand 0 0 0 0 0 0 20 0 0 0
TOTAL 11985 157 12317 184 5534 69 12561 80 665 3
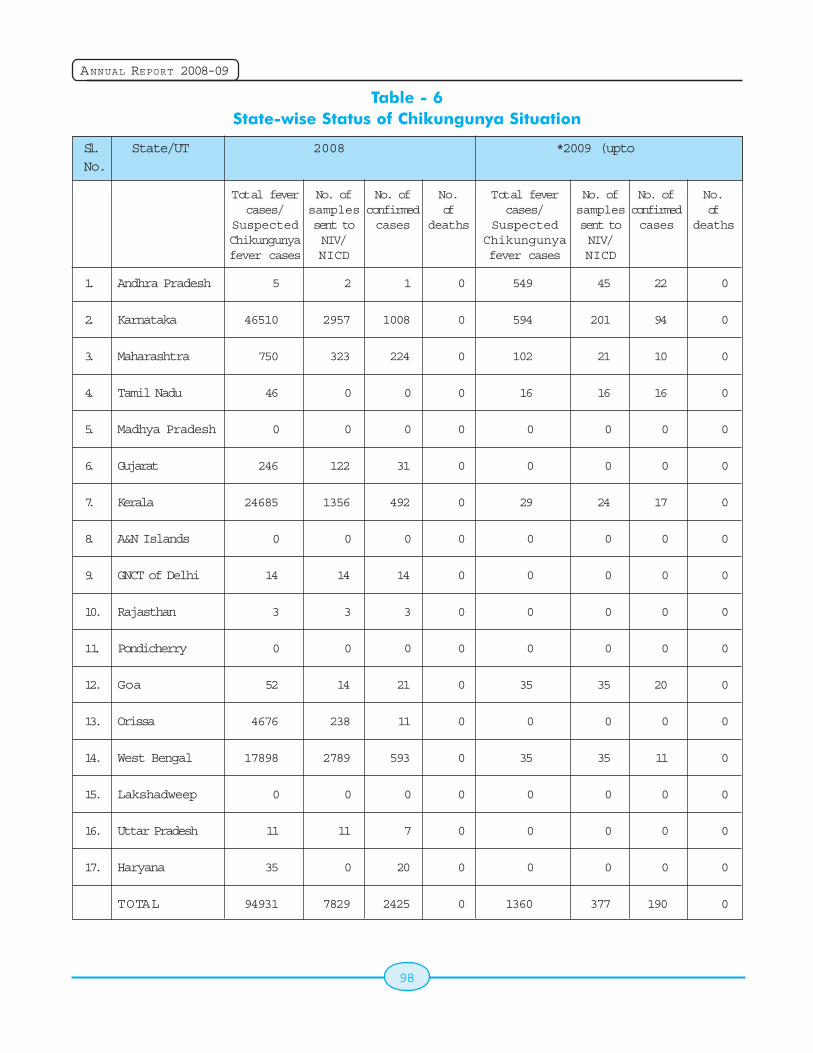
98
ANNUAL REPORT 2008-09
Table - 6State-wise Status of Chikungunya Situation
Sl. State/UT 2008 *2009 (uptoNo.
1. Andhra Pradesh 5 2 1 0 549 45 22 0
2. Karnataka 46510 2957 1008 0 594 201 94 0
3. Maharashtra 750 323 224 0 102 21 10 0
4. Tamil Nadu 46 0 0 0 16 16 16 0
5. Madhya Pradesh 0 0 0 0 0 0 0 0
6. Gujarat 246 122 31 0 0 0 0 0
7. Kerala 24685 1356 492 0 29 24 17 0
8. A&N Islands 0 0 0 0 0 0 0 0
9. GNCT of Delhi 14 14 14 0 0 0 0 0
10. Rajasthan 3 3 3 0 0 0 0 0
11. Pondicherry 0 0 0 0 0 0 0 0
12. Goa 52 14 21 0 35 35 20 0
13. Orissa 4676 238 11 0 0 0 0 0
14. West Bengal 17898 2789 593 0 35 35 11 0
15. Lakshadweep 0 0 0 0 0 0 0 0
16. Uttar Pradesh 11 11 7 0 0 0 0 0
17. Haryana 35 0 20 0 0 0 0 0
TOTAL 94931 7829 2425 0 1360 377 190 0
Total fevercases/
SuspectedChikungunyafever cases
No. ofsamplessent toNIV/NICD
No. ofconfirmedcases
No.of
deaths
Total fevercases/
SuspectedChikungunyafever cases
No. ofsamplessent toNIV/NICD
No. ofconfirmedcases
No.of
deaths
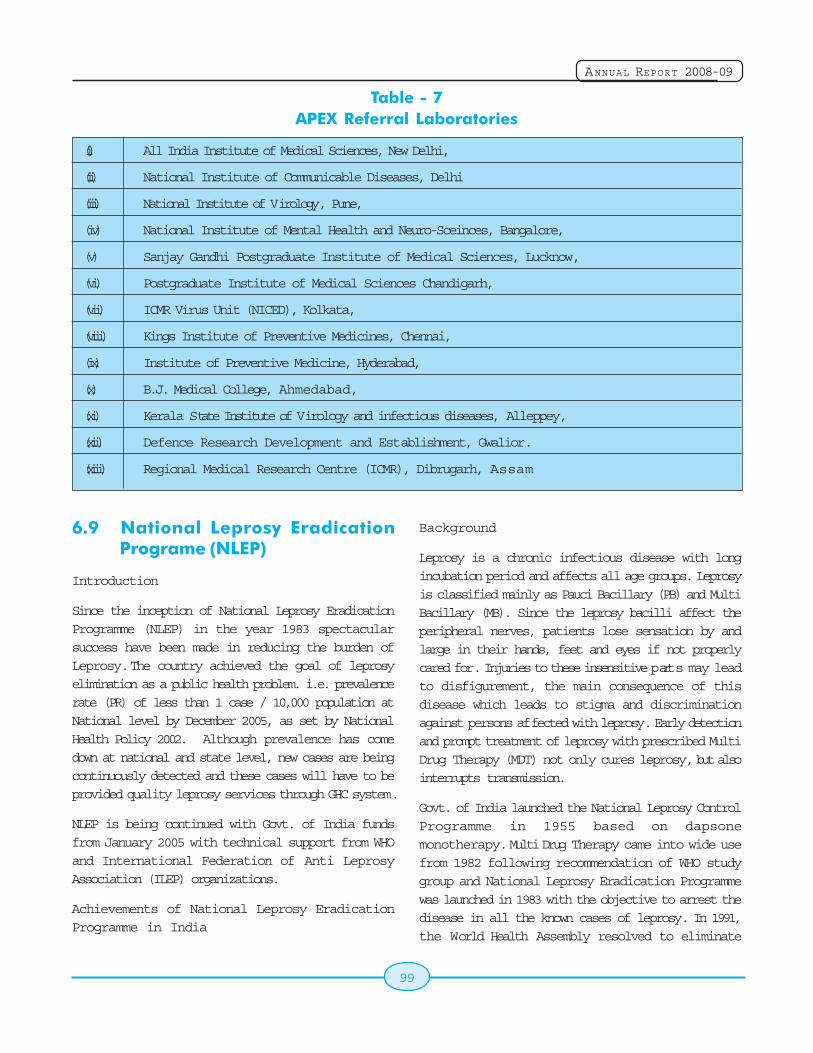
99
ANNUAL REPORT 2008-09
Table - 7APEX Referral Laboratories
(i) All India Institute of Medical Sciences, New Delhi,
(ii) National Institute of Communicable Diseases, Delhi
(iii) National Institute of Virology, Pune,
(iv) National Institute of Mental Health and Neuro-Sceinces, Bangalore,
(v) Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow,
(vi) Postgraduate Institute of Medical Sciences Chandigarh,
(vii) ICMR Virus Unit (NICED), Kolkata,
(viii) Kings Institute of Preventive Medicines, Chennai,
(ix) Institute of Preventive Medicine, Hyderabad,
(x) B.J. Medical College, Ahmedabad,
(xi) Kerala State Institute of Virology and infectious diseases, Alleppey,
(xii) Defence Research Development and Establishment, Gwalior.
(xiii) Regional Medical Research Centre (ICMR), Dibrugarh, Assam
6.9 National Leprosy EradicationPrograme (NLEP)
Introduction
Since the inception of National Leprosy EradicationProgramme (NLEP) in the year 1983 spectacularsuccess have been made in reducing the burden ofLeprosy. The country achieved the goal of leprosyelimination as a public health problem. i.e. prevalencerate (PR) of less than 1 case / 10,000 population atNational level by December 2005, as set by NationalHealth Policy 2002. Although prevalence has comedown at national and state level, new cases are beingcontinuously detected and these cases will have to beprovided quality leprosy services through GHC system.
NLEP is being continued with Govt. of India fundsfrom January 2005 with technical support from WHOand International Federation of Anti LeprosyAssociation (ILEP) organizations.
Achievements of National Leprosy EradicationProgramme in India
Background
Leprosy is a chronic infectious disease with longincubation period and affects all age groups. Leprosyis classified mainly as Pauci Bacillary (PB) and MultiBacillary (MB). Since the leprosy bacilli affect theperipheral nerves, patients lose sensation by andlarge in their hands, feet and eyes if not properlycared for. Injuries to these insensitive parts may leadto disfigurement, the main consequence of thisdisease which leads to stigma and discriminationagainst persons affected with leprosy. Early detectionand prompt treatment of leprosy with prescribed MultiDrug Therapy (MDT) not only cures leprosy, but alsointerrupts transmission.
Govt. of India launched the National Leprosy ControlProgramme in 1955 based on dapsonemonotherapy. Multi Drug Therapy came into wide usefrom 1982 following recommendation of WHO studygroup and National Leprosy Eradication Programmewas launched in 1983 with the objective to arrest thedisease in all the known cases of leprosy. In 1991,the World Health Assembly resolved to eliminate
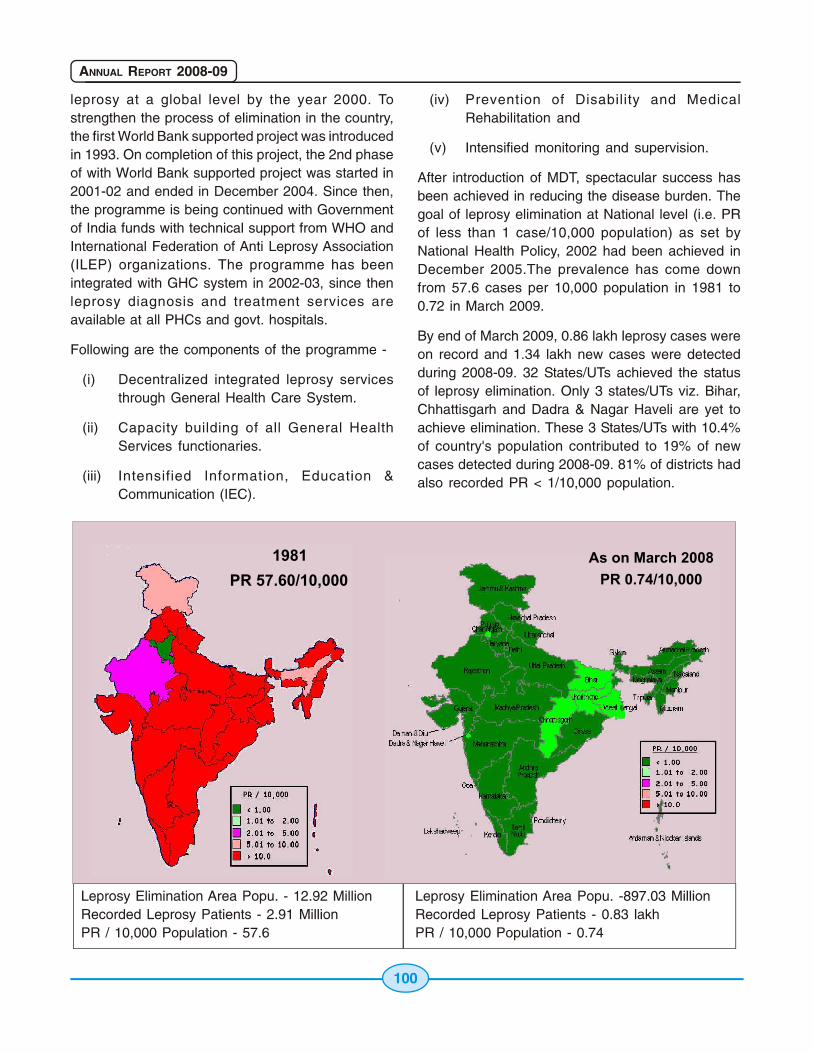
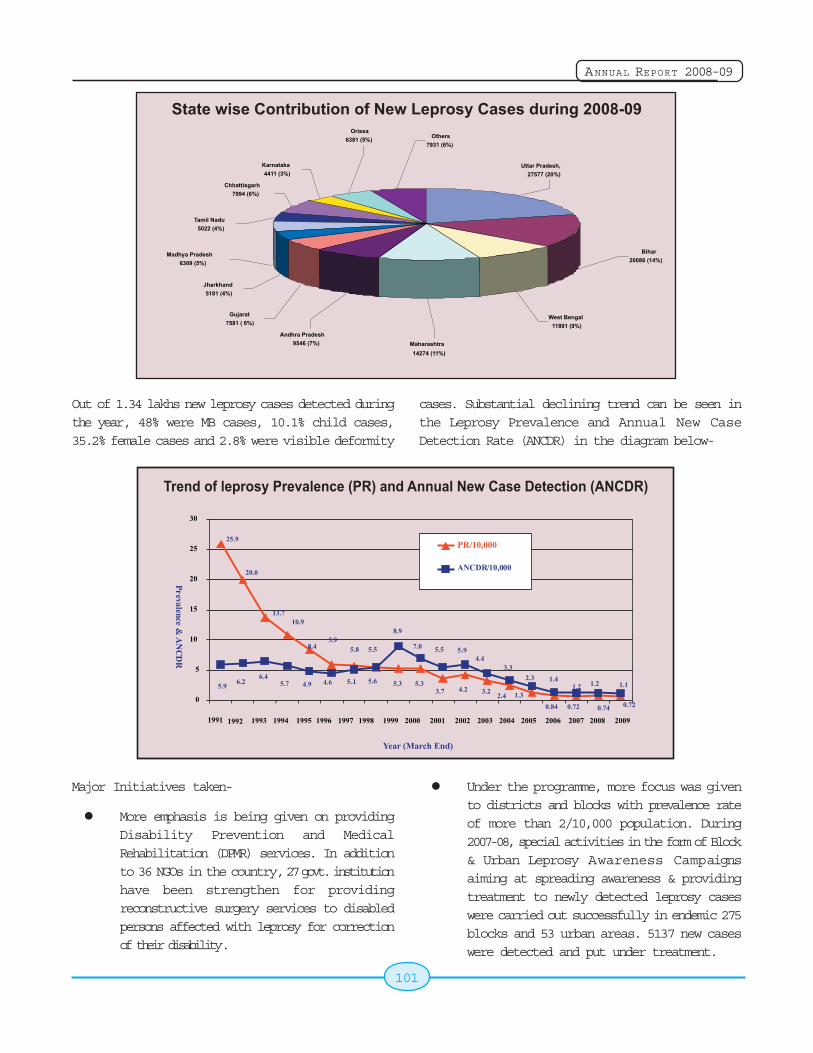
101
ANNUAL REPORT 2008-09
Out of 1.34 lakhs new leprosy cases detected duringthe year, 48% were MB cases, 10.1% child cases,35.2% female cases and 2.8% were visible deformity
cases. Substantial declining trend can be seen inthe Leprosy Prevalence and Annual New CaseDetection Rate (ANCDR) in the diagram below-
Major Initiatives taken-
More emphasis is being given on providingDisability Prevention and MedicalRehabilitation (DPMR) services. In additionto 36 NGOs in the country, 27 govt. institutionhave been strengthen for providingreconstructive surgery services to disabledpersons affected with leprosy for correctionof their disability.
Under the programme, more focus was givento districts and blocks with prevalence rateof more than 2/10,000 population. During2007-08, special activities in the form of Block& Urban Leprosy Awareness Campaignsaiming at spreading awareness & providingtreatment to newly detected leprosy caseswere carried out successfully in endemic 275blocks and 53 urban areas. 5137 new caseswere detected and put under treatment.
102
ANNUAL REPORT 2008-09
More focus has now been given to new casedetection rather than prevalence which onlygive the number of cases on record at a pointin time. The New Case Detection Rate is themain indicator for programme monitoring nowbeing calculated on quarterly basis by thestate as per the guidelines.
Treatment Completion Rate (TCR) has beentaken as an important indicator to becalculated on regular basis every year allover the country as an inbuilt component ofthe programme. The guidelines for calculationof TCR by Cohort Analysis had been issuedto states and the rates for the reporting year2006-07 and 2007-08 have been receivedas base line information.
IEC campaigns with the theme 'TowardsLeprosy Free India' was started from 30thJanuary 2008 with focus on further reductionin leprosy burden in the community, earlyreporting of cases & treatment completion,provision of quality leprosy services andreduction of stigma & discrimination.
New Paradigms-
After elimination of leprosy, the programme hasexpanded the scope of providing leprosy services tothe patients, their families and community at large.To sustain leprosy services for many years to come,there has been a shift from campaign like eliminationapproach, towards the long term process ofsustaining integrated high quality leprosy services.
New paradigms under the programme take intoconsideration the following-
i) More focus on new case detection andtreatment completion.
ii) Improvement of quality of leprosy serviceswhich are accessible to all and follow theprinciple of equity & social justice.
iii) Strengthening referral services with morefocus on long term care of the leprosy affectedpersons.
iv) Support of NRHM for improving delivery ofleprosy services by involvement of ASHA,Village Health & Sanitation Committees andRogi Kalyan Samities.
v) Community Based Rehabilitation of leprosyaffected persons.
vi) Renewed focus on reduction of stigma &discrimination against leprosy affectedpersons and their family members.
To streamline the activities and to guide the states/UTs in proper implementation of the "New Paradigmsin NLEP", following guidelines were issued-
Guidelines for use of Treatment completionrate as an Indicator under the Nationalleprosy Eradication Programme.
Guidelines on Quarterly assessment of NewCase Detection Rate (NCDR) under NationalLeprosy Eradication Programme.
NLEP- Monitoring and Evaluation tools forimplementation of New Paradigms during 11thPlan period.
NLEP quality service indicators- Significance& actions required.
Guidelines on "other cases" under NLEP.
Disability, MB & Child proportion-Epidemiological significance & interpretations.
Guidelines on Community BasedRehabilitation.
Guidelines on reduction of Stigma andDiscrimination.
Guidelines strategy for Behavioral ChangeCommunication.
Guidelines for facilitating ReconstructiveSurgery in Leprosy.
Urban Leprosy Control Programme-
To address the complex problem like largerpopulation size, migration, poor health infrastructure
103
ANNUAL REPORT 2008-09
and increasing prevalence in urban areas, the UrbanLeprosy Programme was initiated in 2005.
Urban Leprosy Control Programme has beenimplemented since 2005 under which assistance isbeing provided by Govt. of India to 422 urban areashaving population size of more than 1 lakh. For thepurpose of providing graded assistance, the urbanareas are grouped in four categories i.e. Township I,Medium Cities I, Medium Cities II, Mega Cities.
Involvement of NGOs-
Non Governmental Organizations (NGOs) have beeninvolved for the cause of leprosy elimination for manydecades and their contributions have made a positiveimpact in reducing the prevalence of leprosy.Presently 38 NGOs are getting grant-in-aid fromGovt. of India under Survey, Education and Treatment(SET) scheme. Few NGOs have been givenrecognition for conducting reconstructive surgeries(RCS) where facilities for these services areavailable.
The NGOs serve in remote, inaccessible, uncovered,urban slums, industrial / labour population and othermarginalized population groups. The various activitiesundertaken by the NGOs are, IEC, Prevention ofImpairments and Deformities, Case Detection andM D T Delivery. From financial year 2006 onwards,Grant-in-aid is being disbursed to NGO through StateLeprosy Society. Under SET scheme, Rs. 2.22crores were released to NGOs during 2008-09.
ILEP Agencies
International Federation of Anti-leprosy Association(ILEP) is actively involved as partner in NLEP. InIndia, ILEP is constituted by 10 Agencies viz. TheLeprosy Mission, Damien Foundation of India Trust,Netherland Leprosy Relief, German Leprosy ReliefAssociation, Lepra India, ALES, AIFO, Fontilles -India, AERF - India and American Leprosy Mission.A MOU was signed with ILEP partners in October2008 for providing technical support to the programmetill March 2012. ILEP is providing support in the formof planning, monitoring & supervision of theprogramme, capacity building of GHC staff, providingre-constructive surgery services and socio economicrehabilitation of persons affected with leprosy.
WHO Support-
WHO support the programme in the form of providingfinancial assistance to the state leprosy societies andtechnical support through State/Zonal NLEPCoordinators in the high endemic states. Financialsupport to NLEP is also extended by WHO forconducting periodic review meetings at national level.WHO continues to provide requirement of anti-leprosy(MDT) drugs to the country free of cost withassistance from NOVA RTIS.
IEC-
Four video spots of IEC of Leprosy wereproduced with the help of TLM Media Centre,Noida.
Leprosy free India campaign was launchedon 30th January, 2008. Advertisement on'Leprosy Free India' was published in countrywide newspapers.
Mass Media campaign was done on fourchannels viz. D.D, Aaj Tak, Zee News andETV.
Independent evaluation of IEC activities ofthe programme were conducted by Centrefor Media Studies, New Delhi
Disability Prevention & Medical Rehabilitation(DPMR)-
The main activities carried out during the year 2008-09 are as under -
1. Implementation of DPMR activities as perguidelines and reporting its outcome -Outcome of DPMR activities e.g. treatmentof 'Leprosy Reaction', ulcers, Physiotherapy,Reconstructive Surgery and providing MCRshoes /protective aids is being reportedthrough 'Monthly Progress Report' from thestates to Central Leprosy Division. 2960persons were operated and benefited byRCS services, 39325 MCR foot wears weregiven to needy cases having anesthesia sole,28058 were provided with self care kits toprevent & treat recurrent ulcers and 11805
104
ANNUAL REPORT 2008-09
cases of Leprosy reaction were treated byPrednisolone.
2. The number of institutes providingReconstructive Surgery services has beenincreased to 63. In addition to 20 Govt.Hospitals recognized for re-constructivesurgery in the 11th Plan (PIP) another 7 Govt.Hospitals / Medical Colleges have beenrecognized in 2008-09. Similarly, 4 more NGOHospitals have been recognized in 2008-09bringing the total number NGO hospitals to36.
3. Integrating DPMR services - There areprovision of services to Persons withDisability' (PWD) by various departmentsunder different ministries. Convergence ofNLEP services into NRHM facilitated thisintegration.
4. Training of GHC staff - Many states havecarried out trainings of GHC staff to improvethe quality of DPMR services delivered byPHC system. Training of surgeons andsurgical team of medical college hospitals inleprosy surgery has enhanced the servicesof 'Reconstructive Surgery' for persons withdisability due to leprosy.
5. Monitoring DPMR activities - Analysis ofreports, feedback to states and reviewmeetings remain main activities to monitor theDPMR program. Field visits and reviewmeetings at state level has furtherstrengthened the monitoring of DPMRprogram.
6. Ministry of Health and Family Welfare iscoordinating with other ministries /departments and state governments foridentifying and striking down thediscriminatory provision existing in variousActs, Laws, Rules, Govt. Orders etc. againstleprosy affected persons.
Monitoring and Evaluation of NLEP-
NLEP has an inbuilt information system for monitoring
and supervision of the programme activities atCentral, State, District & Peripheral level.
Simplified Information System (SIS) wasintroduced in 2002 so that GHC servicepersonnel can easily adapt to the system ofrecording and reporting under theprogramme. This system has drasticallyimproved recording, reporting and itstransmission. The programme is monitoredat District, State and Central level throughscrutiny of regular monthly reports.
Leprosy Elimination Monitoring (LEM)exercise were undertaken with WHO supportthrough the NIH&FW, New Delhi, to assessthe programme achievement in identifiedindicators during the year 2002, 2003 and2004. Immediate actions were initiated on thedeficiencies observed.
An independent evaluation of the programmewas carried out during 2007-08 through theIndian Institute of Health ManagementResearch, Jaipur.
Evaluation of IEC activities under theprogramme was carried out through CentreFor Media Studies (CMS), an independentagency.
The programme is reviewed at District andPHC level in monthly meetings. Quarterlyreview meetings were held at State level forthe District Leprosy Officers and otherpartners, which are also attended by officersfor the Central Leprosy Division.
For the North Eastern and also Northernstates, Regional level meetings wereorganized in the year 2008-09, which werealso attended by all the partners'organizations.
Future Strategy-
Although the prevalence has come down at nationallevel, yet large numbers of new leprosy cases are beingdetected every year. These new cases will continue tooccur and will have to be provided quality leprosy
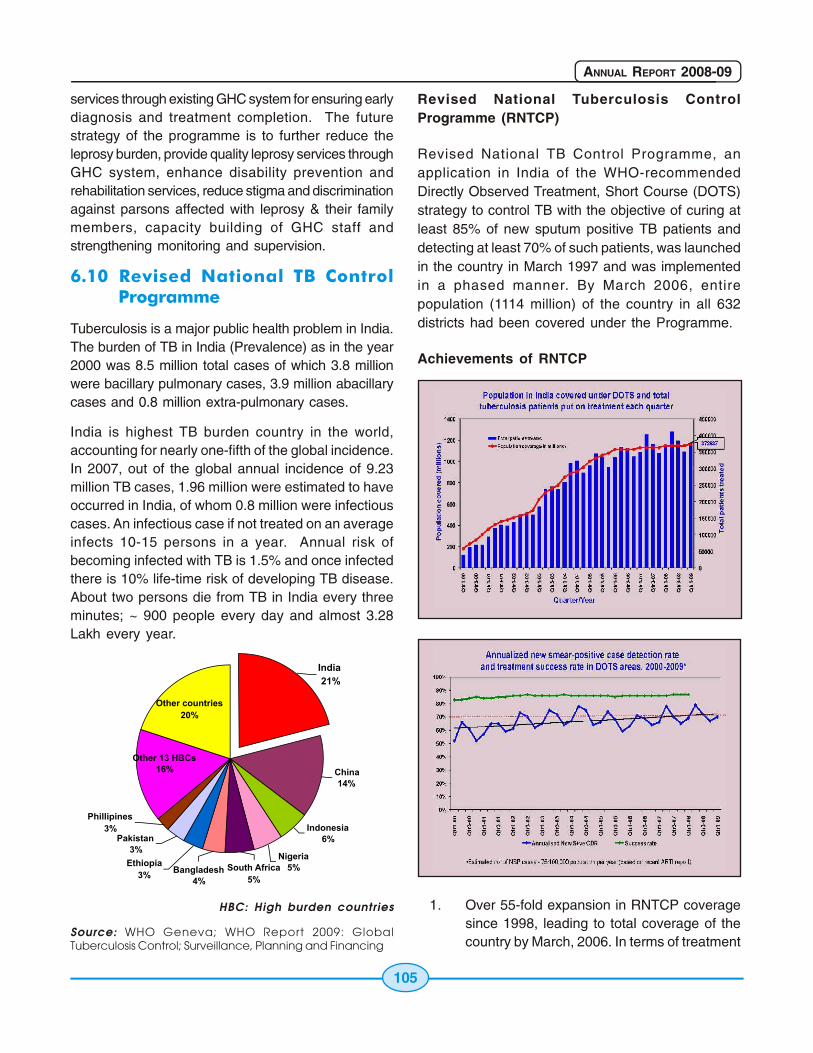
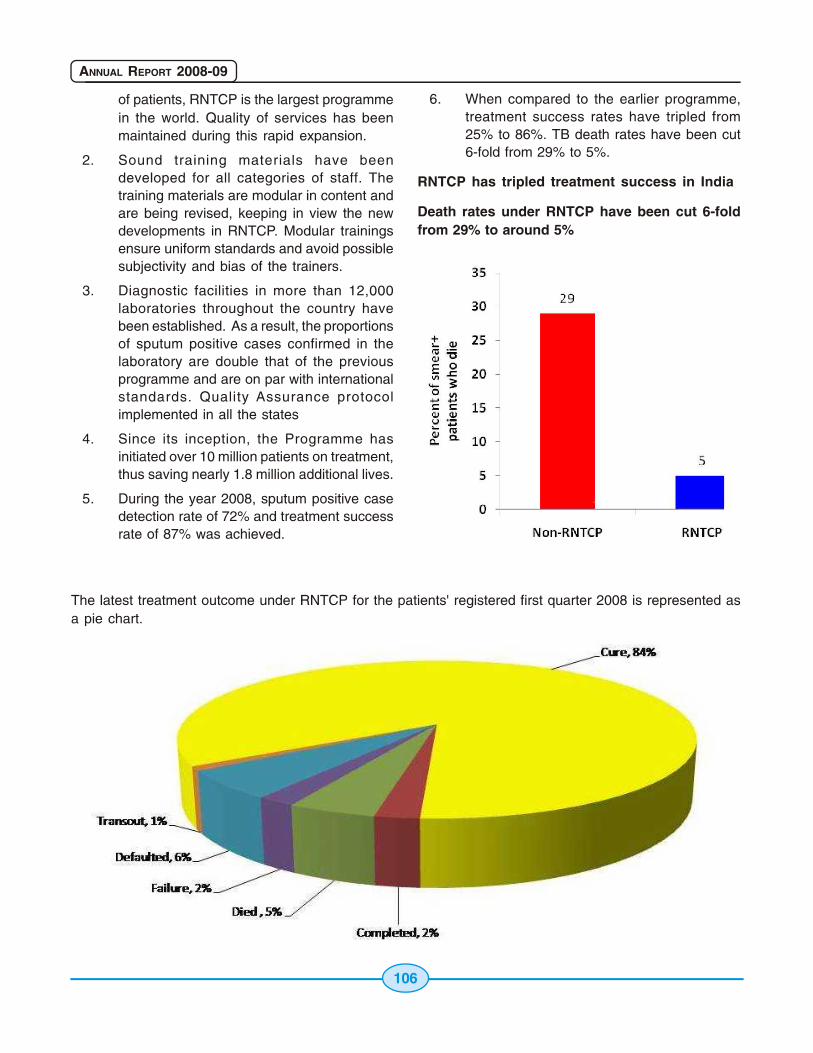
107
ANNUAL REPORT 2008-09
In 1st quarter 2009, 372,837 TB patientshave been registered for treatment.
91% of the diagnosed smear positive casesliving in the district are being put underDOTS.
~ 125,000 patients being put on DOTS everymonth.
7. Involvement of other sectors: Over 2345NGOs, 19202 Private practitioners, and 150corporate houses have been involved in theprovision of RNTCP services. Presently, 267medical colleges (including private colleges)have been involved in RNTCP and areestimated to contribute nearly 10-15% ofcase detection in the districts that havemedical colleges. Health facilities ingovernment sectors outside Health Ministryhave been involved viz. ESI, Railways, Portsand the ministries of Mines, Steel, coal, etc.Collaboration for increased participation ofall sectors in RNTCP is being strengthenedthrough constant interaction with all stakeholders, including professional bodies like theIndian Medical Association, IndianAssociation of Pediatricians.and Faith BasedOrganisations such as Catholic BishopsConference of India.
8. TB-HIV collaboration: The collaborativeactivities which were being undertaken in 14states earlier have been scaled up to involveall the states in 2007. NACP & RNTCP havedeveloped "National framework of joint TB/HIV Collaborative activities" in 2007 (laterrevised in 2008) which redefines the scopesof TB/HIV collaborative activities beingimplemented in the country. In 2008, morethan 195,055 TB suspects were referred fromICTCs to RNTCP and of them more than25,000 were diagnosed as having TB andinitiated on DOTS. More than 136,622 TBpatients were tested for HIV and of them about11,800 were diagnosed as HIV positive andwere offered access to HIV care.
9. DOTS Plus services for the management ofMDR-TB
a. The programme is in the process ofestablishing a network of about 27accredited Culture and DrugSusceptibility testing IntermediateReference Laboratories (IRL) across thecountry in a phased manner fordiagnosis and follows up of MDR TBpatients. The IRLs at Gujarat,Maharashtra, Andhra Pradesh, Delhi,Kerala, Tamil Nadu, Rajasthan havebeen accredited recently. Another 7 IRLs(Haryana, West Bengal, Uttarakhand,Chattisgarh, Jharkhand Uttar Pradesh-lucknow and Orissa) are under theaccreditation process and are expectedto be accredited in 2009. The reainingIRLs will be accredited in 2010.
b. To supplement and support the IRLnetwork the programme is also involvingMycobacteriology laboratories ofGovernment Medical Colleges as welllaboratories in the NGO and PrivateSector. Till date, two such labs (CMC-Vellore and BPRC-Hyderabad) havebeen accredited and about 12 such labshave applied for accreditation.
c. DOTS Plus services for management ofMDR TB have been rolled out in thestates of Gujarat, Maharashtra, AndhraPradesh, Haryana, Delhi, Kerala, WestBengal, Tamil Nadu and Rajasthan. Tilldate a total of around 400 MDR-TBpatients are on treatment in these states.
d. Remaining states will be covered underDOTS Plus in 2009-10.
10. Advocacy, Communication and SocialMobilization (ACSM): A training module forimproved Inter-Personal Communication(IPC) skills has been developed andincorporated in the existing modules. IECstrategy at different levels has been planned.Web based resource centre for IEC materialshas been made available on the programmewebsite. In addition to this,
o A media agency has been hired to
108
ANNUAL REPORT 2008-09
support the IEC activities at the nationallevel
o Most of the states have appointedcommunication facilitators to support theIEC activities at the district level
o Quarterly reporting on IEC activities is inplace and is monitored at the state andcentral level
11. Impact of the programme:
a. TB mortality in the country has reducedfrom over 42/lakh population in 1990 to28/lakh population in 2007 as per theWHO global report 2009.
b. The prevalence of TB in the country hasreduced from 586/lakh population in1990 to 283/lakh population by the year2007 as per the WHO global TB report,2009
c. Repeat population surveys conducted byTRC indicate an annual decline inprevalence of disease by 12%.
d. Programme is currently undertakingrepeat A RTI survey (2007-09), diseaseprevalence surveys (2007-09) toadditionally monitor the progress towardsMDGs.
RNTCP Phase II
The RNTCP Phase II of the World Bank project hasbeen approved by the Government for the periodOct 2006 to Sep 2011 for a total outlay of Rs 1,156Crore (USD 256.9 million) which includes credit fromWorld Bank of Rs 765 Crore (USD 170 million) andcommodity assistance of anti-TB drugs from DFIDthrough WHO for Rs 287 Crores (USD 63.7 million)with balance of RS 191 Crore (USD 42.5 million) willbe given by GoI. In addition, 385.5 crores is availablethrough GFATM (for 110 million population in Biharand Uttar Pradesh under Round 2, and 110 millionpopulation in the states of Andhra Pradesh andOrissa under Round 4; and 60 million population inthe states of Chhatisgarh, Jharkhand and
Uttarakhand from the Round 6) and USAID ( for entire21 million population of Haryana)
The second phase of the RNTCP is consolidating,maintaining and further improving the achievementsof the first phase. Phase II of the RNTCP is a steptowards achieving the TB-related MillenniumDevelopment Goal (MDG) targets. DOTS remain thecore strategy. In addition to the ongoing activities,the following new activities have been envisaged inthe second phase.
the scaling up of the State-level intermediatereferral laboratories (IRL) capacity for nation-wide implementation of external qualityassessment (EQA) of sputum smearmicroscopy services and provision of cultureand drug sensitivity testing.
Implementation of DOTS-Plus for multi-drugresistant TB cases will occur in a phasedmanner
Major Initiatives
Public Private Mix in RNTCP
The RNTCP employs the Public Private Mix (PPM)which is the strategy to diagnose and treat TBpatients reporting to all sectors of health care underRNTCP through a mix of different types of healthcare providers.
NGO/PPs: Currently, for enhancing the involvementof NGOs and PPS under RNTCP, the guidelines havebeen revised with enhanced financial outlays. Theprogramme has entered into a Memorandum ofunderstanding with large NGOs/ProfessionalAssociations like RK Mission, World Vision, ChristianMedical Association of India, Catholic HealthAssociation of India, Indian Medical Association etc.In addition, many local NGOs support programmeactivities to improve access of RNTCP in difficult anduncovered areas.
Medical colleges/TB Hospitals and others: Medicalcolleges are being provided with manpower andlogistic support to facilitate their participation in theprogramme. The involvement of medical colleges ismonitored by the Task Force mechanism at the State/Zonal and National levels.
109
ANNUAL REPORT 2008-09
Other sectors -All the 16 centrally owned ESIhospitals, Zonal Railway Hospitals, Coal, Steel andmines health facilities, Port trust hospitals, CGHShospitals and 150 corporate hospitals are involvedin RNTCP services.
Urban DOT Projects-The four Urban DOT projectsfunded through GFATM (round 2) at Mumbai,Hyderabad, Varanasi and Indore have completed twoyears of project with increase in case detection at allthe sites as a result of improved quality and reach ofRNTCP to special groups like slum dwellers andmigrants, through more "patient friendly" treatmentobservation, involvement of private and NGO sectorsand IEC.
Urban TB for slum dwellers - Recognizing the problemand impact of TB on urban slum population RNTCPintends to provide greater levels of access to itsservices to the urban slum population. In addition, aspecial PPM scheme for Urban Slum dwellers hasbeen introduced under the recently revised PPMschemes.
Other initiatives-
The IMA has formed a National Working Group forRNTCP and has selected National and Statecoordinators. National, state and local workshops arebeing organized by the IMA to sensitise the opinionleaders. The PPM project assisted by GFATM (round6) has been launched from April '07 which is to beimplemented in the states of UP, AP, Maharashtra,Punjab, Haryana, and Chandigarh.
There has also been a Professional coalition againstTB by IMA with IAP(Indian Academy ofPediatrics),NCCP (National College of ChestPhysicians),ICS (Indian Chest Society),FPAI(Federation of Family Physicians Association of India)as its members.
The RNTCP has adopted the recently published"International Standards for TB Care" (ISTC)document to improve the standards of TBmanagement across all sectors of health care inIndia, and to recruit and involve additional healthcare providers in RNTCP activities. As the RNTCPconforms to all standards laid down in the ISTC, the
central government has urged all providers of healthcare to adopt RNTCP to ensure adherence to theinternationally recognized standard of care for TB.
The 14 pilot districts under the intensified PPMsurveillance started in 2003 continue to be as sentinelsites.
TB/HIV coordination: Globally, the HIV epidemic isworsening the TB situation, by increasing the numberof tuberculosis cases and accelerating the spreadof the disease. HIV increases a person'ssusceptibility to TB infection and Tuberculosisincreases morbidity and mortality in HIV infectedpersons. HIV is the most potent risk factor forprogression of TB infection to disease. Since 2001,Government has been implementing a joint actionplan in co-ordination with National AIDS ControlProgramme (NACP), to counter the growingincidence of the HIV-TB Co-infection, initially in thesix high HIV prevalence States of Maharashtra, TamilNadu, Andhra Pradesh, Karnataka, Manipur andNagaland. Services for HIV infected TB patients areprovided through linkages between the IntegratedCounseling and Testing Centre (ICTC) supported bythe HIV/AIDS Programme and DesignatedMicroscopy Centres (DMCs) supported by RNTCP,joint IEC activities and infection control measures.
In 2007, the national action plan for TB/HIV has beenrevised. RNTCP & NACP have formulated a Nationalframework for joint TB/HIV Collaborative activitieswhich replaces the action plan. The documentelaborates the various activities that need to beundertaken at the National, State & district level andprovides the guidelines for the same. Under theNational framework there is enhanced focus on theprovision of HIV care including A RT, for all knownHIV infected TB patients in order to reduce mortalityin this group of TB patients. With the formulation ofNational framework, the TB/HIV collaborative activitiesare being extended to the entire country. Theframework looks to establish mechanisms forcoordination between the two programmes at all level.Technical working groups with the key staff of boththe programmes as members have been establishedat the National and State level, which are meeting ona monthly basis.
110
ANNUAL REPORT 2008-09
A RT- DOTS linkages are being established at all theA RT centres of the AIDS control programme to ensureoptimal access to TB diagnostic and treatmentservices to the HIV positives at advanced stage ofdisease. Medical officers posted at the A RT Centreshave been trained in RNTCP so as to prioritize jointtraining modules on TB/HIV have been formulatedfor various categories of staff of RNTCP and NACPand the training activities are being scaled up. TO Tshave been conducted for State and District leveltrainers and the training of field staff is on-going andis at various stages in the different States. IECmaterials regarding TB are being made available atNACP facilities. Selective IEC material on HIV isdisplayed at RNTCP facilities.
MDR-TB: Another challenge to TB control in India isthe MDR-TB. The data available to date shows thatlevels of MDR-TB remain relatively low, at around3%, amongst new patients and 12-17% in re-treatment cases. However, these relatively lowpercentage figures translate into large absolutenumber of MDR-TB cases, which increase themagnitude and severity of TB epidemic and pose amajor threat to TB control. Guidelines formanagement of MDR TB cases (DOTS Plus) havebeen formulated and published. The ProgrammeDivision has an ambitious plan to scale up servicesfor management of MDR-TB patients in the countryand is in the process of securing funding for the same.
Information, Education and communication (IEC) orAdvocacy, Communication and Social Mobilization(ACSM) continue to be an important component ofthe programme. In line with the Stop TB strategy,replacement of the terminology with 'Advocacy,Communication, and Social Mobilization' (ACSM) isbeing promoted, as the term ACSM has advantageover IEC as it clearly defines the components andinitiatives.
The IEC strategy in RNTCP envisages that:
1. IEC is a long term commitment where in IECis a process and not product oriented.Implementing IEC activities is based onanalysis of the needs, and developingstrategy to plan need based, locally
appropriate activities. Communicationstrategies for TB control takes care ofopportunities for interactive communication,such as engaging cured patients to convinceand support others, group meetings todiscuss all aspects of TB control, includingthe social aspects.
2. It focuses on decentralized planning, choiceof communication channels and monitoringto ensure contextual relevance and widereach of information. The states and districtshave to take active part in this process whileCentre continues to provide leadership,develop core messages, mass media andadvocacy events.
3. IEC takes care to address social issuesrelated to TB such as stigma and gender,and special communication initiatives toaddress the needs of the special groups and'hard to reach populations'
RNTCP emphasizes on decentralized planning andimplementation of health communication initiatives.States and districts develop need based annual actionplans and implement activities using local popularmedia. To support the districts in planning andimplementing, Communication Facilitators have beenengaged who identify opportunities and networkthrough which communication activities areundertaken to spread information about TB andavailability of free diagnosis and DOTS treatment.Other important role of Communication Facilitatorsis to integrate communication about TB within thecontext of other health programmes and NRHM.
RNTCP encourages states to: i) systematic planningand implementation of communication activities basedon the needs, knowledge of target groups, using thelocal appropriate media; ii) to undertake IEC activityfor maintaining desired level of awareness,motivation, support and services in patient friendlyenvironment; and iii) monitor IEC activities regularlylike other components of the programme.
RNTCP is also working to increase in state and districtlevel capacity to plan and execute IEC activities. Forthis purpose, each state has undertaken an IEC audit
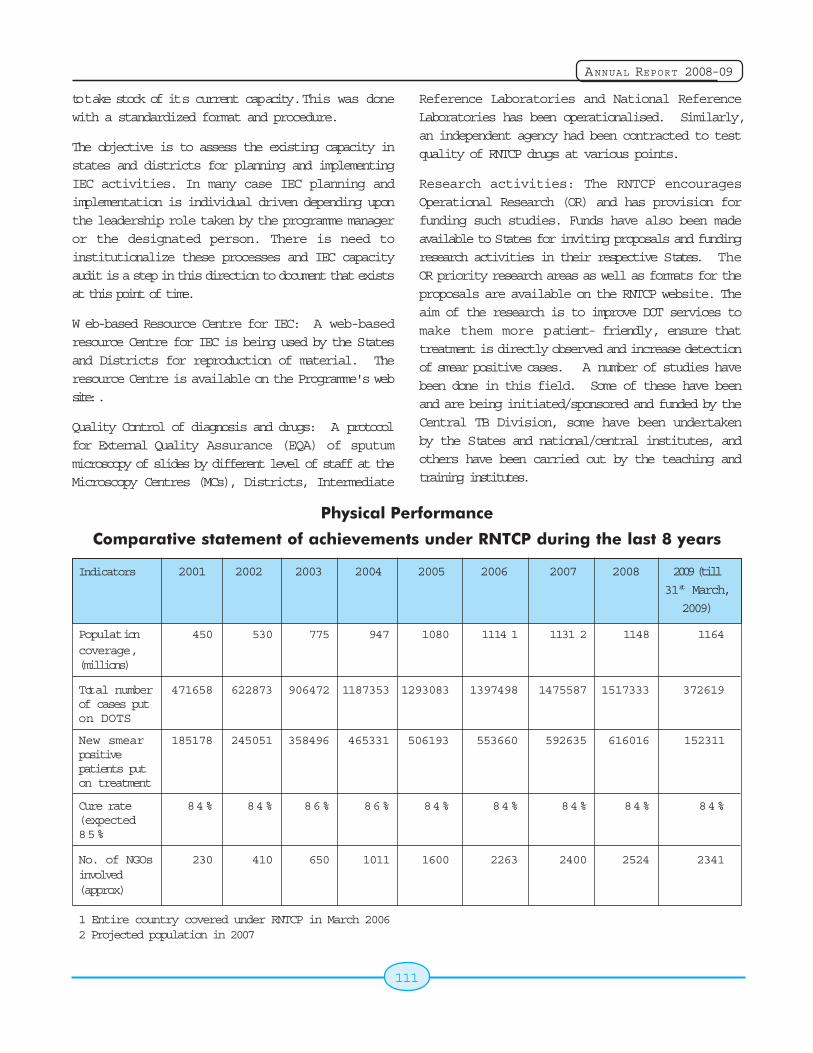
111
ANNUAL REPORT 2008-09
to take stock of its current capacity. This was donewith a standardized format and procedure.
The objective is to assess the existing capacity instates and districts for planning and implementingIEC activities. In many case IEC planning andimplementation is individual driven depending uponthe leadership role taken by the programme manageror the designated person. There is need toinstitutionalize these processes and IEC capacityaudit is a step in this direction to document that existsat this point of time.
W eb-based Resource Centre for IEC: A web-basedresource Centre for IEC is being used by the Statesand Districts for reproduction of material. Theresource Centre is available on the Programme's website: .
Quality Control of diagnosis and drugs: A protocolfor External Quality Assurance (EQA) of sputummicroscopy of slides by different level of staff at theMicroscopy Centres (MCs), Districts, Intermediate
Reference Laboratories and National ReferenceLaboratories has been operationalised. Similarly,an independent agency had been contracted to testquality of RNTCP drugs at various points.
Research activities: The RNTCP encouragesOperational Research (OR) and has provision forfunding such studies. Funds have also been madeavailable to States for inviting proposals and fundingresearch activities in their respective States. TheOR priority research areas as well as formats for theproposals are available on the RNTCP website. Theaim of the research is to improve DOT services tomake them more patient- friendly, ensure thattreatment is directly observed and increase detectionof smear positive cases. A number of studies havebeen done in this field. Some of these have beenand are being initiated/sponsored and funded by theCentral TB Division, some have been undertakenby the States and national/central institutes, andothers have been carried out by the teaching andtraining institutes.
Physical Performance
Comparative statement of achievements under RNTCP during the last 8 years
Indicators 2001 2002 2003 2004 2005 2006 2007 2008 2009 (till
31st March,
2009)
Population 450 530 775 947 1080 1114 1 1131 2 1148 1164coverage,(millions)
Total number 471658 622873 906472 1187353 1293083 1397498 1475587 1517333 372619of cases puton DOTS
New smear 185178 245051 358496 465331 506193 553660 592635 616016 152311positivepatients puton treatment
Cure rate 84% 84% 86% 86% 84% 84% 84% 84% 84%(expected85%
No. of NGOs 230 410 650 1011 1600 2263 2400 2524 2341involved(approx)
1 Entire country covered under RNTCP in March 20062 Projected population in 2007
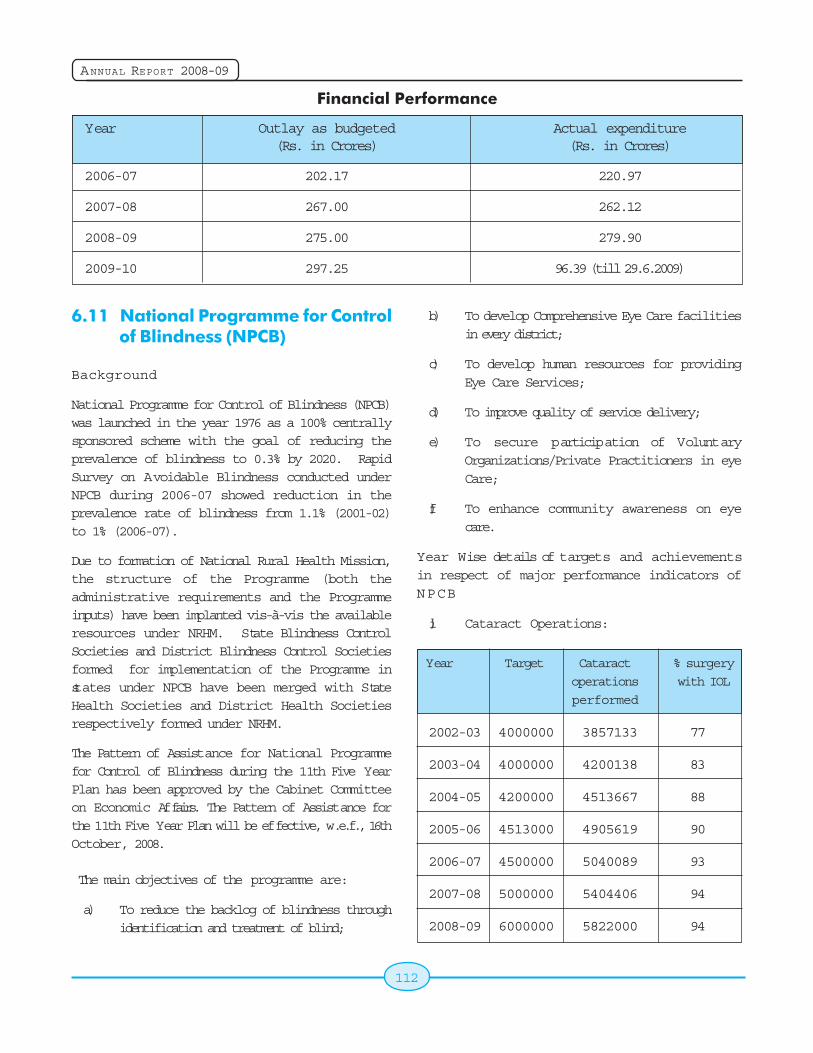
112
ANNUAL REPORT 2008-09
Financial Performance
Year Outlay as budgeted Actual expenditure(Rs. in Crores) (Rs. in Crores)
2006-07 202.17 220.97
2007-08 267.00 262.12
2008-09 275.00 279.90
2009-10 297.25 96.39 (till 29.6.2009)
6.11 National Programme for Controlof Blindness (NPCB)
Background
National Programme for Control of Blindness (NPCB)was launched in the year 1976 as a 100% centrallysponsored scheme with the goal of reducing theprevalence of blindness to 0.3% by 2020. RapidSurvey on Avoidable Blindness conducted underNPCB during 2006-07 showed reduction in theprevalence rate of blindness from 1.1% (2001-02)to 1% (2006-07).
Due to formation of National Rural Health Mission,the structure of the Programme (both theadministrative requirements and the Programmeinputs) have been implanted vis-à-vis the availableresources under NRHM. State Blindness ControlSocieties and District Blindness Control Societiesformed for implementation of the Programme instates under NPCB have been merged with StateHealth Societies and District Health Societiesrespectively formed under NRHM.
The Pattern of Assistance for National Programmefor Control of Blindness during the 11th Five YearPlan has been approved by the Cabinet Committeeon Economic Affairs. The Pattern of Assistance forthe 11th Five Year Plan will be effective, w.e.f., 16thOctober, 2008.
The main objectives of the programme are:
a) To reduce the backlog of blindness throughidentification and treatment of blind;
b) To develop Comprehensive Eye Care facilitiesin every district;
c) To develop human resources for providingEye Care Services;
d) To improve quality of service delivery;
e) To secure participation of VoluntaryOrganizations/Private Practitioners in eyeCare;
f) To enhance community awareness on eyecare.
Year Wise details of targets and achievementsin respect of major performance indicators ofNPCB
i) Cataract Operations:
Year Target Cataract % surgery
operations with IOL
performed
2002-03 4000000 3857133 77
2003-04 4000000 4200138 83
2004-05 4200000 4513667 88
2005-06 4513000 4905619 90
2006-07 4500000 5040089 93
2007-08 5000000 5404406 94
2008-09 6000000 5822000 94
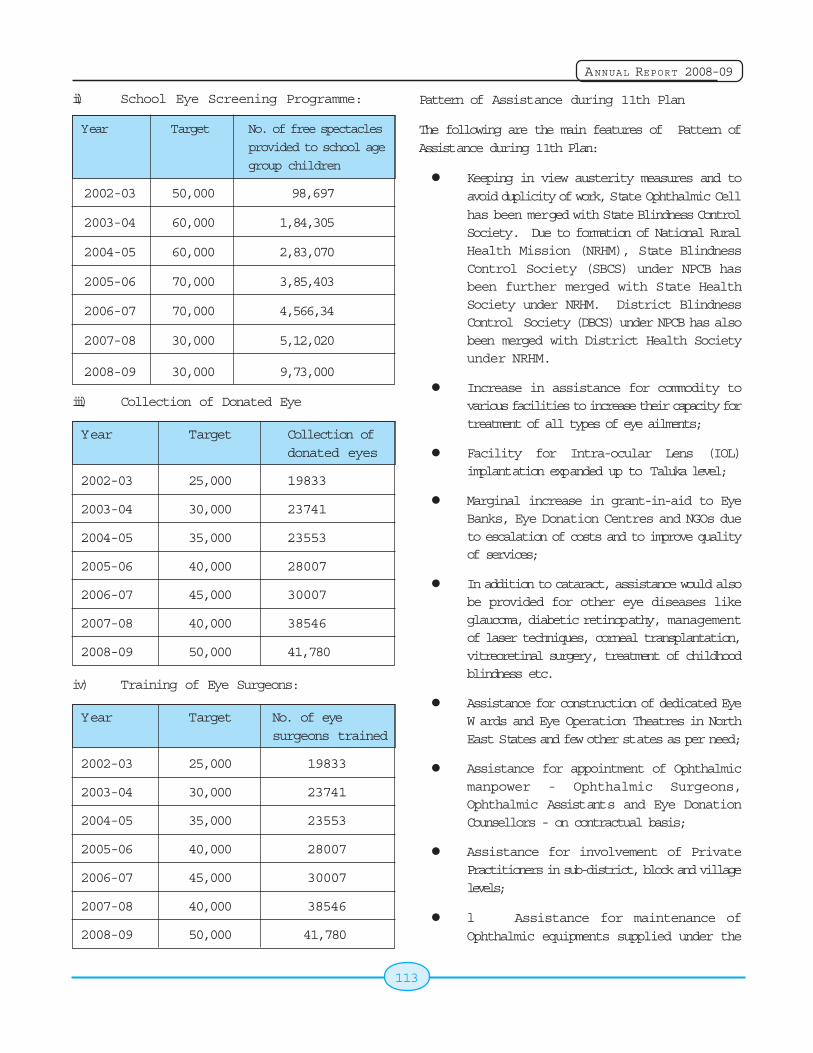
113
ANNUAL REPORT 2008-09
ii) School Eye Screening Programme:
Year Target No. of free spectacles
provided to school age
group children
2002-03 50,000 98,697
2003-04 60,000 1,84,305
2004-05 60,000 2,83,070
2005-06 70,000 3,85,403
2006-07 70,000 4,566,34
2007-08 30,000 5,12,020
2008-09 30,000 9,73,000
iii) Collection of Donated Eye
Year Target Collection ofdonated eyes
2002-03 25,000 19833
2003-04 30,000 23741
2004-05 35,000 23553
2005-06 40,000 28007
2006-07 45,000 30007
2007-08 40,000 38546
2008-09 50,000 41,780
iv) Training of Eye Surgeons:
Year Target No. of eyesurgeons trained
2002-03 25,000 19833
2003-04 30,000 23741
2004-05 35,000 23553
2005-06 40,000 28007
2006-07 45,000 30007
2007-08 40,000 38546
2008-09 50,000 41,780
Pattern of Assistance during 11th Plan
The following are the main features of Pattern ofAssistance during 11th Plan:
Keeping in view austerity measures and toavoid duplicity of work, State Ophthalmic Cellhas been merged with State Blindness ControlSociety. Due to formation of National RuralHealth Mission (NRHM), State BlindnessControl Society (SBCS) under NPCB hasbeen further merged with State HealthSociety under NRHM. District BlindnessControl Society (DBCS) under NPCB has alsobeen merged with District Health Societyunder NRHM.
Increase in assistance for commodity tovarious facilities to increase their capacity fortreatment of all types of eye ailments;
Facility for Intra-ocular Lens (IOL)implantation expanded up to Taluka level;
Marginal increase in grant-in-aid to EyeBanks, Eye Donation Centres and NGOs dueto escalation of costs and to improve qualityof services;
In addition to cataract, assistance would alsobe provided for other eye diseases likeglaucoma, diabetic retinopathy, managementof laser techniques, corneal transplantation,vitreoretinal surgery, treatment of childhoodblindness etc.
Assistance for construction of dedicated EyeW ards and Eye Operation Theatres in NorthEast States and few other states as per need;
Assistance for appointment of Ophthalmicmanpower - Ophthalmic Surgeons,Ophthalmic Assistants and Eye DonationCounsellors - on contractual basis;
Assistance for involvement of PrivatePractitioners in sub-district, block and villagelevels;
l Assistance for maintenance ofOphthalmic equipments supplied under the
114
ANNUAL REPORT 2008-09
programme; Development of MobileOphthalmic Units with Tele-ophthalmologyNetwork and some fixed tele-models to coverdifficult hilly terrains and difficult areas;
Critical posts of 228 Eye Surgeons and 510Ophthalmic Assistants sanctioned during the9th Plan and continued during 10th Plan,would be integrated within the State Plan ina phased manner;
Strengthening of Management InformationSystem;
Intensification of IEC activities.
New Initiatives during 11th Five Year Plan
1. Construction of dedicated Eye Wards & EyeO Ts in District Hospitals in North-EasternStates, Bihar, Jharkhand, J&K, HimachalPradesh, Uttarakhand and few other Stateswhere dedicated Operation Theaters are notavailable as per demand.
2. Appointment of Ophthalmic manpower(Ophthalmic Surgeons, OphthalmicAssistants and Eye Donation counselors oncontractual basis.
3. Grant-in-aid to NGOs for managementof other Eye diseases other than Cataractlike Diabetic Retinopathy, GlaucomaManagement, Laser Techniques, CornealTransplantation, Vitreoretinal Surgery,Treatment of childhood blindness etc. of Rs.750 per case for Cataract/IOL ImplantationSurgery and Rs.1000 per case of other majorEye Diseases as described above.
4. Development of Mobile Ophthalmic Units inNE States, Hilly States & difficult Terrains fordiagnosis and medical management of eyediseases.
5. Involvement of Private Practitioners in SubDistrict, Blocks and Village Level.
6. Maintenance of Ophthalmic Equipmentssupplied to Regional Institutes of Ophthalmo-
logy, Medical Colleges, District/Sub-DistrictHospitals, PHC/Vision Centres.
6.12 National Iodine DeficiencyDisorders Control Programme
Iodine is an essential micronutrient required daily at100-150 micrograms for normal human growth anddevelopment. Deficiency of Iodine can causephysical and mental retardation, cretinism, abortions,
stillbirth, deaf mutism, squint & various types of goiter.
Results of sample surveys conducted in 325 districts
covering all the States/Union Territories have
revealed that 263 districts are endemic where theprevalence of Iodine Deficiency Disorders is more
than 10%. It is estimated that more than 71 million
persons are suffering from goiter and other Iodine
Deficiency Disorders.
Objectives:
Surveys to assess the magnitude of the
Iodine Deficiency Disorders.
Supply of iodated salt in place of commonsalt.
Resurveys to assess iodine deficiency
disorders and the impact of iodated salt after
every 5 years.
Laboratory monitoring of iodated salt and
urinary iodine excretion.
Health Education and Publicity.
Achievements:
Consequent upon liberalization of Iodated salt
production, Salt Commissioner has issued
licenses to 824 salt manufacturers out of
which 532 units have commenced production.
These units have an annual production
capacity of 124 lakh metric tones of Iodatedsalt.
A production of Iodated salt of 49.61 lakh MT
was recorded during the period from April 07
to March 2008 against 50.00 lakh MT targetfor the year 2007-08.
115
ANNUAL REPORT 2008-09
The Ministry of Health & Family Welfare have
issued notification banning the sale of Non
Iodized salt for direct human consumption in
the entire country w.e.f.17th May,2006 for
effective implementation of NIDDCP at the
state level.
For effective implementation of NIDDCP 31
States/UTs have established IDD Control
Cells at the State Health Directorate.
In order to monitor the quality of Iodated salt
and Urinary Iodine excretion 18 States/UTs
have already set up IDD monitoring
laboratories while the remaining States are
in the process of establishing the same.
For ensuring the quality of Iodized salt at
consumption level, a total No. of 25857 salt
samples were analyzed out of which 22613
(87.55%) salt samples were found confirming
to the standards during the year 2006-07.
IDD survey was conducted in the Cuttack
district of Orissa State during the month of
January 2008. The State Government of
Punjab has conducted 3 District surveys in
their state during the year 2007-08.
Global IDD prevention day was observed
throughout the country on 21st October,
2007. Massages on benefits of consumption
of iodated salt in prevention and control of
IDD were published in National and Regional
News papers on the eve of Global IDD Day .
A Two Days National workshop on NIDDCP
was organized on the occasion at vigyan
bahvan, New Delhi.
Information Education &Communication
Activities
Activities through Song and Drama
Song and Drama Division carried out extensive IECcampaign activities, through their field units in 16States till 31st March, 2008.
Activities through the Directorate of FieldPublicity
The Directorate of Field Publicity carried out special
programmes through their 207 regional units in 29
States for extensive IEC campaigns in the country
regarding consumption of Iodated salt in prevention
and control of IDDs. The activities include Film
shows, Group discussion and other special
programmes
Activities through Doordarshan
IDD Spots containing messages on consequences
of Iodine Deficiency Disorders and benefits of
consuming Iodated salt were telecast (i) through the
National Network of Doordarshan on an average 4-
5 times daily and telecast of the IDD messages thrice
in a week under the Health Magazine Kalyani
Programme from the 8 regional Kendaras of
Doordarsahn in regional languages.
Activities through All India Radio
IDD spots containing messages on consequences
of Iodine Deficiency Disorders and benefits of
consuming Iodated salt were broadcast by the All
India Radio through its 40 regional channels, 123
primary channels and 22 FM channels from April
2007.
Activities through the Directorate of
Advertisement and Visual Publicity
Messages for consumption of Iodated salt to
overcome the problem of Iodine Deficiency Disorders
were published in the leading 543National as well as
regional Newspapers on the occasion of Global IDD
Day on 21.10.2007.
Activities through the State Health Directorate
State Governments have also provided grants for
undertaking IEC activities at the local level in their
regional languages to make the impact of IEC
activities more effective including celebration of
Global IDD prevention day in their all districts.

116
ANNUAL REPORT 2008-09
117
ANNUAL REPORT 2008-09
Chapter 7
7.1 Introduction
Public policy and communication strategies influenceboth individual and collective change. The interfacebetween these two components provides theframework to position behaviour change. In otherwords, the balance between communication and
policy facilitates health seeking behaviour. Over the
years the thrust of the Department has been to place
IEC as an intervention tool to generate demand for
the range of services under the umbrella framework
of National Rural Health Mission (NRHM).
The Communication Strategy aims to facilitate
awareness, disseminate information regarding
availability of and access to quality health care within
our Public Health System. The key objective of the
strategy is to encourage a health seeking behaviour
that is doable in the context in which people live.
The strategy views recipients of health services as
not merely users of services but key participants in
generating demand for services.
During the year, the communication strategy has
focused on sustaining behaviour change on key
health issues through multi media tools. This implies
that it was not enough to just give information and
raise awareness about a particular health issue,
awareness and information dissemination should be
used as tools to provide tools to the community to
press for changes to improve access to health service
provisions.
Under the framework for implementation in the
National Rural Health Mission, norms have also been
outlined for supporting IEC activities. The framework
incorporates a variety of activities involvingcommunities and also the media.
Information, EducationInformation, EducationInformation, EducationInformation, EducationInformation, Educationand Communicationand Communicationand Communicationand Communicationand Communication
IEC initiatives undertaken during the year underNRHM:
To position focussed visibility through multimedia tools
Branding of the key IEC intervention underNRHM
To create enabling environment for Healthproviders through on intra communicationprocess
Communication tools to inter-link demandgeneration with access and availability ofservices
Strong emphasis on integrated IEC forfocused content delivery
Combination of mass media, social mobilizationand inter-personal communication methods
Close monitoring of actual media utilizationand behavioral outcomes along with financialallocations
Designing innovative strategies
National Immunization Day(NID) held in Jan.-Feb. 2009.
The following tools were used during the year:
Interpersonal Communication
Community Channels
Mass Media
Folk and Traditional Media
Outdoor Media
118
ANNUAL REPORT 2008-09
Advocacy
Events, Image management, PR and Publicity
Intra communication
The target audiences included:
Direct Healthcare Providers(ANM, ASHA,
AW W )
Healthcare Managers / Administrative
functionaries
Health Communicators
Grass-root functionaries
Other Govt. Departments, e.g. Panchayati
Raj, WCD, Water & Sanitation
NGOs, Civil society stake holders and Media
During the year, the following issues were being
highlighted through multi-media tools:
Janani Suraksha Yojana
ASHA
Age at Marriage
Routine Immunization
PNDT and Girl Child
Contraceptive choice and spacing
Breast Feeding
Use of Iodized Salt
Care of New born
Institutional delivery
Maternal Care, Positioning of ASHA, Village
and Health Nutrition Day, JSY, IMNCI and also
awareness campaign on age at marriage,
PNDT, spacing and contraception.
Adolescent health
RCH and HIV/AIDS
Communicable and non communicablediseases Platform for integration
A Budget allocation of Rs. 186.31 Crores wasprovided for IEC for the year 2008-09 for IEC.
Major achievements during 2008-09 were as under:
- Reinforcing the brand identity for NRHM.
- Innovations at State level for NRHM advocacy
- Intra Communication strategies forimplementation at State level
- New content for multi-media tools
- Integrated IEC management through KalyaniProgramme News Magazine format throughPrasar Bharati being telecast from EAGStates and Assam.
- Special publications on achievements ofNRHM capturing developments in States
- Sponsorship of Access Cards at TirumalaTirupati Devasthanams for disseminatingHealth Messages under NRHM.
- Reinforced presence in Cable and SatelliteTV channels and Private FM Radio.
- Special theme based issues for NRHMNewsletter.
The IEC strategy of the Department has undergonea strategic shift. The communication challenge todayis not only demand generation, creating awareness,but at the same time initiating a comprehensiveunderstanding of behavior change communicationin the socio-cultural framework of our Public HealthSystem. A number of initiatives were taken toprofessionalize IEC activities and emphasis was laidon intensive media planning and inter-personaltechniques for effective rollout of programmes andmessages.
7.2 Activities through Media Units ofI & B Ministry
The Media Units of the Ministry of Information andBroadcasting provide communication support to the
119
ANNUAL REPORT 2008-09
FW Programmes as per the requirements andguidelines of the IEC Division of MOHFW. The focusis on mother and child health issues, populationgrowth, status of women, small family norms, theCommunity Needs Assessment Approach and alsoother issues related to health programmes such asOphthalmology, Cancer, Tobacco etc.
Doordarshan
Doordarshan telecasted video spots at prime timeon a range of NRHM issues including PolioEradication. Spots were telecast on regional channelsas well. Doordarshan also telecasted variousprogrammes including panel discussions, interviewsand covered important functions related to NRHMactivities in the States. A half an hour MagazineProgramme entitled 'Kalyani' I & II is being telecastfrom regional kendras of Doordarshan of 9 States.Spots in regional languages of N.E. Region weredubbed for telecast in N.E.States as a specialcampaign. Video Spots were not only being telecastfrom Prasar Bharti but also from the satellite channelsin Hindi and regional languages. A tele-serial ''Atmaja'of 13 episodes was telecast on Doordarshan. KyonkiJeena Isi ka Naam Hai - A teleserial on the theme ofNRHM produced by UNICEF and M/O Health andFamily Welfare and was telecast on DD-I at primetime.
Special campaign on Safe Motherhood and BreastFeeding and Save the Girl Child were launched.Panel discussions and programmes were alsotelecast under the Kalyani Programme. The videoSpots on Emergency Contraceptive Pill, NSV andCuT-380-A were telecast through discussions alsoincorporated in Kalyani-II Programme.
D AVP
D AVP produced a number of video spots under theNRHM programme. These spots were dubbed inregional languages and were telecast on PrasarBharti/Satellite channels.
Cinema Theatres
Cinema Theatre is a new initiative. The medium ofcinema theatre was used to disseminate health
messages. NRHM spots were shown in cinematheatres throughout the country.
Song and Drama Division
To educate the people about Family Welfare issues,
Song & Drama Division organized live entertainment
programmes like puppet shows, dance, dramas, folk
shows, during India International Trade Fair 2008.
All India Radio
At present the major Programme on All India Radio
are also follows.
- The spots of 30 second duration are also
being broadcast 12-14 times on popular
programme and a film on woman programme
on rural programme and also before and after
Regional news being broadcast from primary
channels in 18 States.
- Ministry has also hired slots in the National
News for the broadcast of NRHM spots of 30
second duration before National News at 7.59
a.m., between the National News and at 8.10
a.m. before the National News at 8.44 p.m.
and between the National News in the
evening.
- NRHM spots were also being broadcast at
prime time on private FM channels like Radio
Mirchi, Radio City, Red FM, Go FM and other
channels through DAVP.
7.3 Press Information Bureau
It provided media coverage on important occasions,
events, activities, policies and programmes of the
Department. PIB arranged coverage of Family
Welfare Melas, World Population Day functions,
Pulse Polio Programme and other important events.
7.4 Activities in the States/UnionTerritories
Activities were given multi-dimensional and integrated
thrust to increase the outreach and impact of
Reproductive and Child Health and Family Welfare
messages with the objective of bridging the gap
120
ANNUAL REPORT 2008-09
between awareness and acceptance. Annual plansfor 2008-2009 with an outlay of Rs. 186.31croreswere formulated through closer interactions withStates, keeping in view the differential approach.
7.5 Training of IEC Personnel
The IEC Division organised a series of capacitybuilding programmes for IEC personnel at Central,States and district level through NIHFW, New Delhiand other State Training Centres. The awarenessgeneration training coordinated by the NationalInstitute of Health & Family Welfare for healthfunctionaries of the State & district level include amodule on inter-personal communication.
7.6 World Population Day
Like every year, the World Population Day wasobserved on 11th July, 2008. The function wasorganized at Patna.
7.7 Exhibition in IITF, 2008
The main theme of the Family Welfare Exhibition was"Swastha Bharat Samardha Bharat" covering issuesof National Rural Health Mission(NRHM). Progressand services under following schemes: JananiSurakshya Yojana(JSY); Safe Motherhood;Accredited Social Health Activists (ASHA);Observation of Village Health Day in AnganwadiCentre and supplementary nutrition; UniversalImmunization Programme and immunization Care ofinfant; Reproductive and Child Health (RCH);Comprehensive Primary Health Care; PNDT;Adolescent Health and Right Age of Marriage;Promotion of Healthy Life Style; Anti-tobaccocampaign and related health hazard like Cancer, T.B.,etc. along with vector borne diseases controlledprogramme, were incorporated and displayedthrough pictures, TV spots and laser show.
Free health checkups i) Blood test, ii) Height test, iii)Weight test, iv) Eye test, vi) Family planningcounseling and services for male, vii) Family planningcounseling and services for female with various familywelfare methods, viii) treatment for communicableand non communicable diseases were arranged bythe systems of Allopathic, Ayurvedic, Homeopathic,
Unani, etc. of CGHS Wing and NCT Delhi to patrons. Non Scalpel Vasectomy (NSV) counseling and 249NSV operation were performed in the pavilion; AIDS/HIV counseling and free HIV test was performed. Oneperson was found positive. Live Yoga performancewas organized by the Morarji Desai Rashtriya YogaSansthan, New Delhi for adopting healthy life styleto live healthy. Educative live cultural shows wereorganized in foreground near entrance of pavilionby the Song and Drama Division. In addition to aboveUNICEF, HLL, VHAI, JSK, Heart Care Foundation, etc.also participated in our exhibition.
The jury of the India Trade Promotion Organization,ITPO adjudged our pavilion for excellence and theUnion Minister of State for Commerce and Power,Mr. Jairam Ramesh awarded to this Ministry GoldMedal and certificate of excellence on 27.11.08.
7.8 Adolescent Health Programme
Adolescent health is a critical component of RCHprogramme. The strategy for addressing AdolescentSexual and Reproduction Health in the RCH-IIprogramme was approved. A two-pronged strategywas adopted for mainstreaming adolescent healthin the public health management system. In the firstcomponent, the Deptt. would incorporate adolescentissues in all RCH training programmes and all contentrelated to RCH in order to facilitate behavior change.This would entail interventions for addressing unmetneed for contraception and pregnancy care,prevention of STIs including HIV/AIDS. In the secondstage of the strategy, the overall conceptualframework would be implemented in selected districtsidentified across the country. The objective being tointroduce adolescent health in the public healthsystem in a phased manner so as to cover 75 Districtsin the country.
It may be mentioned that adolescent development isa broad issue of which Ministry of Youth Affairs andSports is the Nodal Ministry.
7.9 Print Software/Print Publicity
Press Advertisements:
The IEC Campaign through Press Advertisements
121
ANNUAL REPORT 2008-09
enabled the division to highlight key initiatives in bothnational and regional media. A number of campaignswere launched through the national and regionalpress. Especially designed full page colouradvertisement on the occasion of World Health Dayand half page advertisement on Safe MotherhoodDay 2008 were released in the newspapers all overthe country to generate mass awareness on healthissues. Colourful advertisements on National RuralHealth Mission were released to the newspapers onthe occasion of Independence Day, Gandhi Jayantiand Republic Day2009. Special campaign in the formof full page colour advertisement highlightinginitiatives and achievements of various programmesunder National Rural Health Mission were alsoreleased in the newspapers on 25.2.09, 26.2.09,27.2.09 and 01.3.09.
The most intensive print media campaign was forthe Pulse Polio Programme which was donesystematically through a series of pressadvertisements in numerous newspapers on all Indiabasis, on and before all the rounds of the PPIProgramme. This included thematic advertisementsdesigned by IEC Division in the PPI programmebefore the Pulse Polio rounds.
The IEC Division also released advertisement basedon focused theme such as save the girl child, PNDTrelated issues, Maternal Child Health Care, WorldPopulation Day, IITF etc. The Division as part of anintegrated IEC campaign covered a range of issueson NRHM related themes which provided a platformfor information dissemination and awareness buildingan advocacy through the print media.
Print Software:
In order to showcase NRHM as a flagship programme,emphasis was laid on publishing a series ofdocuments. Each document reflected critical areasof NRHM and related programmes. Thesedocuments were distributed at major advocacymeetings and programmes to all stake-holders. Theprominent documents published during the yearwere:
a) NRHM: Making a difference everywhere;
b) India Guaranteeing Quality PrimaryHealthcare for All;
c) Bulletin on Rural Health Statistics in India;
d) 3 Books on Indian Public Health Standardsfor Sub-Centres, PHCs & CHCs;
e) 5 Books on Indian Public Health Standardsfor Sub-Div./Sub-District and DistrictHospitals; and
f) Guidelines for VHSC, Untied Funds for SCs,PHCs & Rogi Kalyan Samities etc.
The IEC Division also published a number of posterson Health issues in English, Hindi and regionallanguages to generate awareness among thepeople.
7.10 NRHM Newsletter
The NRHM Newsletter is now established as animportant publication for promotion of theprogrammes under National Rural Health Mission.The NRHM Newsletter is being published in Hindi,English, Assamese, Urdu, Oriya and Tamil for healthfunctionaries and NGOs working at the Sub-Centre,PHC, CHC and District level. The Newsletter publishesview points of all development partners, viz. NGOs,donor agencies etc.
During the year, a special issue of Newsletter on"Save the Girl Child Campaign" was brought out. Thefocus of this special issue was adverse sex ratio andimplementation of PC&PNDT Act in States/UTs andsave the girl child.
Another special issue was on "Janani SurakshaYojana" and Public-Private Partnerships inHealthcare. The issue highlighted demand drivenintervention for promotion of safe delivery, reductionof maternal and neo-natal mortality. This issue alsofocused on Public-Private partnership for betterhealthcare service in rural areas.
There has been tremendous response to theNewsletter, especially from the grass-root healthworkers from different regions. A number of healthrelated issues, in the form of reader's response havebeen discussed through these Newsletter editions.

122
ANNUAL REPORT 2008-09
7.11 Annual Wall Calendar
This year special efforts were made to design theCalendar on integrated themes with poster value.The Calendar, designed in-house, has come out withinnovative designs highlighting initiative taken onvarious health & family welfare issues. Special effortswere made through visual publicity like this year'sCalendar for spreading message on health issuesas an integrated theme of the Ministry. The Calendarwas circulated to all the health set ups in the country.
7.12 Handbook Diary
Handbook diary with detailed information about theimprovements in different programmes under theNational Rural Health Mission was brought out in ahandy and useful form. Slogans on different healthissues on every page highlight the campaign.Important Health Days have been included in thisHandbook Diary. This would be very useful book forhealth functionaries.
7.13 Mass Mailing Unit (Press)
The Mass Mailing Unit (Direct Mail Communication)whose main objective is to build up an effective mailinglist of the opinion leaders from different parts of thecountry with a view to utilize their services to bringawareness and attitudinal changes among commonpeople. To educate, inform and motivate thesepersons regularly, it has been proposed to bringabout a large number of periodicals and publicationsregularly through direct mailing up to grass root level.
At, Present , Mass Mailing Unit, Deptt. of Health &Family Welfare is disseminating the Ministry's regularJournals NRHM News letters in Engl8ish, Hindi, Oriya,Assamese, Urdu and Tamil quarterly and WallCalenders annually. Apart from this regular dispatch,the Mass Mailing Unit has Mailed various type ofpublicity materials, like posters leaflets, pamphletson Health and Family Welfare Programmes providedby various sections of the Ministry to the HealthFunctioneries all over the country.
123
ANNUAL REPORT 2008-09
Chapter 8
Partnership With Non-Partnership With Non-Partnership With Non-Partnership With Non-Partnership With Non-Government OrganisationsGovernment OrganisationsGovernment OrganisationsGovernment OrganisationsGovernment Organisations
8.1 Introduction
The National Rural Mission (NRHM) seeks to buildgreater ownership of the program among thecommunity through involvement of Non-GovernmentOrganizations. Promotion of Public-PrivatePartnership for achieving public health goals is oneof the strategies initiated by the department in thisregard. This partnership will reinforce the strategyof involvement of NGOs already spelt out in theNational Population Policy 2000.
The Government of India is committed to voluntaryand informed choice in family planning, reproductiveand Child health care services. Towards this end,the Government, the corporate sector, voluntary andnon-voluntary sector are expected to work togetherin partnership. The professional bodies like IndianMedical Association, Federation of Obstetricians &Gynaecologists are also involved in the partnershipto achieve the desired goal.
8.2 Partnership with Non-Government Organizations
The Government of India envisages collaboration withNGOs through enhanced participation by the StateGovernments also. Under RCH-II, the ownership ofthe programme has been decentralized to the StateGovernments. The planning process now starts fromthe district level. The scheme has been included inthe State PIP for NRHM under RCH-II.
NGOs in particular, have been assignedsupplementary or complementary role to that of theGovernment health care delivery, thus aiding themin reaching the masses meaningfully. They have acomparative advantage of flexibility in procedures,rapport building with communities and are at the
cutting edge of programme implementation. NGOswill be involved in ASHA's training, activities relatingto National Disease Control Programmes, PNDT actand service delivery in addition to health educationand awareness programmes.
8.3 New Guidelines
According to the revised guidelines of NGO Scheme,the States have been given an important role inselection/approval of the NGOs and overseeingimplementation of the projects undertaken by them.An inbuilt mechanism of monitoring the working ofthe NGOs and various activities undertaken underthe project, in addition to the mid-term appraisal, etc,by the designated evaluating agencies/organizations, has been built into the guidelines:
The key features are:-
Decentralization of the schemes to the Stateand District level.
Integration with NRHM.
Training of ASHA
Activities relating to various National DiseaseControl Programmes
Awareness relating activities concerningPNDT Act.
Shift from exclusive IEC and awarenessgeneration to Service Delivery.
Delivery of RCH services by NGOs inunserved and under served areas.
Clearly defined eligibility criteria forRegistration, Experience, Assets andJurisdiction.
124
ANNUAL REPORT 2008-09
Rationalization of the jurisdiction
area serviced by the NGO to provide in
depth service and optimize resources.
Mainstreaming gender issues in all
intervention areas.
Enhanced male participation and involvement
in delivery of all RCH services.
Emphasis on measurable, qualitative and
quantitative performance indicators.
Selection, approval, funding and monitoring
of MNGO/SNGO projects by State and District
RCH committees.
Increased interface of NGOs with local
government bodies.
8.4 Service NGO (SNGO) Scheme
The Service NGOs (SNGOs) are, those NGOs, which
are expected to provide clinical service and other
specialized aspects such as Dai training, MTP, male
involvement, covering 100,000 population and
contributing to achieving the RCH objectives.
NGOs with an establishment institutional and
infrastructure for service delivery are encouraged
to compliment the public health care delivery system
in achieving the goals of RCH-II programme. These
SNGOs will cover an area co-terminus to that of a
CHC/block PHC with approximately 1,00,000
population or around 100 villages. Service NGOs are
expected to provide a range of clinical and non-
clinical services, directly to the community, as an
integrated package of RCH-II services. Some of the
services expected to be provided by SNGOs include
safe deliveries, neo-natal care, treatment of
diarrhoea and ARI, abortion and IUD services, RTI/
STI etc.
Currently, 338 MNGOs are working in 450 districts.
MNGO selection process has been completed in the
states/UTs of Gujarat, Chattisgarh, Uttarakhand,
Himachal Pradesh, Maharashtra, Sikkim, Goa, West
Bengal and Orissa. The numbers of MNGOs are likely
to increase steadily to cover the entire country.
Institutional Framework for ProgrammeManagement:
The programme management under the revisedscheme is decentralized to the State and districtAuthorities. The State Govt. forms State RCH Society,which has the responsibility for the overall
management of the scheme. The State NGO
committee will be responsible for MGNO selection,
recommendation of projects for MNGO selection,
recommendation of projects for Government of India
approval, fund disbursement, capacity building,
monitoring and evaluation. The District RCH society
is responsible for all the operational aspects of the
programme management at the district level. The
district NGO committee holds the responsibility for
recommendation of MNGO composite proposals to
State RCH Society, facilitating the signing of MOU
with the MGNO and passes it on for fund release to
state RCH society, undertakes review meetings and
periodic monitoring in the field for assessing FNGO/
MNGO performance.
Role of Government of India is related to provision
of policy guidelines, final approval of proposals, and
technical support for capacity building of NGOs and
fund release to State governments.
8.5 State NGO Coordinators(SNGOCS):
The SNGOCs are responsible for monitoring the
implementation, facilitating timely submission of NGO
reports to the state government, providing
government feed back to NGOs, communicating
government policies and programmes, and facilitating
NGO dialogue with district health system.
At present there are 13 SNGOCs in position and
other states are in active process of positioning
them soon.
8.6 Institutional Framework for NGOCapacity Building
The Regional Resource Centres (RRCs) and the
Best Practice Centres (BPC), are the two institutional
mechanisms available to support this programme.

125
ANNUAL REPORT 2008-09
The RRC pool has expanded to 11 and process has
begun to select 14 more RRCs, to make the
programme more effective. NGOs with expertise and
experience in RCH and having national level stature,are identified as RRCs.
The RRCs are playing role to be a catalyst, advocacyand net working with state governments, strengthen
managerial and technical competencies of theMNGOs, support and oversee FNGO training,document and disseminate best practices, collect anddisseminate RCH policies, laws, and programme fromthe respective states, where they work, andmaintenance of database on technical and humanresources related to RCH.

126
ANNUAL REPORT 2008-09

127
ANNUAL REPORT 2008-09
Chapter 9
9.1 Introduction
The National Family Planning Programme launchedin 1952 was primarily aimed at populationstabilization and the strategy was to regulate birthby providing fertility control methods both for limitingand spacing. The programme is presently beingrepositioned not only to achieve populationstabilization but also to reduce maternal mortality andinfant and child mortality. The birth rate has beenbrought down to 24.8 and TFR to 2.8 due to thesuccessful intervention of this programme. Howeverthere still remains a huge unmet need for familyplanning methods with concomitant interstatevariations. The main reasons for the high unmet needand unwanted fertility are the non availability ofquality services, lack of skilled providers and genderbiased programme with poor male participation.
ICPD in 1994 identified and emphasized therelevance of bringing about population stabilizationby integrating the various health determinants in awholesome manner thereby ensuring populationdevelopment. Another reproductive need to beaddressed is the fertility promotion for the infertilecouples who constitute nearly 10 to 15% of the totalpopulation in India.
The Family Planning Division has formulated manyinterventions for increasing contraceptive choicesand meeting the unmet need in contraception therebyreducing the TFR.:
9.2 Quality Assurance in FamilyPlanning
Quality assurance in family planning services is amajor decisive factor in the acceptance of the service.The guidelines to be followed on Quality care andStandards in FP services in the implementation ofthe national program are provided by the division.
The Quality Assurance Committees set up at theState and District level monitor the sterilisationservices and conduct medical audits and at thecentral level these activities are monitored throughreports and field visits.
Actions and Achievements
Quality Assurance manuals revised andprinted in 2006- 07 ( last edition in 1996)
Manual on Standards for Female and MaleSterilisation revised and printed in 2006-07(last edited 1999)
Six Regional Dissemination Workshops onQuality Assurance on the revised Standardsand QA manuals held countrywide coveringall the states with the objective ofstrengthening the quality in Sterilisationservices.
The reference manual on IUCD for MedicalOfficers has been revised, printed anddistributed countrywide (2007-08).
The reference manual on IUCD for NursingPersonnel has been revised and is in print(2007-08).
A manual on Standard Operating Procedures(SOP) to ensure the quality in camps hasbeen developed for the first time and is inprint.
The manual on Emergency Contraceptive Pillhas been revised and is awaiting printing.
9.3 Repositioning of IUD as a Longand Short Term Spacing Methodin the Family Planning Programme
The acceptance of spacing methods in the countryis still very low in spite of the large unmet need and
Family PlanningFamily PlanningFamily PlanningFamily PlanningFamily Planning
128
ANNUAL REPORT 2008-09
one of the main reasons is lack of skilled manpower.To address this problem an alternative methodologyof training in IUD services using pelvic models hasbeen developed and the pilot phase of thisintervention had been launched in 12 states.
Based on the positive feed back received from thevarious pilot states, the strategy was expanded tocover the rest of the 23 states.
The programme is being administered directly by theGovernment of India and the trainings are beingmonitored diligently from the central level with thehelp of technical consultants.
Actions and Achievements
Three National level training of mastertrainers have been conducted at NIHFW Delhiin collaboration with JPHEIGO and USAID forall the 12 pilot states of the first phase.
Four National level trainings of mastertrainers have been completed for the rest ofthe 35 second phase states with the one forNorth Eastern states held at Guwahati andthe other three held at NIHFW, Delhi.
11 of the 12 first phase states and five ofthe second phase states have completed thestate level master trainers' training.
10 of the states have gone ahead with theirdistrict level training.
More than 3000 medical and paramedicalpersonnel have been trained so far in thestates in a short span of 6 to 8 months
The Government of India has approved theintroduction of a new improved IUD, namely Multiload375 as an added choice to the existing IUD 380 A ina bid to increase the contraceptive choice as well ascontraceptive prevalence in spacing methods.
Actions and Achievements
As approved in the minutes, a protocol isbeing developed by ICMR for a six monthsfast track pilot in some states, medicalcolleges and NGOs to study the operational
problems, requirements for training,acceptability by clients, provider biases,logistical issues as well as possiblemanagerial and programmatic problemsenvisaged in synergizing with the use of theexisting IUD 380 A.
The multiload 375 will be officially launchedonce the results of the trial are favourable
9.4 Male Participation in PlannedParenthood Including No ScalpelVasectomy (NSV)
With the aim to bring men to the forefront inpopulation and reproductive health programmesspecial budgetary provisions have been made in thetenth plan under the Male Participation.
The No Scalpel Vasectomy (NSV), a modified malesterilization technique, was introduced in 1997 in theNFWP as a simple and safe technique with very littlechance of complications compared to femalesterilization.
The camp approach adopted by states like MP, AP,Punjab and UP has shown that a well conceived andintensive advocacy, combined with assured serviceprovision, results in significantly increasedacceptance. Based on the experiences of thesestates, a strategy on advocacy and communitymobilization for increasing NSV acceptance throughcamps has been introduced in the Family PlanningProgramme in 2005. The guidelines have been sentto all states/UT Government.
The camp approach is gradually becoming popularin many districts.The camp approach has since beenrevised with the fund allocation for holding suchcamps being rationalized with the idea of betterconduct of the camps in sterilization services. Thedetailed order is on the website of the Ministry atw w w.mohfw.nic.in under guidelines for familyplanning.
Programmatic shortcomings for promotion ofNSV:
Lack of trained providers (manpower)
Lack of assured service delivery points
129
ANNUAL REPORT 2008-09
Less thrust at the state level
Poor dissemination of the method
Lack of counseling services
Actions and Achievements
Manpower Development: Development of
manpower for service provision is not uniform in all
the states. The well performing states have stepped
up their training of service providers in NSV which is
not seen in the other states. To address this concern,
a three pronged strategy has been developed
namely:
Surgical faculty training: As NSV is overlooked
during under graduate training in Medical Colleges,
a new strategy of hands on training of Surgical
Faculty of the Medical Colleges in NSV has been
started this year so as to involve them in training of
undergraduates and post graduates, which will in turn
help in increasing the pool of trained service
providers. About 200 members of the surgical
faculties of medical colleges have been trained in
52 courses held at 6 designated training centres in
the country during 2007-08. The trainings are going
on in 2008-09, and the data would be compiled at
the end of the financial year.
District Trainers Training: It been taken up at
Maulana Azad Medical College, Delhi to have a
qualitative, uniform training of District Trainers
certified to train Medical Officers in NSV in a
decentralized and faster manner since Jan'06 and
also to attain the goal of having one district trainer
per district for all the 632 districts in the country. 12
District trainers' courses have been held till date
and 6 states - Punjab, Rajasthan, HP, Uttarkhand,
Haryana, Chattisgarh have become self sufficient with
a minimum of one District trainer per district. NSV
providers training at the district level through funds
released from RCH II flexipool is being conducted up
by the various states
A National NSV workshop was conducted to
take stock of the NSV scenario in the country
where 23 states participated and the states
wereapprised on their performance andaccordingly felicited.
The performance in NSV has almost doubledin 2007-08
In six states the performance of NSV to totalsterilization has been more than 10%
In six other states the performance of NSV tototal sterilization has been between 5 - 10%
9.5 Introduction of NewerContraceptives
Introduction of newer contraceptive in the programincreases the basket of choice for eligible couples.
Actions and Achievements
Funds have been released to ICMR for Postmarketing surveillance study in Centchroman,a non steroidal oral contraceptive developedindigenously by CDRI, Lucknow, beforeintroducing it in the National Program.
Study on Cyclofam (one month injectable )and Net En (two monthly injectable ) havebeen completed and presented before theSecretary (Health & Family Welfare)
A 3 year pre introductory study on Net-ENand Cyclofem has been approved by theResearch Advisory Committee to beconducted by ICMR at its HRRCs and MedicalColeges. Prior to introduction in the NationalProgramme.
9.6 Ensuring Availability of FamilyPlanning Services at All Levels ofHealth Care Delivery System
Under NRHM efforts are being made to strengthenCHC, PHCs, Subcentres with infrastructure andhuman resource to IPHS standards. This will alsoensure the provision of various types of terminal andspacing methods of fertility regulation at Govt.institutions. In addition to the governmentfunctionaries ASHA , the accredited social healthactivist, is seen as a major catalyst for bringing about
130
ANNUAL REPORT 2008-09
behavioral change in the community in all mattersrelated to RCH services including contraception
9.7 Revised Compensation Schemefor Acceptors of SterilizationServices
Government of India has been providingcompensation to the acceptors of sterilization for theirloss of wages and giving infra structural support tothe state for providing quality services incontraception.
Actions and Achievements
This scheme has been revised in Sept. '07,taking into consideration the rise in the costof living especially for the BPL/SC/ST familiesas well as the need to promote vasectomymore than tubectomy to address the existinggender inequity.
Funds in the scheme have also beenearmarked for the compensation to the poolof service providers who perform this extrawork in difficult terrain and difficult conditionsin the national interest. The detailed schemeis available on the ministry's website.
The same has contributed handsomely toalmost 10% improvement in sterilizationperformance in the country in 2007-08
9.8 National Family PlanningInsurance Scheme
Government of India launched the National FamilyPlanning Insurance Scheme on Nov 11th 2005 forcompensation to the acceptors of sterilization or his/her nominee in the unlikely event of his/ her death,failure or complications following a sterilizationoperation. The scheme also provides for Indemnityinsurance cover to the Medical officers and thefacilities for up to four cases of litigation per year he/she or the facility may face as a consequence ofperforming sterilization operations.
Actions and Achievements
The Insurance scheme has been renewedwith the ICICI Lombard Insurance company.
The servicing of the claims have improvedsubstantially over last year
A new clause has been added to pay the
family of the bereaved a compensation of
Rs.50,000 immediately from the Rogi Kalyan
Samity funds, to be recouped from the
insurance company once the mandatory
paper works are completed
The detailed scheme is available on theministry's website at www.mohfw.nic.in
9.9 Assisted Reproductive Technolo-gies (ART) for Infertility
As per WHO data the incidence of infertility in various
countries including India is around 10-15%. There
has been an increased demand for assisted
reproduction from these infertile couples. This haslead to mushrooming of infertility clinics in India and
in many of these centres the quality of services is in
question. The National Guidelines on A RT has been
developed by ICMR and National Academy of Medical
Sciences for Government of India for regulating and
supervising the functioning of A RT clinics and thiswould help the A RT clinics in providing safe and
ethical services.
Actions and Achievements
Draft bill on A RT prepared and sent to ICMR
for finalisation.
9.10. Improved Performance in FamilyPlanning in 2007-08
From the absolute figures available it is observedthat sterilization had a marginal increase from 2000-
01 till 2003-04. Thereafter subsequently there was
a drop in sterilization by 4.1% in 2005-06 over
2004-05 and a further drop of 3.8% in 06-07 over
05-06.
The following factors are thought to have contributed
in the gradual fall in the achievements in Family
planning in the past decade
Supreme Court directives on ensuring quality
in Sterilisation services
131
ANNUAL REPORT 2008-09
The mandatory 5 year post degree
experience clause reduced the pool ofservice providers.
Previously many states were allowingMBBS doctors to perform laparoscopicsterilizations which promptly stopped
ISM doctors were also performing mini-lap sterilizations who too were withdrawn.
Medical Officers were reluctant toperform sterilizations in view of increasedawareness on quality among the publicand consequent rising litigations.
Surgeons' apathy
Lack of skilled providers
Withdrawal of payments to the motivatorsfrom the community
The dependence on the camp approach:
Shift away from the focus on Family Planningpost ICPD in Cairo 1994.
9.11 Corrective Actions Taken byGovernment of India forAddressing these Areas ofConcern
The following steps were taken by the Governmentof India to address the concerns of the providersand acceptors alike and the programme in general-
National Family Planning InsuranceScheme since 29.11.05: which covers boththe clients as well as the providers againstany mishaps like deaths, complications andfailures and the ensuing litigations
Orders dated 26th July 2007 ofHon'ble Supreme Court: The orders
relating to 5 years experience criteria werewaived off.
The revision of Compensation packagein Sept.2007 to compensate for loss ofwages.
Promoting Acceptance of No ScalpelVasectomy to ensure male participation.
Promoting IUD 380A intensively as aspacing method because of its longevity of10 years and advantages over other IUDs
Increasing skills of IUD providers throughalternative training strategy in IUD insertionin all the states in the country.
Fixed Day Static Services round the year.
Setting up performance levels (ELA -estimated level of achievement) for States inTerminal and Spacing methods based on localunmet need
Increasing the basket of choice bysystematically and carefully introducing newand effective contraceptives in theprogramme
Holding of workshops, seminars,advocacy meet and frequentinteractions with the states to orient themon the GOI's strategy
As a result of the above measures and the focusedstrategy at the Government of India level with closestate wise monitoring as also the opportunitiesafforded under NRHM in terms of plugging theloopholes and bolstering the demand side financingin the new revised compensation scheme, the deficithas not only been wiped out but has also shown ahealthy 10.99% increase over 06 -07. Performancethis year (07-08) has been 50,12,766 as against in45,48,811 in 06-07.
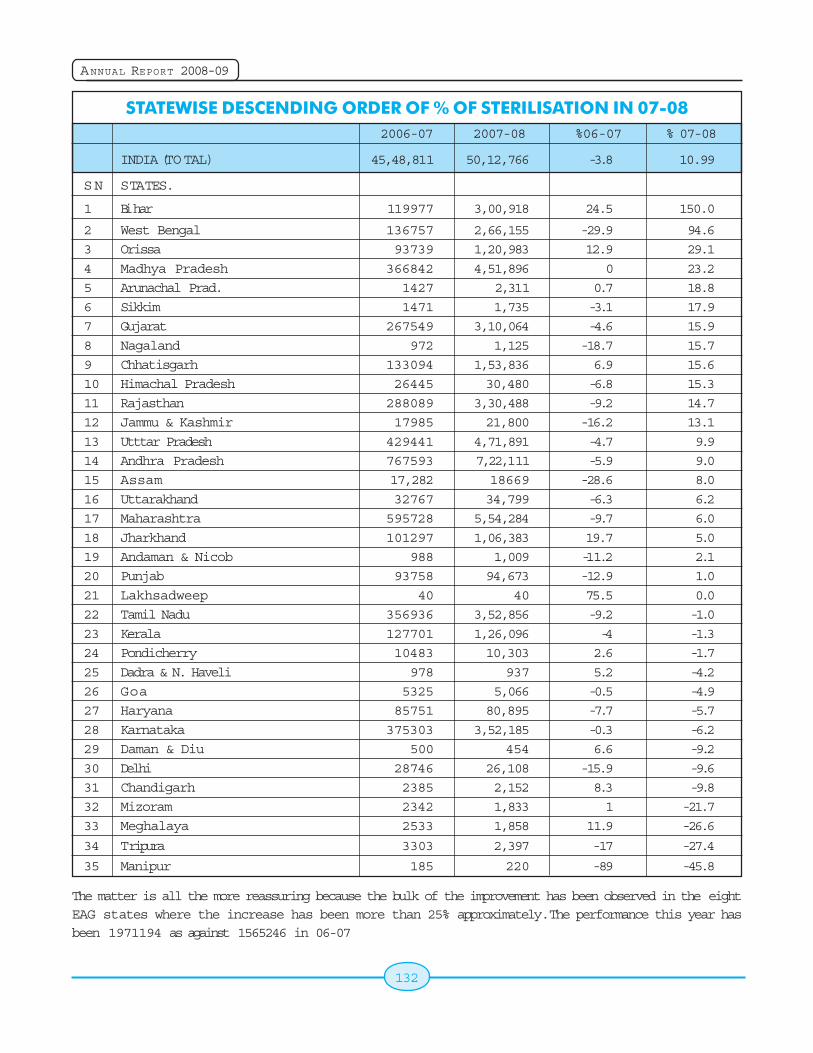
132
ANNUAL REPORT 2008-09
STATEWISE DESCENDING ORDER OF % OF STERILISATION IN 07-082006-07 2007-08 %06-07 % 07-08
INDIA (TOTAL) 45,48,811 50,12,766 -3.8 10.99
SN STATES.
1 Bihar 119977 3,00,918 24.5 150.0
2 West Bengal 136757 2,66,155 -29.9 94.6
3 Orissa 93739 1,20,983 12.9 29.1
4 Madhya Pradesh 366842 4,51,896 0 23.2
5 Arunachal Prad. 1427 2,311 0.7 18.8
6 Sikkim 1471 1,735 -3.1 17.9
7 Gujarat 267549 3,10,064 -4.6 15.9
8 Nagaland 972 1,125 -18.7 15.7
9 Chhatisgarh 133094 1,53,836 6.9 15.6
10 Himachal Pradesh 26445 30,480 -6.8 15.3
11 Rajasthan 288089 3,30,488 -9.2 14.7
12 Jammu & Kashmir 17985 21,800 -16.2 13.1
13 Utttar Pradesh 429441 4,71,891 -4.7 9.9
14 Andhra Pradesh 767593 7,22,111 -5.9 9.0
15 Assam 17,282 18669 -28.6 8.0
16 Uttarakhand 32767 34,799 -6.3 6.2
17 Maharashtra 595728 5,54,284 -9.7 6.0
18 Jharkhand 101297 1,06,383 19.7 5.0
19 Andaman & Nicob 988 1,009 -11.2 2.1
20 Punjab 93758 94,673 -12.9 1.0
21 Lakhsadweep 40 40 75.5 0.0
22 Tamil Nadu 356936 3,52,856 -9.2 -1.0
23 Kerala 127701 1,26,096 -4 -1.3
24 Pondicherry 10483 10,303 2.6 -1.7
25 Dadra & N. Haveli 978 937 5.2 -4.2
26 Goa 5325 5,066 -0.5 -4.9
27 Haryana 85751 80,895 -7.7 -5.7
28 Karnataka 375303 3,52,185 -0.3 -6.2
29 Daman & Diu 500 454 6.6 -9.2
30 Delhi 28746 26,108 -15.9 -9.6
31 Chandigarh 2385 2,152 8.3 -9.8
32 Mizoram 2342 1,833 1 -21.7
33 Meghalaya 2533 1,858 11.9 -26.6
34 Tripura 3303 2,397 -17 -27.4
35 Manipur 185 220 -89 -45.8
The matter is all the more reassuring because the bulk of the improvement has been observed in the eightEAG states where the increase has been more than 25% approximately. The performance this year hasbeen 1971194 as against 1565246 in 06-07
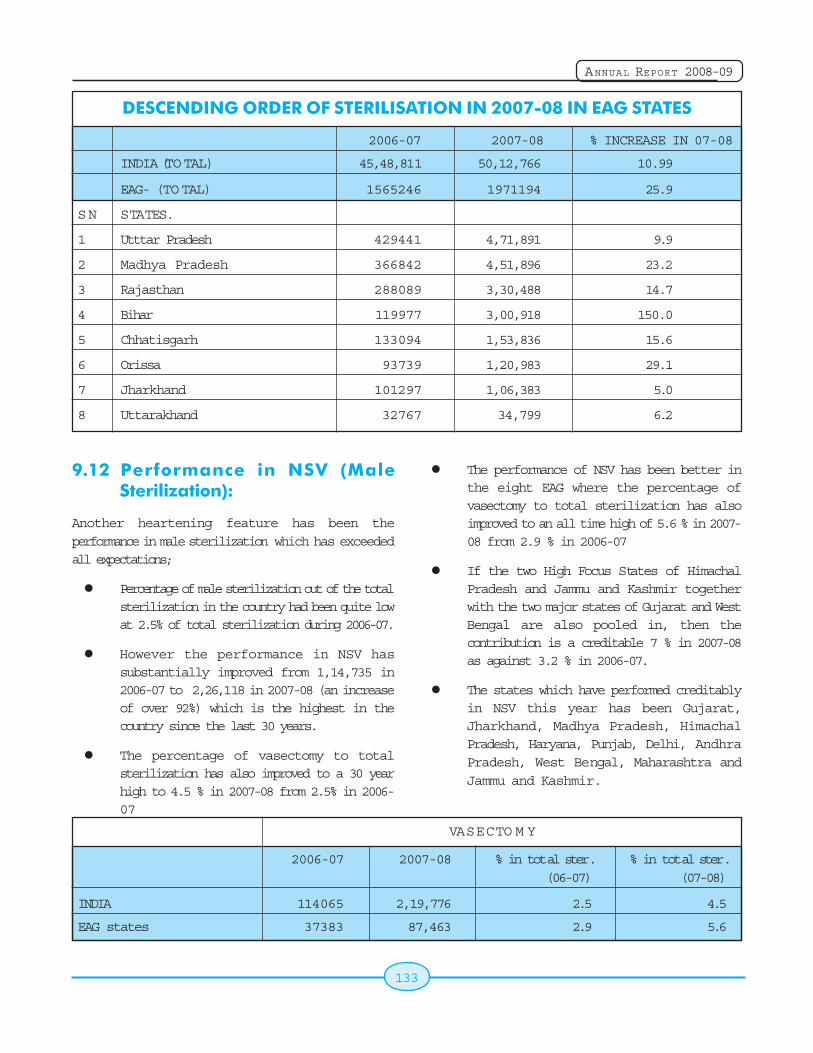
133
ANNUAL REPORT 2008-09
9.12 Performance in NSV (MaleSterilization):
Another heartening feature has been theperformance in male sterilization which has exceededall expectations;
Percentage of male sterilization out of the totalsterilization in the country had been quite lowat 2.5% of total sterilization during 2006-07.
However the performance in NSV hassubstantially improved from 1,14,735 in2006-07 to 2,26,118 in 2007-08 (an increaseof over 92%) which is the highest in thecountry since the last 30 years.
The percentage of vasectomy to totalsterilization has also improved to a 30 yearhigh to 4.5 % in 2007-08 from 2.5% in 2006-07
The performance of NSV has been better inthe eight EAG where the percentage ofvasectomy to total sterilization has alsoimproved to an all time high of 5.6 % in 2007-08 from 2.9 % in 2006-07
If the two High Focus States of HimachalPradesh and Jammu and Kashmir togetherwith the two major states of Gujarat and WestBengal are also pooled in, then thecontribution is a creditable 7 % in 2007-08as against 3.2 % in 2006-07.
The states which have performed creditablyin NSV this year has been Gujarat,Jharkhand, Madhya Pradesh, HimachalPradesh, Haryana, Punjab, Delhi, AndhraPradesh, West Bengal, Maharashtra andJammu and Kashmir.
DESCENDING ORDER OF STERILISATION IN 2007-08 IN EAG STATES
2006-07 2007-08 % INCREASE IN 07-08
INDIA (TOTAL) 45,48,811 50,12,766 10.99
EAG- (TO TAL) 1565246 1971194 25.9
SN STATES.
1 Utttar Pradesh 429441 4,71,891 9.9
2 Madhya Pradesh 366842 4,51,896 23.2
3 Rajasthan 288089 3,30,488 14.7
4 Bihar 119977 3,00,918 150.0
5 Chhatisgarh 133094 1,53,836 15.6
6 Orissa 93739 1,20,983 29.1
7 Jharkhand 101297 1,06,383 5.0
8 Uttarakhand 32767 34,799 6.2
VASECTO M Y
2006-07 2007-08 % in total ster. % in total ster.(06-07) (07-08)
INDIA 114065 2,19,776 2.5 4.5
EAG states 37383 87,463 2.9 5.6
134
ANNUAL REPORT 2008-09
The data also reflects that in 18 out of the 29 statesin the country, there has been a perceptible shift in
focus on male sterilization. Many reasons have been
put forth for this. However the main reason identified
is the emphasis given by the state government to
the programme. The brightest examples are the
states of Gujarat, Jharkhand and West Bengal.
9.13 Factors Responsible for theUpsurge in Sterilization Services
Frequent monitoring of the programme
through telephones and email
Emphasizing the GOI’s state specific
strategy of servicing the local unmet need
at all the forum of interactions with the states
like state JRMs, RCH review, NRHM review
and NPCC sub group and final meetings.
Frequent state tours to attend CMOs’
meetings to make presentations on the
family planning strategy of the GOI in the
focus states and undertake field visits to
clarify doubts about various aspects of the
programme.
The revised compensation scheme,
considering that 80% of the operations have
been conducted since September 2007 when
the new scheme was operationalised.
Prompt payment to the acceptors at most
places for their loss of wages to undergo the
surgery. This has empowered them to avail
of the services,
Graded payment to the service
providers has been one of the force
multipliers. The providers are no more a
disgruntled lot as their concerns are being
addressed.
Systematic manpower development plan from
the central level especially in NSV.
Unfortunately the uptake in IUD services has not
picked up as much as the sterilization services.
However the decline of 8% in the last year has been
stalled and the graph has shown a 2 % rise this year
(07-08).
With the new alternative training strategy in IUD
services being piloted in all the states and concrete
plans in place for rolling out in the remaining states
in the country by August this year, the much needed
boost in spacing methods would be injected in the
programme at the central level and the states are
expected to follow suit. With the implementation of
this strategy it is hoped the IUD uptake would rise in
the near future.
9.14 Future Strategies to Maintain theMomentum
Moreover the ministry has also set in motion new
approaches to sustain the momentum gained in the
sphere of population stabilization this year, some of
which are as follows:
Organizing six regional dissemination
workshops countrywide shortly in 2007-08
to orient the states on the comprehensive
family planning strategy of the Government
of India.
Statewide dissemination of advocacy
material developed by the ministry in
collaboration with experts in the field,
comprising audio, video and print materials
which have of late has been conspicuous by
its absence in the whole country.
Rolling out the comprehensive training
plan for development of trained manpower
in family planning services which has been
an area of concern for quite some time now.
Ensuring the fixed day static services
round the year for delivery of family planning
services through increasing the service
centres as well as the pool of trained
manpower
Increasing the basket of choices in
contraceptives offering more options to the
clients.

135
ANNUAL REPORT 2008-09
Repositioning the Family Planning
Programme not just for achieving population
stabilization but also substantially reducing
the maternal mortality and infant and child
mortality and morbidity.
As regards sterilization services the all round
improvement seen in the programme both in terms
of service delivery as well as manpower
development, it is hoped that the performance in
08-09 improves further over 07-08 and especially
NSV will regain its preeminent position in sterilization
services in the near future with the men shouldering
the responsibility of family planning and rectifying
the gender inequity prevalent in the society hitherto,
and family planning becomes a way of life with the
people of the country.

136
ANNUAL REPORT 2008-09

137
ANNUAL REPORT 2008-09
Chapter 10
10.1 Introduction
Availability of qualitative services to the community
depends largely upon the efficacy with which health
functionaries discharge their responsibilities, which,
in turn would depend mainly upon their education
and training. Department of Family Welfare had
recognized the crucial role of training of health
personnel in providing effective and efficient health
care to the rural community from the very beginning
of the Five Year Plans. The pre-service and in-
service training for different categories of health
personnel are imparted through the following
schemes/activities:
10.2 ASHA Under NRHM
The Government of India in April 2005 has launched
the NRHM to improve access of people, especially
the poor women and children to quality primary health
care services. Accredited Social Health Activist
(ASHA) is a major strategic intervention under the
mission. Initially the scheme was for the 10 high focus
States namely, Uttar Pradesh, Uttaranchal, Bihar,
Jharkhand, Madhya Pradesh, Chhattisgarh, Orissa,
Rajasthan, Assam and Jammu & Kashmir. Later on it
has been extended to NE states and tribal areas of
other states.
ASHA is envisaged as a trained women community
health volunteer who will reinforce community action
for universal immunization, safe delivery, new born
care, prevention of water borne and communicable
disease, improved nutrition and promotion of
household toilets. She will inform, interact, mobilize
and facilitate improved access to preventive and
promotive health care and also provide basic curative
care through her drug kits. She will assist informulation of village health plan by the village healthand sanitation committee. There will be one ASHAper 1000 population. In tribal, hilly, desert areas,their norm could be relaxed to one ASHA perhabitation, depending on workload etc.ASHA mustbe primarily a woman resident of the village - married/ widow/ divorced, literate with formal education upto class VIIIth and preferably in the age group of 25to 45 years. This may be relaxed only if suitableperson with this qualification is not available.
Training and Selection of ASHA
It was envisaged that selection and training processof ASHA will be given due attention by the concernedState to ensure that at least 50% trained ASHAs arein place by 2007 and 100% by 2008. ASHAs are tobe selected by the community, from among theresidents within the community. She is to work in closecoordination with AWW and ANM and these will beintegrating in their roles with use of common resourcefacilities like AWW centres etc. Capacity building ofASHA is critical in enhancing her effectiveness andthis has been seen as a continuous process. Theinduction training of ASHA would be completed in 23days spread in five rounds over a period of 12 monthsto be followed by periodic re-training for about twodays once every alternate month. For the trainingof ASHA, four training modules based on thematicapproach have been developed. These have alreadybeen disseminated to the states. The States have
translated the training modules in the local language
for use in the training of ASHAs. Progress made in
selection and training of ASHAs (as on 27.2.09)
given in following on next page: -
Training ProgrammeTraining ProgrammeTraining ProgrammeTraining ProgrammeTraining Programme
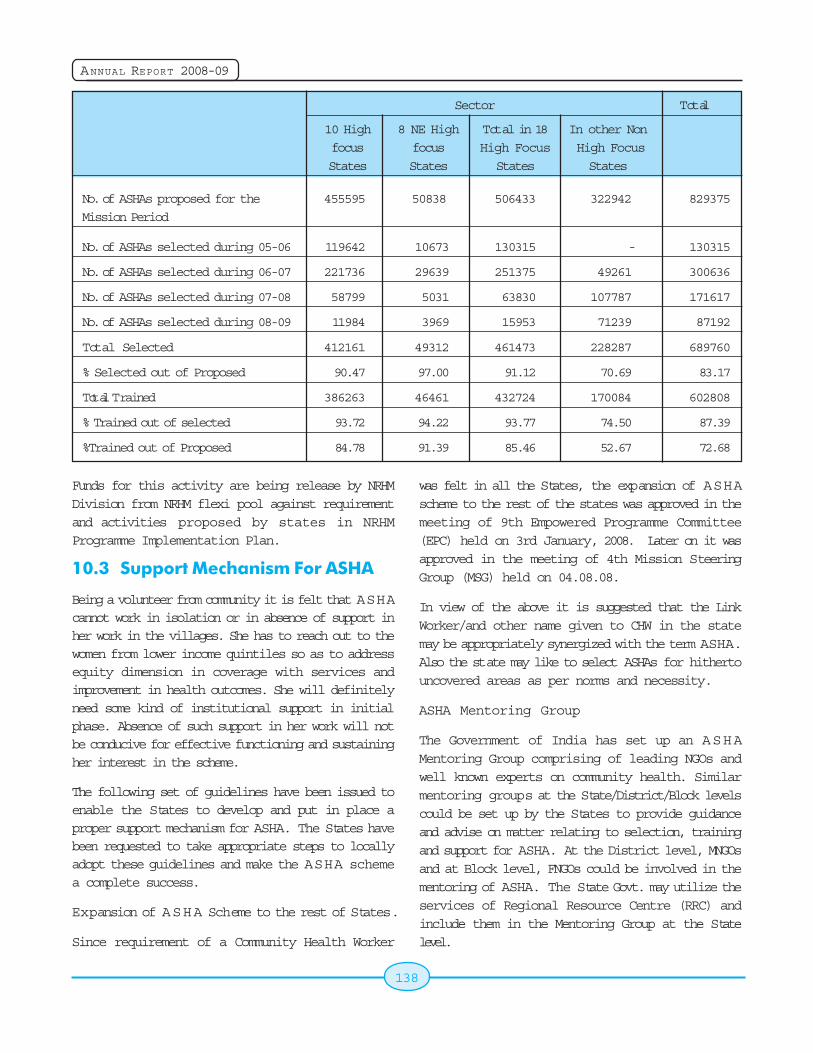
138
ANNUAL REPORT 2008-09
Sector Total
10 High 8 NE High Total in 18 In other Non
focus focus High Focus High Focus
States States States States
No. of ASHAs proposed for the 455595 50838 506433 322942 829375
Mission Period
No. of ASHAs selected during 05-06 119642 10673 130315 - 130315
No. of ASHAs selected during 06-07 221736 29639 251375 49261 300636
No. of ASHAs selected during 07-08 58799 5031 63830 107787 171617
No. of ASHAs selected during 08-09 11984 3969 15953 71239 87192
Total Selected 412161 49312 461473 228287 689760
% Selected out of Proposed 90.47 97.00 91.12 70.69 83.17
Total Trained 386263 46461 432724 170084 602808
% Trained out of selected 93.72 94.22 93.77 74.50 87.39
%Trained out of Proposed 84.78 91.39 85.46 52.67 72.68
Funds for this activity are being release by NRHMDivision from NRHM flexi pool against requirementand activities proposed by states in NRHMProgramme Implementation Plan.
10.3 Support Mechanism For ASHA
Being a volunteer from community it is felt that ASHAcannot work in isolation or in absence of support inher work in the villages. She has to reach out to thewomen from lower income quintiles so as to addressequity dimension in coverage with services andimprovement in health outcomes. She will definitelyneed some kind of institutional support in initialphase. Absence of such support in her work will notbe conducive for effective functioning and sustainingher interest in the scheme.
The following set of guidelines have been issued toenable the States to develop and put in place aproper support mechanism for ASHA. The States havebeen requested to take appropriate steps to locallyadopt these guidelines and make the ASHA schemea complete success.
Expansion of ASHA Scheme to the rest of States.
Since requirement of a Community Health Worker
was felt in all the States, the expansion of ASHAscheme to the rest of the states was approved in themeeting of 9th Empowered Programme Committee(EPC) held on 3rd January, 2008. Later on it wasapproved in the meeting of 4th Mission SteeringGroup (MSG) held on 04.08.08.
In view of the above it is suggested that the LinkWorker/and other name given to CHW in the statemay be appropriately synergized with the term ASHA.Also the state may like to select ASHAs for hithertouncovered areas as per norms and necessity.
ASHA Mentoring Group
The Government of India has set up an ASHAMentoring Group comprising of leading NGOs andwell known experts on community health. Similarmentoring groups at the State/District/Block levelscould be set up by the States to provide guidanceand advise on matter relating to selection, trainingand support for ASHA. At the District level, MNGOsand at Block level, FNGOs could be involved in thementoring of ASHA. The State Govt. may utilize theservices of Regional Resource Centre (RRC) andinclude them in the Mentoring Group at the Statelevel.

139
ANNUAL REPORT 2008-09
Selection of ASHA
As ASHA will be in the village on a permanent basis,she should be selected carefully through the processlaid down in the first set of ASHA guidelines. It ispossible that the selected ASHA drops out of theprogramme. It is, therefore, necessary to keep arecord of such cases at Subcentre/ PHC level. In theabove circumstance, a new ASHA could be selectedfrom the panel of three names previously preparedon the recommendation of the Gram Sabha.
Training of ASHA
The guidelines already issued on ASHA envisage atotal period of 23 days training in five episodes.However, it is clarified that ASHA training is a continuousone and that she will develop the necessary skills &expertise through continuous on the job training. Aftera period of 6 months of her functioning in the village itis proposed that she be sensitized on HIV / AIDS issuesincluding STI, RTI, prevention and referrals and alsotrained on new born care.
Training for the 5th Module
To further strengthen the activist role of the ASHA,the 5th Module for Training of ASHAs has beendeveloped by Chetna, an NGO. It has already beenplaced before the ASHA Mentoring Group at thenational level. Given the contents of the 5th module,a lot of the emphasis is on the self actualization ofthe ASHA as the community activist. The NRHMFramework for Implementation has already providedfor setting up of grants in aid committee at the Statelevel to process proposals of NGOs. A network ofNGOs is also available through the NGO Division ofthe Ministry of Health and Family Welfare with RRCsMNGOs, FNGOs etc. at various levels. Theorganization which has prepared the module has alsoaccepted the responsibility for training of mastertrainers who can then rollout the 5th module in thefield. The National Health System Resource Centre(NHSCR) which is now the Secretariat for the ASHAMentoring Group at the national level is also willing,to facilitate the rollout of the 5th module with the activeinvolvement of the NGOs in the States under the overall direction and supervision of State/UTGovernments.
Familiarizing ASHA with the village
After the selection of ASHA, the next step would beto familiarize her with the health status of the villagers
and facilitate her adoption to the village conditions.
Although, ASHA hails from the same village, she may
not be having knowledge and information on the
health status of the village population. For this
purpose, she should be advised to visit every
household and make a sample survey of the
residents of village to understand their health status.
This way she will come to know the villagers, the
common diseases which are prevalent amongst the
villagers, the number of pregnant women, the number
of newborn, educational and socio economic status
of different categories of people, the health status
of weaker sections especially scheduled castes/
scheduled tribes etc. She can be provided a simple
format for conducting the surveys. In this the AW W
and the Village Health & Sanitation Committee should
support her.
The Gram Panchayat will be involved in supporting
ASHAs in her work. All ASHAs will be involved in this
Village Health and Sanitation Committee of the
Panchayat either as members or as special invitees
(depending on the practice adopted by the State).
ASHAs may coordinate with Gram Panchayats in
developing the village health plan. The untied funds
placed with the Sub-Centre or the Panchayat may
be used for this purpose. At the village level, it is
recognized that ASHA cannot function without
support. The SHGs, Woman's Health Committees',
Village Health and Sanitation Committees' of the
Gram Panchayat will be major sources of support to
ASHA. The Panchayat members will ensure secure
and congenial environment for enabling ASHAs to
function effectively to achieve the desired goal.
Maintenance of Village Health Register
A village health register is maintained by the AW W,
which is not always complete. ASHA can help AW W
to complete and update this register by maintaining
a daily diary. The diaries, registers, health cards,
immunization cards may be provided to her from theuntied funds made available to the Sub-Centres.
140
ANNUAL REPORT 2008-09
Organization of the Village Health and NutritionDay
All State Governments are presently organizingmonthly Health and Nutrition day in every village(Anganwadi centers) with the help of AWW/ANM.ASHA along with AWW should mobilize women,children and vulnerable population for the monthlyhealth day activities like immunization, carefulassessment of nutritional status of pregnant/lactatingwomen, newborn & children, ANC/PNC and otherhealth check-ups of women and children, takingweight of babies and pregnant women etc. and allrange of other health activities. The ANM and theAWW will guide the ASHA during the monthly healthdays. The organization of the monthly Health andNutrition Days ought to be jointly monitored by theCDPO, LHVs, and the Block Supervisor of the ICDSperiodically.
Co-ordination with SHG Groups
ASHA would be required to interact with SHG Groups,if available in the villages, along with AW W, so that awork force of women will be available in all the villages.They could jointly organize check up of pregnantwomen, their transportation for safe institutionaldelivery to a pre-identified functional health facility.They could also think of organizing health insuranceat the local level for which the Medical Officer andothers could provide necessary technical assistance.
Meeting with A N M
ANM should have a monthly meeting with the ASHAsstationed (5-6 ASHAs) in the villages of her work areaat the Anganwadi Centre during the monthly Healthand Nutrition Day to assess the quality of their workand provide them guidance.
Monthly meetings at PHC level
The Medical Officer In-charge of the PHC will hold amonthly meeting which would be attended by A N Mand ASHAs, LHVs and Block Facilitator. During thisperiod, the health status of the villages will becarefully reviewed. Payment of incentive to ASHAsunder various schemes could be organized on thatday so that ASHA need not visit the PHC many times
to receive her incentives. States may ensure thatpayments to ASHAs are made promptly through asimplified procedure. During these meetings, thesupport received from the Village Health andSanitation Committee and their involvement in allactivities also should be carefully assessed. TheASHA kits also could be replenished at that time.Replenishment of kit should be prompt, automaticand through a simplified procedure.
Monthly meetings of ASHAs
A meeting of ASHA could be organized on the daymonthly meetings are organized at the PHC level toavoid unnecessary travel expenditure and wastageof time. The idea is that apart from the meeting withofficials they should be given opportunity to sharesometime of their own experience, problems, etc.They will also get an opportunity to independentlyassess the health system and can bring about muchneeded changes.
In addition to monthly meetings at PHC, periodicretraining of ASHAs may be held for two days oncein every alternate month where interactive sessionswill be held to help then to refresh and upgrade theirknowledge and skills, as provided for in the originalguidelines for ASHA.
Block level management
At the block level, the BMO will be in overall chargeof ASHA related activities. However, an officer will bedesignated as Block level organizer for the ASHA tobe assisted by Block Facilitators (one for every 10ASHAs). Block Facilitators could be appointed asprovided for under the first set of guidelines on ASHAalready issued to the States. The Block Facilitatormust necessarily be women. However, male membersif any, who may have already been appointed earlieras Block Facilitator may continue. The BlockFacilitators would provide feedback on thefunctioning of ASHAs to the BMO & Block levelorganizers. They shall also visit the ASHAS in villages.
Management Support for ASHA
Officials in the ICDS should be fully involved in ASHAsactivities and their support should be provided for at
141
ANNUAL REPORT 2008-09
every level i.e. PHCs, CHCs, District Society etc. Themanagement support which would be provided underRCH/NRHM at the Block, District & State level shouldbe fully utilized in creating a network for support toASHA including timely disbursement of incentives, atvarious levels.This support system should have fullinformation on the number of ASHAs, quality of theirout put, outcomes of the Village Health and NutritionDay, periodic health surveys of the villages to assessher impact on community etc.
Community monitoring
Periodic surveys are envisaged under NRHM in everyvillage to assess the improvement brought about byASHA and other interventions. The funding for thesurvey will be provided out of the untied fundsprovided to the Sub-Centre. The first survey wouldprovide the base line for monitoring the impact ofhealth activities in the village.
Role of District Health Missions:
The District Health Mission in its meetings will speciallyassess the progress of selection of ASHAs, theirtraining and orientation, usefulness to the villagesetc. They should also have a Cell in the DPU to collectall information related to ASHA and the community,which should be available on the computer network.This information should be accessible by the StateHealth Missions as well as the Mission at the nationallevel.
Linkages with Health Facility
The success of NRHM to great extent depends onperformance of ASHA and her linkage with functionalhealth system. The health system has to give duerecognition to ASHA and take prompt action on thereferrals made by her; otherwise the system cannotbe sustained. Every ASHA must be familiar with theidentified functional health facility in the respectivearea where she can refer or escort the patients forspecific services. The persons manning these healthfacilities should be sensitized to effectively respondto the instant needs of the local people. Fundsavailable under IEC programme may be used foreducation and publicity in respect of above services.The role of the State & District level Missions would
be to provide support to ASHA from village to thedistrict level without any blockage on the way.
Funding Norms
Under the present funding norms Rs. 10000/- perASHA are available out of which Rs. 6415/- areearmarked for selection process, training of ASHA,training of trainers, drug kit. Remaining part of Rs.3585/- can be used by State Govt. for ASHA supportsystem which includes funding support for ASHAresource center, programme management unit atdistrict health society, at block level and at PHC level.
Compensation to ASHA
ASHA is an honorary volunteer and would not receiveany salary or honorarium. Her work would be sotailored that it does not interfere with her normallivelihood.
However ASHA could be compensated for her timein the following situations:
i. For the duration of her training both in termsof TA and DA. (So that her loss of livelihoodfor those days is partly compensated)
ii. For participating in the monthly/bi-monthlytraining, as the case may be. (For situations(i) and (ii), payment will be made at the venueof the training when ASHAs come for regulartraining sessions and meetings).
iii. Wherever compensation has been providedfor under different national programmes forundertaking specific health or other socialsector programmes with measurable outputs,such tasks should be assigned to ASHAs onpriority (i.e. before it is offered to other villagevolunteers) wherever they are in position.(For situation iii. Disbursement ofcompensation to ASHAs will be made as perthe specific payment mechanism built intoindividual programmes).
Other than the above specific programmes, a numberof key health related activities and service outcomesare aimed within a village (For example all eligiblechildren immunized, all newborns weighed, all
142
ANNUAL REPORT 2008-09
pregnant women attended an antenatal clinic etc).The Untied Fund of Rs.10,000/- at the Sub-Centerlevel (to be jointly operated by the ANM and theSarpanch) could be used as monetary compensationto ASHA for achieving these key processes. Theexact package of processes that form the packagewould be determined at the state level dependingon the supply - side constraints and what is feasibleto achieve within the specified time period) forsituation iv. The payment to ASHAs will be made atPanchayats).
It has been felt that a wider range of public healthfunctions be brought under the performance basedpayment arrangements for ASHAs. An illustrative listof such public health functions is as follows:
I. Organizing Village health & Nutrition Day.
II. Making a series of five family visits in the firstmonth of life of which one visits is in the firsttwo hours-for home based newborn care andearly detection of sickness in the neonate.
III. Maintaining and updating a village healthregister that could be used in village healthplanning and promotion of completeregistration of births and deaths.
As regards the delayed performance basedpayments, the current arrangement is to provide thispayment under the approved programmes ofgovernment. While efforts have been made toensure timeliness of such payments, the States mayconsider, if feasible(if account could be maintainedand expenditure reported periodically), creating apermanent advance of Rs.5000/- at the level of thesub centre head in the joint account of ANM andSarpanch to facilitate performance based paymentsfor activities which are not covered under existingapproved programmes. The Gram Panchayat shallmake the decision for payment based on the prioritiesand the approved norms for the specific region. Theprovision for a permanent advance at the Sub centrerlevel has been provided in the Framework forImplementation of NRHM State Governments, maylike to operationalize this to facilitate both thetimeliness of payments as also the wider range ofperformance based arrangement that will meet
region specific health channels. While Submittingtheir PIPs, the States will have to provide completedetails of activities for which performance basedpayments will be admissible to the ASHAs. Thepayment arrangements from programme funds mustbe taken into account before determining the activitiesfor which the Gram Panchayat shall provide paymentsto entire that there is no duplication or delay.
States to decide in the context of their needs toensure that the Accredited Social Health Activistsremains a community worker accountable to localcommunity institutions like the village Health andSanitation Committee. This is being emphasized toretain the character of the ASHA worker as a memberof the community rather that the last rung in thehealth bureaucracy.
10.4 NHSRC Support for StrengtheningCommunity Process Under NRHM
1. Drafting out 'Terms of Reference' foreffectively functional 'ASHA Resource Center'or 'Community Process Resource Center' forsetting up of support structures at the State,districts and block levels of programmefacilitation - Draft TOR and work plan is readyfor States of Uttarakhand, Orissa, MadhyaPradesh, Rajasthan and Jharkhand. This isfinalized for Orissa which is presently underimplementation. In case of other states thework plan is approved incrementally.
2. Capacity building of State 'ASHA ResourceCentres' in setting up 'Support Structures'and Training of District level and Block levelsupport team on 'Community Processes'-
Processes initiated for the 'Communityprocesses Resource Center' in Orissa(Recruitment and Training of DistrictCoordinators completed)
Processes of recruitment of Districtcoordinators initiated in Jharkhand
Madhya Pradesh, Rajasthan the processof District Coordinators deployment is yetto begin
143
ANNUAL REPORT 2008-09
Deployment of Block level facilitatorscovering 50% of districts in MadhyaPradesh is completed - orientation planis in place
Orientation on PIP review and input torevision of 'Annual work Plan' relating to'Community Processes' is initiated
Assisted State of UP for the recruitmentof District ASHA Coordinators - forimplementation support to ASHA Scheme
3. Establishing and operationalising guidelineson 'periodic review and supportivesupervision' for effective monitoring ofCommunity Processes - ASHA & VHSCs andinvolvement of PRIs and NGOs - FacilitatorsManual for ' Community Processes' is madeavailable in all these states where NHSRCState Facilitators are in Place.
4. Handholding of district support mechanism,reporting & documentation on state specificstrategies, facilitation of support system atthe state level in coordinating Department ofHealth, Mission Directorate and NHSRC fortechnical assistance - Ongoing activity.
5. Secretariat for the 'ASHA Mentoring Group'in organization and coordination of Statelevel AMG for optimizing NGO involvement inCommunity Processes-Facilitation of threeNational AMG consultations including oneRegional AMG Consultation for the NE statesalong with state level AMG consultation forstates of Rajasthan, Orissa, Jharkhand andMadhya Pradesh in initiated.
6. Mobilizing NGO involvement throughGovernment-NGO cooperation in organizationof TOT for Module V in respective state leveland rolling out of ASHA training at block levelinvolving Mother NGOs/Field NGOs/RRCsand NHSRC - initiated in the states ofUttarakhand, Assam for the master trainerstraining on Module V. This will follow similarexercise for the states of Jharkhand, Orissaand Madhya Pradesh in the same order.
Dialogue initiated with state of UP fororganizing master trainers training on ModuleV in four different zones in the state.
7. Conducting Assessments of 'State specificinnovations for initiating mid-coursecorrections' and suggesting states for scalingup of best practice problem solving strategieson 'Sustaining Community Processes underNRHM' - An ongoing supportive supervisionexercise is carried out bi-monthly by reviewingState Facilitator's performance, status ofASHA implementation support, revised workplan for the subsequent period specific toconcerned state. This is mostly facilitatedjointly with the Training Division, MOHFW,GOI. This is communicated to NRHM, MissionDirector through NHSRC State Facilitators'in these States along with Training Division& ED, NHSRC on a regular basis.
10.5 Centrally Sponsored Scheme of"Basic Training of ANM/LHV"
ANMs/LHVs play a vital role in MCH and FamilyWelfare Service in the rural areas. It is therefore,essential that the proper training to be given to themso that quality services be provided to the ruralpopulation.
For this purpose 318 ANM/Multipurpose HealthWorker (Female) schools with an admission capacityof approximately 13,000 & 42 promotional trainingschools for LHV/ Health Assistant (Female) with anadmission capacity of 2600.
These training institutions are imparting pre-servicetraining to prepare required number of ANMs andLHVs to man the Sub centres, Primary HealthCentres, Community Health Centres, Rural FamilyW elfare Centres and Health posts in the country. Theduration of training programme of ANM is one andhalf years and minimum admission requirement forthis course is 10th pass. Senior ANM with five yearsof experience is given six months promotional trainingto become LHV/ Health Assistant (Female). HealthAssistant(Female) provides supportive supervisionand technical guidance to the ANMs in sub-centres.Curricula of these training courses are provided bythe Indian Nursing Council.
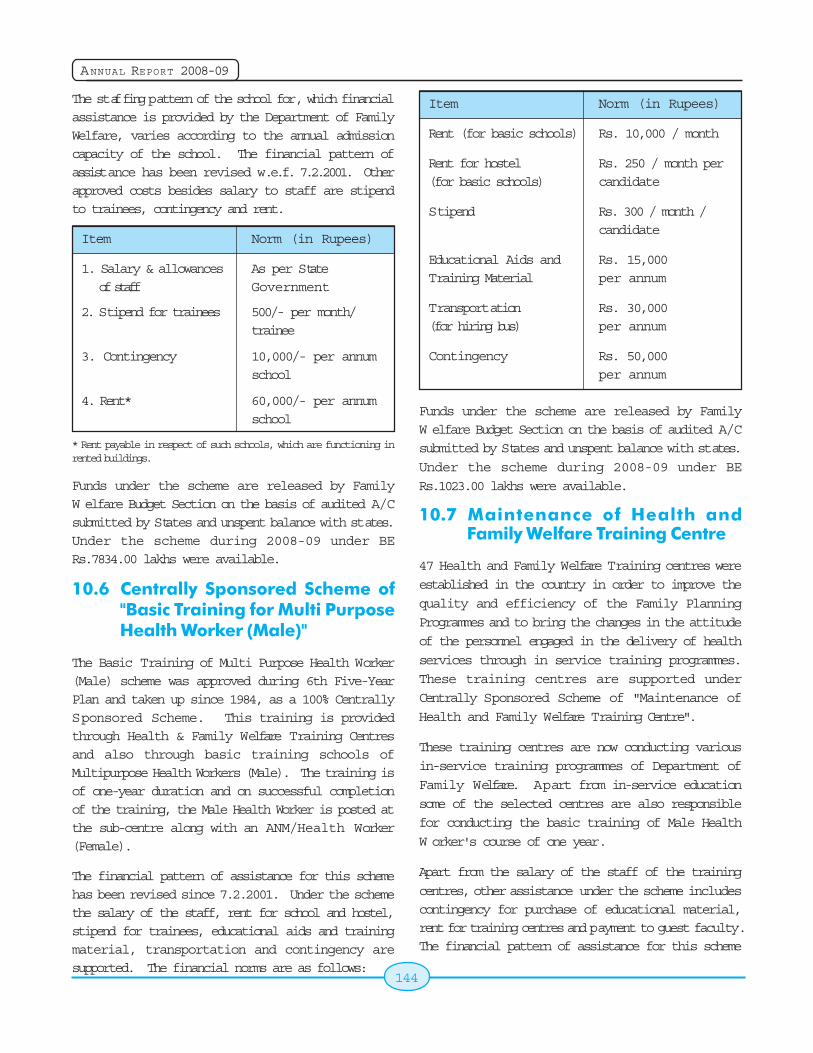
144
ANNUAL REPORT 2008-09
The staffing pattern of the school for, which financialassistance is provided by the Department of FamilyWelfare, varies according to the annual admissioncapacity of the school. The financial pattern ofassistance has been revised w.e.f. 7.2.2001. Otherapproved costs besides salary to staff are stipendto trainees, contingency and rent.
Item Norm (in Rupees)
1. Salary & allowances As per Stateof staff Government
2. Stipend for trainees 500/- per month/trainee
3. Contingency 10,000/- per annumschool
4. Rent* 60,000/- per annumschool
* Rent payable in respect of such schools, which are functioning inrented buildings.
Funds under the scheme are released by FamilyW elfare Budget Section on the basis of audited A/Csubmitted by States and unspent balance with states.Under the scheme during 2008-09 under BERs.7834.00 lakhs were available.
10.6 Centrally Sponsored Scheme of"Basic Training for Multi PurposeHealth Worker (Male)"
The Basic Training of Multi Purpose Health Worker(Male) scheme was approved during 6th Five-YearPlan and taken up since 1984, as a 100% CentrallySponsored Scheme. This training is providedthrough Health & Family Welfare Training Centresand also through basic training schools ofMultipurpose Health Workers (Male). The training isof one-year duration and on successful completionof the training, the Male Health Worker is posted atthe sub-centre along with an ANM/Health Worker(Female).
The financial pattern of assistance for this schemehas been revised since 7.2.2001. Under the schemethe salary of the staff, rent for school and hostel,stipend for trainees, educational aids and trainingmaterial, transportation and contingency aresupported. The financial norms are as follows:
Item Norm (in Rupees)
Rent (for basic schools) Rs. 10,000 / month
Rent for hostel Rs. 250 / month per(for basic schools) candidate
Stipend Rs. 300 / month /candidate
Educational Aids and Rs. 15,000Training Material per annum
Transportation Rs. 30,000(for hiring bus) per annum
Contingency Rs. 50,000per annum
Funds under the scheme are released by FamilyW elfare Budget Section on the basis of audited A/C
submitted by States and unspent balance with states.
Under the scheme during 2008-09 under BE
Rs.1023.00 lakhs were available.
10.7 Maintenance of Health andFamily Welfare Training Centre
47 Health and Family Welfare Training centres were
established in the country in order to improve the
quality and efficiency of the Family Planning
Programmes and to bring the changes in the attitude
of the personnel engaged in the delivery of health
services through in service training programmes.
These training centres are supported under
Centrally Sponsored Scheme of "Maintenance of
Health and Family Welfare Training Centre".
These training centres are now conducting various
in-service training programmes of Department of
Family Welfare. Apart from in-service education
some of the selected centres are also responsible
for conducting the basic training of Male Health
W orker's course of one year.
Apart from the salary of the staff of the training
centres, other assistance under the scheme includes
contingency for purchase of educational material,rent for training centres and payment to guest faculty.The financial pattern of assistance for this scheme
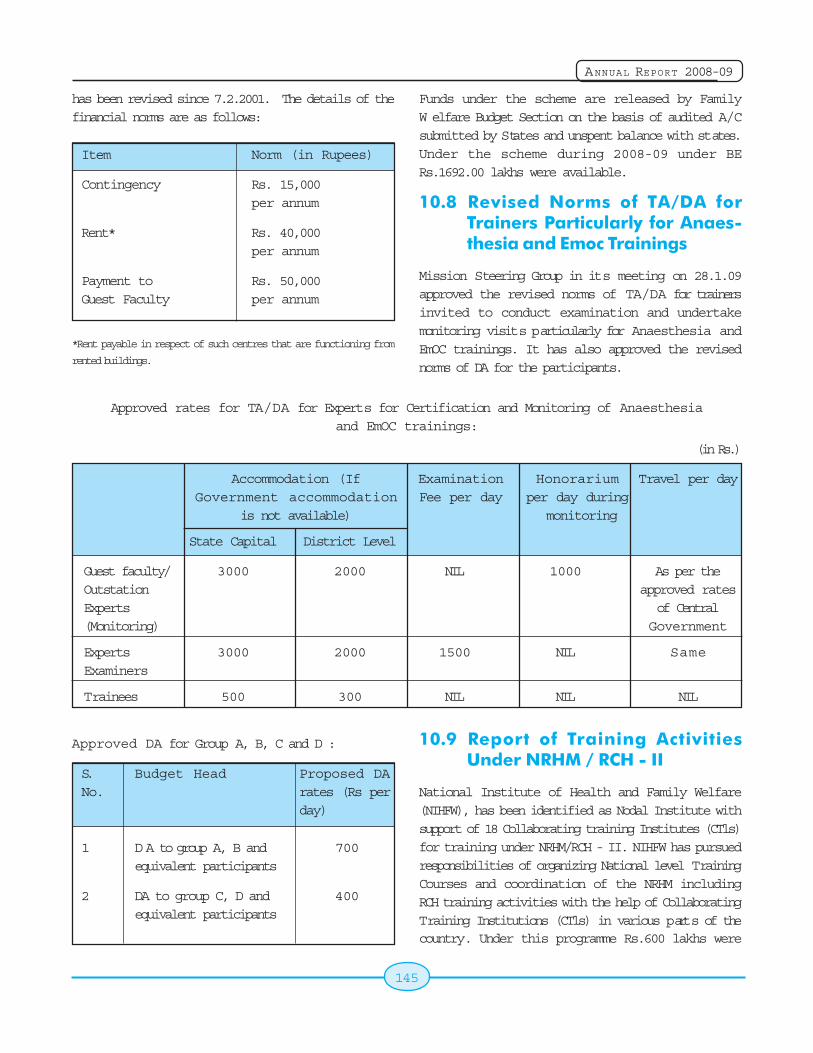
145
ANNUAL REPORT 2008-09
Approved rates for TA/DA for Experts for Certification and Monitoring of Anaesthesiaand EmOC trainings:
(in Rs.)
has been revised since 7.2.2001. The details of thefinancial norms are as follows:
Item Norm (in Rupees)
Contingency Rs. 15,000per annum
Rent* Rs. 40,000per annum
Payment to Rs. 50,000Guest Faculty per annum
*Rent payable in respect of such centres that are functioning from
rented buildings.
Funds under the scheme are released by FamilyW elfare Budget Section on the basis of audited A/Csubmitted by States and unspent balance with states.Under the scheme during 2008-09 under BERs.1692.00 lakhs were available.
10.8 Revised Norms of TA/DA forTrainers Particularly for Anaes-thesia and Emoc Trainings
Mission Steering Group in its meeting on 28.1.09approved the revised norms of TA/DA for trainersinvited to conduct examination and undertakemonitoring visits particularly for Anaesthesia andEmOC trainings. It has also approved the revisednorms of DA for the participants.
Accommodation (If Examination Honorarium Travel per dayGovernment accommodation Fee per day per day during
is not available) monitoring
State Capital District Level
Guest faculty/ 3000 2000 NIL 1000 As per theOutstation approved ratesExperts of Central(Monitoring) Government
Experts 3000 2000 1500 NIL SameExaminers
Trainees 500 300 NIL NIL NIL
Approved DA for Group A, B, C and D :
S. Budget Head Proposed DANo. rates (Rs per
day)
1 D A to group A, B and 700equivalent participants
2 DA to group C, D and 400equivalent participants
10.9 Report of Training ActivitiesUnder NRHM / RCH - II
National Institute of Health and Family Welfare(NIHFW), has been identified as Nodal Institute withsupport of 18 Collaborating training Institutes (CTls)for training under NRHM/RCH - II. NIHFW has pursuedresponsibilities of organizing National level TrainingCourses and coordination of the NRHM includingRCH training activities with the help of CollaboratingTraining Institutions (CTls) in various parts of thecountry. Under this programme Rs.600 lakhs were
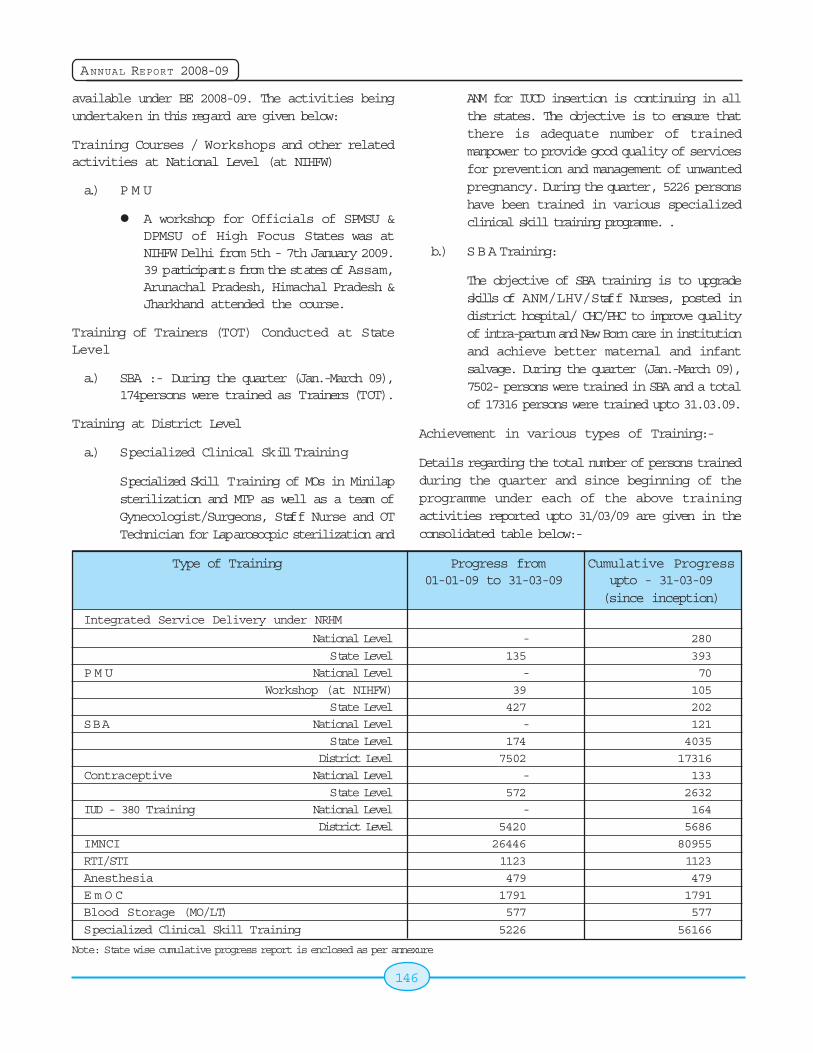
146
ANNUAL REPORT 2008-09
available under BE 2008-09. The activities beingundertaken in this regard are given below:
Training Courses / Workshops and other relatedactivities at National Level (at NIHFW)
a.) P M U
A workshop for Officials of SPMSU &DPMSU of High Focus States was atNIHFW Delhi from 5th - 7th January 2009.39 participants from the states of Assam,Arunachal Pradesh, Himachal Pradesh &Jharkhand attended the course.
Training of Trainers (TOT) Conducted at StateLevel
a.) SBA :- During the quarter (Jan.-March 09),174persons were trained as Trainers (TOT).
Training at District Level
a.) Specialized Clinical Skill Training
Specialized Skill Training of MOs in Minilapsterilization and MTP as well as a team ofGynecologist/Surgeons, Staff Nurse and OTTechnician for Laparosocpic sterilization and
ANM for IUCD insertion is continuing in allthe states. The objective is to ensure thatthere is adequate number of trainedmanpower to provide good quality of servicesfor prevention and management of unwantedpregnancy. During the quarter, 5226 personshave been trained in various specializedclinical skill training programme. .
b.) SBA Training:
The objective of SBA training is to upgradeskills of ANM/LHV/Staff Nurses, posted indistrict hospital/ CHC/PHC to improve qualityof intra-partum and New Born care in institutionand achieve better maternal and infantsalvage. During the quarter (Jan.-March 09),7502- persons were trained in SBA and a totalof 17316 persons were trained upto 31.03.09.
Achievement in various types of Training:-
Details regarding the total number of persons trainedduring the quarter and since beginning of theprogramme under each of the above trainingactivities reported upto 31/03/09 are given in theconsolidated table below:-
Type of Training Progress from Cumulative Progress01-01-09 to 31-03-09 upto - 31-03-09
(since inception)
Integrated Service Delivery under NRHM
National Level - 280
State Level 135 393
P M U National Level - 70
Workshop (at NIHFW) 39 105
State Level 427 202
SBA National Level - 121
State Level 174 4035
District Level 7502 17316
Contraceptive National Level - 133
State Level 572 2632
IUD - 380 Training National Level - 164
District Level 5420 5686
IMNCI 26446 80955
RTI/STI 1123 1123
Anesthesia 479 479
E m O C 1791 1791
Blood Storage (MO/LT) 577 577
Specialized Clinical Skill Training 5226 56166
Note: State wise cumulative progress report is enclosed as per annexure
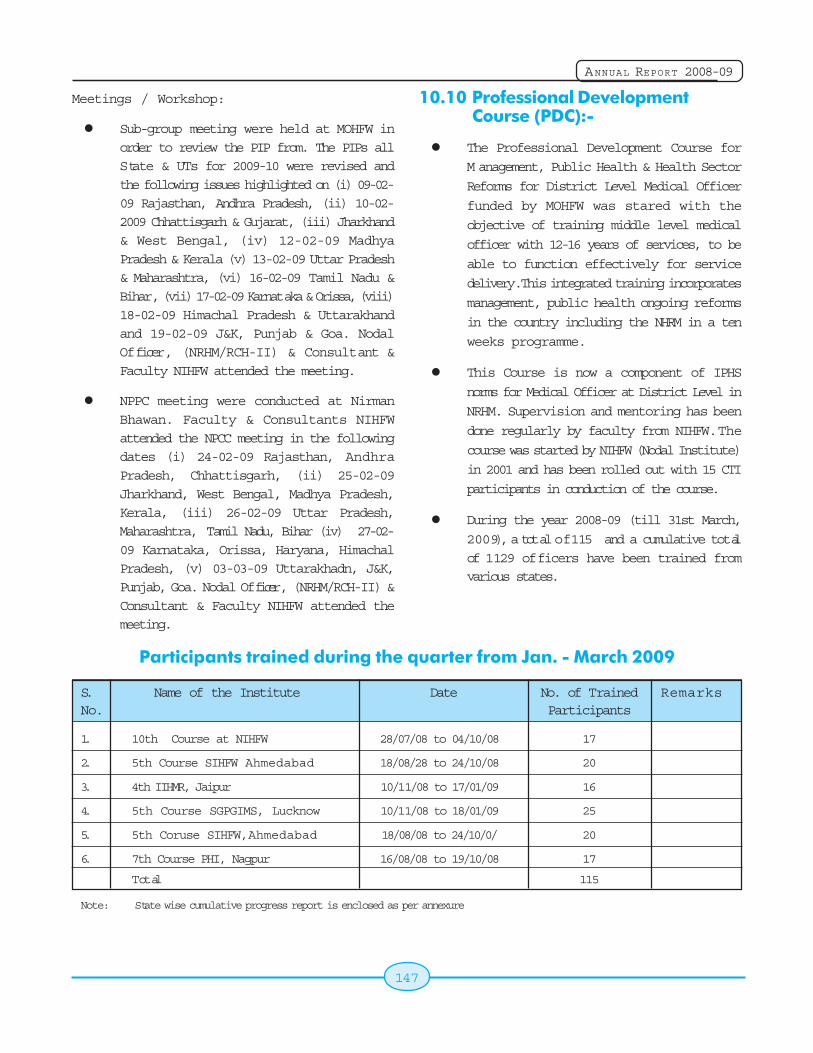
147
ANNUAL REPORT 2008-09
Meetings / Workshop:
Sub-group meeting were held at MOHFW in
order to review the PIP from. The PIPs all
State & UTs for 2009-10 were revised and
the following issues highlighted on (i) 09-02-
09 Rajasthan, Andhra Pradesh, (ii) 10-02-
2009 Chhattisgarh & Gujarat, (iii) Jharkhand
& West Bengal, (iv) 12-02-09 Madhya
Pradesh & Kerala (v) 13-02-09 Uttar Pradesh
& Maharashtra, (vi) 16-02-09 Tamil Nadu &
Bihar, (vii) 17-02-09 Karnataka & Orissa, (viii)
18-02-09 Himachal Pradesh & Uttarakhand
and 19-02-09 J&K, Punjab & Goa. Nodal
Officer, (NRHM/RCH-II) & Consultant &
Faculty NIHFW attended the meeting.
NPPC meeting were conducted at Nirman
Bhawan. Faculty & Consultants NIHFW
attended the NPCC meeting in the following
dates (i) 24-02-09 Rajasthan, Andhra
Pradesh, Chhattisgarh, (ii) 25-02-09
Jharkhand, West Bengal, Madhya Pradesh,
Kerala, (iii) 26-02-09 Uttar Pradesh,
Maharashtra, Tamil Nadu, Bihar (iv) 27-02-
09 Karnataka, Orissa, Haryana, Himachal
Pradesh, (v) 03-03-09 Uttarakhadn, J&K,
Punjab, Goa. Nodal Officer, (NRHM/RCH-II) &
Consultant & Faculty NIHFW attended the
meeting.
10.10 Professional Development Course (PDC):-
The Professional Development Course for
M anagement, Public Health & Health Sector
Reforms for District Level Medical Officer
funded by MOHFW was stared with the
objective of training middle level medical
officer with 12-16 years of services, to be
able to function effectively for service
delivery. This integrated training incorporates
management, public health ongoing reforms
in the country including the NHRM in a ten
weeks programme.
This Course is now a component of IPHS
norms for Medical Officer at District Level in
NRHM. Supervision and mentoring has been
done regularly by faculty from NIHFW. The
course was started by NIHFW (Nodal Institute)
in 2001 and has been rolled out with 15 CTI
participants in conduction of the course.
During the year 2008-09 (till 31st March,
2009), a total of 115 and a cumulative total
of 1129 officers have been trained fromvarious states.
S. Name of the Institute Date No. of Trained RemarksNo. Participants
1. 10th Course at NIHFW 28/07/08 to 04/10/08 17
2. 5th Course SIHFW Ahmedabad 18/08/28 to 24/10/08 20
3. 4th IIHMR, Jaipur 10/11/08 to 17/01/09 16
4. 5th Course SGPGIMS, Lucknow 10/11/08 to 18/01/09 25
5. 5th Coruse SIHFW, Ahmedabad 18/08/08 to 24/10/0/ 20
6. 7th Course PHI, Nagpur 16/08/08 to 19/10/08 17
Total 115
Note: State wise cumulative progress report is enclosed as per annexure
Participants trained during the quarter from Jan. - March 2009

148
ANNUAL REPORT 2008-09
149
ANNUAL REPORT 2008-09
Chapter 11
11.1 Research Activities Under RCHProgramme
The need for research and development in the areasrelated to the RCH is extensive. The researchactivities in the country in the field of contraceptivesresearch have been modest due to meager financialsupport for Research and Development activities andalso because research expertise beyond ICMR wasnot utilized. With a view to increase research effortsthe National Committee on Research in HumanReproduction (NCRHS) constituted a committee inSeptember 1997 and identified national priorities.Presently the committee is called as "ResearchAdvisory Committee (RAC) for RCH andContraceptive study" which is chaired by theSecretary (H&FW) and meets regularly to scrutinizeand fund the various proposals received from NGOsand other Government institutions.
Guidelines for the submission of projects and theareas identified for research has been put up onthe website of this ministry. Presently manyresearch projects are in different stages ofimplementation.
11.2 Indian Council of MedicalResearch (ICMR)
The Indian Council of Medical Research (ICMR),the apex body for the planning, organization,implementation and coordination of medicalresearch in the country promotes biomedicalresearch through a network of its 21 permanentInstitutes and 6 Regional Medical Research Centresdistributed throughout the country and also throughgrants-in-aid given to projects in non-ICMRInstitutes. The budget allocation for ICMR for 2008-2009 was : Plan Rs. 286.00 Crores and Non-PlanRs.110.00 Crores.
11.3 Central Drug Research Institute(CDRI, Lucknow)
The mission of the institute is to strengthen andadvance the field of drug research in India. It hasthe following charter of activities:
Development of new drugs and diagnostics.
Cellular and molecular studies to understanddisease processes and reproductivephysiology.
Development of contraceptive agents anddevices.
Systematic evaluation of medicine propertiesof natural products.
Development of technology for drugs,intermediates and biological.
Dissemination of information in the field ofdrug research, development and production.
Consultancy and development of technicalma npower.
Among the notable achievements of this institutionin the contraceptives field is the development ofCentchroman, an oral non steroidal contraceptiveand CONSAP a contraceptive cream. Both theproducts are now available in the market.Government of India provides grant in aid to thisinstitution for its research activities.
11.4 Testing Facility at IIT, Kharagpur
In order to ensure that quality equipments are utilizedin the program, a national centre for testing of IUDand tubal ring was set up at the Bio-medicalEngineering wing at IIT, New Delhi in 1986-87 withfinancial assistance from UNFPA. Since April, 1992
ResearchResearchResearchResearchResearch
150
ANNUAL REPORT 2008-09
the Centre is being funded by Government of India.IIT is imparting training to personnel of different testinglaboratories in good testing procedures and alsogives training on good manufacturing procedures tothe industries manufacturing contraceptives and NSVinstruments. It is also engaged in the process ofconducting research in development of newcontraceptives and contraceptive technologies. Thecentre is now functioning from the School of Medicaland Biological Sciences at IIT, Kharagpur.
11.5 Indian Medical Association
The Indian Medical Association (IMA) with itsheadquarters in Delhi has been functioning for over65 years through a network of 1200 branches with atotal membership of over 1,30,000 medical
professionals throughout the country. It is one ofthe largest voluntary organizations working in the fieldof public health, medical education and forpropagation of Family Welfare Programme throughits local branches in the States/UTs.
The Government of India has entrusted the followingactivities to IMA :
Holding of seminars/trainings/workshops oncontraceptive updates to propagate themessage of small family norm and adoptionof spacing and permanent methods;
Establishment of Family Welfare Cell at IMAheadquarters for dissemination of informationon family welfare and the existing policy.
151
ANNUAL REPORT 2008-09
Chapter 12
Several National Health Programmes are now underthe umbrella of NRHM. Details of other NationalHealth Programmes are in this chapter.
12.1 National Cancer ControlProgarmme
Cancer is an important public health problem with 8to 9 lakh cases occurring every year. At any point oftime, it is estimated that there are nearly 25 lakhcases in the country. Every year about 4 lakh deathsoccur due to cancer. 40% of the cancers in thecountry are related to tobacco use. Hence Tobacco-related cancers are very common among malesnamely cancers of the lungs and oral cavity. Amongwomen, cancer of uterine cervix and breast arecommon.National Cancer Control Programme waslaunched in 1975-76 with the objectives of primaryprevention, early detection, treatment andrehabilitation. In view of the magnitude of the problemand the requirement to bridge the geographical gapsin the availability of cancer treatment facilities acrossthe country, the programme was revised in 1984-85and subsequently in December 2004.
National Cancer Control Programme (NCCP) has thefollowing schemes: -
Recognition of New Regional Cancer Centers(RCCs): A one-time grant of Rs.5.00 crores is beingprovided for New RCCs.
Strengthening of existing Regional CancerCenters: A one-time grant of Rs.3.00 crores isprovided to the existing Regional Cancer Centers.
Development of Oncology Wing: GovernmentHospitals & Government Medical Colleges areprovided with a grant of Rs.3.00 crores for thedevelopment of Oncology Wing.
District Cancer Control Programme: A grant-in-aid of Rs.90.00 lakhs spread over a period of 5 yearsis provided for the District Cancer Control Program.
Decentralized NGO Scheme: A grant of Rs.8000/-per camp is provided to the NGOs for IEC activitiesthrough nodal agency of the State Govt.
Guidelines for the various schemes are available onthe official website of the Ministry of Health & FamilyWelfare at www.mohfw.nic.in.
The EFC for the 11th five year plan in respect ofNational Cancer Control Programme is at final stageswhich also includes a component of "Public PrivatePartnership". It has also been propose to enhancethe quantum of assistance under various schemes.
Regional Cancer Centres : As of now, there are27 Regional Cancer Centres (RCC) in different partsof the country mainly responsible for carrying outresearch activities and for providing comprehensivecancer care services.
Oncology wing: Support has been given to bothGovernment Medical Colleges and GovernmentHospitals for development of Oncology wing. Atpresent there are 210 institutions having more than350 teletherapy facilities across the country.
IEC Activities: Health education is an important toolfor prevention and early detection of cancers, whichis given importance in every scheme under theNational Cancer Control Programme. The programmesupports activities of health magazine 'Kalyani' andtelecast by Prasar Bharti targeting especially thoseliving in the most populous States.
It is an interactive programme which provides aninterface to the people with experts on various healthand social issues. Kalyani is telecasted through
Other National Health ProgrammesOther National Health ProgrammesOther National Health ProgrammesOther National Health ProgrammesOther National Health Programmes

152
ANNUAL REPORT 2008-09
9 capital Doordarshan stations and 12 sub regionalstations. IEC materials in the form of audio-videospots, posters, leaflets, flipcharts etc. have beendeveloped and advertisements have been insertedin the leading dailies for creating awareness amongthe general masses.
Onconet- India: All 27 RCCs will be linked with eachother and also each RCC would in turn be linked to4 peripheral centres thus facilitating telemedicineservices and continued medical education.Telemedicine Services including tele-consultations,tele-referral, tele-pathology etc. will be provided.
Early detection, treatment, follow-up andmanagement of cancer cases are the main servicesto be provided by this project.
National Cancer Awareness Day: The birthanniversary of Nobel Laureate Madam Curie, 7thNovember is being observed as National CancerAwareness Day since 2001, to create moreawareness about cancer. The slogan for this yearwas "Detect Early, Save Life'. Like all the years thesame was observed by the Regional Cancer Centresby conducting activities related to creating awarenessabout cancers.
On 7th November, 2008 Regional Cancer Centresat Kancheepuram, Bikaner, Shimla and Kolkataconducted camps for early detection of cancer cases,workshops for health care workers, rally etc whichare shown above.
Establishment of Health Minister's Cancer PatientFund - Approval of Competent Authority has beenobtained for establishment of Health Minister'sCancer Patient Fund with a total outlay of Rs. 100.00crore from the National Cancer Control Programme.
153
ANNUAL REPORT 2008-09
Budget Allocation: The tentative budget for the11th Five Year Plan for NCCP is Rs. 2400.00 croresand the budget allocation for 2008-09 is Rs. 120.00crore.
12.2 National Mental HealthProgramme
It is estimated that about 1-2% of the population sufferfrom major mental disorders and about 5% of thepopulation from minor depressive disorders. It is alsoestimated that 25% of people who attend primaryhealth care clinics suffer from various types ofpsychological problems. Around 20% of all patientsseen by primary health care professionals have oneor more mental disorders. One in four families is likelyto have at least one member with a behavioural ormental disorder. These families not only providephysical and emotional support, but also bear thenegative impact of stigma and discrimination. Togetherthese disorders accounted for 12% of the globalburden of disease (GBD) and an analysis of trendsindicates this will increase to 15% by 2020. Most ofthem (>90%) remain un-treated. Poor awarenessabout symptoms of mental illness, myths & stigmarelated to it, lack of knowledge on the treatmentavailability & potential benefits of seeking treatmentare important causes for the high treatment gap.
However, most of mental illness do not requirehospitalization and are manageable by OPDtreatment and follow up care. The new thinking onmental health at the national and international levelis to make the services of mental health, communitybased rather than hospital based. Such community-based services are cost-effective, accessible, help
to ensure respect for human rights, limit stigma and
lead to early treatment and recovery.
To address the huge burden of mental disorders,
National Mental Health Programme (NMHP) was
started in 1982 with the following objectives:
i) To ensure availability and accessibility of
minimum mental health care for all in the near
foreseeable future, particularly to the most
vulnerable sections of the population.
ii) To encourage mental health knowledge and
skills in general health care and social
development.
iii) To promote community participation in mental
health service development and to stimulate
self-help in the community.
As reflected in the National Health Policy 2002, the
objectives of the NMHP and global trend of
community care of mentally ill, community based
mental health care at district level was initiated as
District Mental Health Programme (DMHP) in 1996
and it was extended to 27 Districts across 22 states/
UTs in the IXth plan.
NMHP during Xth Plan
An evaluation of the NMHP was undertaken in 2003
and the programme was restrategised to incorporate
expansion of DMHP to 100 districts all over the
country, modernisation of state run Mental Hospitals,
upgradation of Psychiatry wings in the Govt. Medical
Colleges/General Hospitals, IEC activities, Research
& Training in Mental Health for improving service
delivery.
The Xth Five Year Plan had an outlay of Rs.139
crores. Expenditure during 10th Plan was Rs.106.46
crores. During the 10th Five Year Plan, DMHP was
extended to 109 Districts, Upgradation of Psychiatric
Wings of 71 Medical Colleges/General Hospitals and
modernisation of 23 Mental Hospitals was funded.
Status of NMHP
As on date 123 District have been covered under
D M H P, Psychiatric Wings of 75 Medical Colleges/General Hospital and 26 Mental Hospitals have beenfunded.
Areas of Concern/Programme Weakness
The following areas of concern/weakness have beenidentified in implementation of the programme.
i) Poor availability of skilled manpower inpsychiatry and allied specialties impedesrecruitment of staff for DMHP.
154
ANNUAL REPORT 2008-09
ii) Lack of Awareness regarding MentalIllnesses.
iii) Stigma attached to Mental Illness
iv) Lack of Coordination between stateDepartments e.g. DMHP being implementedthrough the Medical Education Departmentand District health system coming under theHealth Department.
v) Lack of community involvement.
vi) Non-availability of standardized trainingmanuals/ modules.
vii) Many aspects of mental illness e.g. Suicideprevention, Workplace stress management,School and College counselling were notcovered.
Strategy for XIth Plan
To address the above stated areas of concern,strategies for implementation of NMHP during XIthPlan have been redefined. These are enumeratedbelow:
District Mental Health Programme:
Following the globally accepted trends in MentalHealth As envisaged in National Health Policy 2002and following globally accepted trend of communitycare of mentally ill, it has been planned to extendDMHP to more under served Districts in the countryin a phased manner during the XIth plan period. Inline with felt needs of the community new componentsof School Mental Health Services, CollegeCounselling services, Work place Stressmanagement and Suicide Prevention services arebeing planned under the DMHP. DMHP would beextended to more districts following the outcome ofan independent evaluation of the existing DMHPswhich is likely to be complete by the end of November2008.
Manpower Development
As against an estimated requirement of 11500Psychiatrists, 17250 Clinical Psychologists, 23000PSWs & 3000 Psychiatric nurses only approximately
3000 Psychiatrists, 500 Clinical Psychologists, 400PSWs & 900 Psychiatric nurses are available in thecountry. The training infrastructure in the countryproduces approximately 280 Psychiatrists, 50 ClinicalPsychologists, 25 PSWs & 185 Psychiatric nursesper year. Due to shortage of manpower in mentalhealth, the implementation of DMHP sufferedadversely in previous plan periods. To address theacute shortage of qualified mental healthprofessionals in the country two schemes formanpower development are proposed:
Centres of Excellence in Mental Health: It isproposed to establish Centres of Excellence in thefield of Mental Health by upgrading andstrengthening identified existing mental healthhospitals/institutes for addressing the acutemanpower gap & provision of state of the art mentalhealth care facilities in the long run. These instituteswill focus on production of quality Man Power inMental health with primary aim to fulfill manpowerneeds of the NMHP. It is proposed to establish atleast 11 Centres of Excellence under the Schemeduring the plan period. This would result in increasein at least 44 PG seats in Psychiatry, 176 M.Phil.seats in Clinical Psychology & PSW each and 220DPN seats in Psychiatric Nursing each year.
Scheme for Manpower Development in MentalHealth: To provide an impetus for development ofManpower in Mental Health it is proposed that othertraining centers (Government Medical Colleges/Government General Hospitals/ State run MentalHealth Institutes) be supported for starting PGcourses or increasing the intake capacity for PGtraining in Mental Health. It is proposed to supportsetting up/strengthening 30 units of Psychiatry, 30departments of Clinical Psychology, 30 departmentsof PSW and 30 departments of Psychiatric Nursing.It is expected to generate about 60 Psychiatrists, 240Clinical Psychologists, 240 PSWs and 600 PsychiatricNurses per year.
Research & Training- There is gap in research inthe field of mental health in the country. Funds willbe provided to institutes/ organizations for carryingbasic, applied and operational research in mentalhealth field.
155
ANNUAL REPORT 2008-09
In order to address shortage of manpower on medium& short-term basis training strategies are requiredto be developed. Short term training courses throughtele-networking, e-mode would be supported forPsychiatry and allied specialties in identified centersduring the plan period. This would be in addition totraining under DMHP and on the job training.
Information, Education & Communication: It has beenobserved that there is very low awareness amongcommunities regarding mental illness and itstreatment. There is a lot of stigma attached to MentalIllness leading to poor utilisation of available mentalhealth resources.
Innovative IEC strategies involving Mass media atCentral/Regional level to reduce stigma attached tomental illness and to increase awareness regardingmental health, available treatment and mental healthcare facilities is considered essential. Increasedawareness regarding provisions under Mental HealthAct 1987 is also required for its ground levelimplementation.
A media plan for mass media IEC activity is plannedto begin from October 2008.
NGO /PPP
The burden of mental disorders is very high andgovernment efforts need to be supplemented byNGOs/voluntary organizations working in this field.Many of these organizations need financial supportto scale up their activities. Services for homelessmentally ill, Out of school adolescents, slum dwellers,other vulnerable groups etc. is planned to beimplemented through dedicated & credible NGOpartners. Innovative schemes on pilot basis withinvolvement of NGOs/PPP basis are also planned totest the success and subsequent up scaling of theprojects.
Monitoring, Implementation & Evaluation
It is planned to have a dedicated teams at State &Center level for monitoring and implementation ofthe programme.
Spill Over of XTH Plan Schemes
Some State run Mental Hospitals still remain to be
modernized. A grant of upto Rs. 3 crore per mental
hospital would be provided to mental hospitals for
modernisation of facilities and equipments. Similarly,
psychiatry department of government medical
colleges which have not been funded earlier need
to be supported during the plan period. Some of the
deserving areas where there is no well established
Govt. Medical colleges, Government General
hospitals/District hospitals could be funded for
establishment of a psychiatry wing. The grant to be
provided would be upto Rs. 50 lacs/ college for
Upgradation of facilities and equipments. Preference
would be given to colleges/ hospitals planning to
start/increase seats of PG (MD/DPM/DNB) courses
in Psychiatry.
5.8. The NMHP be mainstreamed by integrating it
with NRHM and NUHM.
6.0 The allocation for National Mental Health
Programme for XIth Plan is Rs.1000 crore.
12.3 Guinea Worm EradicationProgramme (GWEP)
In 1983-84, National Institute of Communicable
Diseases (NICD) was made the nodal agency by the
Ministry of Health & Family Welfare, Govt. of India,
for planning, co-ordination, guidance and evaluation
of Guinea Worm Eradication Programme (GWEP).
The last guinea worm case was reported in July 1996
in Jodhpur district of Rajasthan. World Health
Organization certified India as guinea worm disease
free country in February 2000. However, WHO
recommended routine surveillance and IEC to becontinued till global eradication of the disease, whichare being undertaken in all formerly guinea wormdisease endemic states.
12.4 Yaws Eradication Programme(YEP)
Yaws Eradication Programme (YEP) was launchedas a centrally sponsored scheme in 1996-97 to coverall the 51 yaws endemic districts in ten states ofAndhra Pradesh, Orissa, Maharashtra, MadhyaPradesh, Chhattisgarh, Tamil Nadu, Uttar Pradesh,Jharkhand, Assam and Gujarat during the 9th Plan
156
ANNUAL REPORT 2008-09
period. The programme aims to reach the un-reached tribal areas of the country.
National Institute of Communicable Diseases hasbeen identified as nodal agency for the planning,monitoring and evaluation of the Programme. TheProgramme is implemented by the State HealthDirectorates through the existing health care system.The number of reported cases has come down from3751 to NIL during the period from 1996 to 2004 andsubsequently no case has been reported from anyof the states till September 2008.
Funds in the form of "Grant-in-aid" are beingprovided to the States.
12.5 Integrated Disease SurveillanceProject (IDSP)
Integrated Disease Surveillance Project (IDSP) waslaunched by Hon'ble Union Minister of Health & FamilyWelfare in November 2004. It is intended to detectearly warning signals of impending outbreaks andhelp to initiate an effective response in a timelymanner. Total Budget for the project from 2004-09is Rs 408.36 crores
Objectives
! To establish a decentralized state basedsurveillance system for communicablediseases to detect the early warning signals,so that timely and effective public healthactions can be initiated in response to healthchallenges in the country at the district, stateand national level.
! To improve the efficiency of the existingsurveillance activities of disease controlprograms and facilitate sharing of relevantinformation with the health administration,community and other stakeholders so as todetect disease trends over time and evaluatecontrol strategies.
Components:
- Integrating and decentralization ofsurveillance activities
- Human Resource Development - Training of
State Surveillance Officers, DistrictSurveillance Officers, Rapid Response Team,other medical and paramedical staff on
principles of disease surveillance
- Use of Information Technology for collection,
collation, compilation, analysis and
dissemination of data
- Strengthening of public health laboratories
For Project implementation, Surveillance Units have
been set up at Central, State and District level.
The components wise details are as under:
Data Management:
Under IDSP data is collected on a weekly (Monday-
Sunday) basis. The information is collected on three
specified reporting formats, namely "S" (suspected
cases), "P" (presumptive cases) and "L" (Laboratory
confirmed cases) filled by Health Workers, Clinician
and Clinical Laboratory staff. The weekly data gives
the time trends.
Whenever there is a rising trend of illnesses in any
area, it is investigated by the Medical Officers/Rapid
Response Teams (RRT) to diagnose and control the
outbreak. Data analysis and action are being
undertaken by respective units. Emphasis is being
laid on reporting of surveillance data from major
hospitals both in public and private sector and also
Infectious Disease hospitals. IDSP receives weekly
disease surveillance data from 606 districts and for
the year January 2008 to March 2009, 55% of phase
I, II & III states have reported.
Outbreak Surveillance and Response:
Central Surveillance Unit, IDSP receives disease
outbreak reports from the states/UTs as and when
reported as on weekly basis. Even NIL weekly
reporting is mandated and the report is shared with
all stakeholder & Prime Minister's Office (PMO),
Hon'ble Health & Family Welfare Minister, Hon'ble
Minister of State (HFW), Secretary (H&FW), DGHS
(H&FW), Addl. Secretary & Mission Director (NRHM),
Addl. Secretary (GB) and Joint Secretary (RSS).
157
ANNUAL REPORT 2008-09
On an average 10 to 12 outbreaks are reported to
CSU weekly. A total of 587 outbreaks were detected
and responded to by the states/UTs through IDSP
from January 2008 to March 2009.
Media Scanning and Verification Cell:
Media scanning is one of the important systems of
surveillance in detecting the Early Warning Signals.With this background, media scanning andverification cell was established on 24 July 2008 atNICD, Delhi. On an average 8-12 media alerts onoccurrence of unusual health events are beingdetected and verified per week and from January2008 to March 2009 416 media alerts were detectedand verified.
Entomology Unit:
Vector borne epidemic prone diseases (VBD) likeMalaria, JE, Dengue/ Chikungunya, Kala-azar, andPlague are the major public health concern. Everyyear outbreak / epidemics occur in different parts ofthe country wherein high morbidity and mortality arereported. These outbreaks of VBD are reported morefrequently from newer and newer areas and diseaselike plague and chikungunya in the areas where theywere quiescent for long time. In addition to abovedisease like KFD, Tick typhus and other tick miteborne diseases though are of localized importancebut gradually spread from their area of influence andare reported in the areas where they were notreported earlier. Keeping these in view, anEntomology unit in the CSU, IDSP has beenestablished in December 2008, with the followingobjectives:
! Regular dissemination of data onentomological surveillance and other vectoraspects from district to state with the liaisonof state SPO(NVBDCP) and Entomologistsworking in different zones of the country withthe help of newly recruited Entomologistunder NRHM.
! To provide technical support to state/ districtRRT in vector related issues
! Under take field visits as per the schedule to
monitor and evaluate the timeliness andquality of spray such as IRS, insecticidetreated nets and distribution of larvivorousfishes.
! Under take entomological surveillance. Mapand monitor entomological density andbionomics and sensitivity to insecticides.
Information & Communication Network:
ICT plays an integral and most powerful role inimplementing IDSP across the country. One of theimportant components of the project is datamanagement, analysis and rapid communication incase of impending outbreaks. To strengthen thetransmission of data IDSP has established linkageswith State Head Quarters, District Head Quarters andall Government Medical Colleges on a SatelliteBroadband Hybrid Network. The details are as under:
Data Centre Equipments
National Informatics Centre (NIC) has establishedbroadband connectivity at 760 out of 796 sites ofwhich 352 sites have been established from January2008 to March 2009. The objective of Data Centreis speedy data transmission and online entry of datato central servers.
Training Centre Equipments
Training centre equipments has been installed at 275out of 396 sites of which 155 sites have been installedfrom January 2008 to March 2009. State to districtcommunication is possible by NICs E-Learning Portal(http://e-learning.nic.in/lms), which has facility inmanaging life virtual classrooms for training (State/Area specific discussion on disease surveillanceactivities), e-learning, interactive electronicdiscussion (Chat rooms, Boards, Mailing Lists) andreviewing & monitoring project related activities.
Video Conferencing
Indian Space Research Organization (ISRO) hasinstalled 330 out of 400 EDUSAT/V-SAT sites of which90 sites have been installed from January 2008 toMarch 2009. In States, Medical Colleges, Videoconferencing (VC) has been used for discussion with
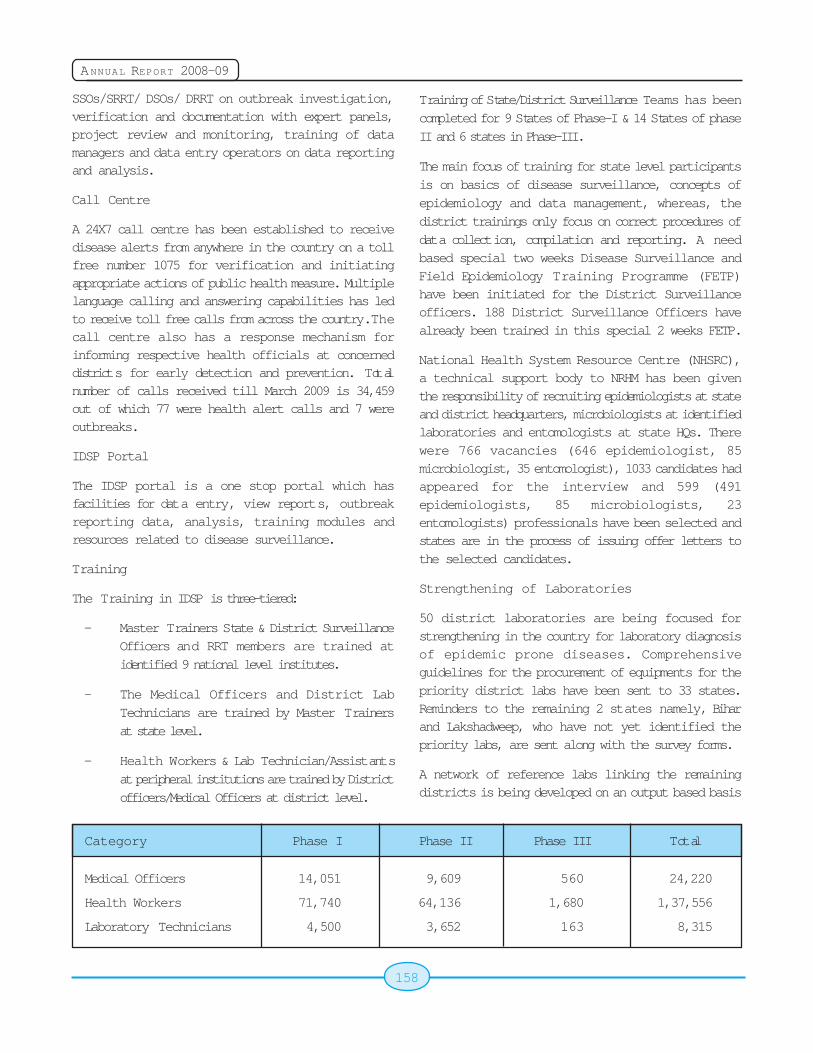
158
ANNUAL REPORT 2008-09
SSOs/SRRT/ DSOs/ DRRT on outbreak investigation,verification and documentation with expert panels,project review and monitoring, training of datamanagers and data entry operators on data reportingand analysis.
Call Centre
A 24X7 call centre has been established to receivedisease alerts from anywhere in the country on a tollfree number 1075 for verification and initiatingappropriate actions of public health measure. Multiplelanguage calling and answering capabilities has ledto receive toll free calls from across the country. Thecall centre also has a response mechanism forinforming respective health officials at concerneddistricts for early detection and prevention. Totalnumber of calls received till March 2009 is 34,459out of which 77 were health alert calls and 7 wereoutbreaks.
IDSP Portal
The IDSP portal is a one stop portal which hasfacilities for data entry, view reports, outbreakreporting data, analysis, training modules andresources related to disease surveillance.
Training
The Training in IDSP is three-tiered:
- Master Trainers State & District SurveillanceOfficers and RRT members are trained atidentified 9 national level institutes.
- The Medical Officers and District LabTechnicians are trained by Master Trainersat state level.
- Health Workers & Lab Technician/Assistantsat peripheral institutions are trained by Districtofficers/Medical Officers at district level.
Training of State/District Surveillance Teams has beencompleted for 9 States of Phase-I & 14 States of phaseII and 6 states in Phase-III.
The main focus of training for state level participantsis on basics of disease surveillance, concepts ofepidemiology and data management, whereas, thedistrict trainings only focus on correct procedures ofdata collection, compilation and reporting. A needbased special two weeks Disease Surveillance andField Epidemiology Training Programme (FETP)have been initiated for the District Surveillanceofficers. 188 District Surveillance Officers havealready been trained in this special 2 weeks FETP.
National Health System Resource Centre (NHSRC),a technical support body to NRHM has been giventhe responsibility of recruiting epidemiologists at stateand district headquarters, microbiologists at identifiedlaboratories and entomologists at state HQs. Therewere 766 vacancies (646 epidemiologist, 85microbiologist, 35 entomologist), 1033 candidates hadappeared for the interview and 599 (491epidemiologists, 85 microbiologists, 23entomologists) professionals have been selected andstates are in the process of issuing offer letters tothe selected candidates.
Strengthening of Laboratories
50 district laboratories are being focused forstrengthening in the country for laboratory diagnosisof epidemic prone diseases. Comprehensiveguidelines for the procurement of equipments for thepriority district labs have been sent to 33 states.Reminders to the remaining 2 states namely, Biharand Lakshadweep, who have not yet identified thepriority labs, are sent along with the survey forms.
A network of reference labs linking the remainingdistricts is being developed on an output based basis
Category Phase I Phase II Phase III Total
Medical Officers 14,051 9,609 560 24,220
Health Workers 71,740 64,136 1,680 1,37,556
Laboratory Technicians 4,500 3,652 163 8,315

159
ANNUAL REPORT 2008-09
utilizing the functional laboratories in MedicalColleges\ existing public health laboratories. Ameeting was held in Karnataka in to develop statespecific plan for laboratory strengthening on 18thand 19th March 2009. Action plan based on AideMemoir of Laboratory component is framed up. SOP's& course curriculum for various levels are being made.A technical committee for giving technical inputs forlab component as per Aide Memoir is beingconstituted.
NCD Risk Factors Survey
NCD Risk factor survey is done under this project ina phasic manner. NCD risk factor survey Phase Iwas done by ICMR. The risk factors to be studiedare Height, Weight, Waist Circumference, PhysicalInactivity, Diet, Socio Demographic Profile, FastingPlasma Glucose, Cholesterol, and consumption ofAlcohol and Smoking. The survey was taken up in 7states i.e. Andhra Pradesh, Tamil Nadu, Kerala,Maharashtra, Madhya Pradesh, Uttrakhand andMizoram in 2007-2008 and is completed. Draft reportof this survey is ready for all the states and the finalreport will be submitted by April 15th 2009.
Advertisement for Phase-II survey was published inthe major newspapers. Evaluation of the Expressionof Interest is under process.
Urban Surveillance:
Urban Surveillance is proposed for 4 metropolitansof Delhi, Mumbai, Chennai and Kolkata. In the citiesof Mumbai, Kolkata & Chennai Urban Surveillanceplans have been developed. Kolkata has alreadybegun activities. Mumbai and Chennai have signedMOU and funds are released
Community Based Surveillance:
It is planned to strengthen community basedsurveillance through active involvement ofcommunity institutions and volunteers, utilizing thelarge number of community groups/institutionspresent in districts such as the Panchayati RajInstitutions, Village Health and Sanitation Committees,Mahila Mandals, Self Help Groups (SHG), YouthClubs, Schools (Primary and Secondary), NGOs,Traditional/Private Health Care providers.
IDSP has started a pilot project for strengtheningcommunity based disease surveillance in 3 states(Maharashtra, Orissa and Karnataka).Dashamantapur (Koraput-Orissa), Similiguda(Koraput-Orissa), Akkalkuwa (Nandurbar-Maharashtra) and Taloda (Nandurbar-Maharashtra)have started community based surveillance activities.
Infectious Disease Hospital SurveillanceNetwork:
7 Infectious Disease Hospitals, one each in fourmetros and Bangalore, Ahmedabad and Hyderabadhave been given funds for strengthening reportingfrom ID Hospitals.
Prevention and Control of Avian Influenza:
IDSP is supporting activities related to Avian Influenzaunder IDSP with total outlay of Rs. 20.85 crores forthree years (2006-09) for Human Component. Anetworking model has been developed with 10laboratories and additionally ICMR with its four branchlaboratories. MoU is being modified with respect toregional laboratory. The procurement of equipmentsfor these labs is in progress.
Project Monitoring:
The IDSP progress is being reviewed by the SeniorOfficers of the Ministry of Health and Family Welfare,Government of India. The project is biannuallyreviewed by World Bank Team comprising ofmembers from CDC, WHO and UNAIDS. The lastreview meeting by World Bank was held from 12thJanuary to 29th January 2009. The states are rankedfor healthy competition. Teams from Centre forDisease Control and Prevention, (CDC) Atlanta alsovisit India regularly to support IDSP.
Finance
Budget estimate for 2008-09 was fixed for Rs 72.00crores. Due to slow implementation of projectactivities by states funds could not be released asexpected. Besides this less expenditure made oncontingencies and AI lab network. Therefore reviseestimates was scaled down to Rs 30.00 crores. Againdue to less work on AI lab network our expenditureachieved to the tune of Rs 21.90 crores during thefinancial year 2008-09.
160
ANNUAL REPORT 2008-09
India ratified WHO Framework Convention on tobacco on 5th February 2004.
Keeping in view our past achievements we have putforward our budget estimates for the financial year2009-10 at Rs 48.50 crores. Out of this EAP is Rs37.15 crores and DBS is Rs11.35 crores. We haveearmarked Budget Estimates for Northeast at Rs 3.00
crores out of total budget of Rs 48.50 crores.
12.6 Tobacco Control Legislation
A comprehensive tobacco control legislation titled
"The Cigarettes and Other Tobacco Products
(Prohibition of Advertisement and Regulation of
Trade and Commerce, Production, Supply and
Distribution) Act, 2003 was notified in the official
gazette on 19th May, 2003. The Act is applicable to
whole of India and covers all types of tobacco
products. The important provisions of the Act are as
follows:
a) To prohibit direct and indirect advertisement
of and provide for regulation of the trade and
commerce in, production, supply and
distribution of all tobacco products.
(implemented w.e.f. 1st May 2004)
b) No person shall engage in smoking in a
public place; (Rules have been notified
and has come into effect on 2nd
October, 2008)
c) No person shall sale tobacco products to any
person below the age of 18 years.
(implemented w.e.f. 1st May 2004)
d) There shall be a total ban on sponsoring of
any sport /cultural events by cigarette and
other tobacco product companies.
(implemented w.e.f. 1st May 2004)
e) Ban of sale of tobacco products within 100
yards of educational institutions.
(implemented w.e.f. 1st December 2004)
f) No person shall trade in any tobacco products
including imported products unless the
specified warnings are indicated. (Rules
have been notified and would come intoeffect on 31st May, 2009)
There are various strategies envisaged for reductionof demand and reduction of supply of tobacco. Mostof the provisions of FCTC are contained underTobacco Control Act, 2003 except those relating toproviding alternative livelihood to tobacco farmer andworkers engaged in tobacco industry / manufacturingand environmental issues. Also FCTC providesguideline for implementation of its various articlese.g. testing of tobacco products for their contentsand emission, protection from secondhand smoke,ban on tobacco advertising, promotion andsponsorship etc.
In order to have effective tobacco control measuresand implementation of various provisions of the Actand at the same time creating awareness about illeffects of tobacco. The pilot phase of NationalTobacco Control Programme was launched in 2007-08 in 18 districts of 9 States and upscaled to cover24 districts of 12 States during the year 2008-09.
The proposed programme broadly envisages-
! Mass media anti-tobacco campaign
161
ANNUAL REPORT 2008-09
! Establishing tobacco testing labs
! Capacity building at the State and District
Level by setting up State Tobacco Control
Cells and District tobacco control cell. This
component would be integrated with NRHM
activities.
! Pertaining with Ministry of Rural Development
and social welfare for providing alternative
livelihood to tobacco farmer/ workers. Ministry
of Health and Family Welfare has also
released Grant-in-aid to Central Tobacco
Research Institute (CTRI), Rajahmundry,
Andhra Pradesh for pilot studies on
alternative cropping to tobacco.
First Global Adult Tobacco Survey (ATS) in India is
also being conducted with the technical assistance
from WHO and CDC Atlanta. The main aim of ATS is
to establish the State wise prevalence of tobacco
use, ascertain levels of awareness/ knowledge about
the ill-effect of the tobacco products. This survey will
also provide baseline data for capacity of the States
in tobacco control initiative.
During 2008-09, Ministry of Health and Family
Welfare conducted one National and five regional
advocacy workshop to sensitize the stakeholder for
implementation of the Tobacco Control Programme.
Setting up of a National Tobacco Regulatory Authority
(NTRA) for effective monitoring and enforcement of
law and the programme is also under consideration.
Budget allocation for the Tobacco Free Initiative for
the year 2008-09 is 39.00 Cr. (including 6.00 Cr. for
NE region and 9.00 Cr. received from IEC Division),
out of which an amount of Rs 35.17 Cr. has been
incurred for under the said Programme.
12.7 Nutrition
The Nutrition Cell in the Directorate General of Health
Services provides technical advise in all matters
related to policy making, Programme implementation,
monitoring & evaluation, training content for different
levels of Medical ;and Para ;Medical workers. It takes
up technical scrutiny of standards and labels for
foods, fortification of foods, proposals, projectevaluation, review of research project etc.
The cell has been making efforts in creatingawareness regarding prevention of micronutrientdeficiency disorders, diet related chronic disordersand promotion of Healthy life style throughdissemination of various types of material. So far,posters and pamphlets on the above mentionedissues, video spots on IDD were developed. Videofilms on National iodine Deficiency Disorders ControlProgramme, Diet related non communicable chronicDiseases and Promotion of Healthy Life Style in Hindiwere also developed along with Radio Programmeon under nutrition, including Micronutrient deficiencyin different Regional languages. Updation of thepublication entitled "Guidelines for StandardizedHospital Diets" has been under process.
The Cell organizes meetings and workshops (National& Regional levels workshops ) on core issues relatedto nutrition i.e. micronutrient, hospital diets, fluorosis,diet related chronic disorders & promotion of healthylife style, fast/junk food etc. Technical Committeemeeting was convened to examine issues related toSoya bean.
An expert group meeting was organised to finalizethe content of " Comprehensive Therapy Guidlilnesin Clinical Practices - A handbook for Physicians,Dieticians and Nurses held at Vigyan Bhavan on 29th-30th September 2008.
In order to address the problem of fluorosis in thecountry a new initiative i.e. "National Programme forPrevention & Control of Fluorosis (NPPCF)" has beenapproved for implementation in 100 districts withfinancial allocation of Rs. 68 crores during the 11thFive year Plan. 1st phase of the programme is to beimplemented from current year. A preparatorymeeting for the new Health Initiative entitled," NationalProgramme for Prevention & Control of Flulorosiswas convened on 19th January, 2009.
The Nutrition Cell also keeps State Nutrition Divisionlocated in 17 States/UTs. updated on development
in the field of nutrition, micronutrient deficiencies, diet
related chronic non-communicable disease, junk/fast
foods etc.
162
ANNUAL REPORT 2008-09
12.8 Strengthening of EmergencyFacilities of State HospitalsLocated on National Highways
With a view to provide immediate treatments to the
victims of road accident, the Ministry of Health &
Family Welfare has been implementing a Project for
up gradation and strengthening of emergency
trauma care facilities in State Government Hospitals
located on National Highways under the Scheme -
"Assistance for Capacity Building", under which
financial assistance was provided upto a maximum
of Rs. 150 lakhs per hospital or actual requirement
of the hospital, whichever was less, during the Xth
Plan.
However, during the XIth Five Year Plan, a revised
new scheme at a total outlay of Rs. 732.75 crores
has been approved for developing a network of
Trauma Centres along the Golden Quadrilateral,
North-South and East-West corridors of the National
Highways, This project would be a major stepping
stone in moving towards the desired objective of
bringing down preventable deaths in road accidents
to around 10% subsequently National Highways
(other than GQ & NE corridor) with substantial number
of accidents and
! Connecting two capital cities
! Connecting major cities other than capitalcities
! Connecting ports to major cities
! Connecting industrial townships with capitalcities
Could also be covered by the proposed network/system of trauma care, keeping in view the fact thatinstead of random selection of hospitals as had beendone in the past, the scheme should focus ondevelopment of a network of trauma care facilitiesalong the selected corridors of National Highwaysand also to bring down the morbidity and mortalityon account of accidental trauma in India.
The trauma care network has been so designed thatno trauma victim has to be transported for more than
50 Kilometers and a designated trauma centre isavailable at every 100 Kilometers. The project,therefore, comprises of well equipped life supportAmbulance at every 50 Kilometers of the NationalHighways with well-equipped & staffed trauma centreat every 100-200 Kilometers of the National Highways.
During the 11th Plan period, in the year 2007-08,financial assistance have been sanctioned to 26 StateGovt. Hospitals/Medical Colleges of 6 States andduring the year 2008-09, 55 State Govt. Hospitals/Medical Colleges of the 10 States have beensanctioned financial assistance under this schemewhich includes 6 hospitals of Assam State in the North-East Region.
12.9 National Programme forPrevention and Control ofDiabetes, Cardiovascular Diseaseand Strokes
Considering the fact that Non-CommunicableDiseases (NCDs) are surpassing the burden ofcommunicable Disease in India and the existingHealth system mainly focused on communicablediseases, need for National Programme forPrevention and Control of Diabetes, CardiovascularDiseases and Stroke (NPDCS) was envisaged.During the 11th Five Year Plan, and outlay of Rs.1660.50 crores has been provided for theProgramme. The Programme is being implementedin phased manner with a piloting being done in thefirst phase. Subsequently, the Programme isproposed to be implemented across the country.
A pilot scheme has been launched in January, 2008and encompasses 10 States with one District eachnamely, Kamrup, Assam; Jalandhar, Punjab, Bhilwara,Rajasthan, jabalpur, Madhya Pradesh, Shimoga,Karnataka, Kancheepuram, Tamil Nadu,Thiruvananthapuram, Kerala.
The Pilot Programme aims at prevention and controlof (NCDs) using health promotion and healtheducation advocacy, early detection of persons withhigh level of risk of developing diseases throughopportunistic screening capacity building of healthsystem at all levels to tackle NCDs and improvement
163
ANNUAL REPORT 2008-09
of quality of care and developing trained manpowerat various health care set-up in Districts/States.
12.10 National Programme forPrevention and Control ofDeafness
Hearing impairment / deafness is the second mostcommon cause of disease morbidity in the country.There has been no national level intervention on oneof the most common preventable cause of disability.
MOHFW has therefore launched the new NationalProgramme on Prevention and Control of Deafness(NPPCD). This programme has been approved bythe competent authority and approximately 80 districtsare being covered in 2008-09. The key componentsinclude early detection and screening; medical andsurgical treatment; rehabilitation of children withhearing aids; awareness campaigns.
As part of the strategy two personnel will be deployedin each district - One Audiometric Assistant and oneInstructor/lecturer. The shortage of AudiometricAssistant is being met by introduction of new DHLSProgram from AIISH, Mysore. This programmeintroduced in 2007 has already trained more than75 Audiometric Assistants. The Programme is beingupscaled from 5 centres to 11 centres this year, eachof which are linked to interactive Audio-visualconnectivity, making it possible for the e-educationfrom AIISH, Mysore.
12.11 National Programme forPrevention and Control ofFluorosis
Fluorosis, a public health problem is caused byexcess intake of fluorosis through drinking water/foodproducts/industrial pollutants over a long period. It
results in major health disorders like dental fluorosis,skeletal fluorosis and non-skeletal fluorosis besidesinducing ageing. These harmful effects beingpermanent and irreversible in nature are detrimentalto the health of an individual and the community whichin turn has an impact on growth developmenteconomy and human resource development of thecountry.
A new initiative has been conceived during the 11thFive Year Plan with a goal to prevent & controlFluorosis in the country. The objectives under theprogramme are to collect assess and use the baselinesurvey data of fluorosis of Department of Drinkingwater Supply for starting the project; Comprehensivemanagement of fluorosis in the selected areas;Capacity building for prevention, diagnosis andmanagement of fluorosis cases.
The strategies under the porogramme are trainingto health personnel for prevention health promotionearly diagnosis and prompt intervention; Capacitybuilding of district and medical college hospital forreconstructive surgery and rehabilitation;Establishment of diagnostic facilities in the districthospitals; Health education for prevention andcontrol of Fluorosis cases.The activities of theprogramme are to be implemented in phased manner(Fluorosis affected) in 100 districts of the country.
The National Programme for Prevention & Controlof Fluorosis" (NPPCF) has been already initiated in6 districts namely Nellore (Andhra Pradesh),Jamnagar (Gujarat), Ujjain (Madhya Pradesh),Nayagarh (Orissa), Nagaur (Rajasthan) &
Dharmapuri (TamilNadu) in the current financial year
2008-09. The Programme is planned for expansion
to 14 more districts of the country during the year2009-10.

164
ANNUAL REPORT 2008-09
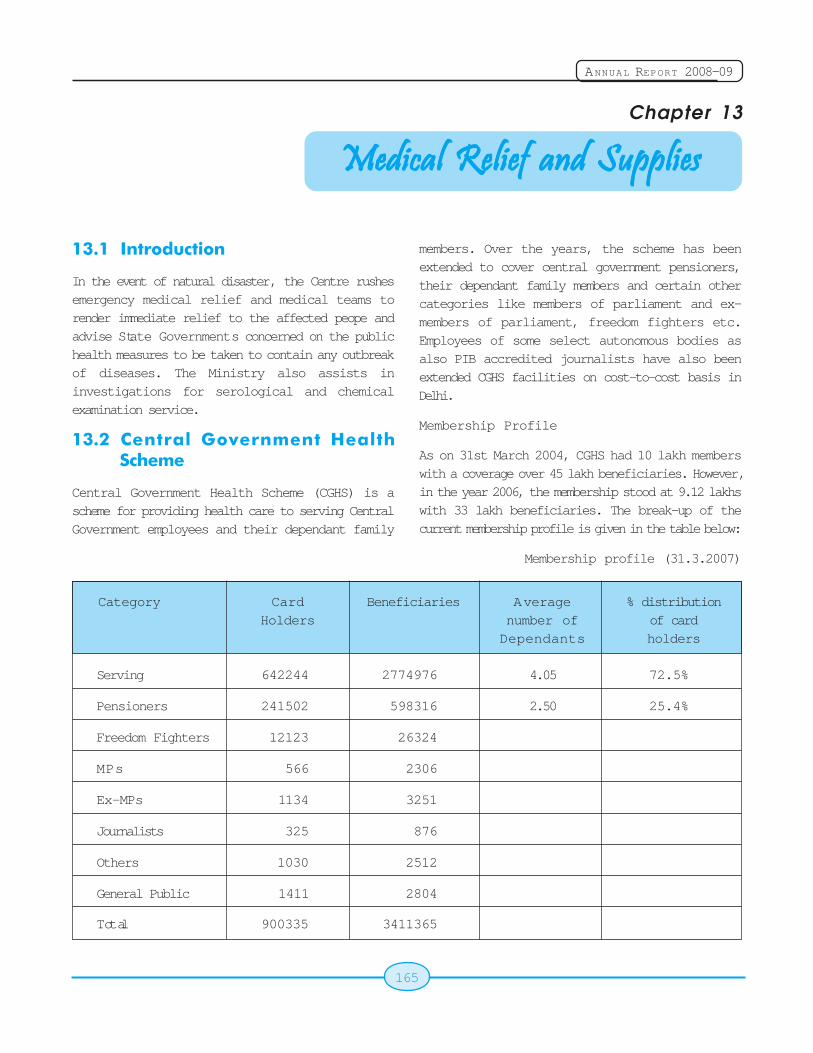
165
ANNUAL REPORT 2008-09
Chapter 13
13.1 Introduction
In the event of natural disaster, the Centre rushesemergency medical relief and medical teams torender immediate relief to the affected peope andadvise State Governments concerned on the publichealth measures to be taken to contain any outbreakof diseases. The Ministry also assists ininvestigations for serological and chemicalexamination service.
13.2 Central Government HealthScheme
Central Government Health Scheme (CGHS) is ascheme for providing health care to serving CentralGovernment employees and their dependant family
Medical Relief and SuppliesMedical Relief and SuppliesMedical Relief and SuppliesMedical Relief and SuppliesMedical Relief and Supplies
members. Over the years, the scheme has beenextended to cover central government pensioners,their dependant family members and certain othercategories like members of parliament and ex-members of parliament, freedom fighters etc.Employees of some select autonomous bodies asalso PIB accredited journalists have also beenextended CGHS facilities on cost-to-cost basis inDelhi.
Membership Profile
As on 31st March 2004, CGHS had 10 lakh memberswith a coverage over 45 lakh beneficiaries. However,in the year 2006, the membership stood at 9.12 lakhswith 33 lakh beneficiaries. The break-up of thecurrent membership profile is given in the table below:
Membership profile (31.3.2007)
Category Card Beneficiaries Average % distributionHolders number of of card
Dependants holders
Serving 642244 2774976 4.05 72.5%
Pensioners 241502 598316 2.50 25.4%
Freedom Fighters 12123 26324
MPs 566 2306
Ex-MPs 1134 3251
Journalists 325 876
Others 1030 2512
General Public 1411 2804
Total 900335 3411365
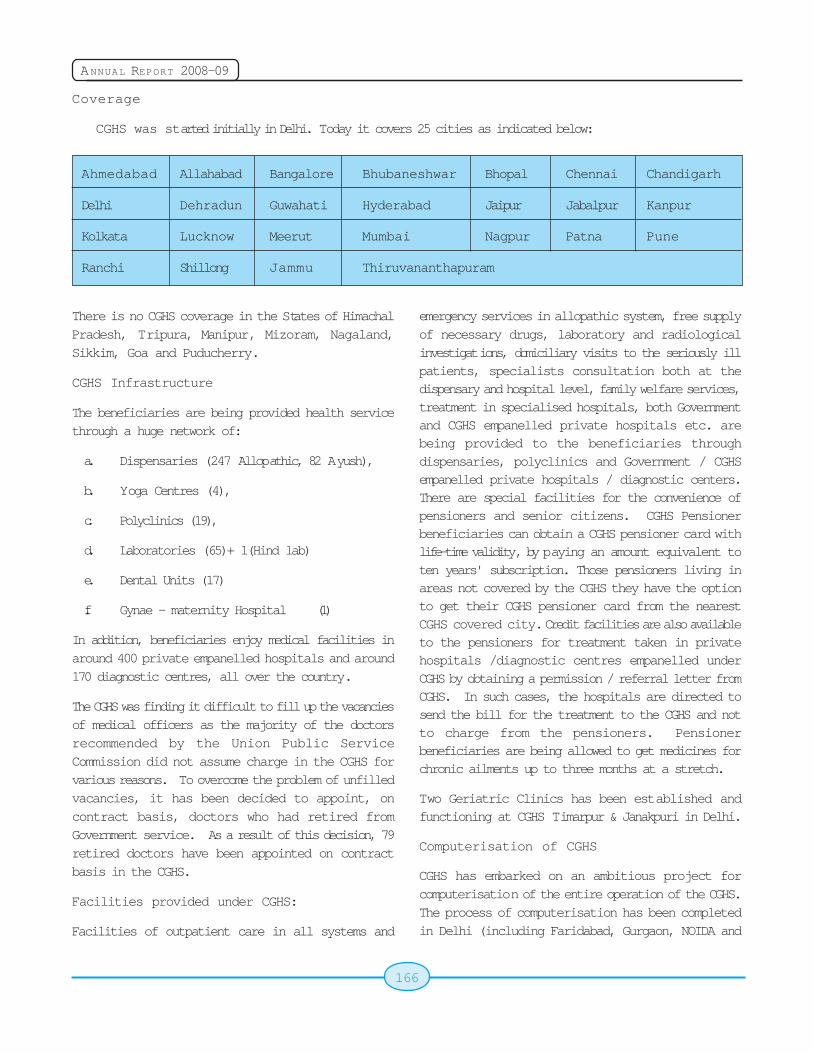
166
ANNUAL REPORT 2008-09
Coverage
CGHS was started initially in Delhi. Today it covers 25 cities as indicated below:
Ahmedabad Allahabad Bangalore Bhubaneshwar Bhopal Chennai Chandigarh
Delhi Dehradun Guwahati Hyderabad Jaipur Jabalpur Kanpur
Kolkata Lucknow Meerut Mumbai Nagpur Patna Pune
Ranchi Shillong Jammu Thiruvananthapuram
There is no CGHS coverage in the States of HimachalPradesh, Tripura, Manipur, Mizoram, Nagaland,Sikkim, Goa and Puducherry.
CGHS Infrastructure
The beneficiaries are being provided health servicethrough a huge network of:
a. Dispensaries (247 Allopathic, 82 Ayush),
b. Yoga Centres (4),
c. Polyclinics (19),
d. Laboratories (65)+ 1(Hind lab)
e. Dental Units (17)
f. Gynae - maternity Hospital (1)
In addition, beneficiaries enjoy medical facilities inaround 400 private empanelled hospitals and around170 diagnostic centres, all over the country.
The CGHS was finding it difficult to fill up the vacanciesof medical officers as the majority of the doctorsrecommended by the Union Public ServiceCommission did not assume charge in the CGHS forvarious reasons. To overcome the problem of unfilledvacancies, it has been decided to appoint, oncontract basis, doctors who had retired fromGovernment service. As a result of this decision, 79retired doctors have been appointed on contractbasis in the CGHS.
Facilities provided under CGHS:
Facilities of outpatient care in all systems and
emergency services in allopathic system, free supplyof necessary drugs, laboratory and radiologicalinvestigations, domiciliary visits to the seriously illpatients, specialists consultation both at thedispensary and hospital level, family welfare services,treatment in specialised hospitals, both Governmentand CGHS empanelled private hospitals etc. arebeing provided to the beneficiaries throughdispensaries, polyclinics and Government / CGHSempanelled private hospitals / diagnostic centers.There are special facilities for the convenience ofpensioners and senior citizens. CGHS Pensionerbeneficiaries can obtain a CGHS pensioner card withlife-time validity, by paying an amount equivalent toten years' subscription. Those pensioners living inareas not covered by the CGHS they have the optionto get their CGHS pensioner card from the nearestCGHS covered city. Credit facilities are also availableto the pensioners for treatment taken in privatehospitals /diagnostic centres empanelled underCGHS by obtaining a permission / referral letter fromCGHS. In such cases, the hospitals are directed tosend the bill for the treatment to the CGHS and notto charge from the pensioners. Pensionerbeneficiaries are being allowed to get medicines forchronic ailments up to three months at a stretch.
Two Geriatric Clinics has been established andfunctioning at CGHS Timarpur & Janakpuri in Delhi.
Computerisation of CGHS
CGHS has embarked on an ambitious project forcomputerisation of the entire operation of the CGHS.The process of computerisation has been completedin Delhi (including Faridabad, Gurgaon, NOIDA and
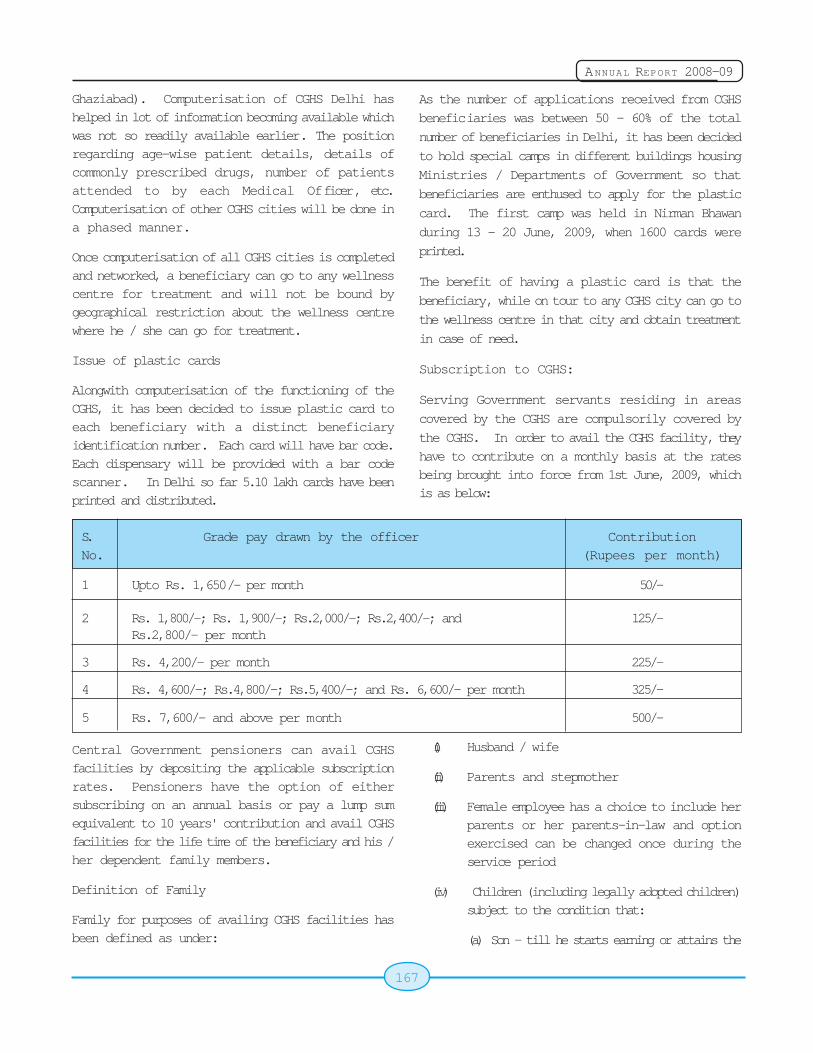
167
ANNUAL REPORT 2008-09
Ghaziabad). Computerisation of CGHS Delhi hashelped in lot of information becoming available whichwas not so readily available earlier. The positionregarding age-wise patient details, details ofcommonly prescribed drugs, number of patientsattended to by each Medical Officer, etc.Computerisation of other CGHS cities will be done ina phased manner.
Once computerisation of all CGHS cities is completedand networked, a beneficiary can go to any wellnesscentre for treatment and will not be bound bygeographical restriction about the wellness centrewhere he / she can go for treatment.
Issue of plastic cards
Alongwith computerisation of the functioning of theCGHS, it has been decided to issue plastic card toeach beneficiary with a distinct beneficiaryidentification number. Each card will have bar code.Each dispensary will be provided with a bar codescanner. In Delhi so far 5.10 lakh cards have beenprinted and distributed.
As the number of applications received from CGHS
beneficiaries was between 50 - 60% of the total
number of beneficiaries in Delhi, it has been decided
to hold special camps in different buildings housing
Ministries / Departments of Government so that
beneficiaries are enthused to apply for the plastic
card. The first camp was held in Nirman Bhawan
during 13 - 20 June, 2009, when 1600 cards were
printed.
The benefit of having a plastic card is that the
beneficiary, while on tour to any CGHS city can go to
the wellness centre in that city and obtain treatment
in case of need.
Subscription to CGHS:
Serving Government servants residing in areas
covered by the CGHS are compulsorily covered by
the CGHS. In order to avail the CGHS facility, they
have to contribute on a monthly basis at the ratesbeing brought into force from 1st June, 2009, whichis as below:
S. Grade pay drawn by the officer ContributionNo. (Rupees per month)
1 Upto Rs. 1,650/- per month 50/-
2 Rs. 1,800/-; Rs. 1,900/-; Rs.2,000/-; Rs.2,400/-; and 125/-Rs.2,800/- per month
3 Rs. 4,200/- per month 225/-
4 Rs. 4,600/-; Rs.4,800/-; Rs.5,400/-; and Rs. 6,600/- per month 325/-
5 Rs. 7,600/- and above per month 500/-
Central Government pensioners can avail CGHSfacilities by depositing the applicable subscriptionrates. Pensioners have the option of eithersubscribing on an annual basis or pay a lump sumequivalent to 10 years' contribution and avail CGHSfacilities for the life time of the beneficiary and his /her dependent family members.
Definition of Family
Family for purposes of availing CGHS facilities hasbeen defined as under:
(i) Husband / wife
(ii) Parents and stepmother
(iii) Female employee has a choice to include herparents or her parents-in-law and optionexercised can be changed once during theservice period
(iv) Children (including legally adopted children)subject to the condition that:
(a) Son - till he starts earning or attains the
168
ANNUAL REPORT 2008-09
age of 25 years, whichever is earlier. Ason, if married, even if he is dependenton his parents and is below 25 years' ofage will not be part of the family for CGHSpurposes.
Son, even if he is more than 25 years' ofage, but is suffering from permanentdisability and is fully dependent on hisparents will be entitled to CGHS facility
(b) Daughter - Till she starts earning or getsmarried, whichever is earlier, irrespectiveof age-limit. Widowed dependentdaughters; divorced / separateddaughters if dependent on her parentswill be entitled to CGHS facilityirrespective of age-limit.
(v) Sisters including unmarried / divorced /abandoned or separated from husband /widowed sisters, if dependent on theGovernment servant will be entitled to CGHSfacilities irrespective of age-limit.
(vi) Minor brothers
Dependency Criteria
Members of the family (other than one spouse) whoseincome from all sources is less than Rs.3,500/- plusan amount equivalent to the DA announced by theGovernment from time to time will be treated asdependent on the Government servant and henceare entitled to avail CGHS facilities.
Empanelment of private hospitals anddiagnostic centres
As CGHS does not adequate facilities to offer medicaltreatment to its beneficiaries in Governmenthospitals, it empanels private hospitals anddiagnostic centres in all CGHS covered cities. Forthis purpose tenders were floated in 2004 calling forprivate hospitals and diagnostic centres interestedin being empanelled under CGHS to offer their ratesfor various procedures / tests, etc. Based on therates quoted by the private hospitals and diagnosticcentres, the lowest rate in respect of each procedure/ test was offered to the private hospitals and
diagnostic centres and those private hospitals anddiagnostic centres which accepted the rates wereempanelled under CGHS.
Private hospitals and diagnostic centres which wereempanelled under CGHS were required to sign a MOAwith the CGHS. Any violation of the provisions of theMOA meant that fines would be levied on these privatehospitals and diagnostic centres and bank guaranteecould also be utilised.
Action has been initiated to revise the rates for theprocedures / tests. For this purpose speciality-wisecommittees were formed under the chairmanship of,Additional Directorate General of Health Services torecommend removal of obsolete procedures, etc.,and to recommend inclusion of newer procedures,etc. which are presently not on the list. The numberof procedures now to be brought under package rateregime will go up substantially and is likely to bearound 2,000 from the present 1,400.
Procedure for referral to empanelled hospitals& diagnostic centres
The CGHS beneficiary first visits the dispensary (nowrenamed as Wellness Centre) for treatment of anailment. The CMO in the wellness centre will refer tothe patient to a specialist in a Government hospitalfor suggesting the procedure / tests, etc., to beundergone by the patient. If the CGHS beneficiaryis a pensioner, then the wellness centre will issue areferral letter to the private hospital and diagnosticcentre where the beneficiary wants to be treated.The private hospitals and diagnostic centres willprovide credit facility to the beneficiary and raise theirbill on the CGHS.
If, however, the CGHS card holder is a serving CentralGovernment servant, then he / she will have to obtainpermission from his / her Ministry / Department.
Change in procedure for payment of hospital /diagnostic centres' bills:
Private hospitals and diagnostic centres haveto provide credit facility to pensioner CGHSbeneficiaries referred to it by the CGHS. Due topaucity of funds, settlement of the bills of private
169
ANNUAL REPORT 2008-09
hospitals and diagnostic centres got delayed withthe result that many private hospitals and diagnostic
centres refused to extend credit facility without
receiving payment towards the bills already
submitted. To overcome the problem, it has been
decided to engage Third Party Administrators (TPA)
for processing of bills and release of payments
electronically through a bank. After the bank makes
the payment through electronic medium, will lodge
its claim on the CGHS for recoupment of the
payments made. CGHS will, then, release payments
to the bank. CGHS will pay service charge / interest
to TPA and banks. This procedure will be introduced
in Delhi in the first phase and later on extended to
other CGHS cities in a phased manner.
CGHS will then carry out medical audit of the bills
passed for payment by the TPA
Supply of medicines to beneficiaries
Medicines for CGHS are procured by HSCC / Medical
Stores Depot on the basis of the indents made by
different wellness centres, and supplied to the
wellness centres. The medicines prescribed by the
treating doctor, if available in the store of the wellness
centre, are supplied to the beneficiary. If, however,
the prescribed medicine is not available by the brand
name but in another brand name or there is another
medicine with the same active ingredients, then the
same is supplied to the beneficiary.
Treatment for Cancer
As there is no private hospital empanelled under
CGHS for treatment of cancer patients (both old and
new), ad-hoc arrangements for treatment of cancer
patients in view of the hardships faced by CGHS
beneficiaries undergoing treatment for cancer,
patients can be referred to the any hospital offering
treatment to CGHS beneficiaries suffering from
cancer.
In addition, orders have been issued treating the
following Regional Cancer Centres to be treated as
to have been deemed as empanelled under CGHS /CS (MA) Rules
Regional Cancer Centres deemed to be empanelledunder CGHS:-
1. Kamla Nehru Memorial Hospital, Allahabad,Uttar Pradesh;
2. Chittaranjan National Cancer Institute,Kolkata, West Bengal;
3. Kidwai Memorial Institute of Oncology,Bangalore, Karnataka;
4. Regional Cancer Institute (WIA), Adyar,Chennai, Tamil Nadu;
5. Regional Cancer Centre,Thiruvananthapuram;
6. Gujarat Cancer Research Institute,Ahmedabad, Gujarat;
7. MNJ Institute of Oncology, Hyderabad, AndhraPradesh;
8. Dr. B.B. Cancer Institute, Guwahati, Assam;
9. Indian Rotary Cancer Institute (AIIMS) , NewDelhi;
10. RST Hospital & Research Centre, Nagpur,Maharashtra;
11. Tata Memorial Hospital, Mumbai,Maharashtra; and
12. Indira Gandhi Institute of Medical Sciences,Patna, Bihar.
Regional Cancer Centres deemed to be empanelledunder CS(MA) Rules, 1944
1. Acharya Harihar Regional Cancer Centre forCancer Research & Treatment, Cuttack,Orissa;
2. Pondicherry Regional Cancer Society,JIPMER, Pondicherry;
3. Regional Cancer Control Society, Shimla,Himachal Pradesh;
4. Cancer Hospital and Research Centre,Gwalior, Madhya Pradesh;

170
ANNUAL REPORT 2008-09
5. Pt. JNM Medical College, Raipur,Chhatisgarh;
6. Acharya Tulsi Regional Centre Trust andResearch Institute (RCC), Bikaner, Rajasthan;and
7. Regional Cancer Centre, Pt. B. D. SharmaPost Graduate Institute of Medical Sciences,Rohtak, Haryana.
Other facilities
CGHS beneficiaries in Kolkata can avail treatment /facilities in the Afternoon Pay Clinics run by theGovernment of West Bengal, with provision forreimbursement of the consultation fee. The OPDconsultation fee charged by the Pay Clinics will bereimbursed at the rate of Rs. 100/- (Rupees onehundred only) for the first visit and Rs. 60/- (RupeesSixty only) for subsequent visits. The reimbursementof the expenditure will be made by the concernedDepartment / Ministry in case of serving employeesand by CGHS in case of pensioner beneficiaries.
It has been decided that all the laboratories on thepanel of CGHS have to get certificate issued by theNational Accreditation Board for Testing andCalibration Laboratories under the Quality Councilof India.
Beneficiaries under CGHS possessing a validCGHS card can avail treatment / investigationfacilities at Nizam's Institute of Medical Sciences,Hyderabad, for which prior referral / permission /approval will not be necessary from the concernedDepartment / CGHS Dispensary. Similarly,beneficiaries under Central Services (MedicalAttendance) Rules, 1944 can also avail treatment/ investigation facilities at Nizam's Institute ofMedical Sciences, Hyderabad without prior referral/ permission / approval. Beneficiaries who areliving outside Hyderabad and wish to undertaketreatment at the Institute without being referred bythe competent authority will not be entitled to claimTA / DA for the journey to be performed by themfor the purpose of treatment.
Local indenting of medicines
Each wellness centre holds certain quantity of
branded and generic drugs, which are distributed to
the beneficiaries on the basis of prescriptions of
specialists. If any drug is not available in stock, then
the wellness centre places an indent on the locally
authorised chemist for the wellness centre for the
supply of the drugs.
As it is not possible for the wellness centres keep in
stock all the drugs that are prescribed by the
specialists and if drugs with the same active
ingredients are also not available, then the wellness
centre is authorised to place an indent on the locally
authorised chemist for the supply of the drug
prescribed by the specialist.
Local authorised chemist for each wellness centre is
appointed on the basis of tenders floated by the
CGHS for such appointment. The selection of the
chemist is done on the basis of the highest rebate
offered by the chemist on the printed MRP. Before
the chemist is appointed his premises is inspected
to ensure that he has the capacity to handle the
volume of indents that will be placed by the wellness
centre on the chemist.
Grievance redressal mechanism
Local Advisory Committees
Instructions have already been issued to all CGHS
cities that meetings of Local Advisory Committees
be held on Second Saturday of every month in each
dispensary. The meetings are held under the
chairmanship of CMO in charges of the dispensaries
in which Area Welfare Officers, representatives of
pensioners' associations, are members to discuss
local problems faced by the dispensaries and to
resolve the issue.
All wellness centres have been directed to keep a
Complaints / Suggestions Box and also to maintain a
Complaints / Suggestions register. The Complaints
Box will be opened at the time of the meeting of the
LAC.
Holding of claims adalats in Delhi
Complaints were received in the CGHS and in the
Ministry that old cases of reimbursement of medical
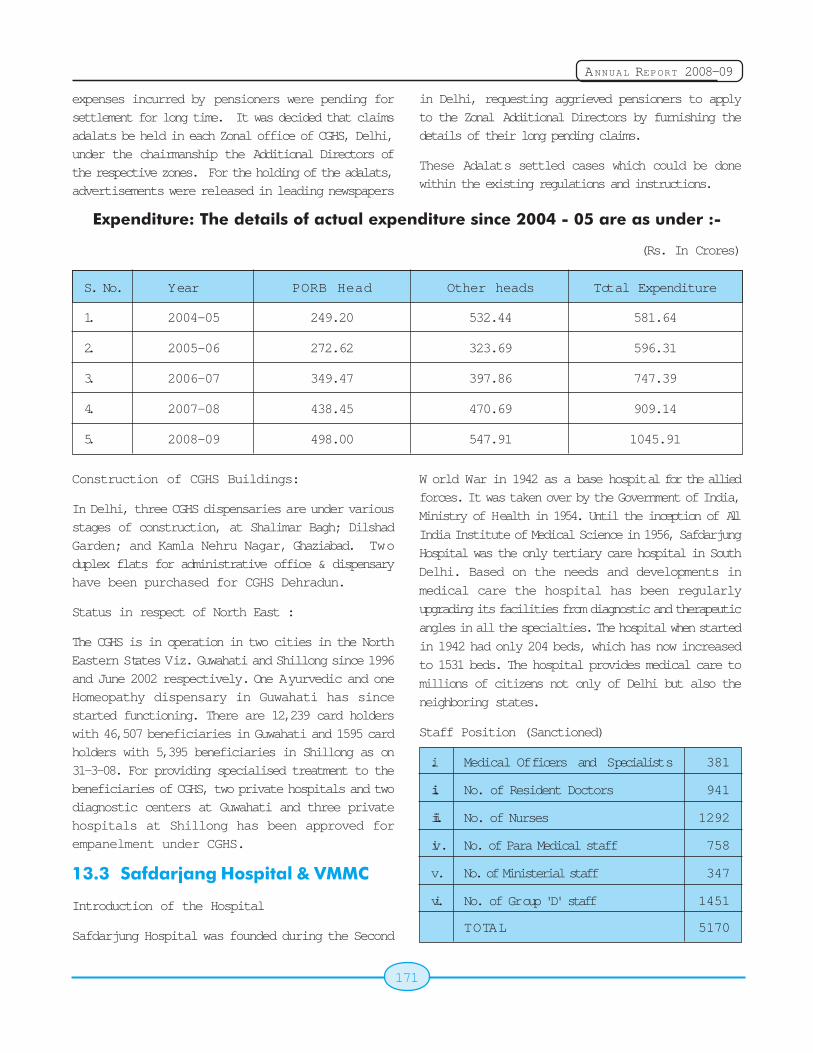
171
ANNUAL REPORT 2008-09
expenses incurred by pensioners were pending forsettlement for long time. It was decided that claimsadalats be held in each Zonal office of CGHS, Delhi,under the chairmanship the Additional Directors ofthe respective zones. For the holding of the adalats,advertisements were released in leading newspapers
in Delhi, requesting aggrieved pensioners to applyto the Zonal Additional Directors by furnishing thedetails of their long pending claims.
These Adalats settled cases which could be donewithin the existing regulations and instructions.
Expenditure: The details of actual expenditure since 2004 - 05 are as under :-
(Rs. In Crores)
S. No. Year PORB Head Other heads Total Expenditure
1. 2004-05 249.20 532.44 581.64
2. 2005-06 272.62 323.69 596.31
3. 2006-07 349.47 397.86 747.39
4. 2007-08 438.45 470.69 909.14
5. 2008-09 498.00 547.91 1045.91
Construction of CGHS Buildings:
In Delhi, three CGHS dispensaries are under variousstages of construction, at Shalimar Bagh; DilshadGarden; and Kamla Nehru Nagar, Ghaziabad. Twoduplex flats for administrative office & dispensaryhave been purchased for CGHS Dehradun.
Status in respect of North East :
The CGHS is in operation in two cities in the NorthEastern States Viz. Guwahati and Shillong since 1996and June 2002 respectively. One Ayurvedic and oneHomeopathy dispensary in Guwahati has sincestarted functioning. There are 12,239 card holderswith 46,507 beneficiaries in Guwahati and 1595 cardholders with 5,395 beneficiaries in Shillong as on31-3-08. For providing specialised treatment to thebeneficiaries of CGHS, two private hospitals and twodiagnostic centers at Guwahati and three privatehospitals at Shillong has been approved forempanelment under CGHS.
13.3 Safdarjang Hospital & VMMC
Introduction of the Hospital
Safdarjung Hospital was founded during the Second
W orld War in 1942 as a base hospital for the alliedforces. It was taken over by the Government of India,
Ministry of Health in 1954. Until the inception of All
India Institute of Medical Science in 1956, Safdarjung
Hospital was the only tertiary care hospital in South
Delhi. Based on the needs and developments in
medical care the hospital has been regularly
upgrading its facilities from diagnostic and therapeutic
angles in all the specialties. The hospital when started
in 1942 had only 204 beds, which has now increased
to 1531 beds. The hospital provides medical care to
millions of citizens not only of Delhi but also the
neighboring states.
Staff Position (Sanctioned)
i. Medical Officers and Specialists 381
ii. No. of Resident Doctors 941
iii. No. of Nurses 1292
iv. No. of Para Medical staff 758
v. No. of Ministerial staff 347
vi. No. of Group 'D' staff 1451
TOTAL 5170
172
ANNUAL REPORT 2008-09
The hospital runs many specialties, super-specialties
and special clinics like Neurology, Urology, CTVS,
Nephrology, Respiratory Medicine, Burns & Plastics,
Pediatric Surgery, Gastroenterology, Cardiology,
Arthroscopy and Sports Injury clinic, Diabetic Clinic,
Thyroid Clinic. Further, it has two Whole Body CT
Scanner,MRI, Colour Doppler, Digital X-ray, Cardiac
Cath. Lab. A Homoeopathic OPD and Ayurvedic OPD
are also running within this hospital premises.
Training and Teaching
Teaching of post-graduate degree and / or diploma
to the students of Delhi/IP University in the
Departments of Medicine, Surgery, Orthopedics,
Obstetrics and Gynaecology, Paediatrics,
Anaesthesia, Radiology, Radiotherapy, Ophthalmo-
logy, ENT, Dermatology and Rehabilitation is
undertaken. Every year 2 students are enrolled in
the department of Burns & Plastic Suregery and 1
student in the Department of CTVS for M.Ch.
courses. Every year 46 MD, MS and 37 Diploma
students are enrolled. Training of DNB students
through National Board of Examination in the
departments of Medicine, Surgery, Orthopaedics,
Obstetrics and Gynaecology, Paediatrics,
Anaesthesia, Radiology, Radiotherapy, Ophalmo-
logy, ENT, Dermatology and Rehabilitation, Urology,
CTVS, Paed.-Surgery, Neuro-Surgery is undertaken
and DNB training is going to start from session
January 2009 in the department of Cardiology and
Resp. Medicine.
The college has started a PhD course in Physiology
from this academic year. The regular courses are
also being run for Nurses Training, Medical Lab.
Technology (MLT) apprenticeship; Diploma in Lab
Technology; Pre-hospital trauma Technician course
and courses in pharmacy. Medical Record Technician
(MRT) and Medical Record Officer training,
Physiotherapy training, O.T. Assistants training and
Short term laboratory training programs for all MLT
are being conducted regularly.
School of Nursing has been upgraded to College of
Nursing which has admitted 1st Batch of 100 students
this year for a 3 year Degree Course and is affiliated
with I.P. University.The hospital is also conducting
short-term courses for Medical and paramedical
personnel sponsored by various Central and State
organizations to update their knowledge and
skills.The hospital has been selected by the
Directorate General to give training to para medical
staff working in the Government of India, placed at
various peripheral center. Besides the above, the
hospital is an WHO approved center for training and
observer-ship in various discipline. OBC reservation
has been given in Post Graduate Course.
Web Site
VMMC & Safdarjang Hospital had launched its web
site (www.vmmc-sjh.nic.in) which was inaugurated on
17.09.2002 by the then Union Health Minister, Shri
Shatrughan Sinha. The website has been recently
redesigned and upgraded. The new website was
launched July 2008. The new website is more user
friendly and is regularly upgraded by specially trained
staff of the hospital.
OPD Services
The hospital has an ever increasing attendance of
21,17,201 in the year 2006 -2007 i.e. @ 7056 per
working day of patients in the OPD. To cater to this
load and for convenience of the patients a new OPD
Block was commissioned in August, 1992. All
departments run their OPD in the new OPD block.
There are several disciplines for which the OPD
services are provided daily. The OPD complex has
a spacious registration hall with 18 registration
windows. The OPD registration services have been
computerized and the new system is functional since
mid February 2005. The first floor of the OPD
complex caters to the department of G. Medicine and
allied super-specialties; the second floor caters to
the Department of General Surgery and allied super-
specialties; the third floor is occupied by Pediatrics
and Homeopathy; the fourth floor houses the ENT &
Eye OPD's and the fifth floor is occupied by the
Department of Skin & STD. The out - patient
attendance for the last 5 years are as under (Jan toDec):
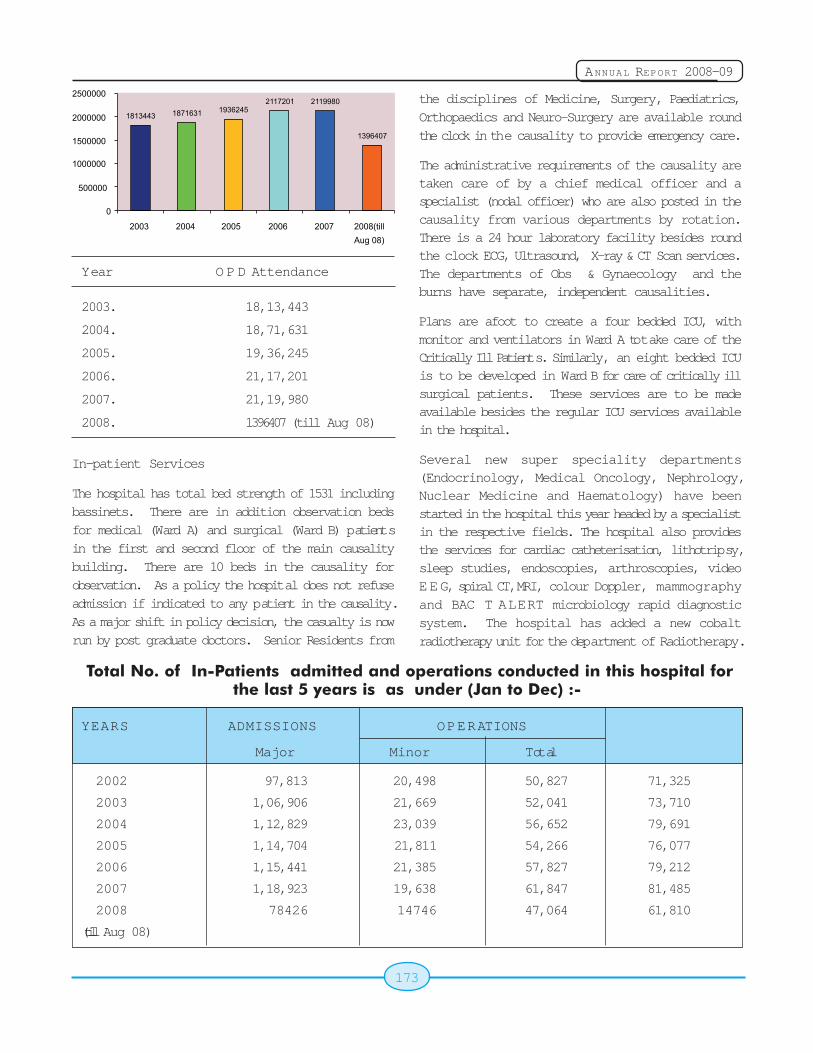
173
ANNUAL REPORT 2008-09
Year O P D Attendance
2003. 18,13,443
2004. 18,71,631
2005. 19,36,245
2006. 21,17,201
2007. 21,19,980
2008. 1396407 (till Aug 08)
In-patient Services
The hospital has total bed strength of 1531 includingbassinets. There are in addition observation bedsfor medical (Ward A) and surgical (Ward B) patientsin the first and second floor of the main causalitybuilding. There are 10 beds in the causality forobservation. As a policy the hospital does not refuseadmission if indicated to any patient in the causality.As a major shift in policy decision, the casualty is nowrun by post graduate doctors. Senior Residents from
the disciplines of Medicine, Surgery, Paediatrics,Orthopaedics and Neuro-Surgery are available roundthe clock in the causality to provide emergency care.
The administrative requirements of the causality aretaken care of by a chief medical officer and aspecialist (nodal officer) who are also posted in thecausality from various departments by rotation.There is a 24 hour laboratory facility besides roundthe clock ECG, Ultrasound, X-ray & CT Scan services.The departments of Obs & Gynaecology and theburns have separate, independent causalities.
Plans are afoot to create a four bedded ICU, withmonitor and ventilators in Ward A to take care of theCritically Ill Patients. Similarly, an eight bedded ICUis to be developed in Ward B for care of critically illsurgical patients. These services are to be madeavailable besides the regular ICU services availablein the hospital.
Several new super speciality departments(Endocrinology, Medical Oncology, Nephrology,Nuclear Medicine and Haematology) have beenstarted in the hospital this year headed by a specialistin the respective fields. The hospital also providesthe services for cardiac catheterisation, lithotripsy,sleep studies, endoscopies, arthroscopies, videoEEG, spiral CT, MRI, colour Doppler, mammographyand BAC T ALERT microbiology rapid diagnosticsystem. The hospital has added a new cobaltradiotherapy unit for the department of Radiotherapy.
Total No. of In-Patients admitted and operations conducted in this hospital forthe last 5 years is as under (Jan to Dec) :-
YEARS ADMISSIONS OPERATIONS
Major Minor Total
2002 97,813 20,498 50,827 71,325
2003 1,06,906 21,669 52,041 73,710
2004 1,12,829 23,039 56,652 79,691
2005 1,14,704 21,811 54,266 76,077
2006 1,15,441 21,385 57,827 79,212
2007 1,18,923 19,638 61,847 81,485
2008 78426 14746 47,064 61,810
(till Aug 08)
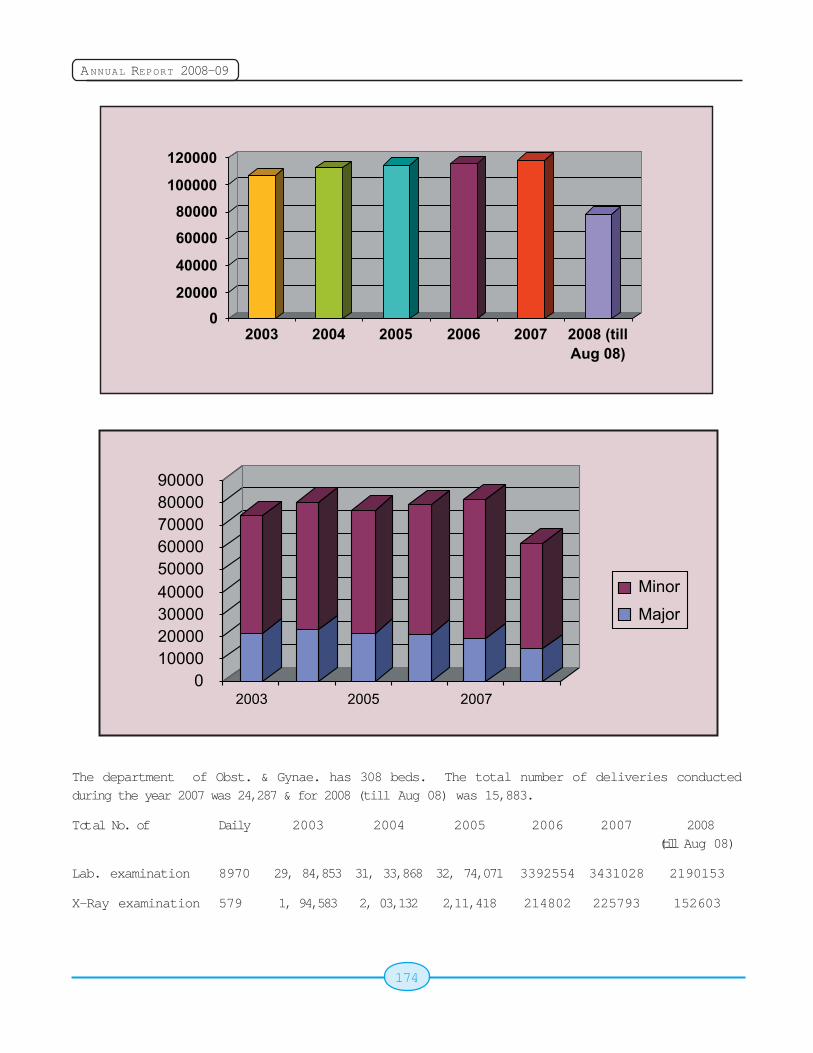
174
ANNUAL REPORT 2008-09
The department of Obst. & Gynae. has 308 beds. The total number of deliveries conductedduring the year 2007 was 24,287 & for 2008 (till Aug 08) was 15,883.
Total No. of Daily 2003 2004 2005 2006 2007 2008(till Aug 08)
Lab. examination 8970 29, 84,853 31, 33,868 32, 74,071 3392554 3431028 2190153
X-Ray examination 579 1, 94,583 2, 03,132 2,11,418 214802 225793 152603
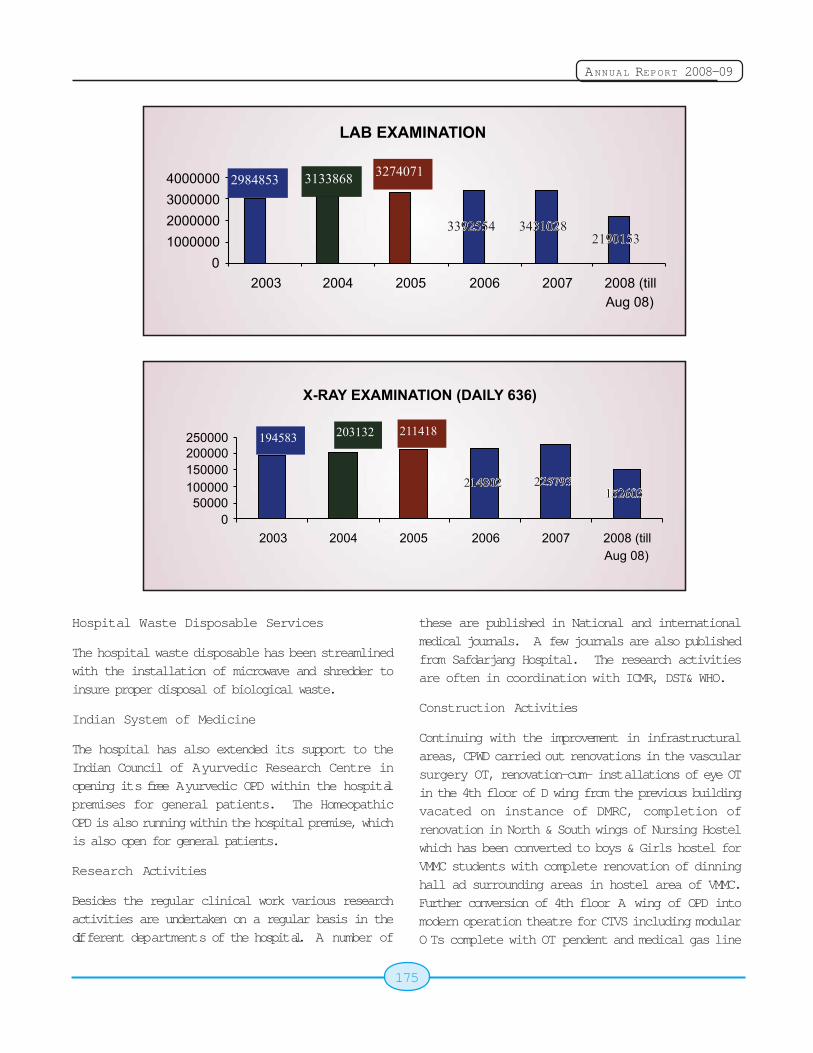
175
ANNUAL REPORT 2008-09
Hospital Waste Disposable Services
The hospital waste disposable has been streamlinedwith the installation of microwave and shredder toinsure proper disposal of biological waste.
Indian System of Medicine
The hospital has also extended its support to theIndian Council of Ayurvedic Research Centre inopening its free Ayurvedic OPD within the hospitalpremises for general patients. The HomeopathicOPD is also running within the hospital premise, whichis also open for general patients.
Research Activities
Besides the regular clinical work various researchactivities are undertaken on a regular basis in thedifferent departments of the hospital. A number of
these are published in National and internationalmedical journals. A few journals are also publishedfrom Safdarjang Hospital. The research activitiesare often in coordination with ICMR, DST& WHO.
Construction Activities
Continuing with the improvement in infrastructuralareas, CPWD carried out renovations in the vascularsurgery OT, renovation-cum- installations of eye OTin the 4th floor of D wing from the previous buildingvacated on instance of DMRC, completion ofrenovation in North & South wings of Nursing Hostelwhich has been converted to boys & Girls hostel forVMMC students with complete renovation of dinninghall ad surrounding areas in hostel area of VMMC.Further conversion of 4th floor A wing of OPD intomodern operation theatre for CTVS including modularO Ts complete with OT pendent and medical gas line
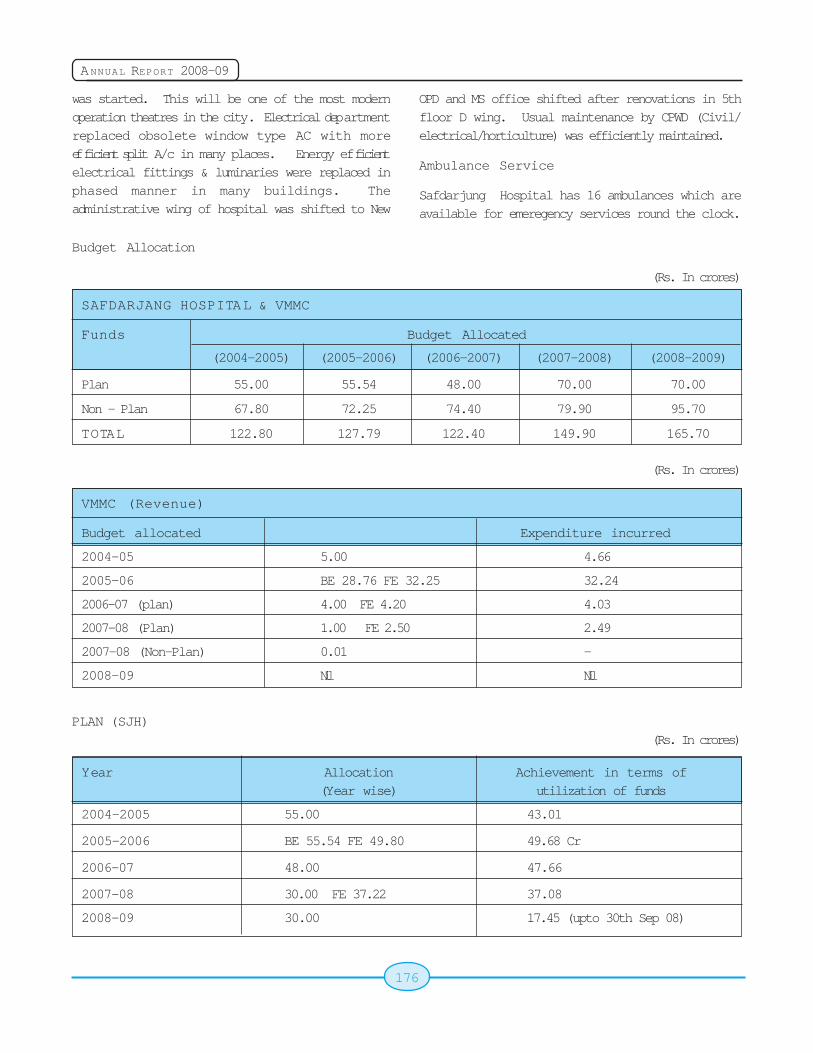
176
ANNUAL REPORT 2008-09
was started. This will be one of the most modernoperation theatres in the city. Electrical departmentreplaced obsolete window type AC with moreefficient split A/c in many places. Energy efficientelectrical fittings & luminaries were replaced inphased manner in many buildings. Theadministrative wing of hospital was shifted to New
OPD and MS office shifted after renovations in 5thfloor D wing. Usual maintenance by CPWD (Civil/electrical/horticulture) was efficiently maintained.
Ambulance Service
Safdarjung Hospital has 16 ambulances which areavailable for emeregency services round the clock.
Budget Allocation
(Rs. In crores)
SAFDARJANG HOSPITAL & VMMC
Funds Budget Allocated
(2004-2005) (2005-2006) (2006-2007) (2007-2008) (2008-2009)
Plan 55.00 55.54 48.00 70.00 70.00
Non - Plan 67.80 72.25 74.40 79.90 95.70
TOTAL 122.80 127.79 122.40 149.90 165.70
(Rs. In crores)
VMMC (Revenue)
Budget allocated Expenditure incurred
2004-05 5.00 4.66
2005-06 BE 28.76 FE 32.25 32.24
2006-07 (plan) 4.00 FE 4.20 4.03
2007-08 (Plan) 1.00 FE 2.50 2.49
2007-08 (Non-Plan) 0.01 -
2008-09 Nil Nil
PLAN (SJH)(Rs. In crores)
Year Allocation Achievement in terms of(Year wise) utilization of funds
2004-2005 55.00 43.01
2005-2006 BE 55.54 FE 49.80 49.68 Cr
2006-07 48.00 47.66
2007-08 30.00 FE 37.22 37.08
2008-09 30.00 17.45 (upto 30th Sep 08)
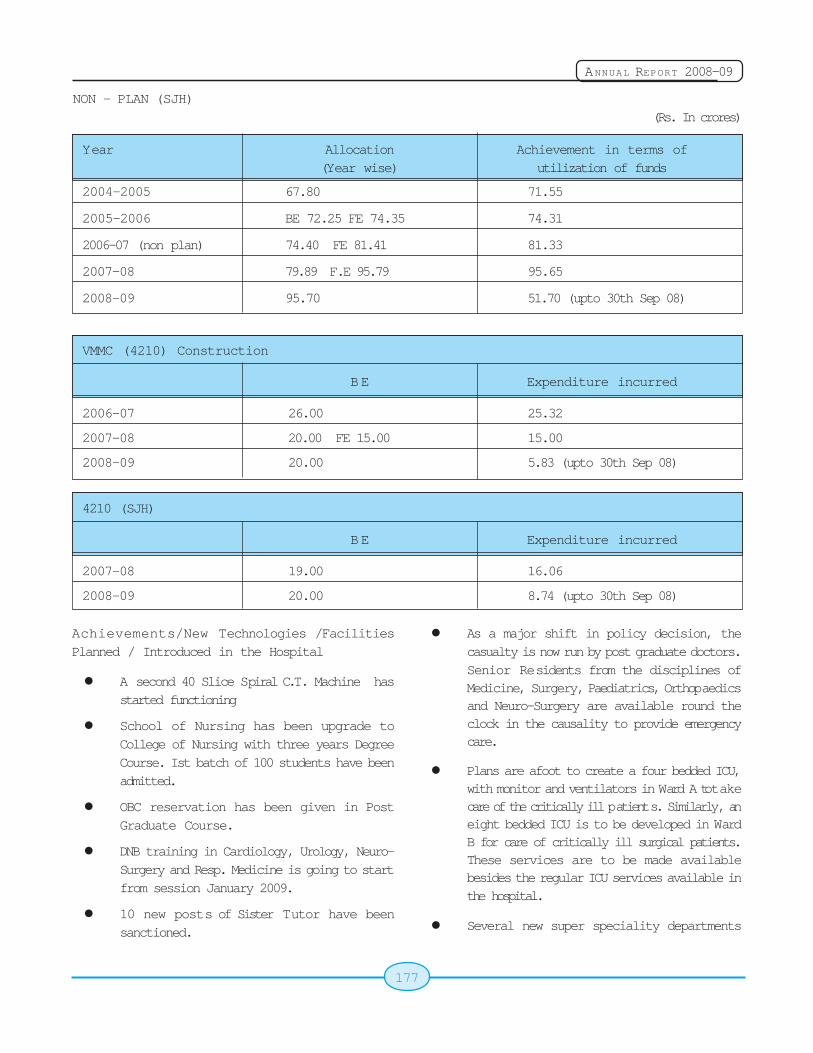
177
ANNUAL REPORT 2008-09
NON - PLAN (SJH)(Rs. In crores)
Year Allocation Achievement in terms of(Year wise) utilization of funds
2004-2005 67.80 71.55
2005-2006 BE 72.25 FE 74.35 74.31
2006-07 (non plan) 74.40 FE 81.41 81.33
2007-08 79.89 F.E 95.79 95.65
2008-09 95.70 51.70 (upto 30th Sep 08)
VMMC (4210) Construction
BE Expenditure incurred
2006-07 26.00 25.32
2007-08 20.00 FE 15.00 15.00
2008-09 20.00 5.83 (upto 30th Sep 08)
4210 (SJH)
BE Expenditure incurred
2007-08 19.00 16.06
2008-09 20.00 8.74 (upto 30th Sep 08)
Achievements/New Technologies /FacilitiesPlanned / Introduced in the Hospital
! A second 40 Slice Spiral C.T. Machine hasstarted functioning
! School of Nursing has been upgrade toCollege of Nursing with three years DegreeCourse. Ist batch of 100 students have beenadmitted.
! OBC reservation has been given in PostGraduate Course.
! DNB training in Cardiology, Urology, Neuro-Surgery and Resp. Medicine is going to startfrom session January 2009.
! 10 new posts of Sister Tutor have beensanctioned.
! As a major shift in policy decision, thecasualty is now run by post graduate doctors.Senior Residents from the disciplines ofMedicine, Surgery, Paediatrics, Orthopaedicsand Neuro-Surgery are available round theclock in the causality to provide emergencycare.
! Plans are afoot to create a four bedded ICU,with monitor and ventilators in Ward A to takecare of the critically ill patients. Similarly, aneight bedded ICU is to be developed in WardB for care of critically ill surgical patients.These services are to be made availablebesides the regular ICU services available inthe hospital.
! Several new super speciality departments
178
ANNUAL REPORT 2008-09
(Endocrinology, Medical Oncology,Nephrology, Nuclear Medicine andHaematology) have been started in thehospital this year headed by a specialist inthe respective fields.
! Upgradation of one of the Ambulances withAdvance Life Support System is underprocess.
! All Cardiac Surgeries are done free, patientshave to pay only the cost of implants.
! Angiography and Dialysis has been madenearly free to all poor patients.
! Number of seats increased in PG/DiplomaCourses.
! 250 rooms hostel in under construction andwill be completed in this financial year.
! Animal House of Pharmacology Sanction hasbeen given and in progress or underconstruction.
! Lay out of Internet lane is under process.
! OT IInd floor is renovated.
! EOT is under renovation.
! 170 rooms in the hostel have been renovatedand are occupied by girl students.
! Semester system has been started in MedicalCollege.
! Post Doctoral Course in (M.Ch. CardiacSurgery) has been started.
13.4 Dr. Ram Manohar Lohia Hospital
Backgrounder
The Hospital, originally known as Willingdon Hospitaland Nursing Home, renamed as DR. RAM MANOHARLOHIA HOSPITAL, was established by the BritishGovernment in the year 1933. The hospital has thussurpassed over 75 years of its existence and alsoemerged as a Centre of Excellence in the HealthCare under the Government Sector Hospitals. Its
Nursing Home was established during the year 1933-35 out of donations from His Excellency Marchionerof WILLINGDON. Later, its administrative control wastransferred to the New Delhi MunicipalCommittee(NDMC). In the year 1954, this hospitalwas taken over by the Central Government. In therecent past, the Old Building portion of the hospitalhas been declared as a Heritage Building.
Starting with 54 beds in 1954, the hospital expandedto meet the ever-increasing demand on its servicesand now is a 1074 bedded hospital, spread over anarea of 34 acres of land. The hospital caters to theneeds of C.G.H.S. beneficiaries and Hon'ble MPs,Ex-MPs, Ministers, Judges and other V.V.I.P.dignitaries besides other general patients. Themandate of the hospital is to provide utmost patientcare and the hospital authorities are making all outefforts to fulfill the mandate for which it has beenset-up. The hospital is providing comprehensivepatient care including specialized treatment toC.G.H.S. beneficiaries and General Public. NursingHome facilities are available for entitled CGHSbeneficiaries. The Nursing Home is having 75 bedsfor the CGHS and other beneficiaries
The hospital is one of the most prestigiousGovernment Hospitals not only because of its centrallocation, near the Parliament House and in closeproximity to North and South Block where most ofthe V.V.I.Ps stay but also because of availability ofexpertise and super specialties. The Government ofIndia has chosen this Hospital for NABH accreditation,an international hallmark for health care serviceprovider, through the Quality Council of India (QCI).The accreditation application is being made to QCIshortly for undertaking inspection to get theaccreditation and to become the first CentralGovernment Hospital.
The hospital annually provides health care servicesto approximately 14 lacs outdoor patients and admitsaround 50000 patients indoor. About 1.5 lacspatients are attended in the Emergency and CasualtyDepartment annually. The hospital has round-the-clock emergency services and does not refuse anypatient requiring emergency treatment irrespectiveof the fact that beds are available or not. All the
179
ANNUAL REPORT 2008-09
services in the hospital are free of cost except NursingHome treatment and some nominal charges forspecialized tests.
The Services Available
The hospital provides services in the followingSpecialties and Super Specialties covering almostall the major disciplines:
Clinical Services
" Accident & Emergency Services
" Anesthesia Services
" Dermatology
" Eye
" ENT
" Family Welfare
" General Medicine
" General Surgery
" Gynecology & Obstetrics
" Orthopedics
" Pediatrics
" Psychiatry
" Physiotherapy
! Dental
Super Speciality Departments / Units
" Neuro-Surgery
" Burns & Plastic Surgery
" Cardiology
" Cardio Thoracic & Vascular Surgery
" Gastroenterology
" Neurology
" Pediatrics Surgery
" Urology
" Nephrology
" Endocrinology
Departmental Special Clinics
" Diabetic Clinic
" Asthma Clinic
! Pre Anesthetic Clinic
! ART Clinic
! ARC Clinic
Paediatrics & Neonatology Speciality Clinics
" Neonatology & Well Baby Clinic
" Follow - up clinic
" Neurology Clinic
" Nephrology Clinic
" Rheumatology Clinic
" Asthma Clinic
" Thalassemia clinic
" Nutrition Clinic
Gynecology & Obstetrics
" Antenatal Clinic
" Infertility Clinic
Psychiatry
" Child Guidance Clinic
" Drug De-addiction Clinic
" Marriage counseling
" Psycho-Sexual Clinic
! Geriatric Psychiatry Clinic
! Yoga Centre for cardiac and other patients
Skin
" Leprosy Clinic
" Leukoderma
Eye
I.O.L
" Glaucoma
" Retina
180
ANNUAL REPORT 2008-09
Dental
" Dental Fracture
Unani OPD (Daily)
Diagnostic Services
" Hematology
" Pathology
" Microbiology
" Histopathology & Cytology
" Biochemistry
" Radiology including CT Scan, digital X-ray,Color Doppler, Ultrasound & MRI
" Blood Bank
Support Services
State of the art Library
" C.S.S.D
" Laundry
" Pharmacy
" Bank
" Post Office
" ISD, STD, PCO Booth
! Mortuary including Hearse Van
! Hospital Waste Management Facilities
! Departmental Canteen
! Ambulance Services
Emergency & Trauma Care Services
This hospital has well- established Emergencyservices including round- the-clock services inMedicine, Surgery, Orthopedic and Paediatrics whileother specialties are also available on call basis. Allservices like laboratory, X-Ray, CT-Scan, Ultra-sound,Blood Bank and Ambulances are available round theclock. A well established Coronary Care Unit (CCU)and an Intensive Care Unit (ICU) exist in the hospitalfor serious Cardiac and Non-Cardiac patients. TheCoronary Care Unit of the hospital has been
completely renovated recently with new equipmentsand infrastructure. The hospital has a well laid downdisaster action plan & disaster beds, which are made
operational in case of mass casualties and disasters.
A Disaster Management Unit is also functioning in
the Casualty Department to attend the serious
patients with the desired care. The hospital handled
meticulously victims including the serious patients
during the serial blasts in Delhi in 2005 & 2008.
They were treated and managed very well which
brought appreciation from the Media and the people
alike.
The Hospital has comprehensive trauma care facility
with 74 beds at the Trauma Care Centre started in
March,2008 in readiness to shoulder the added
responsibility of providing comprehensive & timely
emergency medical care to victims of trauma in the
event of any accidents occurring in Delhi especially
in Lutyen's Delhi.
Sanitation & Beautification of HospitalCampus
The hospital has given high importance to the
sanitation and beautification of entire campus to
create a nature friendly ambience. Under a Special
Drive, remodeling of Plants, landscaping of Central
Park Lawns, relaying of grass, creation of Artificial
W ater Falls & Fountains and a beautiful Herbal
Garden in the Nursing Home Block to give a
refreshing look to the visitors and the patients alike.
Special Sanitation Drives are undertaken at regular
intervals to ensure proper cleanliness and hygienic
atmosphere in the hospital.
Recent Achievements of the Hospital
The following are the latest additions of the patient
care facilities in the hospital;
Resident Doctors' Hostel:The construction work
of the extension of Resident Doctor's Hostel for
additional rooms has been completed. With the
addition of these rooms (total 143 rooms), the
availability of resident doctors on duty in the campushas significantly improved.

181
ANNUAL REPORT 2008-09
Hyper baric Oxygen Chamber Therapy: Dr. RMLHospital is the only Government Hospital in Indiawhere facility of Hyper baric Oxygen Therapy exists.This therapy involves giving hundred percent oxygento body tissues at high pressure to treat the patientsof Head Injury, non-healing Ulcers, Post PlasticSurgery with excellent results. There are two Hyperbaric Chambers installed in the Department ofAnesthesia.
Anti Retroviral Therapy Centre: Anti RetroviralTherapy (ART) Centre has been started in thehospital under National AIDS Control Organisation(NACO) and assisted by WHO. This is helping theAIDS patients to get the treatment effectively andalso free medicines. Till now, this clinic has enrolled4637 patients and all the eligible 1464 clinicallyeligible patients are under treatment. A VoluntaryCounseling & Testing Centre (VCTC) for thescreening of patients for HIV has also been setup.
Department of Physical Medicine and Rehabilitation:A new Department of Physical Medicine andRehabilitation has also been started in 2008.
College of Nursing: The Hospital's School ofNursing set up in 1963 with 25 students capacity peryear has been upgraded into College of Nursingwith intake capacity of 50 students, at an estimatedproject cost of Rs.4.08 Crores from the year 2008-2009 in the Nurses Hostel of this hospital. TheConstruction work of the new campus of college hasalmost been completed by HSCC to shift it to newcampus in July, 2009.
Dharamshala: A Dharamshala for attendants ofpatients has been planned to be constructed on oneacre of land allotted to hospital near the Birla Mandirto help the attendants/relatives of the outpatientscoming from different parts of the country. Thedesigns /clearances have been approved &estimates are under approval.
Computerization: The computerization ofcentralized OPD Registration was started from 2005to facilitate the outdoor patients to get theirregistration done from any of the 16 Counters in theOPD Block. Four more counters are being added atdifferent locations to facilitate the timely registration
of outdoor patients and to reduce their waiting timein the hospital. There are separate RegistrationCounters opened for Senior Citizens, physicallyhandicapped persons and the staff. Thecomputerization of Accounts & Administration workhas also been started for easy retrieval of information/record. Only recently, NIC has undertaken thecomprehensive E-Hospital Project with approved costof 3.50 crores to cover all the activities under itsumbrella. OPD registration & Repeat visits, IPDregistration & ward allotment, Casualty registration,transfer and discharges under E-Hospital softwarehad been implemented. E-Hospital implementationcovering all aspects of patient care, Labs, HumanResources of the Hospital, Inventory control Systemfor the Hospital and IT induction in PGIMER areexpected to be completed by end of July, 09. Inaddition to the above, and implementation of LibraryManagement Software called e-Granthalaya andintroduction of e-Procurement System for the Hospitalare being planned. Moreover, a proposal fordigitization of entire medical record is also underconsideration.
Renovation of existing departments: Therenovation of the Department of Bio-Chemistry,Neuro-Surgery, Burns and Plastics, Anaesthesia,Emergency Block, Library, Nephrology, Physiotherapy,Family Welfare, Radiology, Psychiatry, Accounts, etchas been done to provide better infrastructure andworking condition for the patients and working staff.
Departmental Canteen has also been revampedsignificantly to provide cost effective food items tothe staff as well as the visitors coming to the hospital.Moreover, the Kiosks of Mother Dairy, Saras & Amulhave also been opened in the campus to facilitatethe availability of healthier and good quality food itemsin the campus at reasonable rates.
Improvements in the Services: The hospital hasfocused attention towards the patient care andimproved services. Many new and sophisticated typesof equipment have been procured in the hospital toupdate the hospital services.
These equipments include Julabo Shaking WaterBath, Video Gastroscope, Pressure Dye Intector,

182
ANNUAL REPORT 2008-09
Patient Monitoring System, Blood Gas Analyser,Autoclave Electric Drill, X Ray Tube, CT Scanner,Laproscope set, hemodylasis Machine, LecialOperating Microscope, Echo Cardiography Machine,Color Doppler, Central Monitoring Station, 4 ICUVentilators, Bronchoscope, Fully Auto Blood CellCounter, Heart Lung Machines, 1000 MA DigitalRadiography System, 16 Spiral/Slice CT Scanners,Cardiac Cath Lab., Chemistry Analyzer, PatientMonitoring System, ICU Ventilators, OT Tables, OTLights. The approximate cost of these equipments isRs. 15.30 Crore.
The proposal for construction of additional floors etcin Laundry/ OPD Blocks is under consideration. Thecentralized CCTV based Surveillance System &Public Address Systems has been planned in thehospital during the year 2009-2010.
Upgradation of Library & Information System: In theage of knowledge and information, the hospital hasgiven the focused attention for providing the latestinformation in the field of Medical Sciences andResearch made at international levels. The prestigiousmedical journals(more than 1500) and books worthRs. 1 Crore have been purchased to facilitate thefaculty, students and staff to keep them abreast oflatest developments. A proposal for the digital libraryis also being started in the Hospital Library.
Focus on Environment: The hospital has givendue importance to the improved environment andeco-friendly solutions. The rain-water harvestingsystems in the major buildings of the hospital havebeen undertaken. A Tree Plantation Drive launchedin January 2008 involved the senior faculty and thestaff alike to plant more than 120 saplings forimproving greenery in the campus. A Bio-MedicalW aste Management system has been set up in thehospital. The Hospital has a sound Hospital WasteDisposal System. Two incinerators, one plasticshredding machine and one Micro Wave Unit existfor this purpose. A chemical de-contamination planthas also been completed and commissioned recently.
Citizen Charter & Public Grievance Redressal
The Hospital has adopted a Citizen Charter since1998 and as per the directives of Hon'ble High Court
of Delhi, Public Grievance Redressal Machinery hasalso been set up to inform the patients about thefacilities available and also redressal of theirgrievances, if any. There are 19 Complaint &Grievance Boxes placed at various strategiclocations which are opened periodically and put upbefore a High Powered Committee headed by aConsultant & HOD & reviewed by a Designated AddlMS and also by the Medical Superintendent. Thecomplainants are given an opportunity to speak inperson to the CMO in charge and a written reply ofthe outcome of the complaint is also sent to thecomplainant.
Post Graduate Institute of Medical Education &Research (PGIMER), DR. RML Hospital, NewDelhi
PG Courses in Medical Education have beencontinuing in Dr. RML Hospital for decades together.The students were sent by Delhi University forpursuing their PG Courses. With the growth of Dr.RML Hospital whereby the number of disciplinesincreased and Super-Specialities were added, aneed was felt to have a full-fledged Post GraduateInstitute of Medical Education & Research (PGIMER).EFC was submitted to the Government and it wasrecommended to construct a separate building withbudget allocation of over Rs. 60 crores. HospitalServices Consultancy Corporation (India) Limited(HSCC) was entrusted the task of construction ofPGIMER on a piece of approx. 4 acres of landadjoining the Hospital. The building constructed byHSCC(I) Ltd. comprises of Administrative Block,

183
ANNUAL REPORT 2008-09
Academic Block, Library Block, Examination Hall,State-of-art Auditorium having seating capacity of 400plus, Guest House, Cafetaria and other Conference/Seminar Halls, etc. The ambience of the Campus isconducive to the academic activities. VariousDepartments are holding their Seminars/Conferencesand other academic activities in the Conference &Meeting Rooms of PGIMER.
PG & Super- Speciality Seats:
EFC recommended 49 PG Degree/Diploma seats and20 seats in Super-Speciality courses for PGIMER. TheInstitute is presently affiliated to Guru Gobind SinghIndraprastha (GGSIP) University, Delhi. In the year2008, the Government sanctioned a total of 26 PGDegree/Diploma seats and 2 seats in Super-Specialitycourses. The Institute started functioning from theacademic year 2008-09 and all the seats sanctionedby the Government were filled up. Seats earmarkedfor reserved category including OBC candidates werealso filled up. Subsequently 9 additional PG Degree/Diploma seats have been sanctioned during this yearand they have been included for being filled up in thecurrent session 2009-10. A High Powered Committeeconstituted by DGHS also visited the Hospital in therecent past to examine the available infrastructure,bed strength and the existing faculty for makingrecommendations regarding the enhancement ofnumber of seats in PGIMER. The decision of theGovernment in this regard is awaited.
Faculty:
PGIMER is utilising the available faculty in Dr. RMLHospital for teaching of PG/Post Doctoral Students.During the year 2005, GGSIP University grantedEquated Teaching Designation to 107 Facultymembers in Dr. RML Hospital. With the existing facultybecoming eligible for enhancement/grant of equatedteaching designation, another proposal has beensent to the University for considering 61 more facultymembers for this purpose. We have yet to receivethe decision of the University in this regard.
Library:
Dr. RML Hospital Library was established in 1957.Year after year it made a steady and good progress.
After construction of the PGIMER building, which hasa separate Library Block having two Floors, theLibrary of Dr. RML Hospital has since been shifted inthat Block. There are 5 computers available in theLibrary for the use of faculty and students. 2 InternetConnections have also been provided for e-mailfacility.
It has collection of 26,000 medical books and 12,000bound journals. Annual intake of periodicals onvarious subjects is about 205 (both Indian andInternational).
The Library timings are :
Monday to Friday - 10.00 a.m. to 6.00 p.m.
Saturday - 10.00 a.m. to 2.00 p.m.Closed on OPD Holidays
Electronic Retrieval Medical (ERMED) Resourcesfacility is available. ERMED currently provides accessto a collection of 1500+ journals (Electronic + Print),from NML and other publishers. Aidop vodepCassettes amd CDs amd Xerox facility are alsoavailable in the Library.There is a separate readingroom where users can take their books and readingmaterial. Older editions of books and journals areissued to Members of the Library. SeparateDepartmental Libraries have also been provided toeach Department in PGIMER.
Financial Allocations: -
The financial allocations made to the hospital duringthe last five financial years are given in next page:
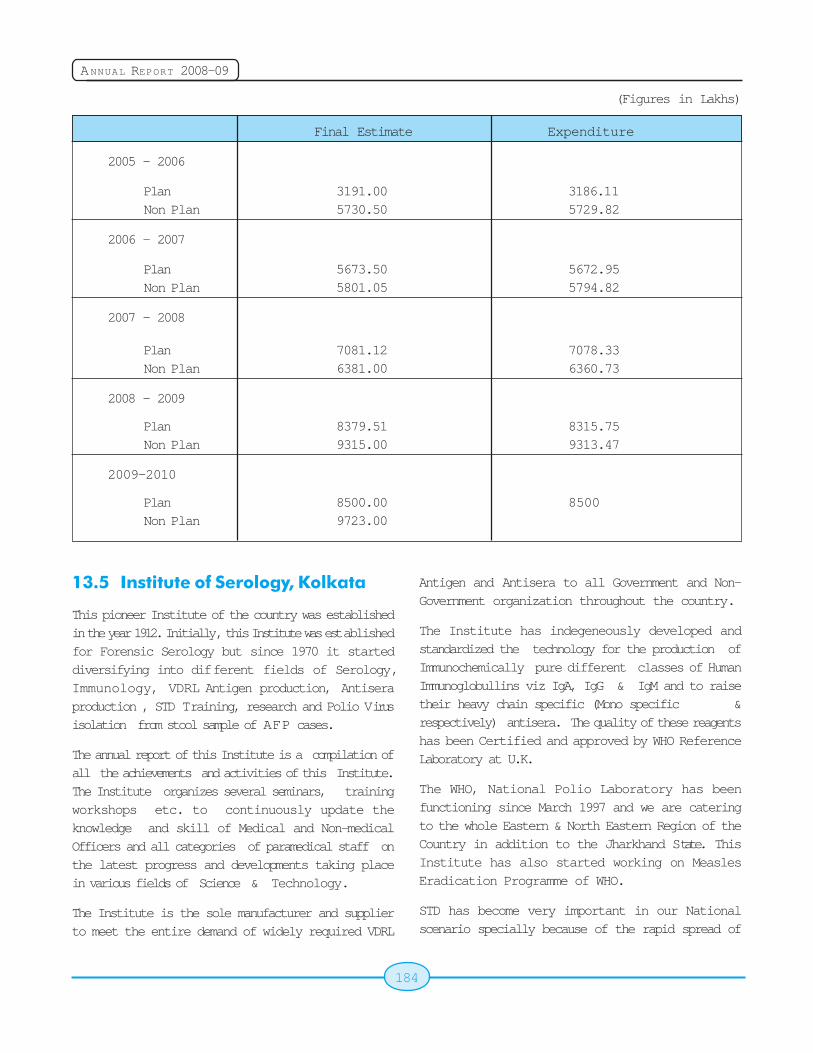
184
ANNUAL REPORT 2008-09
(Figures in Lakhs)
Final Estimate Expenditure
2005 - 2006
Plan 3191.00 3186.11Non Plan 5730.50 5729.82
2006 - 2007
Plan 5673.50 5672.95Non Plan 5801.05 5794.82
2007 - 2008
Plan 7081.12 7078.33Non Plan 6381.00 6360.73
2008 - 2009
Plan 8379.51 8315.75Non Plan 9315.00 9313.47
2009-2010
Plan 8500.00 8500Non Plan 9723.00
13.5 Institute of Serology, Kolkata
This pioneer Institute of the country was establishedin the year 1912. Initially, this Institute was establishedfor Forensic Serology but since 1970 it starteddiversifying into different fields of Serology,Immunology, VDRL Antigen production, Antiseraproduction , STD Training, research and Polio Virusisolation from stool sample of AFP cases.
The annual report of this Institute is a compilation ofall the achievements and activities of this Institute.The Institute organizes several seminars, trainingworkshops etc. to continuously update theknowledge and skill of Medical and Non-medicalOfficers and all categories of paramedical staff onthe latest progress and developments taking placein various fields of Science & Technology.
The Institute is the sole manufacturer and supplierto meet the entire demand of widely required VDRL
Antigen and Antisera to all Government and Non-Government organization throughout the country.
The Institute has indegeneously developed andstandardized the technology for the production ofImmunochemically pure different classes of HumanImmunoglobullins viz IgA, IgG & IgM and to raisetheir heavy chain specific (Mono specific &respectively) antisera. The quality of these reagentshas been Certified and approved by WHO ReferenceLaboratory at U.K.
The WHO, National Polio Laboratory has beenfunctioning since March 1997 and we are cateringto the whole Eastern & North Eastern Region of theCountry in addition to the Jharkhand State. ThisInstitute has also started working on MeaslesEradication Programme of WHO.
STD has become very important in our Nationalscenario specially because of the rapid spread of
185
ANNUAL REPORT 2008-09
HIV/AIDS infection in the country . STD and AIDS isa global problem that the country is facing today.Regional STD Reference Laboratory for EasternZone under NACO was established in this Institute.We are the regional STD Co-ordinator for Eastern &North Eastern Region for laboratory diagnosis ofSexually Transmitted Diseases and to extend ourlaboratory support to other Government and Non-Government organizations. Furthermore, thislaboratory conducts inter-laboratory Evaluation ofVDRL test with other laboratories of Kolkata. Thelaboratory is also working in STD interventionprogramme and work in collaboration with STD clinicsof different medical colleges of Kolkata amongst highrisk population. We also impart STD training forlaboratory Technicians, conduct research activitiesin this field.
Chief Objectives & Newer Activities
! Production & supply of various diagnosticreagents like VDRL Antigen, specific Antiseraetc. to the Government and Non-GovernmentInstitution all over the country.
! To undertake blood group serology , and tooffer expert opinion about different types ofMedico-legal exhibits or biological materialssend to this Laboratory and to resolvepaternity dispute or maternity questioned.
! To establish this department as fore runnerin the country in the field of Serology,Immunology, Virology and Quality Assurancewith products of various Antisera, VDRLAntigen, Anti-H Lectin, Anti-A1 Lectin andCoomb's reagent.
! Preparation, standardization andcharacterization of Heavy Chain specificantisera against human IgG, IgA and IgMrespectively and IgG specific antisera againstdifferent animals.
! Training of Laboratory Technicians in variousfields of serology and Sexually TransmittedDiseases and imparting training in ForensicSerology to different scientists and Policepersonale.
! To involve our department with National &State run health projects where ourlaboratory's role is very useful.
! Isolation of Polio Virus from stool samples ofsuspected Polio cases from whole EasternRegion as part of surveillance of Pulse PolioImmunization.
! To provide Laboratory support to STD andother projects.
Our Plan
! To develop Polymerase Chain Reaction(PCR) technique in the Institute, for thediagnosis of various diseases.
! To start Serological tests for diagnosis ofdengue.
The Institute has the following infrastructure forperforming specialized jobs. These are:-
Forensic Serology Section
i) M.L.-I
ii) M.L.-II
Antigen Production Unit for production of VDRLAntigen.
Antisera Production Unit.
Immunology & Immunochemistry Division.
! Immunochemistry division is engaged in theFractionation, Characterization andStandardization of different classes ofImmunochemically pure humanimmunoglobulin fractions and to raise theirmonospecific antisera (Heavy Chain).
! To raise the IgG specific antisera againstdifferent Animal species.
Quality Assurance & Control and Inter-laboratory Evalustion Laboratory.
STD Serology: -
! VDRL Laboratory

186
ANNUAL REPORT 2008-09
! Regional STD Reference Center.
Regional STD Training & Research Center underNACO
! Clinical Room
! Microscopy Room
! Regional STD Reference Laboratory
National Polio Laboratory under WHO
At the behest of National Immunization Mission,
Department of Family Welfare this Institute has also
taken up the assignment of Isolation of Polio Virus
from stool samples of suspected AFP cases from
March 1997.
Measles Eradication Programme of WHO:
Our Institute has started working on this
programme of WHO
W ashing & Sterilization Section.
Animal House.
Hindi Section
Training Division
! Conference Room.
! Library.
! Audiovisual & Health Education.
! Student Laboratory, Seminar Room,
Demonstration Room.
13.6 Indian Red Cross Society
The Indian Red Cross Society (IRCS) is the largest
autonomous humanitarian organization of India. It is
a huge family of 12 million volunteers and members
and staff exceeding 3500. It reaches out to the
community through 700 branches spread through
out the country. With a variety of activities in health,
disaster and organizational development, it is also
working towards achieving the Global Agenda and
Millennium Development goals.
IRCS is a recognised force in the disastermanagement sector in the South Asia region. Duringthe floods of 2008 it released relief items to the tuneof Rs. 7.5 crores to the affected States. It alsodeployed Water & Sanitation Units in the flood-affected states of Assam & Bihar for providing cleandrinking water. 5000 to 10,000 litres of clean drinkingwater can be made available within one hour with
the help of a single unit, which would suffice to theneeds of 10,000 beneficiaries per day. It alsosucceeded in establishing video-conferencingsystem in Red Cross State Branches 11 most disasterprone States and six IRCS regional warehouses.
During the reporting period, the focus in the field ofhealth continued on: (i) HIV; (ii) voluntary non-remunerated blood donation; (iii) emergency healthand (iv) community- based health. HIV interventions

187
ANNUAL REPORT 2008-09
included prevention, care and support, as well asanti-stigma and anti-discrimination initiatives. It hasscaled up services in line with the commitment madeunder the Global Alliance on HIV. Efforts have beenintensified to establish IRCS blood banks in stateCapitals and modernization of the existing blood bankat the National Headquarters. During the reportingperiod the blood bank at the National Headquartersorganized 291 blood donation camps and collected26169 units of blood out of which replacementdonation was 4374, voluntary accounted to 19565and in-house 2228. Public health in emergenciestrainings and workshops were conducted to addressthe preparation and response mechanisms and tostrengthen the capacity of the IRCS and targetedcommunities. Brochures and pamphlets were revisedand printed on bird flu and polio. IRCS alsocollaborated with National Legal Services Authorityin organizing Judicial Colloquium for the survivors oftrafficking and HIV/AIDS.
Under the capacity building and organizationaldevelopment, focus was on human resourcedevelopment. Policy and guidelines have beendrafted to facilitate recruitment and management ofvolunteers. During the reporting period, vehicleswere provided to the Red Cross branches for theirrelief and welfare activities.
The National Headquarters in cooperation withInternational Committee of the Red Cross tookforward emblem seminars to minimize the misuse ofRed Cross Emblem, Conflict Preparedness First Aid
programmes and Mine Risk Education trainingprogramme at State/District level. Under RestoringFamily Links 107 Red Cross Messages weredelivered to the addressees. In the reporting yearthere were 24 active tracing cases out of which 12cases were successfully closed and for the rest FNSdepartment is doing continuous follow-up with thebranches and other National Societies.
Post Graduate Diploma Course in DisasterPreparedness and Rehabilitation started in 2006-07 with 27 students enrolled, 35 students in the 2ndbatch and 40 students are undergoing the course inthe current batch.
The Society has launched Anjar IntegratedEarthquake Recovery Project and Tamil NaduIntegrated Community Recovery Programme.
During the reporting period the Society is in theprocess of developing a new strategic plan for 2009-12, wherein priorities and focus are on strengtheningactivities in areas such as disaster management,health care, organizational development andhumanitarian values.
13.7 St. John Ambulance for the Year2006-07
St. John Ambulance functions as a network spreadall over the country with approximately 680 State/UT/Railway Centres formed in different states,security forces, railways etc.
Its activities are carried through the Association Wingand Brigade Wing. While the Association Wing carriesout the instructional work in first aid and alliedsubjects, membership drive, training and enrolmentof lecturers, formation of new Centres etc., theBrigade Wing is a dedicated body of trained first aidvolunteers who provide first-aid cover, on demand,wherever and whenever needed.
Association Wing
Instructional Work: The State/Railway/UT Centresorganized training classes in which 5,74,445 personsqualified for proficiency certificates in First Aid, HomeNursing, Hygiene & Sanitation, Mother Craft & Child
188
ANNUAL REPORT 2008-09
Welfare etc. 16,713 persons were re-examined infirst aid/home nursing.
Membership: During the period 579 membershipcertificates were issued in favour of membersenrolled in State/UT Centres.
Lecturers Training Courses: The State/UT Centrescontinued to organize training courses to enhancethe panel of lecturers on the approved list of theNational Headquarters. Sixty six revalidated and 363new lecturers' certificates were issued.
The National Council, which met on 04.12.2007,approved the formation of the new UT Centre inDadra & Nagar Haveli, 1 district center in WestBengal and 2 district and 15 taluk centers inKarnataka.
The Brigade
The Brigade Wing functions as a para-medical forceto provide first aid and transportation service to thesick and wounded through first-aid posts set-up bythem. The other activities of the Brigade Wing weresetting up of eye and health camps, setting up specialfirst-aid posts on the occasion of Republic day,Independence day, Rath Yatra, Trade Fair, theInternational Fairs and other public congregations.
During the period under report, 23 Ambulance, 5Nursing, 1 Cadet Ambulance and 3 Cadet Nursinggroups were formed with the strength of 798volunteers. The Commissioner-in-Chief, St.JohnAmbulance Brigade, approved the appointment of64 officers in different positions in Delhi, Karnataka,Orissa, Punjab, Uttar Pradesh, West Bengal,Northern Railway, Southern Railway and RCFKapurthala Brigade District.
13.8 Emergency Medical Relief
Health Sector Disaster Management:
Ministry of Health & FW Emergency Medical ReliefDivision (EMR) of Directorate General of HealthServices, Ministry of Health & Family Welfare, Govt.of India is mandated for prevention, preparedness,mitigation and response on health sector disastermanagement activities and coordinates health
activities in terms of manpower and material logisticssupport to the states.
Preparedness Measures by EMR Division
Preparedness for disasters:
The Emergency Support Functions plan has beenupdated and circulated to all concerned. This ESFPlan contains the emergency support functionsassigned to the MOHFW which includes details ofnodal officers for coordination, crisis managementcommittee & quick response team at Hqrs. and fieldlevel, resource inventory etc. The ESF plan alsocontains instructions regarding deployment ofresources in the event of disasters. TheContingency Plan to combat droughts and floods wascirculated in the pre-monsoon period to all the States.
Preparedness for Avian Influenza
Ministry of Health and Family Welfare, Governmentof India took adequate measures to contain thehuman cases of Avian Influenza if it is to happen.The Joint Monitoring Group reviewed the situationand preparedness measures regularly. The Influenzasurveillance network under ICMR was strengthened.Actions have been initiated to develop NationalInstitute of Communicable Diseases as secondNational Influenza Centre. A national surveillance forInfluenza is being planned. The stockpile ofOseltamivir (Tamiflu) and personal protectiveequipments were maintained and reviewed.
Table Top Exercises were conducted for the Statesof southern regional to sensitize the State publichealth administrators/ and technical experts in AvianInfluenza / Pandemic Influenza preparedness andresponse and to assess the current level ofpreparedness, identify the gaps and review the Stateplan. Refresher training for Rapid Response teamswere conducted for the States of southern, northern,western and north-eastern region.
Influenza pandemic preparedness
The strategic plan for pandemic preparedness wasformalized earlier. IEC activities are being plannedand implemented in a phased manner.

189
ANNUAL REPORT 2008-09
Response
Deputation of Central Teams
Ministry of Health and Family Welfare was
represented in the central damage assessment
teams of the Ministry of Home Affairs which visited
flood affected state of Punjab and Bihar.
Bihar Floods:
Due to a breach in the river Kosi near Indo Nepal
border, its course changed and shifted over 120 km
eastwards. As a result, large areas of Supaul,
Madhepura, Katihar, Saharsa and Araria were
inundated and affected severely.
A high level central team after assessment
recommended strengthening the public health system
to prevent water borne, vector borne and respiratory
diseases. Accordingly, six public health teams were
deputed to worst affected districts to monitor public
health measures by conducting daily field visits.
There have been no disease outbreaks. The
activities included measles vaccination for the age
group of 6 months to 14 years, maternal healthcare
and vector control measures. All logistic support were
provided by supplying essential medicines [36
generic drugs] requested by the State Govt. To
strengthen public health measures items like 5 MT
of malathion, 100 fogging machines, diagnostic kits,
bednets, 2 crore chlorine tablets, 150 MT of bleaching
powder were supplied.
To support medical relief activities, 50 ambulances
were mobilized from Gujarat, Andhra Pradesh, Delhi
and Central Govt. Hospitals and deployed in the
affected areas for more than a month. Indian Red
Cross Society provided 12,000 family packs
[consisting of sarees, dhotis, towels, bed sheets,
mosquito nets, kitchen sets, blankets for each family
of 5 members]; 10,000 Tarpaulin sheets, 10,000
mosquito nets and 550 family tents and seven water
purification units.
Orissa Floods
Emergency medical supplies were provided asrequired by the State Government to meet the flood
situation. The public health situation was monitoredand there were no outbreak of diseases.
Advanced HAZMAT Life Support Training
Advanced HAZMAT Life Support (AHLS) is the mostcomprehensive training program available in USA toprovide the critical skills needed to treat victimsexposed to toxic substances and covers acts ofterrorism, industrial accidents, chemical spills etc.This program enables the hospital and pre-hospitalmedical professionals to be able to rapidly recognizethe symptoms of toxic exposure and immediatelyprovide appropriate treatment. This training coursewas organized in New Delhi from 5th to 9th March,2009. Two providers course led to training of 77doctors in AHLS. Twenty one of them have beenidentified for instructor course and trained.Instructors have been identified in apex traininginstitutes for future training. This training hasenhanced specialized capability in health sector forthe Commonwealth Games-2010.
Outbreak investigations and management
EMR division coordinated outbreak investigations inthe States of Manipur and West Bengal [childrendeaths], Gujarat and Andaman Nicobar Islands[leptospirosis] and Assam [Cholera]. Ministry of Health& F.W. deputed high level central team to the affectedareas and assessed the situation. The concernedstate governments were advised on prevention andcontainment measures.
Avian Influenza
Outbreak of Avian Influenza and actions takenby MOHFW West Bengal [January-May, 2008]
Department of Animal Husbandry, Dairying andFisheries, Govt. of India notified Avian Influenza inpoultry in Birbhum and Dakshin Dinajpur Districts on15th January, 2008 which spread to other areasinvolving fifteen districts namely Birbhum, DakshinDinajpur, Murshidabad, Nadia, Bankura, Malda,Cooch behar Burdwan, Hoogly, Howrah, Purulia,South 24 Parganas, Paschim Medinipore, Darjeelingand North 24 Parganas. In total 59 blocks and 6municipalities were involved. The containment
190
ANNUAL REPORT 2008-09
measures were instituted. A total of 70 epicentreswere notified by the DAHDF. The last outbreak wasnotified in Darjeeling District on 09.05.2008.
Active House to House Human Surveillance is overin all the Districts. In the earlier affected districts apopulation of about 42 lakh in 0-10 Kms werecovered under active surveillance. 428 Fever/ URIcases with exposure history were followed up. 30samples were tested. No suspect case wereidentified during active house to house surveillance.In these districts passive surveillance is maintainedto detect Influenza Like Illness [ILI].
MOHFW established a Sub-Office manned by NICDin ROHFW for better liaison with state Government.Apart from deploying Rapid Response Teams to allthe affected districts, Ministry of Health and F.W.supported the Government of West Bengal with 4.20lakh capsules of Oseltamivir, 6500 personal protectiveequipments, 6500 N-95 masks and 20 ventilators.For the surveillance and related activities MOHFWhas also provided a cash assistance of Rs. 173.00lakhs to the state Govt.
UNICEF translated the IEC materials (prepared byGovernment of India and UNICEF) to Bangla inconsultation with the State Govt. It has been telecastover prime channels as also aired over AIR and FMchannels. The posters have been duplicated by thestate Government for use at field level. Apart fromthe Central RRT teams providing hands on trainingto field teams at the operational level, MOHFWtrained a team of 30 physicians and 28microbiologists from the State of West Bengal atKolkata.
W est Bengal [December, 2008 -March, 2009]
Avian Influenza Outbreak was notified in Englishbazarblock, Malda District of West Bengal on 15.12.2008and in village Binay Krishnapally in Mathegara blockof Darjeeling district on 2.1. 2009. Further, outbreakswere notified in two villages namely Uttar Dankoba[block Mathabhanga-I], Nagar Bhagni [block Dinhata-I] in the district of Coochbehar, West Bengal on 30thJanuary, 2009, in Baramahar Village [blockHarirampur], district Dakshin Dinajpur on 17thFebruary, 2009, in Punding Forest Busty [block
Kurseong], district Darjeeling on 24th February, 2009in Bara Chenga Village [block Mirik], districtDarjeeling on 12th March, 2009 and in DasparaVillage [block Chopra], district Uttar Dinajpur on 27thMarch, 2009. Containment measures have beeninstituted and were completed. Adequate logisticswere available with the State Government.
Tripura [April, 2008]
Outbreaks were also notified in Tripura in BlockSalema [Village: Mohanpur], district Dhalai on07.04.2008, Village Hatearra; Block: Mohanpur[outbreak notified on 21.4.2008] and Village Nadilak,Block Bishalgarh [outbreak notified on 24.4.2008].Central Rapid Response Team has assisted the Statein containment procedures. MOHFW has supplied500 Personal Protective Equipments, 700 N-95masks, 10000 pieces of three layered surgicalmasks, 10000 capsules of Tamiflu and 2 ventilators.
Active House to House Surveillance were carried outon daily basis in 0-3 Km area and in rounds in 3-10Km area. Four Lakh population were covered underactive surveillance. A health facility near to theepicenter has been identified and strengthened tomanage human cases. About 5000 fever and UpperRespiratory Tract infection cases were monitored inthe 0-10 Km area. No suspected human case of avianinfluenza has been reported.
IEC activities were carried out in the operational areathrough miking and word of mouth communication.The media materials (TV Spots/ Radio Spots, Posters)prepared jointly by GOI and UNICEF and translatedinto Bangla for the Health authorities to run it in localchannels/ cable TV/ and AIR/ FM audio channel
Assam [November, 2008 - January, 2009]
Outbreak of Avian Influenza was notified in Assamon 27.11.2008 in Kamrup District. 17 otherepicenters, spread over eight districts have beennotified upto 24.12.2008. The containment measureswere instituted and over in epicenters initially notifiedand were continuing in other areas as on first weekof January, 2009. A cumulative population of about92 lakh in 0-10 Kms were covered under activesurveillance. 3108 Fever/ URI cases were identified

191
ANNUAL REPORT 2008-09
and followed up. No suspect cases were identifiedduring active house to house surveillance. 40,000capsules of Tamiflu, 12,000 surgical masks, 1200personal protective equipments, 400 N-95 masks,50 bottles of tamiflu syrup and 8 ventilators havebeen supplied by MoHFW. Sufficient anti-viral drugsand PPE were in stock with the State Government.Messages to create public awareness are beingtelecast/ broadcast in local channels and AIR. Localcampaign such as miking and interpersonalcommunication were followed in all epicenters.
Redressal of Pubilic Grievances
Grievance Redress Cell of EMR division receivescomplaints referred to it regarding negligence intreatment in three central Govt. hospitals. Thesecomplaints are examined, and action taken report iscommunicated to the complainant. One complaintwas received and enquiry report has been obtained.Complaints relating to medical treatment addressedto MOHFW received from the States/Union Territoriesis also dealt in this cell. Eleven complaints werereceived between April, 2008 to March, 2009 and
were sent to States/UTs concerned for necessaryaction.
Medical Care Arrangements on SpecialOccasions
Medical care arrangements were organised by the
Dte.G.H.S. for all the important national events which
includes Republic Day and Independence Day
celebrations and International Conferences etc.
Medical care arrangements were also made during
the State Visits of Heads of States and Distinguished
Guests of Greece, Mauritius, Hungary, Denmark,
United Kingdom, Maldives, Russian Federation,
Tanzania, Iran, Brunei Darussalam, Syria, Bhutan,
Lao PDR, Afghanistan, New Zealand, Nepal,
Palestine, Egypt and Belgium. Medical Care
arrangements were made during Third Summit of
India, Brazil and South Africa (IBSA) Dialogue Forum,
Second Summit of the BIMSTEC (Bay of Bengal
Initiative on Multisectoral, Technical and EconomicCooperation (BIMSTEC) and India - Africa ForumSummit.

192
ANNUAL REPORT 2008-09
193
ANNUAL REPORT 2008-09
Chapter 14
14.1 Prevention of Food AdulterationProgramme and Food Safety &Standards Act, 2006
Ministry of Health and Family Welfare is responsiblefor ensuring safe food to the consumers. This is donethrough the Prevention of Food Adulteration (PFA)Act 1954 and the PFA Rules 1955 made thereunder.The subject of the Prevention of Food Adulterationis in the concurrent list of the Constitution. However,in general, the enforcement of the Act is done by theState/U.T Governments. The Central Governmentprimarily plays an advisory role in its implementationbesides carrying out various statutory functions/duties assigned to it under the various provisions ofthe Act.
The Food Safety and Standards Act, 2006 (FSSA)was enacted to consolidate the laws relating to foodbeing administered by different Ministries /Departments and to establish the Food Safety andStandards Authority of India for laying down sciencebased standards for articles of food and to regulatetheir manufacture, storage, distribution, sale andimport, to ensure availability of safe and wholesomefood for human consumption and for mattersconnected therewith or incidental thereto. The Act,upon its full implementation, would replace the variousfood related laws including the PFA Act 1954 andthe PFA Rules 1955, as provided in its SecondSchedule of the FSSA.
As per the provisions of the Food Safety andStandards Act, 2006, the Food Safety and StandardsAuthority of India (the Food Authority), an autonomousorganisation under the Ministry of Health and FamilyWelfare, has been set up. Full body constitution of
the Food Authority with names of the Chairperson
and 22 members of the Authority has been notified
vide Ministry of Health & Family Welfare notification
S.O. No.2165 dated 5.9.2008. Shri P.I. Suvrathan, a
former Secretary to Government of India in the
Ministry of Food Processing Industries has been
appointed as the Chairperson of the Food Authority.
Shri G. Balachandran, IAS, Additional Secretary,
Ministry of Health and Family Welfare, was appointed
as its first Chief Executive Officer and Member-
Secretary of the Authority. Shri V.N. Gaur, IAS has
now replaced him as the next Chief Executive Officer
and Member-Secretary.
So far sections 3 to 18, 30, 81-88, 90-93 and 101 (a
total of 30 out of 101 sections) of the said Act have
already been enforced. As per the provisions of
section 90 of the said Act, employees of various
Ministries / Departments related with food laws,
including those of the PFA Division of DGHS under
this Ministry and various Central Food Testing
Laboratories, have been transferred to the Food
Authority. The Food Authority has already been
allocated separate budget by way of regular Grants-
in-Aid. The Food Authority has also been provided a
separate office building in FDA Bhavan, Kotla Road,
New Delhi.
New Food Labeling Provisions
New food labeling provisions notified vide notification
GSR 664 dated 19.9.2008 have come into effect w.e.f.
19.3.2009. However, an advisory has been issued
to the State Governments by this Ministry's letter
dated 19.3.2009 not to book cases of violation of
these provisions during the initial period of threemonths of their implementation.
Quality Control in Food & DrugsQuality Control in Food & DrugsQuality Control in Food & DrugsQuality Control in Food & DrugsQuality Control in Food & DrugsSector, Medical StoresSector, Medical StoresSector, Medical StoresSector, Medical StoresSector, Medical Stores
194
ANNUAL REPORT 2008-09
Notifications Amending the PFA Rules, 1955 duringthe year 7 draft notifications inviting public commentsrelating to amendments to the PFA Rules, 1955 and4 final notifications amending the PFA Rules, 1955have been published during the year 2008-2009.
14.2 CODEX
Since the signing of SPS and TBT agreements underthe WTO, the issue of International Trade in Foodhas become very important. Food Standards at theInternational level are set by the Codex AlimentariusCommission. The Codex Alimentarius Commissionwas created in 1963 by FAO and WHO to developfood standards, guidelines and related texts suchas codes of practice under the Joint FAO/WHO FoodStandards Programme. The main purposes of thisProgramme are protecting health of the consumersand ensuring fair trade practices in the food trade,and promoting coordination of all food standards workundertaken by international governmental and non-governmental organizations. India has participatedin the meetings of this Commission and has effectivelyadvocated the stand of the developing countriesregarding the process of standard setting so thattheir interests are kept in view. An attempt is beingmade to harmonise to the extent possible thestandards under the PFA Rules with Codex.
14.3 Central Drugs Standard ControlOrganisation (CDSCO)
The Central Drugs Standard Control Organization(CDSCO) in the Directorate General Health Servicesalong with Drug Control Organization in the Statesare responsible for safety, efficacy and quality ofdrugs, their import, manufacture, distribution, saleand standards. This is regulated under the Drugs &Cosmetics Act, 1940 and the Rules, 1945 made thereunder.
Drugs and Cosmetics (Amendment) ACT, 2008
The Drugs and Cosmetics (Amendment) Bill 2005providing for inter alia stricter penalties for offencesrelating to spurious and sub standard drugs andmaking offences under the Drugs and Cosmetics Actcognizable and non-bailable has recently beenpassed by Parliamewnt and enacted as the Drugs
and Cosmetics (Amendment) Act, 2008. Theprovisions of this amendment has, however, not beenenforced in view of representations received ondifficulties in its implementation and the concernedexpressed at its misuse. A committee under the DrugsController General (India) [DCG(I)] is looking into thematter.
Recent Initiatives
a) Two Sub Zonal offices of CDSCO atAhmedabad and Hyderabad elevated toZonal Offices
b) Two New Sub Zonal offices being proposedat Chandigarh and Bangaluru
c) CDTL Guwahati has become the first NABLAccredited Central Drugs Testing Laboratory.
a) Exclusive Pharmaceutical Zones are beingcreated at Airports and Port Offices.
b) New building for CDTL Mumbai and CFLMumbai has been constructed.
c) CDSCO West Zone has been shifted to newCDTL Mumbai Building
d) Computerization of all States and Centraldrug control offices and laboratories andcountrywide networking is under way throughIT-enables services
e) 62 new posts of DI and 10 new posts of TOshave been created and are being filled.
f) 45 Technical Data Associates and 28 DataEntry Operators have been recruited oncontractual basis
g) Draft Guidelines on Medical Devices havebeen developed
Notifications amending the Drugs & CosmeticsRules, 1945 during the year: 6 draft notificationsinviting public comments relating to amendments tothe Drugs and Cosmetics Rules, 1945 and 6 finalnotifications amending the Drugs and CosmeticsRules, 1945 have been published during the year2008-2009.

195
ANNUAL REPORT 2008-09
14.4 Central Indian PharmacopoeiaLaboratory and IndianPharmacopoeia Commission
The Central Indian Pharmacopoeia Laboratory,Ghaziabad which was so far functioning as a testinglaboratory of samples, as appellate laboratory fortesting of condoms and as a laboratory attached tothe Indian Pharmacopoeia has now beenamalgamated / merged into the IndianPharmacopoeia Commission (IPC), an autonomousbody registered as a Society under SocietiesRegistration Act, 1860 (No.21 of 1860) under theMinistry of Health & Family Welfare w.e.f. 1.1.2009.The mandate of the IPC is revision and publicationof the Indian Pharmacopoeia and the NationalFormulary of India on a regular basis.
Activities and Achievements
Release of Addendum 2008 of IndianPharmacopoeia 2007
Regular updating of the Indian Pharmacopoeia (IP)is the necessity of the day for bringing out an overallimprovement in the quality of drugs in the country.The Addendum 2008 to IP 2007 was released byShri Naresh Dayal, Secretary H&FW and Chairman,IPC on 16-01-2009 on the occasion of the 2ndGeneral Body meeting of the Commission held atNew Delhi. The Addendum contains amendments toIP 2007 and adds 73 new monographs on differenttherapeutic groups representing synthetic, herbalsand biological drugs. IP 2007 and its Addendum willfacilitate the manufacturers and other stakeholdersto ensure compliance with the technologicaladvancements taken place in the related fields
IP Reference Substances
Validation and certification of 77 IP Referencesubstances have been carried out during the period.
Research Activity/Research Project/ ResearchPapers Published
The Commission enjoys the status of Centre for
Shri Naresh Dayal, Secretary H&FW and Chairman, IPC releasing Addendum 2008to IP 2007 on 16-01-2009
196
ANNUAL REPORT 2008-09
Advance Studies by U P Technical University, BHU and
Meerut University. A number of post graduate
students are pursuing Ph.D out of which two have
submitted their thesis. Project based training has
been provided to graduate and undergraduate
students from pharmacy and allied disciplines. During
the period more than two dozen research papers
have been published / communicated in leading
scientific journals.
! Rigorous work is on for publication of Indian
National Formulary (INF).
! MOU with USP has been renewed in the year
2008.
! Dialogue is on for MOU with BP Commission
and EDQM.
! The visit of EDQM in the year 2008 has
opened new dimensions for collaboration to
accord an observer status to India.
! Testing of 173 Drug samples for assuring the
quality of drugs have been carried out during
the period
14.5 National Institute of Biologicals
The Ministry of Health & Family Welfare has
established the National Institute of Biologicals (NIB)
as an apex autonomous scientific Institution in the
country at an estimated cost of Rs. 269.24 crore. It
was registered under the Society's Registration Act
1860 in January 1992. The Institute shall be a
National Control Laboratory (NCL) for assuring
availability of high standards and good quality of
biological products namely vaccines, blood products,
recombinant DNA products reagents,
Immunodiagnostic kits etc. that are indigenously
manufactured or for exports and also those that are
imported into the country. The EFC has approved
staff strength of 363. The present staff strength is
75. The Ministry of Health and Family Welfare has
created 27 posts in 2008 and the recruitment process
in the final stages for filling up these posts.
The scientific activities of the Institutes are supported
by laboratories which carry out the quality control
testing of various types of Biologicals. The Blood
Reagents Laboratory at NIB is a notified CDL under
the Drugs & Cosmetics Act for quality control testing
and batch release certification of Blood Grouping
Reagents. The Institute, besides dealing with legal
samples referred by CDSCO, also certifies the quality
of Blood Grouping Reagents for safe blood
transfusion services.
14.6 World Bank Assisted CapacityBuilding Project (CBP) for Foodand Drugs
Under the World Bank assisted Capacity Building
Project (CBP), various food and drug laboratories of
the Central and State Governments have been
provided assistance for creating backup of resources
in the form of equipments, procurement of land,
construction of Laboratory building, Manpower and
initial operationalization, etc. Following the Detailed
Implementation Review (DIR) report from the World
Bank, the CBP assistance expired on 30th June, 2008
and the project has been wrapped up.
14.7 Drug DE-addiction Programme
Drug addiction in India has of late emerged as a
matter of great concern both concerned both due
to the social and economic burden caused by
substance use and due to its establishment linkage
with HIV/AIDS. The onus of responding to the
problems associated with drug use lies on the central
and state governments. The constitution of India
under Article 47, enjoins that the state shall
endeavor to bring about prohibition of the
consumption, except for medical purposes, of
intoxication drinks and of drug, which are injurious
to health. The activities to reduce the drug use
related problems in the country could broadly be
divided into tow arms supply reduction and demand
reduction. The supply reduction activities which aim
at reducing the availability of illicit drugs within the
country come under the purview of the Ministry of
Home Affairs with at the Department of Revenue as

197
ANNUAL REPORT 2008-09
the nodal agency and are executed by various
enforcement agencies. The demand reduction
activities focus upon awareness building, treatment
and rehabilitation of drug using patients. These
activities are run by agencies under the Ministry of
Health and Family Welfare, and the Ministry of social
Justice and Empowerment.
Ministry of Health and Family Welfare
The role of Ministry of Health & Family Welfare in thearea of Drug De-addiction is demand reduction by
way of providing treatment services. The Drug De-
addiction Programme in the Ministry of Health &
Family Welfare was started in the year 1987-88 which
was later modified in 1992-93. The programme was
initiated as a scheme with funding from the centralgovernment and implementation through the states.
Under the scheme, a one time grant in aid of Rs.
8.00 lakhs was given to states for construction of
each Drug De-addiction Centre and a recurring grant
of Rs. 2.00 lakhs was given to Drug De-addiction
Centres established in North Eastern Regions tomeet the expenses on medications and other
requirements. At present 122 such Centres have
been established across the country including
centres in Central Government hospitals and
institutions of which 43 Centres have been
established in the North Eastern Region. Under this
programme, a national nodal centre, the "National
Drug Dependence Treatment Centre", has been
established under the All India Institute of Medical
Sciences (AIIMS), New Delhi which is located in
Ghaziabad while two centres i.e. NIMHANS, Banglore
and PGI, Chandigarh have also been upgraded by
this Ministry. The purpose of these centres would
not only to provide de-addiction and rehabilitation
services to the patients but also to conduct research
and provide training to medical doctors in the area
of drug de-addiction.
National Drug Dependence Centre, AIIMS
National Drug Dependence Treatment Centre, AIIMS
which was established during the year 1987-88 and
functioning at Deen Dayal Upadhyay Hospital, Hari
Nagar has now shifted in its own building constructed
at CGO complex, Kamla Nehru Nagar, Ghaziabad
started indoor facilities w.e.f. 12.1203. Community
Clinic of this centre at Trilokpuri has been functioning
from 1.08.2003. Under the community based drug
de-addiction activities in India, the centre has started
services in tribal area in one district of Madhya
Pradesh (Distt. Mandsaur), Assam (Distt. Moregoan)
and Chhattisgarh (Distt. Bastar) that includes
multifarious activities of drug de-addiction. Apart from
rendering patient-care services, the centre is
engaged in a number of research projects and CME
activities.
National Drug Dependence Centre, AIIMS, CGO complex, Kamla Nehru Nagar,Ghaz iabad
198
ANNUAL REPORT 2008-09
During 2008 from April 2008 to November 2008, atotal of 2733 (new), 32215 (old) patients were seen inthe OPD, 33419 in the Community clinic (old & new),30 patients in the Adolescent Drug Abuse clinic, and457 patients in the Tobacco Use Cessation clinic and171 patients in the Dual Diagnosis clinic were seen. Atotal of 788 patients were admitted in the ward.
During this period, laboratory investigationscarried out were: Drugs of abuse screened(9000), biochemistry (12500), haematology (2200),and HIV screening (256, positive-6.6 %.).
Ongoing Funded Research:
! Post Marketing Surveillance of Addnok-N(combination of Buprenorphine andNaloxone)
! Effect of Nitric Oxide Synthase Inhibitor 7-NIon Sensitization to the Operant DecrementProduced by Naloxone in Morphine TreatedRats.
! Oral Substitution Treatment withBuprenorphine, Funded by United NationsOffice on Drugs and Crime, Regional Officefor South Asia
! Database on Drug Abuse and HIV/AIDSsponsored by UNOD-ROSA
! Assessment of Increase Treatment Seekingand Faridkot, joint project of NDDTC,Faridkot Medical College and Art of Living.
! Oral Substitution Treatment in Tihar Prisons,project supported by UNODC-ROSA
! NDDTC has given full support and feedbackto DDAP Cell of the Ministry of Heath andFamily Welfare for conducting " Indian Profilefor Global Survey on Alcohol and Health andAtlas on Resource for Treatment andPrevention of Substance Use" of WHO.
The following WHO Biennium (2008-09) activities arebeing carried out:
! Development of manual-Minimum standardsof care
! Management of alcohol and drugdependence in primary care settings
! Training programme on agonist maintenance
! Assessment of drug abuse among adolescent
! Training of trainers
! Training by trainers
The centre organized training programme for doctors
in
! District Moregaon (Assam) and Mandsaur
(MP)
! Conducted regional meetings to formulate
treatment policy in Drug and Alcohol use in
Assam, Bangalore, Mumbai and Ranchi
! Has initiated district based model for provision
of care for 'substance use disorder' at
Meerut, Mandsaur and Moregaon
! Conducted a training programme for
psychiatrists from the state of Punjab
The faculty visited several sites (visits to De-addiction
centres in various states; Manipur, Mizoram and
Nagaland) to assess outcome of patients following
their treatment. The Centre's Chief was appointed
as member Expert Advisory Panel to Punjab State
Planning Board. The faculty published several
research articles in various national and international
journals.
De-Addiction Centre, National Institute of
Mental Health and Neuro Sciences Bangalore
Drug De-addiction Centre at NIMHNS, Banglore was
established during the 1991. A separate building has
constructed with the cost of Rs. 5.10 Crore and
currently houses 30 in patient's beds and also has
rooms for inpatient and outpatient therapeutic
groups. The De-addiction Centre, NIMHANS, is
recognized as the regional center for Southern India.
The centre is involved in various research and
training activities of the Region.

199
ANNUAL REPORT 2008-09
Release of the manual on "Psychosocial Interventions for Persons with Substance Abuse: Theory andPractice by Dr. Anbumani Ramadoss, Minister for Health and Family Welfare
During 2008 the De-addiction centre caters to morethan 1600 new patients and follows up around 4800patients. The out-patient service occurs twice weeklyand caters to persons with alcohol dependence andabuse, opiate dependence, nicotine dependence and
other substance abuse and dependence. There is acomprehensive inpatient programme consisting ofindividual therapy, group counseling, familycounseling and aftercare.
One month Orientation programme on Substance abuse held during the month of November 2008.

200
ANNUAL REPORT 2008-09
The Centre also conduct training programsto MD/DNB, psychiatry trainees, social workers,psychologists from medical colleges all over thecountry. The Deaddiction centre conductsworkshops, seminars and teaching programscontinuously. Every week there is a teachingprogram for the MD residents who are posted. Apartfrom this 3 training workshops for medical officersin the state of Karnataka were conducted. A monthorientation program for medical officers in substanceabuse management was conducted in the month ofNovember. It was well received by all theparticipants.
During the current year one occupational therapist,a junior scientific officer for HPTLC lab and two aftercare counselors have been recruited. Theoccupational therapist is actively involved inconducting creative activities for the patients likecollage, mosaic, creative writing, drama, free handdrawing, painting, general discussion and debate ongeneral issues etc.
To monitor substance abuse in patients, the De-addiction centre has been relying on verbalinformation from the patient and also by commerciallyavailable ready-to-use test of urine samples for illicitdrugs. But for proper diagnosis and qualitative andquantitative analysis of drugs and their metabolites,the centre initiated the toxicology laboratory from sep2008. The laboratory caters to the De-addictioncentre OPD, inpatient services and psychiatricpatients from the hospital. The lab is fully equippedto carry out chemical tests to monitor drug abuse inpatients with addiction and/or psychiatric disorders.The laboratory currently tests cannabis and itsmetabolites, opioids and benzodiazepines in urinesamples. The laboratory is planning to extend thetests to barbiturates, amphetamines, lysergide (LSD)and gamma-hydroxybutyric acid. The laboratory hasalready standardized 20 different screening testsand HPTLC (High performance thin layerchromatography) based analysis of different drugs.The laboratory is also involved in a research projectwhich involves chemical analysis of illicit drugs inpatients suffering from phase I psychosis.
Based on clinical diagnosis and previous drug use,
all the urine samples are first screened for presenceof specific drugs. Once a particular drug/group ofdrugs is indicated by the screening test, such samplesare confirmed by HPTLC. Following analysis, thefinal report is submitted to the clinician/treatingdoctor. Since two months, the toxicology laboratoryhas tested 55 patients (No. of samples: 56; male=53;female=3) for cannabis, opiates andbenzodiazepines.
Tobacco Cessation Center, NIMHANS, an outpatientcessation clinic and carries out awareness andtreating activities have been initiated. Employeeawareness programs were conducted in manyorganizations including Robert Bosch, GoldmanSachs, and Deccan Herald through sessions,exhibitions and information kiosks. NIMHANS groupD employees functioning in the department ofPsychiatry were also covered by tobacco awarenessprograms during the year. As a part of the tobaccoprevention activities, awareness programs wereconducted in 2 premier educational institutions (St.Joseph's PU College, Bhagwan Mahaveer JainCollege) where approximately 1150 students werecovered through lectures, exhibitions and kiosk.
Capacity building programs for health professionalshave also been conducted during the year in whichvarious professionals such as dentists, physicians,counselors, and psychiatrics were trained. TCC hasorganized 2 major training programs and beenactively part of one training program. About 65professionals have been thoroughly trained onvarious aspects of tobacco cessation during theseprograms.
Articles published by TCC staff on major news dailiesreceived an enthusiastic response following whichthe numbers of enquiries and distress calls haveincreased considerably.
NIMHANS continues to coordinate the activities ofTCCs, by acting as the Tobacco Cessation ClinicResource Center (TCCRC) during this year also.Apart from providing consultancy services, TCCRChave also launched a website for the tobacco usersand health professionals practicing tobacco cessationwith support from WHO and Ministry of Health andFamily Welfare, Government of India.

201
ANNUAL REPORT 2008-09
The De-addiction Centre has also initiated fourresearch projects on 1. Investigation of CorticalInhibitory Circuits in individuals at high risk for alcoholdependence: A Paired-Pulse TMS study. 2.Prevalence of substance use in first episodepsychosis patients 3. The relationship of symptomsof Schizophrenia and drug related side effects toareca nut use and 4. Correlates of anger amongalcohol users. One project has been approved bythe ethics committee and the others are awaitingethical clearance. The Centre has also beensanctioned a WHO project on outcome in alcoholdependence which will be initiated in this biennium.In collaboration with the NDDTC, the center is alsoinvolved in another WHO projects.
In the last trimester of the financial year, two moreworkshops for medical officers from 2 districts ofKarnataka, a workplace prevention of psychosocialstresses including drug abuse in conjunction withDeccan Herald Bangalore, a state wide sensitizationworkshop on Tobacco use prevention are planned.
Drug De-addiction Centre, PGI, Chandigarh:
Drug De-addiction Centre, PGI, Chandigarh wasestablished during 1988-89. Currently, The cemtrehas been shifted in a separate building in which 30bedded inpatient facilities are available as well asseparate OPD services has been included. Thecentre has Community Clinic at Kharar, Punjab thatrun by the Doctors and Paramedics of PGIChandigarh. During 2008 approximately 5500 have
been seen and nearly 38,000 follow-up visits of old
patients have been carried out at the DDTC OPD;
nearly 2900 patients have been treated as inpatients.
Under the Community clinic at Civil Hospital, Kharar,
Punjab numbers of patients are examined and
treated than and more sick patients have been
referred to the DDTC inpatient section of PGI.
The Centre has seen 250 subjects as inpatients and
370 subjects as new cases in the OPD during the
year 2008. The Institute is running a social
assessment and rehabilitation services for the
psychosocial assessment and therapy sessions at
the Institute and in the community and efforts at socio-
occupational rehabilitation in the community also.
The centre conducted weekly clinic at Kharar Civil
Hospital and launch monthly De-addiction camps in
villages to spread awareness among the masses
about the problem of substance use and the sources
of health and treatment available in the community.
The Institute helps 12 Camps and covered 400
substance abusers.
The Centre is involved in research activities and
conducted training in various aspects of drug abuse
for many categories of staff and personnel from both
within and outside the Institute. The Institute has
also developed material for heath education and
training. The centre has organized the IEC camp in
the Institute in which various stakeholders have been
participated.

202
ANNUAL REPORT 2008-09
203
ANNUAL REPORT 2008-09
Chapter 15
15.115.115.115.115.1 IntroductionIntroductionIntroductionIntroductionIntroduction
The Centre has set up regulatory bodies formonitoring the standard of medical education,promoting training the research activities. This isbeing done with a view to sustain the production ofmedical and para-medical manpower to meet therequirements of health care delivery system at thePrimary, Secondary and Tertiary levels in the country.This chapter discusses the status of these activitiesconducted by the various bodies and institutions.
15.215.215.215.215.2 Medical Council of IndiaMedical Council of IndiaMedical Council of IndiaMedical Council of IndiaMedical Council of India
The Medical Council of India was established as astatutory body under the provisions of the IndianMedical Council Act, 1933, which was later, replacedby the Indian Medical Council Act, 1956 (102 of1956). The main functions of the Council are (1)Maintenance of uniform standard of Medicaleducation at undergraduate and postgraduate level;(2) Maintenance of Indian Medical Register; (3)Reciprocity with foreign countries in the matter ofmutual recognition of medical qualifications; (4)Provisional/permanent registration of doctors withrecognised medical qualifications, registration ofadditional qualifications, and issue of Good standingcertificates for doctors going abroad (5) ContinuingMedical Education, etc.
Inspections: The Medical Council of India from April2008 to August, 2008 carried out 26 Inspections forEstablishment of new Medical College, 43 Inspectionsfor renewal of permission, 33 compliance verificationinspection + Estt. + 11(2) + Surprise Inspections, 07Inspection for approval of the college, 12 Inspectionsfor increase of seats, 13 Inspections for renewal ofpermission for increase of seats, 4 Complianceverification inspections for increase of seats +increase + 11(2) and 42 Periodical inspections.
Further, the Council also carried out 08 inspectionsfor starting of Postgraduate medical courses atvarious colleges/institutions and 01 inspection forincrease of seats for which the request was receivedthrough Central Government under Section 10A ofthe IMC Act, 1956. The Council also carried out 115inspections for recognition of postgraduatequalifications. 25 inspections for recognition ofcompliance verification.
Registration: The Council has registered 424doctors with their additional qualifications underSection 26 of the Indian Medical Council Act, 1956.The Council also issued 567 Good StandingCertificates to doctors who desired to seek Registrationwith Medical Councils of foreign countries. Further,the Council issued 721 Provisional and 791 PermanentRegistration Certificates under Section 25(2) and 23of the IMC Act, 1956 respectively.
Continuing Medical Education: During the year2008-2009 the Council has planned to hold 150-200CME programmes. Till August, 2008, 135 CMEprogrammes have been approved of which 105Continuing Medical Education programmes are likelyheld at various medical institutions in the country.
Accounts & Establishment: The following outlay hasbeen approved by the Central Government as Grant-in-aid (Plan & Non-Plan) for the year 2008-2009:
Outlay approved (Rs.)
Plan (including CME) 100 Lakh
Non-Plan 60 Lakh
A sum of Rs. 22,28,01,856/- has been received bythe Council till August 2008 from other resources inaddition to Grants-in-aid received from the CentralGovernment.
Medical Education, Training & ResearchMedical Education, Training & ResearchMedical Education, Training & ResearchMedical Education, Training & ResearchMedical Education, Training & Research
204
ANNUAL REPORT 2008-09
Policy regarding Establishment of Medical College:As on date August, 2008 there are 283 medicalcolleges in the country out of which 205 medicalcolleges have been recognised under Section 11(2)of the IMC Act, 1956 by Medical Council of India.The remaining 78 colleges have been permittedunder Section 10A of the IMC Act, 1956 for startingMBBS course. Out of the 283 medical colleges, 137are Govt. Medical College, 4 are University collegesand remaining 142 are private medical colleges. Theadmission capacity in these colleges is approx.30,588 students per year.
15.315.315.315.315.3 Dental Council of IndiaDental Council of IndiaDental Council of IndiaDental Council of IndiaDental Council of India
The Dental Council of India is a statutory bodyconstituted by an Act of Parliament viz. Dentists Act,1948 (XVI of 1948) with the main objective ofregulating the Dental Education, Dental Profession,Dental ethics in the country and recommend to theGovt. of India to accord permission to start a DentalCollege, start higher course & to increase of seats.For this purpose the Council periodically carries outinspection to ascertain the adequacy of courses andfacilities available for the teaching of Dentistry.
The Council had received 151 applications inprescribed form/Scheme from the Central Govt. for(i) establishment of new Dental colleges, (ii) startingMDS Courses & (iii) increase of seats in BDS/MDSCourses for evaluation & recommendation inaccordance with the provision of the Section 10A ofthe Dentists Act, 1948. During the said period, theCentral Govt. on recommendation of the Council hadpermitted 04 new Dental Colleges, Starting MDSCourses in 107 specialities at 34 Dental Colleges,05 Dental Colleges for increase/restoration ofadmission capacity in BDS Course and 06 DentalColleges for increase of seats in MDS Courses in 15specialities. The Central Govt. on recommendationof the Council had allowed/ renewed its permissionfor 2nd/3rd/4th/5th/6th year BDS course in 76 DentalColleges and renewed its permission for 2nd/3rd/4th/5th/6th year MDS Courses in 62 Dental Colleges in289 specialities and renewed its permission forincrease of seats for 2nd/3rd/4th/5th/6th year BDS Courseat 21 Dental Colleges and for increase of seats for2nd/3rd/4th/5th/6th year MDS Courses in 40 specialities
at 10 Dental Colleges. 323 Inspections of the variousDental Colleges in the country had been carried outby the Council's Inspectors/Visitors during this period.The Council had granted its permission to start DentalMechanic Courses at 02 Dental Colleges & DentalHygienist Course at 04 Dental Colleges.
The Govt. of India on the recommendation of theCouncil had issued 42 notifications of recognition ofBDS/MDS qualifications awarded by the 22 IndianUniversities & 03 Foreign Universities under Section10(2) & 10(4) of the Dentists Act, 1948. A sum ofRs.19 Lakhs has been provided as grant-in-aid tothe Council during the year 2008-2009.
15.415.415.415.415.4 Pharmacy Council of IndiaPharmacy Council of IndiaPharmacy Council of IndiaPharmacy Council of IndiaPharmacy Council of India
The Pharmacy Council of India (PCI) is a bodyconstituted under section 3 of the Pharmacy Act,1948 to regulate the profession and practice ofPharmacy. The objectives of the Council is toPrescribing minimum standard of education requiredfor qualification as a pharmacists; Uniformimplementation of education standards; Approval ofcourse of study and examination for Pharmacists;withdrawal of approval; Approval of qualificationsgranted outside India; and Maintenance of CentralRegister of Pharmacists.
The Council arranged 148 inspections of diplomaand degree institutions. The approval of 68 Diploma& Degree institutions has been extended UnderSection 12 of the Pharmacy Act, 17 new Diploma &Degree institutions has been granted approval u/s12 of the Pharmacy Act. 16 new Pharm. D. institutionshas been granted approval for the conduct of courseand 8 new Pharma D. (Post Baccalaureate)institutions has been granted approval for theconduct of course.
At present 523 institutions have been approved with31,513 admissions for Diploma in Pharmacy and 326institutions with 19,125 admissions for degree inPharmacy.
National School of Pharmacy
It has envisaged the need to set up National Schoolsof Pharmacy jointly by PCI and Pharmacy industry
205
ANNUAL REPORT 2008-09
as a centre of excellence which will produce highquality Pharmacist workforce tailor-made to suit therequirements of the industry. A committee of expertshas been constituted to frame an action plan formaking the proposed National School of Pharmacya reality.
Introduction of Pharm. D and Pharm. D (PostBaccalaureate) Programmes:-
To meet the growing requirements of the practiceside and to overcome the problems being faced byIndian Pharmacy graduates in practicing thepharmacy profession in foreign countries, it has beenproposed to introduce Pharma D. and PharmaD.(Post Baccalaureate) programmes as registrablequalifications.
Continuing Education Programmes:-
The PCI from its own resources is giving a financialassistance of Rs.10,000/- per course subject toceiling of 12 courses to the state Pharmacy Councilsfor the conduct of Continuing Education Programmefor Pharmacists.
15.515.515.515.515.5 Indian Nursing CouncilIndian Nursing CouncilIndian Nursing CouncilIndian Nursing CouncilIndian Nursing Council
The Indian Nursing Council is an autonomous bodyunder the Government of India Ministry of Health andFamily Welfare constituted under the Indian NursingCouncil Act, 1947 to establish a uniform standard oftraining for nurses, midwives and health visitors andANMs in India.
First Inspection
The Council undertake the first inspection to assesssuitability with regard to Physical infrastructure,clinical facility and teaching faculty in order to givepermission to any organization under the CentralGovernment, State Government, Local body or aPrivate Trust, Mission, Voluntary Organizationregistered under society Registration Act or acompany registered under company's Act wishes toopen a school/college of Nursing. First Inspection isconducted on receipt of the proposal received fromthe institute to start any nursing programmeprescribed by India Nursing Council.
Re-Inspection
Re-inspection are conducted for those institutions,which are found unsuitable/not permitted by IndianNursing Council.
Periodical Inspection
Indian Nursing Council conducts periodical (after 3years) inspection of the institution once the institutionis found suitable by Indian Nursing Council to monitorthe standard of nursing education and the adherenceof the norms prescribed by INC. Institutions arerequired to pay annual affiliation fees every year.Indian Nursing Council also conducts inspection ofthe institution once the institution is found suitableby Indian Nursing Council and on receipt of the feesand the proposal for Enhancement of seats.
Number of Inspections
During the year 2007-08 a total number of 934Nursing Institutions were inspected.
Source of Income
During the year 2007-08 sums of Rs. 11 lakh (Non-Plan) and Rs. 20.00 lakh (Plan) was received fromthe Government of India as grant. A sum of Rs.4,50,31,255/- has been received from the traininginstitution as inspection/affiliation fee.
Court Cases
Out of the 65 court case in various High Courts ofIndia, 26 have been disposed off.
New Syllabuses
Five new syllabuses viz(i) Post Basic Diploma inNeonatal (ii) Post Basic Diploma in Critical CareNursing (iii) Post Basic Diploma in Oncology Nursing(iv) Post Basic Diploma in Emergency and DisasterNursing (v) Post Basic Diploma Nurse Practitioner inMidwifery have been notified during the year 2007-08.
Institutions Recognized by INC
At present 1620 GNM Schools, 329 ANM Schools,883 College of Nursing for conducting graduationprogramme and 105 college of Nursing for conducting
206
ANNUAL REPORT 2008-09
Post Graduate Course in Nursing are functioning inthe Country upto 31.3.2008.
Number of Qualified Nurses Registered
So for 9,30,528 Nurses, 5,26,242 ANMs and 51,183Health Visitors have been registered with variousState Nursing Councils upto 31st December, 2006.
National Consortium for Ph.D in Nursing
National Consortium for Ph. D in Nursing has beenconstituted by Indian Nursing Council to promoteresearch activities, in various fields of Nursing incollaboration with Rajiv Gandhi University of HealthSciences, supported by WHO. Total 93 studentshave been enrolled under National Consortium ofPh. D in Nursing.
Website of Council
The website of Council - www.indiannursingcouncil.org.& www.indiannursingcouncil.co.in are being updatedregularly.
15.615.615.615.615.6 Development of Nursing ServicesDevelopment of Nursing ServicesDevelopment of Nursing ServicesDevelopment of Nursing ServicesDevelopment of Nursing Services
In order to improve the quality of Nursing Services,the following activities are being implemented underthe scheme of Development of Nursing Services: -
� Training of Nurses.
� Strengthening of existing Schools/Collegesof Nursing.
� Upgradation of Schools of Nursing attachedto Medical Colleges into Colleges of Nursingby providing one time non-recurringassistance of Rs. 1.50 crores to states.
� Providing recurring assistance to Schools ofNursing which were opened during IX planwith assistance under the scheme ofDevelopment of Nursing Services.
� Establishment of College of Nursing atJIPMER, Pondicherry.
� Strengthening of R.A.K. College of Nursingas "Center of Excellence".
� Upgradation of Schools of Nursing intoColleges of Nursing attached to Dr. R.M.L.Hospital, S.J. Hospital and Lady HardingMedical College, New Delhi.
Training of Nurses.
In order to update the knowledge and skills of theNursing personnel, Continuing Nursing EducationProgramme was started in the following areas: -
Category of Nursing Area of continuingpersonal Education
Staff Nurses � Different clinical specialty
Nurse Administrators � Management Technique
Nursing Educators � Educational Technology
Duration of training � 10 days
No. of Participants per � 30
Training programme � Rs.75, 000 perPattern of Assistance training Programme.
A sum of Rs. 1.00 crore has been allocated for theyear 2007-08 to train 4000 Nursing personnel. Asum of Rs. 60.00lakhs has been released in 2007-08 to 11 Institutions for conducting 80 courses fortraining 2400 nurses. A provision of Rs. 8.60 croreshas been made for training of nurses during the year2008-09.
Strengthening of Schools/Colleges of Nursing.
In order to improve the quality of training imparted atthe existing Schools and Colleges of Nursing, a sumof Rs. 10.00 lakhs is sanctioned towardsprocurement of A.V Aids, improvement of library,additions and alterations of School/College/Hostelbuilding and transport. It is proposed to increase theamount of Rs. 10.00 lakhs to Rs. 25.00 lakhs as theamount of Rs. 10.00 lakhs is not sufficient to makesubstantial improvement in the nursing institutions.A sum of Rs.3.40 crores has been released during2007-08 to strengthen 34 institutions on existingpattern. A provision of Rs.5.40 crores has been madefor Strengthening of Schools/ Colleges during theyear 2008-09
207
ANNUAL REPORT 2008-09
Upgradation of Schools of Nursing attached toMedical Colleges into Colleges of Nursing.
A one time assistance of Rs. 1.5 crores to the StateGovernment is given for upgrading a School ofNursing attached to Medical College into College ofNursing in order to increase the availability ofgraduate nurses . Te funds are released to theInstitute subject to the condition that StateGovernment/Institution will bear the recurringexpenditure. The financial assistance is meant forcivil works including addition and alteration of schooland hostel building and for furniture, audio- visualaids and transport. Keeping in view therecommendations of the National Health Policy, andthe report of the National Commission onMacroeconomics and Health, the National Task Forceon Development of Strategic Framework for Nursingfor XIth Plan has suggested the need for improvingthe quality of nursing and felt need to continue theupgradation of Colleges during the XIth plan period.It is proposed to increase the amount of Rs. 1.50crores to Rs. 6.00 crores (consisting of Rs. 5.50crores as non-recurring and Rs. 0.50 crore asrecurring) for upgrading per Nursing School.
Upgradation of Schools of Nursing intoColleges of Nursing attached to Dr. R.M.L.Hospital, S.J. Hospital and Lady Harding MedicalCollege, New Delhi.
College of Nursing at JIPMER, Pondicherry has beenestablished during 2006-07 and the School ofNursing at Lady Hardinge Medical College, New Delhihas been upgraded into College of Nursing during2007-08. The School of Nursing at Dr. RML Hospitaland Safdarjung Hospital has bee upgraded duringthe current year of 2008-09. A sum of Rs.8.78 croreshas been released during the year 2007-08 for thepurpose.
Providing recurring assistance to Schools ofNursing which were opened during IXth Plan.
There was a provision in the IXth Plan for providingassistance under the scheme for opening newSchools of Nursing with financial implication of Rs.82.68 lakhs per school. 48 Nursing Schools have
been sanctioned under the programme. However,this programme has been discontinued during the10th Plan. It was decided to provide remainingrecurring assistance to these schools opened duringIXth Plan. Keeping in view the slow progress of settingup these schools by the states, some of theinstitutions have yet to be released the recurringassistance earmarked for them and this needs to beprovided to them during XIth Plan. A provision Rs.0.34 crores have been allocated during 2008-09 forthe purpose.
Revival of National Award for NursingPersonnel.
National Awards for Nurses are given as a mark ofhighest recognition for the meritorious services ofthe nurses and Nursing profession in the country.From 2007 onwards this award has been revived withthe consent of Hon,le President of India and namedas National Florence Nightingale Award". During theyear 2008-09 26 nurses had been honoured withthis prestigious award. Each award carries aCertificate of Merit and Cash Award of Rs. 50,000/- .A sum of Rs. 0.50 lakhs has been earmarked duringthe year 2008-09.
New Scheme under Human Resource.
� Establishment of 24 Center of Excellence
� Opening of 131 ANM Schools
� Opening of 137 GNM Schools
� Strengthening of State Nursing Cell / StateNursing Council
� Establishment of 6 Colleges of Nursing :
The EFC for a sum of Rs. 120.00 crore has beenapproved for Establishment of 6 Colleges of Nursingat sites for AIIMS like Institutions.
Establishment of Regional Institutes of Nursing.
It is proposed to establish 4 Regional Institutes ofNursing @ Rs. 50.00 crore per Institution. A sum ofRs. 178.00 crore have been allocated for the year2008-09 for implementing the new scheme.
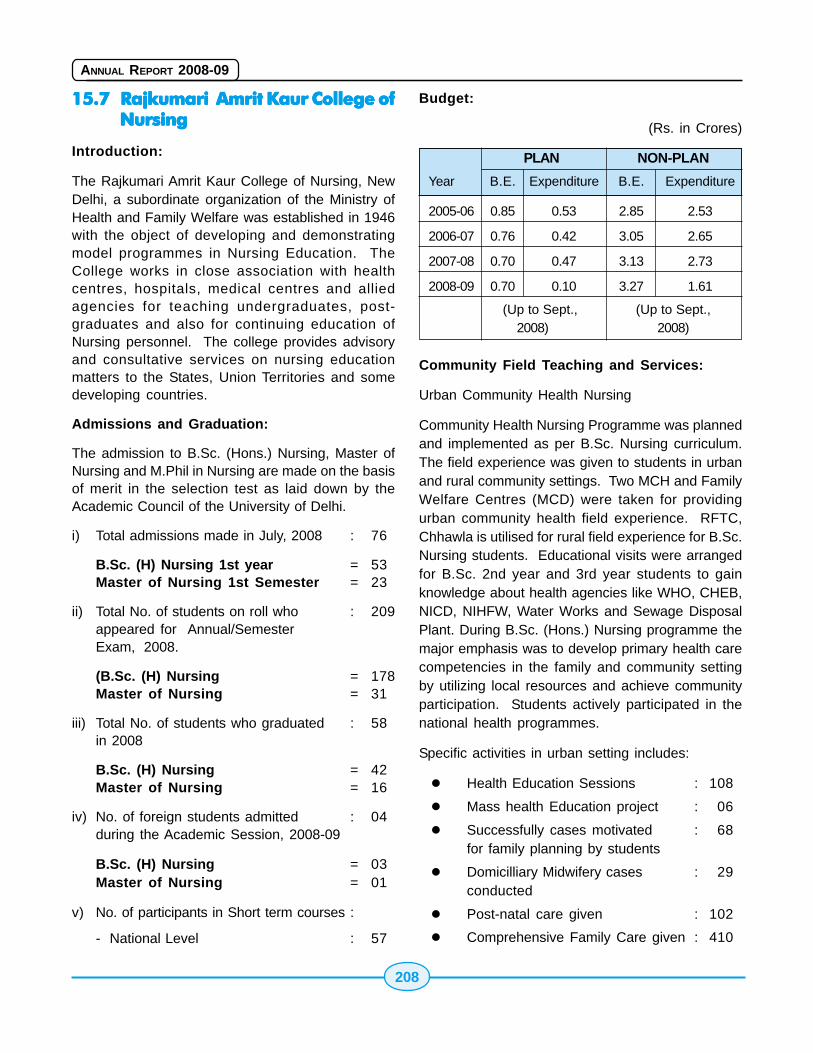
208
ANNUAL REPORT 2008-09
15.715.715.715.715.7 Rajkumari Amrit Kaur College ofRajkumari Amrit Kaur College ofRajkumari Amrit Kaur College ofRajkumari Amrit Kaur College ofRajkumari Amrit Kaur College ofNursingNursingNursingNursingNursing
Introduction:
The Rajkumari Amrit Kaur College of Nursing, NewDelhi, a subordinate organization of the Ministry ofHealth and Family Welfare was established in 1946with the object of developing and demonstratingmodel programmes in Nursing Education. TheCollege works in close association with healthcentres, hospitals, medical centres and alliedagencies for teaching undergraduates, post-graduates and also for continuing education ofNursing personnel. The college provides advisoryand consultative services on nursing educationmatters to the States, Union Territories and somedeveloping countries.
Admissions and Graduation:
The admission to B.Sc. (Hons.) Nursing, Master ofNursing and M.Phil in Nursing are made on the basisof merit in the selection test as laid down by theAcademic Council of the University of Delhi.
i) Total admissions made in July, 2008 : 76
B.Sc. (H) Nursing 1st year = 53Master of Nursing 1st Semester = 23
ii) Total No. of students on roll who : 209appeared for Annual/SemesterExam, 2008.
(B.Sc. (H) Nursing = 178Master of Nursing = 31
iii) Total No. of students who graduated : 58in 2008
B.Sc. (H) Nursing = 42Master of Nursing = 16
iv) No. of foreign students admitted : 04during the Academic Session, 2008-09
B.Sc. (H) Nursing = 03Master of Nursing = 01
v) No. of participants in Short term courses :
- National Level : 57
Budget:
(Rs. in Crores)
PLAN NON-PLAN
Year B.E. Expenditure B.E. Expenditure
2005-06 0.85 0.53 2.85 2.53
2006-07 0.76 0.42 3.05 2.65
2007-08 0.70 0.47 3.13 2.73
2008-09 0.70 0.10 3.27 1.61
(Up to Sept., (Up to Sept.,2008) 2008)
Community Field Teaching and Services:
Urban Community Health Nursing
Community Health Nursing Programme was plannedand implemented as per B.Sc. Nursing curriculum.The field experience was given to students in urbanand rural community settings. Two MCH and FamilyWelfare Centres (MCD) were taken for providingurban community health field experience. RFTC,Chhawla is utilised for rural field experience for B.Sc.Nursing students. Educational visits were arrangedfor B.Sc. 2nd year and 3rd year students to gainknowledge about health agencies like WHO, CHEB,NICD, NIHFW, Water Works and Sewage DisposalPlant. During B.Sc. (Hons.) Nursing programme themajor emphasis was to develop primary health carecompetencies in the family and community settingby utilizing local resources and achieve communityparticipation. Students actively participated in thenational health programmes.
Specific activities in urban setting includes:
� Health Education Sessions : 108
� Mass health Education project : 06
� Successfully cases motivated : 68for family planning by students
� Domicilliary Midwifery cases : 29conducted
� Post-natal care given : 102
� Comprehensive Family Care given : 410
209
ANNUAL REPORT 2008-09
Field Experience to three Master of Nursing studentswho opted for Community Health Nursing electivewere provided clinical experience at MCH and FamilyWelfare Centre, Sri Niwas Puri. The major purposeof the experience was to assist students gaincompetencies in rendering comprehensive care tohigh risk families on the priority basis using problem-solving approach. They also planned need-basedcommunity health action programme for a definedurban slum population, utilizing community resourcesand mobilizing team effort.
The M.N. student organized two days health campon "Prevention of Substance Abuse" Sri Niwas PuriCentre. The students opted to do further field workand study in St. Stephen's Community Health Centres,Kalpadi and Sunder Nagari,. All B.Sc. (H) Nursingstudents participated in Pulse Polio Programme.
Medical-Surgical Nursing:
During the year 2008-09, teaching, supervision andevaluation of Medical-Surgical Nursing wasundertaken for Master of Nursing and B.Sc. (H)Nursing students. Clinical experience, clinicalteaching and supervision was provided to studentsin different hospitals mainly in Safdarjang Hospital,G.B. Pant Hospital and National Institute of T.B. andallied chest diseases, New Delhi.
Three areas of specialization were offered to postgraduate students under Medical-Surgical electivefor advance study i.e. Intensive Nursing Care,Cardiothoracic and Cancer Nursing. These studentsopted to do further clinical work and study in RajivGandhi Cancer Institute, New Delhi, Rama ChandraMedical College and Rresearch Institute, JawaharLal Nehru Cancer Hospital and research Centre,Bhopal, Sher-e-Kashmir Institute of MedicalSciences, Saura, Srinagar etc.
Paediatric Nursing:
The Paediatric Field Experience for B.Sc. 3rd yearand Interns was conducted as per stated objectives.The clinical experience was offered at PaediatricMedical-Surgical Wards and Neonatal Nursery atSafdarjang Hospital Under Five Clinics and FrankAnthony Public School, Lajpat Nagar, New Delhi.
Child Guidance Experience was given at R.A.K.College of Nursing and Crèche at AIIMS.
Psychiatric Nursing:
During the year 2008-09, teaching and supervisionof Psychological Foundations was undertaken forMaster of Nursing and B.Sc. (H) Nursingstudents.B.Sc. (H) Nursing Interns conducted groupproject on various aspects of Psychology.
Practical session were conducted for B.Sc. (H)Nursing 2nd year students on Psychometric Tests intwo batches. For M.N. Practical session wereconducted in intelligence Test, Personality Test,Aptitude Test, Attitude Measurements etc.
Obstetrics and Obstetrical Nursing:
Obstetrical Nursing experience for B.Sc. (H) Nursingand Master of Nursing students was offered atSafdarjang Hospital, New Delhi. The ClinicalExperience was offered in post-natal wards, antenatalclinics, labour room, maternity OT, Nursery and familywelfare clinic. B.Sc. (H) Nursing 3rd year studentsconducted group project on antenatal care, diet inpregnancy and lactation and post-natal care in thematernity wards. Learning experience was providedas per objectives of the programme.
B.Sc. Interns celebrated breast feeding promotionweek by conducting a project o0n breast feedingpromotion with display of posters, demonstration andskit. Group projects were also conducted by B.Sc.(H) Nursing interns on various aspects of obstetricalcare i.e. antenatal and postnatal care.
Total four M.N. students opted for Obstetrics andObstetrical Nursing as the elective subject. Clinicalexperience was provided to them in both the low riskand high risk areas of obstetrical department atSafdarjang Hospital. They also conducted a groupproblem solving project on "Nurses practitioners inMidwifery in India" to create awareness about thesame topic among B.Sc. (H) Nursing Interns. TheM.N. Students had their summer field experience atLady Harding Medical College & Hospital.
210
ANNUAL REPORT 2008-09
Nutrition:
Nutrition and Dietetics courses were offered to B.Sc.(H) Nursing students as per academic plans.
Continuing Education:
During the period under review, continuing educationcourses were conducted for nursing personnel. Onenational level short-term course on "QualityAssurance in Nursing" was conducted during theyear 2008-09.
Rural Field Teaching Centre, Chhawla:
The Rural Field Teaching Centre was established in1950 for the purpose of providing objective orientedRural Community Health Nursing experience to thestudents. It covers 7 villages with approximatelypopulation of 17000 and is situated 35 Kms. awayfrom the College. The Centre provides an integratedcomprehensive health and family welfare servicesto the community. Special emphasis is given on MCHservices, family planning, immunization, nutrition andhealth education programme by the students andstaff of rural unit in collaboration with the staff of PHC,Najafgarh. Staff and students also participate inNational Health programme like Malaria controlprogramme, revised National tuberculosis controlprogramme, AIDS Control Programme, DiarrhoealDiseases control programme etc. The Centre alsohas DOTS and Microscopic Centre for screening andtreatment of T.B . patients. Chief Medical Officer ofthe R.A.K. College of Nursing is the In-charge of theR.F.T.C. and DOTS Centre. In addition, the Centreprovides mobile Van clinic services to seven villageswith special emphasis on Primary, secondary andtertiary level. R.F.T.C. is a team movement point forPulse Polio Programme.
B.Sc. (H) Nursing 1st year students learnt to makehealth assessment of individual and effect of healthdeterminants in community setting and madeobservation of community health and health alliedresources.
Second year students learnt to give health educationin different community setting and gain insight ofepidemiological triad. They also learnt to identify
the health problems by family interaction andobservation of environmental factors.
B.Sc. (H) Nursing Interns and 3rd year studentsdevelop competency in providing comprehensivehealth care to the individual, family and community.They also learnt to conduct community surveys toidentify specific health needs and problems, plan,organise and evaluate nursing programme based onthe needs identified.
The students were helped in gaining insight of thehealth services rendered to the rural community byproviding need based family health care andorganising health education programme in differentcommunity settings.
Library:
The College Library has total 19637 Books andprocured 392 books in 2008-2009.
Number of purchased Journals:
i) Foreign Journals in 2008 = 35
iii) Indian Journals in 2003 = 5
iv) Newspapers = 05
v) Magazines = 07
The total expenditure on books and journals duringthe period was Rs.800,000/- (Rupees Eight Lacs)only. Xerox facilities and intern library loan facilitieswere provided to the students and staff and MEDLARfacilities obtained whenever necessary.
Student Welfare and Co-curricular Activities:
Student Health Programmes;
The main objectives of the student health programmeare: to help students to promote and maintain theirown health, and to prevent and control the diseasesby early detection and treatment.
Detailed medical examination was done for allnew admissions.
Other activities of the Health Office are periodicalcheck-up, treatment of minor ailments, follow-up,

211
ANNUAL REPORT 2008-09
immunization, individual counseling and guidance.
Students' Activities:
Apart from celebrating various festivals and othercultural programmes, the students of this Collegealso participated in the Perfect Health Mela, 2008,organized by the Heart Care Foundation of India.
Some of the B.Sc. (H) nursing students of our Collegealso won prizes in the various competitions/eventsheld at the said Health Mela site.
Other Activities:
Despite the limitations of accommodation, facultypositions, other restraints and constraints, theCollege has made great strides in the field of nursingand health care. Our faculty is enthusiastic and hardworking. Some teachers of the College are engagedin many areas of research in different fields of nursingand nursing education. Some of them are providingconsultative and advisory services and areparticipating in some projects and meetings atnational level.
Sixteen Nursing research studies were undertakenby post graduate students in various specialties.Apart from that B.Sc. (H) Nursing Interns alsoundertook their research projects in five groups.
Regular sports events were planned and organizedas per academic activities scheduled for B.Sc. (H)Nursing and Master of Nursing students during theyear.
The College (faculty and students) is participatingregularly in Pulse Polio Immunization Programmesince 1995. Students and teachers have beenparticipating in 'House to House' activity for last eightyears. RFTC, Chhawla has been made TMP (TeamMovement Point) for Pulse Polio since 2002.Assembly and zonal Co-ordinators have highlyappreciated the quality of work done by the Collegestudents and teachers in 'House to House' activity ofPulse Polio Programme. The faculty and college areregularly participating in Perfect Health Mela.
The College is also working as a "Regional StudyCentre" for Post-Basic B.Sc. (N) programme of Indira
Gandhi National Open University since 1997. Facultyare participating in clinical teaching of IGNOUstudents of B.Sc. (N) programme and act asCounsellors to implement some courses.
Several faculty members have participated andorganized short course and workshops. Some ofthem have published and presented papers ondifferent themes and different situations. Many ofstaff members are the executive members of variousProfessional organizations.
Achievements:
The modification/renovation work in the Students'Hostel and in the toilets of Teaching-cum-Administrative Block of the College has beencompleted and an amount of Rs.3,29,55,664.00(Three Crores Twenty Nine Lacs Six Hundred andSixty Four) only, out of a total amount of Rs.Rs.,6,52,89,000/- (Six Crores Fifty Two Lacs and EightyNine Thousands) only, received from Ministry ofHealth and Family Welfare, Govt. of India for thepurpose, has already been paid to the HSCC for theabove mentioned work.
15.815.815.815.815.8 All India Entrance ExaminationAll India Entrance ExaminationAll India Entrance ExaminationAll India Entrance ExaminationAll India Entrance Examinationfor Admission to for Admission to for Admission to for Admission to for Admission to MBBSMBBSMBBSMBBSMBBS/////BDSBDSBDSBDSBDSCourses, 2008 Conducted byCourses, 2008 Conducted byCourses, 2008 Conducted byCourses, 2008 Conducted byCourses, 2008 Conducted byCentral Board of SecondaryCentral Board of SecondaryCentral Board of SecondaryCentral Board of SecondaryCentral Board of SecondaryEducation (Education (Education (Education (Education (CBSECBSECBSECBSECBSE)))))
The 22nd All India Pre-Medical/Pre/Dental EntranceExamination was conducted in two stages(Preliminary & Final) by Central Board of SecondaryEducation (CBSE) on 6.04.2008 and 11.05.2009 for15% All India Quota seats in Medical/Dental courseat all over the country. Total 148865 candidatesappeared for Preliminary examination. On the basisof the result of Preliminary Entrance Examination,22014 candidates had been declared qualified forfinal stage examination. The final result was declaredon 07.06.2008 and 4412 candidates were placed inthe merit/waiting list. Allotment was made upto rankUR- 3386 in 114 Government Medical and 27 DentalColleges on 1686 MBBS and 192 BDS course seatsrespectively.

212
ANNUAL REPORT 2008-09
Allotment of College and courses to the successfulcandidates were made as per their rank by VideoConferencing at three centers AIIH&PH, Kolkata,JIPMER, Puducherry and New Delhi by VideoConferencing in two rounds and Extended 2nd Roundwas held at the direction of the Hon'ble SupremeCourt of India from 10-09-08 to 14-09-08. 442candidates appeared for counseling at AIIH&PH,Kolkata, 417 at JIPMER, Puducherry and 3169 atCHEB, New Delhi. The whole admission process of15% All India Quota of MBBS/BDS seats wassuccessfully completed by 14th September, 2008.
15.915.915.915.915.9 All India Entrance ExaminationAll India Entrance ExaminationAll India Entrance ExaminationAll India Entrance ExaminationAll India Entrance Examinationfor Admission to 50% Post-for Admission to 50% Post-for Admission to 50% Post-for Admission to 50% Post-for Admission to 50% Post-Graduate Seats-2008 ConductedGraduate Seats-2008 ConductedGraduate Seats-2008 ConductedGraduate Seats-2008 ConductedGraduate Seats-2008 Conductedby by by by by A.I.I.M.S.A.I.I.M.S.A.I.I.M.S.A.I.I.M.S.A.I.I.M.S. New Delhi. New Delhi. New Delhi. New Delhi. New Delhi.
The Entrance Examination was held at 104 Centersin 15 capital cities in the country on 13.01.08 A total52,689 candidates were registered and 47,340candidates appeared in the examination foradmission to MD/MS/Diploma and MDS courses. Theresult was declared on 15-02-08 for enabling theallotment of seats for the merit/wait list candidates in96 Medical and 20 Dental College all over India.There were 3143 recognized/approved seats in MD/MD/Diploma Courses and 126 approved seats inMDS course under the 50% All India PG Quota for2008. The allotment were made to the successfulcandidates by personal appearance from 23.02.08to 15.03.08 (1st round) & From 22.04.08 to 09.05.08(2nd round and extended 2nd round at direction ofHon'ble Supreme Court of India from 24.05.08 to30.05.08 for merit and wait listed candidates forunallotted Seats). The whole admission process toAll India Quota PG/Diploma seats was successfullycompleted by 30.05.08.
15.1015.1015.1015.1015.10 Allocation of Medical/DentalAllocation of Medical/DentalAllocation of Medical/DentalAllocation of Medical/DentalAllocation of Medical/DentalSeats From Central PoolSeats From Central PoolSeats From Central PoolSeats From Central PoolSeats From Central Pool
MBBS and BDS seats:
A Central Pool of MBBS and BDS is maintained bythe Ministry of Health and Family Welfare by seekingvoluntary contribution from the various States havingmedical colleges and certain other Medical Education
Institutions. In the academic session 2008-09, 262MBBS and 28 BDS seats were contributed by theStates and medical institutions. These seats wereallocated to the beneficiaries of the Central Pool,viz., States/Union Territories, which do not havemedical/dental colleges of their own, Ministry ofDefence (for the wards of Defence Personnel),Ministry of Home Affairs (for the children of para-military personnel and Civilian Terrorist Victims),Cabinet Secretariat, Ministry of External Affairs (formeeting diplomatic/bilateral commitments and for thechildren of Indian staff serving in Indian Missionabroad), Ministry of Human Resource Development(for Tibetan Refugees) and Indian Council for ChildWelfare (for National Bravery Award winningchildren).
MDS Seats:
There are 4 MDS seats in the Central Poolcontributed by Government of Uttar Pradesh, whichare allotted to the in-service doctors sponsored bythe States/Union Territories without MDS teachingfacility on a rotational basis. For the academic session2008-09, in-service doctors sponsored by the Statesof Sikkim, Jammu & Kashmir, Tripura and Mizoramwere nominated against these seats.
Post Graduate Medical Seats for ForeignStudents:
There are 5 P.G. medical seats in the Institute ofMedical Sciences, Banaras Hindu University,Varanasi, reserved for foreign students in a calendaryear. The foreign students against these seats arenominated by the Ministry of Health & Family Welfareon the advice of Ministry of External Affairs. Duringthe year 2008, these seats were allocated to thecandidates from Nepal (2 seats) and Mauritius (3seats).
15.1115.1115.1115.1115.11 National Board of ExaminationsNational Board of ExaminationsNational Board of ExaminationsNational Board of ExaminationsNational Board of Examinations
The National Board of Examinations was establishedin 1975 on the basis of the Report of a WorkingGroup set up by the Government of India. TheNational Board functioned as a wing of the NationalAcademy of Medical Sciences from 1975 to 1982 andthe Government of India, after a review, took a policy

213
ANNUAL REPORT 2008-09
decision to make it an independent autonomous bodywith effect from March 1, 1982 under the Ministry ofHealth and Family Welfare. The Board conductsexamination in 58 specialties and nine Dentalspecialties and has accredited more than 550institutions/hospitals in public and private includingcorporate sector hospitals all over the country forthe purposes of training of candidates in variousspecialties to take the Board's examinations. Duringthe year 2007-2008, the accreditation committeerecommended accreditation to 273 departments ofvarious hospitals accounting for an annual intakecapacity of 362 students in different specialties. Inaddition 316 specialties of various accreditedinstitutions/hospitals were given renewal for 520seats for a further period of three years.
The Diplomate qualifications awarded by the NationalBoard of Examinations have been equated withpostgraduate degree and postdoctoral levelqualifications of universities by the Government ofIndia Ministry of Health and Family Welfare.Considering the fact that India has the expertise invarious sub-specialty areas with centers having hightech equipment and trained manpower performingexceptional quality work and also keeping in mindthe need to increase manpower that can renderhighest degree of professional work the NationalBoard is also conducting Fellowship programme in16 sub-specialties. During the year under reviewcovering June 2007 and December 2007examinations 3466 and 1444 candidates passed thePrimary and final Examinations out of a total of13,405 and 5,110 respectively.
The Government of India, after taking into accountthe expertise and experience gained by the Board inthe conduct of fair examinations entrusted theconduct of Screening Test for Foreign MedicalGraduates from 2002 onwards. During the year underreport two examinations were held in September2007 and March 2008 in which 3681 candidatesappeared and 1280 candidates passed the saidexamination.
The 14th Convocation of National Board of Examinationwas held on 15th March 2008 at Christ College,Bangalore, to confer the Prestigious "Diplomate of
National Board" Degrees to the successful candidatesduring the session of December 2006 and June 2007.On the occasion Dr. Anbumani Ramadoss, Hon'bleUnion Minister of Health and Family Welfare, Govt.of India delivered the convocation address. Prof. ARajasekaran, President of National Board ofExamination presided the Ceremony. In theconvocation, 591 candidates were awarded"Diplomate of National Board" Degrees fromDecember 2006 to June 2007 sessions.Approximately 1300 candidates in 53 specialities wereawarded the degrees in person. Dr. AnbumaniRamadoss awarded following Gold Medals to thecandidates for their outstanding performance invarious broad and super specialties:
The NBE conducted CME programmes for DNBcandidates for in the specialties of orthopedics (22-24 February 2008), medicine (1-3 February 2008 &24th to 26th February 2008), Surgery (8-10February 2008 & 27th too 29th February 2008),OBG(21-23 February 2008 & 27th to 29th March2008), Pediatrics (28th to 20th January 2008 & 24thto 26th February 2008), Ophthalmology(14th to 16thFebruary 2008), Anesthesia(15th to 17th February2008), Orthopedics (22nd to 24th February 2008),radiology (6th to 8th March 2008).
Satellite based interactive CME (teleconferencing)sessions for DNB candidates and intuitions andinteractive CME radio-counseling sessions. NBE hasentered into an agreement with the School of HealthSciences, Indira Gandhi National Open University(IGNOU), in 2006 New Delhi and has started satellitebased interactive CME sessions for DNB students.These sessions provides two way audio and one wayvideo interactions between the subject experts andDNB students and is held once a week. Interactiveteleconferencing sessions for DNB candidates usingfacilities of IGNOU are being done every Thursdayfrom 2.30 PM to 7.30 PM at IGNOU. Interactive radiocounseling sessions for DNB candidates usingfacilities of IGNOU are being done every Thursdayfrom 5.00 PM to 6..00 PM at IGNOU. DVDs for DNBcandidates were developed by the Board in variousspecialties during the year as follows:
214
ANNUAL REPORT 2008-09
Medicine (vol. I to VII) ;Dermatology ( vol. I to IV);Surgery ( Vol. I to XV); OBG (Vol. I to XIII); Radiology( Vol. I to VI): Ophthalmology ( Vol.. I to IX); ENT (Vol. I to VI): Orthopedics ( Vol. I to XVII); Anesthesia( Vol. I to XI); Pediatrics ( Vol. I to IX); Traumaassessment & management (Vol. I to II); Bed sideteaching ( Vol. I); Emergency management ( Vol. I toIII); research methods and statistics ( Vol. I to III);Issues related to clinical practice ( Vol. I to III)
15.1215.1215.1215.1215.12 National Academy of MedicalNational Academy of MedicalNational Academy of MedicalNational Academy of MedicalNational Academy of MedicalSciences (India)Sciences (India)Sciences (India)Sciences (India)Sciences (India)
The National Academy of Sciences (India) wasestablished in 1961 as a registered society with theobjective of promoting the growth of medicalsciences. It recognizes talent and merit throughoutthe country in the form of election of Fellows andMembers of the Academy.
As on 31st August, 2008, the NAMS has on its rolls,6 Hony. Fellows, 756 Fellows and 4203 Members.The Annual Meeting of the Academy was held atAmritsar on 26th, 27th and 28th October, 2007. ShriParkash Singh Badal, Hon'ble Chief Minister of Punjabwas the Chief Guest.
Sixty one candidates were given Scrolls of Fellowshipand Membership of the Academy at the ceremonialoccasion of the Convocation of Academy at Amritsar.Life Time Achievement Award was conferred on Dr.Man Singh Nirankari. The General Body Meetingwas held on 27th October, 2007. Ten Orations andseven Awards were awarded to eminent MedicalScientists of the Country for the 2007-2008.
Since 1982, CME programme is an important activityof the NAMS to keep medical professionals abreastwith newer/current medical problems of the countryand to update their knowledge for better delivery ofmedical education, patient care and health care atlarge.
In this financial year, financial assistance has beenprovided to various Medical Institutions to conductseven seminars, workshops and CME's. EmeritusProfessors of NAMS: In order to strengthen theintramural CME Programmes, the Academy hasappointed 45 eminent Fellows of the Academy for
Emeritus Professorship. The Emeritus Professorshave been assigned the responsibilities viz. (i) toidentify one or more medical colleges where intramuralCME of NAMS can be organized and where lecturescan be given by designated emeritus Professors whowill also strengthen the Postgraduate MedicalEducation through clinical rounds, case discussionor laboratory exercises, (ii) to suggest topics/ subjectrelated to their expertise for intramural CME and wouldassist in organizing and conducting these with NAMSsupport, (iii) to undertake travel to any part of thecountry at least once a year and visit one or twomedical institutions to deliver lectures, seminars andalso contribute towards academic activities andtraining of Postgraduates. The Directory of theEmeritus Professors has been printed and has beensent to the Principals and Vice-Chancellors of MedicalColleges and Universities.
Intramural CME Programmes: The CME Programmecommittee identifies, from time to time, topics ofnational and academic relevance for funding asintramural CME Programmes. The Academy providesTA/DA and honorarium to Fellows who attend theCME programmes as Observers. During the year2007-2008, one intramural CME programmes on"Community Acquired Pneumonia" was organizedby Dr. S. K. Jindal FAMS on 23rd December, 2007 atPostgraduate Institute of Medical Education andResearch, Chandigarh.
In pursuance and furtherance of the objectives ofContinuing Medical Education Programmes ofNational Academy of Medical Sciences (India), theAcademy has established a NAMS - P.G.I.M.E.R.,Chandigarh Centre for tele-education in the HealthSciences. The Annual Symposia are transmitted toIndira Gandhi Medical College, Shimla and Pt. B.D.Sharma P.G. Institute of Medical Sciences, Rohtakvia tele-linkage.
The CME programme also covers Human ResourceDevelopment by sending Junior Scientists to Centresof excellence for providing training in advancedmethods and techniques. Fourteen MedicalScientists/Teachers have been selected for advancetraining at specialized centres out of which sevenhave already completed the advanced training.

215
ANNUAL REPORT 2008-09
During 2008-2009, total grants of Rs. 50.00 lakhsand Rs. 20.00 lakhs under Plan and Non-Planrespectively have been sanctioned. Out of thisRs.37.50 lakhs and Rs.15.00 lakhs under Planand Non-plan respectively have been released bythe Ministry of Health and Family Welfare
15.1315.1315.1315.1315.13 All India Institute of MedicalAll India Institute of MedicalAll India Institute of MedicalAll India Institute of MedicalAll India Institute of MedicalSciences (Sciences (Sciences (Sciences (Sciences (AIIMSAIIMSAIIMSAIIMSAIIMS)))))
All India Institute of Medical Sciences (AIIMS) wasestablished in 1956 by an Act of Parliament as aninstitution of national importance. AIIMS wasconceived to be a center of excellence in modernmedicine with comprehensive training facility. Thiswas in pursuance to the recommendations made bythe Bhore Committee in 1946.
The institute has been entrusted to develop patternsof teaching in undergraduate and postgraduatemedical education in all its branches so as todemonstrate a high standard of medical educationto all medical colleges and other allied institutions inIndia, to bring together at one place educationalfacilities of the highest order for the training ofpersonnel in all important branches of health activity,and to attain self sufficiency in postgraduate medicaleducation. For pursuing academic programmes, theAIIMS has been kept outside the purview of theMedical Council of India. The Institute awards itsown degrees. The AIIMS continues to be a leader inthe field of medical education, research and patient-care in keeping with the mandate of the Parliament.
The Institute is fully funded by the Government ofIndia. However, for research activities, grants arealso received from various sources including nationaland international agencies. While the major part ofthe hospital services are highly subsidized for thepatients coming to the AIIMS hospital, certaincategories of patients are charged for treatment/services rendered to them.
Medical Education
Undergraduate Medical Education
This year Government has increased the OBC seatsin undergraduate courses as well as postgraduate
courses as indicated against each: 27 seats in MBBS,41 seats in MD/MS, 09 seats in M.Sc/M.Biotech, 04seats in M.Sc Nursing, 02 seats in B.Sc (H)Ophthalmic Techniques, 02 seats in B.Sc (H)Radiotherapy, 10 seats in B.Sc (H) Nursing, 04 seatsin B.Sc (PC) Nursing.
This year the Institute is to be admitted 77 studentsto its MBBS course. Out of 77 seats 5 reserved forforeign nationals and 3 seats awaited from waitinglist. 24 students to B.Sc Nursing (post-certificate)course, 60 students to B.Sc (Hons) in NursingCourse, 14 students to B.Sc. (Hons.) in OphthalmicTechniques and 8 students to B.Sc (Hons.) in MedicalTechnology in Radiography.
The MBBS course is spread over 5 ½ years, dividingthe period to 1 year for pre-clinical, 1 ½ year forpara-clinical, 2 year for clinical and 1 year rotatinginternship. Para-medical courses like B.Sc (Hons)in Nursing, Ophthalmic Techniques, MedicalTechnology in Radiography continued to be popularand attracted students from other countries also. Thecurricula of these courses are under constantscrutiny by the faculty of the Institute for purposes ofimprovement.
Post-Graduate Medical Education
During 2008-2009 session (i.e. for the coursescommencing in January 2008 and July 2008, 378students were admitted to various postgraduate,post-doctoral and superspeciality courses i.e. M.D,M.S., M.D.S., M.H.A., Ph.D, M.Ch, D.M. and M.Sc invarious specialities. 43 candidates belonging to theschedule caste (SC), 09 belonging to the scheduletribes (ST) and 28 candidates belonging to otherbackward classes (OBC) got admission to thepostgraduate courses. The Institute provide full timepostgraduate and post-doctoral courses in 57disciplines. In the year under review, manypostgraduate students qualified for various degreesand qualified for various superspeciality degrees.The guiding principle in postgraduate training is totrain them as teachers, researchers and above allas competent doctors to manage and treat thepatients independently.

216
ANNUAL REPORT 2008-09
Continuing Medical Education
The institute organized a number of workshops,symposia, conferences and training programme incollaboration with various national and internationalagencies during the year. Professionals from variousinstitutions all over the country participated in theseseminars and workshops and benefited with updateknowledge. Guest and Public lectures wereorganized by visiting experts and faculty of AIIMS.
Training for Long term/Short term, WHO-in-Country Fellowship and Elective Training to theForeign Nationals Students.
The institute is also providing short/long term training,WHO-in-Country Fellowship and Elective training tothe Foreign Nationals students.
Training for Scheduled Castes (SC) and theScheduled Tribes (ST) Candidates.
The SC and ST candidates are given dueconsideration and weightage in accordance with theGovt. of India guidelines in all selections. During thecurrent year 39 SC/ST candidates were selected forvarious undergraduate courses. 5 SC and 3 STcandidates were selected to the MBBS course, 2 SCand 1 ST candidates were admitted to B.Sc (Hons)Ophthalmic Technique, 1SC and 1 ST candidatesadmitted to B.Sc (Hons) Medical Technology inRadiography course, 3 SC and 8 ST candidatesadmitted to B.Sc Nursing (Post-certificate) course and65 candidates were admitted to B.Sc (Hons) Nursingcourse during the year including 9 SC, 5 ST, 7 OBCand 5 Foreign National candidates.
International Role
The Institute continued to provide consultancyservices in several neighbouring countries underbilateral agreements or under the aegies orinternational agencies. During 2008-2009 theinstitute trained many WHO-Sponsored candidatesto fulfill its international obligations.
Research
As per the mandate given to the All India Institute ofMedical Sciences, research forms an important
component. AIIMS has been at the forefront ofconducting high quality research, both in the fieldsof basic and applied sciences. During the year underreview, the faculty of the AIIMS drew extramuralgrants for various research projects from nationaland international agencies.
Patient-Care Services
The hospital has maintained its tradition of servicesand quality of patient care, in spite of ever increasingnumber of patients that come to this hospital from allover the country as well as from abroad. A total ofmore than 10,00,000 patients attended the generaloutpatient department and specialty clinics of themain hospital and other centres of AIIMS. A total ofmore than 50,000 patients were admitted during theyear in the various clinical units of the Main Hospitaland other centers at AIIMS. A total of more than50,000 of surgical procedures performed during theyear in different surgical disciplines at AIIMS from01.04.2008 to 31.08.2008
Centre/Department wise information regardingimportant achievements and newer facilities for theAnnual Report 2008-2009 of the Ministry of Health &Family Welfare, Govt. of India, period covered01.04.2008 to 31.08.2008.
DR BRA Institute Rotary Cancer Hospital
The Dr. BRA Institute Rotary Cancer Hospital werestarted the following achievements/new facilitiesbetween 1/4/2008 and 31/8/2008 under Dr. VinodRaina, HOD, Medical Oncology, Dr. N.K. Shukla, HOD,Surgical Oncology and overall control of Dr. G.K.Rath, Chief, Dr. BRA Institute Rotary Cancer Hospital.
� Started Lung Cancer Chemotherapy clinic
� Started Transplant Clinic
� IGRT machine started functioning
Neurosurgery
The department is actively involved in patient care,academic activities and research. In the year 2007-2008, about 32000 patients were treated in the OPD,3400 patients were operated and 230 patients
217
ANNUAL REPORT 2008-09
underwent gamma-knife surgery. It is activelypursuing in the fields of vascular, tumor, spine,epilepsy, functional and minimally invasiveneurosurgery. In the field of research, the departmentis pursuing cutting edge research. Notable areas ofresearch include hydrocephalus, the pathologicalbasis and management of severe head injury,genetics of developmental spine, neuromodulationin vascular dementias as well as management of highgrade gliomas. The department has also receivedfunding to the tune of Rs 2 crores from DST forhaving a skull base and microneurosurgical lab.During this year, 4 new OT's in the CN tower havebecome functional with state of art infrastructuresupport. The commission of intraoperative MRI withbrain suite is actively in process and is expected tobe completed soon. The department conductedvarious CMEs, workshops and conferences duringthe year and its faculty continue to receive recognitionand awards for excellence in patient care andresearch. The annual AIIMS microneurosurgeryworkshop has successfully completed 10 years andhas attained National and International status.Faculty and residents won best research paperawards in National and international conferences
Radio-Diagnosis
The Department of Radio-diagnosis was installed thefollowing equipments during April 2008 to July 2008under the supervision of Dr. Arun Kumar Gupta, Head,Department of Radio-diagnosis.
� Radio frequency Ablation System
� Motorized X-ray Film Viewer
� Sonosite Micro max Portable Ultrasound Units
� Digital Flat Panel Detector X-ray Unit
Department of Psychiatry
Besides the Head of the department, the departmentcurrently has 4 Professors, 1 Associate Professorand 2 Assistant Professors.During this period, thedepartment examined 14556 (new and old cases) inthe OPD and, 170 patients were admitted in the ward.Besides these, 367 patients were seen in the ChildGuidance Clinic and 446 patients were seen in theDe- addiction clinic.
The department is involved in training ofPostgraduate students (MD-Psychiatry), Ph.Dprogramme in cl inical Psychology, , underGraduate medical students and students of BSc.Nursing.The department has opened a childrenadolescence psychiatry in-patient division inC1ward in May 2008. The department is providingtechnical expertise in development of 'Familytherapy course' for IGNOU.
In this period, nine research projects on variousaspects of mental health are ongoing and are beingfunded by national and international agencies.Thefaculty of the department delivered invited talks innational and international meetings.
National Drug dependence Treatment Centre
Besides the Chief, the Centre has eight facultymembers: Professors-3, Additional Professor-1Associate Professor-1 and 3 Assistant Professors.
During this period, a total of 14700 (new and old)patients in the OPD, 13000 in the Community clinic,23 patients in the Adolescent Drug Abuse clinic, and340 patients in the Tobacco Use Cessation clinic, 20patients in the adolescent clinic and 130 patients inthe Dual Diagnosis clinic were seen. A total of 340patients were admitted in the ward.
During this period, laboratory investigations carriedout were: Drugs of abuse screened (6098),biochemistry (8000), haematology (2200), and HIVscreening (125, positive-6.6 %.).
The following WHO Biennium (2008-09) activities arebeing carried out:
� Development of manual-Minimum standardsof care
� Management of alcohol and drugdependence in primary care settings
� Training programme on agonist maintenance
� Assessment of drug abuse among adolescent
� Training of trainers
� Training by trainers
218
ANNUAL REPORT 2008-09
The centre organized training programme for doctorsin
� District Moregaon (Assam) and Mandsaur(MP)
� Conducted regional meetings to formulatetreatment policy in Drug and Alcohol use inAssam, Bangalore, Mumbai and Ranchi
� Has initiated district based model for provisionof care for 'substance use disorder' atMeerut, Mandsaur and Moregaon
� Conducted a training programme forpsychiatrists from the state of Punjab
The faculty visited several sites (visits to De-addictioncentres in various states; Manipur, Mizoram andNagaland) to assess outcome of patients followingtheir treatment. The Centre's Chief was appointedas member Expert Advisory Panel to Punjab StatePlanning Board.
In this period four ongoing research projects on'Substance Use Disorder" being funded by nationaland International agencies. The faculty publishedfour research articles in various national andinternational journals.
Combined Activities of the Department and theCentre
The faculty has presented their research papers innational and International meetings and chaired thesession. The faculty of the department and the centrejointly carry out postgraduate teaching that includesjournal discussion, seminar, and case conference andresearch/academic presentations once every week.
Department of Cardiac Anaesthesia
Department of Cardiac Anaesthesia is involved inthe Superspeciality Training Programme of
� DM in Cardiac anaesthesia. (1 candidateadded in July'08).
� M.Sc Perfusion Technology (four newcandidates selected).
� Specialised training in cardiac anaesthesia
and intensive care given to threepostgraduates from Lady Hardinge Hospitaland two from ESI Hospital.
Total number of 754 neonates, infants and childrenwere given anaesthesia for cardiac surgery, Cathlab procedures and CT Angio, MRI.
A total of 1251 adult patients underwent anaesthesiafor valvular, complex congenital, myocardialrevascularization, AICD/pacemaker and other cathlab procedures and CCU Ventilatory care.
Six research projects completed in the Departmentand sixteen are ongoing - of which three are fundedby AIIMS and two by ICMR.
Three research papers are published in National andInternational Journals and eight are accepted forpublication.
The Faculty of the department is involved in trainingJunior and senior residents of AIIMS and residentsfrom other government hospitals in TransesophagealEchocardiography.
Three Faculty members are holding senior positionsin Assosciations like PRAN (Parkinson relatedAwareness) and IACTA (Indian Association ofCardiothoracic Anaesthesiologists).
Community Service - Stress management forCardiac and Neurosurgical patients is run as aspecialized clinic and department is also involved inprogrammes like "Quit Tobacco" and "Stress RelieveProgramme".
Department of Microbiology
The department of Microbiology has started MalariaParasite drug sensitivity assay, Influenza virusisolation and identification from hospital andcommunity patients. We are doing Anti-tuberculardrug sensitivity testing for both the first line and thesecond line drugs especially useful in Multi DrugResistant TB patients, using rapid culture andmolecular methods. Antifungal susceptibility foryeasts and antigen detection for Cytomegalovirusin transplant recipients is also being done.Serological tests for novel infectious agents causing
219
ANNUAL REPORT 2008-09
pneumonia and PCR for agents responsible forgenital tract infections have been started. HIV viralload and drug resistance detection is being donefor HIV patients
The department is contributing to the NationalProgrammes for Tuberculosis and HIV. We arecontributing to the Revised National TB ControlProgramme at the policy level and by organizing anannual conference of all the medical colleges forcontribution to RNTCP. The HIV laboratory is aNational Reference Laboratory and the Virologylaboratory is a WHO Surveillance National NetworkCentre for Influenza and National Reference centrefor Dengue.
The Microbiology faculty serves as experts on severalNational and International bodies of repute.
The department has generated extramural funds tothe tune of eight crores including two internationalprojects funded by CDC, USA.
Pioneering research in the fields of moleculardetection of intestinal parasites causing severediarrhea and pneumonia in immuno-compromisedpatients, and development of DNA sensors to agentscausing gonorrhea, development of rapid molecularmethods for the detection of Extensively drugresistant tuberculosis(XDR-TB) is ongoing and wouldprove to be very useful.
Department of Cardiac-Radiology
The Department of Cardiac-radiology has organizedthe ISVIR Annual Registry meet on 26-27 April, 2008at AIIMS.
The department faculty delivered 10 guest lecturesin National and International Conferences/Workshops from April to August, 2008 and six indexpublications published by the faculty during thatperiod. Currently three research projects areongoing in the department. Patient care from Aprilto August are as follows:
Cine Fluroscopy 2640, Vascular catheter procedures199/1725, Ultrasound 540, CT 516, MRI 209, RoutineX-ray for CTVS and Cardiology 24908.
Department of Cardiology
The Department of Cardiology has catered to over55,000 outpatients. Over 10,000 patients hadundergone echocardiography, and over 2000cardiac catheterizations were performed. Overallaround 550 patients had undergone interventionalprocedures including coronary angioplasty, balloonvalvuloplasty and device implantations during the lastfive months.
Department of Cardiology has been renovating itsexisting facilities to cope with its ever increasingdemands. The Echo lab and Holter lab have beenrenovated and started functioning with addedcapacity. Major renovation work has stated in cardiaccatheterization lab and TMT lab. A new biplanecardiac catheterization laboratory is being installed,which will facilitate catheterization of children.
Department is actively involved in many intramuraland extramural research projects. Newer projectsincluding stem cell research in dilatedcardiomyopathy and ischemic heart disease areunderway. Efforts have been made to refocus theeducational activities of the department to addressthe changing needs of current cardiology practice.
Stem Cell Facility
SCF at AIIMS has started three Multi-centric trials toevaluate the role of stem cells in MyocardialInfarction, Stroke, Limb Ischemia.We are the centralCo-coordinators in Stroke and Limb Ischemia whichinvolves five different centers in India.
The Department of Biotechnology, Govt. of India hassanctioned the proposal for the establishment of"Center of Excellence" in the field of Stem Cell atStem Cell Facility, AIIMS.
Six new research proposals have been approved byICMR and DBT for financial assistance to conductStem Cell research at Stem Cell Facility.
One Workshop on Stem Cell Enumeration by FlowCytometer was conducted by Stem Cell Facility totrain scientists working on various stem cell projectson 15th Sept 2008.Total 4 Ph.D students are
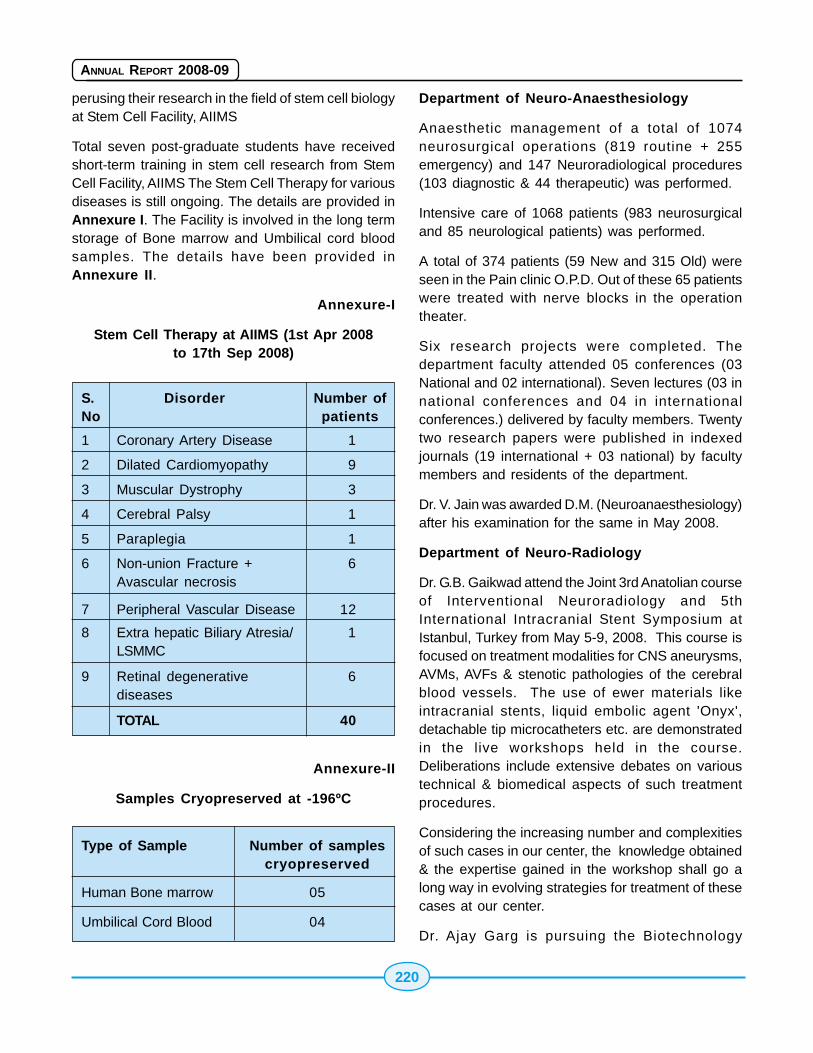
220
ANNUAL REPORT 2008-09
perusing their research in the field of stem cell biologyat Stem Cell Facility, AIIMS
Total seven post-graduate students have receivedshort-term training in stem cell research from StemCell Facility, AIIMS The Stem Cell Therapy for variousdiseases is still ongoing. The details are provided inAnnexure I. The Facility is involved in the long termstorage of Bone marrow and Umbilical cord bloodsamples. The details have been provided inAnnexure II.
Annexure-I
Stem Cell Therapy at AIIMS (1st Apr 2008to 17th Sep 2008)
S. Disorder Number ofNo patients
1 Coronary Artery Disease 1
2 Dilated Cardiomyopathy 9
3 Muscular Dystrophy 3
4 Cerebral Palsy 1
5 Paraplegia 1
6 Non-union Fracture + 6Avascular necrosis
7 Peripheral Vascular Disease 12
8 Extra hepatic Biliary Atresia/ 1LSMMC
9 Retinal degenerative 6diseases
TOTAL 40
Annexure-II
Samples Cryopreserved at -196ºC
Type of Sample Number of samplescryopreserved
Human Bone marrow 05
Umbilical Cord Blood 04
Department of Neuro-Anaesthesiology
Anaesthetic management of a total of 1074neurosurgical operations (819 routine + 255emergency) and 147 Neuroradiological procedures(103 diagnostic & 44 therapeutic) was performed.
Intensive care of 1068 patients (983 neurosurgicaland 85 neurological patients) was performed.
A total of 374 patients (59 New and 315 Old) wereseen in the Pain clinic O.P.D. Out of these 65 patientswere treated with nerve blocks in the operationtheater.
Six research projects were completed. Thedepartment faculty attended 05 conferences (03National and 02 international). Seven lectures (03 innational conferences and 04 in internationalconferences.) delivered by faculty members. Twentytwo research papers were published in indexedjournals (19 international + 03 national) by facultymembers and residents of the department.
Dr. V. Jain was awarded D.M. (Neuroanaesthesiology)after his examination for the same in May 2008.
Department of Neuro-Radiology
Dr. G.B. Gaikwad attend the Joint 3rd Anatolian courseof Interventional Neuroradiology and 5thInternational Intracranial Stent Symposium atIstanbul, Turkey from May 5-9, 2008. This course isfocused on treatment modalities for CNS aneurysms,AVMs, AVFs & stenotic pathologies of the cerebralblood vessels. The use of ewer materials likeintracranial stents, liquid embolic agent 'Onyx',detachable tip microcatheters etc. are demonstratedin the live workshops held in the course.Deliberations include extensive debates on varioustechnical & biomedical aspects of such treatmentprocedures.
Considering the increasing number and complexitiesof such cases in our center, the knowledge obtained& the expertise gained in the workshop shall go along way in evolving strategies for treatment of thesecases at our center.
Dr. Ajay Garg is pursuing the Biotechnology

221
ANNUAL REPORT 2008-09
Associateship at UCSF, San Francisco, USA to learnthe newer methodologies in MR imaging inneurosciences. His experience will enhance thescope of MR applications in patients with neurologicaldiseases at our center.
Total number of investigations including therapeuticprocedures under taken during April 2008 to August2008 are 21315. This includes use of 'Onyx' incerebral AVMs & Intracranial stent assistedprocedures in the department.
Department of Orthopaedics
The Department of Orthopaedics at AIIMS has alwaysbeen adjudged as the leading light of orthopaedicsin the country. Highly complex surgeries in the fieldof trauma, tumor, hand, spine, joint replacement,arthroscopic surgery and paediatric orthopaedics aredone on a regular basis. A number of researchprojects funded by ICMR, DST, DBT and CSIR arebeing carried out in the department. The departmenthas a number of text book and indexed publicationsto its credit. The faculty members have activelycontributed in many CMEs at national andinternational levels. The department has also servedthe country at various health camps at far-flungremote areas. The department continues to enjoythe trust and faith of millions of countrymen and isthe best testimony to its characters.
Department of Nuclear Magnetic Resonance
From Molecular imaging to material characterization,the department has been pursuing research in thefiled of MRI, MRS, fMRI in animal and humans systems.The department has embarked on functional MRI withfeedback response system (capable of visual cueswith response) and stem-cell imaging this year.
Department of Pediatric Surgery
Since 1971, the Department of Pediatric Surgery atAIIMS has always been on the forefront in teaching,patient care and research, including rural healthprograms, matching some of the best centers in theworld. Since 1972, over 70 candidates (under the 3& 6 year training programs) have been trainedreceiving their M.Ch degrees in Pediatric Surgery.
The experienced faculty manages the quality patientcare that includes care of the neonates, infants andchildren with surgical problems (routine andemergency) dealing with neonatal surgery, oncologysurgery, thoracic, urological gastrointestinal, plastic,neurosurgical, traumatology and Endoscopy.
Department of Biochemistry
This period is of importance because the increasedbatch of students MBBS 50 to 77 was admitted forthe first time. The Academic schedule for this batchhas been implemented, within the existing facilities,with some temporary adjustments like practicalclasses in two shifts that extend up to late evening.
Department of Nephrology
Department of Nephrology has been involved inproviding state of art kidney care facilities for patientssuffering from various nephrological problems liketransplantation and dialysis. Uniquely our center isonly Govt. center involved in providing renaltransplant facilities.
Department of Physical Medicine andRehabilitation
The Department of Physical Medicine andRehabilitation has started new facilities this year i.e.(i) Low temperature thermoplastic use started forOrthotics. Initiated sand casting. (ii) Technique fortaking measurement for artificial limbs wherebyreducing requirement for plaster casting. Hencemaking limb fitting faster, less messy andinexpensive. (iii) Started fitting LN 4 hands for belowelbow amputees under donation scheme of Rotariansin the USA.
Department of Medicine
Department of Medicine provides world-class tertiarycare services in all aspects of medicine. It has manyprestigious scientific publications to its credit.Department attracted visiting students and facultiesacross the globe. Department of Medicine runs abusy ICU where patients with multiple co-morbidconditions are managed. We have looked intovarious aspects of ventilator-associated pneumonia,nosocomial infections and nutrition in critically ill
222
ANNUAL REPORT 2008-09
patients. Department continues to providecomprehensive care including free antiretroviraltherapy to more than thousand patients. Thedepartment also advices the Government on variouspolicies and programs for the elderly. Major researchareas have been infections in the elderly, spectrumof diseases in elderly and diabetes in elderly.
Department of Neurology
The major break through in this year was formingresearch proposal for ethical conduct of stem celltherapy for several neurological disorders which donot have any treatment. These areas are staticencephalopathy like Cerebral Palsy, Motor NeuronDisease, Muscular Dystrophy, Spinal Cord injury andother Neurological disorders.
Comprehensive programmes for the managementof patients with Parkinson's Disease, Stroke,Epilepsy are being carried out. The department incollaboration with DST, ICMR and other national/international agencies is actively carrying outresearch activities for various NeurologicalDisorders.
Centre for Community Medicine
The Centre for Community Medicine is activelyinvolved in giving technical inputs for National Ruralhealth Mission, It is also involved with the NationalHealth Systems Resource Centre. The Centre isalso continuing to give inputs in various NationalHealth Programme such as:- (i) National AIDS ControlProgramme (ii) National Iodine Deficiency DisordersControl Programme (III) National Cancer ControlProgramme. A new hostel for students and residentdoctors is under construction at ComprehensiveRural Health Services Project, Ballabgarh.
The Institute has granted preliminary approval forconstruction of a Community Health Centre/PrimaryHealth Centre at Village Fatehpur Billoch, Ballabgarh,District Faridabad. This is required for impartingtraining in the field of health care delivery. Theprocess of transfer of land is under way.
The Centre through its Health Promotion and HealthCommunication Unite has initiated a unique "Pre-
Marriage Training Course". It contributed actively inorganizing relief for Bihar floods.
Department of Gastroenterology & HNU
A molecular biology laboratory was set up with a 65lakhs grant awarded by Department of Science andTechnology (DST), GOI under the FIST program. Astate of the art Endoscopy Theatre with angiographicfacility has been created. 15 papers published inNational and International journals.
15.1415.1415.1415.1415.14 Jawaharlal Institute of PostJawaharlal Institute of PostJawaharlal Institute of PostJawaharlal Institute of PostJawaharlal Institute of PostGraduate Medical EducationGraduate Medical EducationGraduate Medical EducationGraduate Medical EducationGraduate Medical Educationand Research (JIPMER)and Research (JIPMER)and Research (JIPMER)and Research (JIPMER)and Research (JIPMER)
Jawaharlal Institute of Post Graduate MedicalEducation and Research (JIPMER), has now becomean autonomous body w.e.f. 14.7.2008 through anAct of Parliament. The primary functions of thisInstitute are patient care, teaching, training andresearch. During the year under review, the Institutehas made all round progress in all its activities.
The hospital caters to the needs of poor patient byproviding efficient health care in a clean and neatenvironment by a team of dedicated doctors, nursesand other supporting staff. About 4285 patients fromPuducherry and other parts of the country attendOPD everyday. 12,69,201 outpatients and 56,210inpatients were treated during 2007. 36,876operations were performed and 12,950 deliverieswere conducted. Special Clinics have recorded anattendance of 2,28,999 and the attendance inEmergency medical services was 99,208. The bedoccupancy rate for the hospital is above 100.5%.Most of the patients receive free treatment, whichincludes latest advanced superspeciality services likeopen heart surgery, pace maker implantations,angioplasty and other cardiovascular interventionalprocedures.
Hospital Blood Bank conducted 51 blood donationcamps during the year. About 2254 permanentpacemakers were planted by the department mostlyon poor patients from rural areas. A new OPD forPhysical Medicine & Rehabilitation was started andfunctioning from May 2007.
223
ANNUAL REPORT 2008-09
The hospital provides most modern allopathictreatment for all diseases and disorders. It hasmodern sophisticated diagnostic and therapeuticfacilities that are provided free of cost to patients. ADrug Information Centre has been set up in theDepartment of Pharmacology which caters to thequeries related to drugs in clinical practice andrelated information. The buildings of RegionalCancer Centre, Nursing College & Hostel have beenrecently inaugurated by Hon'ble Union Minister forHealth and F.W (Photograph of the inaugural functionof Regional Cancer Centre, Nursing College & Hostel,1000 MA Digital X-Ray Machine, Colour DopplerUltrasound Machine and Patients Shelter isenclosed). A 360 bedded Super Speciality Block,Trauma Care Centre are under construction. Morenew projects like a 400 bedded Maternity & ChildHealth Block etc. are to be taken up in the EleventhPlan. A 1000 MA Digital X-ray machine and anadvanced Colour Doppler Ultrasound machine forthe Department of Radio Diagnosis were equipped.In addition to this, equipments and services havebeen added in Departments like Biochemistry, TB &CD, Orthopaedics, CTVS etc.
This Institute runs Medical and Para-medical trainingcourses, leading to M.B.B.S., MD/MS and Diplomain various specialities. Post-doctoral course i.e. D.M.(Cardiology), M.Ch.(Genito-Urinary Surgery), M.Ch.,(Cardio-Thoracic and Vascular Surgery), M.Sc. inMedical Biochemistry, B.Sc. (Medical LaboratoryTechnology), full time Ph.D. Programme in the Pre-para clinical subjects. All admissions are made on AllIndia basis competitive Entrance Examination.Students from all over the country appear in theseexaminations and merit is the sole criterion foradmission. A number of Research Projects havebeen going on in many Departments of the Instituteviz. Department of Biochemistry, Dermatology & STD,ENT, Microbiology, Opthalmology, Obst. andGynaecology, Pharmacology, Physiology, P & SM etc.A number of conferences and workshops wereorganized by some Departments and paperspresented in most of them.
15.1515.1515.1515.1515.15 Post Graduate Institute ofPost Graduate Institute ofPost Graduate Institute ofPost Graduate Institute ofPost Graduate Institute ofMedical Education andMedical Education andMedical Education andMedical Education andMedical Education andResearch (Research (Research (Research (Research (PGIMERPGIMERPGIMERPGIMERPGIMER),),),),),ChandigarhChandigarhChandigarhChandigarhChandigarh
DERMATOLOGY
1. Dr. Sanjeev Handa was awarded the "IndianCouncil of Medic=l Research Lala Ram ChandKandhari Award-2007" for research in dermatology.
GASTROENTEROLOGY
1. Professor D.K. Bhasin was nominated as aFellow of the prestgious National Academy of MedicalSciences (NAMS).
HEPATOLOGY
1. Prof. Y. Chawla became an internationalEditorial Board Member of the Digestive Diseases &Sciences and Liver International Journals.
2. Dr. R.K.Dhiman received prestigious ICMRAward "Amrut Modi Unchem Award" inGastroenterology in 2007 for his significantcontribution in Portal Hypertension. He also receivedISG-SR Naik Memorial Award from Indian Society ofGastroenterology for the year 2007, for the bestpublished work in the field of diseases of thedigestive tract and liver.
3. Dr. Virendra Singh's paper got thepresidential Poster of Distinction at AmericanAssociation for Study of Liver Disease Conferenceheld at Boston between November 2-6, 2007.
INTERNAL MEDICINE
1. Professor Ajay Wanchu was awardedFellowship of American College of Physicians andAmerican College of Rheumatology.
2. Dr. Aman Sharma, Assistant Professor won the"Young Investigator Award" at the conference of IndianRheumatology Association held in October, 2007.
IMMUNOPATHOLOGY
1. Dr. Sunil K. Arora, Additional Professor visited theLaboratory for Clinical and Biological Studies at the
224
ANNUAL REPORT 2008-09
University of Miami-Miller School of Medicine, Miami,FL, USA as 'Visiting Guest Faculty' from July toDecember 2007 on a fellowship awarded byInternational AIDS Society and HIV Research Trust,UK.
MEDICAL MICROBIOLOGY
1. Professor Arunaloke Charabarti was awardedthe Fellowship of National Academy of MedicalSciences.
2. Dr. Neelam Taneja, Associate Professor wasawarded "International Development Award forYoung Women Scientists" by International Societyof Infectious Diseases for her work on hybrid vibrios.
3. Dr. M.R. Shivaprakash was awarded "ICMRInternational Fellowship for Young Bioscientist-2007-08" to undergo training on"Molecular identificationand typing of the fungi" at Microbiology Unit,University Roviria I Virgili, Reus, Spain.
NEUROLOGY
1. Dr. Parampreet S. Kharbanda completed oneyear fellowship in Clinical Epileptology awarded bythe Epilepsy Society of Australia, at Austin HealthUniversity of Melbourne.
NUCLEAR MEDICINE
1. Dr. B.R. Mittal was selected for the award ofthe Fellowship of the Indian College of NuclearMedicine (FICNM) in December 2007.
OPHTHALMOLOGY
1. Prof. Amod Gupta received "P. Siva ReddyInternational Award" for work on IntraocularTuberculosis, "Distinguished Service Award, 2007"of The Asia-Pacific Academy of Ophthalmology and"V V Khanolkar Oration 2008" of National Academyof Medical Sciences.
2. Dr. Sushmita Kaushik was nominated YoungScientist Researcher from India by the Associationof International Glaucoma Societies.
ORAL HEALTH SCIENCES
1. Prof. H.S.Chawla was nominated for the "Life
Time Achievement Award and Fellow, ISPPD" for theyear 2007-08 by the Indian Society of Pedodontics& Preventive Dentistry.
OTOLARYNGOLOGY
1. Professor Ashok K. Gupta was conferred with"V.P. Sood Oration Award" during the year 2007 atthe 20th All India Rhinology Society Conference atAllahabad.
PAEDIATRICS
1. Dr. Meenu Singh, Additional Professor wasconferred the "Sir Shriram Memorial Award of theNational Academy of Medical Sciences for bestpublished work in Epidemiology and Medical Education.
2. Dr. Joseph L. Mathew was awarded the RoyalCollege of Paediatrics and Child Health Heinz VisitingFellowship 2007.
3. Dr. Bhavneet Bharti received the"International Degree of Diplomate in Environment& Child Health" organized by the InternationalPediatric Association (IPA) under the United NationsEnvironment Programme (UNEP).
PARASITOLOGY
Professor Nancy Malla was selected for the "Dr. H.I.Jhala Award" for 2007 by the Indian Association ofMedical Microbiologists.
PULMONARY MEDICINE
1. Dr. D. Gupta received the "Gold ScholarshipAward" for research presentation at the EuropeanRespiratory Society Annual Meeting held atStockholm, Sweden.
2. Dr. R. Agarwal received the "BronzeScholarship Award" for his research presentation atthe European Respiratory Society Annual Meetingheld at Stockholm, Sweden.
3. Dr. N. Singh was elected Fellow of AmericanCollege of Chest Physicians. He was also selectedby the American Society of Clinical OncologyFoundation to be a recipient of the "2008 InternationalDevelopment and Education Award".
225
ANNUAL REPORT 2008-09
RADIODIAGNOSIS AND IMAGING
1. Dr. N. Khandelwal delivered the prestigious"J.C. Bose Memorial Oration" for the year 2008 bythe Indian College of Radiology and Imaging and wasawarded with "Gold Medal" and a citation at the 61Annual Congress of the Indian Radiological andImaging Association held from January 17-20, 2008at Bangalore.
VIROLOGY
1. Dr. B. Mishra was awarded with theMembership of National Academy of Medical Sciences(NAMS).
15.1615.1615.1615.1615.16 Lady Hardinge Medical College Lady Hardinge Medical College Lady Hardinge Medical College Lady Hardinge Medical College Lady Hardinge Medical College& Smt. S. K. Hospital New Delhi& Smt. S. K. Hospital New Delhi& Smt. S. K. Hospital New Delhi& Smt. S. K. Hospital New Delhi& Smt. S. K. Hospital New Delhi
The Lady Hardinge Medical College, New Delhi wasestablished in the year 1916 with a modest beginningof just 14-16 students. Over the years, the Institutehas matured as a pioneering Institute for MedicalEducation and now it has a present strength of 150admissions per year for MBBS girl students. The 93rdAcademic Year (2007-08) of the College began with668 undergraduates and 127 interns on the rolls.The College, which is affiliated to the University ofDelhi since the year 1949, has continued to admitstudents from all over India, as well as from foreigncountries.
For better maintenance and preservation purpose,all registers are bouned and repaired. The hospitalstatistics for the period 2007-08 is as under:-
Bed Strength 877
OPD Attendance 3,47,437
Indoor Admissions 24001
Deliveries 9978
Bed Occupancy 75.4%
Surgeries performed:-
Minor 6743
Major 4923
Total 11666
The School of Nursing has been changed into Collegeof Nursing (50 students B.Sc., 11th September,2007). The Department of Surgery has started newResearch project. New facility like visual fieldanalyzer, high speed Vitrectomy machine, fundscamera operating microscope etc. has been addedin the Department of Ophthalmology. Departmentof Dental and Oral Surgery have conducted writtenMCQ Entrance exams for JRs. Room for Dermatologyclinic catering patients of sexually transmitted diseaseand HIV and other chronic dermatological diseasehas been added in the outpatient Department ofDermatology and STD.
Department of Community Medicine is providingcomprehensive health care to community throughHealth Care at Palam, Mehrauli and KalyanpuriHealth Care Centre. New state of the building forurban Health Centre is under construction atKalyanpuri and will be commissioned next year.
A number of research projects have been going onin many departments of the Institute viz. Departmentof Forensic Medicine & Toxicology, Department ofSurgery etc. A number of conferences andworkshops have also been organized at the hospital.
15.1715.1715.1715.1715.17 Kalawati Saran Children'sKalawati Saran Children'sKalawati Saran Children'sKalawati Saran Children'sKalawati Saran Children'sHospital, New DelhiHospital, New DelhiHospital, New DelhiHospital, New DelhiHospital, New Delhi
Kalawati Saran Children's Hospital is a premierreferral Childern's hospital of national importance.The Hospital started functioning in the year 1965 forimparting medical care service exclusively forPaediatrics patients upto 18 years of age. At presentit has 370 beds. Under the scheme for theimprovement of KSCH (JICA Project) the bed strengthof this Hospital is being increased to 500.
Kalawati Saran Children's Hospital is one of thebusiest children hospitals in the country and catersto a daily OPD attendance of 800-1000 children, and80-100 new admissions per day from Delhi andneighbouring states. The hospital is a Sentinel Centrefor Poliomyelitis, Tetanus and Measles. It has theunique distinction of having a separate PediatricEmergency with direct inflow of patients. It alsohouses the Diarrhoea Training and Treatment Unit,
226
ANNUAL REPORT 2008-09
the first such unit in the country, which has also beenrecognized by WHO and Govt. of India as a trainingcentre for diarrhoeal diseases. The hospital has alsoserved as a training centre for ARI, UIP and otherNational Health programmes.
Neonatal wing of the hospital, with 85 beds cateringto 15,000 deliveries a year, is the biggest neonatalunit in the country and is providing state of artservices for premature and sick newborns includingventilator care. The institution is a super specialityhospital in real sense with its fully developedsubspecialities like Neurology, Nephrology,Gastroenterology & Nutrition, Hematology,Pulmonology and Endocrinology.
Indo-Japan Friendship Block of Kalawati SaranChildren's Hospital has been constructed with anexpenditure of over Rs.54 crore for the building andthe latest equipment for various sections of thehospital which has been helpful in easing out theproblem of inadequate space and technologicalupgrading of the institution.
Kalawati Saran Children's Hospital was designatedas "Nodal Centre for Pre-service IMNCI (IntegralManagement of Neonatal and Childhood Illness)implementation in NIPI States". The Hospitalorganized Five National Training of TrainersCourses of IMNCI with support of Govt. of India/WHO/ UNICEF.
Infant and Young Child Feeding Counseling Centrewas started in Kalawati Saran Children's Hospital tostrengthen IYCF practices. Autism evaluation cellwas started in the Hospital. 55 children has beenregistered so far. Hemophilia follow-up clinic wasstarted on first Wednesday (afternoon) of everymonth in the Department of Physical Medicine &Rehabilitation Department. Once a month aftercompletion of therapy (ACT) clinic for follow-up ofchildren treated for lymphoma and leukemia wasstarted in the first Monday of every month.
An advanced center of pediatrics care has been setup at the Hosptial. This Center is poised to be oneof the premier center of Paediatrics care in thecountry. The Hospital statics for 2007-08 is as under:-
Total No. of sanctioned beds 370
Total OPD attendance 290412
No. of admissions 30,329
Bed occupancy rate 131.3%
Minor operations 2526
Major operations 1956
Attendance to CHPC 1,00,000
15.1815.1815.1815.1815.18 Mahatma Gandhi Institute ofMahatma Gandhi Institute ofMahatma Gandhi Institute ofMahatma Gandhi Institute ofMahatma Gandhi Institute ofMedical Sciences/KasturbaMedical Sciences/KasturbaMedical Sciences/KasturbaMedical Sciences/KasturbaMedical Sciences/KasturbaHealth SocietyHealth SocietyHealth SocietyHealth SocietyHealth Society, Sevagram,, Sevagram,, Sevagram,, Sevagram,, Sevagram,WWWWWardhaardhaardhaardhaardha
The Mahatma Gandhi Institute of Medical Sciences, isthe first rural based medical school, established in 1969in the Gandhi centenary year. The Institute admits 65students every year on the basis of their performancein a premedical test conducted at Nagpur, Delhi, Mumbaiand Hyderabad. It offers post-graduation in 18specialties. As per the agreed pattern of FinancialAssistance the recurring expenditure of the MGIMS isshared amongst the Central Government, Govt. ofMaharshtra and the Kasturba Health Society itself inthe ratio of 50:25:25 respectively. The Government ofIndia has released the grant-in-aid of Rs. 16.48 croresduring the year 2007-08.
The Govt. of India has launched a new one-year PGdiploma in Public Health Management. Fourinstitutions have been selected from all over thecountry to conduct such courses. The Sushila NayarSchool of Public Health in the Institute has startedPostgraduate Courses in the Mahatma GandhiInstitute of Medical Sciences has been selected fortraining 25 candidates from the states of Karnataka,Maharashtra, Tamil Nadu, Goa and Kerala.
The Institute has introduced in its curriculum manyinnovations like the Orientation camp in whichGandhian values are taught to the students. Dietservey being carried out by student during SocialService Camp. The Institute has promoted genderequality in villages.
The Society has been awarded the 12th Mahaveer
227
ANNUAL REPORT 2008-09
Award for Excellence in the sphere of Education andMedicine for the year 2006. State Award to KasturbaHealth Society for Cataract Blindness Control hasbeen awarded by the Maharashtra State BlindnessControl Society, for excellence in services to KasturbaHealth Society for the year 2007-08.
The Blood Component Unit of the Blood Bank,Department of Pathology has become fullyoperational from 17th August, 2007. This is the onlyblood component unit in the entire Wardha districtand it fulfills a long waited need to the patients. TheDepartment of Pathology has also added a flowcytometer, fluorescent microscope andimmunohistochemistry to its armamentarium recently.
The Department of Medicine commissioned ahaemodialysis unit on 27th October, 2007. The unithas haemodialysis machines and the capacity todialyze two patients simultaneously. The unit will heldreduce mortality due to acute renal failure, andprovide palliation to patients with chronic renal failure.
The unit Alpha-ST mammography machine andattachment for stereotactic biopsy unit, funded bythe National Cancer Control Programme, Ministry ofHealth & Family Welfare, for the early detection ofbreast cancer in women has been installed andcommissioned in the Radiology Department of theInstitute. During the year the facility of Brachytherapyand Digital Substraction Angiography has beenadded for the treatment of patients in the departmentsof Radiotherapy and Radiology respecitively.
In order to address complex needs of older people,the Department of Medicine has started the GeriatricOPD to provide dedicated and comprehensivegeriatric care to the elderly. Its objective is to provideemotional, physical and mental sense of well beingto the elderly through curative, preventative, medicaland psychological services. It is also approachingthe outreach patients.
The Institute is involved in extensive research. Duringthe year about 87 research papers were publishedin the National/ International Journals and 100research papers were presented by the faculty of
the Institute in the various conferences of National/International level. The Institute is also participatingin many national programs and it has received 75extramural research projects from Govt. and Non-Govt. organizations.
The Kasturba Hospital attached to the MedicalCollege is constantly getting a large flow of patients.During the year 2007-08, a total number of 5,45,227OPD patients attended the OPD and in a 760 beddedhospital, 40,244 patients were managed to in theindoor department giving the occupancy rate of131.8% for the year. A total number of 7825 majoroperation were conducted at the Hospital in the year2007-08 and 5,31,695 investigations were conductedin addition to 45,545 X-rays and under the uniqueHealth Insurance scheme, 39,815 Health InsuranceCards were issued which provides 50% discount ontreatment to all beneficiaries. In addition, camps wereheld and through these outreach activities 1,25,543patients were examined and treated.
The facility of 108 bedded Matoshri ManibenChandulal Maganlal Kothari Atithi Gruha for therelatives of the admitted patients is available on veryeconomical rates. It is a boon for patients comingfrom distant villages.
The District Disability Rehabilitation Centre which wastransferred to KHS, Sevagram has been functioningfrom 2nd October, 2004 and is the only one inVidarbha Region. The Kasturba Hospital is extendingCommunity Ophthalmology Services under National(Cataract) Blindness Control in Wardha District.
Kasturba Health Society is also running KasturbaNursing School and Kasturba Nursing College whichare affiliated to Maharashtra University of HealthSciences, Nashik. The intake capacity of KasturbaNursing School is 35 students and that of KasturbaNursing College is 20 students per year.
Information about Gender Budgeting
Total No. of Male Female PercentageEmployees (Female)
800 410 390 48.75%
228
ANNUAL REPORT 2008-09
PPPPPatients Tatients Tatients Tatients Tatients Treated during the Financial Yreated during the Financial Yreated during the Financial Yreated during the Financial Yreated during the Financial Year 2007-08ear 2007-08ear 2007-08ear 2007-08ear 2007-08
Total Patients Male Female Percentage(Female)
OPD 545227 304274 238103 43.67%
Indoor 40244 19373 20871 51.86%
Total No. of beds - 760
(610 teaching and 150service beds)
Male Female Percentage (Female)
Medical studentsUndergraduates - 65 42 23 35.38%
Postgraduates - 55 27 28 50.90%
Nursing Students
Kasturba Nursing School - 35 100%
Kasturba Nursing College
BSc Nursing (Intake Capacity - 20) 03 17 85%
15.1915.1915.1915.1915.19 National Institute of Communi-National Institute of Communi-National Institute of Communi-National Institute of Communi-National Institute of Communi-cable Diseasescable Diseasescable Diseasescable Diseasescable Diseases
National Institute of Communicable Diseases (NICD)is a premier institute in India committed to preventionand control of communicable diseases throughmanpower development, applied research, andservice support to the states and other healthagencies in the country.
NICD has three centres - Centre for Epidemiology &Parasitic Diseases (with divisions of Epidemiologyand Parasitic Diseases), Advanced Centre for HIV /AIDS & related diseases and Centre for MedicalEntomology and Vector Management, and fivespecialized divisions, viz., Biochemistry &Biotechnology, Microbiology, IDSP, Zoonosis, andTraining & Malariology.
NICD has eight field stations operating in different
regions of India carrying out disease-specificactivities, manpower development in the field ofepidemiology and related disciplines and providingfield exposure to the trainees. These are located inthe states of Andhra Pradesh, Bihar, Chhattisgarh,Karnataka, Kerala, Rajasthan, Tamil Nadu and UttarPradesh.
NICD has been recognized as a WHO CollaboratingCentre for Epidemiology & Training, WHOCollaborating Centre for Rabies Epidemiology,Referral Centre for Poliomyelitis for South East AsianCountries, National Referral Centre for Viral Hepatitis& AIDS. The Institute has been recognized by theGuru Gobind Singh Indraprastha University, Delhi a)Advanced Research Centre for Doctoral (Ph.D.)Programmes and (b) Two year Master of PublicHealth (Field Epidemiology) course.
1. Budget Allocation for the year 2008-09.
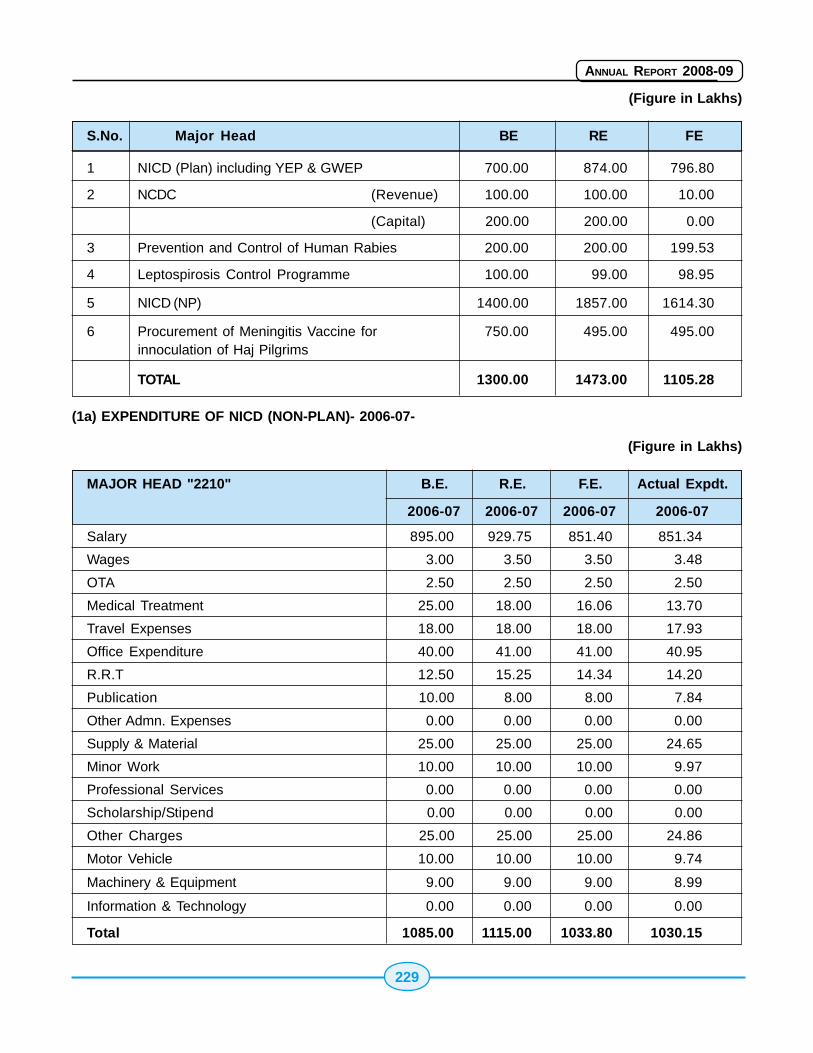
229
ANNUAL REPORT 2008-09
(Figure in Lakhs)
S.No. Major Head BE RE FE
1 NICD (Plan) including YEP & GWEP 700.00 874.00 796.80
2 NCDC (Revenue) 100.00 100.00 10.00
(Capital) 200.00 200.00 0.00
3 Prevention and Control of Human Rabies 200.00 200.00 199.53
4 Leptospirosis Control Programme 100.00 99.00 98.95
5 NICD (NP) 1400.00 1857.00 1614.30
6 Procurement of Meningitis Vaccine for 750.00 495.00 495.00innoculation of Haj Pilgrims
TOTAL 1300.00 1473.00 1105.28
(1a) EXPENDITURE OF NICD (NON-PLAN)- 2006-07-
(Figure in Lakhs)
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2006-07 2006-07 2006-07 2006-07
Salary 895.00 929.75 851.40 851.34
Wages 3.00 3.50 3.50 3.48
OTA 2.50 2.50 2.50 2.50
Medical Treatment 25.00 18.00 16.06 13.70
Travel Expenses 18.00 18.00 18.00 17.93
Office Expenditure 40.00 41.00 41.00 40.95
R.R.T 12.50 15.25 14.34 14.20
Publication 10.00 8.00 8.00 7.84
Other Admn. Expenses 0.00 0.00 0.00 0.00
Supply & Material 25.00 25.00 25.00 24.65
Minor Work 10.00 10.00 10.00 9.97
Professional Services 0.00 0.00 0.00 0.00
Scholarship/Stipend 0.00 0.00 0.00 0.00
Other Charges 25.00 25.00 25.00 24.86
Motor Vehicle 10.00 10.00 10.00 9.74
Machinery & Equipment 9.00 9.00 9.00 8.99
Information & Technology 0.00 0.00 0.00 0.00
Total 1085.00 1115.00 1033.80 1030.15
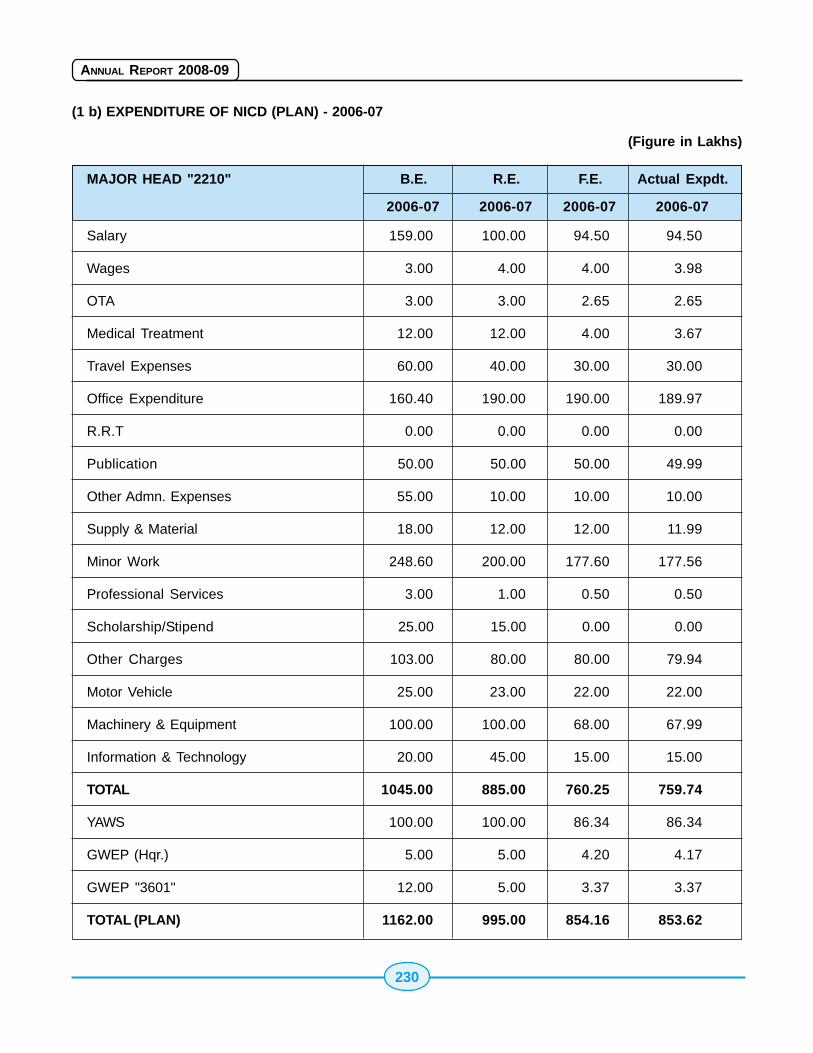
230
ANNUAL REPORT 2008-09
(1 b) EXPENDITURE OF NICD (PLAN) - 2006-07
(Figure in Lakhs)
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2006-07 2006-07 2006-07 2006-07
Salary 159.00 100.00 94.50 94.50
Wages 3.00 4.00 4.00 3.98
OTA 3.00 3.00 2.65 2.65
Medical Treatment 12.00 12.00 4.00 3.67
Travel Expenses 60.00 40.00 30.00 30.00
Office Expenditure 160.40 190.00 190.00 189.97
R.R.T 0.00 0.00 0.00 0.00
Publication 50.00 50.00 50.00 49.99
Other Admn. Expenses 55.00 10.00 10.00 10.00
Supply & Material 18.00 12.00 12.00 11.99
Minor Work 248.60 200.00 177.60 177.56
Professional Services 3.00 1.00 0.50 0.50
Scholarship/Stipend 25.00 15.00 0.00 0.00
Other Charges 103.00 80.00 80.00 79.94
Motor Vehicle 25.00 23.00 22.00 22.00
Machinery & Equipment 100.00 100.00 68.00 67.99
Information & Technology 20.00 45.00 15.00 15.00
TOTAL 1045.00 885.00 760.25 759.74
YAWS 100.00 100.00 86.34 86.34
GWEP (Hqr.) 5.00 5.00 4.20 4.17
GWEP "3601" 12.00 5.00 3.37 3.37
TOTAL (PLAN) 1162.00 995.00 854.16 853.62
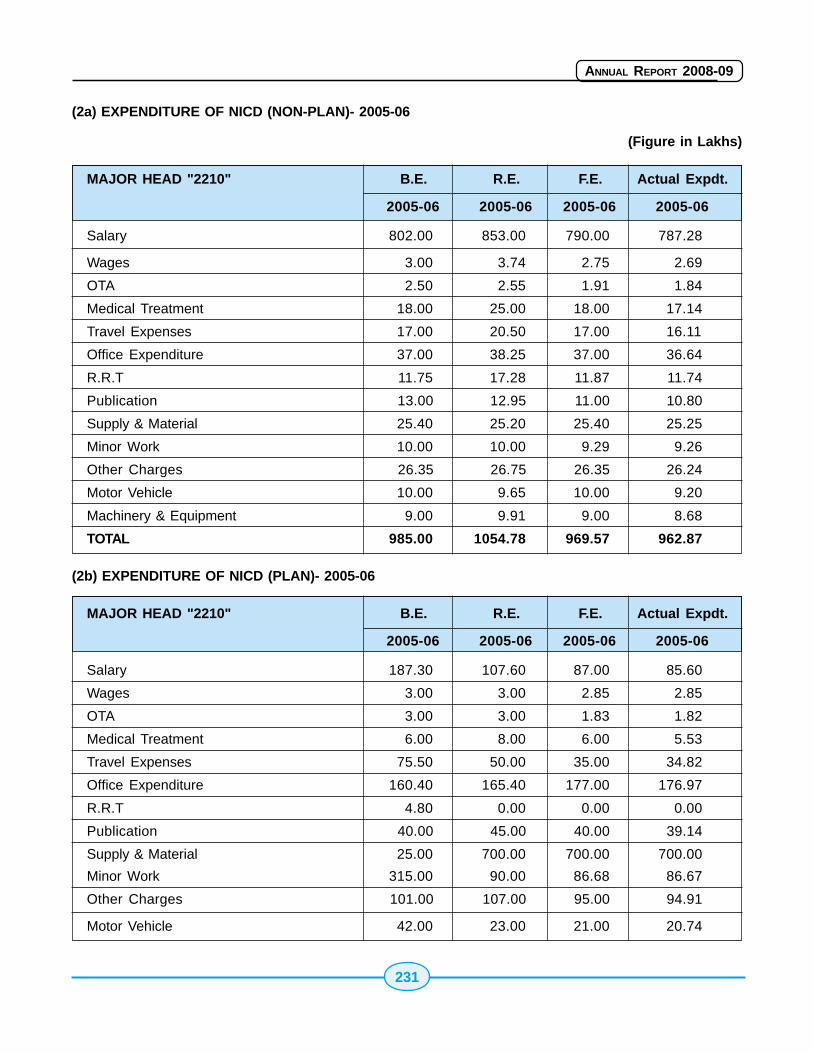
231
ANNUAL REPORT 2008-09
(2a) EXPENDITURE OF NICD (NON-PLAN)- 2005-06
(Figure in Lakhs)
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2005-06 2005-06 2005-06 2005-06
Salary 802.00 853.00 790.00 787.28
Wages 3.00 3.74 2.75 2.69
OTA 2.50 2.55 1.91 1.84
Medical Treatment 18.00 25.00 18.00 17.14
Travel Expenses 17.00 20.50 17.00 16.11
Office Expenditure 37.00 38.25 37.00 36.64
R.R.T 11.75 17.28 11.87 11.74
Publication 13.00 12.95 11.00 10.80
Supply & Material 25.40 25.20 25.40 25.25
Minor Work 10.00 10.00 9.29 9.26
Other Charges 26.35 26.75 26.35 26.24
Motor Vehicle 10.00 9.65 10.00 9.20
Machinery & Equipment 9.00 9.91 9.00 8.68
TOTAL 985.00 1054.78 969.57 962.87
(2b) EXPENDITURE OF NICD (PLAN)- 2005-06
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2005-06 2005-06 2005-06 2005-06
Salary 187.30 107.60 87.00 85.60
Wages 3.00 3.00 2.85 2.85
OTA 3.00 3.00 1.83 1.82
Medical Treatment 6.00 8.00 6.00 5.53
Travel Expenses 75.50 50.00 35.00 34.82
Office Expenditure 160.40 165.40 177.00 176.97
R.R.T 4.80 0.00 0.00 0.00
Publication 40.00 45.00 40.00 39.14
Supply & Material 25.00 700.00 700.00 700.00
Minor Work 315.00 90.00 86.68 86.67
Other Charges 101.00 107.00 95.00 94.91
Motor Vehicle 42.00 23.00 21.00 20.74
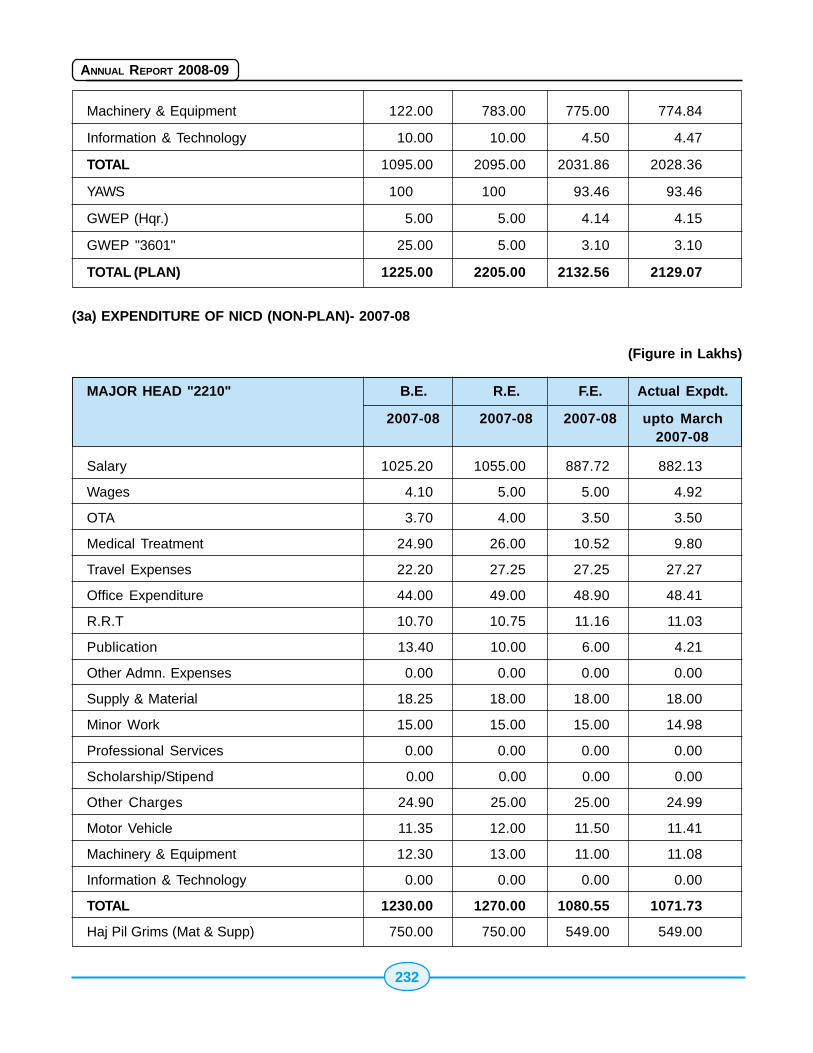
232
ANNUAL REPORT 2008-09
Machinery & Equipment 122.00 783.00 775.00 774.84
Information & Technology 10.00 10.00 4.50 4.47
TOTAL 1095.00 2095.00 2031.86 2028.36
YAWS 100 100 93.46 93.46
GWEP (Hqr.) 5.00 5.00 4.14 4.15
GWEP "3601" 25.00 5.00 3.10 3.10
TOTAL (PLAN) 1225.00 2205.00 2132.56 2129.07
(3a) EXPENDITURE OF NICD (NON-PLAN)- 2007-08
(Figure in Lakhs)
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2007-08 2007-08 2007-08 upto March2007-08
Salary 1025.20 1055.00 887.72 882.13
Wages 4.10 5.00 5.00 4.92
OTA 3.70 4.00 3.50 3.50
Medical Treatment 24.90 26.00 10.52 9.80
Travel Expenses 22.20 27.25 27.25 27.27
Office Expenditure 44.00 49.00 48.90 48.41
R.R.T 10.70 10.75 11.16 11.03
Publication 13.40 10.00 6.00 4.21
Other Admn. Expenses 0.00 0.00 0.00 0.00
Supply & Material 18.25 18.00 18.00 18.00
Minor Work 15.00 15.00 15.00 14.98
Professional Services 0.00 0.00 0.00 0.00
Scholarship/Stipend 0.00 0.00 0.00 0.00
Other Charges 24.90 25.00 25.00 24.99
Motor Vehicle 11.35 12.00 11.50 11.41
Machinery & Equipment 12.30 13.00 11.00 11.08
Information & Technology 0.00 0.00 0.00 0.00
TOTAL 1230.00 1270.00 1080.55 1071.73
Haj Pil Grims (Mat & Supp) 750.00 750.00 549.00 549.00
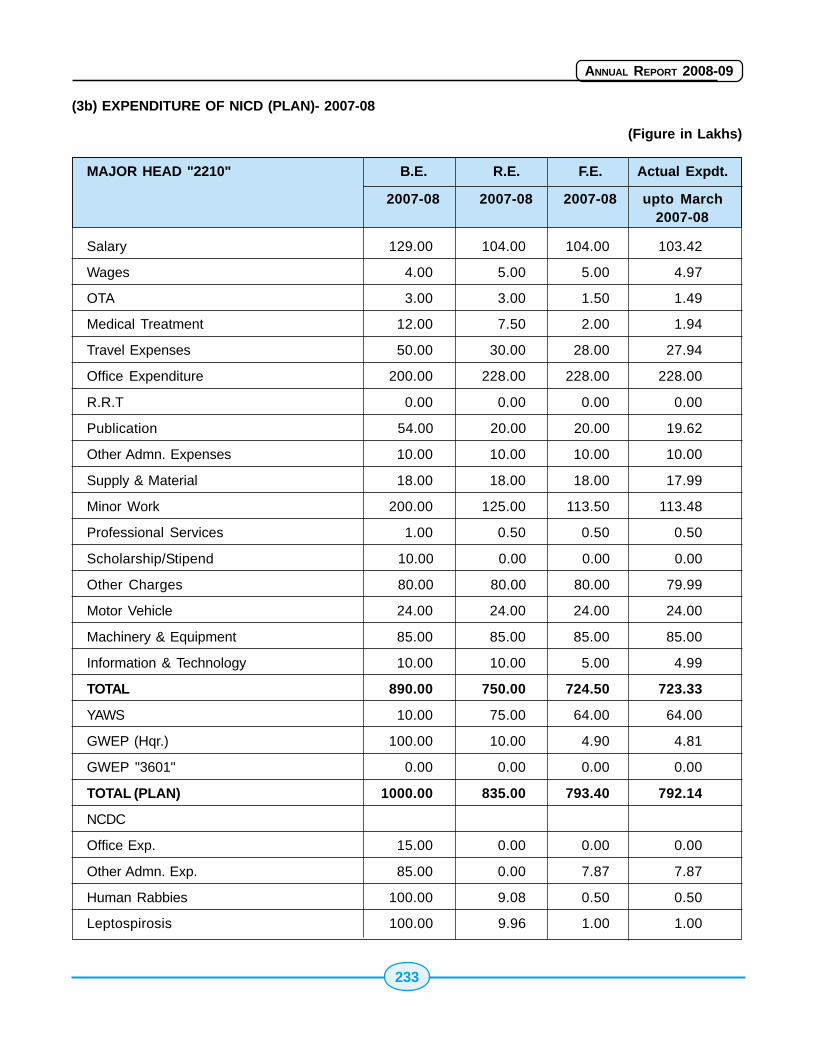
233
ANNUAL REPORT 2008-09
(3b) EXPENDITURE OF NICD (PLAN)- 2007-08
(Figure in Lakhs)
MAJOR HEAD "2210" B.E. R.E. F.E. Actual Expdt.
2007-08 2007-08 2007-08 upto March2007-08
Salary 129.00 104.00 104.00 103.42
Wages 4.00 5.00 5.00 4.97
OTA 3.00 3.00 1.50 1.49
Medical Treatment 12.00 7.50 2.00 1.94
Travel Expenses 50.00 30.00 28.00 27.94
Office Expenditure 200.00 228.00 228.00 228.00
R.R.T 0.00 0.00 0.00 0.00
Publication 54.00 20.00 20.00 19.62
Other Admn. Expenses 10.00 10.00 10.00 10.00
Supply & Material 18.00 18.00 18.00 17.99
Minor Work 200.00 125.00 113.50 113.48
Professional Services 1.00 0.50 0.50 0.50
Scholarship/Stipend 10.00 0.00 0.00 0.00
Other Charges 80.00 80.00 80.00 79.99
Motor Vehicle 24.00 24.00 24.00 24.00
Machinery & Equipment 85.00 85.00 85.00 85.00
Information & Technology 10.00 10.00 5.00 4.99
TOTAL 890.00 750.00 724.50 723.33
YAWS 10.00 75.00 64.00 64.00
GWEP (Hqr.) 100.00 10.00 4.90 4.81
GWEP "3601" 0.00 0.00 0.00 0.00
TOTAL (PLAN) 1000.00 835.00 793.40 792.14
NCDC
Office Exp. 15.00 0.00 0.00 0.00
Other Admn. Exp. 85.00 0.00 7.87 7.87
Human Rabbies 100.00 9.08 0.50 0.50
Leptospirosis 100.00 9.96 1.00 1.00
234
ANNUAL REPORT 2008-09
Epidemiology Division:-
(A) Activities:-
� Organization and coordination of trainingcourses in Epidemiology to develop trainedhealth manpower. Development of teachingmaterials such as Modules. Manuals etc. ondisease surveillance and outbreakinvestigation of epidemic prone diseases.
� Investigation of outbreak of diseases ofknown / unknown etiology and recommendmeasures for their prevention and control tothe States / UTs . Provision of technicalsupport to State governments forinvestigation and control of diseaseoutbreaks.
� Provision of administrative and technicalsupervision to three branches of the Instituteviz., Alwar (Rajasthan), Jagdalpur(Chattisgarh) and Conoor (Tamil Nadu).
� Provision of technical support to variousNational Health Programmes in the form ofdeveloping guidelines for control, manpowerdevelopment, evaluation of differentcomponents / indicators.
� Assisting the Director for publication ofmonthly Bulletin "CD Alert".
� Carry out field research on different aspectsof communicable diseases.
� Carrying out Masters in Public Health (FieldEpidemiology) two year course in affiliationwith Guru Govind Singh InderprasthaUniversity,Delhi.
(B) Outbreaks Investigated/ Rapid HealthAssessment
During the period reported upon, officers from theDivision of Epidemiology carried out investigationsof outbreaks in the country and suggestedcontainment measures to the authorities whichinclude:
� Investigation of reported infant's deaths
following measles vaccination in Thriuvallurdistrict of Tamilnadu.
� Avian influenza outbreak investigations invarious districts of Tripura, and WestBengal .
� Investigation of outbreak of acuteencephalitis in Gorakhpur district of UttarPradesh .
� Investigation of outbreak of suspectedLeptospirosis in South Gujarat.
� Avian influenza outbreak investigations invarious in South Sikkim and various districtsof Assam .
� Investigation of outbreak of Hepatitis B northGujarat.
(C) Manpower Development
National Institute of Communicable Diseases (NICD),Delhi is a WHO Collaborating Center for Epidemiologyand Training. The Division of Epidemiology conductsregular training programmes and numerous othershort-term training activities every year. The coursecurricula of these training programmes are designedand tailor-made to develop the necessary need-based skills for the health professionals. Theparticipants to these courses come from differentStates/ Union Territories of India. In addition, traineesfrom some of the neighboring countries likeBangladesh, Bhutan,DPR Korea, Sri Lanka,Maldives,Myanmar and Nepal also participate in some of thetraining programmes.
Other Activities
1. Organized a Technical session on 'Climatechange and its impact of Health' on theoccasion of World Health Day on 7th April,2008 in collaboration with the IndianAssociation of Epidemiologists
2. Meeting for review and revision of MPH (FE)training programme was organized invitingexperts from national institutes andinternational agencies.
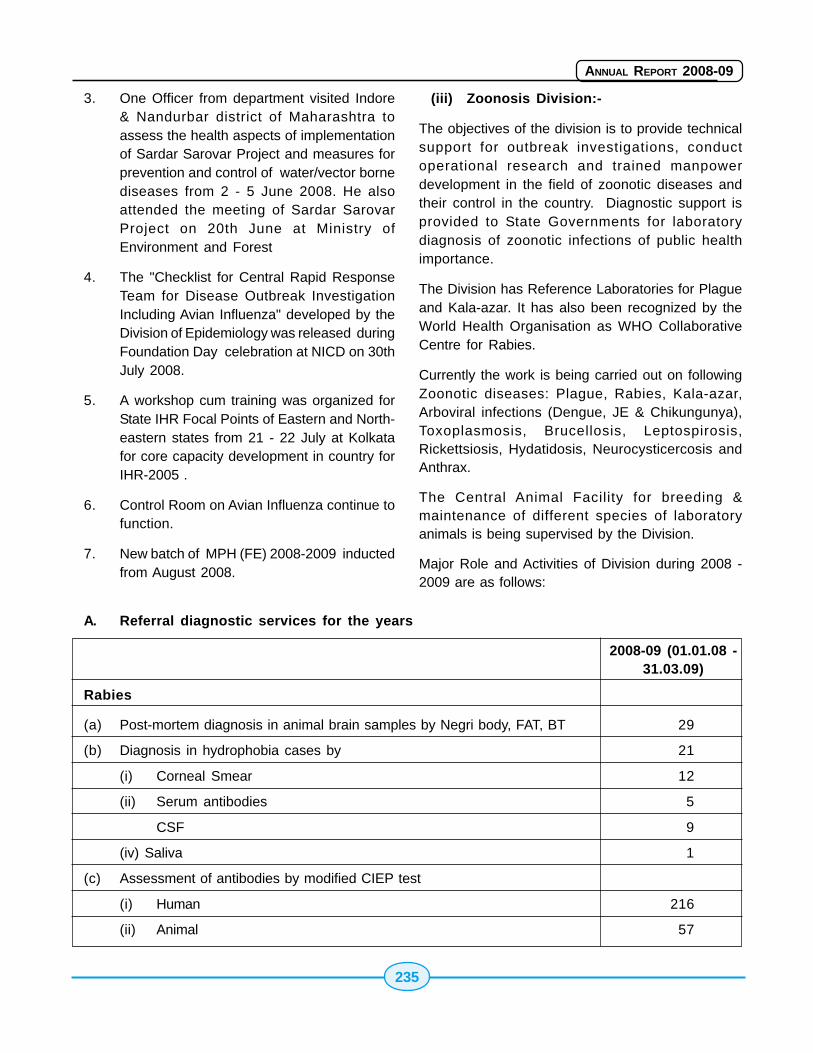
235
ANNUAL REPORT 2008-09
3. One Officer from department visited Indore& Nandurbar district of Maharashtra toassess the health aspects of implementationof Sardar Sarovar Project and measures forprevention and control of water/vector bornediseases from 2 - 5 June 2008. He alsoattended the meeting of Sardar SarovarProject on 20th June at Ministry ofEnvironment and Forest
4. The "Checklist for Central Rapid ResponseTeam for Disease Outbreak InvestigationIncluding Avian Influenza" developed by theDivision of Epidemiology was released duringFoundation Day celebration at NICD on 30thJuly 2008.
5. A workshop cum training was organized forState IHR Focal Points of Eastern and North-eastern states from 21 - 22 July at Kolkatafor core capacity development in country forIHR-2005 .
6. Control Room on Avian Influenza continue tofunction.
7. New batch of MPH (FE) 2008-2009 inductedfrom August 2008.
(iii) Zoonosis Division:-
The objectives of the division is to provide technicalsupport for outbreak investigations, conductoperational research and trained manpowerdevelopment in the field of zoonotic diseases andtheir control in the country. Diagnostic support isprovided to State Governments for laboratorydiagnosis of zoonotic infections of public healthimportance.
The Division has Reference Laboratories for Plagueand Kala-azar. It has also been recognized by theWorld Health Organisation as WHO CollaborativeCentre for Rabies.
Currently the work is being carried out on followingZoonotic diseases: Plague, Rabies, Kala-azar,Arboviral infections (Dengue, JE & Chikungunya),Toxoplasmosis, Brucellosis, Leptospirosis,Rickettsiosis, Hydatidosis, Neurocysticercosis andAnthrax.
The Central Animal Facility for breeding &maintenance of different species of laboratoryanimals is being supervised by the Division.
Major Role and Activities of Division during 2008 -2009 are as follows:
A. Referral diagnostic services for the years
2008-09 (01.01.08 -31.03.09)
Rabies
(a) Post-mortem diagnosis in animal brain samples by Negri body, FAT, BT 29
(b) Diagnosis in hydrophobia cases by 21
(i) Corneal Smear 12
(ii) Serum antibodies 5
CSF 9
(iv) Saliva 1
(c) Assessment of antibodies by modified CIEP test
(i) Human 216
(ii) Animal 57
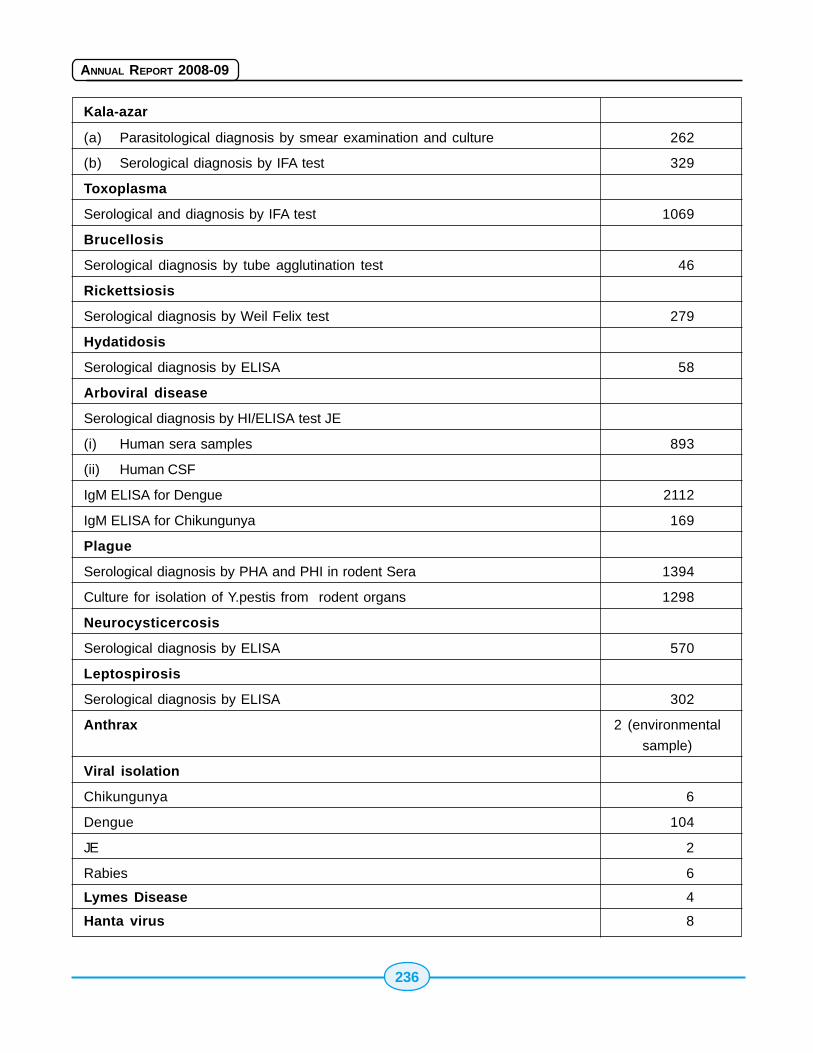
236
ANNUAL REPORT 2008-09
Kala-azar
(a) Parasitological diagnosis by smear examination and culture 262
(b) Serological diagnosis by IFA test 329
Toxoplasma
Serological and diagnosis by IFA test 1069
Brucellosis
Serological diagnosis by tube agglutination test 46
Rickettsiosis
Serological diagnosis by Weil Felix test 279
Hydatidosis
Serological diagnosis by ELISA 58
Arboviral disease
Serological diagnosis by HI/ELISA test JE
(i) Human sera samples 893
(ii) Human CSF
IgM ELISA for Dengue 2112
IgM ELISA for Chikungunya 169
Plague
Serological diagnosis by PHA and PHI in rodent Sera 1394
Culture for isolation of Y.pestis from rodent organs 1298
Neurocysticercosis
Serological diagnosis by ELISA 570
Leptospirosis
Serological diagnosis by ELISA 302
Anthrax 2 (environmental
sample)
Viral isolation
Chikungunya 6
Dengue 104
JE 2
Rabies 6
Lymes Disease 4
Hanta virus 8
237
ANNUAL REPORT 2008-09
B Outbreaks investigated
1 Investigation of outbreak of avian influenzain Bardwan district of West Bengal in January- February 2008.
2 Investigation of outbreak of avian influenzain Birbhum district of West Bengal in January- February 2008.
3 Investigation of outbreak of suspectedanthrax in Kalahandi and Koraput district ofOrissa in February, 2008
4 Investigation of outbreak of avian influenzain Murshidabad district of West Bengal inMarch 2008
5 Investigation of outbreak of suspectedencephalitis in children in Uttar Dirajpurdistrict of West Bengal in July 2008.
6 Investigation of outbreak of acute encephalitisinchildren in Gorakhpur region of UttarPradesh in August -September 2008.
7 Investigation of outbreak of avian influenzain Kamrup district of Assam in November-December 2008.
8 Investigation of outbreak of avian influenzain Chirang district of Assam in December2008.
9 Investigation of outbreak of avian influenzain Nagaon district of Assam in December2008-January 2009.
10 Investigation of outbreak of avian influenzain Namchi district of Sikkim in January 2009.
11 Investigation of outbreak of Hepatitis B inMadosa , Sabarkantha district of Gujarat inMarch 2009.
C Training courses/Expert group meetings
1. Meeting of Standing Committee on Zoonosisheld on 11th April 2008.
2. Interstate Plague Coordination meeting on10 & 11th June 2008.
3. Training Course on laboratory diagnosis ofDengue & Chikungunya for doctors ¶medicals of sentinel hospitals of Delhiin 17th & 18th June 2008 and 24th & 25thJune 2008.
4. Training of core trainer of Gujarat State onvarious aspects of control of leptospirosis on14th June 2008 under pilot project on controlof leptospirosis.
5. Training of core trainer on various aspectsof intradermal inoculation of cell cultureantirabies vaccine and animal bitemanagement along with theory aspects ofepidemiology, pathogenesis, laboratorydiagnosis and animal bite managementguidelines on 2nd & 3rd July, 2008, underpilot project on prevention and control ofhuman rabies.
6. Training of core trainer of Tamil Nadu Stateon various aspects of control of leptospirosison 15th July 2008 under pilot project oncontrol of leptospirosis
7. Training of core trainer of Kerala State onvarious aspects of control of leptospirosis onAugust 2008, under pilot project on controlof leptospirosis.
8. Training course on surveillance and controlof Plague from 29th September to 2ndOctober 2008 at PSU, Bangalore.
9. Training of Doctors & Paramedical staff inlaboratory diagnostic techniques in Rabieson 20th & 21st October, 2008, under pilotproject on prevention and control of humanrabies.
10. Diagnostic Techniques in Leptospirosis to theparticipants of the Pilot Project States Gujaratand Tamil Nadu conducted on 13th & 14thJanuary 2009. Total participants attended 10.
11. Training Programme for Doctors & LabTechnicians in Lab diagnostic techniques inRabies on 26th & 27th March 2009 at NICD,
238
ANNUAL REPORT 2008-09
Delhi. 6 participants attended the Trainingprogramme from Pilot Project cities.
D (1). Research projects undertaken
1. To study the epidemiological profile of Kala-azar patients in Delhi
2. Comparative evaluation of rK39, ELISA & IFAfor serodiagnosis of Kala-azar.
3. Detection of antibodies to Leishmania inblood donors.
4. Developing an indigenous ELISA kit fordetection of leishmania antibodies
5. Serological studies in Toxoplasmosis indifferent Delhi Hospitals.
6. Comparative analysis of various serologicaltests in diagnosis of Toxoplasmosis.
7. Surveillance of Plague in different parts ofthe country.
8. Specificity of Passive haemagglutination Testfor Y.pestis.
9. Use of ELISA in serological diagnosis ofNeurocysticercosis.
10. Molecular characterisation of strains ofLeishmania.
11. Sero-epidemiology of Brucellosis in high riskpopulation in Delhi
12. Standardization of appropriate diagnosticmethods for sero-diagnosis and sero-epidemiology of human and animalleptospirosis
13. Surveillance of arboviral infections in manand animals
14. Isolation of rabies virus in-vitro(Neuroblastoma 2A cell lines).
15. Study of prevalence of Rabies in peridomesticand wild rodents.
16. Standardization of Rapid Fluorescent Focus
Inhibition Test (RFFIT) for rabies antibodytiter.
17. Structural and functional mimicry betweenRabies Antibodies and HumanImmunodeficiency Virus-I (HIV-I) Antibodies.
18. Isolation of Chikungunya virus in mouseneuroblastoma cell lines.
19. Comparative evaluation of diagnostic testsfor serological diagnosis of Dengue, JE,Leptospirosis and Scrub typhus.
D (2) Pilot Projects on Prevention andControl of Human Rabies and Control ofLeptospirosis.
The Zoonosis division is presently undertaking twoprojects as "New initiative" under 11th five year plannamely:-
1. Pilot Project on Prevention and Control ofHuman Rabies
2. Pilot Project on Control of Leptospirosis
Pilot project on Prevention and Control ofHuman Rabies
To prevent human deaths due to rabies a pilot projecthas been approved as a 'New Initiative' in the 11thFive Year Plan in March 2008. The project will becarried out for a period of 2 years. The focus of theproject is:
� Training of health professionals about rabiesand animal bite management.
� Ensuring timely and adequate post-exposuretreatment to all animal bite victims.
� Creating awareness about timely andadequate post exposure treatment to allanimal bite victims in the community.
� Strengthening laboratory diagnosticcapabilities
� Facilitating introduction of intradermal routeof vaccination.
� Sensitizing veterinarians
239
ANNUAL REPORT 2008-09
Activities conducted in the year 2008-2009:
� Inaugural expert group meeting to firm up thestrategy for prevention & control of humanrabies and discuss plan of implementation:Held on 27th March, 2008 at NICD, Delhi.
� City core groups have been formed by allpilot project cities and nodal officer in eachhas been identified.
� The Consultant and data entry operator havebeen appointed at NICD, Delhi
� Two training courses for core trainers from pilotproject cities were conducted on July 2008and Jan 2009 at NICD. The core trainers wereprovided training on appropriate animal bitemanagement including i.d. inoculation of cellculture vaccine. They were provided with thecopy of National guidelines for rabiesprophylaxis and i.d. administration of cellculture rabies vaccines.
� Expert group meeting to develop prototypeIEC material was held at NICD, Delhi inAugust 2008. The prototype material is underprint. This would be distributed to pilot projectcities for translation in local language anddissemination to create awareness in generalcommunity.
� Bangalore, Pune & Madurai have identifiedARCs for implementation of intradermal routeand prepared a protocol for training of localdoctors.
� Laboratory to be strengthened has beenidentified in all pilot project cities.
� Training has been conducted for Doctors &Lab. technicians on lab diagnostic techniquesin October 2008 and March 2009.
� Veterinarians were sensitized during expertgroup meeting held on 27th March 2008.
� Scientific advisory group has beenconstituted to monitor the implementation &progress of project.
� Base line data has been received form pilotproject cities
� Initial visit to pilot project cities have beenundertaken.
A total amount of Rs. 3.26 crore has been allocatedfor the project. Revised estimate for current financialyear is Rs. 1.90 crore out of which an amount of Rs.1.81 crore has been released to pilot project citiesto carry out various activities under the project inthe current financial year. The details are as follows:
Cities Amount (Rs)
Ahmedabad 36,88,000
Bangalore 36,88,000
Delhi 37,80,000
Pune 36,88,000
Madurai 32,80,000
TOTAL 1,81,24,000
Pilot Project on Control of Leptospirosis
Pilot Project on Control of Leptospirosis wasapproved for a period of two years, as "New initiative"under 11th five year plan in Feb 2007. It is beingcarried out in three States: Gujarat, Kerala and TamilNadu. The focus of the project will be on:-
1. Reduction of morbidity and mortality due toLeptospirosis in pilot project area.
2. Strengthening diagnostic laboratories in pilotproject areas.
3. Strengthening of patient care managementfacilities in pilot project areas andsupplementary provision of drugs forchemoprophylaxis.
4. Development of trained manpower.
5. Create awareness regarding timely detectionand appropriate treatment of patients.
6. Sensitization of Animal Husbandry andAgriculture personnel.
7. Information, Education and communication.
240
ANNUAL REPORT 2008-09
Activities conducted in the year 2008-2009
� Inaugural Expert Group Meeting to firm upthe strategy for control of Leptospirosisand discuss plan of implementation was heldat NICD, Delhi in May 2008.
� The 2nd Expert Group Meeting was held on7th Oct 2008 at NICD, Delhi to review theguidelines for prevention and control ofLeptospirosis.
� The reviewed guidelines booklet has beenfinalized and is in the process of printing.
� Core group has been constituted in eachState and the Nodal officer has beenidentified to carry out and monitor theactivities under the pilot project States.
� Veterinarians were sensitized in a groupmeeting held in July and August 2008 inGujarat, Kerala and Tamil Nadu.
� Base line data has been collected from threeStates.
� Training of core trainers in the States beingconducted in July and Aug 2008. Next roundof training was conducted in Gujarat,Tamilnadu in January and February 2009.
� Training of core trainers on laboratorydiagnostic method was conducted on Jan2009 which included Microbiologist,Pathologist and Lab Technicians.
� Consultant and Data Entry Operator hasbeen selected and appointed at NICD,Delhi.
� Visits to review the progress in the PilotProject States have been undertaken.
� Prototype of IEC material have beendeveloped, this would be distributed to pilotproject states for translation anddissemination.
� Process of strengthening of laboratories hasbeen initiated.
� For strengthening of surveillance Performafor monthly data collection have been
Circulated to the pilot project states.
A total amount of Rs. 2.05 cores, one core hasbeen allocated for the year 2008-2009. An amountof Rs. 95,50,000/- (Rupees. 95 Lacs FiftyThousand Only) has been released to the PilotProject States to carry out the various activitiesunder the project in the current Financial Year. Thedetails are as follows:-
State Amount (Rs)
Gujarat 35,50,000
Kerala 30,00,000
Tamil Nadu 30,00,000
TOTAL 95,50,000
Major Activities and Achievement for the periodJanuary, 2008 till March, 2009
Results of participation in National/ InternationalEQAS
� This Center participated in internationalEQAS for HIV, HBV and HCV serologyconducted by the National SerologyReference Laboratory (NSRL), Australia, aWHO Collaborating Centre on HIV/AIDS,Australia, twice during the year. This Centreon both the occasions gave 100%concordant results of HIV, HBV and HCVserology as part of the proficiency testingprogramme.
� This Centre participated in National EQASfor HIV serology conducted by NARI, Pune.The Centre gave 100% concordant resultsof HIV serology.
� Centre participated in EQAS for CD4 cellestimation conducted by National AIDSResearch Institute (NARI), Pune incollaboration with QASI, Canada, thriceduring a year. The Centre consistentlyperformed satisfactorily during the period.
241
ANNUAL REPORT 2008-09
� Participated in EQAS for VDRL/RPR testingconducted by Regional STD Teaching,Training & Research Center, VM Medicalcollege & Safdarjung Hospital, New Delhi. Theresults of qualitative RPR testing of theproficiency panels had 100% concordancewith the report provided by SafdarjungHospital.
Consortium of NRLs
� The National Reference Laboratory at NICDalongwith three other NRLs viz. NARI, Pune,NIMHANS, Bangalore and NICED, Kolkatahave formed a Consortium. This consortiumis being developed with the aim to createparity between the four NRLs which are goingto conduct evaluation and batch testing ofdiagnostic kits for various transfusiontransmitted infection (TTIs).
� As part of the Consortium activity a total of30 standard operative procedure documentshave been developed by the Centre.
Award received by the Center
� The Centre was awarded the certificate ofachievement for outstanding performance asa training institute on 1st November, 2008on the occasion of 11th Foundation day ofDelhi State AIDS Control Society.
External Assessment of National ReferenceLaboratory
� An independent assessment of the NationalReference Laboratory on twelve qualitysystem essentials (QSEs) which arefundamental components used to establisha quality management system was carried outon 10th & 11th July 2008 by assessorsappointed by NACO. This exercise wasconducted to identify and rectify any gap soas to bring all the NRLs up to the Internationalstandard. Out of a total of 13 NRLs that wereassessed, the NRL at NICD achieved a scoreof 77% which categorized the laboratory asa "Silver Medal Laboratory" with an overall4th rank.
Training Activities Organized
i. Conducted training of lab. technicians (22participants) on Laboratory Techniques forHIV for Technical Staff of IntegratedCounseling & Testing Centres (ICTCs) underDelhi State AIDS Control Society (DSACS) atCentre for AIDS & Related Diseases, NICDfrom 17-19th February, 2009.
ii. Organised Technical Session on the occasionof the inauguration of "New Central SeminarHall" on 30th December, 2008. Dr. RajeshKumar, Professor & Head, School of PublicHealth, PGIMER, Chandigarh delivered aguest lecture on "Epidemiological trends ofHIV/AIDS in India".
iii. Organized WHO-in-Country FellowshipTraining Programme on "Quality Assurancefor HIV Testing and Conduction EQAP" from1-12th December, 2008 at Centre for AIDS &Related Diseases, NICD, Delhi. Three WHOFellows from the States of Kerala andManipur participated in this trainingprogramme.
iv. Organised one day training programme oncollection and processing of dried blood spot(DBS) for TI site technician conducted on19th September, 2008 at this Centre.
v. Conducted training of lab. technicians (20participants) on Laboratory Techniques forHIV for Technical Staff of IntegratedCounseling & Testing Centres (ICTCs) underDelhi State AIDS Control Society (DSACS) atCentre for AIDS & Related Diseases, NICDfrom 8-12th September, 2008.
vi. Conducted 3 trainings (20 per Batch) of newlyrecruited laboratory technician from DSACSat Centre for AIDS & Related Diseases from10- 12 June, 17-19 June and 24-27 June2008.
vii. Trained 2 laboratory technicians from RDBP,Jaipuria Hospital, Jaipur Rajasthan.
242
ANNUAL REPORT 2008-09
viii. Trained 2 laboratory technicians from LRSInstitute of TB and Allied Diseases on 06/08/08 at this Centre.
ix. Two M.Sc (Microbiology) students and OneB. Tech (Biotechnology) student completedtheir dissertation work during January-August2008.
x. Two students underwent summer training atthis Centre during June - July, 2008.
xi. 10 students from different universitiesunderwent short term summer training duringJune - July, 2008.
xii. Provided technical support for organizationof one day workshop on Dried Blood Spot(DBS) based HIV testing by Centre forCommunity Medicine, AIIMS, New Delhi on15th July, 2008 at NICD, Delhi.
Centre for Medical Entomology and VectorManagement:-
Centre for Medical Entomology and VectorManagement is reorganized to develop it as aNational Centre par excellence for undertakingresearch, providing technical support and to developtrained manpower in the field of Vector-bornediseases and their control. The Centre providestechnical guidance, support and advice to variousstates and organizations on outbreak investigations,and entomological surveillance of vector-bornediseases and their control. Major achievements arehighlighted below:
Major achievements
1. Dengue virus has been detected from Aedesaegypti mosquitoes collected from eightlocalities of Delhi and from Aedes albopictusfrom Kerala.
2. Japanese encephlalitis virus has beendetected from Culex triataeniorhynchusmosquitoes from Baghpat and Karnal districtsof Haryana State
3. Evaluation of 0.88% and 1.6% Transfluthrin
based mosquito repellent liquid and 1.6%Transfluthrin based sand-core electricmosquito repellent devisers have beencarried out against different vector speciesof mosquitoes under laboratory conditions
4. Laboratory evaluation of Mosquito larvicidaloil (MLO) was carried out against themosquito larvae
5. Three year field trials with Long LastingInsecticide Treated Nets (LLIN) have beencompleted against vectors of malaria andFilariasis.
6. One year field trials with Long LastingInsecticide Treated Nets (LLIN) against sandflies, vector of Kala-azar also has beencompleted
7. Field evaluation of "NOMOS" mosquitorepellent cream has been carried out againstvectors of Malaria, Chikungunya and Denguevectors.
8. Publication on sandflies, vector ofleishmaniasis in Acta Tropica, rated as oneof the top 25 best articles of the year 2008
9. NICD cooler: NICD has signed an MOU withNational Research Development Corporation(NRDC) for commercialization of the cooler.
15.2015.2015.2015.2015.20 Lady Reading Health SchoolLady Reading Health SchoolLady Reading Health SchoolLady Reading Health SchoolLady Reading Health School(((((LRHSLRHSLRHSLRHSLRHS), Delhi), Delhi), Delhi), Delhi), Delhi
Lady Reading Health School, Delhi is considered asone of the pioneer institution and first of its kind fortraining Health Visitors. It was established in 1918under the Countess of Dufferin Fund for trainingNursing personal for M.C.H. programme. In 1931 itcame under the administrative control of the IndianRed Cross Society (Maternity & Child WelfareBureau) in 1952 the Government of India took overthe school and attached Ram Chand Lohia MCHCentre. Total capacity of the school was 24 HealthVisitors trainees from all over India, even thesecandidates were not available at that time. Duration

243
ANNUAL REPORT 2008-09
of the course was one and half years for matriculateswho were qualified midwives, which was replaced bytwo and half years integrated course for health visitorin 1954.
The School aims at providing training facilities tovarious categories of Nursing Personal in communityhealth as well as M.C.H. and family welfare servicesthrough the attached Ram Chand Lohia InfantWelfare Centre.
The Institution is imparting the following courses atpresent.
Diploma in Nursing Education andAdministration
This course is of 10 months duration which startsfrom the 15th July each year with total admissioncapacity of 30 students. 28 students appeared inFinal Examination May, 2008 and all passed out theexamination. At present 30 eligible students wereselected and 28 candidates joined the course andwill appear in May, 2009.
Certificate Course for Health Workers (Female)under Multipurpose Workers Scheme
This course is of six months duration. Students areadmitted twice a year i.e. in January and July everyyear with admission capacity of 20 in each batch. 20students were selected for January, 2008 to June,2008 batch and 18 were joined the said course allpassed out in June, 2008. At present 20 candidatesare selected for July, 2008 to December, 2008 batchout the 12 joined the course and will appear inDecember, 2008 for final examination.
Auxiliary Nurse-Cum-Midwife Course Under(10+2) Vocational Scheme
This course is affiliated to Central Board ofSecondary Education. 20 students were promotedto class XIIth. 20 students appeared in the finalexamination for CBSE, held in March, 2008 and allcandidates were passed out. At Present admissioncapacity in class XIth is increased 20 students to 40students and enrolled 40 students in class XIth.
Students Health : Minor ailments were treated atthe MCH Centre attach to school but for majorproblems students were referred to Smt. S.K.Hospital for further treatment.
Clinical Experience : The students have theirclinical experience in Rural and Urban Health Centre,different Hospitals and Institutions in Delhi and outof Delhi.
Ram Chand Lohia Infant Welfare Centre, under LadyReading Health School provides field practice areafor Urban Health experience for the students andgives integrated M.C.H. Family Welfare Services toover 45,000 population.
A survey was conducted to find out the recent statusof Immunization and number of target couple in thecommunity under the control of Lady Reading HealthSchool and the beneficiaries of family planningmethod. The target couple detected during the periodwas 8300 and it is found that there is 92% to 95%coverage of all immunization.
On the basis of different surveys conducted, HealthEducation Programme organized in the school centeras well as in the community by different approachesi.e. Film shows, baby shows, magic show, culturalprogrammes, puppet show, role play followed by thegroup exhibitions, speech competition on child careupto 2 years.
The Total Budget for the institution and familywelfare staff of Rs. 1, 87,00,000/- (Rs. one croreand eighty seven lacs only). (2008-2009). Staffand students actively participated in 'Pulse PolioProgramme', Reproductive Child Health Programmeand Perfect Health Mela etc. during the year.
15.2115.2115.2115.2115.21 Pasteur Institute of India (Pasteur Institute of India (Pasteur Institute of India (Pasteur Institute of India (Pasteur Institute of India (PIIPIIPIIPIIPII)))))CoonoorCoonoorCoonoorCoonoorCoonoor
The Institute started functioning as Pasteur Instituteof Southern India on 6th April, 1907 and the Institutetook a new birth as the Pasteur Institute of India(registered as Society under the SocietiesRegistration Act, 1860) and started functioning as
244
ANNUAL REPORT 2008-09
an autonomous body under the Ministry of Health &Family Welfare, Government of India, New Delhi from10th February, 1977.
The Institute has a well stocked library with 4158books and 12199 bound volumes, 11 internationaljournals, 15 Indian journals and WHO publication(Global subscription).
Activities undertaken during 2007-08 were:-
� Production of Tissue Culture Anti-rabiesVaccine for humans. The Institute is a pioneerin the production of Rabies Vaccine since itsestablishment. In the year 2001, the Vero CellDerived Purified Rabies vaccine was releasedfor human use, after testing at Central DrugsLaboratory, Kasauli.
� Production of DTP group of vaccine for EPIprogramme. It produced DPT group ofvaccines for the national programme ofimmunization in 1982.
� Training programmes and post-graduateprogrammes. The Institute offers trainingprogrammes to University students pursuingMedicine, Pharmacy, Microbiology,Biotechnology and related subjects. During2007-08, 6 short term courses were arrangedfor exposure to 53 post graduate students invarious basic techniques of vaccineproduction.
� Centre for training in Rabies VaccineProduction and DTP group of vaccines andQuality Control.
� Academic programme for Ph.D affiliated toBharathiar University, Coimbatore andM.D.(Microbiology) affiliated to Tamilnadu Dr.M.G.R. Medical University, Madras. It is affiliatedto Bharathiar University, Coimbatore forconducting Ph.D programme in Microbiologyas full time and part time basis. It is also affiliatedto Dr. MGR. Medical University, Chennai fordoing MD in Microbiology.
� Continuous in-house Research and
Development on existing vaccine producedby the Institute.
Present activities (upto 13th January, 2009):
Breeding of Mice and Guinea pigs for Experimentalpurpose (Testing of vaccines)- A total of 2518numbers of mice and 105 numbers of guinea pig havebeen applied to various production and quality controldivision for regulatory test/R&D experiments. Inaddition, 2320 numbers of mice and 327 numbers ofguinea pigs have been supplied to neighbouringinstitutes, having Committee for the Purpose ofControl and Supervision of Experiments on Animal(CPCSEA) registration, for breeding/experiments. Ascientific study on breeding performance ofconventionality reared out bred Swiss mice understandard and enriched environment was carried outand a brief report of its finding has been prepared topresent it in the upcoming National symposium atCDRI, Lucknow. To increase the breeding strengthof guinea pig, a total of 229 numbers of guinea pigshave been purchased from neighbouring CPCSEAregistered breeding facility. Guinea pig breeding inrack system. Instead of conventional pan system,has also been carried out to monitor the productivity.Health monitoring of guinea pigs and mice has beenperformed.
NPSP/Clinical Laboratory: A new set up of ClinicalLaboratory was functioning from 21/7/2008. 174blood/urine samples were tested for tests like Bloodgrouping, Haemoglobin, Blood TC, DC, ESR,Glucose, Triglycerides, Cholesterol, HDL Cholesterol,LDL Cholesterol, Urea, Uric Acid, Creatinine, Bilirubintotal, direct, SGOT, SGPT, Alkaline, Phosphates,Widal, RF and Urine analysis.
QCD/ Rapid Fluorescent Focus Inhibition Test(RFFIT) test: Potency test on TCARV vaccine wascarried out. One batch of Mouse adopted ChallengeVirus preparation for NIH Potency test was preparedand the titre value was confirmed by virus titrationtest performed at three different occasions in mice.Potency test on two batches of Tetanus Vaccinereceived from Shantha Biotechnics Pvt. Ltd.,Hyderabad, was also carried out. 489 Sera samples
245
ANNUAL REPORT 2008-09
were tested for the detection and qualification ofrabies neutralizing antibody by Rapid FluorescentFocus Inhibition Test (RFFIT). This includes serasamples received from our dispensary and variousprivate organizations. Two batches of rabiesconjugate have been prepared using highly purifiedrabies Immunoglobulin for our day to day regular use.Two batches of Murine -neuroblastoma-2A cell strainhave been stored into Liquid nitrogen forcryopreservation for future use. Two batches ofRabies Virus (PV 3462) adopted to Neuro cells haveprepared and aliqoted into 87 vials and stored into -80degree C deep freezer for future use.
Training activities: Various officers of the Institutehave attended different training programmes andworkshops within India during the year. Internaltraining programme on various topics such as ClinicalLaboratory, Clean Room, Purchase Procedures,Clinical Microbiology have also been organized forofficials up to the level of Research Assistants/Technical Assistants staff.
Academic Activities: The Institute revived theIndustrial visit to Graduate and Post-Graduatestudents from different college/universities. 55Batches of Students from different colleges anduniversities visited to enrich their scientif icknowledge and to create awareness in vaccineproduction and immunization procedures etc. Atpreset for M.Sc., Final year students' project workis in process. Project duration is 15th December,2008 to 15th March, 2009. 40 students haveenrolled for project work. Norms have been arrivedat for Project work for a period of 3 months and forPh. D in Microbiology field (affiliated to BharathiarUniversity, Coimbatore).
The library is connected with internet to utilize the E-journal service to the maximum. Journals Club andScientific Club are formed. Enrolled as a member inVirtual Library - regional resource sharing consortiumcentre to share the Electronic Resources.
Facilities Commissioned/Installed: SewageTreatment Plant (STP) to comply with the norms ofthe Tamil Nadu Pollution Control Board.
Quality Assurance: Restructured the QualityAssurance section and the following activities werecarried out:
� To strengthen the Good ManufacturingPractices, copies of WHO Technical Reportseries No. 823 and Scheduled-M documentmade available to all the Officers up to thelevel of Assistant Research Officer Cadre.
� Actively participated during the ExpertCommittee's visit to Pasteur Institute of Indiafrom 10th to 12th July, 2008 under theChairmanship of Dr. Surinder Singh, DCG (I).
� Verification of stock of biological at differentstages were undertaken.
� Compilation of Protocols and batchprocessing records pertaining to TissueCulture Rabies Vaccine carried out.
� Regular monitoring of cold storage of seedcopies (DPT group of vaccines)
� Stock verification of working seed copies(DPT group) available at productionlaboratories carried out and brought back tothe custody of Quality Assurance section.
� Environmental monitoring at Animal HouseBreeding Centre carried out (Particle andViable Counts made)
� Organized re-Investigation of toxicity inpurified Tetanus & Diphtheria pools available.
� In the proposed Measles vaccine productionlab (modified old DPT stores) functioning ofHot and cold rooms and Air Handling systemInspected and a detailed Infra-structurecompletion reports along with theQualification documents prepared.
Revenue earned during 2007-08 and 2008-09:
The revenue earned during the financial year 2007-08 was Rs.832.67 lakhs. The details of the allocation,supply and revenue earned during 2007-08 are asunder:
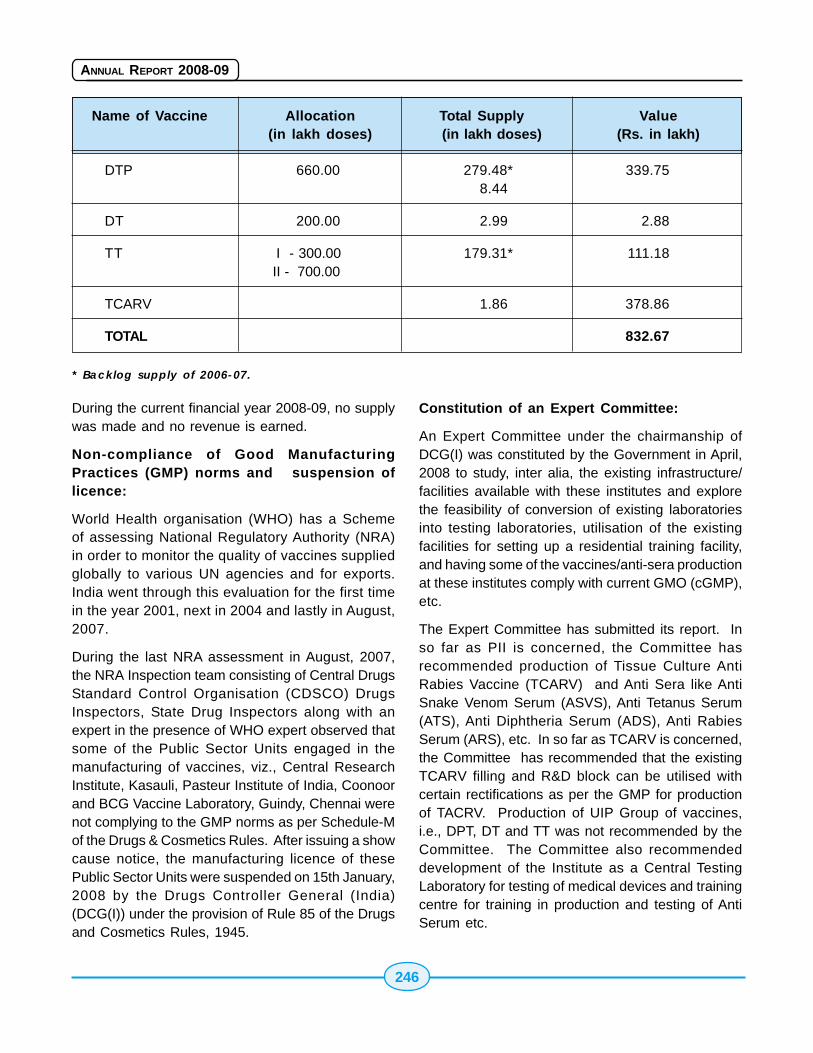
246
ANNUAL REPORT 2008-09
Name of Vaccine Allocation Total Supply Value(in lakh doses) (in lakh doses) (Rs. in lakh)
DTP 660.00 279.48* 339.758.44
DT 200.00 2.99 2.88
TT I - 300.00 179.31* 111.18 II - 700.00
TCARV 1.86 378.86
TOTAL 832.67
* Backlog supply of 2006-07.
During the current financial year 2008-09, no supplywas made and no revenue is earned.
Non-compliance of Good ManufacturingPractices (GMP) norms and suspension oflicence:
World Health organisation (WHO) has a Schemeof assessing National Regulatory Authority (NRA)in order to monitor the quality of vaccines suppliedglobally to various UN agencies and for exports.India went through this evaluation for the first timein the year 2001, next in 2004 and lastly in August,2007.
During the last NRA assessment in August, 2007,the NRA Inspection team consisting of Central DrugsStandard Control Organisation (CDSCO) DrugsInspectors, State Drug Inspectors along with anexpert in the presence of WHO expert observed thatsome of the Public Sector Units engaged in themanufacturing of vaccines, viz., Central ResearchInstitute, Kasauli, Pasteur Institute of India, Coonoorand BCG Vaccine Laboratory, Guindy, Chennai werenot complying to the GMP norms as per Schedule-Mof the Drugs & Cosmetics Rules. After issuing a showcause notice, the manufacturing licence of thesePublic Sector Units were suspended on 15th January,2008 by the Drugs Controller General (India)(DCG(I)) under the provision of Rule 85 of the Drugsand Cosmetics Rules, 1945.
Constitution of an Expert Committee:
An Expert Committee under the chairmanship ofDCG(I) was constituted by the Government in April,2008 to study, inter alia, the existing infrastructure/facilities available with these institutes and explorethe feasibility of conversion of existing laboratoriesinto testing laboratories, utilisation of the existingfacilities for setting up a residential training facility,and having some of the vaccines/anti-sera productionat these institutes comply with current GMO (cGMP),etc.
The Expert Committee has submitted its report. Inso far as PII is concerned, the Committee hasrecommended production of Tissue Culture AntiRabies Vaccine (TCARV) and Anti Sera like AntiSnake Venom Serum (ASVS), Anti Tetanus Serum(ATS), Anti Diphtheria Serum (ADS), Anti RabiesSerum (ARS), etc. In so far as TCARV is concerned,the Committee has recommended that the existingTCARV filling and R&D block can be utilised withcertain rectifications as per the GMP for productionof TACRV. Production of UIP Group of vaccines,i.e., DPT, DT and TT was not recommended by theCommittee. The Committee also recommendeddevelopment of the Institute as a Central TestingLaboratory for testing of medical devices and trainingcentre for training in production and testing of AntiSerum etc.
247
ANNUAL REPORT 2008-09
Current Status of functioning of PII, Coonoor:
Currently, the manufacturing license of the PIICoonoor is under suspension. No production ofvaccine and sera is being undertaken. Therecommendations of the Expert Committee underDCG(I) are under consideration.
15.2215.2215.2215.2215.22 All India Institute of PhysicalAll India Institute of PhysicalAll India Institute of PhysicalAll India Institute of PhysicalAll India Institute of PhysicalMedicine and RehabilitationMedicine and RehabilitationMedicine and RehabilitationMedicine and RehabilitationMedicine and Rehabilitation(((((AIIPMRAIIPMRAIIPMRAIIPMRAIIPMR), Mumbai), Mumbai), Mumbai), Mumbai), Mumbai
The All India Institute of Physical Medicine andRehabilitation, Mumbai, established in 1955 is an apexInstitute in the field of Rehabilitation Medicine underthe administrative control of D.G.H.S.
Objectives of the Institute -
1. To provide need based Medical RehabilitationServices including provision of Prosthetic &Orthotic appliances for persons with neuro-musculo-skeletal (locomotor) disorders.
2. To provide training at Under Graduate andPost Graduate level to all categories ofRehabilitation professionals.
3. To conduct research in the field of PhysicalMedicine and Rehabilitation (P.M.R.).
4. To provide and promote community basedprogrammes of Disability Prevention &Rehabilitation for the rural disabled.
Provision of comprehensive rehabilitation servicesto the Physically Disabled demands interdisciplinaryteam approach.
The following Rehabilitation Science Departmentsprovide standard services to the physically disabledattending this institute after thorough assessmentand goal setting.
(i) Medical Rehabilitation department, 60bedded ward for reconstructive surgeries andindoor rehabilitation programme.
(ii) Radiology
(iii) Pathology
(iv) Rehabilitation Nursing.
(v) Physiotherapy
(vi) Occupational Therapy
(vii) Speech & Audiology Section.
(viii) Prosthetic & Orthotic (with Workshop)
(ix) Medical Social Work
(x) Vocational Training
(xi) Hindi Cell.
xii) Vocational Guidance
(xiii) Academic
(xiv) Bio-Medical Engineering Dept.
All the departments are adequately equipped withstate of the art equipments and highly skilledmanpower.The building complexes in the institutepremises are totally barrier free, accessible to thepersons with disability.
The Institute has initiated several steps forcommencing new service lines to meet the challengesarising from increasing incidence of disability due tonon -communicable disorders. In the current FiveYear Plan the institute has proposed to build up itscapacity further which are mentioned below in orderto reach more physically challenged people leavingin the institute accessible areas.
� Expansion of AIIPM&R and setting upRegional Center.
� Rehabilitation services as part of primaryhealth care.
� Domiciliary Services for Persons withdisability in urban slum.
� Pilot Project on Tele Rehabilitation.
� Diabetic foot rehabilitation programme.
Research and Development Activities
� Institute has set up Gait & Motion Analysislaboratory for undertaking Bio-mechanicalResearch Activities in the field of muscularskeletal disorder for objective assessment
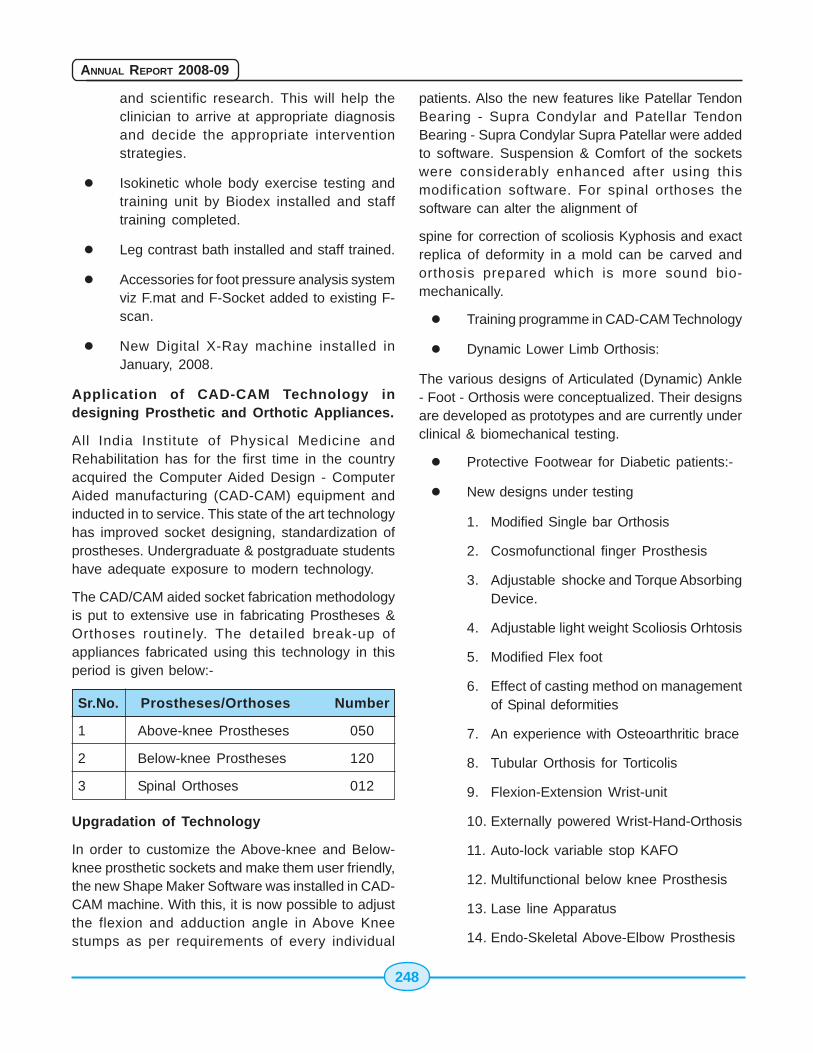
248
ANNUAL REPORT 2008-09
and scientific research. This will help theclinician to arrive at appropriate diagnosisand decide the appropriate interventionstrategies.
� Isokinetic whole body exercise testing andtraining unit by Biodex installed and stafftraining completed.
� Leg contrast bath installed and staff trained.
� Accessories for foot pressure analysis systemviz F.mat and F-Socket added to existing F-scan.
� New Digital X-Ray machine installed inJanuary, 2008.
Application of CAD-CAM Technology indesigning Prosthetic and Orthotic Appliances.
All India Institute of Physical Medicine andRehabilitation has for the first time in the countryacquired the Computer Aided Design - ComputerAided manufacturing (CAD-CAM) equipment andinducted in to service. This state of the art technologyhas improved socket designing, standardization ofprostheses. Undergraduate & postgraduate studentshave adequate exposure to modern technology.
The CAD/CAM aided socket fabrication methodologyis put to extensive use in fabricating Prostheses &Orthoses routinely. The detailed break-up ofappliances fabricated using this technology in thisperiod is given below:-
Sr.No. Prostheses/Orthoses Number
1 Above-knee Prostheses 050
2 Below-knee Prostheses 120
3 Spinal Orthoses 012
Upgradation of Technology
In order to customize the Above-knee and Below-knee prosthetic sockets and make them user friendly,the new Shape Maker Software was installed in CAD-CAM machine. With this, it is now possible to adjustthe flexion and adduction angle in Above Kneestumps as per requirements of every individual
patients. Also the new features like Patellar TendonBearing - Supra Condylar and Patellar TendonBearing - Supra Condylar Supra Patellar were addedto software. Suspension & Comfort of the socketswere considerably enhanced after using thismodification software. For spinal orthoses thesoftware can alter the alignment of
spine for correction of scoliosis Kyphosis and exactreplica of deformity in a mold can be carved andorthosis prepared which is more sound bio-mechanically.
� Training programme in CAD-CAM Technology
� Dynamic Lower Limb Orthosis:
The various designs of Articulated (Dynamic) Ankle- Foot - Orthosis were conceptualized. Their designsare developed as prototypes and are currently underclinical & biomechanical testing.
� Protective Footwear for Diabetic patients:-
� New designs under testing
1. Modified Single bar Orthosis
2. Cosmofunctional finger Prosthesis
3. Adjustable shocke and Torque AbsorbingDevice.
4. Adjustable light weight Scoliosis Orhtosis
5. Modified Flex foot
6. Effect of casting method on managementof Spinal deformities
7. An experience with Osteoarthritic brace
8. Tubular Orthosis for Torticolis
9. Flexion-Extension Wrist-unit
10. Externally powered Wrist-Hand-Orthosis
11. Auto-lock variable stop KAFO
12. Multifunctional below knee Prosthesis
13. Lase line Apparatus
14. Endo-Skeletal Above-Elbow Prosthesis
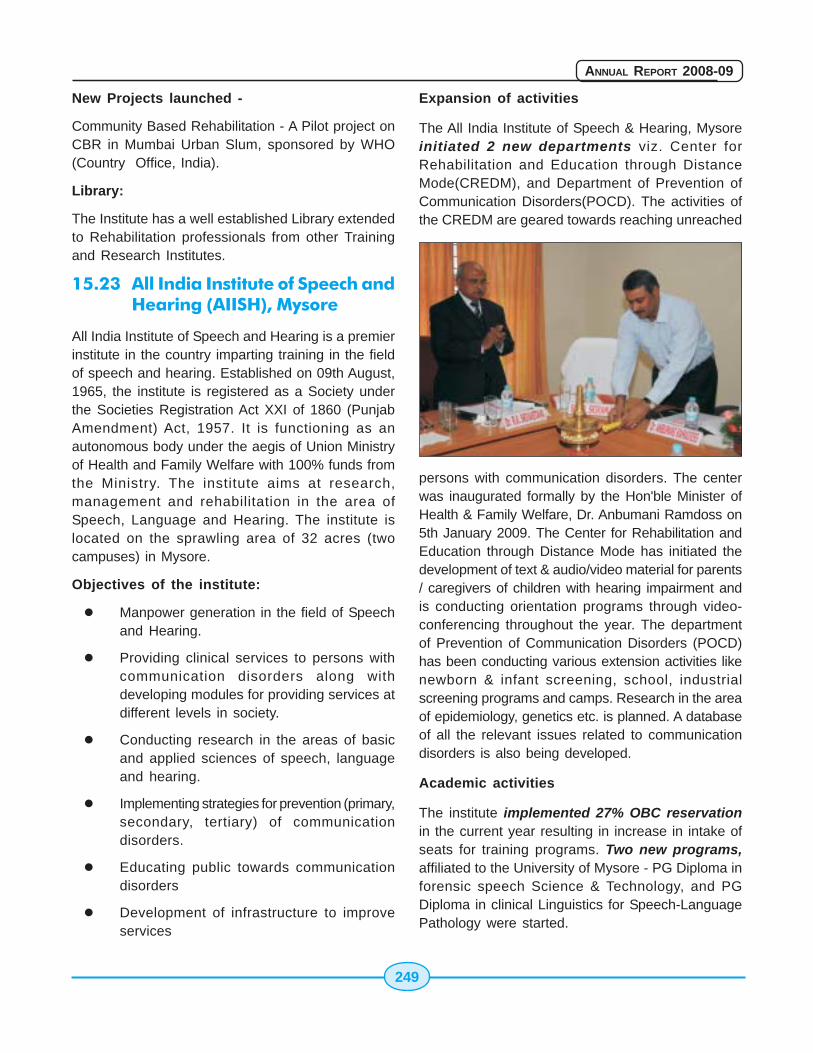
249
ANNUAL REPORT 2008-09
New Projects launched -
Community Based Rehabilitation - A Pilot project onCBR in Mumbai Urban Slum, sponsored by WHO(Country Office, India).
Library:
The Institute has a well established Library extendedto Rehabilitation professionals from other Trainingand Research Institutes.
15.23 All India Institute of Speech andHearing (AIISH), Mysore
All India Institute of Speech and Hearing is a premierinstitute in the country imparting training in the fieldof speech and hearing. Established on 09th August,1965, the institute is registered as a Society underthe Societies Registration Act XXI of 1860 (PunjabAmendment) Act, 1957. It is functioning as anautonomous body under the aegis of Union Ministryof Health and Family Welfare with 100% funds fromthe Ministry. The institute aims at research,management and rehabilitation in the area ofSpeech, Language and Hearing. The institute islocated on the sprawling area of 32 acres (twocampuses) in Mysore.
Objectives of the institute:
� Manpower generation in the field of Speechand Hearing.
� Providing clinical services to persons withcommunication disorders along withdeveloping modules for providing services atdifferent levels in society.
� Conducting research in the areas of basicand applied sciences of speech, languageand hearing.
� Implementing strategies for prevention (primary,secondary, tertiary) of communicationdisorders.
� Educating public towards communicationdisorders
� Development of infrastructure to improveservices
Expansion of activities
The All India Institute of Speech & Hearing, Mysoreinitiated 2 new departments viz. Center forRehabilitation and Education through DistanceMode(CREDM), and Department of Prevention ofCommunication Disorders(POCD). The activities ofthe CREDM are geared towards reaching unreached
persons with communication disorders. The centerwas inaugurated formally by the Hon'ble Minister ofHealth & Family Welfare, Dr. Anbumani Ramdoss on5th January 2009. The Center for Rehabilitation andEducation through Distance Mode has initiated thedevelopment of text & audio/video material for parents/ caregivers of children with hearing impairment andis conducting orientation programs through video-conferencing throughout the year. The departmentof Prevention of Communication Disorders (POCD)has been conducting various extension activities likenewborn & infant screening, school, industrialscreening programs and camps. Research in the areaof epidemiology, genetics etc. is planned. A databaseof all the relevant issues related to communicationdisorders is also being developed.
Academic activities
The institute implemented 27% OBC reservationin the current year resulting in increase in intake ofseats for training programs. Two new programs,affiliated to the University of Mysore - PG Diploma inforensic speech Science & Technology, and PGDiploma in clinical Linguistics for Speech-LanguagePathology were started.

250
ANNUAL REPORT 2008-09
The distance mode Diploma in Hearing,Language and Speech program was extendedto new 6 study centers - (a) Chatrapati ShahujiMaharaj Medical University, Lucknow, Uttar Pradesh,(b) Indira Gandi Medical College, Shimla, HimachalPradesh, (c) Rajendra Institute of Medical Sciences,Ranchi, Jharkhand, (d) Jawahar Lal Nehru MedicalCollege and Associated Group of Hospitals, Ajmer,Rajasthan, (e) S. C. B. Medical College, Cuttack,Orissa, and (f) Netaji Subhash Chandra Bose MedicalCollege, Jabalpur, Madhya Pradesh. The study centerat Maulana Azad Medical College, New Delhi wasshifted to Dr. Ram Manohar Lohia Hospital, New Delhi.
The monthly lecture series continued and 15 lectureson various topics related to communication disorderswere conducted during the period.
Clinical Services
A total of 20652 new clients, and 28455 repeat clientsregistered during the period year. A total of 10429clients (50042 sessions of 45 minutes each) weregiven in speech-language therapy, listening training,AAC rehabilitation and PT/OT. In the preschool 165children were trained with 19106 sessions. 10 groupsof parents were empowered in 2259 sessions. 1748hearing aids were issued to patients under ADIPscheme and hearing aid sale. 254 ENT majoroperations were carried out at K R Hospital and 33minor operations were done at AIISH. Appendix Ishows the details of clinical services.
Research activities
The institute has undertaken four extramural funded
projects - two from WHO, one each from theDepartment of Science & Technology and Society ofBiomedical Technology.
Major Projects
A project on sensitizing teachers on academicproblems in school children in Karnataka has alsobeen taken up as a collaborative project with SarvaShikshana Abhiyaan, Karnataka. In addition 7 AIISHResearch Fund projects were taken up by the facultyof the institute. A total of 21 workshops/ seminarswere conducted during the period. AIISH hosted theRCI meet of course Coordinators of BASLP andMASLP Courses held on 24th & 25th February 2009.
Administration
Sixth Central Pay Commission pay scales asapproved by GOI were implemented to the staff ofthe institute. The Vigilance week was observed atthe institute with oath taking and debate on corruption.Hindi Saptah, Women's day etc. were also celebrated.The AIISH Gymkhana was active through out the yearwith Vidya Vikas program, open day, science dayand intercollegiate cultural festival while the electionswere held in the month of August 2008 for new officebearers.
Library and Information Centre
A total of 695 text books were added to the AIISHlibrary and Information Center and digitization of thelibrary is in progress. The Journal of AIISH which isindexed (No. ISSN 0973 - 662 X) brought out its 27thvolume.
Future Development
The institute sent an application for DeemedUniversity status which was forwarded by theMinistry of Health & Family Welfare to UGC. Theinstitute also made a start towards the upgradationto a super specialty center and had four meetingsas directed by the committee from the Ministry ofHealth & Family Welfare. The project proposal forupgradation of the institute to the super specialtycentre of excellence is being processed at theMinistry.
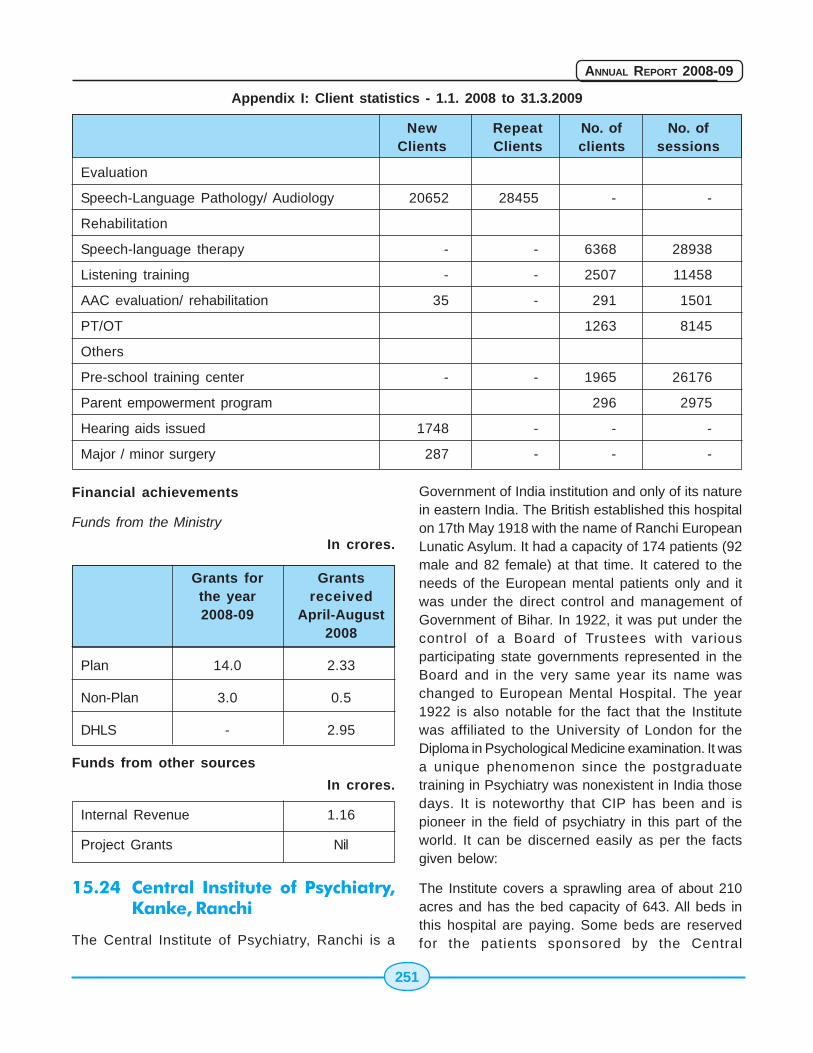
251
ANNUAL REPORT 2008-09
Appendix I: Client statistics - 1.1. 2008 to 31.3.2009
New Repeat No. of No. ofClients Clients clients sessions
Evaluation
Speech-Language Pathology/ Audiology 20652 28455 - -
Rehabilitation
Speech-language therapy - - 6368 28938
Listening training - - 2507 11458
AAC evaluation/ rehabilitation 35 - 291 1501
PT/OT 1263 8145
Others
Pre-school training center - - 1965 26176
Parent empowerment program 296 2975
Hearing aids issued 1748 - - -
Major / minor surgery 287 - - -
Financial achievements
Funds from the Ministry
In crores.
Grants for Grantsthe year received2008-09 April-August
2008
Plan 14.0 2.33
Non-Plan 3.0 0.5
DHLS - 2.95
Funds from other sources
In crores.
Internal Revenue 1.16
Project Grants Nil
15.24 Central Institute of Psychiatry,Kanke, Ranchi
The Central Institute of Psychiatry, Ranchi is a
Government of India institution and only of its naturein eastern India. The British established this hospitalon 17th May 1918 with the name of Ranchi EuropeanLunatic Asylum. It had a capacity of 174 patients (92male and 82 female) at that time. It catered to theneeds of the European mental patients only and itwas under the direct control and management ofGovernment of Bihar. In 1922, it was put under thecontrol of a Board of Trustees with variousparticipating state governments represented in theBoard and in the very same year its name waschanged to European Mental Hospital. The year1922 is also notable for the fact that the Institutewas affiliated to the University of London for theDiploma in Psychological Medicine examination. It wasa unique phenomenon since the postgraduatetraining in Psychiatry was nonexistent in India thosedays. It is noteworthy that CIP has been and ispioneer in the field of psychiatry in this part of theworld. It can be discerned easily as per the factsgiven below:
The Institute covers a sprawling area of about 210acres and has the bed capacity of 643. All beds inthis hospital are paying. Some beds are reservedfor the patients sponsored by the Central
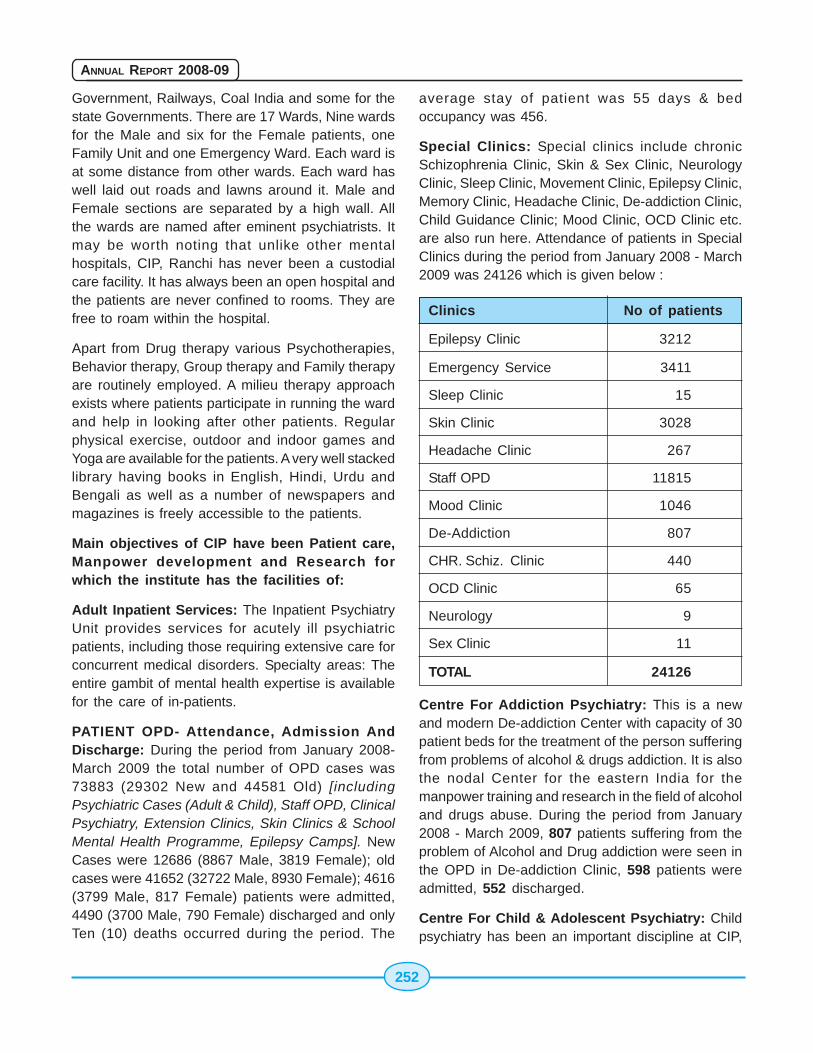
252
ANNUAL REPORT 2008-09
Government, Railways, Coal India and some for thestate Governments. There are 17 Wards, Nine wardsfor the Male and six for the Female patients, oneFamily Unit and one Emergency Ward. Each ward isat some distance from other wards. Each ward haswell laid out roads and lawns around it. Male andFemale sections are separated by a high wall. Allthe wards are named after eminent psychiatrists. Itmay be worth noting that unlike other mentalhospitals, CIP, Ranchi has never been a custodialcare facility. It has always been an open hospital andthe patients are never confined to rooms. They arefree to roam within the hospital.
Apart from Drug therapy various Psychotherapies,Behavior therapy, Group therapy and Family therapyare routinely employed. A milieu therapy approachexists where patients participate in running the wardand help in looking after other patients. Regularphysical exercise, outdoor and indoor games andYoga are available for the patients. A very well stackedlibrary having books in English, Hindi, Urdu andBengali as well as a number of newspapers andmagazines is freely accessible to the patients.
Main objectives of CIP have been Patient care,Manpower development and Research forwhich the institute has the facilities of:
Adult Inpatient Services: The Inpatient PsychiatryUnit provides services for acutely ill psychiatricpatients, including those requiring extensive care forconcurrent medical disorders. Specialty areas: Theentire gambit of mental health expertise is availablefor the care of in-patients.
PATIENT OPD- Attendance, Admission AndDischarge: During the period from January 2008-March 2009 the total number of OPD cases was73883 (29302 New and 44581 Old) [includingPsychiatric Cases (Adult & Child), Staff OPD, ClinicalPsychiatry, Extension Clinics, Skin Clinics & SchoolMental Health Programme, Epilepsy Camps]. NewCases were 12686 (8867 Male, 3819 Female); oldcases were 41652 (32722 Male, 8930 Female); 4616(3799 Male, 817 Female) patients were admitted,4490 (3700 Male, 790 Female) discharged and onlyTen (10) deaths occurred during the period. The
average stay of patient was 55 days & bedoccupancy was 456.
Special Clinics: Special clinics include chronicSchizophrenia Clinic, Skin & Sex Clinic, NeurologyClinic, Sleep Clinic, Movement Clinic, Epilepsy Clinic,Memory Clinic, Headache Clinic, De-addiction Clinic,Child Guidance Clinic; Mood Clinic, OCD Clinic etc.are also run here. Attendance of patients in SpecialClinics during the period from January 2008 - March2009 was 24126 which is given below :
Clinics No of patients
Epilepsy Clinic 3212
Emergency Service 3411
Sleep Clinic 15
Skin Clinic 3028
Headache Clinic 267
Staff OPD 11815
Mood Clinic 1046
De-Addiction 807
CHR. Schiz. Clinic 440
OCD Clinic 65
Neurology 9
Sex Clinic 11
TOTAL 24126
Centre For Addiction Psychiatry: This is a newand modern De-addiction Center with capacity of 30patient beds for the treatment of the person sufferingfrom problems of alcohol & drugs addiction. It is alsothe nodal Center for the eastern India for themanpower training and research in the field of alcoholand drugs abuse. During the period from January2008 - March 2009, 807 patients suffering from theproblem of Alcohol and Drug addiction were seen inthe OPD in De-addiction Clinic, 598 patients wereadmitted, 552 discharged.
Centre For Child & Adolescent Psychiatry: Childpsychiatry has been an important discipline at CIP,

253
ANNUAL REPORT 2008-09
Ranchi. A child guidance clinic was started in 1950and an independent 50-bed child psychiatry unit in1975. This unit also imparts training to residentdoctors and postgraduate students in the field of childand adolescent mental health. It caters the needs ofgrossly psychotic children, children with developmentdisorders and mental retardation. The parents arerequired to stay with their children for the duration ofthe treatment. During the period from January 2008- March 2009, 5834 (New-1747, Follow-up-4087)patients attended OPD for treatment.
Department Of Clinical Psychology
The Clinical Psychology department at the CentralInstitute of Psychiatry was established in 1948 and
PSYCHOSOCIAL UNIT
is the oldest independent department of ClinicalPsychology in India. Over a period of years thedepartment has gained excellence in the field ofteaching, training, research and clinical services.
Teaching And Training
Initially, the department was involved in the patientcare only; however, later in the year 1962 a teachingcourse in Clinical Psychology was also started. Thecourse was known as Diploma in Medical and SocialPsychology (now known as M.Phil in Medical andSocial Psychology). In 1972 Ph.D. in ClinicalPsychology was started. At present, each year, 12M.Phil and 4 Ph.D. seats are filled through an opennational level entrance examination. Our faculty
includes 1 Professor, 2 assistant professor, 2assistant psychologists and 1 lab assistant.
Clinical Services
The department provides non-pharmacologicalmanagement for the patients of wide rangingpsychiatric problems with the help of psychotherapy,counseling, group meetings, psycho-education,psycho-diagnostic testing, intelligence testing andso forth. Apart from the patients coming to thehospital, the department is also involved in providingservices at various extension clinics as well asschools. There is a separate out-patient unit of thedepartment. The out-patient unit either gets referralfrom the general OPD of the hospital or people candirectly come and seek help for their psychologicalproblems. The psychosocial OPD, as it is called,caters to the needs of those patients who suffer fromminor psychological problems and who can be belowexclusively by psychological methods viz counseling,behaviour therapy or biofeedback or relaxationtherapy. Recently we have started an extension clinicfor development of Military Psychiatry in DeepatoliCantt, Ranchi where the complete team of mentalhealth professionals visits weekly to offer theirservices to the families of the army personnel.
Psychology Labaratory
The clinical psychology lab was established for thefirst time in India in 1949. It has various psychologicaltests, rating scales, instruments and apparatus whichaid in the management of the patients. The lab hasthese tests designed for use with both children aswell as adult population. There are in total 13equipments and apparatuses, 43 tests for theassessment of cognitive functions, 19 tests for theassessment of personality which includes projectiveand objective tests and there are 44 various scales.These tests are for use with both child-hood as wellas adult population. There are also 66 new testswhich the lab has acquired which assess variousdomains of personality and cognition.
Departmental Activities
Apart from management of the patients, thedepartment holds weekly academic exercises in the
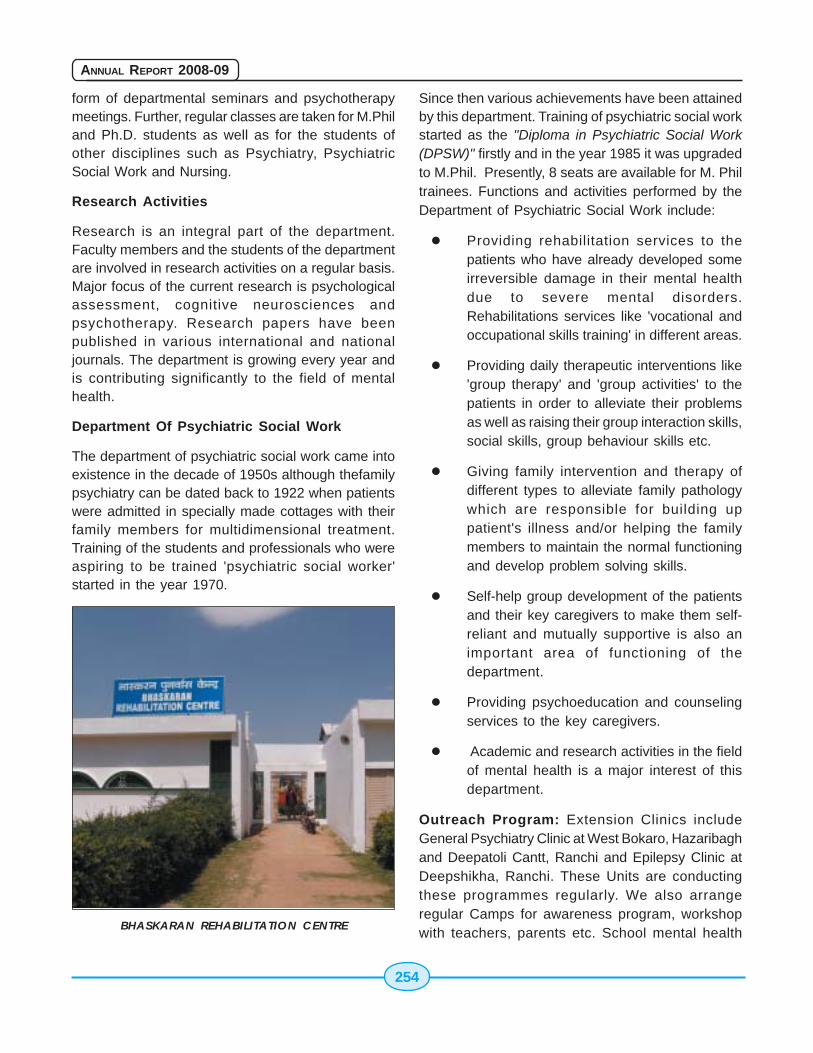
254
ANNUAL REPORT 2008-09
form of departmental seminars and psychotherapymeetings. Further, regular classes are taken for M.Philand Ph.D. students as well as for the students ofother disciplines such as Psychiatry, PsychiatricSocial Work and Nursing.
Research Activities
Research is an integral part of the department.Faculty members and the students of the departmentare involved in research activities on a regular basis.Major focus of the current research is psychologicalassessment, cognitive neurosciences andpsychotherapy. Research papers have beenpublished in various international and nationaljournals. The department is growing every year andis contributing significantly to the field of mentalhealth.
Department Of Psychiatric Social Work
The department of psychiatric social work came intoexistence in the decade of 1950s although thefamilypsychiatry can be dated back to 1922 when patientswere admitted in specially made cottages with theirfamily members for multidimensional treatment.Training of the students and professionals who wereaspiring to be trained 'psychiatric social worker'started in the year 1970.
BHASKARAN REHABILITATION CENTRE
Since then various achievements have been attainedby this department. Training of psychiatric social workstarted as the "Diploma in Psychiatric Social Work(DPSW)" firstly and in the year 1985 it was upgradedto M.Phil. Presently, 8 seats are available for M. Philtrainees. Functions and activities performed by theDepartment of Psychiatric Social Work include:
� Providing rehabilitation services to thepatients who have already developed someirreversible damage in their mental healthdue to severe mental disorders.Rehabilitations services like 'vocational andoccupational skills training' in different areas.
� Providing daily therapeutic interventions like'group therapy' and 'group activities' to thepatients in order to alleviate their problemsas well as raising their group interaction skills,social skills, group behaviour skills etc.
� Giving family intervention and therapy ofdifferent types to alleviate family pathologywhich are responsible for building uppatient's illness and/or helping the familymembers to maintain the normal functioningand develop problem solving skills.
� Self-help group development of the patientsand their key caregivers to make them self-reliant and mutually supportive is also animportant area of functioning of thedepartment.
� Providing psychoeducation and counselingservices to the key caregivers.
� Academic and research activities in the fieldof mental health is a major interest of thisdepartment.
Outreach Program: Extension Clinics includeGeneral Psychiatry Clinic at West Bokaro, Hazaribaghand Deepatoli Cantt, Ranchi and Epilepsy Clinic atDeepshikha, Ranchi. These Units are conductingthese programmes regularly. We also arrangeregular Camps for awareness program, workshopwith teachers, parents etc. School mental health
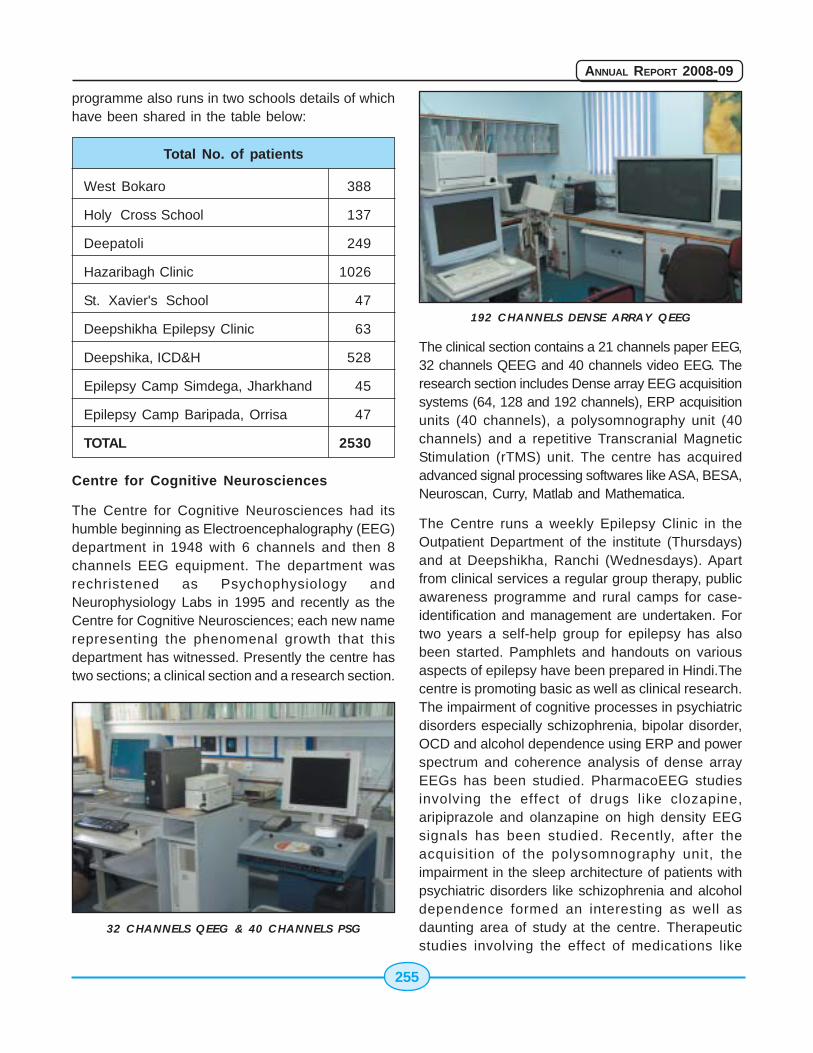
255
ANNUAL REPORT 2008-09
programme also runs in two schools details of whichhave been shared in the table below:
Total No. of patients
West Bokaro 388
Holy Cross School 137
Deepatoli 249
Hazaribagh Clinic 1026
St. Xavier's School 47
Deepshikha Epilepsy Clinic 63
Deepshika, ICD&H 528
Epilepsy Camp Simdega, Jharkhand 45
Epilepsy Camp Baripada, Orrisa 47
TOTAL 2530
Centre for Cognitive Neurosciences
The Centre for Cognitive Neurosciences had itshumble beginning as Electroencephalography (EEG)department in 1948 with 6 channels and then 8channels EEG equipment. The department wasrechristened as Psychophysiology andNeurophysiology Labs in 1995 and recently as theCentre for Cognitive Neurosciences; each new namerepresenting the phenomenal growth that thisdepartment has witnessed. Presently the centre hastwo sections; a clinical section and a research section.
32 CHANNELS QEEG & 40 CHANNELS PSG
192 CHANNELS DENSE ARRAY QEEG
The clinical section contains a 21 channels paper EEG,32 channels QEEG and 40 channels video EEG. Theresearch section includes Dense array EEG acquisitionsystems (64, 128 and 192 channels), ERP acquisitionunits (40 channels), a polysomnography unit (40channels) and a repetitive Transcranial MagneticStimulation (rTMS) unit. The centre has acquiredadvanced signal processing softwares like ASA, BESA,Neuroscan, Curry, Matlab and Mathematica.
The Centre runs a weekly Epilepsy Clinic in theOutpatient Department of the institute (Thursdays)and at Deepshikha, Ranchi (Wednesdays). Apartfrom clinical services a regular group therapy, publicawareness programme and rural camps for case-identification and management are undertaken. Fortwo years a self-help group for epilepsy has alsobeen started. Pamphlets and handouts on variousaspects of epilepsy have been prepared in Hindi.Thecentre is promoting basic as well as clinical research.The impairment of cognitive processes in psychiatricdisorders especially schizophrenia, bipolar disorder,OCD and alcohol dependence using ERP and powerspectrum and coherence analysis of dense arrayEEGs has been studied. PharmacoEEG studiesinvolving the effect of drugs like clozapine,aripiprazole and olanzapine on high density EEGsignals has been studied. Recently, after theacquisition of the polysomnography unit, theimpairment in the sleep architecture of patients withpsychiatric disorders like schizophrenia and alcoholdependence formed an interesting as well asdaunting area of study at the centre. Therapeuticstudies involving the effect of medications like
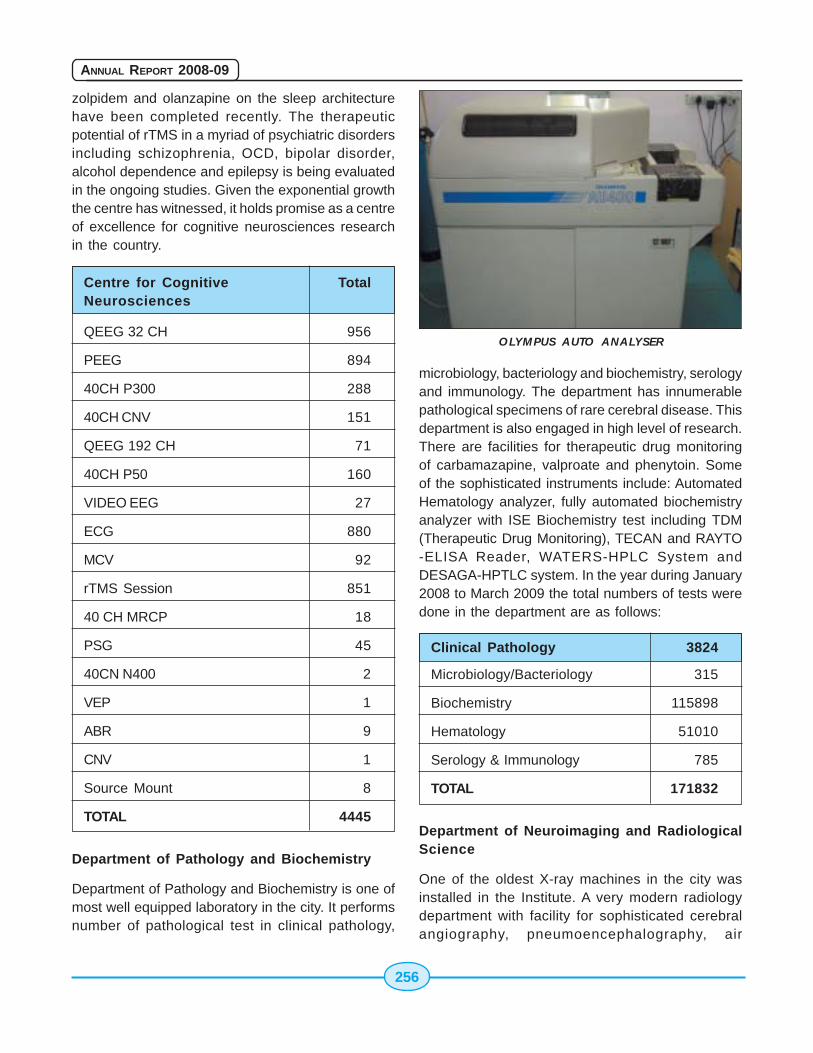
256
ANNUAL REPORT 2008-09
zolpidem and olanzapine on the sleep architecturehave been completed recently. The therapeuticpotential of rTMS in a myriad of psychiatric disordersincluding schizophrenia, OCD, bipolar disorder,alcohol dependence and epilepsy is being evaluatedin the ongoing studies. Given the exponential growththe centre has witnessed, it holds promise as a centreof excellence for cognitive neurosciences researchin the country.
Centre for Cognitive TotalNeurosciences
QEEG 32 CH 956
PEEG 894
40CH P300 288
40CH CNV 151
QEEG 192 CH 71
40CH P50 160
VIDEO EEG 27
ECG 880
MCV 92
rTMS Session 851
40 CH MRCP 18
PSG 45
40CN N400 2
VEP 1
ABR 9
CNV 1
Source Mount 8
TOTAL 4445
Department of Pathology and Biochemistry
Department of Pathology and Biochemistry is one ofmost well equipped laboratory in the city. It performsnumber of pathological test in clinical pathology,
microbiology, bacteriology and biochemistry, serologyand immunology. The department has innumerablepathological specimens of rare cerebral disease. Thisdepartment is also engaged in high level of research.There are facilities for therapeutic drug monitoringof carbamazapine, valproate and phenytoin. Someof the sophisticated instruments include: AutomatedHematology analyzer, fully automated biochemistryanalyzer with ISE Biochemistry test including TDM(Therapeutic Drug Monitoring), TECAN and RAYTO-ELISA Reader, WATERS-HPLC System andDESAGA-HPTLC system. In the year during January2008 to March 2009 the total numbers of tests weredone in the department are as follows:
Clinical Pathology 3824
Microbiology/Bacteriology 315
Biochemistry 115898
Hematology 51010
Serology & Immunology 785
TOTAL 171832
Department of Neuroimaging and RadiologicalScience
One of the oldest X-ray machines in the city wasinstalled in the Institute. A very modern radiologydepartment with facility for sophisticated cerebralangiography, pneumoencephalography, air
OLYMPUS AUTO ANALYSER

257
ANNUAL REPORT 2008-09
ventriculography, myelography etc. was establishedin 1954, long before it was started in theNeurosurgery Department in Rajendra
Medical College, Ranchi.This department has beenrenovated in 1997 by acquiring MES 100 Ma X-RayMachine, Radiograph of various body part werecarried out by the same. In 2002, another X-RayMachine Allengers 300Ma Machine was installed. In2003, Transcranial Doppler Machine (DWL System)was installed in this department. Since then clinicalworks and various dissertation study is going on tillnow. Five research works has been since completedusing the Doppler. In 2006, ultrasound and ColourDoppler Machine (Philips) was installed. Since thenclinical works are going on regularly in this machinetill now. C.T. Scan Machine, Siemens Emotion 16 (16Slice Spiral CT Scanner Machine) has been installedin 2008. Since February, 2008 clinical and researchworks have started with this machine. This CT Scanmachine, is equipped to perform, CT Angiography,CT Guided intervention and phasic studies withcontrast agent. With USG machine we can performColour Doppler study of various body parts, (Carotid,Abdominal, peripheral etc.) and also USU guidedintervention. From Jan. 2008 to March 2009 we haveperformed about 2583 (radiographs, abdominalultrasound study and CT Scans of various bodyparts).
We also plan to install a digital X-Ray machine and 3Tesla MRI machine. The MRI facilities will enable into do structural as well as functional imaging alongwith Spectroscopy studies, which is very much
16 SLICE WHOLE BODY CT SCANNER
essential for clinical and various research activitiesin Neurology and Psychiatry.
Emergency Services: A 24 hours emergencyservice is also available in the OPD of the institutewith bed strength of 16 patients (8 for male and 8 forfemale patients).
24 Hours Services of Telephonic Helpline & e-MAIL Helpline: During January to March 2009, 1192helpline calls and 322 e-mails were attended.
Training Programme: In the training program, Caseconference, Seminar, journal clubs were regularlyheld every week. Nursing Department arranged 3Continuing Nursing education programme CNEP (100participants), 1 In-service Nursing education/Training programs, which were attended by 38participants, Seminar-39 (1697 participants), CaseConference-38 (1674 participants), Journal Club-28 (1014 participants), In-service Trainingprograms for Ward attendents-1 (19 participants).
Library: This hospital has medical library as well aslibrary for the patients. The medical library hasprocured a good number of books and journals.Library has very good collection of books andjournals. It has nearly 50,000 bound volumes ofbooks and journals. Total no. of books purchasedduring 2008 is 1600 (approx.), Total no. of printjournals is 450, most of it are available in electronicform also. Total no. of e-journals available online isnearly 1800 through ERMED consortia. Apart fromabove library also has nearly 1200 nos. ofdissertation and thesis. Nearly 50 new dissertationand thesis are being added every year.
Major Achievement in Recent Years
Achievement in the Year 2008 -09
� New Medical Library Building, extension ofDe-addiction Block, extension of teachingBlock, Examination Halls, Toilets & BathroomComplex for patients have been completedduring 2008 and the Institute is awaiting totake over these.
� 51 candidates out of total 54 seats were
258
ANNUAL REPORT 2008-09
admitted for the various courses conductedby CIP, Ranchi in the session starting from1st May, 2008
� Bio Chemistry auto analyzer, Coils forMagnetic Stimulator Machine, RadioFrequency identification system for Books &Journals for Medical Library, Digitization ofMedical Records, EEG Records, OfficeRecords, Fiber-Optic networking of theCampus and heavy duty switches for CampusServer have been added to the Institute.
� Installation of 380 KVA DG set, 400 KVAtransformer & underground electric cablingand development of lawns in the hospital.
Clinical & Research
Marked increase in the number of cases attendingOPD, inpatient admission and sharp decline inmortality rates, expansion of community outreachprogramme, increase in the number of researchpaper publication, publication of research journal-Indian Journal of Social Psychiatry (OfficialJournal of Indian Association of Social Psychiatry),increase in the number of students admitted tovarious courses, conversion of microfilms into digitalformats.
Machine, Equipment & Scientific Tools
The following instruments have been procured:
MINOLTA PAGE UP SCANNER
Campus server computer (64 Opteron clusterserver), 16 slices spiral CT scanner, ComputerizedECT system (Thymatron), Multichannel, multimodalitybiofeedback system, Cambridge automatedneuropsychological test battery (CANTAB),
Computerized versions of Luria-Nebraska
Neuropsychological battery (LNNB) & Minnesotamultipurpose personality inventory (MMPI),Computerized biometric attendance system for staff& students, development of a network encompassingall departments, labs, centers & wards along withcustom made software for office automation andclinical use.
Capital Works
List of Construction of new buildings etc. done inrecent years include extension of teaching block,extension of drug de-addiction ward, Radiologybuilding for CT scanner & other equipments, buildingfor Medical Library, 90 nos. Residential quarters,construction of a boundary wall of entire campus ofCIP, repair & widening of roads, Renovation of oldnon-residential buildings (Seven of existing 12wards have been renovated with roof treatment,marble flooring, wall tiles, and renovation of toilet-bathrooms in all the wards. Rest of the buildingsare in process of getting renovated) and Renovationof Men's Hostel & Ladies hostel.
EXTENSION OF SATYANAND TEACHING BLOCK
259
ANNUAL REPORT 2008-09
Budgetary Provision
(Rs. in thousand)
Financial Plan Non-planYear Budget Revised Final Expenditure Budget Revised Final Expenditure
Estimate Estimate Estimate Estimate Estimate Estimate
2008-09 Revenue 70000 72900 69641 69478 131500 192000 191512 190554
Capital 99000 16130 15730 14370 - - - - - - - -
TOTAL 169000 89030 85371 83848 131500 192000 191512 190554
Miscellaneous
Solar energy: Provision of Solar indoor & streetlights, Solar water heating systems in all the wards,solar water pumps etc, Pest Control measures formosquitoes, flies & rates, installation of 380 KVADG set, 400 KVA transformer & undergroundelectric cabling and development of lawns in thehospital.
15.24 Central Research Institute (CRI),Kasauli
Introduction:
Central Research Institute was established on 3rdMay, 1905 as Pasteur Institute for North India It is asubordinate office of Directorate general of HealthServices, under the Ministry of Health & F.W. of India.The institute has a huge complex which divided inseven sub-sections i.e. Establishment, Academic,Auxiliary Facilities, Production Division, QualityControl Division, Animal House and Research &Surveillance Division. It has a network of large oflaboratories engaged in manufacturing vaccines/sera and research activities. The details of thefacilities engaged in manufacturing of the vaccine/sera, other auxiliary, supporting and surveillancefacilities. Central Research Institute is engaged in (i)large scale production of Bacterial and Viral Vaccines& Sera. (ii) Research and Development in the filedof immunology and vaccinology. (iv) Teaching andtraining in vaccinology and Microbiology. (v) QualityControl of immunologicals. Since its inception theinstitute has developed into a premier institute inresearch and production of a numberimmunobiologicals.
Staff Strength: There are 835 sanction posts in CRI-Kasauli. The number of sanction posts of group A,B, C, and D are 50, 34, 229 and 522 respectively.The total staff in-position is 632. The staff in-positionof groups A, B, C and D is 20, 21, 196 and 39564 BIT CLUSTUR SERVER
260
ANNUAL REPORT 2008-09
respectively. Total Vacant posts are 203. The vacantposition of group A, B, C and D are 30, 13, 33 and
127 respectively. Consolidated status of the staff isgiven in the table No.1.
TTTTTable No. 1able No. 1able No. 1able No. 1able No. 1
Group-wise staff position of CRI Kasauli as on March 2008. Group-wise staff position of CRI Kasauli as on March 2008. Group-wise staff position of CRI Kasauli as on March 2008. Group-wise staff position of CRI Kasauli as on March 2008. Group-wise staff position of CRI Kasauli as on March 2008.
S. No. Staff Sanctioned Staff Vacant % Vacanciespositions in-position positions
1 Group-A 50 20 30 60.00
2 Group-B (Gaz) 9 4 5 55.60
3 Group-B(Non-Gaz) 25 17 08 32.00
4 Group-C 229 196 33 14.04
5 Group-D 522 395 127 24.300
TOTAL 835 632 203 24.30
Budget for the year 2008-09: The budget allocationfor 2008-09 is Rs. 2797.00 lakhs (non plan Rs.1797.00 lakhs and Plan Rs. 1000.00 lakhs).
Consolidated allocation of budget 2008-09 is givenin table No. 2.
TTTTTable No. 2able No. 2able No. 2able No. 2able No. 2 (Rs. in Lakh)
Plan Non Plan Total
BE (2008-09) 1000 1797 2797
Expenditure till Sept.08 203 652 855
RE (2008-09) proposed 999.09 2205.90 3204.99
BE (2009-10) 2387.00 3482.67 5869.67
Central Drugs Laboratory: CDL is establishedunder Drugs & Cosmetic Act, 1945 which is lookedafter by one Drug Analyst working under directadministrative control of Director, CRI Kasauli. CDLis accredited by WHO and this laboratory is on theWHO web site for the testing of vaccines, meant forUN Agencies. The activities are as follows.
NCL
At present CDL is the only National ControlLaboratory for the testing & release of variousImmunobiologicals viz. Vaccines, Sera and Bloodproducts in the country. During the period 10190samples of various products have been tested and
released of indigenous and importedimmunobiologicals on protocol /testing basis.
CDL
At present CDL is taking part in testing of Measlesand Protusis proficiency panels. C.D.L. has beendesignated as WHO Global Training Network (GTN)Centre on Vaccine quality since 2006.
Teaching Activities: The Institute has beenrecognized as a Microbiology Department of HimachalPradesh University, Shimla and the Director of theInstitute is recognized as Head of the MicrobiologyDepartment. Under this Department B.Sc./M.Sc.
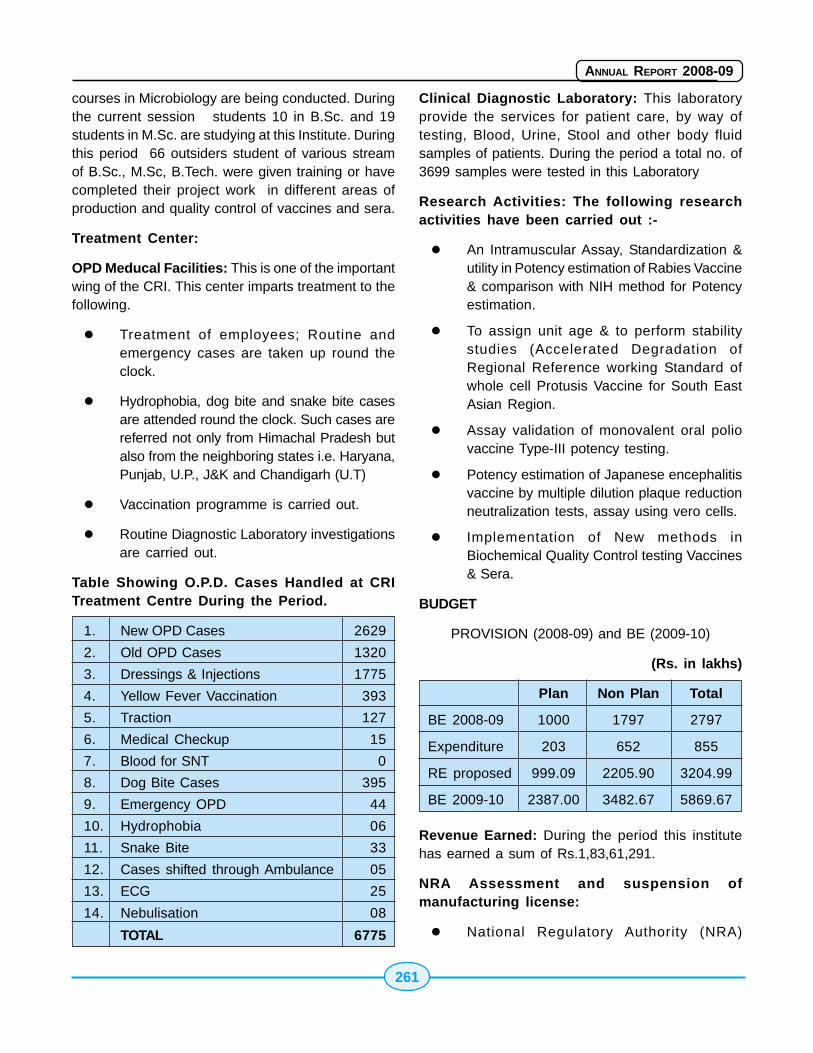
261
ANNUAL REPORT 2008-09
courses in Microbiology are being conducted. Duringthe current session students 10 in B.Sc. and 19students in M.Sc. are studying at this Institute. Duringthis period 66 outsiders student of various streamof B.Sc., M.Sc, B.Tech. were given training or havecompleted their project work in different areas ofproduction and quality control of vaccines and sera.
Treatment Center:
OPD Meducal Facilities: This is one of the importantwing of the CRI. This center imparts treatment to thefollowing.
� Treatment of employees; Routine andemergency cases are taken up round theclock.
� Hydrophobia, dog bite and snake bite casesare attended round the clock. Such cases arereferred not only from Himachal Pradesh butalso from the neighboring states i.e. Haryana,Punjab, U.P., J&K and Chandigarh (U.T)
� Vaccination programme is carried out.
� Routine Diagnostic Laboratory investigationsare carried out.
Table Showing O.P.D. Cases Handled at CRITreatment Centre During the Period.
1. New OPD Cases 2629
2. Old OPD Cases 1320
3. Dressings & Injections 1775
4. Yellow Fever Vaccination 393
5. Traction 127
6. Medical Checkup 15
7. Blood for SNT 0
8. Dog Bite Cases 395
9. Emergency OPD 44
10. Hydrophobia 06
11. Snake Bite 33
12. Cases shifted through Ambulance 05
13. ECG 25
14. Nebulisation 08
TOTAL 6775
Clinical Diagnostic Laboratory: This laboratoryprovide the services for patient care, by way oftesting, Blood, Urine, Stool and other body fluidsamples of patients. During the period a total no. of3699 samples were tested in this Laboratory
Research Activities: The following researchactivities have been carried out :-
� An Intramuscular Assay, Standardization &utility in Potency estimation of Rabies Vaccine& comparison with NIH method for Potencyestimation.
� To assign unit age & to perform stabilitystudies (Accelerated Degradation ofRegional Reference working Standard ofwhole cell Protusis Vaccine for South EastAsian Region.
� Assay validation of monovalent oral poliovaccine Type-III potency testing.
� Potency estimation of Japanese encephalitisvaccine by multiple dilution plaque reductionneutralization tests, assay using vero cells.
� Implementation of New methods inBiochemical Quality Control testing Vaccines& Sera.
BUDGET
PROVISION (2008-09) and BE (2009-10)
(Rs. in lakhs)
Plan Non Plan Total
BE 2008-09 1000 1797 2797
Expenditure 203 652 855
RE proposed 999.09 2205.90 3204.99
BE 2009-10 2387.00 3482.67 5869.67
Revenue Earned: During the period this institutehas earned a sum of Rs.1,83,61,291.
NRA Assessment and suspension ofmanufacturing license:
� National Regulatory Authority (NRA)
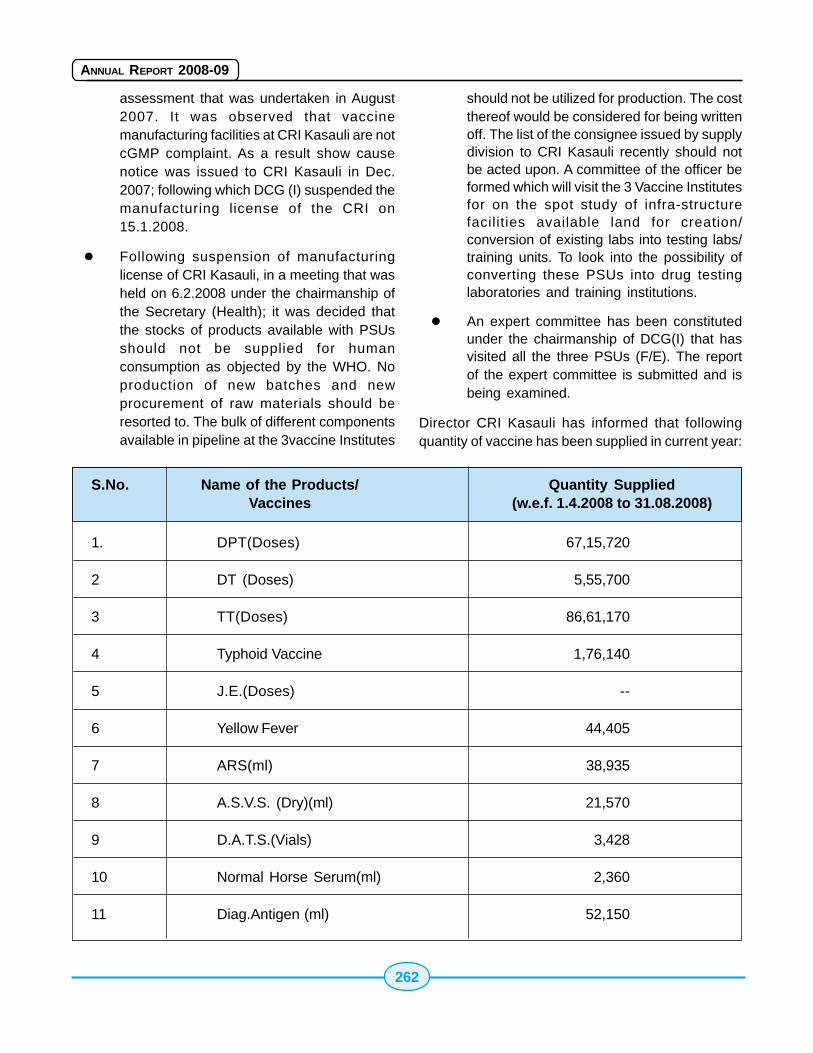
262
ANNUAL REPORT 2008-09
assessment that was undertaken in August2007. It was observed that vaccinemanufacturing facilities at CRI Kasauli are notcGMP complaint. As a result show causenotice was issued to CRI Kasauli in Dec.2007; following which DCG (I) suspended themanufacturing license of the CRI on15.1.2008.
� Following suspension of manufacturinglicense of CRI Kasauli, in a meeting that washeld on 6.2.2008 under the chairmanship ofthe Secretary (Health); it was decided thatthe stocks of products available with PSUsshould not be supplied for humanconsumption as objected by the WHO. Noproduction of new batches and newprocurement of raw materials should beresorted to. The bulk of different componentsavailable in pipeline at the 3vaccine Institutes
should not be utilized for production. The costthereof would be considered for being writtenoff. The list of the consignee issued by supplydivision to CRI Kasauli recently should notbe acted upon. A committee of the officer beformed which will visit the 3 Vaccine Institutesfor on the spot study of infra-structurefacilities available land for creation/conversion of existing labs into testing labs/training units. To look into the possibility ofconverting these PSUs into drug testinglaboratories and training institutions.
� An expert committee has been constitutedunder the chairmanship of DCG(I) that hasvisited all the three PSUs (F/E). The reportof the expert committee is submitted and isbeing examined.
Director CRI Kasauli has informed that followingquantity of vaccine has been supplied in current year:
S.No. Name of the Products/ Quantity SuppliedVaccines (w.e.f. 1.4.2008 to 31.08.2008)
1. DPT(Doses) 67,15,720
2 DT (Doses) 5,55,700
3 TT(Doses) 86,61,170
4 Typhoid Vaccine 1,76,140
5 J.E.(Doses) --
6 Yellow Fever 44,405
7 ARS(ml) 38,935
8 A.S.V.S. (Dry)(ml) 21,570
9 D.A.T.S.(Vials) 3,428
10 Normal Horse Serum(ml) 2,360
11 Diag.Antigen (ml) 52,150
263
ANNUAL REPORT 2008-09
15.26 V15.26 V15.26 V15.26 V15.26 Vallabhbhai Pallabhbhai Pallabhbhai Pallabhbhai Pallabhbhai Patel Chestatel Chestatel Chestatel Chestatel ChestInstitute(Institute(Institute(Institute(Institute(VPCIVPCIVPCIVPCIVPCI), University of), University of), University of), University of), University ofDelhiDelhiDelhiDelhiDelhi
Brief Background
The Vallabhbhai Patel Chest Institute (VPCI), amaintained institution of University of Delhi underordinance XX (ii) administered by a Governing Bodyconstituted by Executive Council of the University iswholly financed by Grant in Aid from the Ministry ofHealth and Family Welfare, Government of India. Thefoundation stone of the Institute was laid by SardarVallabhbhai Patel on 6th April 1949. The Institute wasformally opened by Rajkumari Amrit Kaur, the thenUnion Minister of Health on 12th January 1953.. DrR Vishwanathan was appointed the first Director ofVPCI. Dr Rajendra Prasad, the then President of Indiainaugurated the Clinical Research Centre (renamedas Viswanathan Chest Hospital) attached to theInstitute on 24th October 1957. The regularGoverning Body was constituted by the ExecutiveCouncil of the University of Delhi for the managementand administration of the Institute on January 21st1955.
Main Objectives:
The main objectives of the Institute are to trainpostgraduate students in Pulmonary Medicine,Biochemistry, Microbiology, Pharmacology andPhysiology, to provide specialized diagnostic andtreatment services to patients suffering from chestdiseases and to conduct research in basic and clinicalsciences related to chest medicine and alliedsciences.
I - Patient Management services
A state of the art 8 bedded Intensive Care Unit (I.C.U)provided services to patients regularly since 10thJanuary 2006. A total of 53257 patients were treatedin the OPD of the Raman Vishwanathan Hospital wingof this Institute. 1837 patients were admitted asindoor cases. The 24 hour Respiratory Emergencyservice which started in the year 2000 has renderedservices to 18090 patients and 385 patients wereprovided ventilatory (invasive and non-invasive)
treatment in ICU during 2007-08. Specialized serviceswere rendered to 92 patients with sleep disorders.Total number of major investigations done were asfollows: pulmonary function tests (PFT) 19251,bronchscopy 186, brochoalveolar lavage 94, X rays17145, arterial blood gases 3502, Ultrasonogram(USG) examinations 408, CT scans and CT guidedFNAC 2120. Immunodiagnostic tests for HIV wereconducted on 103 occasions. Other diagnosticservices provided to patients were haemotologicaltests 36677, urine and microscopic examinations9223, allergy/skin tests 773, sputum examinationsfor acid fast bacilli (AFB) 6740, clinical biochemistry13943, cardiopulmonary exercise testing 86,Mycological investigations 941, Histopathology155,Cytology 788 and Flow Cytometric tests 1070,HBs Ag tests 7 and other pathogens 2713,Electrocardiogram 4474.
Research activities
Notable contributions during the year on researchinclude development of novel therapeutics basedupon natural products from Indian medicinal plants.Assessment of the effects of high particulatepollutants on pulmonary health status in selectedmega-cities of South Asia. Environmental prevalenceof Cryptococcus neoformans, its mycoserologic andgenotypic characterization and role in pulmonaryinfections and prospects for the development of anti-tubercular drugs based on transacetylase functionof glutamine synthase. A study to assess the efficacyof UNIM-352 (ZN5) in bronchial asthman wascontinued. Other studies undertaken areresponsiveness of airway rapidly adapting receptorsto cigarette smoke inhalation in normal and sensitizedrabbits, real time PCR based on rapid detection ofMycobacterium tuberculosis from peripheral bloodsamples, a comparative study of breath CO level ofpassive smokers , multisite monitoring of humaninfluenza in India- Phase I and a study of viralreplication inhibition by down regulation of NS1 geneof influenza virus.
II - Post Graduate Teaching and training
A total of 9 MD students for academic year 2007-10and 10 DTCD students for academic year 2007-09
264
ANNUAL REPORT 2008-09
were enrolled. In addition, 28 students were giventraining under the MD and DTCD programmes.Twenty research scholars pursued their PhDprogrammes.
As part of imparting updated knowledge regardingvarious progress in respiratory diseases, the Institutehad conducted 7th CME course entitled, "RecentAdvances in Bronchial Asthma" on May 06,2007 andthe Delhi Medical Council had accredited the course.
Tobacco Cessation Clinic (TCC)
Since the inception of anti smoking clinic in 2001,the smoking cessation intervention had been doneby intensive patient education, counseling andpharmacotherapy in a scientific manner. A total of761 new cases and 208 old cases were followed upat TCC during 2007-08. As compared to 2006-07,there has been a rise in the number of patients. Newcases jumped to nearly 42% and old cases follow uprose by 92%. This shows a much higher rate increation of awareness for tobacco related cessationactivities leading to increased health advantages. Aworkshop on Tobacco Free Environment, Delhi washeld on August 29th 2007.
Cardio-Pulmonary Rehabilitation
A Cardio-Pulmonary Rehabilitation facility was startedon 18th January 2007 for comprehensive pulmonaryrehabilitation of patients suffering from ChronicRespiratory diseases.
Conferences / Workshops conducted
A national symposium on "Lung Pathology" on theeve of 58th Foundation Day celebrations wasconducted on 5th April 2007.
The 9th "Prof R.Vishwanathan - VPCI oration" washeld on 6th April 2007. The oration was delivered byProf K.K Talwar, Director, P.G.I.M.E.R , Chandigarh onthe topic titled "Heart Failures- Options and Hopes"
The 3rd Prof A.S Paintal Memorial Oration was heldon 24th September 2007. The Oration was deliveredby Prof P.N Srivastava former Vice-Chancellor, J.N.U,New Delhi on the topic titled, "Quality of IndianScience: Complacency We Suffered With"
The 41st Annual Conference of the Indian Collegeof Allergy, Asthma and Applied Immunology"ICAAICON-2007" was organized by VPCI from 09thDecember to 12th December 2007.
Publication
The Institute continues to expand the aims andprogrammes and disseminates recent advances inchest medicine by publishing the "The Indian Journalof Chest Diseases and Allied Sciences" on quarterlybasis and this journal is also available online at thewebsite address http://www.vpci.org.in. A specialGolden Jubilee volume of Indian Journal of ChestDiseases and Allied Sciences was published in 2008.Further 55 research papers authored by Institute'sfaculty members were published in distinguishednational and international journals and bookchapters.
Budget during the year
Plan Rs 7.00 crores
Non Plan Rs 11.00 crores
Infrastructure Development
As part of continuing efforts in upgrading andmodernization of the Institute, various equipmentsrelating to patient care, research and developmentwere procured. The equipments purchased are asfollows. Biomemory freezer, micro 5000 spirometrysystem, automated hematology analyzer, plateletaggregation profiler, ice flaking machines,microscope, bench top high speed centrifuge,RESMED reslink system, capno check sleepcapnograph, microstream CO2 module for spectrummonitors, refrigerated molecular incubators,transilluminator etc. Renovation/upgradation wascompleted in the hospital wing and external façadeof the hospital buildings.
15.27 Central Bureau of Health15.27 Central Bureau of Health15.27 Central Bureau of Health15.27 Central Bureau of Health15.27 Central Bureau of HealthIntelligence (Intelligence (Intelligence (Intelligence (Intelligence (CBHICBHICBHICBHICBHI)))))
Established in 1961, CBHI is the National NodalInstitution for Health Intelligence in the country withthe broad objectives to: -
265
ANNUAL REPORT 2008-09
� Maintain and Disseminate the Data on (i)National Health Profile of India, (ii) HealthSector Policy Reform Options Database (HS-PROD), (iii) Inventory & GIS Mapping ofGovernment Health Facilities in India, etc and
� Facilitate Capacity Building & HumanResource Development, and
� Need Based Operational Research forEfficient Health Information System (HIS) andFamily of International Classification ofmorbidity, mortality, functions / disability andhealth interventions. (ICD10, ICF & ICHI).
Organization.
� In Dte. GHS / GOI, the CBHI headed byDeputy Director General as its Director, hasfour divisions viz. (i) Policy & Infrastructure,(ii) Training, Collaboration & Research, (iii)Information & Evaluation, and (iv)Administrative.
� Six Health Information Field Survey Units(FSUs) of CBHI are located in differentRegional Offices of Health and FamilyWelfare (ROHFW) of GOI at Bangalore,Bhopal, Bhubaneswar, Jaipur, Lucknow &Patna; each headed by a Dy. Director withTechnical & Support staff, who function underthe supervision of Sr./Regional Director(HFW/GOI).
� Regional Health Statistics Training Centre(RHSTC) of CBHI at Mohali, Punjab (nearChandigarh) and Other Training Centres viz.(i & ii) Medical Record Department & TrainingCentre of Safdarjung Hospital, New Delhi andJIPMER Puducherry; conduct CBHI InserviceTraining Courses.
MAJOR ACTIVITIES OF CBHI.
Maintain and Disseminate the National HealthProfile of India on-
Demography
� Population Statistics
� Vital Statistics
Socio-Economic
� Education
� Social Indicators
� Economic Indicators
� Employment
� Housing & Amenities
� Drinking water & Sanitation
� Health Legislation in India
� Survey on Morbidity, Health Care AndCondition of the Aged.
Health Status
� Morbidity & Mortality
i. Communicable Diseases
ii. Non Communicable Diseases
� Incidents of Deaths due to Accidents
� Major Outbreaks Investigated by NICD
� Reproductive & Child Health
� Disability
� Coverage for Mass Administration forLymphatic Filariasis
Health Finance
� Five Year Plan Outlays
� Health Expenditure & Financing Agents
Human Resources in Health Sector, including AYUSH
Health Infrastructure, including AYUSH
� Education Infrastructure (Medical, Nursing &Paramedical)
� Service Infrastructure
� Vaccine-wise and Institution-wise status ofproduction, demand and supply
� Directory of Health Research Institution inIndia

266
ANNUAL REPORT 2008-09
Health Sector Policy Reform Option Database(HS-PROD) of India.
Though States / UTs of India have undertaken reformsin the health sector, a lot of this goes unnoticed andhence not documented. Thus, MOHFW/ GOI underits Sector Investment Programme funded byEuropean Commission, entrusted CBHI to developand maintain HS-PROD. It is a web-enabled databasethat documents and further creates a platformfor sharing of information on good practices,innovations in health services management whilealso highlighting their failures that are very importantfor the success of NRHM. The HS-PROD website(www.hsprodindia.nic.in) till date has documentedmore than 260 reform options from a varied rangeof fields and stakeholders like the State / UTgovernments, development partners, NGOs andcategorized them under 16 subject areas. A nationaldissemination workshop was organized by CBHI on23rd March 2007, which was inaugurated by UnionSecretary (HFW). CBHI solicits information on suchreforms from state / UT governments, HealthProgramme Managers, Researchers, Teachers andPublic Health Institutions in order to regularly updatethis national database. Sense of ownership and prideis to be taken in an effort like HS-PROD by all publichealth professionals.
In order to continuously capture information on goodpractices, renovations and reforms know how totackle common management problems in the healthsector, CBHI proposed to continue this activity.
Inventory & GIS Mapping of Government HealthFacilities in India:
For creation of an electronic database of governmenthealth facilities, educational institutions, trainingcenters, and other health care establishments inIndia, CBHI has prepared a database of the Govt.health facilities for their mapping using GeographicalInformation System (GIS) for its wider disseminationthrough the CBHI website. It is an ICT based approachto strengthen the health care resources managementand planning for efficient health services delivery asenvisaged under NRHM. Data has been collectedfrom all the 35 States/UTs from the periphery and
other source agencies including Statutory Councilsand GIS mapping of the Govt. health facilitiesuploaded on the national website www.cbhighf.nic.induring February 2008. All the States/UTs now havealso been requested to validate as well as updatethe Govt. health facilities online. Once the updationis done, the GIS view will be opened for web surfer'saccess for public.
Millennium Development Goals.
The Millennium Declaration adopted by the GeneralAssembly of the United Nations in its Fifty-fifth sessionduring September 2000 reaffirmed its commitmentto the right to development, peace, security andgender equality, to the eradication of manydimensions of poverty and to overall sustainabledevelopment. These are intended for the MemberCountries to take efforts in the fight against poverty,illiteracy, hunger, lack of education, gender inequality,infant and maternal mortality, diseases andenvironmental degradation. The MillenniumDeclaration adopted 8 development goals, 18 time-bound targets and 48 indicators to be achieved by2015, of which 3 MDGs are directly related to healthsector viz. reduce child mortality, improve maternalhealth and combat HIV/ AIDS, malaria and otherdiseases; for which CBHI is responsible forcompilation in Dte.GHS/MOHFW/GOI.
Trained Manpower Development.
CBHI conducted / initiated following in service nationaltraining courses during 2008-09 (details are availablein CBHI website): viz. four batches of Medical RecordTechnicians (6 months), two batches of MedicalRecord Officers (12 months), fourteen OrientationCourses on Health Statistics for Non-MedicalPersonnel (5 days), two Orientation Courses onHealth Statistics for Medical Officers (5 days),fourteen Orientation Courses on ICD 10 for Non-medical personnel (5 days) and two Workshops ofState / district level coordinator for training onMorbidity and Mortality Coding Using ICD 10 for tenNRHM States (3 days); through CBHI TrainingCentres situated at Safdarjung Hospital, New Delhi,JIPMER, Puducherry, RHSTC / CBHI, Mohali and
267
ANNUAL REPORT 2008-09
CBHI FSUs at Bangalore, Bhopal, Bhubaneswar,Jaipur, Lucknow, Patna.
During 2007-08, 523 Personnel were trained invarious courses and in 2008-09 more than 540personnel are expected to be trained through variousCBHI In service Training Courses.
Capacity Building, Operational Research &Reviews.
CBHI FSUs located in Regional Offices of Health &FW/GOI at Bangalore, Bhubaneswar, Bhopal, Jaipur,Lucknow and Patna help CBHI in getting thevalidated health information from States/UTs andfacilitate in capacity building of health care deliveryfunctionaries as well as operational research keepingin view the objectives of CBHI. The CBHI regularlyundertakes half yearly meetings to review functioningof all the FSUs and Training Centres and during2008-09, these meetings were held on 15th February2008 at Nirman Bhawan, New Delhi and 12-13August 2008 at ROHFW/ Bengaluru.
WHO Collaborating Centre on Family ofInternational Classification (FIC) of diseases,mortality, related health aspects and function /disabilities as well as health interventions (ICD,ICF & ICHI) at CBHI:
CBHI Dte.GHS/MOHFW, GOI has been now (Sept.,2008) officially declared to function as "WHOCollaborating Centre on FIC (ICD, ICF & ICHI)"for coding morbidities, mortality, related healthaspects, function and disabilities as well as healthinterventions in India as well as South East AsiaRegion and also, linking with Asia Pacific network onFIC.
CBHI organised &/or co-hosted following threeevents with respect to FIC: -
� A National Workshop on designing theStrategy for advocacy and implementation ofICF in the Country, 21-22 August 2008, NewDelhi,
� WHO - FIC Network Annual Meeting, 25 - 31October 2008 at The Heritage Village,Manesar, Gurgoan/NCR, Delhi.
� WHO Meeting on Public Health Informatics,3-4 November 2008, Manesar, Gurgoan/NCR, Delhi.
Maintenance of CBHI National web sites.
Presently CBHI with the assistance of NIC, hasredesigned & reformatted its three websites viz.(i) www.cbhidghs.nic.in (ii) www.hsprodindia.nic.in(iii) www.cbhighf.nic.in, for online data transmission.
� CBHI website www.cbhidghs.nic.in containsgeneral information about CBHI, NationalHealth Profile, Mortality Statistics in India(2006), Right to Information Act, NationalRecommendations on improving andstrengthening Health Information System, aswell as use of ICD 10 in country, CBHI casestudy & recommendations on human healthresource requirement, CBHI in-servicetraining programmes/ calendar along withapplication forms, Module & Work Book onICD 10, Reporting formats for health datafrom States/UTs to CBHI, etc.,
� CBHI is also maintaining a Websitewww.hsprodindia.nic.in containing entriesrelated to Health Sector Policy Reform DataBase of India and being updated from timeto time.
� CBHI's third website www.cbhighf.nic.incontaining inventory & GIS mapping of theGovt. health facilities, was launched byDGHS/GOI in February 2008.
Publications of CBHI - brought out during 2008.
(i) Annual Publication 'National Health Profileof India-2007',
(ii) Managing Human Resources for Health inIndia 2007- A case study of Madhya Pradesh& Gujarat,
(iii) India Country Profile on Road Safety forWHO's Global Road Safety Report, 2008.
Participation & Contributions made by CBHIOfficers in the International Meeting during2008.
(i) Sh. Nand Lal, Joint Director (NFSG)-CBHI, in
268
ANNUAL REPORT 2008-09
(a) "First Conference of the InternationalFederation of Health Records Organisation(IFHRO), 21-23 October, 2008 " Denpasar,Bali, Indonesia", (b) "Annual Meeting ofWHO-FIC Network, 25-31 October 2008,Manesar, India".
(ii) Dr. Ashok Kumar, Dy.DG & Director CBHI -Annual Meeting of WHO-FIC Network, 25-31October 2008, Manesar, India.
(iii) Dr. Ashok Kumar, - WHO/International Meetingon Public Health Informations, 3-4 November2008, Manesar, India.
(iv) Mr. Biswajit Das, Joint Director, CBHI- WHO/International Meeting on Public HealthInformations, 3-4 November 2008, Manesar,India.
Special Projects under WHO/GOI CollaborativeActivities, Biennium 2008-2009:
Development of District Action Plan for EfficientHIS.
In order to ensure an improved and effective HealthInformation System, CBHI had already held fourregional workshops with the States/UTs for improvingand strengthening the Health Information System,the combined report & recommendations of whichhave been communicated to all the State/UT healthauthorities and conducted three workshops to reviewstates/UT specific action plan for improving the HIS.This review necessitates the development a districtlevel action plan for efficient HIS by the States/UTs.Hence, in continuation to earlier years, during thecurrent biennium action was taken to facilitate thedevelopment of district action plan in Bihar, Orissa,Madhya Pradesh & Uttar Pradesh where theimplementation of HIS needs to be furtherstrengthened.
CBHI - On Line Data Entry System throughwebsite www.cbhidghs.nic.in.
State/UT HFW directorates are responsible forpunctually and regularly furnishing the (i) WeeklyEpidemiological Report on Cholera/Plague, (ii)Monthly Communicable Diseases (iii) Monthly Non-
Communicable Diseases, and (iv) Annual Data onMedical/Nursing/Para-Medical education &infrastructure in the prescribed formats to CBHI/Dte.GHS. Based on this information from all theStates/UTs and other reporting agencies, CBHI isrequired to weekly send Country's updatedinformation on Cholera to WHO under theInternational Health Regulation and provide up-to-date data related to morbidity & medical/healthinfrastructure for framing reply to the ParliamentQuestions. CBHI also brings out annual publication
"National Health Profile" which serves as NationalReference Document for policy, planning andevaluation of health related activities in the country.The above requisite health information are being sentby the States / UTs through post /e-mail and at mostinstances delays are experienced. CBHI thus feltthe need for web based data entry system andaccordingly in consultation with NIC has developedan online data entry system for regular and timelyupdated information flow from States / UTs. A NationalWorkshop of States/UTs HIS Nodal Officers on "OnLine Data Entry through CBHI Website for NHP, HS-PROD and GIS Mapping of Government Facilities inIndia was held on 13-14 February 2008 and handon training was imparted to the participants of States/UTs.
A number of States/UTs has started sending data toCBHI through this on line data transmission system.
Study on Human Resource Requirement forHealth in India.
In order to understand the gaps in health work forceand to plan for capacity building and HumanResource Development for filling the gaps as hasbeen envisaged to achieve the objective of NRHM,CBHI undertook the study on Human Resourcerequirement for Health in India is undertaken, during2007, while involving a consultant of agency "AdventHealth Care Group". This study involved primary datacollection from States, Districts and Sub District levelson different health human resources in Govt. sectorat primary and secondary levels as two States ofMadhya Pradesh & Gujarat.
The objectives are to appropriately look at human

269
ANNUAL REPORT 2008-09
resource requirements in the short and long run. Thestudy also includes an analysis of recruitmentprocess permanent & contractual; mechanismadopted in the planning for recruitment process andfilling up the vacancies, performance parameters,rewards system etc. The study report has beenreleased in early 2008.
Multicentric study to Improve and StrengthenEfficient Electronic flow of Health Informationfrom periphery to CBHI with Public PrivatePartnership.
CBHI collects health data from all 35 States/UTs,States/UTs in turn collect data from the districts andthe districts from grass root (peripheral) levelestablishments. Data transmission by usual postalmode takes lot of time. In order to avoid delay intransmission of data, it is required to improve andstrengthen the electronic flow of Health Informationfrom periphery to up levels. In this direction, aplanned study has been conducted by CBHI in theselected States/UTs where efforts have been pilotedfor an efficient system of Electronic Flow of HealthInformation and based on this studyrecommendations and suggestions are being workedout for an Efficient Electronic Flow of HealthInformation System from periphery to above level,while involving Public Private Partnership forcomplete data.
Review Study to Improvise Health ManagementUnder Primary Health Care System in India.
To assess the present status of Health InformationSystem (HIS) under Primary Health Care, CBHI hasformed Multi-Centric Research Team of its officersfrom its all the six Field Survey Units (FSU) situatedat ROHFWs Bengaluru, Bhopal, Bhubaneswar,Jaipur, Lucknow and Patna. The objectives of thestudy are (i) to assess the present status of HealthInformation System (HIS) under Primary HealthCare;(ii) define the Essential Health Indicators andHealth Information those need to be compiled atHealth Sub-Center, PHC, CHC and District level;(iii)designing appropriate minimal records and reportsto be maintained at Health Sub-center, PHC, CHCand District levels and (iv) to recommend an
improvised operationally feasible & cost-effectivemechanism of information flow, its analysis,interpretation and feedback under Primary HealthCare System in India. The system is underprogress.
Millennium Development Goals related to HealthSector.
A workshop to Review and Strengthen National andSub national Information System for MillenniumDevelopment Goals related to Health Sector was heldon 23rd May 2008 at Nirman Bhawan, New Delhi,under Chairmanship of DGHS/GOI.
Budget.
CBHI under this budget head "Health Informationand Monitoring System" has been allocated anamount of Rs.240.00 lakhs in plan and Rs.90.00lakhs in non-plan for the financial year 2008-09.
15.2815.2815.2815.2815.28 North Eastern Indira GandhiNorth Eastern Indira GandhiNorth Eastern Indira GandhiNorth Eastern Indira GandhiNorth Eastern Indira GandhiRegional Institute of Health andRegional Institute of Health andRegional Institute of Health andRegional Institute of Health andRegional Institute of Health andMedical Sciences (Medical Sciences (Medical Sciences (Medical Sciences (Medical Sciences (NEIGRIHMSNEIGRIHMSNEIGRIHMSNEIGRIHMSNEIGRIHMS),),),),),ShillongShillongShillongShillongShillong
North Eastern Indira Gandhi Regional Institute ofHealth and Medical Sciences (NEIGRIHMS) hasrecently been established in Shillong, on the lines ofAIIMS, New Delhi, and PGIMER, Chandigarh, with theobjective of providing advanced specialized Health-care to the people of North East Region. So farCentral Government has made an investment ofabout Rs. 400 Crore for development of the Institute.An amount of Rs. 1266.38 crore has been allocatedfor the Institute in the 11th Plan. This Institute isplanned for a 500 bed referral hospital with 35teaching department at post graduate level in variousspecialties and super-specialties. A 50 seats NursingCollege and under graduate MBBS College hasalready started functioning from the Institute. Duringthe year 2008-09, Rs. 60.28 Crore has beenallocated to the Institute, while Rs. 59.00 Crore hasbeen released. A Regional Cancer Center, expansionof the Nursing College and creation of additionalfacilities for the Medical College are planned for theInstitute.

270
ANNUAL REPORT 2008-09
15.2915.2915.2915.2915.29 National Institute of BiologialsNational Institute of BiologialsNational Institute of BiologialsNational Institute of BiologialsNational Institute of Biologials(((((NIBNIBNIBNIBNIB), Noida), Noida), Noida), Noida), Noida
The Ministry of Health & Family Welfare (MOHFW)has established the National Institute of Biologicals(NIB) as an apex scientific Institution in the country toact as a National Control Laboratory (NCL) for assuringthe availability of high standards and good quality ofbiological product i.e. vaccines, anti-sera, anti-toxins,blood products, recombinant DNA products, reagents,immunodiagnostic kits etc. that are either indigenouslymanufactured within the country or for exports andthose imported into the country.
The Revised Project of Rs.269.24 crore wasapproved by the CCEA in February, 2001. The MainLab & Animal House facility has become fullyfunctional and the Labs are being operationalized.
NIB has the following facilities:-
� Main Lab & Animal House : The work ofconstruction of this main building wasawarded to M/s L&T on 27.02.2003 throughM/s. HSCC who were the official consultantsto the project.
� The Maintenance Engineering Building,essential Staff Quarters and Gate House havebeen completed. These ancillary buildingsare being utilized.
� Administration Block, Cafeteria, Hostel andGuest House are in use.
� Utility infrastructural facilities and ExternalServices (Civil and Electrical) taken overearlier are also under regular use.
� This building was taken over on 21.05.07.Formal inauguration shall be made during 08-09.
For the financial year 2007-08 BE and RE provisionfor the Institute was Rs.22.65 crore and Rs.22.65crore respectively. However, during the year grantof Rs.11.32 Crore was released. The totalexpenditure incurred was calculated to be Rs.9.70crore while the revenue generation during the yearwas Rs.63.61 Lac.
Scientific Report
Blood Reagent Laboratory
Testing of blood Reagents at NIB has been notifiedby Government of India for quality control testing andbatch release certification. The Institute certifies thequality of reagents like Anti-A, Anti-B and Anti-RhDetc. for increasing the safety in blood transfusionbesides dealing with legal samples referred by DrugInspectors have been tested. Samples of differentbatches of blood grouping reagents imported to thecountry or manufactured indigenously are beingreferred by port officer and Drug Inspectors. Duringthe financial year 2007-08 NIB has received 55batches and 41 batches tested and reported of bloodgrouping reagents. For expansion of works, cell andsera panel for rare blood groups have been initiated.
Immunodiagnostic Kit Laboratory
Since 1997, NIB has been doing quality controlevaluation of critical immunodiagnostic kits detectingantibodies of HIV, HCV and HBsAg. The mainfunctions of the diagnostic division are to certify thequality of such diagnostic kits for increasing safetyof blood from the viral diseases at blood banks. Thetypes of kits evaluated were belonging to ELISA, rapid,confirmatory and automated kits etc. These kits areeither indigenously manufactured or imported, andreferred by the port officers and CDSCO offices ofDCG (I). Immunodiagnostic kits of HIV-Ab, HCV-Aband HBsAg, Rapid, ELISA and confirmatory werereceived. These were evaluated as per StandardOperating Procedure prepared based on theguidelines of WHO. The parameters / characteristicslike sensitivity, specificity etc were calculated afterusing indigenously prepared reference panelcharacterized for each type of diagnostic kits. In anongoing exercise expansion of sera panels are inprogress. Newer kits like-syphillis and Tuberculosisare under standardization.
Virology Laboratory :
Quality Control Testing Of Oral Polio Vaccine :
NIB has been identified as a center to test the FieldSamples of Oral Polio Vaccines (OPV) from the states

271
ANNUAL REPORT 2008-09
of Uttar Pradesh, Rajasthan, Madhya Pradesh andGujarat in the year 2003. The laboratory has sincebeen regularly receiving OPV field samples fromvarious districts of Uttar Pradesh, which were testedfor their individual polio virus content (Type 1,2&3)and the toral virus content (TOPV) as per IndianPharmacopoeia 1996. A total of 418 samples of OPVwere received during the year and 126 samples weretested and reported to the Deputy Commissioner &Coordinator, National Immunization Programme,Department of Family Welfare, Ministry of Health &Family Welfare, Nirman Bhawan, New Delhi. Furthertesting of OPV from the field was discontinued fromDecember-2005 as a policy decision of theGovernment of India. The laboratory is ready fortesting and batch release certification of Polio andMMR Vaccine.
Blood Products Laboratory
The laboratory has tested human biological productsviz blood products, human albumin, normal andspecific immunoglobulin, coagulation factors. TheQC tests performed on these products are doubleimmuno-diffusion, pH, potency, protein percentage,infection testing of HIV-Ab, HCV-Ab and HBsAg.Other recommended tests like Anti-A and Anti-Bhaemagglutinin titre, estimation of sodium andpotassium ions, as well as haem content etc. areperformed as per IP requirement.
Laboratories which have become functionalduring the year 07-08
Bacterial Vaccine Laboratory : The laboratory wasproposed to be established in order to augment thevaccine Division by initiating the quality control testingof bacterial vaccines for pre-release batchcertification. The laboratory started functioning inJanuary 2006 for undertaking Quality Control ofbacterial polysaccharide vaccine viz; Haemophilusinfluenzae type b vaccine, Meningococcal vaccine,Pneumococcal vaccine & Vi Polysaccharide Typhoidvaccine. Quality Control testing of B.C.G. and othervaccine has been initiated.
Reference Standards Laboratory :
The laboratory has been set up for in-house
preparation of national reference standards for seedstrains and serum panels of pathogens. Efforts arebeing made to develop well characterized SerumPanels/ Reference of tuberculosis, HIV, HBV, HCVetc. Characterization and cryopreservation of variouscell lines used in production and quality control ofviral vaccine is also proposed to be taken up.
Recombinant Product Laboratory : In concurrencewith the mandates of the institute to ensure safetyand quality of biomedicine the laboratory prioritizedthe recombinant preventive and therapeutics whoseproducts are also manufactured by the Indianmanufacturer. The products in priority are i) Insulin,ii) Inerferon and iii) Erythropoitetin.
Thirteen batches of rh-Insulin received frommanufacturer M/s Wockhardt Ltd., Aurangabad andwere tested for standardization of the Quality controlparameters in accordance with the Pharmacopoeiaspecifications given in EP (2005) and USP (2004).The laboratory is near completion of Standardizationand validation of testings required for insulin andbatch release will be taken up from the next year2008-09.
Nucleic Acid Testing Laboratory: Nucleic AcidTesting laboratory was set up with the main objectiveof the lab being to ensure the quality of DNA/RNA-based diagnostic kits before being released in themarket.
Enzymes and Hormones Laboratory : Thislaboratory is being set up to evaluate the qualitycontrol testing of enzymes and hormones.Sreptokinase testing as per IP have been initiated.
Animal Facility
The Animal House Facility which was registered withCPCSEA in August-2004 to perform QC testing onBiologicals like vaccines, blood products &recombinant therapeutics. At present outbred strainsof mice (Swiss albino) and guinea pigs (Duncan-Hartlley) are being maintained. The newer facilityhas planned to acquire seed stock of inbredcharacterized rodents e.g. mice, rats, hamster,guinea pigs and lagomorphs e.g. rabbits fromNational and International sources. A high capacity
272
ANNUAL REPORT 2008-09
incinerator to discard biohazardous waste such asdead animals has been set up. As animalexperiments are crucial in meeting NIB's qualitycontrol objectives, every care is taken to preservethe clean and sterile environment of the animal houseand to ensure good animal health. The animal houseis well maintained with facilities like changing rooms,washing areas, sterilization room diurnal switch andrepeated temperature monitoring. NIB was inspectedby DCG(I)'s expert team constituted by DGHS fornotification as CDL on 7th & 8th December, 2007.
BUDGET:
The BE for 2008-09 is Rs.10.00 crores.
15.3015.3015.3015.3015.30 BCGBCGBCGBCGBCG V V V V Vaccine Laboratoryaccine Laboratoryaccine Laboratoryaccine Laboratoryaccine Laboratory,,,,,(((((BCGVLBCGVLBCGVLBCGVLBCGVL) Guindy) Guindy) Guindy) Guindy) Guindy
BCG VL Guindy is a sub-ordinate office of theDirectorate General of Health Services (DGHS) underthe Ministry of Health and Family Welfare of theGovernment of India, situated at Guindy, Chennai(Tamilnadu) near King Institute of PreventiveMedicine. The major activities of the institute are asbelow:
� Production of BCG Vaccine (10 doses) forcontrol of childhood Tuberculosis and supply
to Expanded Programme of Immunization(EPI)
� Production of BCG Therapeutic (40 mg) foruse in Chemotherapy of Carcinoma UrinaryBalder
� To act as National Control Authority (NCA)for the BCG Vaccine to be imported to Indiaand manufactured by the private firms.
Organization
The institute has a huge complex which is dividedin five major sub-sections i.e. Establishment,Production Division, Quality Control Division, AnimalHouse and Warehousing & Marketing. The othermajor facilities are Containerization, sterilization,Physical inspection.
Staff Strength
The total sanctioned staff strength is 181 and thestaff in-position is 132. The vacant posts are 49(27.00%). Most of the vacant positions are oftechnical staff i.e. Jr. technical officer, Asstt.Technical Officer and refrigeration Engineer. Thegroup wise staff sanctioned and in position is givenin table 2.
TTTTTable No. 2able No. 2able No. 2able No. 2able No. 2
Group-wise staff position of BCG VL Guindy as on March 2008.Group-wise staff position of BCG VL Guindy as on March 2008.Group-wise staff position of BCG VL Guindy as on March 2008.Group-wise staff position of BCG VL Guindy as on March 2008.Group-wise staff position of BCG VL Guindy as on March 2008.
S. No. Staff Sanctioned Staff Vacant % Vacanciespositions in-position positions
1 Group-A 03 02 01 33.3
2 Group-B (Gaz) 04 01 03 75.00
3 Group-B(Non-Gaz) 08 01 07 87.5
4 Group-C 88 74 14 15.9
5 Group-D 78 54 24 30.8
TOTAL 181 132 49 27.6
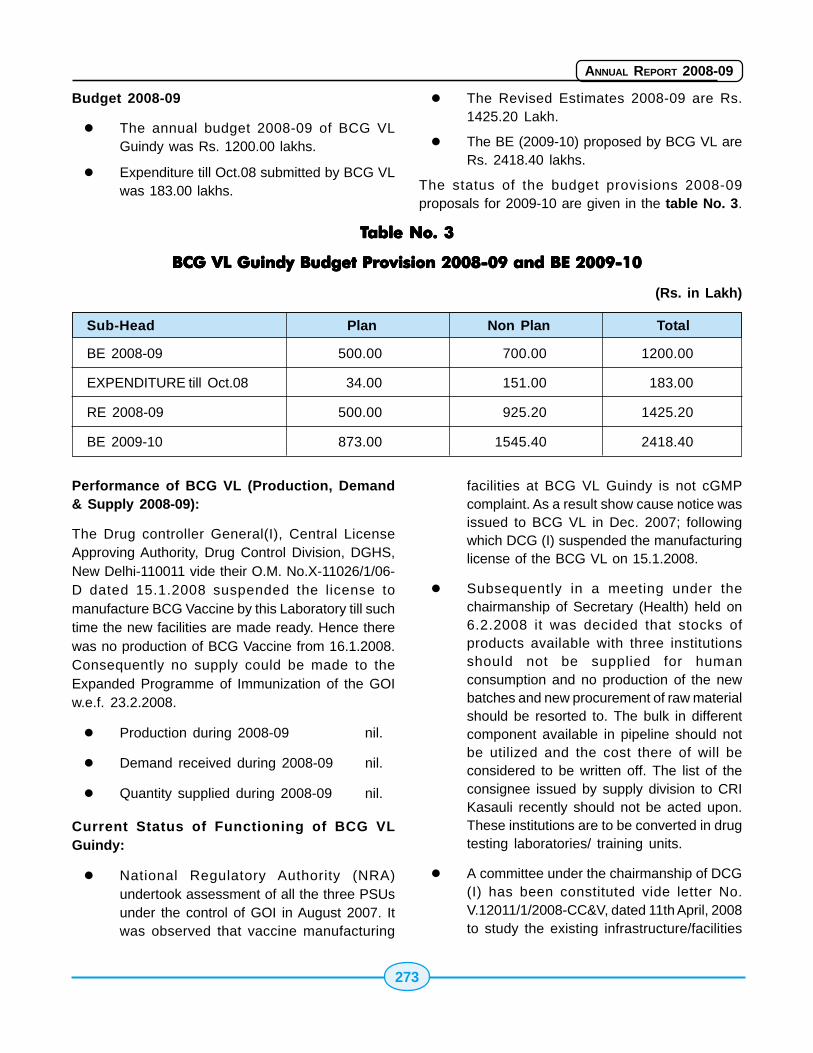
273
ANNUAL REPORT 2008-09
Budget 2008-09
� The annual budget 2008-09 of BCG VLGuindy was Rs. 1200.00 lakhs.
� Expenditure till Oct.08 submitted by BCG VLwas 183.00 lakhs.
� The Revised Estimates 2008-09 are Rs.1425.20 Lakh.
� The BE (2009-10) proposed by BCG VL areRs. 2418.40 lakhs.
The status of the budget provisions 2008-09proposals for 2009-10 are given in the table No. 3.
TTTTTable No. 3able No. 3able No. 3able No. 3able No. 3
BCG VL Guindy Budget Provision 2008-09 and BE 2009-10BCG VL Guindy Budget Provision 2008-09 and BE 2009-10BCG VL Guindy Budget Provision 2008-09 and BE 2009-10BCG VL Guindy Budget Provision 2008-09 and BE 2009-10BCG VL Guindy Budget Provision 2008-09 and BE 2009-10
(Rs. in Lakh)
Sub-Head Plan Non Plan Total
BE 2008-09 500.00 700.00 1200.00
EXPENDITURE till Oct.08 34.00 151.00 183.00
RE 2008-09 500.00 925.20 1425.20
BE 2009-10 873.00 1545.40 2418.40
Performance of BCG VL (Production, Demand& Supply 2008-09):
The Drug controller General(I), Central LicenseApproving Authority, Drug Control Division, DGHS,New Delhi-110011 vide their O.M. No.X-11026/1/06-D dated 15.1.2008 suspended the license tomanufacture BCG Vaccine by this Laboratory till suchtime the new facilities are made ready. Hence therewas no production of BCG Vaccine from 16.1.2008.Consequently no supply could be made to theExpanded Programme of Immunization of the GOIw.e.f. 23.2.2008.
� Production during 2008-09 nil.
� Demand received during 2008-09 nil.
� Quantity supplied during 2008-09 nil.
Current Status of Functioning of BCG VLGuindy:
� National Regulatory Authority (NRA)undertook assessment of all the three PSUsunder the control of GOI in August 2007. Itwas observed that vaccine manufacturing
facilities at BCG VL Guindy is not cGMPcomplaint. As a result show cause notice wasissued to BCG VL in Dec. 2007; followingwhich DCG (I) suspended the manufacturinglicense of the BCG VL on 15.1.2008.
� Subsequently in a meeting under thechairmanship of Secretary (Health) held on6.2.2008 it was decided that stocks ofproducts available with three institutionsshould not be supplied for humanconsumption and no production of the newbatches and new procurement of raw materialshould be resorted to. The bulk in differentcomponent available in pipeline should notbe utilized and the cost there of will beconsidered to be written off. The list of theconsignee issued by supply division to CRIKasauli recently should not be acted upon.These institutions are to be converted in drugtesting laboratories/ training units.
� A committee under the chairmanship of DCG(I) has been constituted vide letter No.V.12011/1/2008-CC&V, dated 11th April, 2008to study the existing infrastructure/facilities
274
ANNUAL REPORT 2008-09
available with these institutes and explorefeasibilities of conversion of the existing unitsinto testing laboratories or training units.Expert committee has been constituted underthe chairmanship of DCG(I) has visited all thethree PSUs. The report of the expertcommittee is submitted and is beingexamined.
� Currently the manufacturing license of theBCG VL Guindy is under suspension and noproduction of BCG vaccine is beingundertaken currently. Further initiativetowards fictionalization Institute w.r.t.manufacturing of vaccine, converting theseinstitutions into drug testing laboratories and/or training units will be undertaken after thereport after expert committee under DCG(I)will be received. No supply of BCG vaccinehas been issued after the suspension of themanufacturing license during 2008-09.
15.3115.3115.3115.3115.31 All India Institute of HygieneAll India Institute of HygieneAll India Institute of HygieneAll India Institute of HygieneAll India Institute of Hygieneand Public Health (and Public Health (and Public Health (and Public Health (and Public Health (AIIH & PHAIIH & PHAIIH & PHAIIH & PHAIIH & PH),),),),),KolkataKolkataKolkataKolkataKolkata
Background
The All India Institute of Hygiene and Public Health(AIIH&PH), Kolkata, a premier organization of theGovernment of India, was established in 1932 withthe assistance of Rockefeller Foundation. In fact, thisinstitute happens to be the oldest School of PublicHealth in the entire South East Asia Region pioneeringin Post-Graduate Teaching and Research in variousdisciplines of health intelligence and health services.The Institute continues to pursue its mandate fordevelopment of human resources in the field of PublicHealth since its inception. The primary objectives ofthe Institute are:
� To develop health manpower by providingpost-graduate training facilities of the highestorder;
� To conduct research directed towards thesolution of various problems of health anddiseases in the community;
� To undertake fundamental and operationalresearch to develop methods for optimumutilization of health resources and applicationof the findings for protection and promotionof health care services;
The Institute also plays a key role in advising variousState Governments on health measures to combatpublic health crises that arise from time to time. It isalso the nodal organisation for administering YellowFever Vaccine.
Institutional set up
The Institute has eleven (11) academic departmentsand two (2) field practice areas, one at Urban HealthCentre, Chetla, Kolkata and the other at Rural HealthUnit & Training Centre, Singur, Dist. Hooghly. TheInstitute also houses a reference library, Two hostels,one for men and another for women, located in thevicinity of the main building of the Institute toaccommodate students & guests. Hostel facilities arealso available at Rural Health Unit & Training Centre,Singur.
In the 2nd Campus, construction of 44 residentialquarters, substation building, int3rnational hostel andguest house along associate services has alreadybeen completed. It is expected to be made fullyoperational by March, 2009. The project is estimatedto cost Rs.41.42 crores.
Budget Allocation
The Institute has been allocated the following BudgetGrant for the financial year 2008-09:
Budget Head Plan Non-plan Total
Grant (Rs. Crores) 20.00 18.75 38.75
Besides, International Agencies like WHO, UNICEF,ICEF, UNDP also provided funds to this Institute tocarry out various projects/research activities in PublicHealth & Hygiene.
Teaching and Training Activities
The AIIH&PH is the only Institute in India whichprovides multi-professional health training facilities
275
ANNUAL REPORT 2008-09
for various disciplines such as doctors, engineers,nurses, nutritionists, statisticians, demographers,social scientists, epidemiologists, micro-biologistsand other allied health professionals. During the year2008-09, the Institute conducted one MD course inCommunity Medicine, master's degree courseVeterinary Public Health, Post Graduate diplomacourses viz., DPH, DMCW, DIH, DHE and Dip-dietand several other short-term orientation and trainingcourses in the field of public health and hygiene.
Initiatives have been taken to introduce five newcourses from the academic year 2008-09. These are(i) Master in Public Health which has already beencleared by the Govt. of West Bengal as required byWBUHS, (ii) M.Sc. (Applied Nutrition) already clearedby the Gov. of West Bengal as required by WBUHS,(iii) MPH (Infectious diseases) to be conducted byNICED, Kolkata as part of the School of Public Healthof ICMR, (iv) Diploma in Public Health Management-1 year course under Calcutta University and (v)Epidemiology Course (FETP) with WHO.
Thirty five students from different Eastern and NorthEastern States have so for joined the DPPHM course.The West Bengal University of Health Sciences hasprovisionally approved the affiliation of the MPH andthe M.Sc. in Applied Nutrition course proposed to beintroduced in the AIIH&PH.
Important Project/ Research Activities:
� Department of Biochemistry and Nutrition wasentrusted by the Ministry of Health & FamilyWelfare, Government of India as a regionalcenter to conduct detailed survey in 11 statesunder World Bank assisted Capacity BuildingProject on 'Food Safety and Quality Controlof Drugs.' The Project envisagesstrengthening the infrastructure of the Food& Drug Laboratories both at the Central andstate level.
� Research Projects on Prevalence ofArsenicosis in West Bengal, funded by theGov. of West Bengal has been completed inthe districts of South 24-Parganas andMaldah and field work is currently going onin Mursidabad District.
� Feasibility study on the Integration of RuralHealth Practitioner in the Health Care DeliverySystem is being done by the Department ofPublic Health Administration.
Other Important Activities:
a. The Department of PHA co-ordinated thetraining of the students of Diploma in TropicalMedicine and Hygiene (DTMH)and MDTropical Medicine, from the School of TropicalMedicine, Kolkata in AIH&PH.
b. The Department of PHA,as the Nodaldepartment, has conducted ProfessionalDevelopment Course (PDC) for District levelofficers, which lis sponsored by Govt. of Indiaand European Commission. The programmeincluded (i) Monitoring and evaluation ofhealth programmes for Health Supervisors,(ii) Sensitization of Health Supervisors onHealth Management Information Systems.
c. The Department of Epidemiology organizedtwo Pre-Surveillance Training Workshops forthe participants from 11 States under HIVSentinal Surveillance HSS - 2008 Workshop.
d. The Institute has been selected as one ofthe Study Center for M.Sc. (DFSM), MastersProgramme in Dietetics and Food serviceManagement by Indira Gandhi National OpenUniversity which is a two years' course.
e. The post graduate and under graduate andunder graduate students of the Departmentof Physiology, Calcutta University, andBurdwan University were trained on diedsurvey and nutritional status assessment ina rural community.
f. Three programmes namely (i) Processingand preservation of fruits and vegetables,using rurally suitable techniques. (ii)Development of simple rurally feasibletechnologies to process food for minimizingarsenic ingestion through food chain (iii)Improvement of quality of Street Food ofKilkata using locally suitable Food Processing
276
ANNUAL REPORT 2008-09
technologies. These progammes have beendesigned, planned and initiated by the Deptt.of Biochemistry and Nutrition in collaborationwith the Department of Food ProcessingIndustries and Horticulture, Govt. of WestBengal land supported by the Ministry ofFood Processing Industries, Govt. of India.
g. As a nodal organization for administeringYellow Fever Vaccine, this Institute isvaccinating around 800 persons in a year.As an HIV surveillance center, the Institutealso tested up to Sept. 2008, 229 samplesfrom different categories of individuals fordetection of HIV. In addition, 153 watersamples, 130 for bacteriology and 70 samplesfor Parasitology have been tested.
h. The Department of Microbiology along withthe Department of epidemiology of thisInstitute has been identified by NACO as theDepartments of Regional Institute (RI) for theHIV Sentinel Surveillance Programme 2008also.
i. Institute is the WHO Collaborating Centre forDisaster Preparedness.
j. The Department of Sanitary Engineeringprovides service of water/waste wateranalysis to various Governmentorganizations, Municipal authorities, NGOsetc.
k. Installation of LAN for RHU&TC Singur andUHC, Chetla units of the Institute has beencompleted.
l. Website for the Institute has been launchedsuccessfully.
m. The Department of Epidemiology as the nodaldepartment for IDSP Training (TOT) for 7North Easter States conducted 3programmes since April 2008.
n. 11 WHO Trainees have been trained indifferent courses in the Institute in theBiennium 2007-07.
o. 30 trainees have so far been nominated byWHO for training in different courses in thebiennium 2008-09.
p. The Department of Microbiology will also beconducting IDSP training programmes for theDistrict Medical Officers for the 3rd phase ofin the North Eastern States of India.
q. The Department of Microbiology is alsoexpected to conduct WHO FellowshipProgramme for the fellows on "Bacteriologicalanalysis of water" for the biennium 2008-09.
Field Practice Units:
Two Field Practice Units viz. Urban Health Centre,Chetla, Kolkata and Rural Health Unit and TrainingCentre, Singur, Hooghly (W. Bengal) are under thedirect control of AIIH&PH. The Rural Health Unit andTraining Centre at Singur covers a population of 0.9lakhs (approx.) consist in of 62 villages, whereas theUHC, Chetla, Kolkata covers a population of about1.04 lakhs spread over an area of 3.9 Sq. Kms. TheCentre at Singur also provides health care servicesthrough its two Primary Health Centres and four Sub-Centres.
Library Services:
The Institute has a large reference library havingabout 64500 (approx) books and journals. The stockof the library is constantly being enlarged andenriched every year through acquisition of latestbooks and journals, periodicals, etc.
Implementation of official language policy:
� A two day Hindi workshop on noting anddrafting was organized on 27.05.2008 andon 28.05.2008.
� Hindi Pakhwara was organized for theofficers/staff of the institute from 1.09.2008to16.09.2008
� The Praveen / Pragya training under HindiTeaching Scheme for July session has beenstarted in the Institute itself and 42 staff andofficers nominated for Praveen / Pragya. A
277
ANNUAL REPORT 2008-09
total 3 officers / staff successfully completedthe Praveen / Pragya training under HindiTeaching Scheme.
15.3215.3215.3215.3215.32 RRRRRegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Teaching &eaching &eaching &eaching &eaching &RRRRResearch Institutes (esearch Institutes (esearch Institutes (esearch Institutes (esearch Institutes (RLRLRLRLRLTRITRITRITRITRI)))))
The four leprosy institutes working under DirectorateGeneral of Health Services, Ministry of Health &Family Welfare, Govt. of India viz. CLTRI,Chengalpattu, RLTRI at Aska, Raipur & Gouripur areinvolved in basic and applied research in leprosyand training of different categories of staff. Theseinstitutes also play important role in management ofreferral patients, providing quality care to chroniculcer and disabled patients with the help of Minor &Major Reconstructive Surgeries. They also help insupervising and providing consultancy services tothe State NLEP Units for better programme planningand implementation.
15.3315.3315.3315.3315.33 Central Leprosy TCentral Leprosy TCentral Leprosy TCentral Leprosy TCentral Leprosy Training andraining andraining andraining andraining andResearch Institute, Chengal-Research Institute, Chengal-Research Institute, Chengal-Research Institute, Chengal-Research Institute, Chengal-pattu, (Tpattu, (Tpattu, (Tpattu, (Tpattu, (Tamil Nadu)amil Nadu)amil Nadu)amil Nadu)amil Nadu)
This institute was established from 1924, it was,however taken by Govt. of India in 1974 with anobjective to provide diagnostic, treatment andreferral services to leprosy patients, trainedmanpower development and research on variousaspects of leprosy and its control. It has separatewings of Epidemiology and Statistics, Clinical,Medicine, Microbiology and Bio-chemistrylaboratories with Animal House facilities, Surgery andPhysiotherapy. The hospital has bed capacity of 125patients and caters to both indoor and outdoorpatients. This Institute is also recognized as one ofthe nodal center by Central Bureau of HealthIntelligence (CBHI), DGHS, Govt. of India forconducting Health Statistics training course forMedical Officers.
In view of the declining trend of leprosy the Institutehas been assigned additional functions in the areaof capacity building for integrated diseasesurveillance programme, epidemiology trainingcourse, microscopy and DOTS, Operationalresearch, Referral Laboratory for external quality
assurance and drug resistance surveillance centerunder RNTCP.
The institute is actively involved in the training ofLaboratory Technician (one year course),Physiotherapy Technician (9 months course), DistrictMedical Officer (5-days), Reconstructive surgery(one month), Medical Officer (5-days), Non-MedicalSupervisor (2 months), Health Statistics (3 days) andCRRI (5-days). In addition to this a special one daytraining for various medical and non-medicalpersonnel are also conducted at CLTRI.
Hospitalized patients include cases of Multi DrugTherapy (MDT) complication, reaction, ulcermanagement, reconstructive surgery required casesand Prevention of Deformity (POD) managementcases. In-patients service also includes expertisemanagement of lepra-reactions with steroids/thalidomide and investigation for drug relapse /resistance. Currently CLT & RI is investigating casesof suspected relapse / treatment failures for drugresistance use Mouse Food Pad (MFP) techniqueand also modern PCR based molecular methods.
OPD provide services for diagnosis of leprosy,relapse, reaction and manageable general diseaseof RFT cases. On average 50 patients are attendingOPD daily.
Research Activities:
� Study on surveillance of RifampicinResistance among Multibacillary cases ofrelapse using Mouse
� Footpad and Molecular biologicaltechniques.
� Application of PCR for the diagnosis ofleprosy
� Application of PCR for the detection of Sub-clinical infection
� Comparison of Molecular biologicaltechniques and conventional bacteriologicaltechniques in the diagnosis of ExtraPulmonary Tuberculosis using differentsamples.

278
ANNUAL REPORT 2008-09
� Application of PCR - SSCP for the rapiddetection of Rifampicin Resistance amongM.tuberculosis using extra pulmonarysamples.
15.3415.3415.3415.3415.34 RRRRRegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Training andraining andraining andraining andraining andResearch Institute, RaipurResearch Institute, RaipurResearch Institute, RaipurResearch Institute, RaipurResearch Institute, Raipur(Chhattisgarh)(Chhattisgarh)(Chhattisgarh)(Chhattisgarh)(Chhattisgarh)
This institute was established in 1979 with 75 bedshospital OPD. The institute provides both indoor &outdoor services to leprosy patients and a numberof Reconstructive surgeries are carried out regularlyfor various type of leprosy deformities in the institute'shospital. The institute also works as a referral centerfor problematic, complicated and intractable cases.It also works as a nodal training and research centerparticularly, program related research activities in theregion for the cause of leprosy elimination. ThisInstitute also provide need based leprosy training tothe various categories of Medical professionals.
The Institute has been assigned with responsibilityof Regional Office of Health and Family Welfare forthe State of Chhattisgarh and various additionalfunctions has also been assigned in the area ofcapacity building for Integrated Disease SurveillanceProgram, Epidemiology Training Course, lymphaticfilariasis ( Disability Management and relatedtraining), Microscopy and DOT centres, OperationalResearch related to RNTCP, Voluntary CounselingCentres (VCC) and diagnostic centre for HIV / AIDS,Disaster management and Various National HealthProgram especially Malaria. Recently the institutehas also been recognized as a centre for conductingreconstructive surgery of persons with poliomyelitisrelated disability.
During 2007-08, 771 new cases of leprosy were giventreatment, 376 cases were admitted in hospital and100 persons affected by leprosy have undergonereconstructive surgery. 928 patients had takenphysiotherapy. Institute also participated in trainingof district nucleus teams. RLTRI, Raipur alsoorganised operational research about integration ofNLEP with general health care system and follow of
cases in the field. Institute is also involved inmonitoring and supervision of the programme.
15.3515.3515.3515.3515.35 RRRRRegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Training &raining &raining &raining &raining &RRRRResearch Institute (esearch Institute (esearch Institute (esearch Institute (esearch Institute (RLRLRLRLRLTRITRITRITRITRI) ) ) ) ) ASKASKASKASKASKAAAAA,,,,,OrissaOrissaOrissaOrissaOrissa
This institute was established in 1977 and has a 50beds hospitals. The in patient services regularlyadmits and treats leprosy. It also works as nodaltraining & research center. Institute is providingtraining to sponsored candidates coming fromvarious States and voluntary organisations. Last yearInstitute had conducted reorientation training coursesfor general health staff including staff nurses, housesurgeons, final year medical students etc.
15.3615.3615.3615.3615.36 RRRRRegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Tegional Leprosy Training andraining andraining andraining andraining andRRRRResearch Institute,Gouripuresearch Institute,Gouripuresearch Institute,Gouripuresearch Institute,Gouripuresearch Institute,Gouripur,,,,,Bankura, (WBankura, (WBankura, (WBankura, (WBankura, (West Bengal) :est Bengal) :est Bengal) :est Bengal) :est Bengal) :
This institute was established in 1984 and has ahospital of 30 beds capacity for admission of patientsand it also provide regular OPD services. Theinstitute has field practice area for covering 2 lakhspopulation. I.E.C. Programme is also carried out.The in-patients services regularly admits, treatsleprosy patients for treatment inulcers, leprosyreactions and physiotherapy . It also works as nodaltraining and research centre particularly programmerelated research activities in the region for the causeof leprosy elimination.
Last year 153 patients were admitted in the Hospitaland 2800 was the OPD attendance. Institute is alsorunning a field unit catering to 2.5 lakhs populationfor IEC and health awareness
15.3715.3715.3715.3715.37 National Medical LibraryNational Medical LibraryNational Medical LibraryNational Medical LibraryNational Medical Library
Introduction
National Medical Library (NML) provide valuablelibrary and information services to support theacademic, research and clinical work of biomedicaland health science professionals in the country. Itoccupies important position in country's health careinformation delivery system. Some of the significantservices provided by NML are:
279
ANNUAL REPORT 2008-09
Activities and Services
Reference services & collection building
One of the greatest strengths of NML is its richestcollection of books, reports, serials, bound volumesof journals and computer databases. This invaluabletreasure of biomedical and health science information,which is often the only source, is widely used byprofessionals from all parts of the country. It hascollection of over 1.31 lakhs books and over 5 lakhsbound journals. The Library subscribed 1510 printjournals worth Rs. 14.8 crore in 2008. Library followsOpen-Access system for shelf arrangement. Libraryadded 1270 volumes (books purchased 836+ serialspurchased 103+Gift books 331) by spending over 17.5lakhs in the year 2008. The books and journalsacquired during the year have been classified andcatalogued by using LIBSYS library software package.
Local Area Network (LAN) and Online PublicAccess Catalogue (OPAC)
Servers and computers in the library are networkedto form a LAN having an integrated LibraryManagement Software Package - LIBSYS. About36,000 records of books are now available throughOPAC computer search by library users. Leasedlines of (100 mbps) and broad band internet facilityis available to provide Internet services includingaccess to full-text of the journals.
Information Retrieval Services
NML has been offering the service using MEDLINECD-ROM since 1990. Besides, it has about 500 CDson different subjects. The biomedical informationsources available free on Internet, namely PUBMED,PUBMED Central, ERMED etc. were also accessed tomeet the requirement of library users. Many articleswere searched through MEDLINE service for gettingreferences and abstracts for research scholars duringthe year. A Workstation having the facility of 10terminals fitted with CD writer is being developed foron-line access of foreign medical journals.
Scheme to "Inter-linking of GovernmentMedical College Libraries with the NML".
Government colleges are provided with financial
assistance to acquire hardware, software, Internetconnectivity and to hire contractual staff. Thisscheme has already covered 78 medical collegelibraries. The project aims to develop informationcommunication technology capability among theparticipating colleges to be able to access the onlineinformation resources available in NML. Librarybrings out a quarterly "List of New books Added toNML". It is also bringing out a weekly "Indian PressIndex on Health" which covers important pressrelease on topics related to health science inprominent Indian newspapers.
Reference and Documentation Services
The library remains open on 359 days of the yearfrom 0900 - 2000 hrs on weekdays and from 0930 -1800 hrs on holidays. Over 200 users visit the libraryevery day for reference, consultation, obtainingphotocopies of required articles and informationretrieval service. Library has been visited byinformation seekers to avail following services:
1. Queries answered 5081
2. New Membership 108
3. Issue/return of documents 1166
4. Inter Library loan (Print documents) 40
Library developed database of over 6000 medicalthesis/dissertation submitted to medical collegesacross the country. The same is available at <SearchMedthes> at www.nml.nic.in. The library alsodeveloped a database of over 4000 medical articlespublished in Indian Medical journals in the country inMARC21 software under the "Index Medicus-India" project.
Document Delivery Service
The Document Delivery Service provides access tothe full text of documents needed by various medicalspecialists. This service is in fact used more widelythan any other service of the library and caterspredominantly to requests for copies of articles injournals (current as well as back files). A largenumber of request for photocopy of articles arereceived from outside Delhi by post, e-mail and fax
280
ANNUAL REPORT 2008-09
through Government as well as private photocopycounters. Photocopies of about 8000 articles permonth are provided to medical research scholarsacross the country, in which postal charges are freefor delivery of articles to outside Delhi states.
ERMED-India e-journal consortium
NML started Electronic Resources in MEDicine(ERMED) India e-journal consortium in 2008 byspending Rs. 2.6 crore for providing 1515 e-journalsto 39 Members from Medical Colleges/Institutes of10 DGHS+28 ICMR institutes and AIIMS. The ERMEDdesigned an independent versatile search portalwww.nmlermed.in for accessing consortiumresources. The consortium made visible impact byproviding more than 57,000 download of full text ofmedical journal articles in 2008.
Training and Consultancy Services of the Library:
A. Library has provided in house practicaltraining to the following Library Sciencestudents as indicated below:
1. Library Science Graduate apprenticedeputed from Board of ApprenticeshipTraining (Northern Region), Kanpur (UP).
2. Certificate in Library Science studentsdeputed from the Delhi LibraryAssociation, New Delhi.
3. BLIS students deputed from Jamia MilliaIslamia, New Delhi.
4. NML provided training to 40 medicalcollege librarians from state medicalcolleges/institutions in Feb., 2008.
B. Consultancy services provide to the libraryof the following Hospitals/Institutes:
1. LRS Institute of Tuberculosis andRespiratory Diseases, New Delhi.
2. National Institute CommunicableDiseases, Delhi.
3. Institute of Human Behaviour and AlliedSciences (IHBAS), Delhi.
4. Institute of Nuclear Medicine and AlliedSciences (INMAS), Delhi.
5. AYUSH, Ministry of Health & F.W., NewDelhi.
6. Dr. RML Hospital, New Delhi.
7. Safdarjung Hospital, New Delhi.
Branch Library
National Medical Library maintains a branch libraryin the Nirman Bhawan to cater to the library andinformation needs of staff and officers in theDirectorate General of Health Services and theMinistry of Health and Family Welfare. Steps arebeing taken to renovate the present library set upand to improve library collection and services atBranch Library.
Library Building
As the library building is 34 years old, severalmeasures have been taken to repair and restore thestructure and modify it as per the modernrequirement. The building needed completerenovation and repair to improve the exterior get upof the library as per its status.
Necessary repairs and renovation of the building hasbeen done. The installation of lift and the dumb waiterare in the final stage of completion.
15.3815.3815.3815.3815.38 Lala Ram Sarup TB HospitalLala Ram Sarup TB HospitalLala Ram Sarup TB HospitalLala Ram Sarup TB HospitalLala Ram Sarup TB Hospital
LRS TB hospital was established by TB Associationof India in 1952. The hospital was upgraded into anautonomous institute in 1991 by Govt. of India. Later,the Institute was renamed as LRS Institute ofTuberculosis & Respiratory Diseases as anautonomous institute under the Ministry of Health &Family Welfare, Government of India. It is now anapex institute of the country in the field of tuberculosisand respiratory diseases.
Tuberculosis is a major health problem in India. Itkills more adults in our country than any otherdisease. It affects a large number of victims who arein the productive age group and results in social and
281
ANNUAL REPORT 2008-09
economic consequences. The institute is activelyinvolved in teaching, training and research in the fieldof T.B. & Respiratory diseases. The institute assiststhe government of India in developing strategies forT.B. Control and in implementation of the same. Theinstitute has a daily OPD with an average OPDattendance of more then 350 patients per day andIndoor wards. The new OPD block has state of artfacilities under one roof. The institute has a well-equipped respiratory intensive care unit & ThoracicSurgery Deptt. with state of art equipments. TheVoluntary counseling and Testing Centre (VCTC) forHIV and AIDS has been functioning under the sameroof. Besides this, the institute has various supportdepartments and sections are as follows :-
I. Departments :
1 Department of Hospital Administrative
2 Department of TB & Respiratory Diseases
3 Department of TB Control & Training
4 Department of Microbiology
5 Department of Anaesthesia
6 Department of Thoracic Surgery SurgicalAnatomy
7 Department of Surgical Anatomy
8 Department of Pathology
9 Department of Bio-Chemistry
10 Department of Paediatric
11 Department of Internal Medicine
12 Department of Epidemiology & PublicHealth
13 Department of Radiology
14 Department of Molecular Medicine & Bio-technology
15 Department of Physiology
II. Sections
1 Respiratory intensive care unit (ICU)
2 Sleep lab
3 Health education section:
4 Biostatistics section
5 Voluntary Counseling and Testing Centre(VCTC)
6 Fibre-optic Bronchoscopy Unit
7 Lung Cancer section
8 Physiotherapy section
9 Library
10 Computer section
11 ART Centre
12 Yoga Centre
13 Allergy and Immunotherapy Clinic
Since the institute is an apex one for diagnosis ofchest diseases, the cases are referred here fordiagnosis and management. The institute has aseparate Bronchoscopy unit for diagnosis ofcomplicated cases like Lung cancer & interstitial lungdiseases etc. The Institute is establishing separateward for Multi Drug Resistance (MDR) TB cases withstate of art infection control measures.
Manpower
At present, the Institute has 37 Group-A, 45 Group-B, 188 Group-C and 178 Group-D Staff in position.In addition, there are 13 senior residents & 21 juniorresidents working on tenure basis.
Posts Group A Group B Group C Group D SR JR Total
No.of Sanctioned Staff 40 45 224 203 13 21 546
Present Staff strength 37 45 188 178 13 21 482
282
ANNUAL REPORT 2008-09
Out Patient Department
The Institute provides treatment for patients withinthe domiciliary area. Patients also visit from non areawithin Delhi and neighbouring states. Further, partof the specified area of LRS institute has beentransferred to Malviya Nagar Chest Clinic, thereforethe specified area under the LRS institute hasreduced and presently RNTCP is functioning through17 DOTS centres covering a population of 1 millionas against the previous 1.8 millions.
Patients data at LRS -OPD (Apr-08 to Aug-08):-
During the period under review, a total of 14887chests symptomatic attended the LRS-OPD. Out ofthese 3309 (22%) came from the LRS specified area,7799 (52%) from Non-Area within Delhi and 3779(25%) from outside Delhi. It is to be noted that someof the area DOTS centres have been transferred toother chest clinic (Malviya Nagar) but the patientsare still visiting the institute for diagnosis, therefore,the proportion of patients from non area is higherthan the area patients, whereas the trend was inreverse order earlier.
Diagnosis of TB cases in LRS -OPD:-
A total of 3154(21%) TB cases were diagnosed outof 14887 symptomatics. Out of these, 2962(94%)were referred out from LRS to LRS DOTS centres/other chest clinics in Delhi or outside Delhi and 192(6%) were registered at LRS for further treatment.
Total patients in the OPD (OPD Load)
The total number of patients who attend the LRSOPD constitute mainly four groups (i)New registration(ii) Subsequent visits for diagnosis (iii) Follow up visitsof TB cases and (iv) Follow up Visits of Non-TBpatients. During the period, a total of 42364 patientsattended the OPD with an average of total 324patients per day including 117 per day as newregistrations.
Patients at DOTS Centres:-
A total of 3250 chest symptomatic attended the DOTScentres from the specified area of the institute. Outof these, a total of 852 patients were diagnosed asTB cases and registered under DOTS (RNTCP).Majority of these TB cases were diagnosed at LRS-OPD and referred to DOTS centres for furthertreatment under DOTS. All these TB cases were puton DOTS treatment and none on conventionaltreatment.
Paediatric OPD:
A Daily OPD for children is being carried out in theMorning from Monday to Saturday. During thisperiod, a total of 1368 symptomatic children wereregistered in the OPD.
Special Clinics: -
The Institute has various specialised clinics, whichare held periodically.
Clinics Days/Timing
Sleep Clinic Tuesday
Clinic for Smoking Cessation Tuesday, Friday (11AM to 1PM)
Clinic for Empyema and Surgical Patients Tuesday, Friday (2 PM to 4PM)
Clinic for Allergy and Immunotherapy Tuesday, Friday (11AM to 1PM)
Anti-Retroviral Therapy Centre/ Clinic Monday to Saturday
Lung Cancer Clinic Tuesday (9AM to 1PM)
283
ANNUAL REPORT 2008-09
Surgical Clinic:
Surgical clinics are held on Tuesday and Friday inafternoon for patients requiring surgical treatmentand follow up post-operative patients. During April2008 to August 2008, 98 new cases for surgical clinicwere registered and 699 follow up cases were seenin the clinic. In surgery department, during the fivemonths period a total of 154 Major, includingEndoscopies and 1000 Minor procedures werecarried out.
Indoor Patient Data:
The Institute provides indoor treatment to theserious patients for the treatment of tuberculosisand respiratory diseases. The Institute has 520beds. These beds are distributed in 16 wards andICU.
The patients requiring hospitalisation are admittedin the institute for the treatment of tuberculosis andother respiratory diseases. These hospitalisedpatients include cases of multi-drug resistant TB,Emergencies such as haemoptysis, pneumothorax,Surgical and seriously ill patients of respiratorydiseases, Cases with diagnostic problems andpatients requiring Intensive Care management forrespiratory diseases.
During the period from April, 2008 to August, 2008,a total of 2292 patients were admitted. A total of 197deaths occurred during April 2008 to August 2008among both TB and Non TB cases. It has beenobserved that majority of the patients came at terminalstage.
All hospitalized TB patients are given DOTS as perRNTCP guidelines and on discharge are refer to theirrespective DOTS centres.
TRAINING:
Training of Medical & Paramedical personal:
The institute is actively involved in the training ofvarious medical and paramedical personnel who visit
from other states of our country, in implementationof strategies under Revised National Tuberculosis
Control Programme (RNTCP), several training
programmes have been conducted by the institute
for Doctors, paramedical personnel (Lab Tech., Sr.
Lab Tech., Treatment organisers, Sr.Treatment
supervisors and programme officers, Administrators)
of several states.
The training is also imparted in the management of
tuberculosis to the nursing students from Rajkumari
Amrit Kaur College of Nursing and the trainee health
visitors from New Delhi TB Centre every year. During
the period 130 participants including doctors were
trained.
DNB course:
The Institute is recognised centre for DNB (TB &
Respiratory diseases) degree course since 1999.
Presently 17 students are under going DNB
course.
Organising the CME & Conferences:
The institute is actively involved in organizing
Continuing Medical Education programme (CME) on
different aspects of diagnosis and management of
tuberculosis.
1. SEARCH Regional HIV/AIDS Training held on
28th July - 8th August 2008.
2. Satellite Workshop on "Management of MDR/
XDR-TB" First International Conference of
SEAR-NATCON, 2008 On 7th September,
2008.
RESEARCH ACTIVITIES:
Research is one of the primary objective of theInstitute. The following research studies were startedduring the year.
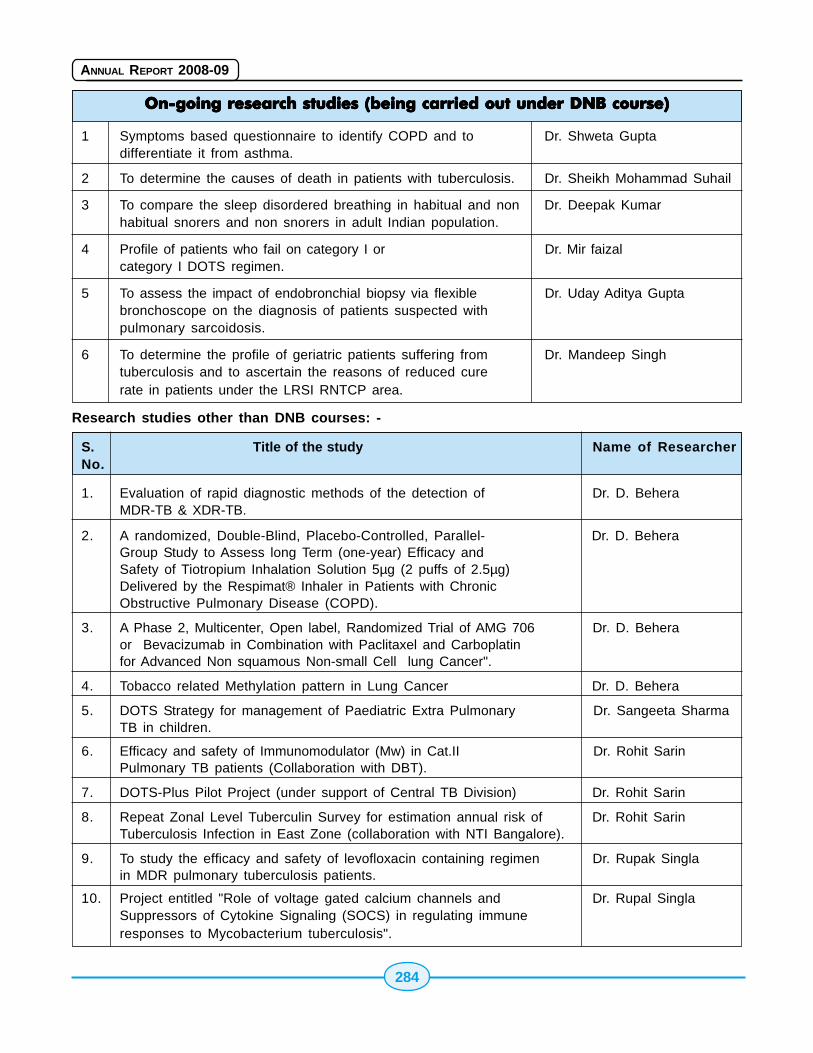
284
ANNUAL REPORT 2008-09
On-going reOn-going reOn-going reOn-going reOn-going research studies (being carried out under DNB course)search studies (being carried out under DNB course)search studies (being carried out under DNB course)search studies (being carried out under DNB course)search studies (being carried out under DNB course)
1 Symptoms based questionnaire to identify COPD and to Dr. Shweta Guptadifferentiate it from asthma.
2 To determine the causes of death in patients with tuberculosis. Dr. Sheikh Mohammad Suhail
3 To compare the sleep disordered breathing in habitual and non Dr. Deepak Kumarhabitual snorers and non snorers in adult Indian population.
4 Profile of patients who fail on category I or Dr. Mir faizalcategory I DOTS regimen.
5 To assess the impact of endobronchial biopsy via flexible Dr. Uday Aditya Guptabronchoscope on the diagnosis of patients suspected withpulmonary sarcoidosis.
6 To determine the profile of geriatric patients suffering from Dr. Mandeep Singhtuberculosis and to ascertain the reasons of reduced curerate in patients under the LRSI RNTCP area.
Research studies other than DNB courses: -
S. Title of the study Name of ResearcherNo.
1. Evaluation of rapid diagnostic methods of the detection of Dr. D. BeheraMDR-TB & XDR-TB.
2. A randomized, Double-Blind, Placebo-Controlled, Parallel- Dr. D. BeheraGroup Study to Assess long Term (one-year) Efficacy andSafety of Tiotropium Inhalation Solution 5µg (2 puffs of 2.5µg)Delivered by the Respimat® Inhaler in Patients with ChronicObstructive Pulmonary Disease (COPD).
3. A Phase 2, Multicenter, Open label, Randomized Trial of AMG 706 Dr. D. Beheraor Bevacizumab in Combination with Paclitaxel and Carboplatinfor Advanced Non squamous Non-small Cell lung Cancer".
4. Tobacco related Methylation pattern in Lung Cancer Dr. D. Behera
5. DOTS Strategy for management of Paediatric Extra Pulmonary Dr. Sangeeta SharmaTB in children.
6. Efficacy and safety of Immunomodulator (Mw) in Cat.II Dr. Rohit SarinPulmonary TB patients (Collaboration with DBT).
7. DOTS-Plus Pilot Project (under support of Central TB Division) Dr. Rohit Sarin
8. Repeat Zonal Level Tuberculin Survey for estimation annual risk of Dr. Rohit SarinTuberculosis Infection in East Zone (collaboration with NTI Bangalore).
9. To study the efficacy and safety of levofloxacin containing regimen Dr. Rupak Singlain MDR pulmonary tuberculosis patients.
10. Project entitled "Role of voltage gated calcium channels and Dr. Rupal SinglaSuppressors of Cytokine Signaling (SOCS) in regulating immuneresponses to Mycobacterium tuberculosis".
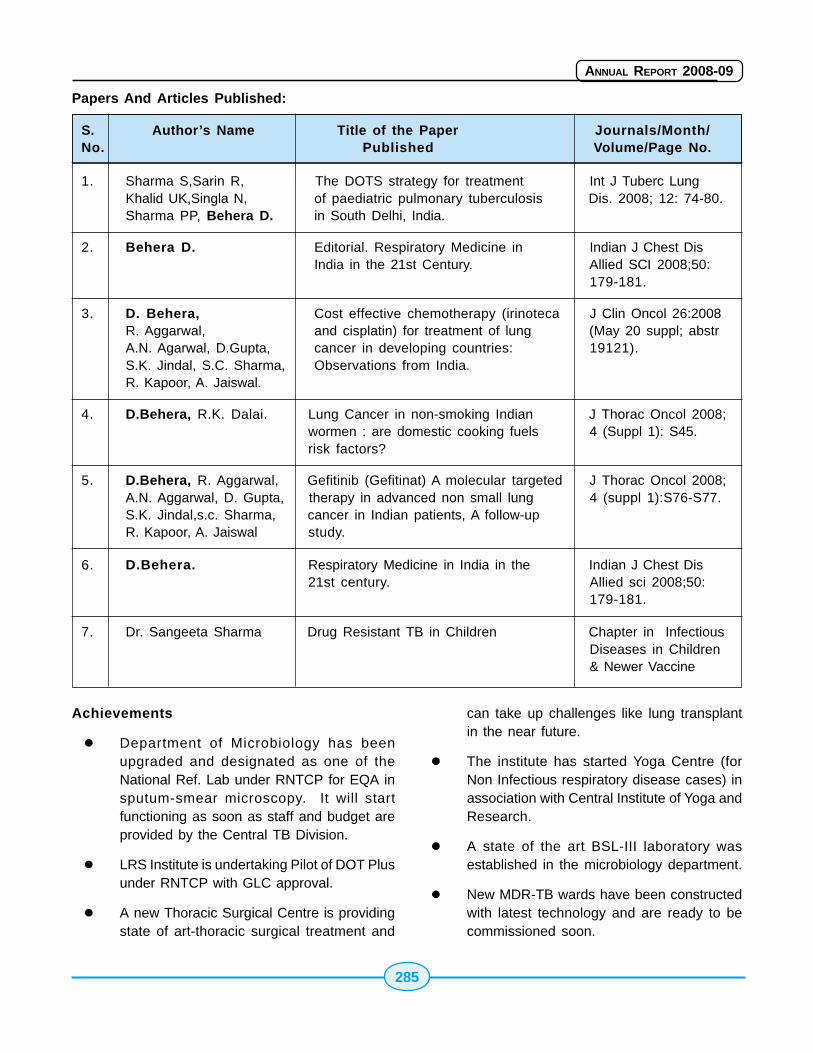
285
ANNUAL REPORT 2008-09
Papers And Articles Published:
S. Author’s Name Title of the Paper Journals/Month/No. Published Volume/Page No.
1. Sharma S,Sarin R, The DOTS strategy for treatment Int J Tuberc LungKhalid UK,Singla N, of paediatric pulmonary tuberculosis Dis. 2008; 12: 74-80.Sharma PP, Behera D. in South Delhi, India.
2. Behera D. Editorial. Respiratory Medicine in Indian J Chest DisIndia in the 21st Century. Allied SCI 2008;50:
179-181.
3. D. Behera, Cost effective chemotherapy (irinoteca J Clin Oncol 26:2008R. Aggarwal, and cisplatin) for treatment of lung (May 20 suppl; abstrA.N. Agarwal, D.Gupta, cancer in developing countries: 19121).S.K. Jindal, S.C. Sharma, Observations from India.R. Kapoor, A. Jaiswal.
4. D.Behera, R.K. Dalai. Lung Cancer in non-smoking Indian J Thorac Oncol 2008;wormen : are domestic cooking fuels 4 (Suppl 1): S45.risk factors?
5. D.Behera, R. Aggarwal, Gefitinib (Gefitinat) A molecular targeted J Thorac Oncol 2008;A.N. Aggarwal, D. Gupta, therapy in advanced non small lung 4 (suppl 1):S76-S77.S.K. Jindal,s.c. Sharma, cancer in Indian patients, A follow-upR. Kapoor, A. Jaiswal study.
6. D.Behera. Respiratory Medicine in India in the Indian J Chest Dis21st century. Allied sci 2008;50:
179-181.
7. Dr. Sangeeta Sharma Drug Resistant TB in Children Chapter in InfectiousDiseases in Children& Newer Vaccine
Achievements
� Department of Microbiology has beenupgraded and designated as one of theNational Ref. Lab under RNTCP for EQA insputum-smear microscopy. It will startfunctioning as soon as staff and budget areprovided by the Central TB Division.
� LRS Institute is undertaking Pilot of DOT Plusunder RNTCP with GLC approval.
� A new Thoracic Surgical Centre is providingstate of art-thoracic surgical treatment and
can take up challenges like lung transplantin the near future.
� The institute has started Yoga Centre (forNon Infectious respiratory disease cases) inassociation with Central Institute of Yoga andResearch.
� A state of the art BSL-III laboratory wasestablished in the microbiology department.
� New MDR-TB wards have been constructedwith latest technology and are ready to becommissioned soon.
286
ANNUAL REPORT 2008-09
� Institute has started a programme of providingcomprehensive management facilities topatients with Lung Cancer & a rehabilitationprogramme for patients with variousrespiratory diseases including pulmonary TB.
� A newsletter of the Institute is now beingpublished regularly every three months forcirculation among the professionalcolleagues.
� A number of high end equipments for patientcare and research were procured for variousdepartments.
� A block of 30 staff quarters (Type-A) hasbeen constructed.
� The institute has signed a memorandum witInternational centre for Genetic Engineeringand Research in order to take a mutuallybeneficial research projects in the field of TBand Respiratory diseases.
15.3915.3915.3915.3915.39 National Institute of MentalNational Institute of MentalNational Institute of MentalNational Institute of MentalNational Institute of MentalHealth and Neuro Sciences,Health and Neuro Sciences,Health and Neuro Sciences,Health and Neuro Sciences,Health and Neuro Sciences,(((((NIMHANSNIMHANSNIMHANSNIMHANSNIMHANS) Bangalore) Bangalore) Bangalore) Bangalore) Bangalore
National Institute of Mental Health and Neuro SciencesNIMHANS, is a specialty hospital for secondary andtertiary care for neurological and psychiatrydisorders. The Institute renders services to thepatients from all over the country as well asneighboring developing countries It has a mandateto develop trained manpower to cater to the needsof the community and carry out research in mentalhealth and neurosciences. The institute has theadded responsibility of formulating and evolving policystatements for implementation in the sphere ofcommunity mental health. With the advent ofoccurrence of natural calamities, various forms ofsocial strife and altered human behaviour, NIMHANShas been in the forefront to develop community basedstrategies for disaster and stress management, thusfacilitating human behaviour congenial to the society.NIMHANS is recognized as a nodal centre to co-ordinate the activities of Psychosocial Rehabilitation.NIMHANS has been declared as a Deemed Universitysince 1994.
The functioning of the Institute is governed byNIMHANS Society with the Union Minister for Healthand Family Welfare as President and the Ministerfor Medical Education, Government of Karnataka asits Vice President. The management of the Instituteis done through Board of Management. The otherstatutory bodies of the Institute are the FinanceCommittee, Academic Council, Planning andMonitoring Board, Selection Committee, Board ofStudies, Selection Committee, Grievance RedressalCommittee, Ethics Committee, Building and WorksCommittee and Hospital Management Committee.
DEPARTMENTS: (1) Biophysics, (2) Biostatistics, (3)Clinical Psychology, (4) Epidemiology, (5) HumanGenetics, (6) Mental Health Education, (7)Neuromicrobiology (8) Neuroanaesthesia (9)Neurochemistry (10) Neurology (11) Neuropathology(12) Neurophysiology (13) Neuro Imaging andInterventional Radiology (14) Neurosurgery (15)Neurovirology (16) Nursing (17) Psychiatry (18)Psychiatric and Neurological Rehabilitation (19)Psychiatric Social Work (20) Psychopharmacology(21) Speech Pathology and Audiology, and (22)Ayurvedic Research Unit
Central Facilities (1) Library and Information Centre(2) Biomedical Engineering, (3) Central AnimalResearch Facility (4) Photography & DocumentationCentre (5) Engineering (6) Publication (7)Reesearch.
New Facilities
2-dimension gel electrophoresis system (IEF Cell-BioRad Laboratories) as a common facility to initiateproteomic analysis at the department ofNeurochemistry.
The New Tecnai G2 Spirit Bio-Twin TransmissionElectron Microscope was installed at the departmentof Neuropathology. Many biopsies and researchsamples have been scanned during the year anddigital images were captured.
Introduction of Gap-in-noise (GIN) test and TEN teststo assess cochlear dead regions was introduced atthe department of Speech Pathology and Audiology.
287
ANNUAL REPORT 2008-09
A new outpatient special clinical service called theMetabolic Clinic in Psychiatry has been initiated.This initiative is perhaps first of its kind incontemporary psychiatry practice to address theclinical need of growing metabolic disorders inpsychiatric population. The importance and need forthe clinic is stressed by the observation of significantprevalence of metabolic abnormalities inantipsychotic-naïve schizophrenia patients in aNIMHANS funded study, published recently in theAmerican Journal of Psychiatry 2007. Over the pasttwo months about 20 patients have beensystematically evaluated and are being followed inthis clinic.
Two information kiosks providing information onsubstance use disorders have been installed in theOPD and the Deaddiction centre to educate the publicin this area. These are used with enthusiasm by thepatients, their relatives and visitors.
Upgradation of High Performance Computing (HPC),IBM-Eserver (Linux Cluster, 32 CPU, 64 GB RAM,0.5 TB storage), has been added to ScientificComputation and Modelling facility for common use ofscientists at the department of Psychopharmacology.
New equipments added
1. 64 Channel Digital EEG/ERP system
2. Stereotactic Planning Software
3. Stereotactic Apparatus
4. RT PCR Machine
5. Blood Gas Analyser
6. Ultra Centrifuges
7. Automated Blood Culture System
8. Gel Documentation System
Hospital Services
NIMHANS is an apex secondary and tertiary carehospital in the fields of psychiatry, neurology andneurosurgery, for inpatient and outpatient care ofthe suffering and subsequent neuro-rehabilitation toenter back into society as useful citizens. The instituterenders services to the patients from all over the
country as well as neighbouring developingcountries. It has a bed strength of 874. During theyear 2007-08, patients numbering 377581 havebeen treated.
Teaching and Training
Number of students admitted to various post graduatedegree/diploma, undergraduate courses includingnursing and certificate courses during 2007-08 - 154.
Number of trainees undergone training at theInstitute:- 3311
One-year psychiatry training programme formedical officers
As a part of work force development in Psychiatryfor implementation of National Mental HealthProgramme(NMHP), the Department of Psychiatry,NIMHANS has initiated this psychiatry trainingprogramme to train medical officers of Jammu &Kashmir (6) and Karnataka (6) states. The aim ofthe course was to train the medical officers indiagnostic and clinical management skills with respectto priority mental disorders. The training programmealso aimed to impart skills to function as a trainerand to develop skills for supervising the medicalofficers during the implementation of District MentalHealth Programme (DMHP). During the year, theparticipants were trained to understand the concept,need, and operational details of the DMHP; impartingcommunication, leadership and problem solving skillsrelevant to implementation of DMHP; networking withcommunity, IEC activities, stimulation of self-helpgroups and community participation. Based onresults and feedback for training programme, themodule for one-year training programme formed,which can be implemented in other training institutesto train medical officers in DMHP.
The postgraduate Certificate Course in ForensicPsychology, conducted by the department of MentalHealth and Social Psychology, was changed toinclude fresh postgraduates in psychology andcriminology in addition to the in service sponsoredcandidates. The second batch for the certificatecourse commenced training on 1.2. 08 and the coursewill be completed on 31.1.09.
288
ANNUAL REPORT 2008-09
The Department of Psychiatric Social Work hasinitiated net-working of Schools of Social Work inSouth India and has currently covered Kerala,Karnataka, Tamil Nadu, Andhra Pradesh and North-East Regions. The objectives of these net-workingis to enhance Psychiatric Social Work knowledge andskills among the students of Social Work, introducecommunity based disaster preparedness, mitigationsand management activities, review Psychiatric SocialWork syllabus and incorporate contemporary issuesin the same. A total of 102 Schools of Social Workunder 10 hubs has been created in the last 2 years.Micro level researches have been initiated andsyllabus revision is under consideration by theSchools of Social Work.
Promotion of Neuroscience / Public Awareness
The public in Bangalore has been made aware ofthe usefulness of brain donation as a part of "cadaverorgan donation" programme to promoteneuroscience. During the year, following explicit willof the person, the deceased sons have donated thebrains and spinal cord (one case of parkinsonism,one case of motor neuron disease). In addition anAnglo-Indian couple and their friends, have pledgedtheir brains for research after their demise, keepingthe "brain donation card" in their possession alwaysand informing their close kith and kin of their free willto donate. HBTR at NIMHANS has been accreditedto collect human heart valves for homografttransplantation and to hand over to the licensedcardiothoracic surgery centers authorized byappropriate authority. These heart valves arecollected from cadavers from medico legal autopsies/road traffic accidents, only with written consent ofthe close relatives. Awareness about cadavericorgan donation is increasing in the society.
Conference Presentations
International 125
National 144
Projects
The total number of projects at the Institute is 128(completed - 29, ongoing 94 and newly sanctioned -5).
Projects completed/nearing completion
1. Psychiatric inpatient centre (open wards)The new Psychiatric wing with 126 beds andall integrated services has facilitated patientcare and management for mentally ill. It wasinaugurated by the Hon'ble Health & FamilyWelfare Minister on 2nd September 2008.
2. New building for Department of Psychiatricand Neurological Rehabilitation Centre.Giving equal importance to rehabilitation ofmental and neurological patients, the n e wblock of rehabilitation department offerscomprehensive and advanced services forneedy patients. This was inaugurated by theHon'ble Health & Family Welfare Minister on2nd September 2008.
3. Golden Jubilee emergency servicesblock.The new state of art and round theclock emergency block with a new 20 beddedICU, 3 operation theatres, digital X-ray andSpect CT, laboratory services with 150 bedswith all other supportive services under oneroof will enable the doctors to provideintegratedand comprehensive services to thepatients. This new facility wasinauguratedby the Hon'ble Health & Family WelfareMinister on 2nd September 2008.
4 15 Nos. cottages north block behind specialwards.This has been built to cater to theneeds of the psychiatric patients and allfacilities are provided as well as one attendantcan stay along with the patient.
5. 150KLD sewage water treatment plant.
6. Supply of 750 KVA DG set to HT 4-Substationat Administrative Block.
7. Providing HT power supply through 66/11 KVAMUSs station to individual HT Sub-stat ion(four nos) NIMHANS. This will have anExpress Feeder where there will powersupply for 24 hours without break, therebythe research work at the laboratories, at theOT and the hospital side will be able to
289
ANNUAL REPORT 2008-09
function more efficiently. Major equipmentsat the hospital which require constant powersupply also will not be hampered, due tocontinuous supply of power.
8 Nursing College.Nursing College has alreadybeen constructed. This is an importantrequirement as the nurses trained inpsychiatric nursing form an importantcomponent of the mental health care deliverysystem. At present there is severe shortageof nurses trained in psychiatry in the country.
9 Nurses Hostel for ladies.The Nurses Hostelhas been completed to accommodate thenurse swho are being trained at NIMHANS.
10. Kabini HostelAnnexe to Kabini Hostel hasbeen added to accommodate the increaseof Students intake due to reservation forOBCs. The ground floor and 1st Floor isnearing Completion and an additional threefloors has been planned andsanctionobtained.
11. Centre for Advanced Research inNeurobiologyThe Advanced Research Centrehas been designed for ground + four floors.NIMHANS is contemplating preimplantationgenetics study as a collaborative project withJawaharlal Nehru Centre for AdvancedResearch and Hope Infertility Clinic and alsotaking up molecular medicine center providingdiagnostic facilities for various neurologicaland psychiatric illnesses. It is also proposedto shift common research facilities to thiscentre as "Common Research Facility ".
12. Construction of Academic Block This buildingwill house the Department of Mental Healthand Social Psychology, Psychiatric SocialWork, Health Education. The work is underprogress. The Public Health Centre will alsobe added to this complex.
Infrastructure Development of The Institute
Proposal of the Institute for infrastructuredevelopment for enhancement of student intake by
54% at a cost of Rs.47.39 crore has been approvedby the Government in the current year. The totalnumber of seats in various courses at the Institutewill be increased from 157 to 241. NIMHANS hasalready increased 32 seats so far.
Support for National Mental Health Programme
Allocation for National Mental Health Programme inthe XIth Five Year Plan is Rs.1000 crore. Necessarysupport work is being carried out by NIMHANS forthe restrategised Programme in the XIth Plan.
Disaster Management
NIMHANS, the nodal centre for psychosocial care forsurvivors of disaster in India continues to carry outthe service, training, research, networking, sharingof information and policy development for survivorsof disaster. The tsunami psychosocial care servicesin the States of Tamil Nadu, Andhra Pradesh, Kerala,Andaman and Nicobar Island have entered thepsychosocial rebuilding phase and activities toinstitutionalize the same and withdrawal of activeinvolvement of NIMHANS is in progress. The workwith survivors of Kashmir Earthquake is beinginstitutionalized with the active support of theDepartment of Health and the Government MentalHealth Institutes in Jammu and Kashmir.
Services
The service activities for the survivors of Tsunamihave been intensified to psychosocial rehabilitationand rebuilding in all the three States and the twoUnion Territories of South India. The objectives ofthe current phase were to (i). continuing providingsupport to the trained manpower, monitor the changein the community, (ii). Strengthen the network systemcreated (iii). Strengthen long term care for personswith mental health problem at primary care centreand district hospital psychiatric units and (iv). Promotepsychosocial competencies especially amongchildren.
Nearly 4000 families with about 20,000 individualswere intensively provided psychosocial supportinclusive of a spectrum of care activities. Referralsof severely affected were made to District Hospital

290
ANNUAL REPORT 2008-09
Psychiatric Units. The population in mild andmoderate areas adopted psychosocial care in theirhealth, welfare, education and development worksin the field area. One another notable feature wasinitiation of psychosocial competencies for thechildren and integration of psychosocial care incommunity based disaster preparedness activitiesthat were carried out in Andhra Pradesh and Kerala.Twenty five mental health awareness camps wereorganized in all the severly affected areas of theabove States and Union Territories. The psychosocialcare work continuation in Kerala and AndamanNicobar Islands have been institutionalized throughsetting up CBOs by the CLWs through 'drop incentres' that are currently managed by thecommunity level workers. In the other areas thefunctionaries of the health, education, welfare andNGOs are carrying out the work.
Training
Higher level training programmes through trainingof the trainers programme for twelve batches ofpersonnel were held at NIMHANS. The trainedtrainers were supported to train other staff in theirorganizations. The higher level trainings included,understanding the family dynamics in disasteraffected population, higher counseling skills,psychosocial competency building for children andpsychosocial care in community based disasterpreparedness. Standardized training kits have beendeveloped and made available in South Indianlanguages. NIMHANS has uploaded all the disasterrelated training materials in its website for use byvarious organizations and institutions. Refreshertraining programme for 55 medical officers werecarried out in the three Districts of Tamil Nadu.NIMHANS also provided technical support to theWHO and Department of Psychiatry, Madurai MedicalCollege initiative on training in psychosocial carethrough the Psychiatrist.
Technical support to organizations
NIMHANS as a nodal centre continues to providetechnical support, training expertise and variousother supportive activities to nearly a dozen ofInternational and National organizations in the area
of psychosocial care and mental health services forsurvivors of disaster. Continuity of technical supportis being carried on for the network of schools of socialwork in South India. NIMHANS is slowly spreadingthe technical support services to the SAARC countriestoo.
NIMHANS has signed a Memorandum ofUnderstanding with the National Institute of DisasterManagement, New Delhi to provide psychosocial caretechnical support in the areas of training,development of disaster psychosocial care materialsand research. As a part of this MOU, four trainingprogrammes were conducted during the current yearfor senior administrators at the Central, State, Districtlevel disaster programme managers. A pilotcollaborative project on psychosocial impact ofsurvivors with physical disability has been completedin the Districts of Cuddalore, Nagapattinam,Kanniyakumari and Karaikal. The proceeding of theIndia Disaster Management Congress has beencompiled and is to be released in the second IDMCto be held in the current year.
Research
The long term study on the impact of psychosocialcare for survivors of Tsunami by community levelworkers through the different phases and the largescale provision of psychosocial care in the five districtsof Tamil Nadu and Andhra Pradesh States werefollowed up with a cohort of 150 each randomlyselected individuals. The outcome of the projectrevealed steady decline in impact of the event,distress, and disability among the populationintervened.
Four international journal publications and twochapters in books were made by NIMHANS facultyon Tsunami psychosocial and mental health services.The faculty and staff made two major presentationsin International Conferences held at Hong Kong andMalaysia on the Tsunami psychosocial care issues.
Healing the mind - policy initiatives support toNDMA
Dr. D. Nagaraja, Director/Vice Chancellor of NIMHANSand Dr. K. Sekar, Professor and Head, Department
291
ANNUAL REPORT 2008-09
of Psychiatric Social Work, are members of thesteering committee on psychosocial support andmental health services area for the 'NationalGuidelines on Medical Preparedness and MassCausalities Management' by the National DisasterManagement Authority (NDMA) released by theHon'ble Health & Family Welfare Minister inNovember 2007. Dr. D. Nagaraja and Dr. K. Sekarare also involved as core group members of theNational Disaster Management Authority 'Guidelineson psychosocial support and mental health servicesin disaster.
Psychosocial care for children in difficultcircumstances
While working with children in disaster NIMHANS hasidentified a large number of children and other highrisk groups in the small epicenters in the workingareas who are in need of psychosocial care andsupport on a long term basis. This helped tounderstand the existence of children in difficultcircumstances like children living on streets, childrensubjected to different kinds of abuse, trafficking, childmarriage, child labour, children who are orphans,
semi orphans, disabled, children abusing drug,children in institutions, children in conflict with law,children affected by HIV/Aids, gender discrimination,children in emergency situations etc. In this regardthere is a need to empower NGO workers who aredirectly dealing with children in various types ofdifficult circumstances with basic knowledge and skillsin identifying the psychosocial problems of childrenand the potential causes there by providing thembasic psychosocial care and support at thecommunity level rather than referring them tospecialized hospitals.
In collaboration with NGOs training workshops wereinitiated for various NGOs working with children. Thefocus of training was on the techniques ofpsychosocial care, process of relating with childrenand spectrum of psychosocial development forcomprehensive psychosocial support to children atvarious levels, identification of problems,psychosocial and pharmacological management andreferrals for higher level mental health problems.Following the training program, the trainees wouldbe able to initiate service provision for the childrenin difficult circumstances.
Budgest Estimates for 2008-09
(Rs. In lakhs)
Year Govt. of India Govt. of Karnataka Total
Plan Non-plan Plan Non-plan
2008-09 4300.00 2500.00 55.00 1334.00 8189.00
15.4015.4015.4015.4015.40 National TNational TNational TNational TNational Tuberculosis Institute,uberculosis Institute,uberculosis Institute,uberculosis Institute,uberculosis Institute,BangaloreBangaloreBangaloreBangaloreBangalore
Introduction
National Tuberculosis Institute (NTI), Bangalore is anorganization under the Directorate General of HealthServices, Ministry of Health and Family Welfare,established in 1959 in close collaboration with theWorld Health Organization (WHO) and UNICEF. Thisis a premier Institute in the field of Tuberculosis
control in South East Asia, which caters to the humanresource needs for TB control in the region. Since1985, the institute has been functioning as a WHOCollaborative Centre for Training and Research. Theinstitute is also involved in carrying out OperationsResearch on various components of TB Controlmainly carried out by the epidemiology and controlsection. The Bacteriological wing of the institute hasbeen recognized as a National Reference Laboratoryfor External Quality Assessment in the TB Controlactivity. It also assists in establishing Intermediate
292
ANNUAL REPORT 2008-09
Reference Laboratory for Culture and DrugSensitivity tests, across the country.
The institute has also been identified as the nodalcenter for operational research related to RNTCP.The major activities as a nodal centre is to organizeworkshops, prepare the research agenda anddissemination of research data through publications.
Major Activities Undertaken During the Year
A. Research
The research studies/projects taken up by theInstitute were:
� Nodal centre for carrying TB DiseasePrevalence Survey under RNTCP
� Nodal Centre for Repeat Zonal ARTI Surveys.
� Default and patient retrieval among newsmear positive patients treated in RNTCPunder different geographic and demographicsettings - covers 20 districts from 6 states ofthe country
� District level intervention study on routinereferral of TB patients to VoluntaryCounseling and Testing Centers in Mysoredistrict
� Assessment of RNTCP diagnostic algorithmfor chest symptomatic and smear negativepatients
� Disease Prevalence Study in NelamangalaTaluk
B. Training
The Institute has pioneered in the field of HumanResources Development. It is involved in conductingthe following training programmes to the TBProgramme Managers positioned at different partsof the country.
1. Ten (10) RNTCP & TB-HIV Modular trainingProgramme were conducted at NTI whereSTDCs, STOs, DTOs, MO-TCs and facultyof Medical Colleges participated. One (1)training of trainers was also imparted.
2. Sixty one (61) orientation programmes of oneday duration were organised for about 1850undergraduate Medical, Microbiology andNursing and Pharmacy students sponsoredby different Institutes across the country.
3. External Quality Assessment (EQA) has beengiven importance under RNTCP in the recentyears. Hence, one (1) training on theprocedures of EQA was imparted to theLaboratory personnel of different parts of thecountry. Five (5) training in Culture & DST /Smear Microscopy were imparted toMicrobiologists/Lab technicians.
4. Two (2) training in TB-HIV were imparted toMedical Officers/District TB Assistants.
5. Six (6) WHO sponsored/collaborated trainingwere conducted during the year.
C. Bacteriology Section
1. Operationalise the EQA for sputum smearmicroscopy network in the states inconjunction with /STDCs or IRLs. Carry outNRL responsibilities of EQA such as OnsiteEvaluation (OSE), Panel testing (proficiencytesting of lab staff) to ten states at least oncein a year for 3-4 days (including one to twodistricts visits), and make visits as and whenrequired depending on the priorities/necessity to improve and help theperformance of labs. Five visits of EQA onsite evaluation were undertaken the fivestates. 95 slides were used for panel testingduring the visits
2. Conducting quality improvement workshopsfor the state level programme managers witha view to find solutions to EQA relatedoperational and technical problems faced inthe field.
3. To implement and verify Random BlindedRechecking (RBRC) procedures and improvethe performance of labs based on analysisof the RBRC data in conjunction with STDCs.
4. Capacity building and strengthening the tenstate level TB laboratories (STDCs) with
293
ANNUAL REPORT 2008-09
respect to proficiency in culture and DrugSusceptibility Testing including second linedrugs.
5. Conducting Anti-TB Drug resistancesurveillances of priority states involvingprocessing of representative sample of thestates to obtain information of prevalence ofdrug resistance, with a view to supportlogistics of DOTS - Plus programmes underexpansion of DOTS and RNTCP andconduct/ participate in National Level diseaseprevalence studies/surveys
6. The Lab team of the Institute carries out onsite evaluation of STDC laboratories ofdifferent states and provides necessaryguidelines to establish quality laboratory toundertake EQA and DRS studies.
D. Monitoring Section
With full coverage of RNTCP in the country, theInstitute is not compiling the reports on NTP. Atpresent, the monitoring activity is being carried outby the Central TB Division under DGHS.
E. Publication Activities
The faculty of the Institute published about 3 researchpapers in the leading journals on TB. Fourpresentations on the basis of the research studiesconducted by the Institute were presented in theNational Conference on TB and Chest Diseases.
F. Other Activities
1. The Faculty and the technical staffparticipated in the appraisal and CentralEvaluation of RNTCP districts as and when
called upon to do so and given the technicalsupport for implementation of RNTCP.
2. The scientific gallery was established todisseminate the general information on TBthe evolution of the programme andachievements of the Institute since itsinception.
Considering the needs of various categoriesof trainees, two methods of display units viz.,Photo Display and Projection facility andInformation Kiosk are available.
Participation in meetings, seminars,conferences, workshops and conductingmedical education programmes:
The Director, faculty and the technical staffparticipated in about 20 meetings/seminarsconducted by the Central TB Division and other TBrelated activities.
Upgradation of Infrastructure
Security arrangements of the Institute have beenstrengthened by increasing the height of thecompound wall at certain places and providing chainlinked mesh.
Asphalting of internal roads of the Institute has beentaken up. Few of the guest rooms which were non a/c earlier were converted to a/c rooms. Constructionof garage for new quarters has been taken up.
G. Financial Outlay & Expenditure
The details of budget allocation for NTI during theyear 2007-08 were as follows:
Category Budget estimate Revised estimate(Rs. In Crore) (Rs. In Crore)
Non - Plan 3.25 3.21
PlanRevenue 1.45 1.45
Capital 0.50 0.50
TOTAL 5.20 5.16

294
ANNUAL REPORT 2008-09
15.4115.4115.4115.4115.41 Hospital Services ConsultancyHospital Services ConsultancyHospital Services ConsultancyHospital Services ConsultancyHospital Services ConsultancyCorportioan (Corportioan (Corportioan (Corportioan (Corportioan (HSCCHSCCHSCCHSCCHSCC), India Ltd.), India Ltd.), India Ltd.), India Ltd.), India Ltd.
Background
HSCC was set up in March 1983 as Public SectorEnterprise under the Ministry of Health & FamilyWelfare. As on 31.03.2008, the Authorised Capitalof the Company was Rs.200 lakhs and the Paid-upCapital of the Company was Rs.160.012 lakhs. Inthe year 2008-09 the Authorised Capital of theCompany was increased to Rs.500 lakhs and paid-up Capital was increased to Rs.240 lakhs. This hasresulted by issue of Bonus Shares amounting toRs.80 lakhs during 2008-09. This is in addition tothe earlier bonus shares issued in the year 2003-04amounting to Rs.160 lakhs. HSCC has been a profitmaking Company continuously for the last 24 yearsand has been retaining its 'Mini Ratna' status sinceSeptember 2002. Over the years, HSCC's net worthhas grown to Rs.5864.59 lakhs as on 31st March2008 which is more than 36 times of its paid-upcapital.
Service Spectrum
HSCC is a multi-disciplinary diversed engineering andproject management Company and it is renownedconsultancy management and procurementmanagement service organization in the health careand other social infrastructure development sectors.Its service spectrum covers feasibility studies, designengineering, detailed tender documentation,construction supervision, comprehensive projectmanagement, procurement support services in allareas of civil, electrical, mechanical, informationtechnology and auxiliary medical service areas. Itsimportant clients include
� Ministry of Health & Family Welfare and itsHospitals / Institutes
� Ministry of External Affairs and other Ministries
� State Governments and their Hospitals /Institutes
� Various Institutes
Financial Performance
HSCC celebrated its Silver Jubilee Year in 2007-08with achieving the highest ever total income ofRs.3096.34 lakhs since its inception. The Companyhas declared a dividend of 130% on the paid-upcapital for the year 2007-08. For the year 2008-09,the Company expects to touch a total income ofRs.2980 lakhs (provisional un-audited) and Net Profitin the range of Rs.900 lakhs (provisional un-audited).
Quality System
The Company is "ISO 9001:2000" certified Companyand has internal quality control as required for itsvarious projects and assignments.
Corporate Governance
The Company has engaged the services of a firmfor carrying out an independent internal audit. TheCompany endeavors to maintain good CorporateGovernance practices. Emphasis is being laid in theCompany on observing transparency, accountabilityand proper disclosures.
Recognition
HSCC has been MOU signing Company with theMinistry of Health & Family Welfare and has secured"Excellent" rating for the year 2007-08 and alsoexpects "Excellent" rating for the year 2008-09 basedon its provisional un-audited results.
During the year 2007-08, the Company was awarded"Bhartiya Shiromani Puraskar" and Gold Medal forenhancing the Image of India at a befitting ceremonyorganized by the Institute of Economic Studies inFebruary 2008.
Company's Affairs
HSCC being knowledge management consultancycompany in health infrastructure sector employscompetitive and highly skilled cadre of architects,engineers, Chartered Accountants, CostAccountants, MBAs and a pool of Consultants in theareas of medicines and corporate planning etc.HSCC enjoys a good working employee relationshipat all levels.
295
ANNUAL REPORT 2008-09
HSCC has successfully completed major health careprojects comprising hospital, medical colleges,laboratories etc. at different locations.HSCC iscontinuously aiming to upgrade its knowledge poolby investing in upgradation of its human resourcehaving regular training and establishing strategicalliances with different organizations to offer worldclass consultancy to its diverse clients.
The Company has recently completed the followingprojects:
� Trauma Centre, AIIMS, New Delhi
� PGIMER, Dr. Ram Manohar Lohia Hospital,New Delhi
� VMMC, Safdfarjung, New Delhi
� FDA Bhawan, New Delhi
� Design Engineering of Mother & ChildHospital, Amritsar
� Development of Medical Campus at Faridkot
HSCC is currently involved in many importantprojects, such as :
� AIIMS Master Plan, New Delhi,
� Under Prime Minister's Swasthay SurakshaYojna for :
- Nizam Institute of Medical Sciences,Hyderabad
- Sanjay Gandhi Post-Graduate Institute ofMedical Sciences, Lucknow
- Kolkatta Medical College, Kolkata
� Housing at Bhubaneswar and Raipur,
� Upgradation of Lokpriya Gopinath BardoloiRegional Institute of Mental Health, Tezpur,
� Construction of North Eastern Institute ofAyurveda & Homoeopathy (NEIAH), Shillong,
� Regional Institute of Medical Sciences (RIMS),Imphal,
� General Hospital, Dickoya, Sri Lanka,
� Bir Hospital at Nepal,
� Hospital Complex at Aizwal,
� Expansion of Lady Hardinge Medical College,New Delhi,
� Project Management of Setting up All IndiaMedical Ayurveda Institute at Sarita Vihar,New Delhi,
� Design and Engineering services forEmployees State Insurance Corporation,
� Detailed Project Report - Hospital Complexat Nahar Lagun,
� Preparation of Detailed Project Report forMedical College at Port Blair,
� Many important procurement servicesassigned.
15.4215.4215.4215.4215.42 Setting Up of Setting Up of Setting Up of Setting Up of Setting Up of AIIMSAIIMSAIIMSAIIMSAIIMS lik lik lik lik likeeeeeInstitionsInstitionsInstitionsInstitionsInstitions
Setting up of Six AIIMS-like Institions under 1stPhase of PMSSY
Government of India has approved the PradhanMantri Swasthya Suraksha Yojana (PMSSY) inMarch, 2006 with the objective of correcting regionalimbalance in the availability of affordable/reliabletertiary healthcare services and also to augmentfacilities for quality medical education in the country.Under the PMSSY, it has been decided to set up 6AIIMS-like institutions, one each in the States of Bihar(Patna), Chattisgarh (Raipur), Madhya Pradesh(Bhopal), Orissa (Bhubaneshwar), Rajasthan(Jodhpur) and Uttaranchal (Rishikesh) at anestimated cost of Rs 332 Crores per institution whichis likely to be revised.
Each institution will have a 960 bedded hospital (500beds for the medial college hospital; 300 beds forSpeciality/Super Speciality; 100 beds for ICU/Accidenttrauma; 30 beds for Physical Medicine &Rehabilitation and 30 beds for Ayush ) intended toprovide healthcare facilities in 39 speciality/super-speciality disciplines. Medical College will have 100
296
ANNUAL REPORT 2008-09
UG intake besides facilities for imparting PG/doctoralcourses in various disciplines.
Progress of setting up of six AIIMS-likeinstitutions in the 1st phase of PMSSY
Pre-construction survey and Environment ImpactAssessment (EIA) study conducted. The proposalsfor EIA clearances are being examined by Ministry ofEnvironment & Forests.
Construction of medical college and hospitalcomplex:-
Design DPR Consultants were selected in October-November, 2007 for preparation of designs and DPRfor Medical College & Hospital Complex at eachinstitution. Lay-out/master plans for AIIMS, Bhopal,Rishikesh and Jodhpur were approved by ProjectManagement Committee on 8.1.2008; forBhubaneswar on 20.2.2008; for Raipur on 12.3.2008;and for Patna on 25.3.2008. The architecturaldesigns were evaluated by the faculty of AIIMS/PGIMER for ensuring functional efficiency; TheEnergy Resource Institute (TERI) for green buildingconcept; and Bureau of Energy Efficiency (BEE) forECBC (Energy Conservation Building Codes)compliance. Project Management Committee (PMC)approved preliminary architectural designs for thesites at Bhopal, Jodhpur and Rishikesh on 22.4.2008and for Patna, Raipur and Bhubaneswar on28.5.2008. Project Consultants for all the six siteswere selected in June, 2008.
The Design-DPR Consultants submitted the DetailedProject Reports (DPRs) for all the six sites, whichwere reviewed by the Technical Committee under thisMinistry. The Committee observed that the DPRswere incomplete and all the details as laid down underthe RFP (Request for proposal) have not beensubmitted. Design-DPR Consultants have been askedto submit the complete DPRs, following which wouldbe reviewed by the Project Consultants andthereafter taken up for approval.
Draft DPRs for six AIIMS-like institutions alongwithrevised cost estimates were placed before the PMCon 25.2.2009. Draft DPRs alongwith revised cost
estimates are being submitted to EFC/CCEA for freshapproval.
Construction of residential (housing & hostels)complex for AIIMS-like institutions:-
The bid for selection of EPC Developer was foundsuccessful for only one site, viz. Jodhpur. M/s.Rajasthan State Road Development Corporation,Jaipur has been selected as EPC Developer forJodhpur site. Work at the site started in November,2007 and 50% of the work has completed so far.The date of completion was rescheduled to October,2009. For Bhopal site, it was proposed that the workof preparation of concept and DPR would beexecuted through the Design-DPR Consultant. Forthe other four remaining sites, the work relating toconstruction of residential complex at Rishikesh andPatna was entrusted to HLL and for Bhubaneswarand Raipur to HSCC on nomination basis.Construction agencies for construction of housingcomplex at five sites have been selected throughopen competitive bidding.
The work at Patna, Rishikesh, Bhubaneswar andRaipur sites has been awarded in August, 2008 andthe contractors have mobilized/started civilconstruction at all sites in September, 2008 and thework is expected to be completed by March, 2010.Construction work at Bhopal site has started inNovember, 2008 and is expected to be completedby May, 2010.
Upgradation of 13 medical college institutionsunder PMSSY
The medical college institutions being upgradedunder the 1st phase of PMSSY are as under:-
1. Govt. Medical College, Jammu (J&K)
2. Govt. Medical College, Srinagar (J&K)
3. Kolkatta Medical College, Kolkatta (W.B.)
4. Sanjay Gandhi Post Graduate Institute ofMedical Sciences, Lucknow (U.P)
5. Institute of Medical Sciences, BHU, Varanasi(UP),
297
ANNUAL REPORT 2008-09
6. Nizam Institute of Medical Sciences,Hyderabad(A.P)
7. Sri Venkateshwara Institute of MedicalSciences,Tirupati (A.P) (50% cost ofupgradation will be borne by the TTD Trust)
8. Govt. Medical College, Salem (T.N.)
9. B.J. Medical College, Ahmedabad (Gujarat)
10. Bangalore Medical College, Bangalore(Karnataka)
11. Medical College, Thrivananthapuram,(Kerala)
12. Rajendra Institute of Medical Sciences(RIMS), Ranchi
13. Grants Medical College & Sir J.J. Group OfHospitals, Mumbai, (Maharashtra )
Upgradation of the above institutions was approvedby CCEA on 22.6.2006 except RIMS, Ranchi, forwhich CCEA approval was obtained on 26.4.2007.
The work relating to Project Consultancy andexecution of upgradation of the medical collegeinstitutions has been assigned to M/s. HospitalServices Consultancy Corporation (India) Ltd., M/s.Hindustan Latex Ltd. and CPWD.
Upgradation of the medical college institutionsbroadly envisages strengthening the existingdepartments, through procurement of equipment. Itis also proposed to build a Super Speciality Block,Nursing College, OPD etc. for many of theinstitutions. Out of the 13 medical college institutionsbeing upgraded, 3 medical colleges have onlyprocurement of equipments for existing facilities andthe remaining 10 have both civil work andprocurement components. Civil work has started at9 institutions and for remaining 1 (RIMS, Ranchi)where there is civil work, the tenders are underfinalization. Civil construction work in most of theinstitutions will be completed by the end of 2009.
Progress of civil work:-
� Thiruvananthapuram Medical College:-Work started for construction of 253 bedded
Super Speciality Block in January, 2008 andis progressing as planned. 51% of the workhas so far been completed. It is expected tobe completed by June, 2009.
� Mohan Kumaramangalam GovernmentMedical College, Salem:- Work started for319 bedded Super Speciality Block and 122bedded Trauma Centre in January, 2008.The work is scheduled to be completed byMarch, 2009. Approximately 47% of work hasbeen completed and there has been somedelay in work due to shortage of labour.
� Kolkata Medical College:- Work startedfor construction of OPD and Academic Blockin January, 2008. The work is scheduled tobe completed by March, 2009. 29% of workhas been completed so far and there is somedelay due to services and structures foundin the foundation area, heavy rains and non-removal of existing structure in AcademicBlock. Construction of Super Speciality Blockwill be started thereafter. HSCC, ProjectConsultant has been requested to prepareDPR for SSB.
� SGPGIMS, Lucknow:- Work started forconstruction of 230 bedded Super SpecialityBlock in January, 2008. The work isscheduled to be completed by April, 2009.27% of work has been completed so far andthere is some delay due to delay in gettingclearances for tree cutting and heavy rainfall.
� Jammu Medical College:- Work started forconstruction of 200 bedded Super SpecialityBlock in February, 2008. The work isscheduled to be completed by Sept, 2009.41% of work has been completed. Progressof the work delayed for 2-3 months due tocivil disturbance/agitation in the State.
� Bangalore Medical College:- Workstarted for construction of 203 bedded SuperSpeciality Hospital and Nursing College inJanuary, 2008. The work is scheduled to becompleted by October, 2009. Approximately29% of the work has been completed. There

298
ANNUAL REPORT 2008-09
has been slight delay in progress of work dueto delay in shifting of power cables by theBESCOM authorities.
� NIMS, Hyderabad:- Work started forconstruction of 300 bedded Super SpecialityBlock and 200 bedded Accident (Trauma) &Emergency Hospital in March, 2008. Thework is scheduled to be completed by June,2009. 27% of work has been completed.There has been a slight delay due tounforeseen circumstances such as cutting ofhard rock, restricted entry of materials andtorrential rains.
� Srinagar Medical College:- Work startedfor construction of 200 bedded Trauma CareCentre in March, 2008. 12% of work hasbeen completed. Shortfall is due to civildisturbance/agitation in J&K and non-availability of labour. The work is expectedto be completed by March, 2010.
� IMS, BHU, Varanasi:- Work started forconstruction of 334 bedded Trauma Centrein October, 2008.
� RIMS, Ranchi:- Tenders under finalizationfor construction of 172 bedded SuperSpeciality Block and 68 bedded Oncologyblock.
Procurement of Equipments
� Specification of common and high endequipments for all the departments wasfinalized by Technical SpecificationCommittee.
� Strategy for decentralized procurement ofequipments for the medical collegeinstitutions has been worked out and detailedguidelines to be followed by the institutions/State Governments have been issued inMay, 2008 and also put on MoHFW's website.
� Procurement of low end and uncommonequipment would be made by the beneficiaryinstitutions/State Governments.
� Medical College Institutions/StateGovernments have been asked to executeMoU for release of funds for procurement oflow end equipment. MoUs are yet to beexecuted.
� Advance payment for procurement ofequipment was made to Trivandrum MedicalCollege, SGPGI, Lucknow, Grants MedicalCollege, Mumbai, BJ Medical College,Ahmedabad and SVIMS, Tirupati.
� In the case of procurement of common andhigh end equipment, MoHFW, through HLL,would carry out central procurement ofequipment for obtaining benefits of scale.
� Integrated Purchase Committee (IPC)approved Centralized procurement ofcommon and high end equipment forRadiology and Trauma departments on 10thNovember, 2008 and Cardiologydepartment on 5th December, 2008. HLL,Procurement Consultant is in the process ofissuing Letters of award to suppliers.
� Bid Process for other equipment will becompleted by June, 2009.
2nd phase of PMSSY
Cabinet, in its meeting held on 5.2.2009, approvedthe proposal for setting up of 2 more AIIMS-likeinstitutions, one each in the State of Uttar Pradeshand West Bengal at an estimated cost of Rs.823crore each and upgradation of the following 5 existingGovernment medical college institutions at anestimated cost of Rs.150 Cr.
- Government Medical College, Amritsar,Punjab;
- Government Medical College, Tanda,Hmachal Pradesh;
- Government Medical College, Madurai, TamilNadu;
- Government Medical College, Nagpur,Maharashtra and
299
ANNUAL REPORT 2008-09
- Jawaharlal Nehru Medical College of AligarhMuslim University, Aligarh.
In addition, Cabinet has also accorded 'in principle'approval for upgradation of Government MedicalCollege in Haryana, subject to the State Governmentfulfilling its obligations and terms and conditionsbeing firmed up and submitted for approval of thePrime Minister after inter-ministerial consultations.Haryana Government has now identified Pandit B.D.Sharma Postgraduate Institute of Medical Sciences,Rohtak for upgradation and also committed tofulfilling all its obligations as envisaged under thescheme.
Upgradation of each medical college institution willbe at an estimated cost of Rs.150 Crores, out ofwhich Central Government will contribute Rs.125 Cr.and a minimum amount of Rs.25 crore will be borneby the respective State Governments. In respect ofAligarh Muslim University, Rs.25 crore will be providedby Ministry of Human Resource Development.
15.4315.4315.4315.4315.43 International Institute forInternational Institute forInternational Institute forInternational Institute forInternational Institute forPopulation Sciences (Population Sciences (Population Sciences (Population Sciences (Population Sciences (IIPSIIPSIIPSIIPSIIPS)))))MumbaiMumbaiMumbaiMumbaiMumbai
Introduction
International Institute for Population Sciences,Mumbai, was established in 1956 as the DemographicTraining and Research Centre. The Institute is a"Deemed University" functioning under theadministrative control of the Ministry of Health andFamily Welfare, to impart training, conduct researchand provide consultancy services in the field ofPopulation Studies. The Institute has six departmentsviz. Department of Mathematical Demography andStatistics, Department of Fertility Studies, Departmentof Public Health and Mortality Studies, Departmentof Migration and Urban Studies, Department ofPopulation Policies and Programmes, andDepartment of Development Studies. In addition,Department of Extra Mural Studies is functioning sinceAugust 1993 on yearly project basis. Apart from theDirector & Senior Professor, the faculty consists of33 members, who are engaged in both teaching andresearch.
Training
During the year 2007-08, the Institute offered thefollowing five regular courses:- (a) Diploma inPopulation Studies (DPS), (b) Diploma in HealthPromotion Education (DHPE), (c) Post GraduateDiploma in Community Healthcare (PGDCH), (d)Master of Population Studies (MPS), and (e) Masterof Philosophy in Population Studies (M.Phil.). Thecourses, (a), (b) and (d) are of one year duration,the course (c) is of fifteen months duration, and thecourse (e) is of eighteen months duration. Apart fromthe above regular courses, the Institute also offersMaster of Population Studies (MPS) and Diploma inPopulation Studies (DPS) through correspondence.
Short-term training/instructional courses
The following short-term training programmes wereorganized at the institute during the year 2007-2008.These short-term training programmes areconducted either at the request of funding institutionsor as part of resource mobilisation academicactivities.
1. Two week training programme on "Applicationof Qualitative Methods of Data Collection inPopulation Research". 18-29 June, 2007.
2. One month training programme on"Demography, Gender and ReproductiveHealth" for the participants from NordicCountries (Sweden, Denmerk, Finland,Norway and Iceland). 8th July - 5th August,2007.
3. Two week training programme on "LargeScale Sample Surveys in Demographic andHealth Research" 11-23 February, 2008.
4. One week training programme on'Construction of Life-Tables and PopulationProjections' for the probationers of IndianStatistical Service. 24-28 March, 2008.
Study Tour
As an integrated part of Diploma in PopulationStudies (DPS) and Master in Population Studies(MPS) courses students were taken for study tour to

300
ANNUAL REPORT 2008-09
get acquainted with the academic and researchactivities of various institutions. The Study tour ofDPS and MPS students for the current academic year(2007-2008) was undertaken during 15-31 March,2008. The teak left Mumbai for Dehradun on 15thMarch, 2008. During 17-19 March, 2008 the studentsactiviely participated in the National conference on"Population, Environment and Development inUttarakhand" which was being organized by IIPS,Mumbai in Dehradun. They also visited local scenicplaces like Mussoorie, Haridwar and Rishikesh, etc.The students were in Delhi during 20-25 March,2008. During this period, they visited Ministry ofHealth and Family Welfare, National Institute of Healthand Family Welfare, Registrar General and CensusCommissioner of India, AC Nelson-ORG ResearchPvt. Ltd., TNS India, Institute for Economic Growth,UNFPA and Jawaharlal Nehru University and werebriefed by the respective organizations about theiractivities. The students visited Punjab University,especially the PRC and the Dept. of Geography inChandigarh and were briefed about their activities.They also visited the Centre for Research in Ruraland Industrial Development (CRRID) which is anICSSR funded research organization during 26-27March, 2008. The students were taken to Amritsarduring 27-29 March, 2008. They visited the Dept. ofUrban Planning and the Dept. of Economics in GuruNanak Dev University.
Research
The Institute had completed 4 Research Projectsduring 2007-2008. There are 20 on-going researchprojects, which were initiated during the year 2006-2007 and are in different stages of completion. Also,4 new research projects are being taken up duringthe year 2007-2008. There are 11 on-going researchproject funded by the outside agencies. The mostprominent among them are the National Family HealthSurvey (NFHS), District Level Household Survey underReproductive and Child Health project (DLHS-RCH)and YOUTH in India. The Institute has undertaken onenew project funded by outside agency
Consultancy Services:
During the year the Institute provided consultancy
services to various institutions in India in the field ofPopulation.
Publications
The institute brings out a quarterly Newsletter, whichpublishes information about various ongoing activitiesof the Institute. During the year 2007 08, the institutepublished two issues covering four numbers of IIPSNews Letter.
Library
The Institute maintains an excellent library with mostrecent books on population and related topics. Thereare 77885 books, 13285 bound periodicals and16063 reprints in the library. The library receivesabout 325 Indian, as well as foreign journals out ofwhich 200 journals were received by way ofsubscription and another 125 journals were receivedas gift/exchange. The library also receives largenumber of documents in electronic mode. The libraryhas books on different disciplines such asDemography, Statistics, Public Health, FamilyPlanning, Mathematics, Economics, Sociology,Psychology, Health Education, Politics, Geography,Computer Programming etc. published by UnionGovernment, State Governments, Corporate Bodies,International Agencies and Commercial Publishersof India as well as abroad.
The library subscribe following online databases:
(i) www.indiastat.com
(ii) www.scopus.com
(iii) www.sciencedirect.com
(iv) www.jstor.org
The library provides content indexing, abstracting,current awareness services, selective disseminationservices, documentation, reference, inter-library loanand xeroxing facilities. Guided computerised searchfacilities are extended to faculty/students on theirtopic of research interest. As on date all documentshave been computerized.
The major activities of digitalization of (old) Indiancensus volumes to explore the INFLIBNET services

301
ANNUAL REPORT 2008-09
with introduction of RFID technology will take shapein near future.
Computer Centre
The Computer Center of the institute is well equippedwith the latest computers and statistical softwarerequired for data analysis. The computer center ishaving the one main classroom/lab room with 36Pentium - IV and higher generation computers andthe softwares installed on these computers are SPSS,STATA, Spectrum , Mortpac and GIS which are usedby the research scholars and students for analyzingtheir research data. Of the 36 computers, 12computers are configured for internet access. TheComputer center is having a Network attachedstorage (Nasstor) server which stores the data fromCensus, NFHS, RCH , etc. and the one mail serverfor providing the internal email facility to the institute.To meet the requirement of Internet facility in theinstitute computer center has a 1 Mbps Leased Lineconnection which is distributed among the differentusers through Local Area Network. To secure theinternet access Fortigate Firewall is installed in thecomputer center.
Recently a second class room has been establishedin the computer center with 14 first generationcomputers to meet the requirement to run the ShortTerm courses and regular classes simultaneously.This second class room can also be used bystudents and research scholars for their researchdata entry and analysis.
Data Centre
The Data center of the institute acquired the datasets of Census of 1991 and 2001, National FamilyHealth Survey 1 & 2 , RCH ( Round 1 ) andDemographic Health Surveys ( DHS ) and NationalSample Survey (NSS) data on CD -ROM media, whichare sold to the researchers. E-book in the CD-ROMmedia containing the full papers of DPS/MPS/M.Phillstudents' seminar has been prepared and six e-books on topics related to the reproductive health ,child and maternal mortality are also prepared.
At present, the users are directly accessingresources such as Demographic data sets and
POPLINE databases, which are stored on server.Further server based software like GIS and OPAC(Library Information) can be accessed throughcampus network including the internet.
Observance of World Population Day:
The World Population Day for the year 2007 wasobserved at the Institute on 11th July, 2007. A halfday symposium on "Challenges of UrbanDevelopment" was organized.
Founders Day
On the occasion of `Founders Day' Institutecelebrated `Cultural Evening' on August 14, 2007.
Annual Sports Week
During this academic year, the IIPS Annual SportsMeet was convened during January 2007 with funfair.A number of sports activities comprising both indoorand outdoor games were organized. Students, staffand faculty members participated in the even veryenthusiastically.
Notable Achievements of the Institute
National Family Health Survey-3:
The third National Family Health Survey, 2005-06(NFHS-3) is currently in the last phase. NFHS-3 iscarried under the stewardship of the Ministry ofHealth and Family Welfare (MOHFW), Governmentof India. The International Institute for PopulationSciences has been appointed as the nodal agencyresponsible for coordinating the project. MacroInternational, USA is providing the technicalassistance for the project, and USAID, UNICEF, DFID,the Gates Foundation, UNFPA, and Government ofIndia are funding the NFHS-3. The survey providesstate level estimates of demographic and healthindicators by urban/rural residence.
District level household project underReproductive and Child Health (RCH) project &Facility survey-3, India
Project coordinators: Prof L.Ladu singh, Dr. b.Paswan, Dr. Sayeed Unisa, Dr. Rajiva Prasad, Dr.T.V.Sekher and Dr. Chander Shekhar.
302
ANNUAL REPORT 2008-09
Introduction:
The District Level Household and Facility Survey(DLHS) was initiated in 2007 with a view to assessthe utilization of services provided by governmenthealth care facilities and people's perception aboutthe quality of services. The DLHS -3 is designed toprovide estimates on important indicators onmaternal and child health, family planning and otherreproductive health services.
DLHS-3 covered about seven lakh samplehouseholds from 611 districts of the country.
Progress :-
1) The data collection work has been completedin all states except Arunachal Pradesh andNagaland.
2) The National Level Dissemination Seminarwas organized at New Delhi on 8th December,2008. The DLHS-3 results of 27 States andUTs (including 15 states of Phase-I and 12states of Phase-II) were presented in theSeminar.
3) The District Level Fact Sheets of all States(15 States) of Phase-I have been printed andwe have started distribution of Fact Sheets.
4) The State Level Fact Sheets of all States (15States) of Phase-I have been printed and wehave started distribution of Fact Sheets.
5) The preparation and printing of District Leveland State Level Fact Sheets of the remainingStates are in progress.
6) The first Policy Brief highlighting thepreliminary findings of 15 states (Phase I) waspublished in September, 2008.
7) The first State Level Report of DLHS-3 willbe printed in February, 2009. The printedreports of all the states will be ready by June,2009.
8) We have planned to bring out the NationalLevel Report of DLHS-3 by July, 2009.
9) The State Level Dissemination Seminars forPunjab and Haryana have been scheduledon 5th March, 2009 at Chandigarh. The StateLevel Seminars for the remaining States hasbeen planned from March to July, 2009.
10) The National Level and State Level wall chartswill be printed by July, 2009.
11) The DLHS website (www.rchiips.org) hasbeen launched. All the details of DLHS-3,including questionnaires, manuals, factsheets at state and district levels, policy briefscan be accessed from this website. DLHS-3information is also available on the websiteof Ministry of Health and Family Welfare,Govt. of India.
Youth in India: situation and needs study
The Institute is collaboration with the PopulationCouncil has undertaken a pioneering research todocument young people's transition to adulthood insix states namely Maharashtra, Andhra Pradesh,Tamil Nadu, Rajasthan, Jharkhand and Bihar. Bothqualitative and quantitative approaches are usedcovering behaviors and experiences ranging fromschooling to marriage and sexual behavior. Genderrole attitudes and relations with parents will also bestudied. The MacArthur and Packard Foundationsprovide the funding for this project.
Strengthening state plans for humandevelopment (SPHD)
Seminar organized at IIPS
The International Institute for Population Sciences(IIPS) with financial assistance from UNDP, New Delhiand UNFPA, New Delhi organized a two-days seminaron Exploring Key Measurement Issues in MillenniumDevelopment Goals in Districts in India" during 12-13 December, 2008 at IIPS, Mumbai. A total of 125delegates attended the seminar. In all, 24 paperswere presented in six technical sessions. Dr. N.Tumkaya, UNFPA country representative, India, wasthe Chief guest and Dr. Ashish Bose delivered thekey note address at the seminar.
303
ANNUAL REPORT 2008-09
Global Adult Tobacco Survey (GATS)
The project is sponsored by the Ministry of Healthand Family Welfare, Government of India and WHOSEARO, New Delhi with technical support from CDC,Atlanta, U.S.A and Research Triangle Institute (RTI),North Carolina.
The specific objectives of GATS-India are asfollows:
� Provide estimates of the levels of tobaccouse, and smoking, second hand exposure,and cessation attempts among men andwomen separately for urban and rural areasof India, a country as a whole.
� Provide estimates of the levels of tobaccouse, and smoking, second hand exposure,cessation attempts among men and womenin each geographical region for urban andrural areas.
� Provide estimates of the levels of tobaccouse, and smoking, second hand exposure,cessation attempts among men and womenfor all 29 states and two Union Territories.
� Provide estimates of the levels of tobaccouse, and smoking, second hand exposure,cessation attempts among men and womenby selected background characteristics atnational, and regional level
ENVIS Centre on Population and Environment
The Ministry of Environment and Forests,Government of India under the EnvironmentalInformation System (ENVIS) Centre on populationand Environment at IIPS. The centre collects,collates and disseminates data on various aspectsof population and environment relationship such aspopulation growth and land use, urbanisation andair pollution, household environment and morbidityand mortality etc. The centre maintains a websitehttp://www.iipsenvis.nic.in connected to NIC server.
Longitudinal Ageing Study in India (LASI - Pilot)Project
The International Institute for Population Sciences,Mumbai and the Harvard School of Public Health are
undertaking a collaborative study entitled,'Longitudinal Ageing Study in India (LASI)
The short-term goal of LASI is to carry out a pilotsurvey to assess the health and wellbeing of theelderly population in Karnataka, Kerala, Punjab andRajasthan in India. The timeline for pilot survey isOctober 2008-December 2010.
LASI-pilot is funded by the National Institute on Agingof the United States National Institutes of Health andNational Institute of Ageing (NIA) of the nationalInstitute of Health, USA.
Study of global Ageing and Adult (SAGE) - India2007
The International Institute for Population Sciences,Mumbai in collaboration with the World Healthorganization, Geneva is undertaking the Study onGlobal Ageing and Adult Health (SAGE), 2007 in India.SAGE is part of global longitudinal studyimplemented in six countries - China, India, Ghana,Mexico, Russia and South Africa. In India, SAGE isbeing conducted in six states - Assam, Karnataka,Maharashtra, Rajasthan, Uttar Pradesh and WestBengal. SAGE will cover a sample of 10600households across the six states.
The primary objective of SAGE is to assess healthand well-being of the elderly persons in age 50 andabove and their social determinants.
Funding for SAGE is being provided by the WorldHealth Organization, Geneva and USAID, New Delhi.
15.4415.4415.4415.4415.44 Family WFamily WFamily WFamily WFamily Welfare Telfare Telfare Telfare Telfare Training andraining andraining andraining andraining andResearch Centre (Research Centre (Research Centre (Research Centre (Research Centre (FWTRCFWTRCFWTRCFWTRCFWTRC),),),),),MumbaiMumbaiMumbaiMumbaiMumbai
Family Welfare Training and Research Centre,(F.W.T. & R.C.) Mumbai is a Central Training Institute,responsible for in service training in the key healthareas for different categories of health personnel allover the Country Training related to Primary HealthCare, Family Welfare, R.CH.,HIV/AIDS and otherintegrated National Health Programmes imparted tovarious categories of health professionals of state &district levels i.e. DHOs, DEMOs, Key trainers etc.
304
ANNUAL REPORT 2008-09
Apart from training, Centre is also involved incommunity-based Research Work in the field ofHealth & FW., Population, AIDS etc. in rural as wellas in the urban areas.
During the year 2008-09, following trainingprogrammes were organized.
Contact Classes
Centre has been identified by National Institute ofHealth & Family Welfare for conducting contactclasses on " Certificate Course in Health & F.W.Management " and " Hospital Management" throughdistance learning for the students of thepostgraduate.
Training Programme on IEC/BCC For D.E.M.O.S:-
A training programme on IEC/BCC for the D.E.M.Os.from the State Govt. of Maharashtra and BMC,working in different districts of Maharashtra andMumbai was conducted at FWTRC, Mumbai on 21stto 23rd Nov., 2007. The objective of the programmewas to enable the participants to plan, implement,monitor and supervise the district level IEC activities.
Two training programmes on IEC/BCC was alsoorganized for DEMOs from the State Governmentworking in different districts on Maharashtra, AndhraPradesh and Goa from -
i) 23rd to 25th April, 2008 and
ii) 28th to 30th April, 2008
W.H.O. Fellow Ship Programe:-
Centre has been identified by WHO and Ministry ofHealth and Family Welfare, New Delhi as acollaborative Institute for conducting trainingprogrammes for international students under theWHO Fellowship programme. During the year 2008W.H.O. fellowship training programme has beenconducted in the filed "Reproductive HealthProgramme Management" from 10th Nov., to 28thNov.,2008 for 2 Fellows from MALE.
A programme on "Programme Management inPopulation & Reproductive Health Research" from
10th Nov., to 19th Dec.,2008 for 3 Fellows from Koreahas also been conducted.
Diploma In Community Health Care:-
With the launch of Government of India's NationalRural Health Mission and the present health careServices, the Centre proposed to start a Post-graduate Diploma in Community Health Care.
Clinical Services:-
Service delivery to mother and Children Continuedat the Centre during the year 2008-09, though itsclinic and Laboratory, Medical and Health Careservice were delivered to the patients attended theclinics during the year.
Looking towards the future developments of theInstitute and organizing more and more trainingprogrammes for medical and para medical personnelto deliver better health care service, it has beenproposed to shift this Institute to a new Institutionalpremises at New Panvel, Navi Mumbai. With this view,a piece of land admeasuring 5000 Sq. Mtrs. For theconstruction of office premises, with traininginfrastructure including hostel has been purchasedto shift the activities of the Institute to a new premises.A Piece of land measuring 1700 sq. mtrs. has alsobeen purchased for residential purpose, near theInstitutional complex at Navi Mumbai.
15.4515.4515.4515.4515.45 National Institute of Health andNational Institute of Health andNational Institute of Health andNational Institute of Health andNational Institute of Health andFamily WFamily WFamily WFamily WFamily Welfare (elfare (elfare (elfare (elfare (NIHFWNIHFWNIHFWNIHFWNIHFW), New), New), New), New), NewDelhiDelhiDelhiDelhiDelhi
The National Institute of Health and Family Welfare(NIHFW) is an autonomous, apex technical instituteunder Ministry of Health and Family Welfare,Government of India working for the promotion ofPublic Health in the country. Our vision is to be seenas an Institute of Global repute in public health andfamily welfare management & Mission is to act asthink tank, catalyst & innovator for management ofpublic health and related health & family welfareprogrammes by pursuing multiple functions ofEducation & Training, Research & Evaluation,Consultancy & Advisory services as well as provisionof specialized services through inter-disciplinaryteams. The thrust areas are Health & related Policies,

305
ANNUAL REPORT 2008-09
Public Health Management, Health Sector Reforms,Health Economics & Financing, PopulationOptimization, Reproductive Health, HospitalManagement, Communication for Health and TrainingTechnology in Health. The areas of concern are RuralHealth (Theme 2005: National Rural Health Mission),Health of Urban Slum Dwellers, Tribal Health,Decentralization, Inter & Intersectoral Coordination,Community Ownership, NGOs, Public-PrivatePartnership, Human Resources for Health, FinancialManagement, Social/ Community Health Insurance,Care of Elderly, Gender Sensitivity & Care of GirlChild, Adolescent Health, Emergency Contraception,Population Education, Medical Ethics, HealthLegislations, Medical Waste Management, HMIS,Health Informatics.
Major Committees
Governing Body
The major responsibility for management of theInstitute's affairs has been entrusted with theGoverning Body, constituted under the Chairmanshipof the Honourable Union Minister for Health andFamily Welfare and Director of the Institute acts asits member secretary.
Standing Finance Committee
This is another important committee, which deals withthe financial matters of the Institute. This committeefunctions under the chairmanship of the Secretary,Health & Family Welfare, Ministry of Health and FamilyWelfare, Government of India. Director of theInstitute acts as the member secretary of thiscommittee.
Programme Advisory Committee
NIHFW has a Programme Advisory Committee toreview various activities in regard to education andtraining, research and evaluation, specializedprojects and consortium activities etc. The committeenormally meets at least once or twice in a year. Theexperts of the committee represents variousdisciplines who are drawn from Central and StateGovernments as well as from Central and StateLevels Training Institutes, either directly or indirectly
involved in the promotion of health and family welfareprogrammes in the country. The Director, Instituteof Health Management Research, Jaipur is currentlychairman of the Programme Advisory Committee.
Educational Activities
Teaching Activities:
The educational activities of the Institute are plannedto impart basic education and promote academicexcellence in the areas having a bearing on thehealth and family welfare programmes in the country.The educational activieres include the following:
M.D. inCommunity Health Administration, Diploma inHealth Administration, Post Graduate CertificateCourse in 'Health and Family Welfare Management,Post Graduate Certificate Course in HospitalManagement, Post graduate Diploma in Public HealthManagement, Ph.D. Programme, Summer Training.
Training Activities (Institute's Funded)
Training of in-service health personnel of variouscategories has been the major mandate of theInstitute. NIHFW conducts various short term trainingcourses, ranging from one to ten weeks duration.70 training courses and 15 workshops for variouscategories of health personnel have been organizedin the year 2008-2009. More than 2000 participantswere trained across the country. The areas coveredare on RCH, monitoring and evaluation, humanresource management, health sector reforms, publichealth management, use of medical bio-statisticalsoftware and use of software for GeographicalInformation System, Professional Development ofSenior District Medical Officers, public health nutrition,counseling and quantitative and qualitative researchmethodology. WHO sponsored candidates alsoattended the training.
Professional Development Course
NIHFW is also conducting a ten weeksProfessional Development Course forManagement, Public Health & Health Sector Reformsfor District Level Medical Officer funded by MOHFWwas started with the objective of training middle levelmedical officers with 12-16 years of services, to be
306
ANNUAL REPORT 2008-09
able to function effectively for service delivery. Thisintegrated training incorporates management, publichealth ongoing reforms in the country including theNHRM in a ten weeks programme.
Strengthening Training in Public Health withInternational Collaboration
To address an impending need for capacitydevelopment of NIHFW faculty and subsequently thehealth professionals at various levels, and tostrengthen the public health services in the country,the Institute entered into collaboration with variousinternational agencies. These include Harvard Schoolof Public Health, World Health Organization (WHO),UNICEF, UNAIDS, UNFPA, WBI, USAID, DFID, GTZ,Partners in Population and Development (PPD),SEAPHEN and INCLEN. These collaborativeventures were preceded by the Director's visit toWorld Bank Institute at Washington DC and HarvardSchool of Public Health, Boston, USA to negotiateon the partnership deals.
Research and Evaluation
The Institute gives priority to research in differentaspects of health and family welfare. Most of theresearch studies are initiated by the Institute, whilea few of the projects are sponsored by the Ministryof Health and Family Welfare and other collaboratingNational and International agencies. In the year 2008-2009, Institute was engaged in 39 studies in all, ofwhich 24 have been completed: 9 under MD (CHA)programme, 12 under Rapid Appraisal of HealthInterventions (RAHI) project and remaining 15,including 9 under MD (CHA) Programme are atdifferent stages of execution.
New Initiatives in Research Studies
In the year 2008-09, many new initiatives have beentaken of which national and International partnershipsand collaborations have been the significant initiativestaken by the NIHFW:
Rapid Appraisal of Health Interventions (RAHI-I) was a unique initiative taken in the year 2007-08under the wider umbrella of 'Public Health Educationand Research Consortium (PHERC)' of the National
Institute of Health and Family Welfare (NIHFW) fordeveloping partnership with different organizationsworking in the field of health and family welfare. Inthe first phase of RAHI project, the United NationsPopulation Fund (UNFPA) India office supported 12health system research projects to bring closeracademia and district health system in order to findout the gaps and solutions at State/District HealthSystem and Sub-system. In the first phase, 5 lowperforming States of India were included under thisinitiative. Initially, proposals were invited from MedicalColleges, NGOs and other health institutions. Afterrigorous screening of the proposals by the TechnicalAdvisory Committee consisting of eminent publichealth experts, 12 projects were finalized in a nationalworkshop conducted at NIHFW. All 12 projects havebeen completed. In the year 2008-09, 12 moreprojects were undertaken which are at the final stageof completion.
Technology Development in Reproductive Bio-medicine was a great milestone of the year. ThermoStable Elisa Kits and Laboratory Kits for testingSperm Functions were developed by our scientists,and the same were handed over to the NationalResearch Development Cooperation (NRDC) forcommercialization. In the year 2008-09, two patentsare granted by the Indian patent Office.
Establishment of New Centres
� The National Child Health Resource Centre(NCHRC) has been established at the NIHFWwith the approval from the Ministry of Healthand Family Welfare, Government of India andwith financial support from NIPI-UNOPS.Norway-India Partnership Initiative (NIPI) is acommitment of the Government of India andthe Government of Norway to collaboratetowards reduction of childhood mortality inIndia to achieve the MDG 4 (Reduce by two-third the mortality rate among children underfive years). A multi speciality team i.e.Paediatrician, IT professional and Nutritionconsultant is working for the aboveprogramme.
� NIHFW established the eighth ClinicalEpidemiology Unit in the current year.
307
ANNUAL REPORT 2008-09
IndiaCLEN is a cluster of seven regional,clinical and epidemiology units that aremembers of the International ClinicalEpidemiology Network (INCLEN) and arehoused in medical schools.
� With WHO support, a Health Financing Unitwas established to strengthen the researchfor devising appropriate implementationstrategies related to health financing andhealth insurance in India in the year 2008-2009.
� The World Bank Institute, Washington iscollaborating with NIHFW to start Web BasedPost Graduate Certificate Course in HospitalManagement through Blended Learningmode. Also video conferencing facility isdeveloped at NIHFW with the technicalsupport from GDLN (World Bank Institute).
� Online resource Centre has been started byNIHFW-WBI Initiative.
Workshops
� The Partners in Population and Development(PPD) South - South collaboration has 24countries of which Hon'ble Union of Healthand Family Welfare, India is the Chairman.It has three regions National Institute ofHealth and Family Welfare is the NodalInstitute to execute the various programmesand activities under PPD in Asian region. Ataskforce for the same has been constitutedat the Ministry of Health and Family Welfare,Govt. Of India and Joint Secretary (RCH) isthe Chairperson for the same with theSecretariat at NIHFW. A national workshopon "National Support for South - SouthCooperation in Population and Development"was jointly organized by Partners inPopulation and Development, Dhaka,Bangladesh, MOHFW and NIHFW on 11thDecember, 2008
� The Institute organized a BrainstormingMeeting for the 'Mahila Sarpanch' for activeinvolvement of Panchayati Raj Institutions
(PRIs) in the Population Stabilization incollaboration with 'Jan Sankhaya SthirthaKosh' (JSK). The meeting generated a lot ofissues of concern and action areas for themahila sarpanches who attended thismeeting under the leadership of Ms. ShailejaChandra, Executive Director, JSK.
� NIHFW in collaboration with A2Z, theMicronutrient project, USAID, organized aworkshop on 'Child Anaemia' at the instituteon 6 February, 2008.
Networking for Public Health
'Public Health Education and Research Consortium- Network and Partnership has been developed withthe objective of sharing experiences and promotingpublic health in the country. The consortium includes173 Medical Colleges, 94 Nursing Colleges, 26SIHFWs/CTIs and 65 NGOs and the number iscontinuously increasing.
Distinguished Visitors
The Institute had the privilege of receiving thedistinguished visitors from Harvard School of PublicHealth, Boston, USA and the Executive Director,Partners in Population and Development (PPD),Dhaka, Bangladesh during the year. Guest lectureswere organized during the last year by the eminentscholars coming for as part of US projects to India.
Clinical Services
The Institute has a long history and reputation asone of the centres in the area of reproductive healthresearch. The laboratory facilities for an in-depthinvestigation for the causes for the reproductivedisorders such as endocrinological, anatomical/surgical, genetic and others are provided to thepatients. The scientific approaches adopted in themanagement of endocrinological and reproductivedisorders and infertility management have paid richdividends.
Management of Infertility: In the diagnosis andmanagement of reproductive disorders newerapproaches are underway in the Institute. Theservices on ante-natal care, immunization, iron and
308
ANNUAL REPORT 2008-09
folic acid, vitamin A supplementation, etc. areprovided to the patients by the Institute.
Family Planning Services: The Institute organizedNSV camp in which 72 men had undergone theoperation. All spacing methods contraceptives areprovided at the clinic. Counselling of couples foradoption of appropriate methods of family planningmethods is also done in the clinic.
Adolescents and Youth Clinic: Adolescents andyouth have special needs. They require guidanceand help for adoption of healthy life style. Theadolescents and youth clinic of the Institute, providesinformation, counselling and other services relatedto their reproductive health needs in a friendlyatmosphere. This clinic functions on every Tuesdayfrom 2.00PM to 4.00 PM.
Clinical Laboratory Services: The laboratoryservices form backbone of preventive and curativeaspects of health care services. Five laboratoriesnamely, routine test (haematology and urine),andrology, semenology, bio-chemistry and serologyhave been functioning in addition to a central facilityfor blood sample collection. These services areprovided to the patients at a nominal charge. Inaddition, services for ABO, Rh, blood groups andmalaria parasites are also provided. A total of 65H.S.G., 1939 Ultrasounds, 7 X-Ray, 74 TesticularFNAC and 101 Endometrial Biopsy were done in theLabs of the clinic.
National Nodal Agency for Specialized Projectsof MOHFW:
NIHFW has been identified by the Ministry of Healthand Family Welfare as the Nodal Institute forcoordinating in-service training under 'NRHM/RCH-II', supervision, analysis and 'Annual SentinelSurveillance for HIV Infection'.
Training Activities under NRHM/RCH-II Project
National Institute of Health & Family Welfare (NIHFW),was designated by the Government of India inDecember, 1997 as the National Nodal Agency fortraining under the RCH programme. Since 2006,NIHFW has been designated as the National Nodal
Agency for training under NRHM. It has pursued theresponsibility of coordinating and monitoring thetraining activities under both RCH & Diseases ofprogramme with the help of 18 Collaborating TrainingInstitutions (CTIs) in various parts of the country. Themajor activities of NIHFW have been:
� Development of training material andguidelines for training
� Training of Trainers
� Monitoring of training activities- physical andfinancial
� Development of National Training strategy forin-service training under NRHM
Annual Sentinel Surveillance for HIV Infection
The Annual Sentinel Surveillance started in 1998 andNIHFW since then has been shouldering theresponsibility of supervision, monitoring for ensuringdata quality, data collection analysis andinterpretation to prepare a country report every yearon behalf of NACO. The surveillance activity followsthe strategy of "unlinked anonymous" and data arecollected from sentinel sites situated in each states,for the high risk groups based on 250 STD patients/sentinel site and low risk group of 400 antenatalcases/sentinel site. Data is collected from about 1134sentinel sites. The task of supervision is shared by 5Regional Institutes. RCTs who monitor the stateassigned to each team under the coordination ofNIHFW and submit a state report to the respectiveState AIDS Control Societies and NIHFW at the endof the surveillance period. The M&E Officers and dataentry operators have been trained by NIHFW on theweb based software for data entry & analysisdeveloped by this Institute. NIHFW in cooperationwith ICMR's National Institute for Medical Statisticsworks on the estimation of HIV infections in the countrysince 2004. A GIS package on HIV data has beendeveloped and linked with census and district healthsurvey data under RCH to draw relevantinterpretations at the state and district level. TheCountry Report 2006 has been printed anddistributed and the Country Report 2007 is underprint.
309
ANNUAL REPORT 2008-09
DLHS -III
National Institute of Health and Family Welfare hasbeen designated as the Nodal Agency forcoordinating the activities of monitoring, training,mapping and listing and field survey in DLHS-3.NIHFW has the help of 8 agencies for undertakingthe monitoring. In addition, NIHFW is alsoresponsible for monitoring DLHS-3 Survey for theStates of Western Uttar Pradesh and Chhattisgarhin Phase-I and Delhi and Haryana in Phases-II ofthe survey.
Immunization Strengthening Project
Under immunization strengthening project, trainingfor district managers has been started by all the 5identified training institutions (NICED, Kolkata; IIHFW,Hyderabad; PGI, Chandigarh; FWTRC, Mumbai;NICD, Delhi).
Deemed to be University status for NIHFW
The Governing Body of the Institute has approvedthe proposal of Deemed University status for NIHFW.In this regard, the decision process is at the finalstage with University Grant Commission. It isexpected that NIHFW may become Deemed Universityin the early part of the year 2009. This will enablethe institute to start various diploma and degreecourses in Public Health, Health Economics andFinances, Health Policy & Planning, Population &Development Public Health Nutrition etc. DraftMemorandum of Association as per the UGCguidelines have been prepared for getting theapproval of competent authority as per therequirements of the UGC.
Publications
Since its inception, the Institute has published morethan hundred and fifty (150) technical reports,training modules for various categories of healthfunctionaries, research reports, health status reports,national health programme series, books, etc. forthe benefit of students, scientists, healthadministrators, programme managers, etc.
During the year, the Institute has come up withpublications, such as -
� PFA Programme,
� Control & Treatment of OccupationalDiseases,
� Drug De-addiction Programme and
� National Population Education Project.
Journal of Institute
The Institute like every year published its quarterlyjournal, 'Health and Population: Perspectives andIssues', with articles on research studies conductedall over the country and it has been abstracted/indexed by national and international abstractingagencies.
The Journal is indexed/abstracted by 9 National andInternational abstracting agencies. The journal is alsoavailable on the Institute's web site i.e.,www.nihfw.org.Volume 31, Jan-March,2008 issue ofthe journal HPPI has been published and issue ofApril-June,2008 is under print.
A Publication in Hindi called 'Dhaarna' is continuedwith articles contributed by faculty and staff membersof the Institute. 13 Volumes of 'Dhaarna' HindiMagazine has been published and 14th is in thepress.
Newsletter
In an effort to disseminate the activities of the Instituteto a large number of readers in the country as wellas abroad, the Institute regularly brings out aquarterly Newsletter. This is very informative,educative and useful to the readers. Recently,NIHFW has published quarterly Newsletter Vol.X No.4October-December, 2008.
The Newsletter is also available on the Institute'sweb-site i.e. www.nihfw.org
State of Art Computer Facilities
The Institute has provided computer access to all itsfaculty, research staff, students and administrativestaff. About 300 Pentium IV Desktops and 45 Laptopsare provided to staff of the Institutes. The Institutehas computerized its various Administrative and

310
ANNUAL REPORT 2008-09
Financial activities. The Institute has developed astate of art computer centre with 35 work stations forusers in the year 2008-09. The NIHFW has its ownweb site i.e. www.nihfw.org.
National Documentation Centre
The National Documentation Centre of NIHFWendeavours to acquire process, organize anddisseminate global information to fulfil the informationneeds of the administrators, planners, policy makers,researchers, teachers, trainers, programmepersonnel and public concerned with health,population and family welfare throughout the country.The library facilities available at NDC are probablyone of the best in India in this field. Over a period oftwo decades, the NDC has developed a well balancedand up-to-date collection of over 65,000 documents;including books, periodicals, technical reports, annualreports, statistical reports, conference proceedings,modules, non-book materials etc. in the field ofhealth, population and family welfare and allied areascarrying worldwide information. NCHRC is establishedat NDC.
Demographic Data Centre
The purpose of the centre is to develop a data bankfor collection of information available from differentsources at national and state level on socio-demographic, health and family welfare, etc. forproviding ready reference materials to theprofessionals. The Demographic Data Centreprocured NFHS-1, NFHS-2, NFHS-3, DLHS-1, DLHS-2, DLHS-3, various rounds of NSSO Data, Census-1991 and 2001 Data. These Data are analysed andpublished from time to time. The data center hasanalysed the data and prepared report of"Determinants of Maternal Mortality" and "Utilizationof Selected RCH Services using DLHS Data" in theyear 2007-08.
Official Language Implementation
The Institute attaches due importance to the use ofHindi by the faculty and staff members. The OfficialLanguage implementation in the Institute is regularlymonitored by a committee duly constituted for thispurpose. An incentive scheme is in practice for the
progressive use of Hindi in official work by the facultyand staff members.
15.4615.4615.4615.4615.46 Rural Health TRural Health TRural Health TRural Health TRural Health Training Centre,raining Centre,raining Centre,raining Centre,raining Centre,Najafgarh, New DelhiNajafgarh, New DelhiNajafgarh, New DelhiNajafgarh, New DelhiNajafgarh, New Delhi
Introdution
Rural Health Training Centre, (RHTC), Najafgarh,New Delhi was et up as health unit in 1937 with thefinancial support from Rockefeller Foundation tocover an area of about 162 sq. miles and a populationof 44,000 scattered over 35 villages for primaryhealth care services through dispensary and teamof Para-medical staff.
After the adoption of Bhore Committee, the unit wasupgraded to a Primary Health Centre. It was re-organized in 1954 to carry out to the functions of anOrientation Training Centre on regional basis to trainthe Rural Health Workers for community developmentprograms. The activities of the center were furtherexpanded with the addition of two more Primary HealthCenters at Ujwa (1955) and Palam (1957).
The center was reorganized as Rural Health TrainingCentre, Najafgarh in 1960, under the administrativecontrol of Directorate General of Health Services(DGHS), Govt. of India. In 1961 a decision was takento declare PHC, Najafgarh as a center for impartingcommunity health training for Medical Interns of LadyHarding Medical College under Rural Orientation ofMedical Education (ROME) Scheme. In 1965,another health program of School Health waslaunched at Najafgarh. Subsequently other centrallysponsored schemes under National Health Programslike National Vector Borne Diseases Control Program,Revised National TB Control Programme, NationalDiabetes Control program (NDCP), National Programfor Control of Blindness (NPCB) and so on werelaunched at Najafgarh. In 1978, it was declaredNational Scientific Institute. In 1981 a Post partumunit under All India Hospital Post Partum Programwas set up with the assistance of Family WelfareDepartment. To strengthen the Rural HealthServices, an ANM School was started in 1985 andvocationalized in 1991.
311
ANNUAL REPORT 2008-09
The population of the Najafgarh Block, situated onSouth West of Delhi, at present is 1.05 million. Theregistered population with the Rural Health TrainingCentre, Najafgarh is nearly 5,00,000. Rural HealthTraining Center, Najafgarh, PHCs of Najafgarh,Palam and Ujwa and 16 sub centers is spread overan area of 432.6 km covering 73 villages.
Activities at RHTC, Najafgarh for the Year 2008-09.
Trainig Programmes at RHTC, Najafgarh
� RHTC produces 20 Auxiliary Nurse Mid-Wife(ANM) under 10+2 vocational CBSE Courseannually. The ANM Training Course, whichwas de-recognized, is now recognized andadmissions have commenced since 2007.Attempts are being made to increase theseats to 40. 20 Auxiliary Nurse Mid-WifeStudents under 10+2 Vocational CBSECourse successfully completed their coursein the year 2008.
� RHTC provides rural training toundergraduates and medical interns fromLady Harding Medical College, VardhamanMahavir Medical College and SafdarjungHospital & Dr. RML Hospital. RHTC,Najafgarh, trained 360 Medical Interns in theirRural posting under PSM in the year 2008-2009.
� General Nursing students, B.Sc. (Nursing) M.Sc. (Nursing), PGD/Mch. Food & Nutritionstudents etc. of different college/Schools ofNursing of Delhi and other states are giventraining. The rural training to undergraduateunder Community Medicine, 148 Interns weretrained in PSM posting along with nursingstudents of B.Sc. (Nursing), M. Sc. (Nursing)and general Nursing Students.
� Various lectures/seminar are being organizedto impart knowledge of Public Health toMedical & Nursing Students.
Providing Clinical Services And 24/7 EmergencyServices
� Addition facilities were started for the generalpublic attending the Emergency. A nebuliserfor asthma patent, ECG Machine for heartpatents and other minor equipment i.e.stretcher, wheel chair were made available.
� OPD attendance has arisen in the year 2007-08. OPD Patents 6.9% increase as comparedup to last year September 2007.
� Emergency Patients 88.9% (number ofpatients up to September 2007 attended 7569as compared to 14300 up to September2008) increase as compared up to last yearSeptember 2007.
� Laboratory of PHC Najafgarh up till now wasproviding basic minor tests to the patients,which included Haemogram, Urine & Stoolanalysis. In this Financial Year Rh ABOgroup testing & Pregnancy test wereadded in initial phases. Purchase of twoGlucometers helped in adding Blood Sugartests for Diabetes Patients. HIV testingfacilities were also made available with thehelp of Delhi Aids Control Society. Anautoanalyser has been purchased and allbiochemical tests can be performed at RHTC.
� Pathology services were enhanced with morenumber of tests being provided and thusbringing the total number of test availed bypatients to 450.
� The operation theatre was not used for lastmany years. Only this year special effortswere made to modernize the existingoperation theatre on which the work is inprogress and it is very likely that it will befunctional in the beginning of next financialyear with all modern facilities. The necessarycivil work has been completed.
� The PHC building was restructured along withthe necessary repairs, which were badlyneeded. This gave the building a fresh look.
312
ANNUAL REPORT 2008-09
The Labour Room was overhauled with thereplacement of Delivery Table. OT Light anda Sterilizer.
� RHTC provides the total package of ANC.Delivery and Post partum care through itsvarious infrastructure like subentries (16),PHCs (3) and OT. In the last year the numberof deliveries conducted at RHTC, hasincreased. Deliveries cases 135.7% increaseas compared up to last year September2007.
� All immunizations are done as routine; RHTCis a nodal center for Polio immunization.
� Medical Officers of RHTC have undergonevarious trainings for increasing their skills.
� Camps for elderly/cataract patients, PulsePolio & Family Planning are held under theaegis of RHTC, Najafgarh, Govt. of NCT Delhiis providing Malaria & TB Clinics where Blood& Sputum Test are conducted in PHCs ofNajafgarh of Najafgarh and Palam &treatment is being given.
� This year the Nursing Cadre wasstrengthened with the recruitment of threeStaff Nurses, thus replacing the Lady HealthVisitor (LHV) and Auxiliary Nurse Midwife(ANM) who were up to now running theEmergency services of Primary Health CenterNajafgarh. This brought a qualitativeimprovement in the functioning of Emergencyservices of Primary Health Center in thefunctioning of the Emergency services ofPrimary Health Center Najafgarh thusrelieving these ANM & LHV for the field duties.Three new ANM were recruited against vacantfield Services.
� Four additional Medical Officers of CHS cadreagainst existing vacancies were added toGroup A cadre in RHTC Najafgarh thus tosome extent alleviating the severe shortageof Medical Officers. This in turn facilitatedthe extension of 24/7 Emergency Servicesto the general public.
� Hot case, Air conditioner, coolers and newfurniture was made available for the Staff intheir duty rooms. A water Cooler with aquaguard was reinstalled to make cold potablewater for general public and staff
Other Activities
� In the last financial year active and successfulattempts were made to improve the generalcondition of the buildings/campus andfacilities to the staff and the public.
� In view of providing impeccable cleanliness,the services of Sulabh were provided in thewards/OPD & PP Unit. This resulting in goodstandards of cleanliness and maintenancein these areas.
� The security till year before last was madeavailable through local daily wagers. Infinancial year 2007-08, the private agencieswere handed over the security of PHCs ofRHTC, Najafgarh. This resulted inprofessional and competent performance.
Field Services
Mobile Unit for various areas were restarted with thehelp of Medical Staff and in the process the medicalinterns are being given field training as well. TheseHealth Units are directly under the Supervision ofDirector who is a Public Health Specialist.
15.4715.4715.4715.4715.47 Gandhigram Institute of RuralGandhigram Institute of RuralGandhigram Institute of RuralGandhigram Institute of RuralGandhigram Institute of RuralHealth and Family WHealth and Family WHealth and Family WHealth and Family WHealth and Family Welfare Telfare Telfare Telfare Telfare Trustrustrustrustrust(((((GIRHFWTGIRHFWTGIRHFWTGIRHFWTGIRHFWT)))))
Established in 1964 with financial support from FordFoundation, Government of India and Governmentof Tamilnadu,
The Health and Family Welfare Training Centre atGIRHFWT is one of 47 such training centres in thecountry. It trains Health and Health relatedfunctionaries working in Primary Health Centres,Corporations / Municipalities, Tamil Nadu IntegratedNutrition Projects. The type of training programmesincluded - orientation training, refresher training,skill training on different Health & Family Welfare
313
ANNUAL REPORT 2008-09
issues for various categories of health personnelwhich is affiliated to Tamil Nadu Dr. M.G.R MedicalUniversity.
Gandhigram Institute is also engaged in upgradingthe capabilities of ANMs, staff nurses and studentsof nursing colleges through the Regional HealthTeachers Training Institute (RHTTI). The RHTTIhas under taken following activities during 2005-06.
i) Diploma in Nursing Education andAdministration (DNEA): 13 number ofstudents were trained during 2004-05 and 7numbers during 2005-06.
ii) Promotional course for the Female HealthWorkers and Auxiliary Nurse /Mewives: 18number of students were trained during 2004-05 and 30 numbers of students during 2005-06 and 30 numbers of students during Jan2006 - July 2006.
iii) Short- term training in community healthnursing: In short term training in communityhealth nursing out of total number of 943,94for FNM, 36 for DNEA, 672 for BSc, 41 forMSc and 120 for NGO were trained in all.
The institute has been conducting this one yearDiploma course since 1964 in order to prepare basiclevel professionals as health Educators.
For this activity during 2008-09 Rs.140.00 lakhs wereavailable under BE.
15.4815.4815.4815.4815.48 Hindustan Latex Limited (HLL)Hindustan Latex Limited (HLL)Hindustan Latex Limited (HLL)Hindustan Latex Limited (HLL)Hindustan Latex Limited (HLL)
Introduction
Hindustan Latex Limited (HLL) began its journeywith as a corporate entity under the Ministry of Healthand Family Welfare, Government of India on March1, 1966. HLL was set up in the natural rubber richstate of Kerala for the production of malecontraceptive sheaths, also known as Condoms forthe National Family Planning Programme. TheCompany commenced its commercial operations onApril 5, 1969.
Manufacturing Units
HLL has five manufacturing units located across thecountry with state-of-the-art facilities, which are:
1. Perrokada Factory, Thiruvananthapuram(Male Condoms)
2. Akkulam Factory, Thiruvananthapuram(Healthcare Products)
3. Kanagala Factory, Belgaum (Condom andPharmaceutical products)
4. Kakkanad Factory, Cochin was set up in theSEZ area in 2005 (Female condoms).
5. Manesar Factory, Gurgaon was set up inNovember 2007 (Rapid Diagnostic Kits).
Products /Services
Hindustan Latex is the only company in the worldmanufacturing and marketing the widest range ofContraceptives that includes Female Condoms,Intra Uterine Devices, Oral Contraceptive Pills -steroidal, non-steroidal and emergency contraceptivepills; Contraceptive Cream, and Tubal Rings.
HLL's healthcare product range include: BloodCollection Bags, Surgical Sutures, Auto DisableSyringes, Hydrocephalus Shunt, Tissue Expanders,Needle Destroyers, Blood Bank equipment, Iron andFolic Acid Tablets, Medicated Plasters, Sanitary Napkins,Oral Rehydration Salts and Pregnancy Test Kits.
Besides, HLL offers Consultancy Services throughits Procurement Consultancy Division (PCD) andInfrastructure Division (ID). PCD offers procurementconsultancy services and ID offers consultancy tohealthcare infrastructure projects.
The Company has set up a Diagnostic Centre in NewDelhi under the banner "HINDLABS" to provide qualitydiagnostic services to the beneficiaries of CentralGovernment Health Scheme (CGHS).
Diversification /Expansion Projects
In year 2007-08, HLL executed the followingdiversification /expansion projects.
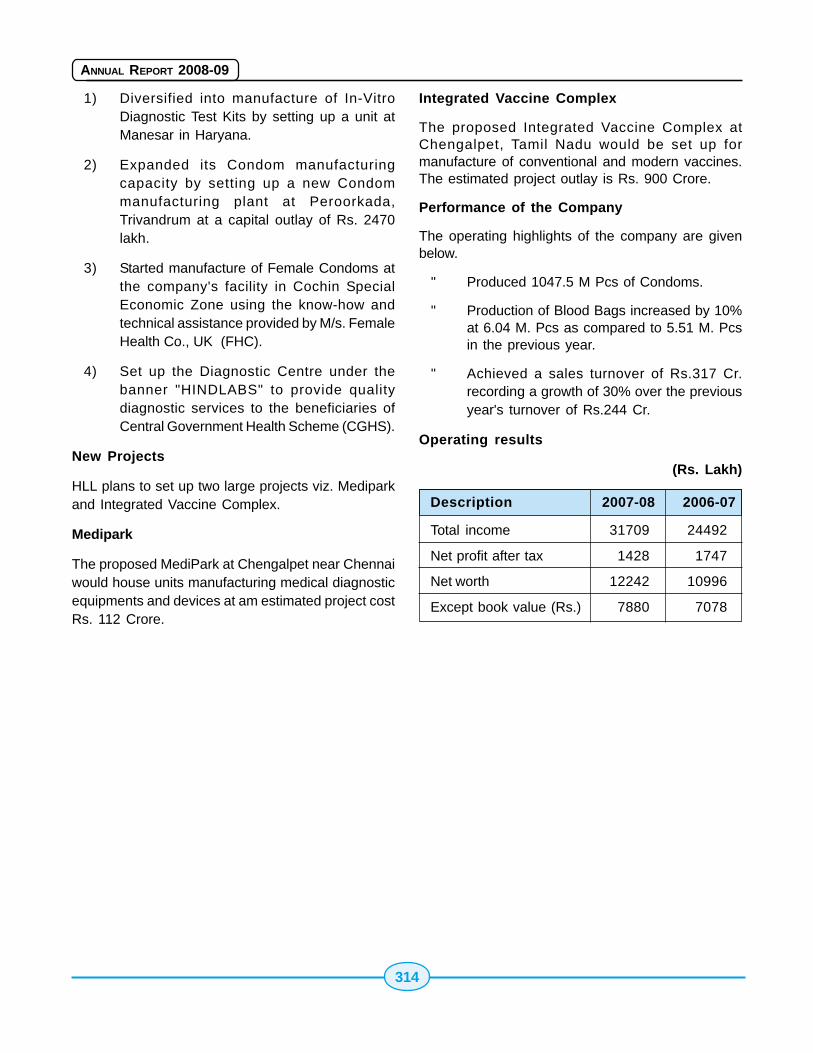
314
ANNUAL REPORT 2008-09
1) Diversified into manufacture of In-VitroDiagnostic Test Kits by setting up a unit atManesar in Haryana.
2) Expanded its Condom manufacturingcapacity by setting up a new Condommanufacturing plant at Peroorkada,Trivandrum at a capital outlay of Rs. 2470lakh.
3) Started manufacture of Female Condoms atthe company's facility in Cochin SpecialEconomic Zone using the know-how andtechnical assistance provided by M/s. FemaleHealth Co., UK (FHC).
4) Set up the Diagnostic Centre under thebanner "HINDLABS" to provide qualitydiagnostic services to the beneficiaries ofCentral Government Health Scheme (CGHS).
New Projects
HLL plans to set up two large projects viz. Mediparkand Integrated Vaccine Complex.
Medipark
The proposed MediPark at Chengalpet near Chennaiwould house units manufacturing medical diagnosticequipments and devices at am estimated project costRs. 112 Crore.
Integrated Vaccine Complex
The proposed Integrated Vaccine Complex atChengalpet, Tamil Nadu would be set up formanufacture of conventional and modern vaccines.The estimated project outlay is Rs. 900 Crore.
Performance of the Company
The operating highlights of the company are givenbelow.
" Produced 1047.5 M Pcs of Condoms.
" Production of Blood Bags increased by 10%at 6.04 M. Pcs as compared to 5.51 M. Pcsin the previous year.
" Achieved a sales turnover of Rs.317 Cr.recording a growth of 30% over the previousyear's turnover of Rs.244 Cr.
Operating results
(Rs. Lakh)
Description 2007-08 2006-07
Total income 31709 24492
Net profit after tax 1428 1747
Net worth 12242 10996
Except book value (Rs.) 7880 7078
315
ANNUAL REPORT 2008-09
Chapter 16
16.116.116.116.116.1 IntroductionIntroductionIntroductionIntroductionIntroduction
The Scheduled Castes and Scheduled Tribes Cellin the Ministry continued to look after the service-interests of these categories of employees during2006-2007. The Cell assisted the Liaison Officer inthe Ministry to ensure that representation fromScheduled Castes/Scheduled Tribe, OBCs andPhysically Handicapped Persons in the establishment/services under this Ministry received properconsideration.
The Cell circulated various instructions/ ordersreceived from the Department of Personnel andTraining on the subject to the peripheral units of theministry for guidance and necessary compliance. Italso collected various types of statistical data on therepresentation of Scheduled Castes/ScheduledTribes/OBCs/Physically Handicapped Persons fromthe subordinate Offices/Autonomous/Statutorybodies of this Ministry as required by the Departmentof Personnel and Training, National Commission forScheduled Castes and Scheduled Tribes etc. TheCell also rendered advice on reservation proceduresand maintenance of reservation particularly postbased rosters.
During 2006-2007 inspection of rosters was carriedout in respect of Twenty three offices namely 1)National Institute of Health & Family Welfare, NewDelhi 2) Port Health Organization, Mumbai 3) AirportHealth Organization, Mumbai 4 ) GovernmentMedical Store Depot, Mumbai 5) Central DrugsStandards Control Organisation (West Zone),Mumbai 6) Central Drugs Standards Control
Organisation (DITS), Mumbai 7) Assistant DrugsController(I), Mumbai 8) All India Institute of PhysicalMedicine & Rehabilitation, Mumbai 9) Family WelfareTraining and Research Centre, Mumbai 10) CentralGovernment Health Scheme, Mumbai 11)International Institute of Population Sciences, Mumbai12) Regional Office for Health & F.W., Pune 13)Central Government Health Scheme, Pune 14)National Tuberculosis Institute, Bangalore 15)National Institute of Mental Health & Neuro Sciences,Bangalore 16) Central Government Health Scheme,Bangalore 17) Regional Office for Health & F.W,Bangalore 18) All India Institute of Speech andHearing, Mysore 19) Hindustan Latex Limited,Thiruvananthapuram 20) Central Government HealthScheme, Thiruvananthapuram 21) Regional Officefor Health & FW, Thiruvananthapuram 22) Port HealthOrganisation, Cochin 23) Central Drugs StandardControl Organisation, Cochin.
The salient aspects of the scheme of reservationwere emphasised to the participating units/offices.Suggestions were made to streamline themaintenance and operation of rosters in theseInstitutes/Organisations. The defects andprocedural lapses noticed were brought to theattention of the concerned authorities, for immediaterectification.
The representation of Scheduled Castes andScheduled Tribes in (i) The Central Health ServicesCadre (administered by this Ministry) and (ii) TheMinistry-its Attached and Subordinate Offices as on1.1.2007 is as given in next page:-
Facilities for Scheduled CastesFacilities for Scheduled CastesFacilities for Scheduled CastesFacilities for Scheduled CastesFacilities for Scheduled Castesand Scheduled Tribesand Scheduled Tribesand Scheduled Tribesand Scheduled Tribesand Scheduled Tribes
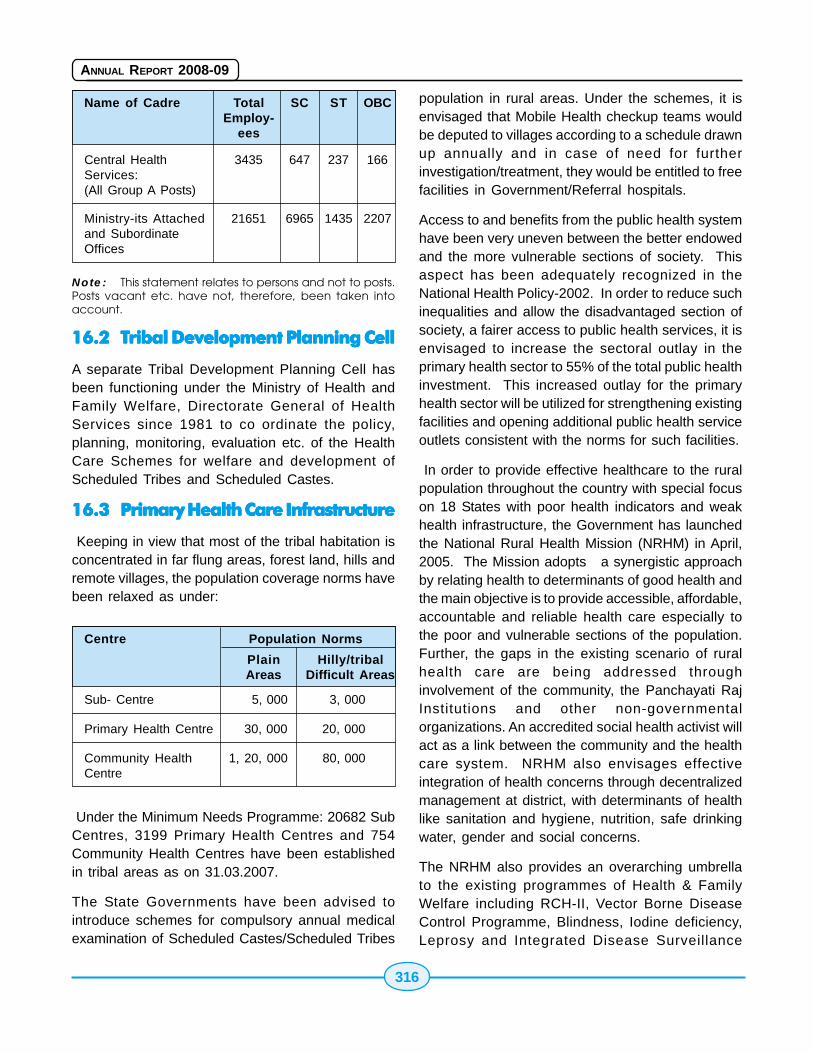
316
ANNUAL REPORT 2008-09
Name of Cadre Total SC ST OBCEmploy-
ees
Central Health 3435 647 237 166Services:(All Group A Posts)
Ministry-its Attached 21651 6965 1435 2207and SubordinateOffices
Note: This statement relates to persons and not to posts.
Posts vacant etc. have not, therefore, been taken into
account.
16.216.216.216.216.2 TTTTTribal Development Planning Cellribal Development Planning Cellribal Development Planning Cellribal Development Planning Cellribal Development Planning Cell
A separate Tribal Development Planning Cell hasbeen functioning under the Ministry of Health andFamily Welfare, Directorate General of HealthServices since 1981 to co ordinate the policy,planning, monitoring, evaluation etc. of the HealthCare Schemes for welfare and development ofScheduled Tribes and Scheduled Castes.
16.316.316.316.316.3 Primary Health Care InfrastructurePrimary Health Care InfrastructurePrimary Health Care InfrastructurePrimary Health Care InfrastructurePrimary Health Care Infrastructure
Keeping in view that most of the tribal habitation isconcentrated in far flung areas, forest land, hills andremote villages, the population coverage norms havebeen relaxed as under:
Under the Minimum Needs Programme: 20682 SubCentres, 3199 Primary Health Centres and 754Community Health Centres have been establishedin tribal areas as on 31.03.2007.
The State Governments have been advised tointroduce schemes for compulsory annual medicalexamination of Scheduled Castes/Scheduled Tribes
population in rural areas. Under the schemes, it isenvisaged that Mobile Health checkup teams wouldbe deputed to villages according to a schedule drawnup annually and in case of need for furtherinvestigation/treatment, they would be entitled to freefacilities in Government/Referral hospitals.
Access to and benefits from the public health systemhave been very uneven between the better endowedand the more vulnerable sections of society. Thisaspect has been adequately recognized in theNational Health Policy-2002. In order to reduce suchinequalities and allow the disadvantaged section ofsociety, a fairer access to public health services, it isenvisaged to increase the sectoral outlay in theprimary health sector to 55% of the total public healthinvestment. This increased outlay for the primaryhealth sector will be utilized for strengthening existingfacilities and opening additional public health serviceoutlets consistent with the norms for such facilities.
In order to provide effective healthcare to the ruralpopulation throughout the country with special focuson 18 States with poor health indicators and weakhealth infrastructure, the Government has launchedthe National Rural Health Mission (NRHM) in April,2005. The Mission adopts a synergistic approachby relating health to determinants of good health andthe main objective is to provide accessible, affordable,accountable and reliable health care especially tothe poor and vulnerable sections of the population.Further, the gaps in the existing scenario of ruralhealth care are being addressed throughinvolvement of the community, the Panchayati RajInstitutions and other non-governmentalorganizations. An accredited social health activist willact as a link between the community and the healthcare system. NRHM also envisages effectiveintegration of health concerns through decentralizedmanagement at district, with determinants of healthlike sanitation and hygiene, nutrition, safe drinkingwater, gender and social concerns.
The NRHM also provides an overarching umbrellato the existing programmes of Health & FamilyWelfare including RCH-II, Vector Borne DiseaseControl Programme, Blindness, Iodine deficiency,Leprosy and Integrated Disease Surveillance
Centre Population Norms
Plain Hilly/tribalAreas Difficult Areas
Sub- Centre 5, 000 3, 000
Primary Health Centre 30, 000 20, 000
Community Health 1, 20, 000 80, 000Centre

317
ANNUAL REPORT 2008-09
Programme. It addresses the issue of health in thecontext of sector-wide approach with focus onsanitation and hygiene, nutrition and safe drinkingwater.
In addition, several health programmes and diseasecontrol programmes have also been initiated forcontrol of AIDS, Cancer, Mental Health, TobaccoControl etc. A number of initiatives have been takenin these programmes for facilitating more effectivedelivery, enhanced coverage and better integration.Depending on the endemicity and disease burden,a focused strategy and approach has been evolvedfor controlling these diseases.
Under these programmes, facilities are available toall sections of the community and these are alsoequally accessible by Scheduled Castes andScheduled Tribes. However, Programme Officershave been directed to ensure that plan funds to theextent of 8.1% for Tribal Sub Plan (TSP) & 16.5% forScheduled Caste Sub Plan (SCSP) are allocated inproportion to the total population as per 2001 censuswherever it is feasible to allocate funds separatelyfor STs and SCs.
16.416.416.416.416.4 Centrally Sponsored SchemesCentrally Sponsored SchemesCentrally Sponsored SchemesCentrally Sponsored SchemesCentrally Sponsored SchemesImplemented By States/UT'sImplemented By States/UT'sImplemented By States/UT'sImplemented By States/UT'sImplemented By States/UT's
National Vector Borne Disease Control Programme:National Vector Borne Disease Control Programmeis in operation throughout the country for preventionand control of Malaria, Kala-Azar, Filaria, JapaneseEncephalities, Dengue/Dengue Hemorrhagic Fever(DHF) and Chikungunya. Additional inputs are beingprovided to highly malarious areas. These are farflung remote areas and are dominated by tribalpopulation. The seven North Eastern states havingtribal population are being provided 100% centralassistance since December 1994 which includesoperational cost of the programme. 100 per centcentral assistance is also provided to Sikkim since2003.
1045 PHCs in 100 districts of 8 states (AndhraPradesh, Chattisgarh, Gujarat, Jharkhand MadhyaPradesh, Maharashtra, Rajasthan and Orissa)predominantly inhabited by tribal population were
being provided 100 per cent support includingoperation expenses under the Enhanced MalariaControl Project (EMCP) with World Bank assistancefrom 1997 to 2005. New World Bank Project onmalaria control and Kala-azar elimination has alsobeen approved since July,2008 and these stateswould be provided the additional inputs.
Intensified Malaria Control Project (IMCP) withassistance from Global Fund to fight against AIDS,Tuberculosis and Malaria (GFATM) is beingimplemented in 10 states (7 NE states & selectedhigh risk areas including tribal areas of Orissa,Jharkhand and West Bengal) under which theassistance is provided to increase access to rapiddiagnosis and treatment in remote and inaccessibleareas, reduce malaria transmission risk by use ofinsecticide treated bed nets (ITNs) and enhancecommunity awareness about malaria control andpromote community, NGO and private sectorparticipation.
National Leprosy Eradication Programme:Leprosy services are uniformly available to allincluding Scheduled Castes & Scheduled Tribepopulation irrespective of caste and religion. Underthe programme, funds are allotted to NGOs, few ofwhich are working in tribal areas providing serviceslike IEC, prevention of deformity and follow up ofcases. Intensified IEC activities have also beenstepped up through various media including the ruralmedia under which population residing in remote,inaccessible and tribal areas are been covered asone of the target groups where awarenessgeneration activities are more focused.
Disaggregated data on SC & ST population is beingcollected under the Simplified Information System.During the year 200-08, the proportion of SC andST cases among newly detected cases were 18.90%and 13% respectively at national level.
Revised National TB Control programme: UnderRevised National T B Control Programme, thebenefits of the programme are available to all on auniform basis irrespective of caste, gender, religion.etc. The sputum microscopy and treatment servicesincluding supply of anti TB drugs are provided free
318
ANNUAL REPORT 2008-09
of cost to all for full course of treatment. However inlarge proportion of tribal and hard to reach areas,the norms for establishing Microscopy centres hasbeen relaxed from 1 per 100,000 population to50,000 and the TB Units for every 250,000 (asagainst 500,000).
To improve access to tribal and other marginalizedgroups, there is also provision for:
� Provision of additional TB Units and DMCs intribal/difficult areas
� Compensation for transportation of patient& attendant in tribal areas
� Higher rate of salary to contractual staffposted in tribal areas
� Enhanced vehicle maintenance and travelallowance in tribal areas
� Provision of TBHVs for urban areas
Under the TB Programme, funds are released to theState Societies for implementation of the programmein the State. The State Societies submit theconsolidated expenditure statement. No separaterecord of release and expenditure is maintained in r/o SC and ST population and also no separate targetsunder the TB Programme are set for SC and ST.
319
ANNUAL REPORT 2008-09
Chapter 17
Hindi is the Official Language of the Union. Therefore,the Ministry of Health and Family Welfare is alsotaking necessary steps for promoting rthe use of Hindiin Offical Work.
There is arrangement in the Ministry for undertakingtranslation work relating to Department of Health andFamily Welfare and Department of Ayurved, Yoga &Naturapathy, Unani, Sidha & Homoeopathy (AYUSH)Steps are taken for implemetation of official languagepolicy of the Union in the Ministry and its attached/subordinate offices, public sector undertakings andother institutiions under the Ministry.
More than 95 percent officers and employees of theMinistry posses working knowledge of Hindi and theMinistry is notified under rule 10(4) of the OfficialLanguage Rule, 1976.
During the year, a number of officials have beenimparted training in Hindi under Hindi TeachingScheme in order to see that they possess workingknowledge of Hindi.
Letters received in Hindi were replied to in Hindi anddirections were issued to make maximum use of Hindiin official correspondence.
Efforts were made to achieve the targerts set in theAnnual Progremme of the year 2008-09 issued bythe Departmwent of Official Language. An incentivescheme for providing cash prizes for writing originalnotes and drafts in Hindi is in operation.
Hindi fortnight was organised in the Ministry and itsattached and subordinate offices during September,2008. The messages from Secretary, Health &Family Welfare and Minister of Home Affairs werecirculated. A number of steps were taken to promotethe use of Hindi during the fortnight. Hindi competionswere organized in which a number of officers/
employees participated. Hindi fortnight was observedfrom 15.9.2008 to 29.9.2008 in the Department ofHealth and Family Welfare.
A scheme for promotion of the books, orginally writtenin Hindi or translated into Hindi on various medicaland public health subjects is in operation underwhich the authors and translators of such books areawarded cash prizes by the Ministry. The followingprizes are provided under the scheme foruseful books originally written in Hindi in the fieldof medical science and public health, a first prize ofRs. 25,000/-, a second prize of Rs. 20,000/-, a thirdprize of Rs. 15,000/-, a fourth prize of Rs. 10,000/-and three consolation prizes of Rs. 5,000/- each aregiven. For Hindi translation of medical text bookswritten in English or in any Indian Language byeminent doctors/authors, there are three prizes viz.a first prize of Rs. 20,000/-, a second prize of Rs.15,000/- and a third prize of Rs. 10,000/-. The booksshould be any one of the following subjects :-
(1) Primary Health Care
(2) Community Medicine
(3) Maternity and Child Health
(4) Public Health
(5) Hygiene and Sanitation
(6) Preventiion of Communicable Diseases
(7) Manuals/Text books for Para MedicalWorkers
(8) Nutrition
(9) Prevention of Disabilities
(10) Mental Health
Use Of Hindi In Official WorkUse Of Hindi In Official WorkUse Of Hindi In Official WorkUse Of Hindi In Official WorkUse Of Hindi In Official Work
320
ANNUAL REPORT 2008-09
(11) Indian Systems of Medicine
(12) Population Control
(13) Immunization Programme
(14) AIDS Control Programme
On Expiry of its term of three years, the HindiSalahkar Samiti of the Ministry is being reconstitutedand after reconstitution its meeting will beconvened.
As far as use of Hindi in the attached/subordinateoffices, public sector undrtakings and autonomous
institutions etc. under the Ministry is concerned, theHindi Division of the Ministry monitors the progressby reviewing the quarterly progress reports of theseoffices. After reviews of quarterly reports,shortcomings found therein are brought to the noticeof the concerned offices and instituions. 40 officesfalling under the control of Ministry of Health andFamily Welfare were inspected upto March, 2009 tofind out the position of the use of Hindi.
The Committee of Parliament on Official Languageconducted inspection of 5 offices under the Ministryof Health & Family Welfare.
321
ANNUAL REPORT 2008-09
Chapter 18
IntroductionIntroductionIntroductionIntroductionIntroduction
Various International organisations and Unitednations Agencies continued to provide significanttechnical and material assistance for many Healthand Family Welfare programme in the country. TheStatus of international assistance from variousagencies is discussed in this chapter.
18.218.218.218.218.2 WWWWWorld Health Organizationorld Health Organizationorld Health Organizationorld Health Organizationorld Health Organization(WHO)(WHO)(WHO)(WHO)(WHO)
World Health Organisation is one of the main UNagencies collaborating in the Health Sector with theMinistry of Health & Family Welfare, Government ofIndia. WHO provides technical support in the majorareas of Health & Family Welfare programmes andhealth care facilities in the country.
Activities under WHO are funded through twosources :- the Country Budget which comes out ofcontributions made by member countries and ExtraBudgetary Resources which comes from (a)donations from various sources for general orspecific aspects of health; and (b) funds routedthrough the WHO to countries by other membercountries or institute agencies. India is the largestbeneficiary of the country budget. The budget isoperated on a biennium basis, calendar year wise.
As a member country of WHO, India makes regularcontribution to WHO for each biennium. For thecurrent biennium 2008-2009, the total assessedcontribution to the working capital of WHO, to be paidby Government of India is US $ 41,79,780. Out ofwhich, Government of India has paid US $ 38,89,890in two instalments. Besides, an amount of US $ 60,000has been paid towards voluntary contribution for
WHO/UNDP/World Bank Special Programme forResearch and Training in Tropical Diseases (TDR)and Special Programme for Research Developmentand Research Training in Human Reproduction (HRP)and for the year 2008. The current biennium 2008-09 will end on 31st December, 2009.
WHO funding is available for taking services of theexperts on contractual basis on specific terms andreferences; training within and outside the country;holding of workshops, seminars and meetings forraising awareness or exchange of information andmedical supplies of equipment, viz: (i) ContractService Agreement; (ii) Fellowship; (iii) Agreementfor Performance of Work; (iv) Local Cost Subsidy;and (v) Supplies and Equipment etc.
Since the current biennium 2008-09, 11 StrategicObjectives have been introduced under which theGOI/WHO collaborative activities are beingimplemented. Monitoring the activities for timely andeffective utilization of funds and their properaccounting is one of the main tasks. The areas ofwork financed by WHO, inter alia cover HIV/AIDS,communicable and non communicable diseases,mental health, drug abuse, environment, food safety,maternal and child health besides health policy, healthfinancing & social protection as well as emergencypreparedness & response. WHO has also switchedover to the system of Direct Financial Cooperation(DFC) from the earlier system of Local Cost Subsidies(LCS). The new procedure envisages completion ofvarious stages and reporting the progress to WHObefore further financing the activities.
WHO Fellowships: Under WHO Fellowshipsprogramme, 232 and 332 nominations have beenmade for abroad and within the country fellowship
International Co-Operation forInternational Co-Operation forInternational Co-Operation forInternational Co-Operation forInternational Co-Operation forHealth & Family WelfareHealth & Family WelfareHealth & Family WelfareHealth & Family WelfareHealth & Family Welfare
322
ANNUAL REPORT 2008-09
courses respectively, in more than 100 differentfields.
18.318.318.318.318.3 Assistance fromAssistance fromAssistance fromAssistance fromAssistance from Japan Japan Japan Japan Japan
Successful completion of JICA-NICEDCollabrative Project
A JICA-NICED collaborative project titled "Project forPrevention and Control of Emerging DiarrhoealDiseases" was initiated at NICED, Kolkata in February,1998 for a period of 5 years. Later this project wasextended as Phase-II for a period of another 5 yearscommencing in July, 2003 which ended in June, 2008.The project had provisions for supply of machineryand equipments and exchange of technical expertisein various fields. The project has fulfilled aim ofproviding training to the scientists representingdifferent labs in the country in identification of majorenteric pathogens and molecular typing.
26th Meeting of Ministers of Health of countriesof South East Asia Region (SEAR) of WHO in NewDelhi, 8 - 9 September, 2008 :
The 26th Meeting of Ministers of Health of thecountries of South East Asia Region (SEAR) of WHOi.e. Bangladesh, Bhutan, DPR Korea, Indonesia,Maldives, Myanmar, Nepal, Sri Lanka, Thailand andTimor Leste was hosted by Ministry of Health & FamilyWelfare, Government of India at Hotel Ashok, NewDelhi during 8-9 September, 2008. The meetingprovides a forum for ministers to discuss importanthealth issues in the region as well as for forgingbilateral arrangements. Health Ministers/Representatives of the respective countries alongwith a country delegation participated in the meeting.The Health Ministers' meeting was followed by the61st Session of Regional Committee of WHO SEARcountries held in South East Asia Regional Office ofWHO in New Delhi during 10-11 September, 2008.
18.418.418.418.418.4 Airport Health Organisations/Airport Health Organisations/Airport Health Organisations/Airport Health Organisations/Airport Health Organisations/Port Health OrganisationsPort Health OrganisationsPort Health OrganisationsPort Health OrganisationsPort Health Organisations
Airport and Port Health organizations (APHO/PHOs)are subordinate offices of Directorate General ofHealth Services. At present there are 9 PHOs and 5
APHOs established at all major international Airportsand Ports of the country. There is also one borderquarantine centre at Attari border, Amritsar. Inaddition to these, the health offices at Bangalore andHyderabad Airports have also been established andstarted functioning in full swing and action has beentaken to set up the health offices at ahmedabad,Lucknow and Trivendrum Airports. These arestatutory organizations and are discharging theirregulatory functions as delineated under IndianAircraft (Public Health) Rules 1954 and Port HealthRules 1955 respectively.
Apart from this, India is also signatory to InternationalHealth Regulations (IHR) framed by WHO andtherefore it is obligatory on our part to implementthese regulations. Accordingly both Indian Air craftPublic Health Rules as well as the Indian Port HealthRules have been framed in agreement with theseInternational Health Regulations.
Main objective of the APHO/PHOs is to preventspread of infectious disease of epidemic proportionfrom one country to another with minimuminterference to the world traffic. Some of theimportant functions of these organization are, healthScreening of International passengers , Quarantine,Clearance of dead bodies, Supervision of airportsanitation, clearance for imported food items,vaccination to international passengers, vectorcontrol etc. Apart from this, issuance of derattingexemption certificate is another major responsibilityat international ports.
WHO has notified a list of yellow fever endemiccountries under IHR and any person coming to Indiafrom these notified endemic countries is required toposses valid yellow fever vaccination certificate,failing which such passengers are quarantined for amaximum period of six days. In the light of changingglobal health scenario, existing IHR has been revisedby WHO and these new IHR have come to effect fromJune, 2007. Now, this Ministry is in the process ofrevising our own rules in tune with the revised IHR.
18.5 WTO Cell18.5 WTO Cell18.5 WTO Cell18.5 WTO Cell18.5 WTO Cell
The WTO Cell in the Ministry of Health and Family
323
ANNUAL REPORT 2008-09
Welfare began working since 2004. The aim of theWTO Cell is to help in ascertaining impacts on publichealth due to globalisation and suggest ways toformulate effective legislation and policy initiativesto deal with it. The work being done by the Cellincludes review of the existing system, available dataand information, identifying the data gaps andproviding evidence-based information, interventionoptions, and potential solutions/strategies withrespect to trade related agreements and its impacton health issues. In addition, the Cell conductsquantitative and qualitative studies related tointernational trade agreements and health issues.The WTO Cell also participates in and organisesworkshops, seminars and meetings. In particular, thefunctions of the WTO Cell includes providingtechnical assistance to the MoH&FW in the area ofinternational trade related agreements, such asTRIPS, GATS, SPS and TBT.
The following workshops and studies focusing oncritical aspects of international trade and its impacton health were organised/commissioned by the WTOCell in the year 2007-08.
Workshops:
� "Meetings of the Core Group for theimplementation of Global Strategy and Planof Action on Public Health, Innovation andIntellectual Property", September 2008, NewDelhi
� Apart from the above-said workshops, onemore workshop is in the process of beingorganised: National Consultation onImplementation of the Global Strategy andPlan of Action on Public Health, Innovationand Intellectual Property in India - February/March 2009
Studies:
� R&D Gaps in the context of Global Strategyand Plan of Action on Public Health, Innovationand Intellectual Property (GSPOA)-2008 byNIPER, Punjab
� Drug Discovery Research for NeglectedDiseases: Designing an Appropriate PolicyFramework - ICRIER, New Delhi
� Status of the mandated actions under theGlobal Strategy and Plan of Action on PublicHealth, Innovation and Intellectual Property(GSPOA) that are already completed or theongoing activities in India
� NISTADS, New Delhi
� Awareness generation of issues mandatedunder GSPOA: what and how? CENTAD, NewDelhi
The future programme of the WTO Cell is broadly todeepen its efforts within its mandate and also to takeforward the recommendations from earlier andpresent workshops and studies.
18.618.618.618.618.6 Foreign TForeign TForeign TForeign TForeign Travel by Senior Officersravel by Senior Officersravel by Senior Officersravel by Senior Officersravel by Senior Officers
For the year 2008-2009, a provision of Rs.200.00lakhs has been made against Foreign TravelExpenses under Non-Plan. Out of this, theexpenditure till March, 2009 is Rs. 1.81 lakhs(approx.)
18.718.718.718.718.7 Visit on Fellowship/ConferenceVisit on Fellowship/ConferenceVisit on Fellowship/ConferenceVisit on Fellowship/ConferenceVisit on Fellowship/ConferenceAbroadAbroadAbroadAbroadAbroad
During the period under report (up to March, 2009),185 medical personnel were permitted to participatein International conference/symposia etc. abroad.This includes 21 medical personnel from CHS cadrewho have been granted financial assistance subjectto a maximum of Rs.1,00 lakh- each to attendInternational Conference abroad under the schemewhich provides financial assistance to attendseminars/conferences abroad in order to acquaintthemselves with the latest developments in the fieldof medicine and surgery in other countries and toexchange views with their counterparts.
18.818.818.818.818.8 State Health SystemsState Health SystemsState Health SystemsState Health SystemsState Health SystemsDevelopment Projects withDevelopment Projects withDevelopment Projects withDevelopment Projects withDevelopment Projects withWWWWWorld Bank Assistanceorld Bank Assistanceorld Bank Assistanceorld Bank Assistanceorld Bank Assistance
State Health Systems Development Projects startedwith the World Bank assistance are aimed atimproving/upgrading secondary level health carefacilities. The details of these projects which havebeen completed/under implementation, is as under:-
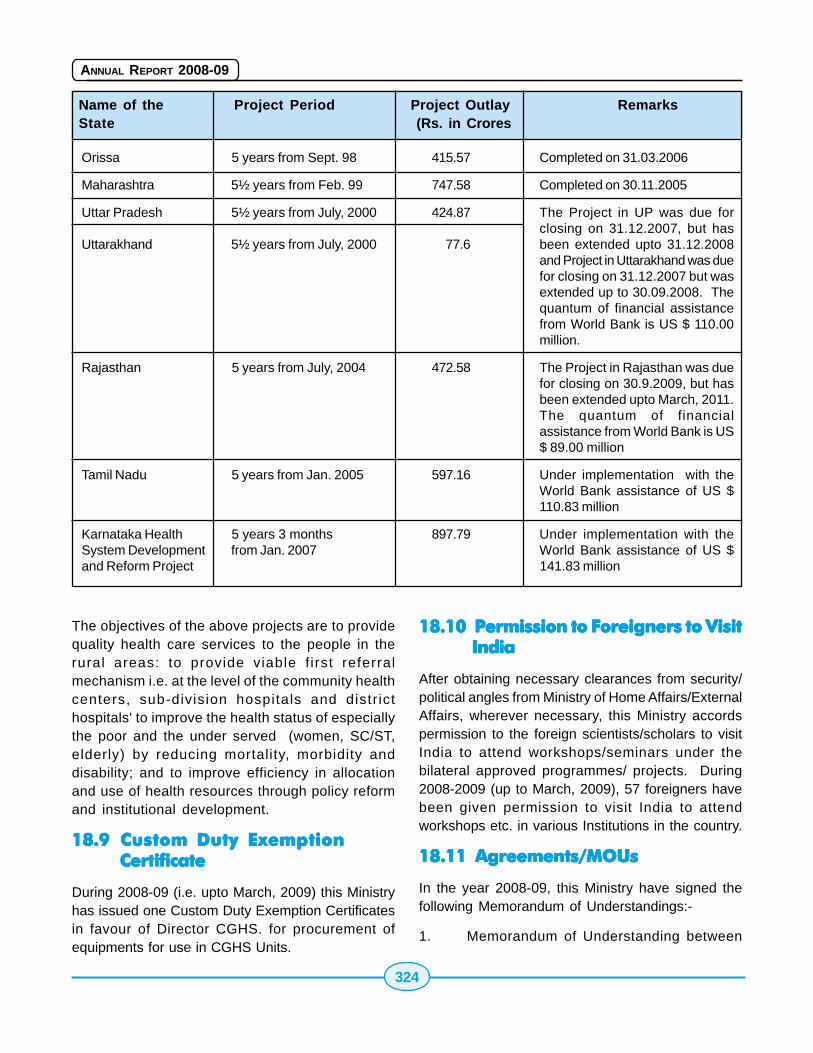
324
ANNUAL REPORT 2008-09
Name of the Project Period Project Outlay RemarksState (Rs. in Crores
Orissa 5 years from Sept. 98 415.57 Completed on 31.03.2006
Maharashtra 5½ years from Feb. 99 747.58 Completed on 30.11.2005
Uttar Pradesh 5½ years from July, 2000 424.87 The Project in UP was due forclosing on 31.12.2007, but has
Uttarakhand 5½ years from July, 2000 77.6 been extended upto 31.12.2008and Project in Uttarakhand was duefor closing on 31.12.2007 but wasextended up to 30.09.2008. Thequantum of financial assistancefrom World Bank is US $ 110.00million.
Rajasthan 5 years from July, 2004 472.58 The Project in Rajasthan was duefor closing on 30.9.2009, but hasbeen extended upto March, 2011.The quantum of financialassistance from World Bank is US$ 89.00 million
Tamil Nadu 5 years from Jan. 2005 597.16 Under implementation with theWorld Bank assistance of US $110.83 million
Karnataka Health 5 years 3 months 897.79 Under implementation with theSystem Development from Jan. 2007 World Bank assistance of US $and Reform Project 141.83 million
The objectives of the above projects are to providequality health care services to the people in therural areas: to provide viable f irst referralmechanism i.e. at the level of the community healthcenters, sub-division hospitals and distr icthospitals' to improve the health status of especiallythe poor and the under served (women, SC/ST,elderly) by reducing mortality, morbidity anddisability; and to improve efficiency in allocationand use of health resources through policy reformand institutional development.
18.918.918.918.918.9 Custom Duty ExemptionCustom Duty ExemptionCustom Duty ExemptionCustom Duty ExemptionCustom Duty ExemptionCertificateCertificateCertificateCertificateCertificate
During 2008-09 (i.e. upto March, 2009) this Ministryhas issued one Custom Duty Exemption Certificatesin favour of Director CGHS. for procurement ofequipments for use in CGHS Units.
18.1018.1018.1018.1018.10 Permission to Foreigners to VisitPermission to Foreigners to VisitPermission to Foreigners to VisitPermission to Foreigners to VisitPermission to Foreigners to VisitIndiaIndiaIndiaIndiaIndia
After obtaining necessary clearances from security/political angles from Ministry of Home Affairs/ExternalAffairs, wherever necessary, this Ministry accordspermission to the foreign scientists/scholars to visitIndia to attend workshops/seminars under thebilateral approved programmes/ projects. During2008-2009 (up to March, 2009), 57 foreigners havebeen given permission to visit India to attendworkshops etc. in various Institutions in the country.
18.11 Agreements/MOUs18.11 Agreements/MOUs18.11 Agreements/MOUs18.11 Agreements/MOUs18.11 Agreements/MOUs
In the year 2008-09, this Ministry have signed thefollowing Memorandum of Understandings:-
1. Memorandum of Understanding between
325
ANNUAL REPORT 2008-09
India and Maldives concerning Manpowerrequirements of Indira Gandhi MemorialHospital (IGMH), Male was signed in NewDelhi on 19th September, 2008
2. Memorandum of Understanding betweenIndia and Egypt on cooperation in the fieldof Health and Medicine was signed in NewDelhi on 18th November, 2008.
3. Memorandum of Understanding between theGovernment of the Republic of India and theGovernment of the Kingdom of Sweden inthe field of Health Care and Public Health wassigned on 24th Feb, 2009
18.1218.1218.1218.1218.12 Meetings/Conferences UnderMeetings/Conferences UnderMeetings/Conferences UnderMeetings/Conferences UnderMeetings/Conferences Underthe Aegis of Internationalthe Aegis of Internationalthe Aegis of Internationalthe Aegis of Internationalthe Aegis of InternationalCooperationCooperationCooperationCooperationCooperation
India-Brazil-South Africa Trilateral Meeting underIBSA MOU and India-Brazil-South Africa JointWorking Group Meeting were held in July andSeptember, 2008 respectively in New Delhi. Further,the India-Russia-China Trilateral Meeting on Public
Health and Medicine was held in September, 2008in New Delhi.
Minister/official level Bilateral Meetings between Indiaand Bahrain, Brazil, South Africa, Bhutan, Denmarkand Sweden, China, Maldives, Mexico city were heldwith a view to improving the bilateral relations in theHealth Sector during the year 2008-2009.
A team of Indian doctors visited China which wasfollowed by the visit of a delegation of Chinesedoctors to India in commemoration of the Dr. KotnisMedical Mission to China. A delegation of the SouthAfrican Pharmacy Council visited India. A high leveldelegation from China led by Vice Minister visitedIndia to hold discussions in the field of populationand Family Planning.
18.1318.1318.1318.1318.13 Permission for InternationalPermission for InternationalPermission for InternationalPermission for InternationalPermission for InternationalConferencesConferencesConferencesConferencesConferences
In the year 2008 (upto December, 2008),permissions were granted to 48 Organizations/Institutions for holding health related internationalConferences in India.

326
ANNUAL REPORT 2008-09
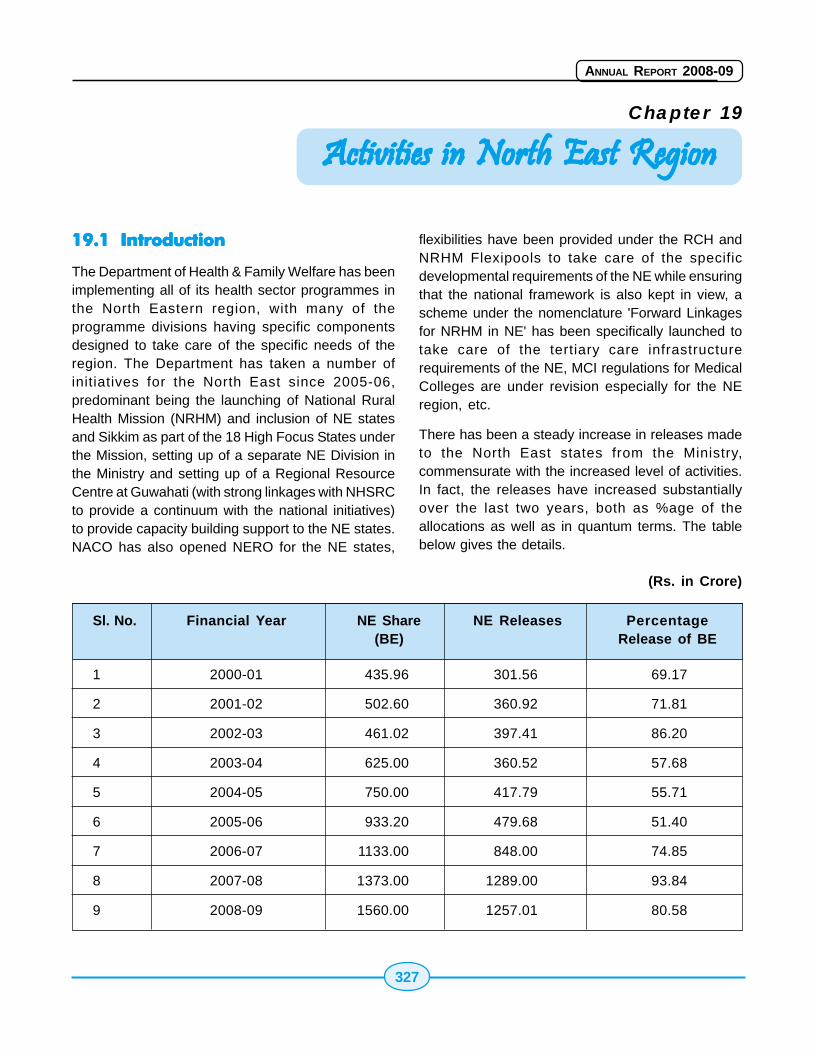
327
ANNUAL REPORT 2008-09
Chapter 19
19.119.119.119.119.1 IntroductionIntroductionIntroductionIntroductionIntroduction
The Department of Health & Family Welfare has beenimplementing all of its health sector programmes inthe North Eastern region, with many of theprogramme divisions having specific componentsdesigned to take care of the specific needs of theregion. The Department has taken a number ofinitiatives for the North East since 2005-06,predominant being the launching of National RuralHealth Mission (NRHM) and inclusion of NE statesand Sikkim as part of the 18 High Focus States underthe Mission, setting up of a separate NE Division inthe Ministry and setting up of a Regional ResourceCentre at Guwahati (with strong linkages with NHSRCto provide a continuum with the national initiatives)to provide capacity building support to the NE states.NACO has also opened NERO for the NE states,
Activities in North East RegionActivities in North East RegionActivities in North East RegionActivities in North East RegionActivities in North East Region
flexibilities have been provided under the RCH andNRHM Flexipools to take care of the specificdevelopmental requirements of the NE while ensuringthat the national framework is also kept in view, ascheme under the nomenclature 'Forward Linkagesfor NRHM in NE' has been specifically launched totake care of the tertiary care infrastructurerequirements of the NE, MCI regulations for MedicalColleges are under revision especially for the NEregion, etc.
There has been a steady increase in releases madeto the North East states from the Ministry,commensurate with the increased level of activities.In fact, the releases have increased substantiallyover the last two years, both as %age of theallocations as well as in quantum terms. The tablebelow gives the details.
(Rs. in Crore)
Sl. No. Financial Year NE Share NE Releases Percentage(BE) Release of BE
1 2000-01 435.96 301.56 69.17
2 2001-02 502.60 360.92 71.81
3 2002-03 461.02 397.41 86.20
4 2003-04 625.00 360.52 57.68
5 2004-05 750.00 417.79 55.71
6 2005-06 933.20 479.68 51.40
7 2006-07 1133.00 848.00 74.85
8 2007-08 1373.00 1289.00 93.84
9 2008-09 1560.00 1257.01 80.58
328
ANNUAL REPORT 2008-09
There are a number of challenges in the HealthSector in the North East, which are being addressedthrough the various interventions of the Departmentof Health & Family Welfare in the North EasternRegion. Some of these are given in brief below.
� Shortage of trained medical manpower - Theshortage runs across the spectrum ofspecialists, doctors, nurses and otherparamedical staff. Nursing Schools are beingset-up or strengthened. Setting up MedicalColleges is a more complex affair and thesmaller states like Nagaland, Mizoram andArunachal Pradesh are being encouraged orassisted to strengthen their State levelfacilities and thus, gradually, develop facilitiesfor Medical Colleges.
� Providing access to sparsely populated,remote, far flung areas; backward areas andinsurgency prone areas - Despite relaxednorms for setting up of SCs, PHCs and CHCs,the location of these health facilities is eithernot uniformly covering the entire populationor the available facilities in the problem areasare not manned. Ambulances and referralservices are being provided. Providing healthfacilities through MMUs, Boat clinics,helicopter sorties are being tried withconcerns about sustainability. Rationalisingand relocating health facilities based onbetter planning (using modern tools like GISmapping) and providing incentives formanpower to be stationed in these areas(monetary or local selection) are sustainablebut more difficult to implement.
� Improvement of Governance in the Healthsector - This is linked to an extent with theexternalities like law and order issues, overallgovernance structure of the State, etc.Though handholding through NE-RRC,capacity building by infusion of additionalprogramme management staff at the state,district and block level is being made, thelarger issues of externalities remain to betackled and the traditional weaknesses in
monitoring, supervision and reporting aredifficult to surmount.
� Need for improved quality of health servicesrendered - Norm based approach for thevarious categories of health facilities is beingtried and service guarantees are built intothe NRHM Implementation Framework. Acoordinated approach towards developmentof facilities to meet the infrastructure,manpower, training needs and improvedinternal protocols of functioning is beingstressed.
� Making effective and full utilisation of existingfacilities - Contractual appointments ofdoctors and staff, improvement of existinginfrastructure and supply of drugs is helpingin better service delivery but the shortagesof Male Health Workers in the Sub-Centres,who have to be recruited and paid for by theStates continue. Similarly, the PHCs areunable to provide 24X7 facilities due toshortage of doctors especially in Nagalandand Mizoram. There is a shortfall of LabTechnicians and Pharmacists at certainlocations.
� Effective and timely utilisation of financialresources available.
� Morbidity and Mortality due to Malaria.
� High level of tobacco consumption and theassociated high risk to cancer.
� High incidence of HIV/AIDS in Nagaland,Manipur and the increasing incidence inMizoram and Meghalaya.
19.219.219.219.219.2 National Rural Health MissionNational Rural Health MissionNational Rural Health MissionNational Rural Health MissionNational Rural Health Mission(((((NRHMNRHMNRHMNRHMNRHM) in North East) in North East) in North East) in North East) in North East
The National Rural Health Mission (NRHM) has beenlaunched with a view to bringing about dramaticimprovement in the health system and the healthstatus of the people, especially those who live in therural areas of the country. The Mission providesspecial focus to 18 states, which include the 8 North
329
ANNUAL REPORT 2008-09
Eastern states, which have weak public healthindicators and/or weak infrastructure.
The Mission seeks to provide universal access toequitable, affordable and quality health care whichis accountable at the same time responsive to theneeds of the people, reduction of child and maternaldeaths as well as population stabilization, gender anddemographic balance. In this process, the Missionwould help achieve goals set under the NationalHealth Policy and the Millennium Development Goals.To achieve these goals NRHM is:
� Facilitating increased access and utilizationof quality health services by all.
� Forging a partnership between the Central,state and the local governments.
� Setting up a platform for involving thePanchayati Raj institutions and community inthe management of primary healthprogrammes and infrastructure.
� Providing an opportunity for promoting equityand social justice.
� Has introduced mechanisms to provideflexibility to the states and the community topromote local initiatives.
� To develop a framework for promoting inter-sectoral convergence for promotive andpreventive health care.
The core strategies of the Mission are:
� Train and enhance capacity of PanchayatiRaj Institutions (PRIs) to own, control andmanage public health services.
� Promote access to improved healthcare athousehold level through the female healthactivist (ASHA). The high focus States(including the 8 NE states) are beingsupported for having an Accredited SocialHealth Worker (ASHA) in all villages with apopulation of 1000
� Health Plan for each village through VillageHealth Committee of the Panchayat.
� Strengthening sub-centre through betterhuman resource development, clear qualitystandards, better community support and anuntied fund to enable local planning andaction and more Multi Purpose Workers(MPWs).
� Strengthening existing (PHCs) through betterstaffing and human resource developmentpolicy, clear quality standards, bettercommunity support and an untied fund toenable the local management committee toachieve these standards.
� Provision of 30-50 bedded CHC per lakhpopulation for improved curative care to anormative standard. (IPHS definingpersonnel, equipment and managementstandards, its decentralized administration bya hospital management committee and theprovision of adequate funds and powers toenable these committees to reach desiredlevels)
� Preparation and implementation of an intersector District Health Plan prepared by theDistrict Health Mission, including drinkingwater, sanitation, hygiene and nutrition.
The supplementary strategies of the Mission are:
� Regulation for Private sector including theinformal Rural Medical Practitioners (RMP)to ensure availability of quality service tocitizens at reasonable cost.
� Promotion of public private partnerships forachieving public health goals.
� Mainstreaming AYUSH - revitalizing localhealth traditions.
� Reorienting medical education to supportrural health issues including regulation ofmedical care and medical ethics.
� Effective and visible risk pooling and socialhealth insurance to provide health securityto the poor by ensuring accessible,affordable, accountable and good qualityhospital care.
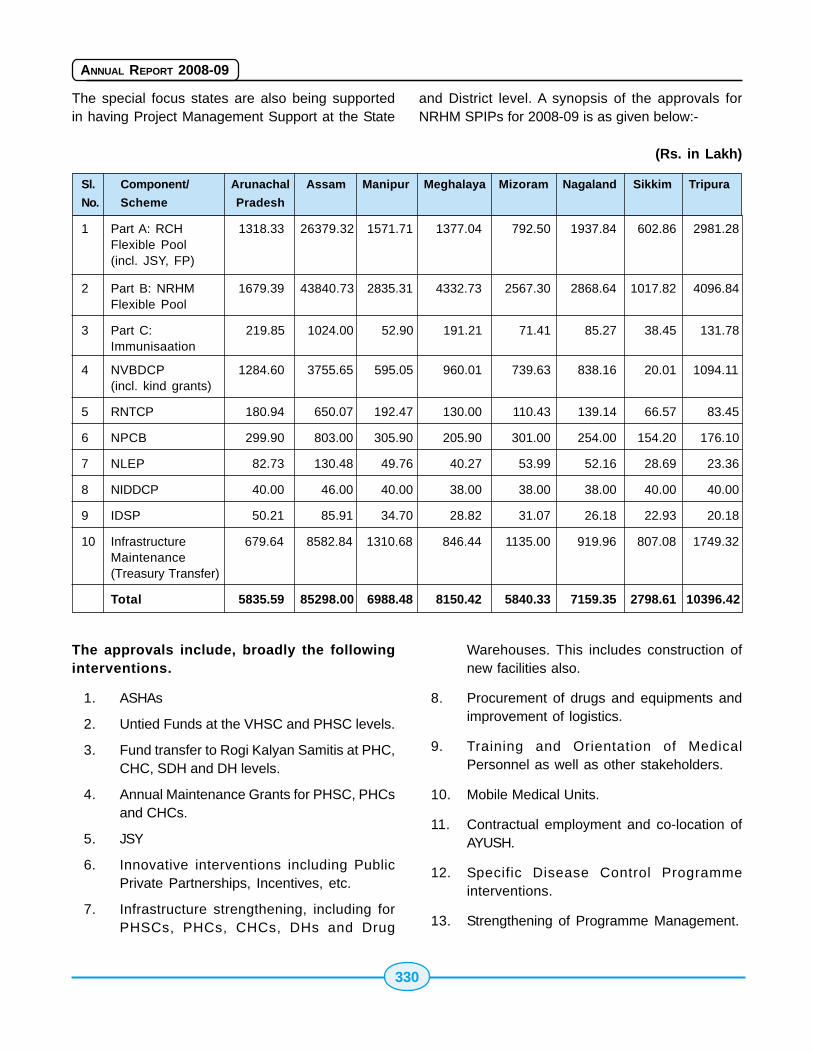
330
ANNUAL REPORT 2008-09
The special focus states are also being supportedin having Project Management Support at the State
and District level. A synopsis of the approvals forNRHM SPIPs for 2008-09 is as given below:-
(Rs. in Lakh)
Sl. Component/ Arunachal Assam Manipur Meghalaya Mizoram Nagaland Sikkim Tripura
No. Scheme Pradesh
1 Part A: RCH 1318.33 26379.32 1571.71 1377.04 792.50 1937.84 602.86 2981.28Flexible Pool(incl. JSY, FP)
2 Part B: NRHM 1679.39 43840.73 2835.31 4332.73 2567.30 2868.64 1017.82 4096.84Flexible Pool
3 Part C: 219.85 1024.00 52.90 191.21 71.41 85.27 38.45 131.78Immunisaation
4 NVBDCP 1284.60 3755.65 595.05 960.01 739.63 838.16 20.01 1094.11(incl. kind grants)
5 RNTCP 180.94 650.07 192.47 130.00 110.43 139.14 66.57 83.45
6 NPCB 299.90 803.00 305.90 205.90 301.00 254.00 154.20 176.10
7 NLEP 82.73 130.48 49.76 40.27 53.99 52.16 28.69 23.36
8 NIDDCP 40.00 46.00 40.00 38.00 38.00 38.00 40.00 40.00
9 IDSP 50.21 85.91 34.70 28.82 31.07 26.18 22.93 20.18
10 Infrastructure 679.64 8582.84 1310.68 846.44 1135.00 919.96 807.08 1749.32Maintenance(Treasury Transfer)
Total 5835.59 85298.00 6988.48 8150.42 5840.33 7159.35 2798.61 10396.42
The approvals include, broadly the followinginterventions.
1. ASHAs
2. Untied Funds at the VHSC and PHSC levels.
3. Fund transfer to Rogi Kalyan Samitis at PHC,CHC, SDH and DH levels.
4. Annual Maintenance Grants for PHSC, PHCsand CHCs.
5. JSY
6. Innovative interventions including PublicPrivate Partnerships, Incentives, etc.
7. Infrastructure strengthening, including forPHSCs, PHCs, CHCs, DHs and Drug
Warehouses. This includes construction ofnew facilities also.
8. Procurement of drugs and equipments andimprovement of logistics.
9. Training and Orientation of MedicalPersonnel as well as other stakeholders.
10. Mobile Medical Units.
11. Contractual employment and co-location ofAYUSH.
12. Specific Disease Control Programmeinterventions.
13. Strengthening of Programme Management.
331
ANNUAL REPORT 2008-09
Achievements under NRHM(till Mar'09):
� Total number of ASHAs selected in the NEStates comes to 50,702.
� 649 PHCs functioning as 24X7 basis in theNE States.
� 195 CHCs functioning as 24X7 basis in theNE States.
� 214 CHCs selected for upgradation to IPHSand physical upgradation completed in 131CHCs.
� 41 District Hospitals(DH) taken up forupgradation.
� 95 centres operational as First ReferralUnits(FRU), including DHs, SDHs, CHCs &other levels.
� 70 Districts are having working MobileMedical Unit (MMU).
� Ayush facilities is available in 341 Centres,including DHs, CHCs, PHCs and other healthfacilities above SCs but below block level.
� 32 Health Melas held during 2008-09.
� 4.49 Lakh Institutional Deliveries done during2008-09.
� 3.39 Lakh beneficiaries of JSY recordedduring 2008-09.
� 4.25 Lakh Children fully immunized during2008-09.
Forward Linkages to NRHM in NE
With a view to complement the initiatives under theNRHM by improving the Tertiary and Secondary levelhealth infrastructure in the region, the Scheme forForward Linkages to NRHM in NE has beenintroduced in the 11th Plan with an outlay (to befinanced from likely savings from other Healthschemes) of Rs. 900 Crore. The scheme envisageshandholding the States in strengthening andupgrading select tertiary and secondary level healthfacilities in the States in a comprehensive manner.
The upgradation of Gauhati Medical College hasalready been approved and Rs. 30.00 Crorereleased during 2008-09 under the Scheme, whilethe proposal for upgradation/strengthening of StateCivil Hospital at Naharlagun, Arunachal Pradesh atan estimated cost of Rs. 130.00 Crore has also beenagreed to by the Planning Commission. DetailedProject Report(DPR) in this respect is being preparedby the Hospital Services Consultancy Corporation(HSCC) Ltd.
19.319.319.319.319.3 YYYYYaws Eradication Programme inaws Eradication Programme inaws Eradication Programme inaws Eradication Programme inaws Eradication Programme inNorth EastNorth EastNorth EastNorth EastNorth East
o Yaws is a disfiguring, disabilitating non-venereal bacterial infection and has beenendemic in India since long. Yaws is acontagious disease transmitted by direct(person-to-person) contact with the infectiousyaws lesion. Early lesions of this diseasemanifest in the form of skin lesions, which onhealing show little scarring. Yaws isamenable to eradication as it does not haveany extra human reservoir of infection,organism is sensitive to a single dose of longacting penicillin and yaws infection is limitedto a small pocket.
o Govt. of India approved Yaws EradicationProgramme (YEP) as a central sector healthscheme as a Pilot Project for undividedKoraput district, Orissa during the financialyear 1996-97. In March 1999, the programmewas extended to cover all 10 endemic states.In Assam, North-Cachar Hills district wasendemic.
o The strategy followed by NICD under YawsEradication Programme (YEP) includedtrained man power development, activedetection of cases and contacts, IECactivities harnessing multisectorial approach.
o The number of reported cases in the countryhas come down from more than 3500 to Nilduring the period from 1996 to 2003. Assamreported last case during 2002. Since then,no new case has been reported from any ofthe ten states under YEP, including Assam.
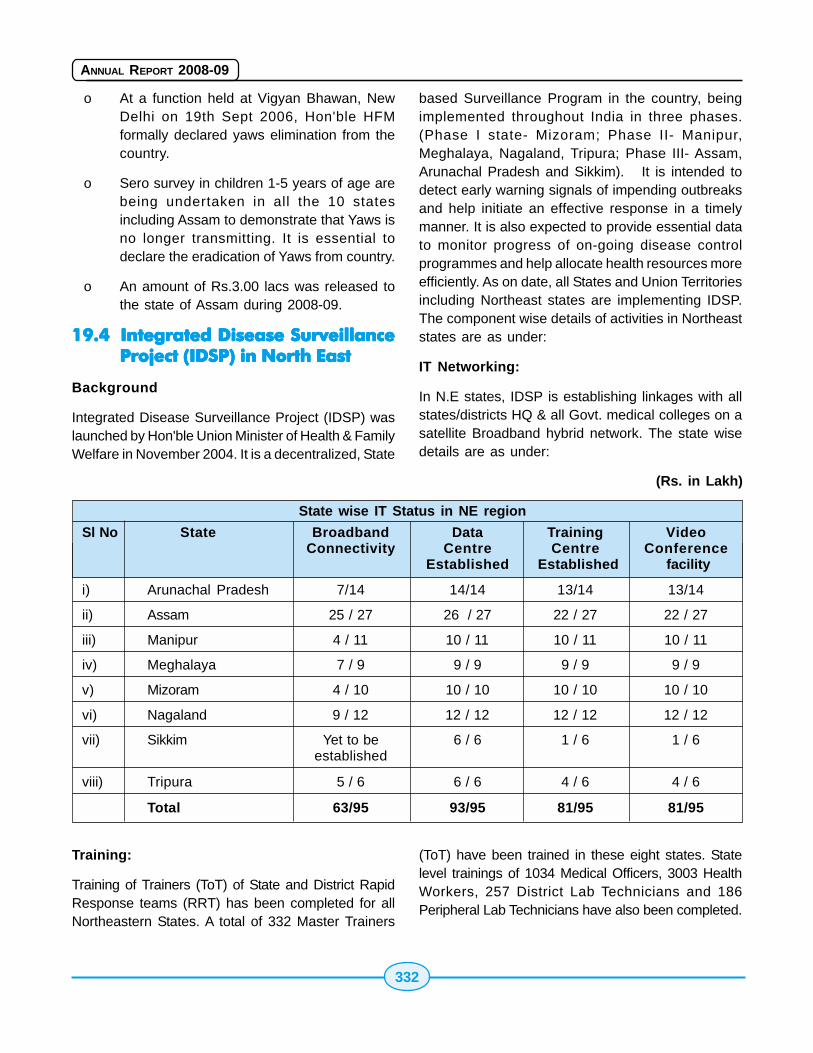
332
ANNUAL REPORT 2008-09
o At a function held at Vigyan Bhawan, NewDelhi on 19th Sept 2006, Hon'ble HFMformally declared yaws elimination from thecountry.
o Sero survey in children 1-5 years of age arebeing undertaken in all the 10 statesincluding Assam to demonstrate that Yaws isno longer transmitting. It is essential todeclare the eradication of Yaws from country.
o An amount of Rs.3.00 lacs was released tothe state of Assam during 2008-09.
19.419.419.419.419.4 Integrated Disease SurveillanceIntegrated Disease SurveillanceIntegrated Disease SurveillanceIntegrated Disease SurveillanceIntegrated Disease SurveillanceProject (Project (Project (Project (Project (IDSPIDSPIDSPIDSPIDSP) in North East) in North East) in North East) in North East) in North East
Background
Integrated Disease Surveillance Project (IDSP) waslaunched by Hon'ble Union Minister of Health & FamilyWelfare in November 2004. It is a decentralized, State
based Surveillance Program in the country, beingimplemented throughout India in three phases.(Phase I state- Mizoram; Phase II- Manipur,Meghalaya, Nagaland, Tripura; Phase III- Assam,Arunachal Pradesh and Sikkim). It is intended todetect early warning signals of impending outbreaksand help initiate an effective response in a timelymanner. It is also expected to provide essential datato monitor progress of on-going disease controlprogrammes and help allocate health resources moreefficiently. As on date, all States and Union Territoriesincluding Northeast states are implementing IDSP.The component wise details of activities in Northeaststates are as under:
IT Networking:
In N.E states, IDSP is establishing linkages with allstates/districts HQ & all Govt. medical colleges on asatellite Broadband hybrid network. The state wisedetails are as under:
(Rs. in Lakh)
State wise IT Status in NE region
Sl No State Broadband Data Training VideoConnectivity Centre Centre Conference
Established Established facility
i) Arunachal Pradesh 7/14 14/14 13/14 13/14
ii) Assam 25 / 27 26 / 27 22 / 27 22 / 27
iii) Manipur 4 / 11 10 / 11 10 / 11 10 / 11
iv) Meghalaya 7 / 9 9 / 9 9 / 9 9 / 9
v) Mizoram 4 / 10 10 / 10 10 / 10 10 / 10
vi) Nagaland 9 / 12 12 / 12 12 / 12 12 / 12
vii) Sikkim Yet to be 6 / 6 1 / 6 1 / 6established
viii) Tripura 5 / 6 6 / 6 4 / 6 4 / 6
Total 63/95 93/95 81/95 81/95
Training:
Training of Trainers (ToT) of State and District RapidResponse teams (RRT) has been completed for allNortheastern States. A total of 332 Master Trainers
(ToT) have been trained in these eight states. Statelevel trainings of 1034 Medical Officers, 3003 HealthWorkers, 257 District Lab Technicians and 186Peripheral Lab Technicians have also been completed.
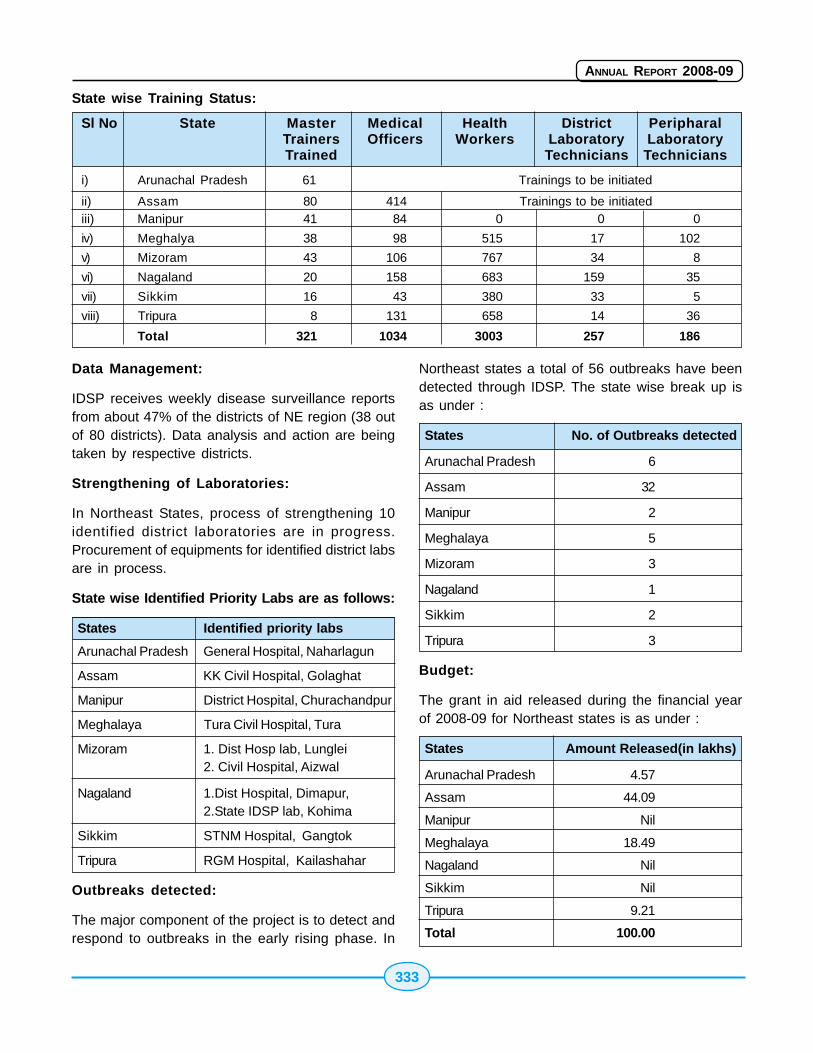
333
ANNUAL REPORT 2008-09
State wise Training Status:
Sl No State Master Medical Health District PeripharalTrainers Officers Workers Laboratory LaboratoryTrained Technicians Technicians
i) Arunachal Pradesh 61 Trainings to be initiated
ii) Assam 80 414 Trainings to be initiatediii) Manipur 41 84 0 0 0
iv) Meghalya 38 98 515 17 102
v) Mizoram 43 106 767 34 8
vi) Nagaland 20 158 683 159 35
vii) Sikkim 16 43 380 33 5
viii) Tripura 8 131 658 14 36
Total 321 1034 3003 257 186
Data Management:
IDSP receives weekly disease surveillance reportsfrom about 47% of the districts of NE region (38 outof 80 districts). Data analysis and action are beingtaken by respective districts.
Strengthening of Laboratories:
In Northeast States, process of strengthening 10identified district laboratories are in progress.Procurement of equipments for identified district labsare in process.
State wise Identified Priority Labs are as follows:
States Identified priority labs
Arunachal Pradesh General Hospital, Naharlagun
Assam KK Civil Hospital, Golaghat
Manipur District Hospital, Churachandpur
Meghalaya Tura Civil Hospital, Tura
Mizoram 1. Dist Hosp lab, Lunglei2. Civil Hospital, Aizwal
Nagaland 1.Dist Hospital, Dimapur,2.State IDSP lab, Kohima
Sikkim STNM Hospital, Gangtok
Tripura RGM Hospital, Kailashahar
Outbreaks detected:
The major component of the project is to detect andrespond to outbreaks in the early rising phase. In
Northeast states a total of 56 outbreaks have beendetected through IDSP. The state wise break up isas under :
States No. of Outbreaks detected
Arunachal Pradesh 6
Assam 32
Manipur 2
Meghalaya 5
Mizoram 3
Nagaland 1
Sikkim 2
Tripura 3
Budget:
The grant in aid released during the financial yearof 2008-09 for Northeast states is as under :
States Amount Released(in lakhs)
Arunachal Pradesh 4.57
Assam 44.09
Manipur Nil
Meghalaya 18.49
Nagaland Nil
Sikkim Nil
Tripura 9.21
Total 100.00
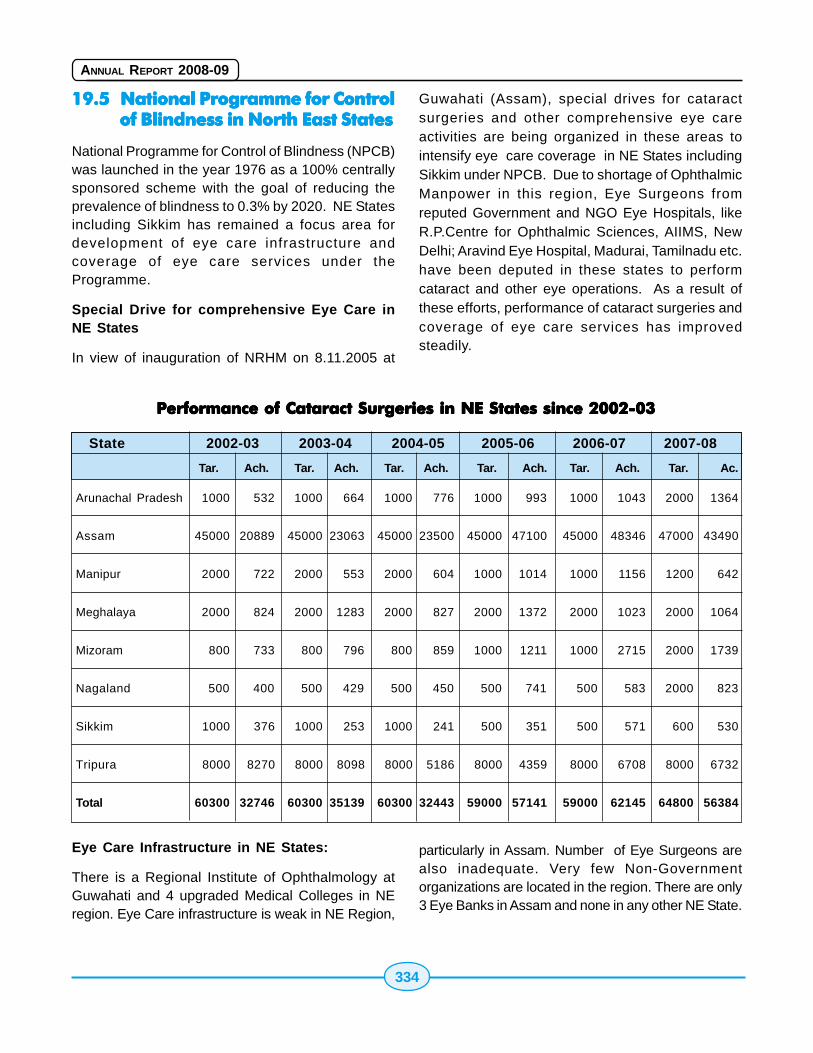
334
ANNUAL REPORT 2008-09
19.519.519.519.519.5 National Programme for ControlNational Programme for ControlNational Programme for ControlNational Programme for ControlNational Programme for Controlof Blindness in North East Statesof Blindness in North East Statesof Blindness in North East Statesof Blindness in North East Statesof Blindness in North East States
National Programme for Control of Blindness (NPCB)was launched in the year 1976 as a 100% centrallysponsored scheme with the goal of reducing theprevalence of blindness to 0.3% by 2020. NE Statesincluding Sikkim has remained a focus area fordevelopment of eye care infrastructure andcoverage of eye care services under theProgramme.
Special Drive for comprehensive Eye Care inNE States
In view of inauguration of NRHM on 8.11.2005 at
Guwahati (Assam), special drives for cataractsurgeries and other comprehensive eye careactivities are being organized in these areas tointensify eye care coverage in NE States includingSikkim under NPCB. Due to shortage of OphthalmicManpower in this region, Eye Surgeons fromreputed Government and NGO Eye Hospitals, likeR.P.Centre for Ophthalmic Sciences, AIIMS, NewDelhi; Aravind Eye Hospital, Madurai, Tamilnadu etc.have been deputed in these states to performcataract and other eye operations. As a result ofthese efforts, performance of cataract surgeries andcoverage of eye care services has improvedsteadily.
Performance of Cataract Surgeries in NE States since 2002-03Performance of Cataract Surgeries in NE States since 2002-03Performance of Cataract Surgeries in NE States since 2002-03Performance of Cataract Surgeries in NE States since 2002-03Performance of Cataract Surgeries in NE States since 2002-03
Eye Care Infrastructure in NE States:
There is a Regional Institute of Ophthalmology atGuwahati and 4 upgraded Medical Colleges in NEregion. Eye Care infrastructure is weak in NE Region,
particularly in Assam. Number of Eye Surgeons arealso inadequate. Very few Non-Governmentorganizations are located in the region. There are only3 Eye Banks in Assam and none in any other NE State.
State 2002-03 2003-04 2004-05 2005-06 2006-07 2007-08
Tar. Ach. Tar. Ach. Tar. Ach. Tar. Ach. Tar. Ach. Tar. Ac.
Arunachal Pradesh 1000 532 1000 664 1000 776 1000 993 1000 1043 2000 1364
Assam 45000 20889 45000 23063 45000 23500 45000 47100 45000 48346 47000 43490
Manipur 2000 722 2000 553 2000 604 1000 1014 1000 1156 1200 642
Meghalaya 2000 824 2000 1283 2000 827 2000 1372 2000 1023 2000 1064
Mizoram 800 733 800 796 800 859 1000 1211 1000 2715 2000 1739
Nagaland 500 400 500 429 500 450 500 741 500 583 2000 823
Sikkim 1000 376 1000 253 1000 241 500 351 500 571 600 530
Tripura 8000 8270 8000 8098 8000 5186 8000 4359 8000 6708 8000 6732
Total 60300 32746 60300 35139 60300 32443 59000 57141 59000 62145 64800 56384
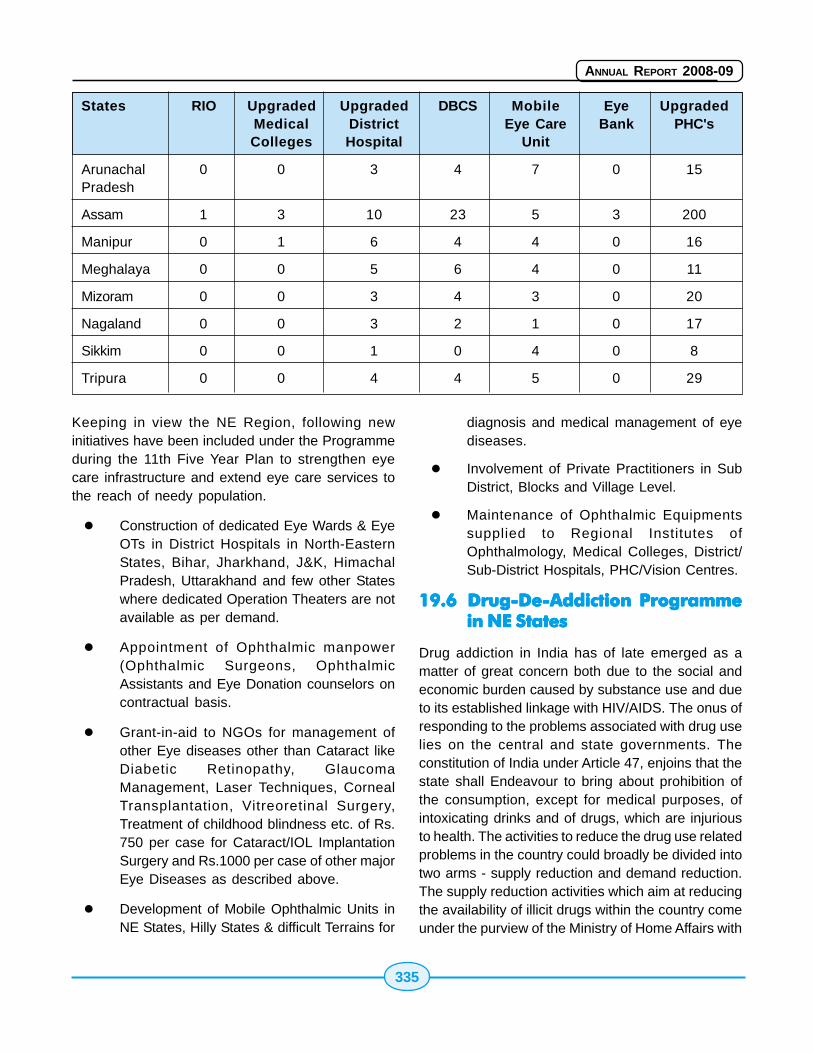
335
ANNUAL REPORT 2008-09
States RIO Upgraded Upgraded DBCS Mobile Eye UpgradedMedical District Eye Care Bank PHC'sColleges Hospital Unit
Arunachal 0 0 3 4 7 0 15Pradesh
Assam 1 3 10 23 5 3 200
Manipur 0 1 6 4 4 0 16
Meghalaya 0 0 5 6 4 0 11
Mizoram 0 0 3 4 3 0 20
Nagaland 0 0 3 2 1 0 17
Sikkim 0 0 1 0 4 0 8
Tripura 0 0 4 4 5 0 29
Keeping in view the NE Region, following newinitiatives have been included under the Programmeduring the 11th Five Year Plan to strengthen eyecare infrastructure and extend eye care services tothe reach of needy population.
� Construction of dedicated Eye Wards & EyeOTs in District Hospitals in North-EasternStates, Bihar, Jharkhand, J&K, HimachalPradesh, Uttarakhand and few other Stateswhere dedicated Operation Theaters are notavailable as per demand.
� Appointment of Ophthalmic manpower(Ophthalmic Surgeons, OphthalmicAssistants and Eye Donation counselors oncontractual basis.
� Grant-in-aid to NGOs for management ofother Eye diseases other than Cataract likeDiabetic Retinopathy, GlaucomaManagement, Laser Techniques, CornealTransplantation, Vitreoretinal Surgery,Treatment of childhood blindness etc. of Rs.750 per case for Cataract/IOL ImplantationSurgery and Rs.1000 per case of other majorEye Diseases as described above.
� Development of Mobile Ophthalmic Units inNE States, Hilly States & difficult Terrains for
diagnosis and medical management of eyediseases.
� Involvement of Private Practitioners in SubDistrict, Blocks and Village Level.
� Maintenance of Ophthalmic Equipmentssupplied to Regional Institutes ofOphthalmology, Medical Colleges, District/Sub-District Hospitals, PHC/Vision Centres.
19.619.619.619.619.6 Drug-De-Addiction ProgrammeDrug-De-Addiction ProgrammeDrug-De-Addiction ProgrammeDrug-De-Addiction ProgrammeDrug-De-Addiction Programmein NE Statesin NE Statesin NE Statesin NE Statesin NE States
Drug addiction in India has of late emerged as amatter of great concern both due to the social andeconomic burden caused by substance use and dueto its established linkage with HIV/AIDS. The onus ofresponding to the problems associated with drug uselies on the central and state governments. Theconstitution of India under Article 47, enjoins that thestate shall Endeavour to bring about prohibition ofthe consumption, except for medical purposes, ofintoxicating drinks and of drugs, which are injuriousto health. The activities to reduce the drug use relatedproblems in the country could broadly be divided intotwo arms - supply reduction and demand reduction.The supply reduction activities which aim at reducingthe availability of illicit drugs within the country comeunder the purview of the Ministry of Home Affairs with

336
ANNUAL REPORT 2008-09
the Department of Revenue as the nodal agency andare executed by various enforcement agencies. Thedemand reduction activities focus upon awarenessbuilding, treatment and rehabilitation of drug usingpatients. These activities are run by agencies underthe Ministry of Health and Family Welfare, and theMinistry of Social Justice and Empowerment
Role of Ministry of Health and Family Welfare
The role of Ministry of Health & Family Welfare in thearea of Drug De-addiction is demand reduction byway of providing treatment services. The Drug De-addiction Programme in the Ministry of Health &Family Welfare was started in the year 1987-88 whichwas later modified in 1992-93. The programme wasinitiated as a scheme with funding from the centralgovernment and implementation through the states.Under the scheme, a one time grant in aid of Rs.8.00 lakhs was given to states for construction ofeach Drug De-addiction Centre and a recurring grantof Rs. 2.00 lakhs was given to Drug De-addictionCentres established in North Eastern Regions tomeet the expenses on medications and otherrequirements. At present 122 such Centres havebeen established across the country includingcentres in Central Government hospitals andinstitutions of which 43 Centres have beenestablished in the North Eastern Region. Under thisprogramme, a national nodal centre, the "NationalDrug Dependence Treatment Centre", has beenestablished under the All India Institute of MedicalSciences (AIIMS), New Delhi which is located inGhaziabad while two centres i.e. NIMHANS, Bangloreand PGI, Chandigarh have also been upgraded bythis Ministry. The purpose of these centres wouldnot only to provide de-addiction and rehabilitationservices to the patients but also to conduct researchand provide training to medical doctors in the areaof drug de-addiction. During current financial year(2008 -2009) we have released an amount of Rs.16.00 Lakh as recurring grant to 8 de-addictioncentres @ Rs. 2.00 lakh up to 31st December 2008.The National Drug Dependence Treatment Centre,AIIMS is also responsible to develop to upgrade theknowledge and improve the de-addiction facilities inthe North Eastern Region.
Community Based Project to Control SubstanceUse Disorder in N.E. Region
The National Centre of Drug De-addictionProgramme of Ministry of Health and Family Welfarei.e. National Drug Dependence Treatment Centre hasinitiated a community-based project for strengtheningdrug-dependence treatment services at the districtlevel in one of the north east states of India. CurrentlyNDDTC, AIIMS is implementing this project at DistrictMoregaon in Assam. This project has been fundedby the Drug De-addiction Programme of Ministry ofHealth and Family Welfare. The project is beingimplemented in collaboration with the Department ofPsychiatry, Medical College, Guwahati and the districtadministration, Moregaon of Assam. Total area of thedistrict is 1704 Sq.km. and the population being about10 lacs and has sizable tribal population about 16%.The district has 1 civil hospital, 3 PHCs, 2 CHCs and125 sub-centres. In the Moregaon the majorsubstance of alcohol abuse is Alcohol. TheMoregaon district has chosen as no facilities fortreatment of substance use disorder in the districtwas available.
The findings from this project will be helpful indesigning such projects and implementing them inother areas of the country. The unique feature ofthe project is collaboration between academia, localadministration as well as the local health-caresystem. Various activities will be designed as per theidentified needs of the community. At every step theproject envisages to move ahead in the participatorymanner implementing all the activities in a 'bottoms-up' approach.
19.719.719.719.719.7 National VNational VNational VNational VNational Vector Borne Diseaseector Borne Diseaseector Borne Diseaseector Borne Diseaseector Borne DiseaseControl Programme in North EastControl Programme in North EastControl Programme in North EastControl Programme in North EastControl Programme in North EastStatesStatesStatesStatesStates
Malaria situation in Northeastern states
NE states namely Arunachal Pradesh, Assam,Meghalaya, Mizoram, Manipur, Nagaland, Sikkim andTripura together contribute 4% of the country'spopulation 12% of malaria cases, 17% of Pf casesand 33% of malaria deaths reported in the countryduring 2008.
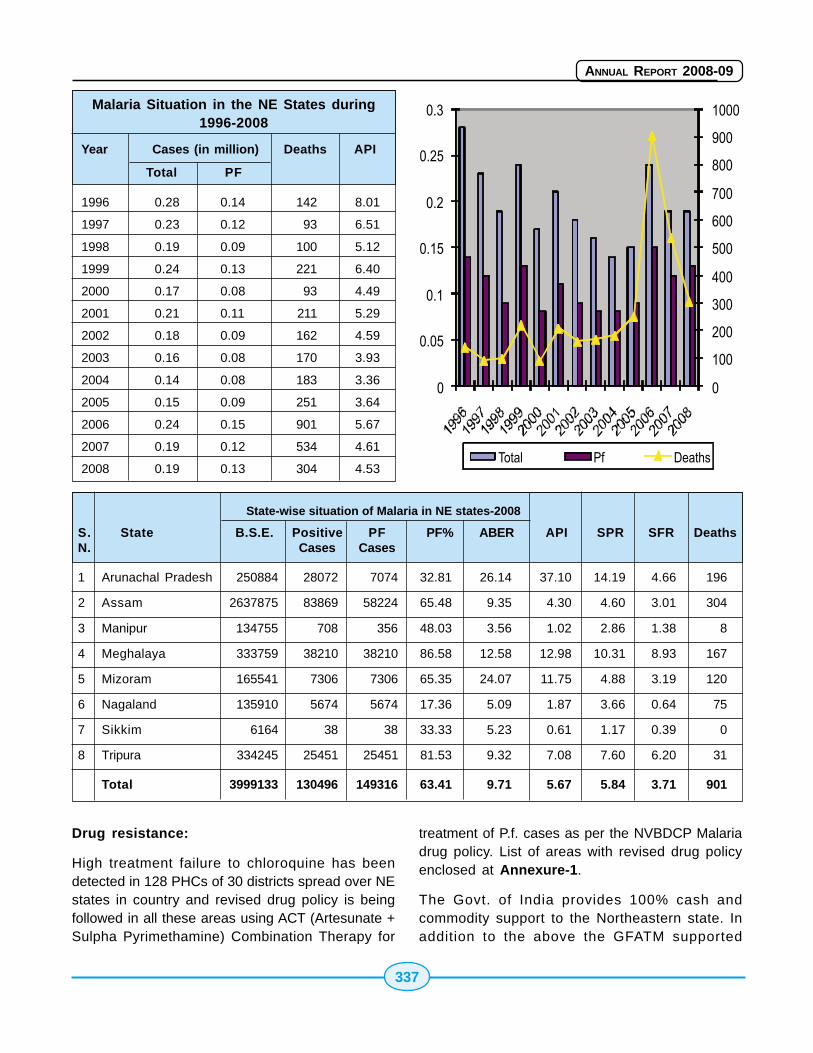
337
ANNUAL REPORT 2008-09
State-wise situation of Malaria in NE states-2008
S. State B.S.E. Positive PF PF% ABER API SPR SFR DeathsN. Cases Cases
1 Arunachal Pradesh 250884 28072 7074 32.81 26.14 37.10 14.19 4.66 196
2 Assam 2637875 83869 58224 65.48 9.35 4.30 4.60 3.01 304
3 Manipur 134755 708 356 48.03 3.56 1.02 2.86 1.38 8
4 Meghalaya 333759 38210 38210 86.58 12.58 12.98 10.31 8.93 167
5 Mizoram 165541 7306 7306 65.35 24.07 11.75 4.88 3.19 120
6 Nagaland 135910 5674 5674 17.36 5.09 1.87 3.66 0.64 75
7 Sikkim 6164 38 38 33.33 5.23 0.61 1.17 0.39 0
8 Tripura 334245 25451 25451 81.53 9.32 7.08 7.60 6.20 31
Total 3999133 130496 149316 63.41 9.71 5.67 5.84 3.71 901
Malaria Situation in the NE States during1996-2008
Year Cases (in million) Deaths API
Total PF
1996 0.28 0.14 142 8.01
1997 0.23 0.12 93 6.51
1998 0.19 0.09 100 5.12
1999 0.24 0.13 221 6.40
2000 0.17 0.08 93 4.49
2001 0.21 0.11 211 5.29
2002 0.18 0.09 162 4.59
2003 0.16 0.08 170 3.93
2004 0.14 0.08 183 3.36
2005 0.15 0.09 251 3.64
2006 0.24 0.15 901 5.67
2007 0.19 0.12 534 4.61
2008 0.19 0.13 304 4.53
Drug resistance:
High treatment failure to chloroquine has beendetected in 128 PHCs of 30 districts spread over NEstates in country and revised drug policy is beingfollowed in all these areas using ACT (Artesunate +Sulpha Pyrimethamine) Combination Therapy for
treatment of P.f. cases as per the NVBDCP Malariadrug policy. List of areas with revised drug policyenclosed at Annexure-1.
The Govt. of India provides 100% cash andcommodity support to the Northeastern state. Inaddition to the above the GFATM supported
338
ANNUAL REPORT 2008-09
"Intensified Malaria Control Project" is beingimplemented in the state. National Vector BorneDisease Control Programme is the national nodalagency for the prevention and control of major vectorborne diseases of public health importance namelyMalaria, Filaria, Japanese Encephalitis (JE), Kala-Azar, Dengue and Chikungunya. NVBDCP providestechnical support, antimalarial drug, insecticides,larvicides and bed nets. Assistance is also providedfor training and IEC. The State Governments areresponsible for programme implementation,infrastructure and decentralized logistics. SinceDecember 1994, Govt. of India is providing 100%central assistance (under Plan budget) to 7 N.E.States. Sikkim is also being provided 100% centralassistance since 2003-2004.
Govt. of India is implementing three prongedstrategies as indicated below:-
I Disease Management
* Early case Detection and Prompt Treatment(EDPT).
* Strengthening of referral services
* Epidemic preparedness and rapid response
II Integrated Vector Management forreducing mosquitoes density
* Indoor Residual Spraying in selected high riskareas
* Use of Insecticide treated bed nets
* Use of Larvivorous fishes in the perennialwater bodies.
* Anti larval measures in urban areas includingbiolarvicides
* Minor environmental engineering
III Supporting Interventions:
* Behavior Change Communication
* Public Private Partnership & Inter-sectoralconvergence
* Human Resource Development throughcapacity building
* Operational research including studies ondrug resistance and insecticide susceptibility.
* Monitoring and evaluation through periodicreview/field visits and operationalisation ofweb-based computerized National AntiMalaria Management Information System(NAMMIS).
The Global Fund supported Intensified MalariaControl Project (IMCP)
The GFATM project focuses on the poor andvulnerable groups settled in the poorest and thedifficult terrain parts of the country. About 37 millionpopulation is estimated to live in chloroquine resistantareas, of which about 75% lives in the project area.The criteria for including 100 million population in106 districts in 10 states namely 7 NE States andselected high risk areas of Orissa, Jharkhand andWest Bengal is based on the disease burden due tomalaria - 0.46 million cases out of a total of 1.84million and 464 deaths out of a total of 973 in 2002were from these districts (9.76% population reporting25% of total cases and 47% of deaths).
Goal of the proposal is to reduce malaria morbidityand mortality in 100 million population in 10 statesby 30% and by 50% respectively within 5 years. Theproject has following objectives:
i. Increase access to diagnosis and treatmentin high endemic areas, with particular focuson remote and inaccessible areas throughcommunity participation, upgradation ofperipheral health facilities and small hospitalsin the diagnosis and treatment of severemalaria
ii. Malaria Transmission Risk Reduction throughintegrated vector control
iii. Enhance awareness about malaria controland promote community, NGO and privatesector participation
The strategies of the project are Early diagnosis andprompt treatment with special reference to the drugresistant pockets, integrated vector control, includingpromotion of ITN, use of larvivorous fish throughintensive IEC and capacity building and efficientpublic-private partnership among, CBO, NGO, andother voluntary sectors and training the healthworkers, community volunteers.
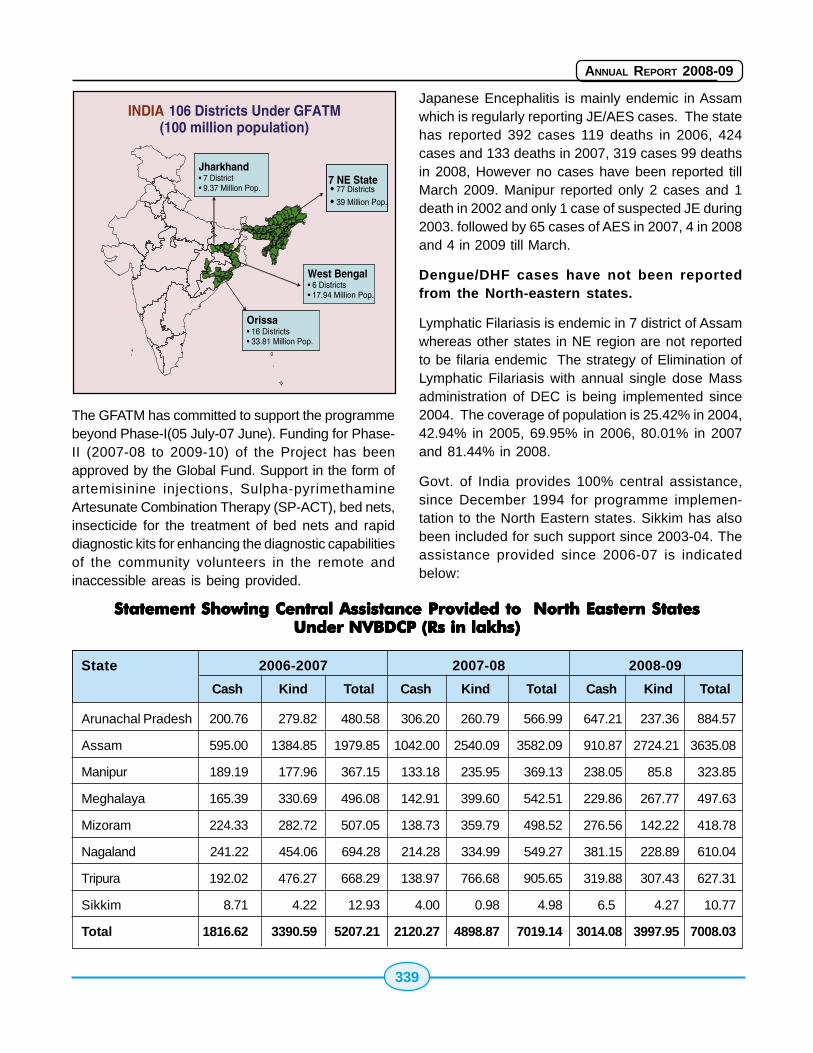
339
ANNUAL REPORT 2008-09
Japanese Encephalitis is mainly endemic in Assamwhich is regularly reporting JE/AES cases. The statehas reported 392 cases 119 deaths in 2006, 424cases and 133 deaths in 2007, 319 cases 99 deathsin 2008, However no cases have been reported tillMarch 2009. Manipur reported only 2 cases and 1death in 2002 and only 1 case of suspected JE during2003. followed by 65 cases of AES in 2007, 4 in 2008and 4 in 2009 till March.
Dengue/DHF cases have not been reportedfrom the North-eastern states.
Lymphatic Filariasis is endemic in 7 district of Assamwhereas other states in NE region are not reportedto be filaria endemic The strategy of Elimination ofLymphatic Filariasis with annual single dose Massadministration of DEC is being implemented since2004. The coverage of population is 25.42% in 2004,42.94% in 2005, 69.95% in 2006, 80.01% in 2007and 81.44% in 2008.
Govt. of India provides 100% central assistance,since December 1994 for programme implemen-tation to the North Eastern states. Sikkim has alsobeen included for such support since 2003-04. Theassistance provided since 2006-07 is indicatedbelow:
Statement Showing Central Assistance Provided to North Eastern StatesStatement Showing Central Assistance Provided to North Eastern StatesStatement Showing Central Assistance Provided to North Eastern StatesStatement Showing Central Assistance Provided to North Eastern StatesStatement Showing Central Assistance Provided to North Eastern StatesUnder NVBDCP Under NVBDCP Under NVBDCP Under NVBDCP Under NVBDCP (Rs in lakhs)(Rs in lakhs)(Rs in lakhs)(Rs in lakhs)(Rs in lakhs)
The GFATM has committed to support the programmebeyond Phase-I(05 July-07 June). Funding for Phase-II (2007-08 to 2009-10) of the Project has beenapproved by the Global Fund. Support in the form ofartemisinine injections, Sulpha-pyrimethamineArtesunate Combination Therapy (SP-ACT), bed nets,insecticide for the treatment of bed nets and rapiddiagnostic kits for enhancing the diagnostic capabilitiesof the community volunteers in the remote andinaccessible areas is being provided.
State 2006-2007 2007-08 2008-09
Cash Kind Total Cash Kind Total Cash Kind Total
Arunachal Pradesh 200.76 279.82 480.58 306.20 260.79 566.99 647.21 237.36 884.57
Assam 595.00 1384.85 1979.85 1042.00 2540.09 3582.09 910.87 2724.21 3635.08
Manipur 189.19 177.96 367.15 133.18 235.95 369.13 238.05 85.8 323.85
Meghalaya 165.39 330.69 496.08 142.91 399.60 542.51 229.86 267.77 497.63
Mizoram 224.33 282.72 507.05 138.73 359.79 498.52 276.56 142.22 418.78
Nagaland 241.22 454.06 694.28 214.28 334.99 549.27 381.15 228.89 610.04
Tripura 192.02 476.27 668.29 138.97 766.68 905.65 319.88 307.43 627.31
Sikkim 8.71 4.22 12.93 4.00 0.98 4.98 6.5 4.27 10.77
Total 1816.62 3390.59 5207.21 2120.27 4898.87 7019.14 3014.08 3997.95 7008.03
340
ANNUAL REPORT 2008-09
19.819.819.819.819.8 The National Iodine DeficiencyThe National Iodine DeficiencyThe National Iodine DeficiencyThe National Iodine DeficiencyThe National Iodine DeficiencyDisorders Control ProgrammeDisorders Control ProgrammeDisorders Control ProgrammeDisorders Control ProgrammeDisorders Control Programme(((((NIDDCPNIDDCPNIDDCPNIDDCPNIDDCP) in ) in ) in ) in ) in NENENENENE
The National Iodine Deficiency Disorders ControlProgramme (NIDDCP) is being implemented in all theNorth Eastern States including Sikkim. IDDprevalence surveys have been conducted in all thestates. State level IDD Control Cell has been set up,in all the NE States. However, IDD monitoringlaboratory is yet to be set up in the state of Assam.Resurveys done in the State of Arunachal Pradesh,Manipur and Mizoram have indicated a decline inthe prevalence of IDD as a result of iodated saltconsumption.
19.919.919.919.919.9 National Leprosy EradicationNational Leprosy EradicationNational Leprosy EradicationNational Leprosy EradicationNational Leprosy EradicationProgramme in NEProgramme in NEProgramme in NEProgramme in NEProgramme in NE
All the States of north east region have achievedelimination of leprosy at state and also at district level,except for 2 districts in Arunachal Pradesh andNagaland. As on March 2008, there were 1424 leprosycases on record in these states giving a PR of 0.32/10,000 population. During the year, 1573 new leprosycases were detected with Annual New Case DetectionRate of 3.57/1,00,000 population. North east regioncontributed to 3.82% of country's population and only1.1% of country's new cases detected during the year.Leprosy services have already been integrated withGeneral Health Care system in all NE states andleprosy diagnosis and treatment (MDT) services areavailable in all the PHCs and Government hospitals/dispensaries. All the Medical Officers and GHC staffare being adequately trained in leprosy. The districtnucleus teams are being actively involved inprogramme monitoring and supervision.
19.1019.1019.1019.1019.10 Revised National TB ControlRevised National TB ControlRevised National TB ControlRevised National TB ControlRevised National TB ControlProgramme in NEProgramme in NEProgramme in NEProgramme in NEProgramme in NE
The entire population of the North Eastern statesincluding Sikkim has been covered under the RevisedNational TB Control Programme (RNTCP).
o Over the years, a strong network of RNTCPdiagnostic and treatment services has beenestablished in NE States through the generalhealth system. 136 sub-district TB Units and601 RNTCP Designated Microscopy centres
have been upgraded till date. As the NE regionhas large proportion of tribal and hard to reachareas, the norms for establishing Microscopycentres has been relaxed from 1 per 100,000population to 50,000 and the TB Units forevery 250,000 (as against 500,000).
o The states have shown considerableimprovement in programme performance,and in 2007, the new smear positive casedetection rate for the region was 55%,treatment success rate has been consistentlymaintained over 85%.
o RNTCP has initiated over 58 thousandpatients on treatment in 2007, thus savingover 11 thousand additional lives in the NorthEast Region.
o The programme has collaborated with privateand public sector health institutions in thearea. Innovative methods have beensuccessfully implemented with the teagardens in Assam. Collaboration with thedefence health services has also beenachieved in some of the states.
o HIV-TB coordination activities have beenimplemented in all the North Eastern states.Cross referral activities are being reportedby all the states.
New activities under RNTCP are:
o Procurement and distribution of paediatricdrug boxes for improved care of paediatriccases is currently in progress.
o Quality sputum microscopy is an importantcomponent of RNTCP. All the states in NorthEast have implemented the External QualityAssurance (EQA) protocol. Scaling up of theState-level intermediate referral laboratories(IRL) capacity for implementation of externalquality assessment (EQA) of sputum smearmicroscopy services and provision of cultureand drug sensitivity testing.
� Guwahati, Assam
� Sikkim
� Manipur
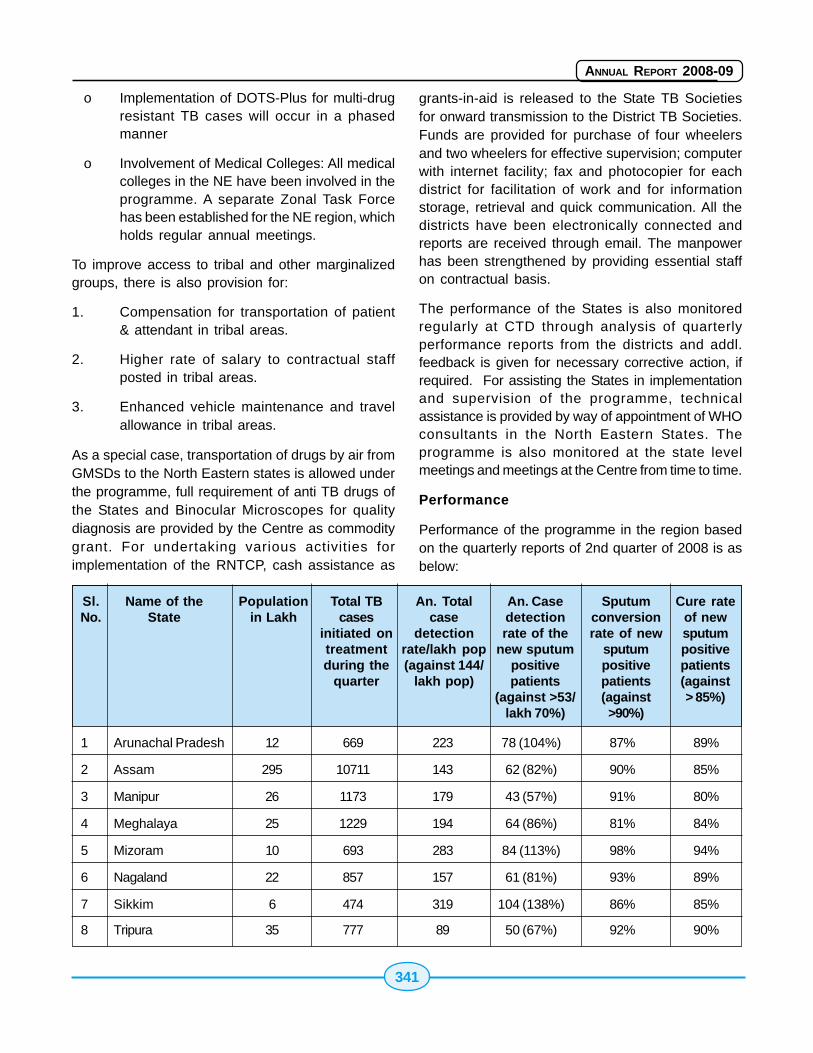
341
ANNUAL REPORT 2008-09
o Implementation of DOTS-Plus for multi-drugresistant TB cases will occur in a phasedmanner
o Involvement of Medical Colleges: All medicalcolleges in the NE have been involved in theprogramme. A separate Zonal Task Forcehas been established for the NE region, whichholds regular annual meetings.
To improve access to tribal and other marginalizedgroups, there is also provision for:
1. Compensation for transportation of patient& attendant in tribal areas.
2. Higher rate of salary to contractual staffposted in tribal areas.
3. Enhanced vehicle maintenance and travelallowance in tribal areas.
As a special case, transportation of drugs by air fromGMSDs to the North Eastern states is allowed underthe programme, full requirement of anti TB drugs ofthe States and Binocular Microscopes for qualitydiagnosis are provided by the Centre as commoditygrant. For undertaking various activities forimplementation of the RNTCP, cash assistance as
grants-in-aid is released to the State TB Societiesfor onward transmission to the District TB Societies.Funds are provided for purchase of four wheelersand two wheelers for effective supervision; computerwith internet facility; fax and photocopier for eachdistrict for facilitation of work and for informationstorage, retrieval and quick communication. All thedistricts have been electronically connected andreports are received through email. The manpowerhas been strengthened by providing essential staffon contractual basis.
The performance of the States is also monitoredregularly at CTD through analysis of quarterlyperformance reports from the districts and addl.feedback is given for necessary corrective action, ifrequired. For assisting the States in implementationand supervision of the programme, technicalassistance is provided by way of appointment of WHOconsultants in the North Eastern States. Theprogramme is also monitored at the state levelmeetings and meetings at the Centre from time to time.
Performance
Performance of the programme in the region basedon the quarterly reports of 2nd quarter of 2008 is asbelow:
Sl.No.
Name of theState
Populationin Lakh
Total TBcases
initiated ontreatmentduring the
quarter
An. Totalcase
detectionrate/lakh pop(against 144/
lakh pop)
An. Casedetectionrate of the
new sputumpositivepatients
(against >53/lakh 70%)
Sputumconversionrate of new
sputumpositivepatients(against>90%)
Cure rateof newsputumpositivepatients(against> 85%)
1 Arunachal Pradesh 12 669 223 78 (104%) 87% 89%
2 Assam 295 10711 143 62 (82%) 90% 85%
3 Manipur 26 1173 179 43 (57%) 91% 80%
4 Meghalaya 25 1229 194 64 (86%) 81% 84%
5 Mizoram 10 693 283 84 (113%) 98% 94%
6 Nagaland 22 857 157 61 (81%) 93% 89%
7 Sikkim 6 474 319 104 (138%) 86% 85%
8 Tripura 35 777 89 50 (67%) 92% 90%
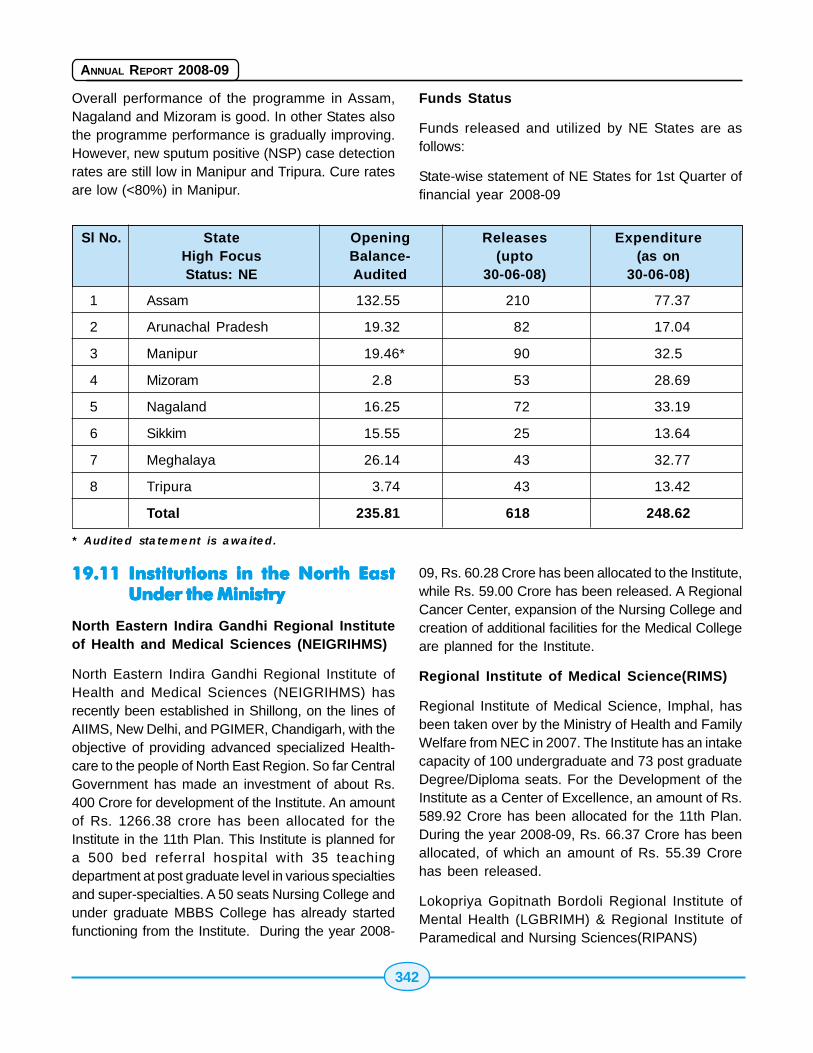
342
ANNUAL REPORT 2008-09
Overall performance of the programme in Assam,Nagaland and Mizoram is good. In other States alsothe programme performance is gradually improving.However, new sputum positive (NSP) case detectionrates are still low in Manipur and Tripura. Cure ratesare low (<80%) in Manipur.
Funds Status
Funds released and utilized by NE States are asfollows:
State-wise statement of NE States for 1st Quarter offinancial year 2008-09
Sl No. State Opening Releases ExpenditureHigh Focus Balance- (upto (as onStatus: NE Audited 30-06-08) 30-06-08)
1 Assam 132.55 210 77.37
2 Arunachal Pradesh 19.32 82 17.04
3 Manipur 19.46* 90 32.5
4 Mizoram 2.8 53 28.69
5 Nagaland 16.25 72 33.19
6 Sikkim 15.55 25 13.64
7 Meghalaya 26.14 43 32.77
8 Tripura 3.74 43 13.42
Total 235.81 618 248.62
* Audited statement is awaited.
19.1119.1119.1119.1119.11 Institutions in the North EastInstitutions in the North EastInstitutions in the North EastInstitutions in the North EastInstitutions in the North EastUnder the MinistryUnder the MinistryUnder the MinistryUnder the MinistryUnder the Ministry
North Eastern Indira Gandhi Regional Instituteof Health and Medical Sciences (NEIGRIHMS)
North Eastern Indira Gandhi Regional Institute ofHealth and Medical Sciences (NEIGRIHMS) hasrecently been established in Shillong, on the lines ofAIIMS, New Delhi, and PGIMER, Chandigarh, with theobjective of providing advanced specialized Health-care to the people of North East Region. So far CentralGovernment has made an investment of about Rs.400 Crore for development of the Institute. An amountof Rs. 1266.38 crore has been allocated for theInstitute in the 11th Plan. This Institute is planned fora 500 bed referral hospital with 35 teachingdepartment at post graduate level in various specialtiesand super-specialties. A 50 seats Nursing College andunder graduate MBBS College has already startedfunctioning from the Institute. During the year 2008-
09, Rs. 60.28 Crore has been allocated to the Institute,while Rs. 59.00 Crore has been released. A RegionalCancer Center, expansion of the Nursing College andcreation of additional facilities for the Medical Collegeare planned for the Institute.
Regional Institute of Medical Science(RIMS)
Regional Institute of Medical Science, Imphal, hasbeen taken over by the Ministry of Health and FamilyWelfare from NEC in 2007. The Institute has an intakecapacity of 100 undergraduate and 73 post graduateDegree/Diploma seats. For the Development of theInstitute as a Center of Excellence, an amount of Rs.589.92 Crore has been allocated for the 11th Plan.During the year 2008-09, Rs. 66.37 Crore has beenallocated, of which an amount of Rs. 55.39 Crorehas been released.
Lokopriya Gopitnath Bordoli Regional Institute ofMental Health (LGBRIMH) & Regional Institute ofParamedical and Nursing Sciences(RIPANS)
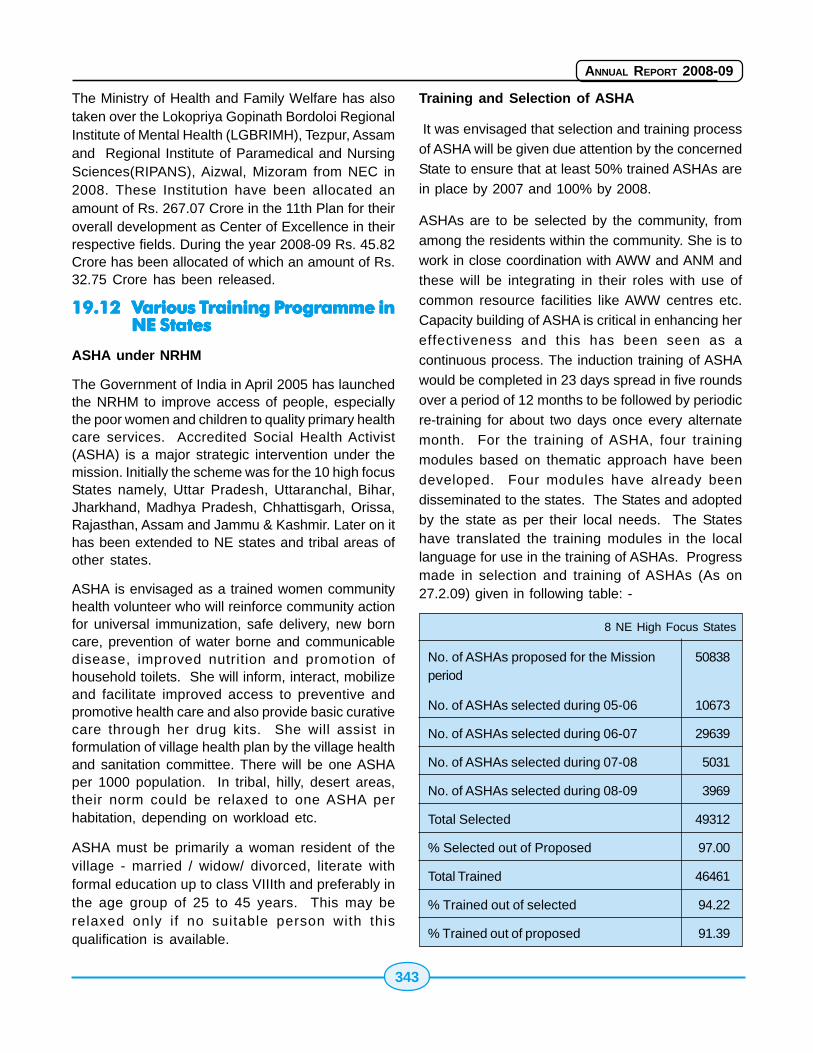
343
ANNUAL REPORT 2008-09
The Ministry of Health and Family Welfare has alsotaken over the Lokopriya Gopinath Bordoloi RegionalInstitute of Mental Health (LGBRIMH), Tezpur, Assamand Regional Institute of Paramedical and NursingSciences(RIPANS), Aizwal, Mizoram from NEC in2008. These Institution have been allocated anamount of Rs. 267.07 Crore in the 11th Plan for theiroverall development as Center of Excellence in theirrespective fields. During the year 2008-09 Rs. 45.82Crore has been allocated of which an amount of Rs.32.75 Crore has been released.
19.1219.1219.1219.1219.12 VVVVVarious Tarious Tarious Tarious Tarious Training Programme inraining Programme inraining Programme inraining Programme inraining Programme inNE StatesNE StatesNE StatesNE StatesNE States
ASHA under NRHM
The Government of India in April 2005 has launchedthe NRHM to improve access of people, especiallythe poor women and children to quality primary healthcare services. Accredited Social Health Activist(ASHA) is a major strategic intervention under themission. Initially the scheme was for the 10 high focusStates namely, Uttar Pradesh, Uttaranchal, Bihar,Jharkhand, Madhya Pradesh, Chhattisgarh, Orissa,Rajasthan, Assam and Jammu & Kashmir. Later on ithas been extended to NE states and tribal areas ofother states.
ASHA is envisaged as a trained women communityhealth volunteer who will reinforce community actionfor universal immunization, safe delivery, new borncare, prevention of water borne and communicabledisease, improved nutrition and promotion ofhousehold toilets. She will inform, interact, mobilizeand facilitate improved access to preventive andpromotive health care and also provide basic curativecare through her drug kits. She will assist informulation of village health plan by the village healthand sanitation committee. There will be one ASHAper 1000 population. In tribal, hilly, desert areas,their norm could be relaxed to one ASHA perhabitation, depending on workload etc.
ASHA must be primarily a woman resident of thevillage - married / widow/ divorced, literate withformal education up to class VIIIth and preferably inthe age group of 25 to 45 years. This may berelaxed only if no suitable person with thisqualification is available.
Training and Selection of ASHA
It was envisaged that selection and training processof ASHA will be given due attention by the concernedState to ensure that at least 50% trained ASHAs arein place by 2007 and 100% by 2008.
ASHAs are to be selected by the community, fromamong the residents within the community. She is towork in close coordination with AWW and ANM andthese will be integrating in their roles with use ofcommon resource facilities like AWW centres etc.Capacity building of ASHA is critical in enhancing hereffectiveness and this has been seen as acontinuous process. The induction training of ASHAwould be completed in 23 days spread in five roundsover a period of 12 months to be followed by periodicre-training for about two days once every alternatemonth. For the training of ASHA, four trainingmodules based on thematic approach have beendeveloped. Four modules have already beendisseminated to the states. The States and adoptedby the state as per their local needs. The Stateshave translated the training modules in the locallanguage for use in the training of ASHAs. Progressmade in selection and training of ASHAs (As on27.2.09) given in following table: -
8 NE High Focus States
No. of ASHAs proposed for the Mission 50838period
No. of ASHAs selected during 05-06 10673
No. of ASHAs selected during 06-07 29639
No. of ASHAs selected during 07-08 5031
No. of ASHAs selected during 08-09 3969
Total Selected 49312
% Selected out of Proposed 97.00
Total Trained 46461
% Trained out of selected 94.22
% Trained out of proposed 91.39
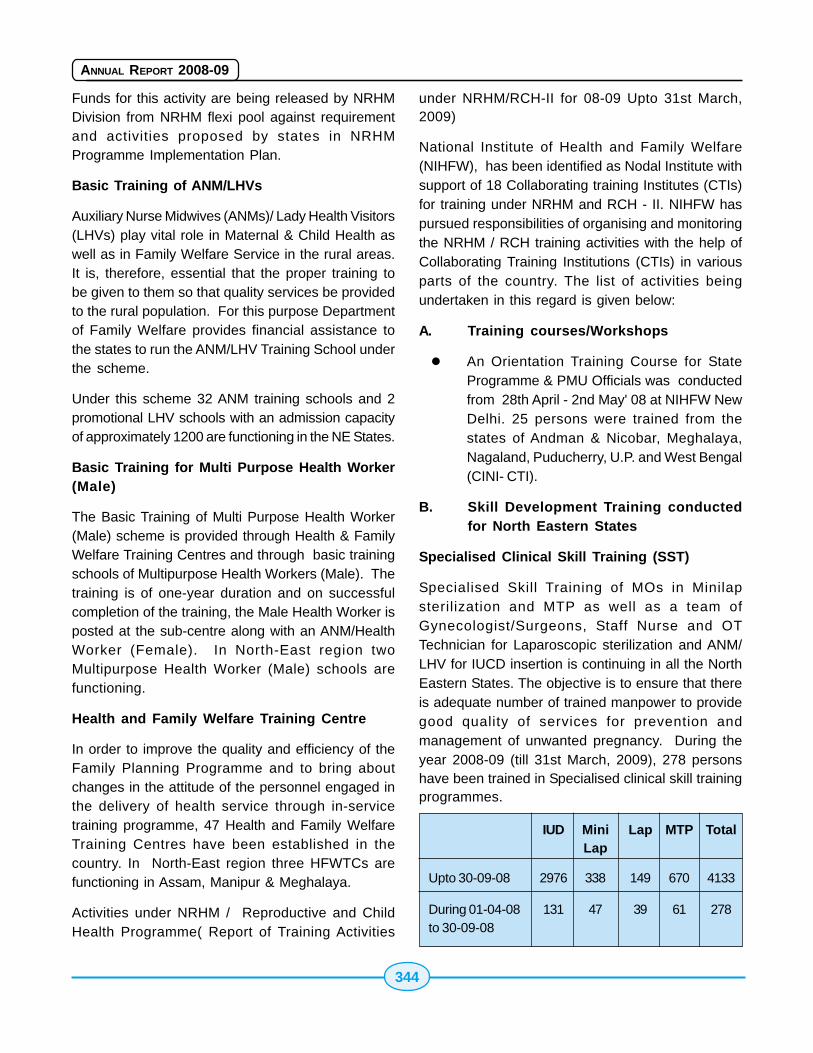
344
ANNUAL REPORT 2008-09
Funds for this activity are being released by NRHMDivision from NRHM flexi pool against requirementand activities proposed by states in NRHMProgramme Implementation Plan.
Basic Training of ANM/LHVs
Auxiliary Nurse Midwives (ANMs)/ Lady Health Visitors(LHVs) play vital role in Maternal & Child Health aswell as in Family Welfare Service in the rural areas.It is, therefore, essential that the proper training tobe given to them so that quality services be providedto the rural population. For this purpose Departmentof Family Welfare provides financial assistance tothe states to run the ANM/LHV Training School underthe scheme.
Under this scheme 32 ANM training schools and 2promotional LHV schools with an admission capacityof approximately 1200 are functioning in the NE States.
Basic Training for Multi Purpose Health Worker(Male)
The Basic Training of Multi Purpose Health Worker(Male) scheme is provided through Health & FamilyWelfare Training Centres and through basic trainingschools of Multipurpose Health Workers (Male). Thetraining is of one-year duration and on successfulcompletion of the training, the Male Health Worker isposted at the sub-centre along with an ANM/HealthWorker (Female). In North-East region twoMultipurpose Health Worker (Male) schools arefunctioning.
Health and Family Welfare Training Centre
In order to improve the quality and efficiency of theFamily Planning Programme and to bring aboutchanges in the attitude of the personnel engaged inthe delivery of health service through in-servicetraining programme, 47 Health and Family WelfareTraining Centres have been established in thecountry. In North-East region three HFWTCs arefunctioning in Assam, Manipur & Meghalaya.
Activities under NRHM / Reproductive and ChildHealth Programme( Report of Training Activities
under NRHM/RCH-II for 08-09 Upto 31st March,2009)
National Institute of Health and Family Welfare(NIHFW), has been identified as Nodal Institute withsupport of 18 Collaborating training Institutes (CTIs)for training under NRHM and RCH - II. NIHFW haspursued responsibilities of organising and monitoringthe NRHM / RCH training activities with the help ofCollaborating Training Institutions (CTIs) in variousparts of the country. The list of activities beingundertaken in this regard is given below:
A. Training courses/Workshops
� An Orientation Training Course for StateProgramme & PMU Officials was conductedfrom 28th April - 2nd May' 08 at NIHFW NewDelhi. 25 persons were trained from thestates of Andman & Nicobar, Meghalaya,Nagaland, Puducherry, U.P. and West Bengal(CINI- CTI).
B. Skill Development Training conductedfor North Eastern States
Specialised Clinical Skill Training (SST)
Specialised Skill Training of MOs in Minilapsterilization and MTP as well as a team ofGynecologist/Surgeons, Staff Nurse and OTTechnician for Laparoscopic sterilization and ANM/LHV for IUCD insertion is continuing in all the NorthEastern States. The objective is to ensure that thereis adequate number of trained manpower to providegood quality of services for prevention andmanagement of unwanted pregnancy. During theyear 2008-09 (till 31st March, 2009), 278 personshave been trained in Specialised clinical skill trainingprogrammes.
IUD Mini Lap MTP TotalLap
Upto 30-09-08 2976 338 149 670 4133
During 01-04-08 131 47 39 61 278to 30-09-08
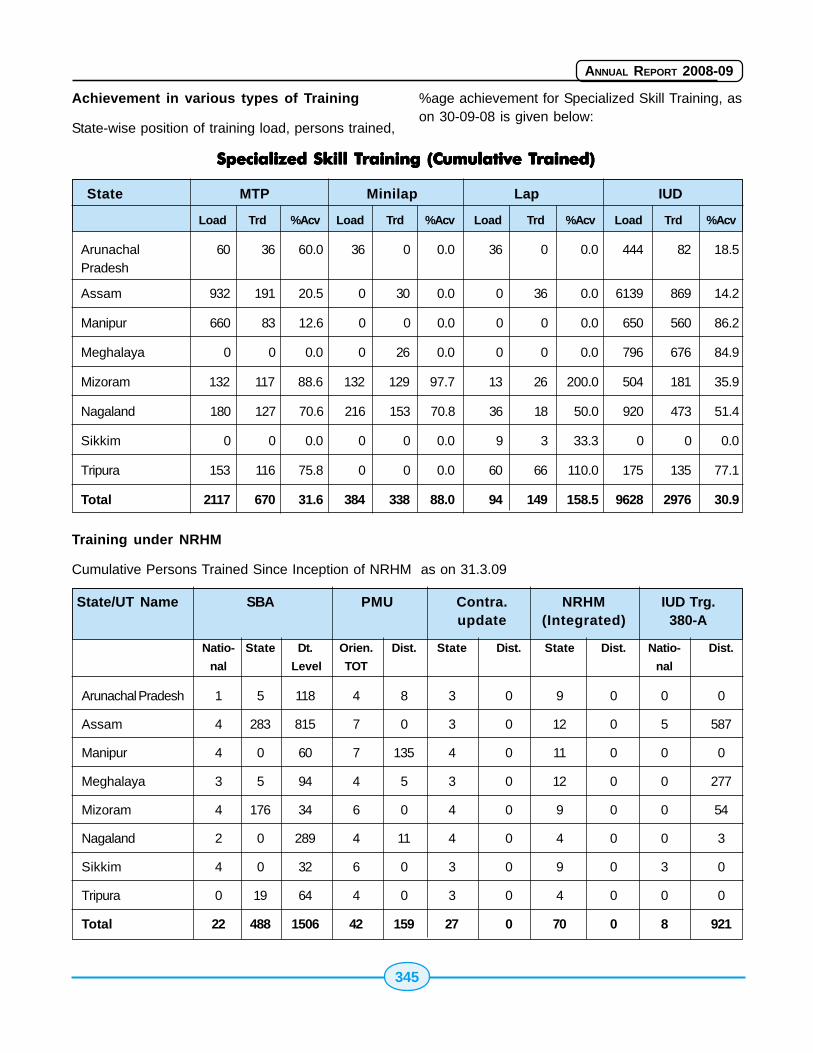
345
ANNUAL REPORT 2008-09
Achievement in various types of Training
State-wise position of training load, persons trained,
%age achievement for Specialized Skill Training, ason 30-09-08 is given below:
Training under NRHM
Cumulative Persons Trained Since Inception of NRHM as on 31.3.09
Specialized Skill TSpecialized Skill TSpecialized Skill TSpecialized Skill TSpecialized Skill Training (Cumulative Training (Cumulative Training (Cumulative Training (Cumulative Training (Cumulative Trained)rained)rained)rained)rained)
State MTP Minilap Lap IUD
Load Trd %Acv Load Trd %Acv Load Trd %Acv Load Trd %Acv
Arunachal 60 36 60.0 36 0 0.0 36 0 0.0 444 82 18.5Pradesh
Assam 932 191 20.5 0 30 0.0 0 36 0.0 6139 869 14.2
Manipur 660 83 12.6 0 0 0.0 0 0 0.0 650 560 86.2
Meghalaya 0 0 0.0 0 26 0.0 0 0 0.0 796 676 84.9
Mizoram 132 117 88.6 132 129 97.7 13 26 200.0 504 181 35.9
Nagaland 180 127 70.6 216 153 70.8 36 18 50.0 920 473 51.4
Sikkim 0 0 0.0 0 0 0.0 9 3 33.3 0 0 0.0
Tripura 153 116 75.8 0 0 0.0 60 66 110.0 175 135 77.1
Total 2117 670 31.6 384 338 88.0 94 149 158.5 9628 2976 30.9
State/UT Name SBA PMU Contra. NRHM IUD Trg.update (Integrated) 380-A
Natio- State Dt. Orien. Dist. State Dist. State Dist. Natio- Dist.
nal Level TOT nal
Arunachal Pradesh 1 5 118 4 8 3 0 9 0 0 0
Assam 4 283 815 7 0 3 0 12 0 5 587
Manipur 4 0 60 7 135 4 0 11 0 0 0
Meghalaya 3 5 94 4 5 3 0 12 0 0 277
Mizoram 4 176 34 6 0 4 0 9 0 0 54
Nagaland 2 0 289 4 11 4 0 4 0 0 3
Sikkim 4 0 32 6 0 3 0 9 0 3 0
Tripura 0 19 64 4 0 3 0 4 0 0 0
Total 22 488 1506 42 159 27 0 70 0 8 921
346
ANNUAL REPORT 2008-09
19.1319.1319.1319.1319.13 Development of NursingDevelopment of NursingDevelopment of NursingDevelopment of NursingDevelopment of NursingServices in NEServices in NEServices in NEServices in NEServices in NE
Under the Programme of Development of NursingServices following schemes are implemented.
1) Training of Nurses
2) Strengthening / Up gradation of ExistingSchools/Colleges of Nursing
3) Providing recurring assistance to Schools ofNursing that were opened during IXth planperiod.
Training of Nurses
In order to update the knowledge and skills of thenursing personnel, Continuing Nursing EducationProgramme was started in the area of NursingSpecialty for the Staff Nurses, Education Technologyfor the faculty of the Schools and Colleges of Nursing,Management Techniques for the NursingAdministrators. It is conducted for 10 days. Thevenue will be in the selected College of Nursing inthe state. As per the pattern of assistance, Rs. 75,000per course is provided to train 30 Nurses. A sum ofRs. 7.5 lakhs have been released for conducting 10courses during the year 2008-09
Up gradation of Schools of Nursing intoColleges of Nursing.
It is proposed to upgrade Schools of Nursing, whichare attached to the Medical Colleges into Collegesof Nursing. The objective of the scheme is to trainmore Graduate Nurses. One time assistance of Rs.
1.50 crores is provided as non-recurring assistanceto the State Govt/Institution subject to the conditionthat State Govt. gives an undertaking that they willbear the recurring assistance of the College ofNursing. So far a grant of Rs. 3.00 crores has beenreleased to 2 institutions in the N.E. States forupgrading School of Nursing into College of Nursingat Aizwal, Mizoram and School of Nursing at Kohima,Nagaland.
Strengthening of Existing Schools/Colleges ofNursing
In order to improve the quality of training imparted atthe existing Schools and Colleges of Nursing grantis released towards procurement of A.V Aids,furniture, improvement of library, additions/alterationsof building and transport. A grant of Rs. 10.00 lakhsis provided per institution during the Xth Plan period..One institution has been released financial assistancefor strengthening during the year 2007-08.
Providing recurring assistance to School ofNursing which were opened during IXth plan.
There was a provision in the IXth Plan for providingassistance under the scheme for opening newSchools of Nursing with financial implication of Rs.82.68 lakhs per school. Out of 48 Nursing Schoolsopened during the IX plan period, 20 Nursing Schoolsare in the North Eastern States. During the year 2007-08 a sum of Rs, 104.00 lakhs have been released to6 institutions in the N.E States. A sum of Rs. 15.00lakhs have been released so far during the year2008-09.
Part - II
Department ofAyurveda, Yoga-Naturopathy
Unani, Siddha &Homoeopathy(AYUSH)
348
ANNUAL REPORT 2008-09
349
ANNUAL REPORT 2008-09
1. Holistic health has almost become a mantrain today's world given the myriad of health problemsthat mankind is facing on account of modern stressedout lifestyles. It is being increasingly accepted by theglobal community, both by patients and medicalpractitioners, that no single system can address allthe health needs of modern day society. India as weall know has a long and ancient tradition of holistichealth care systems like Ayurveda, Siddha and Unani.They are not merely symptomatic treatment systemsbut lay emphasis on the fact that the basic premiseof good health is a healthy lifestyle. This makes themideally placed to provide answers to the health careneeds of modern society.
2. As we all know Ayurveda in India is older thanhistory itself. It has its beginnings in the prehistoricforest dwelling tribes who used their knowledge ofplants for treating a variety of ailments. About 5000years ago the greatest intellects of those timesgathered this knowledge and developed it as ascience to alleviate physical, mental and spiritualsufferings of mankind. With the advent of westernscience with its over emphasis on empirical evidencethese systems were dismissed as no more thansuperstition. Fortunately a few dedicated scientistsrealizing the limitations of modern medicine,understood the holistic nature of Traditional Medicine,undertook extensive studies of the ancient texts andattempted to validate the knowledge with tools usedby modern science. Today with a plethora of lifestylerelated, chronic diseases plaguing mankind the worldis increasingly turning to Traditional Medicine in aquest for answers to their health problems. With thisglobal resurgence of interest in Traditional Medicineour responsibility is doubled. On the one hand wehave to establish scientific validation for thesesystems and on the other, it is incumbent on us tocash in on the opportunity provided by a rekindledinterest in Traditional Medicine to establish the
primacy of these systems which are already validated
by centuries of practice. Ayurveda, Siddha, Unani
and Yoga are well documented also.
3. The Department of AYUSH is more than
aware of this responsibility and has taken a number
of initiatives over the past few years. The 11th Plan
allocation of the Department of AYUSH has increased
four fold over that of the 10th Plan to approx. Rs.4000
crore. Several new initiatives have been launched
in the 11th Plan. While the existing Schemes of the
department have been redesigned and revamped
several new schemes have been started.
4. The Central sector scheme for 'Development
of AYUSH Industry Clusters' with an outlay of Rs 100
crores is based on the recognition that the cluster
approach is participatory, cost effective and provides
critical mass for customization of the enterprises on
'collaborating while competing' principle. So far we
have sanctioned our first cluster in Thrissur at Kerala
and others are in the pipeline.
5. Identification of reputed AYUSH knowledge
institutions in Non Governmental/Private Sector and
supporting them to upgrade their functions and
facilities to levels of excellence is another novel
scheme of the department. Eight such centres are
already being supported under this scheme.
6. AYUSH drugs have the potential to tackle
community health problems resulting from nutritional
deficiencies, epidemics and vector-borne diseases,
recognising this the department has initiated the
Scheme of AYUSH intervention in Public Health. The
scheme is aimed at supporting innovative proposals
of Government and private organizations to promote
AYUSH interventions for community health care and
to encourage utilization of AYUSH practitioners in
public health programmes.
OverviewOverviewOverviewOverviewOverview

350
ANNUAL REPORT 2008-09
7. In coordination with National Manuscripts
Mission, Department of Culture, Government of India
the scheme for acquisition, cataloguing, digitization
and publication of manuscripts, has been started. Alarge body of AYUSH knowledge exists in the country
in the form of classical text material, manuscripts,
scientific outcomes, personal experiences, folklore,
local health practices, ethno-medicine, tribal medicine
etc. This information needs to be properly catalogued
and digitized in a user-friendly manner so as to makeit accessible to a wider audience while at the
sametime protecting. So far about Rs. 60 lakhs have
been spent under this scheme.
8. Apart from the codified systems of Medicine
of India, substantial knowledge exists in the form of
Local Health Traditions in various parts of the country.
The department has launched a new scheme of grant-in-aid to NGOs working with rural communities to
revitalise these local health traditions.
9. In an effort to introduce AYUSH practitioners
to the latest trends in teaching and clinical practice
and to upscale their skills in new and emerging fields
like IT enabled learning, the Central Sector Schemefor supporting Re-orientation Training, Continuing
Medical Education and Exposure programs of
AYUSH, was started. Calendars for RoTP/CME have
been drawn up for the current year. Over Rs 5 crores
have been spent on this programme so far.
10. The Centrally Sponsored Drug Quality ControlScheme has also been revised for upscaling the
financial assistance being provided to ASU&H
manufacturing units for becoming GMP compliant.
Under the revised Scheme, the Department would
be giving a subsidy of upto 30% of the project cost
subject to a maximum of Rs.30 lakh to ASU&Hmanufacturing units having a turn-over of upto Rs.20
crore for setting up their in-house quality control
laboratories or to upgrade their manufacturing
facilities to WHO GMP level.
11. Another feather in the cap of the department
is the approval by the cabinet of the National Mission
on Medicinal Plants at an outlay of Rs 630 crores forthe 11th plan period. This addresses the entire gamut
of issues facing the raw material sector of AYUSH
from cultivation of medicinal plants over 80,000hectares to setting up seed centres, nurseries,medicinal plants processing facilities, post harvestmanagement, testing for quality, Good collection andagricultural practices to providing marketing support.
12. Apart from specific schemes like the onesmentioned above we have started collaborations withinstitutions of excellence like the one at the NationalInstitute of Ayurveda (NIA), Jaipur, wherein aSpecialized Eye Clinic has been started incollaboration with the Sreedhareeyam Ayurvedic EyeHospital, Ernakulam, Kerala, which is a unique Centreof Excellence in the field of Ayurveda for eye care.This arrangement not only introduces the best ofeye care in Ayurveda to the people of Northern India,but also provides training in best practices in eyecare to the UG/ PG students and teachers. There isa daily OPD of 35 to 45 patients just to avail of thissingle service.
13. In order to upgrade the quality of teachingand practice of AYUSH in the country NationalInstitutuions along the lines of AIIMS have beenvisualised like The All India Institute of Ayurveda, NewDelhi, North Eastern Institute of Folk Medicine,Passighat, and The North Eastern Institute ofAyurveda and Homoeopathy, Shillong, and work onthem is continuing.
14. AYUSH has a fairly large infrastructure ofabout 7 lakh registered practitioners, 3000 hospitals,21000 dispensaries and over 450 UG/PG teachingcolleges with an admission capacity of nearly 30,000students. In order to take the benefits arising out ofthese to the people, steps have been taken tomainstream AYUSH in the health care delivery setup of the country. The road map includes posting anAYUSH doctor in every PHC/CHC. Over 4000 doctorshave been appointed on contract and AY U S Hfacilities have been created in 203 district hospitals,1798 PHCs and 2350 CHCs. So far 27 States haveprojected mainstreaming of AYUSH components inthe integrated Programme Implementation Plans(PIPs) under NRHM for the year 2008-09. Rs. 70.00crores have been sanctioned for contractual hiringof Manpower and training under NRHM during 2008-09.
351
ANNUAL REPORT 2008-09
15. What were once the preferred systems ofhealth care for the masses are increasingly gettingconfined to a small section of western educated urbanelite. As part of the strategy to bring back thesesystems into the mainstream the unique initiative oflaunching National Campaigns on select AYUSHthemes was taken, the themes were developedkeeping in mind specific areas of strengths that thedifferent systems of AYUSH have. The broad formatof the National Campaigns envisages the launch ofthe campaigns by a 2 day workshop at the Nationallevel followed by workshops at the State level andthen at the district and sub-district levels. Thus acascading effect is envisioned to spread theoutcomes of the National Workshop from the Centreupto the district and the panchayat levels. So farfour such campaigns have been launched. The firstin the series being on Ksharsutra Therapy, which isan Ayurvedic para surgical procedure for treatmentof Ano-rectal disorders. The technique not onlystands duly validated by ICMR, but is being practicedby modern doctors in countries like Japan for over20 years now. The Second was Homoeopathy formother and child care. As we all know the health careneeds of children and especially pregnant andlactating mothers are very different from thepopulation at large. Homoeopathy being safe,effective, palatable and free from side effects isideally suited to meet this need. The third Campaignwas "Ayurveda and Siddha for Geriatric Care". Thefact that the global population today is becomingincreasingly grey is well documented. The chronicinflammatory and degenerative conditions that theelderly suffer from need special care, but with ahealth infrastructure already creaking under theburden of a growing population, care of the elderlyis not a priority. Given this backdrop, Ayurvedaprovides the ideal health option with its Rasayanatherapy which is a dedicated branch of Ayurveda forthe care of the elderly. This was one of the 8 branchesof Ayurveda developed millennia ago, and today inthe 21st century we are looking to it for solutions.The fourth campaign was on Quality Assurance ofAYUSH drugs, which aims at a shift from: 'qualitycontrol' to 'quality assurance' mindset withenforcement agencies and industry working inrandem.
Some of the interesting outcomes of the differentcampaigns :
i. During the Ksharasutra campaign it becameincreasingly evident that here was an ancienttechnique which was not only validated byICMR but had many takers amongstallopathic practitioners, who wantedorientation courses on the technique. Twentystate campaigns have been organized onKsharsutra in different states.
ii
ii
. A core group of homoeopaths and allopathshas been set up to list out the specificconditions, which can safely and effectivelybe treated by Homoeopathy.
i. Both the ASU&H Industries and theenforcement agencies should work closelyfor capacity building for transition from qualitycontrol mindset to quality assurance mindsetwhich includes process validation andconverting textual knowledge into processtechnology and documentation at every stageof the production cycle as per GMPrequirements
iv. A module for training of both AYUSH andAllopathic doctors on Geriatrics andKsharsutra has been prepared.
16. Pioneering work has been done in the fieldof laying down of pharmacopoeial standards forASU&H drugs through the involvement oflaboratories of our own Department and that of CSIR.Standards for 540 Ayurvedic classical drugs havealready been published. Second volume ofpharmacopoeial standards for 51 poly-herbalformulations has been released. Pharmacopoeialstandards for 200 Unani drugs and 71 Siddhaformulations have been published. The 9th Volumeof the Homoeopathic Pharmacopoeia of 100 rawdrugs has been published. PLIM which has beenmodernized and is being designated as a WHOCollaborative Centre, has developed an HPTLCFinger Print Atlas of 80 Ayurvedic single Drugs.
17. As part of the on going Indian effort to reachan understanding with ASEAN countries, on various

352
ANNUAL REPORT 2008-09
sectors of trade and commerce, the Department ofAYUSH hosted an Indo-ASEAN conclave onTraditional Medicine. Given the vitality of traditionalmedicine systems in both the Indian subcontinentand the rest of South East Asia, it is only natural thatwe share each others strengths in the sector andestablish a synergistic relationship for the growth anddevelopment of Traditional Medicine. As an outcomeof this an MoU between India and ASEAN countrieshas been drafted and communicated to the ASEANSecretariat. An MoU on Traditional Medicine was alsosigned with China.
18. Efforts have been made to partner with like
minded institutions for furthering the cause of AYUSHsystems, like deputation of Ayurveda Experts to USMedical Schools. There is a Proposal to start a PGDiploma course of one year duration for medicaldoctors in Debrecen and other Universities in Europe.Steps have been taken for setting up a Centre forResearch in Indian Systems of Medicine (CRISM) withthe National Centre for Natural Products Research(NCNPR) at the University of Mississippi. This is acollaborative project between the Department ofAYUSH, Indian Institute of Integrative Medicine (IIIM)Jammu and National Cernre for Natural ProductsResearch (NCNPR). A mirror centre has already beenset up at IIIM Jammu.
353
ANNUAL REPORT 2008-09
Chapter 1
1.1 The Department is headed by a Secretaryto the Government of India. The Secretary isassisted by two Joint Secretaries and three Directors/Deputy Secretaries, three Advisers and DeputyAdvisors of Ayurveda, Siddha, Unani andHomoeopathy.
The total sanctioned staff strength of the Departmentin Group A,B,C & D is 268, which include Secretariatand Technical posts.
1.2 The Department has, over the years,developed a broad institutional framework to carryout the activities in the field of AYUSH. The institutionalframework consists of:
i. Statutory regulatory bodies
! Central Council of Indian Medicine (CCIM);and
! Central Council of Homoeopathy (CCH)
The duties of these bodies are
! laying down minimum standards of education,
! recommending recognition of medicalqualifications,
! registering the practitioners and laying downof ethical codes.
! To prescribe Standards of ProfessionalConduct, Etiquette and Code of Ethics to beobserved by the practitioners.
! To consider applications received by theGovernment of India for the establishmentof new Ayurveda, Siddha, Unani andHomoeopathy medical colleges, to start newor higher courses of study or training andto increase intake capacity in existingcolleges.
ii
i
. Apex research bodies
! Central Council for Research for Ayurvedaand Siddha, (CCRAS)
! Central Council for Research in UnaniMedicine, (CCRUM)
! Central Council for Research inHomoeopathy,(CCRH)
! Central Council for Research in Yoga andNaturopathy (CCRYN)
ii. Apex educational institutions
! National Institute of Ayurveda (NIA), Jaipur
! National Institute of Homoeopathy (NIH),Kolkatta
! National Institute of Naturopathy (NIN), Pune
! National Institute of Unani System of Medicine(NIUM), Bangalore
! Institute of Post Graduate Teaching andResearch in Ayurveda (IPGTRA), Jamnagar
! Morarji Desai National Institute of Yoga(MDNIY), New Delhi
! Rashtriya Ayurveda Vidyapeeth (RAV)
iv. Apex Laboratories
! Pharmacopoeial Laboratory for IndianMedicine (PLIM), Ghaziabad
! Homoeopathic Pharmacopoeial Laboratory(HPL), Ghaziabad
v. Public Sector Undertakings
! Indian Medicines Pharmaceutical CorporationLtd. (IMPCL),:- IMPCL is a Government of
OrganizationOrganizationOrganizationOrganizationOrganization

354
ANNUAL REPORT 2008-09
India Enterprise under the administrativecontrol of the Department of AYUSH havingits registered office and factory at Mohan,District. Almora (a notified backward area) inUttarakhand. The company was incorporatedin July 1978 and started commercialproduction in June 1983. The company whichis a 'MINI RATNA' has Authorised Sharecapital and the Paid-up Share capital ofRs.700 lakh.
The primary objective of the company is tomanufacture and supply authentic quality Ayurvedicand Unani products. The IMPCL products are mainlyused in the Central Government Health Scheme(CGHS), Government Hospitals, Dispensaries andby the various AYUSH Research Councils. Thecompany also sells its products to some StateGovernments and in the open market.
vi. National Medicinal Plants Board
The National Medicinal Plants Board (NMPB) was setup in the 10th Plan as a follow-up ofrecommendations of the Task Force on conservationand sustainable utilization of medicinal plants by thePlanning Commission, vide Cabinet Resolutionnotified on 24th November, 2000. The Board wasestablished with the objective of having an agencyat the National level which would be responsible forco-ordinating all matters relating to the developmentof the medicinal plants sector including drawing uppolicies and strategies for conservation, proper
harvesting, cost-effective cultivation and marketing,of raw material.
vii. Pharmacopoeial Committees
Four different Pharmacopoeial Committees, oneeach for Ayurveda, Siddha, Unani and Homoeopathyare working for preparing official formularies/pharmacopoeias of Ayurveda, Siddha, Unani andHomoeopathy drugs.
1.3 A Drug Control Cell (AYUSH) is working inthe Department to deal with the matters pertainingto Drug Quality Control and regulation of Ayurveda,Siddha and Unani drugs under the provision of Drugsand Cosmetics Act, 1940 and Rules, 1945. The Cellis looking after the activities of Ayurveda, Siddha,Unani Drug Technical Advisory Board (ASUDTAB)and Ayurveda, Siddha, Unani Drugs ConsultativeCommittee (ASUDCC). The Drug Control Cell alsodeals with the Traditional Knowledge Digital Library(TKDL) and matters relating to Intellectual PropertyRights (IPR) as also coordination with Governmentof India Ministries/Departments concerned with IPR.
1.4 An information, Education andCommunication (IEC) Cell and a Facilitation Centreare also functioning in the Department.
1.5 The Department constituted an EducationPolicy Section to deal with the matters related to grantof permission for opening of new colleges, increasingadmission capacity and starting new or higher coursesin Ayurveda, Siddha, Tibb and Homoeopathy.
355
ANNUAL REPORT 2008-09
Chapter 2
2.1 The National Health Policy, 1983 referred to
our rich heritage of medicinal knowledge and
suggested that it was necessary to initiate measures
to enable India's rich medicinal heritage to develop
in accordance with its genius. It took note of the fact
that a vast infrastructure is available in Indian
Systems of Medicine and Homoeopathy and that it
should be integrated at the appropriate level
especially in regard to the preventive, promotive and
public health objectives.
2.2 The Central Council for Health and Family
Welfare in 1999 also recommended, inter-alia, that
at least one physician from the Indian Systems of
Medicine and Homoeopathy should be available in
every Primary Health Center and that vacancies
caused by non-availability of allopathic personnel
should be filled by ISM&H physicians. The Council
also resolved that specialist ISM&H treatment centers
should be introduced in rural hospitals and that a
wing should be created in existing state and district
level government hospitals for extending health careto the public.
National PolicyNational PolicyNational PolicyNational PolicyNational Policy
Main Objectives of the National Health Policy on AYUSH (2002)
! The promotion of good health and the extension of health care facilities through AYUSH systems.
! Improving the quality of AYUSH teachers and clinicians.
! Ensuring affordable AYUSH services and medicines which are safe and efficacious.
! Increasing the availability of authentic raw drugs so as to improve the quality of AYUSH drugs.
! Integration of AYUSH systems into the health care delivery system and the national healthprogrammes.
! Reorienting and prioritizing research in order to validate therapies and drugs.
! Creating awareness about the strengths of AYUSH systems in India and abroad.
! Ensuring the growth and development of AYUSH systems and the utilization of their potential.
2.3 The National Policy on Indian Systems ofMedicine and Homoeopathy, 2002 outlined thefollowing basic objectives:
(a) To promote good health and expand theoutreach of health care to our people,particularly those not provided with healthcover, through preventive, promotive andcurative interventions through ISM&H.
(b) To improve the quality of teachers andclinicians by revising curricula tocontemporary relevance by crating modelinstitutions and Centres of Excellence andassistance for creating infrastructuralfacilities.
(c) To ensure affordable ISM&H services anddrugs which are sage and efficacious.
(d) To facilitate availability of raw drugs which areauthentic and contain essential componentsas required under pharmacopoeial standardsto help improve quality of dregs, for domesticconsumption and edport.
356
ANNUAL REPORT 2008-09
(e) To integrate ISM&H in the health care deliverysystem and National Programmes and ensureoptimal use of the infrastructure of hospitals,dispensaries and physicians.
(f) To re-orient and prioritize research in ISM&Hto gradually validate therapy and drugs toaddress in particular the chronic and new lifestyle related emerging diseases.
(g) To create awareness about the strengths ofthese systems in India and abroad andsensitize other stakeholders and providersof health.
(h) To provide full opportunity for the growth anddevelopment of these systems and utilizationof their potential, strength and revival of theirglory.
2.4 The following strategies have been outlinesin the National Policy on AYUSH, 2002:
(a) Taking legislative measures to checkmushrooming of substandard colleges.
(b) Raising the standards of medical educationby reinforcing Course curricula so as toequip trainees for managing national healthprogrammes.
(c) Prioritising research in, pharmacology,toxicology, standardization and study ofpharmaco-kinetics in respect of alreadyidentified areas of strength.
(d) Addressing the issues of conservation andsustainable use of medicinal plants throughpromotion of remunerative farming, andregulation of medicinal farms.
(e) Enabling the Medicinal Plants Board toacquire statutory status to be able to regulateregistration of farmers and cooperativesocieties, transportation, marketing ofmedicinal plants and proper procurement andsupply to the pharmaceutical industry.
(f) Protecting India's traditional medicinalknowledge through the unique TraditionalKnowledge Digital Library.
(g) Integrating and mainstreaming ISM&H in thehealth care delivery system and in NationalHealth Programmes.
(h) Developing a range of options for utilizationof AYUSH manpower in the healthcaredelivery system by assigning specific goaloriented roles and responsibilities to theISM&H work force.
(i) Encouraging Allopathic hospitals to set upAYUSH health facilities like those forPanchkarma and Ksharshutra
(j) Consolidating ISM&H infrastructure andhealth services in the states.
(k) Expediting Pharmacopoeial work related toAyurveda, Unani, Siddha and HomoeopathyDrugs.
(l) Encouraging Industry to make use of qualitycertification and acquisition of GMP and ISO9000 certification.
(m) Setting up Quality Control Centers on aregional basis to standardize the in-processquality control of Ayurveda, Siddha, Unani(ASU) products and to modernize traditionalprocesses without compromising the basicconcepts of ISM.
(n) Augmenting facilities for drug manufactureand testing in the States.
(o) Operationalising the use of ISM inReproductive and Child Health (RCH ineleven identified areas, where the Indiansystems of medicine would be useful forantenatal, intra-natal, post-natal and neo-natal care.
(p) Providing support to develop infrastructureand awareness of ISM in the North EasternStates, which are rich in medicinal plants.
(q) Formulating modules for introducingAyurveds and Yoga to medical schools andinstitutions abroad so as to expose theirmedical graduates to the concepts andpractices of ISM
(r) Launching Awareness programmes on theutility and effectiveness of ISM&H through theelectronic and print media.
2.5 The following measures have been taken bythe Department of AYUSH to give effect to the abovepolicy directions:
357
ANNUAL REPORT 2008-09
(a) There has been a four fold increase in thebudgetary allocation for the AYUSH sector inthe 11th plan as compared to the 10th plan.Expenditure during the 10th plan periodstood at Rs.1030.15 crores, while theprojected outlay for the 11th plan isRs.3988.00 crore.
(b) As in the 10th Plan, efforts are being weremade to strengthen the existing NationalInstitutes set up so as to lay down benchmarksfor teaching, research and clinical practicesof different systems.
(c) The Department is continuing to prevent thegrowth of sub-standard colleges and hassought the active involvement of theregulatory Councils and States Governmentsto achieve these objectives. Under theamended Indian Medicine Central Council Act,1970 and the Homoeopathy Central CouncilAct, 1973, prior permission of the CentralGovernment is now mandatory forestablishing new colleges; starting new orhigher courses of study and for increasingadmission capacity in Ayurveda, Siddha,Unani and Homoeopathy colleges. Theamended Indian Medicine Central Council Act,1970 also provides for ensuring conformityto laid down standards in existing collegeswithin 3 years of enactment. These provisionshave already curbed the growth of sub-standard medical colleges..
(d) The IMCC (Amendment) Bill, 2005 and theHCC (Amendment) Bill 2005 have beenintroduced in the Parliament with a view tobringing about transparency andaccountability in the functioning of theregulatory Councils as a part of theDepartment's focus on improving thestandards of graduate and postgraduateeducation in Ayurveda, Siddha, Unani andHomoeopathy. The Indian Medicine andHomoeopathy Pharmacy Council Bill 2005 hasalso been introduced in Parliament toestablish a Central Pharmacy Council forIndian Medicine and Homoeopathy toregulate and standardize Pharmacyeducation.
(e) Standardization of drugs and Quality Controlcontinued to receive the focused attentionof the Central Government. Department ofAYUSH has sensitized all the State LicensingAuthorities and State Departments who areresponsible for the administration of theIndian Drugs & Cosmetics Act, 1940 and theDrugs & Cosmetics Rules, 1945 to ensurecompliance by all Ayurveda, Siddha andUnani drug manufacturing units to theprovisions relating to display of all ingredientsused in the preparations together with thequantity of each ingredients on the labels ofmedicines. All the State Ayurveda, Siddha,Unani and Unani Drug Licensing Authoritieshave also been instructed to take actionagainst the defaulting ASU drugmanufacturers for failure to comply with theGood Manufacturing Practices (GMP) notifiedunder Schedule 'T' of the Drugs andCosmetics Rule, 1945.
(f) To address domestic as well as globalconcerns relating to the presence of heavymetals in Ayurveda, Siddha and Unaniformulations, the Department of AYUSH hasinitiated a research project under the GoldenTriangle Project in collaboration with theCenral Council for Research in Ayurveda andSiddha (CCRAS), Council of Scientific andIndustrial Research (CSIR) and IndianCouncil of Medical Research (ICMR) forphysicochemical characterization safetystudies of eight most widely used Bhasmas(herbo-metallic compounds) prepared inaccordance with the classical texts. TheDepartment of AYUSH has also introducedmandatory testing for heavy metals likeArsenic, Lead, Mercury, Cadmium, etc. in allpurely herbal Ayurveda, Siddha and Unanidrugs which are meant for export w.e.f. 1stJanuary, 2006 to ensure that these purelyherbal medicines do not contain any heavymetal by way of contamination.
(g) In the 11th Five Year Plan, a new provisionfor financial assistance to ASU drugmanufacturing units to acquire sophisticated
358
ANNUAL REPORT 2008-09
quality control and R&D equipment by wayof a subsidy upto 30 percent of the projectcost subject to a maximum of Rs. 30.00 lakh,whichever is less, has been incorporated.The Department also plans to encourage thesetting up of common facilities for AYUSHindustry clusters in 15 to 20 major centers ofproduction of ASU drugs.
(h) Integration of AYUSH in the health caresystem is the key strategy under the NationalRural Health Mission (NRHM). TheDepartment of AYUSH has been providingsubstantial financial assistance to States foropening of AYUSH wings in district hospitalsand Speciality/OPD clinics in other hospitalswith a view to provide AYUSH facilities alongwith modern medicine under one roof. Anambitious initiative is also under way toprovide the services of AYUSH doctors inCHCs/PHCs under the NRHM.
(i) Substantial financial assistance has beenprovided to Government and Governmentaided AYUSH UG/PG colleges for upgradingtheir infrastructure. It is also proposed toprovide financial assistance for thedevelopment of selected AYUSH UG/PGinstitutions into Centres of Excellence forAYUSH education in the 11th Plan.
(j) The Department of AYUSH has assigned thehighest priority to the laying down ofpharmacopoeial standards for ASU and Hdrugs. The work of laying down ofpharmacopoeial standards of single crudedrugs has been more or less completed andit is proposed to lay down pharmacopoeialstandards for 300 to 400 most widely usedAyurvedic medicines in the next three years.In order to expedite the work, the ResearchCouncils have been declared as theSecretariats for the PharmacopoeiaCommittees. During the year API Part I Vol.VI (101 monographs) and API Part II Vol. II(51 Formulations) was published.
(k) The Pharmacopoeial Laboratory for IndianMedicine (PLIM), Ghaziabad has been
modernized with a view to expediting thelaying down of pharmacopoeial standards.
(l) National Medicinal Plants Board has been setup by the Government of India and StateMedicinal Plants Board have beenconstituted in most of the States to coordinatethe activities of cultivation and conservationof medicinal plants. So far more than 1.5 lakhacres of land has been brought under in-situconservation and ex-situ cultivation ofmedicinal plants.
(m) In the 11th Plan an ambitious scheme hasbeen drawn up by the National MedicinalPlants Board for the provision of marketingand value added services to the growersthrough State Medicinal Plant Boards andHerbal Mandis.
(n) With a view to protecting India's traditionalmedicinal knowledge, a TraditionalKnowledge Digital Library (TKDL) has beencreated in five international languages inorder to enable access by InternationalPatent Offices under a non-disclosureagreement for facilitating patent searches soas to prevent the grant of wrongful patentsbased on Indian traditional medicinalknowledge already in the public domain.
(o) Establishment of an All India Institute ofAyurveda at Sarita Vihar, New Delhi has beeninitiated which would be a center of excellencefor development and scientific validation ofAyurveda.
(p) Keeping in view the global resurgence ofinterest in complementary and alternativesystems in general and Ayurveda inparticular, the AYUSH drug manufacturingindustry was provided incentives forparticipation in national and internationaltrade fairs / exhibitions to improve the visibilityof AYUSH products.
(q) The Department organized an Indo-ASEANconclave on Traditional Medicine on thesidelines of Arogya at Delhi, during which afruitful exchange of ideas took place betweenexperts from all the participating countries
359
ANNUAL REPORT 2008-09
Chapter 3
3.1 Introduction
3.1.1 AYUSH is an acronym for Ayurveda, Yoga,Naturopathy, Unani, Siddha and Homoeopathy whichare the systems, which originated in India as well asoutside but got adopted and adapted here in thecourse of time. These systems are popular in a largenumber of States in the country. Ayurveda is moreprevalent in the States of Kerala, Himachal Pradesh,Gujarat, Karnataka, Madhya Pradesh, Rajasthan,Uttar Pradesh and Orissa. The Unani System isparticularly popular in Andhra Pradesh, Karnataka,Tamilnadu, Bihar, Maharashtra, Madhya Pradesh,Uttar Pradesh, Delhi & Rajasthan. Homoeopathy iswidely practiced and in Uttar Pradesh, Kerala, WestBengal, Orissa, Andhra Pradesh, Maharashtra,Punjab, Tamil Nadu, Bihar, Gujarat and the NorthEastern States.
3.2 Ayurveda System of Medicine
3.2.1 The literal meaning of Ayurveda (Ayu (life) +Veda (Science)) is "Science of Life". Ayurvedadeveloped out of the various Vedic hymns describingthe fundamental philosophies about life, diseasesand medicines. Around 1000 B.C, Ayurvedicknowledge was comprehensively documented in theCharak Samhita and Sushruta Samhita. Accordingto Ayurveda, health is considered a pre-requisite forachieving the goals of life, i.e., dharma, artha, kamaand moksha. Ayurveda takes an integrated view ofthe physical, mental and spiritual and social aspectsof human beings and about the interrelationshipsbetween these aspects.
3.2.2 The philosophy of Ayurveda is based on thetheory of Panchmahabhutas (five element theory)
Ayurveda, Yoga and Naturopathy, Unani,Ayurveda, Yoga and Naturopathy, Unani,Ayurveda, Yoga and Naturopathy, Unani,Ayurveda, Yoga and Naturopathy, Unani,Ayurveda, Yoga and Naturopathy, Unani,Siddha and Homoeopathy (AYUSH)Siddha and Homoeopathy (AYUSH)Siddha and Homoeopathy (AYUSH)Siddha and Homoeopathy (AYUSH)Siddha and Homoeopathy (AYUSH)
which postulates that all objects and living bodiesare composed of these five elements. Thecombinations of these five elements are representedin the form of Tridoshas viz. Vata (Ether+ Air), Pita(Fire) and Kaph (Water + Earth). These threeD̀oshas' are physiological entities in living beings,whereas Satva, Rajas and Tamas are the mentalattributes. Ayurveda aims to keep these structuraland functional entities in a state of equilibrium whichsignifies good health (Swastha). Any imbalance dueto internal or external factors causes disease andthe treatment consists of restoring the equilibriumthrough various techniques, procedures, regimen,diet and medicine.
3.2.3 Ayurveda considers the human being as amicrocosm (Yatha pinde tatha brahmande) which isa replica of the macrocosm (Universe). The treatmentin the Ayurveda system is holistic and individualizedand has two components; (a) preventive; and (b)curative. The preventive aspect of Ayurveda is calledSvasth-Vritt and includes personal hygiene, regulardaily routine, appropriate social behaviour andRasayana Sevana, i.e, use of rejuvenative materials/food and rasayana drugs. The curative treatmentconsists of three major categories (i) Aushadhi(drugs); (ii) Various procedures includingPanchakarma and Surgery; (iii) Satvaraja(Methodsfor Mind control including Psychological ).
3.2.4 During the Samhita period (1000 BC),Ayurveda developed eight branches or specialities,which was a reason for it being called AshtangAyurveda. These are: -
(1) Kayachikitsa (Internal Medicine)
(2) Kaumar Bhritya (Pediatrics)
360
ANNUAL REPORT 2008-09
(3) Graha Chikitsa (Psychiatry)
(4) Shalakya (Eye and ENT and dentistry)
(5) Shalya Tantra (Surgery)
(6) Visha-Tantra (Toxicology)
(7) Rasayana (Geriatrics)
(8) Vajikarna (Science of virility)
3.2.5 The above eight branches have over theyears and specifically during the last 50 yearsexpanded into twenty-two specialties. These are: -
(1) Ayurveda Sidhanta (Fundamental Principlesof Ayurveda)
(2) Ayurveda Samhita
(3) Rachna Sharira (Anatomy)
(4) Kriya Sharira (Physiology)
(5) Dravya Guna Vigyan (Materia Medica andPharmacology)
(6) Ras-Shashtra (Pharmaceuticals usingminerals and metals)
(7) Bhaishajya Kalpana (Pharmaceuticals)
(8) Kaumar Bhritya - Bala Roga (Pediatrics)
(9) Prasuti -Tantra evum Stri Roga (Obstetricsand Gynaecology)
(10) Swasth-Vritta (Social and PreventiveMedicine)
(11) Kayachiktisa (Internal Medicine)
(12) Rog Nidan avum Vikriti Vigyan (Pathology)
(13) Shalya Tantra (Samanya)(Surgery)
(14) Salya Tantra - Ksar Karma avum AnushastraKarma (Kshars Karma and Para-surgicalprocedure)
(15) Shalkya Tantra - Netra Roga
(16) Shalakya Tantra - Shiro-Nasa-Karna AvumKantha Roga (ENT)
(17) Shalakya Tantra - Danta Avum Mukha Roga(Dentistry)
(18) Manovigyana avum Manas Roga(Psychiatry)
(19) Panchakarma
(20) Agad Tantra avum Vidhi Vaidyaka (Toxicologyand Jurisprudence)
(21) Sangyaharana (Anaesthesiology)
(22) Chhaya avum Vikiran Vigyan (Radiology)
3.3 Siddha System of Medicine
3.3.1 The Siddha System is one of the oldestsystems of medicine in India and is practised mainlyin Tamil Nadu and some other parts of South India.The term Siddha means 'achievements' and Siddharswere saintly persons who achieved 'results' inmedicine. Eighteen Siddhars were said to havecontributed towards the development of this medicalsystem. Siddha literature is in Tamil and it. is largelytherapeutic in nature.
3.3.2 The diagnosis of diseases in Siddha involvesidentifying its causes through the examination ofpulse, urine, eyes, study of voice, colour of body,tongue and the status of the digestive system.
3.3.3 The Siddha system of Medicine emphasizesthat medical treatment is oriented not merely todisease but has to take into account the patient, theenvironment, age, sex, race, habits, mental frame,habitat, diet, appetite, physical condition,physiological constitution, etc. This means thetreatment has to be individualistic and this ensuresthat there is a lower probability of mistakes beingmade in diagnosis or treatment.
3.3.4 During the last four decades, there has beencontinuous development in Siddha medicaleducation and this has led to the establishment ofthe following six specialties in post-graduate teachingand training:
I. Maruthuvam (General Medicine)
II
II
. Sirappu Maruthuvam (Special Medicine)
I. Kuzhanthai Maruthuvam (Paediatrics)
IV. Gunapadam (Pharmacology)
V. Noi Nadal (Pathology)
VI. Nanju Nool and Maruthuva Neethinool(Toxicology)
3.4 Unani System of Medicine
3.4.1 The Unani System of Medicine, whichoriginated in Greece and passed through many
361
ANNUAL REPORT 2008-09
countries before establishing itself in India during the
medieval period. It is based on well-established
knowledge and practices relating to the promotion
of positive health and prevention of diseases. TheUnani System has grown out of the fusion of
traditional knowledge of ancient civilizations like:
Egypt, Arabia, Iran, China, Syria and India. It
emphasizes the use of naturally occurring, mostly
herbal, medicines and also uses some medicines of
animal, marine and mineral origin. The system ofmedicine was documented in Al-Qanoon, a medical
Bible, by Sheikh Bu-Ali Sina (Avicena) (980-1037 AD),
and in Al-Havi by Razi (850-923 AD) and in many
other books written by the Unani physicians.
3.4.2 The Unani system is based on the Humoral
theory i.e, the presence of blood, phlegm, yellow bile
and black bile in a person. The temperament of aperson can accordingly be sanguine, phlegmatic,
choleric and melancholic depending on the presence
and combination of humors. According to Unani
theory, the humors and medicinal plants themselves
are assigned temperaments. Any change in quantity
and quality of the humors, brings about a change inthe status of the health of the human body. A proper
balance of humors is required for the maintenance
of health.
3.4.3 The treatment consists of three components,
namely, preventive, promotive and curative. Unani
system of Medicine has been found to be efficaciousin conditions like Rheumatic Arthritis, Jaundice,
Filariasis, Eczema, Sinusitis and Bronchial Asthma.
3.4.4 For the prevention of disease and promotion
of health, the Unani System emphasizes six
essentials (Asbab-e-Sitta Zarooria):- (a) pure air
(b) food and water (c) physical, movement and rest(d) psychic movement and rest (e) sleep and
wakefulness and (f) retention of useful materials and
evacuation of waste materials from the body.
3.4.5 There are four forms of treatment in Unani
medicine - Pharmacotherapy, Dietotherapy,
Regimental Therapy and Surgery.
3.4.6 Regimental therapy (Ilaj Bid Tadbir) isspeciality of the Unani system of medicine under which
various methods of treatment are used for specificand complicated diseases.
3.4.7 During the last 50 years, seven PostGraduate specialities have been developed (i)Kulliyat (Fundamentals of Unani System of Medicine)(ii) Ilmul Adviya (Pharmacology) (iii) Amraze Niswan(Gynecology) (iv) Amraze Atfal (Paediatrics) (v)Tahafuzzi wa Samaji Tib (Social and PreventiveMedicine) (vi) Moalejat (Medicine) and (vii) Jarahiyat(Surgery).
3.4.8 Four volumes of National Formulary of UnaniMedicines (NFUM) containing 812 compoundformulations and five volumes of UnaniPharmacopoeia of India (UPI) containing 248monographs on single drugs have been published.
3.5 Homoeopathy
3.5.1 Homoeopathy is a method of treatingdiseases by administering drugs which have beenexperimentally proved to possess the power toproduce similar symptoms on healthy human beings.
3.5.2 Physicians from the time of Hippocrates(around 400 B.C.) have observed that certainsubstances could produce symptoms of a diseasein healthy people similar to those of people sufferingfrom the disease. However, it was a GermanPhysician, Dr. Christian Friedrich SamuelHahnemann (1755 -1843) who examined thisphenomenon scientifically and codified thefundamental principles of Homoeopathy.
3.5.3 The first principle Similia SimilibusCurentur, says that a medicine which could inducea set of symptoms in healthy human beings wouldbe capable of curing a similar set of symptoms inhuman beings actually suffering from the disease.The second principle of Single Medicine says thatone medicine should be administered at a time to aparticular patient during the treatment. The thirdprinciple of Minimum Dose states that the bareminimum dose of a drug which would induce acurative action without any adverse effect should beadministered. Another principle of Homoeopathy isthe assumption that the causation of a disease mainlydepends upon the susceptibility or proneness of an

362
ANNUAL REPORT 2008-09
individual to the incidence of the particular diseasein addition to the action of external agents likebacteria, viruses, etc. Treatment in Homoeopathy,which is holistic in nature, focuses on an individual'sresponse to a specific environment. It is the individualperson who is treated in Homoeopathy and not thedisease per se.
3.5.4 In Homoeopathy, medicines are preparedmainly from natural substances such as plantproducts, minerals and animal sources. Thesehomoeopathic medicines do not have any toxic orpoisonous effect since it is not the chemical orpharmacological effects but the pharmaco-dynamicproperties of the medicines that are acting on thehuman system. Homoeopathy has its own areas ofstrength in therapeutics and it is particularly usefulfor allergies, autoimmune disorders and viralinfections. Many surgical, gynaecological andobstetrical and paediatric conditions and ailmentsaffecting the eyes, nose, ear, teeth, skin, sexualorgans etc. are amenable to homoeopathictreatment. Behavioural disorders, neurologicalproblems and metabolic diseases can also besuccessfully treated by Homoeopathy. Homoeopathycan also be useful in the de-addiction from drugs,tobacco and alcohol and is highly effective in reducingthe craving for these substances. Apart from thecurative aspects, Homoeopathic medicines are alsoused in preventive and promotive health care. Inrecent times, there is an emergence of interest inthe use of Homoeopathic medicines in veterinarycare, agriculture, dentistry, etc.
3.4.5 Homoeopathy was brought into India around1810 A.D. by European missionaries and militarypersonnel. It got official patronage in 1839 when Dr.John Martin Honigberger, a disciple of Hahnemann,successfully treated Maharaja Ranjit Singh of Punjab.
3.6 Yoga
3.6.1 Yoga is primarily a way of life propounded byPatanjali in a systematic form. It consists of eightcomponents namely, restraint, observance ofausterity, physical postures, breathing exercise,restraining of sense organs, contemplation,meditation and samadhi. These steps in the practiceof Yoga have the potential to improve social and
personal behaviourI and to improve physical healthby encouraging better circulation of oxygenatedblood in the body, restraining the sense organs andthereby inducing tranquillity and serenity of mind.The practice of Yoga has also been found to be usefulin the prevention of psychosomatic disorders/diseases and improves individual resistance andability to endure stressful situations.
3.6.2. Though Yoga is primarily a way of life,nevertheless, its promotive, preventive and curativeinterventions are efficacious. A number of posturesare described in Yogic works to improve health, toprevent diseases and to cure illness. The physicalpostures are required to be chosen judiciously andhave to be practised in the correct way so that thebenefits of prevention of disease, promotion of healthand therapeutic use can be derived from them.
3.6.3 Studies have revealed that the Yogicpractices improve intelligence and memory and helpin developing resistance to situations of strain andstress and also help individuals to develop anintegrated personality. Meditation can stabilizeemotional changes and prevent abnormal functionsof the vital organs of the body. Studies have shownthat meditation not only restrains the sense organsbut also controls the nervous system.
3.7 Naturopathy
3.7.1. Naturopathy is a drugless non invasivetherapy involving the use of natural materials in itstreatment based on the theory of vitality, the theoryof toxicemia, the theory of self heating capacity ofthe body and the principles of Healthy Living.Naturopathy is not only a system of treatment butalso a way of life.
3.7.2. The primary causes of disease as perNaturopathy, are- i)Lowered vitality, Ii)abnormalcomposition of blood & lymph, and , iii) accumulationof foreign or morbid matter. The main principle ofNaturopathy treatment is "Unity of Disease and Unityof Cure". The advocates of Naturopathy payparticular attention to eating and living habits,adoption of purificatory measures, use ofhydrotherapy, cold packs, mud packs, baths,massages, etc.
363
ANNUAL REPORT 2008-09
4.1 Central Council of IndianMedicine
4.1.1 The Central Council of Indian Medicine(CCIM)is a statutory body established under the IndianMedicine Central Council Act, 1970 vide Governmentof India Gazette Notification Extraordinary Part IISection 3(ii) dated 10.8.1971. The main objectivesof the Central Council are as under:-
(i) To prescribe minimum standards of educationin Indian Systems of Medicine viz. Ayurveda,Siddha and Unani Tibb.
(ii
i
) To advise the Central Government in mattersrelating to the recognition (includingwithdrawal) of medical qualifications in theSecond Schedule to the Indian MedicineCentral Council Act, 1970.
(ii) To maintain a Central Register of IndianMedicine and to revise the Register from timeto time.
(iv) To prescribe Standards of ProfessionalConduct, Etiquette and Code of Ethics to beobserved by the practitioners.
(v) To consider and furnish the recommendationon the applications received by theGovernment of India for the establishment ofnew Ayurveda. Siddha and Unani medicalcolleges, to start new or higher courses ofstudy or training and to increase intakecapacity.
4.1.2 The Central Council of Indian Medicine withthe previous sanction of the Central Government asrequired under Section 36 of the Indian MedicineCentral Council Act, 1970 and after obtaining thecomments of the State Governments as requiredunder Section 2 of the said Act has prescribed
courses for Under Graduate and Post Graduate
education in Ayurveda, Unani and Siddha through
the following Regulations:-
(a) Under Graduate Course
1. Indian Medicine Central Council (Minimum
Standards of Education in Indian Medicine)
(Amendment) Regulations, 1989 further
amended in 2005 for Ayurvedacharya
(Bachelor of Ayurvedic Medicine Surgery)
Course.
2. Indian Medicine Central Council (Minimum
Standards of Education in Indian Medicine)
Amendment Regulations, 1995 for Kamil-e-
tib-o-Jarahat (Bachelor of Unani Medicine
Surgery) Course.
3. Indian Medicine Central Council (Minimum
Standards of Education in Indian Medicine)
Amendment Regulations, 2006 for Siddha
Maruthuva Arignar (Bachelor of Siddha
Medicine and Surgery) BSMS Course.
(b) Post Graduate Course
1. Indian Medicine Central Council (Post-
graduate Education) (Amendment)
Regulations, 2005 for Ayurved Vachaspati
MD (Ay.).
2. Indian Medicine Central Council (Post-
graduate Unani (Education) Regulations,
2007 for Mahir-e-Tib (Doctor of Medicine) and
Mahir-e-Jarahat (Master of Surgery).
3. Indian Medicine Central Council (Post-
graduate Education) Regulations, 1979
further amended in 1986 for Siddha
Maruthuva Perarignar MD (Siddha) Course.
Chapter 4
EducationEducationEducationEducationEducation
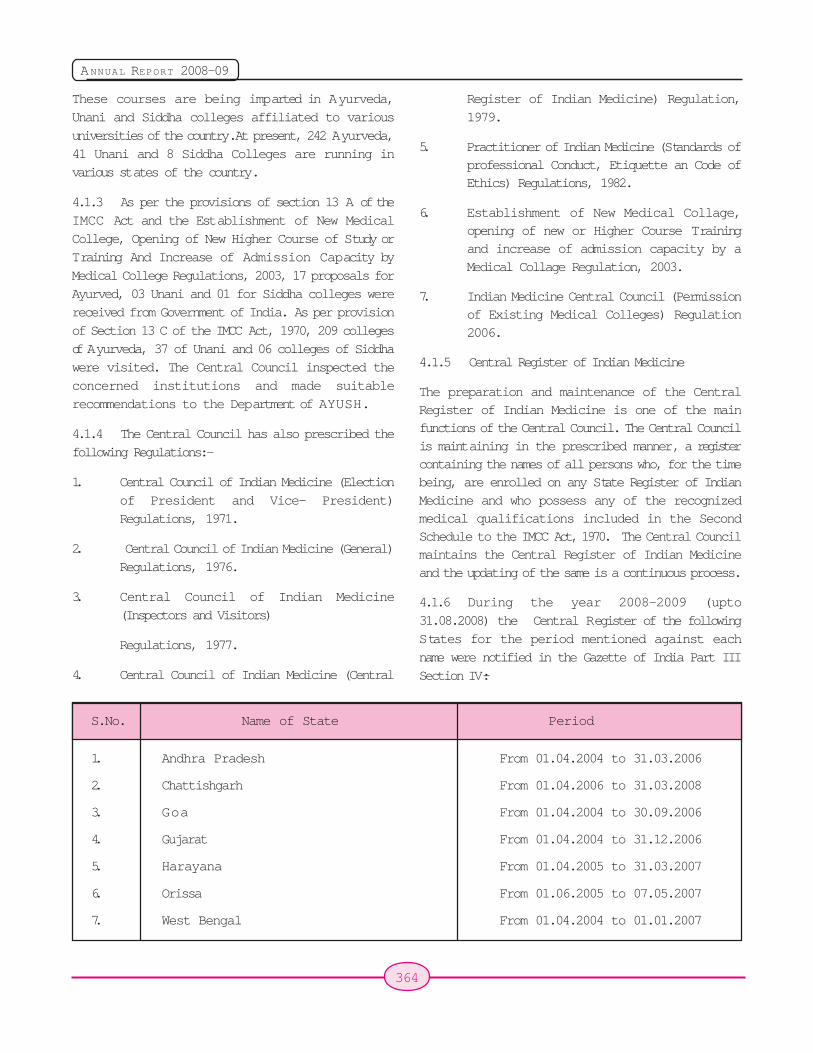
364
ANNUAL REPORT 2008-09
These courses are being imparted in Ayurveda,Unani and Siddha colleges affiliated to variousuniversities of the country. At present, 242 Ayurveda,41 Unani and 8 Siddha Colleges are running invarious states of the country.
4.1.3 As per the provisions of section 13 A of theIMCC Act and the Establishment of New MedicalCollege, Opening of New Higher Course of Study orTraining And Increase of Admission Capacity byMedical College Regulations, 2003, 17 proposals forAyurved, 03 Unani and 01 for Siddha colleges werereceived from Government of India. As per provisionof Section 13 C of the IMCC Act, 1970, 209 collegesof Ayurveda, 37 of Unani and 06 colleges of Siddhawere visited. The Central Council inspected theconcerned institutions and made suitablerecommendations to the Department of AYUSH.
4.1.4 The Central Council has also prescribed thefollowing Regulations:-
1. Central Council of Indian Medicine (Electionof President and Vice- President)Regulations, 1971.
2. Central Council of Indian Medicine (General)Regulations, 1976.
3. Central Council of Indian Medicine(Inspectors and Visitors)
Regulations, 1977.
4. Central Council of Indian Medicine (Central
Register of Indian Medicine) Regulation,1979.
5. Practitioner of Indian Medicine (Standards ofprofessional Conduct, Etiquette an Code ofEthics) Regulations, 1982.
6. Establishment of New Medical Collage,opening of new or Higher Course Trainingand increase of admission capacity by aMedical Collage Regulation, 2003.
7. Indian Medicine Central Council (Permissionof Existing Medical Colleges) Regulation2006.
4.1.5 Central Register of Indian Medicine
The preparation and maintenance of the CentralRegister of Indian Medicine is one of the mainfunctions of the Central Council. The Central Councilis maintaining in the prescribed manner, a registercontaining the names of all persons who, for the timebeing, are enrolled on any State Register of IndianMedicine and who possess any of the recognizedmedical qualifications included in the SecondSchedule to the IMCC Act, 1970. The Central Councilmaintains the Central Register of Indian Medicineand the updating of the same is a continuous process.
4.1.6 During the year 2008-2009 (upto31.08.2008) the Central Register of the followingStates for the period mentioned against eachname were notified in the Gazette of India Part IIISection IV:-
S.No. Name of State Period
1. Andhra Pradesh From 01.04.2004 to 31.03.2006
2. Chattishgarh From 01.04.2006 to 31.03.2008
3. Goa From 01.04.2004 to 30.09.2006
4. Gujarat From 01.04.2004 to 31.12.2006
5. Harayana From 01.04.2005 to 31.03.2007
6. Orissa From 01.06.2005 to 07.05.2007
7. West Bengal From 01.04.2004 to 01.01.2007
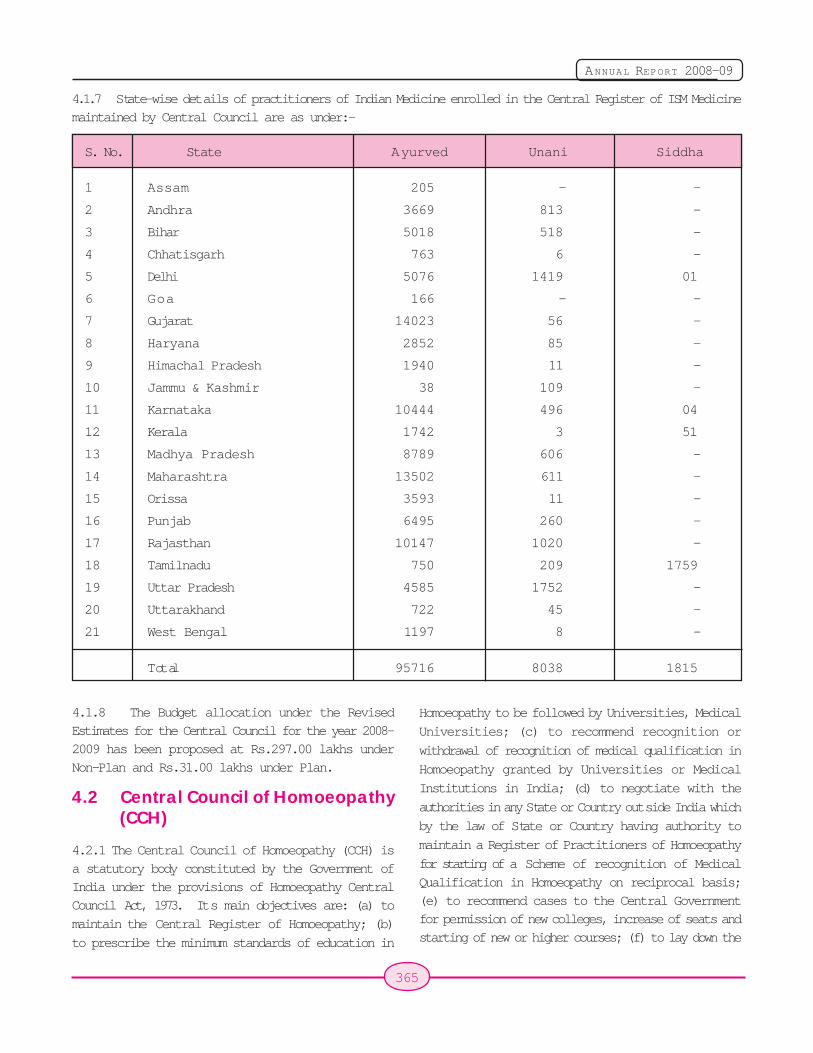
365
ANNUAL REPORT 2008-09
4.1.7 State-wise details of practitioners of Indian Medicine enrolled in the Central Register of ISM Medicinemaintained by Central Council are as under:-
S. No. State Ayurved Unani Siddha
1 Assam 205 - -
2 Andhra 3669 813 -
3 Bihar 5018 518 -
4 Chhatisgarh 763 6 -
5 Delhi 5076 1419 01
6 Goa 166 - -
7 Gujarat 14023 56 -
8 Haryana 2852 85 -
9 Himachal Pradesh 1940 11 -
10 Jammu & Kashmir 38 109 -
11 Karnataka 10444 496 04
12 Kerala 1742 3 51
13 Madhya Pradesh 8789 606 -
14 Maharashtra 13502 611 -
15 Orissa 3593 11 -
16 Punjab 6495 260 -
17 Rajasthan 10147 1020 -
18 Tamilnadu 750 209 1759
19 Uttar Pradesh 4585 1752 -
20 Uttarakhand 722 45 -
21 West Bengal 1197 8 -
Total 95716 8038 1815
4.1.8 The Budget allocation under the RevisedEstimates for the Central Council for the year 2008-2009 has been proposed at Rs.297.00 lakhs underNon-Plan and Rs.31.00 lakhs under Plan.
4.2 Central Council of Homoeopathy(CCH)
4.2.1 The Central Council of Homoeopathy (CCH) isa statutory body constituted by the Government ofIndia under the provisions of Homoeopathy CentralCouncil Act, 1973. Its main objectives are: (a) to
maintain the Central Register of Homoeopathy; (b)
to prescribe the minimum standards of education in
Homoeopathy to be followed by Universities, Medical
Universities; (c) to recommend recognition or
withdrawal of recognition of medical qualification in
Homoeopathy granted by Universities or Medical
Institutions in India; (d) to negotiate with the
authorities in any State or Country outside India which
by the law of State or Country having authority to
maintain a Register of Practitioners of Homoeopathy
for starting of a Scheme of recognition of Medical
Qualification in Homoeopathy on reciprocal basis;(e) to recommend cases to the Central Governmentfor permission of new colleges, increase of seats andstarting of new or higher courses; (f) to lay down the

366
ANNUAL REPORT 2008-09
standards of professional conduct, etiquette andcode of ethics to be observed by the practitioners ofHomoeopathy.
4.2.2 The CCH is constituted of elected membersfrom the State Boards/Councils of Homoeopathy andfrom the University Faculties/Departments ofHomoeopathy and of members nominated by theCentral Government. The Council functions throughvarious Committees like the Executive Committee,Finance Committee, PG Committee etc. The GeneralBody of the Council is its apex decision making body.During the period under report, there were 49members in the Central Council of Homoeopathybesides its President and Vice President.
4.2.3 The Homoeopathy Central Council Act, 1973was amended in 2002 and the power to grantpermission for starting new colleges, introducing newor higher courses of study and increasing thenumber of seats in a College is now vested with theCentral Government.
4.2.4 The Central Council maintains the CentralRegister of Homoeopathy in the prescribed manner.It has published Central Register of Homoeopathy inthe Official Gazette during 1993, 1996, 2003, 2004and 2007. Another part of the Central Register hasbeen sent to Government Press for publication inthe Official Gazette. The Council has completed thework regarding renewal of Central Register ofHomoeopathy (published in 1993, in respect of bothParts I and II), by sending the list of names forremoval from said Register, to the Controller ofGovernment Publications. The Central Council alsoissues Direct Registration as per prescribedprocedure. 94 practitioners possessing recognisedmedical qualification have been given directregistration by the Council during the period underreport. Inspection of 39 Colleges has beenundertaken alongwith inspection of 9 BHMSExaminations centres.
4.2.5 The Central Council has recommended toCentral Government the qualifications for inclusionin the IInd Schedule of Homoeopathy Central CouncilAct, 1973 regarding: (a) M.D.(Hom) qualificationawarded by Dr. B.R. Ambedkar University, Agra from
October, 2005 (b) M.D.(Hom) qualification awardedby University of Mumbai from January, 2005 insubjects of Materia Medica, Homoeopathy Philosophyand Repertory. (c) BHMS degree qualificationawarded by Dr. Hari Singh Gour University, Sagar(M.P.) upto December, 2010. and (d) recognition of5 colleges.
4.2.6 The Central Council has finalizedamendments in Homoeopathy (Minimum Standard ofEducation) Regulations for onward submission toCentral Government for sanction. The Councilconducted a Workshop on "Research Methodology"for teachers of Post Graduate HomoeopathicColleges on 27.8.2008 at New Delhi.
4.2.7 The Central Council of Homoeopathy issupported by the Central Government throughannual budget grants. The budget sanctioned toCentral Council of Homoeopathy by the CentralGovernment for the year 2008-2009 is Rs.7.00 lakhsunder Plan and Rs.100.00 lakhs under Non-Plan.
National Institutes of the Department
4.3 National Institute of Ayurveda(NIA), Jaipur
4.3.1 This Institute was established in February1976 by the Government of India as an apex Instituteof Ayurveda in the country to develop high standardsof teaching, training and research in all aspects ofthe Ayurvedic system of medicine. It is affiliated tothe Rajasthan Ayurved University, Jodhpur.
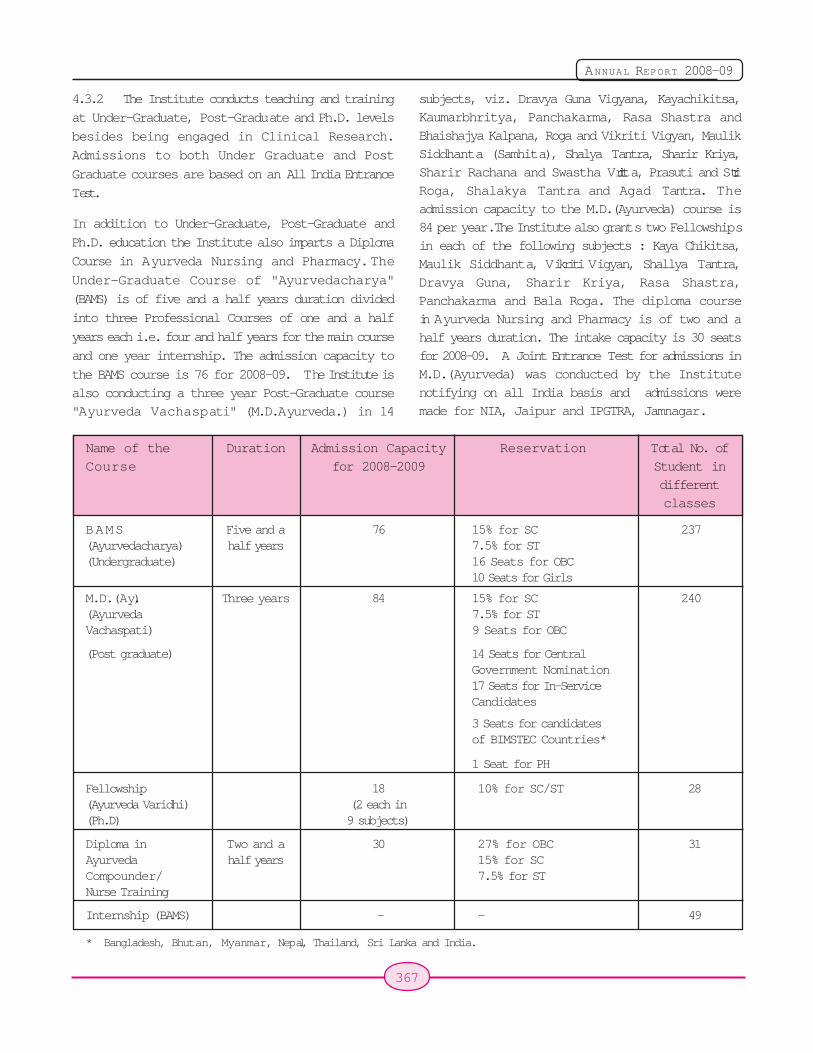
367
ANNUAL REPORT 2008-09
4.3.2 The Institute conducts teaching and training
at Under-Graduate, Post-Graduate and Ph.D. levels
besides being engaged in Clinical Research.
Admissions to both Under Graduate and Post
Graduate courses are based on an All India Entrance
Test.
In addition to Under-Graduate, Post-Graduate and
Ph.D. education the Institute also imparts a Diploma
Course in Ayurveda Nursing and Pharmacy. The
Under-Graduate Course of "Ayurvedacharya"
(BAMS) is of five and a half years duration divided
into three Professional Courses of one and a half
years each i.e. four and half years for the main course
and one year internship. The admission capacity to
the BAMS course is 76 for 2008-09. The Institute is
also conducting a three year Post-Graduate course"Ayurveda Vachaspati" (M.D.Ayurveda.) in 14
subjects, viz. Dravya Guna Vigyana, Kayachikitsa,Kaumarbhritya, Panchakarma, Rasa Shastra andBhaishajya Kalpana, Roga and Vikriti Vigyan, MaulikSiddhanta (Samhita), Shalya Tantra, Sharir Kriya,Sharir Rachana and Swastha Vritta, Prasuti and StriRoga, Shalakya Tantra and Agad Tantra. Theadmission capacity to the M.D.(Ayurveda) course is84 per year. The Institute also grants two Fellowshipsin each of the following subjects : Kaya Chikitsa,Maulik Siddhanta, Vikriti Vigyan, Shallya Tantra,Dravya Guna, Sharir Kriya, Rasa Shastra,Panchakarma and Bala Roga. The diploma coursein Ayurveda Nursing and Pharmacy is of two and ahalf years duration. The intake capacity is 30 seatsfor 2008-09. A Joint Entrance Test for admissions inM.D.(Ayurveda) was conducted by the Institutenotifying on all India basis and admissions weremade for NIA, Jaipur and IPGTRA, Jamnagar.
Name of the Duration Admission Capacity Reservation Total No. ofCourse for 2008-2009 Student in
differentclasses
BAMS Five and a 76 15% for SC 237(Ayurvedacharya) half years 7.5% for ST(Undergraduate) 16 Seats for OBC
10 Seats for Girls
M.D.(Ay.) Three years 84 15% for SC 240(Ayurveda 7.5% for STVachaspati) 9 Seats for OBC
(Post graduate) 14 Seats for CentralGovernment Nomination17 Seats for In-ServiceCandidates
3 Seats for candidatesof BIMSTEC Countries*
1 Seat for PH
Fellowship 18 10% for SC/ST 28(Ayurveda Varidhi) (2 each in(Ph.D) 9 subjects)
Diploma in Two and a 30 27% for OBC 31Ayurveda half years 15% for SCCompounder/ 7.5% for STNurse Training
Internship (BAMS) - - 49
* Bangladesh, Bhutan, Myanmar, Nepal, Thailand, Sri Lanka and India.
368
ANNUAL REPORT 2008-09
Reservation of 15% for SC, 7½ % for ST candidatesis available in admissions to Under-Graduate, Post-Graduate and Diploma Courses and 10% for SC andST for the Ph.D. course. There is a reservation of10 seats for women candidates in the BAMS courseand 3 seats are reserved for candidates fromBIMSTEC countries (Bangladesh, Myanmar, SriLanka, Thailand, Nepal, Bhutan, India) in the PostGraduate course.
The stipend being paid to PG scholars is Rs. 7000in the 1st Year, Rs. 7500 in the 2nd Year and Rs.8000in the 3rd Year. The stipend for Ph.D. scholarsis Rs. 8275 for the 1st Year and Rs. 8550 for the2nd Year.
(c) Hospital Activities: The NIA has twoHospitals with a total of 180 beds along with variousdiagnostic facilities for pathological and bio-chemicaltests, X-ray, ECG, TMT, Spirometry, Dental, Audiometryetc. Medicines, to the maximum extent possible, aredispensed free both in the OPD and IPD. During theyear, (up to August 08). 1266 new Indoor and 27511new Outdoor patients were treated. The Institute alsoorganizes Medical Camps for the benefit of SC andST inhabited and Kacchi Basti areas in the State ofRajasthan. During the year(up to August 2008) 3six-day, and 2 one-day Mobile Clinical camps wereorganized during which 2584 patients were providedmedical checkups and medicines worth Rs.2,19,657were distributed free of cost. An Ayurvedic Centre ofExcellence for Eye Disease (NIASACEED) has beenstarted in collaboration with SreedhareeyamAyurvedic Eye Hospital and Research Centre,Ernakulam. This is an exclusive Ayurvedic EyeHospital providing non-surgical treatment to variouseye disorders and diseases like Diabetic Retinopathy,Glaucoma, Cataract, Macular Degeneration, Myopiaetc.
Geriatric and Dietary clinics are providingconsultation, advice and also medicines to thepatients. As part of the initiative to expand patientcare activities to a larger segment of the populationin the City, the NIA opened its first Satellite Clinic atJawahar Nagar. A Nature Cure Unit is also functioningat the Institute.
The Institute has a separate fully equipped
Panchakarma Hospital. A total of 39077 karmas wereperformed (upto Aug. 2008) on a total number of14694 patients. NIA has a Central Laboratory dividedinto 6 units for conducting investigations for patientcare and research purposes for all the Departments.About 37327 diagnostical investigations, pathologicaltests have been performed during 2008-09 (uptoAugust 2008). Apart from these, 1706 test(Spirometry, ECG, CTMT, Sonography and X-Ray)were also performed. The Institute has been provideda highly sophisticated High Performance LiquidChromatograph (HPLC) and new generationapparatus of International Standard by WHO for plantbased research work.. In addition, the institute has aDrug Standardization and Quality Control Laboratory,Drug Testing Laboratory, Physiology Laboratory anda well equipped pharmacy. Tele Medicine Programmehas been started with 3 Divisional Headquarters ofJodhpur, Udaipur and kota.
(d) General Activities : The Budget Allocationproposed for 2008-09 is Rs. 825 lakhs under Planand Rs. 1000 lakhs under Non-Plan. The WomenComponent is provided at Rs. 61 lakhs in Plan andRs. 57 lakhs in Non Plan. The Institute has acquired8 Hectares of land from State Government fordevelopment of its Second Campus and HerbalGarden which will set an example for otherinstitutions in the country. This Herbal Garden willbe used both for demonstration, teaching, training,research and pharmaceutical purposes.
4.4 National Institute of Siddha (NIS),Chennai
4.4.1 The National Institute of Siddha (NIS),Chennai is an autonomous organization under thecontrol of the Department of AYUSH, Ministry ofHealth and Family Welfare, Government of India.The Institution was dedicated to the nation on 3rdSeptember 2005 by Dr. Manmohan Singh, Hon'blePrime Minister of India. And is being developed as aCentre of Excellence for the Siddha system ofMedicine. Post Graduate courses in Siddha areconducted along with providing medical care andconducting research to develop, promote andpropagate the system. The Institute has beenestablished by the Government of India as a joint

369
ANNUAL REPORT 2008-09
venture with the Government of Tamil Nadu at anestimated cost of Rs.47.00 crores with the capitalexpenditure being shared in the ratio of 60:40 andthe recurring expenditure in the ratio of 75:25between the Central and State Governments.
A view of NIS campus, Chennai at night
4.4.2 The Post Graduate courses are of 3-yearduration and are available in in six specialisedbranches of Siddha viz. i) Maruthuvam, ii)Gunapadam, iii) Sirappu Maruthuvam, iv) Noi Nadal,v) Kuzhanthai maruthuvam and vi) Nanju NoolumMaruthuva Neethi Noolum. Admissions are made onthe basis of an Entrance Examination.
4.4.3 The admission capacity to the MD (S) coursehas been increased from 30 to 46 per year from 2008-09 on account of 27% OBC reservation. Of the totalseats of 46, one seat is allotted to a Foreign studentfrom BIMSTEC countries every year by rotation fromany one of the existing branches. Of the total seats,15% are reserved for SC, 7.5% for ST and 27% for
OBC Candidates. OBC reservation has beenimplemented from the academic year 2008-09. Hostelfacility for 30 male and 60 female students is available.
4.4.4 The stipend to the PG students is being paid@ Rs.7000/- + DA per month in the 1st Year, Rs.7500/- + DA per month in the 2nd Year and Rs.8000/- DAper month in the 3rd Year.
4.4.5 Ayothidass Pandithar Hospital at NationalInstitute of Siddha has a total capacity of 120 beds.Various diagnostic facilities like Clinical Pathology,Microbiology, Bio Chemistry, are also available in thehospital. Medicines are dispensed free of cost bothin the OPD and with diet in IPD. The OPD and IPDservices are extended on all the 365 days of theyear. Special OPD for geriatric patients is being run.The treatment service include Yoga, Varma,Thokanam (Physiotherapy) etc. The occupancy ofIPD remains 100%.
4.4.6 On an average, about 1100 - 1200 patientsare being attended daily at OPD. Patients from allgroup of economic strata are seeking treatment fromOPD. A total of 1.6 lakhs cases have been treated atOPD from 1st April to 31st August 2008. The publicresponse is highly encouraging and patient reportingis steadily increasing.
4.4.7 National Institute of Siddha has signed the MoUwith Anna University, Chennai, Tuberculosis ResearchCentre, Chennai (ICMR) and Central CouncilResearch of Ayurveda and Siddha (CCRAS), NewDelhi for undertaking collaborative research in SiddhaMedicine. WHO sponsored project on "Developmentof Siddha Treatment guidelines for selected diseases"is on-going. National Institute of Siddha has beenrecognized as Regional Pharmocovigilence /Peripheral Pharmacovigilence Centre.
4.4.8 Two Health Camps were organized one atTirunavallur in Tindivanam in Tamil Nadu and anotherat Muttathur, Vikkiravandi Block for the benefit of ruralpeople. A Free Medical camp at Government HigherSecondary School. Pulicat (Pazhaverkadu),Tiruvallur District (Supermbadur ParliamentaryConstituency) was conducted on 22nd November2008. Nearly 250 patients benefited by this camp.Medicine were given free of cost.
370
ANNUAL REPORT 2008-09
4.4.9 Ladies Hostel, Guest House and Opening ofAyothidoss Pandithar Bust was inaugurated on 25thOctober, 2008 by the Hon'ble Union Minister ofChemical and Fertilizers and Minister of Steel Shri.Ram Vilas Paswan in the presence of Hon'ble Ministerof Health and Family Welfare, Dr. AnbumaniRamadoss and Hon'ble Minister of State of Healthand Family Welfare, Smt. Panabaka Lakshmi atNational Institute of Siddha(NIS), Chennai.
4.4.10 A biennial Journal of Siddha has been startedby NIS and the inaugural issue was released by theHon'ble Minister of Health and Family Welfare, Dr.Anbumani Ramadoss, Government of India on 25thOctober, 2008 at National Institute of Siddha.
4.4.10 The Institute is planning for the establishmentof International standard Drug testing laboratory,Computerization of OPD / IPD services forstrengthening the management and quality ofservices, Recognition of NIS as center for carryingout Ph.D work, Digitization of Siddha literature,Release of Journal of Siddha and Establishment ofPharmacy manufacturing unit.
4.4.11 The Government of India has allocated grantin aid of Rs.10.74 crore in the Revised Estimatesduring 2008-09 to the Institute.
4.5 National Institute ofHomoeopathy (NIH), Kolkata
4.5.1 The National Institute of Homoeopathy wasestablished on 10th December 1975 in Kolkata asan Autonomous Institution under the Ministry of
Health and Family Welfare, Government of India, tobe a model institute in Homoeopathy in the country.
4.5.2 The Governing Body of the institute is headedby the Hon'ble Union Minister of Health & FamilyW elfare. There is a Standing Finance Committee(SFC) constituted by the Department of AYUSH tosupervise the developmental and financial aspectsof the institute.
4.5.3 The NIH was affiliated to the University ofKolkata up to 2003-04 but is affiliated to the WestBengal University of Health Sciences, Kolkata from2004-05 onwards. Presently the Institute conductstwo regular courses in Homoeopathy viz. Bachelorof Homoeopathic Medicine & Surgery i.e., BHMS andthe Doctor of Medicine in Homoeopathy i.e., MD(Hom.). The Institute also arranges Re-OrientationTraining courses for Teachers of differentHomoeopathic Colleges.
4.5.4 The BHMS course is of 5 ½ year's duration(including one year compulsory internship) and wasstarted in December 1987. Presently the20th batchis on. Candidates possessing Higher Secondary(10+2) or equivalent qualification with 5 subjectsincluding English, Physics, Chemistry & Biology with50% marks aggregate (45% in case of SC/ST) areeligible for admission. 60 seats are available amongwhich 14 are allotted to those candidates who arenominated from the States and Union Territorieswhere no homoeopathic colleges exists. 10 seats arereserved for candidates sponsored by Governmentof Sri Lanka. 30 candidates (15% SC, 7.5% ST andrest General) get admission on the basis of All IndiaEntrance Examination and 01 seats is reserved forforeign nationals on self financing basis nominatedby the Ministry of Health & Family Welfare,Government of India and 5 seats are reserved forcandidates nominated by Indian Council for CulturalRelations under BIMSTIC quota.
4.5.5 The MD (Hom) course is run by the Institutein three subjects viz. Organon of Medicine, Repertoryand Materia Medica. Six seats are available in eachsubject. Ten batches have been enrolled through AllIndia Entrance examination so far.
4.5.6 The Institute had conducted 44 seminars
371
ANNUAL REPORT 2008-09
during the year 2007-08.During the year 2008-09,29 seminars have been conducted till 21.11.2008and 18 more such seminars are designed to becompleted during the remaining period of the year.
4.5.7 The Hospital has both outpatient & in-patientdepartments to provide medical care to patients.Besides the general clinics, specialized clinics arealso in service. These are equipped with investigationfacilities comprising of clinical pathology, radiology,ultra sonography and ECG. Facilities for sophisticatedbiochemical investigations are also available.Investigations are done at nominal cost. The Institutehas been presently providing indoor facilities through100-bedded hospital. 10 beds are earmarked forsurgery and 10 for maternity. As this is an academicInstitution, patients suffering from different ailmentsare admitted for curative purpose as well as for clinicaltraining of the under-graduate and post-graduatestudents. Registration of patients in OPD iscomputerised which is connected by LAN system.During the financial year 2007-08, 137402 no. ofpatients attended OPD and 681 patients were treatedin IPD. Besides NIH rendered medical service toaround 24000 patients through its peripheral OPDat Kalyani and Gobardanga.
4.5.8 Every year the Institute sends a medical teamto the Ganga Sagar Mela in South 24 Parganas(West Bengal) district to provide homoeopathictreatment, on the spot, to ailing pilgrims from all overthe country.
4.5.9 The Institute has participated in three ArogyaMelas during the period 2007-08, one was atDehradun (20th to 23rd April 07), second wasInternational Arogya Mela at New Delhi (26th to 29thOctober, 2007) conducted by Ministry of Health &Family Welfare, Government of India and the thirdat Amritsar(14th to 17th March, 08). During the year2008-09, the Institute has participated in ArogyaMelas at Indore and at New Delhi.
4.5.10 At present the research wing is involved inconducting clinical research on:
Thyroid Research, Psoriasis, Spondylosis andAllergic Rhinitis
4.5.11 The Kalyani Herb Garden situated 60 kmaway from Kolkata was envisaged for acclimatizingexotic plants which are of importance in homoeopathyand building of repository of medicinal plants for useby students and researchers. A small herb gardenhas also been developed within the NIH campus forteaching purpose.
4.5.12 The Library and Information Service divisionhas more than 19845 documents (macro & micro)including rare homoeopathy treatises. There are1042 bound journals. 61 periodicals subscribed toregularly, 43 periodicals were received as gift. Itprovides various services i.e. Documentation,Reference, Referral, Current Awareness Service(CAS), Selective Dissemination Information (SDI),Document delivery, Internet etc. to the in-housereaders. Book Bank service for students has beenintroduced since academic session 2003-04onwards.
4.5.13 The NIH is fully funded by the Governmentof India through grant-in-aid. The budget provisionfor the financial year 2007-08 was Rs.20.5 crores(Plan Rs.19 crores and Non-Plan Rs.1.50 crores).The budget for the financial year 2008-09 is Rs.18.65crores (Plan Rs. 17 crores and Non-Plan Rs.1.65crores).
4.6 National Institute of Naturopathy(NIN), Pune
4.6.1 National Institute of Naturopathy (NIN) isregistered under the Societies Registration Act., 1860and came into existance on 22-12-1986. This institutehas a "Governing Body" headed by the UnionMinister for Health & Family Welfare as its President.
4.6.2 National Institute of Naturopathy (NIN) islocated in a historical building called "Bapu Bhavan"which is situated at Tadiwala Road, Pune. "BapuBhavan" is named after Mahatma Gandhi, Father ofthe Nation, who stayed here for 156 days and madethis institution his home whenever he was in Punefrom the year 1934. Formerly this place was knownas "Nature Cure Clinic and Sanatorium" which wasrun by late Dr. Dinshaw K. Mehta. The All India NatureCure Foundation Trust was established in this Centre
372
ANNUAL REPORT 2008-09
by Dr. Dinshaw K. Mehta. Mahatma Gandhi becameits life long Chairman. Gandhiji conducted hisNaturopathy experiments and organised National andInternational activities while staying here. The presentcomplex was handed over to Government of Indiaon 17-03-1975 by Dr.Dinshaw K. Mehta for startingthe National Institute of Naturopathy.
Th statue of Mahatma Gandhi at the campusat NIN.
4.6.3 Naturopathy is a drugless non-invasiverational and evidence based system of medicineimparting treatments with natural elements based onthe Theory of vitality, theory of toxemia, theory ofself healing capacity of the body and the principlesof healthy living. The applied aspects of Naturopathyincludes mainly fasting and diet supported bytreatments with natural elements which includesHydrotherapy, Chromotherapy, Mud Therapy,Manipulative therapy, Electrotherapy,Magnetotherapy, Physiotherapy, Exercise & YogaTherapy.
4.6.4 The NIN has an OPD clinic with freeconsultation services where various Naturopathytreatments are given to the patients at a verysubsidized rate of Rs.250/- per week. The institutealso conducts 8 Yoga classes daily. A health Shop isbeing run in the institute where Natural food anddrinks, products free from chemicals and fertilizersare made available to the public. Books onNaturopathy, Yoga and other Health subjects andvarious instruments used in the treatment ofNaturopathy are kept for sale.
Visitors taking a look at the publications at NIN
4.6.5 The Institute publishes "Nisargopachar varta"- a bilingual magazine(Hindi/English) every month."rational Hydrotherapy" - a classical work by theAmerican Naturopath Dr. J. H. Kellogg - has beenreprinted by the NIN and the copies are available forsale. During the current year upto 30th September23 free guest lectures were organized featuringeminent speakers on Procedures and Benefits ofNaturopathy and Yoga for treating different commonailments. NIN organized six one day workshops ondifferent diseases for general public. Workshops areconducted on Research Methodology andContinuing Medical Education (CME) programme forthe BNYS graduates and Re-orientation programmefor full time Naturopathy practitioners. NIN has a richLibrary with more than 8000 books.
4.6.6 A Naturopathic Diet Centre is being run forproviding diet facilities to patients and to the generalpublic who visit the institute.
4.6.7 Fifty students are undergoing 1 year FullTime Treatment Attendant Training Course (TATC)with a stipend of Rs.2000/- p.m. Twelve BNYS internsfrom different Naturopathy colleges are undergoingInternship Programme with a monthly Stipend ofRs.3500/-.
4.6.8 Free Acupressure Treatment is given topatients for six days in a week. Average 1372 patientsper month were treated upto September, 08.
4.6.9 In order to promote self health and healthawareness among public on naturopathic lines,
373
ANNUAL REPORT 2008-09
financial aid was given to NGOs in different parts ofthe country. A total of 855 programmes wereconducted up to September, 08 in States other thanthe North East & Sikkim. The NIN sponsored 159programmes in North Eastern States of Manipur,Sikkim, Assam etc. till September, 08.
4.6.10 A 5-days Naturopathy Food Exhibition washeld in this Institute from 27th to 31st August, 2008.Various natural recipes devoid of additives,chemicals, spices, artificial sweeteners etc. weremade available during the five days. People from allwalks of life visited the exhibition and learnt abouthealthy dishes as well as the healthy methods ofpreparing them. A 3-day "National Conference onNaturopathy" was also organised at the AlpabachatBhavan, Pune from 8th to 10th Dec.07. 450delegates participated in the conference. Smt.Panabaka Lakshmi, Hon'ble Minister of State,Government of India, Ministry of Health & FamilyWelfare was the Chief Guest.
4.6.11 NIN celebrated the Naturopathy day on 2ndOct.'07 by observing 3-days fast on water from 2ndOctober to 4th October 2007. About 35 officers andstaff members and ten volunteers from publicparticipated in the group fasting. Dr. Knox, an expertChiropractor from United States held a specialsession on "Chiropractic" for the fasting group.
4.7 National Institute of UnaniMedicine (NIUM), Bangalore
4.7.1 National Institute of Unani Medicine (NIUM)was established in 1984, as an autonomousorganization under the Department of AYUSH,Ministry of Health & Family Welfare. It was registeredunder the Societies Registration Act on 19thNovember 1984 and is sought to be developed as aCentre of Excellence for the propagation of the Unanisystem of Medicine. NIUM. is a joint venture of theGovernment of India and the State Government ofKarnataka. It is affiliated with the Rajiv GandhiUniversity of Health Sciences (RGUHS), Bangalore,Karnataka.
The Institute is being developed as a model PostGraduate, teaching, training, and research institution
in the Unani System. There is a 100 bed Hospital,Academic Block, Hostel Building, AdministrativeBlock, and Library.
4.7.2 The Institute follows the curriculum prescribedby the Central Council of Indian Medicine and hasbeen able to attract students from all parts of thecountry. Post Graduate Courses in M.D. Unani areofferred in the following four disciplines.
1. Moalijat (Medicine)
2. Ilmul Qablat wa Amraz-e-Niswan-wa-Atfal(Obstetrics and Gynecology)
3. Hifzan-e-Sehat (Preventive and SocoalMedicine)
4. Ilmul Advia (Pharmacology)
4.7.3 Post Graduate courses in Kulliyat and IlmulSaidla are to be started in 2008-09. It has also beendecided to start a certificate course for providingorientation in the Unani system of Medicine to foreignnationals, who are qualified in other systems ofMedicine.
4.7.4 The Entrance Test for the fourth Batch P.GUnani was held on 22.09.2007 and classescommenced from 1.11.2007. The Examination of thebatch 2006-07 was held from 5th to 8th September,2007.
4.7.5 The meetings of the Institutional Animal EthicsCommittee for reviewing the project proposals of P.G.Scholars for Ethical consideration and InstitutionalEthics Committee for Clinical Research was held on15.12.2007 to finalize the projects of P.G. scholars(Batch 2007-08) of Department of Moalijat and IlmulQabalat wa Amraze Niswan and also projects of somefaculty members.
4.7.6 Reorientation Training Programme forteachers of Moalejat (Medicine) and Ilmul Advia wereorganized in this Institute w.e.f 17.03.2008 to22.03.2008 & 26.03.2008 to 31.03.2008respectively. Teachers from most of the UnaniColleges from all over the country and ResourcePersons from reputed institutions participated in theTraining Programme.
374
ANNUAL REPORT 2008-09
4.7.7 The Institute has taken active participationin AROGYA fairs organized by the Department ofAYUSH.
4.7.8 During the year under report a RadiologyUnit was established, Construction of residentialquarters, girls hostel and animal house under the2nd phase were completed. The Institute is engagedin collaborative research with other Institutions andOrganizations viz. Government Nizamia TibbiyaCollege, Hyderaband Aligarh Muslim University,Aligarh, Jamia Hamdard, New Delhi, Al-Ameen Collegeof Pharmacy, Bangalore, NIMHANS etc.
4.7.9 The Institute has waived off the registrationfees for SC/ST patients besides giving them a 50%rebate on all medical investigations. A separatepharmacy to cater to the needs of the increasingnumber of patients has been established. Theadministrative block has been connected with theLAN and the work on the computerization of thehospital and library is under progress. A FreeVaccination Unit has been started with thecollaboration of the District Medical Authorities,Government of Karnataka and Polio drops areregularly administered to children. The Library hasthe latest books, rare Manuscripts, Journals etc. withXerox, internet and Reading room facilities for boththe staff and students. The Institute has earmarked3 acres of land for the development of a herbalgarden with more than 500 medicinal plants. A playground has also been developed. The DOTS centerunder RNTCP is also functioning in the NIUM. FreeMedical Camps, Guest Lectures, Seminars andeducational tours are conducted regularly. A fewCamps have been organized specifically for SC/ST,OBC and for people below the poverty line.
4.8 Institute for Post GraduateTeaching and Research inAyurveda (IPGTRA), Jamnagar(Gujarat)
4.8.1 The Institute for Post Graduate Teaching andResearch in Ayurveda (IPGTRA) was established bythe Government of India in the year 1956 and wasput under the governance of the Gujarat AyurvedUniversity, Jamnagar in 1965. Since then 51 batches
have been admitted and more than 1300 graduateshave received PG Degree and 110 PhD Degree fromthis Institute. Post Graduates of this Institute aremanaging premier Institutions of Ayurveda in Indiaand abroad like Nepal, Mauritius, Bangladesh andSri Lanka. It is now one of the constituents of theGujarat Ayurved University. It is one of the oldestAyurveda Post Graduate teaching centres in thecountry. The Institute is fully financed by theGovernment through grants-in-aid for itsmaintenance and development.
4.8.2 There are 9 teaching departments in theInstitute with facilities for teaching and research in12 specialties at the Post-Graduate and doctorallevel. There are 5 well equipped laboratories in theInstitute viz. Pathology, Bio-chemistry, Pharmacology,Pharmacognosy, Modern Medicine, andPharmaceutical Chemistry. The Institute is alsoconducting M. Pharma (Ayurved) and M Sc(Ayurvedic Medicinal Plants) courses under the SelfFinancing scheme. During the year 15 students havebeen given admission in M Pharma (Ayurveda)course.
4.8.3 The Institute participated in the NationalHealth Programmes of the Government of India.During the last year, Government of India startedtwo National campaigns i.e. National Campaign inGeriatric Health Care and National Campaign onKshara Sutra. The Institute implemented theseprogrammes and organized various out-reachactivities for these programmes and conductedNidan-Chikitsa camps in the rural areas of Gujarat.During the year, six diagnostic and treatment campswere organized at the remote villages of Jamnagardistrict having predominantly SC, ST & OBCpopulation.
4.8.4 The Institute organized Six ReorientationTraining Programmes (RoTP) for the teachers ofAyurveda i.e. Basic Principles (July 2007),Rasashastra (August 2007), Rogavijnan (November2007), Shalakya (January 2008), Samhita (February2008) and Rasashastra (March 2008). Theseprogrammes were conducted under the Sponsorshipof Department of AYUSH, Government of India. A twodays National workshop on Research Methodology
375
ANNUAL REPORT 2008-09
was also organized on the occasion of 52ndfoundation day of Institute for Post GraduateTeaching and Research in Ayurveda on 20th July
2007.
4.8.5 A Pharmacovigilance workshop Under WHO
bi-annual support scheme was organized by the
Institute during 3rd and 4th December, 2007. The
Institute is sought to be declared as National
Pharmacovigilance Resource Centre for Ayurveda
Siddha & Unani drugs (ASU). A Pharmacovigilance
cell has been established which is the first of its kind
to be set up in any of the Ayurvedic Institutes.
4.8.6 The I.P.G.T. & R.A. organized various
training programs for the foreigners. A three-months
Introductory Course of Ayurveda was conducted
during November 2007 to January 2008. 13 students
from various countries like Spain, Latvia, Brazil,
Canada, France, Germany, Switzerland, and U.S.A.
participated in the training programmes. Gujarat
Ayurved University has MOU with 6 Foreign Institutes
under which clinical and practical training is provided
to students of these Institutes. During the year 2007-
08, students from Fundecion De Salud, Ayurveda
Prema of Argentina belonging to the Latin American
countries like Uruguay, Paraguay, Bolivia, Mexico,
Spain, and Brazil were given 10 days intensive clinical
and practical training. During the year many
foreigners visited the Institute including Dr. (Mrs)
Barzac, ex Health Minister, France and her husband,
Prof. Lebas, a Professor of Community Medicine in
Paris.
4.8.7 The Institute is being re-designated as a
WHO collaborating centre. During the reporting year
06 persons from Myanmar visited the Institute as
WHO follows. Five traditional medicine doctors from
Bhutan have been give a training in Panchakarma
for four months on deputation from Government of
Bhutan.
4.8.8 The institute has a well managed Hospital
with O.P.D. and I.P.D. facilities. During the year
124851 patients were treated as out door patient,
which included 61134women and 7461 children. 1642
patients were admitted to the various wards of the
hospital as I.P.D. patients. During the year nearly
50638 Panchakarma procedures were performed onthe patients out of whom 24276 were women.
4.8.9 During the year 2008-09 in the REs, the Non-plan allocation is Rs.1226.00 Lakhs and the Planallocation is Rs.350.00 Lakhs.
4.9 Rashtriya Ayurveda Vidyapeeth(RAV), New Delhi
4.9.1 The Rashtriya Ayurveda Vidyapeeth (RAV)is an autonomous organization under the Departmentof AYUSH, Ministry of Health & Family Welfare,Government of India and Registered under theSocieties Registration Act, 1860.
4.9.2 The RAV imparts practical training toAyurvedic graduates and post graduates below theage of 45 years through the Guru ShishyaParampara i.e. the traditional method of transfer ofknowledge. The two-year course of Member ofRashtriya Ayurveda Vidyapeeth (MRAV) facilitatesliterary research for the acquisition of knowledge ofthe Ayurvedic Samhitas and commentaries thereonin order to enable the students to become goodteachers, research scholars and experts in texts ofAyurveda. The students, who have completed postgraduation in Ayurveda are admitted for critical studyon Samhitas, related to their P.G. studies. TheShishyas get sufficient time for interaction anddiscussion on the issues taken for study.
4.9.3 In the one-year Certificate Course ofRashtriya Ayurveda Vidyapeeth (CRAV) thecandidates possessing Ayurvedacharya (BAMS) orequivalent degree in 1st attempt with a minimum of55% of marks are trained under eminent Vaidyas insome Ayurvedic clinical practices. Admission to thesecourses is done on the basis of a written test andinterview after advertisement on All India basis.During the year 2007-08, 24 students of one-yearcourse and one student of two-year course qualifiedthe courses and were conferred certificates of theR AV (MRAV & CRAV). During the year 2008-2009,47 students are undergoing the CRAV course under17 Gurus.
4.9.4 The Vidyapeeth organizes Seminars/Workshops every year to disseminate traditional
376
ANNUAL REPORT 2008-09
knowledge and research outcome to practitionersand researchers. The RAV organized a two-dayNational Seminar on 'Ayurvedic management of
Obesity and its disorders' on 25-26 February, 2008
which was attended by about 300 delegates. Twenty
scientific papers were presented and a souvenir
containing 44 selected full papers was also published
and released during the inaugural function.
4.9.5 The Vidyapeeth also conducts interactive
workshops for the discussion of controversial
technical issues between students and teachers so
as to provide clarity for further utilization in the fields
of education, research and patient care. During the
year 2007-2008, the RAV organized two National
Interactive Workshops, one held at Jalandhar on
Cardio-respiratory system (Pranavaha Srotas)
disorders on 12th - 13th October, 2007 and the other
at Tirupati (A.P.) on Disorders of Bones & Joints and
Fractures (Ashthivaha Srotas) and their
Management' from 24th to 26th March, 2008. About
80-90 selected students and teachers of Ayurveda
colleges attended each of the workshops. Besides,
books containing questions and answers on various
issues pertaining to these subjects were also
released and distributed. The books on such subjects
published by this Vidyapeeth are of immense value
for the Ayurvedic Practitioners and teachers as well
as students of Ayurveda.
4.9.6 R AV is coordinating as Nodal Office for the
Central Sector Scheme of ROTP and CME of the
Department of AYUSH. The scheme which was a
Centrally Sponsored Scheme during the 9th & 10th
Plan periods, has been introduced as a separate
scheme in the Central Sector in the 11th Plan, on
the basis of feedback received, with objectives of
updgrading the knowledge of teachers, medical
officers and other personnel of AYUSH system and
providing them the latest advancement and research
outcome in the fields of diagnosis, management,
drugs etc. During 2007-08, a total of 46 ROTPs and
6 CMEs were approved for AYUSH institutions and
an amount of Rs.194.15 lakhs was released. During
2008-09, 131 ROTPs and 126 CMEs have been
approved to be held in 87 AY USH institutions with abudget of Rs.900.40 lakhs.
4.9.7 The budget for 2008-2009 is Rs.96.00 lakhsunder Plan and Rs.24.00 lakhs under Non Plan.
4.10 Morarji Desai National Instituteof Yoga (MDNIY), New Delhi
4.10.1 The Morarji Desai National Institute of Yoga(MDNIY) is an autonomous organization under theMinistry of Health and Family Welfare, Departmentof AYUSH, Government of India. The main objectivesof the MDNIY are:-
i. to act as a Centre of Excellence for Yoga;
ii
ii
i
ii
. to develop, promote and propagate Yoga,and;
i. to provide and promote facilities of training,teaching and research to fulfill the aboveobjectives.
4.10.2 From the current academic year MDNIY hasrenamed 'Diploma in Yoga Studies' (DYS) one yearduration as "Diploma in Yoga Science" (DYSc). Thetotal number of seats has been increased from 75 to95. In addition to this, two seats each for A&N Islandsand North-East States and one seat for foreignstudents have been reserved. These five candidatesare entitled for Rs.8,000/- per month as Fellowship.Diploma in Yoga Therapy (DYT) of two years duration(2nd Batch) is in progress. The 1st batch of DYT isin the Internship.
4.10.3 The Institute is running the following four YogaTherapy and Research Centres in Governments/Tertiary Hospitals in Delhi in order to enable thereferral of patients from the regular departments ofthe Hospitals for specific Yoga Therapy :
i) Vallabhbhai Patel Chest Institute, Universityof Delhi, North Campus, Delhi.
i) Rajan Babu Tuberculosis Hospitals, DhakaColony, Kingsway Camp, Delhi.
i) LRS Institute of Tuberculosis and RespiratoryDiseases, Sri Aurbindo Marg, Mehrauli, NewDelhi.
iv) Institute of Human Behavior and AlliedSciences, Jhilmil Colony, Dilshad Garden,Delhi.
377
ANNUAL REPORT 2008-09
Total number of people benefitted from above Yoga
Therapy and Research Centres from June, 2007 toAugust, 2008 are 4282.
4.10.4 These centres have become extremelypopular and the hospitals have found them to beextremely useful in the treatment of certain conditions.About 4282 number of patients have benefited fromthe above Yoga Therapy and Research Centersduring the reporting period.
4.10.5 The Institute plans to start a Yoga Educationand Therapy Centre at AYUSH Hospital, Port Blair,Andaman & Nicobar Islands and a Yoga Therapy andTraining Centre at DSR District Head QuartersHospital, Nellore, Andhra Pradesh and PreventiveHealth Care Units of Yoga in CGHS Dispensaries ofDelhi. Initially the Institute intends to start such unitsin 10 Dispensaries.
4.10.6 A Traditional Knowledge Digital Library(TKDL) (Yoga) project, in collaboration with CSIR,has started functioning from the Campus of MDNIYsince January, 2008.
4.10.7 The Institute has established Advanced YogaEducation, Therapy and Research Centres in thefollowing leading Medical Institutes of the country:-
i) Advanced Centre for Yoga Therapy andResearch in Mental Health andNeurosciences at National Institute of MentalHealth and Neurosciences (NIMHANS),Bangalore.
ii
ii
) Advanced Centre for Yoga Education,Therapy and Research in Cardio-vascularDiseases and Diabetes Mellitus at JawaharlalInstitute of Post Graduate Medical Educationand Research (JIPMER), Poducherry.
i) Advanced Centre for Yoga Training andResearch at Defence Institute of Physiologyand Allied Sciences (DIPAS), Delhi.
4.10.8 The Institute conducted Yoga TrainingProgrammes and certificate course in Yoga Science inParliament House, Ministry of Health & F.W, SupremeCourt of India in Supreme Court Campus, DefenceResearch and Development Organization (DRDO), for
the Intelligence Bureau Officers, Ministry of Home Affairs,New Delhi. And three months certificate cource in Yoga(CY Sc.) for Air Force Personnel.
4.10.9 The Institute organized "National Yoga Week-2008" from 25-29 February, 2008, a mass awarenessprogramme for health, happiness and harmony forall through Yoga. The Conference "Yoga forPrevention and Management of Chronic DisordersAssociated with Obesity" was organized in technicalcollaboration with WHO, India and DGHS. AnotherSeminar was also organized on "Standardization ofYogic Curriculum and Programmes". The event wasinaugurated by Dr. Anbumani Ramadoss, Hon'bleUnion Minister of Health and Family Welfare, Govt.of India. The Valedictory session was concluded bySmt. Panabaka Lakshmi, Hon'ble Minister of Statefor Health & Family Welfare, Govt. of India on 29thFebruary, 2008. Eminent experts of Yoga, ModernMedicine and other related fields had shared theirexperience and knowledge in this mega event.
4.10.10 The MDNIY convened several ConsultativeCommittee meetings of Yoga Experts in connectionwith the Accreditation of Yoga Courses andProgrammes and finalized six different courses inYoga. Also, the process of establishing a SelfRegulatory Body - Indian Yoga Association by theexperts of leading Yoga Schools of India has beenfinalized under the President ship of Dr. B.K.S.Iyenger, President, Remamani Iyenger Memorial YogaInstitute, Pune. Memorandum of Association andRules and Regulations of the Association have beendrafted. It is being registered shortly under SocietiesRegistration Act XXI of 1860.
4.10.11 The Institute organized National Seminaron "Yogic Management of Cardio-RespiratoryDiseases" in collaboration with Vallabhbhai PatelChest Institute, University of Delhi, North Campus,Delhi from 5th to 6th April, 2008. The Institute alsoconducted Summer Yoga Camp-2008 from 5th May,2008 for two months duration in 47 parks at differentzones of Delhi. These Camps were concluded on5th July, 2008. A total of 1990 participants availed
the benefit out of these camps. Also, the students of
DYS Course have conducted 15 days Yoga Camps
at 59 .different places in Delhi and National Capital
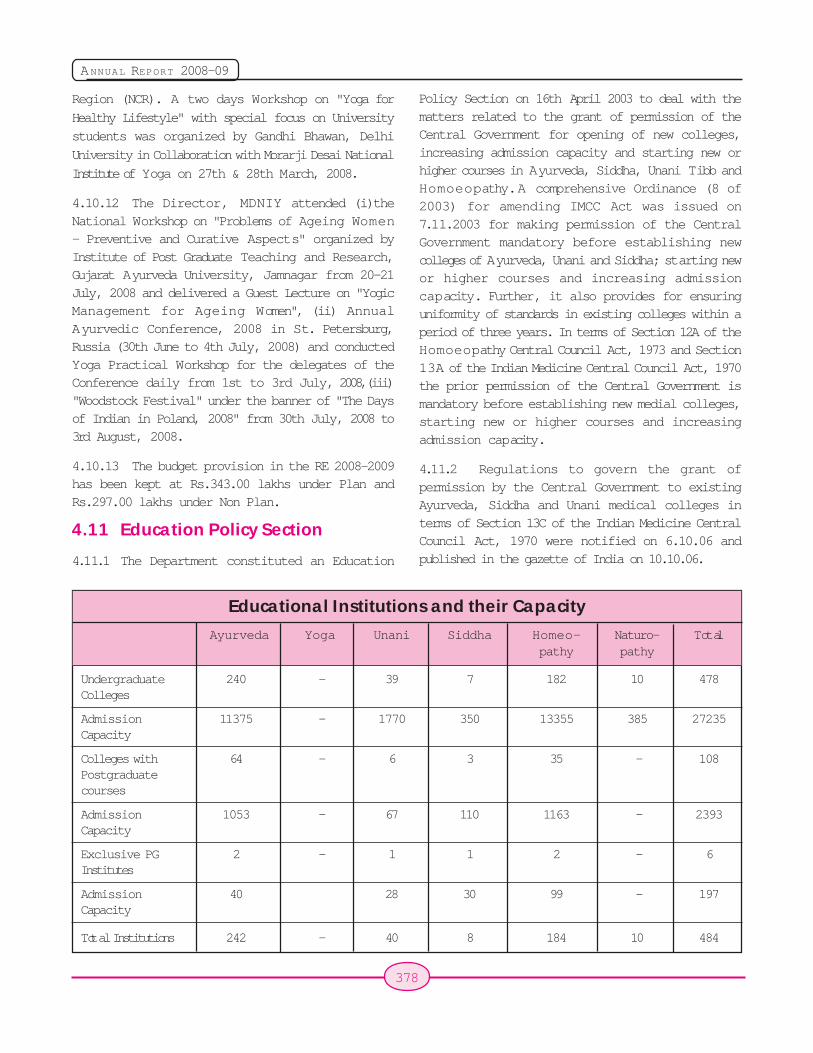
378
ANNUAL REPORT 2008-09
Region (NCR). A two days Workshop on "Yoga for
Healthy Lifestyle" with special focus on University
students was organized by Gandhi Bhawan, Delhi
University in Collaboration with Morarji Desai National
Institute of Yoga on 27th & 28th March, 2008.
4.10.12 The Director, MDNIY attended (i)theNational Workshop on "Problems of Ageing Women- Preventive and Curative Aspects" organized byInstitute of Post Graduate Teaching and Research,Gujarat Ayurveda University, Jamnagar from 20-21July, 2008 and delivered a Guest Lecture on "YogicManagement for Ageing Women", (ii) AnnualAyurvedic Conference, 2008 in St. Petersburg,Russia (30th June to 4th July, 2008) and conductedYoga Practical Workshop for the delegates of theConference daily from 1st to 3rd July, 2008,(iii)"Woodstock Festival" under the banner of "The Daysof Indian in Poland, 2008" from 30th July, 2008 to3rd August, 2008.
4.10.13 The budget provision in the RE 2008-2009has been kept at Rs.343.00 lakhs under Plan andRs.297.00 lakhs under Non Plan.
4.11 Education Policy Section
4.11.1 The Department constituted an Education
Policy Section on 16th April 2003 to deal with thematters related to the grant of permission of theCentral Government for opening of new colleges,increasing admission capacity and starting new orhigher courses in Ayurveda, Siddha, Unani Tibb andHomoeopathy. A comprehensive Ordinance (8 of2003) for amending IMCC Act was issued on7.11.2003 for making permission of the CentralGovernment mandatory before establishing newcolleges of Ayurveda, Unani and Siddha; starting newor higher courses and increasing admissioncapacity. Further, it also provides for ensuringuniformity of standards in existing colleges within aperiod of three years. In terms of Section 12A of theHomoeopathy Central Council Act, 1973 and Section13A of the Indian Medicine Central Council Act, 1970the prior permission of the Central Government ismandatory before establishing new medial colleges,starting new or higher courses and increasingadmission capacity.
4.11.2 Regulations to govern the grant ofpermission by the Central Government to existingAyurveda, Siddha and Unani medical colleges interms of Section 13C of the Indian Medicine CentralCouncil Act, 1970 were notified on 6.10.06 andpublished in the gazette of India on 10.10.06.
Ayurveda Yoga Unani Siddha Homeo- Naturo- Totalpathy pathy
Undergraduate 240 - 39 7 182 10 478Colleges
Admission 11375 - 1770 350 13355 385 27235Capacity
Colleges with 64 - 6 3 35 - 108Postgraduatecourses
Admission 1053 - 67 110 1163 - 2393Capacity
Exclusive PG 2 - 1 1 2 - 6Institutes
Admission 40 28 30 99 - 197Capacity
Total Institutions 242 - 40 8 184 10 484
Educational Institutions and their Capacity
379
ANNUAL REPORT 2008-09
4.11.3 In the light of representations made byState Governments and the colleges about more timebeing needed by the colleges to comply with theprovisons of the IMCC Act and the relevantregulations regarding the provision of infrastructureand staff in exisiting colleges, it was decided that allthe existing medical colleges which had applied wouldbe permitted to go ahead with admissions for the2007-08 academic session subject to the conditionthat at least 80% of the full complement of teachingstaff, as prescribed in the relevant regulations, wouldbe in position before the commencement ofadmissions and further subject to the removal of allthe deficiencies relating to teaching staff,infrastructure, etc. by the end of March, 2008, failingwhich they would not be permitted to admit studentsduring the 2008-09 academic session.
4.11.4 During 2007-08 (as on 27.10.2008), theDepartment had received a total number of 133applications seeking the permission of the CentralGovernment under section 13A of the Indian MedicineCentral Council (IMCC) Act, 1970 and section 12A ofthe Homoeopathy Central Council (HCC) Act, 1973for starting new colleges, opening new or highercourses and increasing the intake capacity inAyurveda, Siddha, Unani and Homoeopathy MedicalColleges. After due inspection and recommendationsof CCIM, the permission of the Central Governmenthas been granted for establishment of 7 newAyurveda Colleges and 3 new HomoeopathicColleges. Permission has also been granted forstarting of Higher Courses (Post-graduation) in 11Ayurvedic Colleges, 2 Unani colleges and 2Homoeopathy Colleges. Permission to increase theadmission capacity in existing courses has beengranted in 6 Ayurvedic Colleges.
4.11.5 A total of 253 applications (Ayurveda-210,Siddha-6 and Unani-37) received from existingAyurveda, Siddha and Unani Medical Colleges forgrant of permission of the Central Government undersection 13C of the IMCC Act, 1970, were forwardedto the CCIM for carrying out an inspection andsending their recommendations. The Departmentunder-took a vigorous exercise to examine therecommendations and inspection reports of the CCIMin respect of all these colleges. The Department has
processed the cases strictly in terms of the provisionsof the IMCC Act and the relevant regulations.Personal hearings in terms of the provisions of theIMCC Act were given in all cases where it was feltthat permission could not be granted on account ofserious deficiencies and shortcomings of staff,infrastructure, etc. Final decisions on whether or notpermission should be given were made on the basisof a careful examination of the application, therecommendations of the CCIM and the oral andwritten submissions made at the hearings.Conditional permission has been accorded for theyear 2008-09 to 105 Ayurveda colleges, 11 Unanicolleges and 3 Siddha colleges subject to rectificationof the shortcomings by December 31, 2008, failingwhich the permission will be withdrawn for the year2009-10.
4.12 Grant-In-Aid Scheme forDevelopment of AYUSHEducational Institutions
4.12.1 The Department is committed to thedevelopment and propagation of Ayurveda, Yoga andNaturopathy, Unani, Siddha and Homoeopathysystems and attaches great importance toimprovement of standards of medical education inthese systems. The AYUSH teaching institutions arerequired to provide the infrastructure and staff asspecified in the the Minimum Standards Regulationsand the Regulations for Undergraduate and Post-Graduate education issued by CCIM amd the CCH.
4.12.2 There are over 458 AYUSH colleges/teaching institutions in the country. The Departmenthas been implementing schemes for assisting theteaching institutions as it was found that a numberof teaching institutions do not meet the requirementsprescribed in the Minimum Standards and otherrelevant Regulations for infrastructure and staff. Inorder to assist the colleges to fill the critical gaps,this Department has formulated the Schemes for theprovision of financial assistance to AYUSH teachinginstitutions. The Scheme of Grant-in-aid forupgradation and Strengthening of AYUSH collegesseeks to supplements their efforts in order to makethe task of upgradation of educational standardseasier.
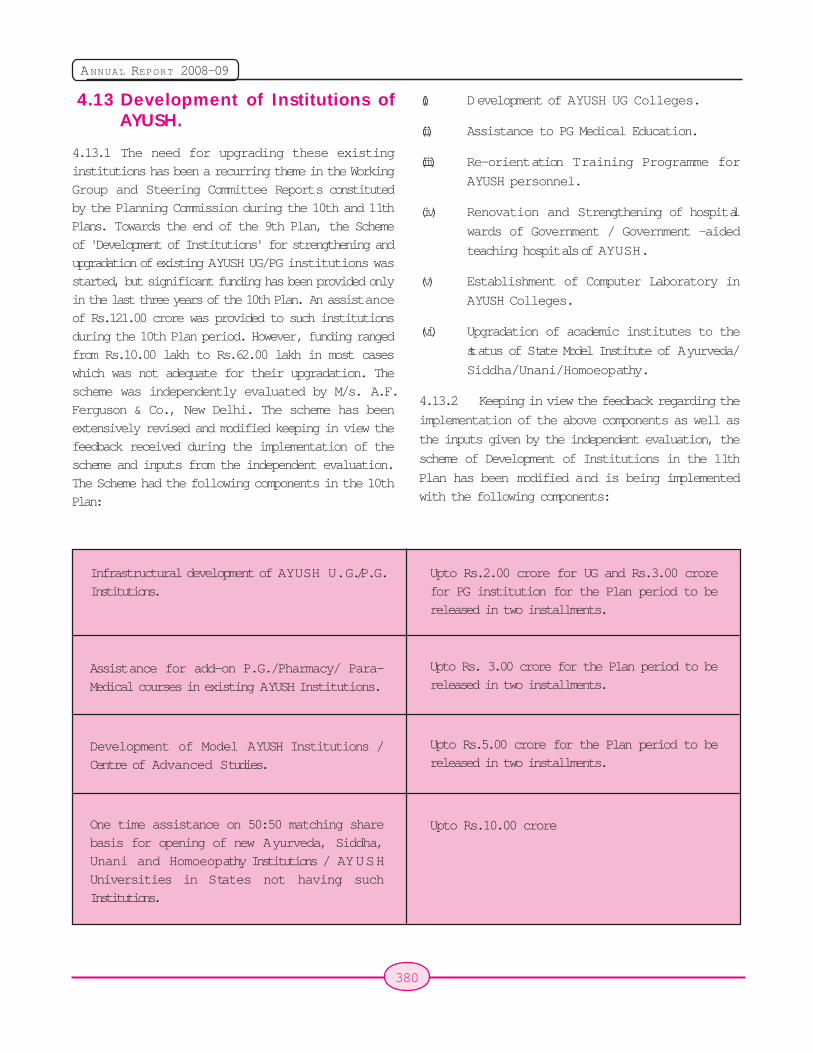
380
ANNUAL REPORT 2008-09
4.13 Development of Institutions ofAYUSH.
4.13.1 The need for upgrading these existinginstitutions has been a recurring theme in the WorkingGroup and Steering Committee Reports constitutedby the Planning Commission during the 10th and 11thPlans. Towards the end of the 9th Plan, the Schemeof 'Development of Institutions' for strengthening andupgradation of existing AYUSH UG/PG institutions wasstarted, but significant funding has been provided onlyin the last three years of the 10th Plan. An assistanceof Rs.121.00 crore was provided to such institutionsduring the 10th Plan period. However, funding rangedfrom Rs.10.00 lakh to Rs.62.00 lakh in most caseswhich was not adequate for their upgradation. Thescheme was independently evaluated by M/s. A.F.Ferguson & Co., New Delhi. The scheme has beenextensively revised and modified keeping in view thefeedback received during the implementation of thescheme and inputs from the independent evaluation.The Scheme had the following components in the 10thPlan:
(i) Development of AYUSH UG Colleges.
(ii
i
) Assistance to PG Medical Education.
(ii) Re-orientation Training Programme for
AYUSH personnel.
(iv) Renovation and Strengthening of hospital
wards of Government / Government -aided
teaching hospitals of AYUSH.
(v) Establishment of Computer Laboratory in
AYUSH Colleges.
(vi) Upgradation of academic institutes to the
status of State Model Institute of Ayurveda/
Siddha/Unani/Homoeopathy.
4.13.2 Keeping in view the feedback regarding the
implementation of the above components as well as
the inputs given by the independent evaluation, the
scheme of Development of Institutions in the 11th
Plan has been modified and is being implemented
with the following components:
Infrastructural development of AYUSH U.G./P.G.Institutions.
Assistance for add-on P.G./Pharmacy/ Para-Medical courses in existing AYUSH Institutions.
Development of Model AYUSH Institutions /Centre of Advanced Studies.
One time assistance on 50:50 matching sharebasis for opening of new Ayurveda, Siddha,Unani and Homoeopathy Institutions / AYUSHUniversities in States not having suchInstitutions.
Upto Rs.2.00 crore for UG and Rs.3.00 crorefor PG institution for the Plan period to bereleased in two installments.
Upto Rs. 3.00 crore for the Plan period to bereleased in two installments.
Upto Rs.5.00 crore for the Plan period to bereleased in two installments.
Upto Rs.10.00 crore
381
ANNUAL REPORT 2008-09
4.13.3 Infrastructural development ofAYUSH U.G/ P.G. Institutions
Under this component Government/Government-aided institutions duly recognized by the CentralGovernment for the last 5 years, having at least 80%of the teachers as per CCIM and CCH norms, andon the basis of a Detailed Project Report forupgradation of the Institutions duly appraised by aCommittee comprising of the Principal of theInstitution, nominee of the affiliating university andthe nominee of the State Directorate of ISM&H, aregiven financial assistance in order to help them toachieve the standards laid down by the CentralCouncil of Indian Medicine (CCIM) or the CentralCouncil of Homoeopathy (CCH) as well as tostrengthen the infrastructure of the colleges. Theassistance is also provided to private but not for profitmaking AYUSH Institutions subject to the conditionsthat the institution should be duly recognized by theCentral Government for at least 8 years, must have80% teachers as per CCIM and CCH norms in positionfor at least 3 years (Income Tax deduction in Form16 is to be provided in respect of the teachers forthe last 3 years), must have 60% bed occupancy inthe IPD and OPD average daily attendance of at least150 patients during the last 3 years, and appraisalof the college specific Detailed Project Report by theScheduled Bank to administer the scheme andsanctioning of loan. 70% of the Grant sanctionedshall be utilized for the construction of OPD/IPD/Teaching Departments/Library/Laboratories/Girls'and Boys' Hostels etc. and remaining 30% of Grantshall be utilized for the purchase of the equipment,furniture, library payment of stipend for PG Institutionetc.
4.14 Assistance for add-on P.G./Pharmacy/Para-Medical coursesin existing AYUSH Institutions.
4.14.1 Considering the shortage of trained P.G.,Ppara-medical and pharmacy personnel in the AYUSHsystems and in line with the need to start P.G. andPharmacy Education as laid down in the NationalPolicy, financial assistance is given to Government/Government aided institutions duly recognized by theCentral Government for the last 5 years, having at
least 80% of the teachers as per CCIM and CCHnorms, and on the basis of a Detailed Project Reportfor upgradation of the Institutions duly appraised bya Committee comprising of the Principal of theInstitution, nominee of the affiliating University andthe nominee of the State Directorate of ISM&H.. Theassistance is also provided to private but not for profitmaking AYUSH Institutions subject to the conditionsthat the institution should be duly recognized by theCentral Government for at least 8 years, must have80% teachers as per CCIM and CCH norms in positionfor at least 3 years (Income Tax deduction in Form16 is to be provided in respect of the teachers forthe last 3 years), must have 60% bed occupancy inthe IPD and OPD average daily attendance of at least150 patients during the last 3 years, and appraisalof the college specific Detailed Project Report by theScheduled Bank to administer the scheme andsanctioning of loan. 50% of the Grant sanctionedshall be utilized for the construction of OPD/IPD/Teaching Departments/Library/Laboratories/Girls'and Boys' Hostels and other requisite structure, andremaining 50% of the Grant shall be utilized on therecurring expenditure on engagement of newteachers as per norms, stipend of PG students/equipment, furniture, library books etc. (Payment ofsalary to teachers and stipend to PG students willbe as per the State norms.)
4.15 Development of Model AYUSHInstitutions/Centre of AdvancedStudies.
4.15.1 This scheme is designed mainly fordevelopment of a centre for advanced studies/training/research in particular specialties. Under thiscomponent of the scheme, assistance is provided tothe Government/Government-aided institutionsidentified by the State Government and/or torenowned AYUSH Experts based on the criteria ofgood infrastructure for Post Graduate Education,Research and Significant contribution in the areasof academic and clinical research, and on the basisof a Detailed Project Report duly appraised by aCommittee comprising Principal of the Institution, arenowned expert nominated by the Department ofAYUSH and nominee of the State Directorate ofISM&H. 60% of the Grant sanctioned shall be utilized
382
ANNUAL REPORT 2008-09
for the construction of OPD/IPD/Pharmacy/AnimalHouse/Herbal Garden/Sepciality Clinics/SeminarRoom/Laboratories, etc. and remaining 40% of Grantshall be utilized for the purchase of the equipment/computerization/furniture/ library books and otherrecurring expenditure on salaries of additional staff/stipend of students, etc.
4.16 One time assistance on 50:50matching share basis for openingof new Ayurveda, Siddha, Unaniand Homoeopathy Institutions/AYUSH Universities in States nothaving such Institutions.
4.16.1 This scheme is admissible only to suchStates which do not have an AYUSH University orAyurveda, Siddha, Unani and Homoeopathyinstitutions in the Government sector. It is completelya project based proposal to be appraised by aCommittee comprising of State Secretary/StateDirector of ISM&H, concerned Advisers fromDepartment of AYUSH and a renowned academicianto be nominated by the Department of AYUSH. NewInstitutes/Universities are also eligible for grant underthis component of the scheme subject to theconditions that one time grant is provided for theestablishment of a new Institution/University in Statenot having AYUSH Institution / AYUSH University,minimum 7.5 acre of land is allotted by StateGovernment and a Detailed Project Report dulyappraised by the nominees of the Department ofAYUSH, State Directorate of AYUSH and tworenowned AYUSH expert nominated by theDepartment of AYUSH.
4.17 Re-orientation TrainingProgramme / ContinuingMedical Education of AYUSHPersonnel
4.17.1 Considering the critical importance ofcontinuous improvement of the skills and knowledgeof AYUSH practitioners and teachers, the Departmenthas been supporting re-orientation training in AYUSHinstitutions since the 8th Five Year Plan. There is anadditional requirement now to train AY U S Hpractitioners adequately about the delivery of the
National Health Programmes on account of theirparticipation in these programmes through the NRHM.Therefore, this Department is implementing anadditional component of Continuing MedicalEducation (CME) scheme for this purpose.
4.17.2 AYUSH Institutions in the Government,
Private or N.G.O.sector are eligible for assistance
under this scheme. Teachers and doctors from
Government or Govt. Aided, private and non-aidedprivate AYUSH institutions are eligible for this training.
However, preference is given to Government colleges
and to Government teachers and doctors.
4.17.3 During the 10th Plan (2002-07) this was
implemented as a component of the Centrally
Sponsored Scheme "Development of AY U S HInstitutions. During 2007-08, Rs. 194.15 lakhs has
been released to 31 institutions for 52 programs.
For the 11th Five Year Plan (2007-2012), this
component has been made a separate Central Sector
Scheme scheme comprising six components -
(i) Orientation training programmes and
Exposure Visits
(ii
i
) Continuing Medical Education (CME)
Programmes and exposure visits for AYUSH
doctors.
(ii) Web-based educational programmes
(iv) Publication of quarterly CME journals /Peer-reviewed Scientific Journals in AYUSH sector.
(v) Re-orientation Training/CME related
innovative tools, programs and activities for
use of AYUSH personnel.
(vi) National and Regional Level Workshops /
Conferences for CME.
4.17.4 During 2008-09, a total of 124 RoTP and129 CME programs in 90 institutions have been
approved for an amount of about Rs.880.00 lakhs.
Until 10th December, 2008, 113 RoTPs and 66 CMEs
have been funded in 67 AYUSH institutions.
4.17.5 The budget provision for grant-n-aid forROTP/CME including Other Charges in the RE 2008-2009 has been kept at Rs.900.00 lakhs under Plan.

383
ANNUAL REPORT 2008-09
4.18 Assistance for ExchangeProgramme / Seminar/Conference / Workshop onAYUSH.
4.18.1 Department of AYUSH is committed todevelop AYUSH systems of medicine with scientificculture. The Department has been implementing ascheme, namely, "Assistance for ExchangeProgramme/ Seminars/ Workshops" with the objectiveto promote and propogate scientific culture in AYUSH;increase involvement of professional/ researchersfor dissemination of the proven results of Researchand Development in the field of AYUSH.
4.18.2 Assistance is provided to institutions/bodiessuch as State Governments, Autonomous Bodies
functioning under the Department of AYUSH, Central/State Government institutions involved in thepromotion of the cause of ISM &H, reputed NGOsand individuals (Indian and Foreign) involved in thedissemination of proven results of AYUSH, promotionand development of AYUSH and having at least 3years experience in the field; and Apex / recognizedassociations of trade and industry working in the fieldof AYUSH.
An amount of Rs. 40.00 lakh was kept in the RE2007-08 under the scheme. An amount of Rs 39.50lakh has been incurred during the financial year 2007-08. An amount of Rs.33.00 lakh has been sanctionedtill 12th September, 2008 for holding Seminar/Conference/Workshop etc. during the financial year2008-09.

384
ANNUAL REPORT 2008-09
385
ANNUAL REPORT 2008-09
Chapter 5
5.1 The four Research Councils, viz. (i) CentralCouncil for Research in Ayurveda and Siddha(CCRAS); (ii) Central Council for Research in UnaniMedicine (CCRUM) (iii) Central Council for Researchin Homoeopathy (CCRH) and (iv) Central Council forResearch in Yoga and Naturopathy (CCRYN),continued to initiate, guide, develop and coordinatescientific research, both fundamental and applied,in different aspects of their respective systems,. TheResearch Councils, which are fully financed by theGovernment of India, are the apex bodies for scientificresearch in the concerned systems of medicine. Theresearch activities of the Research Councils aremonitored and reviewed periodically in order toensure that the research is focused and that it isundertaken in a time bound manner. The outputs ofthe research studies are disseminated amongeducationists, researchers, physicians,manufacturers and the common man..
5.2 Central Council for Research inAyurveda and Siddha (CCRAS)
5.2.1 The Central Council for Research in Ayurvedaand Siddha (CCRAS) is an autonomous body underDepartment of AYUSH, Ministry of Health & FamilyWelfare, Govt. of India, setup for the formulation,coordination, development and promotion of researchon scientific lines in Ayurveda and Siddha. Theactivities are carried out through its 35 peripheralInstitutes/Centres/Units located all over India and alsothrough collaborative studies with various ISMInstitutions/Hospitals and premier modern scienceInstitutes and Hospitals. The Council also financesresearch studies in Ayurveda, Siddha and the alliedsciences. The emphasis is on finding effective andlow cost remedies for various diseases throughsystematic research. Research activities of the Councilinclude Literature Research, Fundamental Research,Drug Research, Clinical Research and Family Welfare
Research. Now the council has also stepped into thefield of Neutraceutical and Cosmeceutical research,Pharmaco Vigilance of Ayurveda and Siddha Drugsand also Documentation of claims on Vector Bornediseases.
5.2.2 Clinical Research
(A) Ayurveda : The research areas identifiedunder previous programme projection are beingcontinued. The Clinical Research studies on 23diseases/conditions have been conducted during thereporting period and 1616 research cases werestudied. The hospitals functioning under the Councilprovided medical aid at OPD level to 4,49,844patients; out of which 1,75,180 were new patientsand 2,74,664 were old patients while 2451 patientswere provided treatment at IPD level. The clinicalresearch on the said diseases are completed andthe results are found encouraging in most of thedisease conditions.
! Drug Development : The pre-clinicalformalities viz. standardization, pre-clinicaltoxicity, biological activity studies etc. werecarried out on the following formulations :-
i) AYUSH Rasayan-A and AYUSH Rasayan-
B as a rasayana
ii
ii
i
) AYUSH QOL for improving quality of life
in cancer patients,
i) AYUSH-RP for Sickle Cell Anaemia,
iv) AYUSH-Osto for Osteoporosis and
fractures,
v) AYUSH-LIV for Hepatitis B & C,
vi) AYUSH-M for Migraine,
vi) AYUSH-SL Capsules
Research and DevelopmentResearch and DevelopmentResearch and DevelopmentResearch and DevelopmentResearch and Development
386
ANNUAL REPORT 2008-09
viii) AYUSH-SL External application for Morbidcases of Filariasis,
ix) AYUSH Manas for Mental retardation,
x) AYUSH QOL-2 for improvement of qualityof life in HIV/AIDS and cancer patients.
! Reverse Pharmacological Studies : onDhatri lauha and Annabhedi Chenduramwhich were initiated at multicentric level in IronDeficiency Anaemia.
! Open Observational Study : OpenObservational study on Clinical Safety ofAyurvedic /Siddha Herbo-mineral and MetallicPreparations was started at four centers ofCCRAS viz. Central research Institutes (CRI)Delhi; CRI, Cheruthuruthy; CRI, ,Kolkatta andCRI(Siddha),Chennai on 9 selected (6Ayurvedic and 3 Siddha) drugs, out of whichstudies on two Ayurvedic drugs and all threesiddha drugs has been completed andstatistical analysis is under process. In caseof the remaining four drugs, Clinical protocoland other preliminary formalities have beencompleted and clinical study is under process.
(B) Siddha: The Clinical Research studiesconducted on 8 disease conditions and 640 researchcases were studied and medical aid was provided to58,861 patients through Out Patient Departments,out of which 14,989 were new patients and 40,872were old patients while 193 were admitted in IPD.
(C) Sowa Rigpa (Amchi) Research : SowaRigpa Research Centre, Leh is engaged in clinicalresearch and development of Sowa-Rigpa and onthe conservation and documentation of medicinalplants and literary research. In clinical research onhypertension, 44 research cases have been studied.1255 patients were treated at OPD level. Out of them,857 were new and 398 were old. The detailedclassification and study of works of Nagarjuna inTibetan Buddhist Canon Stan-Gyur. is being carriedout. Centre has surveyed the Amchi literature andcollected 5 books, viz. Yoga Sataka, Vaidya Jivasutra,Acharya Nagarjuna Bhasitava Bhesajakalp andAryarajanama Vatika and AryamulakosaMahashabdavali.
5.2.3 Tribal Health Care Research-Demographical Research:
Under this programme, a team of research personnelvisits each and every house in selected villages ortribal pockets to collect information on folk medicine,food habits, socio-economic status and the types ofhealth care available The team also provides medicalcare. The programme is modulated to have Tribaldata on health related demograph so that benefitsof the research programme carried out can reach tothe grass root level. During the reporting period 31villages and 24,436 people have been covered.Health care services have been provided to 5,140patients and 13 new Folk claims were collected.
5.2.4 Family Welfare Research & RCHProgramme
The National Population Policy-2000 (NPP-2000)recommends the mainstreaming of ISM & H in theNational RCH Programme. The Council has initiated"Feasibility of Introducing India Systems of Medicine(Ayurveda & Siddha) in the National 'Reproductiveand Child Health' Programme at the Primary HealthCare (PHC) Level in five states". CCRAS and ICMRare collaborating on this project. Standardization andStandard Operative Procedures (SOP) for thepreparation of medicines for 16 RCH Ayurvedic drugshave been completed.
5.2.5 Nutraceuticals Research
The development of Nutraceuticals as a mid day mealsupplement for school going children for improvingmemory and cognitive functions is under progresswith Amul India Ltd, Gujarat.
5.2.6 Medico-Botanical Survey, Cultivation ofMedicinal Plant & Drug StandardisationResearch:
Medico-Botanical Survey Cultivation of MedicinalPlants, Pharamcognostical, and Phytochemicalstudies besides Drug Standardization ResearchProgramme are being carried out at different Institutes.The 12 Medico-Botanical Survey tours were conductrfand 692 specimen and 816 Museum samples and 84folk claims were collected. Under the drugstandardization 31 single drugs and 30 compound
387
ANNUAL REPORT 2008-09
formulations have been standardized. TLC/ HPTLCstudies of 65 single drugs and 17 compoundformulations have also been carried out in addition todetermination of heavy metal and pesticide residuein certain formulations. 8 Active principle / chemicalconstituents have been isolated together with shelflife studies of 4 drugs. A WHO project on "HPTLCfingerprint ATLAS of 50 Ayurvedic Single plant drugsmentioned in API, Vol.- III & IV" has been completed.NABL accreditation for Captain Srinivas Murthy DrudResearch Institute (CSMDRI ), Chennai and GMPCertification for CRI , Patiala, have been obtained.The GMP certification for CRI, Kolkata, CRI,Cheruthurthy and CRI (S) Chennai is in progress.
5.2.7 Pharmacology/Toxicity Research : Underthe Pharmacology / Toxicity ResearchProgramme of the Council, the following havebeen completed.
! Sub-acute toxicity on nine formulations viz.Manasamitra vataka, Cancergajkesari,Mahalaxmivilas rasa with gold, Ayush Manas,Ayush QOL-2, Ayush OSTO, Mahasudarshanchoorna, Gesari pills, Ayush Rasayan A
! Sub acute toxicity of four coded Bhasma i.e.' e,u,v and an'
! Chronic toxicity of one Coded bhasma 'e'
! Chronic toxicity of four Ayush coded drugsviz. Ayush MANAS, Ayush SL, Ayush M,Ayush QOL2
! Biological activity study (Evaluation ofimmunomodulatory and anti oxidant activity)of three coded drugs Ayush Manas, AyushRasayan B, Ayush QOL-2.
5.2.8 Literary Research
The Council is bringing out 3 journals namely JRAS,JDRAS and JIIHM .Translation work of 6 Ayurvedicand 5 Siddha texts / manuscripts have beencompleted. Beside this 13 Ayurvedic & Siddhabooks/manuscripts have been published.
5.2.9 Campaigns/ Workshops /Seminars
The Council successfully organized 2 national levelworkshops one on Ksharasutra and another onGeriatrics at New Delhi and 4 Workshops /Seminarson different Research disciplines at New Delhi andperipheral Institutes of the Council, as part of theNational Campaigns. The CCRAS also participatedin 14 Melas / Arogyas / Exhibitions in different partsof India and abroad.
Smt. Panabaka Lakshmi, Hon'ble Minister of State for Health and Family Welfare, Governmentof India inaugurating the National workshop on Geriatric Healthcare.
388
ANNUAL REPORT 2008-09
5.2.10 Golden Triangle Partnership Project -AYUSH (CCRAS/CCRUM/ CCRH)/CSIR/ ICMR)
The Golden Triangle Partnership is a project involvingDepartment of AYUSH (CCRAS/CCRUM/CCRH),ICMR and CSIR for the development of evidence-based Ayurvedic drugs. Under the GTP Scheme, 23disease conditions have been identified as prioritiesfor research. Sixteen brainstorming sessions for 8disease conditions viz. Mutra vikara, Sleep disorders,Rasayana, Joint disorders, Cardiac disorders, HIV/AIDS, Malaria and Menopausal syndrome have beenconducted to identify suitable formulations and as aresult of this exercise 39 formulations have beenidentified by CCRAS. 20 formulations have beenselected for Urinary Disorders, Sleep disorders,Rasayana, Joint disorders and Cardiac disorders.The work regarding drug development for Malariahas been initiated at CSMDRIA&S, Chennai. ParijataGhana Vati is the identified drug for this. Physico-chemical analysis of 8 Rasayogas (Herbo- mineral /metallic preparations) has been completed andsafety/toxicity studies are in progress. In addition,the AYUSH industry is also involved in the GTP drugdevelopment under Public private PartnershipSchemeA project on HIV-AIDS has been sanctionedto ICMR in collaboration with CCRAS, AIIMS andAYUSH industry. The drug dossier of 5 diseases forDyslipidaemia, Hypertension, Anxiety neurosis,Attention Deficit Hyperactive Disorders (ADHD) andSleep disorders are ready for clinical trials. ICMRhas finalized clinical protocols for Dyslipidaemia,Hypertension, Anxiety neurosis, Attention DeficitHyperactive Disorders (ADHD), HIV/AIDS and takeninitiatives for clinical trials at selected Modern andAyurvedic centers.
5.2.11 Extra Mural Research Scheme
Under this Scheme, during the period from August2007 to July 2008, 124 Projects were received and10 projects were approved for financial support. Sofar, out of 13 ongoing projects, 2 projects viz. "Clinicalevaluation of selected therapies and concepts ofAyurveda" and "Pharmacological and Molecularstudies on cardio protective potential of medicinalplants" have been completed and final reports havebeen accepted. The monographs of both the projects
are under preparation. Final report of another projecton "Double blind randomized clinical trial ofPolyherbal formulation Ashokarishta on postMenopausal status in females" is under evaluation.Action has been initiated for the preparation ofMonographs in respect of completed projects.
5.2.12 Ayurvedic Pharmacopoeial Committee(APC)
The APC is concerned with the development ofpharmacopoeial standards of single and compounddrugs, shelf life studies and the generation of safetyand toxicity data on various groups of medicines.
! Fifty monographs on compound formulationshave been published.
! 51 Fifty one monographs on compoundformulations have been finalized and are inprocess of publication.
! Twenty one monographs on single drugs(Authentic Raw Mineral & Metals) have beenfinalized and are in process of publication.
! One hundred one monographs on Singleplant drugs have been finalized and are inprocess of publication.
! Monographs on Aqua and Hydro-alcoholicExtracts of 15 single plant drugs are in finalstage.
! Among the projects for estimation of HeavyMetals, Microbial Load and PesticideResidues in Single Drugs of Plant Origin,analysis of heavy metals (Pb, Cd, Hg) andArsenic (As) has been completed on 1000samples.
! There are many exotic but domesticatedherbal single drugs from which, APC hasidentified 100 drugs (Namatah AnuktaDravyas) for the preparation of monographsto be published as Extra Pharmacopoeioa ofIndia.
5.3 Central Council for Research inUnani Medicine (CCRUM)
The Central Council for Research in Unani Medicine
389
ANNUAL REPORT 2008-09
(CCRUM) is an autonomous body under theDepartment of AYUSH, Ministry of Health & FamilyWelfare, Govt. of India, setup for the formulation,coordination, development and promotion ofresearch on scientific lines in the Unani system ofMedicine.
5.3.1 The research programme of the CentralCouncil for Research in Unani Medicine (CCRUM)comprises clinical research, drug research, surveyand cultivation of medicinal plants and literaryresearch. The research activities of the Council arebeing carried out through a network of 20 Institutes/Units functioning in different parts of the country.These include :-
! two Central Research Institutes of UnaniMedicine - one each at Hyderabad andLucknow;
! eight Regional Research Institutes of UnaniMedicine - one each at Chennai, Bhadrak,Patna, Aligarh, Mumbai, Srinagar, Kolkata andNew Delhi (with an extension centre at Dr.Ram Manohar Lohia Hospital, New Delhi),
! A Regional Research Centre at Silchar(Assam) (with an extension centre atKarimganj (Assam),
! four Clinical Research Units - one each atAllahabad, Bangalore, Bhopal andBurhanpur;
! A Drug Standardisation Research Institute atGhaziabad;
! A Drug Standardisation Research Unit atNew Delhi;
! A Chemical Research Unit at Aligarh
! A Literary Research Institute in New Delhi withtwo smaller nucleus centres one each at -Meerut and Edathala (Kerela).
During the reporting period, programmes allotted forXI Five Year Plan were continued besidesconsolidating the studies completed during the X FiveYear Plan. The new initiatives during the reporting
period include undertaking clinico pharmacologicalstudies/clinical trials on new formulations in differentdiseases and their reverse pharmacology and safetyevaluation. Besides, work on the development ofSOPs of different Unani regimental therapies alsocontinued. Under the drug research programme,development of SOPs for compound Unaniformulations continued besides publishing the newvolumes of Unani pharmacopoeia of India and aNational Formulary of Unani Medicine The literaryresearch programme was further augmented with newpublications of important classical books.Development of data base of Unani medicinal plantsand tribal folk claims continued with the addition ofnew information collected during ethanobotanicalsurvey of new forest areas. Interaction with thefarmers to promote cultivation of genuine Unanimedicinal plants also continued. Agro techniquesdeveloped for some important plants were transferredto the farmers. Collaborative studies with otherscientific Organizations continued in differentdisciplines. With a view to disseminate the newresearch findings among the scientists, scholars andpractitioners, the Council organized a number ofseminars/workshops. Steps were taken to globalizethe Unani system in the countries including SouthAfrica, Nigeria, Iran, Dubai, U.K. and U.S.A..
5.3.2 Clinical Research:
Under the Clinical Research Programme, therapeutictrials of Unani drugs on 21 diseases continued atthe Council's centres. The diseases on which trialscontinued were : Bars (Vitiligo), Nar-e-Farsi(Eczema), Daus Sadaf (Psoriasis), Iltehab-e-Tajaweef-e-Anf (Sinusitis), Iltehab-e-Kabid (InfectiveHepatitis), Waja-ul-Mafasil (Rheumatoid arthritis),Zeequn Nafas (Bronchial Asthma), Iltehab-e-Shobate Muzmin (Chronic Bronchitis) , ZiabetusSukkari (Diabetes Mellitus), Kasrat-e-Shahmuddam(Hyperlipidemia), Muzmin Zubeh-e-SadariyaSabit, (Chronic stable angina), Zaghtuddam Qawi(Essential Hypertension), Saman-e-Mufrit (Obesity),Qarah-e-Meda wa Asna-e-Ashari (Duodenal Ulcer),Zaheer-e-Muzmin (Bacillary dysentery), Humma-e-Ijamia (Malaria), Daul Feel (Filariasis), KalaAzar (Lishminiasis) and Takhalkhul-e-Azam

390
ANNUAL REPORT 2008-09
(Osteoporosis). Besides, preclinical studies onSartan (Cancer) and HIV also initiated. During the
reporting period, 6830 research patients were
registered in various diseases at different centres of
the Council. Clinical trials completed on the diseasesincluding Iltehab-e-Kabid (Infective hepatitis), Iltehab-
e-Tajaweef-e-Anf (Sinusitis), Zeequn Nafas
(Bronchial Asthma) and Waja-ul-Mafasil (Rheumatoid
arthritis) during the X Five Year Plan were
consolidated and compiled for publication.
Collaborative clinical studies with other scientific
organizations/institutions including Obesity andPsoriasis at AIIMS, New Delhi, Bronchial Asthma at
Patel Chest Institute, New Delhi, in Infective hepatitis
at Lady Harding Medical College, New Delhi and in
Duodenal ulcer and viral hepatitis at Deccan Medical
College, Hyderabad are in progress.
5.3.3 Fundamental Research:
New studies on physiological aspects of differenthumours and temperaments continued to validate
the concept scientifically. Study on the susceptibility
of acquiring different disease in relation to the
temperament of the patients also consolidated.
5.3.4 Unani Regimental Therapy Experimen-
tation:
Twelve regimental therapies of Unani Medicine were
documented in order to develop Standard Operating
Procedures (SOPs ) for these therapies and for their
scientific validation.
5.3.5 Research Oriented General O.P.D.
Programme :
Research oriented General OPD programmecontinued at 17 centres of the Council. The aim of
this programme is to get research feedback from the
cases attending the General OPD for common
ailments and also to provide treatment for common/
seasonal ailments through Unani medicines. During
the reporting period, 98160 cases were registeredat different centres of the Council.
5.3.6 Mobile Clinical Research Programme:
Research oriented mobile medicare programme
continued in 10 adopted urban slums/rural pocketscovering a total population of two lakhs including80,000 SC population and 20,000 ST population.During the reporting period 13,180 patients weretreated for different diseases through mobile OPDsat different centres of the Council. These patientswere treated with Unani kit medicines developed bythe Council. Health awareness meets were organizedat regular intervals to educate the population undercoverage on preventive and promotive healthaspects. Health check-up of 3,150 school childrenwas done in the adopted schools.
5.3.7 Activities under Special Component Planfor Scheduled Castes :
The Council has adopted six rural pocketspredominately inhabited by Scheduled Castespopulation in Allahabad for a period of three years.A baseline health survey was conducted andmorbidity data collected. During the reporting periodintervention phase continued in these pockets. Inputwas given in the form of health education and healthcare. Besides, pockets specific to SC populationwas also covered at other centres of the Council.Treatment was provided to the population undercoverage through mobile OPDs at their doorsteps.During the reporting period 4,216 patients, most ofwhom belonged to under privilege section of thesociety, were treated.
5.3.8 Activities Under Tribal Sub Plan :
Under Tribal sub-plan, health promotion activities forScheduled Tribes continued at different centres ofthe Council. The mobile OPDs continued treatmentfacilities for Scheduled Tribes nearer to theirdoorsteps at Burhanpur (M.P) and Bhadrak (Orissa).During the reporting period, 3,215 patients belongingto Scheduled Tribes were treated. Research casesof diseases including Humma-e-Ijamia (Malaria),Daul Feel (Filariasis), Nar-e-Farsi (Eczema) andZusantaria Mevi (Amoebic Dysentery) & Iltehab-e-Kabid (Infective hepatitis) were registered in the tribalpopulation.
5.3.9 Activities under Gender Component Plan :
Research studies on diseases specific to women

391
ANNUAL REPORT 2008-09
continued at different centres of the Council.Validation trials of Unani drugs that were developedby the Council in Sailan-ur-Raham (Leucorrhoea)and Awariz-e-Tams (Menstrual disorders) continuedat different centres of the Council. New researchstudies on Osteoporosis were initiated. During thereporting period 39,264 female patients wereregistered in the General OPD programme atdifferent centres of the Council.
5.3.10 Activities in North Eastern States :
The Council's Clinical Research Unit at Silchar wasupgraded to Regional Research Centre with anExtension Centre at Karimganj (Assam). This is theonly centre of Unani Medicine in the region. Thiscentre continued research and healthcare servicesin Silchar and Karimganj. Research studiescontinued on Humma-e-Ijamia (Malaria), Ishal(Diarrhoea) and Zusantaria Mevi (AmoebicDysentery) at these centres. Besides General OPDfor common ailments also continued. During thereporting period 6,250 patients were registered andtreated at these centres.
5.3.11 Drug Standardisation Research:
Under the Drug Standardisation ResearchProgramme developing pharmacopeal standards on100 drugs continued. Standard OperatingProcedures on nine drugs completed and on the restof the drugs are in progress. Besides, 50monographs each for Unani Pharmacopea-Part-I,Vol. VI and Unani Pharmacopea - Part II, Vol. I alsofinalized. The National Formulary for UnaniMedicine, Vol. VI containing 178 drugs was alsopublished during the reporting period .
5.3.12 Literary Research:
Under the Literary Research Programme, editing/translation/reprinting of out of print classical bookscontinued. Urdu translation of the books publishedduring the reporting period included Kitab-al-Hawi,Vol. XV and XVII, Kitab-ul-Fakhir. Translation workalso continued on Akseer-e-Azam, Vol. II, Moheet-e-Azam, Vol. I, Tazkira oolilalbab, Minhaj udd-Dukkancontinued. Reprint of Biaz-e-Kabir and Tazkiraoolilalbab was also brought out.
5.3.13 Survey and Cultivation of MedicinalPlants Programme:
Under the Survey and Cultivation of Medicinal PlantsProgramme, ethno-botanical explorations of Atmakurand Srisalem forest division in Andhra Pradesh wasconducted. Experimental cultivation work on somemedicinal plants such as Asgandh (Withaniasomnifera Dunal), Brahmi (Centella asiatica L.(Urban.), Ushba-e-Hindi (Hemidesmus indicus L.(R.Br.), Jadwar (Delphinium denudatum Wall), Kutki(Picrohiza kurroa Royle ex Benth.) Kalonji, (Nigellasativa) Arusa (Adhatoda vasica Nees.) andGurmarbuti (Gymmema sylvester R. Br.) to observegrowth and domestication also continued.
Large scale cultivation of Atrilal (Ammi-majus Linn.)and Gulnar Farsi (Punica granatum Linn.) (Abortivevariety), and Sambhalu (Vitex negundo L.), was alsoundertaken in the herb gardens of the Council atAligarh and Chennai. New plant species were addedin the nurseries of Unani medicinal plants developedat Regional Research Institutes of Unani Medicine,Aligarh (Uttar Pradesh), Srinagar (J&K), Chennai(Tamil Nadu) and Central Research Institute of UnaniMedicine, Hyderabad (Andhra Pradesh). Eightresearch papers were published in different scientificjournals. The Council also published a book entitledUnani medicinal plants of "Tarai Forests in KumaonRegion of Uttarakhand, India". Farmer meets wereorganized in the Ranga Reddy district of AndhraPradesh to create awareness among the farmers forprospectus of taking up the cultivation of Unanimedicinal plants. Agro techniques developed forcultivation of different Unani medicinal plants weretransferred.
5.3.14 Unani Treatment Centre and SpecialityClinic at Dr. Ram Manohar Lohia Hospital, NewDelhi.
The Council has been running a Unani OPD-cum-speciality clinic at Dr. Ram Manohar Lohia Hospital,New Delhi since January 1998. This centre isproviding speciality treatment for common andchronic ailments through Unani Medicine. Duringthe period, a total of 18,120 new patients wereregistered in the General OPD and speciality clinicat this centre.
392
ANNUAL REPORT 2008-09
5.3.15 Participation in Pulse Polio Programmes:
All the clinical centres of the Council continued toparticipate in the Pulse Polio Programme during thereporting period.
5.3.16 Collaborations:
CCRUM has taken an initiative to develop CCRUM -NRDC, IPR collaborating centre for Unani productswith the objectives of Information and knowledge ofpatents, status of patents of Unani products in Indiaand other countries, patent search, interpretation andsearch based intellectuals property relatedtechnology, Prior Art Scenario, Invention mining,Patentability opinion, Infringement and analysisopinion, Freedom to operate opinion, Providingtraining and short term courses in IPR, IPR supportsystem, Store house for supplying IPR relatedinformation on Unani Products. CCRUM is lookingforward to invest initially in various aspects of IPRrelated to Unani products to be developed by industryand research institutes to be commercially exploitedby Unani drug industry.
5.3.17 Organisation of Seminars/Conferences
The Council organized three workshops one onbiomedical ethics at Aligarh, the other on ManagingStress and Effective Interpersonal Relations, NewDelhi and the third on patenting of drugs and IPRissues at Srinagar. These workshops were attendedby the researchers of the Council, research scholarsof PG Departments and faculty members of PGinstitutes of the Universities. Besides, researchersof the Council also attended a number ofinternational/national seminars. In these seminarsa total of 70 research papers were presented indifferent disciplines during the reporting period.
5.3.18 Short-term Research Enquiries :
The Council awarded short-term research enquiriesin the areas of clinical research, pharmacology,chemistry, bio-chemistry and toxicity to reputedInstitutes/universities. During the reporting period10 such projects were continued.
5.3.19 Extramural Research Projects ofDepartment of AYUSH :
The Council co-ordinated in awarding the extramural
research projects of Department of AYUSH relatedto Unani Medicine to different scientific organizations,universities and hospitals. During the reporting periodresearch work continued on 18 ongoing projects.
5.3.20 Unani Pharmacopoeia of India:
The Council served as the secretariat for work relatedto compilation and publication of the UnaniPharmacopoeia of India. Work continued on Unanipharmacopea-Part-I, Vol. VI and Part-II, Vol. I TheNational Formulary of Unani Medicine, Volume-VI waspublished during the reporting period.
5.3.21 Digitization of Unani Manuscripts:
The Council initiated a project to identify anddigitalized classical Unani manuscripts available indifferent libraries globally. Survey to identify suchmanuscripts in different libraries in India has beeninitiated with a view to develop a data base of thesemanuscripts. Eight manuscripts including Al-Kafi fitTib (Arabic), Kitabul Aghzia (Arabic), Kitab fi hifzesehat wa izlat-e-Marz (Arabic), Jame-ul-Shifa (Arabic),Ainul Hyat (Arabic), Jame-ul Jawami (Persian), Shifa-ul-Amraz (Persian) and Dastoor-ul-Hunood (Persian)have been selected for digitilization.
5.3.22 Traditional Knowledge Digital Library(TKDL):
The Council continued co-ordination in the workrelated to development of Traditional KnowledgeDigital Library (TKDL) of Unani Medicine with theCSIR. So far 1,12,756 formulations were identified.Out of these 1,08,740 formulations were transcribed.1,01,206 formulations were scanned. Editing of95,511 was completed by the Unani experts. Out ofthese 82,900 formulations were peer reviewed bythe eminent Unani experts. 38,754 formulations werefinalized.
5.3.23 Medical Relief Camps:
The Council organized medical relief camps duringfloods at Balasore, Orissa and Saharsa, Madherpura,Katihar, Ararya, Purniya and Supol in Bihar. Seventeams - one at Balasore and six in Bihar were deputedin affected areas. Free Unani treatment was providedto the affected people for treatment of various
393
ANNUAL REPORT 2008-09
diseases. Over 10,000 patients were treated in thesecamps.
5.3.24 Publications:
During the reporting period, the Council brought outabout 17 publications. These include; monographs,journals and IEC material. Some of the IEC materialwere also translated into Thai language andpublished.
5.3.25 Establishment of Bio-informatic Centre :
Bioinformatics is the application of computertechnology in the management of biologicalinformation. Computers are used to gather, store,analyze and integrate biological and geneticinformation which can then be applied to gene-baseddrug discovery and development. The need forBioinformatics capabilities has been precipitated bythe explosion of publicly available genomic informationresulting from the Human Genome Project. The goalof this project - determination of the sequence of theentire human genome. The science of Bioinformatics,which is the melding of molecular biology withcomputer science, is essential to the use of genomicinformation in understanding human diseases andin the identification of new molecular targets for drugdiscovery. In recognition of this, the Council haveinitiated efforts to setup bioinformatics groupsconsisting of computational biologists andbioinformatics computer scientists and Unani expertsto collaborate in this work. Such groups will be keyto unraveling the mass of information generated bylarge scale sequencing efforts underway inlaboratories around the world.
5.3.26 Budget:
During the current financial year, a budgetaryallocation of Rs. 1,800 Lakhs under Plan schemesand Rs.1,300 lakhs under Non-Plan schemes hasbeen made for the Council.
5.4 Central Council for Research inHomoeopathy (CCRH)
5.4.1 The Central Council for Research inHomoeopathy (CCRH) is an autonomous organization
of Department of AYUSH, Ministry of Health andFamily Welfare, Government of India. Establishedon 30th March 1978, it is a premier organization,fully financed by the Government of India, conductingresearch on various aspects of Homoeopathy. TheCouncil functions through its 24 Institutes/ Unitsspread all over the country with its headquarters atDelhi. The main aim of the Council is to coordinate,develop and promote research in Homoeopathy.
5.4.2 Clinical Research
Clinical Research is necessary to validate the efficacyof the therapies in specific diseases. Good qualityClinical Research studies, based on scientificprotocols, can establish homoeopathic research atpar with the research in Allopathy. Considering theimportance of Clinical Research in the developmentof the science, Council is paying prime attention on17 Clinical studies viz. HIV/AIDS (Disease related),HIV/AIDS (Drug related), Benign ProstaticHyperplasia, Gastroenteritis, Furunculosis,Urolithiasis, Vitiligo, Diabetic Distal SymmetricPolyneuropathy, Diabetic Foot Ulcer, AcuteDiarrhoeal Diseases in Children, DepressiveEpisode, Schizophrenia, Acute Tracheobronchitis,Chronic Sinusitis, Acute Rhinitis in Children, Distressduring Climacteric years and Chronic Bronchitis. Newprotocol for pilot study on Leptospirosis was alsoprepared and approved by the Ethical Committee,the Special Committee on Clinical Research and theScientific Advisory Committee of the Council. Thestudy on Acute Rhinitis in Children has beenconcluded in June 2008.
5.4.3 Clinical Verification
Clinical Verification involves verifying the drugproving data clinically to determine reliableindications of the drugs, on which therapeuticprescriptions can be based. The Council isconducting Clinical Verification of 35 drugs provedby the Council on improved protocol. Acomprehensive Materia Medica of these 35 drugshas been prepared, collating the drug provingsymptoms along with the symptoms alreadyavailable in the literature. A total of 478 cases wereenrolled under the Clinical Verification Programme.
394
ANNUAL REPORT 2008-09
5.4.4 Drug Proving
Drug Proving (Homoeopathic Pathogenetic Trial orHPT) forms the basis of Homoeopathy and has,therefore, been a focused activity of the Council. Thedouble blind placebo controlled methodology hasbeen adopted in the Drug Proving Programmethrough an improved protocol. The Council hasinvolved some of the homoeopathic medical collegesin the Drug Proving programme, where the Council'sresearch centers are located. During the period,proving of 06 coded drugs is in progress.
5.4.5 Drug Standardization
Drug Standardization is a multidisciplinary approachencompassing pharmacognostic, pharmacologicaland physico-chemical studies, so as to establish thequalitative and quantitative characteristics of thedrugs used in Homoeopathy. The Council isconducting Drug Standardization studies on animproved protocol as to evaluate the safety andefficacy of the drugs. Pharmacognostic studies of04 drugs and physico-chemical studies of 03 drugshave been undertaken. Standardization data of03drugs was compiled for HomoeopathicPharmacopoeia Committee.
5.4.6 Survey, Collection and Cultivation ofMedicinal Plants
The Survey, Collection and Cultivation of MedicinalPlants Unit of the Council located at Emerald Post,Udhagamandalam, Nilgiri Distt., Tamil Nadu, maintainsa herbal research garden, where medicinal plantsused in Homoeopathy are cultivated and maintained.The Unit also supplies raw drug material to the DrugStandardization Units of the Council. During thereporting period, the Unit supplied raw drug plantmaterial to the Central Research Institute, Noida, DrugStandardization Unit, Hyderabad for drugstandardization studies and to M/s. Kerala StateHomoeopathic Co-operative Pharmacy Ltd. for theirown use.
5.4.7 Collaborative Studies
Council has taken collaborative research studies withrenowned Institutions having adequate expertise and
information, like: School of Tropical Medicine,Kolkata, Jawaharlal Institute of Post-graduate MedicalEducation and Research, Puducherry, OsmaniaUniversity, Hyderabad, Central Institute of Medicinaland Aromatic Plants, Lucknow, Jamia Hamdard,Delhi, Central Institute of Psychiatry, Ranchi, IndianInstitute of Technology, New Delhi, Bose Institute,Kolkata, Society for Promotion of Youth and Masses,New Delhi, Indian Veterinary Research Institute, IzatNagar (U.P.), High Security Animal DiseasesLaboratory, Bhopal, Homoeopathic ResearchFoundation, Lucknow and with Scientists of BhabhaAtomic Research Centre, Trombay & DefenceInstitute of Physiology and Allied Sciences, New Delhi.In total, 02 collaborative research studies have beencompleted and 14 studies are going on.
5.4.8 Homoeopathy Research in North EasternStates
The Council has five Clinical Research Units in theNorth Eastern Region, i.e. Agartala (Tripura),Guwahati (Assam), Imphal (Manipur), Shillong(Meghalaya) and Gangtok (Sikkim). These Units areconducting evidence based Clinical Research Studieson HIV/AIDS, Acute Rhinitis in Children, Urolithiasis,Benign Prostate Hyperplasia, AcuteTracheobronchitis, Furunculosis, Chronic Bronchitis,Gastroenteritis, Diabetic Distal Symmetry, Poly-Neuropathy, Malaria, besides providing medicalfacilities to the patients. The study of Acute Rhinitisin Children has been concluded in June 2008.
5.4.9 Publications
During this period, one booklet on HIV/AIDS titled'Red Ribbon wants to speak to you' and a book i.e.'Clinical Research Series' (Volume 1), 'Indian Journalof Research in Homoeopathy' (Volume 2, Number 2)and CCRH News No.- 46 were published.
5.4.10 Monitoring and Review of ResearchStudies
To maintain quality of the research studies,monitoring and review has been done, time to time,at the headquarters and at the Unit levels. Internaland external review of the ongoing research studiesat various Institutes/Units of the Council was
395
ANNUAL REPORT 2008-09
conducted from June to September 2008 by various
Committees consisting of experts from Modern
Medicine & Homoeopathy. The Committees have
recommended how to improve the implementationof the research studies and ensure quality output.
The experts suggested to conclude the study of Acute
Rhinitis in Children by June 2008 where the targets
were achieved and other acute diseases (Acute
Diarrhoea, Gastroenteritis, Furunculosis and Acute
Tracheobronchitis) by September 2008, which wereapproved by the Scientific Advisory Committee also.
5.4.11 International Recognition
After the outbreak of Avian Influenza in some countries
including India in 2005, the human transmission of
H5N1 was feared. To meet such menace through
Homoeopathy, the reputed Homoeopathic
associations and experts met at Paris in November2005 to draw strategies and action plans. The
International Federation of Classical Homoeopathy
(IFCH), European Committee of Homoeopathy (ECH),
Royal London Homoeopathic Hospital (RLHH), and
the American Institute of Homoeopathy (AIH) formed
an International Forum International ScientificCommittee on Homoeopathy and Influenza (ISCHI).
This forum also included Central Council for Research
in Homoeopathy. The mandate of this international
body is to promote research studies on prevention
and treatment of Influenza through Homoeopathy. The
Committee consists of 13 members from UK, USA,France, India, Brazil, Belgium and Israel with Dr. Peter
Fisher, internationally reputed homeopathic physician
from London as its chairman. Director CCRH is the
representative from India. The members discuss on
the research proposals through teleconferences and
meetings.
5.4.12 Extra Mural Research Scheme
CCRH is co-ordinating various research projects
under Extra Mural-Research Scheme of the
Department of AYUSH. A meeting of the Project
Evaluation Committee (PEC) of the Extra-Mural
Research Scheme for projects related to
Homoeopathy was held at CCRH headquarters on28th April 2008 which met on 21st August 2008 and
recommended the following new projects for grant-
in-aid: subject to approval of the ScreeningCommittee of the Department of AYUSH:
1. 'A study of unipolar mood (depressive)disorders in Hyderabad urban populationwith a Homoeopathic approach'at AndhraPradesh Homoeopathic Association,Hyderabad.
2. 'Exploration of natural products, aspotentized Homoeopathic drugs and non-potentized botanical extracts, an alternativeto synthetic fungicides against thedestructive diseases of Rice and Rice basedcrop groundnut' at Central Research RiceInstitute, Cuttack.
3. 'Modulation of Cytokine profiles byHomoeopathic Drugs in Rheumatoid Arthritis :An In-vitro study' at JIPMER, Puducherry.
Studies completed during the period:
! Study of Heart and Nerve Conduction causedby Homoeopathic Potentized Drugs vis-à-visAllopathic Drugs on Experimental Animals atIndian Institute of Technology, Kharagpur
! Clinical Study of effects of HomoeopathicConstitutional & Organopathic medicines inpatients suffering from Benign Hypertrophyof Prostate at Dr. A. C. HomoeopathicMedical College & Hospital, Bhubaneswar.
! Evaluation of anti-proliferative, apoptotic andimmunomodulatory activity of some IndianSystem and homoeopathic anticancer drugsat All India Institute of Medical Sciences(AIIMS), New Delhi
5.4.13 Major Events:
The Council organized the following major eventsduring the reporting period.
(a) Training-cum-Workshop on 'Establishment /Administration and Accounts' at CCRHHeadquarters from 5th -7th May 2008, and
(b) Workshop on 'Development of Hindi in North-East India' at Shillong on 28th May 2008

396
ANNUAL REPORT 2008-09
Shri V.S. Achuthanandan, Hon. Chief Minister of Kerala, inaugurating the state level campaign onHomoeopathy for Mother and Child care
5.4.14 Gender Issues
Council has been sensitive to the gender issues andattempted to give due importance to diseases ofwomen in its research programmes, particularly inthe clinical research. Currently, one clinical researchstudy on Distress during Climacteric Years is inprogress at five Institutes/Units of the Council atShimla, Ranchi, Puducherry, Chennai andHyderabad. Scientific Advisory Committee of theCouncil has approved two more research projectsrelated to diseases of women viz. 'Uterine Fibroid'and 'Dysmenorrhoea' to be undertaken at the Units/ Institutes of the Council in future.
A Gender Budget Cell has been constituted at theheadquarters of the Council. This Cell continues tocompile the data of the female patients gettingbenefit of the treatment for various diseases at theperipheral Institutes/ Units of the Council under clinicalresearch, clinical verification programme and general
OPD. The members of the Gender Budget cell havealso proposed to start a pilot study on Iron deficiencyanaemia during pregnancy.
5.4.15 Budget
During the current financial year (2008-09), abudgetary allocation of Rs. 1343.00 lakhs under PlanSchemes and Rs 750.00 lakhs under Non-PlanSchemes has been made for the Council.
5.5 Central Council for Research inYoga & Naturopathy (CCRYN)
5.5.1 Central Council for Research in Yoga andNaturopathy (CCRYN) is a society registered underthe Societies Registration Act XXI of 1860 on30.3.1978 and is functioning as an autonomous bodyunder the Deptt. of AYUSH, Ministry of Health & FamilyWelfare. The basic objective of the Council is toconduct Scientific Research in the field of Yoga andNaturopathy, Education, Training and Propagational
397
ANNUAL REPORT 2008-09
aspects of these disciplines. At present, the Councilis looking after the overall development of these
traditional systems. The Council is executing its
various activities/ programmes by providing grants-
in-aid to various Naturopathy & Yoga Institutions.
5.5.2. The Council provides financial assistance to
premier research organizations and functional Yoga
& Naturopathy Hospitals for the following Schemes:-
a) Clinical Research Scheme;
b) Treatment-Cum-Propagation Centre Scheme
(20 Beds Hospital);
c) Patient Care Centre Scheme (10 Beds
Hospital);
d) Literary Research/ Translation/ Publication
Work
e) Seminar/ Workshop/ Conference
The other activities of the Council are as given below:
1. Running fulltime OPD of Yoga & Naturopathy
6 days a week at:
a) Safdarjung Hospital, New Delhi
b) Lady Hardinge Medical College, New
Delhi
c) Specialized OPD for Cardiac patients at
Dr. R.M.L. Hospital, New Delhi
d) University College of Medical Sciences,
Dilshad Garden, Delhi
e) The Council's Headquarters, Janak Puri,
New Delhi
2. Publication of a quarterly bulletin 'Yogic
Prakritik Jeevan Sandesh' and other books
on Yoga & Naturopathy.
3. Conducting 5 Yoga Classes for the local
public at Headquarters Office 6 days a week.
4. Participating in Arogya melas - all over India.Live Yoga demonstration, Health Counselingand Natural Health Food Corner.
5. Running Yoga fitness classes at UdyogBhavan, New Delhi for Government.employees.
6. Running Yoga Classes at 'Integral HealthClinic', Deptt. of Physiology, AIIMS, New Delhi.
5.5.3 The Council is also running followingthree schemes:
A. Yearly National Award to eminent Yoga &Naturopathy Expert as under:-
(i) Maharishi Patanjali Award Rs.25,000/-(for Yoga expert)
(ii) Mahatma Gandhi Award(for Naturopathy expert) Rs.25,000/-
B. Young Scientist Award Rs.10,000/-
C. Awarding Fellowship to Rs. 6,000/- p.m.Ph.D. students (maximum5 students per year) (forthree years)
5.5.4. The Council has been undertaking researchon various aspects of Yoga & Naturopathy by givinggrants-in-aid to various institutions. Presently 9clinical research projects are going on. LeadingMedical as well as Yoga institutions like All IndiaInstitute of Medical Sciences (AIIMS), New Delhi,National Institute of Mental Health & Neruro-Sciences(NIMHANS), Bangalore, Dr. RML Hospital, New Delhi,King George Medical University, Lucknow andVivekananda Yoga Anusandhan Sansthan,Bangalore etc. are conducting Clinical Research inthe field of Yoga with the financial support of theCouncil.
5.5.5. The findings of the completed researchproject revealed that in a number of diseases suchas Amoebiasis, Anxiety Neurosis/Depression,Arthritis, Allergic Skin Diseases, Bronchial Asthma,Constipation, Cervical Spondylosis, Diabetes,Gastritis, Hemiplegia, Hypertension, Irritable BowelSyndrome, Obesity, Peptic Ulcer, Respiratory TractInfections etc. the systems of Yoga & Naturopathycan play a good role in their management. Theproject, "Effect of an integrated approach of Yoga
398
ANNUAL REPORT 2008-09
Therapy for metastatic breast cancer patients andstudy of DNA repair mechanisms relevant to cancer"was completed at Vivekananda Yoga ResearchFoundation, Bangalore. The study threw startlingresults. A significant decrease in anxiety, depression,perceived stress, improvement in role function,emotional function, cognitive function, social functionand overall quality of life was observed in subjects.There was also a significant reduction in symptomssuch as pain, fatigue, nausea and vomiting,dyspnoea, insomnia, diarrhea and loss of appetitein yoga group as compared to control group. ASignificant Decrease in physical distress,psychological distress, total distress and activitiesof daily living in yoga group as compared to controlswas also observed. There was a decrease insymptom distress, sleep disturbance, frequency andseverity of fatigue and fatigue interference in yogagroup as compared to control group. A SignificantDecrease in absolute lymphocyte counts only in Yogagroup following intervention was also noticed. Theother projects of All India Institute of MedicalSciences, NIMHANS, etc. are showing significantresults in their respective subjects of study.
5.5.6 The Council has also published following fourresearch monographs based on the researchfindings of research projects with a view todisseminate the findings among practitioners &general public.
i) Coronary Atherosclerosis Reversal Potentialof Yoga Lifestyle Intervention
ii
ii
) Clinical Research Profile
i) Yoga and Biofeedback for the treatment ofIrritable Bowel Syndrome
iv) Research Methodology in Naturopathy &Yoga
5.5.7 At present, the Treatment-cum-PropagationCentre Scheme (20 beds) is operated in 74 centresand Patient Care Centre Scheme (10 beds) at 34centres at difference places with the financialassistance by CCRYN. These schemes are aimedat strengthening the existing facilities of Yoga andNaturopathy at the Hospitals as well as to propagate
the principles, concepts & practices of these systems
among the masses.
5.5.8 The financial assistance provided under the
Treatment-cum-Propagation Centre & Patient Care
Centre Schemes by the Council is as follows:
Treatment-cum- - Rs.3,00,000/- per annum
Propagation Centre
(TCPC)
(20 Beds Hospital)
Patient Care Centre - Rs.1,20,000/- per annum
(PCC)
(10 Beds Hospital)
5.5.9. The Council has brought out a number of
priced publications and free publicity material for the
benefit of general public by making them aware about
the health care benefits of these sciences in the
management of various lifestyle disorders. It is also
planning to print some more books under its Literary
Research/ Publication and Translation Scheme. The
Council has produced CDs on different aspects of
Yoga and Naturopathy in Hindi, English and Tamil
languages. These CDs are helpful in spreading the
message of Yoga and Naturopathy among the
masses.
5.5.10 Workshop/Seminar
The Council organized a three days 'Training
Workshop on Research Methodology in Naturopathy
& Yoga' at Council's Hq. from 26th - 28th March, 2008.
It was highly successful.
5.5.11 Budget
During the current financial year 2008-09, a
budgetary allocation of Rs.566.00 lakh under Plan
and Rs.130.00 lakh under Non-Plan in the Revised
Estimates 2008-09 has been made for the CCRYN.
5.5.12 North-Eastern States
The Council has spent Rs.17.53 lacs on North-East
States under various schemes up to Sept. 2008,
which is 10.82% of the total grants-in-aid released
by the Council.

399
ANNUAL REPORT 2008-09
5.6 New Institutions of Ayurveda,Homoeopathy and Folk Medicine
The Department proposes to set up the followingthree autonomous institutions in the 11th Plan period.
5.6.1 All India Institute of Ayurveda(AIIA), New Delhi
The need for establishment of a Centre of Excellencededicated to tertiary care and research in Ayurvedahas been felt for a very long time. The Departmenthas acquired about 11 acres of land at Sarita Vihar,New Delhi from the Delhi Development Authority forthe proposed All India Institute of Ayurveda (AIIA).The foundation stone of the Institute was laid byHon'ble Vice President of India on 14th February,2004. The proposed institute would facilitate qualityresearch and develop benchmarks for Ayurvediceducation, research and health care. The institutewill be mandated to undertake interdisciplinaryeducation and research programmes in collaborationwith premier national and international institutions.It also aims to forge linkages between Ayurveda andmodern sciences with the help of reputed institutionslike AIIMS, CSIR and NIA, etc. for expanding the reachof Ayurveda. Besides, it will focus on developmentand documentation of best practices, safety andefficacy data and standard treatment protocols ofAyurveda.
The Cabinet approval for the establishment of theAIIA has been received. A High Level Committee underthe chairpersonship of Secretary AYUSH to overseethe implementation of the project has beenconstituted. The Environment Impact Assessmentwork has been awarded to WAPCOS. An MoU withHSCC, appointing them as in-house technicalconsultant has been signed. M/S HSCC, being thein-house Consultant of the project, have beeninstructed to award the work to M/S Kothari AssociatesPvt. Ltd., New Delhi for preparation of Detailed ProjectReport and engineering designs, including statutoryclearances. Preconstruction survey at the site atSarita Vihar, New Delhi is on. Joint Secretary (AYUSH)is the OSD of the project.
The proposed project is estimated to be completedwithin the 11th Plan period. It is intended to makethe hospital operational within 30 to 36 months. Total
cost of the project in 11th Plan is estimated at Rs.155.00 crores out of which Rs. 134.00 crores is
towards capital works with Rs.21.00 crores for
recurring expenditure on salary and wages,
consumables, medicines, maintenance, etc.
5.6.2 Establishment of the North-Eastern Instituteof Ayurveda and Homoeopathy (NEIAH) in Shillong,
Meghalaya
The Department has proposed to establish a North
Eastern Institute of Ayurveda and Homoeopathy in
the North Eastern Indira Gandhi Regional Institute
of Health & Medical Sciences (NEIGRIHMS) campusin Shillong, Meghalaya. The Institute is envisaged to
have an Ayurveda college with admission capacity
of 60 students and a Homoeopathy college with
admission capacity of 50 students along with a 120
bed Ayurveda hospital and a 50 bed Homoeopathy
hospital, a Documentation cum R&D center and anAyurvedic Pharmacy with a Drug Testing Laboratory.
The setting up of the Institute will address the serious
shortage of trained Ayurvedic and Homoeopathic
physicians in the region. The co-location of the
proposed Institute in the NEIGRIHMS campus will
enable cross referral of patients and collaborativeteaching and research between the Allopathic and
AYUSH institutions. The co-location would also enable
the sharing of certain common infrastructure and
facilities and this which would lead to greater
efficiency and lower costs. Residential facilities for
students and staff would also be established.
The Cabinet approval for the establishment of theNEIAH at Shillong has been received. A Task Force,headed by Secretary (AYUSH), for implementationof the project, has been constituted. In pursuance ofthe Cabinet decision for implementation of the projecton turnkey basis, an agreement has been signedwith M/S HSCC for the construction of the building.The creation of necessary infrastructure andappointment of staff as per statutory norms forAyurveda and Homoeopathy colleges is expected tobe completed by the end of the December, 2009 sothat the admission of the first batch of students couldbe started from July, 2010. The total cost of the firstphase of the project is estimated at Rs. 67.51 crore,out of which Rs. 56.50 crore is towards non-recurring
400
ANNUAL REPORT 2008-09
expenditure on capital works and Rs. 11.01 crore forrecurring expenditure on salary and wages,consumables, medicines, maintenance, etc. Theproject cost would be met from the 10 percent shareof the North Eastern Region earmarked within thetotal Plan outlay of the Department.
5.6.3 Establishment of North Eastern Instituteof Folk Medicine at Pasighat, ArunachalPradesh
The Department of AYUSH has proposed to set upthe North Eastern Institute of Folk Medicine atPasighat in order to harness the rich traditions ofFolk medicine and Tribal Health practices in theregion through documentation, validation and thecapacity building of traditional healers. There is anecessity to set up the Institute to ensure theprotection and dissemination of the knowledgecontained in Folk medicine and Tribal healthpractices in the region by way of systematicdocumentation and by making itself a repository ofnatural resources used in Folk medicine and LocalHealth traditions. The Cabinet approval has sincebeen received for the establishment of the NorthEastern Institute of Folk Medicine at Pasighat,Arunachal Pradesh. For implementation of theproject a Task Force has been constituted. Twomeetings of the Task Force have been held till now.A Project Monitoring Committee under thechairpersonship of Secretary (AYUSH) has also beenconstituted.
The Government of Arunachal Pradesh had alreadyallotted about 40 acres of land in an institutional areain Pasighat (East Siang District) for the Institute, butit was later realized the the land was forest land. TheState Government has been appraised of the matterand efforts are on to procure an alternate site forthe institute. In the meantime the Institute has startedoperations from rented premises. A workshop withstakeholders has been held. Research Officer,Regional Research Institute, Itanagar has beenappointed as Project Incharge of the Institute andDr. Ramashankar of CCRAS has been appointed asOSH. In pursuance of the Cabinet decision forimplementation of the project on turnkey basis, anagreement has been signed with M/S HSCC for the
construction of the building. The Institute is expectedto be fully functional by the end of the 2010 and theproject cost is estimated to be around Rs. 32.88crores.
5.7 Scheme for Extra Mural Research
5.7.1 A scheme for Extra Mural Research is beingimplemented since the 9th Plan, scheme with the aimof involving reputed individual scholars andinstitutions.in research in AYUSH Systems. Anadditional component called the 'Golden TrianglePartnership' was added on to the Extra MuralResearch Scheme in 2004, as an integratedtechnology mission, involving the Department ofAYUSH, CSIR and ICMR for the development ofAyurveda and traditional medical knowledge basedon synchronized working of modern medicine,traditional medicine and modern science. The ExtraMural Research Scheme would be continued in the11th Plan with certain procedural modifications.
5.7.2 Objectives of EMR
! Development of Research & Development(R&D) based AYUSH Drugs for prioritizeddiseases
! Generate data on safety, standardization andquality control for AYUSH products andpractices;
! To develop evidence based support on theefficacy of AYUSH drugs and therapies;
! Encourage research on classical texts andinvestigate fundamental principles of AYUSHSystems;
! Generate data on heavy metals, pesticideresidues, microbial load, safety/toxicity etc.in the raw drugs and finished Ayurveda,Siddha, Unani and Homoeopathy drugs;
! Develop AYUSH products having IntellectualProperty Rights (IPR) potential for increasingAYUSH exports
! Develop the potential Human Resource inAYUSH systems, especially to inculcate
401
ANNUAL REPORT 2008-09
scientific aptitude and expertise relating toAYUSH systems;
! Develop joint research ventures betweenthe Department of AYUSH and otherOrganizations/Institutes.
Under the Scheme, financial assistance is providedto reputed research organizations like MedicalColleges, University Departments, ResearchInstitutions, both in the public and private sectors forundertaking research projects in areas prioritizedunder the scheme. The Scheme aims at utilizing thepotential of eminent research institutions in thecountry for broadening and deepening the scope ofAYUSH research in the country. The ResearchCouncils invite proposals through open advertisementin the newspapers which are then evaluated byProject Evaluation Committees comprising of subjectexperts with final approval being given by a high levelScreening Committee.
5.8 Golden Triangle PartnershipProject
5.8.1 The Golden Triangle Partnership concept asexplained above was initially aimed at setting up anintegrated technology mission involving AYUSH, CSIRand ICMR, for the development of Ayurveda andtraditional medical knowledge. The Scheme has nowbeen expanded to include Siddha, Unani andHomoeopathy. The three organizations namelyDepartment of AYUSH/CCRAS, CSIR and ICMR areworking together to undertake scientific validationand development of safe, effective and standardizedclassical products for identified disease conditionsand to develop new products effective in diseaseconditions of national/global importance.
5.8.2 Objectives of GTP
! Bring safe, effective and standardized ASUand H (Ayurveda, Siddha, Homoeopathy andUnani) products for the identified diseaseconditions;
! Develop new Ayurvedic / Siddha / Unani /Homeopathic products effective in thedisease conditions of national/global
importance. Products should be better thanthe available products in the market for such
disease conditions;
! Utilize appropriate technologies for
development of single and poly-herbal
products to make it globally acceptable;
! Promote collaborative research on AYUSH
with modern medicine/ modern science
institutions.
5.8.3 The scheme has been modified to make it
more focused. The following priority areas for
research have now been determined for each of the
AYUSH systems individually considering their areas
of strength :-
! Joint disorders,
! Memory disorders,
! Menopausal syndrome,
! Bronchial allergy, Fertility & infertility,
! Cardiac disorders (Cardio-protective and
anti-atherosclerotic),
! Sleep disorder, Vision disorders, Urolithiasis
and Benign Prostatic
! Hypertrophy (BPH),
! Diabetes mellitus, Standardization
! Safety and toxicity studies of metallic
bhasmas and mineral based formulations
including Kupipakwa Rasayanas, HIV/AIDS,
! Skin diseases,
! Obesity and Cancer,
5.8.4 The Department of AYUSH jointly implements
the GTP scheme with CCRAS, CSIR and ICMR. CSIR
is extending the use of their laboratories and
scientists and. ICMR is providing all support for the
conduct of clinical studies. Three task force
Committees for Ayurveda, Unani and Homoeopathy
for each drug development Program will be set up.
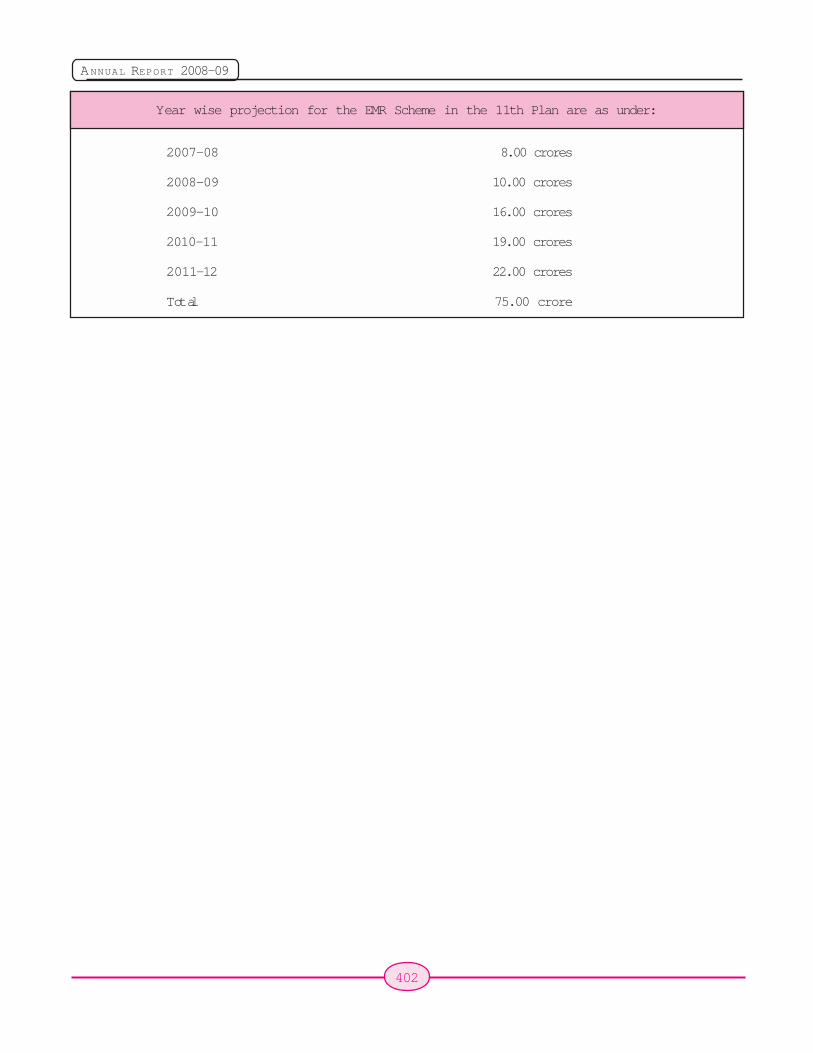
402
ANNUAL REPORT 2008-09
Year wise projection for the EMR Scheme in the 11th Plan are as under:
2007-08 8.00 crores
2008-09 10.00 crores
2009-10 16.00 crores
2010-11 19.00 crores
2011-12 22.00 crores
Total 75.00 crore
403
ANNUAL REPORT 2008-09
Chapter 6
6.1 India has a very rich heritage of plant basedhealth care system viz. Ayurveda, Unani, Siddha,Homoeopathy and various folk lore systems ofmedicines. These systems have a very high degreeof social acceptance for the quality health care theyhave been providing to a large segment of ourpopulation. There is resurgence of use of traditionalsystems and a large number of health care productsbased on the traditions systems, across the globe,for various health care needs. The demand of rawmaterial procured from medicinal plants has,therefore, been increasing steadily. The forests andwastelands have been the traditional source ofmedicinal plants. However, this practice may notcontinue for various reasons. First, the forestresources are depleting and a number of specieshave already reached on the verge of extinction.Secondly, there are concerns world wide pointingtowards conservation of natural resources andagainst the use of raw material sourced from wildwithout proper collection techniques.
6.2 National Medicinal Plants Board(NMPB)
6.2.1 Considering the above, a need had been feltfor quite long to have concerted steps fordevelopment of the Medicinal Plants sector. TheNational Medicinal Plants Board (NMPB) was set upthrough Government Resolution notified on 24thNovember 2000 under the Chairmanship of UnionHealth & Family Welfare Minister. The objective ofestablishing the Board was to establish an agencywhich would be responsible for coordination of allmatters relating to medicinal plants, includingdrawing up policies and strategies for conservation,proper harvesting, cost-effective cultivation, researchand development, processing, marketing of raw
material in order to promote and develop this sector.This was considered necessary as medicinal plantsas a subject is handled by different Ministries/Departments like Environment & Forests, Agriculture,Science & Technology and Commerce. The Board,therefore, has the function of co-ordination withMinistries/Department/Organizations/State/UTGovernments for development of medicinal plants ingeneral and specifically in the following fields: -
i) Assessment of demand/supply positionrelating to medicinal plants both within thecountry & abroad;
ii
ii
i
) Advise the concerned Ministries/Departments/Organisations/State/UTGovernments on policy matters relating toschemes and programmes for developmentof medicinal plants;
i) Provide guidance in the formulation ofproposals, schemes and programmes etc. tobe taken by agencies having access to landfor cultivation and infrastructure for collection,storage transportation of medicinal plants;
iv) Identification, inventorization andquantification of medicinal plants;
v) Promotion of ex-situ and in-situ cultivationand conservation of medicinal plants;
vi) Promotion of co-operative effort amongcollectors and growers and assisting them tostore, transport and market their productseffectively;
vi) Setting up of database on medicinal plants,dissemination of information and facilitatingprevention of patents on plants used intraditional systems;
Increasing the Availability of MedicinalIncreasing the Availability of MedicinalIncreasing the Availability of MedicinalIncreasing the Availability of MedicinalIncreasing the Availability of MedicinalPlants for Raw MaterialPlants for Raw MaterialPlants for Raw MaterialPlants for Raw MaterialPlants for Raw Material
404
ANNUAL REPORT 2008-09
viii) Matters relating to import/export of rawmaterial, as well as value added productseither as medicine, food supplements or asherbal cosmetics including adoption of bettertechniques for marketing of products toincrease their reputation for quality andreliability in the country and abroad;
ix) Undertaking and awarding Scientific,technological research and cost-effectiveness studies;
x) Development of protocols for cultivation andquality control, and
xi) Encouraging the protection of Patent Rightsand IPR.
6.2.2 Schemes/Projects for Financial Assistanceimplemented by the National Medicinal Plants Board
In order to address various issues and problems ofthe medicinal plants sector, the Board has identifiedimportant areas for development of the sector andformulated schemes for financial support. These are:
(A) Promotional Schemes:
! Survey and Inventorization of medicinalplants
! In-situ conservation and ex-situ cultivation ofmedicinal plants.
! Production of Quality Planting Material.
! Extension activities - Information educationand communication.
! Study of demand supply position andmarketing of medicinal plants for domesticand global market.
! Research & Development in medicinal plantssector.
! Promote co-operative efforts among growersand collectors of medicinal plants.
! Undertake/assist or encourage scientifictechnological and economic research onmedicinal plants.
(B) Contractual Farming Scheme:
The scheme was implemented to provide financialassistance to farmers / growers for cultivation ofidentified medicinal plants with commercial potentialand market demand.
Brahmi
(C) Commercial Schemes:
! Production and assured supply of qualityplanting material in bulk.
! Area expansion of selected species andcultivation.
! Value addition - for developing properharvesting techniques, semi-processing ofproduce viz. Collection, grading, drying,storage, packing etc.
6.3 Salient Achievements andInitiatives of National MedicinalPlants Board (NMPB):
6.3.1 35 State Medicinal Plants Boards (SMPBs)have been set up in States / UTs for implementationof programmes / schemes of NMPB in States/ UTsand monitoring thereof. Financial assistance is alsoprovided for their maintenance, functioning andspecifically for monitoring of sanctioned /implemented projects.
6.3.2 The National Medicinal Plants Board has sofar sanctioned more than 6,832 projects involving
405
ANNUAL REPORT 2008-09
financial assistance of approximately Rs. 68.64crores for cultivation of medicinal plants on about50,355 hectares. 1,071 projects involving financialoutlay of about Rs. 153.34 crores sanctioned underPromotional Scheme since the year 2001-02. About31,684 hectare land has been covered underprogrammes for conservation (in-situ and ex-situ) ofmedicinal plants.
6.3.3 The country specific Good AgriculturalPractices on the pattern of Good Agricultural andCollection Practices (GACP) developed by WHOhave been formulated for dissemination andvoluntary adoption. Another project in collaborationwith WHO is under implementation for developmentof Good Field Collection Practices (particularly withreference to medicinal plants from wild resources).NMPB has published first volume of reports on agro-techniques of 50 medicinal plants under projectsallocated to various agricultural universities andresearch institutions. NMPB plans to publish thesecond volume of the report consisting of agrotechnique of another 50 plants shortly.
6.3.4 NMPB implemented the scheme for settingup of Herbal Gardens in schools for creation ofawareness among school children regardingmedicinal plants. Projects have been sanctioned forcoverage of 1,110 schools so far.
6.3.5 NMPB completed a nationwide study forassessment of demand and supply of medicinalplants through FRLHT, Bangalore. Salient findingsof the Study reveal that:
(i) The annual demand of botanical raw drugsin the country is about 3,19,500 MTs.
(ii
i
) Annual trade value is estimated to be aroundRs. 1,069 crores.
(ii) 178 species are in trade with volumes inexcess of 100 MTs per year
(iv) Out of 178 species, 34 are reported to besourced through cultivation, 46 from waste /fallow lands, 91 from forests and the rest areimported.
(v) Out of 178 species in high trade, 21 species
have been categorized RET (rare,endangered and threatened)
(vi) The quantity estimated to be sourced fromcultivation is 1,46,400 MTs and the cultivationarea is about 1,43,000 hectare.
6.3.6 This study has been made the basis forfunding new projects so that species that are ofconservation concern and are otherwise in highdemand are taken up for regeneration andconservation (both in- and ex-situ).
6.3.7 Considering the shortage of manpower, theBoard has outsourced the appraisal and scrutiny ofcultivation projects received from farmers/ growersto M/s NABARD Consultancies and M/s AgricultureFinance Corporation Limited.
6.3.8 With a view to improving the quality ofimplementation and monitoring, the grants-in-aid forcultivation projects is released in a consolidatedmanner through the SMPBs who in turn are requiredto inspect the project sites, verify necessarydocuments and thereafter release the subsidy.
6.3.9 Dissemination of market information is the keyto promoting cultivation. For this purpose the Boardhas developed e-portal which seeks to disseminateinformation on medicinal plants and their prices invarious mandies on a weekly basis. The portal canalso function as a virtual mandi for trading medicinalplants by exchange of information between buyersand sellers. Printed bulletins on market informationare also distributed to State Medicinal Plants Boardfor dissemination to growers.
6.3.10 Special projects for raising medicinal treesthrough forest nurseries have been sanctioned toaddress the critical shortage of tree based medicinalplants products.
6.4 Medicinal Plants in the ActionPlans of National HorticultureMission and Technology Missionfor Horticulture for North Eastand other Hilly States.
6.4.1 On the initiative of the Board, the National
406
ANNUAL REPORT 2008-09
Horticulture Mission and Technology Mission forHorticulture for NE and other Hilly States of theDepartment of Agriculture and Cooperation hasagreed to include medicinal plants under theirprogramme. Instructions have already been issuedto State Horticulture Missions to make adequateprovisions for medicinal plants in their Action Plans.There is greater convergence between NHM and
NMPB as the State Medicinal Plants Boards arerepresented on the Steering Committees of the StateMission Directorates of NHM. Also, the Action plan ofstate under NHM have started covering medicinalplants in their area expansion component of theMission. Projects have been sanctioned by NMPBfor cultivation and development of identified medicinalplants.
Inauguration of school herbal garden scheme byNFM
Herbal garden at WHO (h.q.), Geneva Visit of medicinal plants farm
6.5 Other Important Achievement
6.5.1 Strengthening of National MedicinalPlants Board
The National Medicinal Plants Board has been facinga shortage of officers / staff for quite long. Matterregarding creation of various posts has been taken
up by the Board for quite long. Subsequently, theBoard was able to have the approval of Departmentof Expenditure for creation of 10 posts.
6.5.2 Strengthening of State Medicinal PlantsBoards
The Standing Finance Committee of NMPB in its 29th
Grass root training programme
407
ANNUAL REPORT 2008-09
meeting held on 22.02.2008 has approved theenhanced allocation of funds of Rs. 10.00 lacs peryear for States having fulltime CEO/full-fledged SMPBand Rs. 5.00 lacs per year for States which do nothave a fulltime Board for maintenance of NucleusCentre.
6.5.3 Special projects for rare andendangered species of medicinal plants
i) A study on demand and supply of medicinalplants in India carried out by the Board duringyear 2007-08 brought out alarming shortagesof some of the plants used by the Ayurvedicindustry. The Board, thereafter, launchedspecial drive to invite proposals forconservation and plantation of some of therare and endangered species in high demandfrom states.
ii) The Board, sanctioned conservation /plantation of Guggal over 4,000 hectares offorest areas in Gujarat and Rajasthan, SitaAshoka over 800 hectares in the states ofKarnataka, Orissa and Kerala and Dashmooltrees over 1,100 hectares in the states ofGujarat, Madhya Pradesh, Tamil Nadu,Karnataka, Kerala, Tripura and AndhraPradesh . Projects on high altitude plantslike Ateesh, Kutki, Kuth have also beensanctioned for implementation through CivilSociety organizations working with people inthe Himalayas.
Ashok
Guggal
6.5.4 Facilitation Centres ( FCs) for Extensionand Support Services on medicinal plants
Since SMPBs in states / UTs are not adequatelyequipped with staff and infrastructure support, NMPBhas set up Facilitation Centres in State AgricultureUniversity and R&D Institutions. These centres areto act as one stop shop for growers and other stakeholders and would be required to work in closecoordination with SMPBs. In all 23 FacilitationCentres have been set up so far. The State ChiefSecretaries have been requested to set upMonitoring Committees under the chairpersonshipsof the Agricultural Production Commissioners tooversee the functioning of the FCs.
6.5.5 Development of Good Agricultural andGood Collection Practices for medicinal plants
NMPB has implemented projects for development ofGood Agricultural and Good Collection Practices formedicinal plants in association with WHO. The GoodField Collection Practices for medicinal plantscollected from the wild are being finalized forpublication. Guidelines on Good Field CollectionPractices for medicinal plants collected from wild arealso being formulated under the other projectimplemented in collaboration with WHO.
408
ANNUAL REPORT 2008-09
Shatavar
6.6 Implementation of RevisedSchemes during 11th Plan
6.6.1 Revised Central Sector Scheme viz."Central Sector Scheme for Conservation,Development and Sustainable Management ofMedicinal Plants"
National Medicinal Plants Board has beenimplementing a "Central Sector Scheme of setting upMedicinal Plants Board" during the 10th Plan. Thiswas an umbrella scheme which covered a range ofpromotional and conservation related activitiesincluding commercial cultivation. With a view toimplement the programmes with a sharper focus, thescheme has been revised both in the range of activitiesto be covered under the scheme as well as the patternof assistance. Also, while the conservation, R&D andpromotional activities have been retained underrevised scheme the cultivation and commercial
component has been included in a new centrallysponsored scheme. The two schemes are:
(i) Central Sector Scheme for Conservation,Development and Sustainable Managementof Medicinal Plants.
(ii) Centrally Sponsored Scheme of NationalMission on Medicinal Plants.
6.6.2 Central Sector Scheme forConservation, Development and SustainableManagement of Medicinal Plants.
This scheme was approved by Cabinet Committeeon Economic Affairs in its meeting on 26th June,2008 with a total outlay of Rs. 321.30 crores duringthe 11th plan for the activities relating to Survey,inventorisation and In-situ conservation by settingup Medicinal Plants Conservation Areas, support toJoint Forest Management Committee (JFMCs) /Panchayats for value addition, warehousing andmarketing, Ex situ Conservation of Prioritized speciesof Conservation concern, Research andDevelopment - development of comprehensivemonographs, Common Technical Dossiers, agro-techniques and bio-activity guided phyto-chemicalscreening of plants etc., establishing qualitystandards and certification mechanism, Training,Education and Capacity Building of stakeholders,Promotional Activity viz. home/school herbal gardensetc. and Management support.
6.6.3 Year Wise phasing of proposed outlayfor 11th Plan will be as under:
Rs. in lakhs
S. No. Year Non-recurring Recurring (5%) Total
1. 2007 - 08 4790 224 5014
2. 2008 - 09 4058 242 4300
3. 2009 - 10 6950 350 7300
4. 2010 - 11 7328 350 7678
5. 2011 - 12 7474 364 7838
Total 30600 1530 32130
Operational Guidelines for implementation of the scheme have been formulated.
409
ANNUAL REPORT 2008-09
Medicinal Plants Nursery
6.7 Centrally Sponsored Scheme ofNational Mission on MedicinalPlants
6.7.1 Cultivation of medicinal plants that is the keyto quality, efficacy and safety of the AYUSH systemsof medicines. Integrating medicinal plants in thefarming systems also offers an option of cropdiversification and to enhance incomes of farmers.Support for cultivation without backward and forwardlinkages for quality planting material of certified origin,processing and marketing, however, is crucial forsustaining cultivation. Also, support of states forproviding infrastructural facilities such as land, power,road connectivity and a conducive policy andregulatory environment can be more efficientlyorganized through a Centrally Sponsored Scheme.
6.7.2 Keeping in view the need to launch specialinitiative to promote cultivation and bring inconvergence between cultivation and processing,CCEA in its meeting on July 24th, 2008, approved a
new Centrally Sponsored Scheme of National Missionon Medicinal Plants with a totally outlay of Rs. 630crores during the 11th Plan with the following keyactivities:
! Nursery for certified Rs. 40 croresquality planting material
! Plantation (80000- Rs. 400 crores1 lac ha)
! Post Harvest Management Rs.160 crores(PHM), Marketinginfrastructure (creation/upgradation), warehousing,processing, quality testing,Certification & Insurance
! Management support Rs. 30 crores
Total Rs. 630crores
6.7.3 Year Wise phasing of the outlay for 11th Planas per approved proposal will be give in next page:
410
ANNUAL REPORT 2008-09
S. No. Year Non-recurring Recurring (5%) Total
1. 2007 - 08 -- -- --
2. 2008 - 09 48 2 50
3. 2009 - 10 142 8 150
4. 2010 - 11 190 10 200
5. 2011 - 12 220 10 230
Total 600 30 630
Operational Guidelines for implementation of the scheme have been formulated.
Rs. in lakhs
6.8 Outcomes to be achieved duringthe XIth Plan
The Mission, by 2011 - 12 proposes to cover 80,000- 1,00,000 ha. of land under medicinal plants throughdirect financial assistance for cultivation and analmost equal area which will be covered byincentivisation of farmers who may switch over fromtraditional crops to medicinal plants in areas whereinfrastructure for quality planting material,processing, warehousing, marketing, quality testingand certification is promoted through cooperativesof growers, self help groups, corporates etc.
6.8.1 About 200 nurseries will be established, bothin public and private sector, for making availableplanting material of certified quality. Infrastructure oflaboratories for testing raw material will be created inpublic-private partnership mode where suchlaboratories do not exist. In other cases, the existingNABL/AYUSH accredited labs will be utilized for testingof raw material with 50% of the testing charges beingreimbursed to the growers. The scheme seeks topromote cluster based cultivation and post harvestmanagement in about 100 districts in the country. The23 Facilitation Centres (FC) set up in State AgricultureUniversities and R&D institutions of CSIR and ICARby NMPB will provide single window service by way of
information to farmers/growers on all aspects ofmedicinal plants cultivation and marketing. Thefacilities for post harvest managements, both in publicand private sectors, will be enhanced involving storagegodowns, setting up herbal mandies, upgradation ofexisting krishi upaj mandies etc. Recognized groups,cooperatives, corporates, producer companies, selfhelp groups of small and marginal farmers and othereligible groups will be involved in this endeavour.Coupled with awareness creation campaigns/sensitization measures, it is envisaged to bring aboutsignificant increase in production, value addition andquality of medicinal plants products to compete in theworld market. The interventions are expected togenerate approximately 6 crores mandays ofemployment by the year 2011 - 12.
6.8.2 Further, the export of medicinal and valueadded herbal sector is expected to double by theyear 2011 - 12 which is presently of the order Rs.800 - 900 crores. In addition, the percentage of valueadded products which at present is only 30% of thetotal exports, is expected to increase 70% of the totalexport basket of the herbal products. Increasedinfrastructure for processing and marketing will alsopromote crop diversification from traditional crops tomedicinal plants thereby providing greater financialsecurity to growers/cultivators.
411
ANNUAL REPORT 2008-09
Chapter 7
Standardization and Quality ControlStandardization and Quality ControlStandardization and Quality ControlStandardization and Quality ControlStandardization and Quality Controlof ASU&H Drugsof ASU&H Drugsof ASU&H Drugsof ASU&H Drugsof ASU&H Drugs
7.1.1 The department places a high priority tolaying down the pharmacopoeial standards forAyurveda, Siddha and Unani medicine, both for singleand compound drugs. With this objective the Ministryhad taken up the task of developing pharmacopoeialstandards through Pharmacopoeia Committees.Pharmacopoeial standards are mandatory for theimplementation of the drug testing provisions underthe Drugs and Cosmetics Act, 1940 and Rulesthereunder. These standards are also essential tocheck samples of drugs available in the market fortheir safety and efficacy.
7.1.2 Four different Pharmacopoeia Committeesare working for preparing official formularies/pharmacopoeias of Ayurveda, Siddha, Unani andHomoeopathy drugs. These committees are engagedin evolving uniform standards for preparation of drugsof and in prescribing working standards for singledrugs as well as compound formulations.
7.1.3 Standards for around 40% of the rawmaterials and around 15% of formulations have beenpublished by the Pharmacopoeial committees. It hasbeen decided to upgrade these committees into afull fledged modern Pharmacopoeial Commission withadequate representation of stakeholders and todevelop standards that are in line with internationallyacceptable pharmacopoeial standards.
7.2 Ayurvedic PharmacopoeialCommittee (APC)
7.2.1 APC engages in multi disciplinary activity withthe objective of developing PharmacopoeialStandards. As far as Single Drugs are concerned,the APC focuses on the development ofPharmacopoeial standards and on development of
the Method of Preparation. PharmacopoeialStandards of Compound formulations are also beingdeveloped and shelf life studies are being done.Studies on the safety and toxicity of drugs are alsobeing done.
7.2.2 The Ayurvedic Pharmacopoeia Committeehas published 6 volumes of Ayurvedic Pharmacopoeiaof India consisting of 520 monographs on singledrugs and 2 volumes of Ayurvedic PharmacopoeiaPart II containing 101 of Compound formulations.Heavy metals studies on 239 plant drugs, PesticideResidue studies on 183 plant drugs, microbialcontamination studies on 237 plant drugs, aflatoxinstudies on 41 plant drugs, 230 single and compoundformulation are in the pipeline, 10 Minerals andMetals monographs are in the process of draftingfor publication and Single Drugs standardizationstudies on 168 is nearing completion.
7.3 Unani PharmacopoeiaCommittee (UPC)
7.3.1 The Unani Pharmacopoeia Committee (UPC)was constituted on 2nd March 1964 for preparingthe official National Formulary of Unani Medicine(NFUM) and the Unani Pharmacopoeia. ThePharmacopoeia Committee was reconstituted underthe chairmanship of Dr. G. N. Qazi on 24.04.2007.The target of the UPC is to lay down standards for200 single drugs and 200 compound formulations inthe Unani Formulary of India per year. The UPC tookup the work on one hundred compound drugs.
7.3.2 Unani Pharmacopoeia Committee haspublished 198 pharmacopoeial standardsmonographs of single drugs and 55 compound drugsis under publication. In addition 64 pharmacopoeial
412
ANNUAL REPORT 2008-09
standards monographs of single drugs and 50compound drugs are under preparation.
7.4 Siddha PharmacopoeiaCommittee (SPC)
7.4.1 The Government of India constituted theSiddha sub-committee under the AyurvedicPharmacopoeia Committee in February 1964 tostandardize the various compound Siddhaformulations and publish the Siddha Pharmacopoeia.In 1975 the Siddha Pharmacopoeia Committee(SPC), was constituted as an independent body. TheSPC published the official Siddha Formulary of India,Part- I in Tamil and English in 1984 and 1992. Thisformulary consists of 22 sections and covers 248Siddha medicines.
7.4.2 The Siddha Pharmacopoeia of India, Part- I,Vol. I has been prepared. This volume consists of 73single drug monographs. Work on the SiddhaFormulary of India, Part- II and SiddhaPharmacopoeia of India, Part-I, Vol. II is underprogress.
7.5 Homoeopathic PharmacopoeiaCommittee (HPC)
7.5.1 The Homoeopathic PharmacopoeiaCommittee (HPC) was constituted in September1962.. The HPC has Chemistry experts, besidesmanufacturers of Homoeopathic medicines andeminent Homoeopaths as well as officials who areconcerned with the work of drug.testing and research.The Committee was last reconstituted in January,2004 for a term of three years, and still continues inexistence. The Chairman of the Committee haspowers to form Sub-committees whenever requiredand to co-opt experts from outside on Sub-committees.
7.5.2 Homoeopathic drugs are available in themarket in the form of mother tinctures and in differentpotencies. The priority of the HPC is to fix standardsup to the level of mother tincture or equivalent i.e. ofthe raw materials and method of preparation. From1962 onwards, the Committee has finalized NineVolumes of Homoeopathy Pharmacopoeia of India
and recommended standards for the HomoeopathicPharmacopoeia of India containing 1016Monographs. The Homoeopathic PharmaceuticalCodex Vol. I comprising 100 monographs has beenpublished. One hundred monographs were approvedfor inclusion in the 9th volume of the HomoeopathicPharmacopoeia of India. These committees aremaking drugs standardization, which is a pre-requisitefor manufacture of ASU&H drugs. The publication ofabove pharmacopoeial standards of monographs ofAyurveda, Unani, Siddha and Homoeopathy, singleand compound drugs, are based on work undertakenby AYUSH Research Councils and other laboratoriesof CSIR under the supervision of above mentionedpharmacopoeia committees.
7.6 Sub-committee of DrugsTechnical Advisory Board onHomoeopathy
The Sub-Committee of the Drugs Technical AdvisoryBoard (DTAB) was initially constituted in December,1997 to consider issues relating to Homoeopathy.The Sub-Committee was reconstituted on 6th July,2007 for a term of three years.
7.7 Pharmacopoeial Laboratoryfor Indian Medicine (PLIM),Ghaziabad
7.7.1 The Pharmacopoeial Laboratory for IndianMedicine (PLIM), Ghaziabad was established in theyear 1970 as Standard setting-Cum-Drug-testingLaboratory for Indian Medicines (Ayurveda, Unaniand Siddha Systems) at the national level. TheLaboratory is also notified as an appellate laboratoryfor drug testing and quality control. The Laboratoryhas its own three storeyed building in Ghaziabadwhich is well equipped with modern testing facilities.The PLIM also has a medicinal herb garden museumwith a collection of about 2000 genuine raw drugs.The laboratory is imparting training to Drug ControlAuthorities and Quality Control personnel fromGovernment laboratories and private manufacturers.The Department of AYUSH, publishes the worked outstandards in the form of monographs for theAyurvedic, Unani and Siddha Pharmacopoeia of
413
ANNUAL REPORT 2008-09
India. Six volumes of the Ayurvedic Pharmacopoeiaof India containing standards for 527 single drugsand have been published. The Laboratory has beennotified as Central Drug Laboratory for the whole ofIndia. Two volumes of API Part II contains standardson 101 compound formulations.
7.7.2 The laboratory has developedchromatographic profiles of 80 plants drugs forpublishing in the Atlas. During the year, the laboratoryhas tested 250 drugs samples referred to it by legaland official sources. Five orientation trainingprogrammes for Drug Inspectors/Drug Analysts wereorganized during the year. The laboratory alsoorganized National Campaign on Quality Assuranceand GMP for ASU & H medicines.
7.7.3 The PLIM published three books, "LegalStatus of Ayurvedic, Siddha and Unani Drugs","Protocol for Testing of Ayurvedic, Siddha and UnaniMedicines" and "Quality Control Manual for ASUmedicines". PLIM was also involved in the certificationof three private drug testing laboratories for AYUSHproducts. During the year 50 crude drug sampleswere added to the museum for display and referencestandards.
7.7.4 Rs.224.00 lakh and Rs.110.00 lakh have beenprovided to PLIM for the year 2008-2009 under planand non-plan budget, respectively.
7.8 Homoeopathic PharmacopoeiaLaboratory (HPL), Ghaziabad
7.8.1 Homoeopathic Pharmacopoeial Laboratory(HPL), Ghaziabad was set up as a NationalLaboratory for the purpose of laying down standardsand testing for identity, purity and quality ofHomoeopathic medicines. The Laboratory alsofunctions as a Central Drug Laboratory for the testingof Homoeopathic Medicines under Rule 3A for theDrugs and Cosmetics Act. Standards worked out bythe HPL laboratory are published in theHomoeopathic Pharmacopoeia of India (HPI). Todate, nine volumes of the HPI have been publishedcovering standards on 1000 drugs. The Departmentof Science and Technology has recognized HPL asa Scientific and Technological institution.
7.8.2 The significant achievements of thelaboratory are:-
(a) The laboratory prepared 26 monographs for
incorporation in the Homoeopathic
Pharmacopoeia of India, tested 300 survey
and 23 raw drugs samples, screened and
rationalized 49 formulations for weeding out
irrational formulations.
(b) Testing of 1085 samples of Homoeopathic
medicine received from CGHS/Legal/Ports/
Private sources was done. During the year,
twelve new plant species were added to the
medicinal herbal garden and about 80 live
plants were shifted from the old campus to
the new campus.
(c) The Laboratory organized two orientation
programmes for Drug Control Authorities,
Pharmacists, Drug Analysts and Lecturers of
Homoeopathic Pharmacy from Homoeopathic
medical colleges.
(d) A small Herbarium and Museum of medicinal
plants and an experimental garden of
medicinal plants including some rare and very
important exotic medicinal plants was
maintained for the purpose of verification and
comparative studies of standards.
(e) The Laboratory has also put eight volumes
of HPI on its web site.
(f) The Laboratory imparted orientation in
Homoeopathic Pharmacy to 744 students of
26 Homoeopathic medical colleges from
different parts of the country.
(g) The HPL maintained a seed bank of important
exotic medicinal plants.
(h) Under DSU Project of CCRH, standards have
been laid down for eight drugs.
7.8.3 During the current financial year 2008-2009,
allocations of Rs. 116.00 lakhs under Non Plan and
Rs. 116.00 lakhs under plan has been made.
414
ANNUAL REPORT 2008-09
7.9 Drugs Quality Control Cell(AYUSH)
7.9.1 A Drug Control Cell (AYUSH) is working inthe Department to deal with the matters pertainingto Drug Quality Control and regulation of Ayurveda,Siddha and Unani drugs under the provision of Drugsand Cosmetics Act, 1940 and Rules, 1945. The Cellis looking after the activities of Ayurveda, Siddha,Unani Drug Technical Advisory Board (ASUDTAB)and Ayurveda, Siddha, Unani Drugs ConsultativeCommittee (ASUDCC).
7.10 Centrally Sponsored Scheme for QualityControl of Ayurveda, Siddha, Unani and HomeopathyDrugs.
7.10.1 The Centrally Sponsored Scheme for QualityControl of Ayurveda, Siddha, Unani and Homeopathydrugs was implemented in the 9th Plan and continuedin 10th plan with the objective of strengthening/establishing of the infrastructure of Drug TestingLaboratories and Pharmacies of Ayurveda, Siddha,
Unani and Homeopathy drugs owned by the State
Government. 29 State Drug Testing Laboratories and
46 State ASU&H Pharmacies have been assisted sofar. The following initiatives have been taken up underthis scheme:
(a) Strengthening and establishing Ayurveda,Siddha, Unani and Homeopathy Pharmaciesof the State Governments/U.T.s for qualityAyurveda, Siddha, Unani and Homeopathydrugs.
(b) Strengthening and establishing Ayurveda,Siddha, Unani and Homeopathy Drug testinglaboratories (DTLs) in States/U.T.s
(c) Strengthening of State Drug Controllers ofASU&H Enforcement Mechanism.
(d) Providing financial assistance to Ayurveda,Siddha and Unani drug manufacturing units
to improve their infrastructure to meet Good
Manufacturing Practices (GMP) Schedule "T"
requirement.
Budgetary support 2007-08
State Drug Testing Laboratories 2 Nos. Rs.85 lakh
ASU&H Pharmacies 9 Nos. Rs.983.79 lakh
State Enforcement mechanism of ASU drugs 30 Nos. Rs.450.00 lakh
Sample Testing Fee 30 Nos. Rs.60.00 lakh
Good Manufacturing Practices of ASU&H units 5 units in 5 States Rs.11.23 lakh
Total Rs.1590.02 lakh
Budgetary support 2008-09 (Upto November, 2008)
State Drug Testing Laboratories 6 Nos. Rs.234.50 lakh
ASU&H Pharmacies 4 Nos. Rs.352.86 lakh
Total Rs.587.36 lakh
7.11 Ayurveda, Siddha, Unani DrugsTechnical Advisory Board(ASUDTAB) Reconstituted
7.11.1 Ayurveda, Siddha, Unani Drugs TechnicalAdvisory Board was reconstituted on 23.03.2007
under the Chairmanship of Dr. R.K. Srivastava,Director General of Health Services, Government ofIndia. The meeting of Ayurveda, Siddha, Unani DrugsTechnical Advisory Board held on 06.12.2007. Thefollowing issues were discussed:
415
ANNUAL REPORT 2008-09
(a) By-laws of Ayurveda, Siddha and Unani
Drugs Technical Advisory Board has been
approved.
(b) State Govt. have been directed to constitute
an expert committee for consultation
regarding licensing of patent and proprietory
of ASU products.
(c) A sub-committee has been constituted for
introduction of new definition under Drugs &
Cosmetics Act for incorporating new category
of ASU cosmetics. The meeting of the sub-
committee will be called soon.
(d) The guidelines of GMP of Rasaushadhies
(herbo-metallic preparation) of ASU drugs
have been prepared and final notification is
under issue.
(e) The order has been issued to all State
Governments not to use prefix and suffixes
with the classical formulation in patent and
proprietory ASU drugs.
(f) The Rule 169 of the Drugs & Cosmetics Rules
has been amended for allowing permitted
excipients, artificial sweeteners for use in
Ayurveda, Siddha and Unani drugs and
notification has been issued on 23.10.2008.
(g) Draft Notification for amending Rule 170 in
the Drugs & Cosmetics Rules for Guidelines
on evaluation of Ayurveda, Siddha and Unani
drugs and other traditional medicines of India
is under issue.
7.12 National Campaign on QualityAssurance of AYUSH drugs
7.12.1 The National Campaign was organized on 10-
11 June, 2008 at India Islamic Centre, Lodhi Road,
New Delhi, wherein all Stakeholders, State Drug
Controllers, Commissioners, FDAs dealing with ASU
drugs, Research Scientists working in CCRAS, CSIRand other Research Councils participated.
7.13 New initiatives in the 11th Plan
7.13.1 During the 11th plan the existing scheme ofQuality Control of ASU&H drugs has been revisedand is being implemented with the followingcomponents:
(a) Release of balance instalment of financialassistance sanctioned for establishment/strengthening of Drug Testing Laboratoriesand Pharmacies during the 10th Plan.
(b) Reimbursement of expenditure incurred byState Directorate of ISM&H/State Licensingauthorities for testing of Ayurveda, Siddha,Unani and Homoeopathy drugs samplesthrough NABL accredited/other approvedlaboratories for testing of heavy metals/pesticide residue/microbial load/identificationof ingredients etc.
(c) Reimbursement of expenditure incurred byStates for Strengthening of EnforcementMechanism of Ayurveda, Siddha and Unanidrugs at the State level and expenditureincurred in testing of ASU&H medicines byaccredited laboratories.
(d) Assistance to Ayurveda, Siddha & Unani(ASU) drug manufacturing units to establishan in-house quality control laboratory for thepurpose of quality control testing of all rawmaterials/finished products as perPharmacopoeial parameters including testingof ingredients/heavy metals/pesticideresidue/microbial load etc.
(e) Assistance to ASU&H manufacturing unitshaving a turnover of upto Rs.20.00 croresfor acquiring USFDA/EU Good ManufacturingPractices certification for their units.

416
ANNUAL REPORT 2008-09
417
ANNUAL REPORT 2008-09
Chapter 8
Ayurveda, Siddha, Unani and Homoeopathy drugs
industry at present suffers from small scale of
operation and low technology. Keeping this in view,
Department of AYUSH is emphasizing appropriate
technology and use of quality control capacity in the
private sector for upgradation of Ayurveda, Siddha,
Unani and Homoeopathy drugs industry. Good
Manufacturing Practices (GMP) have been made
mandatory for Ayurveda, Siddha and Unani medicines
from 2003 and for Homoeopathy medicines from
2007. Tie up with the private quality control
laboratories have been allowed under GMP. In the
11th Plan, the Department of AYUSH would be
providing back ended subsidy of Rs.30 lakh or 30%
of the project cost, whichever is lower, to Ayurveda,
Siddha, Unani and Homoeopathy drugs
manufacturing units for establishing their in-house
quality control laboratories or to upgrade their
manufacturing facilities to WHO standards. A Central
Sector Scheme for Common facilities for AYUSH
Industry Clusters has also been sanctioned in the
11th Plan for providing common testing facilities for
small and micro enterprises.
Central Govt. brought Ayurveda, Siddha, Unani and
Homoeopathy medicines within the purview of Drugs
and Cosmetics Act and Rules in early 1960s.
Pharmacopoeial Committees, Pharmacopoeial
laboratories and Research Councils were
established in 1970s. As a result pharmacopoeial
standards have been laid down for most of the widely
used medicinal plants and Homoeopathy Mother
Tincture. The work of laying down pharmacopoeial
standards for compound formulations is in hand.
8.1 There are 9228 licensed manufacturing units
in the country with an estimated total annual turnover
of around Rs.8800 crore (Table 2.2.3 and Figure
2.2.1). Most of the units (>90%) are in the small and
cottage scale sector with turnover of less than Rs.1
crore per annum. Less than 1% of the industries
have turnover of over Rs. 25 crore per annum. In
this top 1% segment, around 50 manufacturing units
have turnover in the range of Rs.150-800 crore per
annum. Since 2002, the Good Manufacturing
Practices (GMP) provisions of the Drugs & Cosmetics
Act and Rules have become applicable to the AYUSH
pharmaceutical industry. However, the R&D and
testing in most units is inadequate in terms of the
Quality Control standards prescribed under the Act.
According to a report by the EXIM Bank (2004),
around 70% of the Indian exports from the AYUSH
sector consist of raw materials with an estimated
value of Rs.1000 crore per annum. The balance
(around 30%) consists of finished products including
herbal extracts. The major challenge before the
AYUSH pharmaceutical industry is to transform itself
from a raw material supplier to a knowledge products
industry. This transformation will call for major
investments in upgrading processing technology,
R&D and quality control. It will also call for inter-
sectoral cooperation between AYUSH, CSIR, ICMR,
private sector R&D, NGOs and the Ministry of
Commerce.
AYUSH Pharmaceutical IndustryAYUSH Pharmaceutical IndustryAYUSH Pharmaceutical IndustryAYUSH Pharmaceutical IndustryAYUSH Pharmaceutical Industry
System wise details of Manufacturing Units
System Manufacturing Units
Ayurveda 7955
Unani 324
Siddha 302
Homoeopathy 647
Total 9228
Rs. 8800 crore as estimated in 2007 Demand & Supplyreport on Medicinal Plants.
418
ANNUAL REPORT 2008-09
System wise Details of Manufacturing Units
8.2 Indian Medicines PharmaceuticalCorporation Limited
8.2.1 IMPCL is a Government of India enterpriseunder the administrative control of the Departmentof AYUSH, Ministry of Health & Family Welfare havingits Registered office and Factory at Mohan, Distt.Almora (a notified backward area) Uttarakhand. TheCompany was incorporated in July 1978 and hadstarted its commercial production in June 1983. TheCompany is a 'MINI RATNA' has Authorized ShareCapital and the Paid-up Share Capital of Companyare Rs.700 lakhs.
8.2.2 The primary objective of the Company is tomanufacture and supply authentic quality Ayurvedic
and Unani products. The supply is being made for
use in Central Government Health Scheme (CGHS),
Government Hospitals, Dispensaries, various AYUSH
Research Councils. The company also sells its
products to various State Governments, other
institutions and also in the open market. Efforts are
being made to increase the Company's open market
sales with expansion of distribution net working.
8.2.3 The anticipated profit as per MOU target
(after tax provision) for the year 2008-09 is Rs.453
lakhs. The Audit work of Annual Accounts 2006-07 is
in progress. During the year 2007-08 the Sales of
the company was about Rs.1065 lakhs. The Target
sales for the year 2008-09 is fixed at Rs.2100 lakhs.
During the period 1.4.2008 to 31.08.2008, sales
amounted to 411 lakhs.
8.2.4 Modernization of the Corporation has been
taken up in a big way the phase of which is nearing
completion with construction of new and modern
buildings, procurement of new and state-of-art
equipment, plant and machinery to enhance
production. Quality Control instruments are being
procured to strengthen inhouse testing facility on
priority.
8.2.5 In consonance with medicinal plants mission,
efforts are on to upgrade the existing medicinal plants
garden and to create a cluster of medicinal plants
growers for synergizing their efforts to supply quality
raw material for the best prices.
419
ANNUAL REPORT 2008-09
Chapter 9
9.1.1 The irony is that while the world is recognizingthe benefits of Yoga and Ayurveda in particular, wein India seem to be jettisoning them in favour of theperceived quick relief systems. What were once thepreferred systems of health care for the masses areincreasingly getting confined to a small section ofwestern educated urban elite.
9.1.2 In this background, the Department ofAYUSH, which is mandated to develop, promote andpropagate the Indian System of Medicine &Homoeopathy, conceived of taking the message ofthe relevance of these systems across the lengthand breadth of the country through the medium ofnational campaigns.
9.1.3 It was decided to focus on specific areas ofstrength of different systems in order to developbroad themes for the national campaigns. During2007-08, such campaigns were launched on"Kharasutra for Ano-Rectal Disorders", "Ayurveda forGeriatric Care" and "Homoeopathy for Mother andChild Care" for the current year so far one campaignhas been launched on "Quality Assurance of ASU&HDrugs".
9.1.4 The broad format of the National Campaignsenvisages the launch of the campaigns by aworkshop in Delhi, followed by, workshops at the Statelevel and then at the district levels. Thus, a cascadingeffect is envisioned to spread the outcomes of theNational Workshop upto the district and thepanchayat levels. This has proved to be a verysuccessful model, if the response and feedback fromthe States is anything to go by.
9.1.5 The workshops are attended byrepresentatives form all the groups who have a stakein the subject matter. Broadly, they comprise of policymakers, implementers at the State and grassrootlevels, practitioners of traditional as well as modern
medicine, industry, etc. Technical sessions are heldon different topics, which are steered by a panel ofeminent speakers. The sessions are interactive andthe outcomes of each session are concretized at theend of the workshop as "Workshop Recommenda-tions", which form the basis for charting the futurecourse of action ranging from how to take thecampaign forward to the ways and means ofimplementing the recommendations arising out ofthese deliberations.
9.2 Ksharasutra for Ano-RectalDisorders
Information Education and CommunicationInformation Education and CommunicationInformation Education and CommunicationInformation Education and CommunicationInformation Education and Communication
9.2.1 Fistula-in-ano is a condition which has beenrecognized as a difficult surgical disease in all theancient and modern medical sciences of the world. Itis the recurrent nature of this disease which makesit difficult to treat. It has been categorized as asurgical condition and almost all the surgeons startingfrom Sushruta (about 1500 B.C. - India) toHippocrates (450 B.C. Greece) down to the surgeonsof present times have realized the challenge whichthis disease offers for its surgical/medical/medico-surgical methods of treatment.
9.2.2 Ksharasutra is an ancient Ayurvedictechnique for treating disorders of the anus andrectum. It is a para-surgical procedure involving

420
ANNUAL REPORT 2008-09
introduction of a medicated thread into fistulae ofthe ano-rectal area. The medicines coating thethread acts on the diseased areas.
9.2.3 As compared to this, surgical proceduresprescribed by modern medicine to treat this disorderespecially in chronic and complicated cases, arepainful, require prolonged hospitalization and oftenresult in disfigurement as affected areas are by andlarge excised, apart from having a higher degree ofrecurrence.
9.3 Primary objectives of theCampaign
! To sensitize all stake holders i.e. PolicyMakers, Program evaluators, OpinionMakers, Ayurvedic, Allopathic and otherAYUSH Physicians and NGOs regarding thestrengths of Ksharsutra therapy for Ano-rectal diseases.
! To provide a platform for exchange ofknowledge among Ayurvedic, Allopathic andother Physicians about the Ksharsutratherapy for Ano-rectal disorders.
! To set up Ksharsutra centers at Distt/Allopathic Hospitals, CHCs and medicalCollege Hospital and Ayurvedic Hospitals.
9.3.1 Secondary objectives
! Establish linkage among the Educational/Research Institutions, N.G.Os and the
clinicians to disseminate the efficacy ofKsharsutra in the management of Ano-rectaldisorders.
! Promote greater awareness amongAyurvedic, Allopathic and other practitionersin dealing with issues related to amazing roleof Ksharsutra in Ano-rectal disorders.
! Involve practitioners of other systems ofmedicine to orient them to the strengths ofAyurveda and the role of Ksharsutra therapyin treating Ano-rectal disorders, so thatproper referral system is developed to treatthese disorders with Ksharsutra.
! Generate faith among the general publicas well as the Ayurvedic physicians\Proctologists in Ksharsutra therapy.
9.4 State Level WorkshopsOrganized :
9.4.1 Sixteen national/State campaigns-cum-workshops have been organized during the yearunder report. They are Chhatishgarh, HimachalPradesh, Andhra Pradesh, Karnataka, Punjab,Kerala, Uttarakhand, Maharashtra, Rajasthan, westBengal, Gujarat, Jammu and Kashmir, Uttar Pradesh.
Chief Minister of Chhatisgarh Dr. Raman Singhinaugurating State campaign on 22nd November,
2007 at Raipur
421
ANNUAL REPORT 2008-09
9.4.2 Department of AYUSH has supported BanarasHindu University, Faculty of Ayurveda, Departmentof Shalya and have set up National Resource Centeron Ksharsutra at BHU-Varanasi with the followingobjectives :
! To Promote the Ksharsutra Therapy atNational and International Level
! To Develop National Referral Center forKsharsutra Therapy
! Manufacture and Supply StandardKsharsutra
! Human Resource Development - Teachingand training of PG diploma in Ksharsutra, MS(Ay) Shalya in Kshar evam anushastraKarma, PhD, CME, ROTP Programmes andtraining to both specialists of Ayurveda andModern medicine
! To Develop Central Data Recording System
! To Provide Research Platform to National andInternational bodies for the Development inthe area of Ksharsutra Therapy and Woundhealing
! To Conduct Epidemiological Study, ProvidePreventive measures and community services
! To establish Tele-medicinal Centers forKsharsutra
9.5 National Campaign onHomoeopathy for Mother andChild Care
9.5.1 The 2nd National Campaign was kick-startedby a 2-day Workshop on 5th - 6th November, 2007at the India Islamic Cultural Centre, New Delhi, withthe objective of sensitizing policy makers, medicalpractitioners of the Allopathic and Homoeopathicsystems of medicines, non-governmentalorganizations, industry and the common manregarding the strengths of Homoeopathy for the Careof Mother and Child.
9.5.2 The thrust of the campaign was to increaseawareness about the potential of Homoeopathy and
strengthen health care services through this systemfor women and children.
9.5.3 The health care needs of expectant andlactating mothers and their infants are very differentfrom that of the rest of the population. Homoeopathy,due to its gentle more of administration, palatabilityand free from side-effects can become a veryimportant health care alternative for this segment.Homeopathy has a strong presence in Kerala, WestBengal and the North East. There are 132 collegesimparting degree level education and 33 collegesoffering Post-Graduate education in Homoeopathyin the country. 220858 Registered Practitioners, 228Hospitals, 5770 Dispensaries. India has one of thebest infrastructures in Homoeopathy in the world; andwith 13000 graduates passing out every year in thediscipline, we have one of the largest trainedmanpower in the sector at the country's disposal.
9.5.4 Case studies of the scope of Homoeopathicinterventions during pregnancy, child birth,puerperium, antenatal and postnatal cases werepresented by distinguished homoeopaths like Dr.Diwan Harishchand, Dr. Joyce Frye from the USA,etc. The outreach efforts of NGO, like theMaharashtra based Dhawale Trust on communityhealth in remote rural areas of Maharashtra andGujarat were shared with the participants.
9.5.5 Prof. N.K. Ganguly, Director General, ICMRdisclosed that at the National AIDS Research Institute,Pune, a Homoeopathic drug has been formed to havea high anit-HIV activity.
9.5.6 A highlight of the workshop was the repeatedemphasis by the homoeopaths themselves on thelimitations of the system. The point was time andagain driven home that Homoeopathy was not apanacea and had very little to offer in complicatedcases requiring surgical intervention.
Some of the recommendations of the workshopwere:-
i. Setting up of a core group of homoeopathsand allopaths to list out the specific conditions,which can safely and effectively be treatedby Homoeopathy.
422
ANNUAL REPORT 2008-09
ii
ii
. Improving the quality of obstetric care andgynecological training given in HomoeopathicMedical Colleges.
i. Evolving a CME programme for practitionersexclusively on Mother and Child Care.
iv. Initiating a dialogue with the Medical Councilof India to provide for admission ofHomoeopathic graduated in PG courses ofPreventive & Social Medicine and CommunityMedicine.
v. Drawing up of orientation modules onHomoeopathy for allopathic doctors.
9.5.7 State level workshops have thereafter beenheld in Kerala, Tripura, Uttar Pradesh and AndhraPradesh. In Kerala the local Panchayats have evinceda keen interest in initiating special OPDs on motherand Child Care.
Hoarding on Homoeopathy for Mother and ChildCare at the Pragati Maidan Metro Station
9.6 National Campaign on GeriatricCare through Ayurveda
9.6.1 One of the most significant successes of thetwentieth century has been an increase in lifeexpectancy the world over mainly due to scientificand technological breakthroughs in medicine andhealth care. The downside of this increase in
longevity coupled with a decline in birth rates hasbeen an increase in the numbers of old people, oftensuffering from one or more chronic disorders withthe consequential increasing demand on PublicHealth Systems and on medical and social services.Given this backdrop although longevity may no longerbe an issue, however, the quality of life of the elderlyis certainly something we need to address. Chronicinflammatory and degenerative conditions such asArthritis, Diabetes, Osteoporosis, Alzheimer'sdisease, Depression, Psychiatric disorders,Parkinson's disease and Urinary incontinence thatthe elderly are prone to need special care but in acountry still grappling with meeting the basic needsof the people care of the elderly is not a priority issue,today. However thousands of years ago ourforefathers had actually developed a separatebranch in Ayurveda which is dedicated to the care ofthe elderly called Rasayana or Jara Chikitsa.
9.6.2 This provides numerous single/compoundherbal and herbo-mineral preparations havingdiversified affects on body systems indicated for thepromotion of health as well as treatment of variedproblems. Multiple actions on psycho- somatic setup that includes immuno-modulation (on immunesystem), antioxidant action( prevents bio-oxidationthere by checking age related disorders, autoimmune disorders, degenerative disorders) andadaptogenic affects (on psychoneuroendocrinesystem).
Metro hoarding on Ayurveda for Geriatric Care

423
ANNUAL REPORT 2008-09
The National Campaign on Geriatric Care throughAyurveda was launched by a 2-day workshop at theIndia Habitat Centre. 3 parallel sessions wereorganized, wherein over 600 delegates comprisingof experts, State AYUSH Directorates, HealthSecretaries/Commissioners participated. As a majoroutcome of this, it was decided to introduce a weeklyOPD dedicated to the elderly in all the states.Following this, in states like Himachal Pradesh everyTuesday has been designated in all the PHCs/CHCsas Geriatric OPD day. Other states have also adopedthis to varying degrees. State level geriatriccampaigns have been held in eleven statesthereafter.
9.7 National Campaign on DrugQuality Assurance
9.7.1 One of the major drawbacks that the ISM&Hsuffers from is the lack of trust of consumers in thequality of ASU&H drugs, who are therefore shyingaway from buying these medicines. This lack ofconfidence in the quality of medicines is hinderingus from capitalizing on the global opportunityprovided by increasing interest in traditional medicineall over the world. In India today, there is a need toeducate all the stakeholders in the sector startingwith the policymakers, planners, drug enforcementauthorities, drug manufacturers to consumers, abouthaving a robust quality control and enforcementregime in the country. Industry too needs to beeducated on the spin offs that will be generated interms of higher sales revenues if the consumer isassured of the quality of ASU&H medicines. Betterenforcement, will result in better quality, which willincrease the acceptability of the drugs among theconsumers leading to better profits for Industry, thusresulting in a win-win situation for all.
9.7.2 To address these concerns, the NationalCampaign on Quality Assurance of ASU&H Drugs waskick-started by a 2-days launch workshop at the IndiaIslamic Cultural Centre on 10th - 11th June, 2008.The objective of this Campaign was to strengthenthe ASU&H drug quality control in the Country on theone hand and to ensure the safe and quality medicineto the people on the other. The campaign provideda platform for the State ASU&H drug quality control
machinery, policy makers, manufacturers and expertsto share concerns and opinions to spell out suitablequality control mechanisms, which are efficacious,safe and easily implementable and find out ways andmeans of complying with quality standards bothnational and international for ensuring availability ofsafe and quality drugs to the people.
9.7.3 Recommendations:
1. State Governments who are responsible forenforcement of provisions of Drugs &Cosmetics Act with respect to ASU&H drugsshall strengthen their enforcement machineryfor discharge of their statutory responsibilityand avail of assistance provided byDepartment of AYUSH under the CentrallySponsored Scheme of Drug Quality Controlfor this purpose including testing of samplescollected from manufacturing units and retailstores.
2. Government of India have provided a grantof Rs.1.5 crore for upgradation of every StateDrug Testing laboratory but so far a largenumber of State Drug Testing laboratories arenot functional or not functioning at an optimallevel. State Governments shall immediatelymake the State Drug Testing laboratories fullyfunctional by providing requisite number oftrained drug quality control staff, notificationof State analysists and making arrangementsfor collection of survey and inspectionsamples, sending these samples to the StateDrug Testing laboratories for testing andfurther action. Pharmacopoeial Laboratoryof Indian Medicine has been arrangingtraining for officials of State Drug Testinglaboratories and all the State Governmentsshall make full use of this facility for makingthe State Drug Testing laboratories fullyfunctional.
3. State Governments which are not able tomake their drug testing laboratories functionalshall immediately enter into public privatepartnership with NABL laboratories/pharmacycolleges for making these State drug testinglaboratories fully functional failing which
424
ANNUAL REPORT 2008-09
Department of AYUSH may ask StateGovernments to refund the Central grantgiven to the States for upgradation of theirState drug testing laboratories.
Both the ASU&H Industries and theenforcement agencies should work closelyfor capacity building for transition from qualitycontrol mindset to quality assurance mindsetwhich includes process validation andconverting textual knowledge into processtechnology and documentation at every stageof the production cycle as per GMPrequirements.
4. Need for capacity building of ASU&H SMEsfor GMP compliance by training ofmanagement and quality control personneland engagement of experts as Consultantsand transparent procedures for GMPinspections and monitoring.
5. Need for Industry to create backward linkageswith farmers for cultivation of medicinal plantsbased on Good Agricultural Practices forensuring quality of raw material. Schemesof National Medicinal Plants Board can beutilized for cultivation and processing ofmedicinal plants.
6. ASU&H manufacturing units should mentioncompliance with official pharmacopoeias/formularies on the label of the product forconfidence building in consumers.
7. Greater utilization of NABL accreditedlaboratories and testing infrastructureavailable in the country by ASU&H industryand enforcement agencies.
8. Permissible excipients as per IndianPharmacopoeia should be allowed for moderndosage forms of ASU products subject torational use.
9. Shelf life studies need to be carried out forfixing of shelf life of ASU&H drugs.
10. Substitutes identified in variousPharmacopoeia / formularies should be
adopted by the Industry. There is a need forresearch for identifying alternative plant partslike leaves, fruits instead of roots and hard-wood which are destructive in nature.
11. SOPs of Bhasmas should be frozen andseparate GMPs of Rasa Aushadhies shouldbe identified.
12. Human resource development for ASU&Hindustry by starting ASU&H B.Pharma coursesand training of science graduates and postgraduates in quality control for ASU&Hproducts for utilization by industry.
13. National Campaign on Quality Assurance ofAYUSH drugs should be carried forward byorganization of regional/State levelworkshops to be jointly organized by regionalIndustry associations/NABL laboratories/ASU&H Directorates.
14. Creation of 'Quality Circles' for ASU&HIndustry in Centres of Excellence and GMPtraining in GMP compliant small and mediummanufacturing units.
9.7.4 It is hoped that launching of this NationalCampaign will create a quality assurance movementin AYUSH Sector for providing safe and qualityAyurveda, Siddha, Unani and Homoeopathymedicines to the Indian public as well as to capture afair share of the global market for herbal products.
9.8 AROGYA Fairs
9.8.1 Another initiative of the department topropagate Indian systems of medicine is organizationof Arogya Fairs which began in 2001 as an annualevent in Delhi held in October/November every year.
9.8.2 It has been our endeavour to add somethingnew to successive AROGYAs over the years, so whatbegan as an exhibition of AYUSH products in 2001has expanded to include literature on AYUSH, medicalequipment, publishers and booksellers of AYUSHsystems apart from events which are organized onthe sidelines of A R O G YA like conferences onTraditional Medicine. This year, as part of the on goingIndian effort to reach an understanding with ASEAN

425
ANNUAL REPORT 2008-09
countries, on various sectors of trade and commerce,the Department of AYUSH hosted an Indo-ASEANconclave on Traditional Medicine. Given the vitalityof traditional medicine systems in both the Indiansubcontinent and the rest of South East Asia, it isonly natural that we share each others strengths inthe sector and establish a synergistic relationshipfor the growth and development of TraditionalMedicine. More than 35 delegates from all the 10ASEAN nations participated in the 2 day conferencewhich comprised of lectures from well known experts,panel discussions and interactive sessions.
The popularity of Arogya fairs was such thatmanufacturers of AYUSH drugs felt that such fairsshould be held more often. This prompted theinclusion of holding regional arogyas in the 11th planas a major policy plank. Thus Arogyas are now nolonger confined to Delhi but also have their regionalavtars in the form of State level Arogyas. In the pastyear such fairs were held in Nellore, Coimbatore,Dehradun and Jaipur. In the latter it was held as partof the World Ayurveda Congress while in Dehradunit formed an integral part of the annual cultural festivalcalled Virasat organized with the patronage of theState Government. It is felt that the number of peoplewho get benefited by arogya fairs increases manifoldwhen they are held as part of an existing and wellestablished cultural activity which have their ownclientele rather than when organized as stand aloneexhibitions.
9.9 Awareness drives on AYUSHSystems
9.9.1 The department has over the past yearproduced short films of 8-10 minutes duration onthe following aspects:
! Anxiety Neurosis
! Arthritis
! Ano-rectal disease
! Skin disorders
! Ayurveda as a health care system
9.9.2 Besides these advertisement spots havebeen produced on Homoeopathy for mother and childcare, Unani for skin care, ayurveda for geriatric care,Good Manufacturing Practices (GMP), Misleadingadvertisements, Drugs and Magic Remedies Act andlabeling of AYUSH drugs. These were telecast overDoor Darshan, Star TV, ETV, National Geographic,Lok sabha TV and other channels.
9.9.3 Awareness drives on Ayush systems werelaunched through advertising on railway tickets andby putting up panels in metro stations and metrocoaches.
9.9.4 Apart from all the above IEC material hasbeen printed and distributed/sold to interestedpeople through the department as well as theCouncils and National Institutes. A list is provided atAnnexure I at the end of Annual Report.

426
ANNUAL REPORT 2008-09
427
ANNUAL REPORT 2008-09
Chapter 10
10.1 In keeping with the mandate of the NationalPolicy the Government of India has been striving forthe promotion and propagation of Indian System ofMedicine abroad. The efforts have gained momentumafter the establishment of a separate Department ofIndian Systems of Medicine & Homoeopathy in 1995.Especially in the context of issues highlighted in therecent past by journals like JAMA and Lancet andthe subsequent ban of certain ASU & H drugs in someof the countries, the Department has taken initiativesto sensitize the world community about strengths andefficacy of Indian Medicine Systems.
10.2 The Department was allocated a sum ofRs.150.00 lakhs (BE) in 2006-07 which wasenhanced to Rs.500.00 lakhs (BE) in 2007-08 underits plan scheme viz. the International ExchangeProgramme. A sum of Rs.600.00 lakhs has been keptin BE 2008-09 for the operation of the followingInternational Cooperation Activities :-
i) International exchange of experts andofficers.
ii
ii
) Incentive to drug manufacturers,entrepreneurs, AYUSH institutions etc. forinternational propagation of AYUSH andregistration of their products by USFDA/EMEA/UK-MHRA for exports.
i) Support for international market developmentand AYUSH promotion-related activities.
iv) Promotion of Ayurveda, Homoeopathy, Unaniand Yoga abroad through young PostGraduates.
v) Translation and publication of AYUSH booksin foreign languages.
vi) Establishment of AYUSH information Cells/
Health Centres in Indian Embassies /Missionsand in the Cultural Centres set up by ICCRin foreign countries and deputation ofexperts.
vii) International Fellowship Programme forforeign nationals for undertaking AYUSHcourses in premier institutions in India.
10.3 Achievements in the InternationalCooperation:
10.3.1 Collaboration with China
A Memorandum of Understanding (MoU) with theState Administration of Traditional Chinese Medicine,China was signed on 14th January 2008 for bilateralcooperation for promotion of Traditional Medicine.The MoU envisages bilateral cooperation in thepolicies relating to regulation and administration oftraditional medicine in India and China,standardization of herbal medicines, collaborativeresearch in drug development, and development ofcommon strategies for creating greater awarenessabout the safety and efficacy of traditional medicineproducts.
10.3.2 Collaboration with Russia
A high level delegation comprising of HealthCommittee of Government of St. Petersburg Russiavisited the Department of AYUSH to identify avenuesof cooperation for setting up Ayurvedic Centre/Clinicsin St. Petersburg and to promote Ayurveda in Russia.Dr. Ishwar V. Basavaraddi, Director, Morarji DesaiNational Institute of Yoga, New Delhi and Dr. M.S.Baghel, Director, Institute for Post GraduateTeaching and Research in Ayurveda, University ofGujarat, Jamnagar had visited St. Petersburg toattend the Annual Ayurvedic Conference organizedby Government Institute of Ayurvedic Medicine under
International CooperationInternational CooperationInternational CooperationInternational CooperationInternational Cooperation
428
ANNUAL REPORT 2008-09
St. Petersburg Medical Academy during June- July,2008. During this exchange of delegations threeMoUs have been signed between the GovernmentInstitute of Ayurvedic Medicine, St. Petersburg andIndian Institutes namely National Institute of Ayurveda,Jaipur, Central Council for Research in Ayurveda andSiddha, New Delhi and Morarji Desai National Instituteof Yoga, New Delhi.
10.3.3 Ayurveda Experts deputed to Hungary
An Ayurveda expert and two assistants were deputedto Hungary during May-July, 2008 on request of anNGO based in Hungary to conduct AyurvedaProgrammes on authentic training of Ayurveda healthcare, massage and Panchakarma methods to healthpersonnel and masseurs of wellness units and spas.
10.3.4 Inter-Ministerial Task Force Meeting
The 2nd meeting of the Inter-Ministerial Task Forceconstituted by Department of AYUSH for Promotionof Traditional Indian Medicine in other countries washeld in the Department of AYUSH on 5th Feb, 2008.under the Chairpersonship of Secretary (AYUSH).Shri Swashpawan Singh, Ambassador, PMI, Genevawas the special invitee. Representatives of variousDepartments/Ministries attended the meeting. Apresentation on the International Cooperation ActionPlan for 2007-2009 was made which focused on keyareas like education, research, trade, commerce ®ulatory affairs, interface with bilateral andmultilateral fora and propagation of AYUSH systems.Secretary (AYUSH) sought cooperation from all themembers for identification of focus countries, creationof a database of NGOs working for AYUSH in foreigncountries and AYUSH experts for internationalcooperation activities.
10.3.5 Ayurveda CME Courses in the U.S.
Department of AYUSH has been receiving a numberof requests from foreign institutions for deputationof Ayurveda teachers. The Department deputed twoexperts in 2007 for a period of one month to USA todeliver lectures to medical students under ContinuingMedical Education (CME) modular teaching at theMedical Schools of University of Connecticut andUniversity of Washington. An expert was deputed
during April-June, 2008 to conduct a CME course inUniversity of Connecticut. The Expert also visitedMayo Clinic at Rochester, Minnesota for talks onfuture collaborations
10.3.6 Participation in WIPO- IGC
Secretary, Department of AYUSH participated in the13th Session of the WIPO's IntergovernmentalCommittee on Intellectual Property and GeneticResources, Traditional Knowledge and Folklore from13-17 October 2008 in Geneva, Switzerland
10.3.7 Indo-US Centre for Research on IndianSystem of Medicine (CRISM) at University ofMississippi, USA.
i) The Department of AYUSH has signed aMemorandum of Understanding with theUniversity of Mississippi, USA on 21st August2008 for cooperation in the field of'Development of Ayurveda-Siddha-UnaniHerbal and Botanical Products of GlobalStandards'. Under the aegis of this MoU anIndo-US Centre for Research in IndianSystems of Medicine (CRISM) will be set upin the National Centre for Natural ProductsResearch (NCNPR), University of Mississippi,USA.
ii
ii
) The CRISM is proposed to be a Center ofExcellence for trilateral cooperation forcollaborative research and advocacy forIndian Systems of Medicine betweenDepartment of AYUSH, Indian Institute ofIntegrative Medicine (IIIM), Jammu, andNCNPR.
i) The NCNPR has an institutional interface withUS-FDA which will facilitate Ayurveda, Siddhaand Unani drug manufacturing companies toget their herbal medicines/food supplementsregistered on the basis of Common technicaldossiers to be prepared jointly by CRISM andASU Industry partners. Prof. Larry Walker andProf. Ikhlas Khan of NCNPR will be theDirector and Co-Director from US side andDirector, IIM, Jammu, Adviser (Ayurveda),Deptt. of AYUSH and Director, Central Council
429
ANNUAL REPORT 2008-09
for Research in Unani Medicine, will be theDirector and Co-Directors from Indian sideof this Centre. The progress of collaborativeresearch and advocacy for Indian systemsof medicine will be jointly monitored bySecretary (AYUSH) and Prof. Larry Walker,Director, NCNPR. The activities of this Centrewill be jointly funded by Department of AYUSHand NCNPR
10.4 Visits of officials of Department of AYUSHAbroad
1) Dr. D.R. Lohar, Director PLIM, Ghaziabadattended the 11th Round of Technical LevelNegotiations on Comprehensive EconomicPartnership Agreement (CEPA) between Indiaand Sri Lanka held in Sri Lanka on 2nd to4th January 2008
2) A delegation from the Dept. of AYUSH led bySh. Verghese Samuel visited USA from 5thto 12th March, 2008 in connection with theestablishment of a Center for Research inIndian System of Medicine (CRISM) at theUniversity of Mississippi, USA
3) A delegation from the Department of AYUSHparticipated in the 12th South Asian Healthcare show at Kuala Lumpur, Malaysia on 12thto 14th March, 2008
4) Dr. M.C. Sharma, Director, NIA, Jaipur, visitedBerlin as a member of Scientific AdvisoryBoard of Deutsche Academy of AyurvedaMedizin, Berlin on 13th to 19th March, 2008
5) The Department was represented by Dr. AjaySharma, Prof. & Head, NIA, Jaipur, in 'Indiain Serbia' Trade Manifestation organized bySerbian Chamber of Commerce on 8th-11thApril, 2008
6) Dr. Tanuja Nesari, an Ayurveda expert wasdeputed to University of Connecticut MedicalSchool, USA for conducting a CME courseon Ayurveda from 23rd April to 6th June, 2008
7) Dr. Surinder Katoch, an Ayurveda expert andtwo Panchkarma Assistants were deputed for
six weeks from 27th May to 11th July, 2008on request of an NGO's in Hungary workingfor promotion and propagation of Ayurveda.
8) Dr. D.D. Sharma, Director, Department ofAYUSH was deputed to attend the 3rd JointWorking Group Meeting on pharmaceuticals& Biotechnology held in Brussels, Belgiumfrom 2-3rd June, 2008
9) Dr. H.M. Chandola, Professor, GujaratAyurveda University, Jamnagar, was deputedto Poland from 2nd to 6th June , 2008 toattend the Conference on Diabetesorganized by the Polish Association ofDiabetics in Dabrowa Gornicza, Poland.
10) Shri S.K. Chadha, Director, Department ofAYUSH was deputed for training at theGlobal Intellectual Property AcademyProgramme on Patent at USPTO Alexandra,Virginia Headquarter from June 23-27, 2008
11) Prof. M.S. Baghel, Director, IPGTRA, GujaratAyurveda University and Dr. Ishwar V.Basavaraddi, Director, MDNIY, attended theAnnual Ayurvedic Conference 2008 heldfrom 30th June to 4th July, 2008 in St.Petersburg, Russia
12) Smt. Anita Das, Secretary (AYUSH) and Dr.G.S. Lavekar, Director CCRAS visited Chinafrom 4th-8th July, 2008 to discuss the broadareas of cooperation between the twocountries in the field of traditional medicinein pursuance of the MoU signed between thetwo countries in January, 2008
13) A three member delegation participated in theIndia Fair, Bangkok held from 24-27 July,2008
14) A three member delegation led by Dr. G.S.Lavekar, Director CCRAS attended thesecond Ayurveda Conference organized byCollege of Ayurveda (U.K.), MiddlesexUniversity on 26th & 27th July, 2008 inLondon.
15) A five member delegation led by Dr. I.V.
430
ANNUAL REPORT 2008-09
Basavaraddi, Director, MDNIY participated inWoodstock Festival held from 30th July to3rd August, 2008. The Woodstock festivalwas organized under 'The Days of India inPoland 2008'.
16) Prof. PK Debnath was deputed to Cameroonto attend the panel discussion of the 6thCommemoration of the African TraditionalMedicine (ATM) Day on 31st August 2008.
17) Dr. D.D. Sharma, Director and Dr. D.R. Lohar,Director, PLIM of this Department weredeputed to attend the 13th InternationalConference of Drug Regulatory Authorities(ICDRA) from 16th to 19th September 2008at Bern (Switzerland).
18) Sh. Shiv Basant, Joint Secretary, Departmentof AYUSH attended the Round Table Meetingon Indo-Europe Pharma Industry held on22nd September 2008 at Brussels, Belgium.He also attended the meeting with thePharma Industry on 23rd September 2008after the Round Table Meeting was over.
19) Sh. Verghese Samuel, Joint Secretary,Department of AYUSH attended theAssemblies of member states of WIPO- 45thSeries of Meetings held in Geneva from 24-27th September 2008.
20) Smt. Anita Das, Secretary (AYUSH),attended the thirteenth (13th) Session ofIntergovernmental Committee (IGC) onIntellectual Property and Genetic Resources,Traditional Knowledge and Folklore held atGeneva from 13th to 17th October, 2008.
21) Dr. Rama Shankar Pathak, Research Officerwas deputed to participate in the InternationalTraining Workshop on Study andDevelopment of Traditional Ethno medicineat Guizhou Province, China held from l8thto 31st October 2008.
22) Sh. B.S. Sajwan, Chief Executive Officer,National Medicine of Plant Board, Departmentof AYUSH and Dr. Ravindra Singh R.O. (Sr.
Chemist), Central Council for Research inAyurveda were deputed to participate ASUIndustry in Supply Side West Show held atLas Vegas, USA from 22-24th October,2008.
23) Prof. Abhimanyu Kumar, Professor & Head,Department of Balrog (Ayurvedic Pediatrics),National Institute of Ayurveda, Jaipur wasdeputed to attend the Ayurveda Symposium" Namaste Ayurveda" in the Indian Embassy,Berlin, Germany held on 24th October, 2008.
24) Dr. Mohammed Khalid Siddiqui, Director,Central Council for Research in UnaniMedicine was deputed to attend theInternational Congress of Traditional andComplementary Medicine, Iran which washeld from October, 28th to 31st at 2008 atSari, Mazandraran, Iran.
25) Sh. Verghese Samuel Joint Secretary,Department of AYUSH , Dr. D.R. Lohar,Director, PLIM and Dr. Manoj Nesaeri, Dy.Adviser (Ay.) attended the WHO Congresson Traditional Medicine in Beijing from 7th-9th Nov, 2008.
26) Dr.G.S. Lavekar, Central Council forResearch in Ayurveda & Siddha, New Delhiwas deputed to attend the Global Bio-HerbsEconomic Forum 2008" at PutrajayaInternational Convention Centre, Malaysiafrom November, 15-17, 2008.
27) Dr. S.H. Acharya, Programme Officer,International Center for Ayurvedic Studiesand Head, Panchakarma Department,Gujarat Ayurved University was deputed toUSA where he had participated in groupscientific interaction and delivered lecturesat Osher Center for Integrative Medicine,University of California, San Francisco from1-6th November, 2008.
28) Prof. M.A. Jafri, Director, NIUM, Dr. B.Ravishankar, Head, Pharmacology, IPGTRA& Dr. M. Fazil Khan, Research Officer, CCRUMparticipated in a Seminar on "IndianTraditional Forms of Medicine" Organised by
431
ANNUAL REPORT 2008-09
the Indian Embassy in Muscat on 16thNovember, 2008.
29) Dr. Mohd. Khalid Siddiqui, Director, CCRUMand Dr. A. Pasha, Dy. Adviser (Unani),Department of AYUSH were deputed toparticipate in the International IntegratedMedicine Conference held in Karachi from24-26th November, 2008.
10.5 Visits of Foreign Delegations toDepartment of AYUSH
1) A two member German delegation visited theDepartment of AYUSH on 21st April, 2008, toexplore the collaborative activities forpromotion of Ayurveda in Germany.
2) A high level delegation comprising ofMembers of Health Committee ofGovernment of St. Petersburg, Russiavisited India from 29th April to 5th May,2008. MOUs were signed by the GovernmentInstitute of Ayurvedic Medicine, Mechnikovawith National Institute of Ayurveda, Jaipur andCCRAS, New Delhi.
3) A seven member delegation from Nigeria ona study tour visited India from 17th to 23rdMay, 2008, for the development, promotionand commercialization of Herbal medicinalproducts in Nigeria. Various issues forcollaboration between the two countries, inthe field of traditional medicine werediscussed.
4) A high level delegation from Bhutan led byDirector, Health Services visited India in June,2008 to explore possibilities for cooperationwithin the area of Traditional Medicine. India
and Bhutan share Sowa Rigpa system ofMedicine, which is practiced in trans-Himalayan regions and has lots of similaritieswith Ayurveda
5) Mr. Josef Brinckmann, Consultant, and Ms.Shitaye Lemma, Programme coordinator,International Trade Centre, Geneva visitedIndia during 14th -17th July, 2008. The reporton the Needs Assessment Study preparedby Mr. Brinckmann to prioritize the activitiesfor project development by ITC was discussedduring the meetings held.
6) Prof. Larry Walker and Prof. Ikhlas Khan ofNational Centre for Natural ProductsResearch (NCNPR), University of Mississippi,USA. visited the Department on 21st August2008 and signed a Memorandum ofUnderstanding for cooperation in the field of'Development of Ayurveda-Siddha-UnaniHerbal and Botanical Products of GlobalStandards'. Under the aegis of this MoU anIndo-US Centre for Research in IndianSystems of Medicine (CRISM) will be set upat the NCNPR.
7) Dr. Amala Guha, Asstt. Professor ofImmunology and Medicine, Director ofComplementary & Alternative SupportiveCare, University of Connecticut School ofMedicine, Connecticut visited the Departmenton 4th Nov, 2008 .
8) A three member Swiss delegation led by Sh.Felix Addor, Dy. Director General, SwissFederal Institute of Intellectual Propertyvisited the Department on 18th November,2008 to discuss IPR related bilateral issues.

432
ANNUAL REPORT 2008-09
433
ANNUAL REPORT 2008-09
Chapter 11
Mainstreaming of AYUSH inMainstreaming of AYUSH inMainstreaming of AYUSH inMainstreaming of AYUSH inMainstreaming of AYUSH inNational Health CareNational Health CareNational Health CareNational Health CareNational Health Care
11.1 Mainstreaming of AYUSH
11.1.1 Mainstreaming of AYUSH is one of thestrategies envisaged under National Rural HealthMission with an objective to improve outreach andquality of health delivery in rural areas. UnderNational Rural Health Mission, AYUSH doctors andfacilities are being co-opted in PHCs, CHCs andDistrict Hospitals. At the CHC level two rooms shallbe provided separately for AYUSH practitioner andpharmacist under the Indian Public Health Standards(IPHS) model. At the same time, single Doctor PHCsshall be upgraded to two Doctor PHCs by inductingan AYUSH practitioner at that level.
11.1.2 The guidelines to include AYUSH practitionersat all levels in NRHM including state Health Mission,District Mission and Rogi Kalyan Samitis have beenissued. It is also intended to have total functionalintegration between the AYUSH dispensaries/hospitals and the health care facilities under theallopathic system so that the entire spectrum oftreatments is made available to the rural poor ataffordable costs under one roof.
11.1.3 In the roadmap for mainstreaming of AYUSHcirculated to States it has been clearly spelt out thatwhile re-locating AYUSH dispensaries and on hiringof AYUSH doctors on contractual basis, emphasisshould be given to placement of AYUSH doctors inno doctor or single doctor PHCs. However, actualdeployment of AYUSH doctors is left to the discretionof the States.
11.1.4 Drug kit provided to ASHA contains oneAYUSH preparation in the form of iron supplement"Punarnnavadi Mandur". Other drugs, which are usedin the treatment of common diseases, control of
communicable diseases, as well as drugs promotingmaternal and child health as well as improving qualityof life could be included subsequently. Jointmonitoring visits to health centers to be undertakenby both AYUSH and Health Care Officials at theDistrict level and State levels.
11.1.5 27 States projected Mainstreaming of AYUSHcomponents in the Integrated ProgrammeImplementation Plan (PIPs) under NRHM for theyear 2008-09. Funds were sanctioned underCentrally Sponsored Scheme of Hospitals andDispensaries for creating infrastructure,equipments, machinery and for procuring medicinesat AYUSH facilities in PHCs/CHCs/ DHs. Rs. 70Crores have been sanctioned for contractual hiringof Manpower and training under NRHM Missionflexipool during 2008-09. Under NRHM, more than4000 AYUSH doctors are placed at various PublicHealth Care facilities
11.1.6 A Manual for Doctors on Mainstreaming ofAYUSH under NRHM was published by theDepartment for orienting and sensitizing AYUSHdoctors on their role and responsibility underMainstreaming and NRHM. A national level Trainingof Trainers (TOT) was also initiated by theDepartment with the collaboration of National Instituteof Health and Family Welfare (Munirka), Munirka forconducting a cascade of training activities onMainstreaming.
11.1.7 AYUSH doctors are required to be involvedin health promotion, supervisory activities and allNational Health Care programmes, especially in thepriority areas like MCH etc. It is also envisaged fortraining of AYUSH doctors in Primary Health Careand National Disease Control Programmes.
434
ANNUAL REPORT 2008-09
11.1.8 Revitalization of Local Health Traditions(LHT) is also one of the thrust areas under NRHM.Department of AYUSH supports eligible organizationsunder Central Sector Scheme of survey,documentation and Revitalization of Local HealthTraditions available in various parts of the country.
11.1.9 In order to evaluate the outcome ofMainstreaming of AYUSH in the country, Department ofAYUSH assisted some agencies for evaluating the co-location and integration of AYUSH into health careinfrastructure in States like Maharashtra, Rajasthan etc.
11.2 AYUSH Component in CentralGovernment Health Scheme
11.2.1 AYUSH systems of medicines and its practicesare well accepted by the community and have theirown areas of strength. Medicines are easily availableand prepared from locally available recourses,economical, and comparatively safe from side effects.Because of this fact, the Central Government HealthScheme, introduced in 1954 with only Allopathicdispensaries has introduced as AYUSH componentin its net work.
Sl. No. Systems of Medicine Year
1. Ayurveda 1964
2. Homoeopathy 1967-68
3. Unani 1974-75
4. Siddha 1980-81
11.2.2 Effectiveness of these systems in certaindiseases and conditions for which the AllopathicSystem does not have effective treatments hasgenerated a demand for more such facilities indifferent parts of the country and at present thefollowing facilities are available in the CGHS.
Sl.No Systems of No. ofMedicine dispensaries unit
1. Homoeopathy 36
2. Ayurveda 32
3. Unani 09
4. Siddha 02
5. Yoga 03
11.3 Centrally Sponsored Schemefor AYUSH Hospitals andDispensaries
11.3.1 A Centrally Sponsored Scheme for Promoting
Development of Health Care facilities of Ayurveda,
Yoga and Naturopathy, Unani, Siddha and
Homoeopathy (commonly referred to as the Hospitals
and Dispensaries Scheme) was introduced during
the 10th Plan with the specific objective of promoting
the public health with greater access to AYUSH health
services and in order to encourage the integration
of these systems with the mainstreaming of health
care services. Under the scheme, financial
assistance is provided for setting up general and
specialized AYUSH treatment centers in Allopathic
Hospitals and for the procurement of AYUSH Drugs
and Medicines for AYUSH Dispensaries located in
rural areas. Based on the experience of
implementation of the scheme during the 10th Plan
and on the basis of an independent outside
evaluation, the scheme has been modified and is
being implemented in the 11th Plan. During the 11th
Plan period a budget provision Rs.568.78 crores has
been kept and in the current financial year 2008-09,
there is an outlay of Rs.120.00 crores to implement
the components of the scheme.
11.4 Establishment of SpecializedClinics of AYUSH in CentralGovernment Hospitals
11.4.1 Specialized Clinics in Ayurveda and
Homoeopathy in Safdarjung Hospital and in Unani
and Yoga and Naturopathy in the Dr. Ram Manohar
Lohia Hospital continue to provide services to the
public.. These clinics are being run on experimental
basis by the three Research Councils viz., CCRAS,
CCRH and CCRUM. These clines are attended by a
large number of patients especially those with chronic
diseases.
435
ANNUAL REPORT 2008-09
Chapter 12
12.1 The Department of AYUSH is in the processof upgrading its website to make it dynamic, easilynavigable and user friendly. A unit of NIC is set up inthe department which is responsible for the website.The websites of its subordinate offices, autonomousbodies, National institutes, and regulatory councilsare now hyperlinked with the Departmental site.
12.2 Traditional Knowledge DigitalLibrary (TKDL)
12.2.1 Traditional Knowledge Digital Library (TKDL)is a collaborative project of the Department of AYUSHand the Council of Scientific and Industrial Research(CSIR) and is being implemented by CSIR. The mainobjective of this globally renowned project is toprevent misappropriation of India's rich heritage oftraditional medical knowledge. Since, the traditionalknowledge exists in languages such as Sanskrit,Urdu, Arabic, Persian, Tamil, etc., it is neither availablenor understood by Patent examiners in theInternational Patent Offices (IPOs). TKDL acts as abridge between the local languages and theInternational Patent examiners and will help inpreventing the misappropriation taking place at IPOs.
12.2.2 For creation of the TKDL database, aclassification tool, called the Traditional KnowledgeResource Classification (TKRC) was created. Thistool will not only enable the data entry into thesoftware using Unicode, but will also help the Patentexaminers in data retrieval since concordance hasbeen developed between TKRC and InternationalPatent classification (IPC).
12.2.3 TKDL (Ayurveda)
Activities under the second phase of TKDL Ayurvedawere initiated in August 2004 after the completion ofthe first Phase on 36,000 formulations from 14
authentic Ayurveda texts. A team comprising 10
Ayurveda Experts, 4 Junior Ayurveda Experts, and 4
Patent Examiners are engaged in the project. The
second phase involves identification of 65,000
formulations and transcription of new formulations
from 45 Ayurveda texts. So far, 1,03,600 formulations
have been identified and checked for duplicates,
81,300 formulations have been transcribed, 78,300
formulations have been edited, 74,400 formulations
have been validated and 56,000 formulations have
been freezed.
12.2.4 TKDL (Unani)
Activities under TKDL Unani System of Medicine were
initiated in June, 2004. An interdisciplinary team of
11 Unani Experts, 15 Junior Unani Experts and 3 IT
Experts are working in the project. The transcription
of formulations is being carried out from 19 Unani
books having 67 volumes, which are in Urdu, Arabic
and Persian languages in the patent application
format and in 5 languages. Out of the targeted one
lakh seventeen thousand formulations, approximately
1,13,200 formulations have been identified, 1,09,500
formulations have been transcribed, 1,01,900
formulations have been edited, 82,900 have been
peer reviewed and 46,400 formulations have been
freezed.
12.2.5 TKDL (Siddha)
Four Siddha Experts, five Junior Siddha Experts and
four Project Assistants (IT Experts) are working for
the project. So far 12,200 formulations have been
identified, transcribed and edited, and 800
formulations have been peer reviewed. TKDL Siddha
targets 12,500 formulations from 45 Tamil texts.
Information TechnologyInformation TechnologyInformation TechnologyInformation TechnologyInformation Technology

436
ANNUAL REPORT 2008-09
12.2.6 TKDL (Yoga)
W ith respect to Yoga out of the targeted 1500 asanasand postures from 20 texts, 600 asanas and postureshave been transcribed. Videography clippings foreach of the posture and asana will also be integratedalong with the transcriptions.
12.2.7 Access to International Patent Offices
EPO in 2005, had requested for the access to theTKDL database. The Cabinet Committee hadapproved the proposal in June 2006 for providingthe TKDL database to the International PatentOffices under non-disclosure agreement.Negotiations with European Patent Office (EPO) andUnited States Patent and Trademark Office (USPTO)are at mature stage for providing access to the TKDLdatabase to International Patent Offices. TheAccess Agreement which was vetted at variouslevels was sent to EPO and USPTO. USPTO soughtsome clarifications on the Access Agreement. Themajor points of clarifications sought by EPO andUSPTO relates to automatic extension of the termof use instead of three years, on usage of TKDL
for all patent grant procedures, on usage of TKDLas a prior art tool, disagreeing to indemnificationclause and have desired for a simpler arbitrationprocedures.
12.2.8 The response was submitted by India afterviews were taken in the Access Policy IssueCommittee held in June, 2007 and after seeking legalopinion. EPO has sent its response in June, 2008wherein they have agreed to most of the pointsmentioned in the Access Agreement and have soughtminor modifications of the agreement. It is likely thatthe Access Agreement may be signed in December,2008. The clarifications again sought by USPTO hasbeen responded and it is likely that the AccessAgreement with USPTO would get concluded by early2009.
12.2.9 Access to TKDL to EPO and USPTO patentexaminers would have direct impact on at least 43pipe line cases TK based patent applications at EPOwhich would not get granted. Similarly, the TKDL teamhas carried out detailed studies of the USPTO andfound approx. 40 pipeline cases for getting the patentrights, which will get rejected once access is given toUSPTO.
437
ANNUAL REPORT 2008-09
Chapter 13
13.1 The Department of AYUSH, places dueimportance on gender issues and attaches priorityto diseases of women in its research programmesparticularly in Clinical Research. The ResearchCouncils under the Department have been carryingout Research on various subjects that have abearing on Women Health Care. As a result of suchresearch nine Ayurvedic and five Unani drugs aresupplied under the National Reproductive Child Heath(RCH) Programme being implemented by theDepartment of Family Welfare. These drugs havebeen identified for the treatment of common ailmentsof pregnant women, adoloscent girls and children.Similarly, under National Rural Health Mission oneAyurvedic drug 'Punarnavadi Mandura' for anaemiafor pregnant women and adolescent girls is includedin the ASHA Kit.
13.2 Promotional and Contractual FarmingSchemes of National Medicinal Plant Board alsoprovide significant avenues for income generationfor women. Cultivation of medicinal plants is the keyto quality, efficacy and safety of the AYUSH systemsof medicines. Integrating medicinal plants in thefarming systems also offers an option of cropdiversification and to enhance incomes of farmersincluding women and children.
13.3 National Institute of Ayurveda (NIA), Jaipurprovided for an amount of Rs.57.01 lakhs under Non-Plan for salary and Rs.61.01 lakhs under Plan forsalary and stipend in the women component of theBudget of the Institute.
13.4 At National Institute of Siddha (NIS), Chennai,on an average 1100 - 1200 patients reported dailyat OPD from all groups of economic strata fortreatment. Of the total OPD attendance of 3,49,696in 2007-08, the female patients component was1,66,241. Out of the total of 1.6 lakhs treated at OPD
from 1st April, 2008 to 31st August, 2008, about 40%were women.
13.5 At National Institute of Homoeopathy (NIH),Kolkata, during the financial year 2007-08, about 1.60lakhs patients attended OPD and 681 patients weretreated in IPD, out of which about 30-35% werewomen.
13.6 The Institute for Post Graduate Teaching andResearch in Ayurveda (IPGT&RA), Jamnagar, has awell managed hospital OPD and IPD facilities. Duringthe reporting period, a total of 1,24,851 patients weretreated as outdoor patients which included 61,134women and 7,461 children. Out of the nearly 50,638patients given Panchkarma treatment performed24,276 were women..
13.7 At present about 459 colleges for the UnderGraduate and Post Graduate level exist under theDepartment of AYUSH. These colleges and NationalInstitutes of AYUSH have about 40% womenstudents.
13.8. The hospital functioning under the CentralCouncil for Research in Ayurveda and Siddha(CCRAS provided medical aid at OPD level to about2.50 lakhs patients out of which about 30- 40% ofthe patients were women. Under the Siddha clinicalresearch studies conducted on 8 diseases, 640cases were studied and medical aid was provided toabout 58861 patients including about 35% women.Under the National Population Policy 2000 (NPP-2000) recommending the mainstreaming of ISM&Hin the National RCH programme, the Council incollaboration with ICMR, initiated "Feasibility ofIntroducing India System of Medicines (Ayurvedaand Siddha) in the National 'Reproductive and ChildHealth' Programme at the Primary Health Care (PHC)Level in 5 States"
Gender IssuesGender IssuesGender IssuesGender IssuesGender Issues

438
ANNUAL REPORT 2008-09
13.9 Research studies on diseases specific towomen continued at different centers of the CentralCouncil for Research in Unani Medicine (CCRUM).Validation trials of Unani drugs that were developedby the Council in Sailan-ur-Raham (Leucorrhoea)and Awariz-e-Tams (Menstrual disorders) continuedat different centres of the Council. New researchstudies on Osteoporosis were initiated. During thereporting period 39264 female patients wereregistered in the General OPD programme atdifferent centres of the Council.
13.10 Central Council for Research inHomoeopathy (CCRH) has been sensitive to thegender issues and attempted to give due importanceto diseases of women in its research programmes,particularly in the clinical research. Currently, oneclinical research study on Distress during ClimactericYears is in progress at five Institutes/Units of theCouncil at Shimla, Ranchi, Puducherry, Chennai andHyderabad. Scientific Advisory Committee of theCouncil has approved two more research projects
related to diseases of women viz. 'Uterine Fibroid'and 'Dysmenorrhoea' to be undertaken at the Units/ Institutes of the Council in future. A Gender BudgetCell has been constituted at the headquarters of theCouncil. This Cell continues to compile the data ofthe female patients getting the benefit of treatmentfor various diseases at the peripheral Institutes/ Unitsof the Council under clinical research, clinicalverification programme and general OPD. Themembers of the Gender Budget cell have alsoproposed to start a pilot study on Iron deficiencyanaemia during pregnancy.
13.11 Special OPD for Geriatric Care was held on30th September, 2008 by Central Council for Yogaand Naturopathy (CCRYN) to celebrate theInternational Senior Citizens' Day on 1st October,2008at Janakpuri, (H.Q), Dr. Ram Manohar LohiaHospital, Lady Harding Medical College, SafdarjungHospital and University Colleges of Medical Sciences,Shahadra. Out of the 121 patients, about 30% offemale patients were provided consultation.
Part - III
Department ofHealth Research

440
ANNUAL REPORT 2008-09
441
ANNUAL REPORT 2008-09
A new Department of Health Research has beencreated in the Ministry by amending Allocation ofBusiness Rules. The President of India had notifiedcreation of Department of Health Research underthe Ministry of Health & Family Welfare on17.09.2007. The Department was formallyinaugurated in a function held on 05.10.2007 at NewDelhi. Allocation of work to the newly createdDepartment of Health Research are as under:-
1. Promotion and co-ordination of basic, appliedand clinical research including clinical trialsand operational research in areas related tomedical, health, biomedical and medicalprofession and education throughdevelopment of infrastructure, manpower andskills in cutting edge areas and managementof related information thereto.
2. Promote and provide guidance on researchgovernance issues, including ethical issuesin medical and health research.
3. Inter-sectoral coordination and promotion ofpublic-private-partnership in medical,biomedical and health research relatedareas.
4. Advanced training in research areasconcerning medicine and health, includinggrant of fellowships for such training in Indiaand aboad.
5. International co-operation in medical andhealth research, including work related tointernational conferences in related areas inIndia and aboad.
6. Technical support for dealing with epidemicsand natural calamities.
7. Investigation of outbreaks due to new an
exodic agents and development of tools forprevention.
8. Matters relating to Scientific societies andassociations, Charitable and religiousendowments in medicine and health researchareas.
9. Coordination between organizations andinstitutes under the Central and StateGovernments in areas related to the subjectsentrusted to the Department and forpromotion of special studies in medicine andhealth.
10. Indian Council of Medical Research.
The Department become functional from 01.04.2008with a budget allocation of Rs. 531.75 crores. Withthe appointment of Secretary in the newly createdDepartment of Health Research, the Department hasstarted taking its shape.During the year 2008-09,retirement age of Scientists of ICMR was raised from60 to 62 years of age.
Indian Council of Medical Research
The Indian Council of Medical Research (ICMR), theapex body for the planning, organization,implementation and coordination of medical researchin the country promotes biomedical research througha network of its 21 permanent Institutes and 6Regional Medical Research Centres distributedthroughout the country and also through grants-in-aid given to projects in non-ICMR Institutes. Thebudget allocation for ICMR for 2008-2009 was : PlanRs. 286.00 Crores and Non-Plan Rs.110.00 Crores.
Epidemiology and CommunicabeDiseases
NJIL& OMD, Agra has devised a DNA chip for studying
IntroductionIntroductionIntroductionIntroductionIntroduction

442
ANNUAL REPORT 2008-09
genes encoding efflux pumps and other genesassociated with drug resistance in M.tb. Highest levelof nitric oxide metabolites found in a study in leprosypatients during ENL would help differentiate betweenrelapse and reaction cases. Studies have shown thatcombined regimens of chemotherapy &immunotherapy to be superior to plain MDT inshortening treatment duration in high bacillary loadleprosy. In a door to door resurvey for epidemiologicalstudies of M. leprae at Ghatampur, trends show asteep decline in the prevalence of the disease.Rapidly growing mycobacteria were found to be mostpredominant in the environment. Safety and efficacyof Mycobacterium was immuno-modulator studied atTRC, Chennai in Cat II pulmonary. TB has shown afaster sputum conversion rate after adding Mwwithout any serious side-effects. Three serialpopulation surveys completed in Tiruvallur district tostudy the epidemiological impact of the DOTSstrategy have shown a substantial reduction intuberculosis. A tuberculin survey in Chennai forannual risk of TB infection (ARTI) has shownsignificantly higher risk of infection among childrenof slum area. A drug resistance survey in Gujarathas documented 2.4% and 17% prevalence of MDR-TB in new and re-treated cases of TB respectively.The projects carried out under Center of Advancedresearch in Medical Microbiology at IISc, Bangalorehave resulted in development of potential candidatesubunit vaccines against Rinderpest virus and PPRV,Japanese encephalitis virus, Rabies virus, Coxsackievirus B3. Vector borne disease outbreaks hadbecome rampant in Kerala and eastern UP in thepast few years. In view of this, following approval ofSFC by the Ministry of Health & Family Welfare,ICMR's NIV, Pune set up Field units at Gorakhpurand Allapuzha in March 2008 to serve as a diagnosticlaboratories giving service to Medical College anddistrict hospitals in that region and is involved inestablishment of a laboratory capable of handlingdifferent viruses. EVRC, Mumbai is engaged instudies on all major enteroviruses includingpoliomyelitis. The Centre has developed, tested andvalidated an alternative algorithm for reducing timeof reporting virological test reports in Polio NetworkLaboratories. The new algorithm brought PCR assayas the front line test thereby reducing time line of
reporting from 28 days to 14 days and intratypicdifferentiation from 14 days to 7 days. The newalgorithm was accepted by WHO for implementationin Global network. Presently all the 16 labs in SEARare using the new method. A study was carried outto study the efficacy of short course intermittentchemotherapy regimens in the management of HIV-I seropositive pulmonary tuberculosis at Chennai andPune. The findings show that the response to anti-TB treatment is satisfactory among patients with HIVinfection and there is no difference between patientstreated for six months and nine months. However,high death rates are reported in HIV-infected groupwhen compared to the HIV-uninfected. ICMR carriedout first HIV vaccine trial in India with the HIV vaccineusing adeno associated virus-2 (AAV-2) as a vector.Although this vaccine was found to be safe, it wasnot immunogenic. Another phase I vaccine trial withan MVA based HIV vaccine, showed the vaccine tobe safe and immunogenic in all the volunteers. As apart of the ICMR-DHHS jointly funded humaninfluenza surveillance programme in India, thenetwork currently consisting of nine regional centreshas, during the reported period, antigenicallycharacterized 257 influenza viruses (~4.8%) of whichabout 60% belonged to type B (155), and theremaining type A (25 H1N1 and 77 H3N2). Currentcirculating strains show close genetic relatedness tothe vaccine strains of the corresponding year,showing the effectiveness of the trivalent vaccineavailable in the country. Four regional centres atNew Delhi, Chennai, Kolkata and Pune have beenstrengthened for the use of RT-PCR and forimproved surveillance capacity through moleculardiagnosis, which was reflected during recentoutbreak situations of avian H5N1. Although all theIndian isolates belonged to clade 2.2, the outbreakswere caused by 3 independent introductions ofthe virus.
The NIV, Pune, has been designated as the WHOH5 reference laboratory for H5 diagnosis andresponse in South East Asia region, and thus wouldnow be providing the diagnostic referral services. Amulticentric study conducted on prevalence of viralhepatitis in tribal population of Orissa, MadhyaPradesh, Chattisgarh and Jharkhand revealed that

443
ANNUAL REPORT 2008-09
prevalence of HBs Ag was similar to country widedata on volunteer blood donors, Anti-HCV was highin Mankidia (9.8%) and Juanga (14%) in Orissa andAbhujhmaria (16.6%), Kamar (13%) and Bharia(18%) in M.P. Anti-HAV and Anti-HCV exposure wasalso found to be similar to that reported from variousplaces in India. In a hospital based study carriedout by RMRCT, Jabalpur, 439 patients ofhamoglobinopathies esp. sickle cell disease, themedian age of SCD patients is 10-35 years. Minorintervention like supplementation of folic acid andquick administration of antipyretic and anti-inflammatory drugs on SOS basis alongwith healtheducation has reduced the severity of the diseaseconsiderably.
The NIMR, Delhi continued to provide technicalsupport to the national malaria programme and isplaying a pivotal role in revising the National DrugPolicy for the treatment of malaria. NIMR hassuccessfully completed Phase III and Phase II clinicaltrials, with different artemisinin-based combinationsthis year.
At NICED, Kolkata, studies were carried out for betterformulation of oral rehydration solution (ORS) andon supplementing ORS with Zinc and micronutrients.The molecular mechanism of acquiring resistanceto ciprofloxacin, norfloxacin and obloxacin by Shigelladysenteriae 1 strains was studied traced to amutation at position 83 of the enzyme gyrase (GyrA).The Council's Rajendra Memorial Research Instituteof Medical Sciences, Patna has been identified bythe WHO as the Reference Centre for Leishmaniaand Sera Bank. Validation of sandfly distribution andkala-azar prevalence through remote sensing andGIS in endemic and non-endemic foci has shownencouraging results. Research in the area of filariasisis being conducted at the Centre for Research inMedical Entomology, Madurai; Vector ControlResearch Centre, Pondicherry and Regional MedicalResearch Centre, Bhubaneshwar. A large scalecommunity trial with co-administration of albendazoleand DEC showed their combined usage to have anedge over DEC alone in terms of reducing newinfections of LF. A filariasis transmission risk map hasbeen created for Tamil Nadu, as a case study andstratified into different spatial entitles, "risk' and "non-risk".
Non-Communicable Diseases
Oncology: The network of 20 population based and5 hospital based cancer registries continued toprovide valuable data on cancer occurrence, itsgeographic variations and time trend. A study onpattern of care on some cancer sites is also beingundertaken. Review of guidelines for managementof cancers under a task force project is beingundertaken for 20 cancers sites, with report for fourcancer sites being under review. A study onunderstanding the preparedness of health servicesfor possible introduction of HPV vaccine is beingundertaken in collaboration with PATH. The Instituteof Cytology and Preventive Oncology, New Delhi iscontinuing multidisciplinary research on cancers ofuterine cervix and breast, with focus on humanpapilloma virus and cervical cancer. Breast cancerproject focuses on risk factors, treatment pattern,survival, identification of prognostic factors andsusceptibility genes.
Cardiovascular Diseases: Jai Vigyan Mission ModeProject on "Community Control of RF/RHD" has fourarms including epidemiology, molecular typing ofrheumatogenic strains, RF/RHD registries andresearch towards development of a vaccine againststreptococci. The registry component of the projectshowed RF/RHD prevalence of 0.36 to 1.43 perthousand in the age group 5-14 years. Theprevalence of RF/RHD shown by passive registry atChandigarh, Vellore, Kochi and Indore centre is0.477, 0.504, 0.317 and 0.480 per thousand in allage groups respectively. New strategies for vaccinedevelopment including use of chimeric peptides fromC terminal sequence of M protein as well as Cpeptidase based vaccine are being tried. Studies aregoing to assess normative blood pressure in childrenand adolescents and to study salt sensitivity andcandidate gene polymorphisms in essentialhypertension in tribal population of Mizoram, teagarden communities of Assam and indigenousAssamese population.
Neurosciences: In study of risk factors in strokehigh prevalence of abnormal lipid metabolism wasobserved in stroke cases. Hyper-homocysteinemiawas observed in vegetarians while 33% of the

444
ANNUAL REPORT 2008-09
patients had MTHFR gene mutation. A registry ofepilepsy in pregnant women was initiated atThiruvananthapuram and Delhi.
Mental Health: The task force study on "urbanmental health problems and service needs, beingcarried out at Delhi, Chennai and Lucknow has foundthat common mental disorders were higher in lowersocio-economic strata.
Non Communicable Disease Surveillance: The1st Phase of the NCD disease risk factor surveysunder the Integrated Disease surveillance project hasbeen completed in 7 States (Kerala, Tamil Nadu,Mizoram, Uttaranchal, Maharashtra, MadhyaPradesh, Andhra Pradesh).
North East initiatives: Ongoing studies includeprevalence of paragonimiasis in the ArunachalPradesh hill tribes, control of malaria and JE, andanalysis of the peculiar treatment seeking behaviorof the people of this region. HIV and drug abuse isanother major public health issue that is beingaddressed in the north east besides the relatedopportunistic infections and tuberculosis.
To map the cancers, a system of cancer registries iscontinuing in the north-east region covering sixcentres viz. Dibrugarh, Guwahati, Silcher, Imphal,Aizawl and Gangtok. Six new registries have also beensanctioned. Data collected so far show that theleading site of cancer amongst the males wasoesophagus followed by stomach, lung, tongue andcolorectal cancer. The predominant cancer amongstthe females was breast followed by cervix, stomach,gall bladder and colorectal.
Accidents and injuries: The Council has initiateda feasibility study to test a road traffic injurysurveillance module in NIMHANS, Bangalore and BJMedical college, Pune. Using the findings of the study,a set of 10 simple fact sheets have been developedto highlight individual type of injuries.
Asthama: A 12-centre study on prevalence andaetiological factors of asthma is being undertakenusing a standardized methodology.
Geriatrics: A task force project on determinants ofthe functional status has been completed at two
centres in Delhi. The role of social support networksin performing the physical activities has beenassessed.
Basic Medical Sciences
Haematology
A number of studies were completed on red ellpyruvate kinase deficiency, G6PD mutations andhaplotypes in various ethnic groups in Indiathrombophilia as a cause of unexplained fetal loss,Haemophilia B Glanzzmann's thrombasthenia FLT 3gene mutation in AML spondarthiritis. Studies haveshown that dengue viruses can influence platelet ultrastructure and stimulate platelet function. Patent hasbeen filed in respect of a mismatch PCR techniquefor detecting a common mutation for Haemophilia Bin India.
Pathology
Studies are ongoing on genetic susceptibility andbreast cancer, on gene expression andhypermethylation profiles in early onset breastcancer, tobacco and pesticide related cancers innorth east India (esophageal cancer, pesticideassociated cancer, tobacco associated cancer),virulence-related genes of Leishmania using genomicmicroarray, drug resistance studies on antimonyresistance in field isolates of L. donovani, populationgenetics-genetic heterogeneity investigated in Indianpopulation of Leishmania parasites isolated from KAand PKDL patients etc.
Traditional Medicine
Ongoing research activities include preparation ofdatabase on ethno-medicinal plants of WesternGhats, museum for ethnomedicinal plants of WesternGhats, medicinal plant garden and survey on usage,availability and utility of traditional medicines /formulations in Belgaum region.Initiatives have beentaken by the Council and National InnovationFoundation (NIF) to develop drugs from medicinalplants or multi-herb formulations
Under the Golden Triangle Partnership Deptt ofAyush ( including agencies like Central Council forResearch in Ayurveda and Siddha, Central Council
445
ANNUAL REPORT 2008-09
for Research in Unani Medicines, Central Councilfor Research in Homeopathy, CSIR and ICMR areworking together to achieve safe, effective andstandardized classical Ayurvedic products for theidentified disease conditions and to develop newAyurvedic and herbal products effective in diseaseconditions of national/global importance.
Stem Cell Research
Stem cell research is being supported in the area ofliver disease, corneal epithelial cells, rheumaticdisorders,mesenchymal stem cells directed towardscardiovascular disorders, stem cell and chemokinetherapy for haematological neoplasms, embryonicstem cells for motor functional recovery etc
Human Genetics
A National task force on inborn metabolic disorders-newborn screening for congenital hypothyroidism &congenital adrenal hyperplasia has been initiated.A Clinical Manual for Inborn Metabolic Disorders, hasalso been brought out.
Biomedical ethics
In the area of bioethics workshops have beenconducted for capacity building in various biomedicalinstitutions.
Reproductive Health & Nutrition
Reproductive Health
The Achievements of the NIRRH, Mumbai Instituteinclude stem cell esearch, development of predictivemarkers for diseases, proteomics and genomicslaboratory, Structure and computational biology etc.The construction of quarantine facility at NCPBR,Sasunavghar is completed. The major focus ofresearch is on male (viz. human seminal plasmainhibin (HSPI), 80 kDa proteins), and female fertilityregulation, immuno-contraception, infertility,reproductive tract infection, diagnostics andoperational researches on the fertility attitudes ofmen. Human sperm antigen, 80kDa, has beenidentified from human sperm extract and efforts areto develop this peptide as an immunogen fordeveloping anti-fertility vaccine.
An operational research study on utilisation ofemergency contraception through paramedics inIndia was completed. Follow up of women for sideeffects, EC failure, pregnancy, repeat use andretention of knowledge by paramedical worker wasalso completed. Knowledge about EC availability,usage etc was also done in control area. Report ofthe study is available on the website.
The Multicentric clinical trials and pre-programmeintroduction studies were carried out through thenetwork of human reproduction research centres(HRRCs) to evaluate newer contraceptives for theirpossible use in the programme: newer methodsincluded improved intrauterine devices (CuT220C,CuT 380A, CuT 380ag, LNG IUD), injectablecontraceptives (200mg NET OEN (2 monthly) andcombined monthly injectable), subdermal implants(Norplant II 2 rods) and Norplant (6 capsules),triphasic oral pills non-steroidal weekly oral pill(Centchroman), non-surgical methods for femalesterilization, barrier methods (diaphragm, vaginalpessary) and Billing ovulation methods of naturalfamily planning. Study on sequelae of femalesterilization carried out on 32,000 women indictedthat Minilap may be recommended for National FamilyWelfare Programme. The ICMR has preparednational guidelines for tubal sterilization bylaparoscopy and minilap methods after studying thesequelae of female sterilization.
RISUG Phase III trial is ongoing for malecontraception. Study on nanotech prepared smartRISUG is also in progress. The application ofnaotechnology for reproductive health has beeninitiated four centres. The ART Guidelines for theAssisted Reproductive Technology Bill and Ruleshave been drafted.
Two new diagnostic techniques viz. ELISA for Hb A2for beta thalassaemia and FISH techniques fordetection of specific DNA sequence inmorphologically preserved cells and tissues has beenstandardized.
RU 486 in combination with PGE vaginal gel wasfound to be successful in 90% of women who soughttermination of early pregnancy.

446
ANNUAL REPORT 2008-09
Maternal Health
India is a signatory to the Millennium Declaration andcommitted to attaining the goal of reduction ofmaternal mortality to three-quarters by 2015. Postpartum haemorrhage (PPH), eclampsia and severeanemia are among the important causes of highmaternal mortality. The Council is conductingmulticentric studies to address these challenges. Astudy is ongoing on teenage pregnancy. Forms havebeen pilot tested and are in the process of revision,next year also the forms will be pilot tested andafter that the study will be initiated.
Child Health
The research activities of the Council in the area ofchild health include testing comprehensive newborncare at home level, testing methods suitable formanagement of preterm /low birth weight babiesdelivered at home, zinc supplementation for reducingmorbidity and mortality, HIV infections in pediatric agegroup and childhood cancers.
Nutrition
The Council's research efforts in the field of nutritionare directed towards combating nutritionaldeficiencies and promoting nutritional well-being. Thisis achieved through continuous research, monitoring,extension education and training carried out byNational Institute of Nutrition, Hyderabad and throughnetwork of National Nutrition Monitoring Bureau(NNMB). NNMB since its inception in 1972 has beencarrying out diet and nutrition surveys on regularbasis in the rural and tribal areas, as well as specialsurveys in selected population groups. In order tostudy the time trends in the diet and nutritionalsurveys of the communities, the NNMB has beencarrying out repeat surveys both in the rural andtribal areas by visiting the same villages every 10years.
As part of community study was conducted onprevalence of overweight and obesity amongadolescents of Andhra Pradesh. Studies were alsocarried out to investigate biochemical, molecular andnutritional aspects of cataract and retinal
degeneration. Studies on rat model were carried outto examine the effect of poly-unsaturated fatty acidson plasma glucose clearance and plasma lipoproteinprofile. Stem cell research studies are also beingconducted in-vitro and in-vivo using mice as modelsystem.A multicentre task force study on assessmentof prevalence of osteoporosis in adult population ofIndia is ongoing at New Delhi, Hyderabad, Lucknowand Mumbai.
Publication, Information andCommunication
During the year under review, the Council broughtout a number of publications such as the IndianJournal of Medical Research, the ICMR Patrika andAnnual Report etc. Activities were also undertakenin the field of informatics and communication.
Indian Journal of Medical Research - The IndianJournal of Medical Research (IJMR) continued to beindexed and abstracted by all major global currentawareness and alerting services. The IJMR isavailable full-text free on the internet (www.icmr.nic.in)and is also available in the medIND, the online full-text database of Indian biomedical journals. Theimpact factor of Indian Journal of Medical Research( IJMR) increased to 1.670 in 2007.
Annual Report - The English and Hindi versions ofthe Annual Report of the Council (2007 -2008) werebrought out during the year with improved overallget up. A compact disc (CD) was also brought out foreasy handling and user convenience.
Hindi Publications
Publication of in-house popular Hindi periodical i.e.ICMR Patrika was continued during 2008 -09 andarticles were published on the following topics : 'MridaSancharit Krimi Sankraman ka Janpadik Rogvigyanaur Niyantran' , 'Bharat mein Ashthisushirta ki Sthiti','Poshan evam Asthi Swashthya' , and 'Orissa keVishesh Sandarbh men Aushadh PratirodhiFalciparum Malaria ki Rogjanpadiki .
Some popular medical books in Hindi - (i). Damaevam Allergy : Kaise Chhutkara Payen, ( By : Dr
447
ANNUAL REPORT 2008-09
Rajendra Mehta); (ii). Sukhi Balika ( By : Dr PannaLal) and (iii). Mutra Nali ka Catheter evam AapkaSwasthya (By : Dr Divakar Dalela & Dr Prateek Sinet)were selected for the First (Rs. 50,000/-), Second(Rs. 30,000/-) and Third (Rs. 20,000/-) ICMRPuraskar respectively for the Biennium 2006 -07.
Monographs - During the year Vol. 6 and 7 coveringinformation on about 370 medicinal plants specieswere published.
Quality Standards of Indian Medicinal Plants andmedicinal plants monographs on diseases of publichealth importance are being compiled.
Biomedical Information - The ICMR-NIC Centre'swebpage, http://indmed.nic.in continued to be rankedamongst the top Indian health websites by the Googledirectory; over 700 searches were conducted duringthe year.
The medIND database at present covers 39 journals.The indexing of journals for IndMED database isongoing and at present contains approximately45,000 records. Updating of the Union Catalogueof Biomedical Periodicals is also ongoing .
Separate training programmes were organized formedical librarians and medical professionals on"Biomedical Information Retrieval". Four programmeswere held for medical professionals with little or nointernet experience and those with advancedknowledge of internet resources.
Bioinformatics Centre (BIC) - Six BiomedicalInformatics Centres established by ICMR during atdifferent locations across the country are fullyfunctional. The Coordinating unit is with BioinformaticsCentre, ICMR Headquarters. Homology modeling,structure based drug design, database and softwaredevelopment, training and services towardsapplication of bioinformatics tools in research workof scientists of the host institutes etc. are some ofthe major activities of these Centres.
In addition to routine maintenance of ICMRdatabases, the BIC initiated information systemdevelopment for a technical division of the Council
and developed a web based module for an ICMRtask force project 'Capturing Acute CardiovascularEvents in Hospitals'.
Work on creating video conferencing facility in eightICMR institutes was initiated. Facility managementof networking for all ICMR institutes was renewed forthree years.
Popularity of ICMR website http://www.icmr.nic.incontinued during the year. The site was visited byabout nine lakh visitors. The most frequently usedareas were Annual Reports of ICMR institutes, IJMR,ICMR News etc.
Intellectual Property Rights
A total of 7 patents were filed with Indian Patent Officeduring 2007-2008. During the year the Council alsopublished a handbook on Intellectual PropertyManagement in Health and Agriculture Innovation.Initiatives were undertaken to transfer the Council'stechnologies for commercialization. The Councilsigned a Letter of Consent (LoC) with BiotechConsortium India Limited, New Delhi (BCIL) andshowcased ICMR technologies at the two dayExhibition "FICCI HEAL 2007".
International Health
The ICMR co-ordinates international collaborationin biomedical research between India and othercountries such as France, Germany, USA, Canada,Australia, Bulgaria, Spain etc. and national &international agencies such as WHO, Ministry ofScience & Technology etc. A total of about 70exchange visits of scientists to and from India werearranged under various international collaborativeprojects/programmes. Progress under MOUs of ICMRwith University of Minnesota (USA), CIHR (Canada),University of Sydney (Australia), INSERM (France),BMBF (Germany), Boston University (USA) to worktogether on health issues of mutual importance hasbeen made.
During the year three meetings of Health Ministry'sScreening Committee (HMSC) were organizedwherein approx. 80 projects for international

448
ANNUAL REPORT 2008-09
collaboration/assistance were approved by theCommittee. ICMR International Fellowships havebeen awarded to five senior and ten young Indianscientists for the year 2008-09. The Council hastaken up a project entitled "Managing the Indo-German (ICMR-HGF) Science Centre for InfectiousDiseases (IGSCID).
Social & Behavioural Research
Following studies were carried out - care and needsof people living with HIV/AIDS. A diagnostic study inthe context of long term care, health consequencesof domestic violence with special reference toreproductive health and study of roles and capacitiesof Panchayati Raj institutions to manage the grassroot health system.
Manpower Development Division
During the year the Council awarded 150 JRFs -120 for Life Sciences and 30 for Social Sciencesincluding biostatistics for doing Ph.D. in BiomedicalSciences in different institutions. Financial assistancewas provided to 50 MD/MS/DM/MCH students forcarrying out biomedical research. Under MD, Ph.D.Programme financial support was provided to 25medical graduates with brilliant academic record forpersuing MD and research later. Short term visitingfellowships were provided to scientists employed ina medical college, research institute, university etc.to learn advanced research techniques/methods inuse in other institutes in India.
Part - IV
Department ofAIDS Control
450
ANNUAL REPORT 2008-09
451
ANNUAL REPORT 2008-09
Highlights of the Annual Report
1. India had an estimated 1.8 - 2.9 million HIVpositive persons in 2007, with an estimated adult HIVprevalence of 0.34% (0.25%-0.43%). With the HIVPrevalence among the high risk groups (HRG) beingaround seven to fourteen times that among thegeneral population, India continues to be in thecategory of concentrated epidemic. The sexual modecontinues to be the major mode of transmission,though transmission through injecting drug use andMen having Sex with Men are on the rise in manynew pockets. The annual HIV sentinel surveillancecovered 1,215 sites in 2008-09.
2. The National AIDS Control Programme(NACP) Phase-III (2007-2012) has the overall goalof halting and reversing the epidemic in India overthe five-year period. It places the highest priority onpreventive efforts while, at the same time, seekingto integrate prevention with care, support andtreatment through a four-pronged strategy:
1. Prevention of new infections in high riskgroups and general population through:
a. Saturation of coverage of high riskgroups with targeted interventions (TIs)
b. Scaled up interventions in the generalpopulation
2. Providing greater care, support andtreatment to larger number of persons livingwith HIV/AIDS (PLHA).
3. Strengthening the infrastructure, systems andhuman resources in prevention, care, support andtreatment programmes at the district, state andnational level.
4. Strengthening the nationwide StrategicInformation Management System.
The specific objective is to reduce new infection asestimated in the programme's first year by 60% inhigh prevalence states so as to obtain reversal ofthe epidemic; and by 40% in the vulnerable statesso as to stabilize the epidemic. NACP's organizationalstructure was decentralized to implementprogrammes at the district level, with priority forCategory A and B districts.
3. On 31 March, 2009, 1,271 TargetedInterventions projects were operational under variousState AIDS Control Societies and about 200 morewere managed by partners. These TIs covered 55%of FSW, 73% of IDU and 77% of MSM andtransgender populations. The State Training andResource Centres were established in 14 states toensure the capacity and technical skills of the TI staff.The HRG mapping exercise was conducted in 17states and validated in March, 2009. The existingcentres implementing Oral Substitution Therapy toaddress the HIV risk among the Injecting Drug Userswere assessed and accredited, procurement of themedicines was carried out, and a supply chainmechanism drafted. The Link Worker Schemespecifically covers highly vulnerable villages andaddresses population with high-risk behaviours andyoung people.
4. As a part of the preventive interventions forthe general population, NACO is developing acommunication strategy to make a paradigm shiftfrom awareness generation to effecting behaviourchange. NACO has focused on the reduction ofstigma and discrimination, promotion of services. Aspecial emphasis has been given to youth andwomen who are more vulnerable to the HIV infection.Several multi-media, mid-media and mass mediacampaigns primarily targeted high priority districts.The Red Ribbon Express Project is the world's largestmass mobilization campaign on HIV/AIDS. The train
Highlights of the Annual ReportHighlights of the Annual ReportHighlights of the Annual ReportHighlights of the Annual ReportHighlights of the Annual Report
452
ANNUAL REPORT 2008-09
was flagged off on 1st December, 2007 (World AIDSDay) from Delhi and completed its journey on 1stDecember, 2008 after traveling over 27,000 kmscovering 180 district/halt stations. The projectcovered 41,334 villages and reached out to 6.2million people. 68,244 persons were trained and1,16,183 persons counseled on HIV/AIDS. Anallocation of Rs. 167.3 crores was made under IECfor NACO and SACS during 2008-09.
5. The National Council on AIDS has beenconstituted under the chairpersonship of Hon'blePrime Minister with representation of 33 ministriesand departments to strengthen the Government'smultisectoral response to prevent the spread of HIV.The State Councils on AIDS guide and support themainstreaming efforts at the state level.
6. Condom use was promoted and condomsprovided at all ICTCs, ART centres and STI clinics.During 2008-09, 7,50,000 condoms were soldthrough 8,500 condom vending machines. NACOscaled up the Female Condom Programme in AndhraPradesh, Tamil Nadu, Maharashtra and West Bengalto saturate all the female sex worker TIs. During2008-09, 15 lakh female condoms were procured
7. Access to safe blood was ensured through anetwork of 1,092 Blood Banks including 104 BloodComponent Separation Units and 10 Model BloodBanks. Of the blood units collected in 2008-09, 61.7%was through voluntary blood donation. A total of56,568 blood donation camps were organized.
8. The Integrated Counseling and TestingCentres (ICTC) increased from 982 in 2004 to 4,987in March 2009. The number of persons testedincreased from 17.5 lakhs in 2004 to 101 lakhs in2008-09. In 2008-09, 24,320 HIV-TB co-infectedpatients were diagnosed. The ICTCs providedcounseling and testing to 46.3 lakh pregnant women,of whom 21,483 were found HIV positive. A total of10,494 mother-baby pairs were given prophylaxisdose of Nevirapine.
9. The number of designated STI/RTI clinicsbeing supported by NACO increased from 845 inMarch 2008 to 886 in March 2009. The number of
patients accessing STI/RTI services from these clinicsand STI clinics in TI projects increased from over20.2 lakh in 2006 to 34.8 lakh in 2008. In addition,over 31 lakh STI/RTI episodes were managedthrough sub-district level health facilities under NRHMin 2008 bringing the total number of STI/RTI episodesmanaged to 66.7 lakhs in the country during 2008-09. The STI services are being expanded thougheffective integration with RCH-II programme andinvolvement of private sector. The centrally-procuredcolour-coded syndromic drug kits and RPR/TPHAtest kits were supplied to the designated STI/RTIclinics. The STI/RTI service delivery for HRGpopulation has been strengthened through thepreferred private provider model.
10. The free ART programme was scaled up to211 centres, and 2,17,781 patients were receivingfree ART as of March, 2009. Ten Regional Centresof Excellence provide state-of-art services for PLHAs.The rollout of second line ART was expanded to these10 centres from January 2009, where 401 patientsreceive second line drugs. As of 31 March, 2009,254 Community Care Centres were operational.Under the National Paediatric HIV/AIDS Initiative,47,784 CLHA had been registered for HIV care atART centres, and 14,303 CLHAs received free ARTas of March 2009.
11. The Strategic Information Management Unitsat national and state levels address strategicplanning, monitoring & evaluation, surveillance andresearch. The SIMS project and the smart card projectfor ART patients are in progress.
12. During 2008-09, a sum of Rs 1,037 croreswas spent on NACP against the Revised Estimate ofRs. 1,123.36 crores.
(K. SUJATHA RAO)
Secretary, Department of AIDS Control& Director General,
National AIDS Control Organisation
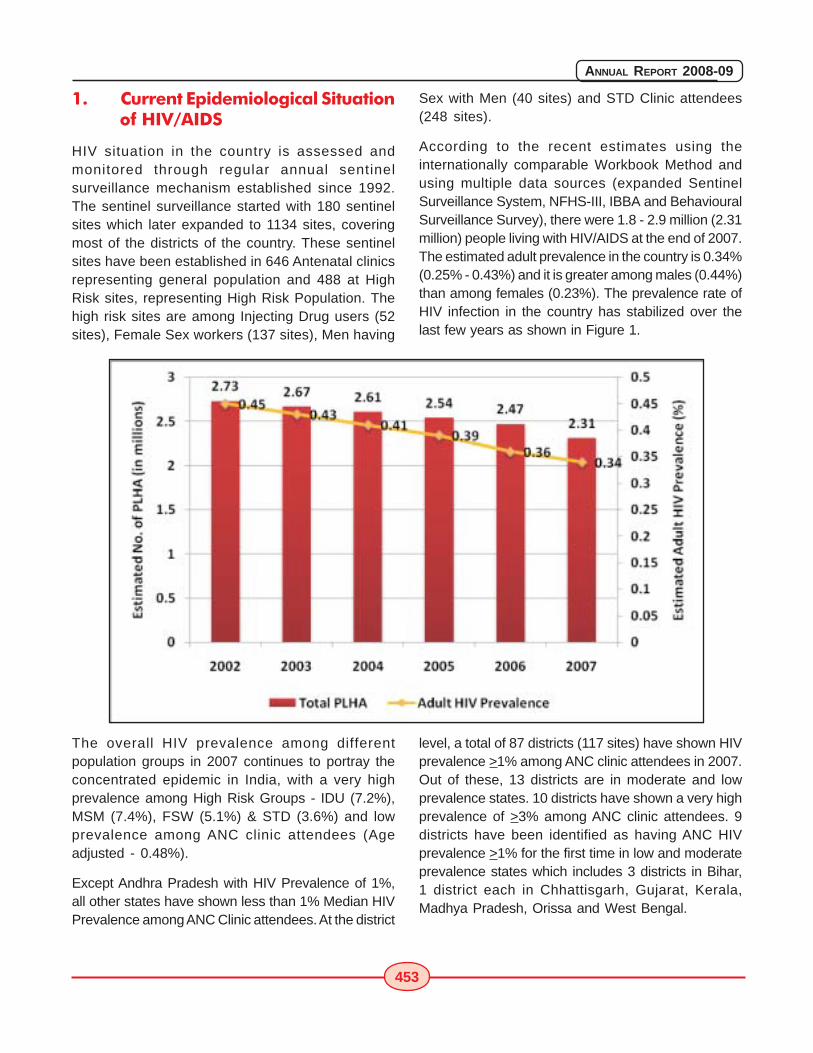
453
ANNUAL REPORT 2008-09
1. Current Epidemiological Situationof HIV/AIDS
HIV situation in the country is assessed andmonitored through regular annual sentinelsurveillance mechanism established since 1992.The sentinel surveillance started with 180 sentinelsites which later expanded to 1134 sites, coveringmost of the districts of the country. These sentinelsites have been established in 646 Antenatal clinicsrepresenting general population and 488 at HighRisk sites, representing High Risk Population. Thehigh risk sites are among Injecting Drug users (52sites), Female Sex workers (137 sites), Men having
Sex with Men (40 sites) and STD Clinic attendees(248 sites).
According to the recent estimates using theinternationally comparable Workbook Method andusing multiple data sources (expanded SentinelSurveillance System, NFHS-III, IBBA and BehaviouralSurveillance Survey), there were 1.8 - 2.9 million (2.31million) people living with HIV/AIDS at the end of 2007.The estimated adult prevalence in the country is 0.34%(0.25% - 0.43%) and it is greater among males (0.44%)than among females (0.23%). The prevalence rate ofHIV infection in the country has stabilized over thelast few years as shown in Figure 1.
The overall HIV prevalence among differentpopulation groups in 2007 continues to portray theconcentrated epidemic in India, with a very highprevalence among High Risk Groups - IDU (7.2%),MSM (7.4%), FSW (5.1%) & STD (3.6%) and lowprevalence among ANC clinic attendees (Ageadjusted - 0.48%).
Except Andhra Pradesh with HIV Prevalence of 1%,all other states have shown less than 1% Median HIVPrevalence among ANC Clinic attendees. At the district
level, a total of 87 districts (117 sites) have shown HIVprevalence >1% among ANC clinic attendees in 2007.Out of these, 13 districts are in moderate and lowprevalence states. 10 districts have shown a very highprevalence of >3% among ANC clinic attendees. 9districts have been identified as having ANC HIVprevalence >1% for the first time in low and moderateprevalence states which includes 3 districts in Bihar,1 district each in Chhattisgarh, Gujarat, Kerala,Madhya Pradesh, Orissa and West Bengal.
454
ANNUAL REPORT 2008-09
An overall decline in HIV prevalence among ANCclinic attendees is noted at all India level and in highprevalence states in south and northeast. Risingtrend among ANC clinic attendees is observed in somelow and moderate prevalence states, especially inthe four states of Gujarat, Rajasthan, Orissa andWest Bengal.
47 districts (48 sites) have shown >5% HIVPrevalence among FSW, which also include FSWsites in low prevalence states namely West Bengal,Bihar and Gujarat. FSW sites in Pune, Mumbai andThane have shown > 30% HIV prevalence amongFSW. Among FSW, there is a decline in South IndianStates reflecting the impact of interventions, whilerising trends are evident in the North East suggestinga dual nature of the epidemic.
Expanded surveillance among MSM has revealedmore than 5% HIV prevalence in Karnataka (17.6%),Andhra Pradesh (17%), Manipur (16.4%),Maharashtra (11.8%), Delhi (11.7%), Gujarat (8.4%),Goa (7.9%), Orissa (7.4%), Tamil Nadu (6.6%) andWest Bengal (5.6%).
Among IDUs, Maharashtra (24.4%), Manipur (17.9%),Tamil Nadu (16.8%), Punjab (13.8%), Delhi (10.1%),Chandigarh (8.6%), Kerala (7.9%), West Bengal(7.8%), Mizoram (7.5%) & Orissa (7.3%) have shownhigh prevalence of >5%. New pockets of epidemicamong IDU identified during 2006 continue to showhigh HIV Prevalence in 2007. Trends among IDUsare on a decline in Manipur, Nagaland and Chennaiwhile there is a clear rise in Meghalaya, Mizoram,West Bengal, Mumbai, Kerala and Delhi.
The epidemic is greater in urban areas than ruralareas, greater among males than females, decreaseswith increasing education level, and is found to behighest among women whose spouses work intransport industry.
Based on the sentinel surveillance data for the lastthree years (2004-2006), all the districts in thecountry have been classified into four categories:there are 156 A category districts, 39 B categorydistricts and the remaining are in categories C & D.
Thus, HIV epidemic in India is a dual epidemic drivenby sexual and IDU routes of transmission,concentrated in nature with high HIV prevalence
among high risk groups and heterogeneous inspread with pockets of infection found in variousdistricts of the country.
2. National Response to HIVEpidemic
2.1. National AIDS Control Programme - PhaseI & II
The first phase of National AIDS Control Programmewas initially from 1992 to 1997 and was extended to1999. NACP-II commenced from April 1999 with thetwin objectives of reducing the spread of HIV infectionand strengthening the capacity of Central and StateGovernments to respond to HIV/AIDS on a long termbasis. Targeted interventions were initiated for highrisk groups and measures were taken to prevent HIVtransmission among the general population. Anti-Retro Viral Therapy was provided to AIDS patientsat selected centres.
The programme implementation has been completelydecentralized to states and UTs. Each state and UThas registered a State AIDS Control Society (SACS)responsible for implementing the programme at theState/ UT level. Mumbai, Chennai and Ahmedabadhave formed Municipal AIDS Control Societies toeffectively implement the programme.
Important policy initiatives taken during NACP-IIinclude adoption of National AIDS Prevention andControl Policy (2002); National Blood Policy; GreaterInvolvement of People with HIV/AIDS (GIPA); launchof the National Rural Health Mission; launch of theNational Adolescent Education Programme; provisionof anti-retroviral treatment (ART); formation of aninter-ministerial group for mainstreaming; and settingup of the National Council on AIDS, chaired by thePrime Minister.
2.2. National AIDS Control Programme - PhaseIII
The overall goal of NACP-III launched in June 2007is to halt and reverse the epidemic in India over thenext 5 years. Considering that more than 99% ofthe population in the country is free from infection,NACP-III will place the highest priority on preventiveefforts while, at the same time, seeking to integrateprevention with care, support and treatment. This
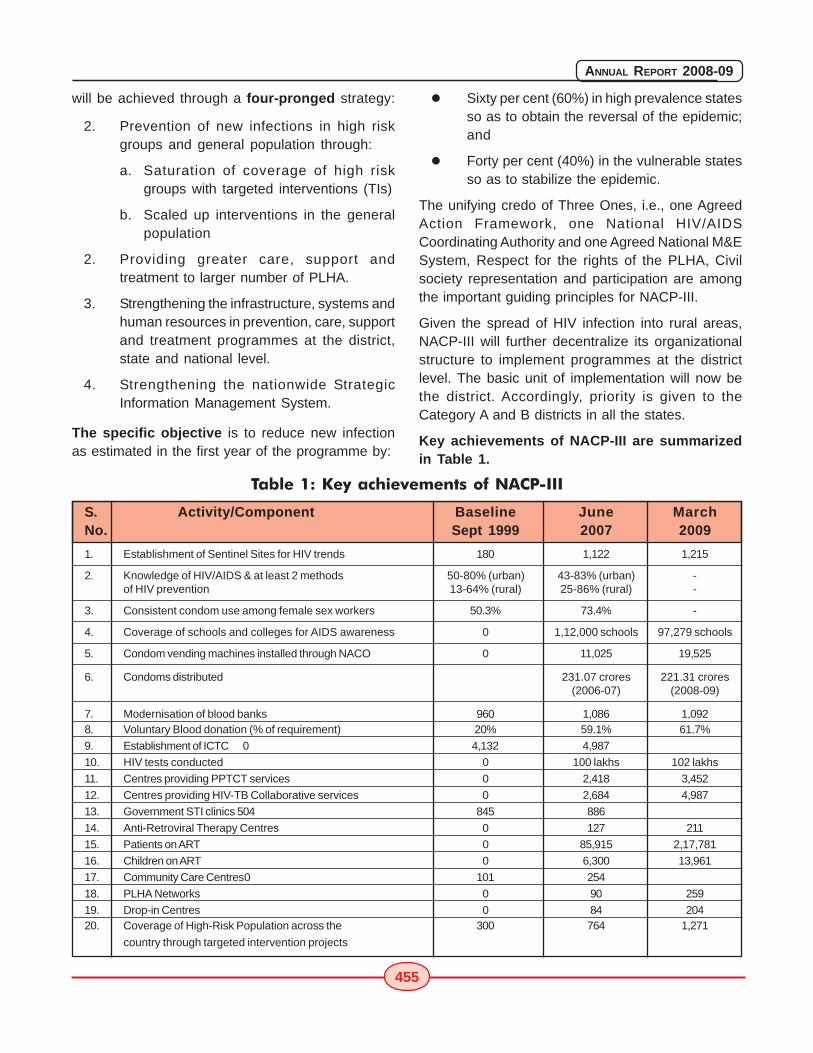
455
ANNUAL REPORT 2008-09
will be achieved through a four-pronged strategy:
2. Prevention of new infections in high riskgroups and general population through:
a. Saturation of coverage of high riskgroups with targeted interventions (TIs)
b. Scaled up interventions in the generalpopulation
2. Providing greater care, support andtreatment to larger number of PLHA.
3. Strengthening the infrastructure, systems andhuman resources in prevention, care, supportand treatment programmes at the district,state and national level.
4. Strengthening the nationwide StrategicInformation Management System.
The specific objective is to reduce new infectionas estimated in the first year of the programme by:
� Sixty per cent (60%) in high prevalence statesso as to obtain the reversal of the epidemic;and
� Forty per cent (40%) in the vulnerable statesso as to stabilize the epidemic.
The unifying credo of Three Ones, i.e., one AgreedAction Framework, one National HIV/AIDSCoordinating Authority and one Agreed National M&ESystem, Respect for the rights of the PLHA, Civilsociety representation and participation are amongthe important guiding principles for NACP-III.
Given the spread of HIV infection into rural areas,NACP-III will further decentralize its organizationalstructure to implement programmes at the districtlevel. The basic unit of implementation will now bethe district. Accordingly, priority is given to theCategory A and B districts in all the states.
Key achievements of NACP-III are summarizedin Table 1.
Table 1: Key achievements of NACP-III
S. Activity/Component Baseline June MarchNo. Sept 1999 2007 2009
1. Establishment of Sentinel Sites for HIV trends 180 1,122 1,215
2. Knowledge of HIV/AIDS & at least 2 methods 50-80% (urban) 43-83% (urban) -of HIV prevention 13-64% (rural) 25-86% (rural) -
3. Consistent condom use among female sex workers 50.3% 73.4% -
4. Coverage of schools and colleges for AIDS awareness 0 1,12,000 schools 97,279 schools
5. Condom vending machines installed through NACO 0 11,025 19,525
6. Condoms distributed 231.07 crores 221.31 crores(2006-07) (2008-09)
7. Modernisation of blood banks 960 1,086 1,0928. Voluntary Blood donation (% of requirement) 20% 59.1% 61.7%
9. Establishment of ICTC 0 4,132 4,987
10. HIV tests conducted 0 100 lakhs 102 lakhs
11. Centres providing PPTCT services 0 2,418 3,452
12. Centres providing HIV-TB Collaborative services 0 2,684 4,987
13. Government STI clinics 504 845 886
14. Anti-Retroviral Therapy Centres 0 127 211
15. Patients on ART 0 85,915 2,17,781
16. Children on ART 0 6,300 13,961
17. Community Care Centres0 101 254
18. PLHA Networks 0 90 259
19. Drop-in Centres 0 84 20420. Coverage of High-Risk Population across the 300 764 1,271
country through targeted intervention projects
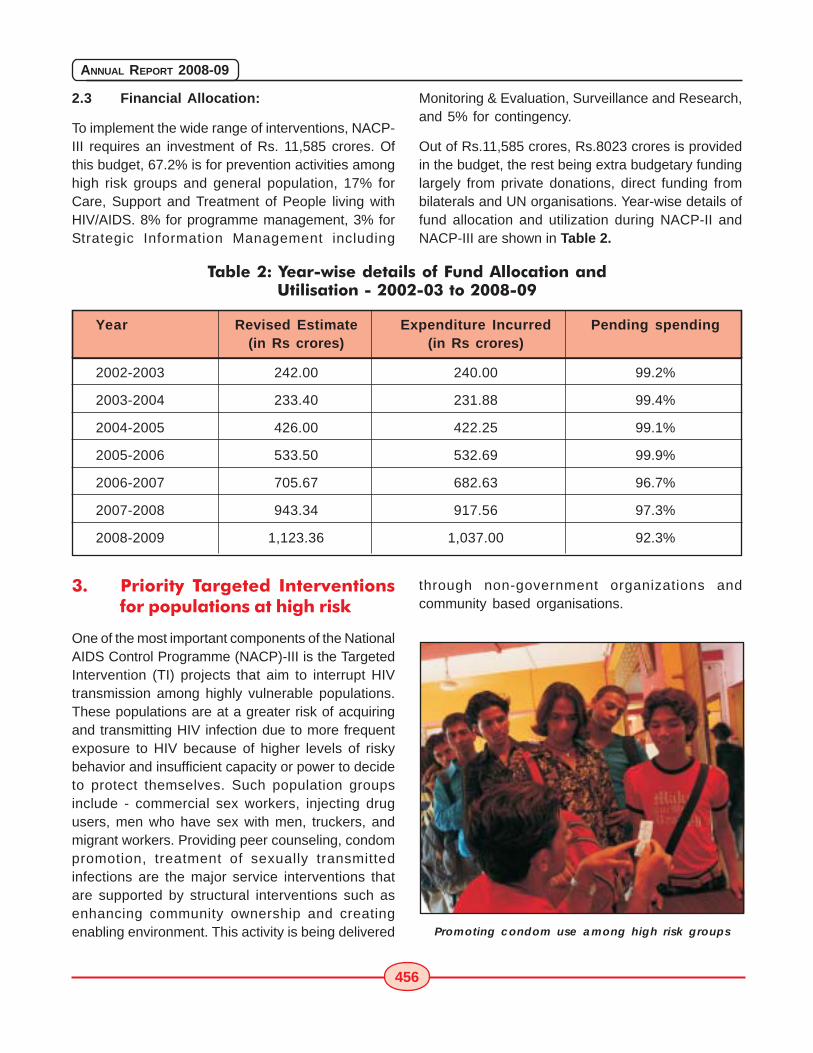
456
ANNUAL REPORT 2008-09
2.3 Financial Allocation:
To implement the wide range of interventions, NACP-III requires an investment of Rs. 11,585 crores. Ofthis budget, 67.2% is for prevention activities amonghigh risk groups and general population, 17% forCare, Support and Treatment of People living withHIV/AIDS. 8% for programme management, 3% forStrategic Information Management including
Monitoring & Evaluation, Surveillance and Research,and 5% for contingency.
Out of Rs.11,585 crores, Rs.8023 crores is providedin the budget, the rest being extra budgetary fundinglargely from private donations, direct funding frombilaterals and UN organisations. Year-wise details offund allocation and utilization during NACP-II andNACP-III are shown in Table 2.
Year Revised Estimate Expenditure Incurred Pending spending(in Rs crores) (in Rs crores)
2002-2003 242.00 240.00 99.2%
2003-2004 233.40 231.88 99.4%
2004-2005 426.00 422.25 99.1%
2005-2006 533.50 532.69 99.9%
2006-2007 705.67 682.63 96.7%
2007-2008 943.34 917.56 97.3%
2008-2009 1,123.36 1,037.00 92.3%
3. Priority Targeted Interventionsfor populations at high risk
One of the most important components of the NationalAIDS Control Programme (NACP)-III is the TargetedIntervention (TI) projects that aim to interrupt HIVtransmission among highly vulnerable populations.These populations are at a greater risk of acquiringand transmitting HIV infection due to more frequentexposure to HIV because of higher levels of riskybehavior and insufficient capacity or power to decideto protect themselves. Such population groupsinclude - commercial sex workers, injecting drugusers, men who have sex with men, truckers, andmigrant workers. Providing peer counseling, condompromotion, treatment of sexually transmittedinfections are the major service interventions thatare supported by structural interventions such asenhancing community ownership and creatingenabling environment. This activity is being delivered
Table 2: Year-wise details of Fund Allocation andUtilisation - 2002-03 to 2008-09
through non-government organizations andcommunity based organisations.
Promoting condom use among high risk groups

457
ANNUAL REPORT 2008-09
Currently, 1,271 Targeted Intervention projects areoperational in the country under various State AIDSControl Societies and around 200 TIs are managedby other partners. These TIs cover 55% of FSW,73% of IDU and 77% of MSM & Transgenderpopulations. The contract renewal of NGOs/CBOs isbased on the annual reviews conducted by externalexperts using a standardised tool developed byNACO. For effective saturation of coverage of targetpopulation, mapping has been conducted in 17states.
Experience has demonstrated that addressing issuesof empowerment of high risk groups is a successfulstrategy for obtaining their adherence to safe sexbehaviour. During NACP III high risk groups will besupported to organise themselves into CommunityBased Organisations (CBOs) (i.e., organisationsmanaged by the target Community themselves) so asto ensure sustainability and reduce their continueddependence on NGOs for accessing critical services.Saturation of all high risk groups through 2,100 TIprojects and development of ownership by communityto ensure the services accessibility to all is the targetaimed at during NACP-III.
In order to ensure the quality of TI programme,capacity building and enhancing the technical skillsof NGO/CBO staff is very important. Therefore, inorder to provide uniform, quality training to differentcategories of staff working with NGOs/CBOs, viz.,program managers, counsellors, financeaccountants, outreach workers, peer educators andlink workers, NACO has institutionalized the trainingand capacity building process with the establishmentof the State Training and Resource Centres (STRC).STRCs function with the objectives of 1) ensuringneed based training of TIs as per NACP III's technicaland operational guidelines; 2) enhancing the capacityof NGOs and civil society organizations in proposaldevelopment for NACP funded targeted interventionprojects; and 3) undertaking operational researchand evaluation of TIs. STRCs have been establishedin 14 states and 6 more are being established.Training modules for programme managers havebeen developed and modules for rest of project staffare in process.
Peer education session for truckers
A new intervention that has been taken up in NACP-III for addressing the HIV risk among Injecting DrugUsers is provision of Oral Substitution Therapy (OST),which has been seen to be an effective strategyworldwide. After obtaining approval of the ExpenditureFinance Committee, the existing centresimplementing OST were assessed and accredited.Simultaneously, the medicines were procured, anda supply chain mechanism drafted.
NACO has also taken initiative to standardiseinterventions among truckers. As per NACP III,truckers' interventions are to be focused on highpriority locations i.e. major trans-shipment locations(TSLs) with 5,000 or more long distance truckershalt on a monthly basis. NACO commissioned anation-wide mapping of truckers' sites so as toidentify locations where interventions could be setup for optimum coverage. A total of 122 sites(including ports) were identified, out of which 18%sites were high priority; 30% were medium priority.Of high priority TSLs, 41% were in the North Zone.Nearly 70% of the high priority TSLs are in AndhraPradesh, Uttar Pradesh and Mumbai. In addition, themapping study also provided micro-maps of thelocations, indicating the presence of condom outletsand STI service providers.
At present, there are 52 truckers interventions, ofwhich 17 are in high-priority locations. The projectsare being implemented by NGOs, although TruckersAssociations have been involved in Tamil Nadu,

458
ANNUAL REPORT 2008-09
Andhra Pradesh and Maharashtra. The revisedcosting guidelines for truckers are being followed andeach intervention aims to provide BCC, IPC, condomsand STI services to a minimum of 5,000 truckersevery month. NACO has established a TechnicalSupport Group (TSG) for truckers to manage theseinterventions. The Transport Corporation of IndiaFoundation (TCIF), functioning as the TSG, overseesquality of services, provides capacity buildingsupport, promotes advocacy with key stakeholders,and regularly monitors the key activities.
The Link Worker Scheme (LWS) under NACP-III hasbeen designed specifically to address population withhigh-risk behaviours (including High Risk Groups andBridge Populations) with the premise that there aresignificant numbers in rural areas and we need toreach out to them in order to saturate the coverageof these groups. In addition the scheme will coveryoung people. LWS is a medium term, meso-levelstrategy, whose scope is limited to five years. Theservices established through LWS will be linked tolocal health governance system at three levels. Thiswill again ensure mainstreaming of the HIV responseproject and, therefore, the project sustainability canbe assured beyond five years.
Monthly meeting of Link Workers
The LWS envisions a new cadre of worker, the LinkWorker, who are motivated, community-level, paidfemale and male youth workers with a minimum levelof education, at the village level who are able to
discuss intimate human relations and practices ofsex and sexuality and help equip high-risk individualsand vulnerable young people with information andskills to combat the pandemic. The Link workersare covering highly vulnerable villages in districtsselected through mapping exercises. They work ineach cluster of villages around a 5,000+ population.They are supported in their work by village-levelvolunteers selected from the available groups in thecommunity.
In every district, the LWS is being implementedthrough one or two District Resource Persons, oneMonitoring & Evaluation Officer, four Supervisors and40 Link Workers. Presently, the LWS is beingimplemented with support from UNDP, UNICEF, USGand GFATM Round 7 as follows:
UNDP: (Through lead NGOs: Plan India,ActionAid & Aide et Action) in 25 districts inthe States of Uttar Pradesh, Bihar, Rajasthan,Chattisgarh and Orissa
UNICEF: (Directly through DAPCU/districtorganization) in 25 districts in the states ofBihar, Andhra Pradesh, Orissa, Rajasthan,Karnataka, Tamil Nadu, Maharashtra,Gujarat, West Bengal and Uttar Pradesh
US Government: (USAID and CDC throughKHPT) in 16 districts in the state of Karnataka.
GFATM (NACO directly through 8 NGOs) in26 districts in the states of Andhra Pradesh,Goa, Gujarat, Karnataka, Kerala, MadhyaPradesh, Manipur, Mizoram, Nagaland, TamilNadu, Tripura, and West Bengal.
4. Preventive Interventions for thegeneral population
Prevention has always been the main stay ofaddressing the HIV/AIDS epidemic. Under NACP-III,it is proposed to integrate and scale-up servicedelivery to sub-district and community levels throughexisting infrastructure in the public and privatesectors. The following is the package of preventiveservices provided under NACP-III:
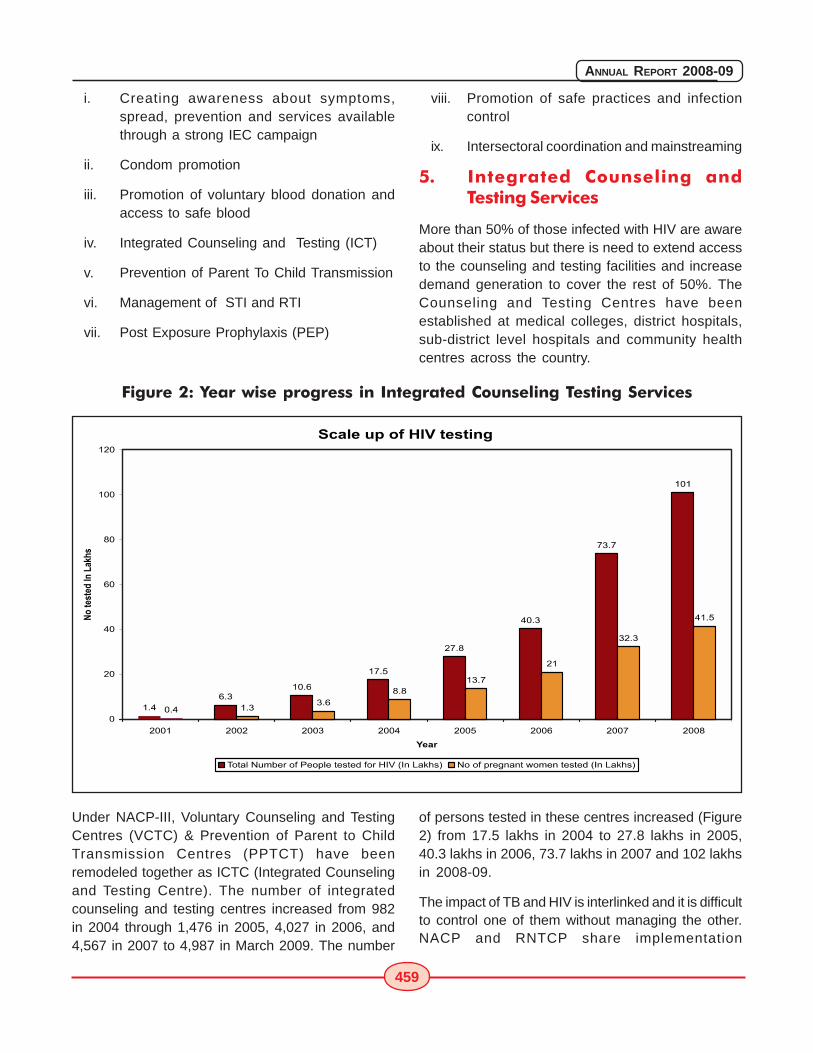
459
ANNUAL REPORT 2008-09
i. Creating awareness about symptoms,spread, prevention and services availablethrough a strong IEC campaign
ii. Condom promotion
iii. Promotion of voluntary blood donation andaccess to safe blood
iv. Integrated Counseling and Testing (ICT)
v. Prevention of Parent To Child Transmission
vi. Management of STI and RTI
vii. Post Exposure Prophylaxis (PEP)
viii. Promotion of safe practices and infectioncontrol
ix. Intersectoral coordination and mainstreaming
5. Integrated Counseling andTesting Services
More than 50% of those infected with HIV are awareabout their status but there is need to extend accessto the counseling and testing facilities and increasedemand generation to cover the rest of 50%. TheCounseling and Testing Centres have beenestablished at medical colleges, district hospitals,sub-district level hospitals and community healthcentres across the country.
Figure 2: Year wise progress in Integrated Counseling Testing Services
Under NACP-III, Voluntary Counseling and TestingCentres (VCTC) & Prevention of Parent to ChildTransmission Centres (PPTCT) have beenremodeled together as ICTC (Integrated Counselingand Testing Centre). The number of integratedcounseling and testing centres increased from 982in 2004 through 1,476 in 2005, 4,027 in 2006, and4,567 in 2007 to 4,987 in March 2009. The number
of persons tested in these centres increased (Figure2) from 17.5 lakhs in 2004 to 27.8 lakhs in 2005,40.3 lakhs in 2006, 73.7 lakhs in 2007 and 102 lakhsin 2008-09.
The impact of TB and HIV is interlinked and it is difficultto control one of them without managing the other.NACP and RNTCP share implementation
460
ANNUAL REPORT 2008-09
arrangements such as ICTC and sputum microscopycentres. HIV/TB coordination earlier emphasized onlyon cross referral of clients between the RNTCPmicroscopy centres and the ICTCs but now it is beingextended to also cross referrals between ARTCentres, CCCs & RNTCP to ensure confirmation ofdiagnosis and early treatment of TB and starting onART at the earliest for identified HIV/TB patients withCD4 counts less than 350 as per the new guideline.In 2007, there were 91,807 cross referrals fromICTCs, 1,32,146 cross referrals from RNTCP and20,925 patients were detected having HIV-TB Co-infection. In 2008, ICTC referrals were 2,49,870 andRNTCP referrals were 1,87,004; 24,320 HIV-TB co-infected patients were diagnosed.
ICTCs also provide PPTCT services to pregnantwomen. The number of pregnant women counseledand tested was 1.8 lakhs in 2004, 13.7 lakhs in 2005,
A pregnant woman being counseled under the PPTCT program
21 lakhs in 2006, 32.3 lakhs in 2007 and 46.31 lakhsin 2008.
In 2008, 21,483 pregnant women were found to beHIV positive. Women who are HIV positive are givena single dose of Nevirapine prophylaxis at the timeof labor and newborn is also given a single dose ofNevirapine within 72 hours of birth. In 2008, a totalof 10,494 mother-baby pairs were given prophylaxisdose of Nevirapine.
NACP-III aims to accomplish the following targets toexpand the outreach of ICTC services:
o All Community Health Centres to have HIVcounseling and testing services
o 24hr Primary Health Centres and Privatehospitals are also being involved
461
ANNUAL REPORT 2008-09
o Mobile ICTCs in hard to access areas incollaboration with NRHM
o Internal and External Quality assurancemechanisms
o Target of 10-15 tests per day per centre
6. Sexually Transmitted Infections(STI) Services
As STI increase the risk of HIV transmissionsignificantly, their care has been given highimportance in NACP-III (Table 3).
NACP-III envisages that about 15 million episodes
with STI/RTI wi l l be treated through theprogramme.
The STI /RTI services are being delivered throughdesignated STI/RTI clinics, TI STI clinics, a networkof STI/RTI private preferred providers and NRHM atsub-district facility.
The Regional STI Reference Research and TrainingCentres are providing high quality laboratory supportto generate scientific evidence for providing goodquality STI/RTI services through monitoring drugresistance to gonococci and implementing SyphilisEQAS so as to review the syndromic protocol on aperiodic basis.
S.No. Name of Centre Number Locationof Centers
1. Designated STI clinics 886 Medical Colleges, District hospitals,selected area hospitals and largeCHCs under SACS/NACO.
2. Targeted Intervention Clinics 1271 In the each district to cater the highrisk population
3. Community based STI/RTI 8515 STI/RTI services to be provided to theservices delivery through network HRG and the clients of HRG throughof "Private Preferred Providers" the network of Private providers"Janani" Scheme in Bihar (Allopath and non allopath) in 100
high priority districts.
4. NRHM facilities 26,415 STI/RTI services delivered at subPHC/CHC district level through NRHM facilities.
5. Regional STI Reference, research 7 In medical colleges - Safdarjung &and training centers Maulana Azad Medical College in
Delhi, Osmania Medical College inHyderabad, B.J. Medical College inAhmedabad, Institute of Serology andCalcutta Medical College in Kolkata,Institute of Venereology in Chennai &Government Medical College inNagpur.
Table 3: Details of STI Services provided under NACP-III
462
ANNUAL REPORT 2008-09
Table 4: STI/RTI episodes managed under NACP III (2008-2009)
S.No. Name of the Number of caseshealth care facility (in lakhs)
1. Designated STI/RTI Clinics 25.7
2. TI STI clinics 9.1
3. PPP Scheme 1.0
4. NRHM facilities 31.0
TOTAL 66.7
A total of 66.7 lakh STI/RTI episodes weremanaged through STI control programme in 2008-09 (Table 4) against the target of 100 lakhepisodes, giving an achievement of 66.7%. Thenumber of designated STI/RTI clinics (situated atgovernment health care facilities at district leveland above) being supported by NACO hasincreased from 845 in 2008 to 886 in 2009. Thereported number of patients accessing STI/RTIservices from these designated STI/RTI clinics andSTI clinics in Targeted interventions (TI) for HRGpopulation supported by NACO has sequentiallyincreased from over 22 lakhs in 2006, 25.9 lakhsin 2007 to 34.8 lakhs in 2008-09. About 0.8 lakhSTI/RTI episodes were also managed by thenetwork of private providers. In addition, as peravailable data, over 31 lakh episodes of STI/RTIhave been managed through sub-district level
health facilities under NRHM in 2008. There has beenan improvement in the reporting through CMIS formats.
To provide good quality STI/RTI services throughdesignated STI/RTI clinics infrastructure werestrengthened, computers were provided forstreamlining reporting, one counselor was posted ineach of these clinics, mentoring and supportivesupervision through the medical college faculty arebeing provided to improve the STI/RTI service delivery.In order to provided standardize quality of STI/RTI careNACO has procured and provided color coded drugkits and RPR/TPHA testing kits to all the designatedSTI clinics for free distribution to the patients. Capacitybuilding and training to the staffs were provided.Training material was developed in joint consultationwith NIHFW and NIRRH, cascaded model of trainingwas done. Total of 3,230 staff were trained (Table 5).
Table 5: Progress in Training under STI Services (2008-09)
S.No. Training of Staff Number of Stafftrained
1. National Resource Faculties 44
2. State Resource Faculties 183
3. Regional Resource Faculties 302
4. Medical Officer of designated STI/RTI clinics 1,022
5. Paramedical Staff (laboratory technician and staff nurse) 595
6. Counsellors 200
7. NRHM staff 884
TOTAL 3,230

463
ANNUAL REPORT 2008-09
During NACP-III, STI/RTI services are being expandedthough effective integration with the RCH-IIprogramme. NACP and RCH programmes have beenproviding training in STI/RTI to the medical andparamedical personnel based on a uniformcurriculum. NACO and RCH division have jointlydrafted technical guidelines on management of STI/RTI so as to ensure uniformity of service deliveryacross all facilities and also to build capacities ofphysicians working at sub district facility. The colorcoded drug kits will be supplied to the NRHM facilitiesfor free distribution to the patients availing g itsservices. NACO has taken initiative to do procurementof the color drug kits for NRHM facility to ensure theiravailability in all the CHC/PHC.
During 2008-09, a Public Private Partnership schemewas launched in 91 priority districts in 14 zones in 16states involving 7 agencies. This scheme wasimplemented as a pilot wherein the agenciesidentified 8,515 private practitioners (including 2,233allopaths and 6,282 non-allopaths) who were highvolume STI/RTI service providers in and around hotzones in the selected districts. These networkedproviders were trained and provided with colour-coded STD drugs to administer the syndromictreatment and provided on-site supervision. Demandgeneration activities were also carried out alongside.As of 31st March, 2009, 1,975 (88%) allopaths and
5,528 (88%) non-allopaths had been trained;1,06,684 STI/RTI cases treated; 1,49,880 clientscounseled; and 15,226 clients referred.
Efforts are being made to strengthen the STI/RTIservice delivery through targeted interventionprogramme for the HRGs. The services to the HRGare provided through TI STI clinics, Preferred PrivateProviders and through linkages to the designatedSTI/RTI clinics. A total of 9 lakh episodes of STI/RTIwere managed in this group in 2008-09.
7. Information, Education &Communication
Information, Education and Communication (IEC) isa cross-cutting and integral part of all programmecomponents of NACP-III. NACO's campaigns focusedon promotion of safe behavioral practices, reductionof stigma and discrimination, promotion of servicesfor counseling & testing and ART, increasing condomuse and voluntary blood donation. Special emphasishas been given to address youth and women whoare more vulnerable to HIV infection. An allocation ofRs. 167.3 crores was made under IEC for NACO andSACS during 2008-09.
7.1. The Response to Red Ribbon ExpressProject:
The Red Ribbon Express (RRE) is one of the world's
464
ANNUAL REPORT 2008-09
largest mass mobilization campaign on HIV/AIDS.Conceptualized by the Rajiv Gandhi Foundation, thecampaign was implemented by NACO in collaborationwith the Ministry of Railways, Ministry of Youth Affairsand UNICEF to spread awareness on HIV/AIDS andpromote safe behavioral practices. The RRE trainconsisted of seven coaches with three coacheshaving exhibition on issues concerning HIV/ AIDS andNRHM messages, one coach dedicated toorientation/sensitization of selected groups such asgovernment officials, teachers, members ofpanchayati raj institutions, anganwadi workers, selfhelp groups, youth and women, and one coachearmarked for counselling with referral services. Thetrain was flagged off by Mrs. Sonia Gandhi,
Chairperson, UPA on the World AIDS Day i.e. 1stDecember 2007 from Delhi. It completed its journeyon 1.12.2008 after traveling over 27,000 kms duringthe year covering 180 districts/halt stations. Attachedto the train were two buses with song and dramatroupes and condom demonstration outlets whichcovered the periphery of the districts through whichthe train passed. The cultural troupes of NYKStravelling in the train spread to nearby villages ofthe halt stations to spread HIV/AIDS messagescovering 30,685 villages. The project covered 41,334villages and reached to 6.2 million people. 68,244people were trained on board the train in the districtsthough which it passed and 1,16,183 people werecounseled on HIV/AIDS.
Glimpses from Red Ribbon Express

465
ANNUAL REPORT 2008-09
7.2. Mass Media Campaign:
The messages on different aspects of HIV/ AIDS weredisseminated through mass media including TV(Doordarshan and Cable & Satellite channels) andRadio (AIR and private FM radio stations). The majorcampaigns conducted through mass media includedthree phases of campaign on condom normalizationnamely, "Jo Jeeta Wohi Sikander" (kabaddi, ringtone and dog), "Condom, it's OK", campaigns on ICTCand PPTCT services, HIV-TB linkage, ART, voluntaryblood donation and stigma & discrimination. Eightepisodes on HIV/ AIDS were broadcast as part of theKalyani programme on Doordarshan on the statenetworks of nine states of Uttar Pradesh,Uttarakhand, Bihar, Jharkhand, Madhya Pradesh,Chattisgarh, Rajasthan, Assam and Orissa inDecember 2008-January 2009. Radio programmeswere started by 13 states on state networks focusingon youth and women. NACO released over 27,000spots on radio and 51,000 on various TV channelson different themes related to HIV/AIDS in additionto releases made by the SACS.
7.3. Multi-Media, Mid-Media and otherinitiatives:
Building on the success of RRE field campaignthrough IEC vans, NACO implemented a mid-mediacampaign in collaboration with SACS primarilytargeting A and B category districts and some highpriority districts with high out-migration. The campaignbranded as "Zindagi Zindabad" comprised exhibitionand film shows through IEC vans, folk theatre showsby song and drama troupes and condomdemonstration stalls. This campaign launched in thestates of Andhra Pradesh, West Bengal,Maharashtra, Uttarakhand, Jammu & Kashmir,Madhya Pradesh, Gujarat, Orissa, HimachalPradesh, Chattisgarh, Jharkhand and Keralareceived an overwhelming response. A total of 10,000folk/street theatre performances were done duringthe field campaigns.
7.4. Mainstreaming HIV for multi-sectoralresponse:
7.4.1. Constitution of the State Councils on AIDS(SCA): As a follow up to the formation of National
Council on AIDS, 23 States / Union Territories haveconstituted the SCA which are guiding and supportingthe mainstreaming efforts at the state level. Severalministries are in the process of mainstreaming HIV/AIDS issues into their polices and programmes. Somenoteworthy achievements are inclusion of HIV/ AIDSas an agenda point for discussions in the meetingsof the three-tier Panchayati Raj Institutions,installation of condom vending machines in ITDChotels, concession in railway fare to People Livingwith HIV/ AIDS for visiting the nearest ART centre,training on HIV/ AIDS of about one lakh persons fromdifferent ministries/departments, corporate andNGOs/CBOs, establishment of seven ART centersin Public Private Partnership with five more in theprocess of establishment. In order to address thevulnerabilities of women, a policy document andoperational plan on "women and HIV" was releasedto facilitate mainstreaming of HIV/ AIDS with womenissues under the various programmes of thegovernment. Action plan with operational guidelinesfor addressing the vulnerabilities of the tribalpopulation are being finalized.
7.4.2. Mainstreaming with civil societyorganizations: Along with mainstreaming HIV withinthe training and education system of cooperativesto reach 500,000 members of cooperatives offisheries, agriculture, labour, dairy and weavers,NACO is also supporting 13 innovative short termprojects on stigma and discrimination through whichchildren affected by HIV, their families and issues oflivelihood will be addressed.
7.4.3. Greater Involvement of People Livingwith HIV (GIPA) under NACP-III: NACP III hasoutlined steps in establishing systems, structures andvarious activities to meaningfully involve people livingwith HIV (PLHIV) in programme design andimplementation to reduce stigma and discriminationassociated with the infected and affected persons.This will also enhance their access to prevention andquality treatment, care, insurance and legal services.Support from NACO has enabled the Indian Networkof Positive People to establish and strengthen up to22 state level networks and 221 district level networksof people living with HIV. These networks aim to
466
ANNUAL REPORT 2008-09
Condom demonstration at an ICTC
mobilize the communities to ensure communityaccess to various services, like ART Centre,Community Care Centres, and Drop-in centers (DIC).At present, a total of 204 DIC are operational acrossthe country out of which 127 are in the 'A' categorydistricts and 27 in the 'B' category districts. NACO isworking towards establishing DIC in all A and Bcategory districts.
7.4.4. Youth interventions, in-school, college,and out-of-school: The Adolescence EducationProgramme (AEP) is placed as a key intervention tohelp adolescents cope with negative peer pressure,develop positive behaviour, improve sexual healthand prevent HIV infections. The Ministry of HumanResource Development is implementing theAdolescence Education Programme (AEP) incollaboration with NACO classroom based co-curricular activity. During 2008-09, 92,000 schoolswere covered under the programme as compared to1,14,000 schools in 2007-08. The programme couldnot be implemented in some states during 2008-09due to the ban/ suspension in view of the protestsfrom some quarters against the toolkit (Flip Chartand Teachers Workbook) over certain pictures. As afollow up, a national toolkit review committeecomprising of educationists, psychologists,representatives of NGO, parents and teachersdeveloped a prototype toolkit which is under the
process of adaptation in different states through statelevel consultations with various stakeholders suchas teachers, academicians, parents, NGOs, andmedia among others. The states which havecompleted the adaptation process of the materialinclude Andhra Pradesh, Tamil Nadu, Kerala, Punjab,West Bengal, Assam, Jharkhand and Maharashtra.Six workshops were organized by these States at Stateand District levels with various stakeholders such asparents, teachers, NGOs, media, political leadershipto seek feedback for the finalization of the saidmaterial under the Adolescence EducationProgramme.
7.4.5. Red Ribbon Clubs in colleges (RRC): Theformation of RRC as a peer-based intervention ininstitutions of higher education was taken up as amajor initiative during 2008-09. The RRC organize anumber of activities such as debates, quiz and essaycompetitions to spread knowledge on HIV/ AIDS. Thepromotion of voluntary blood donation is one of themajor objectives of the RRC. During 2008-09, 4,530RRC were functional in the colleges.
8. Condom Promotion
The NACP-III envisages significant expansion in thecondom use through social marketing for whichpartnerships with private sector and social marketingorganizations were planned.
Interactive session in progress at a youthintervention site in Maharashtra
467
ANNUAL REPORT 2008-09
8.1. Scaling up condom social marketing:NACO supported the social marketing programmesin various states during 2008-09. These programmeswere initially extended for a six month period duringwhich a total of 856 lakh condoms, against the targetof 750 lakh condoms, were marketed and over 2.7lakh outlets, against the target of 2.4 lakh outlets,were covered with socially marketed condoms. Withthe focus on expanding the retail outlet and coverageof non-traditional outlets, 71% of the outlets werethe non-traditional outlets.
Table 6: Retail Condom offtake
(In lakh pieces)
2006-07 2007-08 2008-09
Social market 6395 6393 8353
Commercial 3837 4386 6313
Free 12875 7750 7465
TOTAL 23107 18529 22131
During 2008-09, socially marketed condom off-takeof 83.53 crore pieces (Table 6) and outlet reach of12 lakhs were achieved.
8.2. Scaling up Female Condom Programme:Based on the pre-programme assessment of theFemale Condom Programme, NACO scaled up theFemale Condom Programme in Andhra Pradesh,Tamil Nadu, Maharashtra and West Bengal tosaturate all female sex worker TargetedInterventions. The peer-led programme aims to buildcapacity of two lakh female sex workers. During2008-09, 15 lakh female condoms were procuredfor the programme.
8.3. Installation of Condom VendingMachine: During the year 2008-09, four metrocities and two large towns in Uttar Pradesh weretargeted for the installation of condom vendingmachines. Against 10,025 targeted number ofCVM, 8,500 CVM have already been installed.During 2008-09, 7,50,000 condoms were soldthrough these CVM.
Condom Vending Machine
9. Blood Safety:
� ensuring that regular (repeat) voluntary non-remunerated blood donors constitute themain source of blood supply through phasedincrease in donor recruitment and retention;
� establishing blood storage centres in theprimary health care system for availability ofblood in far-flung remote areas;
� vigorously promoting appropriate use ofblood, blood components and blood productsamong the clinicians; and
� developing long-term policy for capacitybuilding to achieve efficient and self sufficientblood transfusion services.
9.1 Blood collection :
Access to safe blood is ensured by a network of 1,092blood banks including 104 Blood ComponentSeparation Units (BCSU) and 10 Model Blood Banks.NACO supported the installation of blood componentseparation units and also funded modernization ofall major blood banks at state and district levels. Inaddition to constantly enhancing awareness aboutthe need to access safe blood and blood products,NACO has supported the procurement ofequipments, test kits and reagents as well as the
468
ANNUAL REPORT 2008-09
People donating blood at a Blood Bank
recurring expenditure of government blood banksand those run by charitable organizations that weremodernized.
Based on population standards, the requirement ofblood for the country is estimated to be 100 lakhunits annually, whereas the available supply was 74lakh units in 2008-09. During this period, 61.7% ofblood was collected through Voluntary BloodDonation programme. The states of West Bengal,Maharashtra, Tamil Nadu, Gujarat, Tripura, AndhraPradesh, Orissa, Madhya Pradesh, Chandigarh andHimachal Pradesh crossed the national target withover 65% achievement in voluntary blood donationand are good performing states. The states of U.P.,Uttarakhand, Rajasthan, Haryana, Punjab, Jammuand Kashmir, Bihar, Jharkhand, Chattisgarh, Kerala,Delhi, Assam, Manipur, Nagaland and Sikkim are poorperforming states as their achievement for voluntaryblood donation is under 45%.
Several activities have been undertaken, incollaboration with NGOs, to promote publicawareness of the need for voluntary blood donation.In addition, through collaboration with the Indian Red
Cross Society, voluntary blood donation camps andother activities are regularly undertaken to increaseblood collection in the country. During the year 2008-09, 56,568 blood donation camps were organized.The target is to raise voluntary blood donation to 90% by end of NACP-III.
9.2. Strengthening of Blood bank facilities:
9.2.1. District level Blood Banks: In NACP-III, 39newly created districts have been identified whichdo not have a full-fledged blood bank. NACO hastaken the initiative with the respective State Healthdepartment for setting up a blood bank in thesedistricts. Eight blood banks have been madeoperational. In six districts, construction of the buildingis going on and these will be made functional in 2009-10. In the remaining districts, instructions were issuedto set up Blood Storage Centres, till the time the bloodbanks are made operational.
9.2.2. Blood Component Separation Units: Inorder to promote rational use of blood, 103 BloodComponent Separation Units (BCSU) have beenestablished. During NACP-III, 80 component
469
ANNUAL REPORT 2008-09
separation facilities are proposed to be establishedin all the blood banks in tertiary care hospitals attachedto medical colleges. During 2008-09, 19 blood bankswere upgraded as BCSU. Procurement of essentialequipment for the first 40 BCSUs was initiated in 2007-08 and the entire delivery schedule has beencompleted. For remaining 40 blood banks, theprocurement will be completed by July-August 2009.
9.2.3. Blood Storage Centres: The Governmentof India has taken the initiative of setting up BloodStorage Units, in order to ensure safe and qualityblood available in FRUs where a full-fledged bloodbank is not feasible. The National Rural HealthMission (NRHM) and NACO have taken a joint effortto start Blood Storage Units in the First ReferralUnits (FRU). The NRHM will provide the requisiteinfrastructure and manpower, and procure thenecessary equipments for storage and issue ofblood. The NACO will provide an annual recurringgrant of Rs. 10,000 for procurement ofconsumables, linking the centres with the nearestRegional Blood Transfusion Centres (RBTC) forsupply of screened blood on a regular sustainedbasis and training of the staff attached to the storagecentres. It has been proposed to establish 3,222blood storage centres in the identified FRU duringNACP-III. During 2008-09, 425 blood storage unitswere made operational.
9.2.4. Blood Refrigerated Vans: NACO has takenthe initiative to provide 500 refrigerated BloodTransportation Vans to the RBTCs/District Bloodbanks during NACP-III. These vans will transfer bloodunits to the BSC regularly and also on demand/emergency situations. During 2008-09, procurementof 250 Blood Transportation Vans and 1,000 BloodTransportation Boxes (4 Blood Transportation Boxesand 1 Blood Transportation Van is considered to beOne Unit) was initiated by UNOPS. These vans willbe supplied to states by December 2009.
9.3. Blood Safety Training Programme:
Training is essential element to every aspect of bloodsafety. NACO has developed a uniform trainingcurriculum for all aspects of blood transfusion.
Centres have been identified across the country toimpart training on all aspect of Blood Safety involvingBlood Bank personnel, Clinicians and DonorMotivators. During 2008-09, 740 doctors, 1527laboratory technicians and 587 nurses have beentrained in 17 training institutions; 186 counsellorsappointed in BCSU and Major blood Banks were alsotrained.
9.4. Monitoring of blood banks
It is envisaged that quality practices in blood bankactivities can be improved by strengtheningmonitoring and evaluation system by making regularsupervisory visit.
With a large network of blood banks and BloodComponent Separation Facilities in the country, it isessential to supervise various activities undertakenboth among blood bank as well as voluntary blooddonation at different levels.
A State core team has been constituted in everystate to carry out the inspection of each blood bankin the state and voluntary blood donation camps.This core team comprise of three members, whichinclude one Blood Safety Official of SACS, Directorof State Blood Transfusion Council (SBTC) and twonominated experts in the field of TransfusionMedicine. The team makes periodic supervisory visitto the blood banks in their state to assess thefunctional status of the blood banks and preparereport identifying the various constraints andmethods to rectify them.
During 2008-09, supervisory visits to 1068 bloodbanks were undertaken by these teams. Officials ofNACO also made supervisory visits to blood banksduring their visit to each State to inspect the qualitychecks, functional efficiency, identify crisis and toverify the facts as reported (checking of themaintained records).
9.5. Newer initiatives
9.5.1. Centre of Excellence in TransfusionMedicine: As a step to improve the blood transfusionservices in the country, a proposal to set up fourModern Blood Banks as Centres of Excellence in the

470
ANNUAL REPORT 2008-09
four metropolitan cities - New Delhi, Mumbai, Kolkataand Chennai - was submitted for approval. TheseBlood Banks are proposed to be the State-of-the-Artfacilities. The Cabinet Committee approved theproject on 31st July 2008. NACO is liaising with theState Governments of Delhi, Maharashtra, WestBengal and Tamil Nadu to provide land of 1,00,000square feet for the purpose. Expression of Interesthas been issued to invite various entrepreneurs forarchitectural layout and construction of the building.The process for finalizing the Architect andConstruction Company is under way.
9.5.2. Plasma Fractionation Centre: Largevolume of excess plasma in the country is gettingdiscarded, as the Plasma Fractionation Centre inMumbai has not been made functional. The plasmaproducts are being imported from abroad to meetthe patient’s demand and thereby exposing thepatients to diseases prevalent abroad but absentin India. There is an urgent need of a larger plant ofPlasma Fractionation to meet the demand of thecountry. Under the National AIDS Control Programme– Phase III, one more Plasma Fractionation Centrewith a processing capacity of more than 1,50,000litres of plasma, which can fulfill the demand of theNation, has been proposed. The CabinetCommittee has approved the project on 8th October2008. The work on this project will be initiated afterfinal approval on selection of site and DPR.
9.5.3. National Blood Transfusion Authority:
The Government of India has taken the initiative toestablish National Blood Transfusion Authority(NBTA) for development of a world class BloodProgramme in India. NBTA Network will have the totaland ultimate responsibility of ensuring that thecountry’s blood, blood components and bloodproducts supply is accessible, adequate, safe andof the highest quality. It will be responsible forassessing and consolidating the demand andutilization of blood, blood components and bloodproducts throughout the country and ensuring thatthese requirements are met in the most efficient and
effective manner. A Cabinet note on National BloodTransfusion Authority has been prepared andsubmitted to the Ministry for approval.
9.6. Status of utilization of funds
During 2008-09, Rs. 125.02 Crores was allocated forblood safety activities, and the total expenditureincurred was Rs. 120.8 Crores.
10. Care, Support and Treatment forPeople Living with HIV/AIDS(PLHA)
The Care, support and treatment programme underNACP III includes comprehensive management ofPLHA with respect to treatment and prevention ofOpportunistic infections, Antiretroviral therapy (ART),psychosocial support, home based care, positiveprevention and impact mitigation.
The treatment of Opportunistic infections hasalways been an integral part of National AIDSControl programme (NACP) right from thebeginning. Since the launch of Phase - II of theNational AIDS Control Programme (NACP) in 1999,the Government of India (GOI) starting providinglow cost care to people living with HIV/AIDS, in orderto mitigate the impact of HIV related opportunisticinfections. However, high costs and demandingtreatment regimens were the major barriers inintroducing NACP. With advent of new ARV drugswith lesser side effects and lowered costs, it wasconsidered appropriate to introduce provisioningfree ART through public sector health facilities in aphased manner. The Union Ministry for Health &Family Welfare finalized and announced a strongpolicy-cum-programme commitment for provisioninganti-retroviral treatment free of cost, withimplementation starting on 1st April, 2004.
Any person who has a confirmed HIV infection issubjected to further evaluation for determining whetherhe requires ART or not by performing CD4 count andother baseline investigations. All those eligible as pertechnical guidelines are started on ART.
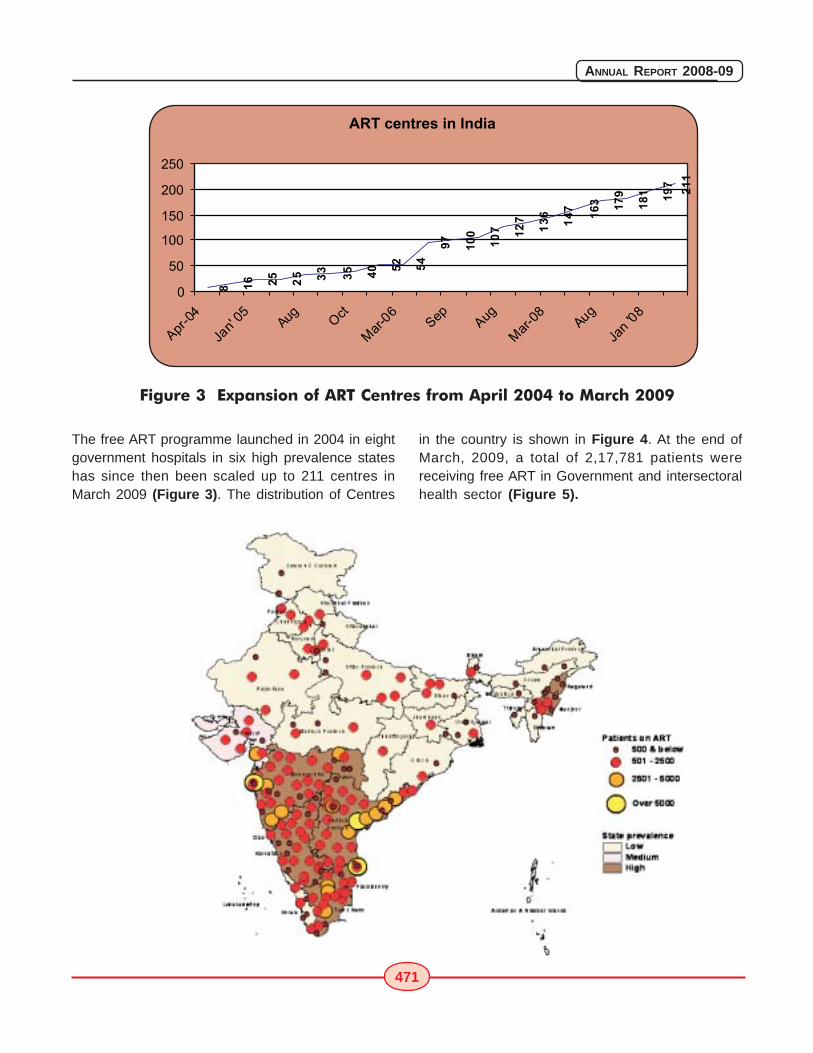
471
ANNUAL REPORT 2008-09
The free ART programme launched in 2004 in eightgovernment hospitals in six high prevalence stateshas since then been scaled up to 211 centres inMarch 2009 (Figure 3). The distribution of Centres
Figure 3 Expansion of ART Centres from April 2004 to March 2009
in the country is shown in Figure 4. At the end ofMarch, 2009, a total of 2,17,781 patients werereceiving free ART in Government and intersectoralhealth sector (Figure 5).
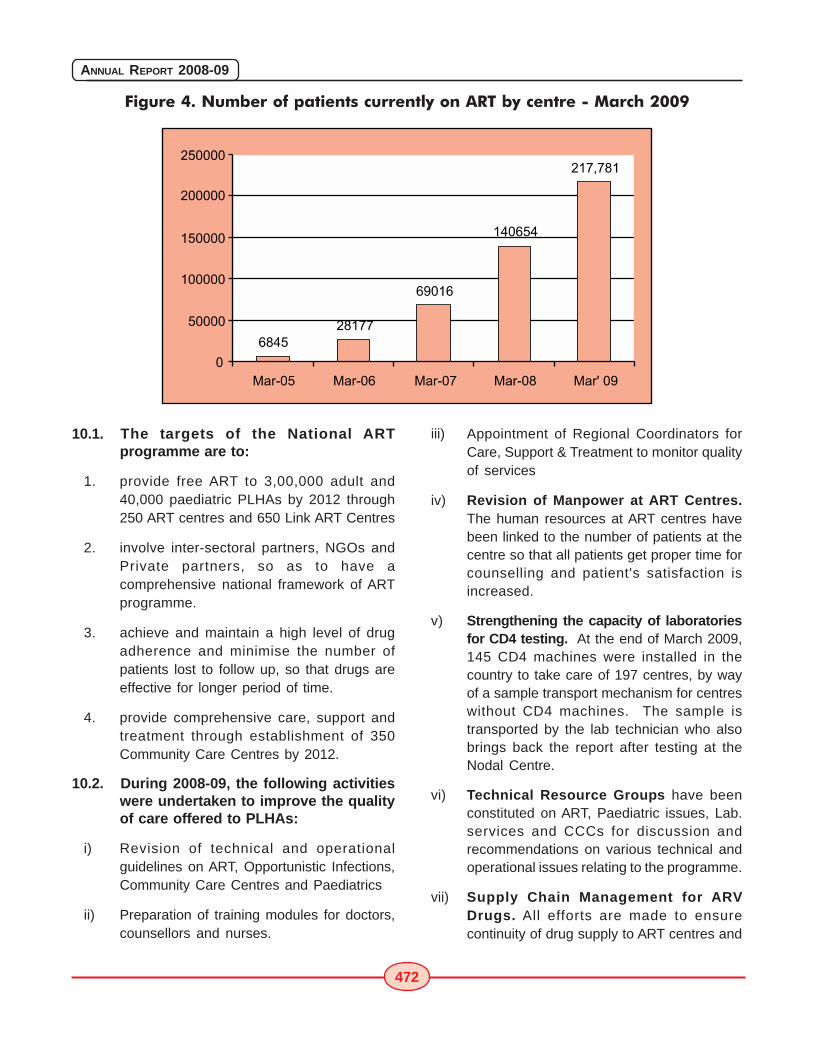
472
ANNUAL REPORT 2008-09
Figure 4. Number of patients currently on ART by centre - March 2009
10.1. The targets of the National ARTprogramme are to:
1. provide free ART to 3,00,000 adult and40,000 paediatric PLHAs by 2012 through250 ART centres and 650 Link ART Centres
2. involve inter-sectoral partners, NGOs andPrivate partners, so as to have acomprehensive national framework of ARTprogramme.
3. achieve and maintain a high level of drugadherence and minimise the number ofpatients lost to follow up, so that drugs areeffective for longer period of time.
4. provide comprehensive care, support andtreatment through establishment of 350Community Care Centres by 2012.
10.2. During 2008-09, the following activitieswere undertaken to improve the qualityof care offered to PLHAs:
i) Revision of technical and operationalguidelines on ART, Opportunistic Infections,Community Care Centres and Paediatrics
ii) Preparation of training modules for doctors,counsellors and nurses.
iii) Appointment of Regional Coordinators forCare, Support & Treatment to monitor qualityof services
iv) Revision of Manpower at ART Centres.The human resources at ART centres havebeen linked to the number of patients at thecentre so that all patients get proper time forcounselling and patient's satisfaction isincreased.
v) Strengthening the capacity of laboratoriesfor CD4 testing. At the end of March 2009,145 CD4 machines were installed in thecountry to take care of 197 centres, by wayof a sample transport mechanism for centreswithout CD4 machines. The sample istransported by the lab technician who alsobrings back the report after testing at theNodal Centre.
vi) Technical Resource Groups have beenconstituted on ART, Paediatric issues, Lab.services and CCCs for discussion andrecommendations on various technical andoperational issues relating to the programme.
vii) Supply Chain Management for ARVDrugs. All efforts are made to ensurecontinuity of drug supply to ART centres and
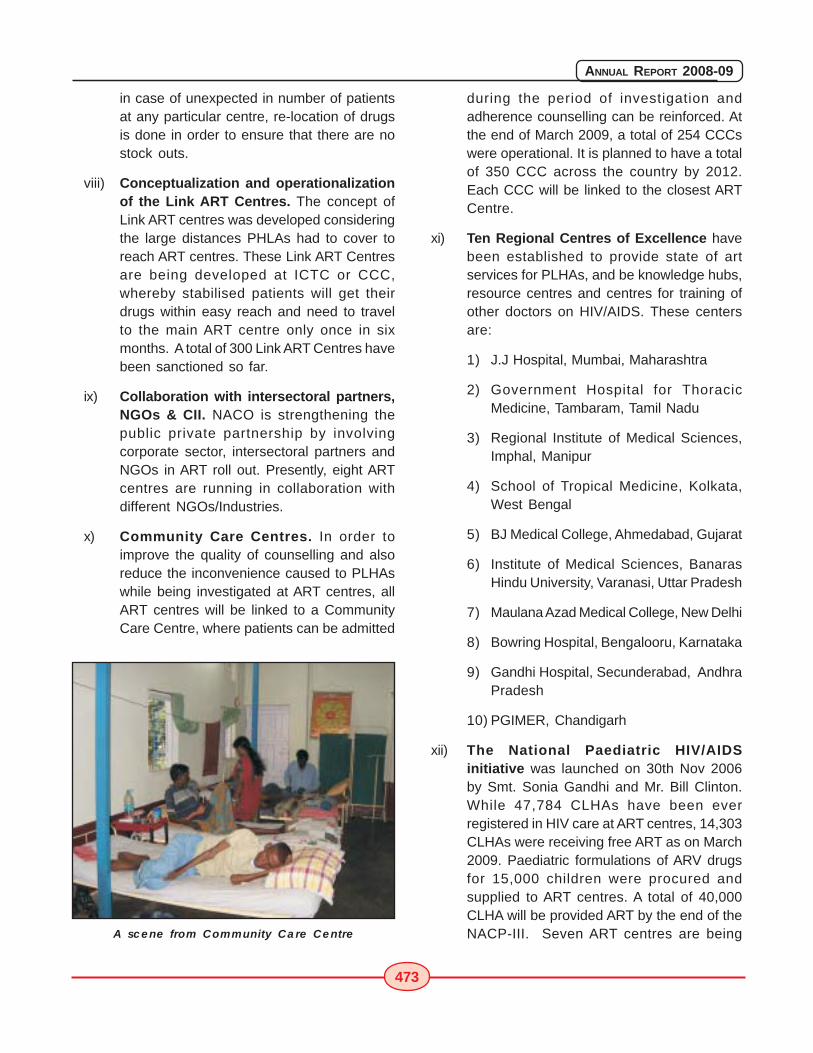
473
ANNUAL REPORT 2008-09
in case of unexpected in number of patientsat any particular centre, re-location of drugsis done in order to ensure that there are nostock outs.
viii) Conceptualization and operationalizationof the Link ART Centres. The concept ofLink ART centres was developed consideringthe large distances PHLAs had to cover toreach ART centres. These Link ART Centresare being developed at ICTC or CCC,whereby stabilised patients will get theirdrugs within easy reach and need to travelto the main ART centre only once in sixmonths. A total of 300 Link ART Centres havebeen sanctioned so far.
ix) Collaboration with intersectoral partners,NGOs & CII. NACO is strengthening thepublic private partnership by involvingcorporate sector, intersectoral partners andNGOs in ART roll out. Presently, eight ARTcentres are running in collaboration withdifferent NGOs/Industries.
x) Community Care Centres. In order toimprove the quality of counselling and alsoreduce the inconvenience caused to PLHAswhile being investigated at ART centres, allART centres will be linked to a CommunityCare Centre, where patients can be admitted
during the period of investigation andadherence counselling can be reinforced. Atthe end of March 2009, a total of 254 CCCswere operational. It is planned to have a totalof 350 CCC across the country by 2012.Each CCC will be linked to the closest ARTCentre.
xi) Ten Regional Centres of Excellence havebeen established to provide state of artservices for PLHAs, and be knowledge hubs,resource centres and centres for training ofother doctors on HIV/AIDS. These centersare:
1) J.J Hospital, Mumbai, Maharashtra
2) Government Hospital for ThoracicMedicine, Tambaram, Tamil Nadu
3) Regional Institute of Medical Sciences,Imphal, Manipur
4) School of Tropical Medicine, Kolkata,West Bengal
5) BJ Medical College, Ahmedabad, Gujarat
6) Institute of Medical Sciences, BanarasHindu University, Varanasi, Uttar Pradesh
7) Maulana Azad Medical College, New Delhi
8) Bowring Hospital, Bengalooru, Karnataka
9) Gandhi Hospital, Secunderabad, AndhraPradesh
10) PGIMER, Chandigarh
xii) The National Paediatric HIV/AIDSinitiative was launched on 30th Nov 2006by Smt. Sonia Gandhi and Mr. Bill Clinton.While 47,784 CLHAs have been everregistered in HIV care at ART centres, 14,303CLHAs were receiving free ART as on March2009. Paediatric formulations of ARV drugsfor 15,000 children were procured andsupplied to ART centres. A total of 40,000CLHA will be provided ART by the end of theNACP-III. Seven ART centres are beingA scene from Community Care Centre
474
ANNUAL REPORT 2008-09
upgraded as Regional Paediatric Centres ofExcellence to provide comprehensivespecialized services to CLHA.
xiii) The Roll out of Second line ART beganfrom January 2008. Initially started at two sites-GHTM, Tambaram and JJ Hospital, Mumbai- on a pilot basis, it was expanded to 10centres of excellence in January 2009. Aprovision was made for providing second linedrugs to 3,000 patients during 2008-09. Asof March 2009, 344 patients were receivingsecond line drugs.
11. Institutional Strengthening andCapacity Building
The aim of NACP-III is to build capacity of theprogramme managers at the national, state anddistrict levels in leadership and strategic management;technical and communication skills of the healthprofessionals and health care providers at all levelsof care and health care organizations, CBOs andNGOs; and technical, communications andcounselling skills of the grass-roots level workers andfunctionaries of various government departments.
Strengthening Human Resource Capacity at NACOby enhancing strategic planning skills, disseminatingbest practices for TIs, establishing and managing anetwork of technical expertise through TechnicalResource Groups (TRGs) in STI/HIV/AIDS,conducting OR and to oversee R&D activitiesnationwide, are some of the thrust areas forstrengthening institutional capacity. NACO has alsodeveloped Project's financial management systemfor effective financial management of the programme.
Regional and state level training were organised aspart of capacity building for health care providers.During 2008-09, a total of 1,35,615 persons weretrained, including specialist doctors of medicalcolleges, general DMOs, nurses, IEC officers,counsellors, NGOs, laboratory technicians, bloodbank officials and district nodal officers. During thisperiod review and printing of training curricula,modules and materials was undertaken, guidelinesfor District Action Plans were laid down, training of
national and state level trainers was completed andrefresher/induction training and Training of Trainerswere held.
12. Strategic InformationManagement
India's response to the evolving HIV epidemic islargely influenced by the available surveillance data,implementation capacities and political commitmentat state level. The HIV surveillance system in Indiahas been characterized by a growing network ofsentinel and facility based HIV sero-prevalencesurveys, used for measuring trends in HIV prevalenceand developing state and national prevalenceestimates. Behavioral surveillance surveys andresearch studies have also been conducted in anumber of states to track HIV related risk behaviours.The Computerized Management Information System(CMIS), established nation-wide, is another sourceof strategic information for programme monitoringand evaluation. NACP has also successfullyestablished a Computerized Project FinancialManagement System (CPFMS).
In order to maximize effective use of all availableinformation and implement evidence based planning,NACP-III established a Strategic InformationManagement Unit (SIMU). It is set up at national andis being set up at state levels to address strategicplanning, monitoring and evaluation, surveillance andresearch. SIMU will assist NACP-III in tracking theepidemic and the effectiveness of the response andhelp assess how well NACO, SACS and all partnerorganizations are fulfilling their commitment to meetagreed objectives.
Key activities being undertaken are
� Establishing a Research Wing/ Division atNACO with strong linkages developed withresearch/academic institutions at regional/state level;
� Strengthening operations research andevaluation studies on the design, strategies,implementation and testing of HIV interventionprogrammes and measure their impactrelated to risk/vulnerability reduction,
475
ANNUAL REPORT 2008-09
behaviour change, stigma reduction, HIVprevalence rate etc.;
� Building capacity for monitoring andevaluating community based interventions,school based adolescent educationprogrammes and support groups of positivepeople;
� Conducting two types of BehaviouralSurveillance Survey, namely, a) annual riskassessment at the district level and b)methodologically rigorous IntegratedBiological and Behavioural Surveillance(IBSS) at district level, once in three years.
12.1. Monitoring and Evaluation
Following activities were undertaken:
12.1.1. Development of an integrated M&E Planfor NACP-III. Based on the principle of three ones,using the M&E strengthening tool, a comprehensiveM&E plan is developed. This plan lays down the basicrules, definitions and operating procedures to ensurea strong M&E system to monitor progression of HIVepidemic in India as well as tracking the performanceof the program in country. This consist of OperationalGuideline for Strategic Information Management Unit(SIMU) and a handbook of core indicators givingdetails of definitions, source of collection, frequency,level of use and strengths and limitations.
12.1.2. Strengthening systems for better M&E.An assessment of existing systems was doneincluding manpower, infrastructure, hardware andsoftware and connectivity etc. Recruitment wasclosely monitored so as to have required capacitiesin place. To ensure supportive supervision, a systemof quarterly review and training of M&E Officers isinitiated. A review on quantity and quality of reportingis done. Directions & guidelines for on-siteverifications are developed and sent to SACS.
12.1.3. Improving Component Specific M&E
1) ART Centers: Training of Trainers organized forimproving recording and reporting includingcomputerization at ART centers. The training of ARTstaff is being organized across the country to cover
all ART centers. The training focuses on basicdefinitions of indicators, orientation on M&E systemsand data analysis and use on critical indicators. AnM&E Training module is developed for purpose withsupport from WHO. The patient tracking software isfurther modified to give list reports and analyticalreports for ART center in-charges and programofficers at SACS and NACO level. Team approachwas used for these training so that there is completeunderstanding of the issue and systems and rolesand responsibilities. For these trainings, PSM in-charges of medical colleges were trained and arebeing used as resource.
2) Integrated Counseling and Testing Centres:For improving HIV-case reporting, it is essential thatthe recording systems at ICTC's are improved. Thestaff at ICTC also need to be oriented on M&E Systemsand computerization. A client line-listing software hasbeen prepared with support from KHPT and is beingpilot tested. An extensive training of ICTC staff (mainlycounselors) on M&E, including basics of computersand the software, is planned. NIIT Ltd. Is beingcontracted for undertaking this training.
3) STI/RTI Reporting: This is one of the componentswhose reporting performance is chronically sub-optimal. The overall efforts for improving theperformance by simplifying the tools, training on thedefintions, communicating clear guidelines andhighlighting issues for action in review meetings ofM&E officers and program officers is helping inimproving reporting - both quality and quantity. TheM&E sessions in trainings of Joint Directors/DeputyDirectors of STD in SACS has also an impact onbetterment.
4) Community Care Centers: A simple uniformrecord-keeping system has been developed toimplement at CCC's. An M&E manual has also beendeveloped, which is being reviewed beforeundertaking the training of CCC staff on M&E.
12.1.4. Improving CMIS and overall Reporting
For improving reporting, a systematic approach wastaken. Some immediate changes in terms of refiningand developing a few output reports, developing
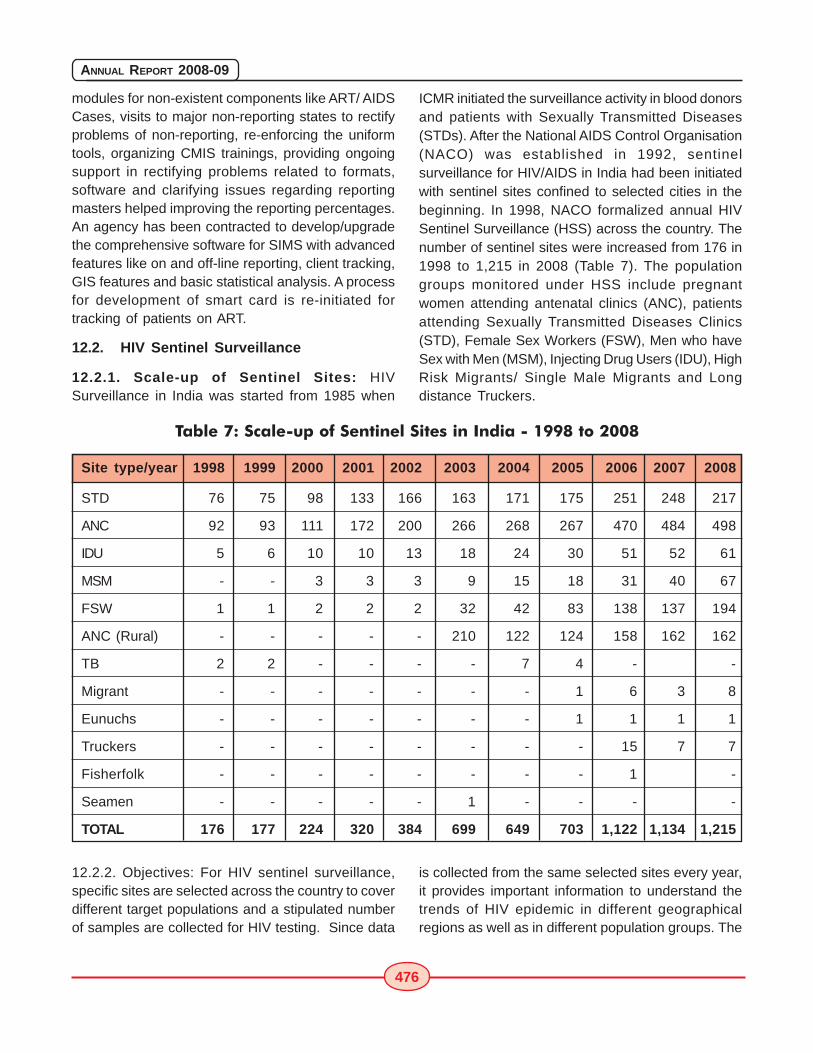
476
ANNUAL REPORT 2008-09
modules for non-existent components like ART/ AIDSCases, visits to major non-reporting states to rectifyproblems of non-reporting, re-enforcing the uniformtools, organizing CMIS trainings, providing ongoingsupport in rectifying problems related to formats,software and clarifying issues regarding reportingmasters helped improving the reporting percentages.An agency has been contracted to develop/upgradethe comprehensive software for SIMS with advancedfeatures like on and off-line reporting, client tracking,GIS features and basic statistical analysis. A processfor development of smart card is re-initiated fortracking of patients on ART.
12.2. HIV Sentinel Surveillance
12.2.1. Scale-up of Sentinel Sites: HIVSurveillance in India was started from 1985 when
ICMR initiated the surveillance activity in blood donorsand patients with Sexually Transmitted Diseases(STDs). After the National AIDS Control Organisation(NACO) was established in 1992, sentinelsurveillance for HIV/AIDS in India had been initiatedwith sentinel sites confined to selected cities in thebeginning. In 1998, NACO formalized annual HIVSentinel Surveillance (HSS) across the country. Thenumber of sentinel sites were increased from 176 in1998 to 1,215 in 2008 (Table 7). The populationgroups monitored under HSS include pregnantwomen attending antenatal clinics (ANC), patientsattending Sexually Transmitted Diseases Clinics(STD), Female Sex Workers (FSW), Men who haveSex with Men (MSM), Injecting Drug Users (IDU), HighRisk Migrants/ Single Male Migrants and Longdistance Truckers.
Table 7: Scale-up of Sentinel Sites in India - 1998 to 2008
Site type/year 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
STD 76 75 98 133 166 163 171 175 251 248 217
ANC 92 93 111 172 200 266 268 267 470 484 498
IDU 5 6 10 10 13 18 24 30 51 52 61
MSM - - 3 3 3 9 15 18 31 40 67
FSW 1 1 2 2 2 32 42 83 138 137 194
ANC (Rural) - - - - - 210 122 124 158 162 162
TB 2 2 - - - - 7 4 - -
Migrant - - - - - - - 1 6 3 8
Eunuchs - - - - - - - 1 1 1 1
Truckers - - - - - - - - 15 7 7
Fisherfolk - - - - - - - - 1 -
Seamen - - - - - 1 - - - -
TOTAL 176 177 224 320 384 699 649 703 1,122 1,134 1,215
12.2.2. Objectives: For HIV sentinel surveillance,specific sites are selected across the country to coverdifferent target populations and a stipulated numberof samples are collected for HIV testing. Since data
is collected from the same selected sites every year,it provides important information to understand thetrends of HIV epidemic in different geographicalregions as well as in different population groups. The
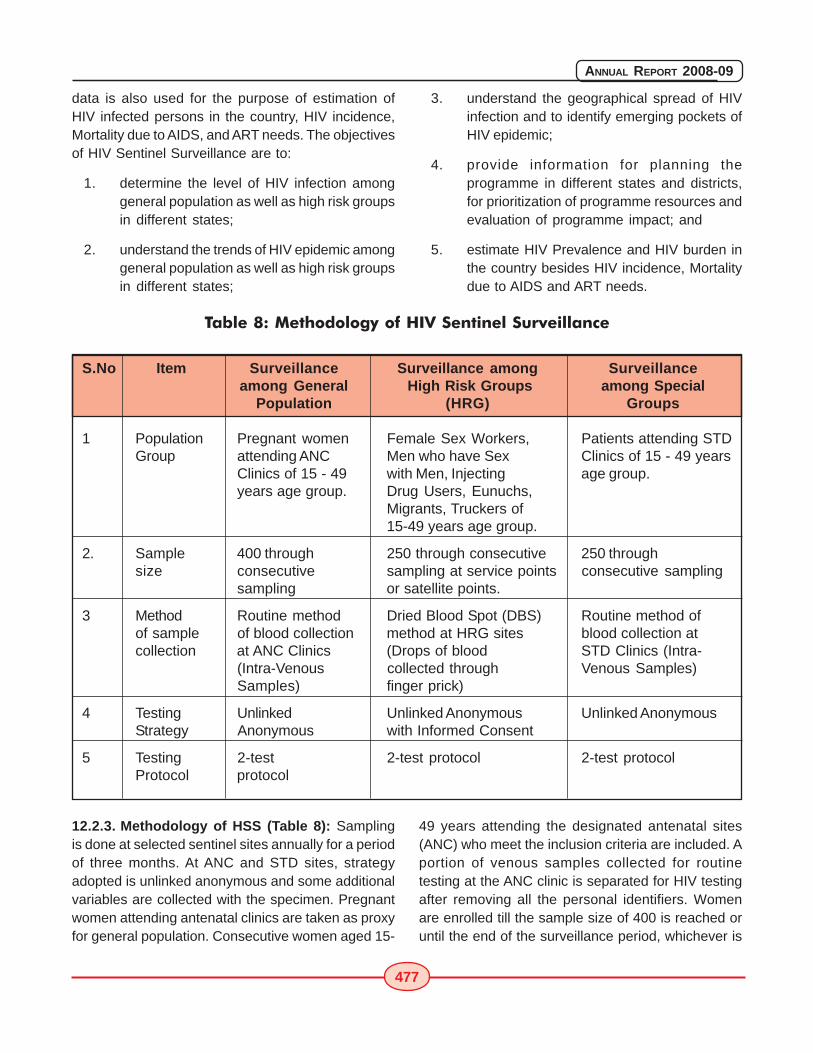
477
ANNUAL REPORT 2008-09
data is also used for the purpose of estimation ofHIV infected persons in the country, HIV incidence,Mortality due to AIDS, and ART needs. The objectivesof HIV Sentinel Surveillance are to:
1. determine the level of HIV infection amonggeneral population as well as high risk groupsin different states;
2. understand the trends of HIV epidemic amonggeneral population as well as high risk groupsin different states;
3. understand the geographical spread of HIVinfection and to identify emerging pockets ofHIV epidemic;
4. provide information for planning theprogramme in different states and districts,for prioritization of programme resources andevaluation of programme impact; and
5. estimate HIV Prevalence and HIV burden inthe country besides HIV incidence, Mortalitydue to AIDS and ART needs.
Table 8: Methodology of HIV Sentinel Surveillance
S.No Item Surveillance Surveillance among Surveillanceamong General High Risk Groups among Special
Population (HRG) Groups
1 Population Pregnant women Female Sex Workers, Patients attending STDGroup attending ANC Men who have Sex Clinics of 15 - 49 years
Clinics of 15 - 49 with Men, Injecting age group.years age group. Drug Users, Eunuchs,
Migrants, Truckers of15-49 years age group.
2. Sample 400 through 250 through consecutive 250 throughsize consecutive sampling at service points consecutive sampling
sampling or satellite points.
3 Method Routine method Dried Blood Spot (DBS) Routine method ofof sample of blood collection method at HRG sites blood collection atcollection at ANC Clinics (Drops of blood STD Clinics (Intra-
(Intra-Venous collected through Venous Samples)Samples) finger prick)
4 Testing Unlinked Unlinked Anonymous Unlinked AnonymousStrategy Anonymous with Informed Consent
5 Testing 2-test 2-test protocol 2-test protocolProtocol protocol
12.2.3. Methodology of HSS (Table 8): Samplingis done at selected sentinel sites annually for a periodof three months. At ANC and STD sites, strategyadopted is unlinked anonymous and some additionalvariables are collected with the specimen. Pregnantwomen attending antenatal clinics are taken as proxyfor general population. Consecutive women aged 15-
49 years attending the designated antenatal sites(ANC) who meet the inclusion criteria are included. Aportion of venous samples collected for routinetesting at the ANC clinic is separated for HIV testingafter removing all the personal identifiers. Womenare enrolled till the sample size of 400 is reached oruntil the end of the surveillance period, whichever is

478
ANNUAL REPORT 2008-09
earlier. In case of STD sites, the samples arecollected from two sources, STD clinic and Obstetricsand Gynaecology (OBG) clinic located in the samehospital. A total of 150 samples from individuals inthe STD clinic and 100 samples from individuals inthe OBG clinic are collected for a sample size of 250.Only consecutive new cases of STDs diagnosedsyndromically (i.e. cases of genital ulcer, urethral orcervical discharge and genital warts) are recruited.
Individuals from high risk groups (HRG) - IDU, FSW,MSM, Single Male Migrants and Truckers - aresampled at service points - for example, de-addictioncentre, drop-in centres, NGO clinics until the samplesize of 250 is reached or until the end of thesurveillance period, whichever is earlier. Strategyadopted is unlinked anonymous with informedconsent. At the HRG sites, the Dried Blood Spot(DBS) method of sample collection has beenintroduced during the current round. An operationalfeasibility study was carried out by AIIMS, New Delhito understand the feasibility issues in implementingthis method at HRG sites.
12.2.4. Testing of samples and Quality Control:Two test protocol is adopted for determining thepositivity. The samples from ANC and STD sites aretested at designated testing laboratories in therespective state. There is a well-defined system ofExternal Quality Assurance Scheme (EQAS) forlaboratory testing. Ten National ReferenceLaboratories are the nodal laboratories for EQASwhere all positive samples and 5% of negativesamples randomly selected from all the testing labsare retested for quality assurance. DBS samples fromHRG sites are tested at eleven laboratoriesdesignated and trained for DBS testing. NARI, Puneprovides EQAS for the testing of DBS samples.
12.2.5. Implementing Structure: The nationalexercise of sentinel surveillance is implementedthrough coordination, support and supervision byNational Institute of Health and Family Welfare, NewDelhi as the national nodal agency and sevenRegional Public Health Institutions in the country.These include Post-Graduate Institute of MedicalEducation and Research, Chandigarh; All IndiaInstitute of Medical Sciences, New Delhi; National
AIDS Research Institute, Pune; National Institute ofEpidemiology, Chennai; All India Institute of Hygieneand Public Health, Kolkata; National Institute ofCholera and Enteric Diseases, Kolkata; and RegionalInstitute of Medical Sciences, Imphal. Apart fromthese, every state has a State Surveillance Team,comprising of public health experts andmicrobiologists who take care of the training of thepersonnel involved in sentinel surveillance systemas well as supervision and monitoring. NACO hasalso appointed epidemiologists at the SACS tosupport data analysis at the state level. Besides,NIHFW, New Delhi conducts supervision through agroup of senior public health experts andmicrobiologists who act as Central Surveillance TeamMembers.
12.2.6. Training under HSS: All training programmesin HSS are conducted under the close supervisionof regional institutes and state surveillance teams.Operational Feasibility Study for implementation ofDried Blood Spot (DBS) method in HIV SentinelSurveillance (HSS) has indicated that training is thecrucial element for successful implementation of DBStechnique. Accordingly, a two-tier training plan wasdeveloped for HRG sites. The first level Training ofTrainers (TOT) was conducted at all RegionalInstitutes (RI) where the RI teams, State SurveillanceTeams and SACS officials were trained as trainers.Experts in DBS method from NFHS-III team wereinvolved as Master Trainers for TOTs. The secondlevel Training of high risk group (HRG) site personnelwas conducted at the respective RI/ SACS. LabTechnicians, nurse/ Counsellor/ doctors wereidentified at every HRG site for collection of DBSsamples. Both the above trainings were of three daysduration with one and half day for skill-buildingpractical/ field exercises. Structured trainingcurriculum, trainers' modules and trainees' moduleswere developed with the support of NARI, Pune andWHO. TOTs and Training for HRG site personnelwere held during December 2008 and January 2009.One day Refresher training for HRG site personnelwas held in all the states during March-April 2009.
12.2.7. Procurement and Supplies: TheOperational Guidelines were revised, printed and
479
ANNUAL REPORT 2008-09
distributed to all the sentinel sites, participatinginstitutions and SACS. Central Procurement (Import)and supply of consumables required for DBS methodhas been completed. Special Sample TransportationBoxes were developed with the support of India Postand Indian Institute of Packaging, Delhi. Speed Posthas been engaged for sample pick up from sentinelsites and transport of DBS samples to the testinglabs.
12.2.8. Supervision and Quality Review: Fourtiers of supportive supervision are in place duringthe period of HIV Sentinel Surveillance - CentralSurveillance Team Members, Regional InstituteTeams, State Surveillance Teams and SACS officers.On-site training is provided to the sites whereproblems are noticed during supervisory visits.Special teams are also constituted to revisit problemsites, review the quality of surveillance process andto validate the data emerging from these sites.
12.2.9. Data Entry: Data entry is done through theweb-based data entry system developed andmaintained by NIHFW, New Delhi. Data entry at SACSand RIs is undertaken followed by matching to ruleout any data entry errors and to ensure clean datafor analysis. Special training was conducted at NIHFW,New Delhi for data entry operators and surveillanceofficers at SACS and RIs in the web-based data entrypackage. The data entry formats were centrallyprinted and supplied to all SACS.
12.2.10. HIV Estimation: National Institute of MedicalStatistics, New Delhi is the nodal agency fordeveloping national estimates of HIV prevalence andburden in India. The first HIV estimation in India wasdone in 1994 based on data from 52 sites. Sincethen, the process of estimation of HIV infectedpersons in the country has evolved to a very greatextent. Since, the sample from which data is collectedthrough sentinel surveillance is not exactlyrepresentative of the general population, certainassumptions were used to generate estimates forthe general population. Over the years, theseassumptions were gradually refined with the help ofother available data sources. The year 2006 provideda unique opportunity when multiple data sourcessuch as a community based HIV prevalence study of
National Family Health Survey-III, Integrated Bio-behavioural Assessment Survey, Endline BehaviouralSurveillance Survey could be utilized along with thedata from the expanded sentinel surveillance systemto arrive at more robust HIV estimates that are morecloser to reality. The Workbook Model of WHO-UNAIDS is adopted that allows internationalcomparability. Special statistical packages such asRandom-effects Model and Spectrum ProjectionSoftware were utilized to make more accurate andreliable estimates during 2006 and 2007.
12.3 Evaluation and OperationalResearch
The main objective of the research agenda is toposition NACO as the leading national body,promoting and coordinating research on HIV/AIDSnationally and in the South Asia region throughpartnership and networking with stakeholders,supporting capacity building for research throughestablished national academic and other researchinstitutions, and as the central repository of allrelevant resources, research documents and database on HIV/AIDS in the country. New Initiatives takenby R&D Division, NACO include:
1. The "Network of Indian Institutions for HIV/AIDS Research (NIIHAR)" has beenconstituted. This consortium of researchinstitutions will undertake operational,epidemiological and bio-medical research inHIV/AIDS. It will have linkages withuniversities, ICMR, CSIR, DST, ICSSR andothers stakeholders including donororganizations, and will pool resources andexpertise to conduct high quality,collaborative, multi-centric research that willhelp evidence based decision making onpolicy, management and evaluation ofinterventions. The following Indian Institutionswere admitted as Members of NIIHAR:
1. National Institute for Health & FamilyWelfare (NIHFW), New Delhi
2. National AIDS Research Institute (NARI),Pune
480
ANNUAL REPORT 2008-09
3. International Institute for PopulationSciences, (IIPS), Mumbai
4. Institute for Economic Growth (IEG), NewDelhi
5. National Institute for Medical Statistics(NIMS), New Delhi
6. National Institute for CommunicableDiseases (NICD), New Delhi
7. All India Institute for Medical Sciences(AIIMS), New Delhi
8. PGIMER, Chandigarh
9. Tata Institute for Social Sciences (TISS),Mumbai
10. National Institute of Mental health andNeuro Science (NIMHANS), Bengalooru
11. Institute of Health and ManagementResearch (IIHMR), Jaipur
12. Tuberculosis Research Center (TRC),Chennai
13. JJ Hospital, Mumbai
14. National Institute for Research inReproductive Health (NIRRH), Mumbai
15. National Institute of Epidemiology (NIE),Chennai
16. National Institute of Cholera and EntericDiseases (NICED), Kolkata
2. The NACO Research Fellowships Scheme forMD/M.Phil/Ph.D students started in 2008-09,facilitates capacity building of youngresearchers in the country for undertakingHIV research including inter-disciplinary,multi-site, action, intervention and operationsresearch, and to increase skills incommunicating research findings forimpacting policy and programme. Thesefellowships serve as an incentive to take upquality and need-based research in HIV/AIDS.
3. The 'NACO Ethics Committee' has beenconstituted involving experts of bio-medical,clinical, epidemiological, behavioral andsocial disciplines, a legal expert and arepresentative of PLHA network. Its mainfunction is to consider and provide ethicalclearance for those research proposals andprojects that involve participation andexperimentation on human participants,where their mental, physical, social andemotional health and well-being may beaffected by the proposed research. Twomeetings of the committee were held inFebruary 2009.
4. A list of priority areas for Evaluation andOperational Research was finalised inconsultation with various stakeholders,donors, members of TRG and Heads ofvarious program Divisions. The proposalsreceived from members of NIIHAR andCenters of Excellence in response to NACO'sinvitation of proposals on OperationalResearch were reviewed by a panel ofexperts. The following three proposals wererecommended by TRG-R&D at its meeting inJanuary 2009 and then by the NACO EthicsCommittee:
� Determinants of drug adherence associatedwith ART in India
� Factors affecting enrolment of PLHAs on ARTin India
� Determining baseline CD4 Counts in Indianpopulation
A study on "Impact Evaluation of TargetedIntervention in India" commissioned jointly by theWorld Bank and NACO will be carried out by aconsortium of three research institutes led by PGIMERChandigarh. NACO has initiated plans for a multi-centric study on 'Psycho-social burden on PLHAsattending ICTCs and ART Centres in India' with theInstitute of Human Behaviour and Allied Sciences,Delhi as the Lead Research Institute.

481
ANNUAL REPORT 2008-09
12. Conclusion
In 2007, the country is estimated to have 1.8 - 2.9million HIV positive persons, with an estimated adultHIV prevalence of 0.34% (0.25% - 0.43%). Trendsof HIV infection indicate a mixed response in thecountry, with increase in some areas and decreasein other. As the HIV Prevalence among high riskgroups is around six to eight times that among generalpopulation, India continues to be in the category ofconcentrated epidemic. Sexual mode continues tobe the major mode of transmission, thoughtransmission through injecting drug use and MSM ison rise in many new pockets.
NACP-III seeks to learn from the lessons of theprevious two phases of programme implementationand build on the strengths thereof. The presentprogramme is based on sound public healthprinciples and NACP-III will place the highest priorityon preventive efforts while, at the same time, seekingto integrate prevention with care, support andtreatment. However, complexities of the epidemic andits exact dimensions are yet to be understoodespecially in the Northern and North Eastern statesof the country. Decentralisation and devolution ofdecision-making powers to the SACS was a right step,but it has to be complemented with capacitydevelopment and technical support. Focused
attention on the HRGs through TIs proved to be aneffective strategy for preventing the spread ofinfection. However, saturation of coverage of HRGsnationwide is yet to be accomplished.
Moving over from awareness to behaviour changeis the main focus of communication strategy. Sub-populations that have the highest risk of exposureto HIV will receive the highest priority for intervention.Those in the general population who have greaterneed for accessing prevention services such astreatment of STIs, voluntary counseling and testingand condoms will be next in the line of priority. NACP-III will ensure that all persons who need treatmentwould have access to prophylaxis and managementof opportunistic infections. Persons who need accessto ART will also be assured first line ARV drugs.Mainstreaming and partnerships will be the keyapproach to facilitate multi-sectoral responseengaging a wide range of stakeholders. Building upof a strong Strategic Information Management Systemand strengthening the Surveillance and Researchcomponents to provide evidence for planning andimplementation will be given major thrust duringNACP-III. National AIDS Control Programme iscurrently focusing on up-scaling of services toimprove coverage and to improve the quality ofservices provided.

ANNEXURE
PART - I
(Organisation Charts)
Ministry of Health &Family Welfare

484
ANNUAL REPORT 2008-09
485
ANNUAL REPORT 2008-09
Organisation Chartsof
Ministry of Health &Family Welfare
Organograms of Department of Health & Family Welfare,
Department of AYUSH , Department of Health Research
and Department of AIDS Control give detailed
Organisational Structure of Divisions, Branches, Sections,
Cells, Units.

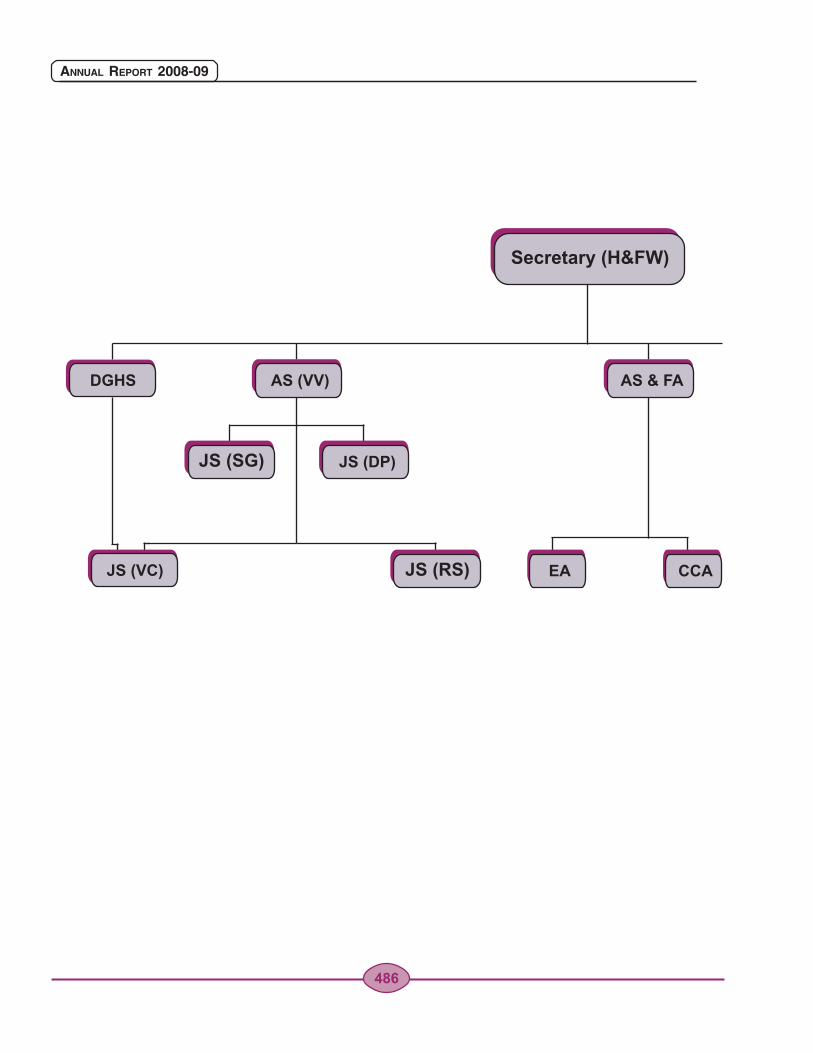
JS (SG)
JS (RS)
486
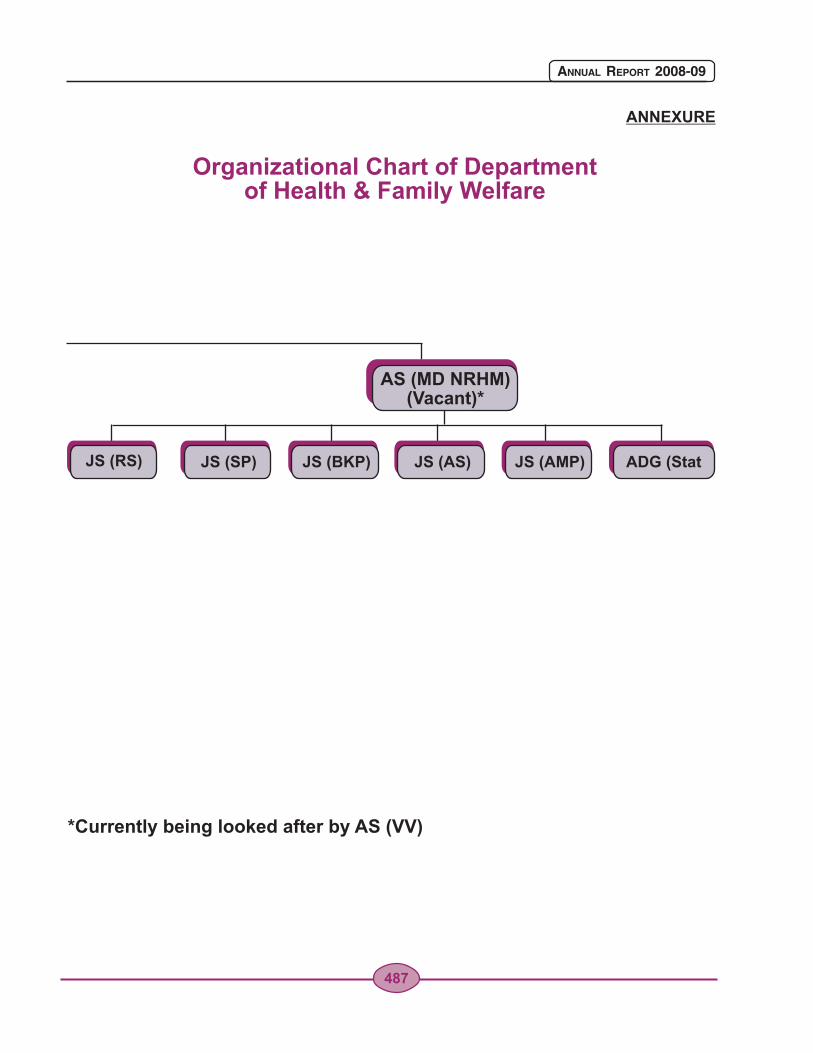
Organizational Chart of Department of Health & Family Welfare
ANNEXURE
AS (MD NRHM)(Vacant)*
487
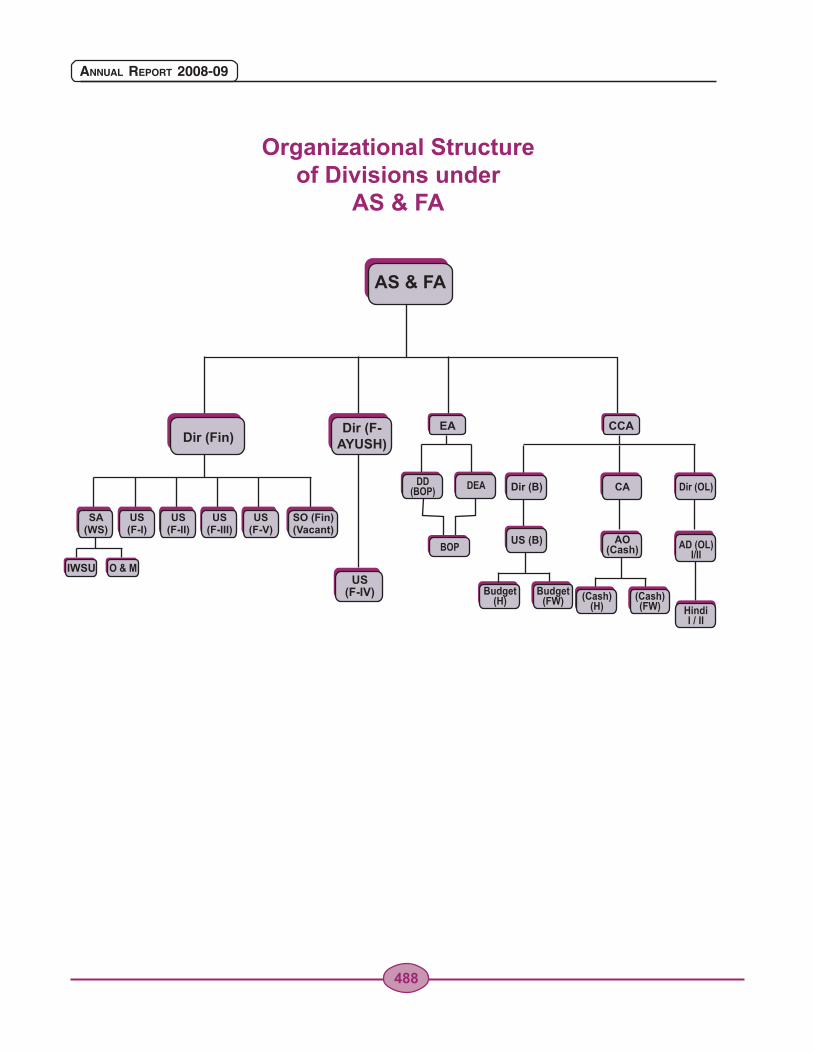
Organizational Structure of Divisions under
AS & FA
AS & FA
Dir (Fin)Dir (F-
AYUSH)
SA (WS)
IWSU O & M
US(F-I)
US(F-II)
US(F-III)
US(F-V)
SO (Fin)(Vacant)
US(F-IV)
EA CCA
DD (BOP) Dir (OL)DEA
BOP
Dir (B)
US (B)
Budget(H)
Budget(FW)
CA
AO(Cash)
(Cash)(FW) Hindi
I / II
AD (OL)I/II
(Cash)(H)
488
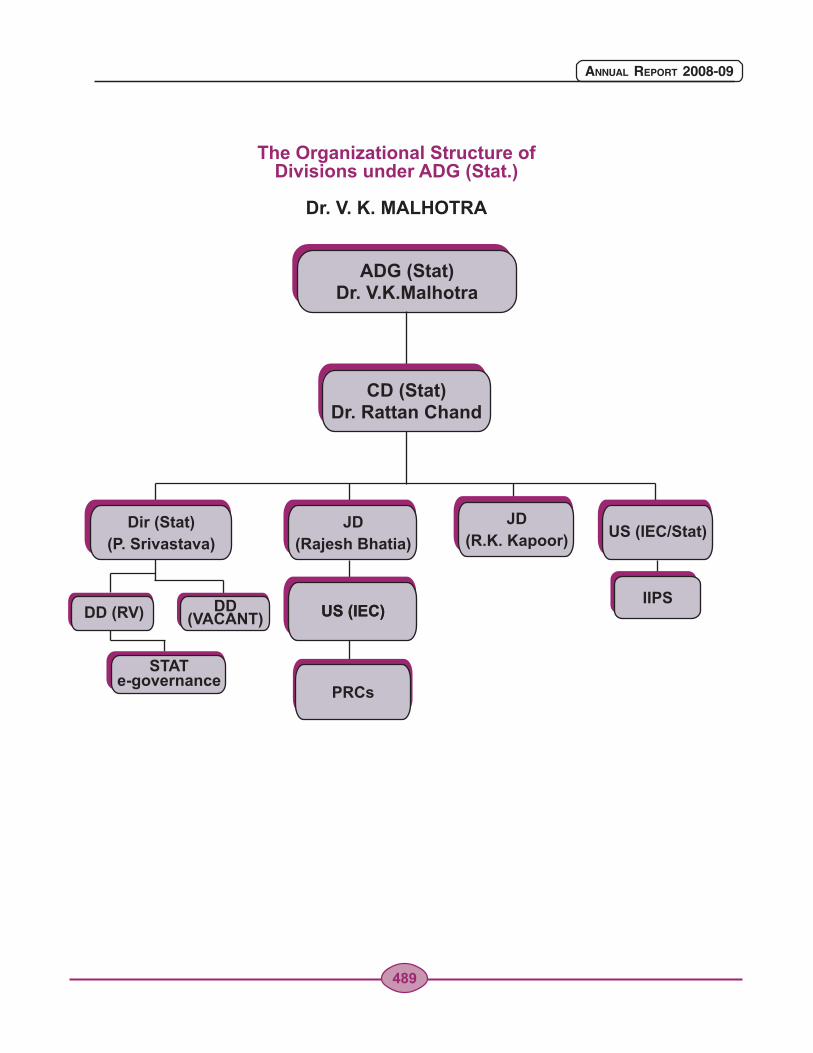
The Organizational Structure of Divisions under ADG (Stat.)
Dr. V. K. MALHOTRA
ADG (Stat)Dr. V.K.Malhotra
CD (Stat)Dr. Rattan Chand
Dir (Stat)
(P. Srivastava)US (IEC/Stat)
JD
(R.K. Kapoor)
PRCs
JD
(Rajesh Bhatia)
US (IEC)US (IEC)DD (RV)
STATe-governance
DD(VACANT)
IIPS
489
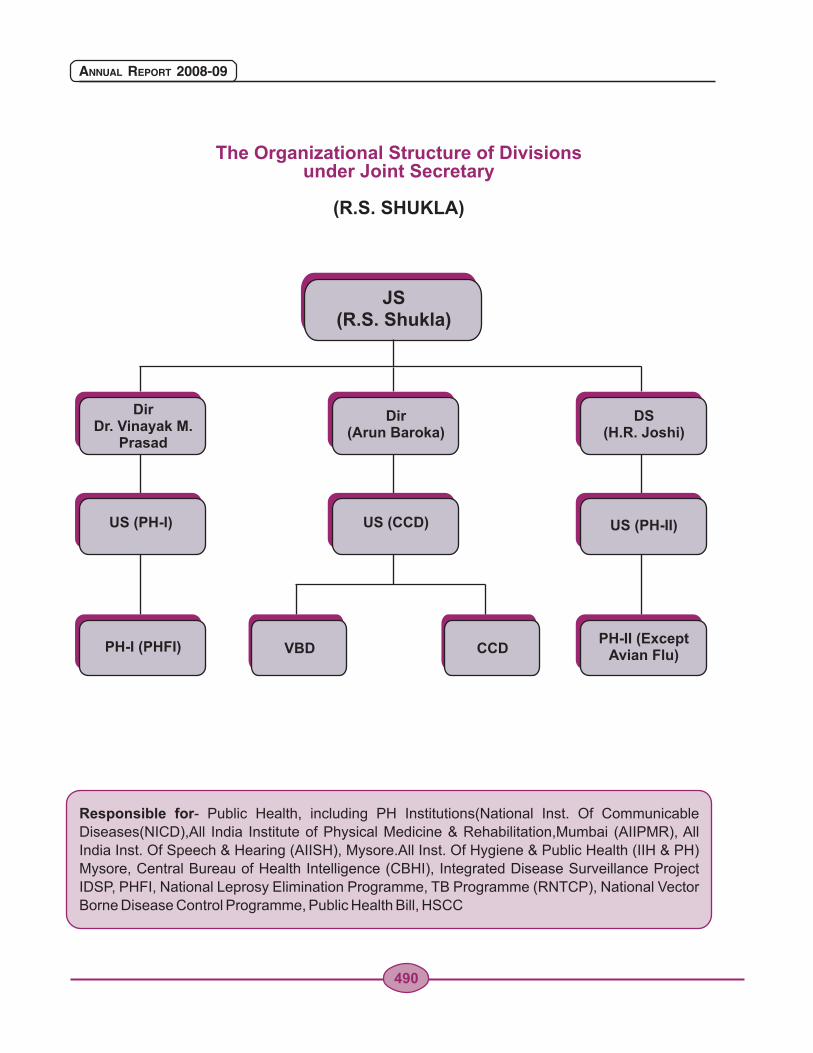
JS(R.S. Shukla)
The Organizational Structure of Divisions under Joint Secretary
(R.S. SHUKLA)
DirDr. Vinayak M.
Prasad
US (PH-I)
PH-I (PHFI)
Dir (Arun Baroka)
DS(H.R. Joshi)
US (CCD)
CCD
US (PH-II)
PH-II (ExceptAvian Flu)VBD
Responsible for- Public Health, including PH Institutions(National Inst. Of Communicable
Diseases(NICD),All India Institute of Physical Medicine & Rehabilitation,Mumbai (AIIPMR), All
India Inst. Of Speech & Hearing (AIISH), Mysore.All Inst. Of Hygiene & Public Health (IIH & PH)
Mysore, Central Bureau of Health Intelligence (CBHI), Integrated Disease Surveillance Project
IDSP, PHFI, National Leprosy Elimination Programme, TB Programme (RNTCP), National Vector
Borne Disease Control Programme, Public Health Bill, HSCC
490
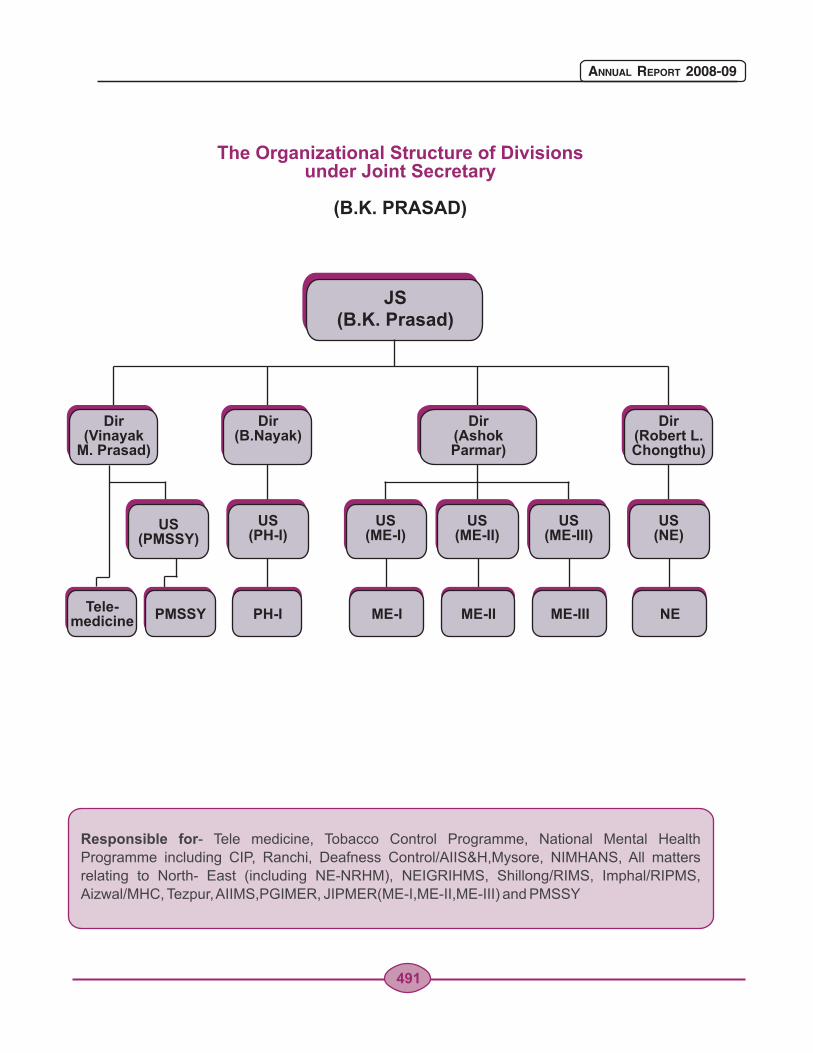
Responsible for- Tele medicine, Tobacco Control Programme, National Mental Health
Programme including CIP, Ranchi, Deafness Control/AIIS&H,Mysore, NIMHANS, All matters
relating to North- East (including NE-NRHM), NEIGRIHMS, Shillong/RIMS, Imphal/RIPMS,
Aizwal/MHC, Tezpur, AIIMS,PGIMER, JIPMER(ME-I,ME-II,ME-III) and PMSSY
JS(B.K. Prasad)
The Organizational Structure of Divisions under Joint Secretary
(B.K. PRASAD)
Dir(Robert L.Chongthu)
Dir(Ashok Parmar)
Dir(B.Nayak)
Dir(Vinayak
M. Prasad)
Tele-medicine
US (PMSSY)
US (PH-I)
US (ME-I)
US (ME-III)
US (ME-II)
US (NE)
PMSSY PH-I ME-I ME-II ME-III NE
491
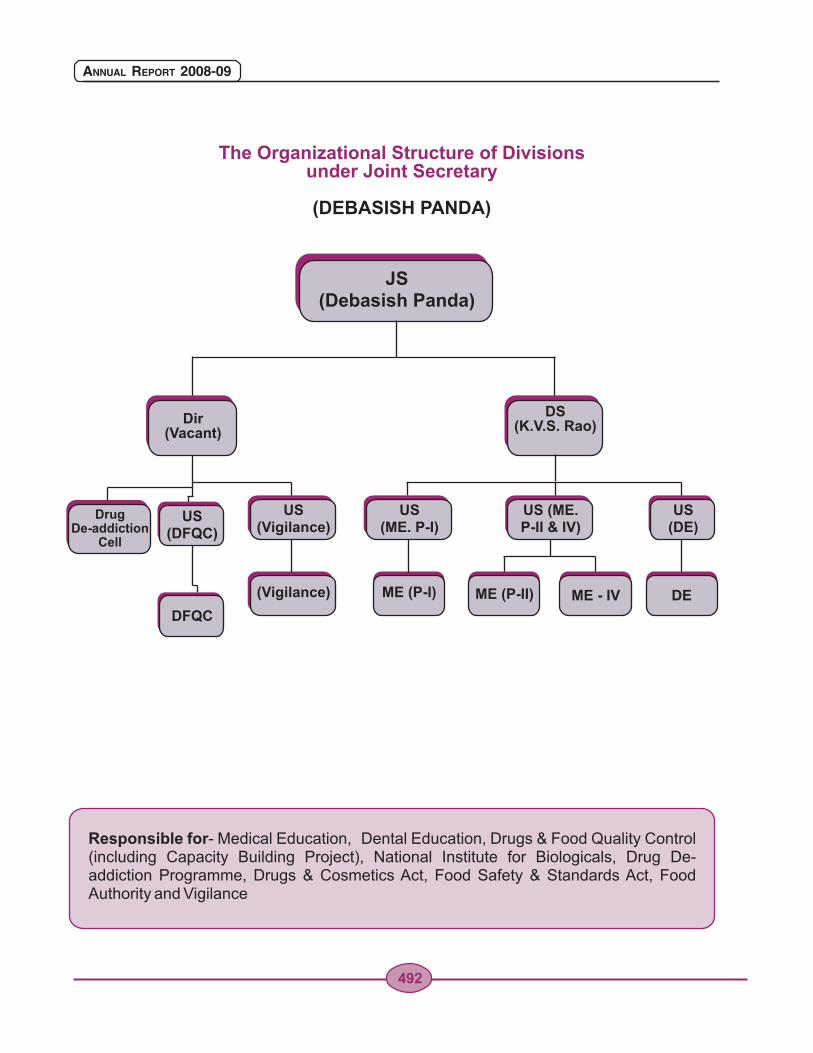
Responsible for- Medical Education, Dental Education, Drugs & Food Quality Control (including Capacity Building Project), National Institute for Biologicals, Drug De-addiction Programme, Drugs & Cosmetics Act, Food Safety & Standards Act, Food Authority and Vigilance
JS(Debasish Panda)
The Organizational Structure of Divisions under Joint Secretary
(DEBASISH PANDA)
DS(K.V.S. Rao)
Drug De-addiction
Cell
US (DFQC)
DFQC
US (DE)
US (Vigilance)
(Vigilance) ME (P-I)
Dir(Vacant)
US (ME. P-I)
US (ME. P-II & IV)
ME (P-II) ME - IV DE
492
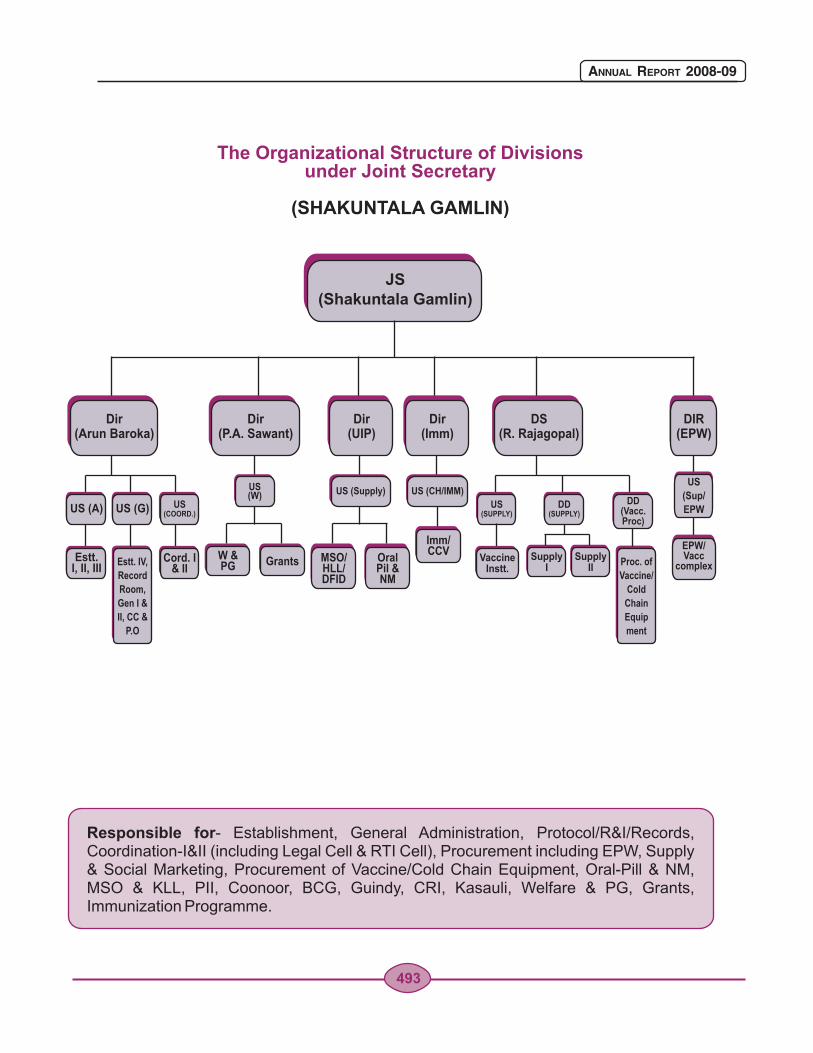
Responsible for- Establishment, General Administration, Protocol/R&I/Records, Coordination-I&II (including Legal Cell & RTI Cell), Procurement including EPW, Supply & Social Marketing, Procurement of Vaccine/Cold Chain Equipment, Oral-Pill & NM, MSO & KLL, PII, Coonoor, BCG, Guindy, CRI, Kasauli, Welfare & PG, Grants, Immunization Programme.
JS(Shakuntala Gamlin)
The Organizational Structure of Divisions under Joint Secretary
(SHAKUNTALA GAMLIN)
Dir(P.A. Sawant)
Dir(UIP)
Dir(Imm)
US (W) US (Supply) US (CH/IMM)
Dir(Arun Baroka)
US (A)
Estt.I, II, III
US (G) US (COORD.)
Cord. I& II
Estt. IV,
Record
Room,
Gen I &
II, CC &
P.O
Proc. of
Vaccine/
Cold
Chain
Equip
ment
DS(R. Rajagopal)
DIR(EPW)
VaccineInstt.
SupplyI
SupplyII
US (SUPPLY)
DD(SUPPLY)
DD(Vacc. Proc)
US
(Sup/
EPW
EPW/Vacc
complexW &PG
MSO/HLL/DFID
Grants OralPil & NM
Imm/CCV
493
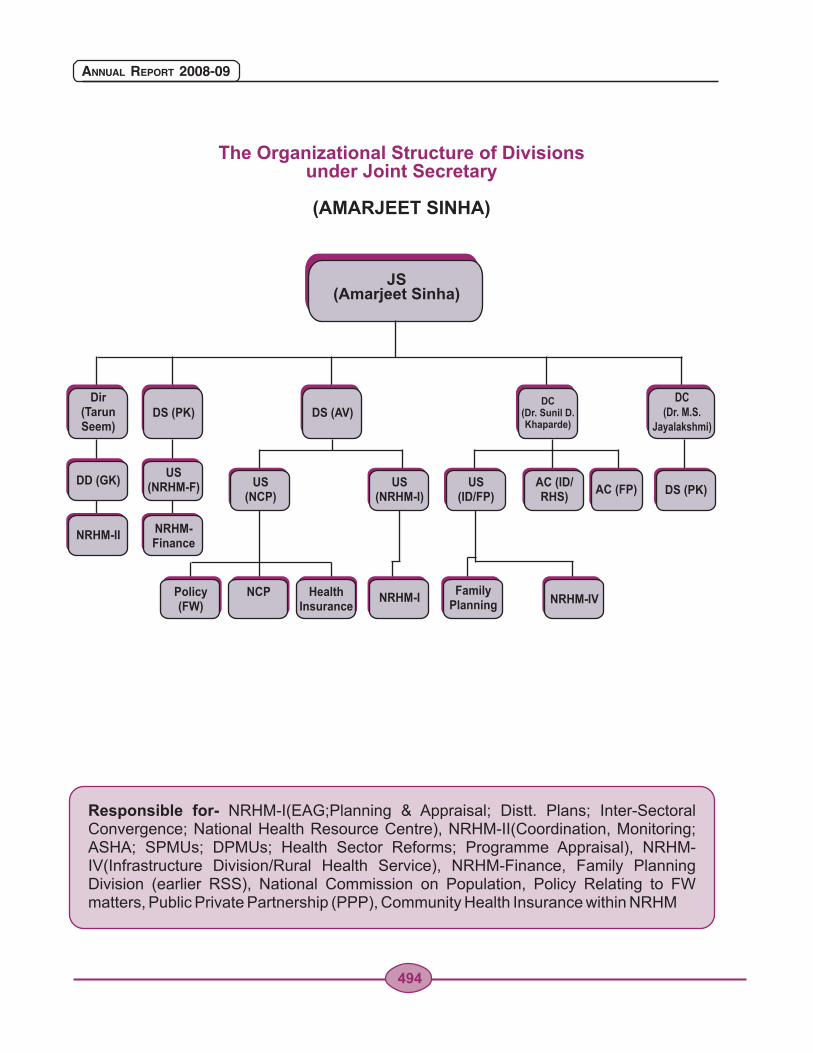
Responsible for- NRHM-I(EAG;Planning & Appraisal; Distt. Plans; Inter-Sectoral Convergence; National Health Resource Centre), NRHM-II(Coordination, Monitoring; ASHA; SPMUs; DPMUs; Health Sector Reforms; Programme Appraisal), NRHM-IV(Infrastructure Division/Rural Health Service), NRHM-Finance, Family Planning Division (earlier RSS), National Commission on Population, Policy Relating to FW matters, Public Private Partnership (PPP), Community Health Insurance within NRHM
JS(Amarjeet Sinha)
The Organizational Structure of Divisions under Joint Secretary
(AMARJEET SINHA)
Dir(TarunSeem)
DC (Dr. M.S.
Jayalakshmi)DS (PK) DS (AV)
DC (Dr. Sunil D.Khaparde)
DD (GK)DS (PK)
US(NRHM-F) US
(NCP)AC (ID/RHS)
US (ID/FP)
US(NRHM-I)
AC (FP)
NRHM-I
NRHM-IINRHM-Finance
Policy(FW)
NCP HealthInsurance
NRHM-IVFamily
Planning
494
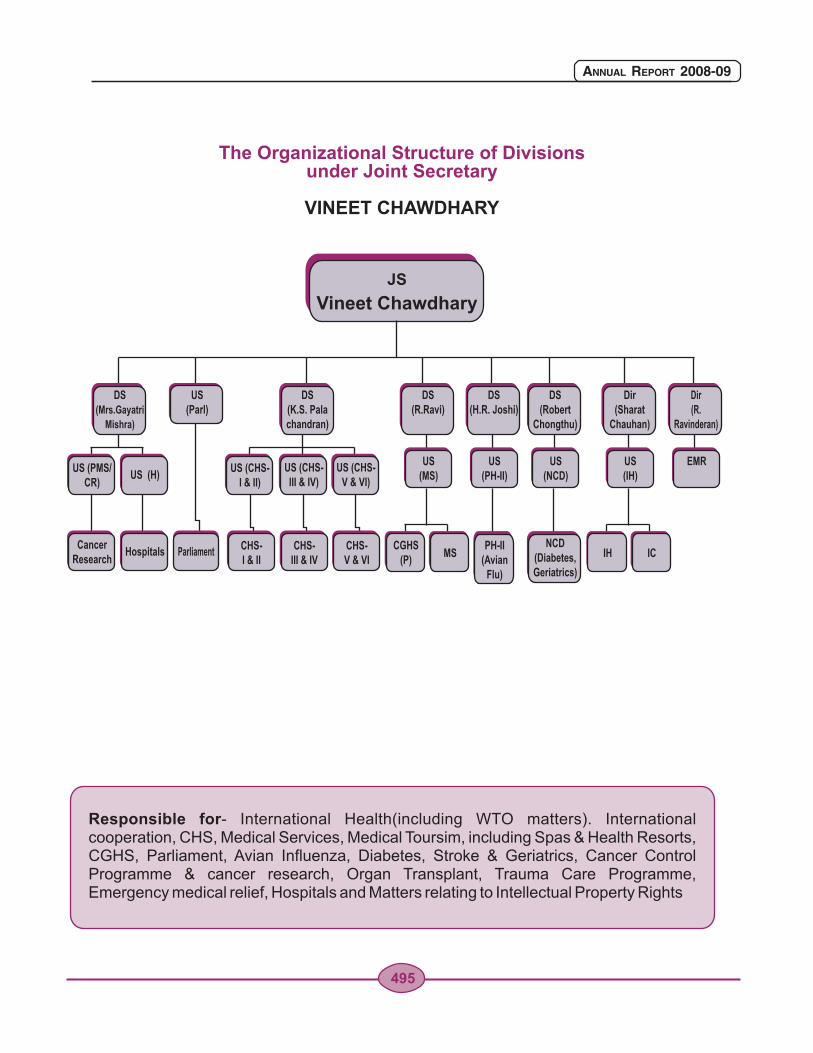
Responsible for- International Health(including WTO matters). International cooperation, CHS, Medical Services, Medical Toursim, including Spas & Health Resorts, CGHS, Parliament, Avian Influenza, Diabetes, Stroke & Geriatrics, Cancer Control Programme & cancer research, Organ Transplant, Trauma Care Programme, Emergency medical relief, Hospitals and Matters relating to Intellectual Property Rights
The Organizational Structure of Divisions under Joint Secretary
VINEET CHAWDHARY
JS
Vineet Chawdhary
DS(Mrs.Gayatri
Mishra)
DS(K.S. Palachandran)
US(Parl)
CancerResearch
CHS-I & II
CHS-III & IV
CHS-V & VI
Hospitals Parliament
US (CHS-I & II)
US (PMS/CR)
US (H)
CGHS(P)
IHMS IC
US (CHS-III & IV)
US (CHS-V & VI)
DS(R.Ravi)
US (MS)
Dir(Sharat
Chauhan)
US (IH)
DS(H.R. Joshi)
Dir (R.
Ravinderan)
DS(Robert
Chongthu)
NCD(Diabetes,Geriatrics)
US (PH-II)
EMRUS (NCD)
PH-II(Avian
Flu)
495
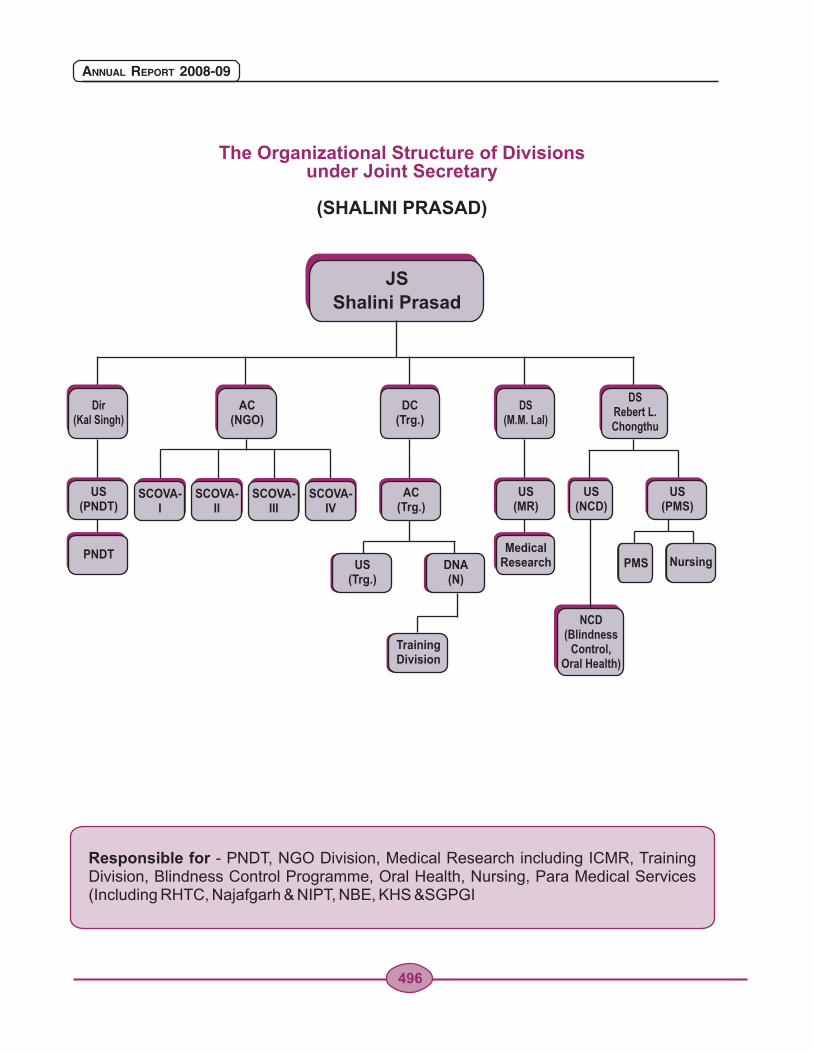
Responsible for - PNDT, NGO Division, Medical Research including ICMR, Training Division, Blindness Control Programme, Oral Health, Nursing, Para Medical Services (Including RHTC, Najafgarh & NIPT, NBE, KHS &SGPGI
JS
Shalini Prasad
The Organizational Structure of Divisions under Joint Secretary
(SHALINI PRASAD)
Dir(Kal Singh)
DS(M.M. Lal)
DSRebert L.Chongthu
AC(NGO)
DC(Trg.)
US (PNDT)
US(MR)
US(PMS)
US(NCD)
AC(Trg.)
US(Trg.)
DNA(N)
PMS NursingPNDT
MedicalResearch
SCOVA-I
SCOVA-II
SCOVA-III
SCOVA-IV
TrainingDivision
NCD (Blindness
Control,Oral Health)
496
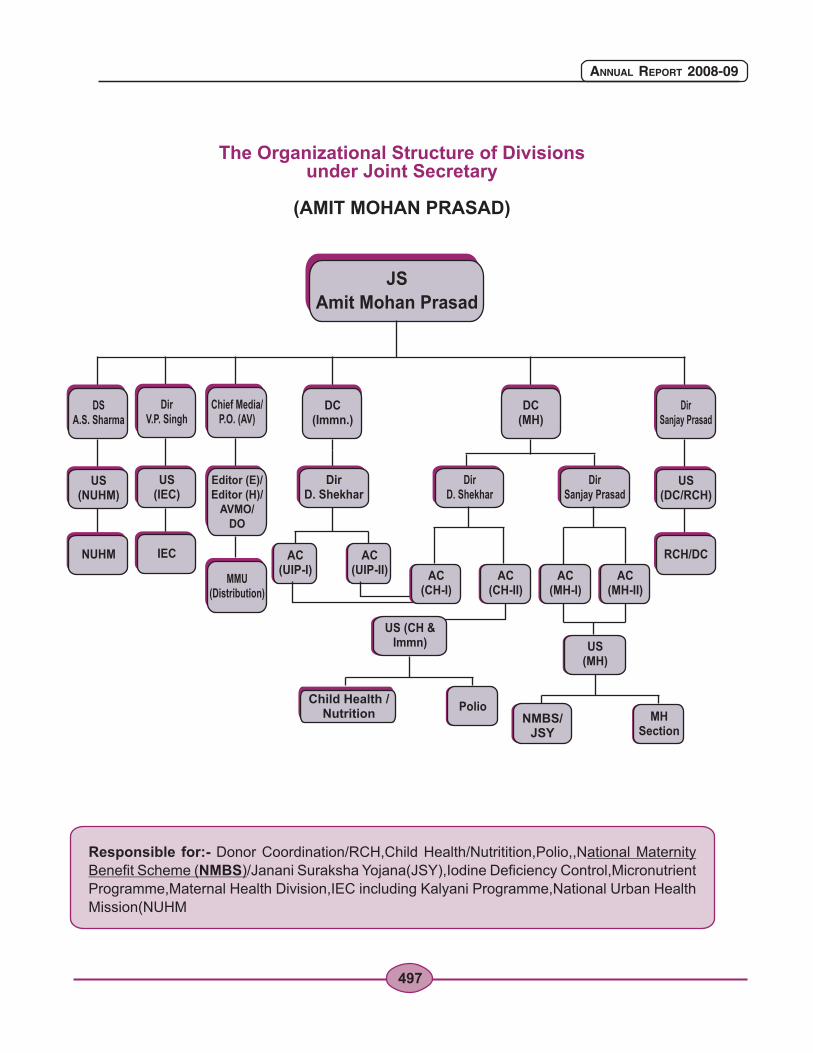
Responsible for:- Donor Coordination/RCH,Child Health/Nutritition,Polio,,National Maternity
Benefit Scheme (NMBS)/Janani Suraksha Yojana(JSY),Iodine Deficiency Control,Micronutrient
Programme,Maternal Health Division,IEC including Kalyani Programme,National Urban Health
Mission(NUHM
JS
Amit Mohan Prasad
The Organizational Structure of Divisions under Joint Secretary
(AMIT MOHAN PRASAD)
DirV.P. Singh
Chief Media/P.O. (AV)
MMU(Distribution)
US (IEC)
Editor (E)/Editor (H)/
AVMO/DO
DC(Immn.)
DC(MH)
DirD. Shekhar
DirD. Shekhar
DirSanjay Prasad
AC (UIP-I)
AC (UIP-II)
DSA.S. Sharma
US (NUHM)
NUHM
DirSanjay Prasad
US (DC/RCH)
RCH/DCIEC
US (CH &Immn) US
(MH)
AC (CH-I)
AC (CH-II)
AC (MH-I)
AC (MH-II)
PolioChild Health /
Nutrition MHSection
NMBS/JSY
497
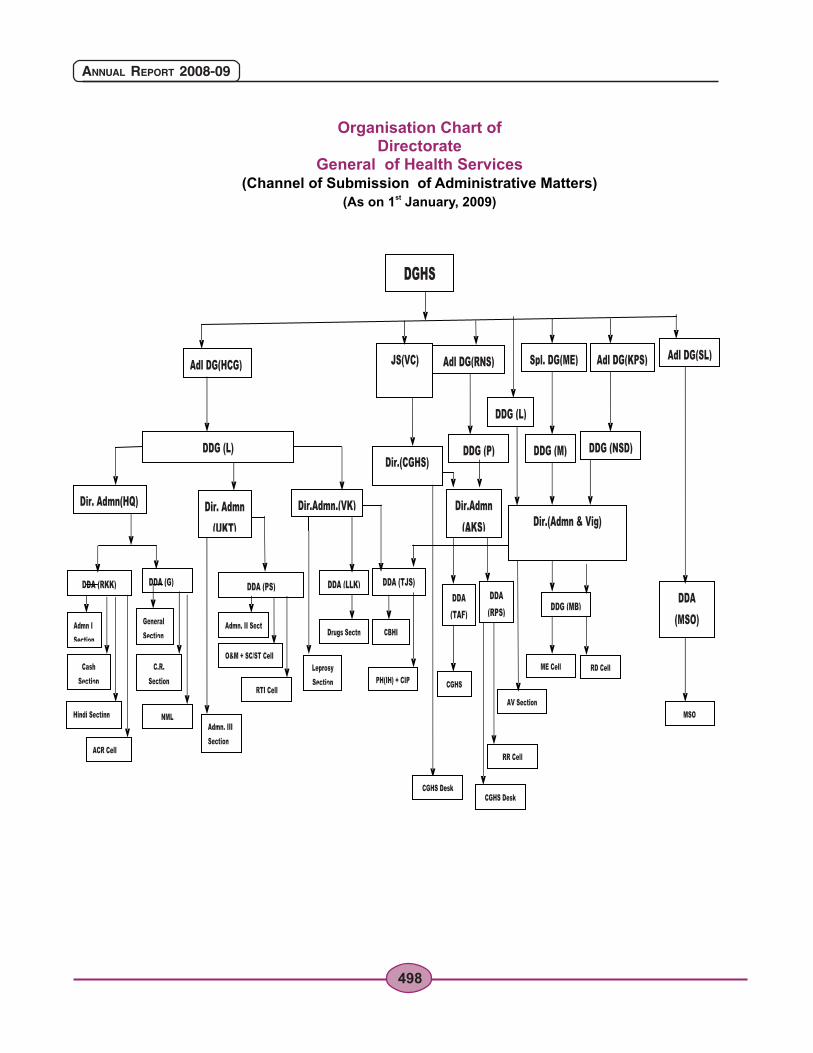
Organisation Chart of Directorate
General of Health Services(Channel of Submission of Administrative Matters)
st(As on 1 January, 2009)
498
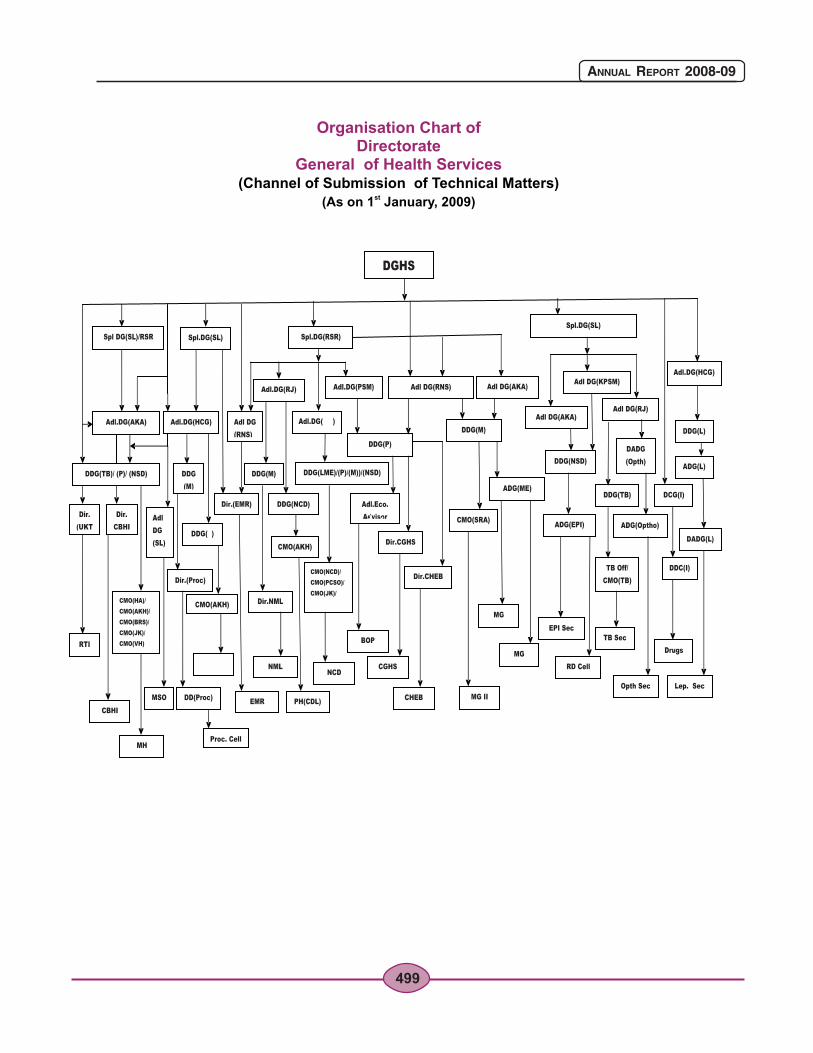
Organisation Chart of Directorate
General of Health Services(Channel of Submission of Technical Matters)
st(As on 1 January, 2009)
499
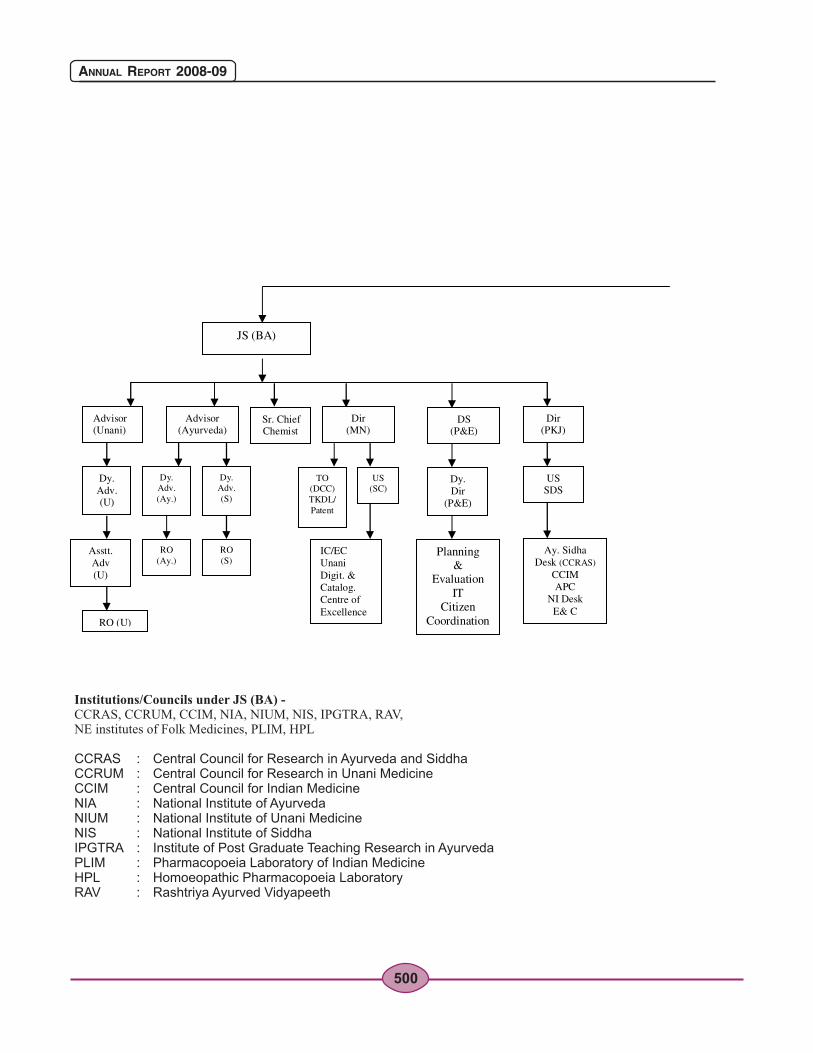
500
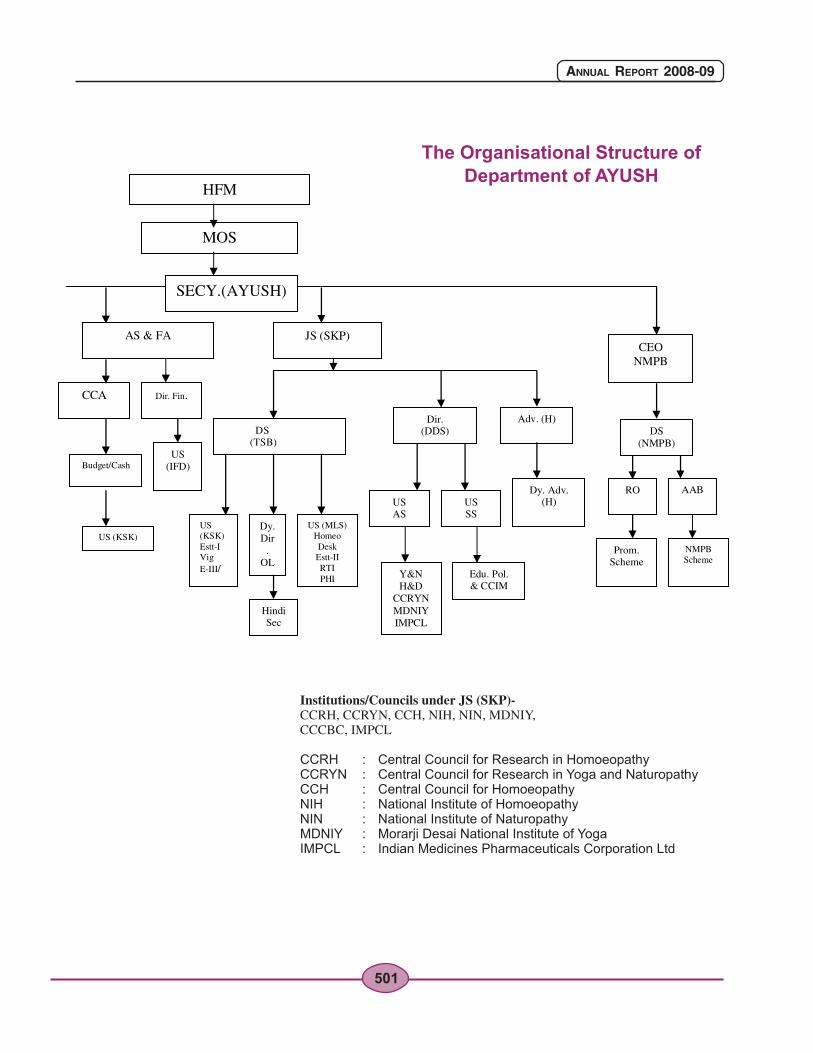
The Organisational Structure of Department of AYUSH
501
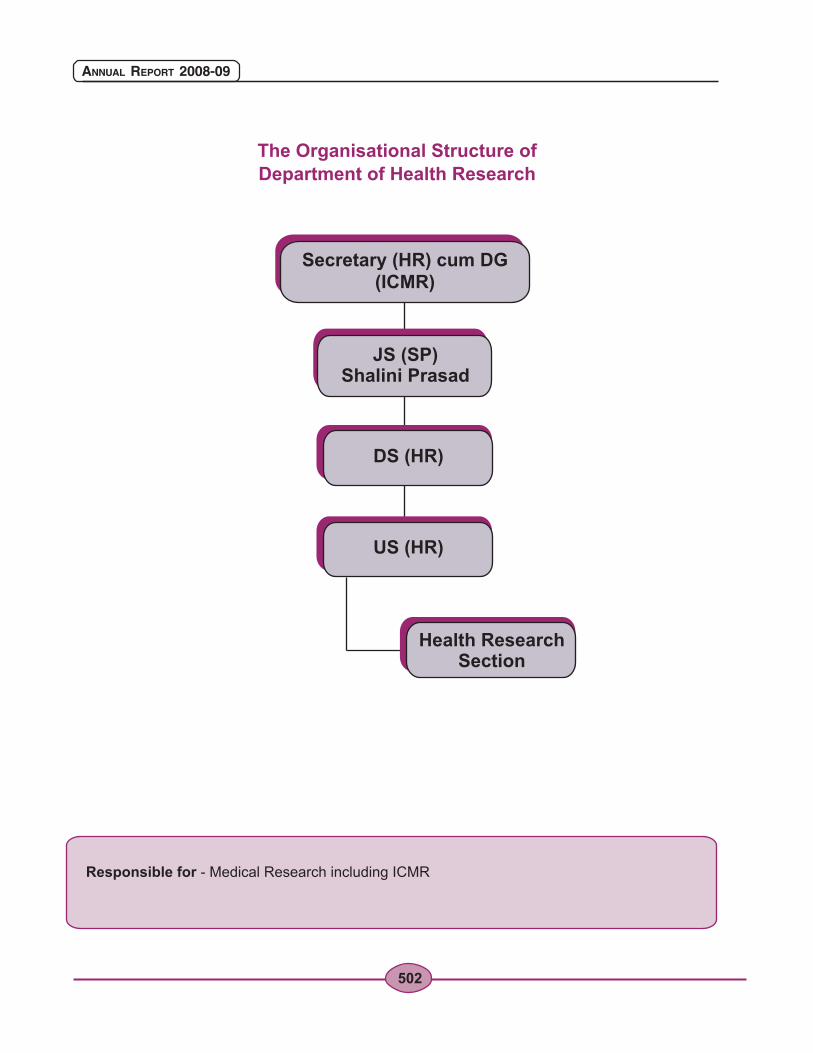
The Organisational Structure of Department of Health Research
Responsible for - Medical Research including ICMR
502
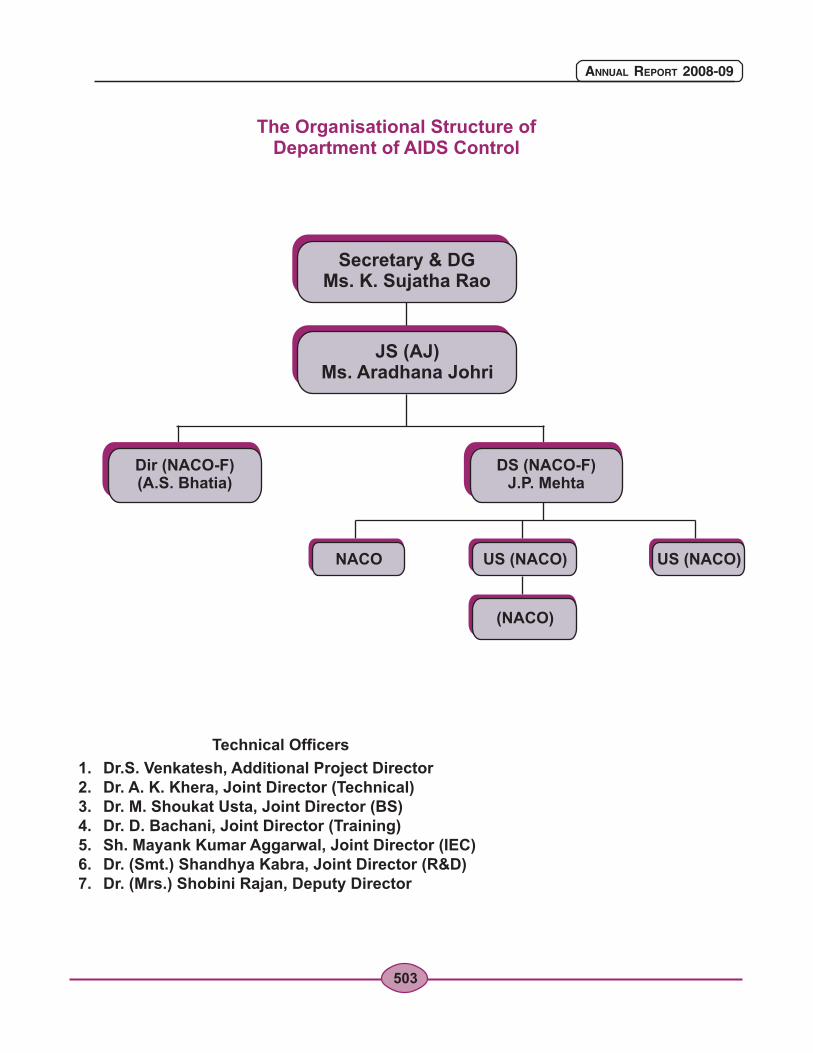
The Organisational Structure of Department of AIDS Control
503

ANNEXURE
PART - II
Department of AYUSH

506
ANNUAL REPORT 2008-09
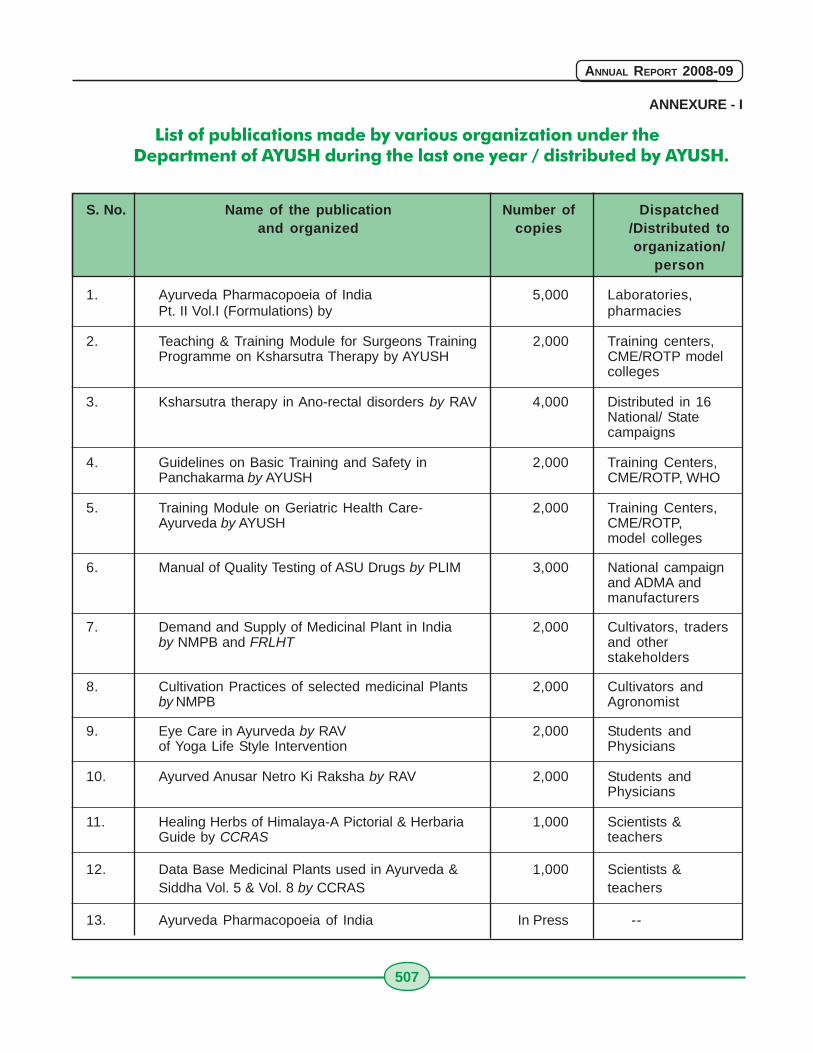
507
ANNUAL REPORT 2008-09
ANNEXURE - I
List of publications made by various organization under theDepartment of AYUSH during the last one year / distributed by AYUSH.
S. No. Name of the publication Number of Dispatchedand organized copies /Distributed to
organization/person
1. Ayurveda Pharmacopoeia of India 5,000 Laboratories,Pt. II Vol.I (Formulations) by pharmacies
2. Teaching & Training Module for Surgeons Training 2,000 Training centers,Programme on Ksharsutra Therapy by AYUSH CME/ROTP model
colleges
3. Ksharsutra therapy in Ano-rectal disorders by RAV 4,000 Distributed in 16National/ Statecampaigns
4. Guidelines on Basic Training and Safety in 2,000 Training Centers,Panchakarma by AYUSH CME/ROTP, WHO
5. Training Module on Geriatric Health Care- 2,000 Training Centers,Ayurveda by AYUSH CME/ROTP,
model colleges
6. Manual of Quality Testing of ASU Drugs by PLIM 3,000 National campaignand ADMA andmanufacturers
7. Demand and Supply of Medicinal Plant in India 2,000 Cultivators, tradersby NMPB and FRLHT and other
stakeholders
8. Cultivation Practices of selected medicinal Plants 2,000 Cultivators andby NMPB Agronomist
9. Eye Care in Ayurveda by RAV 2,000 Students andof Yoga Life Style Intervention Physicians
10. Ayurved Anusar Netro Ki Raksha by RAV 2,000 Students andPhysicians
11. Healing Herbs of Himalaya-A Pictorial & Herbaria 1,000 Scientists &Guide by CCRAS teachers
12. Data Base Medicinal Plants used in Ayurveda & 1,000 Scientists &Siddha Vol. 5 & Vol. 8 by CCRAS teachers
13. Ayurveda Pharmacopoeia of India In Press --
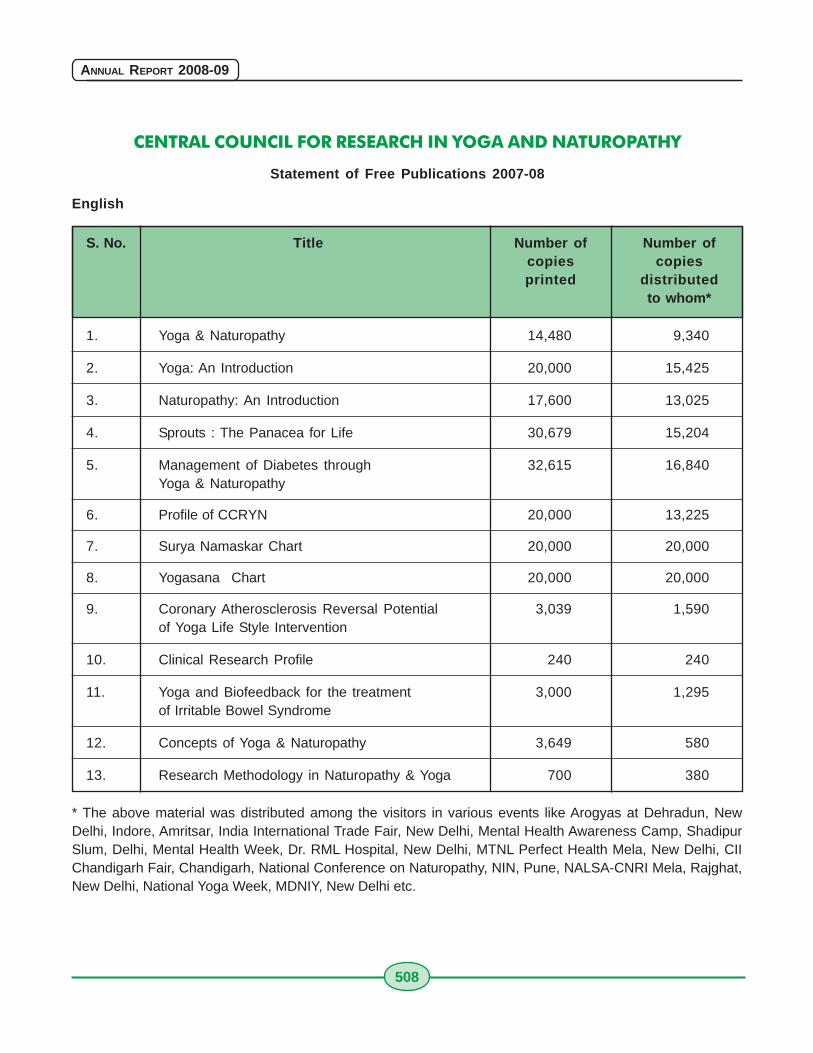
508
ANNUAL REPORT 2008-09
CENTRAL COUNCIL FOR RESEARCH IN YOGA AND NATUROPATHY
Statement of Free Publications 2007-08
English
S. No. Title Number of Number ofcopies copiesprinted distributed
to whom*
1. Yoga & Naturopathy 14,480 9,340
2. Yoga: An Introduction 20,000 15,425
3. Naturopathy: An Introduction 17,600 13,025
4. Sprouts : The Panacea for Life 30,679 15,204
5. Management of Diabetes through 32,615 16,840Yoga & Naturopathy
6. Profile of CCRYN 20,000 13,225
7. Surya Namaskar Chart 20,000 20,000
8. Yogasana Chart 20,000 20,000
9. Coronary Atherosclerosis Reversal Potential 3,039 1,590of Yoga Life Style Intervention
10. Clinical Research Profile 240 240
11. Yoga and Biofeedback for the treatment 3,000 1,295of Irritable Bowel Syndrome
12. Concepts of Yoga & Naturopathy 3,649 580
13. Research Methodology in Naturopathy & Yoga 700 380
* The above material was distributed among the visitors in various events like Arogyas at Dehradun, NewDelhi, Indore, Amritsar, India International Trade Fair, New Delhi, Mental Health Awareness Camp, ShadipurSlum, Delhi, Mental Health Week, Dr. RML Hospital, New Delhi, MTNL Perfect Health Mela, New Delhi, CIIChandigarh Fair, Chandigarh, National Conference on Naturopathy, NIN, Pune, NALSA-CNRI Mela, Rajghat,New Delhi, National Yoga Week, MDNIY, New Delhi etc.
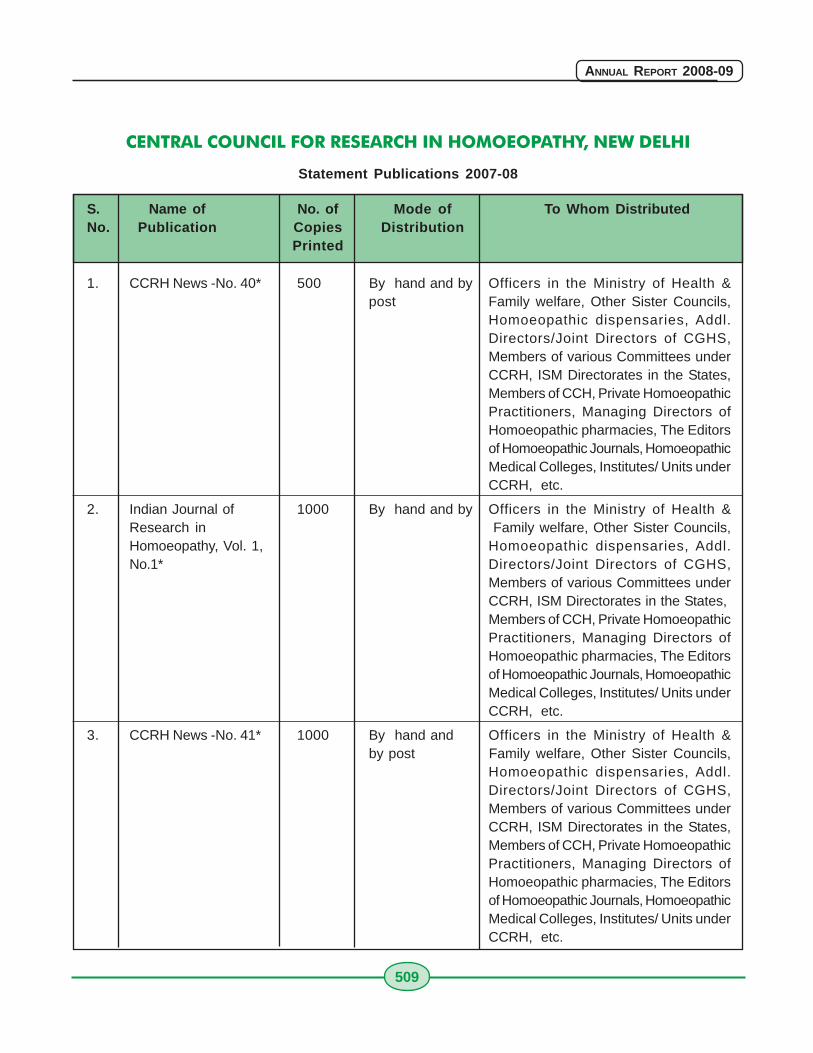
509
ANNUAL REPORT 2008-09
CENTRAL COUNCIL FOR RESEARCH IN HOMOEOPATHY, NEW DELHI
Statement Publications 2007-08
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
1. CCRH News -No. 40* 500 By hand and by Officers in the Ministry of Health &post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
2. Indian Journal of 1000 By hand and by Officers in the Ministry of Health &Research in Family welfare, Other Sister Councils,Homoeopathy, Vol. 1, Homoeopathic dispensaries, Addl.No.1* Directors/Joint Directors of CGHS,
Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
3. CCRH News -No. 41* 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
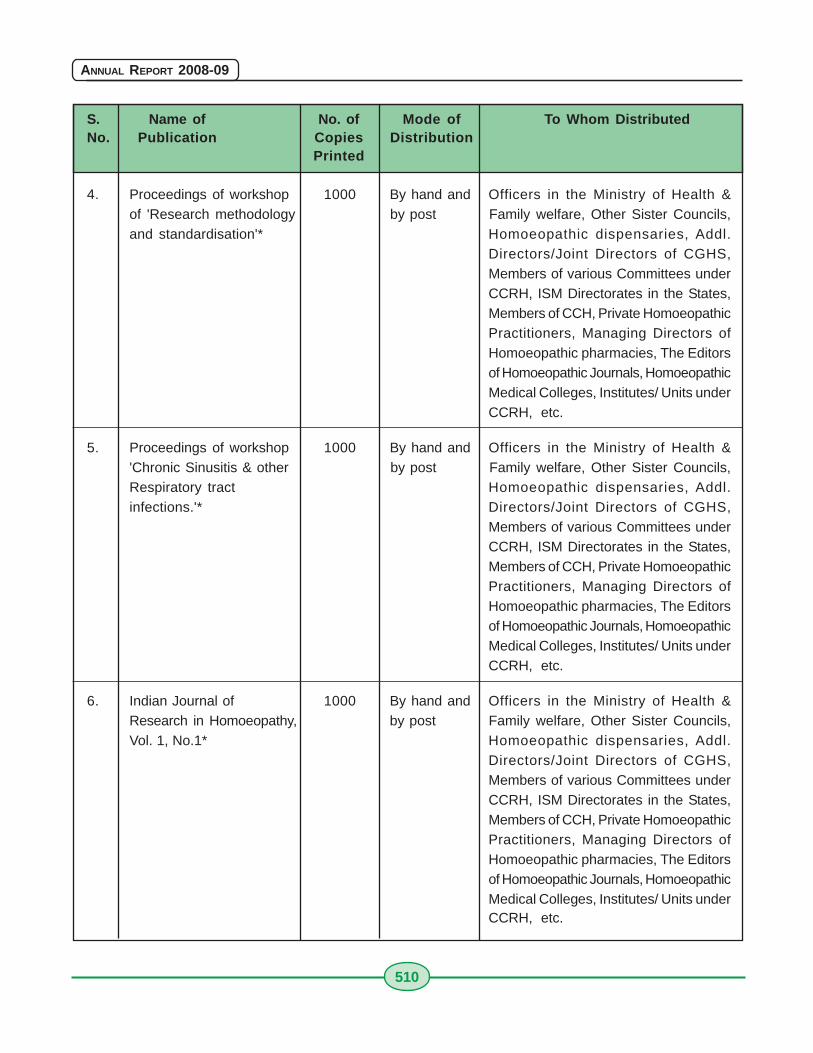
510
ANNUAL REPORT 2008-09
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
4. Proceedings of workshop 1000 By hand and Officers in the Ministry of Health &of 'Research methodology by post Family welfare, Other Sister Councils,and standardisation'* Homoeopathic dispensaries, Addl.
Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
5. Proceedings of workshop 1000 By hand and Officers in the Ministry of Health &'Chronic Sinusitis & other by post Family welfare, Other Sister Councils,Respiratory tract Homoeopathic dispensaries, Addl.infections.'* Directors/Joint Directors of CGHS,
Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
6. Indian Journal of 1000 By hand and Officers in the Ministry of Health &Research in Homoeopathy, by post Family welfare, Other Sister Councils,Vol. 1, No.1* Homoeopathic dispensaries, Addl.
Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
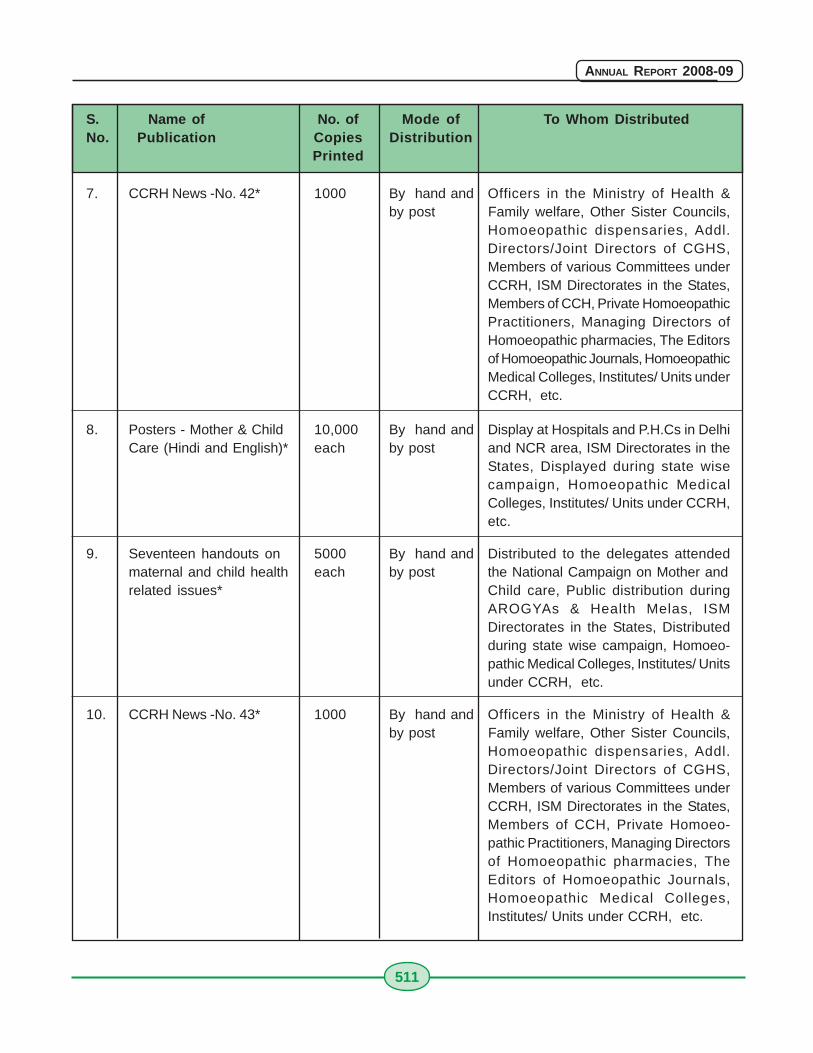
511
ANNUAL REPORT 2008-09
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
7. CCRH News -No. 42* 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
8. Posters - Mother & Child 10,000 By hand and Display at Hospitals and P.H.Cs in DelhiCare (Hindi and English)* each by post and NCR area, ISM Directorates in the
States, Displayed during state wisecampaign, Homoeopathic MedicalColleges, Institutes/ Units under CCRH,etc.
9. Seventeen handouts on 5000 By hand and Distributed to the delegates attendedmaternal and child health each by post the National Campaign on Mother andrelated issues* Child care, Public distribution during
AROGYAs & Health Melas, ISMDirectorates in the States, Distributedduring state wise campaign, Homoeo-pathic Medical Colleges, Institutes/ Unitsunder CCRH, etc.
10. CCRH News -No. 43* 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private Homoeo-pathic Practitioners, Managing Directorsof Homoeopathic pharmacies, TheEditors of Homoeopathic Journals,Homoeopathic Medical Colleges,Institutes/ Units under CCRH, etc.
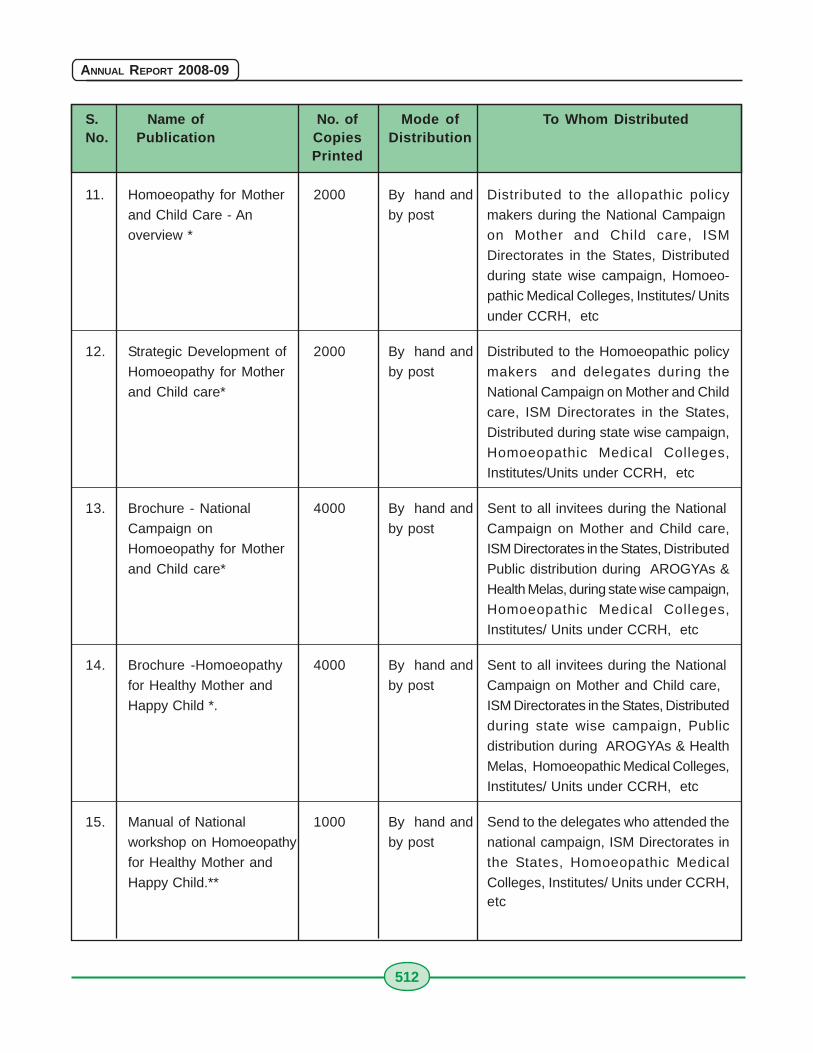
512
ANNUAL REPORT 2008-09
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
11. Homoeopathy for Mother 2000 By hand and Distributed to the allopathic policy
and Child Care - An by post makers during the National Campaign
overview * on Mother and Child care, ISM
Directorates in the States, Distributed
during state wise campaign, Homoeo-
pathic Medical Colleges, Institutes/ Units
under CCRH, etc
12. Strategic Development of 2000 By hand and Distributed to the Homoeopathic policy
Homoeopathy for Mother by post makers and delegates during the
and Child care* National Campaign on Mother and Child
care, ISM Directorates in the States,
Distributed during state wise campaign,
Homoeopathic Medical Colleges,
Institutes/Units under CCRH, etc
13. Brochure - National 4000 By hand and Sent to all invitees during the National
Campaign on by post Campaign on Mother and Child care,
Homoeopathy for Mother ISM Directorates in the States, Distributed
and Child care* Public distribution during AROGYAs &
Health Melas, during state wise campaign,
Homoeopathic Medical Colleges,
Institutes/ Units under CCRH, etc
14. Brochure -Homoeopathy 4000 By hand and Sent to all invitees during the National
for Healthy Mother and by post Campaign on Mother and Child care,
Happy Child *. ISM Directorates in the States, Distributed
during state wise campaign, Public
distribution during AROGYAs & Health
Melas, Homoeopathic Medical Colleges,
Institutes/ Units under CCRH, etc
15. Manual of National 1000 By hand and Send to the delegates who attended the
workshop on Homoeopathy by post national campaign, ISM Directorates in
for Healthy Mother and the States, Homoeopathic Medical
Happy Child.** Colleges, Institutes/ Units under CCRH,etc
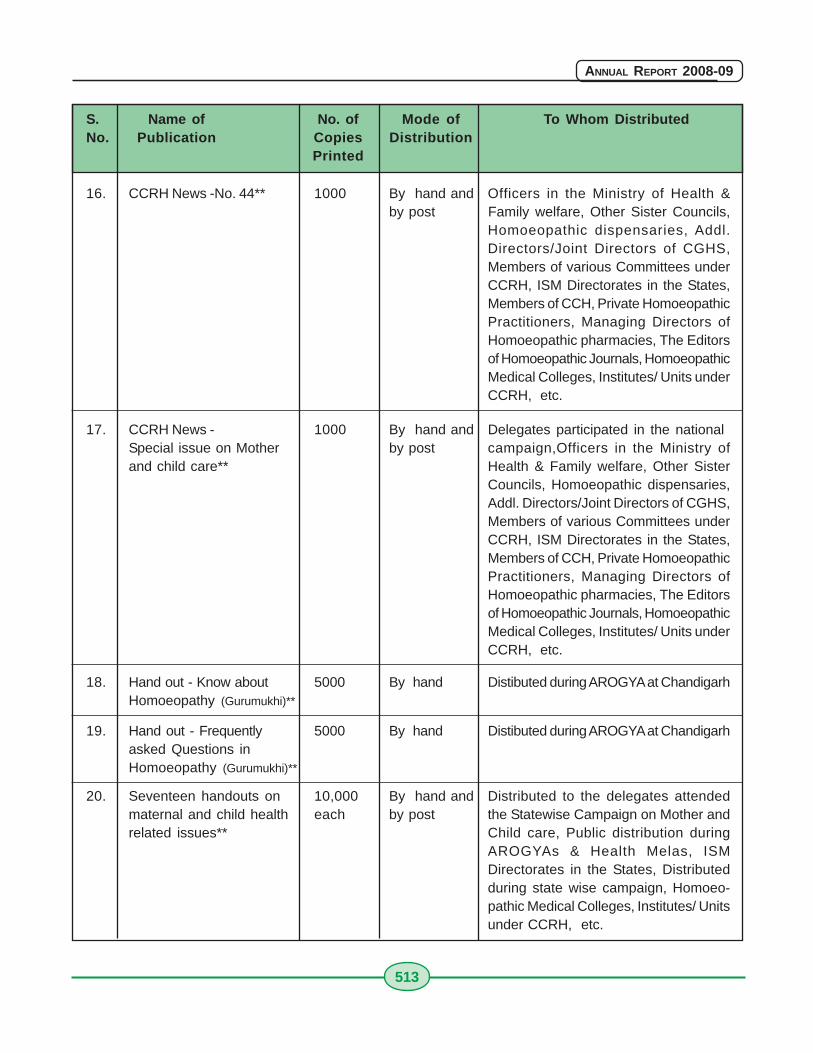
513
ANNUAL REPORT 2008-09
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
16. CCRH News -No. 44** 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
17. CCRH News - 1000 By hand and Delegates participated in the nationalSpecial issue on Mother by post campaign,Officers in the Ministry ofand child care** Health & Family welfare, Other Sister
Councils, Homoeopathic dispensaries,Addl. Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
18. Hand out - Know about 5000 By hand Distibuted during AROGYA at ChandigarhHomoeopathy (Gurumukhi)**
19. Hand out - Frequently 5000 By hand Distibuted during AROGYA at Chandigarhasked Questions inHomoeopathy (Gurumukhi)**
20. Seventeen handouts on 10,000 By hand and Distributed to the delegates attendedmaternal and child health each by post the Statewise Campaign on Mother andrelated issues** Child care, Public distribution during
AROGYAs & Health Melas, ISMDirectorates in the States, Distributedduring state wise campaign, Homoeo-pathic Medical Colleges, Institutes/ Unitsunder CCRH, etc.
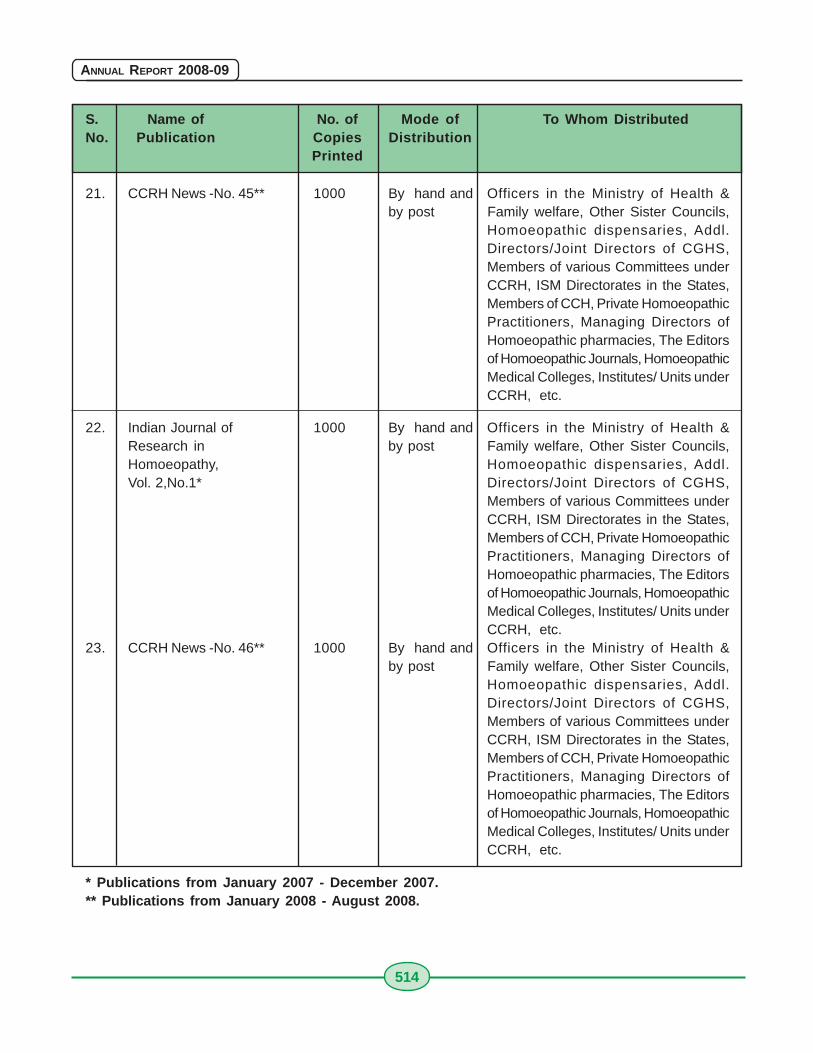
514
ANNUAL REPORT 2008-09
S. Name of No. of Mode of To Whom DistributedNo. Publication Copies Distribution
Printed
21. CCRH News -No. 45** 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
22. Indian Journal of 1000 By hand and Officers in the Ministry of Health &Research in by post Family welfare, Other Sister Councils,Homoeopathy, Homoeopathic dispensaries, Addl.Vol. 2,No.1* Directors/Joint Directors of CGHS,
Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
23. CCRH News -No. 46** 1000 By hand and Officers in the Ministry of Health &by post Family welfare, Other Sister Councils,
Homoeopathic dispensaries, Addl.Directors/Joint Directors of CGHS,Members of various Committees underCCRH, ISM Directorates in the States,Members of CCH, Private HomoeopathicPractitioners, Managing Directors ofHomoeopathic pharmacies, The Editorsof Homoeopathic Journals, HomoeopathicMedical Colleges, Institutes/ Units underCCRH, etc.
* Publications from January 2007 - December 2007.** Publications from January 2008 - August 2008.
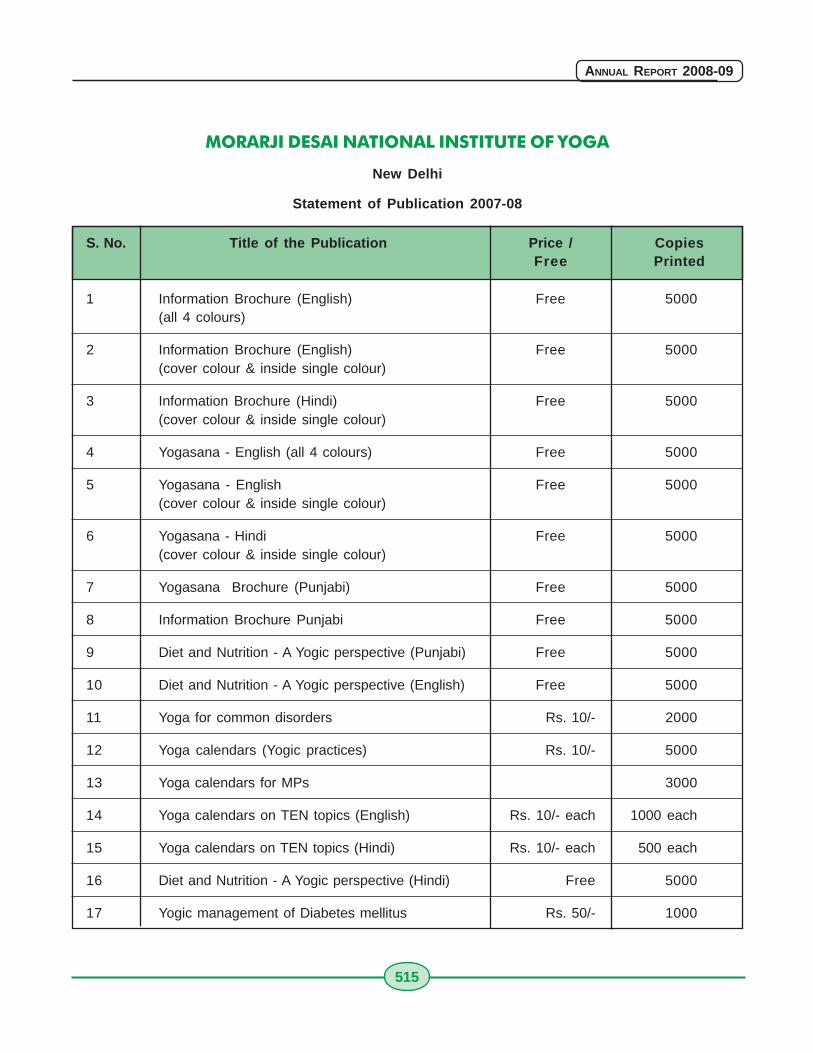
515
ANNUAL REPORT 2008-09
MORARJI DESAI NATIONAL INSTITUTE OF YOGA
New Delhi
Statement of Publication 2007-08
S. No. Title of the Publication Price / CopiesFree Printed
1 Information Brochure (English) Free 5000(all 4 colours)
2 Information Brochure (English) Free 5000(cover colour & inside single colour)
3 Information Brochure (Hindi) Free 5000(cover colour & inside single colour)
4 Yogasana - English (all 4 colours) Free 5000
5 Yogasana - English Free 5000(cover colour & inside single colour)
6 Yogasana - Hindi Free 5000(cover colour & inside single colour)
7 Yogasana Brochure (Punjabi) Free 5000
8 Information Brochure Punjabi Free 5000
9 Diet and Nutrition - A Yogic perspective (Punjabi) Free 5000
10 Diet and Nutrition - A Yogic perspective (English) Free 5000
11 Yoga for common disorders Rs. 10/- 2000
12 Yoga calendars (Yogic practices) Rs. 10/- 5000
13 Yoga calendars for MPs 3000
14 Yoga calendars on TEN topics (English) Rs. 10/- each 1000 each
15 Yoga calendars on TEN topics (Hindi) Rs. 10/- each 500 each
16 Diet and Nutrition - A Yogic perspective (Hindi) Free 5000
17 Yogic management of Diabetes mellitus Rs. 50/- 1000
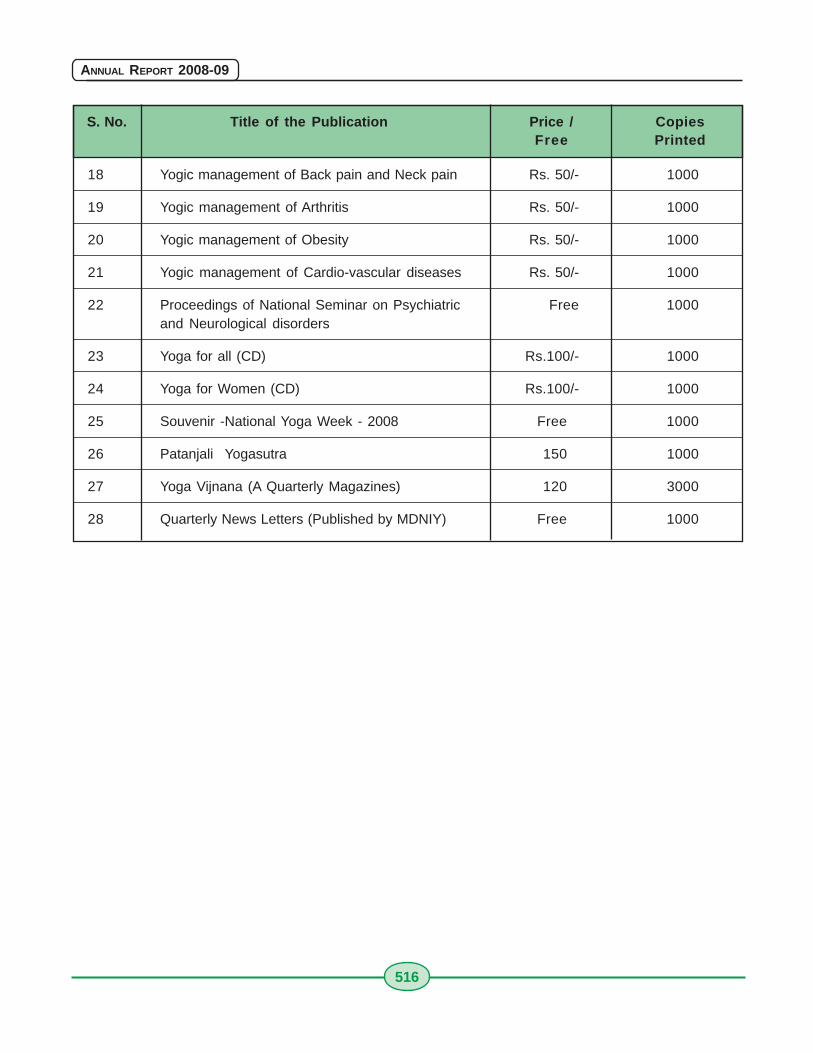
516
ANNUAL REPORT 2008-09
18 Yogic management of Back pain and Neck pain Rs. 50/- 1000
19 Yogic management of Arthritis Rs. 50/- 1000
20 Yogic management of Obesity Rs. 50/- 1000
21 Yogic management of Cardio-vascular diseases Rs. 50/- 1000
22 Proceedings of National Seminar on Psychiatric Free 1000and Neurological disorders
23 Yoga for all (CD) Rs.100/- 1000
24 Yoga for Women (CD) Rs.100/- 1000
25 Souvenir -National Yoga Week - 2008 Free 1000
26 Patanjali Yogasutra 150 1000
27 Yoga Vijnana (A Quarterly Magazines) 120 3000
28 Quarterly News Letters (Published by MDNIY) Free 1000
S. No. Title of the Publication Price / CopiesFree Printed
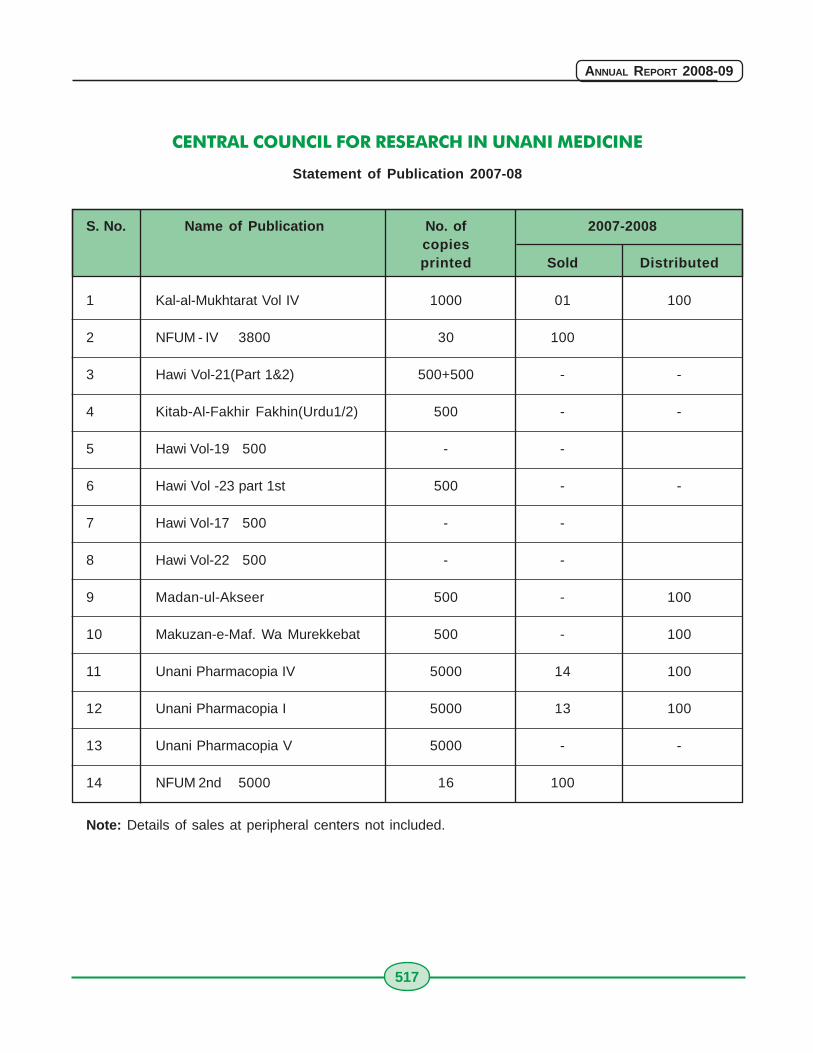
517
ANNUAL REPORT 2008-09
CENTRAL COUNCIL FOR RESEARCH IN UNANI MEDICINE
Statement of Publication 2007-08
S. No. Name of Publication No. of 2007-2008copiesprinted Sold Distributed
1 Kal-al-Mukhtarat Vol IV 1000 01 100
2 NFUM - IV 3800 30 100
3 Hawi Vol-21(Part 1&2) 500+500 - -
4 Kitab-Al-Fakhir Fakhin(Urdu1/2) 500 - -
5 Hawi Vol-19 500 - -
6 Hawi Vol -23 part 1st 500 - -
7 Hawi Vol-17 500 - -
8 Hawi Vol-22 500 - -
9 Madan-ul-Akseer 500 - 100
10 Makuzan-e-Maf. Wa Murekkebat 500 - 100
11 Unani Pharmacopia IV 5000 14 100
12 Unani Pharmacopia I 5000 13 100
13 Unani Pharmacopia V 5000 - -
14 NFUM 2nd 5000 16 100
Note: Details of sales at peripheral centers not included.
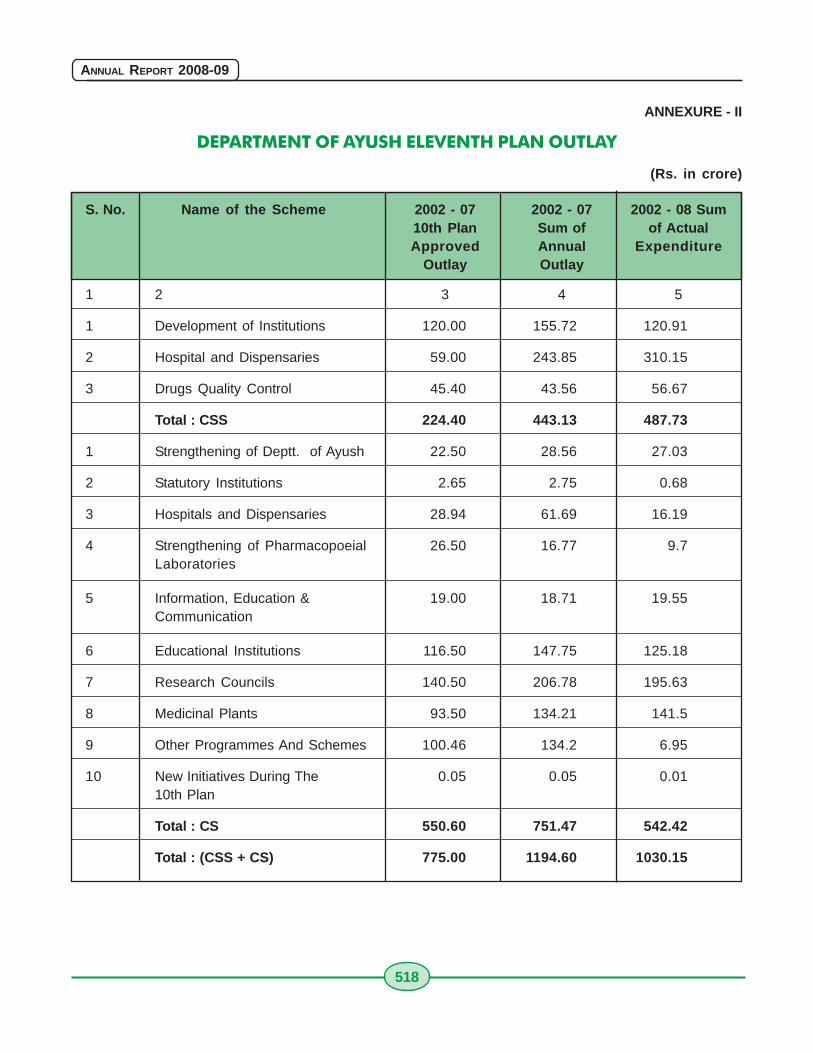
518
ANNUAL REPORT 2008-09
ANNEXURE - II
DEPARTMENT OF AYUSH ELEVENTH PLAN OUTLAY
(Rs. in crore)
S. No. Name of the Scheme 2002 - 07 2002 - 07 2002 - 08 Sum10th Plan Sum of of ActualApproved Annual Expenditure
Outlay Outlay
1 2 3 4 5
1 Development of Institutions 120.00 155.72 120.91
2 Hospital and Dispensaries 59.00 243.85 310.15
3 Drugs Quality Control 45.40 43.56 56.67
Total : CSS 224.40 443.13 487.73
1 Strengthening of Deptt. of Ayush 22.50 28.56 27.03
2 Statutory Institutions 2.65 2.75 0.68
3 Hospitals and Dispensaries 28.94 61.69 16.19
4 Strengthening of Pharmacopoeial 26.50 16.77 9.7Laboratories
5 Information, Education & 19.00 18.71 19.55Communication
6 Educational Institutions 116.50 147.75 125.18
7 Research Councils 140.50 206.78 195.63
8 Medicinal Plants 93.50 134.21 141.5
9 Other Programmes And Schemes 100.46 134.2 6.95
10 New Initiatives During The 0.05 0.05 0.0110th Plan
Total : CS 550.60 751.47 542.42
Total : (CSS + CS) 775.00 1194.60 1030.15
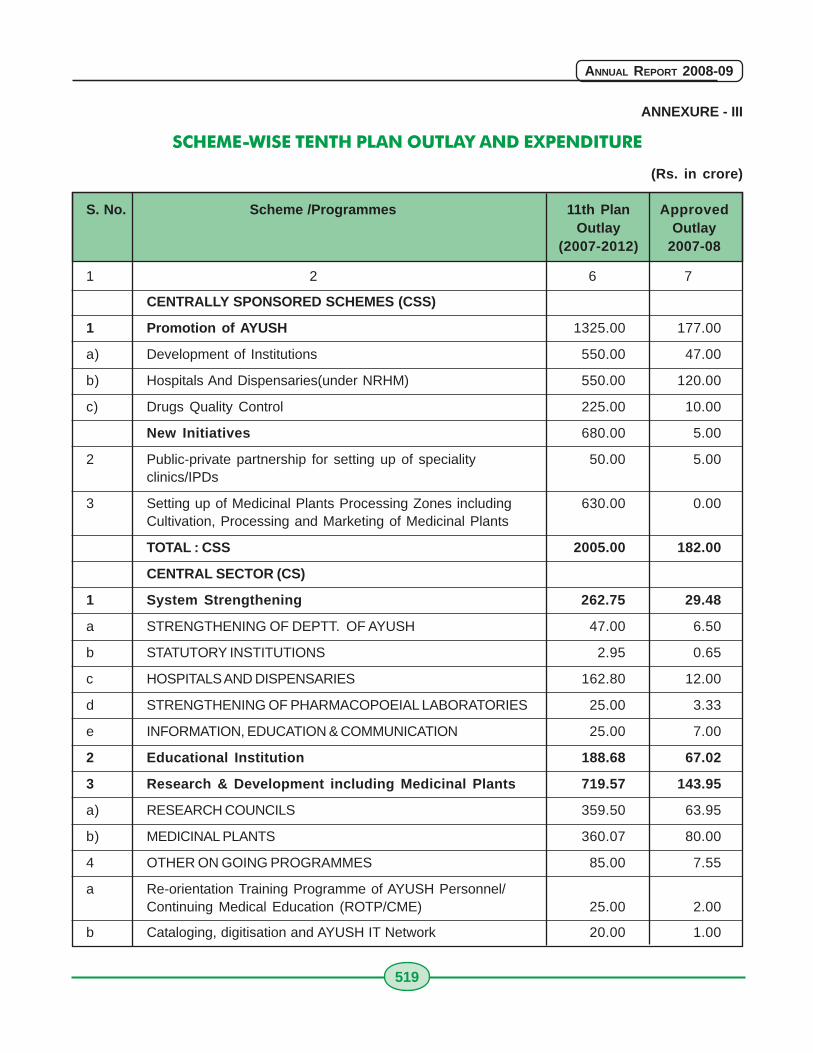
519
ANNUAL REPORT 2008-09
ANNEXURE - III
SCHEME-WISE TENTH PLAN OUTLAY AND EXPENDITURE
(Rs. in crore)
S. No. Scheme /Programmes 11th Plan ApprovedOutlay Outlay
(2007-2012) 2007-08
1 2 6 7
CENTRALLY SPONSORED SCHEMES (CSS)
1 Promotion of AYUSH 1325.00 177.00
a) Development of Institutions 550.00 47.00
b) Hospitals And Dispensaries(under NRHM) 550.00 120.00
c) Drugs Quality Control 225.00 10.00
New Initiatives 680.00 5.00
2 Public-private partnership for setting up of speciality 50.00 5.00clinics/IPDs
3 Setting up of Medicinal Plants Processing Zones including 630.00 0.00Cultivation, Processing and Marketing of Medicinal Plants
TOTAL : CSS 2005.00 182.00
CENTRAL SECTOR (CS)
1 System Strengthening 262.75 29.48
a STRENGTHENING OF DEPTT. OF AYUSH 47.00 6.50
b STATUTORY INSTITUTIONS 2.95 0.65
c HOSPITALS AND DISPENSARIES 162.80 12.00
d STRENGTHENING OF PHARMACOPOEIAL LABORATORIES 25.00 3.33
e INFORMATION, EDUCATION & COMMUNICATION 25.00 7.00
2 Educational Institution 188.68 67.02
3 Research & Development including Medicinal Plants 719.57 143.95
a) RESEARCH COUNCILS 359.50 63.95
b) MEDICINAL PLANTS 360.07 80.00
4 OTHER ON GOING PROGRAMMES 85.00 7.55
a Re-orientation Training Programme of AYUSH Personnel/Continuing Medical Education (ROTP/CME) 25.00 2.00
b Cataloging, digitisation and AYUSH IT Network 20.00 1.00
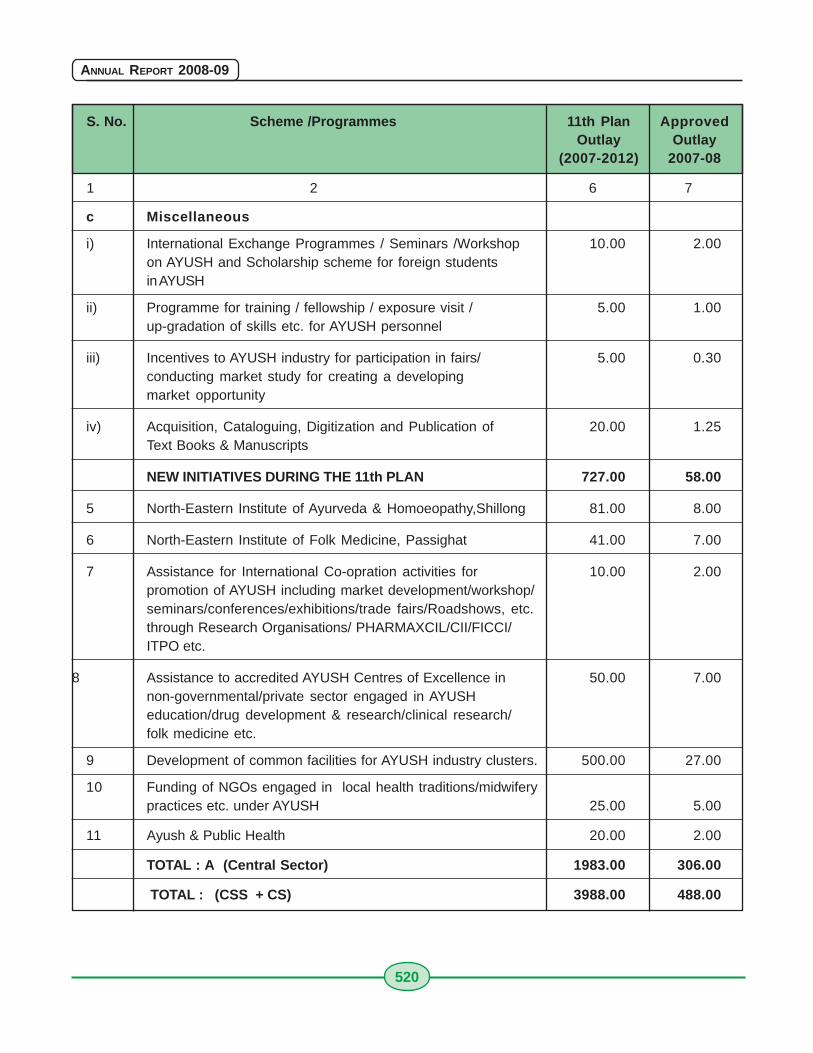
520
ANNUAL REPORT 2008-09
S. No. Scheme /Programmes 11th Plan ApprovedOutlay Outlay
(2007-2012) 2007-08
1 2 6 7
c Miscellaneous
i) International Exchange Programmes / Seminars /Workshop 10.00 2.00on AYUSH and Scholarship scheme for foreign studentsin AYUSH
ii) Programme for training / fellowship / exposure visit / 5.00 1.00up-gradation of skills etc. for AYUSH personnel
iii) Incentives to AYUSH industry for participation in fairs/ 5.00 0.30conducting market study for creating a developingmarket opportunity
iv) Acquisition, Cataloguing, Digitization and Publication of 20.00 1.25Text Books & Manuscripts
NEW INITIATIVES DURING THE 11th PLAN 727.00 58.00
5 North-Eastern Institute of Ayurveda & Homoeopathy,Shillong 81.00 8.00
6 North-Eastern Institute of Folk Medicine, Passighat 41.00 7.00
7 Assistance for International Co-opration activities for 10.00 2.00promotion of AYUSH including market development/workshop/seminars/conferences/exhibitions/trade fairs/Roadshows, etc.through Research Organisations/ PHARMAXCIL/CII/FICCI/ITPO etc.
8 Assistance to accredited AYUSH Centres of Excellence in 50.00 7.00non-governmental/private sector engaged in AYUSHeducation/drug development & research/clinical research/folk medicine etc.
9 Development of common facilities for AYUSH industry clusters. 500.00 27.00
10 Funding of NGOs engaged in local health traditions/midwiferypractices etc. under AYUSH 25.00 5.00
11 Ayush & Public Health 20.00 2.00
TOTAL : A (Central Sector) 1983.00 306.00
TOTAL : (CSS + CS) 3988.00 488.00
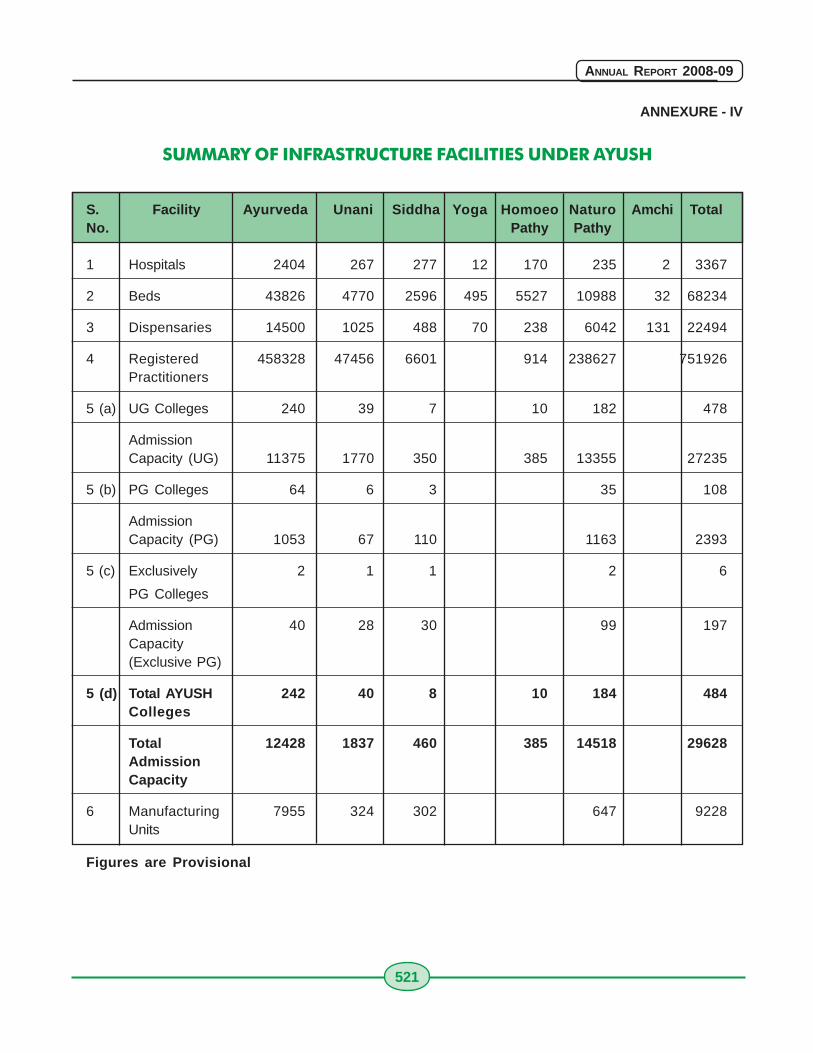
521
ANNUAL REPORT 2008-09
ANNEXURE - IV
SUMMARY OF INFRASTRUCTURE FACILITIES UNDER AYUSH
S. Facility Ayurveda Unani Siddha Yoga Homoeo Naturo Amchi TotalNo. Pathy Pathy
1 Hospitals 2404 267 277 12 170 235 2 3367
2 Beds 43826 4770 2596 495 5527 10988 32 68234
3 Dispensaries 14500 1025 488 70 238 6042 131 22494
4 Registered 458328 47456 6601 914 238627 751926Practitioners
5 (a) UG Colleges 240 39 7 10 182 478
AdmissionCapacity (UG) 11375 1770 350 385 13355 27235
5 (b) PG Colleges 64 6 3 35 108
AdmissionCapacity (PG) 1053 67 110 1163 2393
5 (c) Exclusively 2 1 1 2 6
PG Colleges
Admission 40 28 30 99 197Capacity(Exclusive PG)
5 (d) Total AYUSH 242 40 8 10 184 484Colleges
Total 12428 1837 460 385 14518 29628AdmissionCapacity
6 Manufacturing 7955 324 302 647 9228Units
Figures are Provisional
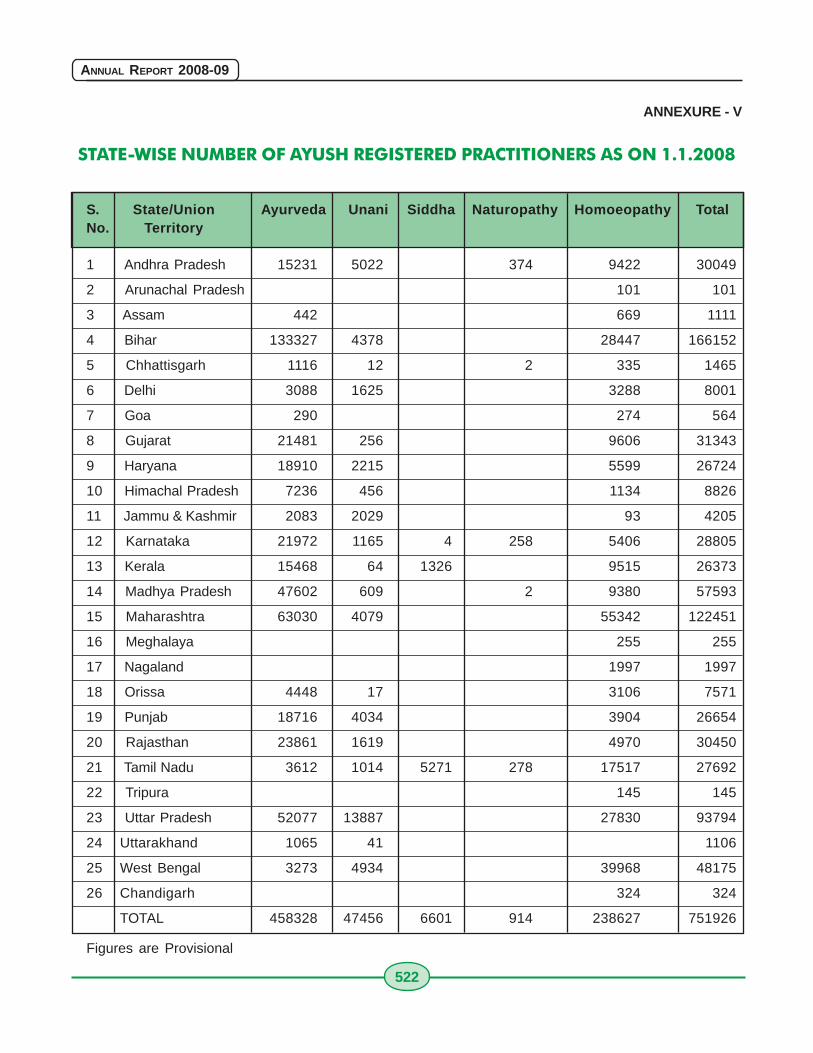
522
ANNUAL REPORT 2008-09
ANNEXURE - V
STATE-WISE NUMBER OF AYUSH REGISTERED PRACTITIONERS AS ON 1.1.2008
S. State/Union Ayurveda Unani Siddha Naturopathy Homoeopathy TotalNo. Territory
1 Andhra Pradesh 15231 5022 374 9422 30049
2 Arunachal Pradesh 101 101
3 Assam 442 669 1111
4 Bihar 133327 4378 28447 166152
5 Chhattisgarh 1116 12 2 335 1465
6 Delhi 3088 1625 3288 8001
7 Goa 290 274 564
8 Gujarat 21481 256 9606 31343
9 Haryana 18910 2215 5599 26724
10 Himachal Pradesh 7236 456 1134 8826
11 Jammu & Kashmir 2083 2029 93 4205
12 Karnataka 21972 1165 4 258 5406 28805
13 Kerala 15468 64 1326 9515 26373
14 Madhya Pradesh 47602 609 2 9380 57593
15 Maharashtra 63030 4079 55342 122451
16 Meghalaya 255 255
17 Nagaland 1997 1997
18 Orissa 4448 17 3106 7571
19 Punjab 18716 4034 3904 26654
20 Rajasthan 23861 1619 4970 30450
21 Tamil Nadu 3612 1014 5271 278 17517 27692
22 Tripura 145 145
23 Uttar Pradesh 52077 13887 27830 93794
24 Uttarakhand 1065 41 1106
25 West Bengal 3273 4934 39968 48175
26 Chandigarh 324 324
TOTAL 458328 47456 6601 914 238627 751926
Figures are Provisional
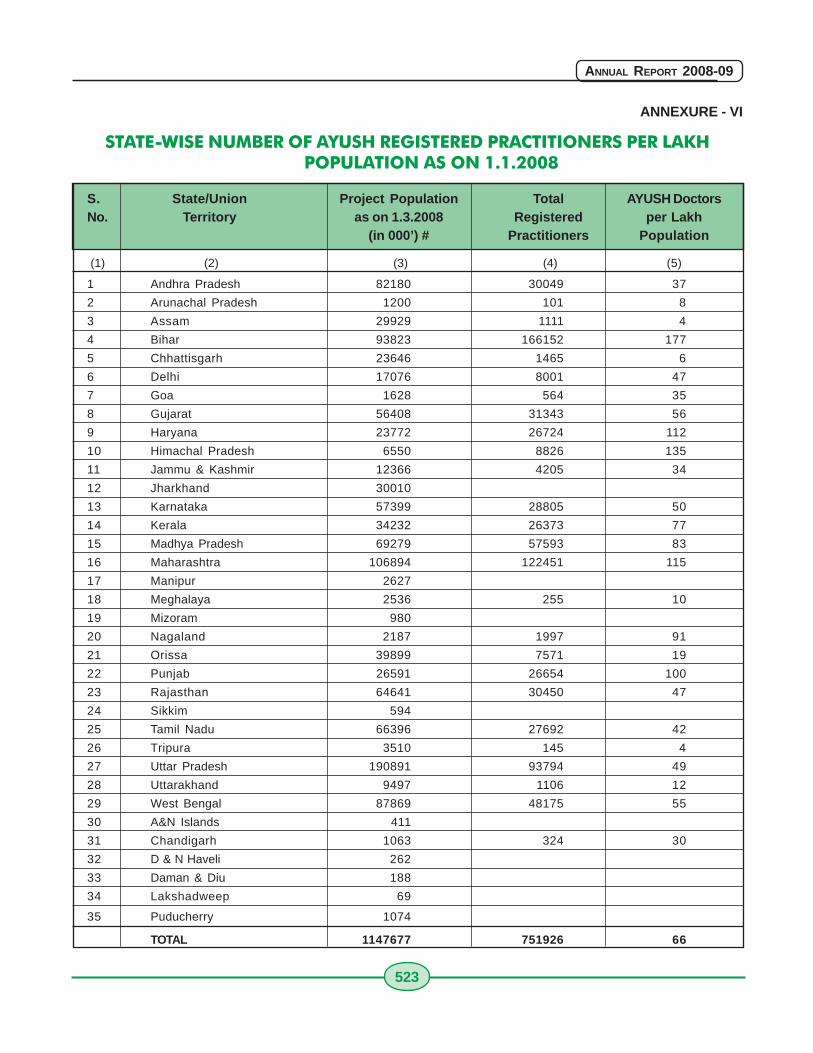
523
ANNUAL REPORT 2008-09
ANNEXURE - VI
STATE-WISE NUMBER OF AYUSH REGISTERED PRACTITIONERS PER LAKHPOPULATION AS ON 1.1.2008
S. State/Union Project Population Total AYUSH DoctorsNo. Territory as on 1.3.2008 Registered per Lakh
(in 000’) # Practitioners Population
(1) (2) (3) (4) (5)
1 Andhra Pradesh 82180 30049 37
2 Arunachal Pradesh 1200 101 8
3 Assam 29929 1111 4
4 Bihar 93823 166152 177
5 Chhattisgarh 23646 1465 6
6 Delhi 17076 8001 47
7 Goa 1628 564 35
8 Gujarat 56408 31343 56
9 Haryana 23772 26724 112
10 Himachal Pradesh 6550 8826 135
11 Jammu & Kashmir 12366 4205 34
12 Jharkhand 30010
13 Karnataka 57399 28805 50
14 Kerala 34232 26373 77
15 Madhya Pradesh 69279 57593 83
16 Maharashtra 106894 122451 115
17 Manipur 2627
18 Meghalaya 2536 255 10
19 Mizoram 980
20 Nagaland 2187 1997 91
21 Orissa 39899 7571 19
22 Punjab 26591 26654 100
23 Rajasthan 64641 30450 47
24 Sikkim 594
25 Tamil Nadu 66396 27692 42
26 Tripura 3510 145 4
27 Uttar Pradesh 190891 93794 49
28 Uttarakhand 9497 1106 12
29 West Bengal 87869 48175 55
30 A&N Islands 411
31 Chandigarh 1063 324 30
32 D & N Haveli 262
33 Daman & Diu 188
34 Lakshadweep 69
35 Puducherry 1074
TOTAL 1147677 751926 66
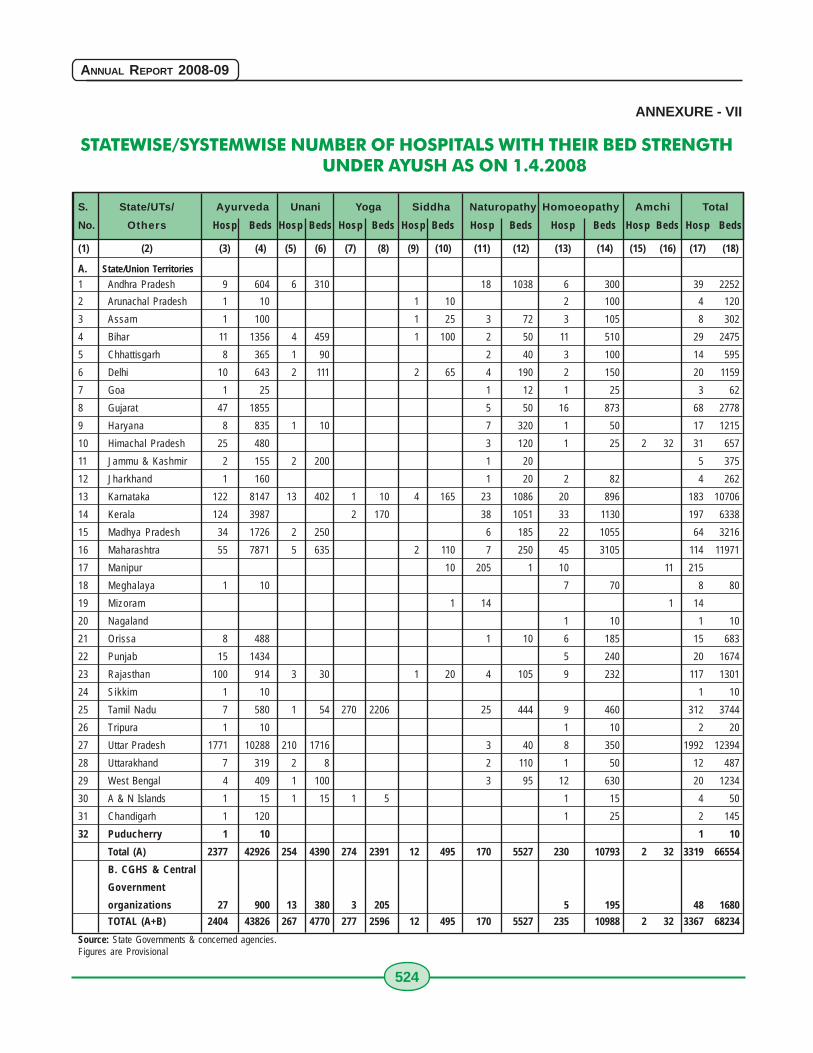
524
ANNUAL REPORT 2008-09
ANNEXURE - VII
STATEWISE/SYSTEMWISE NUMBER OF HOSPITALS WITH THEIR BED STRENGTHUNDER AYUSH AS ON 1.4.2008
S. State/UTs/ Ayurveda Unani Yoga Siddha Naturopathy Homoeopathy Amchi Total
No. Others Hosp Beds Hosp Beds Hosp Beds Hosp Beds Hosp Beds Hosp Beds Hosp Beds Hosp Beds
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18)
A. State/Union Territories
1 Andhra Pradesh 9 604 6 310 18 1038 6 300 39 2252
2 Arunachal Pradesh 1 10 1 10 2 100 4 120
3 Assam 1 100 1 25 3 72 3 105 8 302
4 Bihar 11 1356 4 459 1 100 2 50 11 510 29 2475
5 Chhattisgarh 8 365 1 90 2 40 3 100 14 595
6 Delhi 10 643 2 111 2 65 4 190 2 150 20 1159
7 Goa 1 25 1 12 1 25 3 62
8 Gujarat 47 1855 5 50 16 873 68 2778
9 Haryana 8 835 1 10 7 320 1 50 17 1215
10 Himachal Pradesh 25 480 3 120 1 25 2 32 31 657
11 Jammu & Kashmir 2 155 2 200 1 20 5 375
12 Jharkhand 1 160 1 20 2 82 4 262
13 Karnataka 122 8147 13 402 1 10 4 165 23 1086 20 896 183 10706
14 Kerala 124 3987 2 170 38 1051 33 1130 197 6338
15 Madhya Pradesh 34 1726 2 250 6 185 22 1055 64 3216
16 Maharashtra 55 7871 5 635 2 110 7 250 45 3105 114 11971
17 Manipur 10 205 1 10 11 215
18 Meghalaya 1 10 7 70 8 80
19 Mizoram 1 14 1 14
20 Nagaland 1 10 1 10
21 Orissa 8 488 1 10 6 185 15 683
22 Punjab 15 1434 5 240 20 1674
23 Rajasthan 100 914 3 30 1 20 4 105 9 232 117 1301
24 Sikkim 1 10 1 10
25 Tamil Nadu 7 580 1 54 270 2206 25 444 9 460 312 3744
26 Tripura 1 10 1 10 2 20
27 Uttar Pradesh 1771 10288 210 1716 3 40 8 350 1992 12394
28 Uttarakhand 7 319 2 8 2 110 1 50 12 487
29 West Bengal 4 409 1 100 3 95 12 630 20 1234
30 A & N Islands 1 15 1 15 1 5 1 15 4 50
31 Chandigarh 1 120 1 25 2 145
32 Puducherry 1 10 1 10
Total (A) 2377 42926 254 4390 274 2391 12 495 170 5527 230 10793 2 32 3319 66554
B. CGHS & Central
Government
organizations 27 900 13 380 3 205 5 195 48 1680
TOTAL (A+B) 2404 43826 267 4770 277 2596 12 495 170 5527 235 10988 2 32 3367 68234
Source: State Governments & concerned agencies.Figures are Provisional
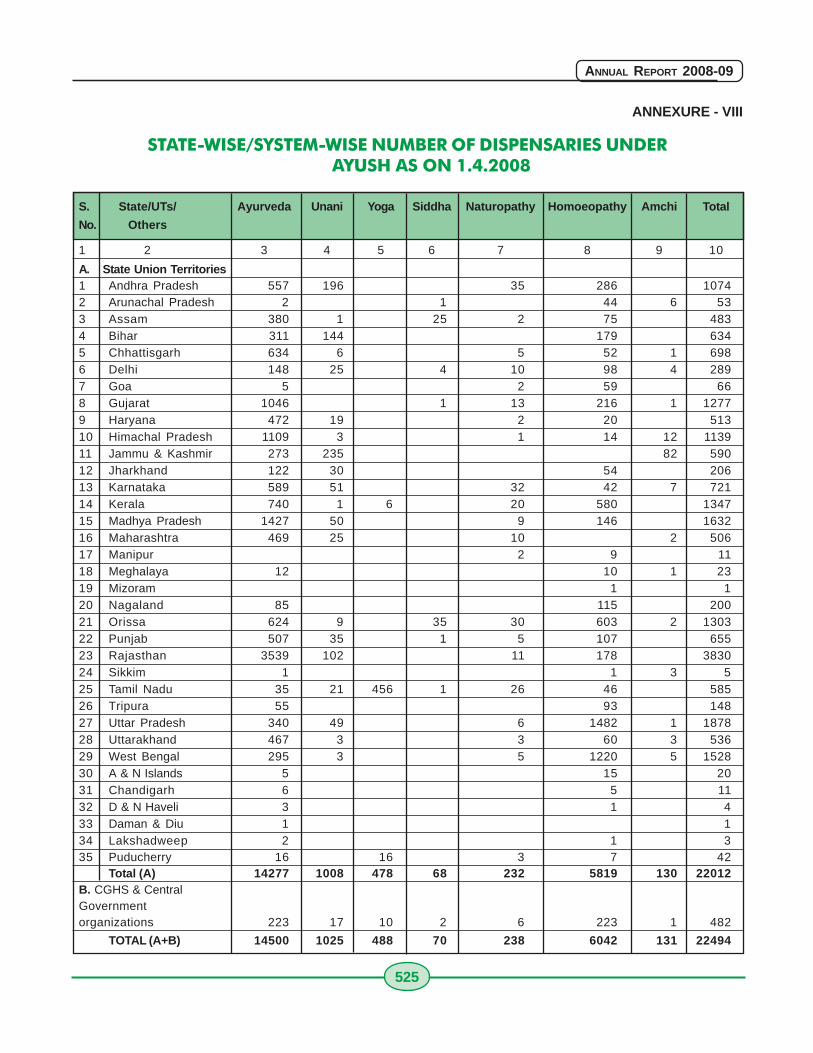
525
ANNUAL REPORT 2008-09
ANNEXURE - VIII
STATE-WISE/SYSTEM-WISE NUMBER OF DISPENSARIES UNDERAYUSH AS ON 1.4.2008
S. State/UTs/ Ayurveda Unani Yoga Siddha Naturopathy Homoeopathy Amchi Total
No. Others
1 2 3 4 5 6 7 8 9 10
A. State Union Territories1 Andhra Pradesh 557 196 35 286 10742 Arunachal Pradesh 2 1 44 6 533 Assam 380 1 25 2 75 4834 Bihar 311 144 179 6345 Chhattisgarh 634 6 5 52 1 6986 Delhi 148 25 4 10 98 4 2897 Goa 5 2 59 668 Gujarat 1046 1 13 216 1 12779 Haryana 472 19 2 20 51310 Himachal Pradesh 1109 3 1 14 12 113911 Jammu & Kashmir 273 235 82 59012 Jharkhand 122 30 54 20613 Karnataka 589 51 32 42 7 72114 Kerala 740 1 6 20 580 134715 Madhya Pradesh 1427 50 9 146 163216 Maharashtra 469 25 10 2 50617 Manipur 2 9 1118 Meghalaya 12 10 1 2319 Mizoram 1 120 Nagaland 85 115 20021 Orissa 624 9 35 30 603 2 130322 Punjab 507 35 1 5 107 65523 Rajasthan 3539 102 11 178 383024 Sikkim 1 1 3 525 Tamil Nadu 35 21 456 1 26 46 58526 Tripura 55 93 14827 Uttar Pradesh 340 49 6 1482 1 187828 Uttarakhand 467 3 3 60 3 53629 West Bengal 295 3 5 1220 5 152830 A & N Islands 5 15 2031 Chandigarh 6 5 1132 D & N Haveli 3 1 433 Daman & Diu 1 134 Lakshadweep 2 1 335 Puducherry 16 16 3 7 42
Total (A) 14277 1008 478 68 232 5819 130 22012B. CGHS & CentralGovernmentorganizations 223 17 10 2 6 223 1 482
TOTAL (A+B) 14500 1025 488 70 238 6042 131 22494






























