Embed Size (px)
Citation preview

R
FS
EA
A
I
AtP“c
1
U2
V3
4
5
g
AFV©d
ESEARCH BRIEF
it WIC: Attitudes, Perceptions and Practices of WICtaff toward Addressing Childhood Overweight
lena Serrano, PhD1; Emily Gresock, MS2; David Suttle, MD3;drienne Keller, PhD4; Elizabeth McGarvey, EdD5
BSTRACT
Objective: To assess the attitudes, perceptions, and practices of staff of the Special SupplementalNutrition Program for Women, Infants, and Children (WIC) in providing nutrition education onchildhood overweight topics with WIC participants.
Design: Descriptive and correlational study.
Setting: WIC clinics in Virginia.
Participants: 106 employees working in direct contact with WIC participants.
Mean Outcome Measure(s): Demographic information; comfort level and frequency of discussingchildhood overweight-related topics with participants; perception of WIC’s ability to prevent andhelp address overweight among children and adults; body mass index (BMI); and attitudes towardpersonal weight.
Analysis: Descriptive statistics, regression, and analysis of variance.
Results: WIC staff in this study reported a lack of comfort, practice, and confidence in addressingand/or preventing childhood overweight with WIC participants, with differences existing based onjob title (P � .05). Barriers to implementing programs included perceived attitudes of participants,transportation, time, cultural issues, and childcare. Staff BMIs were significantly correlated toethnicity, age, feeling overweight, unhappiness with current weight, and comfort level discussingfruit and vegetable intake and physical activity (P � .05).
Conclusions and Implications: Staff training, health promotion programs, and culturally relevanteducational materials are warranted for WIC staff to build a strong knowledge base and promoteself-efficacy about childhood overweight-related topics.
Key Words: WIC, staff, overweight, attitudes
(J Nutr Educ Behav. 2006;38:151-156)
pesii
oTwWNmaae8a
NTRODUCTION
s one of the key food and nutrition assistance programs inhe United States, the Special Supplemental Nutritionrogram for Women, Infants, and Children (WIC) aims tosafeguard the health of low-income women, infants, andhildren up to age 5 who are at nutritional risk.”1 Partici-
Extension Specialist, Assistant Professor, Virginia Polytechnic Institute & Stateniversity
Former Nutrition Liaison, Division of WIC and Community Nutrition Services,irginia
Department of Health Director, Office of Family Health Services, VirginiaDepartment of Health Associate Professor, University of VirginiaAssociate Professor, Director, Division of Prevention Research, University of Vir-inia
ddress for correspondence: Elena Serrano, PhD, Department of Human Nutrition,oods, and Exercise, Virginia Polytechnic Institute and State University, Blacksburg,A 24061-0430; Tel.: (540) 231-3464; Fax: (540) 231-3916; Email: [email protected]
t2006 SOCIETY FOR NUTRITION EDUCATIONoi: 10.1016/j.jneb.2005.11.030
ant benefits include supplemental food packages, nutritionducation, and referrals. To date, WIC has demonstratedeveral positive health and nutrition outcomes, includingmprovements in birth weights and iron-deficiency amongnfants.2,3
In the past few years, childhood overweight and adultbesity have been growing concerns in the United States.4,5
his trend has also been evident among WIC populations,ith the proportion of overweight children participating inIC increasing dramatically.6 In response, the Food andutrition Service (FNS), the agency of the U.S. Depart-ent of Agriculture (USDA) that administers WIC, addednew risk for program eligibility for infants and children,
t-risk of becoming overweight. This risk criterion wasstablished as a child at least 24 months old between the5th and 95th percentile of body mass index (BMI) for agend gender, an infant born to a mother who was obese at
he time of conception or during the first trimester or, for
bb
pioptVotaTti
DS
Otscwp
CatssiCe
S
Aatsmitwtn.t6ts
twp
soaictDdw
W
IttTtcwta
D
TatdpratttmeptmAso
IfscOttRceO
152 Serrano et al/ATTITUDES, PERCEPTIONS, AND PRACTICES OF WIC STAFF CONCERNING CHILDHOOD OVERWEIGHT
oth children and infants, the existence of obesity in one oroth parents.7
Additionally, the FNS awarded grants for a multistateroject, titled Fit WIC, to identify opportunities for address-ng childhood overweight in WIC clinics through a varietyf mechanisms.8 The study reported here represents a com-onent of the Fit WIC project that was conducted to assesshe perceptions, attitudes, and practices of WIC staff inirginia toward addressing key issues related to childhoodverweight with clients. This study provides insight intohe perceived capacity, challenges, and strategies of WIC toddress this growing concern, from the perspective of staff.he results will, in turn, guide the development and pilot
esting of staff development and wellness programs thatnclude “front-line support staff.”
ESCRIPTION OF THE EVALUATIONubjects
f a total of 147 staff members, who were in attendance athe respective WIC clinics in all 11 health districts on aingle day, 106 WIC staff completed and returned a hardopy questionnaire, for a response rate of 72.1%. All staffith direct contact or communication with WIC partici-ants were eligible to complete the questionnaire.
The study was reviewed by the Human Investigationommittee at the University of Virginia prior to its initi-
tion and was exempt as an anonymous survey, with resultso be used for educational purposes. Participation in thetudy was completely voluntary. Confidentiality was en-ured by not requiring names or any form of personaldentification to be included on the survey instrument.ompleted questionnaires were returned to independent
valuators of the WIC program by fax or by mail.
urvey instrument
questionnaire, which included a combination of open-nd closed-ended questions, was developed specifically forhis project by WIC staff working on the grant and univer-ity evaluators, because no comparable evaluation instru-ent existed. The questionnaire, which was developed
mmediately following focus groups with WIC staff, cap-ured and formalized the key items from the focus groups,hile taking into account staff perspectives and attitudes
oward their jobs and childhood overweight. The question-aire was found to have an excellent internal consistency of
852 (Cronbach’s alpha). Further, based on factor analyses,he first eigenvalue for the first principal component was.329 and described 42.7% of the variability, demonstratinghe instrument’s effectiveness in capturing reliable and con-istent responses.
Questionnaire topics covered: attitudes about the par-icipants’ own weight, such as if they felt they were over-eight and if they were happy with their current weight;
erceptions toward how comfortable they were in raising rpecific topics or issues with parents related to childhoodverweight, such as overfeeding; and practices related toctually “talking” to participants about nutrition, parent-ng, and physical activity. Suggestions for implementinghildhood overweight prevention programs in their respec-ive WIC clinics, based on perceived barriers, were elicited.emographic information was also collected on age, gen-er, ethnicity, health district (region), job title, years ofork experience with WIC, and highest level of education.
eight status
n order to determine if weight status influenced attitudesoward childhood overweight topics, WIC staff were askedo report weight (in pounds) and height (feet and inches).hese data were converted to body mass index (BMI), using
he BMI Index Formula.9 Weight status was determined byategories established by the Centers for Disease Control,ith underweight defined as a BMI below 18.5, normal 18.5
o 24.9, overweight 25.0 to 29.9, and obese as 30.0 andbove.10,11
ata analysis
he following job titles were used, based on responsibilitiesnd training: office support staff; nutrition assistants; nutri-ionists; nurses; and managerial staff. Office support staffetermine residential, income, and categorical eligibility,rint checks, and make appointments. Nutrition assistantsequire a high school diploma or equivalent, provide bothdministrative and technical support by helping with officeasks (similar to office support staff), and assist the nutri-ionist with nutrition assessment and education. WIC nu-ritionists have specific training in nutrition, with a mini-um of a bachelor’s degree in nutrition or dietetics, and
ligibility or current licensure as a registered dietitian. Theyerform health and nutrition assessments, along with nu-rition counseling. As with nutritionists, WIC nurses assessedical and nutrition risk of clients, along with counseling.bachelor’s degree in nursing is mandatory, along with
tate licensure. Managerial staff coordinate the operationsf the clinic, as well as counsel clients upon demand.
Statistical evaluation was performed using SPSS (SPSS,nc., Chicago, IL). Frequencies and means were calculatedor all closed-ended responses based on job title and weighttatus, with both variables assigned numerical codes. Per-entages were also calculated, not including nonresponses.ne-way analysis of variance (ANOVA) was used to de-
ermine differences between responses based on WIC jobitle, excluding managerial staff because of small cell sizes.egression analyses were conducted to assess the signifi-ance of BMI with several demographic factors, includingthnicity, age, health district, and responses to questions.pen-ended responses were coded and given numerical
esponses. Frequencies were then calculated based on the

te
LD
Rs(snewl“urpy(eh
W
OBAnotac“a
MawAac(eB�
Co
Ofoto
�dwenh
roti(dtamsthic
Lc
WWo(parlspwsdwer
Co
O3fwoh4vto
Journal of Nutrition Education and Behavior ● Volume 38, Number 3, May/June 2006 153
otal number of responses, including multiple responses toach question.
ESSONS LEARNEDemographic information
espondents included nutritionists (30.3%), nutrition as-istants (31.5%), office support staff (23.6%), nurses10.1%), and managerial staff (4.5%). The subjects repre-ented a broad range of work experience with WIC, withearly one-quarter (22.9%) having less than three years ofxperience and 28.6% more than 10 years. All respondentsere female, with the majority being white (70.7%), fol-
owed by African American (19.2%), Hispanic (6.1%), andother” (4.0%), which included one Asian. Seven individ-als did not report their ethnicity. Ages of respondentsanged from 23 to 64, with a mean age of 42.0. The highestercentage of individuals was in the age category of 40 to 49ears old (39.4%). Over half had at least a bachelor’s degree51.9%). Job title was significantly correlated to level ofducation (P � .05), with senior level positions havingigher levels of education, based on ANOVA.
eight categories
f the 88 who provided weight and height information,MIs ranged from 14.2 to 41.3, with a mean BMI of 24.7.lthough over half of respondents, 58.0%, were consideredormal weight, 3.4% were considered underweight, 26.1%verweight, and 12.5% obese. Based on Pearson correla-ions and univariate regression, BMI was positively associ-ted with feeling overweight and being unhappy about theirurrent weight, with 86.4% of staff who felt “somewhat” orvery much” overweight classified as overweight or obesend 78.9% of those unhappy with their current weight.
BMI was also correlated (P � .01) to age and ethnicity.ean BMI increased with age. Nearly two-thirds (63.6) of
ll respondents between 50 and 64 were classified as over-eight. Significant differences were found between Africanmerican and white subjects, when excluding Hispanics
nd “other” from analyses because of small cell sizes. Afri-an American staff had over twice the rate of overweight66.7%) than white staff (29.5%). When including allthnic groups, African Americans had the highest meanMI at 28.0 (SD � 5.42), followed by Hispanic, 27.0 (SD
4.02), then white, 24.1 (SD � 4.32).
omfort level in addressing childhoodverweight topics
verall, WIC staff felt most comfortable about addressingruit and vegetable intake and least comfortable aboutverweight or obesity with their participants, as shown byhe mean scores in Table 1. All of the responses for this set
f questions were significantly correlated to each other (P b.01). Ethnicity, age, and length of experience with WICid not significantly influence scores. Level of educationas positively correlated (P � .05) to all responses. Theffects of job title were also significant (P � .05). Althoughot included in the analyses, the managerial staff had theighest scores and the office support staff the lowest.
Overall, underweight and normal weight WIC staffeported feeling more comfortable about childhoodverweight-related topics. There were significant associa-ions between BMI and comfort level about fruit/vegetablentake and physical activity (P � .05). Almost two-thirds66.7%) of staff who reported being uncomfortable aboutiscussing physical activity were overweight, and 54.5% ofhose respondents were uncomfortable with discussing fruitnd vegetable intake. In both cases, there was a decline inean comfort level with increasing BMI. Although not
ignificant, obese staff had the lowest overall mean relatedo talking about overweight, 2.55, and underweight theighest, 3.33. Nevertheless, one-half of respondents who
ndicated they felt “very uncomfortable” or “slightly un-omfortable” were of normal weight.
evel of reported communication abouthildhood overweight topics
IC staff reported actually talking or communicating toIC clients about nutrition the most, and parenting and
verweight the least, as shown in Table 1. Over one-third35.6%) of staff indicated that they spent 20 or more hourser week on nutrition, compared to only 8.0% for parentingnd 9.6% for overweight. Conversely, two-thirds (68.0%)eported either never talking about parenting or spendingess than 5 hours per week on the topic. The rate waslightly lower for overweight, 62.8%. With the exception ofarenting, responses varied by job title at the P � .01 level,ith nutritionists talking to participants the most. Weight
tatus, ethnicity, age, and length of experience with WICid not significantly influence scores. Level of educationas correlated (P � .05) to all responses. In general, higherducational attainment was associated with more teachingeported.
onfidence in addressing childhoodverweight
n a scale of “not at all” (1) to “completely” (5), fewer than0% thought it was “very much” or “completely” possibleor WIC staff to prevent children from becoming over-eight, to help overweight children reach a healthy weight,r to help overweight adults reach a healthy weight. Theighest response for each question was “somewhat” (3) at9.0%, 53.3%, and 48.1%, respectively. On the other hand,ery few thought that it was not possible at all. Responseso all three questions were significantly correlated to eachther (P � .01) . There were significant effects (P � .05)
etween African American (mean score of 3.32) and white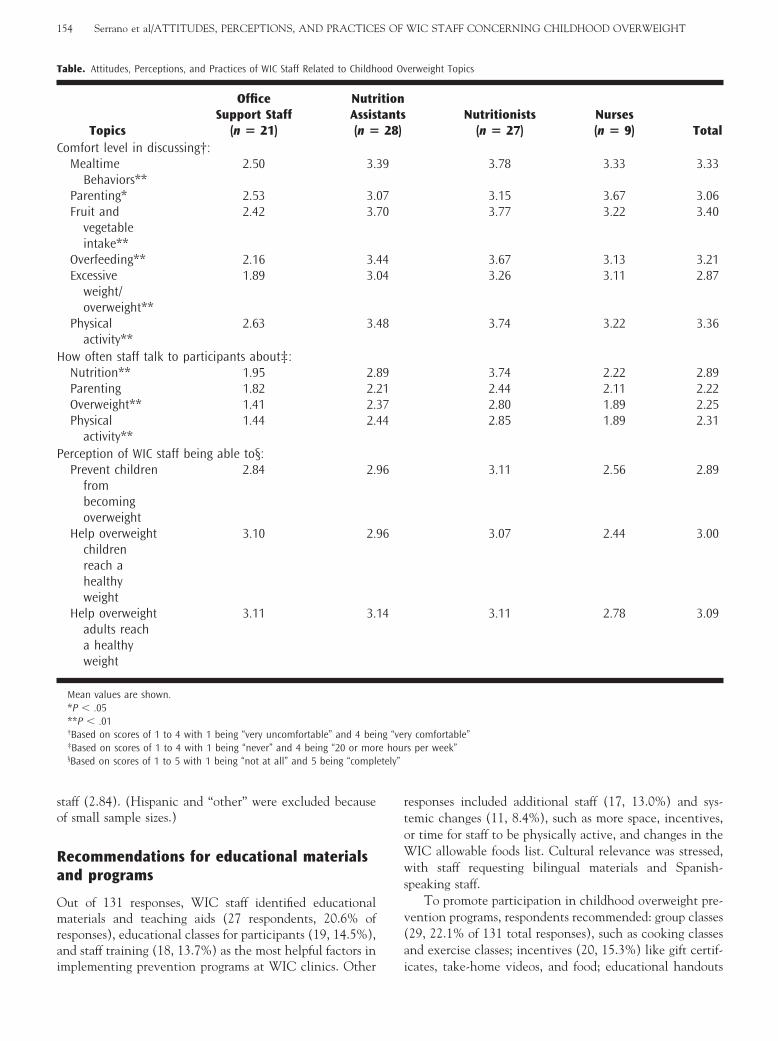
so
Ra
Omrai
rtoWws
v(a
T
C
H
P
etely”
154 Serrano et al/ATTITUDES, PERCEPTIONS, AND PRACTICES OF WIC STAFF CONCERNING CHILDHOOD OVERWEIGHT
taff (2.84). (Hispanic and “other” were excluded becausef small sample sizes.)
ecommendations for educational materialsnd programs
ut of 131 responses, WIC staff identified educationalaterials and teaching aids (27 respondents, 20.6% of
esponses), educational classes for participants (19, 14.5%),nd staff training (18, 13.7%) as the most helpful factors in
able. Attitudes, Perceptions, and Practices of WIC Staff Related to Childh
Topics
OfficeSupport Staff
(n � 21)
NutrAssis(n �
omfort level in discussing†:Mealtime
Behaviors**2.50 3.3
Parenting* 2.53 3.0Fruit and
vegetableintake**
2.42 3.7
Overfeeding** 2.16 3.4Excessive
weight/overweight**
1.89 3.0
Physicalactivity**
2.63 3.4
ow often staff talk to participants about‡:Nutrition** 1.95 2.8Parenting 1.82 2.2Overweight** 1.41 2.3Physical
activity**1.44 2.4
erception of WIC staff being able to§:Prevent children
frombecomingoverweight
2.84 2.9
Help overweightchildrenreach ahealthyweight
3.10 2.9
Help overweightadults reacha healthyweight
3.11 3.1
Mean values are shown.*P � .05**P � .01†Based on scores of 1 to 4 with 1 being “very uncomfortable” and 4 bei‡Based on scores of 1 to 4 with 1 being “never” and 4 being “20 or mor§Based on scores of 1 to 5 with 1 being “not at all” and 5 being “compl
mplementing prevention programs at WIC clinics. Other i
esponses included additional staff (17, 13.0%) and sys-emic changes (11, 8.4%), such as more space, incentives,r time for staff to be physically active, and changes in theIC allowable foods list. Cultural relevance was stressed,
ith staff requesting bilingual materials and Spanish-peaking staff.
To promote participation in childhood overweight pre-ention programs, respondents recommended: group classes29, 22.1% of 131 total responses), such as cooking classesnd exercise classes; incentives (20, 15.3%) like gift certif-
erweight Topics
Nutritionists(n � 27)
Nurses(n � 9) Total
3.78 3.33 3.33
3.15 3.67 3.063.77 3.22 3.40
3.67 3.13 3.213.26 3.11 2.87
3.74 3.22 3.36
3.74 2.22 2.892.44 2.11 2.222.80 1.89 2.252.85 1.89 2.31
3.11 2.56 2.89
3.07 2.44 3.00
3.11 2.78 3.09
y comfortable”s per week”
ood Ov
itiontants
28)
9
70
44
8
9174
6
6
4
ng “vere hour
cates, take-home videos, and food; educational handouts

(aiwacnt
rmidoc1dsfsod
D
EtvoctaW
sfWsounvrSiitrftu
fioti
toriogtpswadt“hme
lqfia
svntnenafiTaipmmblh
IP
Tcitastrp
Journal of Nutrition Education and Behavior ● Volume 38, Number 3, May/June 2006 155
15, 11.5%); convenient scheduling of classes (10, 7.6%);nd policy changes (8, 6.1%), including mandatory partic-pation in childhood overweight-related classes, follow-upith children beyond infancy, and vouchers for free fruitsnd vegetables. A staff member summarized many of theomments with the response, “Make it easy for them to do,ot a lot of reading, cooking low fat classes, exercising withhem.”
Perceived attitudes of participants (33, 22.6% of 146esponses), including defensiveness and helplessness, wereentioned as the biggest perceived barriers to participation
n childhood overweight prevention programs. One respon-ent stated, “People are offended/defensive when told theyr their children are overweight—attitude about weightontrol is poor.” Transportation (31, 21.2%), time (29,9.9%), cultural issues (14, 9.6%), childcare (7, 4.8%), andifficulty in changing behaviors (5, 3.4%) were also con-idered challenges. Cultural issues primarily referred to dif-erent cultural ideals of size and weight. For example, onetaff member responded, “Many of our participants are fromther countries/cultures and see weight issues veryifferently.”
ISCUSSION
ach month WIC serves more than 7 million people acrosshe country, with WIC staff supplying a multitude of ser-ices to participants.12 In this capacity, the program has thepportunity to impact a large number of families. Withhildhood overweight being a huge public health concern,his study aimed to determine how WIC staff felt towardddressing this growing issue and their attitudes about
IC’s capacity to do so.The main findings from this study were that weight
tatus and job title were significant factors in feeling com-ortable about addressing critical weight-related issues with
IC participants. In some ways, these findings are noturprising. First, nearly 40% of respondents were consideredverweight. It is possible that the overweight staff feltncomfortable about talking about behaviors that they mayot be engaging in, such as eating a diet rich in fruits andegetables and/or being physically active. Without furtheresearch, however, we cannot make a firm conclusion.econd, clear distinctions exist in training and responsibil-
ties, particularly between office support staff and nutrition-sts and nurses. Still, office support staff were included inhe study, because focus group discussions indicated thategardless of title, assigned duties, expectations, or supportrom supervisors, they provided advice in the areas of nu-rition, weight, pregnancy, and child-rearing issues, partic-larly while clients are waiting for their appointments.
Staff development and wellness programs were identi-ed as top priorities for WIC to implement childhoodverweight programs, along with additional staff, space, andime. These options may offer opportunities for staff to
mprove their self-efficacy about certain topics, improve sheir body image, and even increase access to educationalpportunities to prevent childhood overweight. In Iowa,esearchers examined staff perspectives on providing smok-ng cessation interventions and found that training was onef the main factors influencing the availability of pro-rams.13 Although substantial resources are required to dohis, a recent study assessed the impact of a breastfeedingromotion program on staff and found that a comprehen-ive intervention, including clinic environment projects,as successful in impacting their overall knowledge, skills,ttitudes, and practices.14 Additionally, a walking programesigned to improve the self-efficacy of WIC staff foundhat intervention site staff were more likely to report asupportive” workplace environment related to makingealthy food choices and being physically active, not toention feeling more comfortable encouraging WIC cli-
nts to engage in physical activity with their children.15
Cultural issues were also identified as growing chal-enges among our study participants, with numerous re-uests for bilingual materials and staff. Several studies haveound that using culturally relevant materials and staff canmprove knowledge and dietary quality of limited resourcesnd WIC audiences.16,17
Several limitations existed with this study. First, theample was not a randomly selected, population-based sur-ey of all health districts in the state, but rather a conve-ience sample that included all regions of the state. Al-hough the response rate was 72.1%, the findings are notecessarily representative of all WIC staff in Virginia orlsewhere. There were also limitations with the question-aire itself. First, it was not tested for concurrent validity,lthough the questions were formed based on focus groupndings with the target audience and found to be reliable.here were no questions included to investigate knowledgebout childhood overweight or personal dietary and phys-cal activity behaviors that might influence their teachingractices. In a clinic setting, given the actual time a staffember is able to spend with each participant, 20 hoursay be difficult to achieve. Finally, BMIs were calculated
ased on self-reported weight and height data, possiblyeading to underestimation of weight and overestimation ofeight.18
MPLICATIONS FOR RESEARCH ANDRACTICE
he results of this study provide valuable feedback abouturrent perceptions and practices of WIC staff on parent-ng, nutrition, and physical activity, as well as insights intohe staff’s self-assessment on the ability of WIC offices toddress childhood or adult overweight. The findings of thistudy suggest the need for health promotion programs andraining among WIC personnel, built upon successful,esearch-based models, in order to provide educational op-ortunities to ensure a strong knowledge base and promote
elf-efficacy about childhood overweight-related topics.
Grstoie(coat
(riiiisf
A
TtNDopmt
R
1
1
1
1
1
1
1
1
1
156 Serrano et al/ATTITUDES, PERCEPTIONS, AND PRACTICES OF WIC STAFF CONCERNING CHILDHOOD OVERWEIGHT
iven the disconnect between perceived and expectedoles, special attention should be given to “front-line” officeupport staff in order to build upon their strengths, contactime, and rapport with clients, yet ensure the disseminationf reliable information. For example, sensitive training top-cs could include: boosting clients’ self-esteem and self-fficacy through positive reinforcement and role-modelingwhich does not require content expertise); responding tolients’ questions (with referrals to WIC printed and/orn-line information and WIC nutritionists and/or nurses);nd working effectively as a team (including the delinea-ion of job responsibilities).
The results also point to the need for the developmentor adaptation) of culturally appropriate educational mate-ials, teaching aids, and handouts for WIC staff and partic-pants. Implementation should take into account logisticalssues of participants and staff. Finally, successful strategies,ncluding systemic and policy changes, for promoting pos-tive, healthy behaviors and healthy weights among WICtaff, and, in turn, among WIC participants should beurther explored and researched.
CKNOWLEDGMENTS
his project was funded primarily with federal funds fromhe U.S. Department of Agriculture (USDA), Food andutrition Service, under a 1999-2001 grant to the Virginiaepartment of Health, Richmond, Virginia. The contentsf this publication do not necessarily reflect the views orolicies of USDA, nor does mention of trade names, com-ercial products, or organizations imply endorsement by
he U.S. government.
EFERENCES
1. Oliveira V, Racine E, Olmsted J, Ghelfi LM. The WIC program:background, trends, and issues. Washington, DC: US Department ofAgriculture; 2002. Food Assistance and Nutrition Research ReportNumber 27.
2. Fox MK, Hamilton W, Lin B-H. Effects of Food Assistance andNutrition Programs on Nutrition and Health: Volume 4, ExecutiveSummary of the Literature. Food Assistance and Nutrition Research
Report No. (FANRR19-4). 2004. Available at: http://www.ers.usda.gov/publications/fanrr19-4/fanrr19-4b.pdf. Accessed April 21,2005.
3. Kowaleski-Jones L, Duncan GJ. Effects of participation in the WICprogram on birthweight: evidence from the National LongitudinalSurvey of Youth. Am J Public Health. 2002;92:799-804.
4. Flegal K, Carroll M, Ogden C, Johnson C. Prevalence and trends inoverweight among US adults, 1999-2000. J Am Med Assoc. 2002;288:1723-1727.
5. Ogden C, Flegal K, Carroll M, Johnson C. Prevalence and trends inoverweight among US children and adolescents, 1999-2000. J AmMed Assoc. 2003;288:1728-1732.
6. Dietz WH. Health consequences of overweight in youth: childhoodpredictors of adult disease. Pediatrics. 1998;101:518-525.
7. US Department of Agriculture, Food and Nutrition Service, Supple-mental Foods Program. WIC Policy Memorandum 98-9, Revision 5,Nutrition Risk Criteria; 2003.
8. US Department of Agriculture, Food and Nutrition Service. WICWorks Sharing Center: Fit WIC. Available at: http://www.nal.usda.gov/wicworks/Sharing_Center/statedev_FIT.html. Ac-cessed April 21, 2005.
9. Centers for Disease Control and Prevention. BMI for adults: bodymass index formula. 2003. Available at: http://www.cdc.gov/nccdphp/dnpa/bmi/bmi-adult-formula.htm. Accessed December 1, 2003.
0. National Institutes of Health. Clinical guidelines on the identifica-tion, evaluation, and treatment of overweight and overweight inadults. Bethesda, MD: National Institutes of Health; 1998. NIHPublication No. 98-4083.
1. Centers for Disease Control and Prevention. BMI—Body Mass Index:BMI for Adults. 2003. Available at: http://www.cdc.gov/nccdphp/dnpa/bmi/bmi-adult.htm. Accessed December 1, 2003.
2. Food and Nutrition Service. Women, Infants, and Children: fre-quently asked questions about WIC. 2003. Available at: http://www.fns.usda.gov/wic/FAQs/FAQ.HTM#3. Accessed April 21, 2005.
3. Aquilino ML, Goody CM, Lowe JB. WIC providers’ perspectives onoffering smoking cessation interventions. MCN Am J Matern ChildNurs. 2003;28:326-332.
4. Khoury AJ, Hinton A, Mitra AK, Carothers C, Foretich C. Improvingbreastfeeding knowledge, attitudes, and practices of WIC clinic staff.Public Health Rep. 2002;117:453-462.
5. Crawford PB, Gosliner W, Strode P, et al. Walking the talk: Fit WICwellness programs improve self-efficacy in pediatric obesity preventioncounseling. Am J Pub Health. 2004;94:1480-1485.
6. Ikeda JP, Pham L, Nguyen KP, Mitchell RA. Culturally relevantnutrition education improves dietary quality among WIC-eligibleVietnamese immigrants. J Nutr Educ Behav. 2002;34:151-158.
7. Taylor T, Serrano E, Anderson J, Kendall P. Knowledge, skills, andbehavior improvements of peer educators and low income Hispanicparticipants after a Stage of Change-based bilingual nutrition educa-tion program. J Commun Health. 2000;25:241-262.
8. Nawaz H, Chan W, Abdulrahman M, Larson D, Katz DL. Self-reported weight and height: implications for obesity research. Am J
Prev Med. 2001;20:294-298.




























