Embed Size (px)
Citation preview

Kidney International, Vol. 7 (1975), p. 111-122
Focal glomerular sclerosis in nephrotic patients:An electron microscopic study of glomerular podocytes
EDITH GRISHMAN and JACOB CHURG
Division of Renal Pathology, Department of Pathology, Mount Sinai School of Medicine of the City University of New York,New York
Focal glomerular sclerosis in nephrotic patients: An electronmicroscopic study of glomerular podocytes. Renal biopsy speci-mens of 16 adult patients with nephrotic syndrome and focalglomerular sclerosis were examined by light and electron micro-scopy. Particular attention was paid to alterations of podocytes.Except for loss of foot processes, five patients had no podocytechanges, five had mild changes and six had severe changes. Ofthe last group (group III), four patients were heroin addicts, thefifth had infectious mononucleosis and the sixth, an apparentidiopathic disease; five patients were males, 16 to 25 yr old.Podocyte changes consisted of cytoplasmic degeneration, de-tachment of epithelial cells from basement membranes, with fill-ing of resulting space by cell debris and new membranes. Under-lying capillaries were often collapsed. Repeat biopsies in threepatients in group III revealed progression of lesions, parallelingrapid clinical deterioration. It is concluded that some cases offocal glomerular sclerosis are associated with severe damage topodocytes which may be caused by drugs, infection or unknownfactors and may contribute to the development and progressionof the glomerular lesions.
Sclérose glomerulaire focale chez les malades atteints de syn-drome néphrotique. Les biopsies rénales de 16 malades adultesatteints de syndrome nephrotique et de lesions de scléroseglomerula ire focale ont été examinée en microscopie photoniqueet electronique. Les alterations des podocytes ont été plus parti-culièrement étudiées. Mis a part Ia disparition des processuspédiculés, ii n'y avait pas de modifications des podocytes chezcinq malades, des moditIcations minimes ont été observées chezcinq autres malades et des alterations sévères chez les six derniers.Dans ce dernier groupe (groupe III) quatre malades étaient deshabitués de l'héroine, le 5e avait une mononucléose infectieuseet le 6e une affection d'apparence idiopathique; cinq maladesétaient de sexe masculin et ages de 16 a 25 ans. Les modificationsdes podocytes consistent en une degénerescence cytoplasmiqueet un éloignement des cellules épithéliales par rapport aux mem-branes basales. L'espace ainsi créé est rempli par des debriscellulaires et de nouvelles membranes. Les capillaires sous-jacents sont souvent en collapsus. Des biopsies itératives cheztrois malades du groupe III ont montré une progression deslesions parallèlement a one détérioration clinique rapide. Onpeut en conclure que quelques cas de sclérose glomérulairefocale sont associés a des lesions sévères des podocytes qui peu-vent être induites par des drogues, des infections ou des facteurs
Received for publication April 29, 1974;and in revised form August 29, 1974,© 1975, by the International Society of Nephrology.
111
inconnus et qui peuvent contribuer a Ia progression des lesionsglomérulaires.
"Focal glomerular sclerosis" (FGS) has beenstudied recently by a number of authors [1—7] whoestablished its main clinical manifestation as protein-uria, usually accompanied by nephrotic syndrome.Histopathologically it is characterized by segmental orfocal glomerular lesions which progress, lead to diffuseglumerular obsolescence and are, in general, not amen-able to therapy.
Electron microscopic studies of FGS have shownelectron dense deposits [8], thickening of basementmembranes and mesangial matrix [9] and fine fila-mentous, matrix-like material in the periphery of thecapillary loop [10]. It is generally accepted that loss offoot processes is present in all glomeruli and that, inthe stricter sense, the lesion represents a diffuse glomer-ular disease.
By immunofluorescence, granular or globular de-posits of 1gM and C3 and to a lesser extent IgG and C4have been demonstrated within the segmental lesions[8, 11].
The etiology and pathogenesis of this disease arestill poorly understood. Hyman and Burkholder [8]suggested that it is a generalized renal disorder "re-sulting from combined injury to the entire nephronand vessels with progressive secondary metabolic andischemic alteration in glomeruli, tubules and interstit-ium." Other authors have suggested immunologicmechanisms.
Since none of these theories appear satisfactory,this study was undertaken in an attempt to furtherelucidate the pathogenesis of this disease in adultpatients and particularly its ultrastructural develop-ment. Having observed podocyte changes in somepatients with focal glomerular sclerosis resembling

112 Grishman/Churg
those of experimental radiation nephritis [12], parti-cular attention was paid to the ultrastructural altera-tions of visceral epithelium. We found a considerablevariety of such changes, and shall attempt to correlatethese structural lesions with the clinical course.
Methods
Renal biopsy specimens were obtained from 16patients over the age of 16 yr who had nephrotic syn-drome and focal, segmental lesions on light micro-scopy. Altogether, 21 biopsy specimens were availablefor light microscopy and 18 for electron microscopy.The patients selected for this study were those on whomrather complete clinical data were available. Since wewere particularly interested in podocyte changes, theselection of patients may be slightly weighted in thatdirection.
Renal tissue was fixed in neutral buffered formalinfor light microscopy and in osmium tetroxide for elec-tron microscopy. Paraffin sections were cut at 3thickness and stained with hematoxylin-eosin and PASstains. All epoxy resin (Epon)-embedded blocks werecut at 1 thickness and stained with PAS-hematoxylin.Blocks showing focal sclerosis of glomeruli wereselected for electron microscopy. Sections were cut ona microtome (LKB), double-stained with uranyl ace-tate and lead citrate and examined with an electronmicroscope (RCA III G).
Results
The patients are tabulated in order of severity ofpodocyte changes on electron microscopy of renal biop-sy specimens and are divided into three groups.Except for various degrees of foot process loss, group I(patients 1 through 5) showed no significant glomer-ular epithelial cell changes; group II (patients 6through 10) had mild epithelial cell changes andgroup III (patients 11 through 16) showed the mostsevere podocyte alterations.
Clinical data. The important clinical data are tabu-lated in Table 1. All patients had nephrotic syndromeat the time of first biopsy. Male patients predominatedin all three groups. The patients varied in age from 16to 60 yr; the average age was 38 yr in group 1, 33 yr ingroup II and 25 yr in group III. The duration of thedisease, measured from the first clinical appearance ofproteinuria and/or the nephrotic syndrome to thetime of biopsy, varied from one week to 30 yr. Forgroup I the average duration was five years; forgroup II, nine years; and for group III, five weeks.Three patients (one in each group) had antecedenthypertension. At the time of biopsy, ten patients werehypertensive (defined as diastolic blood pressure above90 mm Hg), about equally distributed in all groups.Two patients had diabetes mellitus. There were fiveheroin addicts, one in group I and four in group III.One individual in group III (patient 16) had signs andsymptoms of infectious mononucleosis two weeks be-
Group PatientNo.
Age,yr
Sex Race Durationof
disease
Bloodpressure,mm Hg
Drugs Precedinginfection
Blood ureanitrogen,mg/100 ml
Steroidresponse
I 1 35 M W 11 yr 190/110 0 0 30—46 02 48 M W 8yr 170/110 0 0 27 —3 60 M W 1 yr 150/90 0 0 23 +4 16 M N lOmo 130/100 +heroin URI NI5 29 M W 3 yr 140/85 0 URI 30 + Recurrence
II 6 35 M Egypt 30 yr 140/100 0 Diphtheria 19 No steroids7 44 M W I mo 160/100 0 0 13 No steroids8 28 M N 1 mo 120/70 + alcohol Tb 10 No steroids9 17 M PR l4yr 120/90 0 0 23 0
10 43 F W 1 yr 135/90 0 0 10 No steroidsITt 11 25 M W 1 mo 145/100 0 0 32—44 0
12 46 F N 2 wk 170/100 + heroin 0 86—62 .—
13 22 M N 3wk 160/120 +heroin 0 1414 25 M N 4mo 125/95 +heroin 0 12 015 18 M N 5 wk 140/70 +heroin 0 15 +Recurrence16 16 M N 1 wk 124/70 0 Infectious
mononucleosis17 0
aPRpuerto Rican; URI=upper respiratory tract infection; Tb=tuberculosis; NS=nephrotic syndrome; FBS=fasting blood sugar;Rx INH=treatment with isonicotinic acid hydrazide; NI=normal; —=no information; 0=no or negative; + =yes or positive;
weakly positive.
Table 1. Clinical data in 16

Nephrotic syndrome and podocyte degeneration 113
fore onset of edema and weight gain. Allergies werenoted in only one patient of each group.
Two individuals of group II (patients 6 and 9) hadlong-standing nephrotic syndrome, 14 and 30 yr re-spectively, dating back to childhood. It is possible thatthese patients originally had lipoid nephrosis (minimalchange disease), although no biopsy specimens of theearly stages are available.
Both female patients developed their first symptomsduring pregnancy.
Laboratory data. Laboratory data disclosed severeproteinuria in all patients. Only one patient had grosshematuria; the others showed very rare red blood cells(RBC's) on microscopic examination of the urine.Renal function, as measured by blood urea nitrogen(BUN) concentration, was normal in 12 and slightlyimpaired in 4, at time of first biopsy.
Therapy. Ten patients received steroid therapy, fourhad received no steroids, and in two, the mode oftherapy was not recorded (see Table 1). The standardtherapy consisted of 40 to 60mg of prednisone (according to the patient's weight) daily for eight weeks. Ifthere was a good response during that period, the dosewas reduced to 30 mg/day and gradually tapered. Ifthe patient did not respond and had no evidence ofsteroid toxicity, the therapy was continued for anotherfour weeks before the patient was designated assteroid-resistant (0 response—patients 1, 9, 11, 14, 16).Satisfactory response (+ response) was manifested by
cases of focal sclerosis
a decrease of proteinuria to less than 0.5 g/24 hr anddisappearance of edema. Patient 3 responded in twoweeks; patient 5 was treated elsewhere for the initialattack of nephrotic syndrome and was not receivingsteroids when readmitted with recurrence; patient 15was treated at home and responded in eight weeks; hewas asymptomatic and not receiving steroids for ap-proximately four months before recurrence developed.Slight response (± response) was defined as a signi-ficant decrease of prOteinuria (to less than one-half ofthe original value) with a decrease of edema. This wasobserved in patient 4 after six weeks of therapy and inpatient 13 after four weeks. The urine of neither be-came protein-free despite continued steroid admini-stration.
Follow-up data. Eleven patients were followed fromfive months to four years.
Of the ten patients in groups I and 11, one died inrenal failure after four years, one patient died withnephrotic syndrome and early renal failure 11 monthsafter biopsy, four continue to have proteinuria at10 months to two years, and one is clinically well.Four patients could not be traced.
Of the six patients in group III, two are in terminalrenal failure and receiving dialysis, two had early renalfailure at last observation, ten months and one yearafter biopsy, and one patient continued to haveproteinuria. One patient was not available for follow-up.
Follow-up Remarks
Time Renal status
6 yr——
21 mo
2 yr1 yr—
2 yr2 yr
10 mo—
2 yr1 yr3.3 yr5 mo
Died in renal failure——
BUN 11, 4+proteinuria—
AsymptomaticBUN 38, NS
—BUN 13, 2.5g proteinuriaWell, no proteinuriaNS, creatinine 2.8
—
Renal failureBUN 39, NSRenal failureProteinuria
Diabetes and hypertension, 6 yr; proteinuria for 1 yrKnown hypertensive. Proteinuria, 8 yr; NS, 2 moNS for 1 yr; mild diabetes mellitus; FBS, 154; allergy to aspirinHeroin addict. Sore throat 1 wk before cola-colored urineNS for 3 yr; URI at onsetChildhood nephrosis, multiple episodes, spontaneous remissions4 yr hypertension, 1 mo NSProteinuria, 1 yr; gross hematuria. Pulmonary Tb, Rx INHNS at age 3 yr; well until 1 yr prior to admissionHypertension, edema, proteinuria for I yr, started during pregnancySkin rash after antibiotics, rapidly developing NS, urine protein up to 38 g/24 hrHeroin addict for 20 yr. Developed hypertension and edema 5 yr ago during
pregnancy
Died 1 yr after biopsy (overdose of heroin)
Infectious mononucleosis 2 wk prior to NS

114 Grishman/Churg
Ten patients were treated with steroids. One of themresponded to treatment, two had a slight response,while two others responded at first and then had re-currences of nephrotic syndrome. Five patients showedno response to steroid therapy.
Histology. The histologic changes are tabulated in
Tables 2 and 3. On light microscopy (Table 2) thehistologic appearance was quite variable in all threegroups, showing focal or segmental glomerular lesionsor both in different stages of development.
The segmental lesions were characterized by an in-crease of mesangial matrix in some lobules, capillary
Table 2. Light microscopic findings in 16 cases of focal scierosisa
Group Patient Time Glom Obsolete Glomwith Mesang Hyalin Epith Tub Interstitial tissue Arterio-No. interval N glom, N segm scler, prolif prolif atr arteriolo-
of N Fibrosis & Acute sclerosisbiopsies chr inflam infiam
I 1 11 7 1 2+ 1+ 0 1+Ia 2yr 32 18 3 2+ 0 2+ 2+ 0 3+2 6 2 1 0 0 0 2+ 2+ 0 2+3 20 0 4 0 0 1+ 1+ 04 13 0 1 0 0 0 1+ 0 05 16 0 1 1+ 0 1+ 0 1+
II 6 20 2 1 0 1+ 0 0 3+7 13 1 3 0 1+ 1+ 1+ 0 1+8 8 1 1 1+ 2+ 1—2+ 1+ 0 09 9 7 1 0 0 1+ 2—3+ 2+ 0 010 2 0 1 0 0 1+ 1+ 0 0 2—3+
III 11 12 0 4 1+ 0 1+ 1+ 0 012 21 5 5 1+ 1+ 3+ 3+ 3+ 3+13 40 1 7 0 2+ 2+ 2+ 2+ 0
13a 2yr 6 4 0 0 1+ 1+ 3+ 3+ 0 0
14 11 0 5 1+ 0 1+ 1—2+ 1—2+ 2+ 014a lyr 14 6 0 1+ 1+ 0 2+ 2+ 0 015 1 0 0 0 0 0 1+ 0 015a 2wk 13 2 2 1—2+ 0 2+ 2+ 2+ 0 0
15b 8mo 9 4 1 1+ 0 0 2+ 2+ 0 016 11 0 7 0 0 1—2+ 0 1+ 0
aGlom =glomeruli; segm scier = segmental sclerosis; mesang prolif= mesangial proliferation; Epith = epithelial; Tub atr = tubular atrophy;Infiam=infiammation; 0=absent; —3+ =rdegrees of change.
Table 3. Electron microscopic findings in 16 cases of focal scierosisa
Podocytes Mesangium Basement membraneGroup Patient
No. FP loss Degenera- Separa- Cell Matrix Deposits Widening of Gaps Othertion tion prolif increase Lam Rara mt
I 1 — — — — — — —Ia 1+ 0 0 1+ 1+ 1+ 0 0 1±split2 1—2+ 0 0 1—2+ 0 1+ l+split3 3+ 0 0 1—2+ 1+ 0 0 0 04 1+ 0 0 0 0 05 2—3+ 0 0 1+ 1+ 1+ 0 0
II 6 2—3+ 1+ 1+ 1+ 1+ 0 1+ 0 07 3+ 1+ 0 0 2+ 0 Mottled8 0 1+ 0 0 0 1+ 0 l+split9 1+ 2+ 0 1+ 1+ 1+ 1+ 1+ 0
10 0 0 1+ 0 0 2+ 0 Thickened 1+III 11 3+ 3+ 1+ 1+ 1+ 0 1+ 0 0
12 3+ 1+ 2+ 1+ 1+ 0 1+ 0 Thickened 1+13 3+ 2+ 3+ 0 0 0 1+ 0 Wrinkling 2+13a — — — — — — — — —14 2+ 3+ 3+ 1—2+ 1—2+ 1+ 0 0 0I4a 3+ 3+ 2+ 1—2+ 1+ 3+ 0 0 015 3+ 0 2+ 2+ 1+ 0 1+ 0 0ISa 3+ 1+ 2+ 2+ 2+ 0 1+ 0 015b — — — — — —16 3+ 2+ 2+ 0 1+ 0 1+ 0 0
a Prolif=proliferation; FP= foot process; Lam = lamina; —=no information; 0 = absent; =3+ =degree of change.
IVephrof ic syndrome and podocyte degeneration 115
collapse and occasional hyaline or lipid deposits in thecapillaries.
Two individuals of group I (patients 4 and 5) hadvery mild changes: the glomeruli were almost normal,but a few tubules showed mild atrophy. At the otherextreme were four patients (1, 2, 9 and 12) with veryadvanced lesions. They showed between 25 and 70%obsolete glomeruli, segmental collapse and deposit ofhyalin in other glomeruli, marked interstitial fibrosisand tubular atrophy and, usually, severe arterio- andarteriolosclerosis. The remaining ten patients fell be-tween these two extremes with up to 15% obsoleteglomeruli and moderate interstitial and tubular changeson biopsy.
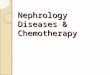
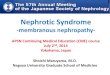
In general, the glomerular lesions in group 111 ap-peared more active, with some lobules showing swell-ing, vacuolization and slight proliferation of visceralepithelial cells (Figs. 1 and 2); segmental widening;slight to moderate cellular proliferation of the mes-angium; and collapse of capillaries (Fig. 3). In fourpatients of group III there was also active interstitialinflammation with polymorphonuclear leukocytic in-filtration encroaching upon the tubules (Fig. 4). Thislast group had very few vascular changes. Four indi-viduals had more than one renal biopsy (patients 1 and13 through 15). Except for patient 1, biopsy specimensshowed progression of the lesions on light microscopy,
Fig. 2. Patient 1/: High power photomicrograph of segmentallesion of Fig. 1. Note swelling, vacuolizat ion and granularity ofpodocytes (PAS stain, x 1,400).
especially in the percentage of obsolete glomeruli andthe degree of tubular atrophy.
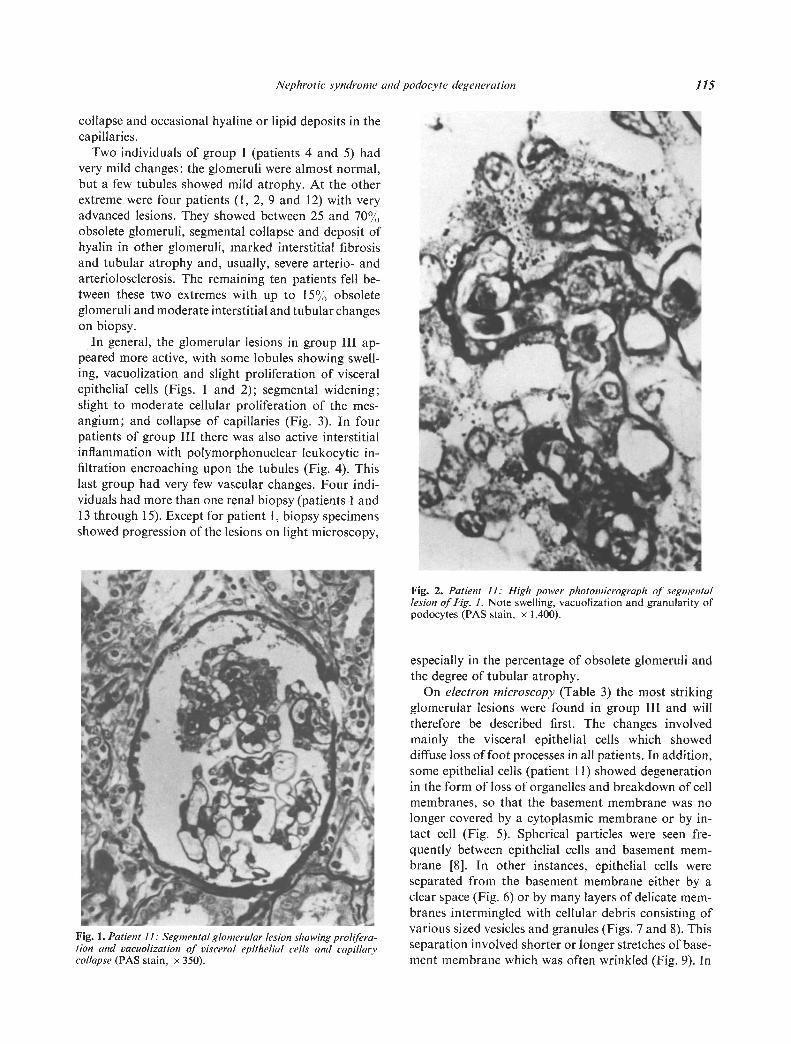
On electron microscopy (Table 3) the most strikingglomerular lesions were found in group III and willtherefore be described first. The changes involvedmainly the visceral epithelial cells which showeddiffuse loss of foot processes in all patients. In addition,some epithelial cells (patient 11) showed degenerationin the form of loss of organelles and breakdown of cellmembranes, so that the basement membrane was nolonger covered by a cytoplasmic membrane or by in-tact cell (Fig. 5). Spherical particles were seen fre-quently between epithelial cells and basement mem-brane [8]. In other instances, epithelial cells wereseparated from the basement membrane either by aclear space (Fig. 6) or by many layers of delicate mem-branes intermingled with cellular debris consisting ofvarious sized vesicles and granules (Figs. 7 and 8). This
Fig. 1. Patient II: Segmental glomerular lesion showing prolifera- .
tion and vacuolization of visceral epithelial cells and capillary separation involved shorter or longer stretches of base-collapse (PAS stain, x 350). ment membrane which was often wrinkled (Fig. 9). In
I

116 Grfshman/Churg
Fig. 3. Patient 14: Segmental glomerular lesion showing inesangialsclerosis and hyperplasia of epithelial cells (PAS stain, x 350).
Fig. 4. Patient 16: Segmental glomerular lesion and acute inter-stitial inflammation (PAS stain, x 600).
Fig. 5. Patient 11: Glomerular capillary wall showing fragmentation ofpodocyte (FP). I. = capillary lumen (x 15,250).
•
- - -. - r :gS a .? -
:1..
I
4-V.'
'I.
4
118 Grishman/Churg
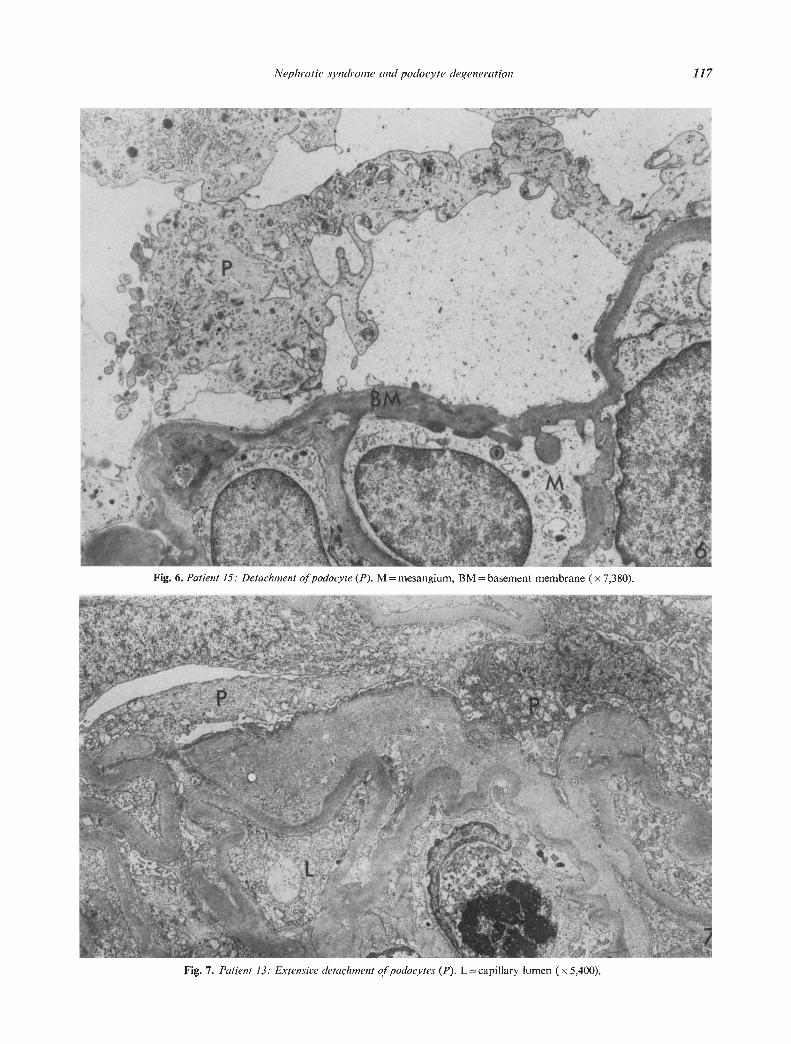
Fig. 8. Patient 13: Detachment of podocyte (P). Space filled with cell debris. Note newly formed thin basement membrane (arrow). (Thisis higher power of Fig. 7.) BM=capillary basement membrane (x21,250).
one patient crystalloids were present in the epithelialcells (Figs. 10 and 11). They were composed of parallelfibrils, measuring about boA in width, separated bya row of small granules, measuring 170 to l9OA indiameter. Lipid droplets were frequently found inepithelial cells.
The five patients of group 11 also showed changes ofpodocytes, but in a much milder degree. There wasfocal degeneration of the cytoplasm with breakdownof cell membranes. Spherical particles were occasion-ally present between basement membrane and epithe-hal cells and in two instances there were breaks inbasement membranes. Detachment of epithelial cellswas only slight and focal. The five patients in group Ihad no degeneration of epithelial cells except for occa-sional lipid droplets and epithelial separation inobsolete glomeruli.
In general, there were only mild degrees of mesangial
cell and matrix proliferation. Only two patients ofgroup III showed moderate focal increase of mesangialcells. One patient (14) showed distinct electron densedeposits in mesangial areas. In others dense depositswere minimal. The basement membrane showed focalwrinkling, mottling and slight thickening. In two biop-sy specimens breaks were observed. The inner outlineof the lamina rara interna was often wavy and, occa-sionally, fine fibrils were seen between the endothehialcells and basement membrane.
Platelets were found four times within capillaries,and myxovirus-like particles were seen in endothelialcells of four other biopsy specimens.
Discussion
All patients presented in this study had severe pro-teinuria with the nephrotic syndrome and a histologic
zJdJ;
c\:-!I.

Nephrotic syndrome and podocyte degeneration 119
Fig. 9. Patient /6: Newly formed membranes (NM) between collapsed capillary and detached podocyte (P) (x 15,250).
Fig. 10. Patient 1/: Crystalloid in podocyte (arrow) (x 21,250).
'ts.
4
:;'• S. 'Ar..,, y'I . •• . %.
_:
'rtt ;i;ee•
'a
- .
... '%): •
10

120 Grishman/Churg
Fig. 11. Patient II: Crystalloid: rows of granules separated by parallel fibrils which are continuous with tonojilaments (arrow) (x 54,000).
picture of focal glomerular sclerosis. However, theyclearly fall into different groups with respect to clinicaland histological findings.
The patients in group III were the youngest in age,included the largest number of heroin addicts and hadthe most severe clinical course with rapidly developingnephrotic syndrome and rapid progression to renalfailure. On light microscopy, the biopsy specimens alsoshowed a more severe disease than those of groups Iand II. This was evidenced by a greater number ofglomeruli with segmental lesions, as well as manyobsolete glomeruli. In addition, there was slightlymore pronounced mesangial and epithelial prolifera-tion (Table 2). In some cases one may even apply theterm "focal glomerulonephritis" which has been usedby some authors for the nephropathy of heroin addicts[14]. Electron microscopic findings corresponded tolight microscopic observations. In addition, there wasa severe degree of podocyte degeneration and detach-ment. One may suppose that the severity of disease hassome relationship to the severity of the podocytedamage, though we can offer no direct evidence thatthis damage is the cause of focal sclerosis. In experi-mental radiation nephritis, detachment of podocytes isaccompanied by capillary collapse, similar to that seenin focal sclerosis; however, in radiation nephritiscapillary endothelium also becomes detached [12].
Podocyte degeneration is not specific for focalglomerular sclerosis. We have seen it in some cases ofsevere mesangio-capillary and extracapillary glomeru-lonephritis. However, in 15 patients with lipoid ne-phrosis (minimal change), no epithelial cell necrosis ordetachment were observed.
An interesting feature of group III is that the renaldisease in nearly all patients appears to be related todrug (heroin) addiction or to infection (infectiousmononucleosis). Renal disease of heroin addicts hasbeen widely discussed lately. Glomerular lesions ofnephrotic addicts vary from minimal [13] to focal pro-liferative glomerulonephritis [14]. Kilcoyne et al [14]found deposits of 1gM and complement in glomeruliand postulated an immune response to drugs, infec-tions or nonspecific contaminants. Eknoyan et al [15]also describe immune-complex deposits in glomeruliof drug addicts with renal disease. However, some of
their patients had bacterial endocarditis or viralhepatitis. Neither of these infections was present in ourpatients. Rao, Nicastri and Friedman [16] observedfocal and segmental glomerular sclerosis in addictswith massive proteinuria. A rather striking finding inall biopsy specimens from heroin addicts was focalacute interstitial inflammation, resembling changesseen in patients with penicillin or methicillin hyper-sensitivity [17].
Renal lesions in infectious mononucleosis were re-ported to consist of patchy interstitial infiltration andtubular degeneration with glomeruli showing onlyminimal changes [18]. This contrasts with the focaland segmental glomerular sclerosis found in our case.
Findings in patients in group II, as well as in onepatient with idiopathic disease in group III, suggestthat a similar process of podocyte degeneration,though usually milder and slower in development,occurs also in at least some patients with focal sclerosisof unknown origin. Recently, Jao et al [19] demon-strated similar, milder lesions in some patients withlipoid nephrosis and mesangial sclerosis and interpre-ted them as basement membrane protrusions.
Of interest are also the crystalloids found in epithe-hal cells of one of our patients. While we have foundno mention in the literature of crystalloids in glomer-ular epithelial cells, very similar structures have beenreported in proximal tubular cells of three species ofmonkeys. They were referred to as "granule-lamellarcomplexes" and interpreted as reorganization of ribo-somes and membranes of the endoplasmic reticulum[20]. Another comparable structure may be theLubarsch crystal in spermatogonia of normal boys andmen which has been shown to possess a similar ultra-structure [211. These structures have been related toactive cell division, a process that may also play a rolein damaged and regenerating podocytes. Measurementof granules and fibrils and continuity of some fibrilswith tonofibrils lead us to believe that the crystalloidsare composed of tonofibrils and ribosomes in anorganized pattern. We recently encountered similarstructures in the podocytes of a patient with lipoidnephrosis.
Two patients in group II showed focal glomerularlesions many years after the onset of childhood ne-
— —.-sd

Nephrotic syndrome and podocyte degeneration /21
phrosis; similar instances have been reported by otherauthors [6, 8, 22]. It has been suggested that there aretwo populations of patients with focal glomerularsclerosis [4]. In one of these, the focal lesions developat the onset of the disease; in the other group theyseem to develop in previously normal kidneys ofpatients with relapsing nephrotic syndrome.
In the two female patients, the disease apparentlybegan during pregnancy. However, one of thesepatients was also a heroin addict, and the glomerularchanges are probably related to this factor.
The frequent occurrence of hypertension in ourpatients is of interest. Of ten hypertensive patients,three developed nephrotic syndrome apparently afterthe onset of hypertension. Frequent occurrence ofhypertension in patients with nephrotic syndrome andfocal glomerulonephritis was also observed byHeptinstall and Joekes [23].
While the size of our sample is too small to drawdefinite conclusions, it appears that a small number ofpatients, especially drug addicts, with nephrotic syn-drome and a severe form of focal glomerular sclerosisfollow a rapidly progressing clinical course. On elec-tron microscopy, the glomeruli of these patients usu-ally show severe podocyte degeneration. The combina-tion of these light and electron microscopic lesions re-suits in a rather characteristic picture and carries apoor prognosis.
Since most of these lesions are observed in a full-blown or late stage, it is not possible at the present timeto evaluate the prognostic significance of early or iso-lated epithelial changes. The fact that epithelial de-generation and detachment are not specific does notnegate the possible etiologic role of epithelial changesin focal sclerosis; they occur in various glomerulardiseases which are characterized by capillary collapseand progression to glomerular obsolescence.
The majority of patients with nephrotic syndromeand focal glomerular sclerosis seem to follow a pro-longed and more benign course and show few epithelialchanges.
It is possible that rapidly progressing focal glomer-ular sclerosis occurring in young drug addicts rep-resents a separate disease entity, which may have anephrotoxic basis. In these patients severe podocytedegeneration may contribute to the development andprogression of the glomerular lesion.
Acknowledgments
This work was supported by Public Health Serviceresearch grant AM-00918 from the National Instituteof Arthritis and Metabolic Diseases. Mr. NormanKatz and Mr. A. Prado provided technical assistance.
Reprint requests to Dr. Jacob Churg, Division of RenalPathology, Department of Pathology, Mount Sinai School ofMedicine, City University of New York, New York City, NewYork 10029, U.S.A.
References
1. GRISI-IMAN E, CHURG J: Pathology of nephrotic syndromewith minimal or minor glomerular changes, in Glomerulo-nephritis, part I, edited by KINcAID-SMITH P, MATHEW TFJ,BECKER EL, New York, John Wiley & Sons, 1973, p. 165
2. CHIJRG J, GRISFIMAN E: Nephrotic syndrome of focalglomerular sclerosis, in Cornell Seminars in Nephrology,edited by BECKER EL, New York, John Wiley & Sons,1973, p. 35
3. CHURG J, HABIB R, WHITE RHR: Pathology of the nephroticsyndrome in children: A report for the International Studyof Kidney Disease in Children. Lancet 1:1299—1302, 1970
4. HABIB R: Focal glomerular sclerosis (editorial). Kidney mt4:355—361, 1973
5. HABIB R,KLEINKNECHT C: The primary nephrotic syndromeof childhood, in Pathology Annual, edited by SOMMER5 SC,NewYork, Appleton-Century-Crofts, 1971, p. 417
6. WHITE RHR, GLASGOW EF, MILLS RJ: Clinicopathologic
study of nephrotic syndrome in childhood. Lancet 1 1353—
1359, 19707. HAYSLETT JP, KRASSNER LS, BENSCH KG, KASHGARIAN M,
EPSTEIN FH: Progression of lipoid nephrosis to renal in-sufficiency. N EnglJ Med 281:181—187, 1969
8. HYMAN LR, BURKHOLDER PM: Focal sclerosing glomerulo-nephropathy with segmental hyalinosis. Lab Invest 28:533—544, 1973
9. NAGI AH, ALEXANDER F, LANNIGAN R: Light and electron-microscopical studies of focal glomerular sclerosis. J C/inPathol 24:846—850, 1971
10. RUMPELTHR, TH0ENE5 W: Focal scierosing glomerulo-pathy (glomerulonephritis)—diffuse process. K/in Woc/,en-schr 50:1143—1146, 1972
11. DRUMMOND KN, MICHAEL AF, GOOD RA, VERNIER RL:The nephrotic syndrome of childhood: Immunologic,clinical and pathologic correlations. J C/in Invest 45:620—630, 1966
12. MADRAZO A, SUZUKI Y, CHURG J: Radiation nephritis:
Acute changes following high dose of radiation. Am JPathol54:507—528, 1969
13. MCGINN T, MCGINN TG, HOFFMAN RS: Nephrotic syn-drome in heroin and cocaine addicts (abstr.). C/in Res 18:699, 1970
14. KILCOYNE MM, DALY JJ, GOCKE DJ, ThoMsoN GE,MELTZER ii, Hsu KC, TANNENBAUM M: Nephrotic syn-drome in heroin addicts. Lancet 1:17—20, 1972
15. EKNOYAN G, GYORKEY F, DICHOSO C, HYDE S, GYORKEY P,SUKI W, MARTINEZ-MALDONADO M: Renal involvement indrug abuse. Arch Intern Med 132:801—806, 1973
16. RAO TKS, NICASTRI AD, FRIEDMAN EA: Natural history ofheroin-associated nephropathy. N EngI J Med 290: 19—23,1974
17. BALDWIN DS, LEVINE B, MCCLUSKEY R, GALLO G: Renalfailure and interstitial nephritis due to penicillin andmethicillin. N EnglJ Med 279:1245—1252, 1968
18. Nephritis in infectious mononucleosis (editorial). Lancet 1:647—648, 1973

122 Grishman/Churg
19. JAO W, POLLAK yE, NORRIS SH, LEWY P. PIRANI CL:Lipoid nephrosis: An approach to the clinicopathologicanalysis and dismemberment of idiopathic nephrotic Syn-drome with minimal glomerular changes. Medicine 52:445—468, 1973
20. BULGER RE: Granulelamellar complex in monkey renalproximal tubular cells. J Ultrastruct Res 24:150—156, 1968
21. SOHVAL AR, SUZUKI Y, GABRILOVE JL, CI-IURG J: Ultra-
structure of crystalloids in spermatogonia and Sertoli cellsof normal human testis. J Ulrrastruct Res 34:83—102,1971
22. MCGOVERN VJ: Persistent nephrotic syndrome: A renalbiopsy study. Aust Ann Med 13:306, 1964
23. HEPTINSTALL RH, JOEKES AM: Focal glomerulonephritis, inCiba Foundation Symposium on Renal Biopsy, edited byWOLSTENHOLME GEW, CAMERON MP, Boston, Little,Brown & Co., 1961









![Dysproteinemias and Glomerular Disease - Loyola Medicine · Patients present with mild renal impairment (median serum creatinine [Scr] of 1.2 mg/dl) and nephrotic-range proteinuria](https://img.pdfslide.net/doc/110x75/5e4a71a71f8eca231e509ca4/dysproteinemias-and-glomerular-disease-loyola-medicine-patients-present-with-mild.jpg)