Embed Size (px)
Citation preview

INFARCT SIZING BY CT/Gray et al.
determination of regional myocardial function in ischemic heartdisease. In Roentgen Video Techniques for Dynamic Studies ofStructure and Function of the Heart and Circulation, edited byHeintzen PH, Bursch JH. Stuttgart, Georg Thieme Verlag,1978, pp 228-234
22. Falsetti HL, Geraci AR, Bunnell IL, Greene DG, Grant C:Estimations of left ventricular volumes and function by one-plane cineangiography in coronary artery disease. (abstr) Cir-culation 39 (suppl III): III-78, 1969
23. Wilson CS, Krueger S, Forker AD, Weaver WF: Correlationbetween segmental early relaxation of the left ventricular walland coronary occlusive disease. Am Heart J 89: 474, 1975
24. Ruttley MS, Adams DF, Cohn PF, Abrams HL: Shape andvolume changes during "isovolumetric relaxation" in normaland asynergic ventricles. Circulation 50: 306, 1974
25. Barry WH, Brooker JZ, Alderman EL, Harrison DC: Changesin diastolic stiffness and tone of the left ventricle during anginapectoris. Circulation 49: 255, 1974
26. Mirsky 1, Cohn PF, Levine JA, Gorlin R, Herman MV,Kreulen TH, Sonnenblick EH: Assessment of left ventricularstiffness in primary myocardial disease and coronary artery dis-ease. Circulation 50: 128, 1974
27. Bristow JD, Van Zee BE, Judkins MP: Systolic and diastolicabnormalities of the left ventricle in coronary artery disease:studies in patients with little or no enlargement of ventricularvolume. Circulation 42: 219, 1970
28. Diamond G, Forrester JS: Effect of coronary artery disease andacute myocardial infarction on left ventricular compliance inman. Circulation 45: 11, 1972
29. Kasparian H, Wiener L: Left ventricular compliance andvolume changes in coronary heart disease (CHD). (abstr) Cir-culation 39 (suppl III): III- 1 19, 1969
30. Amende I, Coltart JD, Krayenbuehl HP, Rutishauser W: Leftventricular contraction and relaxation in patients with coronaryheart disease. Eur J Cardiol 3: 37, 1975
31. Langer GA: Ion fluxes in cardiac excitation and contractionand their relation to myocardial contractility. Physiol Rev 48:708, 1968
32. Lee KS, Ladinsky H, Stuckey JH: Decreased Cal+ uptake bysarcoplasmic reticulum after coronary artery occlusion for 60and 90 minutes. Circ Res 21: 439, 1971
33. Katz AM, Tada M: The "stone heart": A challenge to thebiochemist. (editorial) Am J Cardiol 29: 578, 1972
34. Gibson DG, Prewitt TA, Brown DJ: Analysis of left ven-tricular wall movement during isovolumic relaxation and itsrelation to coronary artery disease. Br Heart J 38: 1010, 1976
35. Upton MT, Gibson DG, Brown DJ: Echocardiographic assess-ment of abnormal left ventricular relaxation in man. Br Heart J38: 1001, 1976
36. Altieri PI, Wilt SM, Leighton RF: Left ventricular wall mo-tion during the isovolumic relaxation period. Circulation 48:499, 1973
Computed Tomography for Localization and Sizingof Experimental Acute Myocardial Infarcts
WILLIAM R. GRAY, M.D., L. MAXIMILIAN BUJA, M.D., HERBERT K. HAGLER, PH.D.,
ROBERT W. PARKEY, M.D., AND JAMES T. WILLERSON, M.D.
SUMIMIARY Computed tomography (CT) has been used to quantitate acute myocardial infarct size in isolated, arrestedcanine hearts. Acute myocardial infarcts were produced in 20 hearts by either left anterior descending (13 dogs) or cir-cumflex coronary artery ligation (seven dogs). Each animal was given iodinated contrast media intravenously immediatelybefore sacrifice 24-72 hours postinfarction. All infarets greater than I g and one of three infarcts 0.5 g or less were detectedhb CT imaging. Infarct volume determined by CT correlated with gross infarct weight (r = 0.83). CT imaging, however,consistently underestimated infarct volume; underestimation was largest in a group of patchy, predominantly subendocardialinfarcts. As adequate equipment and techniques for in vivo studies are developed, CT imaging of the heart may become im-portant in clinical evaluation of myocardial infarction.
BODY COMPUTED TOMOGRAPHY (CT) hasstimulated interest in the possible use of CT in cardiacdiagnosis. Early studies by several groups'4demonstrated the ability of CT to detect experimentalmyocardial ischemia and infarction in vitro. The verysensitive capacity of CT to resolve small differences inx-ray attenuation enables identification of areas ofischemia and infarction. However, it has not been
From the Departments of Radiology, Pathology and InternalMedicine (Cardiac Unit) at the University of Texas SouthwesternMedical School, Dallas, Texas.
Supported in part by NIH Ischemic Heart Disease SCOR GrantH L- 17669.Address for reprints: William R. Gray, Jr., M.D., Department of
Radiology, University of Texas Health Science Center, 5323 HarryHines Boulevard, Dallas, Texas 75235.
Received February 17, 1978; revision accepted May 17, 1978.
clear whether CT is capable of accurate sizing of acutemyocardial infarcts. This in vitro study was performedto assess the potential of CT to identify, localize, andquantitate experimental acute myocardial infarcts inisolated canine hearts and thus to help further es-tablish the potential for CT cardiac imaging in vivo.
Materials and Methods
Twenty adult mongrel dogs weighing 15-25 kg wereevaluated in this study. These animals wereanesthetized with intravenous pentobarbital, in-tubated and ventilated on a Harvard respirator. Theirchests were opened through a left thoracotomy, andeither the proximal left anterior descending coronaryartery (13 dogs) or the circumflex coronary artery(seven dogs) was permanently ligated. Their chestswere closed and the animals were returned to their
497
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
cages. Twenty-four to 72 hours after coronary arteryligation each animal was injected intravenously withheparin (1000 units) and iodinated vascular contrastmedium (methylglucamine iothalamate, 600 mg/kg) 5minutes before sacrifice. The animals then were killedwith an overdose of intravenous pentobarbital. Thechest of each animal was again opened, the greatvessels were ligated, and the heart was removed andsecured in a saline-filled plastic container.The hearts were scanned in the Artronix CT head
scanner which utilizes a pixel size of I X I X 3 mm.The radiographic density scale of the scanner rangesfrom 1024 to +1024 units of attenuation with 0equal to the density of water. Contiguous scans 3 mmthick were made from base to apex. The optimum dis-play factors for visualizing myocardial infarcts weredetermined and remained constant throughout the ex-periment. Scans for these experiments distributed thegrey scale from 38-70 units. An enlargement fromeach scan transparency was made, and the infarct wasoutlined on each 3 mm slice based on visual identifica-tion of density differences between infarcted and non-infarcted myocardium. A 1 cm reference grid wassuperimposed on at least one section from each heart.The area of infarction was determined by sonicplanimetry, and the infarct volumes of the slices weresummed to give an estimate of total infarct volume.
R L
For determination of gross infarct weight, thehearts were sectioned at 1 cm intervals. The heartslices were then incubated in a solution of triphenyltetrazolium chloride.5 The tetrazolium histochemicaltechnique delineates infarcted tissue by intenselystaining normal myocardium.5 Following staining theslices were fixed in formalin. The gross identification,dissection and weighing of the infarcted tissue wereperformed by a cardiac pathologist. With establishedmyocardial infarcts the tetrazolium method has showngood correlation with histological necrosis and tissueenzyme depletion.5 6The infarct volume determined by CT was com-
pared to the gross infarct weight determined by thetetrazolium method and evaluated statistically utiliz-ing a simple linear regression (Pearson's) correlationcoefficient. Gross infarct weight (g) divided by infarctvolume (cm3) determined by CT was calculated to ob-tain estimated infarct density, an evaluation of the ac-curacy of the technique.
ResultsWhen iodinated contrast is given intravenously just
before CT imaging, a myocardial infarct is delineatedas an area of decreased x-ray attenuation due to thelack of contrast medium in the infarct. The ventric-
FIGURE 1. This composite includes several gross slices ofa heart (dog A) with anterior transmural infarctshown with its corresponding computed tomography (CT) images on the right side. The anterior wall is atthe top. The tetrazolium-stained slices delineate normal myocardium as dark gray and infarcted muscle aswhite. On CT scans the ventricular cavity contains the highest concentration of contrast media. The in-farcted area is dark indicating decreased x-ray attenuation from decreased perfusion with iodinated contrastmedia. Orientation accounts for slight differences betwee;, the images and the actual heart slices.
498 CIRCULATION
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from
INFARCT SIZING BY CT/Gray et al.
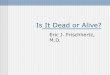
TABLE 1. Myocardial Infarct Sizing by Computerized Tomog-raphy in 20 Dogs
Hours~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~Dog
ABC
D
EF
GH
I
J
KLM
N*0
p
QRS
T
Hourspost-infarct
48
4824
24
24
24
24
24
24
24
24
24
247224
24
24
24
2424
Location
AnteriorAnteriorAnteriorAnteriorAnteriorAnterior
AnteriorAnteriorAnteriorAnteriorAniteriorAnteriorAnteriorPosteriorPosterior
PosteriorPosteriorPosteriorPosteriorPosterior
Involvement
T
SESE
TTT
TT
TT
T
SE
SESET
SET
SESESE
Volumeby CT(cm3)
24.2
0
9.317.622.2
6.3
7.914.1
8.674.3
0
0.5
1.1
16.4
7.4
9.873.49.2
Grossweight
(g)
24.8
0.311.7
27.7
26.2
14.1
11
20.4
18.8
9.87.20.50.5
28.731.726.324
13.2
12.9
17.1*N, the only 72-hour infaret, wxas excluded from the final sizing statistics;
although it was quiiite large, the infarct was extremely patchy.Ahbreviations: CT = computed tomography; SE = patchy, predomi-
nantly subendocardial; T = homogeneous, transmural.
ular cavity is identified as an area of increasedattenuation due to its higher concentration of contrastmedia compared to the ventricular wall (fig. 1).CT readily identified the presence of the experimen-
tal myocardial infarcts in all but the smallest of in-farcts (table 1). Of three infarcts less than 1 g, one in-
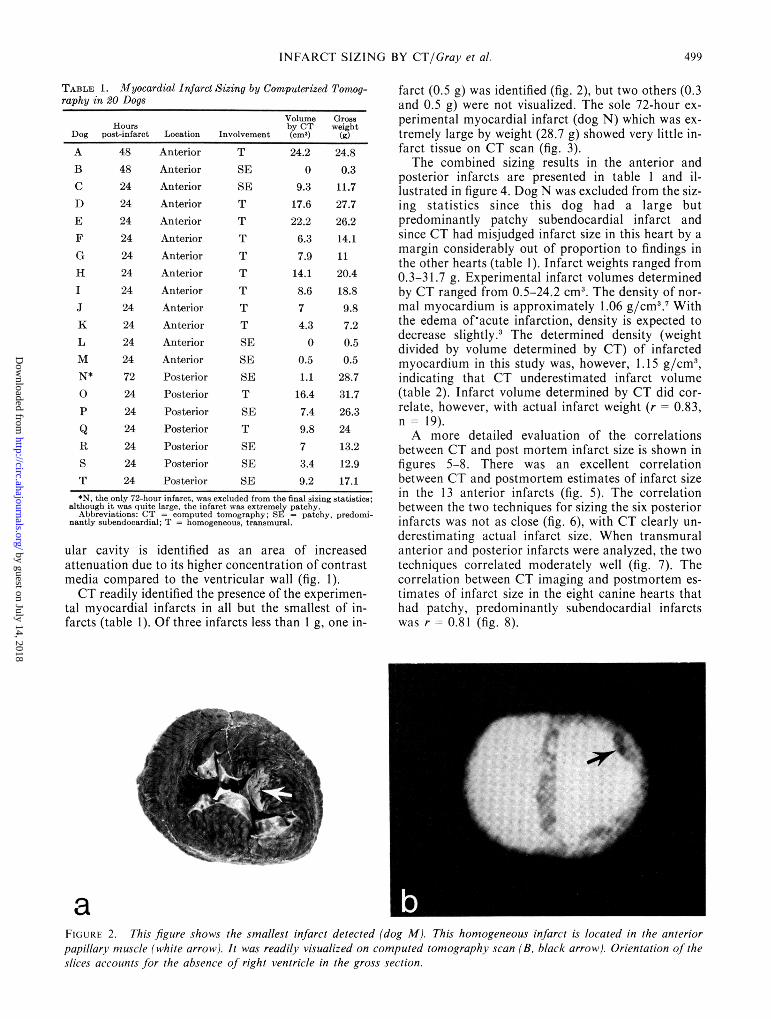
farct (0.5 g) was identified (fig. 2), but two others (0.3and 0.5 g) were not visualized. The sole 72-hour ex-perimental myocardial infarct (dog N) which was ex-tremely large by weight (28.7 g) showed very little in-farct tissue on CT scan (fig. 3).The combined sizing results in the anterior and
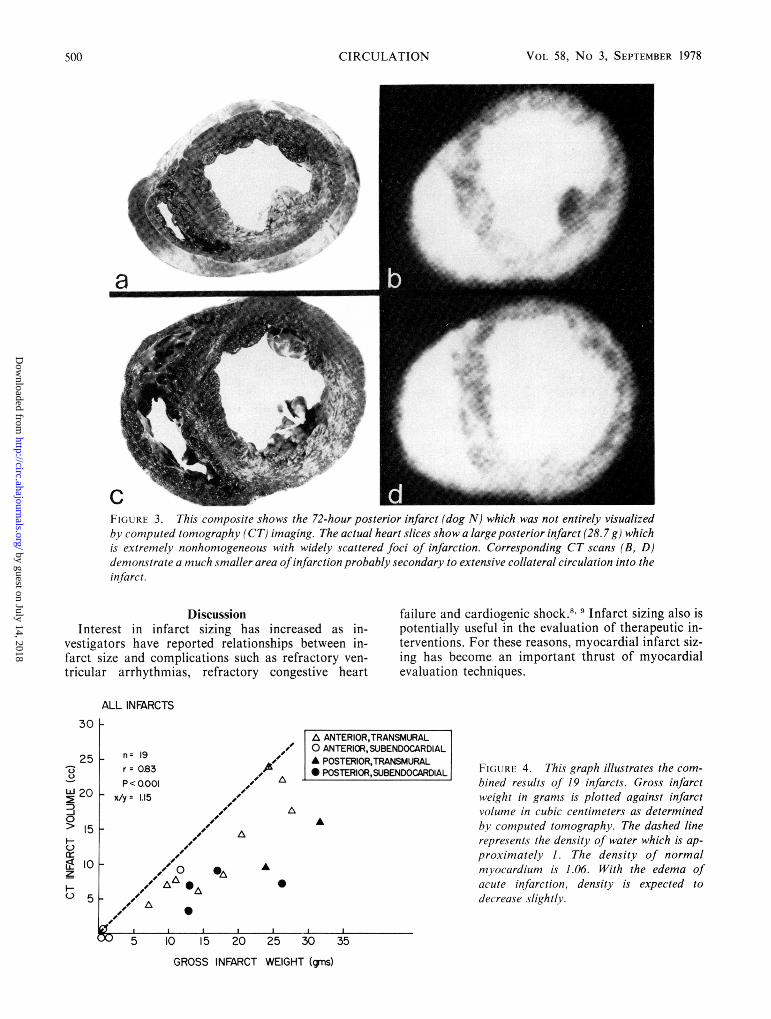
posterior infarcts are presented in table I and il-lustrated in figure 4. Dog N was excluded from the siz-ing statistics since this dog had a large butpredominantly patchy subendocardial infarct andsince CT had misjudged infarct size in this heart by amargin considerably out of proportion to findings inthe other hearts (table 1). Infarct weights ranged from0.3-31.7 g. Experimental infarct volumes determinedby CT ranged from 0.5-24.2 cm3. The density of nor-mal myocardium is approximately 1.06 g/cm3.7 Withthe edema ofhacute infarction, density is expected todecrease slightly.3 The determined density (weightdivided by volume determined by CT) of infarctedmyocardium in this study was, however, 1. 15 g/cm3,indicating that CT underestimated infarct volume(table 2). Infarct volume determined by CT did cor-relate, however, with actual infarct weight (r 0.83,n= 19).A more detailed evaluation of the correlations
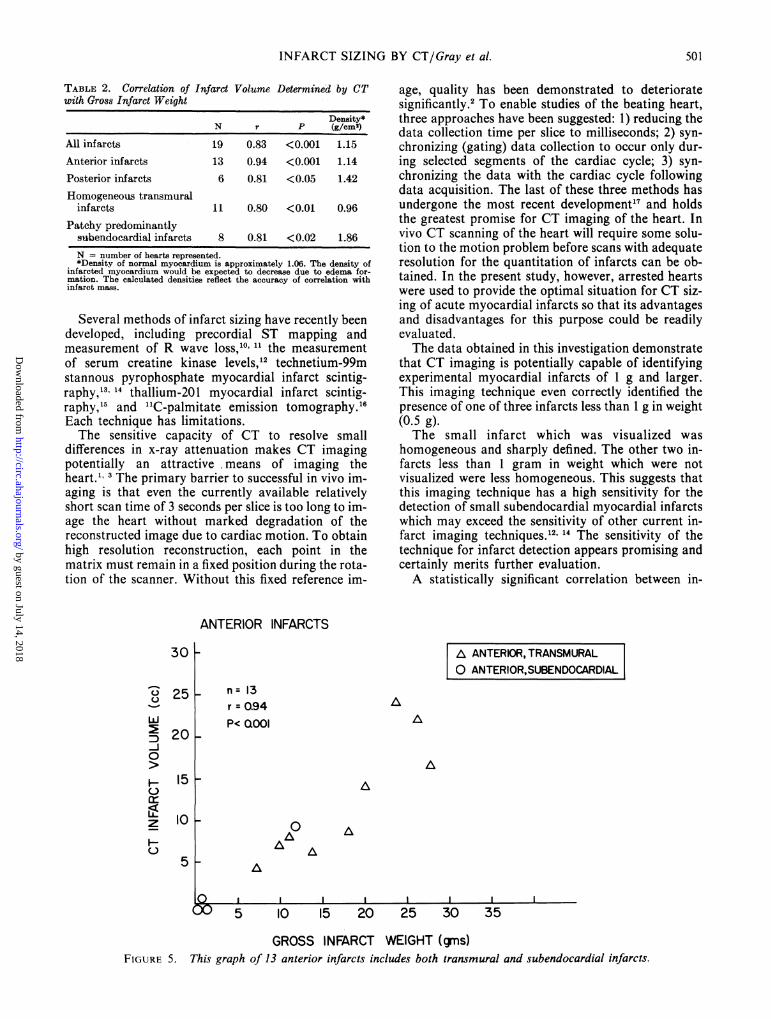
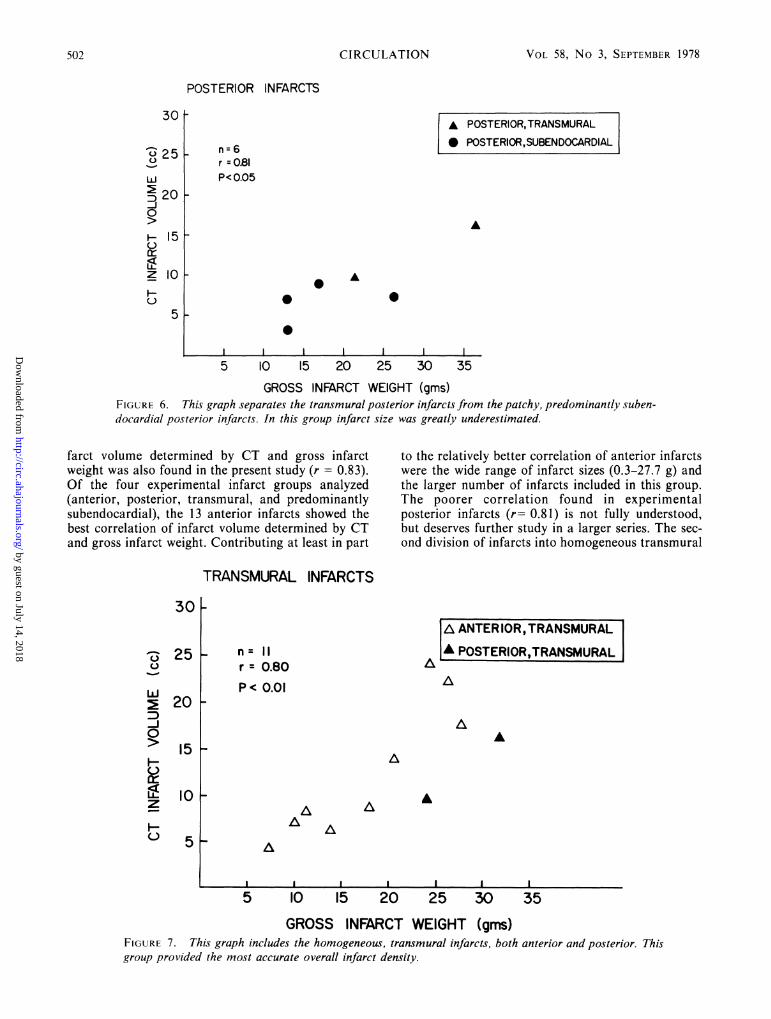
between CT and post mortem infarct size is shown infigures 5-8. There was an excellent correlationbetween CT and postmortem estimates of infarct sizein the 13 anterior infarcts (fig. 5). The correlationbetween the two techniques for sizing the six posteriorinfarcts was not as close (fig. 6), with CT clearly un-derestimating actual infarct size. When transmuralanterior and posterior infarcts were analyzed, the twotechniques correlated moderately well (fig. 7). Thecorrelation between CT imaging and postmortem es-timates of infarct size in the eight canine hearts thathad patchy, predominantly subendocardial infarctswas r 0.81 (fig. 8).
aFiUaRIs 2. This figure shows the smallest infarct detected (dog M). This homogeneous infarct is located in the anteriorpapillariv muscle (white arrow). It was readily visualized on computed tomography scan (B, black arrow). Orientation of'theslices accounts for the absence of right ventricle in the gross section.
---
499
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from
CIRCULATION VOL 58, No 3, SEPTEMBER 1978
a
FIGuR, 3. This composite shows the 72-hour posterior infarct (dog N) which was not entirely visualizedbh computed tomography (CT) imaging. The actual heart slices show a large posterior infarct (28.7 g) whichis extrenmely nonhomogeneous with widely scattered foci of infarction. Corresponding CT scans (B, D)demonvstrate a much smaller area ofinfarction probably secondary to extensive collateral circulation into theinfarct.
DiscussionInterest in infarct sizing has increased as in-
vestigators have reported relationships between in-farct size and complications such as refractory ven-tricular arrhythmias, refractory congestive heart
failure and cardiogenic shock.8 9 Infarct sizing also ispotentially useful in the evaluation of therapeutic in-terventions. For these reasons, myocardial infarct siz-ing has become an important thrust of myocardialevaluation techniques.
ALL INFARCTS
n = 19r = 0.83p < ao.oi
- x/y= 1.15t~~, A
tw A
0~A
II- _---DO 5 10 15 20 25
A ANTERIOR,TRANSMURALO ANTERIOR, SUBENDOCARDIALA POSTERIOR,TRANSMURAL* POSTERIOR,SUBENDOCARDIAL
'A
FIGS RI- 4. This graph illustrates the com-
bined revults of 19 infarcts. Gross infarctweight in grams is plotted against infarctvolume in cubic centimeters as determinedby computed tomography. The dashed linerepresents the density of water which is ap-
proximately 1. The density of normalmyocardium is 1.06. With the edema ofacute infarction, density is expected todecrease slightlv.
30 35
GROSS INFARCT WEIGHT (gms)
500
30
25
0-J0> Is
0> 15
ff 0< 10z
o si
K ----------P---------
4J
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from
INFARCT SIZING BY CT/Gray et al.
Determined by CT
Density*N r P (g/cm2)
All infarcts 19 0.83 <0.001 1.15Anterior infarcts 13 0.94 <0.001 1.14Posterior infarcts 6 0.81 <0.05 1.42Homogeneous transmural
infarcts 11 0.80 <0.01 0.96Patchy predominantly
subendocardial infarcts 8 0.81 <0.02 1.86N = number of hearts represented.*Density of normal myocardium is approximately 1.06. The density of
infarcted myocardium would be expected to decrease due to edema for-mation. The calculated densities reflect the accuracy of correlation withinfarct mass.
Several methods of infarct sizing have recently beendeveloped, including precordial ST mapping andmeasurement of R wave loss,10, 11 the measurementof serum creatine kinase levels,'2 technetium-99mstannous pyrophosphate myocardial infarct scintig-raphy,", 14 thallium-201 myocardial infarct scintig-raphy,"5 and "IC-palmitate emission tomography.l6Each technique has limitations.The sensitive capacity of CT to resolve small
differences in x-ray attenuation makes CT imagingpotentially an attractive means of imaging theheart. ' 3 The primary barrier to successful in vivo im-aging is that even the currently available relativelyshort scan time of 3 seconds per slice is too long to im-age the heart without marked degradation of thereconstructed image due to cardiac motion. To obtainhigh resolution reconstruction, each point in thematrix must remain in a fixed position during the rota-tion of the scanner. Without this fixed reference im-
age, quality has been demonstrated to deterioratesignificantly.2 To enable studies of the beating heart,three approaches have been suggested: 1) reducing thedata collection time per slice to milliseconds; 2) syn-chronizing (gating) data collection to occur only dur-ing selected segments of the cardiac cycle; 3) syn-chronizing the data with the cardiac cycle followingdata acquisition. The last of these three methods hasundergone the most recent development'7 and holdsthe greatest promise for CT imaging of the heart. Invivo CT scanning of the heart will require some solu-tion to the motion problem before scans with adequateresolution for the quantitation of infarcts can be ob-tained. In the present study, however, arrested heartswere used to provide the optimal situation for CT siz-ing of acute myocardial infarcts so that its advantagesand disadvantages for this purpose could be readilyevaluated.The data obtained in this investigation demonstrate
that CT imaging is potentially capable of identifyingexperimental myocardial infarcts of 1 g and larger.This imaging technique even correctly identified thepresence of one of three infarcts less than 1 g in weight(0.5 g).The small infarct which was visualized was
homogeneous and sharply defined. The other two in-farcts less than 1 gram in weight which were notvisualized were less homogeneous. This suggests thatthis imaging technique has a high sensitivity for thedetection of small subendocardial myocardial infarctswhich may exceed the sensitivity of other current in-farct imaging techniques.12' " The sensitivity of thetechnique for infarct detection appears promising andcertainly merits further evaluation.A statistically significant correlation between in-
ANTERIOR INFARCTS
AA
A
A
to AA A
A
I I I I I I
5 10 15 20 25 30 35
GROSS INFARCT WEIGHT (gins)FIGURE 5. This graph of 13 anterior infarcts includes both transmural and subendocardial infarcts.
TABLE 2. Correlation of Infarct Volumewith Gross Infarct Weight
30p
n= 13r = 0.94P< QOOI
A ANTERIOR, TRANSMURAL0 ANTERIOR,SUBENDOCARDIAL
Q0
LI
-J0
LLzH-
25 -
20 k
15 I
10 V
5k
00XInkk..j
501
_nA
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 58, No 3, SEPTEMBER 1978
POSTERIOR INFARCTS
A POSTERIOR,TRANSMURAL* POSTERIOR,SUBENDOCARDIAL
A
A
* 0
5 10 15 20 25 30 35
GROSS INFARCT WEIGHT (gms)FIGURE 6. This graph separates the transmural posterior infarcts from the patchy, predominantly suben-docardial posterior infarcts. In this group infarct size was greatly underestimated.
farct volume determined by CT and gross infarctweight was also found in the present study (r = 0.83).Of the four experimental infarct groups analyzed(anterior, posterior, transmural, and predominantlysubendocardial), the 13 anterior infarcts showed thebest correlation of infarct volume determined by CTand gross infarct weight. Contributing at least in part
to the relatively better correlation of anterior infarctswere the wide range of infarct sizes (0.3-27.7 g) andthe larger number of infarcts included in this group.The poorer correlation found in experimentalposterior infarcts (r= 0.81) is not fully understood,but deserves further study in a larger series. The sec-ond division of infarcts into homogeneous transmural
TRANSMURAL INFARCTS
n= 11r 0.80p< 0.01
AA
AA
A
AA
A A
A
I I I I I I I
5 10 15 20 25 30 35
GROSS INFARCT WEIGHT (gins)FIGURE 7. This graph includes the homogeneous, transmural infarcts, both anterior and posterior. Thisgroup provided the most accurate overall infarct density.
n=6r =021P<0.05
30
0 25
20-J
20
HIS0
15
z 10H
5
I-
30p-
25 V
20
15
I ANTERIOR, TRANSMURALA POSTERIOR,TRANSMURALC)
-J0
I
z
H)
10-
51-
_ _
502 CIRCULATION
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from

INFARCT SIZING BY CT/Gray et al.
SUBENDOCARDIAL INFARCTS
301-
251-
O ANTERIOR, SUBENDOCARDIAL
I* POSTERIOR ,SUBENDOCARDIAL In 8r = 0.81P< 0.02
20-
151-
101- 0 0
50
0
..J 1 l l l 1 1 , I
5 10 15 20 .25 30 35
GROSS INFARCT WEIGHT (gms)FIGURE 8. The graph illustrates the correlation of volume determined by computed tomography in thepatchy, predominantly subendocardial infarcts.
infarcts and patchy, predominantly subendocardial in-farcts did not show improved correlation in eithergroup (r = 0.80 and r = 0.81, respectively). Thegrouping did, however, emphasize a marked differencein CT infarct density (transmurals 0.96 g/cm3 andsubendocardials 1.86 g/cm3), indicating a marked un-derestimation of infarct size in patchy, predominantlysubendocardial infarcts. Calculations of infarct den-sity indicated that the transmural infarcts showed ananticipated decreased density (0.96 g/cm3) associatedwith the edema accompanying acute infarcts com-pared to the density of normal myocardium (1.06g/cm3)3, 7 (table 2). The extreme case of under-estimation occurred with dog N, which had a gross in-farct weight of 28.7 g and a disproportionately smallinfarct volume determined by CT of 1.1 cm3 (table 1).This was the only infarct 72 hours old studied in thepresent series, and its inclusion in the sizing statisticswould have decreased the overall correlationremarkably (r = 0.69). Although this posterior infarctwas the second largest in this series, the infarct was ex-
tremely patchy and predominantly subendocardial.This sizing discrepancy between the CT estimate andinfarct weight seems likely to be related to thepresence of collateral reperfusion of the infarctedarea, as well as the patchy character of the infarct.The perfusion dependence of this CT imaging
technique for quantitative sizing purposes is obvious.Infarcted nonperfused myocardium is easily differen-tiated on CT scans from the surrounding myocardiumwhich is perfused with iodinated contrast medium.The underestimation of infarct volume in this studyseems to be related to collateral flow of contrast into
the infarcted tissue. Patchy infarcts also present someproblem to the technique, since small foci of necrosismay be easily hidden by surrounding normally per-fused myocardium. That this almost certainly oc-curred in the present study is suggested by the markedunderestimation of infarct volume in the patchy,predominantly subendocardial infarcts.
Carlsson and coworkers"8 have recently suggestedthat iodinated contrast media administered intra-venously undergoes three phases of accumulation inregions of myocardial infarction: 1) in the first 5
minutes there is decreased contrast in the infarctrelative to the normal myocardium; 2) in the secondphase there is marked increased accumulation of con-trast ("contrast entrapment") in the infarct relative tothe surrounding normal myocardium; 3) within 45minutes contrast medium in the infarct has washedout. It is possible that improved results could be ob-tained utilizing the second phase of contrast entrap-ment rather than the first phase of decreased contrastwhich was utilized in this study. The data of Carlsson,et al.,18 Powell and associates3 and Higgins, et al.'9also suggest that infarcts may be visualized adequatelywithout iodinated contrast due to the edemaassociated with acute infarction. Underestimation ofinfarct volume, however, may be an inherent problemin these approaches. Additional testing of these ap-proaches will be necessary to allow determination as
to whether contrast medium aids or hinders quantita-tion of infarct size using CT imaging.
In summary, our findings suggest that CT couldrepresent an extremely sensitive technique for myo-cardial infarct detection. CT readily visualized all
C-
C.)O
-J0
H
Ll.z
H
503
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
infarcts greater than 0.5 g in size, and one of threeinfarcts weighing 0.5 g or less was localized and ac-curately sized. CT tended to underestimate infarctvolume, but statistically significant correlation of in-farct volume determined by CT with actual infarctweight was found. It is likely that the under-estimation of infarct volume is due at least partly tothe perfusion dependence of this technique. CT car-diac imaging should allow accurate measurements ofventricular dimensions and be a noninvasive means todetect various regional myocardial abnormalities. Thepractical utilization of this technique now awaits thedevelopment of adequate gating methodology toreduce the detrimental effect of cardiac motion on CTreconstruction. The rapid development of CT imagingsystems for cardiac work is anticipated and certainlywill be the focus of much attention in the immediatefuture.
AcknowledgmentsWe appreciate the technical assistance of Mrs. Dorothy
Gutekunst and Mrs. Katie Wolf. The secretarial assistance of Mrs.Gail Blust and Ms. Mary Rich is also appreciated.
ReferencesI. Adams DF, Hessel SJ, Judy PF, Stein JA, Abrams HL: Com-
puted tomography of the normal and infarcted myocardium.Am J Roentgenol 126: 786, 1976
2. Ter-Pogossian MM, Weiss ES, Coleman RE, Sobel BE: Com-puted tomography of the heart. Am J Roentgenol 127: 79, 1976
3. Powell WJ Jr, Wittenberg J, Maturi RA, Dinsmore RE, MillerSW: Detection of edema associated with myocardial ischemiaby computerized tomography in isolated, arrested caninehearts. Circulation 55: 99, 1977
4. Gray WR Jr, Parkey RW, Buja LM, Stokely EM, McAllisterRT, Bonte FJ, Willerson JT: Computed tomography: in vitroevaluation of myocardial infarction. Radiology 122: 511, 1977
5. Lie JT, Pairolero PC, Holley KE, Titus JL: Microscopicenzyme-mapping verification of large, homogeneous, ex-perimental myocardial infarcts of predictable size and locationin dogs. J Thorac Cardiovasc Surg 69: 599, 1975
6. Vogel WM, Zannoni VG, Abrams GD, Lucchesi BR: Inabilityof methylprednisolone sodium succinate to decrease infarct sizeor preserve enzymatic activity measured 24 hours after cor-onary occlusion in the dog. Circulation 55: 588, 1977
7. Yipintosi T, Scanlon PD, Bassingthwaighte JB: Density andwater content of dog ventricular myocardium. Proc Soc ExperBiol Med 141: 1032, 1972
8. Cox JR Jr, Roberts R, Ambos HD, Oliver GC, Sobel BE:Relations between enzymatically estimated myocardial infarctsize and early ventricular dysrhythmia. Circulation 53 (suppl I):1-150, 1976
9. Page DL, Caulifield JB, Kastor JA, DeSanctis RW, SandersCA: Myocardial changes associated with cardiogenic shock. NEnglJ Med 285: 133, 1971
10. Maroko PR, Libby P, Covell JW, Sobel BE, Ross J Jr,Braunwald E: Precordial ST segment elevation mapping: anatraumatic method for assessing alterations in the extent ofmyocardial ischemic injury. The effects of pharmacologic andhemodynamic interventions. Am J Cardiol 29: 223, 1972
11. Hillis LD, Askenazi J, Braunwald E, Radvany P, Muller JE.Fishbein MC, Maroko PP: Use of changes in epicardial QRScomplex to assess interventions which modify extent of myocar-dial necrosis following-coronary artery occlusion. Circulation54: 591, 1976
12. Shell WE, Kjekshus JK, Sobel BE: Quantitative assessment ofthe extent of myocardial infarction in the conscious dog bymeans of analysis of serial changes in serum creatinephosphokinase activity. J Clin Invest 50: 2614, 1971
13. Stokely EM, Buja LM, Lewis SE, Parkey RW, Bonte FJ,Harris RA Jr, Willerson JT: Measurement of acute myocardialinfarction in dogs with technetium-99m stannouspyrophosphate scintigrams. J Nucl Med 17: 1, 1976
14. Lewis M, Buja LM, Saffer S, Mishelevich D, Stokely EM,Lewis SE, Parkey RW, Bonte FJ, Willerson JT: Experimentalinfarct sizing using computer processing and a three-dimensional model. Science 197: 167, 1977
15. Wackers FJ, Becker AE, Samson G, Sokole EB, vd Schoot JB,Andreas JTM, Lie KI, Durrer D, Wellens H: Location and sizeof acute transmural infarction estimated from thallium201 scin-tiscans: a clinicopathological study. Circulation 56: 72, 1977
16. Weiss ES, Ahmed SA, Welch MJ, Williamson JR, Ter-Pogossian MM, Sobel BE: Quantification of infarction in crosssections of canine myocardium in vivo with positron emissiontransaxial tomography and "IC-palmitate. Circulation 55: 66,1977
17. Harell GS, Guthaner DF, Breiman RS, Morehouse CC, SeppiEJ, Marshall WH Jr, Wexler L: Stop-action cardiac computedtomography. Radiology 123: 515, 1977
18. Carlsson E, Redington RW, Berninger W, Lipton MJ,Dougherty P: Cardiac imaging by computed tomography.Presented at Radiological Society of North America,December 2, 1977
19. Higgins CB, Siemers PT, Schmidt W: Detection, quantitationand contrast enhancement of myocardial infarction utilizingcomputerized axial tomography. Am J Cardiol 41: 361(A),1978
504 CIRCULATION
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from
W R Gray, L M Buja, H K Hagler, R W Parkey and J T Willersoninfarcts.
Computed tomography for localization and sizing of experimental acute myocardial
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1978 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.58.3.497
1978;58:497-504Circulation.
http://circ.ahajournals.org/content/58/3/497the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 14, 2018http://circ.ahajournals.org/
Dow
nloaded from