Embed Size (px)
Citation preview
From Zero to FLS:Implementation & Beyond
National Osteoporosis Society FLS Education Programme
October 2010
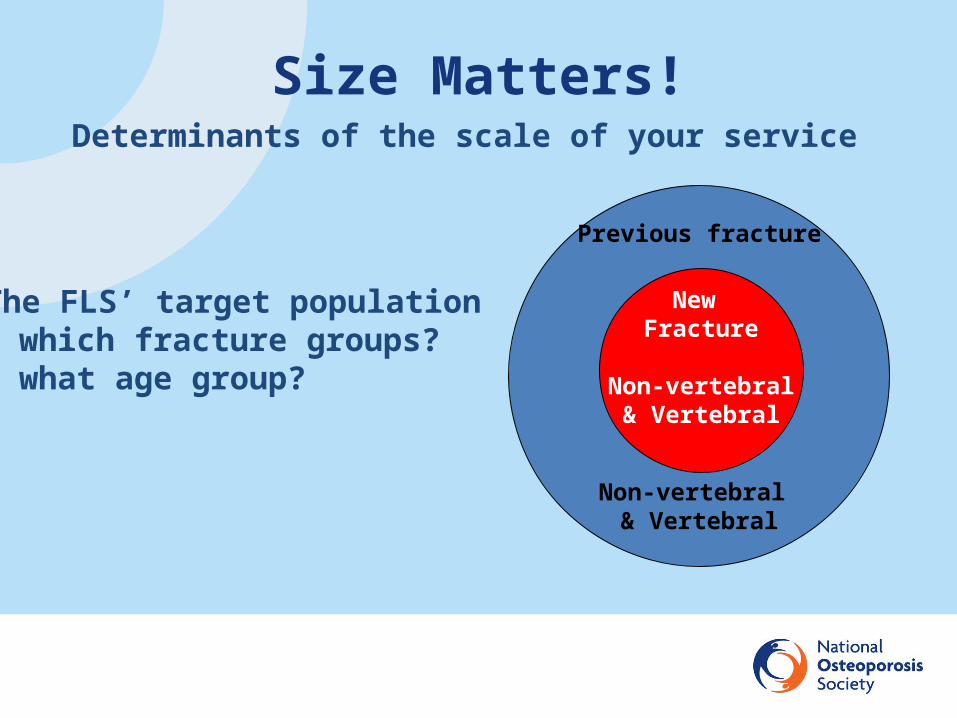
Previous fracture
Non-vertebral & Vertebral
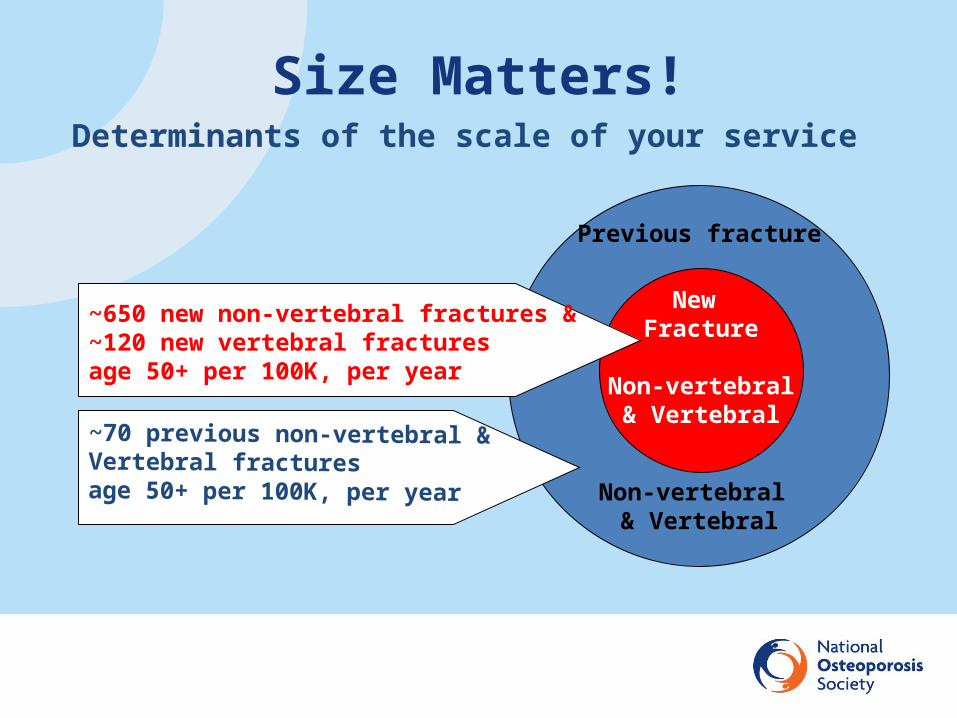
Size Matters!Determinants of the scale of your service
The FLS’ target population- which fracture groups?- what age group?
New Fracture
Non-vertebral& Vertebral
Previous fracture
Non-vertebral & Vertebral
New Fracture
Non-vertebral& Vertebral
Size Matters!Determinants of the scale of your service
~650 new non-vertebral fractures &~120 new vertebral fractures age 50+ per 100K, per year
~70 previous non-vertebral & Vertebral fractures age 50+ per 100K, per year
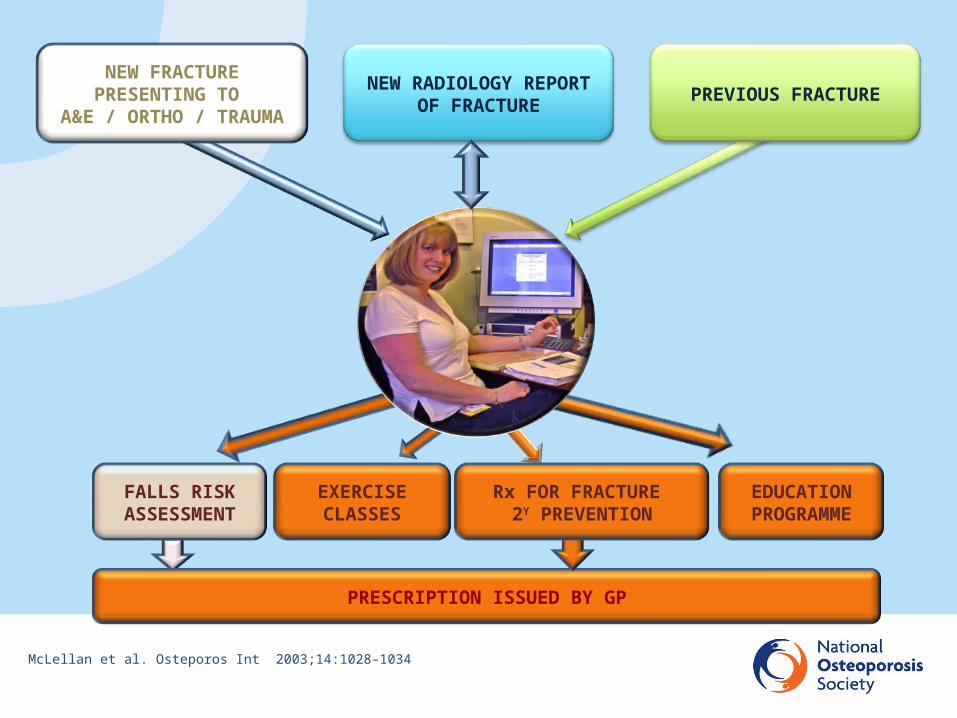
NEW FRACTUREPRESENTING TO
A&E / ORTHO / TRAUMA
EDUCATIONPROGRAMME
EXERCISECLASSES
FALLS RISKASSESSMENT
NEW RADIOLOGY REPORT OF FRACTURE
PRESCRIPTION ISSUED BY GP
Rx FOR FRACTURE 2Y PREVENTION
McLellan et al. Osteporos Int 2003;14:1028–1034
PREVIOUS FRACTURE
From Zero to FLS: Implementation & Beyond
From Zero to FLS: Implementation & BeyondThe first steps
• Appointment of project management team & Chair
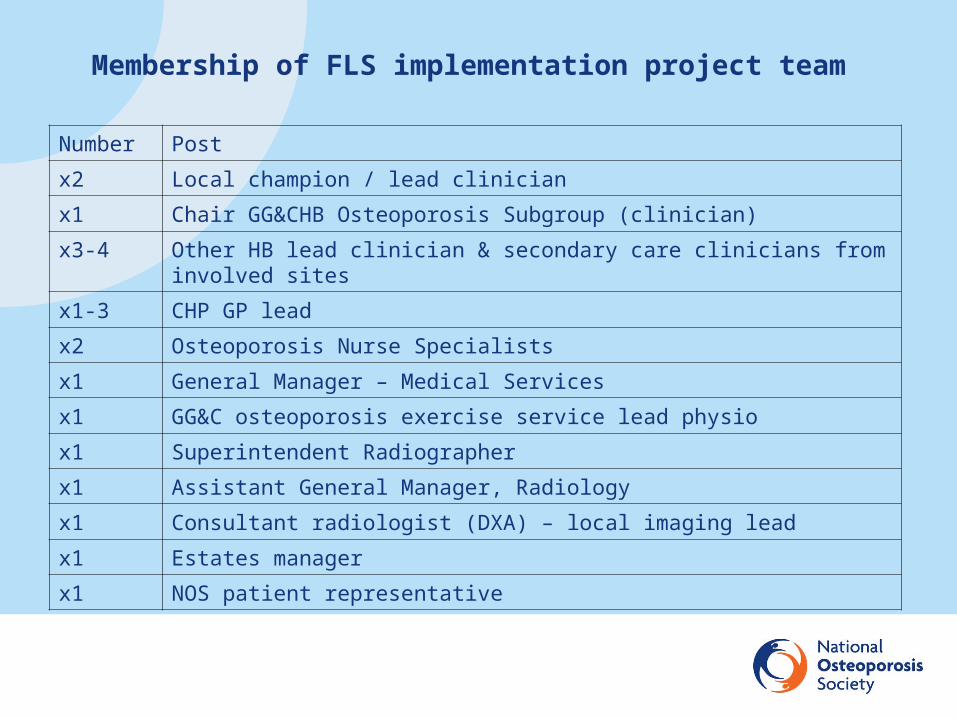
Membership of FLS implementation project team
Number Post
x2 Local champion / lead clinician
x1 Chair GG&CHB Osteoporosis Subgroup (clinician)
x3-4 Other HB lead clinician & secondary care clinicians from involved sites
x1-3 CHP GP lead
x2 Osteoporosis Nurse Specialists
x1 General Manager – Medical Services
x1 GG&C osteoporosis exercise service lead physio
x1 Superintendent Radiographer
x1 Assistant General Manager, Radiology
x1 Consultant radiologist (DXA) – local imaging lead
x1 Estates manager
x1 NOS patient representative
From Zero to FLS: Implementation & BeyondThe first steps
• Appointment of project management team & Chair • Redefine & agree with providers of funding remit of group &
scope of service
1. To roll out an FLS, to provide systematic post-fracture assessment to all men & women age 50+ with new fracture presentations or with new report of vertebral fracture or with previous fracture age 50+
2. To ensure equitable access of all relevant patients in the region
3. To implement these services within the constraints of the proposed funding
4. Case-finding for new fracture presentations & for new reports of vertebral fracture – by the FLS ONS
Remit of group & scope of planned service

5. Case-finding for previous fractures – by primary care
6. Post-fracture, risk assessment based on one-stop consultation with FLS-ONS incorporating DXA, where appropriate
7. All episodes of FLS-patient care recorded in database
8. To provide this for population of x over y sites and covering fracture patients from z hospitals
Remit of group & scope of planned service
From Zero to FLS: Implementation & BeyondThe first steps
• Appointment of project management team & Chair • Redefine & agree with providers of funding remit of group &
scope of service
• Work breakdown
From Zero to FLS: Implementation & Beyond
From Zero to FLS: Implementation & Beyond
From Zero to FLS: Implementation & BeyondThe first steps
• Appointment of project management team & chair • Redefine & agree with providers of funding remit of group & scope
of service
• Work breakdown
• Schedule work & establish timeline for delivery of service
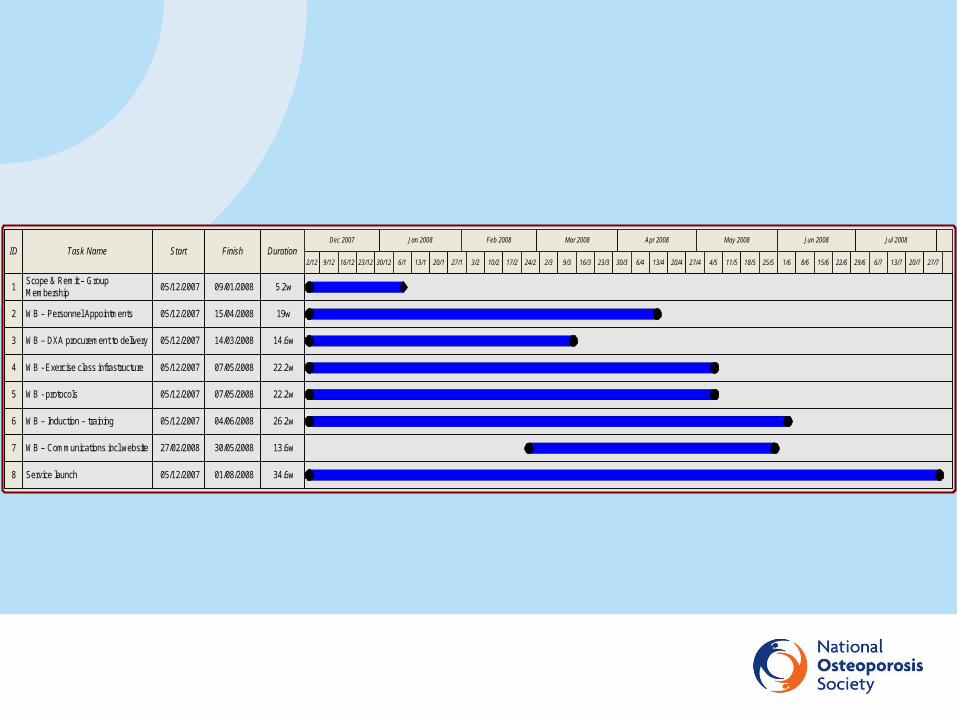
ID Task Name Start Finish DurationDec 2007 Jan 2008 Feb 2008 Mar 2008 Apr 2008 May 2008 Jun 2008 Jul 2008
2/12 9/12 16/12 23/12 30/12 6/1 13/1 20/1 27/1 3/2 10/2 17/2 24/2 2/3 9/3 16/3 23/3 30/3 6/4 13/4 20/4 27/4 4/5 11/5 18/5 25/5 1/6 8/6 15/6 22/6 29/6 6/7 13/7 20/7 27/7
1 5.2w09/01/200805/12/2007Scope & Remit – Group Membership
2 19w15/04/200805/12/2007WB – Personnel Appointments
3 14.6w14/03/200805/12/2007WB – DXA procurement to delivery
4 22.2w07/05/200805/12/2007WB - Exercise class infrastructure
5 22.2w07/05/200805/12/2007WB - protocols
6 26.2w04/06/200805/12/2007WB – Induction – training
7 13.6w30/05/200827/02/2008WB – Communications incl website
8 34.6w01/08/200805/12/2007Service launch
From Zero to FLS: Implementation & Beyond
What do you need to provide a DXA for a FLS service ?
• Space for DXA (may require building works!)
• DXA scanner/s – DXA (VFA) site visit to inform choice
– DXA procurement
• Radiographer/s
• ONS clinic space - near DXA
• Database - reporting system
• Patient transport issues
From Zero to FLS: Implementation & Beyond
Personnel
• Overview– Banding & Grades of Staff– Job descriptions– Appointments processes - job descriptions - adverts – interviews– Consultant Sessions
• How are Consultant sessions best deployed?
• Osteoporosis Nurse Specialist/s– Band 6/7 Osteoporosis Nurse Specialist– ONS line management– ONS where & how will they work?
Personnel
• Administration & Clerical Staff– Band 3 A&C
• Physiotherapist/s for exercise services – Band 6 Physiotherapist
• Radiographer/s – Band 6 Radiographers
From Zero to FLS: Implementation & Beyond
Logistics
• Pathways of care– New fracture presentations in which hospitals & FLS in which centres– New reports of vertebral fractures in which hospitals & FLS in which
centres– Past fractures from across region referred to which centres
• Protocol development
• Access to Mineral Metabolism clinic for those who don’t fit with management protocols
• Liaison re exercise classes
• Liaison with falls service
Logistics
• Communication within secondary care & with GPs
• Standardisation of forms
• Website development to facilitate communication
• Patient education materials
• Patient education classes
• ? Nurse telephone follow up (? Telephone BPR tariff)
• Training & induction
• Launch meeting

What do you need to provide exercise classes?
• Access to health service physio gym– Identify exercise class locations
• Access to leisure centre gyms– Identify exercise class locations
• Patient transport issues

If at first you don’t succeed…

If at first you don’t succeed…you’ve failed!

Pathway to success…& it will be incremental!

What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make to effect improvement?
Pathway to success…& it will be incremental!
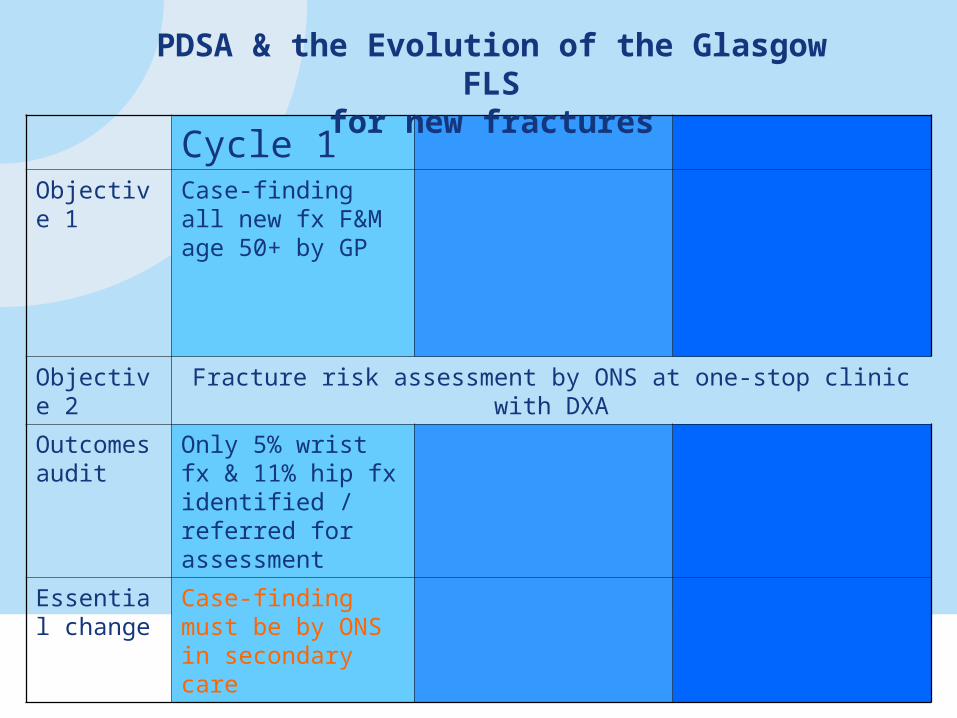
Cycle 1 Objective 1 Case-finding all new
fx F&M age 50+ by GP
Objective 2 Fracture risk assessment by ONS at one-stop clinic with DXA
Outcomes audit
Only 5% wrist fx & 11% hip fx identified / referred for assessment
Essential change
Case-finding must be by ONS in secondary care
PDSA & the Evolution of the Glasgow FLSfor new fractures
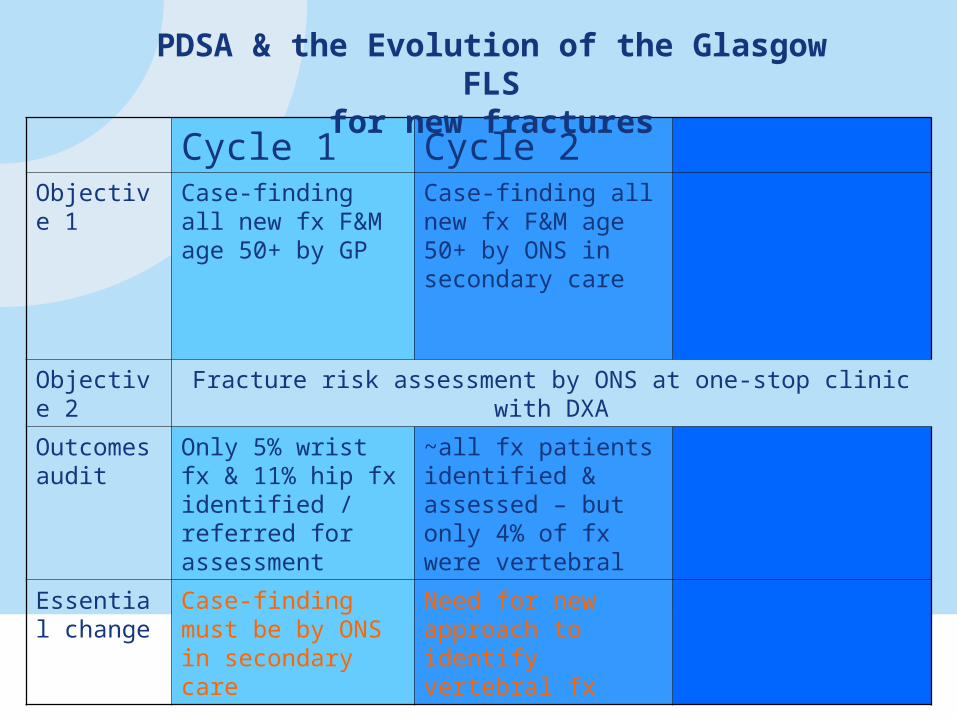
Cycle 1 Cycle 2 Objective 1 Case-finding all new
fx F&M age 50+ by GP
Case-finding all new fx F&M age 50+ by ONS in secondary care
Objective 2 Fracture risk assessment by ONS at one-stop clinic with DXA
Outcomes audit
Only 5% wrist fx & 11% hip fx identified / referred for assessment
~all fx patients identified & assessed – but only 4% of fx were vertebral
Essential change
Case-finding must be by ONS in secondary care
Need for new approach to identify vertebral fx
PDSA & the Evolution of the Glasgow FLSfor new fractures
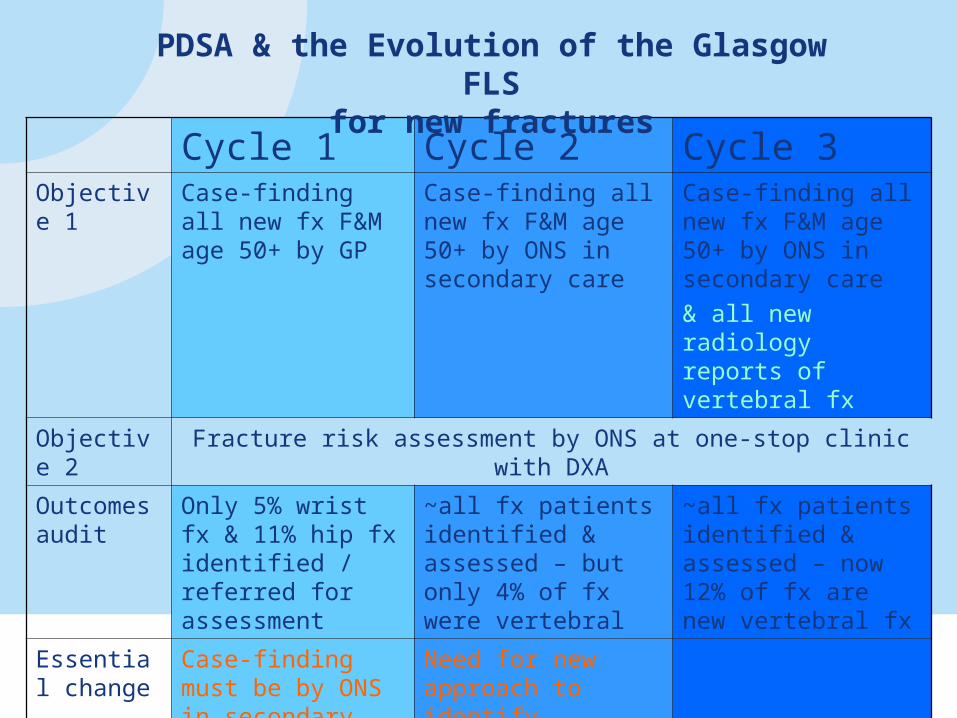
Cycle 1 Cycle 2 Cycle 3Objective 1 Case-finding all new
fx F&M age 50+ by GP
Case-finding all new fx F&M age 50+ by ONS in secondary care
Case-finding all new fx F&M age 50+ by ONS in secondary care
& all new radiology reports of vertebral fx
Objective 2 Fracture risk assessment by ONS at one-stop clinic with DXA
Outcomes audit
Only 5% wrist fx & 11% hip fx identified / referred for assessment
~all fx patients identified & assessed – but only 4% of fx were vertebral
~all fx patients identified & assessed – now 12% of fx are new vertebral fx
Essential change
Case-finding must be by ONS in secondary care
Need for new approach to identify vertebral fx
PDSA & the Evolution of the Glasgow FLSfor new fractures
‘The only place success comes before work is in a dictionary!’