Embed Size (px)
Citation preview

242
Skeletal Muscle Ventricles: Full Versus Half Aortic Ligation Kevin Greer, M.D., Huiren Lu, M.D., Robert Hammond, B. A., Steven Bastian, M.S., Richard Vanderheide, Ph.D., M.D.,* and Larry Stephenson, M.D.
Division of Cardiothoracic Surgery and *Department of Pathology, Wayne State Uni- versity School of Medicine, Detroit, Michigan
ABSTRACT Background: Skeletal muscle ventricles have been shown to provide effective aortic di- astolic counterpulsation in an experimental model. Construction has included full ligation of the thoracic aorta. The authors sought to determine if these muscle pumps could function effectively without fully ligating the aorta. Methods: Skeletal muscle ventricles were constructed in two groups of dogs. Group 1 had their aortas fully ligated (n = 10) while group 2 had their aortas nar- rowed by 50% (n = 10). The animals were followed for 10 weeks. Results:There was no significant difference in femoral diastolic augmentation a t implant or at 10 weeks (19.1% rt 9.940 in group 1 [full ligation] versus 16.340 f 10.2% in group 2 [half ligation] p = 0.502). Survival t o 10 weeks was significantly better in group 1 (full ligation). Nine of 10 animals in this group survived versus 4 of 10 in group 2 (p = 0.019). Two animals survived in the half ligation group with effective augmen- tation and without thrombus formation. Conclusion: Both models produce effective diastolic counterpulsation. Survival was decreased in this model using half ligation, and survival without complication was observed in 2 of 10 animals. Currently the overall results are better with the full aortic ligation model. However, design modifications will probably result in an effective model of diastolic counterpulsation without full aortic ligation. (J Card Surg 7998; 13:242-257)
Our laboratory has investigated the use of blood pumps constructed from skeletal muscle in dogs. We refer to these pumps as skeletal mus- cle ventricles (SMVs). SMVs have been shown to effectively assist the right and left heart in a vari- ety of configurations.14 In our standard model, the SMV is connected to the descending thoracic aorta with a bifurcated graft.
The standard aortic counterpulsation model has been effective in augmentation of aortic di- astolic pressure, both with normal cardiac func- tion and during propranolol-induced profound low
Supported in part by NIH grant number NHLB34778-11. Dr. Greer was supported by NIH National Research Service Award grant number F32 H209292-01. Address for correspondence: Larry W. Stephenson, M.D., Chief, Division of Cardiothoracic Surgery, Harper Hospital, Suite 228, 3990 John R Street, Detroit, MI 48201-2097. Fax: (313) 993-0572.
cardiac output. This model is reproducible and has a low incidence of rupture. The incidence of thrombosis and thromboembolism is also low. An SMV of this type has pumped blood effectively for more than 4 years in one animal. Before we attempt to use this model clinically, it is important to understand whether it is necessary to ligate the thoracic aorta, as has always been done pre- viously.
This study represents a comparison between our standard model of diastolic counterpulsation with ligation of the thoracic aorta and a similar model constructed with aortic narrowing. SMVs were constructed in two groups of 20 dogs, 10 dogs in each group. The purpose was to compare the functional hemodynamic augmentation ob- tained with these two models at implantation and to follow this function over time. In addition, mor- bidity or mortality was compared between the two models.

J CARD SURG 1998; 131242-251
GREER, ET AL. 243 SKELETAL MUSCLE VENTRICLES
MATERIALS AND METHODS
Skeletal muscle ventricle construction and conditioning
Twenty adult mongrel dogs weighing between 15 and 23 kg were operated on in accordance with the "Guide for the Care and Use of Laboratory An- imals" published by the National Institutes of Health (NIH Publication No. 86-23, revised 1985). Anesthesia was induced with thiamylal sodium (15 mg/kg). The animals were then intubated, placed on a ventilator, and maintained on inhala- tional anesthesia using 1 YO to 2% isoflurane.
The SMV was constructed using the left latis- simus dorsi muscle as previously described.5 An incision was made in the left flank that extended from the mid-axillary line to the tip of the 1 2th rib. The latissimus was mobilized from its origin at the spinous processes and l l t h and 12th ribs to in- clude a generous portion of thoracodorsal fascia. The soft tissue attachments and collateral blood supply from the platysma muscle and chest wall were divided. The insertion of the muscle at the humerus was left intact. Care was taken to avoid injury to the neurovascular bundle. A bipolar nerve lead (Medtronic Inc., Minneapolis, MN, USA) was then placed around the thoracodorsal nerve for future stimulation. This lead was con- nected to a neurostimulator (Medtronic model #7420 or #8318) and placed in a subcutaneous pocket along the lateral abdominal wall. A thora- cotomy was then performed through the sixth in- tercostal space. The left phrenic nerve was mobi- lized, and a section of the pericardium with a surface area between 25 to 30 cm2 was removed. A chest tube was placed for evacuation of fluid and air, and the chest was closed in layers. A cylin- drical plastic tube (diameter, 3.4 cm; volume 1.5 to 2.0 cc/kg) with a Teflon felt (USCI [Div. C R Bard], Billerica, MA, USA) sewing ring was used as a mandrel for the SMV construction. The har- vested pericardium was wrapped around the mandrel and sutured to the sewing ring with a 5- 0 polypropylene suture to act as a lining for the SMV. The pericardium was oriented so that the visceral surface formed the inner blood pump sur- face of the SMV. The muscle was then wrapped 1.5 to 2.0 times around the pericardial-covered mandrel. A 4-0 polypropylene suture was used to anchor the fascia1 edge of the muscle to the sewing ring. The SMV was then secured to the chest wall with interrupted absorbable sutures,
and the wound was closed in layers. The chest tube was removed at the end of the procedure.
All animals underwent a 3-week period of vas- cular delay to allow the latissimus to recover from ischemia induced by division of the collateral blood supply.6 Following this, the neurostimulator was activated to deliver a 2-Hz continuous pulse of 1 to 2 V amplitude and 210-psec duration. Stimulation was continued for 5 to 7 weeks. This stimulation protocol has been shown to induce near complete transformation of the muscle from fast-twitch (fatigue sensitive) to slow-twitch (fatigue-resistant) fibers.'
Connection to the circulation
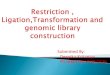
After conditioning, a second operative proce- dure was performed. The animals were again anesthetized, intubated, and maintained on in- halational anesthesia. A femoral arterial catheter was placed to monitor perfusion to the lower ex- tremities during operation. A left thoracotomy was performed through the fourth or fifth inter- costal space to gain access to the heart and aorta. A myocardial sensing lead (Medtronic) was then placed on the surface of the left ventricle. The temporary neurostimulator was then removed and the nerve lead and ventricular sensing lead were connected to a permanent cardiomyostimu- lator (Medtronic, model SP1005). The base of the SMV was dissected free and the mandrel re- moved leaving the sewing ring in place with the pericardium lining the SMV. A bifurcated Gore-Tex (W.L. Gore and Associates, Flagstaff, AZ, USA) graft was then used to couple the SMV to the de- scending aorta. This graft was prepared with two lengths of 14-mm Gore-Tex tube grafts connected to a base cap of Gore-Tex cardiovascular patch material. The first limb was anastomosed just past the takeoff of the subclavian artery while the sec- ond limb was anastomosed approximately 5 cm distally. A side-biting clamp was used for aortic control during completion of the anastomoses. The Gore-Tex base cap was then sutured to the Teflon sewing ring of the SMV. The limbs of the grafts were filled with saline and all clamps were released. In group 1, the aorta was fully ligated with umbilical tape between the two limbs of the graft. In group 2, the diameter of the aorta was measured with calipers and the external diameter was narrowed by 50% with umbilical tape (Fig. 1). In both instances, after the umbilical tape knot

244 GREER, ET AL. SKELETAL MUSCLE VENTRICLES
J CARD SURG 1998;13:242-251
Half Full Figure 1. Diagram showing the connection of the skeletal muscle ventricle (SMVl to the circulation. A bifurcated graft is used to connect the SMV to the descending aorta (Aol just past the takeoff of the subclavian artery. In the group with half-aortic ligation, calipers were used to narrow the aortic diameter by 50%, diverting a portion of the blood flow through the SMV circuit. In the full aortic ligation group, the aorta was completely ligated so that all blood flows through the SMVcircuit. (Note: SMVnot drawn to scale in relation to the aortal.
was placed it was secured with a nonabsorbable suture to prevent slipping.
Throughout the duration of the study, we alter- nately performed full and half aortic ligation. Fol- lowing initial hemodynamic measurements, the wound was closed in layers and the animals were allowed to recover. A chest tube was maintained on 20-cm H,O suction overnight and removed the following morning. Animals were maintained on oral aspirin through the length of the study for its antiplatelet effect.
SMV stimulation while in circulation
The cardiomyostimulator was programmed to chronically deliver a 33-Hz burst of electrical stim- ulation of 2 to 5 V amplitude during diastole. The stimulator was programmed to the mode 2 set- ting, which varies the stimulation ratio based on the native heart rate. Specifically, it delivers one burst for every two cardiac cycles when the heart rate is < 1 10 beats/min (1 :2 burst ratio). It delivers
a 1 :3 burst ratio between 11 0 beats/min and 150 beats/min. The ratio increases to 1.4 when the heart rate is > 150 beatdmin. This means that de- spite changes in the animals' native heart rate, the number of electrical bursts being delivered to the muscle ranged between 35 burstdmin and 55 bursts/min. A fixed delay period was adjusted to equal 30% to 35% of the R-R interval as mea- sured just prior to data collection.
Measurements
Blood pressure was measured using fluid-filled manometers connected to transducers. The fem- oral artery was accessed percutaneously, while the SMV luminal pressure was measured during the initial procedure using a 20-gauge angiocath placed through the Gore-Tex graft near the base of the SMV. Immediately after connection to the circulation, hemodynamic data were collected. At 2 and 4 weeks after implantation, femoral pres- sure was again measured with a percutaneous ar-

J CARD SURG 1998; 131242-251
GREER, ET AL. 245 SKELETAL MUSCLE VENTRICLES
terial catheter under general anesthesia. Ultra- sound examination of the SMV lumen was also performed at this time to assess for the presence of thrombus. At 10 weeks, a terminal procedure was performed under general anesthesia. A carotid arterial cutdown was performed for place- ment of a carotid artery pressure catheter. The femoral artery was accessed percutaneously. while the SMV pressure was measured with an angiocath placed directly through the muscular walls of the SMV. Data were collected with a Gould ES 1000B recording and display system (Gould, Cleveland, OH, USA) and simultaneously with a CODAS on-line data collection program (Dataq Instruments, Akron, OH, USA).
Following final collection of hemodynamic data, the animals were euthanized under general anesthesia with intravenous potassium chloride and an autopsy was performed. The SMVs were removed to assess for thrombus formation. The spleen and kidneys were also removed to assess for distal embolization. If gross examination re- vealed the possibility of distal embolization, this area was examined histologically. The area of the aorta that was narrowed at implantation was also removed for inspection and histologic analysis.
Calculations
Arterial pressure waveforms were examined using a Windaq (Dataq Instruments) data analysis program. Mean pressures were calculated as the average pressure over time. "Diastolic augmenta- tion" refers to the increase in the mean pressure during cardiac diastole seen with the stimulator ON versus OFF. Diastole was defined as the period of time from the dicrotic notch to the beginning of the systolic pressure augmentation associated with the opening of the aortic valve. Comparisons are made between alternating beats while stimulating at a 1 :2 contraction ratio. All measurements were taken over a period of at least 20 cardiac cycles. Data are expressed as the mean t standard devia- tion. Clinical events (SMV rupture, thrombus for- mation, and mortality) were compared between the two groups using a Chi-square analysis. For the purpose of this study, significant thrombus was de- fined as > 5 cc of thrombus in the apex of the SMV (chamber volume = 27 cc to 35 cc). Augmentation of pressure was compared between the two groups using a two-tailed Student's t test. Statisti- cal significance was defined as p c 0.05.
RESULTS
Group 1 (full ligation)
The initial femoral diastolic augmentation for all animals in group 1 was 19.1 % 2 9.9% (p < 0.001). Of the 10 animals that had their aorta fully ligated, 9 survived to completion of the study at 10 weeks. All animals showed significant diastolic augmenta- tion at 10 weeks except one that was found to have a broken nerve lead at autopsy. This animal demonstrated diastolic augmentation a t 4 weeks, however a t 10 weeks no muscular contraction was observed despite a functional stimulator. The average femoral augmentation for the survivors (excluding the animal with a broken lead) was 19.8% -c 8.1 % (p < 0.001) at the time of the ter- minal study. This compared favorably to the initial augmentation of 20.7% 2 9.3% for these eight an- imals. The difference in augmentation initially and at 10 weeks was not statistically significant (p = 0.826). The percentage augmentation in femoral pressure is demonstrated graphically in Figure 2. At 10 weeks this pressure augmentation was also demonstrated in the carotid artery where the av- erage augmentation was 20.5% 2 10.6% (p = 0.003). However six of the eight animals had a carotid pressure tracing available for analysis. Typ- ical pressure tracings from an animal that survived to 10 weeks are shown in Figure 3. The single an- imal that died before 10 weeks was found to have
35% 1
20%
15% -
10%
0% r I
implant 10 weeks
Figure 2. Femoral pressure augmentation, skeletal muscle ventricle (SMV) ON versus OFF, in the eight an- imals with complete aortic ligation that survived to completion of the experiment (excludes one animal that survived but with a broken nerve lead). "Implant" refers to augmentation upon connection to the circula- tion. All surviving animals were euthanized at 10 weeks. There was no significant thrombus present in any of these animals at autopsy. Bold line indicates av- erage augmentation.

246 GREER, ET AL. SKELETAL MUSCLE VENTRICLES
J CARD SURG 1998;13:242-251
. . . .
A
. . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . i . . . . . . . . . . . . . . . . . . . . . . . . . . . : . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
, ; :....:._..: :..._:. . : . . :
.... .... .... . . . . ..... . . . . . . . . . . . . . . . . . . . . . . . . . . . :. . . . . 00 j v ; . . ..; i i ;. ! : . . . . . . . . . .
. . : .
. . . . . . .
BASE 20.690 SEC(TBF) off SEC(TII) off ZEOF B
Figure 3. Pressure waveform recordings taken from an animal with its aorta completely ligated. A: Shows data taken at the time of connection to the circulation, while 13: shows data taken after the skeletal muscle ventricle ISMV) had been pumping blood in the circulation continuously for 70 weeks. The difference in augmentation obtained at implant and at 70 weeks was not statistically significant.

J CARD SURG 1998;13:242-251
GREER, ET AL. 247 SKELETAL MUSCLE VENTRICLES
a rupture of the SMV at the Teflon sewing ring 36 days after implant. This animal also had significant thrombus in the apex of the SMV cavity (20 cc). Thrombus had been noted at the 2-week hemody- namic measurement and had remained stable thereafter. There was no thrombus present in the other animals in group 1 that survived to comple- tion of the study at 10 weeks, including the one with the nonfunctioning SMV.
Group 2 (half ligation)
The initial femoral diastolic augmentation for all animals in group 2 was 16.3% 2 10.2% (p < 0.001). Of the ten animals who had their aorta narrowed by 50%, four survived the full 10 weeks of the study. All four animals showed diastolic augmentation at 10 weeks with an average femoral augmentation of 7.4% 2 3.1% (p = 0.014). This was decreased from an initial aug- mentation of 16.2% 2 8.1 YO for these four ani- mals, although this difference between implant and the 1 O-week augmentation did not reach sta- tistical significance (p = 0.089). The percentage augmentation in femoral pressure is demon- strated graphically in Figure 4. There was also sig- nificant carotid arterial augmentation in these an- imals at 10 weeks with an average augmentation
jDKl
0% I I
implant 10 weeks
Figure 4. Femoral pressure augmentation, skeletal muscle ventricle (SMV) ON versus OFF, in the four an- imals with half aortic ligation that survived to comple- tion of the experiment. "Implant" refers to augmenta- tion upon connection to the circulation. All surviving animals were euthanized at 10 weeks. Two of these animals showed significant thrombus in the SMV chamber at autopsy (indicated b y 0 andxl. Bold line in- dicates average augmentation.
of 9.1 % 2 6.3% (p = 0.032). Pressure waveforms from one animal that survived to 10 weeks are shown in Figure 5.
The cause of death of the animals is listed in Table 1. Five of these six animals died within 17 days of implant. Of the four animals that survived to completion of the study, two of the four ani- mals had significant thrombus in the apex of the SMV (1 5 cc and 20 cc). The presence of this clot had been noted in both animals at the 2-week he- modynamic measurement and had remained sta- ble until the terminal experiment. At autopsy, nei- ther of these animals showed evidence of distal thromboembolization. The clot itself was solid and firmly adherent to the inner surface of the SMV. Inspection of the aortas in this group of an- imals that were narrowed by 50% (estimated measurement) a t implant revealed the inner diameter of the aortic lumen in the area of the lig- ature to be reduced by 33% to 50% (average reduction of 43%) compared to the luminal diam- eter of the surrounding aorta. Histologic exami- nation of the aortic wall in this area showed the wall to be thinned and largely replaced by fibrous tissue. There was no evidence of clot formation in the aortic lumen as a result of the narrowing.
Comparison of group 1 (full ligation) versus group 2 (half ligation)
All animals showed significant augmentation of femoral pressure at the time of implantation ex- cept one animal in the half ligation group. The av- erage augmentation in the fully ligated group was 19.1 % 2 9.9% (p < O.OOl) , while the average augmentation in the half ligation group was 16.3% f- 10.2% (p < 0.001). There was no sta- tistical difference in the degree of augmentation between the two groups initially (p = 0.502).
The difference in femoral pressure augmenta- tion at the terminal experiment (1 9.8% t 8.1 % in the full ligation group vs 7.4% 2 3.1 % in the half ligation group) in the animals that survived 10 weeks was statistically significant (p = 0.01 8). The difference in carotid pressure augmentation at the terminal experiment (20.5% t 10.5% in the full li- gation group vs 9.1 YO 2 6.3% in the half ligation group) in this same group of animals approached, but did not reach, statistical significance (p = 0.091 1. However, as mentioned above, only six of the eight animals in the terminal full ligation group had carotid pressure available for analysis.

248 GREER, ET AL. SKELETAL MUSCLE VENTRICLES
J CARD SURG 1998;13:242-251
off SEC(TH) 70 .4 ZEOP E: .09-05-96 1 4 : 2 4 . 2 2
A
B
Figure 5. Pressure waveforms recordings taken from an animal with its aorta narrowed 50%. A: Shows data taken at the time of connection to the circulation, while B: shows data taken after the SMV had been pumping blood in the circulation continuously for 10 weeks. The difference in augmentation obtained at implant and at 10 weeks was not statistically significant.

J CARD SURG 1998;13:242-251
GREER, ET AL. 249 SKELETAL MUSCLE VENTRICLES
TABLE 1
Ligation Complication in Circulation Number of Days
Full SMV rupture 36 Half Anastornotic disruption 7 Half SMV rupture 9 Half SMV rupture 13 Half Thrornbosed SMV/aorta 14 Half Thrornbosed SMV/aorta 17 Half SMV rupture 67
SMV = skeletal muscle ventricle
The difference in mortality between the two groups was statistically significant. One of ten an- imals in the full ligation group died versus six of the ten in the half ligation group before the end of the 10 weeks in circulation (p = 0.01 9). There was also a trend toward increasing thrombus forma- tion in the half ligation group. The half ligation group had thrombus in five of ten SMVs, while the full ligation group had thrombus in one of ten SMVs. The difference in the incidence of throm- bus formation approached, but did not reach, sta- tistical significance (p = 0.051 1.
DISCUSSION
Our laboratory has previously demonstrated that skeletal muscle ventricles are capable of pro- viding effective diastolic augmentation beyond 2 years in circulation.8.9 Currently one animal has survived beyond 4 years with a pumping SMV. These pumping chambers have been shown to function effectively in the setting of profound heart failure.10 Effective diastolic augmentation was present at the last hemodynamic measure- ment. This animal has had no evidence of throm- bus formation in the SMV cavity or distal throm- boem bolization.
The development of our current model has evolved over time. While other groups have used other skeletal muscles such as the rectus abdo- minis or gluteal muscle^,^^-^^ our work has fo- cused on the latissimus dorsi muscle. In 1991, Anderson et al.14 reported a series of SMVs con- structed from the latissimus dorsi in dogs using complete aortic ligation. These SMVs were lined with autologous pericardium, pleura, or the fi- brous tissue reaction that developed on the sur- face of the muscle itself. The SMVs developed ef-
fective aortic diastolic augmentation at implant. However, a large percentage of these animals de- veloped either rupture of the SMV at the Teflon sewing ring or showed evidence of thrombus for- mation and/or distal thromboembolization. In fact, two-thirds of these SMVs that pumped blood in the circulation for greater than 24 hours ruptured.
Thomas et aI.l5 reported several design modifi- cations that improved survival. They compared SMVs in two groups of dogs that differed only in that one group of SMVs was lined with autolo- gous pericardium while the other was lined with only the fibrous material that forms on the mus- cle surface from contact with the mandrel. Both groups also had inclusion of a wide strip of thora- columbar fascia with the anastomosis to the Teflon sewing ring. Although both groups had a low incidence of thrombus formation, the group lined with pericardium had a substantially lower incidence of rupture (63% in the group with only fibrous lining vs 0% in the group with pericardial lining). Our current series of animals with full aor- tic ligation had a rupture rate of 10% (1 of 101, which is comparable to Thomas' previous series.
Thus we now feel that we have a reproducible, effective aortic diastolic counterpulsator SMV model with a low rate of rupture. Also, the inci- dence of thrombosis and thromboemboli is low. We believe the animal with the SMV in circulation for over 4 years has functioned at least 2 years longer than any type of mechanical LVAD has functioned in either a person or an animal. Before clinical studies are proposed, it should be deter- mined whether full aortic ligation is necessary.
This study represents our first attempt at mod- ification of our SMV model to avoid aortic ligation. Although there was a significant difference in mortality (one of ten in the full ligation group vs six of ten in the half ligation group), there are some encouraging findings for the group 2 model. First, the half ligation group produced sig- nificant diastolic pressure augmentation at im- plantation and after pumping blood in the circula- tion for 10 weeks. Second, two of the half ligation animals that survived to term were free of clot. These two animals showed initial and terminal pressure augmentation that was not significantly different from the other animals in the group with half aortic ligation.
There appeared to be a temporal relationship for the various types of complications that oc- curred over the length of the study. Two animals

250 GREER, ET AL. SKELETAL MUSCLE VENTRICLES
J CARD SURG 1998:13:242-251
in the half ligation group developed SMV throm- bus with extension into the distal aorta. These both occurred early in the course of the experi- ment, at 14 and 17 days postimplant, and re- quired the animals be euthanized because of acute ischemia to the abdominal viscera and hind limbs. Three other animals in the half ligation group developed thrombus in the apex of the SMV over the length of the study. One of these animals subsequently died of SMV rupture and two went on to survive the full 10 weeks. In both of these animals that survived to 10 weeks, the clot had been seen on the 2-week ultrasound ex- amination and had remained stable over the fol- lowing 8 weeks. Interestingly, the pressure aug- mentation demonstrated in the two animals that survived to 10 weeks without clot was not signif- icantly different from the two animals with apical thrombus. The single animal in the full ligation group that developed thrombus also demon- strated this at the 2-week measurement, after which time the clot remained stable until the SMV ruptured on day 36 postimplant.
Thrombosis has been observed in previous se- ries of SMVs. Dogs have a substantially shorter clotting time than humans, and this likely con- tributes to thrombosis in the various canine mod- els. In our standard model with full aortic ligation, all blood flowing in the descending aorta is routed through the SMV. This probably provides effec- tive “washing“ of the SMV with every cardiac cy- cle. In contrast, the half ligation model routes only a portion of the blood flow to the descending aorta through the SMV; the remainder is able to traverse the area of aortic narrowing and mix with the blood flowing through the distal SMV conduit. This area of turbulent flow may lead to activation of platelets and the coagulation cascade, increas- ing the potential for thrombus formation. These animals were not fully anticoagulated because of the requirements for multiple intraoperative mea- surements. If used clinically, low levels of antico- agulation may decrease the complications asso- ciated with thrombosis.
There are several potential criticisms of this study. We repeatedly measured femoral pres- sure augmentation to assess diastolic augmenta- tion, rather than aortic root pressure, which would be more indicative of the degree of dias- tolic augmentation seen by the coronary circula- tion. We have previously measured aortic root pressures in animals with SMVs in acute experi-
ments, however there have been complications with long-term indwelling lines in several of our most recent experiments. Because this study was designed to compare morbidity and mortal- ity as well as function over time, we felt the least invasive measurement was appropriate until the terminal experiment when a carotid arterial catheter was placed.
These studies were performed on animals with healthy hearts. Ideally, it would be desirable to measure this function in the setting of chronic heart failure. We have previously reported data collected from SMVs using propranolol to induce acute heart failure.’O We found that the percent- age of diastolic augmentation obtained in this setting was actually higher than in animals with healthy hearts. There seemed to be no adverse effects on the muscle in these studies. Currently, we are investigating several models of chronic heart failure for use in future experiments.
CONCLUSION
Skeletal muscle ventricles constructed with ei- ther full or half aortic ligation produce effective cardiac assistance that can be maintained over time. Currently the overall results are better with the full aortic ligation model. The full ligation group is associated with a low incidence of mor- bidity and mortality. In this study the half ligation model was more prone to thrombosis. Based on the temporal occurrence of adverse events in this group, it appears this condition stabilizes at ap- proximately 2 weeks. Future efforts should focus on modifying the current half aortic ligation model to improve this initial period of thrombogenicity. Previous studies with other SMV models have shown that slight design modifications can dra- matically improve results.
REFERENCES
Acker MA, Anderson WA, Harnmond RL, et al: Skeletal muscle ventricles in circulation: One to eleven weeks experience. J Thorac Cardiovasc Surg 1987;94: 163-1 74. Greer KA, Lu H, Harnmond RL, et al: Skeletal mus- cle ventricles, left ventricular apex-to-aorta config- uration: 1-1 1 weeks in circulation. Circulation 1997;
Niinami H, Hooper TL, Harnmond RL, et al: Skele- tal muscle ventricles in the pulmonary circulation:
95:497-502.

J CARD SURG 1998;13:242-251
GREER, ET AL. 251 SKELETAL MUSCLE VENTRICLES
Up to 16 weeks' experience. Ann Thorac Surg
4. Hooper TL, Niinami H, Hammond RL, et al: Skele- tal muscle ventricles as left atrial-aortic pumps: Short-term studies. Ann Thorac Surg 1992;54:316- 322.
5. Thomas GA, Lu H, lsoda S, et al: Pericardium-lined skeletal muscle ventricles in circulation up to 589 days. Ann Thorac Surg 1994;58:978-988.
6. lsoda S, Yano Y, Yasuyuki J, et al: Influence of de- lay on latissimus dorsi muscle flap blood flow. Ann Thorac Surg 1995;59:632-638.
7. Mannion JD, Bitto T, Hammond RL, et al: Histo- chemical and fatigue characteristics of conditioned latissimus dorsi muscle. Circ Res 1986;58:298-304.
8. Mocek FW, Anderson DR, Pochettino A, et al: Skeletal muscle ventricles in circulation long-term: 191 to 836 days. J Heart Transplant 1992;ll :S334- S340.
9. Thomas GA, lsoda S, Hammond RL, et al: Peri- cardium-lined skeletal muscle ventricles: Two year in-circulation experience. Ann Thorac Surg 1996;
10. Thomas GA, Lu H, Nakajima H, et al: Skeletal mus-
1992;53:750-757.
62: 1698-707.
cle ventricle aortic counterpulsation: Chronic func- tion with and without propranolol-induced heart failure. Surg Forum 1993;XLIV:327-329.
11. Jeffe A, Ricoy JR, Marquez J, et at: Cardialization: A new source of energy for circulatory assistance. Vasc Surg 1978;12:10-17.
12. Kusserow BK, Clapp JF: A small ventricle-type pump for prolonged perfusions: Construction and initial attempts to power a pump biologically with skeletal muscle. Trans Am SOC Artif Intern Organs
13. Spotnitz HM, Merker C, Malm JR: Applied physiol- ogy of the canine rectus abdominis: Force-length curves correlated with functional characteristics of a rectus powered "ventricle." Potential for cardiac assistance. Trans Am SOC Artif Intern Organs
14. Anderson DR, Pochettino A, Hammond RL, et al: Autogenously lined skeletal muscle ventricles in circulation: Up to nine months experience. J Tho- rac Cardiovasc Surg 1991;101:661-670.
15. Thomas GA, Lu H, lsoda S, et at: Skeletal muscle ventricles in circulation: Decreased incidence of rupture. Ann Thorac Surg 1996;61:430-436.
1964;10:74-78.
1974;20:747-756.