Embed Size (px)
Citation preview
RETINAL DISORDERS
Fundus autofluorescence in patients with retinal pigmentepithelial (RPE) tears: an in-vivo evaluationof RPE resurfacing
Randev Mendis & Noemi Lois
Received: 15 March 2013 /Revised: 30 November 2013 /Accepted: 5 December 2013# Springer-Verlag Berlin Heidelberg 2014
AbstractAim Investigate RPE resurfacing by changes in fundus auto-fluorescence (AF) in patients with retinal pigment epithelial(RPE) tears secondary to age-related macular degeneration(AMD).Methods A retrospective case series of patients presenting withRPE tears from 1 March 2008 to 1 April 2011. The pattern andarea of AF signal distribution in RPE tears were evaluated. Thechange in the size of the area of debrided RPE over the follow-up period was used as the main outcome measure. A reductionin this area was termed “RPE resurfacing”, and an enlargementtermed “progression of RPE cell loss”.Results Thirteen patients (14 eyes) with RPE tears (mean age82 years) were included in this study. The mean baseline area ofreducedAF signal was 4.1mm2 (range 0.33–14.9, median 0.29).“Resurfacing” of the RPE occurred in ten eyes and “progressionof RPE cell loss” in four eyes after a median follow-up of11.5 months (range, 1–39). The mean area of healing was2.0 mm2, and progression was 1.78 mm2.Conclusion A consistent AF pattern was observed in patientswith RPE tears. RPE resurfacing over the area of the RPE tearoccurred, to a varying degree, in the majority of the cases.
Keywords Retinal pigment epithelium . Retinal pigmentepithelial tears . Autofluorescence . Age-relatedmaculardegeneration
Introduction
Retinal pigment epithelial tears, first described by Hoskin andcolleagues with the help of fundus fluorescein angiography(FFA), represent a relatively common complication of age-related macular degeneration (AMD). RPE tears occur mostcommonly in the context of a previously present retinal pigmentepithelial detachment (PED), with ripping developing typicallyat the boundary between attached and detached RPE [1, 2].
Tears of the RPE can occur spontaneously or followingtreatment for neovascular AMD; they have been reportedfollowing laser photocoagulation [3], photo-dynamic therapy(PDT) [4, 5], and, most recently, anti-vascular endothelialgrowth factor (VEGF) therapies [6–9]. An approximate inci-dence of 15 % of RPE tears has been reported in eyes receiv-ing anti-VEGF treatment [10, 11].
An RPE tear may be suspected, on clinical examination, bythe presence of sub-retinal and sub-RPE blood, an often well-defined pigmented line at the site of the rolled RPE, and a de-pigmented area corresponding to the exposed choroid. Thediagnosis of an RPE tear is confirmed by FFA, which dem-onstrates blocked fluorescence at the site if the rolled RPE andmarked hyperfluorescence, from the very early frames of theangiogram, at the site of the exposed RPE [1].
Fundus autofluorescence (AF) imaging allows for an in-vivo,non-invasive evaluation of the RPE [12, 13], as the AF signalderives mainly from lipofuscin in these cells [13, 14]. Using AFimaging, changes in the RPE can be recorded over time [15].
The purpose of this study was to evaluate fundus AF fea-tures in patients with AMD and RPE tears, to study changes in
R. MendisDepartment of Ophthalmology, Grampian University Hospitals–NHS Trust, Aberdeen, Foresterhill, AB25 2ZN Aberdeen, UK
N. Lois (*)Centre for Vascular and Visual Sciences, Queens University,Belfast, Northern Ireland, UKe-mail: [email protected]
R. MendisDepartment of Ophthalmology, ACT Government Health, TheCanberra Hospital, Yamba Drive Garran, Canberra ACT 2605,Australia
Graefes Arch Clin Exp OphthalmolDOI 10.1007/s00417-013-2549-3
the distribution of AF over time, and to investigate in-vivo‘RPE resurfacing’ following this complication [16–18].
Material and methods
The medical records of all consecutive patients diagnosedwith AMD and RPE tear were retrospectively reviewed. Pa-tients were identified using an electronic database available atthe Eye Clinic, Grampian University Hospitals–NHS Trust,Aberdeen, Scotland. The search covered a period of 3 years,from 1 March 2008 to 1 April 2011. Only patients in whomAF images were available prior to or at the time of andfollowing the development of the RPE tear were included.
Patient demographics, distance visual acuity, and type andnumber of treatments received prior to and following thedevelopment of the RPE tear were recorded. Visual acuity,colour fundus photographs, FFA, OCT, and AF images werereviewed. AF and OCT images were interpreted in relation tofindings on colour fundus photographs and FFA.
Distance visual acuity was obtained using the Early Treat-ment Diabetic Retinopathy Study (ETDRS) visual acuitycharts. For the purpose of the statistical analysis, the logarithmof minimum angle of resolution (logMAR) vision was used.
Colour fundus photographs and FFA images were obtainedusing a TOPCON-IMAGENET system (Topcon Medical Sys-tems, Oakland, NJ, USA). The presence of the RPE tear wasconfirmed by FFA. OCT images were obtained using a StratusOCT-3 (Carl Zeiss, Dublin, CA, USA). Fundus AF imageswere obtained using the Heidelberg Retina Angiograph(HRA-2, Heidelberg Engineering, Heidelberg, Germany). Im-ages were evaluated qualitatively, for areas of increased or
reduced AF signal compared with background levels. In addi-tion, a quantitative assessment of the area debrided of RPE (areawith marked reducedAF signal— Fig. 1) was undertaken. Thisarea of reduced signal was measured on the baseline (B) and onthe last follow up (L) image using the image analysis softwaretool made available with the Heidelberg HRA-2. The softwaretool automatically converts pixels into millimetres. All mea-surements were carried out on 30° AF image frames with anoriginal image resolution of 768×768 pixels. Measurementswere repeated three times; the average of the twomeasurementswith less variability was used for the analysis.
The change in the area of reduced AF signal was calculatedby subtracting from the baseline area (B) that determined at lastfollow-up (L) (Fig. 2). “RPE resurfacing” was defined as anyreduction in the size of the area with reduced AF signal frombaseline to last follow-up; “progression of RPE cells loss” wasdefined as any increase in the size of the area of reduced AFsignal at last follow-up comparedwith that measured at baseline.
Results
Thirteen patients (14 eyes) with AMD and RPE tears wereidentified and included in this study; five weremales and eightfemales, with a median age of 82 years (range, 56–92 years).Two other patients with RPE tears and AMD were identifiedbut excluded from the study; one had no follow-up availableafter the RPE tear had occurred, whereas in the other thepreviously established diagnosis of RPE tear could not beconfirmed.
In 12 eyes, a vascularized PEDwas present and detected byFFA and OCT images prior to the development of the RPE
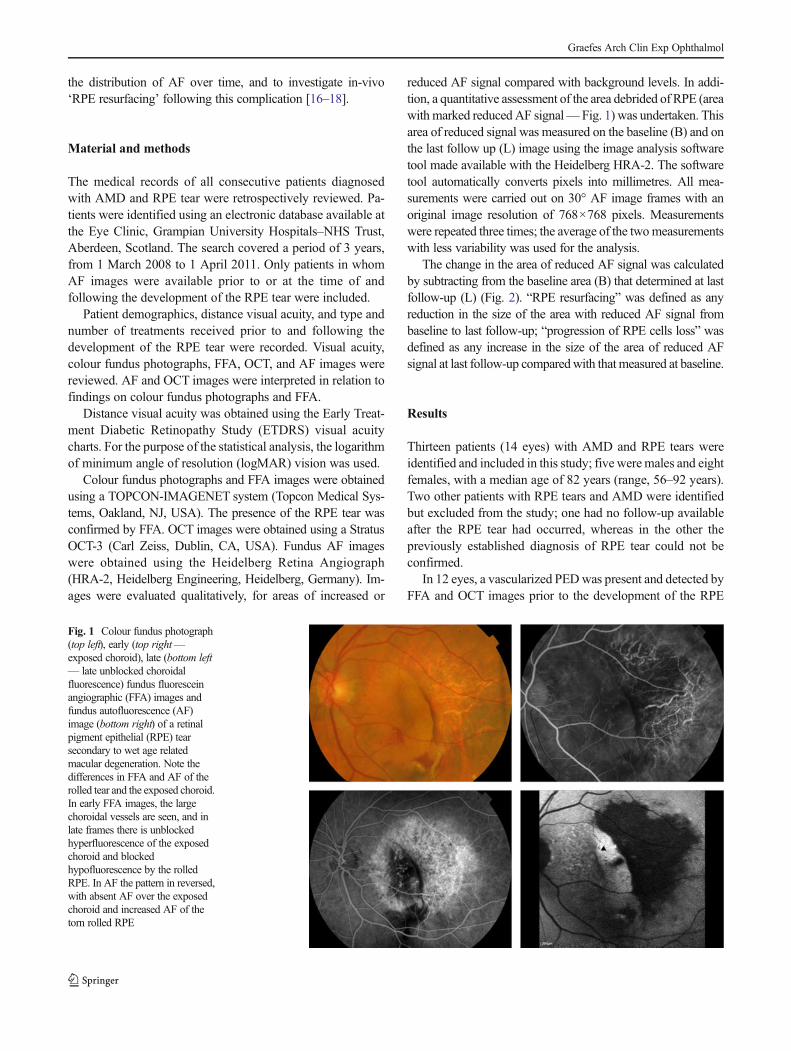
Fig. 1 Colour fundus photograph(top left), early (top right—exposed choroid), late (bottom left— late unblocked choroidalfluorescence) fundus fluoresceinangiographic (FFA) images andfundus autofluorescence (AF)image (bottom right) of a retinalpigment epithelial (RPE) tearsecondary to wet age relatedmacular degeneration. Note thedifferences in FFA and AF of therolled tear and the exposed choroid.In early FFA images, the largechoroidal vessels are seen, and inlate frames there is unblockedhyperfluorescence of the exposedchoroid and blockedhypofluorescence by the rolledRPE. In AF the pattern in reversed,with absent AF over the exposedchoroid and increased AF of thetorn rolled RPE
Graefes Arch Clin Exp Ophthalmol
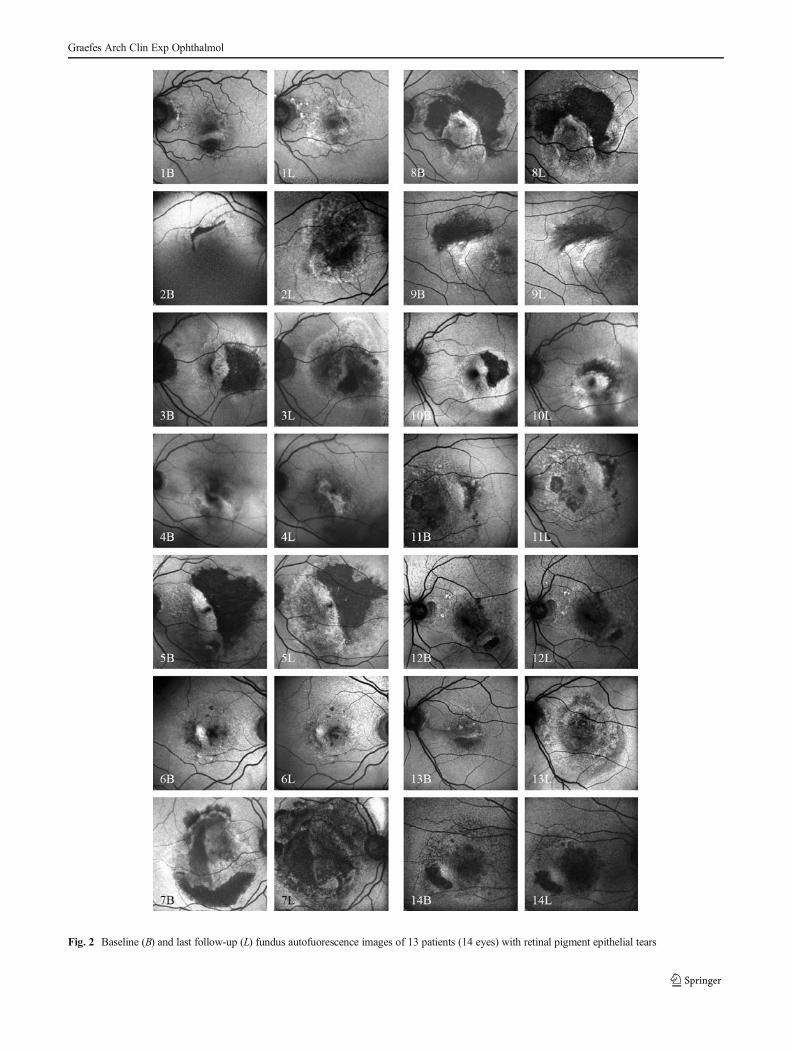
Fig. 2 Baseline (B) and last follow-up (L) fundus autofuorescence images of 13 patients (14 eyes) with retinal pigment epithelial tears
Graefes Arch Clin Exp Ophthalmol
tear; one eye had already at presentation an RPE tear, andanother had a ‘classic’ choroidal neovascular membrane(CNV) with tearing of the RPE associated to it.
Twelve eyes had been receiving treatment with ranibizumab(Genentech, USA) at the time the RPE tear occurred; all ofthese eyes continued on treatment post RPE tear. One eye wascommenced on anti-VEGF therapy post RPE tear, initially withbevacizumab and then with ranibizumab. The remaining eyewas not treated prior to or post RPE tear (Table 1).
The median pre RPE tear logMAR VA was 0.5 (Snellenequivalent, 6/12) and after a median follow-up of 11.5 monthsit decreased to logMARVA 0.8 (Snellen equivalent, 6/36). FFAimages of all patients had the typical features of an RPE tear [1].There was an area with very early hyperfluorescence (“windowdefect”) at the site of the exposed choroid, and an area ofhypofluorescence (“blocked fluorescence”) next to it, corre-sponding to the site where the torn and rolled RPE was present(Fig. 1). On OCT imaging, RPE tears were detected in 13 eyes;in one eye the tear could not be visualised. The OCT features ofthe RPE tear were discontinuity with and without ruffling, andabrupt elevation of the reflectance line corresponding to the RPE.
The median follow-up period between the baseline AFimage, obtained at the time the RPE tear had occurred, andthe last AF image, obtained at last follow-up was 11.5 months(range, 1–39 months) (Table 1). AF images revealed a well-defined area with markedly reducedAF signal corresponding tothe area debrided of RPE (Figs. 1 and 2) (“window defect” onFFA). An area with variably increased AF signal was alsodetected at the site of the rolled, torn RPE, corresponding to
the area of hypofluorescence on FFA (Figs. 1 and 2). Soon afterthe development of the RPE tear, the area of reduced AFcorresponding to the exposed choroid was homogenously dark,with distinct margins. As time went on, the margins of the areaof RPE defect became less distinct. In ten eyes, “RPEresurfacing” was noted, with a median recovery of 1.3 mm2
(range 0.03–6.78). In four eyes, “progression of RPE cells loss”occurred with a median enlargement of the area of reduced AFsignal of 0.7 mm2 (range 0.11–5.58) (Fig. 2).
Discussion
In this small series, RPE tears demonstrated characteristic fea-tures on fundus AF imaging that could be used to establish thisdiagnosis non-invasively. Thus, marked, well-defined reducedAF signal was detected at the site of the exposed Bruch’smembrane/choroid (Figs. 1 and 2), with an adjacent area ofincreased AF signal corresponding to the torn, rolled RPE.“RPE resurfacing” of the area debrided of RPE was observedover time by using in-vivo fundus AF imaging. In these cases,the recovery of the AF signal occurred centripetally, from theedge of the area of the defect towards the centre, with theexception of the border where the rolled RPE was present.
It is not clear whether RPE resurfacing occurred by slidingof RPE cells (RPE cells “stretching” to cover the debridedarea) or by proliferation and migration of adjacent RPE cells.In a study comparing abrasive and hydraulic RPE debride-ment in domestic short-haired cats, Leonard and colleagues
Table 1 Patient data
Pt Age inyears
Eye Dx Pre/postanti-VEGF
BaselineVA LogMAR
Last F/UVA LogMAR
Baseline AF area(mm2) of reducedsignal (B)
Last F/U area(mm2) ofreduced signal
AF area ofsignal change(B-last F/U)
P & R F/Umonths
1 79 LE VPED L/L 0.4 0.18 1.67 0.21 1.46 R 22
2 89 RE Classic 0/A, L 0.9 1.17 1.18 2.01 0.83 P 23
3 89 LE VPED L/L 0.6 1 6.73 2.87 3.86 R 24
4 92 LE RPE Tear L/L 1 1 0.16 0.08 0.08 R 5
5 78 LE VPED L/L 1 0.6 14.96 13.15 1.81 R 12
6 83 RE VPED L/L 0.3 0.4 1.35 0.20 1.15 R 11
7 78 RE VPED 0/0 0.77 1.07 5.24 10.82 5.58 P 39
8 78 LE VPED L/L 0.3 0.9 13.45 6.67 6.78 R 29
9 56 RE VPED L/L 0.69 0.4 6.96 2.34 4.62 R 8
10 83 LE VPED L/L 0.4 1 2.09 1.52 0.57 R 4
11 82 LE VPED L/L 0.07 0.18 0.33 0.93 0.6 P 2
12 83 LE VPED L/L 0.18 0.4 0.44 0.41 0.03 R 1
13 78 LE VPED L/L 0.07 0.7 0.70 0.57 0.13 R 29
14 82 RE VPED L/L 1.07 1 1.89 2.00 0.11 P 10
Pt patient; RE right eye; LE left eye, Dx diagnosis, VPED vascularised pigment epithelial detachment, Pre/post anti-VEGF treatment prior to / treatmentfollowing the development of retinal pigment epithelial (RPE) tear; L ranibizumab,Abevacizumab, 0no treatment; number of treatment; VAvisual acuity;F/U follow-up; RRPE resurfacing; P progression of RPE atrophy
Graefes Arch Clin Exp Ophthalmol

[19] showed that the gentler hydraulic debridement was asso-ciated with nearly normal resurfacing of the Bruch’s mem-brane. The critical determinant of RPE resurfacing ap-peared to be the presence or absence of damage of theBruch’s membrane and the chorio-capillaries. The pres-ervation of these two structures seemed to be morecompatible with an adequate RPE resurfacing. It shouldbe noted that under these experimental conditions, theRPE surrounding the area of damage would be expectedto be “healthy”, which is unlikely to be the case inpatients with AMD. Furthermore, it is likely that thedepth of the cleavage plane may have also an impact onthe degree of RPE resurfacing that may take place.Thus, it has been found that the RPE basement mem-brane is more conducive for RPE resurfacing than thedeeper collagen layer of Bruch’s membrane [20]. Incats, it is reported that RPE cells resurface denudedBruch’s membrane by cell proliferation and migration[19]. It has also been noted that RPE cells repopulatefrom edge to centre rather than from residual cellsremaining in the debrided zone centers [19]. There isalso evidence from human eyes of migration of periph-eral RPE cells to compensate for the death of macularRPE cells [21]. The current in-vivo observations seemto support findings of the above mentioned experimentalwork. Differences in the site of the cleavage plane, inthe healthiness of Bruch’s membrane, and in the size ofthe RPE tear among patients in this series may havedetermined the differences observed in the occurrenceand extension of RPE resurfacing.
In this series, 13 eyes were treated post RPE tear with anti-VEGF; of these, the vision improved in four, remained un-changed in two and deteriorated in eight. This is in keepingwith the findings of Cunningham et al. of better visual out-comes in patients with RPE tears continued on VEGF inhibi-tion [11]. Of the four patients with “progression of RPE loss”,three lost vision. In the ten patients with “RPE resurfacing”,three had visual improvement, one had stable vision and sixlost vision. Caramoy et al. also have recently reported evi-dence of RPE tissue remodelling in RPE tears [22]. Theyindicate that smaller RPE tears may resurface but the largertears may not. In this series, where there were smaller RPEtears, more RPE resurfacing was observed.
Therefore, it could be concluded that RPE tears needcareful evaluation for size and location. To determine this,fundus autofluorescence is valuable, has the advantage ofbeing a non-invasive imaging modality and can be also usedto monitor RPE recovery. This information could in turnunderpin therapeutic decisions on VEGF inhibition in thesepatients.
Conflict of interests The authors have no financial/conflicting intereststo disclose.
References
1. Hoskin A, Bird AC, Sehmi K (1981) Tears of detached retinalpigment epithelium. Br J Ophthalmol 65:417–422
2. Gass JDM (1984) Pathogenesis of tears of the retinal pigment epi-thelium. Br J Ophthalmol 68:513–519
3. Barondes MJ, Pagliarini S, Chisholm IH et al (1992) Controlled trialof laser photocoagulation of pigment epithelial detachments in theelderly: 4 year review. Br J Ophthalmol 76:5–7
4. Gelisken F, Indhofen W, Partsch M et al (1984) Retinal pigmentepithelial tea after photodynamic therapy for choroidal neovascular-ization. Am J Ophthalmol 98:700–706
5. Goldstein M, Heilweil G, Barak A et al (2005) Retinal pigmentepithelial tear following photodynamic therapy for choroidal neovas-cularization secondary to AMD. Eye 19(12):1315–1324
6. Meyer CH, Mennel S, Schmidt JC, Kroll P (2006) Acute retinalpigment epithelial tear following intravitreal bevacizumab (Avastin)injection for occult choroidal revascularization secondary to agerelated macular degeneration. Br J Ophthalmol 90:1207–1208
7. Carvounis PE, Kopel AC, Benz MS (2007) Retinal pigment epithe-lium tears following ranibizumab for exudative age related maculardegeneration. Am J Ophthalmol 143:504–505
8. Bakri SJ, Kitzmann AS (2007) Retinal pigment epithelial tear afterintravitreal ranibizumab. Am J Ophthalmol 143:505–507
9. Chan CK, Meyer CH, Gross JG et al (2007) Retinal pigment epithe-lial tears after intravitreal bevacizumab injection for neovascular age-related macular degeneration. Retina 27:541–551
10. Chang LK, Sarraf D (2007) Tears of the retinal pigment epithelium:An old problem in a new era. Retina 27(5):523–533
11. Cunningham ET Jr, Feiner L, Chung C et al (2011) Incidence ofretinal pigment epithelial tears after intravitreal ranibizumab injectionfor neovascular age-related macular degeneration. Ophthalmology118(12):2447–2452
12. Karadimas P, Paleokastritis GP, Bouzas EA (2006) Fundus autoflu-orescence imaging findings in retinal pigment epithelial tear. Eur JOphthalmol 16(5):767–769
13. von Ruckmann A, Fitzke FW, Bird AC (1995) Distribution of fundusautofluorescence with a scanning laser ophalmoscope. Br JOphthalmol 79:407–412
14. Delori FC, Dorey CK, Staurenhi G et al (1995) In vivo fluorescenceof the ocular fundus exhibits retinal pigment epithelium lipofuscincharacteristics. Invest Ophthalmol Vis Sci 36(3):718–729
15. Schmitz-Valckenberg S, Fleckenstein M, Scholl HP, Holtz FG (2009)Fundus autofluorescence and progression of age-related maculardegeneration. Surv Ophthalmol 54(1):96–117
16. Caramoy A, Kirchhof B, Fauser S (2011) Retinal pigment epitheliumtears secondary to age-related macular degeneration. ArchOphthalmol 129(5):575–579
17. Peiretti E, Iranmanesh R, Lee JJ et al (2006) Repopulation of the retinalpigment epithelium after pigment epithelial rip. Retina 26(9):1097–1099
18. Chuang EL, Bird AC (1998) Repair after tears of the retinal pigmentepithelium. Eye 2:106–113
19. Leonard DS, Zhang XG, Panozzo G et al (1997) Clinicopathologicalcorrelation of localized retinal pigment epithelium debridement.Invest Ophthalmol Vis Sci 38:1094–1109
20. WangH,NinomiyaY, Sugino IK, ZarbinMA (2003) Retinal pigmentepithelium wound healing in human Bruch’s membrane explants.Invest Ophthalmol Vis Sci 44:2199–2210
21. Del Priore LV, Kuo YH, Tezel TH (2002) Age related changes inhuman RPE cell density and apoptosis propotion in situ. InvestOphthalmol Vis Sci 43(10):3312–3318
22. Caramy A, Fauser S, Kirchhof B (2012) Fundus autofluorescenceand spectral domain optical coherence tomography findings suggest-ing tissue remodelling in retinal pigment epithelium tear. Br JOphthalmol 96:1211–1216
Graefes Arch Clin Exp Ophthalmol














![SPECTRALIS - INNOVA · Fundus Autofluorescence in the Abca4[-]/[-] Mouse Model of Stargardt Disease - Correlation With Accumulation of A2E, Retinal Function, and Histology doi: 10.1167/iovs.13-11688](https://img.pdfslide.net/doc/110x75/5ec1d3ad12d1a659545b86a4/spectralis-innova-fundus-autofluorescence-in-the-abca4-mouse-model-of-stargardt.jpg)














