Embed Size (px)
Citation preview

A cause oriented approach to
obesity management
Gabriel I. Uwaifo, MD, FACP, FACE, FTOS,
Department of Endocrinology, diabetes, metabolism and weight
management,
Ochsner medical center

PRESENTATION
OBJECTIVE;
TO DISCUSS THE ROLE OF CAUSES,
COMPLICATIONS AND
ASSOCIATIONS OF OBESITY IN ITS
EFFECTIVE MANAGEMENT
Presentation outline•Detail classification and causes of
obesity.
•Detail complications and associations
of obesity
•Describe relationship between
causes, complications and
associations of obesity with
management strategies
➢Obesity is not one disease but a common final
pathway for many different diseases and thus no two
obese subjects are exactly the same making
individualized, nuanced evaluation and management
key to therapeutic success.
➢The effective management of obesity requires
careful attention to the 5 C’s
▪ The Classification of obesity (Types)
▪ The Causes of obesity (etiologic factors)
▪ The Complications/Consequences of obesity
▪ The Comorbidities/associations of obesity
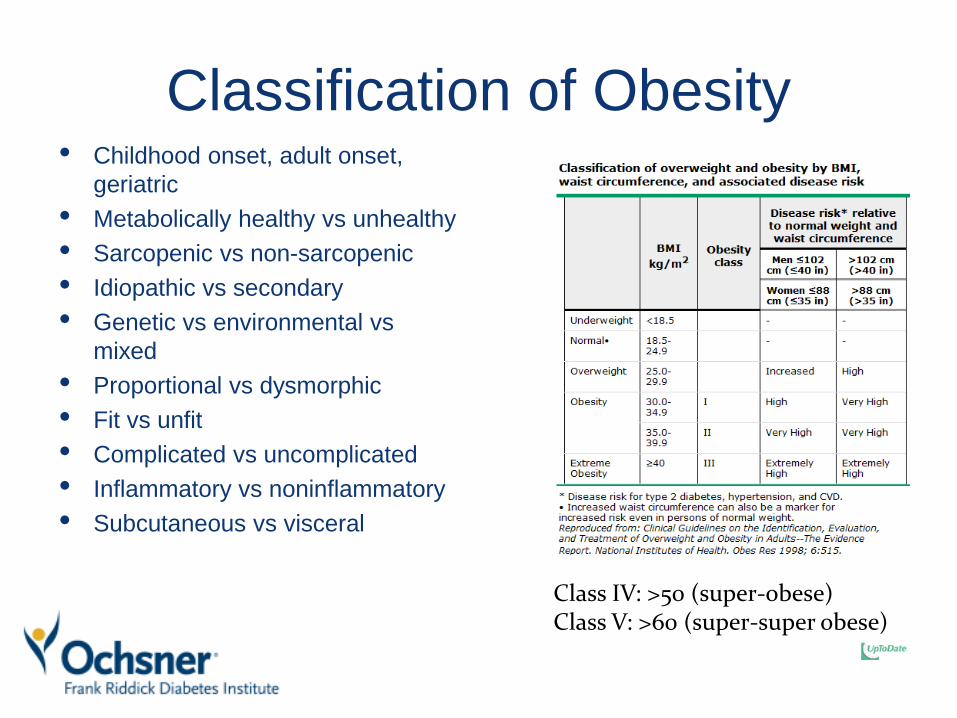
Classification of Obesity• Childhood onset, adult onset,
geriatric
• Metabolically healthy vs unhealthy
• Sarcopenic vs non-sarcopenic
• Idiopathic vs secondary
• Genetic vs environmental vs
mixed
• Proportional vs dysmorphic
• Fit vs unfit
• Complicated vs uncomplicated
• Inflammatory vs noninflammatory
• Subcutaneous vs visceral
Class IV: >50 (super-obese)Class V: >60 (super-super obese))
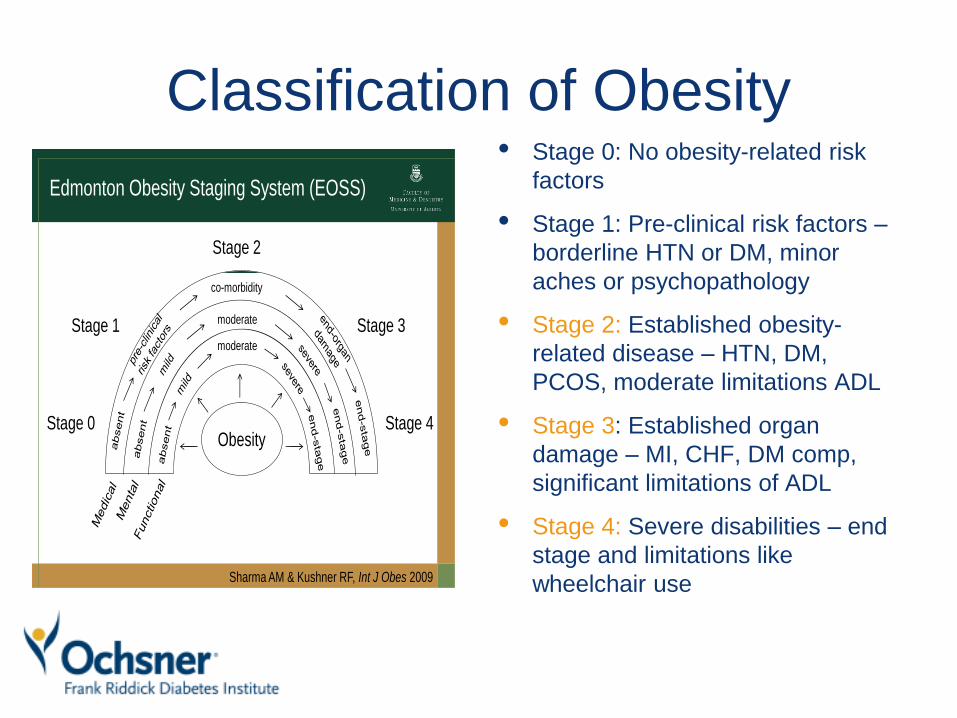
Classification of Obesity• Stage 0: No obesity-related risk
factors
• Stage 1: Pre-clinical risk factors –
borderline HTN or DM, minor
aches or psychopathology
• Stage 2: Established obesity-
related disease – HTN, DM,
PCOS, moderate limitations ADL
• Stage 3: Established organ
damage – MI, CHF, DM comp,
significant limitations of ADL
• Stage 4: Severe disabilities – end
stage and limitations like
wheelchair use
Edmonton Obesity Staging System (EOSS)
Stage 0
Sharma AM & Kushner RF, Int J Obes 2009
Stage 1
Stage 2
Stage 3
Stage 4
co-morbidity
moderate
moderate
Obesity
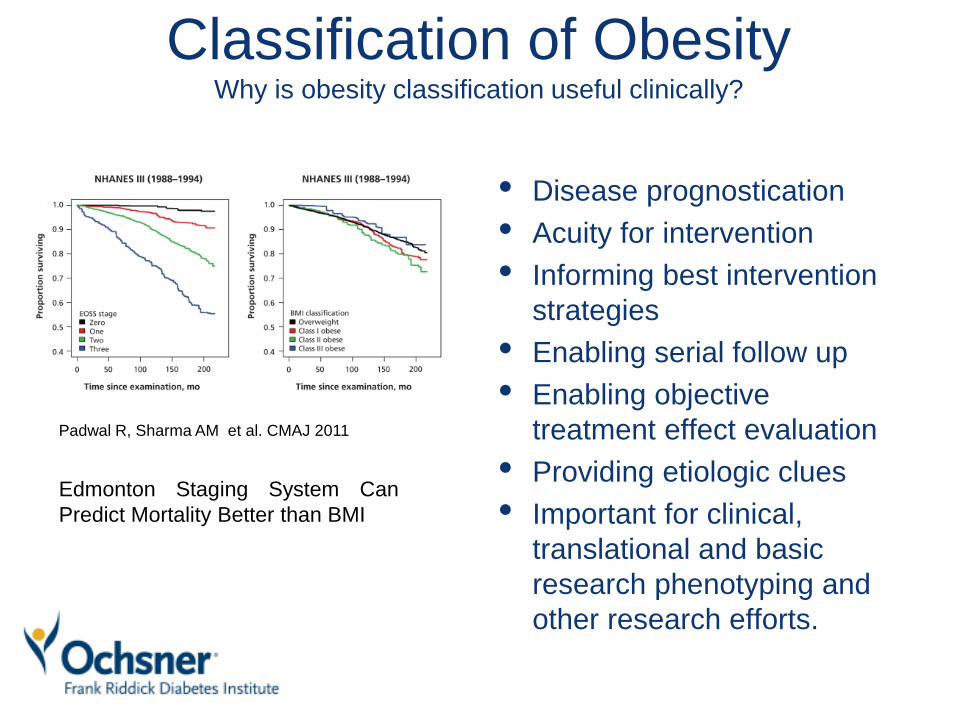
Classification of ObesityWhy is obesity classification useful clinically?
• Disease prognostication
• Acuity for intervention
• Informing best intervention
strategies
• Enabling serial follow up
• Enabling objective
treatment effect evaluation
• Providing etiologic clues
• Important for clinical,
translational and basic
research phenotyping and
other research efforts.
Edmonton Staging System Can
Predict Mortality Better than BMI
Padwal R, Sharma AM et al. CMAJ 2011
Causes of Obesity
• Concepts of etiology, predisposition and
contributory factors.
• The concept of multiplicity of etiologies,
predispositions and contributors
• The concept of nature vs nuture; genetics vs
environment and the epigenetic bridge between
them
• The impact for the clinician; one size does not fit
all.
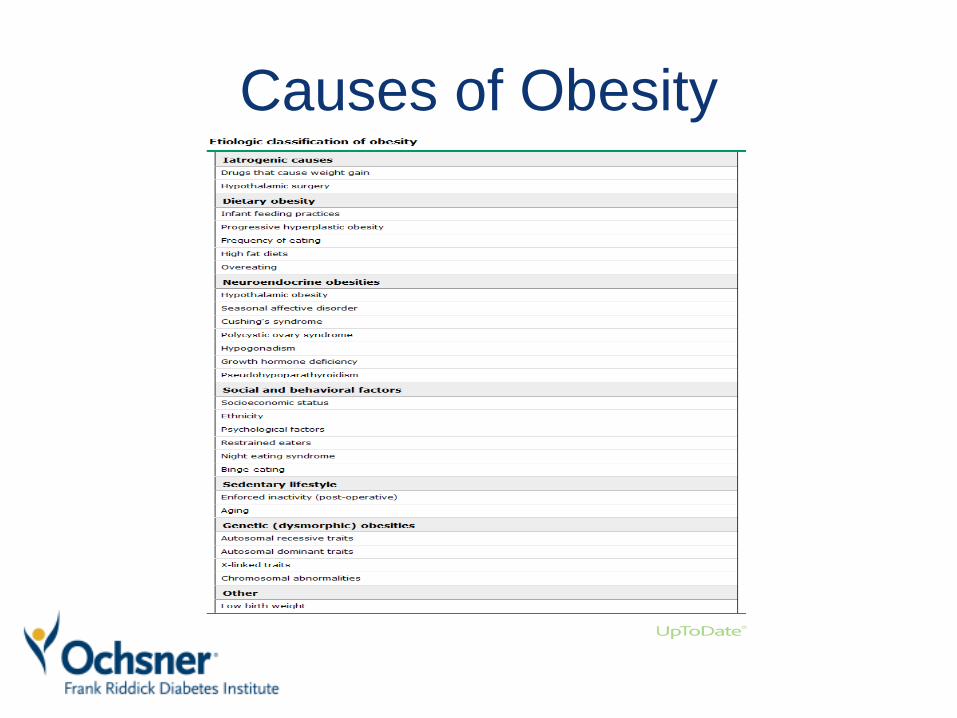
Causes of Obesity
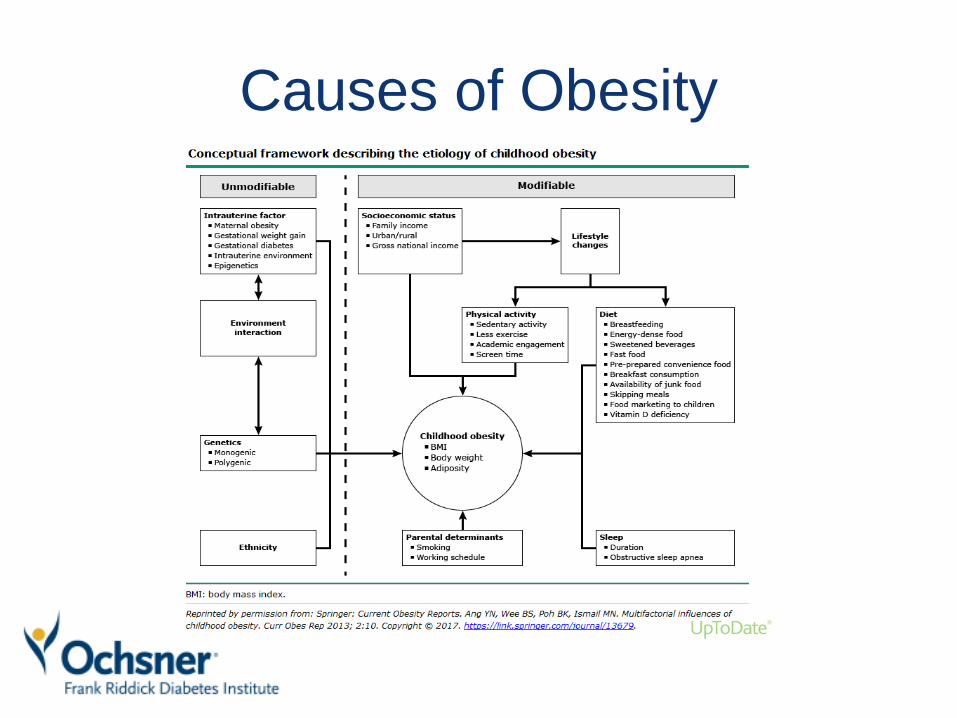
Causes of Obesity
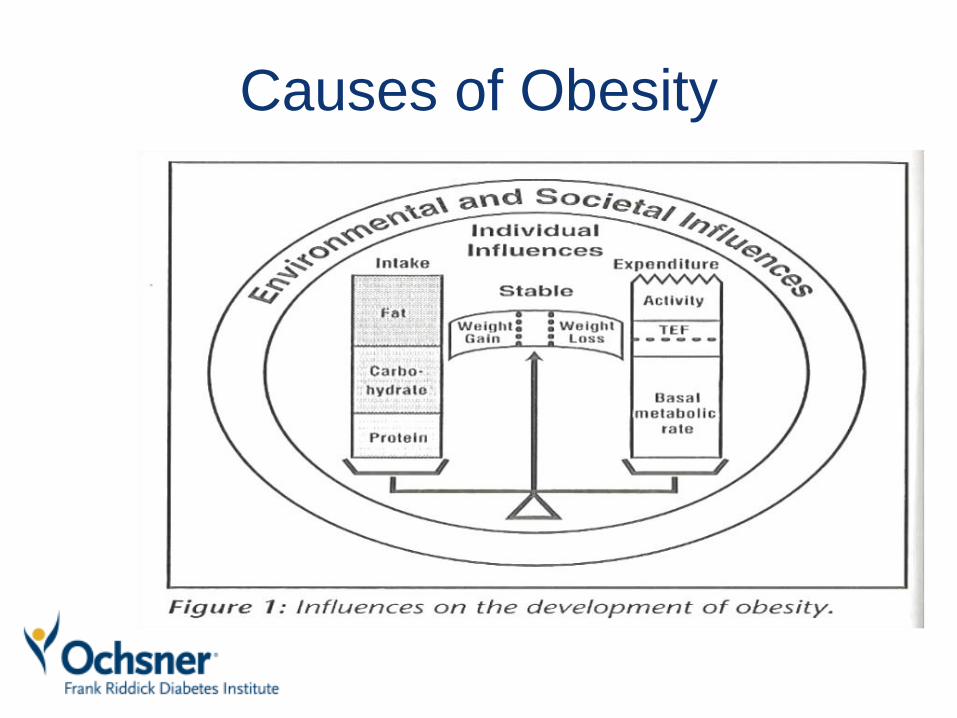
Causes of Obesity

Causes of Obesity

Causes of Obesity

Causes of Obesity; behavioral
considerations• Physical activity and exercise
• Sleep deprivation and sleep
disorders
• Pregnancy
• Dietary patterns
• Eating disorders
• Psychopathology
• Smoking cessation
• Sedentary activity, Screen time
• Alcohol consumption
• Substance abuse
Causes of Obesity;
endocrinopathies• Hypercortisolemia and Cushing’s
syndrome
• PCOS
• Hypoparathyroidism
• Hypopituitarism
• Hypogonadism
• GH deficiency
• Hypoglycemic syndromes
• Diabetes Mellitus
• Hypothyroidism **
• Acromegaly and gigantism
syndromes
• The chicken vs the
egg concept; cause,
consequence or both
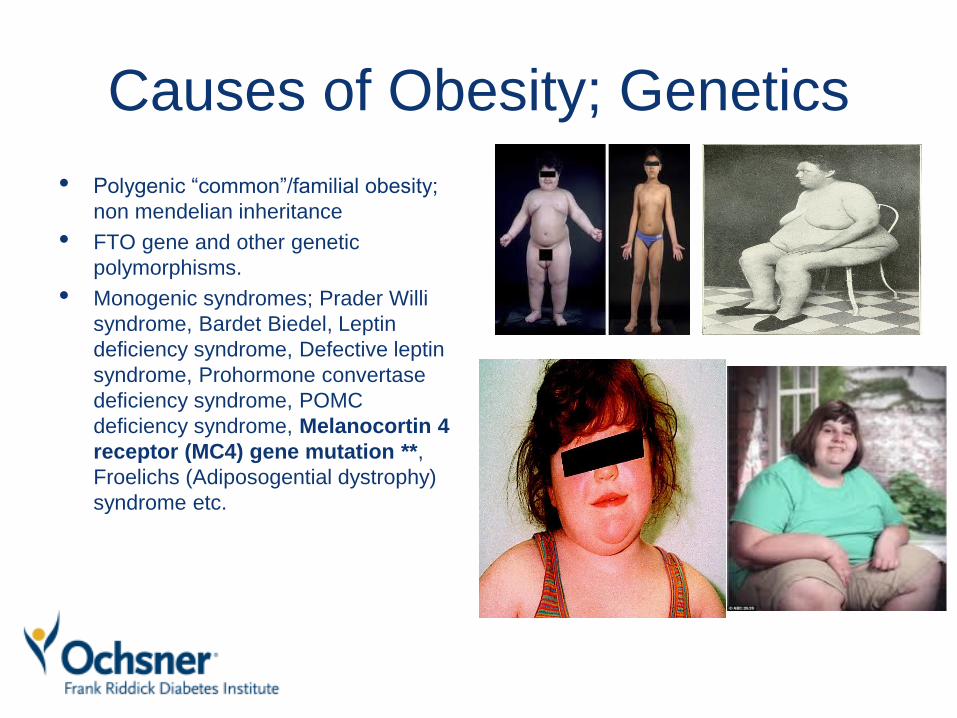
Causes of Obesity; Genetics
• Polygenic “common”/familial obesity;
non mendelian inheritance
• FTO gene and other genetic
polymorphisms.
• Monogenic syndromes; Prader Willi
syndrome, Bardet Biedel, Leptin
deficiency syndrome, Defective leptin
syndrome, Prohormone convertase
deficiency syndrome, POMC
deficiency syndrome, Melanocortin 4
receptor (MC4) gene mutation **,
Froelichs (Adiposogential dystrophy)
syndrome etc.

Causes of Obesity;
Hypothalamic Obesity
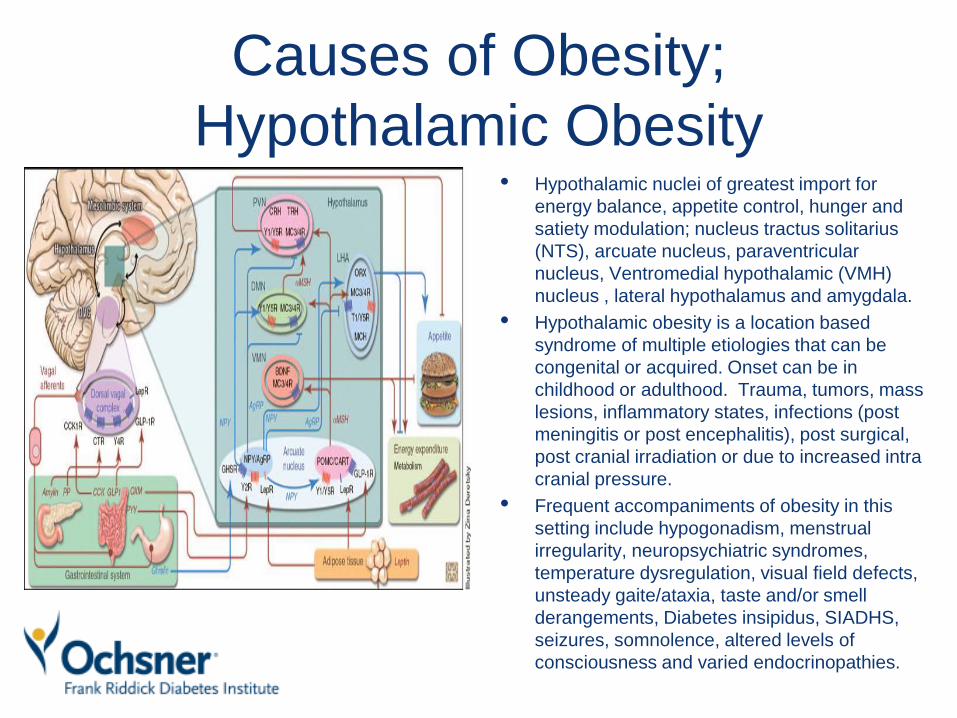
Causes of Obesity;
Hypothalamic Obesity• Hypothalamic nuclei of greatest import for
energy balance, appetite control, hunger and
satiety modulation; nucleus tractus solitarius
(NTS), arcuate nucleus, paraventricular
nucleus, Ventromedial hypothalamic (VMH)
nucleus , lateral hypothalamus and amygdala.
• Hypothalamic obesity is a location based
syndrome of multiple etiologies that can be
congenital or acquired. Onset can be in
childhood or adulthood. Trauma, tumors, mass
lesions, inflammatory states, infections (post
meningitis or post encephalitis), post surgical,
post cranial irradiation or due to increased intra
cranial pressure.
• Frequent accompaniments of obesity in this
setting include hypogonadism, menstrual
irregularity, neuropsychiatric syndromes,
temperature dysregulation, visual field defects,
unsteady gaite/ataxia, taste and/or smell
derangements, Diabetes insipidus, SIADHS,
seizures, somnolence, altered levels of
consciousness and varied endocrinopathies.
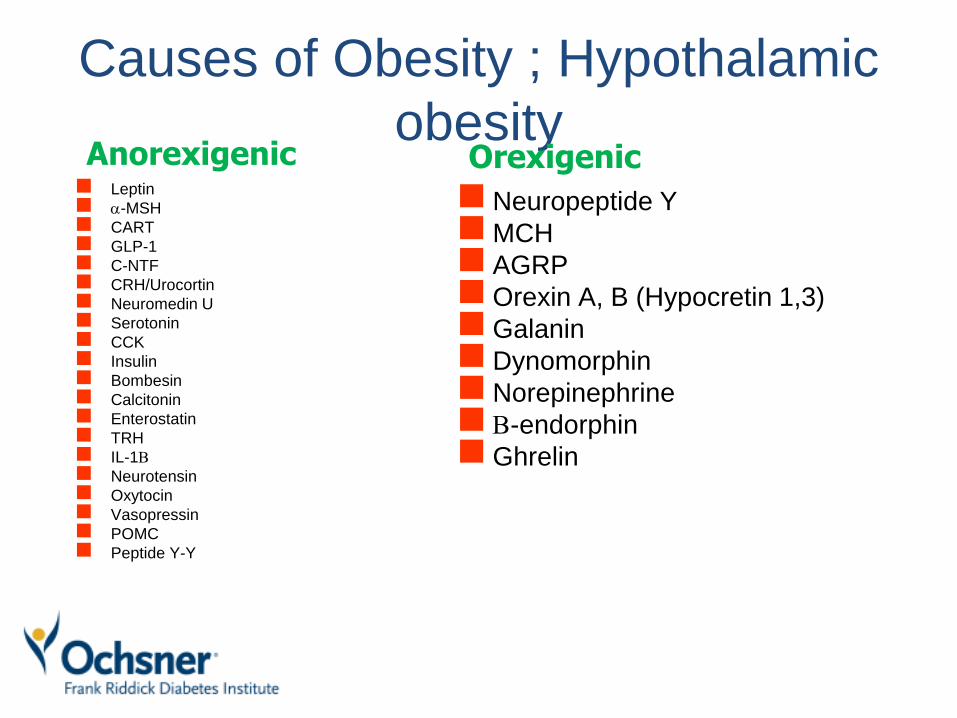
Causes of Obesity ; Hypothalamic
obesity◼ Leptin
◼ a-MSH
◼ CART
◼ GLP-1
◼ C-NTF
◼ CRH/Urocortin
◼ Neuromedin U
◼ Serotonin
◼ CCK
◼ Insulin
◼ Bombesin
◼ Calcitonin
◼ Enterostatin
◼ TRH
◼ IL-1B
◼ Neurotensin
◼ Oxytocin
◼ Vasopressin
◼ POMC
◼ Peptide Y-Y
◼ Neuropeptide Y
◼MCH
◼ AGRP
◼Orexin A, B (Hypocretin 1,3)
◼Galanin
◼ Dynomorphin
◼ Norepinephrine
◼ B-endorphin
◼Ghrelin
Anorexigenic Orexigenic

Causes of obesity; Mental
Health disorders• Depression; melancholic depression and other
syndromic unipolar depression as opposed to
bipolar disorder
• Eating disorders; Night eating disorder, Bulimia
• Seasonal affective disorder
• Schizophrenia
• Certain personality disorders
• The question of the chicken vs the egg; cause or
consequence or both.
Causes of Obesity; other factors• Socioeconomic status
• Gestational history
• Breast feeding history and infantile feeding history
• Ethnicity and racial disparities
• The microbiome and infective etiologies of obesity ***
• The role of viruses (adenovirus 36 and others in
obesity)
• The role of metabolic endotoxemia in obesity
• The role of antimicrobials in obesity.
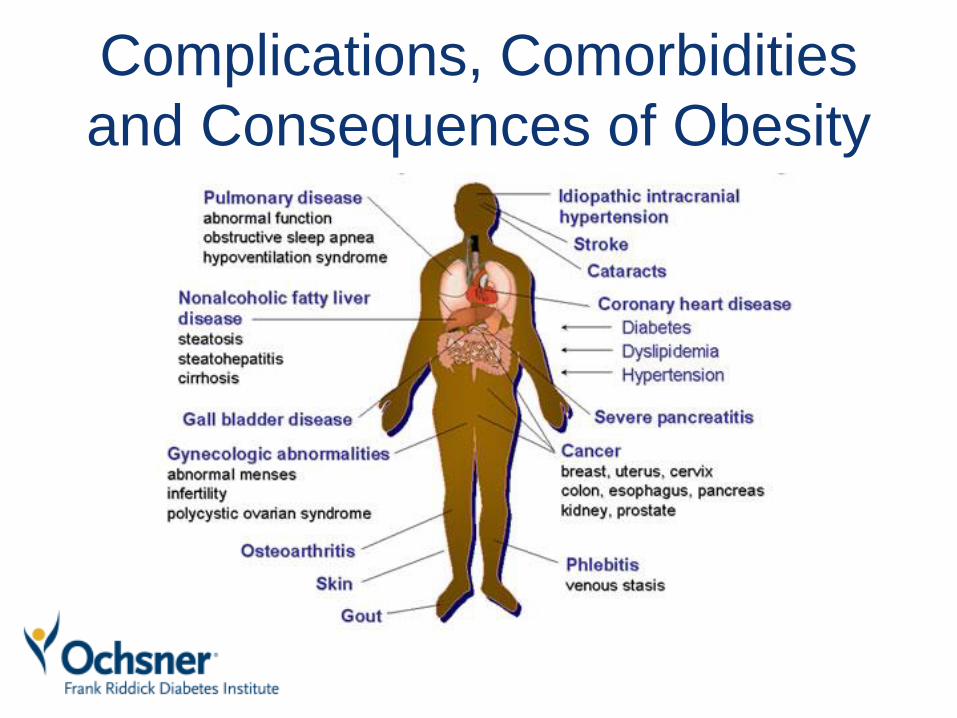
Complications, Comorbidities
and Consequences of Obesity
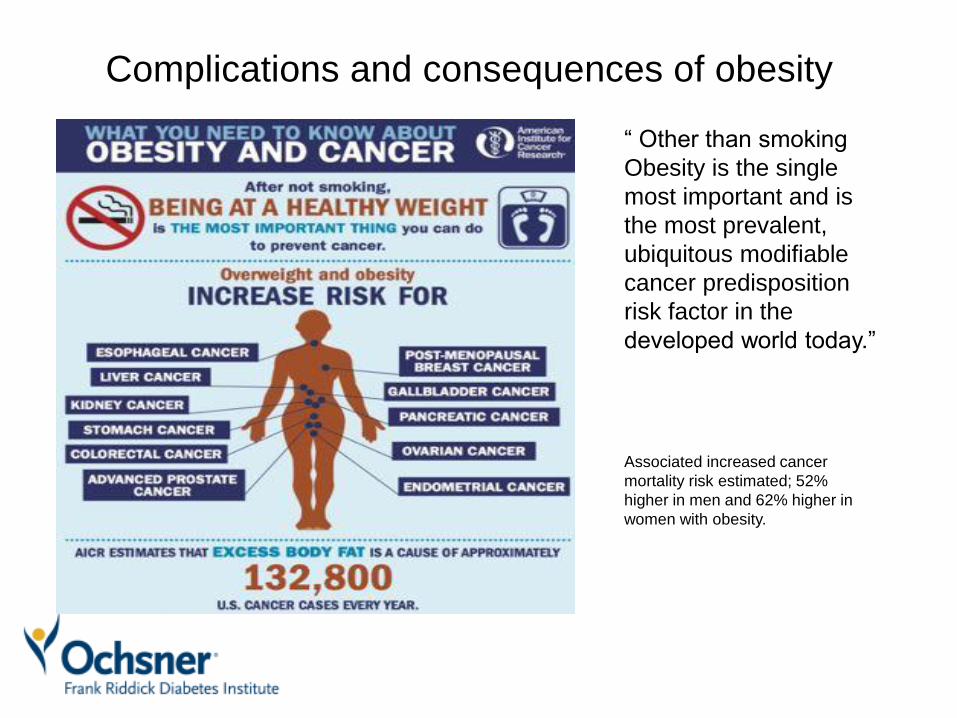
Complications and consequences of obesity
Associated increased cancer
mortality risk estimated; 52%
higher in men and 62% higher in
women with obesity.
“ Other than smoking
Obesity is the single
most important and is
the most prevalent,
ubiquitous modifiable
cancer predisposition
risk factor in the
developed world today.”

Complications, Comorbidities
and Consequences of Obesity
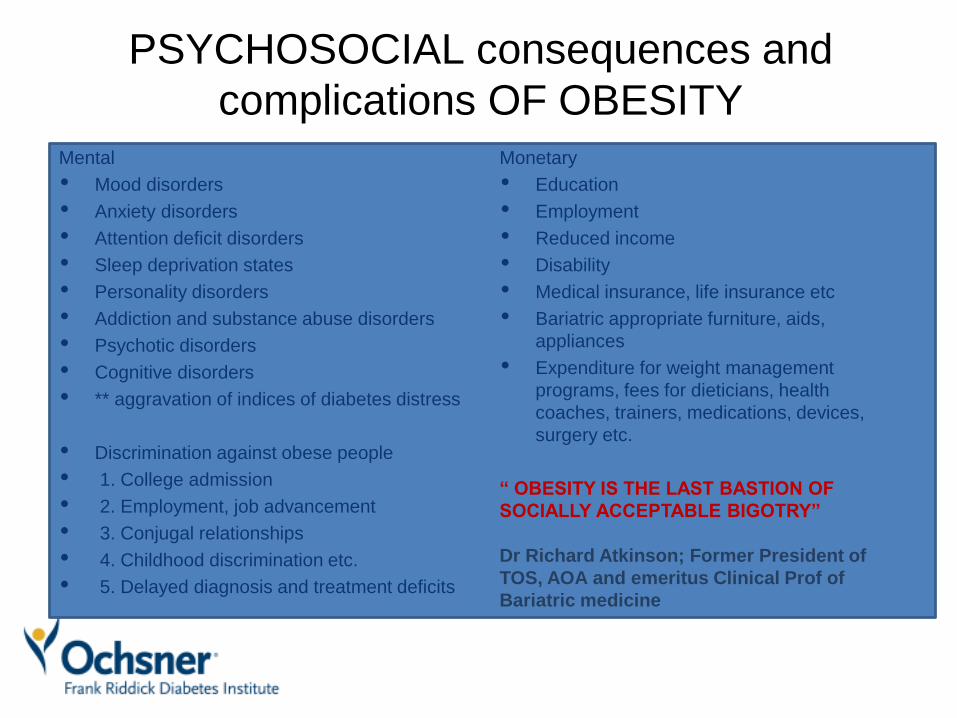
PSYCHOSOCIAL consequences and
complications OF OBESITYMental
• Mood disorders
• Anxiety disorders
• Attention deficit disorders
• Sleep deprivation states
• Personality disorders
• Addiction and substance abuse disorders
• Psychotic disorders
• Cognitive disorders
• ** aggravation of indices of diabetes distress
• Discrimination against obese people
• 1. College admission
• 2. Employment, job advancement
• 3. Conjugal relationships
• 4. Childhood discrimination etc.
• 5. Delayed diagnosis and treatment deficits
Monetary
• Education
• Employment
• Reduced income
• Disability
• Medical insurance, life insurance etc
• Bariatric appropriate furniture, aids,
appliances
• Expenditure for weight management
programs, fees for dieticians, health
coaches, trainers, medications, devices,
surgery etc.
“ OBESITY IS THE LAST BASTION OF
SOCIALLY ACCEPTABLE BIGOTRY”
Dr Richard Atkinson; Former President of
TOS, AOA and emeritus Clinical Prof of
Bariatric medicine
Concluding remarks• Obesity is a complex syndrome that is the final common pathway of many
different chronic cardiometabolic diseases.
• Developing a rationale effective management plan for the individual patient
requires careful attention to identifying the causes, contributors,
comorbidities and complications of obesity for the individual patient.
• Given the complexity of determining the often multifactorial etiology of
obesity in patients a multidisciplinary approach to the clinical evaluation and
care of these patients is invariably a necessity.
• A comprehensive history and examination including medication inventory,
gestation and birth history, behavioral, psychosocial, dietary and weight
history can provide valuable insight to the major contributors and etiologies
of obesity in the individual patient thus guiding a rational management plan.
• No two obese patients are likely to have the same effective management
plan. These must be customized and nuanced based on cause oriented
approach.
THANK YOU VERY MUCH FOR
YOUR KIND ATTENTION
Questions???, Comments???
Bibliography and References• Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US
adults, 1999-2000. JAMA 2002; 288:1723.
• Bardia A, Holtan SG, Slezak JM, Thompson WG. Diagnosis of obesity by primary care physicians and impact on obesity management. Mayo Clin Proc 2007; 82:927.
• Tsai AG, Wadden TA. In the clinic: obesity. Ann Intern Med 2013; 159:ITC3.
• Lyznicki JM, Young DC, Riggs JA, et al. Obesity: assessment and management in primary care. Am Fam Physician 2001; 63:2185.
• Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014; 129:S102.
• Bray GA, Frühbeck G, Ryan DH, Wilding JP. Management of obesity. Lancet 2016; 387:1947.
• Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA 2014; 311:74.
• Ozanne SE. Epigenetic signatures of obesity. N Engl J Med 2015; 372:973.
• Bray GA. A Guide to Obesity and the Metabolic Syndrome, CRC Press, Boca Raton, FL 2011.
• Leslie WS, Hankey CR, Lean ME. Weight gain as an adverse effect of some commonly prescribed drugs: a systematic review. QJM 2007; 100:395.
• Hochberg I, Hochberg Z. Expanding the definition of hypothalamic obesity. Obes Rev 2010; 11:709.
• Knudsen N, Laurberg P, Rasmussen LB, et al. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. J ClinEndocrinol Metab 2005; 90:4019.