Embed Size (px)
Citation preview

Gabriel
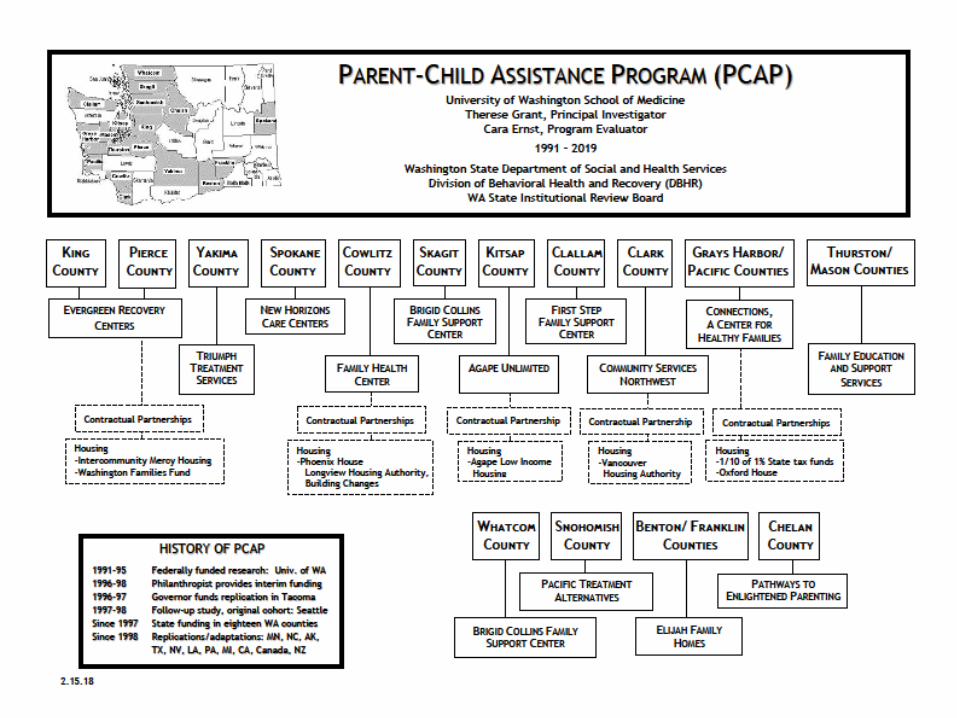
WA State DSHS Division of Behavioral Health and Recovery (DBHR)in conjunction with
University of Washington, Evergreen Recovery Centers, Triumph Treatment Services, New Horizon Care Centers, Family Health Center, Brigid Collins Family Support Center, First Step Family Support Center, Agape Unlimited, Community
Services Northwest, Connections ~ A Center for Healthy Families, Family Education and Support Services, Pacific Treatment Alternatives, Elijah Family Homes, and
Pathways to Enlightened Parenting
http://depts.washington.edu/pcapuw/
Washington State Parent Child Assistance Program (PCAP)
King, Pierce, Yakima, Spokane, Cowlitz, Skagit, Clallam, Kitsap, Clark, Grays Harbor/Pacific, Thurston/Mason, Whatcom, Snohomish,
Benton/Franklin and Chelan Counties
The Problem
Possible effects of prenatal exposure on the child’s health
Likelihood of a compromised home environment
Likelihood that these mothers will have more exposed, affected children
These problems are costly to society and are preventable
Maternal alcohol and drug use puts children at risk because of
An intensive, 3-year home visitation and
case management program
for high risk women who abuse
alcohol/drugs during pregnancy
Serving nearly 1,300 families in eighteen WA State counties
Over 40 PCAP sites located in other states and Canada
Parent-Child Assistance Program (PCAP) 1991- present
To help mothers…
Complete substance abuse treatment, stay in recovery
Build healthy family lives
Prevent future alcohol/drug exposed births
Parent-Child Assistance Program
Primary Aims:
History of PCAP
1991-95 Federally funded research: University of Washington
1996-97 Philanthropist provides interim funding
1996-97 Governor funds replication site in Tacoma
Since 1997 State funding, now in eighteen WA counties
Since 1998 Replications in U.S.: MN, NC, AK, TX, NV, LA, PA, MI, CA. International: 40 sites in Canada
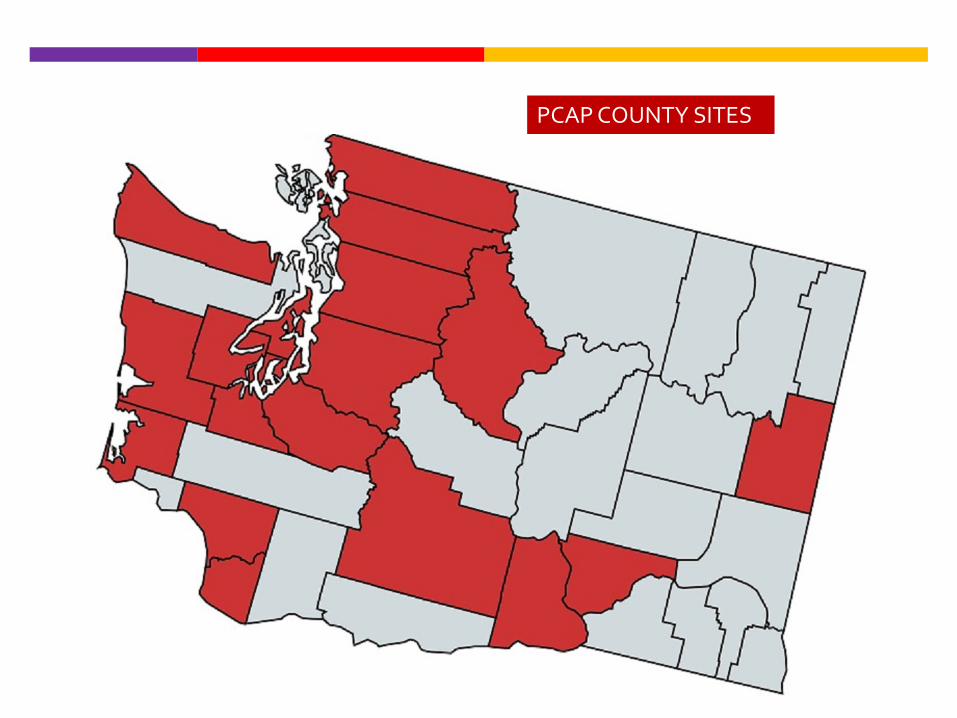
PCAP COUNTY SITES

2012: Best Practice by federal Association of Maternal & Child Health Programs (AMCHP)
2010 , 2013, 2014: California Evidence-Based Clearinghouse for Child Welfare (CEBC)
2005, 2010: Office of Juvenile Justice and Delinquency Prevention’s (OJJDP) Model Programs Guide
August 2004: Substance Abuse and Mental Health Services Administration (SAMHSA) Exemplary Substance Abuse Prevention Award
1997 and 1998: Drug Strategies, Washington D.C. Policy Research Institute
PCAP National Recognition

What do we know about mothers who abuse alcohol and drugs?
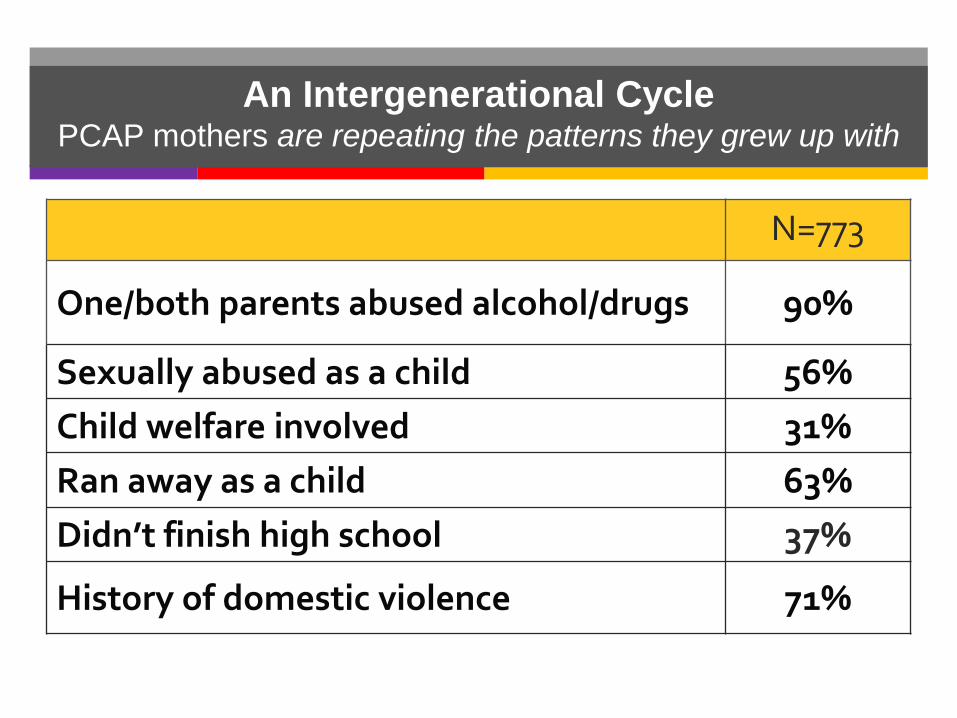
An Intergenerational CyclePCAP mothers are repeating the patterns they grew up with
N=773
One/both parents abused alcohol/drugs 90%
Sexually abused as a child 56%Child welfare involved 31%Ran away as a child 63%Didn’t finish high school 37%
History of domestic violence 71%

The PCAP Model
Offers long-term outreach and engagement to clients
Is based on relational theory, motivational interviewing, harm reduction concepts
Provides structured goal setting, family support, and consistent coaching
The PCAP Model
Case Managers B.A. degrees, highly trained, closely supervised Have caseloads of 16 families Conduct home visits 2x /month for 3 years Connect families with comprehensive community
services, coordinate services, transport as necessary
Are role models who inspire hope

14
Washington State PCAP
PCAP Annual Work Session

PCAP Conceptual Framework
Relational Theory: Positive, nonjudgmental interpersonal relationships within the intervention and recovery settings are critical. “Having a person to talk to who really cares.”
Stages of Change/ Motivational Interviewing: Clients will be at different stages of readiness for change. Helping clients motivate for change is a process that occurs within the context of interpersonal relationships.
Harm Reduction: Any steps toward decreased risk are steps in the right direction. Clients are not asked to leave the program because of relapse or setbacks.
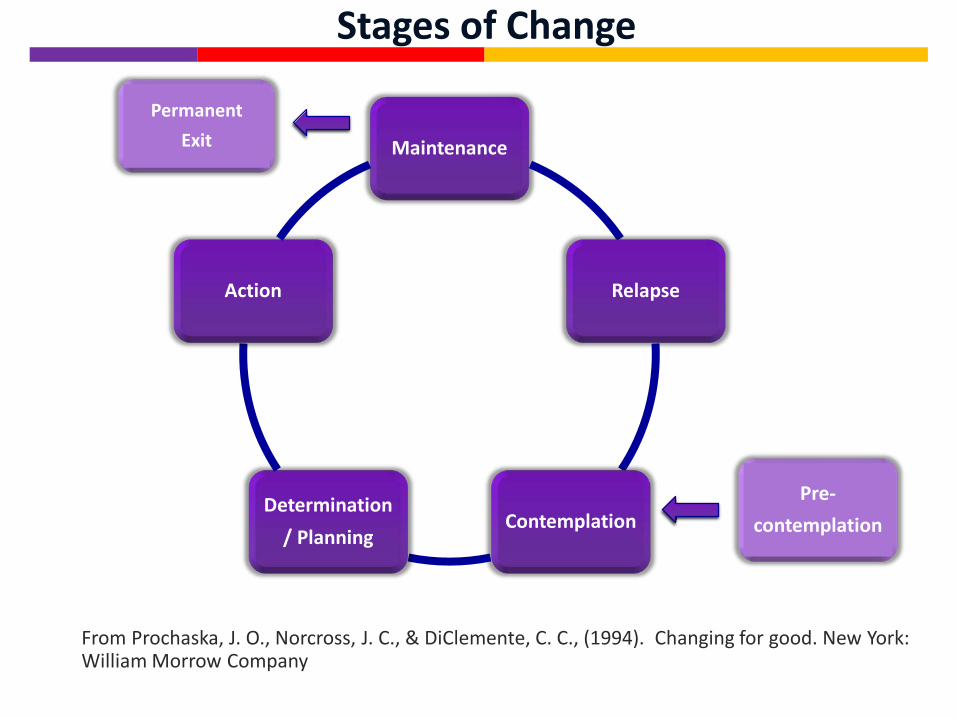
Stages of Change
From Prochaska, J. O., Norcross, J. C., & DiClemente, C. C., (1994). Changing for good. New York: William Morrow Company
Maintenance
Relapse
ContemplationDetermination
/ Planning
Action
Permanent Exit
Pre-contemplation
Self-Efficacy
17
An individual’s belief in her/his ability to accomplish the behaviors required to produce
desired outcomes.
A client’s expectations about self-efficacy are influenced most powerfully
by her own history of accomplishment.
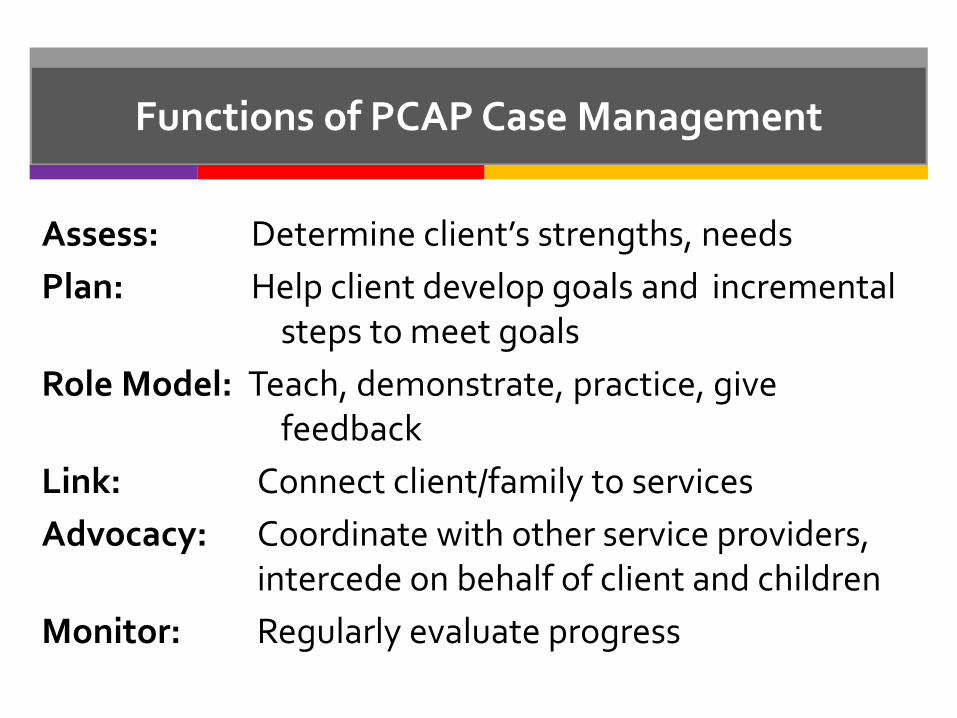
Functions of PCAP Case Management
Assess: Determine client’s strengths, needsPlan: Help client develop goals and incremental
steps to meet goalsRole Model: Teach, demonstrate, practice, give
feedbackLink: Connect client/family to servicesAdvocacy: Coordinate with other service providers,
intercede on behalf of client and childrenMonitor: Regularly evaluate progress
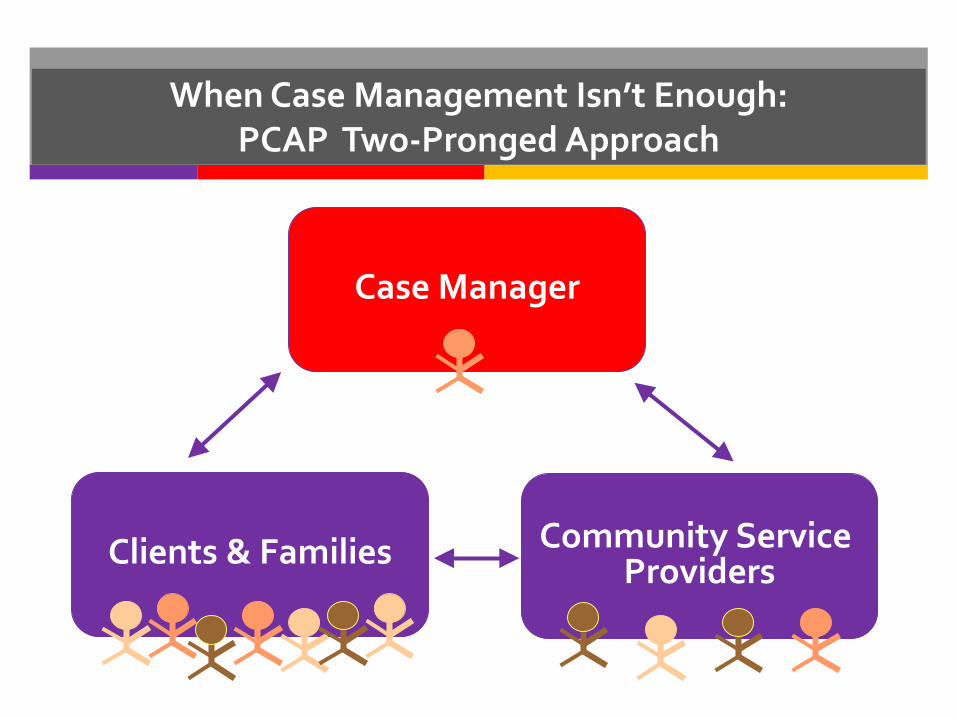
When Case Management Isn’t Enough: PCAP Two-Pronged Approach
Case Manager
Community Service ProvidersClients & Families
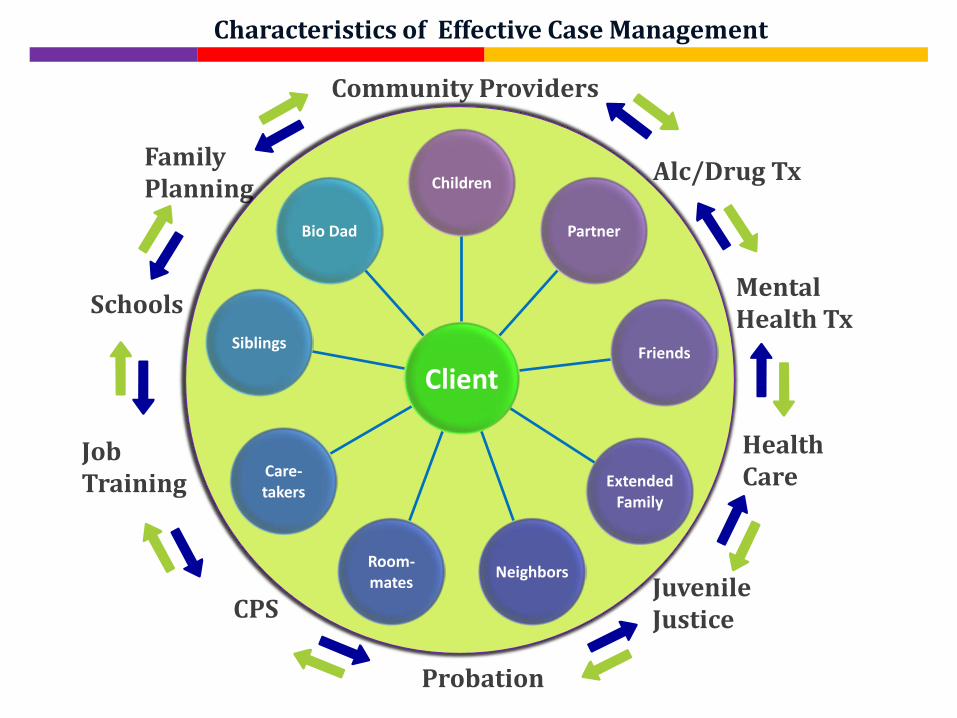
Family Planning
Community Providers
Job Training
Schools
CPS
Alc/Drug Tx
Juvenile Justice
Probation
Mental Health Tx
Health Care
Characteristics of Effective Case Management
Client
Children
Partner
Friends
ExtendedFamily
NeighborsRoom-mates
Care-takers
Siblings
Bio Dad
PCAP Enrollment Criteria
1) Currently pregnant, or up to twelve months postpartum; and
2) Used alcohol/drugs heavily during pregnancy; and
3) Not effectively engaged with community resources
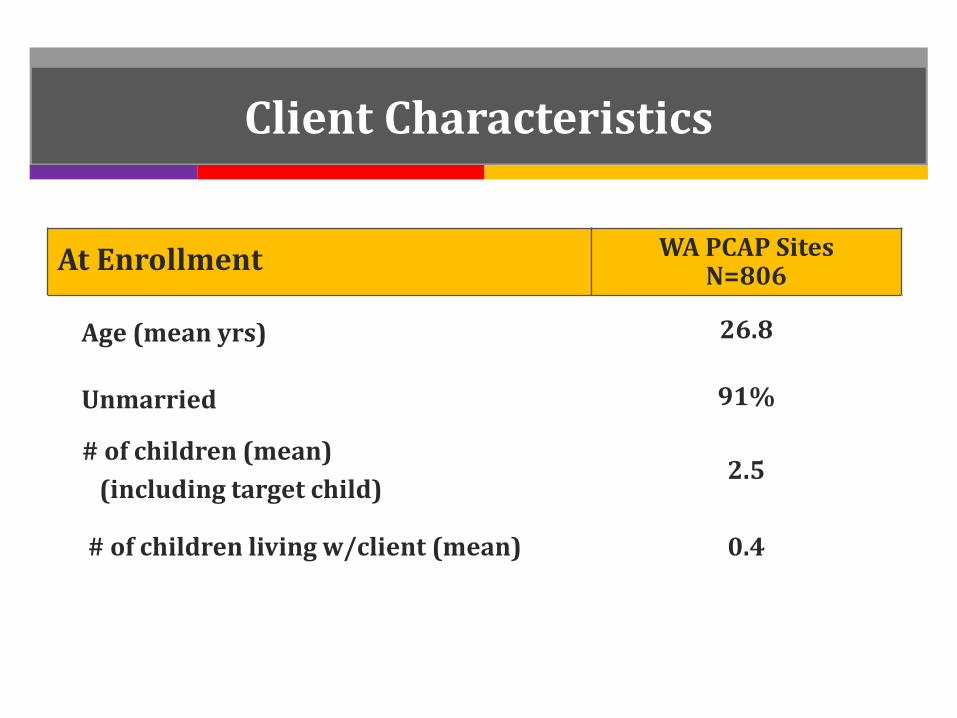
Client Characteristics
At Enrollment WA PCAP SitesN=806
Age (mean yrs) 26.8
Unmarried 91%
# of children (mean) (including target child)
2.5
# of children living w/client (mean) 0.4
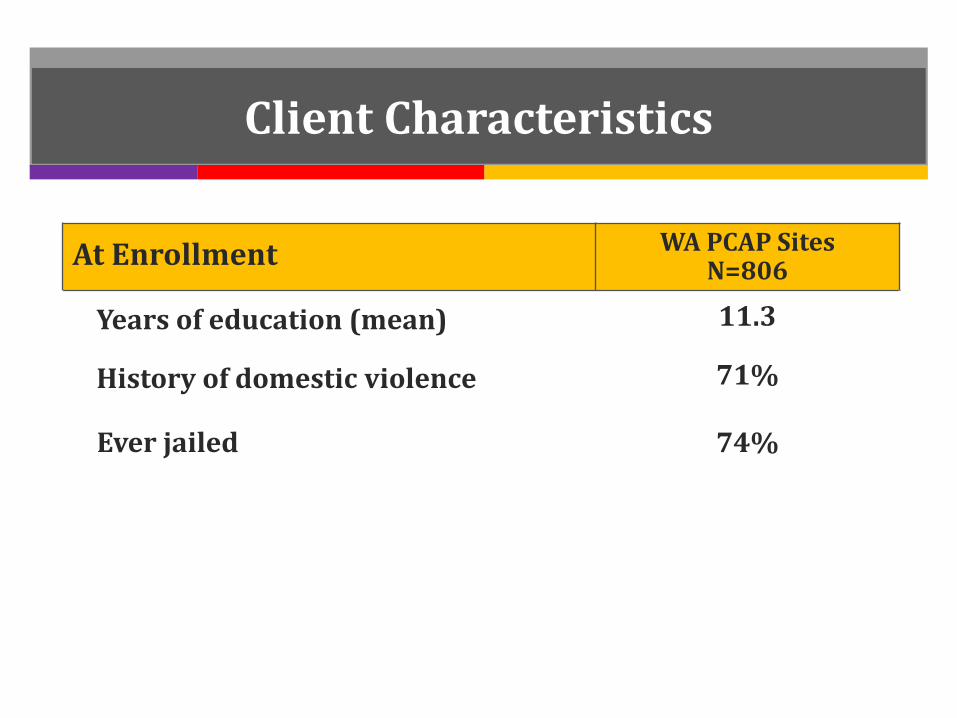
Client Characteristics
At Enrollment WA PCAP SitesN=806
Years of education (mean) 11.3
History of domestic violence 71%
Ever jailed 74%
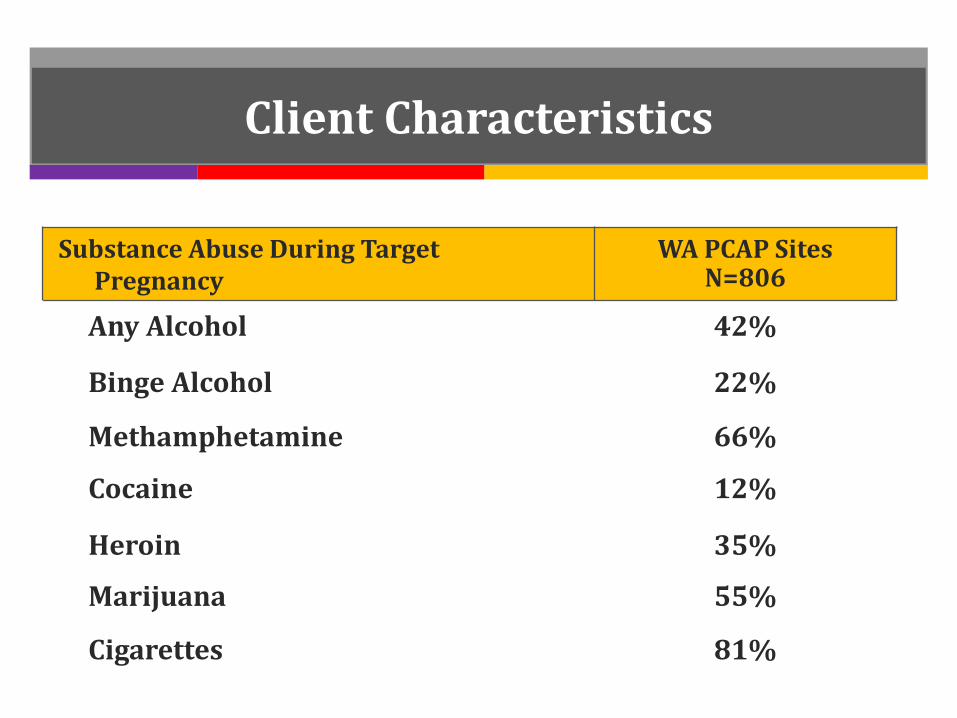
Client Characteristics
Substance Abuse During Target Pregnancy
WA PCAP SitesN=806
Any Alcohol 42%
Binge Alcohol 22%
Methamphetamine 66%
Cocaine 12%
Heroin 35%
Marijuana 55%
Cigarettes 81%
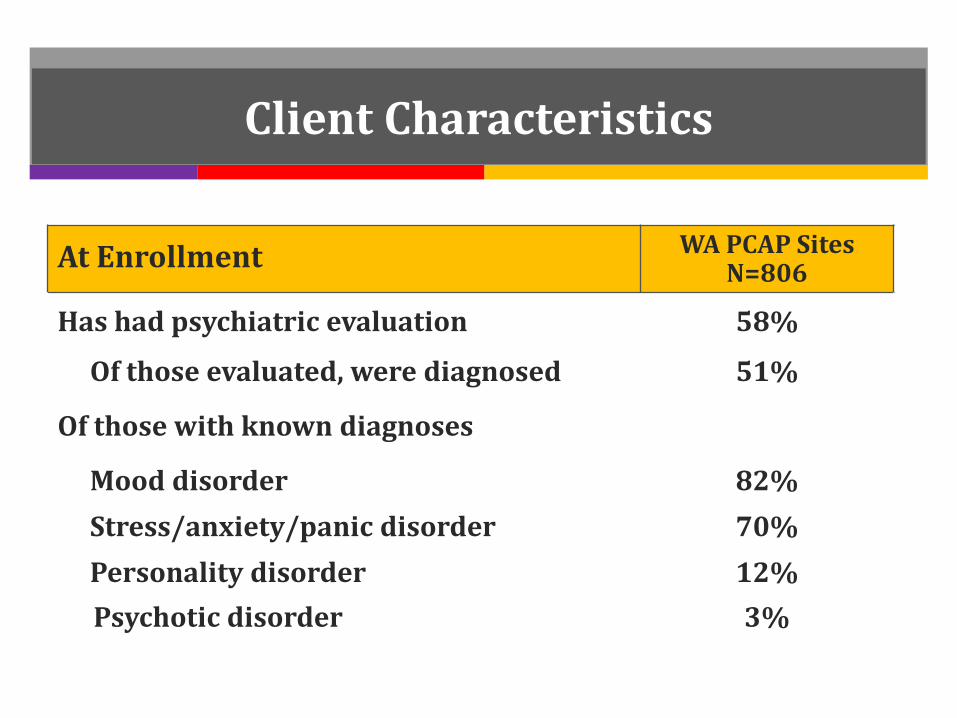
Client Characteristics
At Enrollment WA PCAP SitesN=806
Has had psychiatric evaluation 58%
Of those evaluated, were diagnosed 51%
Of those with known diagnoses
Mood disorder 82%Stress/anxiety/panic disorder 70%Personality disorder 12%Psychotic disorder 3%
IT WOULD MAKE A DIFFERENCE IN MY
LIFE IF I HAD:
MORE EDUCATION
Learning the Client’s Story: The Difference Game
Journal of Contemporary Human Services, 78(4): 429–432

Talk about what you learned in the Difference Game
Identify a goal that is realistic, manageable Break the goal into small steps that are attainable
and that you both will take.
Self-efficacy is about
helping clients accomplish steps successfully.
Reinforce every step in the right direction.
Identify Goals & “Baby Steps” to reach each goal.

PCAP Administrative Strategies
Training: pre-service, in-service, and continuing education
Individual weekly or biweekly supervision
Weekly group staffing
Biannual evaluation feedback
PCAP Evidence Base
Published PCAP Outcomes2014: Improving pregnancy outcomes among high-risk mothers who
abuse alcohol and drugs: Factors associated with subsequent exposed births. Children and Youth Services Review, 46: 11-18.
2011: Maternal substance abuse and disrupted parenting: Distinguishing mothers who keep their children from those who do not. Children and Youth Services Review, 33, 2176-2185.
2005: Preventing alcohol and drug exposed births in Washington State: Intervention findings from three Parent-Child Assistance Program sites. American Journal of Drug and Alcohol Abuse, 31(3), 471-90.
2003: Post-program follow-up effects of paraprofessional intervention with high-risk women who abused alcohol and drugs during pregnancy. Journal of Community Psychology, 31(3), 211-222.
1999: Intervention with high-risk alcohol and drug-abusing mothers: II. 3-year findings from the Seattle model of paraprofessional advocacy. Journal of Community Psychology, 27(1), 19-38.

Substance Abuse and Mental Health Services Outcomes
3-Year Outcomes WA State PCAP(N = 1056)
Follow-up rate
Inpatient or outpatient tx completed or in progress
Mental health service connection
Abstinent at exit for ≥ 6 moAbstinent at exit for ≥ 1 yr
Longest abstinence in PCAP ≥ 1 yr
87%
91%
62%
42% 34%
58%
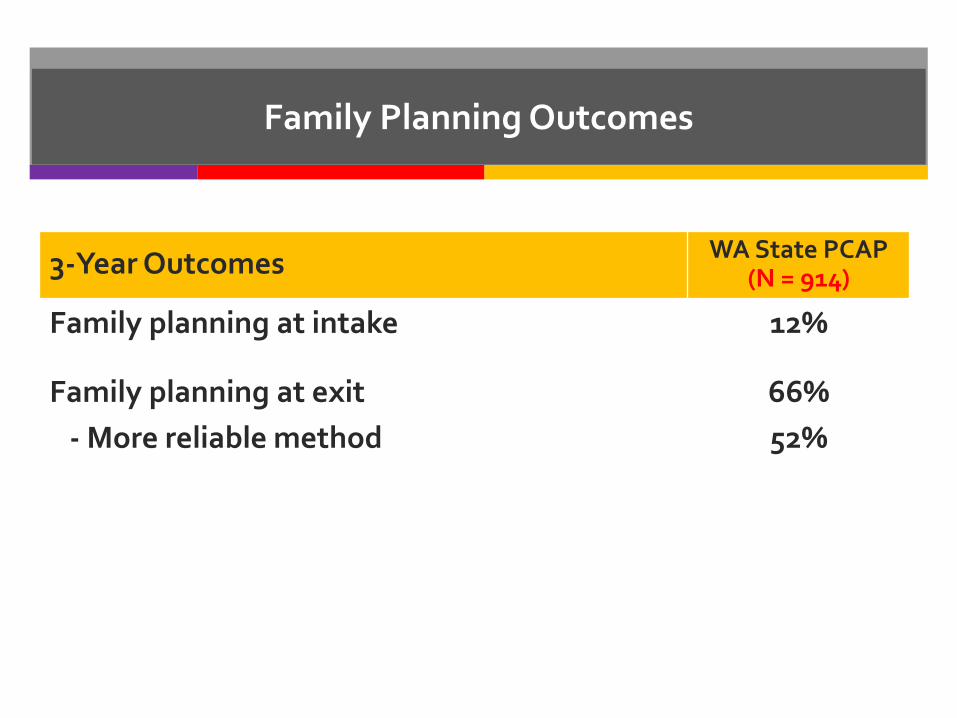
3-Year Outcomes WA State PCAP(N = 914)
Family planning at intake
Family planning at exit- More reliable method
12%
66%52%
Family Planning Outcomes

Preventing future substance-exposed births
At 3-year program exit
• 78.1% of mothers had no subsequent birth (SB)
during PCAP
• 9.6% had a SB not exposed to alcohol or drugs
• 12.3% had a SB exposed to alcohol or drugs
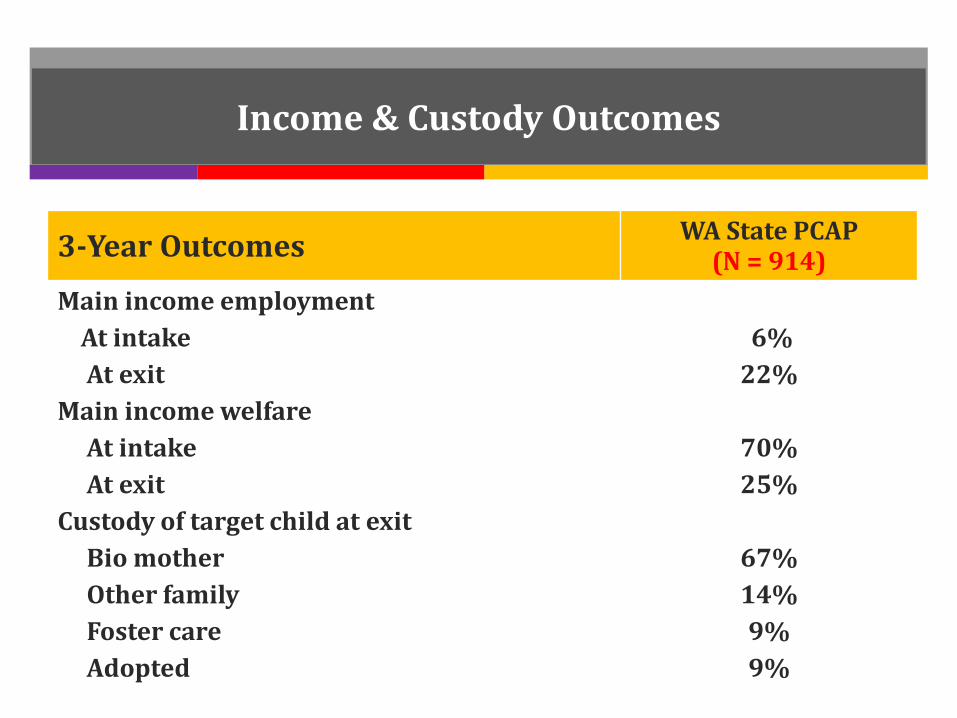
Income & Custody Outcomes
3-Year Outcomes WA State PCAP(N = 914)
Main income employmentAt intakeAt exit
Main income welfareAt intakeAt exit
Custody of target child at exitBio motherOther familyFoster careAdopted
6%22%
70% 25%
67%14%9%9%
Other PCAP/FASD Publications2014: Substance abuse treatment outcomes in women with fetal alcohol spectrum
disorder. International Journal of Alcohol and Drug Research, 3(1), 43-49.
2013: Screening in treatment for fetal alcohol spectrum disorders that could affect therapeutic progress. International Journal of Alcohol and Drug Research, 2(3), 37-49.
2013: The value of the neuropsychological assessment for adults with fetal alcohol spectrum disorders: A case study. International Journal of Alcohol and Drug Research, 2(3), 79-86.
2013: The impact of prenatal alcohol exposure on addiction treatment. Journal of Addiction Medicine, 7(2):87-95.
2013: Parent-Child Assistance Program Outcomes Suggest Sources of Cost Savings for Washington State. Available at: http://depts.washington.edu/pcapuw/inhouse/PCAP_Cost_Savings_Brief_Feb_2013.pdf
2009: Alcohol use before and during pregnancy in Western Washington, 1989-2004: Implications for the prevention of fetal alcohol spectrum disorders. American Journal of Obstetrics and Gynecology, 200(3), 278e1-8.
2008: Suicide attempts among adults with fetal alcohol spectrum disorders: Clinical considerations. Mental Health Aspects of Developmental Disabilities, 11(2), 33-41.
2006: Neonatal cranial ultrasound leads to early diagnosis and early intervention in baby of alcohol-abusing mother. Mental Health Aspects of Developmental Disabilities, 9(4), 125-127.
2005: Quality of life and psychosocial profile among young women with fetal alcohol spectrum disorders. Mental Health Aspects of Developmental Disabilities, 8(2), 33-39.
PCAP is Cost Effective
Casey Family Programs: PCAP outcomes suggest sources of cost savings for Washington State
PCAP children had a shorter average length-of-stay in foster care compared to WA state average (3.8 months vs. 20.4 months). Savings = $21,231 per child.
Reduced dependence on public assistance, from 70% at PCAP intake to 25% at exit.
Increased employment as main source of income, from 6% at PCAP intake to 22% at exit.
Available at: http://depts.washington.edu/pcapuw/inhouse/PCAP_Cost_Savings_Brief_Feb_2013.pdf
Canadian Economic Evaluation of PCAP
Summary: Using PCAP data from Alberta, Canada, this is the first study estimating the incremental cost effectiveness ratio and the net monetary benefit of a PCAP program. Results estimate that PCAP prevented approximately 31 (range 20–43) cases of Fetal Alcohol Spectrum Disorder among 366 clients in a 3-year period. The net monetary benefit is approximately $22 million (range $13–$31 million). Results indicate that the program is cost–effective and the net monetary benefit is significant.
Authors note that the benefit is likely underestimated as the study did not include benefits from the reduction in unemployment and welfare income dependence rates among PCAP participants.
Thanh, N.X., Jonsson, E., Moffatt, J., Dennett, L. Chuck, A., & Birchard, S. (2015). An Economic Evaluation of the Parent–Child Assistance Program for Preventing Fetal Alcohol Spectrum Disorder in Alberta, Canada. Administrative Policy and Mental Health, 42:10–18.
The PCAP Model Maintains Project Fidelity
Monitor quality control Evaluate program
Demonstrate consistent positive outcomes
Participate in the community
Build acceptance, recognition in community
PCAP continues to …..
Systems Working Together
Good things happen when
WA State implements
effective programs and
communities collaborate
to improve outcomes
for families.

“Before PCAP
I never thought about goals.
They showed me the right direction.
They showed me that I am responsible.
That no matter who I am or what I do,
I am somebody.
It is never too late.”-PCAP Client