Embed Size (px)
Citation preview

Vol. 54, No. 1, Winter 1994 39
Gains in Dental Care Use Not Shared by Minority Elders
Judith A. Jones DDS, MPH Director, Geriatric Dental Program VAMC, Bedford, MA, and Assistant Professor Harvard School of Dental Medicine Boston, MA
Denise J. Fedele, DMD, MS Director, Geriatric Dental Program Perry Point, MD, and Clinical Assistant Professor Baltimore College of Dental Surgery University of Maryland at Baltimore, and Clinical Assistant Professor of Medicine University of Maryland Medical School Baltimore, MD
Aljernon J. Bolden, DMD, MPH Assistant Professor Department of Preventive and Community Dentistry University of Iowa College of Dentistry
Barbara Bloom, MPA Health Statistician National Center for Health Statistics Hyattsville, MD
Abstract Americans have steadily increased their reported use
of dental services over the past 30 years. Persons aged 65 years and older have made the greatest gains, from 16 percent in 1957-58 to 43 percent in 1989. This article reviews national data on reported use of dental care over the past three decades, focusing on differences in rates of utilization on the basis of age, race, and national origin. In addition, differences in sample selection, definitions of race and national origin, and data collection methodology were reviewed to identify systematic sources of bias in comparing the data. Findings indicate that reported den- tal care use among minority elders has not increased parallel with elders of all races and national origins. In 1957-59, 17 percent of white elders versus 9 percent of nonwhite elders had seen a dentist within the past year. By 1989 percentages had improved to 45 percent of whites, but only 22 percent of blacks and 40 percent of Hispanics. In addition, reporting and recording race and national origin varied considerably during the three de-
Send correspondence and reprint requests to Dr. Jones, Dental (la), VAMC, 200 Springs Road, Bedford, MA 01730. Manuscript received: 4/19/91; returned to authors for revision: 7/9/91; accepted for publi- cation:4/22/93.
cades, hampering comparisons over time. Finally, pub- lished nationaldata on usual correlates of dental care use (dentition status, insurance, age, income, and education) are inadequate to explain the causes of these discrepan- cies. More research is needed to identify barriers to use of dental care by all Americans, particularly those of African and Hispanic descent. Because these ethnic groups are aging faster than the rest of society, and because dental care use among Hispanic and African American elders lags behind use among all elders, dental and public health professions have a responsibility to investigate the barriers and to plan strategies for improv- ing use of care.
Key Words: dental care for aged, aged, African American, blacks, Hispanic Americans.
Dramatic gains have been made over the past three decades in the proportion of Americans using oral health services. The percentage of persons of all ages reporting use of dental care during the previous year has increased from 37 percent in 1957-58 to 55 percent in 1989 (1,2). Similarly, the increase among persons aged 65 years and
J Public Health Dent 1994;54(1):39-46

40 Journal of Public Health Dentistry
TABLE 1 Percent of Population with Dental Visit in the Past Year by
Age and Year (1-7)
All Ages* Year (%)
1957-58 36.6 1970 46.8 1975 50.3 1981 50.1 1986 57.1 1989 55.4
25-44 Years (%)
45-64 Years (%)
65+ Years (%)
44.1 52.3 54.5 54.2 60.4 60.1
32:3 44.2 48.2 49.6 54.6 56.8
16.2 25.8 30.3 34.6 41.7 43.2
*All ages except under age two.
older who reported using dental care within the previous year has more than doubled, from 16 percent in 1957 to 43 percent in 1989. These increases in use of dental ser- vices have occurred gradually over the 30-year period, as demonstrated by Table 1 (1-7).
National utilization data for minority groups, how- ever, show that the increase in utilization is not evenly distributed across racial and ethnic subgroups, particu- larly since 1975 (2,3,7,8). Former Secretary for Health and Human Services Dr. Louis Sullivan recognized “a seri- ous, deep disparity between the general population and our minority and poor citizens. Each year, while the health status of most of our citizens shows steady im- provement, the same improvements are not as evident for our minority and low-income groups” (9). National examination survey data corroborate Dr. Sullivan’s posi- tion. These data show that the oral health status of minor- ities is, in the aggregate, demonstrably poorer than the majority (10-17). For example, gingivitis is highly preva- lent among Hispanics of all ages, and dentate Cuban American and Puerto Rican adults have twice as many missing teeth as dentate white, non-Hispanic adults (10,14). Using National Institute of Dental Research data, Waldman has pointed out that minority children have more caries, more unfilled caries and more gingival bleeding than their nonminority counterparts (1 1,12). Tooth loss, edentulism, and caries rates are higher in black than in white elders (13). Further, the incidence rate of oral cancer is 30 percent higher among blacks than whites, and the oral cancer mortality rate is twice as high for blacks than for whites (15,161.
Black or African Americans are the largest minority group in America, approximately 12 percent of the total population. Leaders of the African American dental and dental public health communities are concerned that extant national oral health data represent neither the African American population overall, nor the great di- versity within black communities (17). Data fromcurrent research on oral health status severely underestimate the problems, needs, and demands for care among African
Americans; data that do exist are inadequate to describe the psychosocial factorsaffecting African Americans’ use of dental care in general or among subgroups of the population, such as the elderly, the institutionalized, or the homeless.
Variations in oral health status and use of services among minority elders are important because of the in- creases that are expected in both numbers and percent of minorities among the elderly population over the next few decades (18-23). From 1990 to 2020, the number of elders in America is expected to rise from 31.6 to 52.1 million, an increase of over 60 percent. More dramatic, however, is that the number of African American elders is expected to more than double from 2.6 to 5.6 million; the number of Hispanic American elders is expected to more than triple from 1.1 to 3.9 million over this same period. Thus, it is incumbent upon the dental professions to learn more about minority groups’ use of dental care in an effort to better meet their oral health needs in the decades ahead.
The purpose of this paper is to review National Center for Health Statistics (NCHS) data collected over the past three decades and critically examine dental care use by African American and Hispanic American elders as com- pared with white and non-Hispanic elders. Usingdata on dental visits within the past year and mean visits per person, disaggregated by race, ethnic groupings, educa- tion, income, dentition status, and the presence or ab- sence of private dental insurance, this paper will examine factors contributing to racial and ethnic group discrepan- cies. Finally, directions for future research that would assist dental professionals in identifying and eliminating racial and ethnic differences in patterns of dental care use among elders suggested by this review will be discussed.
Methods Since the late 1950s, the National Health Interview
Survey (NHIS)-a national survey of health practices, knowledge, illness levels, and health care use--has been conducted by the National Center for Health Statistics. Field work for the NHIS is performed by the US Bureau of the Census and the data are compiled, analyzed, and published by the National Center for Health Statistics (3). Over the years, these interview surveys have been con- ducted on multistage probability samples of the civilian, noninstitutionalized population of the United States. Sampling procedures have divided the United States into 1,900 primary sampling units (PSUs). Typically, 44,000 households are sampled during each year of the survey, resulting in household interviews of about 134,000 per- sons annually. However, because of funding limitations, the 1986 NHIS was conducted with a sample of approx- imately half the size of the full sample design.
Data collected are adjusted, most recently by a four- step ratio estimating process, to make the sample more closely representative of the target population in age, sex,

Vol. 54, No. 1, Winter 1994 41
race, and residence. For example, in 1989 information about oral health was obtained for 109,603 persons aged 2 years and older and adjusted to provide estimates of dental care use for 235,858,000 civilian noninstitutional- ized persons. Within this group, information on dental care use was obtained from 13,781 non-Hispanic and 464 Hispanic persons aged 65 and older, including 1,638 blacks (17 of which considered themselves to be Hispa- nic, and 1,621 non-Hispanic). These data then were ad- justed by the four-step process to provide estimates of dental care use for the 29,219,000 noninstitutionalized elders in the United States (2).
For this paper, existing health interview data collected and published by the NCHS (except data from 1975 that were published by the American Dental Association in 19771, including age-specific use of dental care by Ameri- cans, were reviewed. Data on visits in the past year were available for 1957-59,1962-63,1963-64,1969,1970,1973, 1974,1975,1978-79,1978-80,1981,1983,1986, and 1989 (1-8,24-39). From this original list, years for which age- specific data were published on the use of care within specific subpopulations of Americans (i.e., blacks, whites, nonwhites, Hispanics, and non-Hispanics) were identified; all other years then were eliminated from the review, leaving 1957-58, 196344, 1975, 1978-80, 1983, 1986, and 1989.
Data Collection Techniques Review. For each year specified above, variations in sample design and selec- tion were reviewed and catalogued. In addition, methods of collecting data on race and national origin were sys- tematically studied and tabulated in an effort to assess comparability from year to year.
Measures of Utilization. Data on use of dental care have been collected primarily by three main questions over the past three decades. One of these questions as- sesses the interval since last dental visit; another, the number of visits in the past two weeks; and a third, the number of visits in the past year. This third basic usage question, added in 1983, allows an edit of the interval since last visit data and the addition of a category of "less than 1 year, time period unspecified," which has in- creased the total number of persons who had seen a dentist in the last year by 2 percent in 1986, and 1.8 percent in 1989-small but important increases during those years when used.
Two measures of dental care use were selected for this review: the percent of the population who reported use of services in under one year, and the mean number of visits per person per year. Inclusion of other measures such as recent use (use in under two years) and nonuse or sporadic use (not seeing a dentist in over five years) might add depth to this analysis; however, in the interest of succinctness, only two are reviewed.
Published Bivariate Findings. Demand for oral health services has, in previous work, been associated with a variety of personal and demographic characteristics in-
cluding age, gender, race, ethnic groups, education, mar- ital status, income, source of care, employment status, cost, insurance, geographic location, access to transpor- tation and information, perceived need, perceived health, dentition status, and health attitudes (40-46). In light of these correlates of dental care use, selected data published in 1986 and 1989 were examined in more detail to identify factors that could contribute to lower rates of reported use of dental care by elders of African and Hispanic American descent.
Results Differences in Sampling. Tabulation and review of
the sampling design over the three decades identified five major differences (1-6,8,24-39). First, the selection of PSUs, counties, or metropolitan areas from the available pool varied over time. Second, the types of terminal segments (yielding a fixed number of households in each survey) changed with time. Sources of terminal segments included census lists, building permits, and geographical areas. Third, the number of households per segment varied between four and nine over the time period stud- ied. Fourth, in 1986 and 1989 the black community was oversampled to improve the precision of NCHS esti- mates for this subset of the population (2,3). Finally, only half of the expected sample was interviewed in 1986 because of cost constraints. The first four of these reflect the evolution of sampling approaches over the decades. Thus, the samples probably better reflected the total ci- vilian population as time went on. There was no evi- dence, however, that any of these changes in sampling procedures affected the comparability of the results from year to year.
Definitions of Race and National Origin. By contrast, definitions of race and how these data were collected and reported during the national surveys reviewed varied considerably and are not comparable over the 30-year period. From 1957 through 1973, persons were catego- rized by the interviewer as either white, Negro, or other; however, when published in conjunction with dental utilization data, the original groupings were collapsed to white and nonwhite or white and all other (1,24-3438). During these years, "other" included '{American Indian, Chinese, Japanese, and so forth"; "white" included Mex- ican Americans. In 1974-76, racial data again were deter- mined by the interviewer and noted on the survey inter- view form as white, black, or other (535,47). Determina- tion of race in 1978-79 also was by survey interviewer observation, unless the interviewer was in doubt, in which case the interviewer was instructed to ask the respondent (8,47). It was not until 1980 that "respon- dent's selfdescription" was used uniformly to determine race. Flashcards were used and the respondents were asked to choose "which number best describes.. . ' s racial background?" Choices were: (1) Aleut, Eskimo, or Amer- ican Indian; (2) Asian or Pacific Islander; (3) black; (4)

42 Journal of Public Health Dentistry
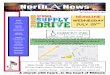
FIGURE 1 Percent of Persons Aged 65+ Using Dental Care within Past Year by Race, National Origin, and Year, USA (1-3,7,8,29,37)
I
50 I 1
FIGURE 2 Mean Dental Visits per Person per Year, Age 65+ by Race,
National Origin, and Year, USA (2,3,25,29,30,36,37)
mean visits 2.5 1
40 2
30 1.5
20 1
10 0.5
n n " 57-8 63-4 75 78-80 83 86 89
year
ALLELDERS NON-WHITE 0 WHITE
BLACK a HISPANIC
" 57-59 63-84 69 78-79 83 86 89
year
ALLELDERS NON-WHITE 0 WHITE
BLACK HISPANIC i white; or (5) other. The only exception was in 1983 when the "other" category was excluded (3,6,3738).
National origin data also have been variably collected over the 30-year time period of theNationa1 Health Inter- view Surveys. From 1957 to 1973, persons of Hispanic descent were not identified as Hispanic (1,4,24-3438). Notes from these years indicate that Mexicans were to be included as whites. Starting in 1976, data on Hispanic national origins were collected via respondent self-de- scription using flashcards (3,6,8,36,37,39,47). Subgroups depicted on the cards varied somewhat over the time period, but generally included Puerto Rican, Cuban, Mexican, Mexicano, Mexican American, Chicano, other Latin American, and other Hispanic. However, reported use of dental care among Hispanics was not published for 1981 or 1983. In 1978-80, the data were reported as all Hispanic, Mexican American, Puerto Rican, Cuban Am- erican, all other Hispanic, and non-Hispanic (8); in 1986 the data were reported as Hispanic, Mexican American, all other Hispanic, and non-Hispanic (3).
Reported Use of Dental Services. The percent of the elder population using dental services in the past year by race, national origin, and year is shown in Figure 1 (1-3, 7,8,29,37). Between 1957 and 1989, persons aged 65 and older increased their use of dental services from 16 per- cent in 1957 to 43 percent in 1989. The increase has been gradual over the 30-year period. A similar increase in reported use of care is noted for whites, who nearly tripled their use from 17 percent in 1957-58 to 45 percent in 1989. Less can be inferred from changes in utilization of dental services for nonwhites, however. The percent of nonwhite persons over the age of 65 who used dental services within the past year was 9 percent in 1957-58. By 1989, only 22 percent of black elders reported use of dental care, half the rate of whites. Notably, there has been little change in the percent of black elders using care since 1975, when 20 percent reported using dental care in less than one year (7). This lack of improvement (since 1975) might seem more striking when we consider the
implications of adding the third dental care use question in 1983. Recall that the use of this question permitted an edit of the "interval since last visit data," which increased the category of "less than one year" in the interval since last dental visit overall by approximately2 percent. How- ever, calculations from the 1986 and 1989 data show that for black elders, this third question resulted in less than a 1 percent change in reported use of dental care.
Data on use by Hispanic elders has only been collected and reported since 1978-80, with essentially no change in reported use of dental care over a decade until 1989, when it jumped from 28 percent (in 1978-80) to 40 percent. This 40 percent is not significantly different statistically from non-Hispanic elders, 43 percent of whom reported use of services (2,837).
Mean numbers of visits per person per year for indi- viduals aged 65 and older are shown in Figure 2 (2,3,25,29,30,36,37). Again, the data for all persons aged 65 years and older demonstrate that mean visits have increased gradually, from 0.8 to 2.1 over the 30-year period. Similarly, a gradual increase over time was noted for white elders, from 0.8 in 1957-59 to 2.2 in 1989. The 1957-59 data for nonwhites show that the mean number of visits (0.3/person/year) was less than half that of whites. Data from 30 years later are not directly compa- rable due to variations in definitions of race, however. Mean visits per person per year for black elders have actually seesawed from 1.0 in 1978-79, to 0.6 in 1983, to 1.2 in 1986, and then back to 0.6 in 1989. Whether these variations represent differences in sampling, or real in- creases and decreases, is not at all clear from published information. Data on mean visits among Hispanic elders were available for 1986 and 1989 only. In 1986, when they averaged 2.0 visits per person per year, the precision of the estimate was questioned by the NCHS (2). In 1989, the mean visits per person per year for Hispanic elders (all races) dropped to 1.2, a value substantially lower than their non-Hispanic counterparts, i.e., 2.0 visits per person per year.

Vol. 54, No. I, Winter 1994 43
FIGURE 3 FIGURE 4 Percent with Dental Visit in Past Year by Private Dental
Insurance, Selected Ages, and Race, USA 1989 (2) Percent of Adults Who Are Edentulous by Selected Ages
and Race, USA, 1989 (2)
80 86. HAS INSURANCE
60 86. NO INSURANCE
66-84 HAS INSURANCE 40
20 66 84 N O INSURANCE
0 85. 75-84 65-74 55-64 45-54
age m WHITE
10080 60 40 20 0 20 40 60 80 100 % %
TABLE 2 Percent of Adults with Dental Visit in Past Year by Selected
Ages, Dentition Status, and Race, USA, 1986 (3)
adults witha dental visit in the last year, by selected ages, dentition status, and race in 1986 (3). Edentulous persons of both races lagged far behind their dentate counter- parts. In this instance, differences were less among blacks than whites, primarily because of low reported utiliza- Age
(Years) Black White Black White tion rates among; dentate blacks. Note, however, that the
% Dentate % Edentulous
45-54 55-64 65-74 45+ 55+
48.0 67.0 35.8 65.8 31.7 65.6 39.0 65.7 32.4 64.9
22.1+ 14.2 11.6* 13.3 11.8
12.1 12.7 9.3
10.2 9.8
530% relative standard error in numerator of percent.
Published (NCHS) Bivariate Findings. Previously published findings of the NCHS regarding usual corre- lates of dental care use were examined for their potential utility in explaining reported use of dental care by elders of different races and national origins. For example, the relevance of private dental insurance to reported dental care use was examined in the 1989 NCHS data. Race or national origin appeared to have little effect on whether elders had dental insurance. The percent who had private dental insurance ranged from a low 11.1 in black elders to a high of 15.6 percent among Hispanic elders, with 15.0 percent of non-Hispanic elders and 15.4 percent of whites having insurance. On a percentage basis, however, elders with dental insurance, regardless of race or national ori- gin, had a greater chance of seeing a dentist in 1989 than elders without insurance, as shown in Figure 3 (2). In addition, the discrepancy between elders with and those without private insurance is somewhat greater among blacks than whites.
Whether or not middle-aged and older adults have teeth is clearly associated with use of dental care as demonstrated by Table 2, which depicts the percent of
data for edentuyous blacks aged 45-54 and 65-74 years have high relative standard errors (>30%). Accordingly, these two values must be excluded when drawing con- clusions from these data.
Because of differences in patterns of use between den- tate and edentulous persons, the number and percent of edentulous elders are salient considerations when look- ing at racial differences in elders’ dental care use. The percents of adults who were edentulous by selected ages and race in 1989 are displayed in Figure 4 (2). No be- tween-race differences are present in persons under age 75. However, among persons aged 75 years and older, the differences between blacks and whites are dramatic, and are of a magnitude to influence the overall picture of differential utilization.
Income and education are two, often related, correlates of utilization. The 1986 data contain information on use of dental care by race, age, income, and education; how- ever, the low number of persons in each of the oldest age groups limits the usefulness of these data (3). When all income levels are grouped together, however, reliable data are available on reported use of dental care by race, age and education for both 1986 and 1989. NCHS data from 1989 on use of dental care by race, age, and educa- tion are shownin Table 3. Note that reported use of dental care declines with advancing age, regardless of race or education. This decline among the older age groups is greater among blacks than whites, however. Reported use of dental care in blacks with 12 or more years of education declined from 61 percent in 45-54-year-olds to 39 percent in the oldest age group, and from 49 percent in 35-44-year-olds to 26 percent in elders with 12 years of

44 Journal of Public Health Dentistry
education. In addition, blacks consistently have lower use of dental care regardless of age and education. How- ever, the magnitude of the racial differences according to education are quite different. In the highest education group, differences between the races widen with age; in the high school education group, differences are rela- tively stable except in the oldest group. Most striking are the relatively small and stable differences between the races in the low education group.
Finally, as shown in Figure 5, differences in dental visits in 1989 based on race are larger among elders than among other age groups (2). Also note that while the reported use by elder Hispanic Americans represents an increase compared with previous years (from 28 percent in 1986 to 40 percent in 1989), Mexican American elders (34 percent) lag considerably behind other Hispanic el- ders (43 percent, not shown).
Discussion Since their inception in 1957, the National Health In-
terview Surveys have provided data on the civilian, non- institutionalized population living in the United States (3). Redesign of the sample has followed each decennial census, permitting the inclusion of advances in statistical methodologies and use of the latest population informa- tion. While the extent to which changes in the sampling design and data collection techniques have differentially influenced survey results can never fully be determined, these data are the best available and in most cases highly reliable because of the size of the samples in survey designs.
Marked refinements have taken place with respect to definitions of race and national origin over the 30-year time period studied. The nonuniformity of definitions and data collection methods severely hampered the com- parability of the data over the three decades studied. Nevertheless, the available data demonstrate a disparity between whites and nonwhites, whites and blacks, and Hispanics and non-Hispanics over the entire period stud- ied. Rather than decreasing over time, however, the ineq- uity appears to be getting worse, at least with respect to black elders. Increases in reported use of care among all
elders and white elders are not seen among black elders. After 1975, elders of all races and whites continued to make gains in utilization, while black elders clearly did not (Figure 1). Further, improvements in mean visits per person per year among black elders seen in previous years appear to have been lost between 1986 and 1989, when they dropped from 1.2 to 0.6 per person. Whether this finding represents a true decline in use or is merely an aberration remains to be seen.
To a lesser degree, differences between Hispanic and non Hispanic elders also have been noted within the past decade. While it appears that by 1989 Hispanic elders caught up to their non-Hispanic counterparts in the per- cent reporting use of care, important differences remain between Hispanic subgroups, as detailed in Figure 5. It is incumbent upon the dental public health community to identify such pockets of nonusers, study them, and improve mechanisms for meeting their oral health needs.
Need for Further Research. Further research is needed to discern the reasons for racial and ethnic discrepancies among elders in their reported use of dental care. Second- ary analysis of existing national data on reported dental care use, using multivariate logistic regression and co- hort methodologies to control statistically for factors
FIGURE 5 Percent of Persons with Dental Visits within Past Year by
Age, Race, and National Origin, 1989, USA (2)
% I
60
50
40
30
20
10
n " 25-44 45-64 65,
age
ALLELDERS WHITE 0 BLACK
HISPANIC MEXICAN AM.
TABLE 3 Percent of the Population with Dental Visit in Past Year by Education, Race, and Age, USA, 1989 (2)
Education
% 4 2 Years % with 12 Years % >12 Years
Age (Years) Black White Black White Black White
3.544 34.0 39.0 48.8 60.3 62.3 74.3 45-54 28.9 35.5 44.2 59.1 61.4 76.5 55-64 27.1 34.1 46.6 57.7 48.6 75.4 65+ 19.4 29.0 25.5 50.6 39.4 68.3

Vol. 54, No. 1, Winter 1994 45
demonstrated to be important by bivariate techniques, may be useful in determining whether race and Hispanic national origin, per se, or sociodemographic factors more strongly influence utilization. What is needed most is a longitudinal interview study in elders designed to test the various models of the dental care process (40-46). A longitudinal design would aid such a project in that it would assess the stability of various components of the process and their influence on health behavior decision making over time. In addition, future consistency in def- initions of race and national origin will aid in sequential comparisons of cross-sectional data sets. Finally, efforts to examine the heterogeneity within the minority pop- ulationsfor example, among African Americans, or be- tween Mexican Americans and Cuban Americans- should be intensified.
Policy Implications. The policy implications of further research in this area are far reaching. Because of the growth expected in the number of elders and minority elders in particular, attempts should be made to identify and alleviate barriers to use of necessary health services, including dental services. Only after such work is accom- plished can the profession make realistic and appropriate recommendations for removal of barriers to care for "un- derserved" groups, thereby extending equitable access to dental care to all. Since the use of dental services in older adults is influenced by dental care patterns developed during earlier years, policy changes affecting children and young adults today ultimately will affect the elders of tomorrow.
References 1. National Center for Health Statistics. Dental care: interval and
frequency of visits, United States, Jul1957-Jun 1959. Washington, Dc: Mar 1960. Public Health Service pub no 584-B14. (Health statistics from the national health survey, series B; no 14; p 12.)
2. Bloom B, Gift HC, Jack SS. Dental services and oral health, United States, 1989. Hyattsville, M D Centers for Disease Control and Revention/ National Center for Health Statistics, 1992; DHHSpub no (PHS)93-1151. (Vital and health statistics; series 10; no 183.)
3. Jack S, Bloom B. Use of dental services and dental health, United States, 1986. Washington, DC: Nationalcenter for HealthStatistics, 1988; DHHS pub no (PHS) 88-1953. (Vital and health statistics; series 10; no 165.)
4. National Center for Health Statistics. Current estimates from the national health survey, United States, 1970. Rockville, M D Public HealthService,May 1972; DHEWpubno (HRA) 72-1054. (Vital and health statistics; series 10; no 72.)
5. National Center for Health Statistics. Current estimates from the national health survey, United States, 1975. Rockville, M D Public Health Service, Mar 1977; DHEW pub no (HRA) 77-1543. (Vital and health statistics; series 10; no 115.)
6. National Center for Health Statistics. Current estimates from the national healthsurvey,UnitedStates, 1981.Hyattsville,MD Public Healthservice, 1982; DHHSpubno(PHS)82-1569. (Vitalandhealth statistics; series 10; no 141.)
7. American Dental Association. Utilization of dental services in the elderly population. Chicago, IL: ADA, 1977.
8. Trevino M, Moss AJ. Health indicators for Hispanic, black, and white Americans, 1978-80. HyattsviUe, M D National Center for Health Statistics 1984; DHHS pub no (PHS)84-1576. (Vital and health statistics; series 10; no 148.)
9.Sullivan LW. Introduction. In: US Department of Health and Human Services. Health status of minorities and low income groups. 3rd ed. Washington, DC: 1991; Public Health Service,
Health Resources and Services Administration, 1991 (US Govern- ment Printing Office, pub no 271-848/40085,1991.)
10. Furino A, Munoz E. Health status among Hispanics: major themes and new priorities. J Am Med Assoc 1991;265(2):2557.
11. Waldman HB. Are minority children getting their fair share of dental services? J Dent Child 1990;57(5):38@4.
12. National Institute of Dental Research. Oral health of United States schoolchildren, 1986-87. Bethesda, M D NIH pub no 89-2247,1989.
13. National Institute of Dental Research. Oral health of United States adults, 1985-86. Bethesda, M D NIH pub no 87-2868,1987.
14. Ismail AI, Szpunar AM. The prevalence of total tooth loss, dental caries, and periodontal disease among Mexican Americans, Cuban Americans and Puerto Ricans: findings from the HHANES 1982-84. Am J Public Health 1990;8O(Suppl):6&70.
15. Manley AF. In: News and trends. Dentistry Today 1991;10(7):19. 16. National Institutes of Health and Center for Disease Control. Can-
cers of the oral cavity and pharynx: a statistics review monograph: 1973-87. Washington, DC: DHHS, 1991.
17. Razzog ME, Robinson E, ed. Black dentistry in the 21st century, June 23-27,1991. Proceedings of a workshop at the University of Michigan. Ann Arbor: University of Michigan School of Dentistry, 1991.
18. US Bureau of the Census. 1980 census of the population, vol 1, charaderisticsof the population (PC80-1), UnitedStatessummary. Washington, Dc. US Bureau of the Census, 1981:91,147.
19. US Bureau of the Census. 1980 census of the population, vol 1, chap B (PC 8@1-B). Washington, Dc: US Bureau of the Census, 1980.
20. US Bureau of the Census. Statistical abstract of the United States: 1988.108th ed. Washington, Dc: US Bureauof the Census, 1987:14 1 7.
21. Spencer G, US Bureau of the Census. Projections of the Hispanic population: 19832080,middleseries. Washington, Dc: USGovern- ment Printingoffice, 1986. (Currentpopulationreports;seriesP-25; no 995:41,43,44.)
22. US Bureau of the Census. Projections of the population of the United States, by age, sex, and race: 1988-2010. Washington, Dc: US Government Printing Office, 1988. (Current population reports; series P-25; no 1017:29,94,95,97,99,100,101,103,105.)
23. Spencer G, US Bureau of the Census. Projections of the population of the United States by age, sex, and race: 1988-2080 (middle series, series 14). Washington, Dc: US Government Printing Office, 1989. (Current population reports; series P-25; no 1018:42,43,62,63,82,83, 86,87.)
24. National Center for Health Statistics. Concepts and definitions in the health household interview survey. DHEW, pub no 584-A3, 1958. (National health survey report; series A; no 3.)
25. National Center for Health Statistics. Dental care: volume of visits, United States, July 1957-June 1959. Washington, DC: US Public Health Service, Apr 1960; pub no 584-Bl4. (Health statistics from the national health survey; series B; no 15.)
26. National Center for Health Statistics. Medical care, health status, and family income. Washington, DC: US Public Health Service, May 1964; pub no IMXI. (Health statistics from the national health survey; series 10; no 9.)
27. National Center for Health Statistics. Current estimates from the health interview survey, United States, July 1963-June 1964. Wash- ington, Dc: US Public Health Service, Oct 1964; pub no 1ooO. (Vital and health statistics; series 10; no 13.)
28. National Center for Health Statistics. Volume of dental visits, United States, July 1963-June 1964. Washington, Dc: US Public Health Service, Oct 1965; pub no 1OOO. (Vital and health statistics; series 10; no 23.)
29. National Center for Health Statistics. Dental visits, time interval sincelastvisit,UnitedStates, July 1963-June1964. Washington,DC: NCHS, Apr 1966. (Vital and health statistics; series 10; no 29.)
30. National Center for Health Statistics. Current estimates from the health interview survey, United States, 1969. Rockville, MD: US Public Health Service, Jun 1971; pub no 1OOO. (Vital and health statistics; series 10; no 63.)
31. National Center for Health Statistics. Current estimates from the health interview survey, United States, 1970. Rockville, M D US Public Health Service, May 1972; DHEW pub no (HSM) 72-1054. (Vital and health statistics; series 10; no 72.)
32. National Center for Health Statistics. Dental visits, volume and interval since last visit, United States, 1969. Rockville, M D US Public Heaith Service, Jul 1972; DHEW pub no (HSM) 72-1066. (Vital and health statistics; series 10; no 76.)

46 Journal of Public Health Dentistry
33. National Center for Health Statistics. Current estimates from the health interview survey, United States, 1971. Rockville, MD: US Public Health Service, Feb 1973; DHEW pub no (HSM) 73-1505. (Vital and health statistics; series 10; no 79.)
34. National Center for Health Statistics. Current estimates from the health interview survey, United States, 1973. Rockville, M D US Public Health Service, Oct 1974; DHEW pub no (HRA) 75-1522. (Vital and health statistics; series 10; no 95.)
35. National Center for Health Statistics. Current estimates from the Health Interview Survey, United States, 1974. Rockville, MD. US Public Health Service, Sept 1975. (Vital and health statistics; series 10; no 100.)
36. National Center for Health Statistics. Dental visits, volume and interval since last visit: United States, 1978 and 1979. Hyattsville, MD: US Public Health Service, Apr 1982; DHHS pub no (PHS) 82-1566. (Vital and health statistics; series 10; no 138.)
37. JackSS,NationalCenterfor HealthStatistics. Useof dentalservices, United States, 1983. Advance data no 122, Aug 8,1986.
38. National Center for Health Statistics. Health survey procedure. Washington, D C US Department of Health, Education and Wel- fare, 1964; PHS pub no 1000. (Vital and health statistics; series l; no 2.)
39. National Center for Health Statistics. Current estimates from the health interview survey, United States, 1983. Hyattsville, M D US
Department of Health, Education and Welfare, Jun 1986; DHHS pub no (PHS) 86-1582. (Vital and health statistics; series 10;no 154.)
40. Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United Sta tes. Milbank Mem Fund Q
41. Aday LA, Andersen R. Framework for the study of access to medical care. Health Serv Res 1974;9208-20.
42. Wolinsky FD. Assessing the effects of predisposing, enabling, and illnessmorbidity characteristics on health services utilization. J Health Soc Behav 1978;19(4):38496.
43. Evashwick C, Conrad D, Lee F. Factors related to utilization of dentalservices by the elderly. Am J Public Health 1982;72(10):1129- 35.
44. Wilson AA, Branch LG. Factors affecting dental utiliza tion of elders aged 75 years and older. J Dent Educ 1986;50(11):673-7.
45. Kiyak HA. An explanatory model for older person’s use of dental services: implications for health policy. Med Care 1987;25(10):936- 52.
46. Grembowski D, Andersen RM, Chen MS. A public model of the dental care process. Med Care Rev 1989;46(4):439-96.
47. Kovar MG, Poe GS. The national health survey design, 1973-84. Hyattsville, MD: National Center for Health Statistics, 1985; DHHS pub no (PHS)85-1320. (Vital and health statistics; series 1; no 18.)
1973;51:95-124.
CALL FOR NOMINEES
AMERICAN DENTAL ASSOCIATION GOLD MEDAL AWARD
FOR EXCELLENCE IN DENTAL RESEARCH
OBJECTIVE To honor individuals who through basic or clinical research contribute to the advancement of the profession of dentistry or to major improvement in the oral health of the community.
AWARD AND RECOGNITION The individual selected will receive $25,000 and a gold medallion at a formal presentation at the 135th Annual Session of the American Dental Association in New Orleans, LA, in October 1994. All expenses for the recipient’s travel and lodging in New Orleans will be provided by the Association. The ADA Gold Medal Award for Excellence in Dental Research will be awarded once every three years.
SPONSORSHIP The award is jointly sponsored by the ADA and Unilever, whose generous support includes half the funding for the award.
NOMINATION PROCEDURE Each candidate’s qualifications should be set forth in a formal letter of nomination that is accompanied by a curriculum vitae and list of publications.
DEADLINE All nominations must be received at ADA headquarters by June 15,1995. Please direct letters of nomination to: Dr. John S. Zapp, Executive Director, American Dental Association, 211 East Chicago Avenue, Chicago, IL 6061 1-2678; tel. 312440-2549.

![Acts 20:17-36. elders bishops pastors Acts 20:27-36 elders bishops pastors elders Acts 20:17-36 - Paul called for the elders from Ephesus [v. 17] - Paul](https://img.pdfslide.net/doc/110x75/55151146550346a87d8b4ad2/acts-2017-36-elders-bishops-pastors-acts-2027-36-elders-bishops-pastors-elders-acts-2017-36-paul-called-for-the-elders-from-ephesus-v-17-paul.jpg)