Embed Size (px)
Citation preview

ANAESTHESIAANAESTHESIA
Generaland
RegionalAnaesthesia
KARIM 2 LF a FN MOTOL

AnaesthesiaAnaesthesia
� The Greek philosopher Dioscorides first used the term anaesthesiain the first century AD to describe the narcotic-like effects of the plant mandragora.
� The term subseguently was defined in Bailey‘s An Universal Etymological English Dictionery (1721) as „a defect on sensation“and again in the Encyclopedia Britannica (1771) as “privation of the senses.“
� The present use of the term to denote the sleeplike state that makes possible painless surgery is credited to Oliver W. Holmes in 1846.
� Use the term anaesthesiology to denote the practice of anaesthesia was first propesed in the second decade of the 20th century (in the USA) to emphasize the growing scientific basis of the specialty.

Modern historyModern history�� DiethyleterDiethyleter-- originally prepared in 1540 by Valerius Cordus, first time originally prepared in 1540 by Valerius Cordus, first time
used as an anaesthetic agent in humans 1842. C.W.Long and used as an anaesthetic agent in humans 1842. C.W.Long and W.E.Clark used it independently on patients. W.E.Clark used it independently on patients. They did not publicize They did not publicize this this discovery. On October 16, 1846 in Boston discovery. On October 16, 1846 in Boston William T.G.Morton William T.G.Morton conducted the first publicised demostration of general anaesthesconducted the first publicised demostration of general anaesthesiaia
�� ChlorophormChlorophorm independently prepared by von Liebig, Gutrrie and independently prepared by von Liebig, Gutrrie and Souberian in 1831, first time used by Holems Coote in 1847Souberian in 1831, first time used by Holems Coote in 1847
�� NN22OO prodused by J.Priestly in 1772, analgesic properties firt notedprodused by J.Priestly in 1772, analgesic properties firt noted by by H. Davy 1800, G. Colton and H. Wells first used as an anesthetH. Davy 1800, G. Colton and H. Wells first used as an anesthetic in ic in humen in 1844humen in 1844
�� CocaineCocaine isolated from coca plant in1855 by Gaedicke, purified in 1860 isolated from coca plant in1855 by Gaedicke, purified in 1860 by A. Neimann, used of topical cocain for surgical anesthesia ofby A. Neimann, used of topical cocain for surgical anesthesia of the the eye in 1884 by C. Koller, first SA 1898 A.Biereye in 1884 by C. Koller, first SA 1898 A.Bier
�� ProcainProcain was synthesized in 1904, within the year used clinicalywas synthesized in 1904, within the year used clinicaly
�� Lumbar epid .anaesthesia was described in 1921Lumbar epid .anaesthesia was described in 1921
Modern historyModern history
�� ThiopentalThiopental synthetised in 1932 by Vorwiler and Tabern, used clinically synthetised in 1932 by Vorwiler and Tabern, used clinically by J. Lundy and R. Waters in 1934 and remains the most common by J. Lundy and R. Waters in 1934 and remains the most common induction agent for anesthesia induction agent for anesthesia
�� KetaminKetamin synthesized in 1962 by Stevens and clin. used by Corssen synthesized in 1962 by Stevens and clin. used by Corssen 1965 (minimal cardiac and resp. depresion)1965 (minimal cardiac and resp. depresion)
�� EtomidatEtomidat synthetised in 1964 and release in 1972 synthetised in 1964 and release in 1972 –– initial enthusiasm initial enthusiasm over its relative lack of circulatory and respir. effects was teover its relative lack of circulatory and respir. effects was tempered by mpered by reports of adrenal suppresionreports of adrenal suppresion
�� Propofol Propofol release in 1989 was a major advace in outpatient ansthesiarelease in 1989 was a major advace in outpatient ansthesia
�� Opiods:Opiods:
Morphin was isolated from opium 1805 and subsequently triedMorphin was isolated from opium 1805 and subsequently tried as an as an intravenous anaestheticintravenous anaesthetic
�� Muscle RelaxantsMuscle Relaxants: Griffith and Johnson 1942 !! Curare: Griffith and Johnson 1942 !! Curare
Neuromuscular blocking agentsNeuromuscular blocking agents
The discovery of surgical anaesthesia is considered one of the most important in human history
Biggest gift dedicatet to medical art.S.B.Nuland: LS.B.Nuland: Léékakařřstvstvíí v prv průůbběěhu stalethu staletíí, Kni, Knižžnníí klub, Praha 2000 klub, Praha 2000

DiferenciesDiferencies

The first operation with ether (1882-1893

ČČechy echy -- 7.2.18477.2.1847
16 weeks after Boston presentetion11 days after Vienaany sefety tests any randomize studyno registration
ONLY FROM THE ARTICLE OF MEDICAL JOURNAL !!
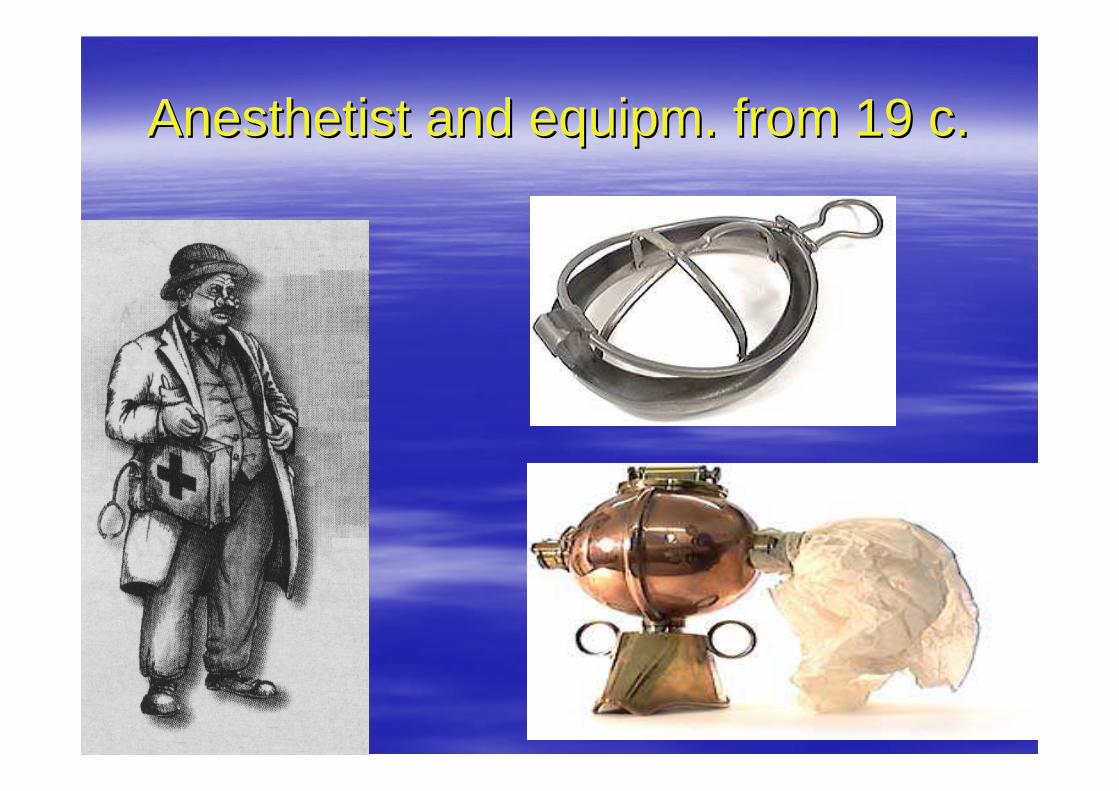
Anesthetist and equipm. from 19 c.Anesthetist and equipm. from 19 c.

Definition of the practice of anaesthesiologyDefinition of the practice of anaesthesiology
� Assessing, consulting and preparing patients for anaesthesia� Rendering patients insensible to pain during surgical, obstetric,
terapeutic, and diagnostic procedures� Monitoring and restoring homeostasis in perioperative and critically ill
patients� Diagnosing and treating painful syndromes� Managing and teaching of cardiac and pulmonary resuscitation� Evaluating respiratory function and applying respiratory therapy� Teaching, supervising, and evaluating the performance of medical and
paramedical personnel involved in anaesthesia, respiratory and critical care
� Conducting research at the basic and clinical science levels to explain and improve the care of patients in terms of physiological function and drug response
� Involment in administration of hospitals, medical schools and outpationet facillities as necessary to implement these responsibilities
Adapted from the American Board of Anesthesiology Bookled, January 2000
AnaesthesiaAnaesthesia
–– Preoperative assessmentPreoperative assessment
–– Anaesthesia: Anaesthesia: general general regional or localregional or local
monitored anestesia caremonitored anestesia care
–– Postoperative analgesiaPostoperative analgesia
………………………………………………………………………………………………………………
–– Chronic pain Chronic pain –– pain clinicpain clinic
–– ICU/ITUICU/ITU
–– CPR CPR -- integral members of resuscitation teamsintegral members of resuscitation teams

PreoperativePreoperative assessmentassessment
�� Routine preoperative evalutionRoutine preoperative evalution
�� ConsentConsent
�� Premedication drugsPremedication drugs
�� FastingFasting
�� Profilaxis of venous trombosisProfilaxis of venous trombosis
�� OptimalizationOptimalization
�� Assesment of risk (ASA 1Assesment of risk (ASA 1--5, MET 15, MET 1--7)7)

Routine preoperative anesthetic Routine preoperative anesthetic evalutionevalution
� History :� Current problem� Other known problems� Medication history
– Allergies– Drug intolerances– Present therapy: Prescription x Nonprescription– Nontherapeutic: Alcohol
Tobacco– Illicid

Routine preoperative anesthetic Routine preoperative anesthetic evalutionevalution
� History :� Previous anesthetics, surgery, and obstetric
deliveries� Family history� Review of organ systems
– General ( including activity level )– Respiratory and Cardiovascular– Renal, GIT, Hematologic, Neurologic– Endocrine, Psychiatric, Orthopedic, Dermatologic
� Last oral intake
Routine preoperative anesthetic Routine preoperative anesthetic evalutionevalution
� Physical examination1. Vital singns
2. Airway3. Heart4. Lungs5. Extremities6. Neurologic examination
� Laboratory evaluation
� ASA classification

Routine preoperative laboratory Routine preoperative laboratory evalution of asymptomatic, aparently evalution of asymptomatic, aparently
healthy patientshealthy patients
� Serun electolyte measusments� Urianalysis� Hematocrit or hemoglobin concentration� Serum glucose and creatinine (or blood urea nitrogen)
concentration� Coagulation studies� ECG� Chest radiograph

Routine preoperative laboratory Routine preoperative laboratory evalution of asymptomatic, aparently evalution of asymptomatic, aparently
healthy patientshealthy patients
� Serun electolyte measusments ?� Urianalysis ?� Hematocrit or hemoglobin concentration (All menstr. women,
pts over 60 years of age, pts who are likely to experince signif. blood loss and may require transfusion!)
� Serum glucose and creatinine (or blood urea nitrogen) concentration ( pts over 60years of age )
� Coagulation studies� ECG ( pts over 40, or female over 50 years of age )
� Chest radiograph ( pts over 60 years of age )

Preoperative physical status Preoperative physical status classification of patient: ASAclassification of patient: ASA
Class Definition 1 A normal healthy patient
2 A patient with mild systemic disease and no functional limitation
3 A patient with moderate to severe systemic disease that results in some functionl limitation
4 A patient with severe systemic disease that is a constant threat to life and functionally incapacitating
5 A moribund patient who is not expected to survive 24 hours with or without surgery
6 A brain-dead patient whouse organs are being harvestedE If the procedure is an emergency,the physical status is
followed by „E“ (for example: „ 2E“)

The anesthetic planThe anesthetic plan� Premedikation� Type of anesthesia
General, /GA/: Airway management, Induction, Maintainance, + - Muscla relaxation
Local or regional anesthesia, /RA/: Technique and agentsMonitored anesthesia care: Supplement oxygen, Sedation
� Intraoperaive managementMonitoring, Positioning, Fluid management, Spec. techniques
� Postoperative management:Intensive care, Postop. ventilation, Hemodynamic monitoringPain control
Informed ConsentInformed Consent� The preoperative assesment culminates in giving the pt. a reasonable
explanation of the options available for anesthesia management: (general, regional, local, etc)
� Regardless of the technique chosen, consent must always be obtained for general anesthesia in case other technicques prove inadequate.
� If any procedure is perfomed without the pt.s consent, the physician may be liable for assault and battery
� Oral consent may be sufficient, written consent is usually advisible for medicolegal purposes
� Consent must be infomed to ensure that the pt. has suficient information about the procedures and their risks to make a reasonable and prudent decision whether to consent

� Form No. 3� FAKULTNÍ NEMOCNICE V MOTOLE� (UNIVERSITY HOSPITAL MOTOL)� ___________________________________________________________________________� V ÚVALU 84, 150 06 PRAGUE 5� Tel.: 2 2443 …….., Fax: 2 2443 ……..� Clinic ………………………………� Informed consent of patient (legal representative) with the administration of anaesthesia in connectio n with examination or with surgery � First name and last name of doctor-anaesthesiologist: ..............………………………….......................� First name and last name of patient: …………………........……Identification number……………..� To be completed by the physician:� Type of anaesthesia/sedation: � � General � � Field blocking � � Sedation during consciousness� � Intubation with fibrescope� I do hereby declare that I have informed the patient (legal representative) about the method of planned anaesthesia/sedation, which will be administered in
connection with the procedure/treatment in the case of the diagnostic procedure chosen. At the same time I have informed the patient about possible complications and risks and especially those, which are most serious:
� General risks of general anaesthesia (harming the veins, teeth, breathing passages, as well as the possibility of post-operational sickness and vomiting, retention of urine, etc.)
� General risks of field blocking (damage to veins, back pain during desensitization in the area of the backbone, rarely difficulties in sensitivity and movement in anaesthetised areas after anaesthesia subsides, retention of urine, etc.)
� Patient (legal representative of patient):� 1. Please read carefully both sides of this page.� 2. If you did not fully understand the doctor’s explanation, or if you need further or complementary information, do not hesitate to ask a doctor. � 3. If you agree with the contents of this text, please sign it. � I the patient (legal representative):� I do hereby declare that I have understood the information provided and was informed in a comprehensible way by the doctor about the character and
procedure of the anaesthesia used, and that I was also informed about possible risks and complications of this procedure. The doctor further informed me about possible alternatives and consequences of anaesthesia used. I have had the opportunity to ask the doctor any other questions, and when I did so, all of my questions were answered, and I understood all of the answers.
�
� On the basis of this statement, I do declare that I agree:� - with the administration of this type of anaesthesia/sedation� - with the possibility that another treatment may be undertaken if my health or life might be endangered if this would not be undertaken.� I am aware of the fact that:� - the mentioned type of anaesthesia/sedation does not have to be administered by the doctor who has examined me and informed of procedures to be
undertaken. � In Prague on …………20…� ……………………………………. …………………………………….................� Doctor´s signature Patient´s signature (his/her legal representative)� Identification of legal representative: � First name and last name: ……………………………………………………� Date of birth: ………………………� Relationship to patient: ………………………

Premedication drugsPremedication drugs
�� Sedatives: anxiolytic Sedatives: anxiolytic -- benzodiazepines, +antihistaminsbenzodiazepines, +antihistamins
(Lorazepam, Oxazepam, Midazolam, +Dithiaden)(Lorazepam, Oxazepam, Midazolam, +Dithiaden)
�� Analgetic: opioids (Morphine, Pethidine)Analgetic: opioids (Morphine, Pethidine)
NSAID, ParacetamolNSAID, Paracetamol
�� Anticholinergic: ( Atropin, Scopolamin, Glycopyrolate ) Anticholinergic: ( Atropin, Scopolamin, Glycopyrolate )
�� Prokinetic: MetoclopramideProkinetic: Metoclopramide
�� Gastric pH incrising: (H2 blockers, protons pump inhibitors)Gastric pH incrising: (H2 blockers, protons pump inhibitors)


General anesthesiaGeneral anesthesia
�� InductionInduction
�� MaintainanceMaintainance
�� End End –– emergeemerge
�� Postoperative pain managmentPostoperative pain managment

Steps before induction of GASteps before induction of GA
�� I.v. canulaI.v. canula
�� Monitoring of vital sings:Monitoring of vital sings:
–– Circulation: Circulation: ECG, BP ECG, BP ––NIBP or aBP, Sat.ONIBP or aBP, Sat.O22, ,
CVP?, SG /PA/ cath., urine cath.CVP?, SG /PA/ cath., urine cath.
–– Others: T st.C, specific (neurosur.)Others: T st.C, specific (neurosur.)
–– Ventilation: Ventilation: endt.COendt.CO22,, TV, RR, (MV) + gases (FiOTV, RR, (MV) + gases (FiO22, inh. , inh. gases)gases)

Drugs for GADrugs for GA
�� Hypnotic /intravenous: Hypnotic /intravenous:
Sod.Thiopenton, PropofolSod.Thiopenton, Propofol, Hypnomidat, diazepins, Hypnomidat, diazepins
�� Inhalation: Halotan, Enfluran,Inhalation: Halotan, Enfluran,
Isofluran, Sevofluran, DesfluranIsofluran, Sevofluran, Desfluran
�� Opioids: Mo., Pethidin?, Piritramid Opioids: Mo., Pethidin?, Piritramid Fentanil + Al., Su., RemiFentanil + Al., Su., Remi

ThiopentalThiopental
�� most useful (until recent years) most useful (until recent years) i.v. anesteticumi.v. anesteticum
�� negative inotropic effect + periferal vazodilatancenegative inotropic effect + periferal vazodilatance
�� transient stimulation, apnoe, decrease of MV, risk transient stimulation, apnoe, decrease of MV, risk of laryngospasmus, bronchoconstrictionof laryngospasmus, bronchoconstriction
�� effect of sedation is terminate by redistributioneffect of sedation is terminate by redistribution
�� ordinary dosis is 5 mg/kgordinary dosis is 5 mg/kg
�� pH 9,5 strictly only i.vpH 9,5 strictly only i.v..

ThiopentalThiopental
Diprivan (propofol)Diprivan (propofol)
�� short acting i.v. anesteticum for induction and also short acting i.v. anesteticum for induction and also for maintenance of anesthesiafor maintenance of anesthesia
�� negativ inotropic + periferal vasodilatancenegativ inotropic + periferal vasodilatance
�� short apnoeshort apnoe
�� dosis dosis
–– 2,02,0--2,5 mg/kg for induction2,5 mg/kg for induction
–– 66--12 mg/kg/hr = 0,112 mg/kg/hr = 0,1--0,2 mg/kg/min. for 0,2 mg/kg/min. for maintenancemaintenance


Hypnomidate (etomidat)Hypnomidate (etomidat)
�� general i.v. anaestheticgeneral i.v. anaesthetic
�� minimal influence of circulatory systemminimal influence of circulatory system
�� ventilation is a little superficial, but no apnoic ventilation is a little superficial, but no apnoic pausepause
�� myoclonic movementsmyoclonic movements
�� depresion of cortiocoid synthesisdepresion of cortiocoid synthesis
�� dosis 0,25 dosis 0,25 -- 0,3 mg/kg0,3 mg/kg
�� for induction of anaesthesia for patients with heart for induction of anaesthesia for patients with heart problemsproblems

Narkamon (ketamin)Narkamon (ketamin)
�� general i.v. anaestetic and general i.v. anaestetic and analgeticanalgetic
�� increases BP and HRincreases BP and HR
�� stimulation of breathingstimulation of breathing
�� no effect on visceral pain ?no effect on visceral pain ?
�� dosage:dosage:
–– 1,01,0--2,0 mg/kg i.v. as anaesthetic2,0 mg/kg i.v. as anaesthetic
–– 55--10 mg/kg i.m. as anaesthetic10 mg/kg i.m. as anaesthetic
–– 0,250,25--0,5 mg/kg i.v. as analgetic0,5 mg/kg i.v. as analgetic

Dormicum (midazolam)Dormicum (midazolam)
�� Effect is dependent on doseEffect is dependent on dose
–– anxiolysisanxiolysis
–– amnesiaamnesia
–– euforiaeuforia
–– sedation till hypnotic effectsedation till hypnotic effect
�� Minimal cardiovascular depressionMinimal cardiovascular depression
�� Mild depression of breathingMild depression of breathing
�� Dose Dose –– always titratealways titrate

CFCF33CHClOCFCHClOCF22H H IsofluranIsofluran
�� Halogenated ether, no analgetic potencyHalogenated ether, no analgetic potency
�� MAC 1,17MAC 1,17 BG 1,4BG 1,4
�� Depression of breathingDepression of breathing
�� Periferal vasodilatance, steal fenomenon?Periferal vasodilatance, steal fenomenon?
�� Minimal metabolism 0,2 %Minimal metabolism 0,2 %
�� Application usualy with NApplication usualy with N22O , in O , in conc. 1,0conc. 1,0--2,5 %2,5 %
CFCF33CFCF33CHOCHCHOCH22FF SevofluranSevofluran
�� Halogenated ether, no analgetic potenceHalogenated ether, no analgetic potence
�� MAC 2 %MAC 2 % BG 0,69BG 0,69
�� No irritatition of airwaysNo irritatition of airways
�� Easy to guideEasy to guide
�� Minimal effect on circulationMinimal effect on circulation
�� not organotoxic !!, but probably cardioprotectivenot organotoxic !!, but probably cardioprotective
�� enviromentallyenviromentally--frendlyfrendly

CF2HOCFHCF3CF2HOCFHCF3 DesfluranDesfluran
�� Halogenated ether, no analgetic potenceHalogenated ether, no analgetic potence
�� MAC 6 %MAC 6 % BG 0,42BG 0,42
�� Easily guidedEasily guided
�� Minimal influence on circulation,mild stimulation of Minimal influence on circulation,mild stimulation of sympaticussympaticus
�� Boiling point 23,5Boiling point 23,5oo C, very different vaporizer C, very different vaporizer (blender)(blender)

Any anestetics has a specific Any anestetics has a specific spectrum of effectsspectrum of effects
Alkire MT: Science 322, 876 (2008)

OpiodsOpiods
�� opiumopium
–– alkaloids morphinealkaloids morphine
–– codeine (metylmorphine)codeine (metylmorphine)
�� semisynthetic opioidssemisynthetic opioids
–– heroin (diacetylmorphine)heroin (diacetylmorphine)
�� syntetic opioids syntetic opioids -- phentanylsphentanyls

Fentanyl grupFentanyl grup
�� fentanylfentanyl
�� sufentanilsufentanil
�� alfentanilalfentanil
�� remifentanilremifentanilfentanyl

General anaestesie General anaestesie -- GAGA
�� i.v. only i.v. only –– TIVATIVA
�� Inhalational only Inhalational only -- VIMAVIMA
�� Combination of i.v. + inhalational Combination of i.v. + inhalational -- balancebalance
..………………………………………………………………………………………………………………......
�� Without protection of airway Without protection of airway –– OO22 mask, face maskmask, face mask
�� With protection of airway With protection of airway –– LMA, LMA, ETT!ETT!

Muscle relaxantsMuscle relaxants
�� Depolarizing: Suxamethoniun Depolarizing: Suxamethoniun
�� NonNon--depolarizing (NDMRs)depolarizing (NDMRs)
–– Clasification according duration Clasification according duration ( short, medium, long)( short, medium, long)
–– Clasification according chemistryClasification according chemistry�� Aminosteroids: pancuronium, Aminosteroids: pancuronium, vecuronium, rocuroniumvecuronium, rocuronium, ,
pipecuroniumpipecuronium
�� Benzylisoquinolineums: mivacurium, atra. + Benzylisoquinolineums: mivacurium, atra. + cisatracuriumcisatracurium
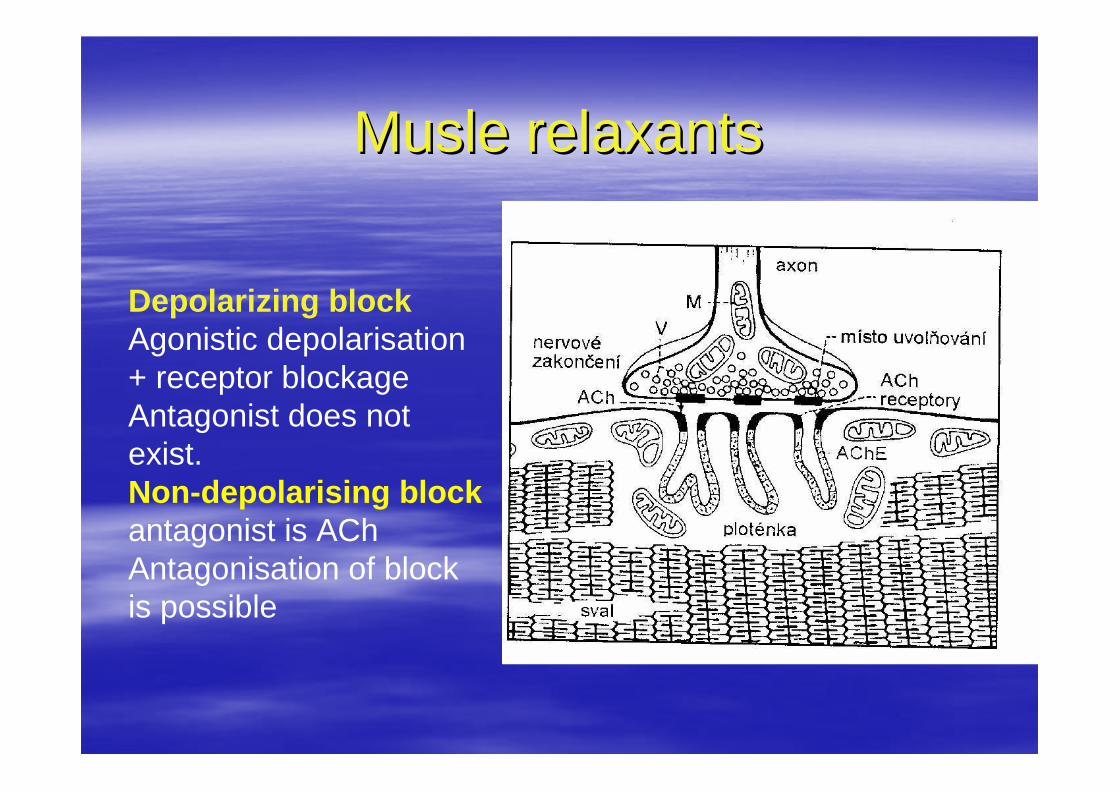
Musle relaxantsMusle relaxants
Depolarizing blockAgonistic depolarisation + receptor blockageAntagonist does not exist. Non-depolarising blockantagonist is AChAntagonisation of block is possible








DecurarisationDecurarisationAntidotum of musle relaxantAntidotum of musle relaxant
�� Nonspecific: increasing Acetylcholine /nicotinic + Nonspecific: increasing Acetylcholine /nicotinic + muscarinic effect:muscarinic effect:–– Neostigmin (2,5 Neostigmin (2,5 –– 5 mg), inhibition of cholinesterasis5 mg), inhibition of cholinesterasis
–– Physostigmin (0,5 Physostigmin (0,5 –– 1 mg)1 mg)
alwais together vith Atropin (1alwais together vith Atropin (1--2mg) or Glycopyrrolate 2mg) or Glycopyrrolate /antimuscarinic/antimuscarinic
�� Specific:Specific:–– Bridion /SugammadexBridion /Sugammadex
Reversal effect for Reversal effect for rocuroniumrocuronium, vecuronium , vecuronium

AnesthesiologicaAnesthesiologica
�� thiopentalthiopental�� propofol, midazolam, etomidate, ketaminepropofol, midazolam, etomidate, ketamine�� isoflurane, sevoflurane, desfluraneisoflurane, sevoflurane, desflurane�� nitrous oxidenitrous oxide�� succinylcholine iodidesuccinylcholine iodide�� vecuronium, rocuronium, vecuronium, rocuronium,
atracurium, cisatracurium, cis--atracuriumatracurium�� fentanyl, sufentanil, alfentanil, remifentanilfentanyl, sufentanil, alfentanil, remifentanil
Fluid managmentFluid managment
CrystaloidsCrystaloids x coloids x blood componentsx coloids x blood components
………………………………………………………………………………………………..�� Minor procedures (1,5 Minor procedures (1,5 –– 2ml/kg/hod.)2ml/kg/hod.)
�� Mild, moderate procedures (4 Mild, moderate procedures (4 –– 5 ml/kg/hod.)5 ml/kg/hod.)
�� Advanced procedures (8Advanced procedures (8--10ml/kg/hod.)10ml/kg/hod.)
………………………………………………………………………………………………
�� Other fluids according to blood and other lost fluids Other fluids according to blood and other lost fluids

Intraoperative transfusion therapyIntraoperative transfusion therapy
� Red cells –PRCs
� Fresh frozen plazma – FFP
� Platelets
� Cryoprecipitate
� Fibrinogene
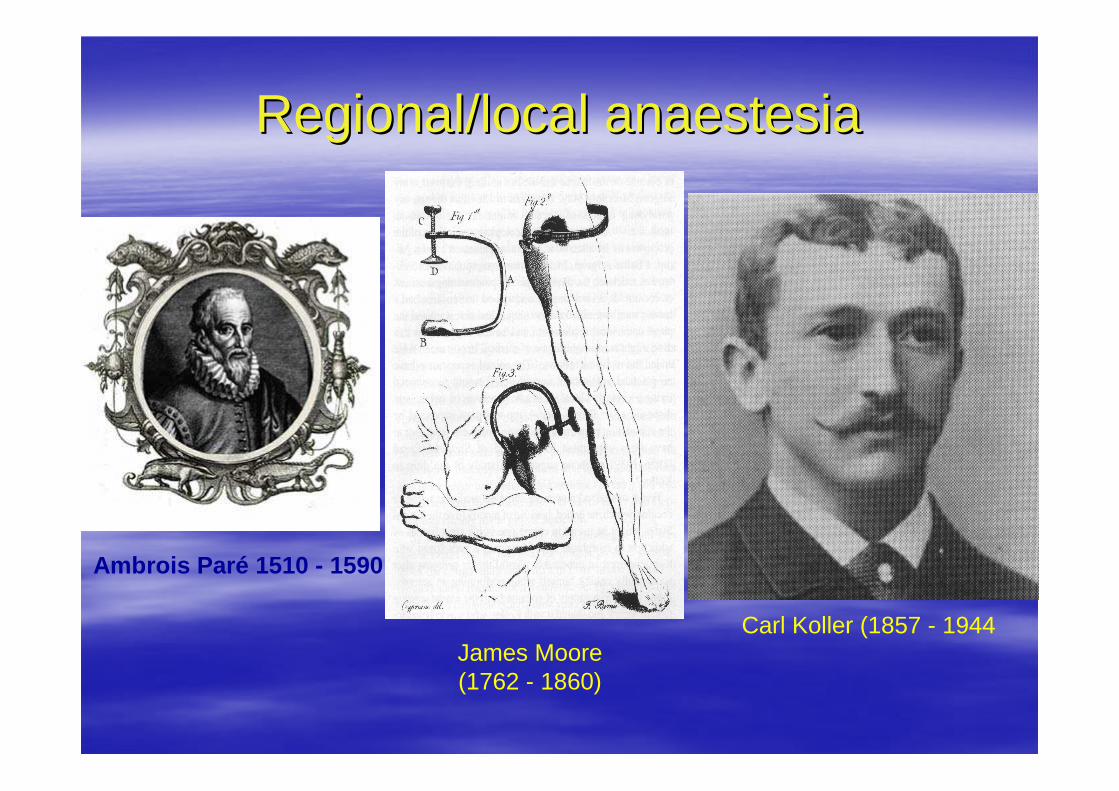
Regional/local anaestesiaRegional/local anaestesia
Carl Koller (1857 - 1944James Moore (1762 - 1860)
Ambrois Paré 1510 - 1590

CocaineCocaine
1855 – Gaedecke: erythroxylin1862 – Niemann: cocaine1884 – Freud: effects on CNS1884 – Koller: cocaine as LA1984 – ESRA: prize of C. Koller

Regional/local anaestesiaRegional/local anaestesia�� Pharmacology of local anestetics:Pharmacology of local anestetics:
–– Esters: old, minim. used today Esters: old, minim. used today (cocaine, procain, benzocain,) (cocaine, procain, benzocain,)
degradation by plasma cholinesterasedegradation by plasma cholinesterase
–– Amid: newer, short, medium or long actingAmid: newer, short, medium or long acting
degradation by microsomal enzymes in the liverdegradation by microsomal enzymes in the liver�� Lidocaine:Lidocaine: rapid onset, short action, moderate vasodilatationrapid onset, short action, moderate vasodilatation
�� Prilocain: short acting, no vasodilatationPrilocain: short acting, no vasodilatation
�� Bupivacain: Bupivacain: long acting, profound cardiotoxicitylong acting, profound cardiotoxicity
�� RopivacainRopivacain: long acting, less cardiotoxicity. Reduced intensity : long acting, less cardiotoxicity. Reduced intensity and duration of motor block and duration of motor block
Combination of diferent LA, LA + opioids, or LA + ClonidiCombination of diferent LA, LA + opioids, or LA + Clonidine, ne, or LA + vasoconstricotrs /epinefrin, phenylephrine,or LA + vasoconstricotrs /epinefrin, phenylephrine,


Local anesthesiaLocal anesthesia
�� Topics: high concentration of drug Topics: high concentration of drug -- sprayspray
cream /EMLA cream /EMLA
�� Infiltrations: usualy in surgeon handsInfiltrations: usualy in surgeon hands
…………………………………………………………………………………………………………………………………………....
�� Blocks: periferal Blocks: periferal -- regional /upper and distal extrem. neck, regional /upper and distal extrem. neck, headhead
central / NAB: spinal, central / NAB: spinal, epidural, epidural, caudalcaudal
Local anaesthetic toxicityLocal anaesthetic toxicity
�� Drug overdoseDrug overdose
–– Direct intravascular injectionDirect intravascular injection
–– Rapid absorption (highly vascular area)Rapid absorption (highly vascular area)
–– Continous infusion of LAContinous infusion of LA
–– Cumulative effect of multiple injectionCumulative effect of multiple injection

Local anaesthetics -wonder drugs or dangerous toxins?
Martin Jöhr

Local anestetic toxicityLocal anestetic toxicity

Local anestetic toxicityLocal anestetic toxicity
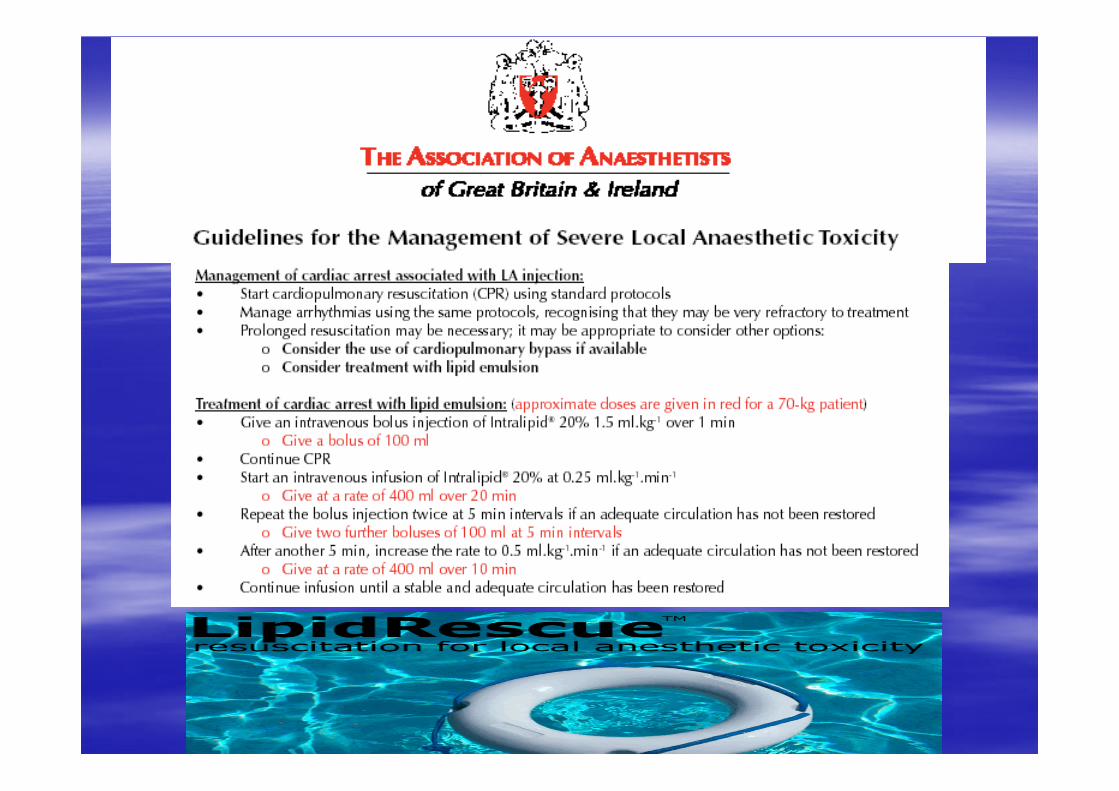
�� TreatmentTreatment–– Stop injection or infusion of LAStop injection or infusion of LA
–– ABCABC
–– Mild symtoms : oxygen + midazolamMild symtoms : oxygen + midazolam
–– Moderate to severe toxicity: cardiovascular collapse is normallModerate to severe toxicity: cardiovascular collapse is normally y preceded by convulsions. The first priority is, therefore, to ppreceded by convulsions. The first priority is, therefore, to prevent revent convulsion and maintain oxygenationconvulsion and maintain oxygenation
–– Consious level deteriorating or covulsions Consious level deteriorating or covulsions –– intubation + CMV intubation + CMV (S.Thiopenton +SCHJ, propofol or midazolam)(S.Thiopenton +SCHJ, propofol or midazolam)
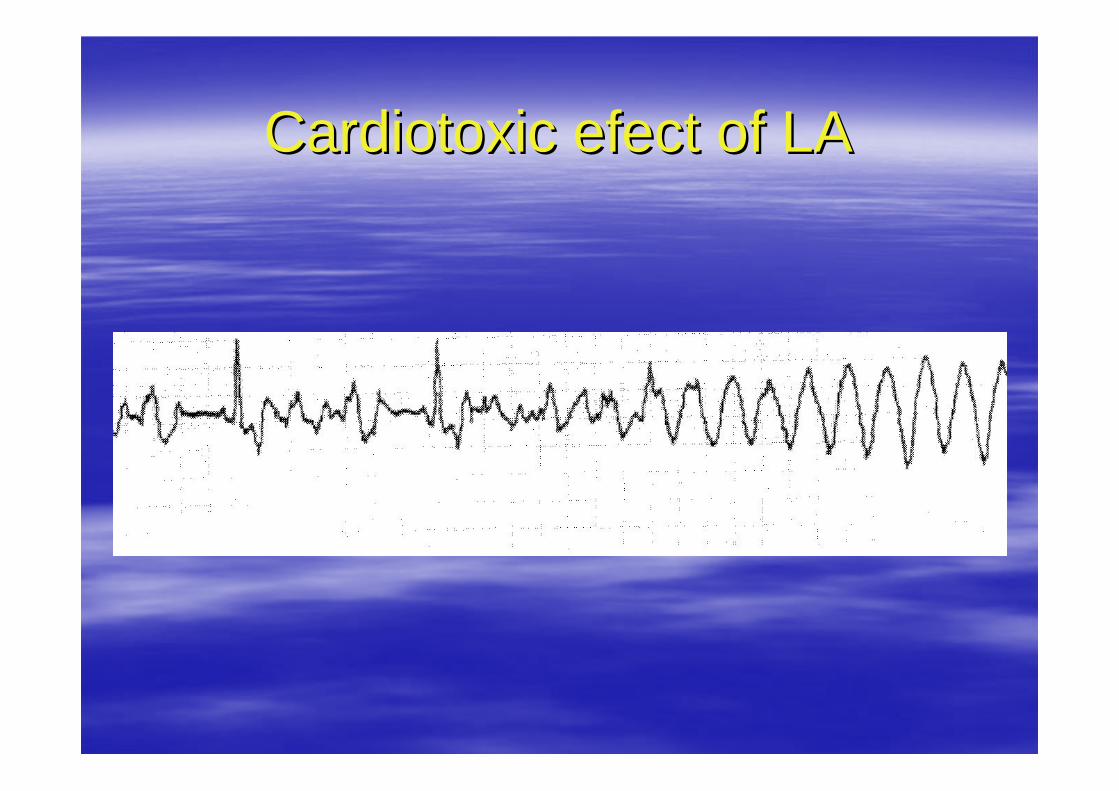
Cardiotoxic efect of LACardiotoxic efect of LA

Cardiotoxic efect of LACardiotoxic efect of LA
Editorial ViewsEditorial ViewsCardiac Arrest Following Regional Anesthesia Cardiac Arrest Following Regional Anesthesia with Etidocaine or Bupivacainewith Etidocaine or BupivacaineGeorge A. AlbrightGeorge A. AlbrightAnesthesiology, vol. 51, 1979, No. 4, pp. 285Anesthesiology, vol. 51, 1979, No. 4, pp. 285--287287
�� Accidental i.v.aplication of E. or B. can lead to Accidental i.v.aplication of E. or B. can lead to critical circulatory complicationcritical circulatory complication
�� Resuscitation of these situation is very difficult.Resuscitation of these situation is very difficult.

BP and Pis not change too muchCO decrease nearly about 40 %, SVR increase amplitude R driminish QRS widenNyström, E.U.M. et al.: Blood Pressure Is Maintained Despite Profound Myocardial Depression During Acute Bupivacaine Overdose in PigsAnesth Analg 1999; 88: 1143-48

Timing of toxic reactionTiming of toxic reaction
W. Zink, B. M. Graf : Toxikologie der Lokalanaesthetika: Pathomechanismen –- Klinik – Therapie. Der Anaesthesist 2003: 52: 1102 -1123
Regional anaestesieRegional anaestesie
�� Alergic reaction, anafylacsicAlergic reaction, anafylacsic
�� Incidence is very low, less 1% from all reaction on Incidence is very low, less 1% from all reaction on LALA

Central Central –– neuraxial blocksneuraxial blocks
�� Spinal block / Subarachnoidal block Spinal block / Subarachnoidal block –– SABSAB
�� Epidural blockEpidural block
�� Caudal blockCaudal block
……………………………………………………………………………………………………
diferences, pro x condiferences, pro x con
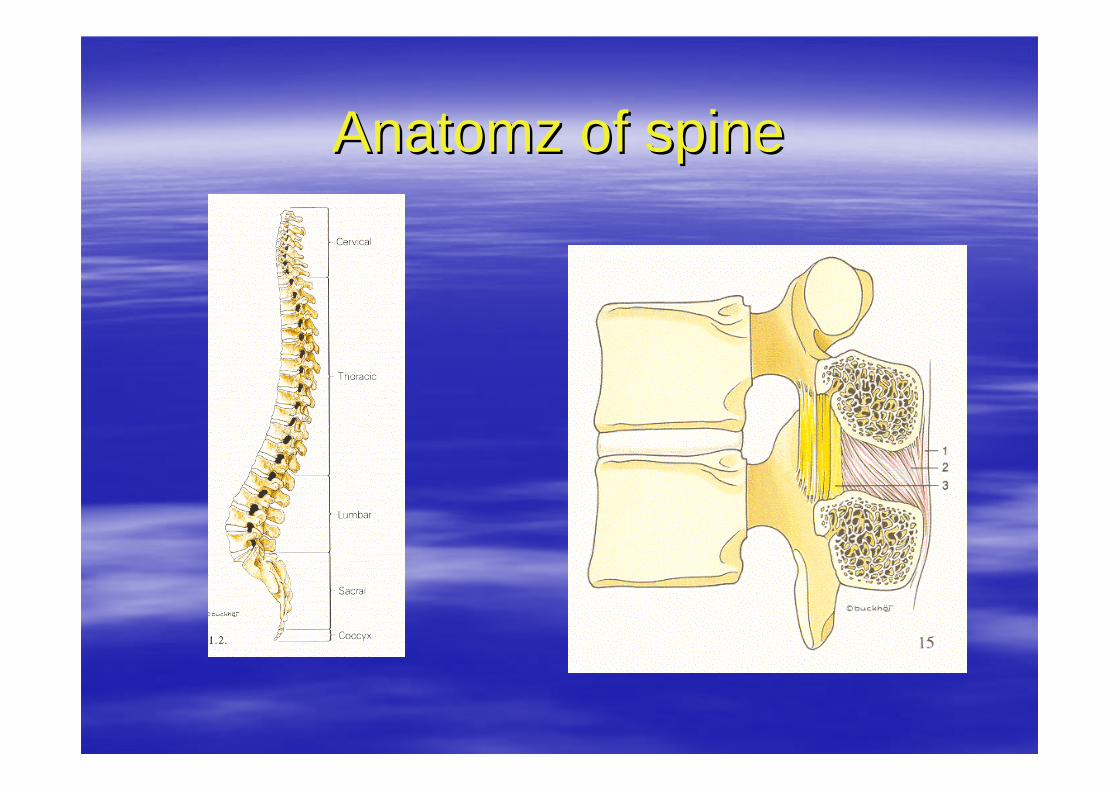
Anatomz of spineAnatomz of spine

Position of patient within Position of patient within puncturepuncture

Positioning of patient for S or EAPositioning of patient for S or EA

Approches to spinal chanelApproches to spinal chanel

SABSAB

SAB complicationSAB complication
�� HypotensionHypotension
�� BackacheBackache
�� HeamatomaHeamatoma
�� Postdural puncure headachePostdural puncure headache

Epidural anesthesiaEpidural anesthesia
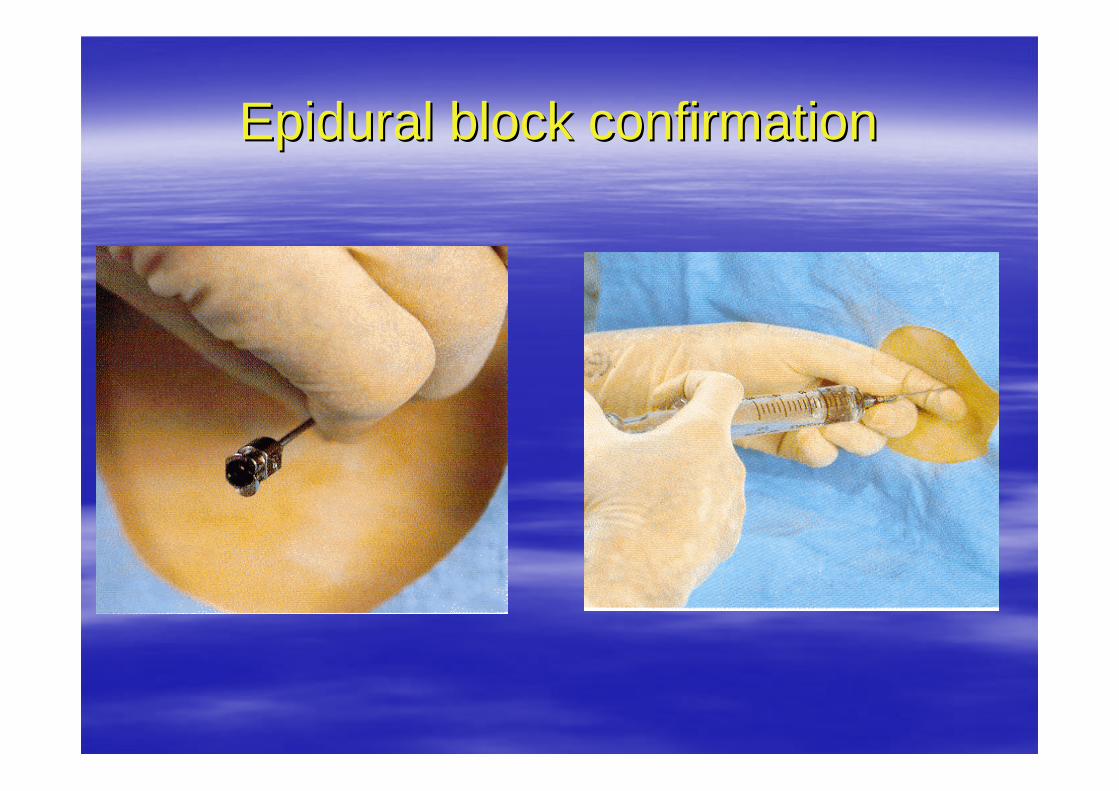
Epidural block confirmationEpidural block confirmation
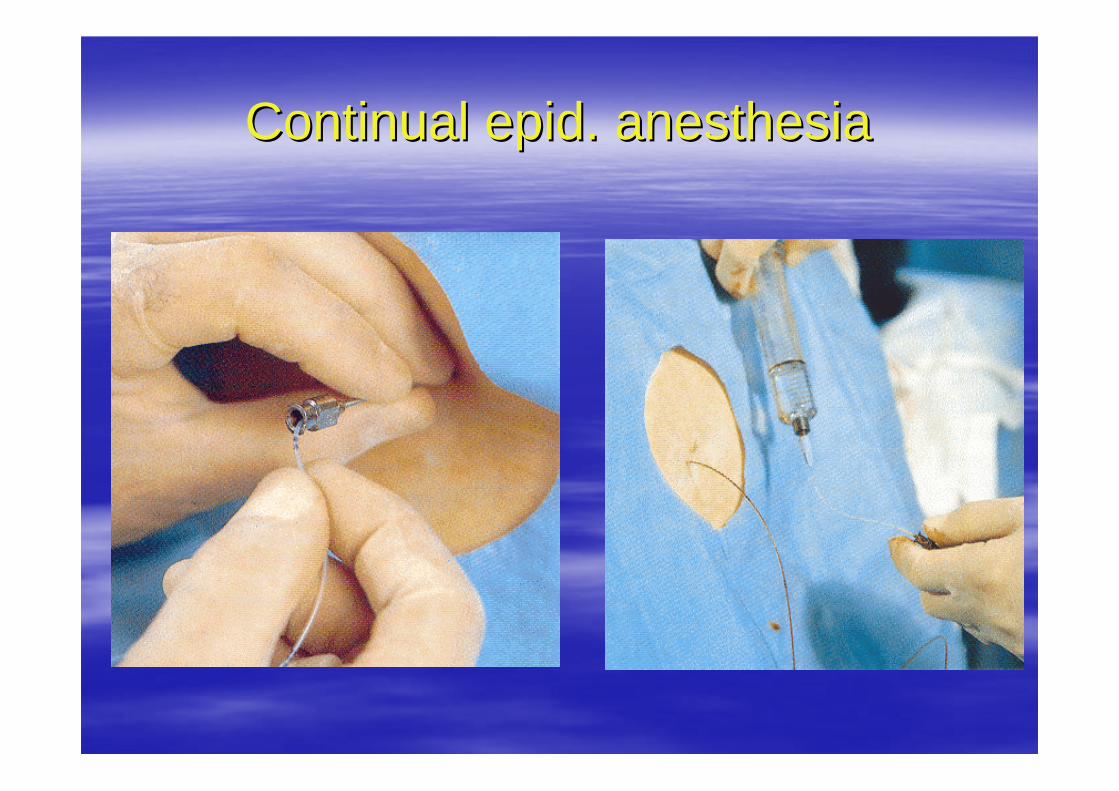
Continual epid. anesthesiaContinual epid. anesthesia
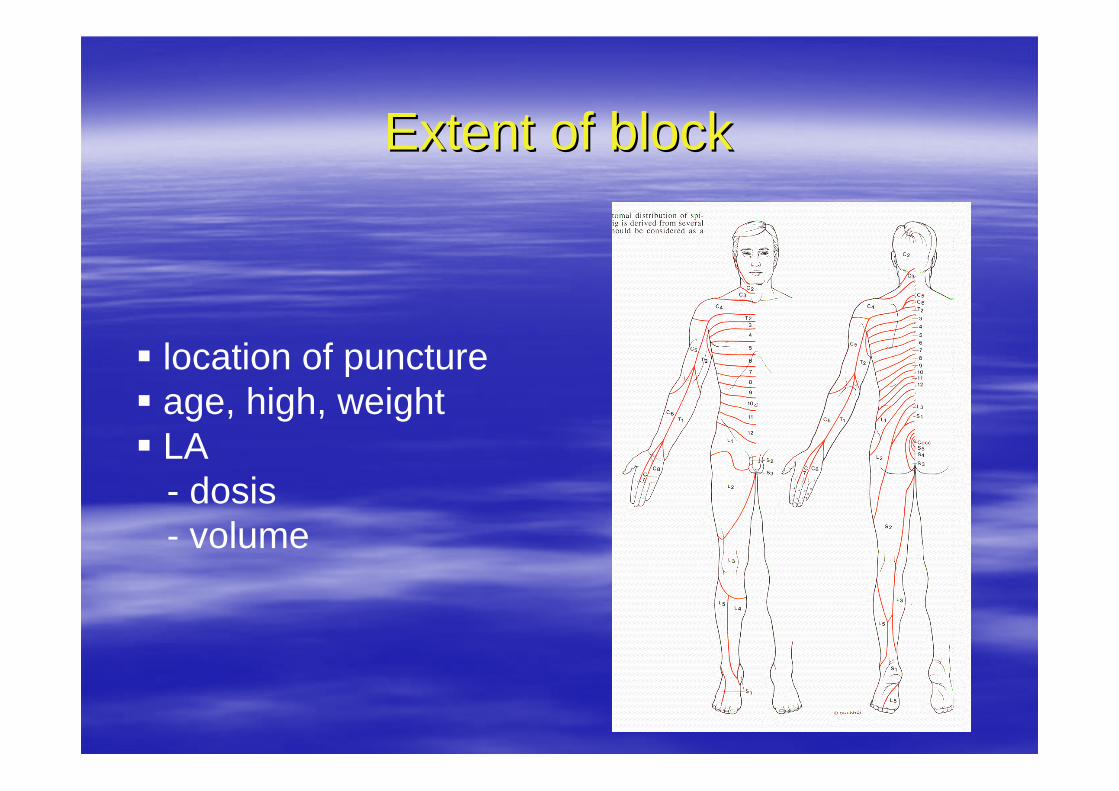
Extent of blockExtent of block
� location of puncture� age, high, weight� LA
- dosis - volume

Diferances between SA and EADiferances between SA and EA
SA SA -- advantageadvantage
�� simplesimple
�� easy localizationeasy localization
�� quick effectquick effect
�� profound anaesthesiaprofound anaesthesia
�� well control level of a.well control level of a.
�� risk of toxicity risk of toxicity ≈≈ 00
EPI EPI -- advantageadvantage
�� no puncture of durano puncture of dura
–– risk of PDPH lowrisk of PDPH low
–– risk of infectoin lowrisk of infectoin low
�� lesser hypotenionlesser hypotenion
�� segmental analgesiasegmental analgesia
�� senzomotoric senzomotoric separationseparation
�� time of time of anaesthesia/analgesiaanaesthesia/analgesia

Caudal blockCaudal block
Contraindications to NAB Contraindications to NAB �� RelativeRelative
–– Neurological disease (medicolegal)Neurological disease (medicolegal)
–– Previous back surgery or severe spinal deformityPrevious back surgery or severe spinal deformity
–– Aortic /mitral stenosis, Hypertrofic cardiomypathyAortic /mitral stenosis, Hypertrofic cardiomypathy
–– Hematological / clotting disorderHematological / clotting disorder
–– General infection /septicemie, bacteriemiaGeneral infection /septicemie, bacteriemia
–– Uncoperative patinetUncoperative patinet
�� Absolute:Absolute:
–– Local infectionLocal infection
–– Full therapeutic anticoagulationFull therapeutic anticoagulation
–– Increase intracranial preassureIncrease intracranial preassure
–– Severe hypovolemiaSevere hypovolemia
–– Severe aortic or mitral stenosisSevere aortic or mitral stenosis
–– Patient refusalPatient refusal
Postoperative analgesia
� Opiods /Mo, Pethidin ? Fentanyl +, Piritramid� NSAIDs / Ibuprufen, Diclofenac, COX2
� ASA /aspirin� Paracetamol – acetaminophen /Parfalgan/� Novalgin � Others /NAB – epidural, regional block…………………………………………………………….
Multimodal treatment approach


CPR CPR -- BLSBLS
NoNo
Unresponsive?
Open airway
Check breathing
Circulation pres.
Assess (for 10s)
Breathe
Recovery position
Chest compression
100/min
Rescue breathing ?
Pulse every min
YesYes
YesYes
Shake and shoutShake and shout
Look, listen and feelLook, listen and feel
Efective breathsEfective breaths
Sign of circulationSign of circulation
Head tilt/ chin liftHead tilt/ chin lift
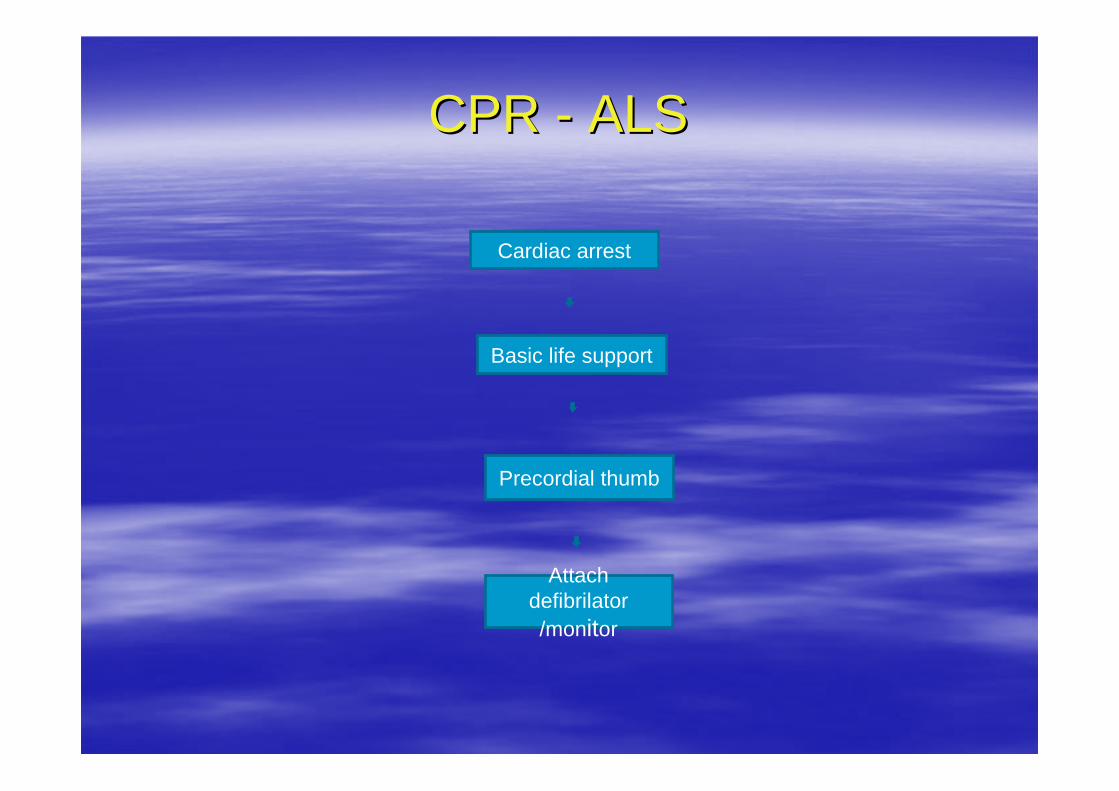
CPR CPR -- ALSALS
Basic life support
Cardiac arrest
Precordial thumb
Attach defibrilator /monitor
no no no no
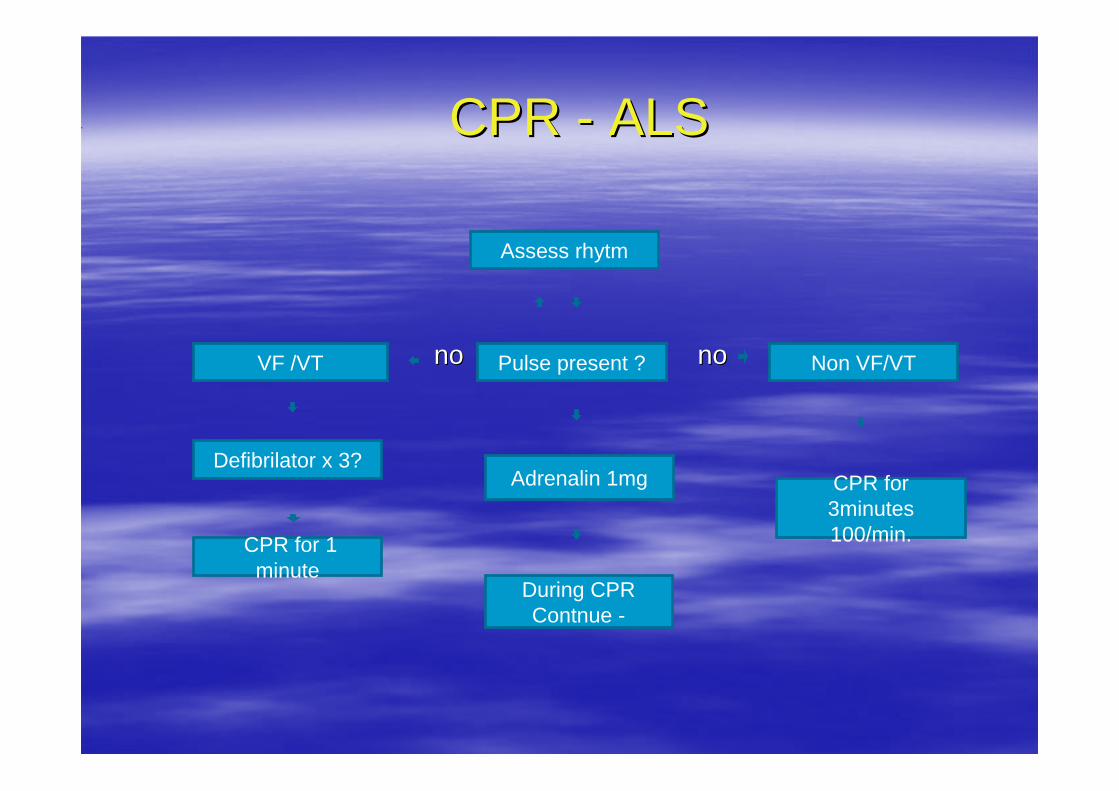
During CPRContnue -
VF /VT
CPR CPR -- ALSALS
Pulse present ?
Assess rhytm
Adrenalin 1mg CPR for 3minutes 100/min. CPR for 1
minute
Non VF/VT
Defibrilator x 3?

Potentially reversible cases (4Hs/4TS)
•Hypoxia, Hypovolemia, Hypotermia, Hypo/Herkalemia+metabolick disorders
•Tension pneumiothorax, Tamponade, Toxic disturbance, Tromboembolic/mechanical obstruction
CPR CPR --ALSALSDuring CPR
Correct any reversible causes• Check electrodes• Verify i.v. acces• Give adrenOxygenation by advance airway (LMA/ ETT)• Adrenalin every 3 minutes• Consider: atropin, pacing, bikarbonate if pH below 7.1, • anti-arrhytmics (after 3 shock)
CPR for 3minutes 100/min.
CPR for 1 minute