Embed Size (px)
Citation preview

Genetics Case: Mary & CharlesAlexandra Costlow, B.S.
Medical AudiologySpring 2011

Case History
Mary (25) and Charles (26) are an African American couple.
Mary and Charles are expecting a
baby in 5 months.
Their physician recommended
genetic counseling as both parents
are deaf.
It does not matter to the parents whether the baby is hearing or deaf.

Audiological Characteristics of Mary & Charles
Mary
Profound sensorineural deafness - Diagnosed at 6 months of age.
Enlarged Vestibular Aqueduct (EVA) - Diagnosed recently by CT Scan.
Does not know if EVA is related to deafness or not.
Charles
Deafened by meningitis at 5 years of age.
He recalls “Hearing very well” prior to onset of deafness at age 5.

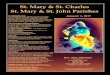
Enlarged Vestibular Aqueduct

Family History of Hearing Loss
Mary
Her parents were suspicious of her deafness prior to diagnosis at 6 months of age.
Older brother, Glen (27) diagnosed with profound deafness at 18 months of age. Glen has an enlarged thyroid (a.k.a.
goiter), for which he does not take any medications.
Glen is married to a hearing woman, and they have 2 boys and 1 girl who are all hearing.
Charles
He is the only deaf person in his family.
Has 3 brothers and 1 sister.
His brother Michael (28) has 1 daughter.

Family History
Both Mary and Charles are African American on both sides of their families.
They deny consanguinity.
Both Mary’s and Charles’ parents are all alive and well.
All of Mary’s and Charles’ grandparents are alive and well, except for Mary’s maternal grandmother who died of a heart attack at age 72.

Pedigree

Important Facts
Mary and her brother Glen are both deaf. Either congenital or progressive (early childhood). Mary has an EVA. Glen has an enlarged thyroid.
Charles’ haring loss is acquired.
Both of their parents are hearing (and healthy).
No family history of hearing loss.
We do not have information about the pregnancy nor birth history of Mary, Glen, and Charles.
We may or may not have all the information about environmental and medical risk factors for hearing loss.

Pendred Syndrome
Identified in 1896 by Vaughan Pendred.
Arose from the description of two siblings with congenital hearing loss and enlarged thyroids.
Fraser (1965) examined 334 cases of Pendred syndrome. Prevalence was estimated to be 7.5 to 10 per 100,000. Females and males are equally affected.
Pendred syndrome may account for 5-10% of cases of congenital deafness.
(Madeo, Pryor, Brewer, Zalewski, King, Butman, Yang, Park, & Griffith, 2006)

Clinical Features of Pendred Syndrome
Similar to many other syndromes that include pre- or peri-lingual hearing loss.
Its distinguishing features are pleiotropic:
Pre- or perilingual sensorineural hearing loss.
Inner ear malformations, especially enlarged vestibular aqueduct (EVA).
Enlarged thyroid gland (goiter), which indicates involvement of the endocrine system.
These characteristics are not found in all people with Pendred Syndrome, and expression of these features is not pathognomonic (does not explicitly indicate Pendred Syndrome).
(Madeo et al., 2006)

Its Impostors
Usher syndrome (autosomal recessive) Jervell and Lange-Nielsen syndrome (autosomal
recessive) Waardenburg syndrome (autosomal dominant) Branchi-otorenal syndrome (BOR) (autosomal dominant) Alport syndrome (X-linked) In utero exposure (environmental)
(Madeo et al., 2006)

Phenotype - Audiological
Textbook Type: Profound, bilateral congenital sensorineural hearing loss. Typical, but not always. Consider ascertainment baises. Not always symmetric.
Configuration: Often downsloping or flat. Possible high-frequency, inverted “U.” Low-frequency conductive hearing loss but with normal
tympanometry*.
(Madeo et al., 2006)

Phenotype - Audiological
Onset: Pre- or perilingual
Progression is not uncommon*.
Fluctuation is not uncommon*.
No permanent recovery of hearing.
Vestibular dysfunction is variable and not fully penetrant.
(Madeo et al., 2006)

Phenotype - Thyroid
Enlarged thyroid (Goiter) Incompletely penetrant. May not be present until the second decade of life. Typically not accompanied by abnormal thyroid stimulating
hormone (TSH) levels.
These factors contraindicate thyroid function testing as a method of screening for goiter. Perchlorate discharge test* identifies patients with the thyroid
defect that occurs with biallelic SLC26A4 mutations.

Phenotype – Inner Ear Malformations
“EVA is always detected when the ears of individuals with PS are evaluated by both computerized tomography (CT) and magnetic resonance imaging (MRI)” (Phelps, Coffey, Trembath, et al., 1998). Can be bilateral or unilateral.
Other malformations seen in PS patients: Complete or incomplete Mondini malformation Abnormal modiolus Incomplete partition of apical turn of cochlea Vestibular malformation

Enlarged Vestibular Aqueduct
From the NIDCD Website: http://www.nidcd.nih.gov/health/hearing/eva-intro.html

Phenocopies
Nonsyndromic hearing loss with EVA. Clusters in families with an autosomal recessive type pattern. Fluctuation and/or progression in hearing sensitivity may
occur. EVA is indistinguishable from PS.
Patients with goiter and early-onset sensorineural hearing loss may be confused with PS patients.

Molecular Characteristics
Nomenclature: SLC26A4 Solute Carrier Family 26 Member 4
Inheritance: Autosomal recessive
Biallelic mutation in SLC26A4 on 7q31. Biallelic = ? 7q31 = ? SCL26A4 codes for the protein _________.

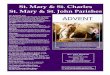
SLC26A4
From the Genetics Home Reference website of the National Institutes of Health: http://ghr.nlm.nih.gov/gene/SLC26A4

Molecular Characteristics
Pendrin [experimentally] transports several ions across plasma membranes, but the exact function of the protein in vivo may be different. Ions: Iodide, chloride, formate, bicarbonate, nitrate.
Pendrin is found in the nonsensory inner ear epithelia, kidney, and thyroid. It’s function/mechanism in the inner ear is unknown.
(Madeo et al., 2006)

Clinical Identification of Pendred Syndrome
Molecular investigation of families and individuals with hearing loss and EVA revealed: Two mutations in 1/3 of participants. One mutation in 1/3 of participants. No mutations in 1/3 participants.
Madeo et al. (2006) suggests that the combination of genetic testing, audiological testing, and perchlorate testing identifies the vast majority of PS patients.

Genetic Testing
SLC26A4 has been mapped and cloned.
SLC26A4 Testing Bidirectional sequencing of all coding exons yields
identification of ~90% of mutations. Because ~2/3 of patients with one mutation had
nonsyndromic hearing loss and EVA, this suggests that one mutation may not be enough to cause PS.
~40% patients with EVA and hearing loss have no mutation, suggesting that aSLC26A4 mutation is not necessary for hearing loss + EVA.
(Madeo et al., 2006)

Genetic Testing
While the frequency of SLC26A4 mutations is similar across populations, the actual mutations are different (Park, Shaukat, Liu, et al., 2003).
New mutations are emerging.
Genetic testing is more effective in some populations (e.g. Korean) that show a dominant mutation/mutations.

So What About Mary & Charles?
PS is autosomal recessive, which requires that the gene be inherited from both the mother and the father. Gloria and John were obligate carriers for Mary and Glen. One of each of Gloria’s and John’s parents were carriers.
Carriers are heterozygous.
Males and females are affected equally.
Horizontal pattern of inheritance within a family.

So What About Mary & Charles?
Mary and Glen should be tested based on their clinical presentations.
Should their spouses be tested?
Mary’s (and Charles’) and Glen’s (and his wife’s) children should be tested as they will at least be carriers (assuming that Mary and Glen’s spouses are not carriers). Indications for the children of their children.
John and Gloria are likely past having children, so they would likely not benefit from genetic testing.

So What About Mary & Charles?
Charles’ hearing loss was acquired due to meningitis and he reportedly had normal hearing prior to that. So, we can pretty safely assume that his hearing loss was not
syndromic. However, people with inner ear malformations are at higher
risk for meningitis. EVA is a type of inner ear malformation. Is there really any reason to suspect that he has PS? Not really,
so long as other risk factors do not surface. He would likely not be a strong candidate for genetic testing.

Referrals
Audiological
Mary, Glen, and Charles should monitor their hearing loss.
Children of Mary and Glen should be evaluated by an audiologist, especially if genetic testing reveals abnormality.
Family members in need of educational counseling should be referred to an audiologist.
Medical
Children of Mary and Glen should be screened to hearing loss at the medical home.
Glen should monitor his goiter.
All family members experiencing pyschological difficulty relating to potential PS diagnoses should be referred.

Referrals
Audiology Amplification Educational resources
Sign Language
Deaf Culture
Medical For MRI/CT Scan Perchlorate testing Counsel about increased risk of hearing loss due to brain injury Counsel about increased risk of meningitis due to inner ear
malformation Counsel about goiter

Referrals
Geneticist Genetic testing
Genetic Counselor Implications for their families and future children Educational materials, support groups, etc …
Psychology/Psychiatry Psychological implications of hearing loss, syndromic hearing
loss, communication, bonding, anxiety, etc …

Discussion

References
Fraser, G.R. (1965). Association of congenital deafness with goiter (Pendred’s syndrome). Annals of Human Genetics, 28, 201-249.
Madeo, A. C., Pryor, S.P., Brewer, C., Zalewski, C., King, K., Butman, J.A., Yang, Y., Park, H., & Griffith, A.J. (2006). Pendred syndrome. Seminars in Hearing, 27, 160-170.
Park, H.K., Shaukat, S., Liu, X.Z., et al. (2003). Origins and frequencies of SLC26A4 (PDS) mutations in east and south Asian: Global implications for the epidemiology of deafness. Journal of Medical Genetics, 40, 242-248.

References
Phelps, P.D., Coffey, R.A., Trembath, R.C. et al. (1998). Radiological malformations of the ear in Pendred syndrome. Clinical Radiology, 53, 268-273.