Embed Size (px)
Citation preview

Journal of Medical Virology 41:ll-17 (1993)
Genomic Typing of BK Virus in Clinical Specimens by Direct Sequencing of Polymerase Chain Reaction Products
Li Jin, Patricia E. Gibson, James C. Booth, and Jonathan P. Clewley Virus Reference Division, Central Public Health Laboratory (L.J., P.E.G., J.P.C.) and Department of Medical Microbiology, St George's Hospital Medical School (J.C.B.), London, England
Two hundred and twelve urine specimens, from several clinical groups, were examined for BK virus (BKV) using the polymerase chain reaction (PCR) to detect the VP1 region of BKV DNA. Posi- tive results were obtained on 14 specimens from 44 post-transplant patients (31.8'/0), 10 speci- mens from 39 pregnant women (25.6%), and 5 specimens from 100 children (5%) but not on any specimens from 29 laboratory staff. Twenty- eight of the amplified BKV genomes, 19 from urine specimens, eight from culture fluid of inocu- lated tissue, and also one from a throat washing were directly sequenced from single-stranded templates immobilized via a biotinylated primer; it was possible to assign al l to one of the four subtypes of BKV which had previously been iden- tified on the basis of variation in nucleotide se- quence of the VP1 region. Serological subgroup classification correlated with the genomic sub- typing results in 21 of the isolates. The distribu- tion of the BKV subtypes and the clinical status of the infected individuals are discussed. 0 1993 Wiley-Liss, Inc.
KEY WORDS: polyomavirus BK, PCR, BKV subtypes
INTRODUCTION The human polyomavirus BK virus (BKV) infects a
high proportion of the population [Shah et al., 1973; McCance and Gardner, 19871. Although its clinical sig- nificance is unclear, there are reports that BKV is asso- ciated with ureteral stenosis in renal allograft recipi- ents [Coleman et al., 1978; Gardner et al., 19841 and haemorrhagic cystitis in recipients of bone marrow transplants [Apperley et al., 1987; Arthur et al., 19851. BKV genomes have been recovered from tumours of brain and pancreatic islet cells [Corallini et al., 1987; Dorries et al., 19871. 0 1993 WILEY-LISS, INC.
BKV was originally isolated from the urine of an immunosuppressed patient [Gardner et al., 19711. Since then, numerous BKV variants have been iso- lated, and these isolates display a variation in the structure of the non-coding control region [Pater et al., 1983; Pagnani et al., 1986; Watanabe and Yoshiike, 1986; Tavis et al., 1989; Rubinstein et al., 19911. It is not yet clear whether these sequence differences are relevant to infection or reactivation in the natural host, and it is not easy to classify BKV variants based on this region.
The VP1 region of the viral genome codes for the major capsid protein of the polyomavirus virion. This protein has a structural role and also bears important antigenic epitopes. It has been reported that a single amino acid change in VP1 accounts for the different phenotypes of the mouse polyomavirus and simian vi- rus 40 [Freund et al., 1991a,b; Dubensky et al., 1991; Barkan et al., 19871. We have characterized four iso- lates of BKV: BK prototype, SB, AS, and IV. These are the sentinel strains of four serological groups of BKV, and each has been characterised by nucleotide sequenc- ing of the VP1 region [Jin et al., 19933. The sequence differences correlate with the results of serological sub- grouping by haemagglutination-inhibition [Knowles et al., 19891. The virus isolates differentiated by serol- ogy are referred to as groups or subgroups [Knowles et al., 19891 whereas those defined by sequence analysis are called types or subtypes in this study.
In this study we examined specimens from several clinical groups by polymerase chain reaction (PCR) us- ing VP1-primers. All four BKV subtypes were detected. The PCR products were directly sequenced for twenty- eight of these specimens. The sequences obtained were
Accepted for publication December 8, 1992. Address reprint requests to Li Jin, Virus Reference Division,
Central Public Health Laboratory, London NW9 5HT, United Kingdom.

12 Jin et al.
compared with those already published for the four sub- types over the range of amino acids 61 to 83 of VP1, which has been suggested to be the epitope responsible for the serotypic differences between BK variants LJin et al., 19931. The results confirm that this region is conserved within each subtype and is responsible for its unique antigenicity.
MATERIALS AND METHODS Clinical Specimens
A total of 212 urine specimens and 1 throat washing were examined. These were obtained from 29 labora- tory staff, 100 children from different patients visiting a District General Hospital, 39 pregnant women (in which inclusion-bearing cells were found in urine), 1 aplastic anaemia patient, and 44 transplant recipients. One ml of each specimen was centrifuged at 10,OOOg for 2 min. Sediments were resuspended in 1 ml PBS and spun again. The pellets were resuspended in 100 p1 distilled water and heated at 95°C for 5 min. The super- natants were collected and stored at -70°C after a 10- sec microcentrifugation. Eight tissue culture superna- tants were tested without any treatment.
Oligonucleotide Primers One set of primers from nucleotides (nt) 1630 to 1956
were used for amplification and sequencing of the 61-83 amino acid (aa) region of VPl. The primers were chosen from two regions of the genome where the four BKV types have an identical nucleotide sequence. They were 5'-CAAGTGCCAAAACTACTAAT (327-1) and 5'- TGCATGAAGGTTAAGCATGC (327-2). The down- stream primer (327-2) was also synthesized with an amino group at the 5' end (bio-327-2). This was done in order to introduce a biotin derivative, using a Biotin-X- NHS ester labelling kit (Cruachem Ltd, Glasgow, UK). The PCR product was 327 base pairs (bp) long. Another pair of primers which produced a 340 bp fragment of both BKV (nt 1,8762,215) and J C virus (nt 1,757- 2,096) was used for comparison. These were 5'-TGTG- GAAATCTACTGATGTG (340-1) and 5'-TTTCATTTC- TACTGGGATCA (340-2). A 20-bp primer VP1-5, 5'- AGGAGTAGAAGTTCTAGAAG (nt 1,656-1,675), was used for sequencing. The numbering system is that used by Seif et al. [1979] and Frisque et al. [1984]. All the primers were synthesized using a 392 DNA synthe- sizer (Applied Biosystems, Foster City, USA).
PCR Amplification Fifty pmol of each primer, 327-1 and 327-2, were used
in a 50 pl reaction containing 1.25 U of Taq poly- merase, 200 pM of each dNTP 50 mM KCl, 1.5 mM Tris-HC1 MgC1, 10 mM Tris-HC1 (pH 8.3), and 0.001% (wt/vol) gelatin (Boehringer Mannheim, Lewes, UK). Ten pl of resuspended urinary sediment or 5 p1 of cul- ture fluid was added to the mix. After a n initial dena- turation a t 94°C for 2 min, thirty-five cycles of 1 min at 55"C, 1 min a t 72"C, and 1 min a t 91°C followed by one cycle of 1 m-in at 55°C and 4 min a t 72°C were performed
using a PREM thermocycler (Quatro Biosystems, Manchester, UK). Seven p1 of each PCR product was electrophoresed on a 3% agarose gel (NuSieve 3:1, Flowgen, Sittingbourne, UK). Five pl of each positive amplification product was added to a second PCR reac- tion to give a product for sequencing, with five pmol of 327-1 as the sense primer and five pmol of bio-327-2 as the antisense primer. The samples were subjected to the same amplification profile as in the first-round PCR. All the experiments were conducted in parallel with positive and negative controls to exclude false- positive and false-negative results.
Immobilization of Genomic DNA Dynal beads M-280 streptavidin (Dynal, Oslo, Nor-
way) were used as a solid phase for the capture and purification of PCR product DNA prepared using a bio- tinylated primer. Immobilization was carried out ac- cording to the manufacturer's instructions (Dynal, Oslo, Norway). Forty pl of PCR product was added to 200 kg of Dynabeads previously washed with binding/ washing buffer (5 mM Tris-HC1 pH 7.5,0.5 mM EDTA, 1.0 M NaCl final concentration), and incubated for 15 min at room temperature. The beads were washed and then incubated in 8 p10.1 M NaOH for 10 min a t room temperature. The NaOH supernatant containing the eluted single-stranded DNA was removed and neutral- ized with 4 pl 0.2 M HC1 and 1 pl 1 M Tris-HC1. The beads containing the immobilized single-stranded DNA were washed sequentially with 50 pl 0.1 M NaOH, 40 p1 binding/washing buffer, and 50 p1 TE buffer (10 mM Tris pH 7 .5 , l mM EDTA). Six p1 of H,O was added to the beads.
Manual Sequencing With Immobilized Template DNA
All sequencing reactions were carried out using the Sequenase Version 2.0 sequencing kit [US Biochemical Co., Cleveland, USA ; Sanger et al., 19771. Two p1 of the reverse-sequencing primer were added to each tem- plate DNA together with 2 pl of 5 x annealing buffer (10 pl in total). A primer:template molar stoichiometry of 20:l is necessary. The annealing mixtures were incu- bated a t 65°C for 10 min and allowed to cool to room temperature for a t least 10 min. For the labelling reac- tion, 1 p1 of extension buffer, 2 pl of Sequenase (1.6 U/pl), 2 pl of labelling mixture (dCTP, dGTP, and dTTP), 1 pl DDT (0.1 MI and 0.5 pl alpha 32P dATP (10 pCi/pl) were added to each annealing mixture and kept at room temperature for 30-60 sec. Then 3.5 p1 of label- ling mixture was added into each prewarmed (at 37°C) 2.5 pl of termination mixture. The termination reac- tions were kept at 37°C for 3 min before adding 4 pl of the stop solution (95% formamide, 20 mM EDTA 0.05% Bromophenol Blue, 0.05% Xylene Cyanol FF).
After heating the reactions at 72°C for 2 min, 2-5 pl of each reaction was loaded onto a 8% sequencing gel. The gels were run for about 3 h r at a constant 1,700 volts.

Typing of BKV 13
TABLE I. Detection by PCR of BKV DNA in Urine SDecimens*
SDecimen Subject No. tested
Healthy adults 29 Children 100 Pregnant 39 Transplant 44
recipients CT 32 BMT 12
Adastic anaemia 1
No. positive % positive
0 0 5 5.0 10 25.6 14 31.8 8 25.0 6 50.0 1 100
*CT = cardiac transplant; BMT = bone marrow transplant.
Urine Inhibition Test It is known that there are inhibitors of enzyme in
urine [Demmler et al., 19881. After the first round of PCR on urine specimens treated as described, 5 pl of each of the negative urine specimens together with 5 pl of a positive control urine, or 1 pg and 100 ag of BKV DNA in 9 pl of urine specimens were added to 40 p1 of a fresh PCR mix, to detect any inhibition of Taq poly- merase. Ten pl of each PCR product was electro- phoresed on a 3% agarose gel containing ethidium bro- mide.
RESULTS Identification of the VP1 Fragment
PCR Product A total of 213 samples from different clinical groups
were subjected to amplification followed by electro- phoresis of the PCR products on 3% agarose gels. This yielded a single band of 327 bp, which contains the coding region for amino acids 61-83. Five out of 100 children (5%), 10 out of 39 pregnant women (25.6%), 14 out of 44 post-transplant patients (31.8%), and 1 aplas- tic anaemia patient were positive for BKV DNA. None of 29 specimens from normal subjects were PCR posi- tive (Table I).
Sensitivity and Specificity of the PCR Reaction for Detection of BKV DNA
The sensitivity and specificity of the primers 327-11 327-2 in PCR were estimated. When tenfold serial dilu-
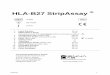
tions of BKV DNA in tissue culture supernatant were amplified, as little as 10 ag of BK viral DNA was detect- able. JCV DNA was not amplified using these primers. By contrast, both BKV and JCV DNA were amplified with primers 340-1 and 340-2, which are complemen- tary to VP1 sequences conserved in JCV and BKV (Fig. 1).
Inhibitors of Taq Polymerase in Human Urine Because urine is known to contain enzyme inhibitors
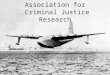
[Demmler et al., 19881, a series of experiments was performed to determine whether urine itself, treated as described, reduced the sensitivity of PCR amplification and caused false-negative results. Fifteen PCR nega- tive urine specimens were each mixed with 5 p1 of PCR- positive urine and amplified. The results showed that the boiled urine specimens did not inhibit PCR (Fig. 2).
Sequences of the VP1 Region in Clinical Specimens
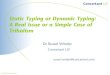
A total of 33 BKV isolates, including five previously reported [Jin et al., 1993; Tavis et al., 19891, were in- vestigated by sequencing the PCR products (nt 1,630 to 1,956, 327 bp). Sequences were compared for identity with part of the variable VP1 region (nt 1,744 to 1,812, 96 bp) for each of the four subtypes of BKV. The 28 isolates fell into the previously defined four genomic subtypes (I, 11, 111, and IV) based on their nucleotide sequence in this region. Four isolates had a single nu- cleotide difference from the sentinel strain (Fig. 3).
The Conserved and Variable Regions of BKV Subtypes
The VP1 region of BKV is 1,089 bp in length and codes for 362 amino acids. The PCR primers used, 327-1 and 327-2, amplify a 327-bp fragment which contains a region responsible for (some) BKV antigenic variation. Twenty-one isolates were both serogrouped by HI and genotyped by PCR sequencing, and there was complete agreement between these two methods (Table 11).
BKV Subtypes and Clinical Status BKV samples from 41 patients with different clinical
conditions were subtyped by sequencing of the appro-
1 7 8 14 15 19 20 26 N M
Fig. 1. Determination of the sensitivity and specificity of the PCR by agarose gel electrophoresis of the products. Serial dilutions from 1 pg to 10 ag of JCV DNA (lanes 1-7) and BKV DNA (lanes 8-14), amplified with primers 340-1 and 340-2. Serial dilutions from 1 pg to 100 ag of JCV DNA (lanes 15-19) and 1 pg to 10 ag of BKV DNA (lanes 2@-26), amplified with primers 327-1 and 327-2. N = negative control; M = 1 kb molecular markers.

14
a b c d a b c d a b c d b c d a M
Jin et al.
Fig. 2. Inhibition of Taq polymerase by human urine. BKV DNA negative urine samples ( 1 3 ) were mixed with BKV DNA and tested it by PCR a, 10 p1 of negative urine; b, 5 p1 negative urine together with 5 p1 of the known positive urine; c, 9 pl negative urine with 1 pg of BKV DNA; d, 9 I J . ~ negative urine with 100 ag of BKV DNA. M = 1 kb molecular marker.
Type Saowlc
I 1 2 3 4 5 6
7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23
I1 24 25 26 27 28
I11 29 30
IV 31 32 33
U C cn AGG GX 7TT AGT CTA AAG CTA AGT GCT GhA AAT GACm AGC AGT GAT AGC CCA GAG A U ..................................................................... ..................................................................... ..................................................................... ......................................................... ..T ......... ......................................................... ..T ......... ............................................................... ..A ... ............................................................... ..A ... ................................................................ ..A ... ............................................................... ..A ... ................................................................ ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ............................................................... ..A ... ................................................................ ..A ... ............................................................... ..c ... ..T ............ .A. ............ .C. ......... .C.... GA. ............ ..C .A. ..T ............ .A. ............ .C. ......... .C.... GA. ............ ..C .A. ..T ............ .A. ............ .C. ......... .C. ... GA. ............ ..C .A. ..T ............ .A. ............ .C. ......... .c.... GA. ............ ..C .A. ..T ............ .A. ............ .C. ......... .C .... GA. ............ ..C .A.
..T ............ .A. ... .AG C.C ............... .C .... GA6 ............ ..C :.. .
..T ............ .A. ... .AG C.C ............... .C .... GA6 ............ ..C ... A.1 G.. ......... .A. ...... .GA ... .C. ...... .C. .C.... GA6 ............ ..C ... A.1 G.. ......... .A. ...... .GA ... .C. ...... .C. .C-... GA6 ............ ..C ... A.1 G.. ......... .A. ...... .GA ... .C. ...... .C. .C.... GA. ............ ..C ...
Fig. 3. Sequences of VP1 nucleotides 1744 to 1812. A total of 33 isolates, including 5 previously reported, were compared. Only differences are indicated. The five previously reported isolates are: 1, BK (Z 19534); 7, GS (Z 19537); 24, SB (Z 19536); 29, AS (M 23122); 31, IV (Z 19535) [Jin et al., 1993; Seif et al., 1979; Tavis et al., 19891. The accession numbers from the EMBL Data Library are bracketed.
priate region of VP1 (Table 111). Although subtype I was the most prevalent strain in all clinical groups except the bone marrow transplant (BMT) patients,
some differences were noted in the distribution of BKV subtypes in the renal transplant (RT), BMT patients, and pregnant women. Subtype I1 was found

Typing of BKV 15
TABLE 11. Comparison of BKV Isolates by DNA Sequencing and HI*
Source of Serological Genomic Strain sequence templates Clinical status group subtype
BK (1) GS (7) DUN (38) SB (24) SB71 (34) SB72 (35) IV (31)
Pregnant 111 IIIb MG (36) AS (29) IR (37) Brain tumour-cloned DNA Tumor (Italy) I I
Culture fluid-PCR RT ( S . Africa) I I Lymphoma I I
J8 (20)
Polyuria (child) I I 57 (19)
Pregnant 111 I11 J6 (18)
BMT I1 I1 54 (30)
BMT I1 I1 SB69 (25)
BMT IV IV 53 (28)
BMT IV IV 52 (33)
Acute lymphatic leukaemia I1 I1 55 (32) J1 (27)
RT I I BMT I1 I1
w 2 (2) Urine-PCR W3 (25) *RT = renal transplant; BMT = bone marrow transplant recipient. "Data from Seif et al. [19791. bData from Tavis et al. 119891.
Culture-cloned DNA RT I I RT I I Wiskott- Aldrich I I" Lymphocytic lymphoma I1 I1 BMT I1 I1 RT I1 I1 RT IV IV RT (S . Africa) IV IV
, , I
,!
! I
TABLE 111. Subtypes and Clinical Status of BKV Isolates*
Clinical Subtype
No. tested I I1 I11 IV
RT 13 10 (77%) 1(8%) 0 2 (15%) BMT 11 3 (27%) 6 (55%) 0 2 (18%) CT 4 4(100%) 0 0 0 Pregnant 5 3 (60%) 0 2(40%) 0 Children 2 2(100%) 0 0 0 Malignant diseases 6 4 (67%) 2 (33%) 0 0 Total 41 26 (63.4%) 9 (21.9%) 2 (4.9%) 4 (9.8%)
*RT = renal transplant recipient; BMT = bone marrow transplant recipient; CT = cardiac transplant recipient.
mostly in BMT patients and subtype I11 mostly in pregnant women.
DISCUSSION PCR is an attractive diagnostic technique because i t
is sensitive and rapid and can be carried out with ex- tremely small amounts of sample. Using primers 327-1 and 327-2, a serial dilution down to 10 ag of cell culture extracted BKV DNA could be amplified and visualized by UV fluorescence. This high sensitivity was not achievable by hybridization (data not shown). The spec- ificity of this pair of primers was tested by using JC virus (JCV) DNA as a template. Even 1 pg of JCV DNA failed to give a detectable amplification product al- though there are only 3/20 nucleotides different be- tween BKV and JCV in the sequence of primer 327-1. This confirms that these primers can be used for diag- nosis and genomic typing of BKV.
With these specific and sensitive primers BKV was detected in several groups of patients. The BKV DNA
which was found in 5% of 100 children (1% by cell cultured, unpublished data) was presumably due to re- cent primary infection in which it has been associated with acute respiratory tract disease [Goudsmit et al., 19821.
It is thought that after infection during childhood BKV persists throughout life. In immunosuppressed patients it is frequently reactivated. In this study, ap- proximately 26% (10139) of pregnant women were posi- tive for BKV DNA by PCR using the VP1 region prim- ers. This rate is higher than the 15% (191129) of pregnant women (using primers from the non-coding control region) reported by Markowitz et al. [1991]. This may be because our specimens all showed evidence of virus-infected cells shed into the urine. In a previous study, based on cell culture, only 12 (9.9%) polyomavi- rus isolates were obtained from 121 cytologically-posi- tive samples [Coleman et al., 19801.
BKV DNA was detected in 25% (8/32) of cardiac transplant (CT) recipients and 50% (6112) of BMT recip-

16 Jin et al.
infections in recipients of bone marrow transplants. Journal of Infectious Diseases 158:563-569.
Barkan A, Welch RC, Mertz J E (1987): Missense mutations in the VP1 gene of Simian virus 40 that compensate for defects caused by deletions in the viral agnogene. Journal of Virology 61:3190-3198.
Coleman DV, Mackenzie EFD, Gardner SD, Podding JM, Amer B, Russell WJI (1978): Human papovavirus (BK) infection and ure- teric stenosis in renal allograft recipients. Journal of Clinical Pa- thology 31:338347.
Coleman DV, Wolfendale MR, Daniel RA, Dhanjal NK, Gardner SD, Gibson PE, Field AM (1980): A prospective study of human poly- omavirus infection in pregnancy. Journal of Infectious Diseases 142:l-8.
Corallini A, Pagnani M, Viadana P, Silini E, Mottes M, Milanesi G, Gerna G, Vettor R, Trapella G, Silvani V, Gaist G, Barbanti- Brodano G (1987): Association of BK virus with human brain tu- mors and tumors of pancreatic islets. International Journal of Can- cer 39:60-67.
Demmler GJ, Buffone GJ, Schimbor CM, May RA (1988): Detection of cytomegalovirus in urine of newborns by using polymerase chain reaction DNA amplification. Journal of Infectious Diseases 158 1 177-1 184.
Dubensky TW, Freund R, Dawe CJ, Benjamin TL (1991): Polyomavi- rus replication in mice: Influences of VP1 type and route of inocu- lation. Journal of Virology 65342-349.
Dunning AM, Talmud P, Humphries SE (1988): Errors in the poly- merase chain reaction. Nucleic Acids Research 16:10393.
Dorries K, Loeber G , Meixensberger J (1987): Association of polyoma- viruses JC, SV40, and BK with human brain tumors. Virology
Freund R, Calderone A, Dawe CJ, Benjamin TL (1991a): Polyomavi- rus tumor induction in mice: Effects of polymorphisms of VP1 and large T antigens. Journal of Virology 65:335-341.
Freund R, Garcea RL, Sahli R, Benjamin TL (1991b): A single-amino- acid substitution in polyomavirus VP1 correlates with plaque size and haemagglutination behaviour. Journal of Virology 65350- 355.
Frisque RJ, Bream GL, Cannella MT (1984): Human polyomavirus JC virus genome. Journal of Virology 51:458-469.
Gardner SD, Field AM, Coleman DV, Hulme B (1971): New human papovavirus (BK) isolated from urine after renal transplantation. Lancet i:1253-1257.
Gardner SD, Mackenzie EFD, Smith C, Porter AA (1984): Prospective study of the human polyomaviruses BK and JC and cytomegalovi- rus in renal transplant recipients. Journal of Clinical Pathology
Goudsmit J, Wertheim-van Dillen P, van Strien A, van der Noordaa J (1982): The role of BK virus in acute respiratory tract disease and the presence of BKV DNA in tonsils. Journal of Medical Virology 10:91-99.
Hayashi K (1990): Mutations induced during the polymerase chain reaction. Technique 2:216-217.
Hogan TF, Borden EC, McBain JA, Padgett BL, Walker DL (1980): Human polyomavirus infections with JC virus and BK virus in renal transplant patients. Annals of Internal Medicine 92:373- 378.
J in J, Gibson PE, Knowles WA, Clewley JP (1993): BK virus antigenic variants: Sequence analysis within the capsid VP1 epitope. Jour- nal of Medical Virology 39:50-56.
Knowles WA, Gibson PE, Gardner SD (1989): Serological typing scheme for BK-like isolates of human polyomavirus. Journal of Medical Virology 28:118-123.
Markowitz R-B, Eaton BA, Kubik MF, Latorra D, McGregor JA, Dynan WS (1991): BK virus and JC virus shed during pregnancy have predominantly archetypal regulatory regions. Journal of Vi- rology 65:4515-4519.
Marshall WF, Telenti A, Proper J , Aksamit AJ, Smith TF (1991): Survey of urine from transplant recipients for polyomavirus JC and BK using the polymerase chain reaction. Molecular and Cellu- lar Probes 5125-128.
McCance DJ, Gardner SD (1987): Papovaviruses: Papilomaviruses and polyomaviruses. In Zuckerman AJ, Banatvala JE, Pattison JR (eds): “Principles and Practice of Clinical Virology.” John Wiley & Sons Ltd., pp 479-506.
Pagnani M, Negrini M, Reschiglian P, Corallini A, Balboni PG, Scher- neck S, Macino G, Milanesi G, Barbanti-Brodano G (1986): MoIec-
i60:268-270.
3 7 : w a - m
ients, which does not differ much from the report of Marshall et a]. [1991]. Their patients showed an overall prevalence of BKV of 31%, with 12 out of 39 post-trans- plant patients having BKV DNA by PCR using primers in T Ag region. In previous studies the detection of BKV was around 1 5 4 9 % in post-transplantation recip- ients, depending on method used [Arthur et al., 1985, 1988; Hogan et al., 19801.
PCR did not detect BKV DNA in any of the 29 healthy adults in this study, nor in any of 12 normal subjects tested in the report of Marshall et a]. (19911. However, 10% (3/30) of healthy adults were reported positive by Arthur et al. [19891. It is still undecided, therefore, whether PCR can be used to discriminate between latent and reactivated infections with human polyomavrruses.
The four reported isolates for which a serological group has already been determined [Knowles et al., 19891 are proposed to be the four main subtypes of BKV. Each has a characteristic sequence over a 69-bp region of VP1 [Jin et al., 19931. Subtype I includes the prototype isolate BK and the GS isolate; subtype I1 to isolate SB; subtype I11 to isolate AS; and subtype IV to isolate IV. Comparison of the nucleotide sequences of these four strains and the GS strain with those of the 28 isolates made directly by PCR, and of 21 other isolates, confirms the stability of amino acids 61-83 in VP1. A few “isolates” derived by PCR amplification showed a single nucleotide change compared to the strains in this subtype-specific region, but there was otherwise no se- quence variation during cell culture and DNA cloning. The variation seen in the PCR products may be due to mutations occurring randomly during amplification by Tuq DNA polymerase [Dunning et al., 1988; Hayashi, 19901.
BKV type I was found most frequently in the human population, followed by subtypes 11, IV, and 111. There were some differences in the distribution of BKV types between BMT, RT, and other groups, but we do not have enough evidence to relate different BKV subtypes with reactivation, particular diseases, or particular groups of immunosuppressed patients.
ACKNOWLEDGMENTS We thank Dr. W. Knowles for supplying the serologi-
cal results, and Professor D.V. Coleman of St. Mary’s Hospital and Dr. M. Moulsdale of Watford General Hos- pital for supplying the specimens.
REFERENCES Apperley JF, Rice SJ, Bishop JA, Chia YC, Krausz T, Gardner SD,
Goldman JM (1987): Late-onset hemorrhagic cystitis associated with urinary excretion of polyomavirus after bone marrow trans- plantation. Transplantation 43:108-112.
Arthur RR, Beckmann AM, Li CC, Saral R, Shah KV (1985): Direct detection of the human papovavirus BK in urine of bone marrow transplant, recipients: Comparison of DNA hybridization with ELISA. Journal of Medical Virology 1629-36.
Arthur RR, Dagostin S, Shah KV (1989): Detection of BK virus and J C virus in urine and brain tissue by the polymerase chain reaction. Journal of Clinical MicrobioIogy 27:1174-1179.
Arthur RR, Shah KV, Charache P, Saral R (1988): BK and J C virus

Typing of BKV
ular and biological properties of BK virus-IR, a BK virus variant isolated from a human tumor. Journal of Virology 59:500-505.
Pater A, Pater MM, Chang L-S, Slawin K, di Mayorca G (1983): Mul- tiple origins of the complementary defective genomes of RF and origin proximal sequences of GS, two human papovavirus isolates. Virology 131:426436.
Rubinstein R, Schoonakker BCA, Harley EH (1991): Recurring theme of changes in the transcriptional control region of BK virus during adaptation to cell culture. Journal of Virology 61: 1600-1604.
Sanger F, Nicklen S, Coulson AR (1977): DNA sequencing with chain- terminating inhibitors. Proceedings of the National Academy of Sciences USA 74:5463-5467.
17
Seif I, Khoury G, Dhar R (1979): The genome of human papovavirus BKV. Cell 18:963-977.
Shah KV, Daniel RW, Warszawski RM (1973): High prevalence of antibodies to BK virus, an SV40-related papovavirus, in residents of Maryland. Journal of Infectious Diseases 128:784-787.
Tavis JE , Walker DL, Gardner SD, Frisque R J (1989): Nucleotide sequence of the human polyomavirus AS virus, an antigenic vari- ant ofBK virus. Journal of Virology 63:901-911.
Watanabe S, Yoshiike K (1986): Evolutionary changes of transcrip- tional control region in a minute-plaque viable deletion mutant of BK virus. Journal of Virology 59:260-266.
![AAP Updates Measles Recommendations - Red Book · PDF fileor identification of measles RNA (by reverse transcriptase-polymerase chain reaction [RT-PCR] assay) from clinical specimens,](https://img.pdfslide.net/doc/110x75/5a91f3e37f8b9a8b5d8bc9b9/aap-updates-measles-recommendations-red-book-identification-of-measles-rna.jpg)