Embed Size (px)
Citation preview

O
GmJ
GmttTptrtssctnercmiteatttmasma
FDF
R2
RTUS6
0©d
www.AJOG.org Reviews
NCOLOGY
estational trophoblastic disease II: classification andanagement of gestational trophoblastic neoplasia
ohn R. Lurain, MD
CWoatalcpcfbhspitm(csurtsmumhac
bsrh
GfiltOstl4rheom1l2rs
ismsctph
estational trophoblastic neopla-sia (GTN) includes invasive
ole, choriocarcinoma, placental siterophoblastic tumor (PSTT), and epi-helioid trophoblastic tumor (ETT).he epidemiology, pathology, clinicalresentation, and diagnosis of theseumors were discussed in part I of thiseview. The overall cure rate in treatinghese tumors is currently �90%. Thisuccess is the result of the inherent sen-itivity of trophoblastic neoplasms tohemotherapy, the effective use of theumor marker human chorionic go-adotropin (hCG) for diagnosing dis-ase and monitoring therapy, the refer-al of patients to or consultation withlinicians who have special expertise inanagement of these diseases, the
dentification of prognostic factorshat predicts treatment response andnhances individualization of therapy,nd the use of combined modalityreatment with chemotherapy, radia-ion, and surgery in the highest risk pa-ients. PSTT and its related ETT re-
ain therapeutic challenges, since theyre more frequently chemotherapy re-istant and do not have the same hCG
arker relationship as invasive molend choriocarcinoma.
rom the John I. Brewer Trophoblasticisease Center, Northwestern Universityeinberg School of Medicine, Chicago, IL.
eceived June 17, 2010; accepted June 30,010.
eprints: John R. Lurain, MD, John I. Brewerrophoblastic Disease Center, Northwesternniversity Feinberg School of Medicine, 250 E.uperior St., Suite 05-2168, Chicago, IL0611. [email protected].
002-9378/free2011 Mosby, Inc. All rights reserved.
oi: 10.1016/j.ajog.2010.06.072
For Editors’ Commentary,
isee Table of Contents
lassification/staginghen the diagnosis of GTN is suspected
r established, a metastatic workup andn evaluation for risk factors is under-aken.1-4 Along with a complete historynd physical examination, the followingaboratory tests should be obtained:omplete blood cell count includinglatelets, coagulation studies, serumhemistries including renal and liverunction panels, blood type and anti-ody screen, and quantitative serumCG level. Recommended radiologictudies include chest x-ray with com-uted tomography (CT) scan of the chest
f the chest x-ray is negative, CT scans ofhe abdomen and pelvis, and CT scan or
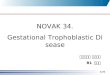
agnetic resonance imaging of the brainFigure). If the physical examination andhest x-ray are normal in the absence ofymptoms, other sites of metastasis arencommon. Measurement of hCG in ce-ebrospinal fluid may be helpful in de-ecting brain involvement. Pelvic ultra-ound or magnetic resonance imaging
ay also be useful in detecting extensiveterine disease for which hysterectomyay be of benefit. Repeat curettage after
ydatidiform mole evacuation is gener-lly not recommended unless there is ex-essive uterine bleeding and evidence of
Gestational trophoblastic neoplasia (GTN) icental site trophoblastic tumor, and epithelin treating these tumors is currently �90%lection of appropriate therapy that maximizNonmetastatic (stage I) and low-risk metastreated with single-agent chemotherapy reHigh-risk GTN (stages II-IV, score �7) reqwithout adjuvant radiation and surgery to a
Key words: chemotherapy, choriocarcinomgestational trophoblastic neoplasia
ntracavitary molar tissue exists on scan, (
JANUARY 2011 Am
ecause it does not often induce remis-ion or influence treatment and it mayesult in uterine perforation andemorrhage.5-8
In 2002, the International Federation ofynecology and Obstetrics (FIGO) de-ned criteria for the diagnosis of postmo-
ar disease and adopted a combined ana-omic staging and modified World Healthrganization (WHO) risk-factor scoring
ystem for GTN.9 The components neededo diagnose postmolar GTN include ateast 1 of the following: (1) hCG plateau forconsecutive values over 3 weeks; (2) hCG
ise of �10% for 3 values over 2 weeks; (3)CG persistence 6 months after molarvacuation; (4) histopathologic diagnosisf choriocarcinoma; or (5) presence ofetastatic disease. The FIGO stage (Table
) is designated by a Roman numeral fol-owed by the modified WHO score (Table) designated by an Arabic numeral, sepa-ated by a colon. PSTTs and ETTs are clas-ified separately.
Treatment is based on classificationnto risk groups defined by the stage andcoring system.10 Patients with non-
etastatic (stage I) and low-risk meta-tatic (stages II and III, score �7) GTNan be treated with single-agent chemo-herapy, with resulting survival rates ap-roaching 100%. Patients classified asaving high-risk metastatic disease
des invasive mole, choriocarcinoma, pla-trophoblastic tumor. The overall cure ratehorough evaluation and staging allow se-hances for cure while minimizing toxicity.
c (stages II and III, score �7) GTN can beting in a survival rate approaching 100%.s initial multiagent chemotherapy with orve a survival rate of 80-90%.
gestational trophoblastic disease,
ncluioid. T
es ctatisuluirechie
a,
stage IV and stages II-III, score �7)
erican Journal of Obstetrics & Gynecology 11

sm�a
Ftwc
TLPlsscehdy(mditl(wt5pfacnmscspmts
2ee1rttectgiemiarhtS
A(swpsL
Reviews Oncology www.AJOG.org
1
hould be treated in a more aggressiveanner with multiagent chemotherapy
adjuvant radiation or surgery tochieve cure rates of 80-90%. Use of the
FIGURERadiologic studies of gestational tr
A
C
, Chest x-ray of classic appearance of pulmonaryGTN). B, Lung computed tomography (CT) showingeen on chest CT scan in 30-40% of patients withoman with uterine hemorrhage and human choriartum. Enlarged uterus contains necrotic tumor; chowing left frontal lobe tumor of 35-year-old womurain. Gestational trophoblastic disease II. Am J Obstet Gyn
TABLE 1Staging for gestational trophoblast
Stage Description
I Disease confined to uterus...................................................................................................................
II Disease extends outside utevagina, broad ligament)
...................................................................................................................
III Disease extends to lungs w...................................................................................................................
IV Disease involves other meta...................................................................................................................
Lurain. Gestational trophoblastic disease II. Am J Obstet Gyne
2 American Journal of Obstetrics & Gynecology J
IGO staging system is essential for de-ermining initial therapy for patientsith GTN to assure the best possible out-
omes with the least morbidity.
hoblastic neoplasia
B
D
tastases from gestational trophoblastic neoplasiacropulmonary metastases in GTN. Metastases are
al chest x-rays. C, Pelvic CT scan of 21-year-oldgonadotropin of 140,000 mIU/mL 8 weeks post-ttage showed choriocarcinoma. D, Brain CT scanith gestational choriocarcinoma.
2011.
neoplasia
..................................................................................................................
but is limited to genital structures (adnexa,
..................................................................................................................
r without genital tract involvement..................................................................................................................
tic sites..................................................................................................................
ccol 2011.
ANUARY 2011
reatmentow-risk diseaseatients with nonmetastatic (stage I) and
ow-risk metastatic (stages II and III,core �7) GTN should be treated withingle-agent methotrexate or actinomy-in D chemotherapy.11,12 Several differ-nt outpatient chemotherapy protocolsave been used, which in mostly nonran-omized, retrospective studies haveielded fairly comparable overall resultsTable 3). The variability in primary re-ission rates reflects differences in drug
osages, schedules, and routes of admin-stration, as well as patient selection cri-eria. In general, the weekly intramuscu-ar (IM) or intermittent intravenousIV) infusion methotrexate and the bi-eekly single-dose actinomycin D pro-
ocols are less effective than one of the-day methotrexate or actinomycin Drotocols and the 8-day methotrexate-
olinic acid regimen. Also, older patientge, higher hCG levels, nonmolar ante-edent pregnancy, histopathologic diag-osis of choriocarcinoma, presence ofetastatic disease, and higher FIGO
core are each associated with an in-reased risk of initial chemotherapy re-istance. Despite these differences inrimary remission rates with initial che-otherapy, almost all patients are even-
ually cured with most being able to pre-erve fertility.
Methotrexate 0.4 mg/kg (maximum5 mg) IM or IV push daily for 5 daysvery other week seems to be the mostffective treatment protocol.13-15 In995, we reviewed nearly 30 years’ expe-ience in treating nonmetastatic GTN athe Brewer Trophoblastic Disease Centero determine effectiveness of therapy,valuate toxicity, and assess factors asso-iated with chemotherapy resistance. Ofhe 253 patients initially treated with sin-le-agent methotrexate 0.4 mg/kg (max-mum 25 mg) IV push daily for 5 daysvery 2 weeks, 226 (89.3%) achieved pri-ary remission, 22 (8.7%) were placed
nto remission with subsequent single-gent actinomycin D, and only 5 (2.0%)equired multiagent chemotherapy orysterectomy for cure, with all 253 pa-ients achieving permanent remission.ignificant toxicity to methotrexate ne-
op
memi
normonicurean wecol
ic
.........
rus
.........
ith o.........
sta.........
essitating a change to another chemo-

tpiiafrmhno9caiit
cod(lTi(pacmibfthtmpnpimolrae
f1aAfmif
uemrd
ermdIccc
((iwpoTrwrwtam
yne
www.AJOG.org Oncology Reviews
herapeutic agent occurred in only 12atients (4.7%); no life-threatening tox-
city occurred. The most common toxic-ty was stomatitis: there was no alopeciand nausea was not a common side ef-ect. Factors found to be associated withesistance to initial methotrexate che-otherapy were: high pretreatment
CG level, nonmolar antecedent preg-ancy, and clinicopathologic diagnosisf choriocarcinoma. Our results of about0% complete response and 100% survivalonfirmed earlier reports from our centernd others that single-agent methotrexaten a 5-day outpatient course every 2 weekss a highly effective and well-toleratedreatment.15
An alternative methotrexate regimenonsists of slightly higher doses of meth-trexate (1.0-1.5 mg/kg) IM every otheray alternating with folinic acid0.1-0.15 mg/kg) IM over 8 days with ateast a 1-week interval between courses.his methotrexate-folinic acid protocol
s reported to have decreased toxicityespecially stomatitis), but is more ex-ensive and inconvenient, and is associ-ted with a more frequent need for ahange in chemotherapy to achieve re-ission.16-22 High-dose methotrexate
nfusion (100 mg/m2 IV push followedy 200 mg/m2 IV 12-hour infusion witholinic acid rescue), with the interval be-ween doses reliant on posttreatmentCG trends, is another modified metho-rexate dosage schedule used for treat-
ent of low-risk GTN. This treatmentrotocol also results in more frequenteed for second-line therapy and is ex-ensive.22-25 Methotrexate administered
n single weekly IM doses of 30-50g/m2, although having the advantages
f convenience, decreased cost, andower toxicity, has the lowest completeesponse rate of any regimen and is notppropriate therapy for metastatic dis-ase or choriocarcinoma.26-28
Actinomycin D (10-12 mg/kg IV dailyor 5 days every other week or as a single.25 mg/m2 IV dose every 2 weeks) is ancceptable alternative to methotrexate.ctinomycin D has a more toxic side ef-
ect profile (nausea, alopecia) thanethotrexate and produces local tissue
njury if IV extravasation occurs. There-
ore, actinomycin D has most often beensed as secondary therapy in the pres-nce of methotrexate resistance or as pri-ary therapy for patients with hepatic or
enal compromise or effusions contrain-icating the use of methotrexate.29-34
Several studies have compared differ-nt methotrexate and actinomycin Degimens for treatment of low-risk,ostly nonmetastatic GTN. Three ran-
omized clinical trials compared weeklyM methotrexate to biweekly actinomy-in D.35-37 In each trial, the primaryomplete response rates were signifi-antly lower for weekly IM methotrexate
TABLE 2Scoring system for gestational trop
Risk factor S
0...................................................................................................................
Age, y �...................................................................................................................
Antecedent pregnancy M...................................................................................................................
Pregnancy event to treatment interval, mo �...................................................................................................................
Pretreatment hCG, mIU/mL �...................................................................................................................
Largest tumor mass, including uterus, cm �...................................................................................................................
Site of metastases �...................................................................................................................
No. of metastases �...................................................................................................................
Previous failed chemotherapy �...................................................................................................................
GI, gastrointestinal; hCG, human chorionic gonadotropin.Total score for patient is obtained by adding individual scores
Lurain. Gestational trophoblastic disease II. Am J Obstet G
TABLE 3Chemotherapy for low-risk gestatio
Chemotherapy regimen
1. MTX 0.4 mg/kg (maximum 25 mg)/d IV or Ievery 14 d
...................................................................................................................
2. MTX 30-50 mg/m2 IM weekly...................................................................................................................
3. MTX 1 mg/kg IM d 1, 3, 5, 7; folinic acid 08; repeat every 15-18 d, or as needed
...................................................................................................................
4. MTX 100 mg/m2 IVP, then 200 mg/m2 in 5folinic acid 15 mg IM or PO q 12 h for 4 doafter start of MTX; repeat every 18 d, or as
...................................................................................................................
5. Act-D 10-13 �g/kg IV qd for 5 d; repeat ev...................................................................................................................
6. Act-D 1.25 mg/m2 IV every 2 wk...................................................................................................................
7. Alternating MTX/Act-D regimens 1 and 5...................................................................................................................
ACT-D, actinomycin D; D5W, dextrose 5% in water; IM, intramtrexate; PO, by mouth; qd, daily.
Lurain. Gestational trophoblastic disease II. Am J Obstet Gyne
JANUARY 2011 Am
49-53%) than for pulsed actinomycin D69-90%). Two retrospective case stud-es compared 5-day IM methotrexateith the 8-day methotrexate-folinic acidrotocol for treatment of low-riskr nonmetastatic postmolar GTN.19,38
here was no difference in remissionates in the study by Wong et al19 (76%)hereas in the study by Smith et al38 the
emission rates were 92% for patientsith methotrexate alone vs 72% for pa-
ients treated with methotrexate-foliniccid. Gleeson et al39 reported primary re-ission rates of 69% and 75% in patients
blastic neoplasia
e
1 2 4..................................................................................................................
�39 � �..................................................................................................................
Abortion Term..................................................................................................................
4-6 7-12 �12..................................................................................................................3 103-104 104-105 �105
..................................................................................................................
3-4 �5 �..................................................................................................................
Spleen, kidney GI tract Brain, liver..................................................................................................................
1-4 5-8 �8..................................................................................................................
� Single drug �2 drugs..................................................................................................................
ach prognostic factor: low risk �7; high risk �7.
col 2011.
l trophoblastic neoplasia
Primary remissionrate, %
or 5 d; repeat 87–93
..................................................................................................................
49–74..................................................................................................................
g/kg IM d 2, 4, 6, 74–90
..................................................................................................................
L D5W over 12 h;beginning 24 hded
69–90
..................................................................................................................
14 d 77–94..................................................................................................................
69–90..................................................................................................................
100..................................................................................................................
ular; IV, intravenous; IVP, intravenous push; MTX, metho-
ho
cor
.........
39.........
ole.........
4.........
10.........
3.........
.........
.........
.........
for e
na
M f
.........
.........
.1 m
.........
00 msesnee
.........
ery.........
.........
.........
usc
col 2011.
erican Journal of Obstetrics & Gynecology 13

wtmLstfptaapnnm5mlmrmasahm(t
msftscbbpsuTiUtllafimmswmcig
s�Fm
uhaatgnpovmsctfwsteesutP
osBotwsc((tsTpmgtppn
msin
dtcapmo
HP(�taOrh1a(atmrf(i8CrtfMiemeimmcp(
hEfrsprsth�
Reviews Oncology www.AJOG.org
1
ith nonmetastatic postmolar GTNreated with weekly IM methotrexate or
ethotrexate-folinic acid, respectively.ertkhachonsuk et al40 randomly as-igned patients with nonmetastatic GTNo treatment with either methotrexate-olinic acid or 5-day actinomycin. Com-lete remission was achieved in 74% ofhe women in the methotrexate-foliniccid arm vs 100% of the women in thectinomycin D arm. Kohorn41 com-ared 5-day actinomycin to pulse acti-omycin for treatment of patients withonmetastatic postmolar GTN. The pri-ary remission rate was 88% for the
-day course vs 78% for the pulsed regi-en. Abrao et al42 retrospectively ana-
yzed patients with low-risk, mostly non-etastatic GTN treated with 5-day
egimens of methotrexate and actino-ycin D or a combination of methotrex-
te and actinomycin D. Complete remis-ion rates were not significantly differentt 69%, 61%, and 79%, respectively;owever, the adverse side effect rate wasuch greater with combination therapy
62%) than with single-agent metho-rexate (29%) or actinomycin D (19%).
Patients categorized as having low-risketastatic GTN (FIGO stages II and III,
core �7) can usually be treated success-ully with initial single-agent chemo-herapy using one of the 5-day dosagechedules of methotrexate or actinomy-in D, as for nonmetastatic disease (Ta-le 3). The weekly methotrexate oriweekly actinomycin D single-doserotocols currently in use for nonmeta-tatic postmolar disease should not besed for treatment of metastatic disease.he combined experience of 3 special-
zed trophoblastic disease centers in thenited States with single-agent metho-
rexate or actinomycin D treatment ofow-risk metastatic GTN yielded excel-ent outcomes. Primary remission waschieved in 48-67% of patients with therst single-agent chemotherapy regi-en. From 1-14% of patients neededultiagent chemotherapy after failed
equential single-agent chemotherapyith or without surgery to achieve re-ission, but eventually all patients were
ured. Risk factors for drug resistance tonitial single-agent chemotherapy in this
roup of patients with low-risk meta- m4 American Journal of Obstetrics & Gynecology J
tatic GTN were pretherapy hCG level100,000 mIU/mL, age �35 years,
IGO score �4, and large vaginaletastases.43-45
Regardless of the treatment protocolsed, chemotherapy is continued untilCG values have returned to normal andt least 1 course has been administeredfter the first normal hCG level. Chemo-herapy is changed to an alternative sin-le-agent if the hCG level plateaus aboveormal during treatment or if toxicityrecludes an adequate dose or frequencyf treatment. If there is a significant ele-ation in hCG level, development ofetastases, or resistance to sequential
ingle-agent chemotherapy, multiagenthemotherapy should be initiated. Hys-erectomy for low-risk GTN may be per-ormed as adjuvant treatment coincidentith the initiation of chemotherapy to
horten the duration of treatment if fer-ility preservation is not desired. Hyster-ctomy may also become necessary toradicate persistent, chemotherapy-re-istant disease in the uterus or to remedyterine hemorrhage from tumor. Hys-
erectomy is the treatment of choice forSTT and ETT.This past year, we updated our results
f treatment of low-risk GTN (FIGOtage I and stages II-III; score �7) at therewer Trophoblastic Disease Centerver the past 28 years. From 1979hrough 2006, we treated 359 patientsith low-risk GTN. The complete re-
ponse rate to the initial single-agenthemotherapeutic drug was 79%: 78%276/352) for methotrexate and 86%6/7) for actinomycin D, with 92% of pa-ients having a complete response toequential single-agent chemotherapy.he remaining 8% of patients were alllaced into remission with the use ofultiagent chemotherapy and/or sur-
ery. Resistance to the initial chemo-herapeutic agent was associated withresence of metastatic disease, clinico-athologic diagnosis of choriocarci-oma, and increasing FIGO score.46
In summary, cure rates for both non-etastatic and low-risk metastatic GTN
hould approach 100% with the use ofnitial single-agent methotrexate or acti-omycin D chemotherapy. Approxi-
ately 20% of low-risk patients will lANUARY 2011
evelop resistance to the initial chemo-herapeutic agent, but �90% will beured by the use of sequential single-gent chemotherapy. Eventually, ap-roximately 10% of patients will requireultiagent chemotherapy with or with-
ut surgery to achieve remission.
igh-risk metastatic diseaseatients with high-risk metastatic GTNFIGO stage IV and stages II-III score
7) should be treated initially with mul-iagent chemotherapy with or withoutdjuvant surgery or radiation therapy.12
ver time, the multiagent chemotherapyegimen of choice for high-risk diseaseas changed. Throughout the 1970s and980s, methotrexate, actinomycin D,nd cyclophosphamide or chlorambucilMAC) was the preferred first-line ther-py, yielding cure rates of 63-71%.47 Inhe early 1980s, the combination regi-
en of cyclophosphamide, hydroxyu-ea, actinomycin D, methotrexate witholinic acid, vincristine, and doxorubicinCHAMOCA) was reported to have anmproved primary remission rate of2%48; however, in a randomized trial ofHAMOCA vs MAC, both the primary
emission rate (65% vs 73%) and the ul-imate cure rate (70% vs 95%) were in-erior for CHAMOCA compared with
AC, and CHAMOCA was more tox-c.49 In the 1980s, etoposide was discov-red to be a very effective agent for treat-ent of GTN, and the addition of
toposide to multiagent chemotherapyn the regimen of etoposide, high-dose
ethotrexate with folinic acid, actino-ycin D, cyclophosphamide, and vin-
ristine (EMA-CO) resulted in im-roved remission and survival ratesTable 4).50
Over the last 15 years, several groupsave confirmed the efficacy of theMA-CO regimen as primary therapy
or high-risk GTN, reporting completeesponse rates of 71-78% and long-termurvival rates of 85-94%.51-58 In our 2 re-orted series, the complete responseates were 71% and 67%, and the overallurvival rates were 91% and 93%, respec-ively.55,56 The only patients who diedad FIGO stage IV disease with scores12. No treatment-related deaths or
ife-threatening toxicity occurred. Neu-

totwatEicctrsdc
t(gtstatgehniompa
csehiAwdewEata(p(fstst
hc
miitMmaamicsorpcsfEloEdccbb
wGbB6fa
pefcwphEta
GiEjdplwncwrttnr
PHtPraspph
yne
www.AJOG.org Oncology Reviews
ropenia necessitating a 1-week delayf treatment, anemia requiring bloodransfusion, and grades 3-4 neutropeniaithout thrombocytopenia were associ-
ted with only 14%, 5.8%, and 1.9% ofreatment cycles, respectively. TheMA-CO protocol, or some variation of
t, is currently the initial treatment ofhoice for high-risk metastatic GTN be-ause of low toxicity allowing adherenceo treatment schedules, high completeesponse rates, and overall high resultanturvival. Chemotherapy for high-riskisease is continued for at least 2-3ourses after the first normal hCG.12
When central nervous system metas-ases are present, whole brain irradiation3000 cGy in 200-cGy fractions), or sur-ical excision with stereotactic irradia-ion in selected patients, is usually givenimultaneously with the initiation of sys-emic chemotherapy. During radiother-py, the methotrexate infusion dose inhe EMA-CO protocol is increased to 1/m2 and 30 mg of folinic acid is givenvery 12 hours for 3 days starting 32ours after the infusion begins. An alter-ative to brain irradiation is the use of
ntrathecal as well as high-dose IV meth-trexate. Reported cure rates with brainetastases are 50-80%, depending on
atient symptoms as well as number, size,nd location of the brain lesions.59-63
Adjuvant surgical procedures, espe-ially hysterectomy and pulmonary re-ection for chemotherapy-resistant dis-ase as well as procedures to controlemorrhage, are important components
n the management of high-risk GTN.pproximately half of high-risk patientsill require some form of surgical proce-ure during the course of treatment toffect cure.64-75 In a series of 50 patientsith high-risk GTN treated withMA-CO as primary or secondary ther-py at the Brewer Center from 1986hrough 2005, 24 (48%) underwent 28djuvant surgical procedures, and 2187.5%) were cured. Fifteen (88%) of 17atients who underwent hysterectomy; 480%) of 5 patients who had resistantoci of choriocarcinoma in the lung re-ected; all 4 patients who had suturing ofhe uterus, uterine artery embolization,mall bowel resection, and salpingec-
omy for bleeding; and the 1 patient who wad uterine wedge resection for resistanthoriocarcinoma survived.70
Despite the use of multimodel pri-ary therapy in high-risk GTN, approx-
mately 30% of patients will have anncomplete response to first-line chemo-herapy or relapse from remission.76-79
ost of these patients will have multipleetastases to sites other than the lung
nd vagina, and many will have had in-dequate chemotherapy. Salvage che-otherapy with drug regimens employ-
ng etoposide and a platinum agent oftenombined with surgical excision of per-istent tumor will result in cure of mostf these high-risk patients. The EMA-EPegimen, substituting etoposide and cis-latin for cyclophosphamide and vin-ristine in the EMA-CO protocol, is con-idered the most appropriate therapyor patients who have responded toMA-CO but have plateauing low hCG
evels or who have developed re-elevationf hCG levels after a complete response toMA-CO.80,81 In patients who have clearlyeveloped resistance to methotrexate-ontaining protocols, drug combinationsontaining etoposide and platinum withleomycin, ifosfamide, or paclitaxel haveeen found to be effective.12,76,82
In 2005, we reported on 26 patientsith persistent or relapsed high-riskTN who received secondary platinum-ased salvage chemotherapy at therewer Center. The overall survival was1.5% (16/26). Of the 16 patients whoailed primary therapy with methotrex-te/actinomycin D-based chemotherapy
TABLE 4Chemotherapy for high-risk gestat
Day Drug Dosing
1 EtoposideActinomycin DMTX
100 mg/m2 IV o0.5 mg IVP100 mg/m2 IVP
...................................................................................................................
2 EtoposideActinomycin DFolinic acid
100 mg/m2 IV o0.5 mg IVP15 mg IM or POof MTX
...................................................................................................................
8 CyclophosphamideVincristine
600 mg/m2 IV1.0 mg/m2 IVP
...................................................................................................................
IM, intramuscular; IV, intravenous; IVP, intravenous push; MTXRepeat cycle on days 15, 16, and 22 (every 2 wk).
Lurain. Gestational trophoblastic disease II. Am J Obstet G
ithout etoposide, 10 (63%) had com- i
JANUARY 2011 Am
lete clinical responses to bleomycin,toposide, and cisplatin; etoposide, ifos-amide, and cisplatin; and ifosfamide,arboplatin, and etoposide, and 10 (63%)ere cured. Of the 10 patients who failedrimary therapy with EMA-CO, 9 (90%)ad complete clinical responses toMA-EP or bleomycin, etoposide, cispla-in, but only 6 (60%) subsequentlychieved a lasting remission.76
In summary, cure rates for high-riskTN of 80-90% are now achievable with
ntensive multimodality therapy withMA-CO chemotherapy, along with ad-
uvant radiotherapy or surgery when in-icated. Approximately 30% of high-riskatients will fail first-line therapy or re-
apse from remission. Salvage therapyith platinum-containing drug combi-ations, often in conjunction with surgi-al resection of sites of persistent tumor,ill result in cure of most of these high-
isk patients with resistant disease. Evenhose patients with metastatic disease tohe brain, liver, and gastrointestinal tractow have a 75%, 73%, and 50% survivalate, respectively.46
STTs and ETTsysterectomy with lymph node dissec-
ion is the recommended treatment forSTT and ETT, because of the relativeesistance of these tumors to chemother-py and their propensity for lymphaticpread. Chemotherapy should be used inatients with metastatic disease and inatients with nonmetastatic disease whoave adverse prognostic factors, such as
al trophoblastic neoplasia
30 min
en 200 mg/m2 in 500 mL D5W over 12 h..................................................................................................................
30 min
ery 12 h for 4 doses starting 24 h after start
..................................................................................................................
..................................................................................................................
thotrexate.
col 2011.
ion
ver
, th.........
ver
ev
.........
.........
, me
nterval from last known pregnancy to
erican Journal of Obstetrics & Gynecology 15

dvctmdisttadd
RWtwtmctttsf(pitpsctp1sefcretfat
FAcqtmibe
ortttordpfituferd
cnrttsmfhiarfstevswcdtttht
kttmrsmaaia
otiicc
R1b32nO3O4aG5atn6Tmb7Rtr98Bcr29Gi21mtsO1tt1RtS1mtG1Tgn1on
Reviews Oncology www.AJOG.org
1
iagnosis �2 years, deep myometrial in-asion, tumor necrosis, and mitoticount �6/10 high power fields. Al-hough the optimal chemotherapy regi-
en for PSTT and ETT remains to beefined, the current clinical impression
s that a platinum-containing regimen,uch as EMA-EP or a paclitaxel/cispla-in–paclitaxel/etoposide doublet, is thereatment of choice. The survival rate ispproximately 100% for nonmetastaticisease and 50-60% for metastaticisease.83-85
easons for treatment failuree recently reviewed our experience in
reating patients with GTN whose careas transferred to the Brewer Center af-
er failing treatment elsewhere to deter-ine causes of treatment failure and to
ompare our results of treating these pa-ients from 1979 through 2006 withhose previously reported from 1962hrough 1978. The most common rea-ons for unsuccessful GTN treatment be-ore transfer to the Brewer Center were:1) use of single-agent chemotherapy foratients with high-risk disease; and (2)
nappropriate use of weekly IM metho-rexate chemotherapy for treatment ofatients with metastatic disease, FIGOcores �7, and/or nonpostmolar chorio-arcinoma. Successful secondary GTNreatment in this patient group im-roved from 59% during 1962 through978 to 93% during 1979 through 2006,eemingly as a result of more experi-nced clinicians administering more ef-ective chemotherapy treatment proto-ols.86 Request for advice from oreferral for treatment to clinicians withxpertise in management of gestationalrophoblastic disease is recommendedor a patient who fails single-agent ther-py for low-risk disease and for any pa-ient with high-risk disease.87
ollow-up after treatment for GTNfter hCG regression to normal andompletion of chemotherapy, serumuantitative hCG levels should be ob-ained at 1-month intervals for 12
onths. The risk of relapse is about 3%n the first year after completing therapy,ut is exceedingly low after that. Physical
xaminations are performed at intervals o6 American Journal of Obstetrics & Gynecology J
f 6-12 months; other testing such as x-ays or scans are rarely indicated. Con-raception should be maintained duringreatment and for 1 year after comple-ion of chemotherapy, preferably usingral contraceptives. Because of the 1-2%isk of a second gestational trophoblasticisease event in subsequent pregnancies,elvic ultrasound is recommended in therst trimester of a subsequent pregnancy
o confirm a normal gestation, the prod-cts of contraception or placentas from
uture pregnancies should be carefullyxamined histopathologically, and a se-um quantitative hCG level should beetermined 6 weeks after any pregnancy.Successful treatment of GTN with
hemotherapy has resulted in a largeumber of women who maintain theireproductive potential despite exposureo drugs that have ovarian toxicity anderatogenic potential. Most women re-ume normal ovarian function after che-
otherapy and exhibit no increase in in-ertility. Many successful pregnanciesave been reported, without an increase
n abortions, stillbirths, congenitalnomalies, prematurity, or major obstet-ic complications. There is no evidenceor reactivation of disease because ofubsequent pregnancies, although pa-ients who have had 1 trophoblastic dis-ase episode are at greater risk for the de-elopment of a second episode in aubsequent pregnancy, unrelated tohether they had previously received
hemotherapy. Patients are advised toelay conception for 1 year after cessa-ion of chemotherapy to allow for unin-errupted hCG follow-up and to permithe elimination of mature ova that mayave been damaged by exposure to cyto-oxic drugs.88-90
Because many anticancer drugs arenown carcinogens, there is concern thathe chemotherapy used to induce long-erm remissions or cures of one cancer
ay induce second malignancies. Untilecently, there were no reports of increasedusceptibility to the development of other
alignancies after successful chemother-py for GTN, probably because of the rel-tively short exposure of these patients tontermittent schedules of methotrexatend actinomycin D and the infrequent use
f alkylating agents. After the introduction mANUARY 2011
f etoposide-containing drug combina-ions for treatment of GTN in the 1980s, anncreased risk of secondary malignancies,ncluding acute myelogenous leukemia,olon cancer, melanoma, and breast can-er, was identified.91 f
EFERENCES. Lurain JR. Treatment of gestational tropho-lastic tumors. Curr Treat Options Oncol 2002;:113-24.. Ngan S, Seckl MJ. Gestational trophoblasticeoplasia management: an update. Curr Opinncol 2007;19:486-91.. Soper JT. Gestational trophoblastic disease.bstet Gynecol 2006;108:176-87.. Berkowitz RS, Goldstein DP. Current man-gement of gestational trophoblastic disease.ynecol Oncol 2009;112:654-62.. Schlaerth JB, Morrow CP, Rodriguez M. Di-gnostic and therapeutic curettage in gesta-ional trophoblastic disease. Am J Obstet Gy-ecol 1990;162:1465-70.. Pezeshki M, Hancock BW, Silcocks P, et al.he role of repeat uterine evacuation in theanagement of persistent gestational tropho-lastic disease. Gynecol Oncol 2004;95:423-9.. van Trommel NE, Massuger LF, VerheijenH, et al. The curative effect of a second curet-
age in persistent trophoblastic disease: a ret-ospective cohort study. Gynecol Oncol 2005;9:6-13.. Garner EI, Feltmate CM, Goldstein DP,erkowitz RS. The curative effect of a secondurettage in persistent trophoblastic disease: aetrospective cohort study. Gynecol Oncol005;99:3-5.. Ngan HYS, Bender H, Benedet JL, et al.estational trophoblastic neoplasia, FIGO stag-
ng and classification. Int J Gynecol Obstet003;83:175-7.0. Lurain JR, Casanova LA, Miller DS, Rade-aker AW. Prognostic factors in gestational
rophoblastic tumors: a proposed new scoringystem based on multivariate analysis. Am Jbstet Gynecol 1991;164:611-6.1. Lurain JR. Pharmacotherapy of gestationalrophoblastic disease. Expert Opin Pharmaco-her 2003;4:1-13.2. Alazzam M, Tidy J, Hancock BW, Osborne. First line chemotherapy in low risk gestational
rophoblastic neoplasia. Cochrane Databaseyst Rev 2009;1:CD007102.3. Hammond CB, Hertz R, Ross GT, et al. Pri-ary chemotherapy for nonmetastatic gesta-
ional trophoblastic neoplasms. Am J Obstetynecol 1967;98:71-8.4. Hammond CB, Borchert LG, Tyrey L, et al.reatment of metastatic trophoblastic disease:ood and poor prognosis. Am J Obstet Gy-ecol 1973;115:451-7.5. Lurain JR, Elfstrand EP. Single-agent meth-trexate chemotherapy for the treatment ofonmetastatic gestational trophoblastic tu-
ors. Am J Obstet Gynecol 1995;172:574-9.
1TaO1MmmR1Tft11wp12Ldl22ple2etp32MtG2dd2Mt22ene2ampg2Amt12Gg13ica3a
tc23ipO3Spc3SmC3Cats3mtn3deato3mtsG3Ne8O4Sfgi24atC4Tdtm4Mb4emG4rw
4am24gtc84mc4ptvpO5etcbG5Ep35EdJ5ftE25bap25Tnnc5ttt5sacp5mtI5esO6G
www.AJOG.org Oncology Reviews
6. Bagshawe KD, Dent J, Newlands ES, et al.he role of low-dose methotrexate and foliniccid in gestational trophoblastic tumors. Br Jbstet Gynecol 1989;96:795-802.7. Garrett AP, Garner EO, Goldstein DP, et al.ethotrexate infusion and folinic acid as pri-ary therapy for nonmetastatic and low-risketastatic gestational trophoblastic tumors. Jeprod Med 2002;47:355-62.8. Berkowitz RS, Goldstein DS, Bernstein MR.en years’ experience with methotrexate and
olinic acid as primary therapy for gestationalrophoblastic disease. Gynecol Oncol 1986;23:11-8.9. Wong LC, Choo YC, Ma HK. Methotrexateith citrovorum factor rescue in gestational tro-hoblastic disease. Am J Obstet Gynecol985;152:59-62.0. McNeish IA, Strickland S, Holden L, et al.ow-risk persistent gestational trophoblasticisease: outcome following initial treatment with
ow-dose methotrexate and folinic acid, 1992-000. J Clin Oncol 2002;20:1838-44.1. Khan F, Everand J, Ahmed S, et al. Low-riskersistent trophoblastic disease treated with
ow-dose methotrexate: efficacy and long termffects. Br J Cancer 2003;89:2197-201.2. Growden WB, Wolfberg AJ, Goldstein DP,t al. Evaluating methotrexate treatment in pa-ients with low-risk postmolar gestational tro-hoblastic neoplasia. Gynecol Oncol 2009;112:53-7.3. Berkowitz RS, Goldstein DP, Bernstein MR.ethotrexate infusion with folinic acid in primary
herapy of nonmetastatic trophoblastic tumors.ynecol Oncol 1990;36:56-9.4. Elit L, Covens A, Osborne R, et al. High-ose methotrexate for gestational trophoblasticisease. Gynecol Oncol 1994;54:282-7.5. Wong LC, Ngan HYS, Cheng DKL, et al.ethotrexate infusion in low-risk gestational
rophoblastic disease. Am J Obstet Gynecol000;183:1579-82.6. Homesley HD, Blessing JA, Rettenmaier M,t al. Weekly intramuscular methotrexate foronmetastatic gestational trophoblastic dis-ase. Obstet Gynecol 1988;72:413-8.7. Homesley HD, Blessing JA, Schlaerth J, etl. Rapid escalation of weekly intramuscularethotrexate for nonmetastatic gestational tro-hoblastic disease: a gynecologic oncologyroup study. Gynecol Oncol 1990;39:305-8.8. Hoffman MS, Fiorica JV, Gleeson NC, et al.single institution experience with weekly intra-uscular methotrexate for nonmetastatic ges-
ational trophoblastic disease. Gynecol Oncol996;60:292-4.9. Osathanondh R, Goldstein DP, PastorfideB. Actinomycin D as the primary agent forestational trophoblastic disease. Cancer975;36:863-6.0. Petrilli ES, Morrow CP. Actinomycin D tox-
city in the treatment of trophoblastic disease: aomparison of the 5-day course to single-dosedministration. Gynecol Oncol 1980;9:18-22.1. Kohorn EI. Is lack of response to single-
gent chemotherapy in gestational trophoblas- Gic disease associated with dose scheduling orhemotherapy resistance? Gynecol Oncol002;85:36-9.2. Twiggs LB. Pulse actinomycin D scheduling
n nonmetastatic gestational trophoblastic neo-lasia: cost-effective chemotherapy. Gynecolncol 1982;16:190-5.3. Schlaerth JB, Morrow CP, Nalick RH, et al.ingle-dose actinomycin D in the treatment ofostmolar trophoblastic disease. Gynecol On-ol 1984;19:53-6.4. Petrilli ES, Twiggs LB, Blessing JA, et al.ingle-dose actinomycin D treatment for non-etastatic gestational trophoblastic disease.ancer 1987;60:2173-6.5. Gilani MM, Yarandi F, Eftekhar Z, et al.omparison of pulse methotrexate and pulsectinomycin D in the treatment of low-risk ges-ational trophoblastic neoplasia. Aust N Z J Ob-tet Gynecol 2005;45:161-4.6. Yarandi F, Eftekhar Z, Shojaei H, et al. Pulseethotrexate versus pulse actinomycin D in the
reatment of low-risk gestational trophoblasticeoplasia. Int J Gynecol Obstet 2008;103:33-7.7. Osborne R, Filiaci M, Schink J, et al. A ran-omized phase III trial comparing weekly par-nteral methotrexate and “pulsed” actinomycins primary management for low-risk gestationalrophoblastic neoplasia: a gynecologic oncol-gy group study. Gynecol Oncol 2008;108:52.8. Smith EB, Weed JC Jr, Tyrey L, et al. Treat-ent of nonmetastatic gestational trophoblas-
ic disease: results of methotrexate alone ver-us methotrexate-folinic acid. Am J Obstetynecol 1982;144:88-92.9. Gleeson NC, Finan MA, Fiorica JV, et al.onmetastatic gestational trophoblastic dis-ase: weekly methotrexate compared with-day methotrexate-folinic acid. Eur J Gynecolncol 1993;14:461-5.0. Lertkhachonsuk AA, Israngura N, Wilailak, et al. Actinomycin D versus methotrexate-
olinic acid as the treatment of stage I, low-riskestational trophoblastic neoplasia: a random-
zed controlled trial. Int J Gynecol Cancer009;19:985-8.1. Kohorn EI. Decision making for chemother-py administration in patients with low-risk ges-ational trophoblastic neoplasia. Int J Gynecolancer 1996;6:279-85.2. Abrao RA, de Andrade JM, Tiezzi DG, et al.reatment for low-risk gestational trophoblasticisease: comparison of single-agent metho-rexate, dactinomycin and combination regi-ens. Gynecol Oncol 2008;108:149-53.3. DuBeshter B, Berkowitz RS, Goldstein DP.anagement of low-risk gestational tropho-lastic tumors. J Reprod Med 1991;36:36-9.4. Soper JT, Clarke-Pearson DL, Berchuck A,t al. Five-day methotrexate for women withetastatic gestational trophoblastic disease.ynecol Oncol 1994;54:76-9.5. Roberts JP, Lurain JR. Treatment of low-isk metastatic gestational trophoblastic tumorsith single-agent chemotherapy. Am J Obstet
ynecol 1996;174:1917-24. tJANUARY 2011 Am
6. Hoekstra AV, Lurain JR, Rademaker AW, etl. Gestational trophoblastic neoplasia: treat-ent outcomes. Obstet Gynecol 2008;112:51-8.7. Lurain JR, Brewer JI. Treatment of high-riskestational trophoblastic disease with metho-rexate, actinomycin D and cyclophosphamidehemotherapy. Obstet Gynecol 1985;65:30-4.8. Begent RHJ, Bagshawe KD. The manage-ent of high-risk choriocarcinoma. Semin On-
ol 1982;9:198-203.9. Curry SL, Blessing JA, DiSaia PJ, et al. Arospective randomized comparison of metho-rexate, actinomycin D and chlorambucil (MAC)ersus modified Bagshawe regimen in “poorrognosis” gestational trophoblastic disease.bstet Gynecol 1989;73:357-62.0. Newlands ES, Bagshawe KD, Begent RJH,t al. Results with EMA/CO (etoposide, metho-rexate, actinomycin D, cyclophosphamide, vin-ristine) regimen in high-risk gestational tropho-lastic tumors (1979-1989). Br J Obstetynecol 1991;98:550-7.1. Bolis G, Bonazzi C, Landoni F, et al.MA/CO regimen in high-risk gestational tro-hoblastic tumor (GTT). Gynecol Oncol 1988;1:439-44.2. Bower M, Newlands ES, Holden L, et al.MA/CO for high-risk gestational trophoblasticisease: results from a cohort of 272 patients.Clin Oncol 1997;15:2636-43.3. Kim SJ, Bae SN, Kim JH, et al. Risk factors
or the prediction of treatment failure in gesta-ional trophoblastic tumors treated withMA/CO regimen. Gynecol Oncol 1998;71:47-53.4. Matsui H, Suzuka K, Iitsuka Y, et al. Com-ination therapy with methotrexate, etoposidend actinomycin D for high-risk gestational tro-hoblastic tumors. Gynecol Oncol 2000;78:8-31.5. Escobar PF, Lurain JR, Singh DK, et al.reatment of high-risk gestational trophoblasticeoplasia with etoposide, methotrexate, acti-omycin D, cyclophosphamide, and vincristinehemotherapy. Gynecol Oncol 2003;91:552-7.6. Lurain JR, Singh DK, Schink JC. Primaryreatment of metastatic high-risk gestationalrophoblastic neoplasia with EMA-CO chemo-herapy. J Reprod Med 2006;51:767-72.7. Turan T, Karacay O, Tulunay G, et al. Re-ults with EMA/CO (etoposide, methotrexate,ctinomycin D, cyclophosphamide, vincristine)hemotherapy in gestational trophoblastic neo-lasia. Int J Gynecol Cancer 2006;16:1432-8.8. Lu WG, Ye F, Shen YM, et al. EMA-CO che-otherapy for high-risk gestational trophoblas-
ic neoplasia: a clinical analysis of 54 patients.nt J Gynecol Cancer 2008;18:357-62.9. Evans AC Jr, Soper JT, Clarke-Pearson DL,t al. Gestational trophoblastic disease meta-tatic to the central nervous system. Gynecolncol 1995;59:226-30.0. Small W Jr, Lurain JR, Shetty RM, et al.estational trophoblastic disease metastatic to
he brain. Radiology 1996;200:277-80.
erican Journal of Obstetrics & Gynecology 17

6Waco6Bt6MwJ6RC6tt16Mb6is26od16ogv7st27UtI7lm
t27TtT27ht27AofG7ap7ga27ge7ccn8rtmr8atwrcp28
tpe18apM8ca68nct48t98obbe28Ipo18pg29Swt29Ccm
Reviews Oncology www.AJOG.org
1
1. Rustin GJ, Newlands ES, Begent RH, et al.eekly alternating etoposide, methotrexate and
ctinomycin D/vincristine and cyclophosphamidehemotherapy for treatment of CNS metastasesf choriocarcinoma. J Clin Oncol 1989;7:900-4.2. Bakri Y, Berkowitz RS, Goldstein DP, et al.rain metastases in gestational trophoblastic
umor. J Reprod Med 1994;39:179-84.3. Newlands ES, Holden L, Seckl MJ, et al.anagement of brain metastases in patientsith high-risk gestational trophoblastic tumors.Reprod Med 2002;47:465-71.4. Mutch DG, Soper JT, Babcock CJ, et al.ecurrent gestational trophoblastic disease.ancer 1990;66:978-82.5. Pisal N, North C, Tidy J, et al. Role of hys-erectomy in the management of gestationalrophoblastic disease. Gynecol Oncol 2002;87:90-2.6. Newlands ES, Bower M, Holden L, et al.anagement of resistant gestational tropho-lastic tumors. J Reprod Med 1998;43:111-8.7. Tomada Y, Arii Y, Kaseki S, et al. Surgical
ndications for resection of pulmonary metasta-es of choriocarcinoma. Cancer 1980;46:723-30.8. Xu L-T, Sun C-F, Wang Y-E, et al. Resectionf pulmonary metastatic choriocarcinoma in 43rug-resistant patients. Ann Thorac Surg985;39:257-9.9. Saito K, Harado K, Nakayama H, et al. Rolef thoracotomy in pulmonary metastases fromestational choriocarcinoma. J Thorac Cardio-asc Surg 1983;85:815-20.0. Lurain JR, Singh DK, Schink JC. The role ofurgery in the management of high-risk gesta-ional trophoblastic neoplasia. J Reprod Med006;51:773-6.1. Vogelzang RL, Nemcek AA, Skrtic Z, et al.terine arteriovenous malformations: primary
reatment with therapeutic embolization. J Vascnterv Radiol 1991;2:517-22.2. Lim AK, Agarwal R, Seckl MJ, et al. Embo-
ization of bleeding residual uterine vascular
alformations in patient with treated gesta- c8 American Journal of Obstetrics & Gynecology J
ional trophoblastic tumors. Radiology 2002;22:640-4.3. Fleming EL, Garrett LA, Growden WB, et al.he changing role of thoracotomy in gestationalrophoblastic neoplasia at the New Englandrophoblastic Disease Center. J Reprod Med008;53:493-8.4. Alazzam M, Hancock BW, Tidy J. Role ofysterectomy in managing persistent gesta-ional trophoblastic disease. J Reprod Med008;53:519-24.5. Doumplis D, Al-Khatib K, Sieunarine K, et al.review of the management by hysterectomy
f 25 cases of gestational trophoblastic tumorsrom March 1993 to January 2006. Br J Obstetynecol 2007;114:1168-71.6. Lurain JR, Nejad B. Secondary chemother-py for high-risk gestational trophoblastic neo-lasia. Gynecol Oncol 2005;97:618-23.7. Yang J, Xiang Y, Wan X, et al. Recurrentestational trophoblastic tumor: managementnd risk factors for recurrence. Gynecol Oncol006;103:587-90.8. Ngan HY, Tam KF, Lam KW, et al. Relapsedestational trophoblastic neoplasia: a 20-yearxperience. J Reprod Med 2006;51:829-34.9. Powles Y, Savage PM, Stebbing J, et al. Aomparison of patients with relapsed andhemo-refractory gestational trophoblasticeoplasia. Br J Cancer 2007;96:732-7.0. Mao Y, Wan X, Lv W, Xie X. Relapsed orefractory gestational trophoblastic neoplasiareated with etoposide and cisplatin/etoposide,ethotrexate, and actinomycin D (EP-EMA)
egimen. Int J Gynecol Obstet 2007;98:44-7.1. Newlands ES, Mulholland PJ, Holden L, etl. Etoposide and cisplatin/etoposide, metho-rexate and actinomycin D (EMA) for patientsith high-risk gestational trophoblastic tumors
efractory to EMA/cyclophosphamide and vin-ristine and patients presenting with metastaticlacental site trophoblastic tumors. J Clin Oncol000;18:854-9.2. Wang J, Short D, Sebire NJ, et al. Salvage
hemotherapy of relapsed or high-risk gesta- tANUARY 2011
ional trophoblastic neoplasia (GTN) withaclitaxel/cisplatin alternating with paclitaxel/toposide (TP/TE). Ann Oncol 2008;19:578-83.3. Papadopoulos AJ, Foskett M, Seckl MJ, etl. Twenty-five years clinical experience withlacental site trophoblastic tumors. J Reproded 2002;47:460-4.4. Hassadia A, Gillespie A, Tidy J, et al. Pla-ental site trophoblastic tumor: clinical featuresnd management. Gynecol Oncol 2005;99:03-7.5. Schmid P, Nagai Y, Agarwal R, et al. Prog-ostic markers and long-term outcome of pla-ental-site trophoblastic tumors: a retrospec-ive observational study. Lancet 2009;374:8-55.6. Kohorn EI. Regional centers for trophoblas-ic disease. Am J Obstet Gynecol 2007;196:5-6.7. Lurain JR, Hoekstra AV, Schink JC. Resultsf treatment of patients with gestational tropho-lastic neoplasia referred to the Brewer Tropho-lastic Disease Center after failure of treatmentlsewhere (1979-2006). J Reprod Med008;53:535-40.8. Woolas RP, Bower M, Newlands ES, et al.
nfluence of chemotherapy for gestational tro-hoblastic disease on subsequent pregnancyutcome. Br J Obstet Gynecol 1998;105:032-5.9. Matsui H, Iitsuka Y, Suzuka K, et al. Earlyregnancy outcomes after chemotherapy forestational trophoblastic tumor. J Reprod Med004;49:531-4.0. Garrett LA, Garner EI, Feltmate CM, et al.ubsequent pregnancy outcomes in patientsith molar pregnancy and persistent gesta-
ional trophoblastic neoplasia. J Reprod Med008;53:481-6.1. Rustin GJS, Newlands ES, Lutz J-M, et al.ombination but not single agent methotrexatehemotherapy for gestational trophoblastic tu-ors (GTT) increases the incidence of second
umors. J Clin Oncol 1996;14:2769-73.