Embed Size (px)
Citation preview
GILBERT HIGH SCHOOL
PRE-PARTICIPATION PACKET FOR ATHLETICS Educational Information found at gilbertathletics.org under Sports Medicine tab
Full Pre-Participation Packets are available at GHS
The GHS Pre-participation Packet for Athletics contains important information regarding health & safety that should be reviewed by athletes and their parents prior to athletic participation at GHS or GMS. Checklist 1. Online @ gilbertathletics.org for your review:
● Parent letter regarding sports medicine services ● Information regarding GHS athletic training staff and team physicians ● Educational information regarding concussion, sickle cell trait, common skin infections, sudden
cardiac death, heat illness, proper tackling technique, blood hygiene, nutrition, dietary supplements, and energy drinks
● Instructions for creating an account, completing required digital pre-participation forms, and uploading the completed SCHSL Physical Exam Form on PlanetHS.com
2. Print SCHSL Physical form. Take form with you to exam to be cleared by healthcare provider. 3. PlanetHS – New athletes and parents should create a PlanetHS account. Returning athletes and parents should log into an existing PlanetHS account. All athletes and parents should complete required digital pre-participation forms.
● Forms to be completed digitally on PlanetHS.com (you can choose to REUSE previous years
forms- see form “Returning (student/parent) Athletic Pre-Participation Forms Registration”) o Pre-participation Physical Exam History Form (Print to take with you when you go to
have physical examination completed by Healthcare professional) o Parent’s Permission & Acknowledgement of Risk for Son/Daughter to Participate in
Athletics o Concussion Acknowledgement and Signature Form o Consent and Medical Information Form
● Forms to be uploaded to Planeths.com(upload a picture or scanned document)
o Pre-participation Physical Examination form (back page of physical that should be completed, dated, and signed by healthcare professional)
o Birth Certificate ● GMS Students please select GHS as “OTHER” school
DearParent:AsGilbertHighSchool’sheadathletictrainer,Iamresponsibleforcoordinationsportsmedicine/athletictrainingservicesforGHSathletes.Oursportsmedicineprogram’sfocusistoprevent,evaluate,treat,andrehabilitateinjuriesincurredbyGHSathletesduringthecourseofpracticeandcompetition.Attachedareafewremindersthathelpusserveyourathletebotheffectivelyandefficiently.PRE-PARTICIPATIONPAPERWORK:Allathletesarerequiredtocompleteandsubmitpre-participationformsonPlaneths.combeforebeingallowedtoparticipationinathletics,includingtry-outsandstrength/conditioningsessions.SCHSLrequiresaphysicaltobeconductedafterApril1st,2021forathleticparticipationin2021-2022schoolyear.ATHLETICINJURIES:Intheeventyourstudent-athletebecomesinjuredduringtheseason,he/sheshouldscheduleanappointmenttobeseenbyaGilbertHighSchoolathletictrainer.Pleaseusethewebaddress,https://gilbertsportsmedicine.setmore.com/,orvisitGilbertAtheltics.organdlookundertheIndiansSportsMedicineTab.Theathletictrainingroomisopenforinjuryevaluationsandtreatmentsthroughouttheschoolday(byappointment)andafterschoolat3:20pm.InmostcasesourATstaffcanhandletheinjurywithoutareferraltoaphysicianoremergencyroom.TheIndiansportsmedicineprogramalsooffersrehabservicesforsportsinjuriessustainedduringparticipationwithatGHS/SCHSL–sanctionedteam.PhysicianReferrals:Whenaphysicianreferralisneeded,wecanassistwiththearrangementoftheappointment.PrismaOrthopedicsservesastheteamphysiciansforourathleticsprograms.Typicallywecanarrangeanappointmentwithin24hours.Ifyouprefertoseeanotherphysician,wemaybeabletoassistwiththatappointmentaswell.Anytimeaphysicianexaminesanathlete,he/sheshouldreturnwithwrittendocumentationfromthedoctorincludingthediagnosis,recommendations,andrestrictionsforathleticparticipation.Pleasereturnthisdocumenttotheathletictraineruponreturningtoschool.ATHLETICACCIDENTINSURACNE:Whileanathlete’sparentisultimatelyresponsibleformedicalbillsincurredbecauseofinjury/illnessduringathleticparticipation,Lexington1doesprovidesecondaryathleticaccidentinsuranceforathleteswhoareinjuredwhileparticipatinginofficialteamfunctions.Thepolicyisintendedtobean“excess”policydesignedtopaysecondarilytotheathlete’sprimaryhealthinsurance.Parentsofaninjuredathlete,whohasbeenreferredtoaphysicianbyastaffathletictrainer,shouldreceiveaclaimform.Theparentshouldcompletetheclaimformandfollowthedirectionstofiletheclaim.Parentsarestronglyencouragedtomakeaphotocopyofthecompletedclaimformfortheirrecords.Intheeventanathleteseesaphysicianforaninjury,butwasnotreferredbyastaffathletictrainer,theathlete’sparentsshouldcontacttheheadathletictrainerASAP.Failuretodosomayresultinaclaimnotbeingfiled.Allclaimsmustbefiledwithin90daysofinjury.INJURIESDURINGAGAME:Intheunfortunateeventthatyourathleteisinjuredduringagame,pleaseremaininthestands.Iunderstandthatthismaybedifficult,butafranticparentrushingthefieldonlystirsemotionsintheinjuredathlete,whichcanmakeassessmentandcareoftheinjurymoredifficult.Aftertheinjuryisevaluatedandinitialtreatmentisprovided,theparentwillbecalledtothesideline/athletictrainingroomtobeinformedofthenatureoftheinjuryalongwithrecommendationsforcare.IndianSportsMedicineiscommittedtoprovidingGHSathleteswiththebestathletichealthcarepossible.PleasecallifyouhaveanyquestionsorconcernsByronMillwood,MS,ATC/SCATHeadAthleticTrainer,GilbertHighSchoolPhone:803-821-1985Fax:803-821-1938Email:bmillwood@lexington1.netFormoreinformationaboutourSportsMedicineProgrampleasevisithttp://gilbertathletics.org
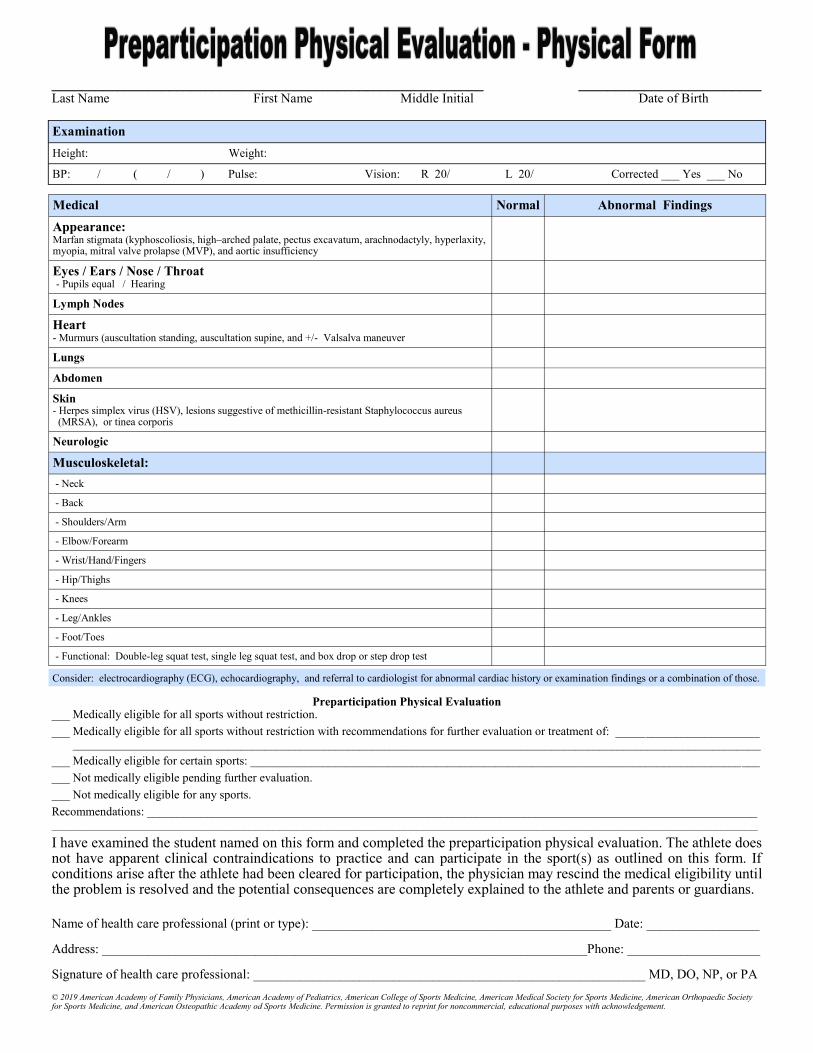
Medical Normal Abnormal Findings
Appearance: Marfan stigmata (kyphoscoliosis, high–arched palate, pectus excavatum, arachnodactyly, hyperlaxity, myopia, mitral valve prolapse (MVP), and aortic insufficiency
Eyes / Ears / Nose / Throat - Pupils equal / Hearing
Lymph Nodes
Heart - Murmurs (auscultation standing, auscultation supine, and +/- Valsalva maneuver
Lungs
Abdomen
Skin - Herpes simplex virus (HSV), lesions suggestive of methicillin-resistant Staphylococcus aureus (MRSA), or tinea corporis
Neurologic
Musculoskeletal:
- Neck
- Back
- Shoulders/Arm
- Elbow/Forearm
- Wrist/Hand/Fingers
- Hip/Thighs
- Knees
- Leg/Ankles
- Foot/Toes
- Functional: Double-leg squat test, single leg squat test, and box drop or step drop test
___________________________________________________________ _________________________ Last Name First Name Middle Initial Date of Birth
Examination
Height: Weight:
BP: / ( / ) Pulse: Vision: R 20/ L 20/ Corrected ___ Yes ___ No
Consider: electrocardiography (ECG), echocardiography, and referral to cardiologist for abnormal cardiac history or examination findings or a combination of those.
Preparticipation Physical Evaluation ___ Medically eligible for all sports without restriction.
___ Medically eligible for all sports without restriction with recommendations for further evaluation or treatment of: ________________________ ___________________________________________________________________________________________________________________
___ Medically eligible for certain sports: _____________________________________________________________________________________
___ Not medically eligible pending further evaluation.
___ Not medically eligible for any sports.
Recommendations: ______________________________________________________________________________________________________ ______________________________________________________________________________________________________________________
I have examined the student named on this form and completed the preparticipation physical evaluation. The athlete does not have apparent clinical contraindications to practice and can participate in the sport(s) as outlined on this form. If conditions arise after the athlete had been cleared for participation, the physician may rescind the medical eligibility until the problem is resolved and the potential consequences are completely explained to the athlete and parents or guardians.
Name of health care professional (print or type): _____________________________________________ Date: _________________
Address: _________________________________________________________________________Phone: ____________________
Signature of health care professional: ___________________________________________________________ MD, DO, NP, or PA
© 2019 American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports Medicine, and American Osteopathic Academy od Sports Medicine. Permission is granted to reprint for noncommercial, educational purposes with acknowledgement.
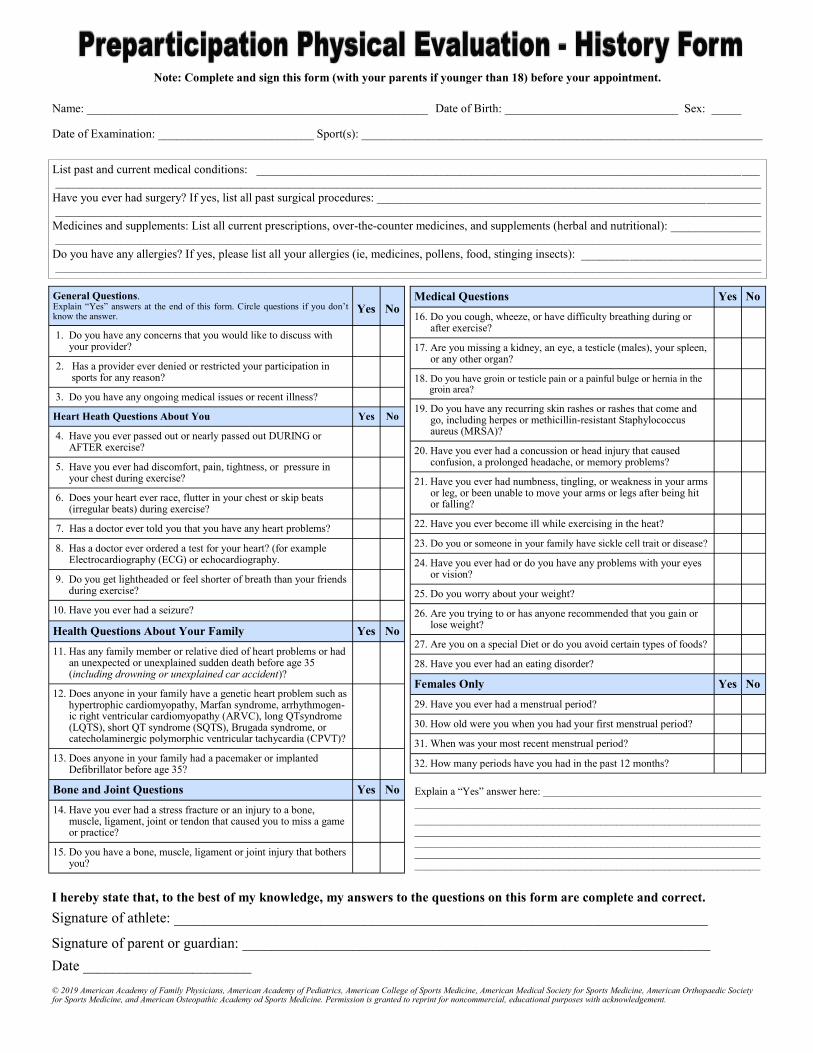
Note: Complete and sign this form (with your parents if younger than 18) before your appointment.
Name: _________________________________________________________ Date of Birth: _____________________________ Sex: _____ Date of Examination: __________________________ Sport(s): ___________________________________________________________________
List past and current medical conditions: ____________________________________________________________________________________ ______________________________________________________________________________________________________________________
Have you ever had surgery? If yes, list all past surgical procedures: ________________________________________________________________ ______________________________________________________________________________________________________________________
Medicines and supplements: List all current prescriptions, over-the-counter medicines, and supplements (herbal and nutritional): _______________ ______________________________________________________________________________________________________________________
Do you have any allergies? If yes, please list all your allergies (ie, medicines, pollens, food, stinging insects): ______________________________ ______________________________________________________________________________________________________________________
General Questions. Explain “Yes” answers at the end of this form. Circle questions if you don’t know the answer.
Yes
No
1. Do you have any concerns that you would like to discuss with your provider?
2. Has a provider ever denied or restricted your participation in sports for any reason?
3. Do you have any ongoing medical issues or recent illness?
Heart Heath Questions About You Yes No
4. Have you ever passed out or nearly passed out DURING or AFTER exercise?
5. Have you ever had discomfort, pain, tightness, or pressure in your chest during exercise?
6. Does your heart ever race, flutter in your chest or skip beats (irregular beats) during exercise?
7. Has a doctor ever told you that you have any heart problems?
8. Has a doctor ever ordered a test for your heart? (for example Electrocardiography (ECG) or echocardiography.
9. Do you get lightheaded or feel shorter of breath than your friends during exercise?
10. Have you ever had a seizure?
Health Questions About Your Family Yes No
11. Has any family member or relative died of heart problems or had an unexpected or unexplained sudden death before age 35 (including drowning or unexplained car accident)?
12. Does anyone in your family have a genetic heart problem such as hypertrophic cardiomyopathy, Marfan syndrome, arrhythmogen- ic right ventricular cardiomyopathy (ARVC), long QTsyndrome (LQTS), short QT syndrome (SQTS), Brugada syndrome, or catecholaminergic polymorphic ventricular tachycardia (CPVT)?
13. Does anyone in your family had a pacemaker or implanted Defibrillator before age 35?
Bone and Joint Questions Yes No
14. Have you ever had a stress fracture or an injury to a bone, muscle, ligament, joint or tendon that caused you to miss a game or practice?
15. Do you have a bone, muscle, ligament or joint injury that bothers you?
Medical Questions Yes No
16. Do you cough, wheeze, or have difficulty breathing during or after exercise?
17. Are you missing a kidney, an eye, a testicle (males), your spleen, or any other organ?
18. Do you have groin or testicle pain or a painful bulge or hernia in the groin area?
19. Do you have any recurring skin rashes or rashes that come and go, including herpes or methicillin-resistant Staphylococcus aureus (MRSA)?
20. Have you ever had a concussion or head injury that caused confusion, a prolonged headache, or memory problems?
21. Have you ever had numbness, tingling, or weakness in your arms or leg, or been unable to move your arms or legs after being hit or falling?
22. Have you ever become ill while exercising in the heat?
23. Do you or someone in your family have sickle cell trait or disease?
24. Have you ever had or do you have any problems with your eyes or vision?
25. Do you worry about your weight?
26. Are you trying to or has anyone recommended that you gain or lose weight?
27. Are you on a special Diet or do you avoid certain types of foods?
28. Have you ever had an eating disorder?
Females Only Yes No
29. Have you ever had a menstrual period?
30. How old were you when you had your first menstrual period?
31. When was your most recent menstrual period?
32. How many periods have you had in the past 12 months?
Explain a “Yes” answer here: _________________________________________ _________________________________________________________________
_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
© 2019 American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports Medicine, and American Osteopathic Academy od Sports Medicine. Permission is granted to reprint for noncommercial, educational purposes with acknowledgement.
I hereby state that, to the best of my knowledge, my answers to the questions on this form are complete and correct.
Signature of athlete: _________________________________________________________________________
Signature of parent or guardian: ________________________________________________________________
Date _______________________
S. Wendell Holmes Jr., MD, is the team physician for Gilbert High School.Call his o� ce at 803-296-9260.
803-29ORTHO | PHUSCOrthoCenter.org
Foot and Ankle | Joint Replacement | Trauma
Pediatric Orthopedics | Interventional Medicine
Spine Sports Medicine Hand and Upper Extremity
You win when you choose our teamOur highly skilled sports medicine team cares for the USC Gamecocks, weekend warriors and
everyone in between. And we’ll guide every step of your treatment — from diagnosis to recovery —
so you can get back to feeling like yourself as quickly as possible.
Put our innovation to work for you. Find your specialist today.
Mickey F. Plymale, MDJe� rey A. Guy, MD
Guillaume D. Dumont, MDMatthew R. Pollack, MD
Frank K. Noojin III, MDS. Wendell Holmes Jr., MD
Christopher G. Mazoué, MD
O� cial team physicians for the USC Gamecocks
Re
turn
ing
(Stu
de
nt/P
are
nt) A
thle
tic Pre
-Pa
rticipa
tion
Fo
rms R
eg
istratio
n
Y
ou
r scho
ol h
as electe
d to
collect p
re-p
articipatio
n fo
rms o
nlin
e. Fo
llow
the step
s belo
w to
re-co
mp
lete pre-p
articipatio
n reg
istration
:
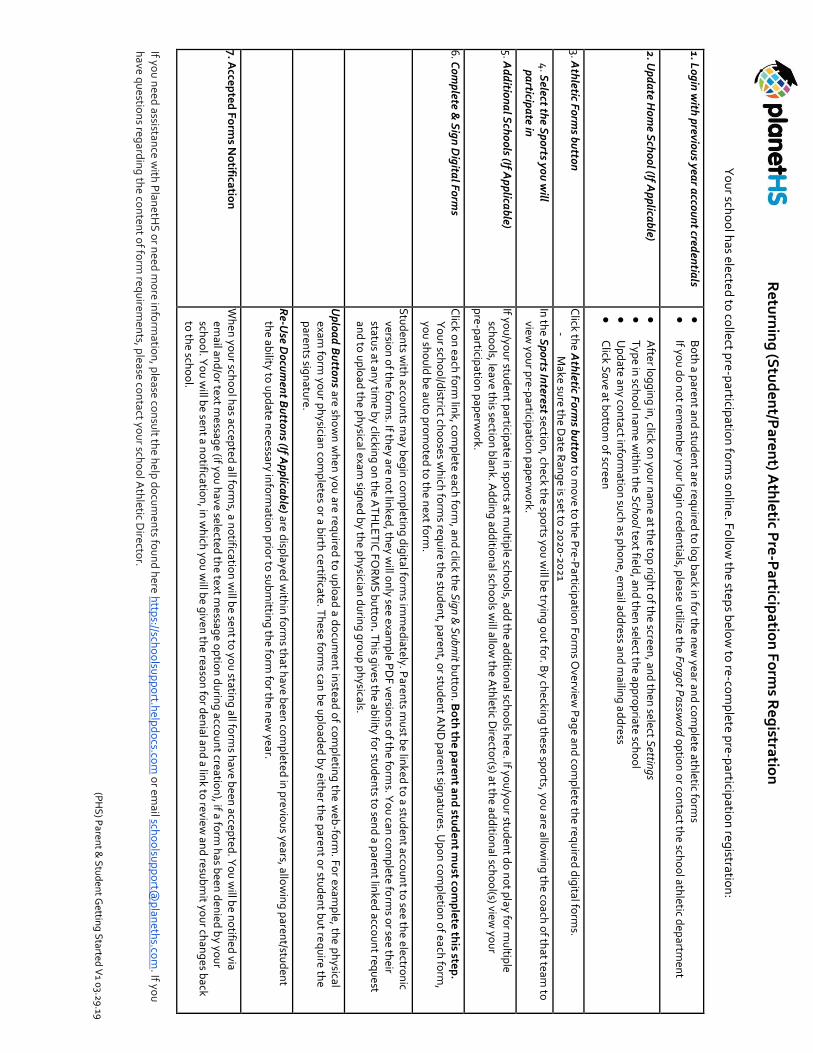
1. L
og
in w
ith p
reviou
s year a
ccou
nt cred
entia
ls ●
B
oth
a paren
t and
stud
ent are req
uired
to lo
g b
ack in fo
r the n
ew year an
d co
mp
lete athletic fo
rms
●
If you
do
no
t remem
be
r you
r log
in cred
entials, p
lease utilize th
e Forgot Pa
ssword
op
tion
or co
ntact th
e scho
ol ath
letic dep
artmen
t
2. Up
da
te Ho
me S
cho
ol (If A
pp
licab
le) ●
A
fter log
gin
g in
, click on
you
r nam
e at the to
p rig
ht o
f the screen
, and
then
select Settin
gs ●
T
ype in
scho
ol n
ame w
ithin
the S
chool text field
, and
then
select the ap
pro
priate sch
oo
l
●
Up
date an
y con
tact info
rmatio
n su
ch as p
ho
ne, em
ail add
ress and
mailin
g a
dd
ress
●
Click S
ave at b
otto
m o
f screen
3. Ath
letic Fo
rms b
utto
n
Click th
e Ath
letic Fo
rms b
utto
n to
mo
ve to th
e Pre-P
articipatio
n F
orm
s Overview
Pag
e and
com
plete th
e req
uire
d d
igital fo
rms.
- M
ake sure th
e Date R
ang
e is set to 2
02
0-2
02
1
4. S
elect the S
po
rts you
will
pa
rticipa
te in
In th
e Sp
orts In
terest section
, check th
e spo
rts you
will b
e trying
ou
t for. B
y checkin
g th
ese spo
rts, you
are allow
ing
the co
ach o
f that team
to
view yo
ur p
re-particip
ation
pap
erwo
rk.
5. Ad
ditio
na
l Sch
oo
ls (If Ap
plica
ble)
If you
/you
r stud
ent p
articipate in
spo
rts at mu
ltiple sch
oo
ls, add
the ad
ditio
nal sch
oo
ls here. If yo
u/yo
ur stu
den
t do
no
t play fo
r mu
ltiple
scho
ols, leave th
is section
blan
k. Ad
din
g ad
ditio
nal sch
oo
ls will allo
w th
e Ath
letic Directo
r(s) at the ad
ditio
nal sch
oo
l(s) view yo
ur
pre-p
articipatio
n p
aperw
ork.
6. C
om
plete &
Sig
n D
igita
l Fo
rms
Click o
n each
form
link, co
mp
lete each fo
rm, an
d click th
e Sign
& S
ubmit b
utto
n. B
oth
the
pa
ren
t an
d stu
de
nt m
ust co
mp
lete
this ste
p.
Yo
ur sch
oo
l/district ch
oo
ses wh
ich fo
rms req
uire th
e stud
ent, p
arent, o
r stud
ent A
ND
paren
t sign
atures. U
po
n co
mp
letion
of ea
ch fo
rm,
you
sho
uld
be au
to p
rom
oted
to th
e next fo
rm.
S
tud
ents w
ith acco
un
ts may b
egin
com
pletin
g d
igital fo
rms im
me
diately. P
arents m
ust b
e linked
to a stu
den
t accou
nt to
see the
electron
ic versio
n o
f the fo
rms. If th
ey are no
t linked
, they w
ill on
ly see examp
le PD
F versio
ns o
f the fo
rms. Y
ou
can co
mp
lete form
s or se
e their
status at an
y time b
y clicking
on
the A
TH
LE
TIC
FO
RM
S b
utto
n. T
his g
ives the ab
ility for stu
den
ts to sen
d a p
arent lin
ked acco
un
t requ
est an
d to
up
load
the p
hysical exam
sign
ed b
y the p
hysician
du
ring
gro
up
ph
ysicals.
U
plo
ad
Bu
tton
s are sho
wn
wh
en
you
are requ
ired to
up
load
a do
cum
ent in
stead o
f com
pletin
g th
e web
-form
. Fo
r exam
ple, th
e ph
ysical exam
form
you
r ph
ysician co
mp
letes or a b
irth ce
rtificate. Th
ese form
s can b
e up
load
ed b
y eithe
r the p
arent o
r stud
ent b
ut re
qu
ire th
e
paren
ts sign
ature.
R
e-Use D
ocu
men
t Bu
tton
s (If Ap
plica
ble) are d
isplaye
d w
ithin
form
s that h
ave been
com
pleted
in p
reviou
s years, allow
ing
paren
t/stud
ent
the ab
ility to u
pd
ate nece
ssary info
rmatio
n p
rior to
sub
mittin
g th
e form
for th
e new
year.
7. Acce
pte
d F
orm
s No
tificatio
n
Wh
en yo
ur sch
oo
l has accep
ted all fo
rms, a n
otificatio
n w
ill be se
nt to
you
stating
all form
s have b
een accep
ted. Y
ou
will b
e no
tified
via em
ail and
/or text m
essag
e (if you
have selected
the text m
essage
op
tion
du
ring
accou
nt creatio
n), if a fo
rm h
as been
den
ied b
y you
r sch
oo
l. Yo
u w
ill be sen
t a no
tification
, in w
hich
you
will b
e given
the reaso
n fo
r den
ial and
a link to
review an
d resu
bm
it you
r chan
ges b
ack to
the sch
oo
l.
If you
need
assistance w
ith P
lane
tHS
or n
eed m
ore in
form
ation
, please co
nsu
lt the h
elp
do
cum
ents fo
un
d h
ere http
s://scho
olsu
pp
ort.h
elpd
ocs.co
m o
r email sch
oo
lsup
po
rt@p
laneth
s.com
. If you
have q
uestio
ns reg
ardin
g th
e con
tent o
f form
requ
iremen
ts, please co
ntact yo
ur sch
oo
l Ath
letic Directo
r.
(PH
S) P
arent &
Stu
den
t Gettin
g S
tarted V
1 03.2
9.19





























