Embed Size (px)
Citation preview
Pathology
Glandular odontogenic cyst: Case report andreview of the literatureOsny Ferreira Júnior, DDS, MS, PhDVLuciana Reis Azevedo, DDS, MEduardo Sant'Ana, DDS, MS. PhDWanessa Soares Lara, DDS, MS.
Glandular odontogenic cyst (GOC) is a rare developmental cyst of the jaws. It is included in the WorldHealth Organization (WHO) histologie typing cl odcntogenic tumors under the terms glandular odonto-genic cyst or sialo-odontogenic cyst. The most common site ct occurrence is the anterior mandible, and itoccurs mostly in middle-aged people, A predilection lor men is observed. Ciinicai findings are not specitic,and an asymptomatic sweliing is frequently observed. A unilocuiar or muitilccular, weli-defined radioiu-cency is usually seen. The microscopic features of GOC. particularly the morphology of the epithelium,strongly suggest an origin from the remains of dental iamina, GOC has an unpredictable and potentiallyaggressive nature, which may indicate a high tendency of recurrence. The treatment of choice is still con-troversial, varying from a curettage to local block excision. A iong-term follow-up should be carried out. Theaim of this article is to report a case of gianduiar odontogenic cyst that recurred four times and fo empha-size the importance of long-term follow-up. The origin, epidemiology, ciinicai and radiographie aspects, andtreatment of the GOC are also discussed. (Quintessence int 2004:35:385-389)
Key words: botryoid odontogenic cyst, glandular odontogenic cyst, jaw cyst, lateral penodontai cyst,odontogenic cyst, sialo-odontogenic cyst
Tbe glandular odontogenic cyst {GOC) is a develop-mental cyst of the jaws that was described iti 1988
by Gardner et al̂ as a distinct entity. Padayachee andVan Wyk̂ had already described the microscopic fea-tures of these cysts but called them -'sialo-odontogeniccysts." The GOC is included in the WHO histologietyping of odontogenic tumors under the terms glandu-lar odontogenic cyst or sialo-odontogenic cyst.'
Glandular odontogenic cysts are rare, with just over50 cases reported in the literature.-'-^ Magnusson et al'analyzed 5,800 biopsies of jaw eysts between 1977 and1995 and observed that only seven cases fulfilled thecriteria for GOC. comprising 0.012''/o of the total The
'Associate Professor, Department of Stomatology (Surgery), Bauru Sohoolof Dentislry, University of Sao Paulo. Sao Paulo, Brazil.
^Graduate Student, Department ol Stomatoiogy. Bauru School of Dentistry,Uriversfly of Sao Pauio, Sao Paulo. Brazii.
^Associate Professor, Departmenl of Stomatology ¡Pathology). BauruSchool of Dentistry, University of Sao Paulo, Sao Paulo, Brazii.
Reprint requests: Dr Osny Ferreira Júnior. Department of Stomatology(Surgery), Bauru School of Dentist/^. University of Sao Paulo. AlamedaOtávio Pinheiro Brizolla 9-75, CEP. 17CÍ43-101 Bauru, Sao Pauio, Brazil.E-maii; [email protected]; [email protected]
most common site for fhis cysf is fhe anterior man-dible, but it can occur in every area of tbe jaws.̂ '-'=Clinically, it appears tbat tbe GOC oceurs mostly inmiddle-aged people'""^"' witb a mean age of 46.7years in males and 50.0 years in females.' The fe-male:male ratio is 19:28,' while other reported casesshow a slight predilection for men.̂ **" Recurrenceshave been described in 21% of tbe cases.
Clinical findings are not specific. An asymptomaticswelhng is frequently observed. Radiograpbieally. aunilocuiar or multilocular, well-defined radiolueency,with scalloped margins is usually seen.^-*"-'̂ '̂ '̂
fn the present study, a case of GOC is reported,emphasizing the potential for recurrence and the im-portance of long-term foUow-up, as well as the origin,epidemiology, clinical and radiographie aspects, andtreatment.
CASE REPORT
A 44-year-old white man was seen in the StomatologyClinic at the Bauru School of Denfistry, Universify ofSao Paulo, complaining of pain in the mandible. He
Quintessence Internationai 385
• Ferreira Júnior étal
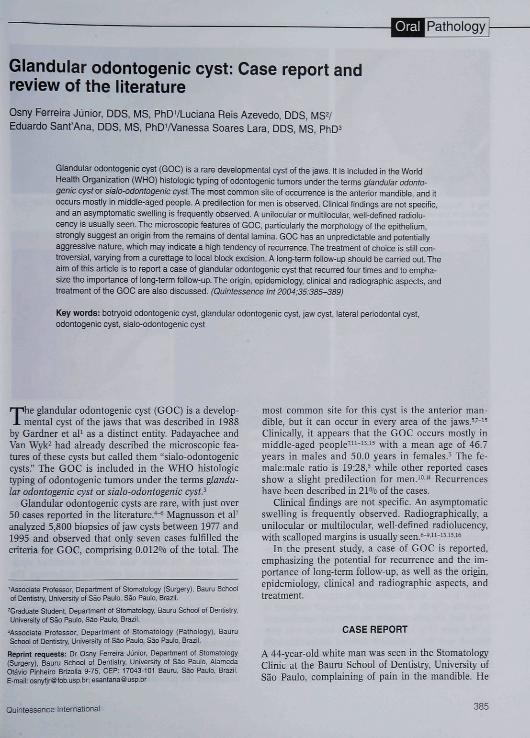
Fig 1 Purple-colored vestibular and lingual Fig 2 Panoramic radiograpti showing a iiultilocuiar radiolucehcy, with well-detined, seal-swelling in the region ol the \síí mandibular ioped margins in (he mandibular left region,lateral incisor to the left first molar
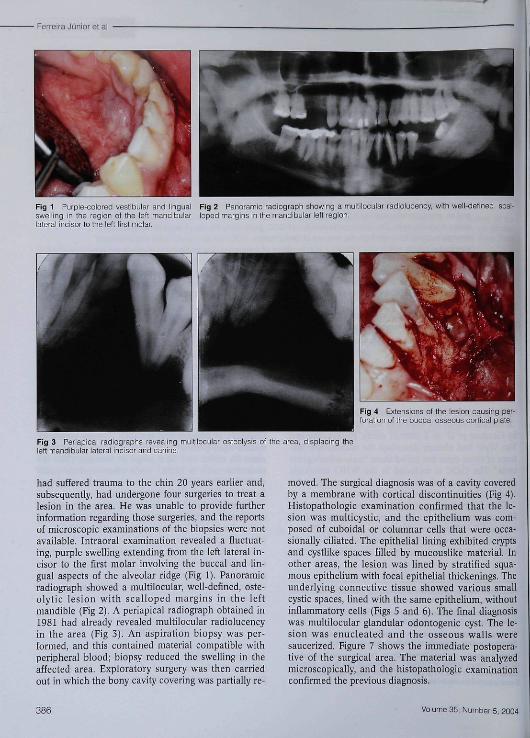
Fig 4 Extensions of the lésion causing per-foration of the buccal osseous cortical plate.
Fig 3 Periapical radiographs revealing multilooular osteolysis of the area, displacing thelett mandibular lateral incisor and canine.
had suftered trauma to the chin 20 years earlier and,subsequently, had undergone four surgeries to treat alesion in the area. He was unable to provide furtberinformation regarding those surgeries, and the reportsof microscopic examinations of fhe biopsies were notavailable, Intraoral examination revealed a fluctuat-ing, purple swelling extending from the left lateral in-cisor to the first molar involving the buccal and lin-gual aspects of the alveolar ridge (Fig 1), Panoramicradiograph showed a multilocular, well-defined, oste-olytic lesion with scalloped margins in the leftmandible (Fig 2), A periapical radiograph obtained in1981 had already revealed multilocular radiolucencyin the area (Fig 3), An aspiration biopsy was per-formed, and this contained material compatible withperipheral blood; biopsy reduced the swelling in theaffected area. Exploratory surgery was then carriedout in which the bony cavity covering was partially re-
moved, Tbe surgical diagnosis was of a cavity coveredby a membrane with cortical discontinuities (Fig 4),Histopathologic examination confirmed that the le-sion was multicystic, and the epithelium was com-posed of cuboidal or columnar cells tbat were occa-sionally ciliated. The epithelial lining exhibited cryptsand cystlike spaces filled by mucouslike material. Inother areas, the lesion was lined by stratified squa-mous epithelium with focal epithelial thickenings. Theunderlying connective tissue showed various smallcystic spaces, lined with the same epithelium, withoutinflammatory cells (Figs 5 and 6}, The final diagnosiswas multilocular glandular odontogenic cyst. The le-sion was enucleated and the osseous walls weresaucerized. Figure 7 shows the immediate postopera-tive of the surgical area. The material was analyzedmicroscopically, and the histopathologic examinationconfirmed the previous diagnosis.
386 Volume 35, Number 5, 2004
•Ferreirs Júnior et al
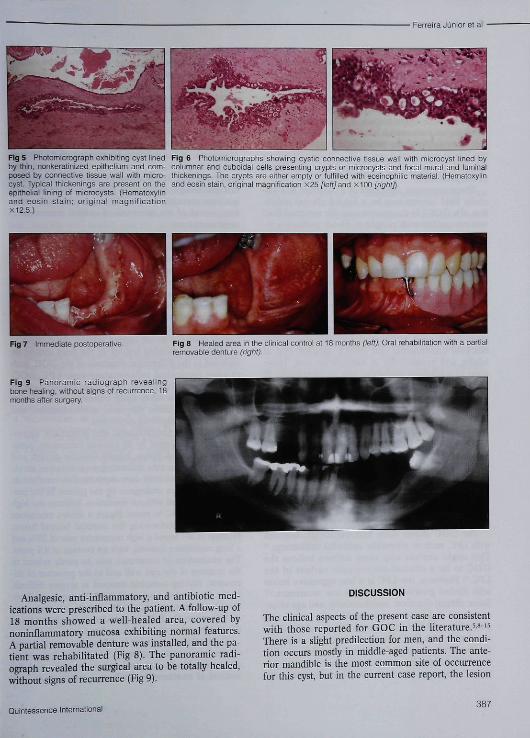
Fig 5 Photomicrograph exhibiting cyst lined Fig 6 Pi"'.-'t,-i--iciographs showing cystic connective (issue wail with microcyst lined byby Ihm, nonkeratinized epithelium and com- columnar and cuboidal cells presenting crypts or microcysts and tooal mural and luminalposed by connective tissue wall with micro- thickenings. The crypts are either empty or fulfilied with eosinophilic material. (Hematcxyiincyst. Typical thickenings are present on the and eosin stain, original magniticaticn x25 [left] and x WO [right}).epitheliai lining of microcysts. (Hematcxyiinand ecsin stain; original magnificationX12,5.]
Fig? Immediate postoperative Fig 8 Healed area in the clinical control at 18 months (left). Oral rehabilitation with a partialremovabie denture (right).
Fig 9 Panoramic radiograph revealingbone healing, without signs of recurrence, 18months after surgery.
Analgesic, anti-inflammatory, and antibiotic med-ications were prescribed to the patient. A follow-up of18 montbs showed a well-healed area, covered bynoninfiammatory mucosa exhibiting normal features.A partial removable denture was installed, and tbe pa-tient was rehabilitated (Fig 8). The panoramic radi-ograph revealed tbe surgical area to be totally healed,without signs of recurrence (Fig 9).
DISCUSSION
The clinical aspects of the present case are consistentwith those reported for GOC in the literature.'^"-''*There is a slight predilection for men, and the condi-tion occurs mostly in middle-aged patients. The ante-rior mandible is tbe most common site of occurrencefor this cyst, but in tbe current case report, the lesion
Quintessenceinternational 387

• i-erreira Junior et ai
extended to the left first moiar, Radiographically, amultilocular radiolucency is usuaily seen, althoughunilocular lesions have been described."-̂ Larger cystsmay produce swelling, as was found in the presentcase. The pain reported by tbe patient was probablydue to stretehing and pressure on the neurovascularbundles, since infiammation is a rare finding. TheGOC has an intraosseous location,'' and it bears no di-rect relationship to the periodontal ligament, as doesthe lateral periodontal cyst (LPC). It usually occursapically in relation to the teeth, but may show inter-dental extensions.'
The preoperative aspiration of a colorless, low-vis-cosity fluid content may be a helpful clinical indica-tion of a GOC' In the present case, the aspirated fluidwas compatible with peripberal blood, perhaps a re-sult of the previous surgeries.
The microscopic characteristics of GOC, particu-larly the morphology of the epithelium, strongly sug-gest an odontogenic epithelial origin, especially fromthe remains of dental lamina,'-'^'e The thin, cuboidalepitbelium in some areas resembles the reducedenamel organ epithelium. Furthermore, mural or lumi-nal plaques of eosinophilic and fusiform or roundedcells are seen in other lesions with accepted odonto-genic origin, such as lateral periodontai cyst (LPC),botryoid odontogenic cyst (BOC), gingival cyst ofadults, and occasionally in dentigerous cyst. Theseareas of epithelium thickening rnay be comparable tothe proliferative changes seen on epithelial cells ofdental lamina. They may be indicative of an activeprocess of proliferation of the odontogenic epitbeliumin their genesis.'' Immunohistochemical studiesstrongly support the odontogenic nature of GOC' '* ' 'The identification of osteodentin^ and the negative re-action for epithelial membrane antigen (EMA) in thearea of glandular structures'^ suggest that these fea-tures are not of true giandular origin and suppott theconcept of odontogenic differentiation in the GOC.The cystic epithelium reacted positively to antibodiesdirected against cytokeratins 7, 13, 14, and 19 and neg-atively to cytokeratins 8 and 18.'^
The GOC shares some histopathologic featureswith LPC, such as plaqueiiiie epithelial thicl<enings.'̂This might explain why some authors believe theGOC to be a clinical-microscopic variant of theLPC" However, the LPC is a less aggressive lesionwith limited growth potential and low recurrence.'"^Some clinical (location, multilocularity, and age of oc-currence) and microscopic (multicystic aspect andplaquelike epithelial thickenings) features of the GOCare shared with BOC. These characteristics might in-dicate a common origin for these lesions. It is possiblethat both lesions are merely variants of the same en-tity.'^" However, based on clinical, radiographie, be-
havioral, and histopathologic features, some authorsbelieve that GOC, LPC, and BOC should be consid-ered different entities.^'"
Although the presence of intraepithelial mucous-containing cysUc spaces is a characteristic shared withother odontogenic cysts, the GOC has microscopicfeatures and biologic behavior distinct enough to beregarded as an entity.^"
The GOC has been linked to the mucoepidermoidcarcinotTta."^ According to Magnusson et al,' the cen-tral mucoepidermoid carcinoma, especially the low-grade variant, is regarded as the most importanthistopathologic differential diagnosis from GOC. Ithas been speculated tbat GOC may represent the mostbenign end of the spectrum of central mucoepider-moid carcinoma.
However, Gardner et al' censured the term sialo-odontogenic cyst because an origin in salivary giandscould not be established. Tbe term was used doe to tbefaet that the mucous pools are often lined byeosinophiiic cuboidal cells, resulting in some resem-blance to salivary gland ducts. A second reason for theuse of the term sialo-odontogenic is the presence of mu-cous cells and pools of mucin in the epithelial lining.However, these features can be found in various odon-togenie eysts and do not imply a salivary gland origin.
Some slow-growing lesions of the jaws should beincluded in tbe differential diagnosis of the GOC, suchas cysts (periapical inflammatory cyst, LPC, BOC.residual cyst, dentigerous cyst, aneurismatic osseouscyst, odontogenic keratocyst); myxoma; central lesionof giant cells; fibrous dysplasia; ameloblastoma; andeentral mucoepidermoid carcinoma.^'"-'^'^'^
GOC has an unpredictable and potentially aggres-sive nature, suggested by its osseous extensions, pene-tration of cortical bones, locally invasive growth andhigh recurrence rate following conservative treat-ment." '̂ •'' The current case supports this conclusion.The four surgeries undergone by the patient in the pre-vious 20 years, all without resolufion, indicate the hightendency of GOC to recur. Figure 4 shows extensionsof the lesion, perforating the cortical buccal tissue.Hussain et al'^ found a high recurrence rate of 55% anda long recurrence interval, with an average of 4.9 years.The mechanism of recurrence may be partly related totbe thinness of tbe cyst wall and to tbe presence of mi-crocysts, making complete removal at surgery difficult.In the 47 reported cases untii 199S, Koppang et al̂ ob-served a recurrence rate of 21%. This number increasesto 30% when the BOC is considered and decreases toC/o to 50% when the LPC is analyzed.
The treatment of choice is sfiU controversial becauseof tbe few reported cases."'>-''*'-'5i« Tbe iesions arequite variable in size and aggressiveness, and thetnethod of treatment varies from a curettage to local
388 Volume 35, Number 5, 2004
• Ferreira Júnior et al
hlock excision.^'lO'^iíisiM^ Gardner and Morency"suggested that curettage or enucleation might be thetreatment of choice for GOC, provided that the clini-cian closely monitors the pafient for several years andthe lesion does not occur in the posterior maxilla be-cause of the difficult̂ ' of controlling recurrences in thisregion. A long-term follow-up shotild be carriedgy( iiziî.is ^ period of 3 years is recommended by theliterature, but some authors suggest that the patientsshotild be followed for at least 5 years after treatment.^Prognosis is good."^
In the present case, a total enucleation of the lesionwas conducted followed by saucerization of the os-seous walls, with the aim of mitiimizing the possibilityof recurrence. Eighteen tnonths after surgery, the areawas cfinically well-healed, and the patient was rehabil-itated (Fig 8). Panoramic radiograph did not show anysign of rectirrence (Fig 9). However, it was advisedthat follow-up should cotitinue.
REFERENCES
1. Gardner DG, Kessler HP, Morency R. Schaffner DL. Theglandular odontogenic cyst: An apparent entity. J OralPathol 1988:17:359-366.
2. Padayachee A, Van Wyk CW. Two cystic lesions with fea-tures of both the botryoid odontogenic cyst and the centralmucoepidermoid tumour: S i alo-odontogenic eyst? J OralPathol 1987:16:499-504.
3. Kramer IR. Pindborg JJ, Shear M. The WHO histologicaltyping of odontogenie tumours, A commentary on the sec-ond edition. Cancer 1992;70:2988-2994.
4. Barreto DC. De Marco L. Castro WH, Gomez RS.Glandular odontogenic cyst: Absence of PTCH gene muta-tion. J Oral Pathol Med 2001:30:125-128.
5. Koppang HS. Johannessen S, Haugen LK, Haanaes HR,Solheim T Donath K. Glandular odontogenic cyst (sialo-odontogenic cyst): Report of two cases and literature reviewof 45 previously reported cases. J Oral Pathol Med 1998:27:455-462. 20.
Tosios KI, Kakarantza-Angelopoulou E, Kapranos N, Immu-nohistoehemical study of bcl-2 protein, Ki-67 antigen andp53 protein in epithelium of glandular odontogenic cystsand dentigerous cysts. J Oral Pathol Med 2000:29:139-144.Magnusson B. Goransson L, Ödesjö B, Gröndahl K, HirschJ-M. Glandular odontogenic cyst. Report of seven eases.Dentomaxillofac Radioi 1997:26:26-31.Noffke C, Raubenheimer EJ. The glandular odontogeniecyst: Clincal and radiological features. Review of the litera-ture and report of nine eases. Dentomaxillofac Radioi2002:31:333-338.
Manor R, Anavi Y, Kaplan I, Calderón S. Radiological fea-tures of glandular odontogenie eyst. Dentomaxillofac Radioi2003;32:73-79.Chavez JA, Richter KJ. Glandular odontogenic cyst of themar!dible. J Oral Ma.\illofac Surg 1999;57:461^64.Gardner DG, Morency R, The glandular odontogenic cyst, arare lesion that tends to recur. J Can Dent Assoc 1993:59:929-930.Hussain K, Edmondson HD, Browne RM. Glandular odon-togenic cysts. Diagnosis and treatment. Oral Surg 1995;79:593-602,Patron M, Colmenero C, Larrauri J. Glandular odontogeniccyst: Clinicopathologic analysis of three cases. Oral Surg1991:72:71-74.Ramer M, Montazem A, Lane S, Lumerman H. Glandularodontogenic cyst. Report of a case and review of the litera-ture. Oral Surg 1997:84:54-57.Toida M, Nakashima E, Okumura Y, Tatematsu N.Glandular odontogenic cyst: A case report and literature re-view. J Oral Ma.-dlloiac Surg 1994;52:1312-I316.Damm DD, Fantasia JE. Anterior mandibular radioluceney.Glandular odontogenic cyst. Gen Dent 2000:48:107Altini M, Shear M. The lateral periodontal cyst: An update.J Orai Pathol Med 1992:21:245-250.Semba I. Kitano M, Mimura T, Sonoda S, Miyawaki A,Glandular odontogenic cyst: Analysis of cytokeratin expres-sion and elinicopathological features. Î Oral Pathol Med1994;23:377-382.de Sousa SO, Cabezas NT, de Oliveira PT, de Araúio VC.Glandular odontogenie cyst: Report of a ease with cytoker-atin expression. Oral Surg Oral Med Oral Pathol OralRadioi Endod 1997:83:478-483,Takeda Y. Glandular odontogenic cyst mimicking a lateralperiodontal eyst: A case report, lnt J Oral Maxillofac Surg1994;23:96-97.
Quintessence international 389






![Index [link.springer.com]978-1-4614-8755-5/1.pdf · Buccal bifurcation cyst (BBC), 254, 255 C Café-au-lait, 139 Calcifyling ghost cell odontogenic cyst, 257, 258 Cancer, 15 Capillary](https://img.pdfslide.net/doc/110x75/5f9e351b16a222075a07ff6d/index-link-978-1-4614-8755-51pdf-buccal-bifurcation-cyst-bbc-254-255.jpg)


![Case Report Orthokeratinized Odontogenic Cyst: A Report of … · 2019. 7. 31. · such as dentigerous cyst or paradental cyst [ , ]. Odon-togenic tumours such as ameloblastoma and](https://img.pdfslide.net/doc/110x75/614074aa1664f1518558c43e/case-report-orthokeratinized-odontogenic-cyst-a-report-of-2019-7-31-such-as.jpg)


















