-
Journal ofNeurology, Neurosurgery, and Psychiatry
1991;54:427-434
Glial swelling following human cerebralcontusion: an
ultrastructural study
R Bullock, W L Maxwell, D I Graham, GM Teasdale, J H Adams
AbstractThe ultrastructural features of cerebralcontusion seen
three hours to 11 daysafter head injury were studied in 18patients
undergoing surgery. Massiveastrocytic swelling ("cytotoxic"
oedema)was seen three hours to three days afterinjury, maximal in
perivascular footprocesses, and compressing some of theunderlying
capillaries. The tight junc-tions were not disrupted.
Neuronaldamage was most marked three to 11days after ijury. The
patho-physiological mechanisms leading tooedema formation and
neuronal degen-eration are discussed.
Cerebral cortical contusions are generallyregarded as the
pathological hallmark of headinjury and are clinically important
for severalreasons.`5 Extensive swelling of the corticalribbon and
underlying white matter mayoccur acutely after cerebral contusions
andmay cause mass effect, brain shift and raisedintracranial
pressure, and these events maycause secondary ischaemic brain
damage ordeath.6 When widespread, contusions causeextensive
destruction of the cortical ribbonparticularly at the tips of the
temporal andfrontal lobes and the orbital surface ofthe frontal
lobes, and this may lead topost traumatic epilepsy, and to the
neuro-psychological and behavioural sequelae,
Institute oftypical of severe head injury.7
Neurological Sciences, Although previous studies have
focusedGlasgow upon the pathogenesis,45 histopathology,1 dis-R
Bullock tribution' 3 and quantification of cerebral con-
D IGraham tusion, many aspects remain unresolved.3GM Teasdale
Why do some cerebral contusions swell andJ H Adams generate raised
intracranial pressure, whileCorrespondence to: others do not? What
proportion of theMr R Bullock, Department neuronal necrosis which
is seen adjacent toof Neurosurgery, Institute of
Neurological Sciences, cerebral contusions is due to primary
contactSouthemn GReer Hospitw, damage, and how much of it is due to
secon-Govan Road, Glasgow G514TF, UK dary factors, such as delayed
reduction inReceived 31 January 1990 blood flow to the contused
area?and in final revised form In studies in which we have mapped30
July 1990.Accepted 18 September 1990 cerebral blood flow following
human cerebral
Table IA Control patients-clinical data
AgeCase (years) Tissue biopsied Indication for surgery
1 65 Cortex and white matter right Deep temporal glioma,
seizurestemporal tip
2 56 Left frontal cortex Partial left frontal lobectomy
forglioma
3 36 Posterior right temporal cortex and Right temporal
lobectomy for gliomawhite matter
4 22 Right temporal cortex Right temporal lobectomy for
severeepilepsy
contusion, zones of profoundly reducedregional blood flow (rCBF)
have been foundadjacent to contusions, and this may be afactor in
the ischaemic neuronal necrosiswhich is a prominent finding in
pathologicalstudies. Alterations to the microvascular bedadjacent
to cerebral contusion may thereforebe an important determinant of
such changes.8The purpose of this study was to determine
ultrastructurally the changes in neuronal, glialand
microvascular morphology which occurwith time following human
cerebral con-tusion, and to determine their role in thepathogenic
processes which are known todamage the brain after severe head
injury.
Patients and methodsEighteen patients with severe cerebral
con-tusion were studied. Clinical details are shownin table lB. In
each patient, contusions wereshown on CT scan, and in seven
patients,mass effect, acute clinical deterioration andassociated
haematomas necessitated urgentoperation, at which the contusion was
resec-ted, and biopsy taken from the margins of theresected tissue.
In a further four patients, ICPmonitoring was initially performed
to ascer-tain the need to remove the contusion, andICP rose
necessitating surgery. In the remain-ing seven patients, delayed
neurologicaldeterioration occurred up to 11 days afterinjury,
precipitating the operation. Specimensof resected cerebral
contusion from thesepatients were compared with specimensprocessed
in an identical manner, from fourcontrol patients, with
macroscopically andradiologically normal brain tissue at the site
ofbiopsy, who had either temporal lobectomyfor epilepsy or
resection of deep temporalglioma. Clinical details of these
patients areshown in table 1A. Rongeur specimensaround 2 cubic mm
in size were taken fromcontused grey and white matter
andimmediately immersed in buffered glutaralde-hyde (350 m osm).
Specimens were thenstored at 4°C for two to seven days
untilprocessing for electronmicroscopy. The sitefrom which the
biopsy was taken was recordedby the surgeon and related as closely
as possi-ble to the CT appearance on the pre-operativescan. The
study was approved by the EthicsCommittee of the Institute of
NeurologicalSciences, Glasgow.
Processingfor electronmicroscopyAfter immersion fixation,
specimens were cutinto 200 p thick sections using a vibrotome,and
ultrasonicated to dislodge non-adherentblood components from the
vessel lumina.
427
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/
-
Bullock, Maxwell, Graham, Teasdale, Adams
Table lB Patients with cerebral contusion-clinical data
Case
2
Age(years)
67
33
Interval betweeninjury and biopsy
3 hours
6 hours
3 68 13 hours
4 18 16 hours
5 52 17 hours
6 18 23 hours
7 29 27 hours
8 17 28 hours
9 59 31 hours
10 55 33 hours
11 68 37hours
12 42 42 hours
13 46 44 hours
14 59 49 hours
15 40 72 hours
16 64 77 hours
17 44 5 days
18 72 11 days
CT diagnosis and clinical details
Fall. Right temporal contusion, small acute subduralhaematoma,
hemispheric swelling, high ICP (died)Fall. Right frontal lobectomy
for massive brain swellingwhen acute subdural haematoma removed.
(Alcoholic withclotting defect-died)RTA. Right temporal contusion
with deterioration ofconsciousness. Good recoveryRTA. Large
traumatic, right frontal intracerebralhaematoma and overlying
contusion, deterioration ofconsciousness. Good recoveryFound
unconscious and drunk. Left temporal contusion("Burst lobe") and
acute subdural haematoma. DisabledRTA. Bifrontal contusions. Left
frontal intracerebralhaematoma, deteriorating consciousness.
DisabledAssault. Focal right parietal contusion and
depressedfracture. Good recoveryRTA. Left hemispheric swelling and
temporalcontusions-ICP monitoring -+ high ICP. DisabledRTA. Acute
right extradural, subdural haematomas andright frontal contusion.
Deteriorating consciousness.DisabledFell while drunk. Delayed
deterioration. Coma. Bifrontalcontusions. Thin left acute subdural
haematoma. GoodrecoveryRTA. Right temporal contusion, small acute
subdural.ICP monitoring -+ high ICP. Good recoveryFound
unconscious. Delayed deterioration. Bitemporalcontusions. This left
acute subdural. Good recoveryFall. Delayed confusion. Right
temporal contusion. ICPmonitoring -. high ICP. Good
recoveryAlcoholic epileptic. ? Fall. Delayed confusion.
Bifrontalcontusions, mass effect. DisabledFall. Right parietal
acute subdural. Delayed ICP risenew low density. Right temporal -*
re-opening craniotomyand right temporal lobectomy. DisabledFall.
Multiple contusions. Left hemisphere, smallextradural haematoma.
Right parietal. Delayeddeterioration. Partial left temporal
lobectomy. DisabledHydrocephalic with shunt. Fell out of bed -.
bifrontalcontusions. Delayed coma. ICP high. Right frontalcontusion
evacuated. DisabledFall. Persistently confused. Right frontal
subacutesubdural, small temporal contusion. (Burst lobe atsurgery).
Disabled
Specimens were then fixed in 2% osmiumtetroxide in phosphate
buffer, and the sliceswere critical-point dried, mounted on
scan-ning electronmicroscopy stubs with silverpaint and
sputter-coated before viewing in aJEOL 300 TS scanning
electronmicroscope.Blood vessels were selected for particularstudy
and micrographs were taken at a mag-nification of 7000 and 1500
times to allowdemonstration of endothelial surface structureand
measure vessel size. After scanning elec-tronmicroscopy specimens
were carefullyremoved from the SEM stubs and washedthree times in
100% acetone to remove thesilver paint. The material was then
embeddedin araldite resin and cut into semi-thin sec-tions stained
with toluidine blue and areas of
Table 2 The time intervalsfor various EMfeatures after cerebral
contusion
Time interval at which EMoccurred after injury EMfeature
3 hours-3 days Astrocyte swelling3 hours-3 days Astrocyte
podocyte swelling3 hours-3 days Astrocytc podocyte disruption3
hours-7 days Vessel lumen compression3 hours-5 days "Swiss cheese
vacuolation" of neuropil on TM3, 16 hours Red cell diapedesis6
hours-3 days Endothelial fenestration on SEM16 hours-3 days
Intravascular clots adherent to walls16 hours-3 days Gross tissue
disruption + haemorrhage16 hours-5 days White matter "loosening"16
hours-l days Peri-vascular red cells3-11 days Pyknosis of
neurons5-7 days Sheet reaction-glycogen granules
-pseudopodial processes from astrocytes5, 11 days Leucocytic
phageocytosis
11 days Collagen deposition
interest selected for transmission electron-microscopy. Thin
sections were cut for thetransmission EM and routinely stained
withlead citrate and uranyl acetate and examinedin a JEOL 100 S
transmission electronmicros-cope.
ResultsBiopsies were obtained at time points rangingfrom three
hours to 11 days after injury. In allthe specimens the quality of
fixation as judgedby preservation of intracellular organelles
wasacceptable.
Control patientsNormal glial, neuronal and vascular
ultra-structure was present in all control patients,and the
neuropil and white matter density wasnormal (fig 1). Scanning
electronmicroscopydemonstrated pit-vesicle activity on
theendothelial surface of the lumen of all vesselsin the control
patients (table 2).
Transmission EM findings in patients withcerebral contusionA)
GROSS DISRUPTION OF TISSUEIn five specimens taken from three
patients thearchitecture of the cortical neuropil was dis-rupted by
red blood cells and plasma. When-ever this was seen, the adjacent
neuropil wasgrossly abnormal, demonstrating markedvacuolation and
lucency of astrocyte cyto-plasm (fig 2).
B) GLIAL CELL SWELLINGThe most consistent finding in both grey
andwhite matter in patients with cerebral con-tusions was severe
swelling affecting par-ticularly astrocytes. This was associated
with"loosening" and apparent pseudo-vacuolationof the neuropil to
produce a "Swiss cheese"appearance, particularly striking on
SEM.This appearance developed rapidly (figs 3, 4a)within three
hours of injury but was stillpresent in specimens taken three days
after
V,. .
' ...:
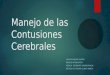
Figure I Thin section of cortical neuropilfrom controlpatient
KW. Preservation of intracytoplasmic organellesis satisfactory and
vacuolation of neuropil is absent.(Magnification: x 2975).
428
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/
-
Glial swelling following human cerebral contusion: an
ultrastructural study
Figure 2 Thin sectionthrough cortical neuropil16 hours after
injury. Notegross swelling of astrocyticcytoplasm (lower right)and
vacuolation ofneuropil caused by swellingastrocytic process.
Notemitochondria apparentlylyingfree within thecytoplasm of
swollenastrocytes (arrow).(Magnification: x 5250).
Figure 3 Scanning EMof a section throughcortical neuropil to
showvacuolation surrounding ablood vessel (arrow)("Swiss
cheese"appearance).(Magnification: x 1000).
injury. In the worst affected astrocytes, cyto-plasmic
disruption was present with completerupture of the cell membrane
(fig 5). Organe-lles such as mitochondria were, however,
stillrecognisable. In the specimens taken five daysafter injury,
astrocytic swelling was lessmarked although still apparent (fig 6a,
b) andthe astrocytes now contained deposits ofglycogen, typical of
the "sheet reaction" des-cribed by Torvick (fig 6).9
Figure 5 Thin section through white matter capillaryshowing
gross astrocytic foot process swelling (a), withdisruption of the
foot process limiting membranes andnarrowing and compression of
vessel lumen (L).(Magnification: x 3750).
C) SWELLING OF PERIVASCULAR PODOCYTICPROCESSESSwelling of
astrocytic perivascular podocyticprocesses were the most obvious
manifesta-tion of glial swelling. This was sufficientlysevere to
suggest compression of the adjacentvessel lumen in some cases (fig
4a, b). Disrup-tion of foot processes was seen in somespecimens
taken at periods from three hoursto three days after injury (fig
5). In specimenswhich were taken at later periods after
injury,astrocytic swelling appeared to be less exten-sive and at
five days astrocytic processes con-tained glycogen deposits and
pseudopodialfolds typical of the "sheet reaction" ofTorvick (fig
6a, b).9 Comparison between thechanges seen in cortex (fig 4a, b)
and those inwhite matter (figs 4, 5, 6) should, however, bemade
with caution.
D) VASCULAR CHANGES (TRANSMISSION ELEC-TRONMICROSCOPY)In the
majority of vessels seen within con-
VA .41 *a. .Figure 4 (A) Thin section through a cortical
capillary, showingflattening of vessel luwnen (L) and massive
swelling ofperivascular astrocytic foot processes (a). The lumen is
narrowed to such an extent that passage of red cells would
beimpossible. (Magnification: x 10 500); (B) ScanningEM preparation
of a larger blood vessel in cortical neuropilshowing collapse of
the vessel lumen andfolding of the tunica intima with adherent clot
(arrow).(Magnification: x 460).
4z29
lp*P.
I
,i..., ----. ,A -,..4i I"
n -t-S
AW
.,A ..
I1*
a
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/
-
Bullock, Maxwell, Graham, Teasdale, Adams
Figure 6 (A) Thinsection of white mattertaken five days
aftercontusion-the swelling ofastrocytic foot processes(a) is less
marked withglycogen accumulation.The sheet reaction
isapparent.(Magnification: x 8200);(B) Thin section ofcortical
neuropil in adifferent patient, operatedupon five days after
headinjury. Swollen astrocyteprocesses and accumulationofglycogen
granulestherein are seen. ( The so-called "sheet
reaction").(Magnification: x 8750).
tused tissue, endothelial cell morphology wasgrossly normal and
in those vessels whereadjacent astrocytic swelling was not
noticed,vessel lumina were not disrupted or occluded.No disruption
of inter-endothelial tight junc-tions was noted, and in the
majority of vesselsstudied, the morphology of the
perivascularbasement membrane was also normal.An increased number
of cytoplasmic folds
and processes on the luminal aspects of endo-thelium were seen
within vessels and thintransmission sections showed a very
irregularluminal profile to the endothelium at two days(fig 7).
Inter-endothelial junctions were notdisrupted despite gross
disruption of theadjacent neuropil. This irregular
endothelialprofile was also seen at five days when theastrocytic
sheet reaction had become wellestablished (fig 8).9Counts of
endothelial pinocytotic vesicles in
the vessels from contusion specimens taken atdifferent times
after injury, showed a declinewith time and the highest numbers of
vesicleswere seen in the control and acute patients(table 3).
Early white matter changes on transmission EMTwelve specimens of
white matter from con-tused tissue were studied. Preservation
ofmyelin was remarkably good. In some patients,swelling of axoplasm
was noted, but this wasnever severe. Cytoplasmic swelling of glial
cellswithin white matter was present but was lessmarked than that
seen in the grey matter.Accumulation of interstitial fluid within
whitematter was marked (fig 5).
[%*wo ; % s- * , ;
;
F^fs i&4>2K
Figure 7 High magnification thin section ofpart of avessel wall
two days after injury to show a thickenedirregular profile of the
endothelium. Microvilli arepresent. Note that the interendothelial
tightjunctions areintact (arrow). Astrocytic foot processes on the
abluminalsurface of the basal lamina are grossly
swollen.(Magnification: x 20 000).
Delayed changesA PYKNOSIS AND SHRINKAGEPyknosis and shrinkage of
both neurons andglia was noted when biopsies were taken atthree or
more days after injury (fig 9). Pyknoticneurons were frequently
surrounded bymicroglia which appeared to be carrying
outphagocytosis of damaged neuropil and cells. Inspecimens from the
two patients who werestudied five and 11 days after injury,
extensiveleucocyte and microglial phagocytosis was seenand
deposition ofcollagen fibres was prominent
Table 3 Microvillus counts (SEM) and pinocytotic vesicle
activity (TEM) after contusion
Endothelial pinocytotic Luminal microvillus counts per 25 p2Time
interval vesicle count mean (SD)after per p2injury mean (SD)
Capillaries (1Op)
Controls - 6 105 (3-51) 9-66 (3 77) 12 916 (3 81)Contusion 3-6
hours 6 125 (2-99) 2-92 (1 59) 22 19 (5-6)
13-23 hours 0-75 (0 45) 5 0 (2 5)24-48 hours 4-72 (3-01) 5-343
(2 44) 4 914 (1-35)2-5 days 1 5 (0 91) 7 166 (2 23) 8 45 (3 45)
11 days 7 91 (2 33) 12 31 (3 63)
430 on June 14, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.5.427 on
1 M
ay 1991. Dow
nloaded from
http://jnnp.bmj.com/
-
Glial swellingfollowing human cerebral contusion: an
ultrastructural study
Figure 8 Highmagnification thin sectiontaken five days
aftercerebral contusion. Notenumerous endothelialmicrovilli
andaccumulation ofglycogengranules in astrocyticperivascular foot
processes(a). (Magnification:x 26 000).
Figure 9 Thin section ofa pyknotic cortical cell,probably a
neuroncontaining lipofuscingranules, taken 72 hoursafter head
injury. Notemarked shrinkage andperi-cellular
vacuolation.(Magnification:x 11 000).
'~~1
.. .i
Figure 10 Thin sectionfrom cortical neuropil inpatient RS 11
days afterhead injury. Noteleucocytic phagocytosis(M) collagen
fibredeposition (outline arrow)andfibroblast (F).(Magnification: x
9250).,
(fig 10), indicating the early stages of scar tissueformation.
In the patient studied 11 days afterinjury, perivascular foot
process swelling wasabsent and the numbers of perivascularmicroglia
were increased, suggesting that thestage ofmaximal cell swelling
had been passed.
Findings on scanning electronmicroscopy inpatients with cerebral
contusionA NEUROPILThe vacuolated "Swiss cheese" appearance of
the neuropil in tissue adjacent to cerebralcontusions was
particularly noticeable on scan-n.g EM in comparison with the
controlpatients (fig 3).
B VASCULAR AND PERIVASCULAR CHANGESVessel morphology was
remarkably normal inall specimens studied. Tears in vessel
wallswere not seen. Blood clots occluding the lumenofvessels were
seen only occasionally, althoughthis may relate to the vibration
and ultrasonica-tion process which was used to visualise thelumina.
In many vessels, however, adherentred cells and leucocytes were
found suggestingan abnormality of endothelial adhesion
charac-teristics. Red cells were seen moving throughfenestrations
in the endothelial membrane toleave the vessel lumen, by a process
ofdiapedesis (fig 1 la, b).
Perivascular accumulations ofred blood cellswere a frequent
finding and in severalspecimens, these caused streak-like
disruptionof tissue architecture.
Pit-vesicle activityPit-vesicle activity was present in both
controland contusion specimens, but was less exten-sive in the
patients with contusions. In someareas, the endothelial luminal
membrane wasdisrupted by coalescent vesicles to formirregular holes
in the vessel walls, and in twospecimens, red cells were seen
passing throughthese (fig 1 la, b). Pit-vesicle activity in
theendothelium was always accompanied byparallel development of
microvillus formation,but the proportion of pit-vesicle
andmicrovillus activity was variable fromspecimen to specimen, and
no clear relation-ship was seen, either to time after injury, or
toother microscopic changes. When the numberof luminal microvilli
per 25 gim2 were countedusing SEM, and correlated with the number
ofvacuoles within the endothelial cytoplasm seenon transmission
electronmicroscopy, (table 3)no relationship was seen in either the
contusionor control material.The mean number of endothelial
micropin-
ocytotic vesicles in control patients was6-105 jim2 and 6-125
gm2 in contusion patientsat three hours after injury, 4-72 jim2 at
24-48hours after injury, and 1-5 pm2 at five days afterinjury. Thus
there was a slight (but not statis-tically significant) decline
over time in thenumber of endothelial pinocytotic vesicles
indamaged tissue.Marked changes in luminal microvillus
activity were seen in the contusion material, atvarious times
after injury (table 3). Incapillaries, microvilli numbers dropped
to theirlowest levels when astrocytic and foot processswelling was
most marked, at 13-24 hours andslowly rose to near control values
by 11 days.By contrast, in larger vessels microvillusactivity
rapidly rose to almost twice controllevels in the first six hours
after injury, thendropped to nearly a third ofcontrol levels at
24-48 hours, and were approaching control levelsby 11 days.
431
CA
.. I11
.Alk
.14..o
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/
-
Bullock, Maxwell, Graham, Teasdale, Adams
Figure 11 (A) ScanningEMpreparation of theluminal surface of
acortical arteriole taken 17hours after head injury.Note the large
fenestr:ae inthe endothelial surfacethrough which erythrocytesare
seen to pass (arrow).(Magnification: x 1780),(B) High
magnificationview of the endothelialsurface 17 hours after
headinjury. Note theendothelial microvilli anderythrocyte
passingthrough the fenestration.(Magnification: x 9700).
ii. . . ' ....................... ': S,'l B l l F ''
...........................................................................
!.: :.t Srsh t!M ; | l l 4 vSX w tleKi;Mes t
..s.X.'B','''.il5.E.s.iy l >lE .. v ;-. w* * r v . S: uS '
....... Y ] X l | S X .. . ..... . .>m A
...... < , . t: - :oR} ,i . g ,S - eSr ; .; ..
.. .8 ......... SX mt' .......................... ze e / * .
_.'. 't S e S, ,g,.,>,> SS ' -; S '' A A. .. , ,, .. W .. ,,,
.. ,,
-
Glial swellingfollowing human cerebral contusion: an
ultrastructural study
studied within the first few days, these changesshould be
interpreted with caution. Serialbiopsies were not taken from the
same patientand the severity of the contusion was variablefrom
patient to patient.For these reasons the mechanisms by which
perivascular astrocytic foot process swellingmay resolve after a
contusion cannot beinferred from this study. Although
specimenstaken at five days or more after the injury showevidence
of astrocytic process sprouting, andapparent reconstitution of the
foot processlimiting membranes, (fig 6a) this may representthe
response to a less severe lesion. To improveour understanding of
these fundamental repairmechanisms, serial biopsy studies will
beneeded, in an animal model, with a controlledseverity of
injury.
Early perifocal oedema has been demon-strated in
microgravimetric studies afterhuman contusion.8 19 The prominence
ofastrocytic swelling early after cerebral con-tusion, and the
integrity of the inter-endoth-elial tight junctions seen in this
study and inanimal models,1011 2021 suggests that this is
acytotoxic process. The relative paucity ofprotein-rich
extracellular fluid (except wheregross tissue disruption was
present), (fig 5)within the neuropil in this study is alsoevidence
against a vasogenic mechanism.This agrees with the results of
studies of
blood-brain barrier permeability which wehave performed at
various time intervals afterfocal cerebral contusion in 20
patients. SPECTscanning after intravenous 9'Tc pertech-netate,
showed that blood-brain barrier chan-ges were seldom detectable
before three daysafter injury, and were maximal at about
10days.8The micro-anatomical basis for the delayed
development of increased vascular per-meability after contusion
is difficult to deter-mine from this study, or from the
animalstudies of other authors. Povlishock, using afluid percussion
model of head injury, demon-strated that Horseradish peroxidase
(HRP)passed rapidly through intact endothelial cellsafter
intravascular injection, and accumulatedbeneath the basement
membrane, and withinendothelial vesicles.2" 22 HRP was found
chieflywithin endothelial cytoplasmic vesicles and thenumber of
vesicles increased rapidly within 15to 30 minutes after trauma.2'
In contrast tothese experimental observations, we havedemonstrated
that after a contusion micro-pinocytotic vesicles decline in number
withtime (table 3). Therefore, it is unlikely thatmicropinocytosis
is an important mechanism indelayed post-contusional oedema.The
role of pit-vesicle activity and
microvillus formation after head injury is notunderstood. Its
presence within hours of injuryafter "pure" diffuse axonal injury
suggests thatit may be a non-specific response to the invaria-ble
hypertensive surge which occurs withinseconds after severe head
injury.2 23-25We have observed coalescence of vesicles to
form ragged holes in the endothelial luminalmembrane, through
which intact erythrocytesare seen to pass (fig 11). This partly
accords
with other studies,22 and may provide amechanism for the
peri-vascular accumulationoferythrocytes, which is a frequent
histologicalfeature after contusion but which has not
beenpreviously explained.'45 Vessel tears maytherefore not be
necessary for perivascular"haemorrhage".Although we and other
authors have shown
that astrocytic swelling is well established aftercerebral
contusion as early as three hoursafter injury, both in this study
and in animalmodels, the cause for this swelling
remainsuncertain.""20 22When cerebral blood flow falls
sufficiently
low to cause failure of neuronal energymetabolism, and membrane
depolarisation(around 14-15 ml/100 gm/min) due to globalor focal
ischaemia, massive astrocytic swellingoccurs as a buffering
mechanism; astrocytesabsorb free K+ ions in an attempt to
maintainextracellular fluid homeostasis.26 27 Globalischaemia is,
however, unlikely to occur as avery early event after focal human
contusionand, moreover, some animal studies haveshown blood
pressure and CBF to be transien-tly elevated after head
injury.2325Faden et al and Becker et al have demon-
strated massive release of excitatory aminoacids after fluid
percussion injury, in tissuesimmediately beneath the impact point,
but notdistant from it.2829 Excitatory neuronal mem-brane
depolarisation may result from thisglutamate release, to cause
subsequent K+ionflooding ofthe extracellular space, and this
maycause astrocytic swelling, which itself mayjeopardise focal
tissue perfusion adjacent to acerebral contusion, and induce
furtherischaemic damage.26 A pathological "viciouscycle" such as
that shown in fig 12, may thus bepostulated, as a cause for
neuronal death incerebral contusion.
Vasoconstrictor substances such as K+,serotonin, or
prostaglandins may also bereleased into the contused tissue,
inducing theprofound fall in regional blood flow, which wehave
demonstrated on SPECT (8).
Further studies are needed to clarify thecauses of astrocytic
swelling, and to explorethe possibilities of therapy for preventing
orattenuating this astrocytic response, which maybe detrimental to
neuronal survival.
We are grateful to the neurosurgeons at the Institute
ofNeurological Sciences, Glasgow who assisted with
obtainingcerebral contusion and control specimens, and to Anne
Semplefor preparing the manuscript.
1 Adams JH, Gennarelli TA, Graham DI. Brain damage innon-missile
head injury: observations in man and sub-human primates. In: Thomas
Smith W, Cavanagh JB, edsRecent advances in neuropathology.
Edinburgh: ChurchillLivingstone, 1982:165-90.
2 Adams JH, Gennarelli TA, Graham DI, et al. Changes
inendothelial morphology of brain vasculature after con-trolled
angular acceleration of the subhuman primatehead. Proc
Physiological Soc 1987:92.
3 Adams JH, Scott G, Parker L, et al. The Contusion Index:
aquantitative approach to cerebral contusions in headinjury.
Neuropathol Appl Neurobiol 1980;6:319-24.
4 Lindenberg R, Freytag E. Morphology of cortical con-tusions.
Arch Pathol 1957;63:23-42.
5 Lindenberg R, Freytag E. The mechanism of cerebralcontusion.
Arch Pathol 1960;69:440-69.
6 Miller JD, Gudeman SK, Kishore PS, et al. Computedtomography
in brain oedema. Advances in neurology Vol28. New York: Raven
Press; 1980:413-22.
7 Levin HS, Grossman RG, Rose JE, et al.
Longtermneuropsychological outcome in closed head injury. J
433
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/
-
Bullock, Maxwell, Graham, Teasdale, Adams
Neurosurg 1979;50:412-22.8 Bullock R, Teasdale GM, Wyper D, et
al. Tomographic
mapping of CBF, CBV and BBB changes after focal headinjury using
SPECT: mechanisms for late deterioration.In: J Hoff, ed. Proc VIIth
Int Symposium IntracranialPressure and Brain Injury. Berlin:
Springer-Verlag1989:637-9.
9 Torvick R, Skjorten F. Electron microscopic observationson
nerve cell regeneration and degeneration, after axonlesions. I.
Changes in the nerve cell cytoplasm. ActaNeuropathol
1971;17:248-64.
10 Allen IV, Kirk J, Maynard RL, et al. An ultrastructuralstudy
of experimental high velocity penetrating headinjury. Acta
Neuropathologica (Berl) 1983;59:277-82.
11 Hekmatpanah J, Hekmatpanah CR. Microvascular altera-tions
following cerebral contusion in rats. J
Neurosurg1985;62:888-97.
12 Jenkins A, Maxwell WL, Graham DI. Experimentalintracerebral
haematoma in the rat: sequential lightmicroscopical changes.
Neuropathol Appl Neurobiol1989;15:477-86.
13 Little JR, Kerr FWL, Sundt TM. Microcirculatory obs-truction
and focal cerebral ischaemia: an electron micros-copic
investigation in monkeys. Stroke 1976;7(1):25-30.
14 Adams JH, Doyle D, Ford I, et al. Diffuse axonal injury
inhead injury. Definition, diagnosis and grading. Histopath-ology
1989;15:49-59.
15 Tenjin H, Mizukawa N, Yamaki T, et al. The investigationof
cerebral haemodynamics in patients with cerebralcontusion:
Evaluation of Positron Emission Tomography(PET). J CBF Metabol
1989;9(Suppl 1):S87.
16 Dietrich WD, Busto R, Ginsberg MD. Cerebral
endothelialmicrovilli and fenestration following global fore
brainischaemia. J Neuropathol Exp Neurol 1984;43:72-83.
17 Mendelow AD, Bullock MRR, Teasdale GM, et al.Intracranial
haemorrhage induced at arterial pressure inthe rat. Pt II. Short
term changes in local cerebral bloodflow measured by
autoradiography. Neurol Res1984;6:189-93.
18 Bullock MRR, Smith R, Favier J, et al. Brain specific
gravityand CT density measurements after human head injury. J
Neurosurg 1985;63:64-8.19 Galbraith S, Cardoso E, Patterson J,
et al. The water content
of white matter after head injury in man. In: Go KG,Baethmann A.
Recent progress in the study and therapy ofbrain oedema. New York:
Plenum Press, 1984:323-9.
20 Olsson Y, Rinder L. Studies on vascular permeabilitychanges
in experimental brain concussion. ActaNeuropathologica (Berl)
1968;11:183-200.
21 Povlishock JT, Becker DP, Sullivan HG, et al.
Vascularpermeability alterations to horse radish peroxidase
inexperimental brain injury. Brain Research 1978;153:223-39.
22 Povlishock JT. The morphopathologic responses toexperimental
head injuries of varying severity. In: BeckerDP, Povlishock JT,
eds. CNS Trauma Status Report.Bethesda, Maryland: NIH,
1986:443-52.
23 Gennarelli TA, Segawa H, Wald U, et al. Physiologicalresponse
to angular accelaration of the head. In: Gross-mann RG, Gildenberg
PL, eds. Head Injury: basic andclinical aspects. New York: Raven
Press 1982:129-39.
24 Maxwell WL, Irvine A, Adams JH, et al. Response of
thecerebral microvasculature to brain inmury. J
Pathology1988;155:327-35.
25 Nilsson B, Nordstrom CH. Experimental head injury in therat.
Pt 3. Cerebral blood flow and oxygen consumptionafter concussive
impact acceleration. J Neurosurg1977;47:262-73.
26 Bourke RS, Nelson KM. Further studies in the K +dependent
swelling ofprimate cerebral cortex in vivo: theenzymatic basis of
the K+ dependent transport ofchloride. J Neurochem
1972;19:663-85.
27 Plum F, Cooper AJL, Craig RP, et al. Glial cells: the
silentpartners of the working brain. The Thomas E DuffyMemorial
Lecture. J CBF and Metabol 1985;5(Suppl1):S1.
28 Becker DP, Katayama Y, Tamura T, et al. Excitotoxic
ionicfluxes and neuronal dysfunction following traumatic
braininjury. J CBF Metabol 1989;9(Suppl 1):302.
29 Faden AI, Demediuk P, Panter SS, et al. The role ofexcitatory
amino acids andNMDA receptors in traumaticbrain injury. Science
1989;244:798-800.
434
on June 14, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.5.427 on 1 May
1991. D
ownloaded from
http://jnnp.bmj.com/