Embed Size (px)
Citation preview

Aged Care Financing Authority
Report to inform the 2016-17 review of amendments to the Aged Care Act 1997
Part One: Analysis and Observations
April 2017

i

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Contents
GLOSSARY........................................................................................................................................................ V
EXECUTIVE SUMMARY.................................................................................................................................. IX
1 INTRODUCTION...................................................................................................................................... I
1.1 BACKGROUND..................................................................................................................................................... I1.1.1 About the Aged Care Financing Authority............................................................................................. i
1.2 APPROACH........................................................................................................................................................ III1.3 CURRENT FUNDING AND PRICING FRAMEWORK.........................................................................................................V
2 INCOME-TESTED AND MEANS-TESTED CARE FEES AND OTHER CHARGES IN HOME AND RESIDENTIAL CARE...................................................................................................................................... VIII
2.1 OVERVIEW OF FUNDING AND FEE ARRANGEMENTS IN HOME AND RESIDENTIAL CARE.....................................................VIII2.2 INCOME TESTING AND FEES IN HOME CARE..............................................................................................................XI
2.2.1 Pre-reform home care fee arrangements............................................................................................xi
2.2.2 Post-reform home care income-testing and fee arrangements...........................................................xi
2.2.3 Key home care data...........................................................................................................................xiii
2.3 ANALYSIS AND OBSERVATIONS: HOME CARE INCOME TESTING AND FEES......................................................................XIV2.3.1 Have the fee arrangements affected access to care?.........................................................................xiv
2.3.2 Are the home care fee arrangements equitable?...............................................................................xiv
2.3.3 Should providers be required to collect income-tested fees in home care?........................................xvi
2.3.4 Have the fee arrangements improved sustainability?.......................................................................xvii
2.4 MEANS-TESTING AND FEES IN RESIDENTIAL CARE...................................................................................................XVIII2.4.1 Pre-reform residential means-testing and fee arrangements...........................................................xviii
2.4.2 Post-reform residential means testing and fee arrangements.........................................................xviii
2.4.3 Key residential fees data....................................................................................................................xxi
2.5 ANALYSIS AND OBSERVATIONS: RESIDENTIAL MEANS TESTING AND FEES.....................................................................XXIII2.5.1 Have the changes to residential means testing improved equity in treatment of different forms of
wealth? xxiii
2.5.2 Is the treatment of the former principal residence appropriate?.....................................................xxiv
2.5.3 Have the means testing reforms contributed to sustainability?........................................................xxv
2.6 CONCLUSION................................................................................................................................................ XXVII2.6.1 Have the annual and lifetime caps been effective?.........................................................................xxvii
2.6.2 Are fees across CHSP, home care and residential care effectively aligned?....................................xxviii
2.6.3 Have the policy objectives been achieved?.......................................................................................xxxi
ii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.6.4 Are there any unintended consequences?.......................................................................................xxxii
2.6.5 Possible future reform directions....................................................................................................xxxiii
3 ACCOMMODATION PAYMENTS IN RESIDENTIAL CARE.............................................................XXXV
3.1 ACCOMMODATION PAYMENTS IN RESIDENTIAL CARE.............................................................................................XXXV3.1.1 Reforms to accommodation payments............................................................................................xxxv
3.1.2 Key accommodation payments data.............................................................................................xxxviii
3.2 ANALYSIS AND OBSERVATIONS.........................................................................................................................XXXIX3.2.1 How are consumers exercising choice?...........................................................................................xxxix
3.2.2 Is there increased diversity in accommodation prices?........................................................................xl
3.2.3 Have changes to accommodation payments impacted access to care?..............................................xli
3.2.4 Is the maximum accommodation payment an effective mechanism for regulating accommodation
prices? xliii
3.2.5 Have the changes to accommodation payments improved viability and investment?......................xliv
3.2.6 Is the MPIR appropriate as the rate to be used in calculating equivalence between lump sums and
daily amounts?...............................................................................................................................................xlvii
3.2.7 Have the accommodation payment reforms contributed to the sustainability of residential care? xlviii
3.3 CONCLUSION..................................................................................................................................................XLIX3.3.1 Have the policy objectives been achieved?........................................................................................xlix
3.3.2 Issues and potential unintended consequences.....................................................................................l
3.3.3 Possible Future Reform Directions........................................................................................................ li
4 ACCESS TO AGED CARE SERVICES.....................................................................................................LIII
4.1 POST-1 JULY 2014 SUPPLY OF SUBSIDISED AGED CARE SERVICES................................................................................LIII4.1.1 How does supply impact access to care?............................................................................................liii
4.1.2 How has the profile of community, home and residential care providers changed since the reforms
commenced?...................................................................................................................................................... lv
4.2 HAVE THE FUNDING AND FINANCING CHANGES IMPACTED CONSUMER ACCESS TO CARE?..............................................LVIII4.2.1 Home care......................................................................................................................................... lviii
4.2.2 Residential care................................................................................................................................... lx
4.2.3 How is the alignment between home-based care and support and residential care impacting
consumer access to care?................................................................................................................................ lxiii
4.2.4 Has there been any impact on access to care for people with low means?........................................lxv
4.3 IS CONSUMER DIRECTED CARE SUPPORTING ACCESS TO CARE?................................................................................LXVI4.3.1 Has Consumer Directed Care impacted provider viability?...............................................................lxvii
4.4 CONCLUSION...................................................................................................................................................LXX4.4.1 Have the policy objectives been achieved?.........................................................................................lxx
4.4.2 Are there any unintended consequences?.........................................................................................lxxi
4.4.3 Possible future reform directions...................................................................................................... lxxi
iii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
5 AGED CARE WORKFORCE............................................................................................................... LXXIII
5.1.1 Workforce supplement....................................................................................................................lxxiii
5.1.2 Wage costs as a proportion of provider expenses...........................................................................lxxiii
5.1.3 2016 Aged Care Workforce Census and Survey..............................................................................lxxvii
iv

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Glossary
Term Definition
Accommodation supplement The accommodation supplement is payable on behalf of residents receiving permanent residential aged care who do not have the capacity to contribute to all or part of the cost of their accommodation.
Aged Care Act 1997 (the Act) The Act is the legislation upon which the Australian Government funded aged care system is based.
Aged Care Financing Authority (ACFA)
ACFA is statutory committee who provides independent advice to the Australian Government on funding and financing issues, informed by consultation with consumers, and the aged care and finance sectors.
Aged Care Funding Instrument (ACFI)
The ACFI is a resource allocation instrument that focuses on care needs related to day to day, high frequency need for care. These aspects are appropriate for measuring the average cost of care in longer stay environments.
Aged Care Pricing Commissioner
The Aged Care Pricing Commissioner is an independent, statutory office holder appointed under the Aged Care Act 1997 and reports to the Minister for Aged Care.
Aged Care Sector Committee(ACSC)
The ACSC provides advice to Government on aged care policy development and implementation and helps to guide future reform of the aged care system.
Agreed accommodation price Accommodation prices agreed between providers and prospective residents prior to entry, as reported by providers through the Aged Care Entry Record.
Bond Guarantee Scheme A Government scheme that guarantees repayment of bond monies to residents if an insolvent or bankrupt provider defaults on its obligation to refund accommodation bonds.
Commonwealth Home Support Programme (CHSP)
From 1 July 2015, the Commonwealth Home Support Programme commenced. The CHSP brings together the Commonwealth HACC Programme, the National Respite for Carers Program, the Day Therapy Centres Program and the Assistance with Care and Housing for the Aged Program. The CHSP is one consolidated program that provides entry-level home support for older people who need assistance to keep living independently at home and in their community.
Consumer Directed Care (CDC)
Consumer Directed Care gives older people and their carers greater choice and control over the types of care services they
v

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
receive and the delivery of those services.
Department of Health (The Department)
The Australian Government department that administers the Act and regulates the aged care industry on behalf of the Australian Government.
Extra Service Status Granted to residential aged care providers that provide a significantly higher than average standard of services including accommodation, range and quality of food, and non-care services such as recreational and personal interest activities.
Facility A residential aged care facility, approved under the Aged Care Act 1997 to provide government subsidised accommodation and care.
Flexible care For those in either a residential or home care setting, that may require a different care approach than that provided through mainstream residential and home care.
Government provider In the context of this Report, the term references a provider that is owned by a local, state or territory government.
High care place A place which is occupied by a ‘high care’ resident, as defined by their ACFI assessment. The distinction between high care and low care was removed from 1 July 2014.
Higher accommodation supplement
A higher maximum accommodation supplement was introduced on 1 July 2014 for aged care homes that have been built or significantly refurbished since 20 April 2012.
Home and Community Care(HACC)
A program of basic maintenance and support services for frail older people, younger people with disabilities and the carers of these people to prevent premature admission to Residential Care Services. It includes home nursing, home help, respite care and assistance with meals and transport. As of 1 July 2015 the Commonwealth HACC programme became part of the new Commonwealth Home Support Programme (CHSP). In 2015-16 the joint Commonwealth-State Home and Community Care (HACC) programs continued to operate separately in Victoria and Western Australia.
On 1 July 2016, Victorian Home and Community Care (HACC) services for people aged 65 years and over (50 years and over for Aboriginal and Torres Strait Islander people) transitioned to the Commonwealth CHSP.
On 1 February 2017, the Australian Government announced the transition of responsibilities for Western Australian HACC services and specialist disability services for older people (aged 65 years and over and 50 years and over for Aboriginal and Torres Strait Islander people) to the Commonwealth. From 1 July 2018, the Commonwealth will assume full funding policy and operational responsibility for these services.
Home care Home based care provided through a home care package to help older Australians to remain in their own homes. Home care is provided through the Home Care Packages Programme (see
vi

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
below).
Home care package A coordinated package of services tailored to meet the care needs of a person living at home. The package is coordinated by an approved home care provider, with funding provided by the Australian Government. Home Care Levels 1 and 2 help people with basic or low level care needs, whilst Levels 3 and 4 help people with intermediate to high care needs. This programme commenced 1 August 2013 and replaced the Community Aged Care Programme, the Extended Aged Care at Home (EACH) and Extended Aged Care at Home Dementia (EACHD) packages.
Low care place A place which is occupied by a ‘low care’ resident, as defined by their ACFI assessment. The distinction between high care and low care was removed from 1 July 2014.
Maximum accommodationcontribution
The maximum accommodation contribution a person can pay is the lower of either a resident’s means-tested accommodation contribution, or the maximum accommodation supplement the facility is eligible to receive.
Maximum accommodation payment
The maximum accommodation payment is determined by the Minister through legislative instrument. The maximum accommodation payment at 1 April 2017 was a refundable deposit of $550,000 or equivalent daily payment of $87.09.
Maximum Permissible Interest Rate (MPIR)
The MPIR is the rate used to calculate the equivalent daily payment of a refundable deposit. The refundable deposit is multiplied by the MPIR and divided by 365 days.
The MPIR is determined in accordance with Section 6 of the Fees and Payments Principles 2014 (No. 2). The MPIR is available on the Department of Health website and is updated quarterly. As at 1 April 2017 it was 5.78 per cent.
Operational ratio The Australian Government regulates the supply of subsidised residential aged care and home care packages by specifying a national provision target of subsidised operational aged care places. These targets are based on the number of persons for every 1,000 people aged 70 years or over. The population-based provision formula ensures that the supply of services increases in line with the ageing of the population, while capping the number of places limits the fiscal risk associated with aged care.
Per resident per annum (prpa)
A measure relating to residential aged care residents that converts service financial data to daily amount per resident.
Per resident per day (prpd) A daily average financial figure relating to Residential aged care residents.
Refundable Accommodation Deposit (RAD)
An amount paid as a lump sum by a post-1 July 2014 resident for their accommodation costs in a residential aged care facility.
Regional Geographic reference to areas classified by the Australian Bureau of Statistics as inner regional, outer regional, remote and very remote.
vii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Report on the Operations of the Aged Care Act 1997 (ROACA)
A legal requirement under the Act, the ROACA is tabled in Parliament in November each year and presents an annual snapshot of facts and figures on Commonwealth funded aged care services in Australia.
Residential aged care A programme that provides a range of supported accommodation services for older people who are unable to continue living independently in their own homes.
Restorative care Is care focusing on enhancing the physical and cognitive function of people who have lost or are at risk of losing condition and independence. The Short-Term Restorative Care (STRC) Programme aims to reverse and/or slow ‘functional decline’ in older people and improve their wellbeing. Funds were allocated in the 2015-16 Budget for the allocation of Commonwealth subsidised short term restorative care places.
Retention amounts An amount that an approved provider is allowed to deduct per month from an accommodation bond for up to five years. The maximum retention amount is set by the Australian Government. Retentions are not permitted for new residents entering residential aged care after 1 July 2014.
Scale (providers) Refers to the number of services operated by a provider.
Survey of Aged Care Homes (SACH)
Each year SACH seeks information on accommodation payments and planned and actual building activity during the previous financial year for each operating residential aged care service.
Viability supplement The viability supplement for residential and home care is a payment made under the Act to assist aged care services in rural and remote areas with the extra cost of delivering services in those areas.
Weighted Average Cost of Capital (WACC)
The average cost of financing the assets of the entity weighted by the use of its debt and equity.
viii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Executive Summary
The Aged Care Financing Authority (ACFA) is a statutory committee whose role is to provide independent, transparent advice to the Australian Government on financing and funding issues in the aged care industry.
As part of significant changes to aged care announced in 2012, a requirement for an independent review of the reforms was included in the Aged Care (Living Longer Living Better) Act 2013. The Review is being led by Mr David Tune AO, PSM.
In November 2015, the former Minister for Health and Aged Care asked ACFA to provide advice on funding, financing and pricing issues affecting the matters specified in the Review’s terms of reference. In particular, ACFA was asked to focus on such issues as they relate to means testing, fees, accommodation prices, access and workforce.
This report provides a summary of the funding and financing changes in home and residential care, presents key data to inform assessment of the effectiveness of the funding and financing changes, and presents analysis and discussion of issues and observations arising from that data.
Chapter 1 Introduction
Broadly put, the reforms to funding and financing arrangements in aged care aimed to:
increase transparency and consumer choice; improve the viability and sustainability of aged care services; and improve the long-term sustainability and equity of the aged care system.
In assessing how effective the reforms were in achieving these aims, ACFA has taken a ‘360-degree view’, analysing their impacts on:
consumers – in terms of equity of access to aged care services; providers – in terms of viability; and government – in terms of the sustainability of the aged care system.
The report is divided into five chapters with additional data contained in Part Two - Appendices:
Chapter 1 – Introduction; Chapter 2 – Means testing; Chapter 3 – Accommodation payments; Chapter 4 – Access to care; and Chapter 5 – Workforce.
The Introduction contains an overview of the current framework.
ix

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Chapter 2 Income-tested and means-tested care fees and other charges
The key means-testing reforms were:
introducing formalised income testing with subsidy reduction for home care; combining the income and assets test for residential care, including a capped value
for the former principal residence; and annual and lifetime caps on income and means-tested care fees.
The changes to means testing aimed to: improve equity in the treatment of income and assets; introduce greater consistency in fee arrangements and improve equity in consumer
contributions; improve sustainability by ensuring those who can afford to contribute to the cost of
their care and accommodation; and maintain protection for residents with low means.
ACFA’s observations on the means-testing reforms are summarised from the consumer, provider and government perspective:
Consumer perspectiveHome care
Lower level packages are not attractive, especially to consumers with greater wealth who would contribute more.
There is greater demand for higher level packages, where annual caps on consumer contributions mean consumers receive comparatively greater value.
There is confusion about the purpose of the basic daily fee and a perception that the fee is too high, especially for lower level packages.
Inconsistent charging of the basic daily fee and the income-tested fee by providers raises equity issues.
Residential care Equity in the treatment of different forms of wealth has improved as a result of the
combined means test, although the treatment of the former residence benefits homeowners over non-homeowners.
There has been no noticeable impact on access to care for consumers with low means.
Provider perspectiveHome care
Some providers do not charge the full basic daily fee and/or full income-tested care fee in home care, resulting in possible impacts on care and/or viability.
Residential care
There has been an increase in providers charging fees for additional services.
x

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Government perspectiveHome care
Home care subsidy reductions have not resulted in expected savings, as the majority of home care consumers’ income-tested care fee is zero.
Residential care
Sustainability has improved, with the government’s share of the overall average cost per resident per year (i.e. including care, accommodation and basic daily living costs) reduced to 65.6 per cent under the post-reform means test, compared with 68.3 per cent if the pre-reform arrangements were applied.
With regard to possible future reform ACFA notes that the role and level of consumer contributions in the aged care system will be a key question. The Aged Care Sector Committee’s Roadmap envisages a greater role for consumer contributions in return for greater consumer choice and control and competition in the provision of services leading to higher quality services.
Having regard to the affordability of a consumer-driven market-based system, the Roadmap proposes that:
all income and assets should be means tested and treated equally; new financial products (e.g. home equity release) will need to be available; fee arrangements across home care and CHSP should be integrated; and consumer subsidies should be aligned across care settings for consumers with the
same care needs.
Chapter 3 Accommodation payments in residential care
The key accommodation payment reforms were:
significant deregulation of accommodation pricing, with previous restrictions such as the types and amounts of payments for high care residents removed;
consumer choice measures such as full consumer choice over accommodation payment type (lump sum or periodic) with the relationship between the lump sum and periodic payment price made ‘equivalent’ by using a standard conversion factor (the maximum permissible interest rate);
consumer protection and competition measures such as requiring publication of accommodation prices on My Aged Care and elsewhere and the introduction of the Aged Care Pricing Commissioner to approve prices over a threshold;
removing the ability for providers to deduct retention amounts from lump sum payments; and
an increase in the accommodation supplement paid by Government for supported residents in new or significantly refurbished homes.
The changes to accommodation payments aimed to: introduce transparency and increase consumer choice; support a more market-based approach to accommodation pricing;
xi

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
encourage investment and development of residential accommodation capacity; improve sector sustainability; and maintain safeguards and access to care for residents with low means.
ACFA’s observations on the accommodation payment reforms are summarised from the consumer, provider and government perspective:
Consumer perspective Greater transparency of accommodation options, improved quality resulting from
increased investment in refurbishment and greater price competition. Average agreed prices are lower than average published prices.
Consumers are exercising more choice of payment, with more consumers choosing to pay by daily payment or combination, although lump sums are still the preferred payment type for non-supported residents.
Consumers have greater discretion in accommodation choices, as they are not restricted by the amount of their net assets (that is, they can agree to a price that, in lump sum terms, is greater than their net assets and pay by daily payment or combination of daily payment and lump sum).
Provider perspective The pool of lump sums continues to grow. New or significantly refurbished homes receive a higher accommodation supplement
for low means residents that is broadly equivalent to the market-based average refundable accommodation deposit paid by non-supported residents.
Government perspective Building activity has increased. Liability for guaranteed lump sums has increased.
With regard to possible future reform, the reforms to accommodation payments have led the way in moving towards a more market-based consumer-focused aged care system.
The publication of accommodation prices on My Aged Care has achieved market-based pricing for accommodation, improving transparency and enabling consumers to compare and negotiate the accommodation price with their preferred provider.
As noted in the Aged Care Sector Committee’s Roadmap an important consideration going forward will be that government continue to provide safeguards for consumers with limited means. The Roadmap also envisages that the market will provide an expanded range of financial products to provide flexible ways for people to pay for their aged care.
Chapter 4 Access to aged care services
Changes which had the potential to affect access to care included:
new income testing and means testing; accommodation payment reforms;
xii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
consumer directed care in home care; increased supply of home care packages; and introduction of the Commonwealth Home Support Program.
The overarching objectives of the reforms from an access perspective were to increase consumer access to home care and to give consumers greater choice, control and flexibility when accessing care. To this end, the reforms to means-testing and fee arrangements and the controlled expansion of home based care were the most significant, along with measures to ensure access by consumers with lesser means.
ACFA’s observations on the impact on access are summarised from the consumer, provider and government perspective:
Consumer perspective:
Home care
Increased availability of home care packages has given more consumers the opportunity to access care while living at home.
Consumer directed care, individual budgets and monthly statements have improved transparency and facilitated consumer choice, although there is some confusion about fees.
There is a low take-up of lower level packages, suggesting fee arrangements have had some impact and some consumers may be seeking services elsewhere or using informal care arrangements.
Residential care
Transparency of accommodation options, quality and price competition has improved.
There is a diverse range of accommodation options available at different price points, though consumer choice may be constrained by supply controls.
People with lower means are still able to access residential aged care.
Provider perspective Some providers do not charge full basic daily and/or income-tested care fees in
home care, depending on financial circumstances.
Government perspective
Home care
Home care recipients are predominantly pensioners. Some consumers are choosing to remain on more generous services under
Commonwealth Home Support Program.
Residential care
Building activity has increased. No noticeable impact on access to care for residents with low means. Use of respite care has increased.
xiii

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Ensuring access to care will be a key question for future reform, especially in the context of the role of supply restrictions and market operation of the aged care system.
The consumer-driven market-based aged care system envisaged by the Aged Care Roadmap is based on the removal of service rationing, allowing the market to respond to demand (although the Roadmap still sees government playing a role in thin markets and access by special needs groups). This would be supported by an independent eligibility and needs assessment process and consumer choice of care setting.
Changes to funding and financing arrangements have better positioned the aged care system for achieving a more market-based, consumer driven system, including the introduction of funding following the consumer in home care in February 2017. This reform is the most significant step taken to date towards achieving a more consumer-driven market-based aged care services sector.
Changes to means-testing and fee arrangements in home and residential care have somewhat improved the alignment of charges between those two care settings. However, further alignment in both means-testing and fees policies would be required across home-based and residential care to support a more integrated system with greater flexibility of access and movement across care settings.
Similarly, whilst the Client Contribution Framework in CHSP is consistent with the principles of the fees policies in home and residential care, further thought needs to be given to a more integrated care at home system in the future.
In terms of supply and demand, ACFA observes that there is currently insufficient data available to understand the extent, if any, of unmet demand for subsidised aged care services, and that a better understanding of this and the private market is needed. Monitoring occupancy rates for the different care types as the overall provision ratio is increased and at the same time re-balanced in favour of home care, and monitoring waiting lists through My Aged Care’s national prioritisation process, should shed further light on the level of unmet need and consumer preference.
Chapter 5 Aged care workforce
There were minimal funding and financing reforms directly related to the aged care labour market. Therefore, ACFA’s analysis of workforce issues is necessarily limited.
As such, the report presents a brief discussion related to workforce, focussed primarily on the workforce supplement introduced as part of the reforms and subsequently re-directed into generalised funding. It also brings together ACFA’s observations from recent annual reports and its study on rural, regional and remote providers about wage costs and implications for provider viability.
The 2012-13 Budget included an allocation of $1.2 billion over five years from 2012-13 (including $471.7 million in 2016-17) to address workforce pressures in aged care.
As part of the 2013-14 Budget, the Government redirected the Workforce Supplement into the general pool of aged care funding. The result being:
residential, home care and flexible care providers received an increase in funding of 2.4 per cent in their basic care subsidy from 1 July 2014.
xiv

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
eligible grant programs such as the Commonwealth Home and Community Care Programme received a 2.4 per cent increase in their funding.
eligible regional, rural and remote providers received a 20 per cent increase to Viability Supplement payments from 1 July 2014.
xv

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
1 Introduction
1.1 Background
1.1.1 About the Aged Care Financing Authority
The Aged Care Financing Authority (ACFA) is a statutory committee whose role is to provide independent, transparent advice to the Australian Government on financing and funding issues in the aged care industry. It is led by an independent Chairman, Ms Lynda O’Grady, complemented by eight members with aged care industry expertise.
ACFA examines issues in the context of maintaining viable, accessible and sustainable aged care services that balance the needs of consumers, providers, the workforce, taxpayers, investors and financiers.
Australia’s aged care industry is undergoing a major transition across both residential and home care. Major changes to the industry since 2012 have had a significant impact on the provision of aged care in Australia. Further changes are underway, particularly in home-based care and support, with further changes expected in the coming years.
1.1.2 About the Aged Care Legislated Review
As part of the changes to aged care announced in 2012, an independent review of the reforms was included in the Aged Care (Living Longer Living Better) Act 2013 (the LLLB Act).1 The Review is being led by Mr David Tune AO, PSM.
The Review will look at the impact of the changes to date and where the system needs to be taken in the future.
A written report of the Review must be completed and provided to the Minister by 1 August 2017. A copy of the report must then be tabled in Parliament within 15 sitting days of receipt.
1.1.3 Scope of ACFA’s contribution to the Review
In November 2015, the former Minister for Health and Aged Care asked ACFA to provide advice on funding and financing issues affecting the matters specified in the Review’s terms of reference. In particular, ACFA was asked to focus on such issues as they relate to means testing, fees, accommodation prices, access and workforce.
1 The terms of reference are set out in section 4 of the Aged Care (Living Longer Living Better) Act 2013, which is available at Aged Care (Living Longer Living Better) Act 2013.
16

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
This is consistent with ACFA’s charter, which is to provide advice to the Minister about the funding and financing of aged care services, particularly in relation to the impact of funding and financing arrangements on the viability and sustainability of the aged care sector and ability of care recipients to access quality aged care.
ACFA’s contribution to the Review has focussed on gathering and analysing key data and information that can be used by the Review to assess the impact of the key funding and financing changes in home and residential care. As such, ACFA’s input in this report provides a summary of the funding and financing changes in home and residential care, presents key data to inform assessment of the effectiveness of the funding and financing changes, and presents analysis and discussion of issues and observations arising from that data.
Monitoring of reform impacts
ACFA has already undertaken significant work monitoring the impact of the 2014 financing reforms in the months following implementation. ACFA consulted with peak sector organisations to develop a survey to monitor the impact of the changes to accommodation payments and means-testing. ACFA also analysed administrative data available to the Department of Health (e.g. the number of admissions to residential and home care), and drew upon feedback received through general engagement with the sector.
ACFA provided seven monthly reports to the relevant Minister from July 2014 until March 2015 and four quarterly reports from September 2015 to September 2016.2 This formal monitoring has now ceased.
Related work
Whilst the Review’s terms of reference include an assessment of the effectiveness of arrangements for protecting lump sums, this is not included in this report as ACFA recently completed a separate project examining the bond guarantee scheme.
ACFA also recently completed a separate project about access to care by supported residents, which was published in February 2017, and is referred to in this report.3
Aged care workforce issues
ACFA’s analysis of workforce issues is necessarily limited, as there were few funding and financing changes directly related to the aged care labour market.
As such, this report’s analysis of workforce impacts is focussed primarily on the workforce supplement introduced as part of the reforms and subsequently re-directed into generalised funding. This brief section also brings together ACFA’s observations from recent annual reports and study on rural, regional and remote providers about wage costs and implications for provider viability.
2 Monthly and quarterly monitoring reports are publically available on the Department of Health website at Monthly and quarterly monitoring reports of the ACFA. 3 ACFA’s report on access to care for supported residents is available on the Department of Health website at ACFA's report on access to care for supported residents.
17

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
1.2 Approach
Broadly put, the reforms to funding and financing arrangements aimed to:
increase transparency and consumer choice, for example, through greater choice of how accommodation payments are made and the publication of prices;
improve the viability and sustainability of aged care services, by increasing flexibility, funding and investment, for example, through deregulation of accommodation pricing such as allowing lump sums to be charged for ‘high care’ places and increasing the accommodation supplement for new and significantly refurbished homes; and
improve the long-term sustainability and equity of the aged care system, by increasing consumer contributions from those who can afford to contribute to their aged care costs and improving equity in how different forms of wealth were counted in means testing arrangements.
In assessing how effective the reforms were in achieving these aims, ACFA has taken a ‘360-degree view’, analysing their impacts on:
Consumers – in terms of equity of access to aged care services; Providers – in terms of viability; and Government – in terms of the sustainability of the aged care system.
Insofar as the reforms aimed to improve accessibility to the aged care system for older Australians, this report places particular emphasis on the impact of funding and financing changes, and other related changes, on the elements that influence how easily older Australians can access care. These are:
availability (e.g. supply and mix of aged care services) affordability (e.g. pricing and subsidisation); and choice (e.g. capacity to choose care and services that reflect need and preferences).
Report structure
Part One: Analysis and observations
Part One presents ACFA’s analysis of the effectiveness of the funding and financing aspects of the reforms, in relation to their impacts on access to care, viability and sustainability. Part One also presents ACFA’s observations about the degree to which the funding and financing changes achieved their policy objectives and any possibly unintended consequences or issues that have arisen. Commentary is also made on how the system is currently placed in relation to possible long term reform directions such as those outlined in the Aged Care Sector Committee’s Aged Care Roadmap.4
Part One is divided into five chapters, supported by data in appendices:
Chapter 1: Introduction
4 The Roadmap is the view of the Aged Care Sector Committee (ACSC), a body representing views of key stakeholders in the sector. Whilst it has been welcomed by Government as a guide for future aged care reform considerations, it is not government policy. Nevertheless ACFA considers it useful to consider how the reforms to date fit against the Roadmap’s future direction.
18

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Chapter 2: Means testing, which covers income testing in home care, means testing in residential care, and the alignment of fees across, home and residential care settings;
Chapter 3: Accommodation payments, including accommodation pricing and regulation; Chapter 4: Access to care, which covers the impacts of the financial reforms as well as
broader elements of the aged care system that impact access to care, such as supply and demand (e.g. admissions and occupancy), funding targeted to special needs groups, and elements of consumer-directed care; and
Chapter 5: Workforce issues, which briefly considers funding and financing issues that impact the aged care workforce.
There is some overlap between the chapters, particularly in relation to access to care, where in some instances specific changes to means testing and accommodation payments have implications for access to care as well as financial viability and sustainability.
Part Two: Appendices
Part Two contains the appendices with supporting and additional data.
Information and data
ACFA has drawn upon data already available to the Department of Health and to ACFA, including:
information collected through ACFA’s monitoring surveys; administrative data collected through the Aged Care Entry Record (ACER); provider claims and payments data; care recipients’ means-testing data; and information submitted by providers to the My Aged Care provider portal.
ACFA has not undertaken any new data collection from providers or consumers specifically for the purposes of this report. However, the Department of Health conducted a survey of home care providers’ practices in relation to fees for the purpose of the Review.
As well as providing an analysis of the effectiveness of the key financial reforms, this report also acts as a ‘data-book’ of existing data that can be used by the Review to assess the impact of the funding and financing reforms in relation to the key measures outlined above.
1.2.1 Limitations of this report
It is important to note that this report focuses on the funding and financing aspects of the reforms, particularly as they relate to provider viability, sustainability of the aged care system and to consumer access to aged care services. This report does not examine broader policy or reform issues, such as the quality of care being provided.
There are a number of limitations to this report that should be noted:
ACFA has drawn on previous sector engagement and anecdotal feedback and has not undertaken a public consultation specifically for this report. ACFA notes that public
19

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
consultation was undertaken in October to December 2016 and in February and March 2017 by the Review, and that the Review is undertaking further sector consultation.
this report draws upon data already available to ACFA and the Department of Health. ACFA has not been able to provide detailed analysis in relation to some issues or aspects of the reforms due to lack of data, and in some cases is limited to recounting anecdotal feedback.
limitations and caveats to individual datasets are included in footnotes throughout this report.
the timing of the report means that in some cases data is only available to the end of the 2014-15 financial year. More recent data is presented where possible.
ACFA notes that only a short time has passed since the implementation of the reforms and that the wealth of consumers is likely to change in the coming decades as superannuation matures.
It is important to note that the data in this report often relates to a particular cohort, for example, post-1 July 2014 residents in care on a particular date or pre-1 July 2014 residents in care on a particular date, and therefore may not correspond to other published data, including in other ACFA reports.
1.3 Current funding and pricing framework
Aged care legislation regulates the subsidies and consumer contributions payable for government approved aged care services:
Commonwealth Home Support Program (CHSP): grant-based funding (e.g. for specified activities).
home care: the government pays care subsidies, up to four specified needs-based package levels, reduced by income-tested care fees paid by consumers, and supplements. All consumers also may be asked to pay a basic daily fee and fees for additional services can be agreed between the provider and the consumer.
residential care: the government pays care subsidies, based on assessed need, reduced by means-tested care fees paid by consumers. The government pays a supplement for accommodation for low means residents, reduced by means-tested accommodation contributions paid by residents. Non-low means residents pay a market-based accommodation price agreed with the home, up to the published price. All residents may be asked to pay a basic daily fee for living expenses. Providers and residents can also agree to fees for extra or additional care and services.
Commonwealth Home Support Programme (CHSP)
The CHSP is a grant-funded program. In October 2015 the Government released the Client Contribution Framework, which outlines the principles that providers need to adopt in setting and implementing their own client contribution policy. This is with a view to ensuring that those who can afford to contribute to the cost of their care do so while protecting those who are most vulnerable.
The Client Contribution Framework states that client contributions should not exceed the actual cost of service provision, and should take into account the client’s capacity to pay.
20

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
There is limited data available about the range or extent to which CHSP providers charge client contributions. Further information about the implementation of the Client Contribution Framework is expected to be available later in 2017.
Home care
Table 1.1 below shows the maximum care subsidy government pays for each home care package level and the maximum income-tested care fees consumers can be asked to pay (note that providers and consumers may also agree to fees for additional care and services).
Table 1.1Home care subsidy and consumer contributions, daily/annual amounts (March 2017 rates)
* Consumer contributions for care show maximum income-tested care fees. The income-tested care fee is capped at $14.49 per day for incomes up to $50,455.60 and at $28.98 for incomes over $61,007.78.^ Basic subsidy rates excluding additional supplements. Actual subsidy paid is reduced by amount of assessed income-tested care fee.
21

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Residential care
Table 1.2 shows the maximum residential care and accommodation subsidies government will pay and the levels of resident fees by the different cost components in residential care, namely basic daily living, care and accommodation (note that providers and residents can also agree to fees for extra or additional care and services).
Table 1.2 Residential care subsidies and resident fees, by cost component, daily/annual amounts (March 2017 rates)
Basic daily living Care* Accommodation^
Government subsidy Up to $244.97 /
$89,414.05Up to $55.09 /
$20,107.85
Low means (fully supported) $49.07 / $17,910.55
Low means (partially supported) $49.07 / $17,910.55
Up to $55.09 / $20,107.85 (partly
subsidised)
Non-supported $49.07 / $17,910.55 Up to $244.97 / $26,380.51 (annual cap)
Market-based accommodation price
* Government subsidy person with HHH ACFI classification plus primary supplements. Means-tested care fees subject to annual and lifetime caps on care fees.^ Maximum rate of accommodation supplement for significantly refurbished facility. Maximum accommodation contribution for person in significantly refurbished facility.
For home care and residential care, the level of subsidies to be paid for specified levels of care are set by government. Another way of thinking about this is that specified subsidy levels set a de-facto ‘regulated price’ on care and services.5
Legislation also prescribes the maximum level of contributions consumers can pay.
Consumer contributions to care depend on an income test (home care) or combined income and asset test (residential care).
Contributions to accommodation costs for low means residents are means tested, whilst non-low means residents fund accommodation privately based on market price.
The respective maximum basic daily fees for home and residential care are prescribed by government and paid for by the consumers.
5 Noting that consumers can agree to purchase additional care and services.
22

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2 Income-tested and means-tested care fees and other charges in home and residential care
This chapter presents ACFA’s analysis of and observations about the effectiveness of changes to income testing in home care and means (income and asset) testing in residential care that took effect from 1 July 2014, and an assessment of the effectiveness of the alignment of fees across home-based care and support and residential care.
These are considered in relation to access to care and equity (consumer perspective), principally in terms of how means testing impacts affordability of aged care services for consumers, as well as viability (provider perspective) and sustainability (government perspective).
The chapter also covers other non-accommodation related fees such as basic daily fees and fees for extra and additional services.
The chapter concludes with an assessment of how well the changes to means testing have achieved their objectives, identifies any issues and unintended consequences, and considers where the system now sits in the context of possible future reform directions.
The means testing reforms consisted of:
introducing formalised income testing with subsidy reduction for home care; combining the income and assets test for residential care, including a capped value for
the former principal residence; annual and lifetime caps on income and means-tested care fees in home care and
residential care respectively.
2.1 Overview of funding and fee arrangements in home and residential care
Income testing (home care) and means testing (residential care) determine the level of contributions consumers can be asked to pay toward the cost of their aged care and services.
The funding framework for aged care services sets out a number of categories for private and government contributions to the costs of residential care.
23

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Table 2.1 and Table 2.2 below illustrate the funding categories in home and residential care, according to the following legend:
Yellow shading indicates areas where consumer contributions or fees are paid directly to providers, with no impact for government (e.g. no subsidy reduction applicable).
Blue shading indicates where the care cost component is fully paid by government. Government sets the ‘price’ that providers receive for each package level. Consumers in this area are assessed as not having capacity to contribute to care and/or accommodation costs.
Green shading indicates areas where consumers are assessed as being able to pay some amount toward their care and/or accommodation costs, which reduces the subsidy paid by government.
Grey shading indicates areas where residents are assessed as able to pay the full cost of their accommodation (residential care only).
The price of accommodation in this area is market-based and paid directly to providers.
Table 2.1 below illustrates the funding categories in home care applicable to post-reform home care consumers.
Table 2.1 Home care funding and consumer contributions
Table 2.2 below illustrates the funding categories in residential care applicable to post-reform residents.
Table 2.2 Residential care funding and resident fees
Hotel/daily livingGovernment set amount
CareSet care subsidies (ACFI)
AccommodationSet accommodation supplement
OtherExtra service fee or fee for other care and services
Low means (fully supported)Low means (partially supported)
Basic daily fee Accommodation contribution
Non-low Means-tested care Accommodation
24

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Hotel/daily livingGovernment set amount
CareSet care subsidies (ACFI)
AccommodationSet accommodation supplement
OtherExtra service fee or fee for other care and services
means fee payment
25

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.2 Income testing and fees in home care
2.2.1 Pre-reform home care fee arrangements6
From 1 August 2013, the Community Aged Care Package (CACP) and Extended Aged Care at Home (EACH) and EACH Dementia programs were replaced by a new Home Care Packages Program.
Four levels of Home Care Packages were introduced: Level 1 supports people with basic care needs; Level 2 supports people with low-level care needs; Level 3 supports people with intermediate care needs; and Level 4 supports people with high-level care needs.
Each package level is funded at different amounts paid by the Australian Government to the service provider.
Prior to the 1 July 2014 changes, home care consumers could be charged a fee, set by the provider, that could include a basic amount up to 17.5 per cent of the basic rate of the single aged pension, plus an amount up to the equivalent of 50 per cent of a person’s income above the basic pension.
Providers had discretion to charge lower or no consumer contributions depending on the consumers’ financial circumstances (thereby providing informal financial hardship assistance).
Prior to the reforms, Government paid the full value of the package through subsidies and supplements to the provider. There were no subsidy reductions, and any income-tested fee levied by the provider to the consumer was in addition to the package level funding.
2.2.2 Post-reform home care income-testing and fee arrangements
Under the 1 July 2014 reforms home care consumers can be charged:7
a basic daily fee up to the equivalent of 17.5% of the basic single age pension (currently a maximum of $3,686.50 per annum), at the discretion of the provider.
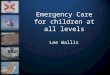
an income-tested care fee if their income is greater than that of a full pensioner, with the consumer’s subsidy reduced by the amount of the fee. Figure 2.1 below shows how this is calculated with full pensioners paying no income-tested care fee with a 50% taper rate then applying above the full pensioner income level.
annual caps, however, limit the income-tested fee with part pensioners paying no more than $5,276.08 per annum and self-funded retirees no more than $10,552.18 per annum. A lifetime cap of $63,313.28 on care fees applies for income-tested care fees in
6 Consumers who started receiving a home care package before 1 July 2014 had their fee arrangements preserved when the 1 July 2014 fee arrangement changes were introduced. These consumers remain under their pre-1 July 2014 fee arrangements unless they leave care for more than 28 days or move to a new home care provider and elect to be covered by the post-1 July 2014 arrangements.7 These fees and caps are indexed.
26

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
home care and means-tested care fees in residential care or the aggregate of both for consumers who change type of care.
any additional amount agreed between the provider and consumer for additional care and services.
Figure 2.1 Home care income thresholds and maximum income-tested care fees, at March 2017
If a basic daily fee is charged, it must be included in the consumer’s care plan and individual budget. Home care providers are also required to provide their consumers with a monthly statement of the available funds and expenditure showing them how their budget is being spent under the package and the balance of remaining funds.
How did this differ to the pre 1 July 2014 arrangements?
The key differences to the pre 1 July 2014 arrangements are that:
the Government’s home care subsidy is reduced by the amount of income-tested care fee that a consumer is assessed as liable to pay; income testing is conducted by the Department of Human Services; and
basic daily and income-tested care fees are now distinct fees.
It was expected that this would see providers almost universally charging the income-tested fee to recover the reduced subsidy. However, a survey of home care providers found this is not the case (see data summary box below).
27

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
In contrast to the income-tested care fee, a subsidy reduction does not apply for any basic daily fee that a provider may choose to charge.
2.2.3 Key home care data8
8 See Chart 5.6 in ACFA’s 2016 annual report for consumer fees as a proportion of home care providers’ revenue sources. Note that consumer fees in this chart include both income-tested fees and basic daily fees.
28
Income-tested care fees payable / Government subsidy reduction:
In 2014-15 $3.2 million of income-tested care fee was payable with an equivalent subsidy reduction – this compares with total government subsidy of $176 million for post-1 July 2014 consumers
In 2015-16 $13.1 million of income-tested care fee was payable with an equivalent subsidy reduction – this compares with total government subsidy of $516 million paid for post-1 July 2014 consumers.
At 30 June 2016, 82 per cent of all post-1 July 2014 home care consumers were assessed as not being able to pay an income-tested care fee (full pensioners). 15 per cent paid an income-tested care fee up to the first cap (part-pensioners), with an average daily amount of $6.30 and 3 per cent paid an income-tested care fee up to the second cap (self-funded retirees), with an average daily amount of $26.80.
A survey of home care providers found:
78 per cent of respondents charge the basic daily fee, however over half of those indicated that they charge less than the maximum amount (i.e. between $0 and $10.10 per day); and
83 per cent of respondents charge the income-tested care fee to post-1 July 2014 consumers.
The maximum basic daily fee that could have been charged in 2015-16 was $3,606.86 per annum. If all consumers were charged the maximum, the total collection would be $218.4 million. The home care survey found that approximately 22 per cent did not charge any basic daily fee and of those that did more than half charged less than the maximum.
There is no data currently available on administration, exit or other amounts charged.

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.3 Analysis and observations: home care income testing and fees
The following sections address the following issues from the perspective of the stakeholders impacted the most:
access to care: efficient marketplace for both providers and consumers;
equity in fee arrangements among consumers;
provider discretion in charging basic daily fees and income-tested care fees; and
sustainability: government funding and provider earning capacity.
2.3.1 Have the fee arrangements affected access to care?
See Chapter 4: Access to Care.
2.3.2 Are the home care fee arrangements equitable?
There are potential equity issues in the fee arrangements for home care.
Same level of basic contribution can be applied to all consumers
First, there is the question of whether it is equitable that consumers can be asked to pay the same level of basic contribution (i.e. the basic daily fee, equivalent to 17.5 per cent of the basic single age pension), regardless of their assessed care needs (i.e. their package level).
(Noting that whilst providers are not required to charge the basic daily fee, the policy assumes the same rate of basic daily fee for all consumers.)
This could be viewed as a minimum consumer payment of $3,686.50 to access the government subsidised home care system.
Purpose and treatment of basic daily fee vs. income-tested care fee
This raises the second, related, issue about the differences in treatment of the basic daily fee compared with the income-tested care fee.
In residential care, there is a clear difference between the purposes of the basic daily fee – which covers the costs of everyday living expenses such as utilities and cleaning – and the means-tested care fee, which is for care and related services only.
In home care there is no explicitly described purpose for the basic daily fee as opposed to the income-tested care fee. It could be viewed as a basic contribution that all consumers are asked to make toward their home care package, or similarly as a standard fee for accessing the home care system.
However, if charged, the basic daily fee must be included in recipients’ individual budget and accounted for under the monthly statement of the available funds and expenditure. As such, it increases the total value of the package and can be used toward consumers’ care costs. Describing the two as distinct fees thereby leads to confusion.
29

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
This confusion is clearly at least partly the result of the introduction of the conceptual distinction between the ‘basic daily fee’ and ‘income-tested care fee’, which was not part of the pre-reform arrangements.
That there are not two clearly distinct purposes for the two fees raises questions about why the care fee is income-tested, attracts a subsidy reduction, and is counted toward the annual and lifetime caps, whereas the basic daily fee is not.
Charges for services in addition to the package amount can add further complexity and confusion to the fee arrangements.
Maximum consumer contributions not linked to care needs
Third, there is the related question of whether total maximum consumer contributions (basic daily fee and income-tested care fee) for lower level packages, particularly Level 1 packages, are too high as a proportion of the overall package value compared with consumer contributions for higher level packages. See Table 2.1 below, which assumes the maximum level of consumer contribution (including the maximum basic daily fee).
Table 2.1 Split of maximum consumer contribution (including basic daily fee) and government subsidy, by home care package level (March 2017 rates)
P: Full pensioner, PP: Part Pensioner, SFR: Self-funded retiree* Consumer contributions for full pensioner limited to basic daily fee. Contributions for part pensioners and self-funded retirees include basic daily fee and income-tested care fee (at annual caps).^ Total package value includes basic home care subsidy rates (excluding supplements) and basic daily fee.
ACFA observes that the relatively high level of consumer contribution for Level 1 packages may be influencing consumers’ decisions to not take up Level 1 packages. Indeed, there is a clear correlation between package level and the proportion of recipients who are part-pensioners and self-funded retirees.
30

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Of post-reform home care consumers receiving a Level 1 package in 2015-16, only 15 per cent were part-pensioners or self-funded retirees.
Of post-reform consumers receiving a Level 4 package in 2015-16, 27 per cent were part-pensioners or self-funded retirees.
This suggests that current fee levels may be sending a price signal resulting in part-pensioners and self-funded retirees in particular seeking services through CHSP, the private market, not at all, or negotiating to receive services to the value of the reduced subsidy, with the difference made through informal care. There is strong anecdotal evidence to suggest that there are consumers receiving ‘packages’ of services through CHSP who will not take up a home care package because they will have to pay significantly more.
The proportion of amounts charged to a package by the provider – e.g. exit amount, amounts for administration and case coordination – may also act as a disincentive to consumers taking up a low level package.
By not linking fees to the level of package, the current arrangements ensure that someone with the capacity to fully pay for a Level 1 package is required to do so or seek services privately. An argument can be made that this is an appropriate outcome. Alternatively some linkage of fees to the level of package could be considered, as was recommended by the Productivity Commission.9
The Review may wish to consider whether it is equitable that consumers can be charged the same maximum level of basic daily fee, which is effectively a minimum consumer contribution for all consumers, regardless of relative levels of income and care needs.
2.3.3 Should providers be required to collect income-tested fees in home care?
ACFA notes that there is a policy question of whether providers should be required to collect basic daily and income-tested care fees from home care recipients.
There is strong anecdotal evidence to suggest that some providers are not collecting, or not collecting the maximum amounts, of basic daily and income-tested care fees. ACFA’s survey of home care providers showed that:
78 per cent of respondents charge the basic daily fee, however over half of those indicated that they charge less than the maximum amount (i.e. between $0 and $10.10 per day).
83 per cent of respondents charge the income-tested care fee to post-1 July 2014 consumers.10
Whether providers actually collect income-tested care fees does not directly impact government expenditure (and overall sustainability from a taxpayer perspective), as the
9 Productivity Commission, Caring for Older Australians, 2012. Available at Productivity Commission, Caring for Older Australians 2012. 10 Further information on and from the survey is in Appendix B.
31

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
package subsidy is reduced by the value of the assessed income-tested care fee regardless of whether it is actually charged to the consumer.
However, it does raise the question of the impact on provider viability and equity in consumer contributions. It also contributes to consumers’ confusion about fees payable.
The fact that providers may not be charging the full income-tested care fee also raises the questions of whether:
providers are absorbing the cost of the subsidy reduction; or
consumers are receiving a lower level of care and services than those for which they have been assessed, or have negotiated to purchase fewer services and avoid paying the income-tested care fee. (ACFA notes that the legislation does not permit providers to reduce the value of a package in this way.)
It is also possible that the financial impact on providers may be lessened by providers charging higher administration, case coordination or exit amounts, or by increasing hourly rates for care and services, thereby reducing the actual care and services to be provided.
This leads to the potential equity issue where some consumers are paying income-tested care fees and basic daily fees and others in similar situations – i.e. with the same financial circumstances and care needs – are not, but are receiving the full package of services.
Moreover, that some consumers appear to be receiving subsidised care and services without making a contribution when they could otherwise afford to do so challenges the principle that consumers are expected to contribute to the costs of their care when they can afford to do so.
ACFA notes that this principle is central to the future viability and sustainability of the aged care system more broadly. Given these considerations, ACFA observes that the Review may wish to consider whether collection of assessed income-tested care fees should be required, or whether consumers should have the discretion to make other arrangements for meeting the balance of their care needs not able to be met under the subsidised portion of the package (e.g. through informal caring arrangements).
2.3.4 Have the fee arrangements improved sustainability?
The amount of income-tested care fees collected, and the amount forecast to be collected, is small in comparison to the amount of subsidies paid. Given the vast majority of home care consumers are pensioners (82 per cent at 30 June 2016), who are not required to contribute any care fee, or part pensioners (15 per cent at 30 June 2016), who can be charged a limited care fee, the income-tested care fees are not providing a significant improvement to fiscal sustainability from a Government perspective.
A significant number of providers are also not maximising their potential fee income by not charging the maximum or in some cases any income-tested care fee or basic daily fee for some consumers. It is unclear, however, what impact these practices have on the level of services provided and profitability, as there is inconsistency and ambiguity as to whether the services are being provided to the value of specified subsidy levels (plus basic daily fee if charged) or to the actual level of funds received from the government and consumer.
32

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.4 Means-testing and fees in residential care
2.4.1 Pre-reform residential means-testing and fee arrangements
Prior to 1 July 2014, two separate tests were applied. A consumer’s contribution to their accommodation costs was based on their assessable assets and a consumer’s contribution to their care costs was based on their income. This resulted in inconsistencies where income-rich, asset-poor consumers paid for care and nothing for accommodation, whilst asset-rich, income-poor consumers paid high accommodation costs but nothing for care.
Consumers could be asked to pay a basic daily fee, an income-tested fee and either an accommodation bond (in low care or an extra service place) or accommodation charge (in high care).11 An income test conducted by the Department of Human Services determined the level of income-tested fee.
2.4.2 Post-reform residential means testing and fee arrangements
The reforms aimed to strengthen means-testing arrangements by combining the income and asset tests to ensure greater consistency in consumer contributions toward accommodation and care costs. The means test is used to determine both a consumer’s eligibility to make certain co-contributions, and the level of co-contribution.
All residential care consumers pay a basic daily fee equivalent to 85 per cent of the basic single age pension (currently a maximum of $17,910.55 per annum). This is intended to contribute to hotel type services such as cleaning, meals and utilities.
Depending on a means test of their assets and income:
some residents will pay no more than the basic daily fee (low means (fully supported) residents in Figure 2.1 below).
Some residents will pay an additional accommodation contribution of an amount determined by the means test (not greater than $55.09 per day) but will not have to pay a means-tested care fee. These are the low means (partially supported) residents in Figure 2.1 below.
some residents will pay an accommodation price agreed with the residential care home and a means-tested care fee determined by the means test. These are the non-low means residents in Figure 2.1 below.
11 All residents entering an extra service place could be asked to pay an accommodation bond and the extra service amount (the sum of the approved extra service fee and 25 per cent of that fee). The additional 25 per cent accounted for the amount of subsidy reduction (often referred to as the extra service ‘clawback’) applied to places with extra service status, equivalent to 25 per cent of the approved extra service fee. The subsidy reduction for extra service places was removed for residents who entered permanent care from 1 July 2014.
33

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Figure 2.1 Residential care assessed income and asset thresholds, March 2017 rates
2.4.3Box 2.1Table 2.1 in section 2.4.3 below shows the number of post-reform residents who fall into each of these fee-paying categories.
How the means test works
Except for the treatment of the former principal residence, all other income and assets, including the value of any refundable accommodation deposit, are fully assessable. The former principal residence is either exempt (if occupied by a protected person) or otherwise capped at $162,087.20 (indexed). While the full market value is not assessed, the capped amount is sufficient to ensure that a person with an unprotected house will not be classified as low means and so will be asked to pay a market-based accommodation price.
The income test taper rate is 50 per cent and the asset test taper rate is 17.5 per cent for assets from $47,500 to $162,087.20 and then 1 per cent up to $391,261.60 and 2 per cent for assets above that amount (as at 20 March 2017).
The means-tested care fee is subject to an annual cap of $26,380.51 and a lifetime cap of $63,313.28 also applies (which also includes any home care income tested fees). The caps are indexed in March and September each year.
Other fees in residential care
34

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
In addition to the above fees, providers can charge:
extra service fees – fees for a defined package of extra services in an approved extra service place with the fee to be approved by the Aged Care Pricing Commissioner.
additional service fees – fees for ‘additional services’ over and above those required to be provided under aged care legislation.
The key differences to the pre 1 July 2014 arrangements are :
the means test assessment (an assessment of income and assets) determines a resident’s contribution to their care and/or accommodation. This replaces a care fee based on income and an accommodation contribution based on assets;
annual and lifetime fee caps on means-tested care fees were introduced; and increased focus on the existing provisions enabling providers to charge additional
amounts for other care and services, with less need for extra service status (i.e. because lump sums can be accepted from all consumers regardless of care level).
35

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.4.3 Key residential fees data12,13
12 It should be noted that subsidy reductions equivalent to means-tested care fees payable will increase over time as the proportion of post-1 July 2014 residents increase and pre-1 July 2014 residents leave care.13 Figures showing provider revenue (e.g. for basic daily fees) in 2014-15 is sourced from Table 7.2 in ACFA’s 2016 annual report.
36
Of all residents in permanent care at 30 June 2016: 18.8 per cent of residents were fully supported 25.8 per cent of residents were partially supported 55.4 per cent of residents were non supported
In 2014-15, provider revenue from basic daily fees was $2,986.3 million. Based on the maximum basic daily fee, residential care providers could charge an estimated $3,142 million in basic daily fees in 2015-16.
The proportion of post-1 July 2014 residents that paid only the basic daily fee on 30 June 2016 was virtually the same as for residents in care on 30 June 2014, at about a quarter of all residents.
The proportion of post-1 July 2014 residents for whom government did not pay any accommodation supplement on 30 June 2016 was the same as for residents in care on 30 June 2014, at around 60 per cent of all residents.
Means-tested care fees payable / government subsidy reduction for post-1 July 2014 residents: In 2014-15 $78.4 million of means-tested care fee was payable with an equivalent
subsidy reduction – this compares with total government subsidy of $1,229 million. In 2015-16 $238.4 million of means-tested care fee was payable with an equivalent
subsidy reduction – this compares with total government subsidy of $3,733 million.
At 30 June 2016 a means-tested care fee was payable by 41,000 post-1 July 2014 residents (44 per cent of post-1 July 2014 residents) with an average amount of $22 per day (compared with average basic subsidy of $156 per day). Approximately 2,000 residents were at that time not paying a means-tested care fee because they had reached the annual cap of $26,380.51 (equivalent to $72.27 per day).
The proportion of post-1 July 2014 residents contributing to their care costs on 30 June 2016 is higher (44 per cent) when compared with residents in care on 30 June 2014 (34 per cent).
At 30 June 2016 approved extra service fees ranged from $1 to $108. The average nationally was $29.72. There were 9,404 residents in an extra service place.
There is no data currently available on additional service fees.

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
below illustrates the profile of post-1 July 2014 residents who were in permanent residential care at 30 June 2016 by low means status and contribution type.
Table 2.1 Permanent post-1 July 2014 residents by contribution type and low means status, as at 30 June 201614
Low means residents Non-low means residentsBa
sic d
aily
fee
(BDF
) on
ly
BDF
+ Ac
com
mod
ation
Co
ntrib
ution
(AC
)
Max
imum
rate
of A
C
BDF,
AC
+ m
eans
-te
sted
car
e fe
e (M
TCF)
*
MTC
F is
capp
ed*
Tota
l15
BDF
+ Ac
com
mod
ation
Pa
ymen
t (A
P)^
BDF,
AP
+ M
TCF
MTC
F is
capp
ed
Tota
l
Post-reform residents 24% 17% 1% 2% 0% 44% 14% 42% 2% 56%
Female residents 21% 16% 1% 2% 0% 39% 14% 46% 2% 61%
Born in Australia 22% 17% 1% 2% 0% 41% 15% 44% 2% 59%
Indigenous Australians 70% 10% 0% 1% 0% 80% 10% 10% 0% 20%
*A resident that is classified as low means on entry to a facility will always be a low means resident in that facility (that is, will never have to pay more than the maximum accommodation supplement that facility is eligible to receive) but may nevertheless be liable to pay a means-tested care fee if their income and/or assets increase sufficiently after they have entered care.
^ A non-low means resident would pay no care fee if their assessable assets and income were equivalent to or less than the applicable threshold or they are otherwise exempt from paying a means-tested care fee under legislation. For example, if a resident’s income was below the income-free area and their only asset was an unprotected former home which had a value greater than the cap, or a resident who had assessable income and/or assets greater than the threshold on entry but whose income and assets subsequently reduced to below the threshold, or for example they have dependent children.
As can be seen in the Table 2.1 above, of the post-1 July 2014 residents in permanent residential care at 30 June 2016, 44 per cent were assessed as low means (including fully and partially supported residents), whilst 56 per cent were non-low means.
14 The proportion of low means residents (44 per cent) in 2.4.3Box 2.1Table 2.1 differs from the proportion of supported residents (46.8 per cent in 2015-16) shown in ACFA’s Report on access to care for supported residents and in section 4.2.4 of this report. This is because the figures for low means residents in 2.4.3Box 2.1Table 2.1 are for post-1 July 2014 residents only, and is at 30 June 2016, whereas the latter figure is for all low means/supported residents in care during the 2015-16 financial year.15 Totals may not add to 100 due to rounding.
37

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
More than half of post-1 July 2014 low means residents were fully supported and paying basic daily fee only.
19 per cent of post-1 July 2014 residents were partially supported and paying an accommodation contribution as well as basic daily fee (two per cent were also paying a means-tested care fee).
About a quarter of post-1 July 2014 non-low means residents (14 per cent of all post-1 July 2014 residents) paid a market-based accommodation payment, but no means-tested care fee.
Three quarters of post-1 July 2014 non-low means residents (42 per cent of all post-reform residents) paid an accommodation payment and a means-tested care fee.
2.5 Analysis and observations: residential means testing and fees
The following sections consider the equity of the new means testing arrangements, including the treatment of the former principal residence, whether they are equitable from consumers’ perspective and the impact on sustainability from the government’s perspective.
2.5.1 Have the changes to residential means testing improved equity in treatment of different forms of wealth?
The funding changes have improved equity in the treatment of different forms of wealth, principally by combining the income and assets tests in residential care. Combining the tests and including the value of the former principal residence up to a capped amount removed the previous inequity where residents made different contributions to their care and accommodation depending on their mix of income and assets.
The subsequent change on 1 January 2016 in the treatment of rental income from the former principal residence under the means test further redressed a previous inequity in the treatment of rental income vis-a-vis other forms of income, the former of which was previously excluded for residents paying some or all of their accommodation by a daily accommodation payment or periodic payment. For residents who have entered care since 1 January 2016, net rental income is included as assessable income regardless of how accommodation is paid for.16
There is some remaining inequity, however, particularly in the treatment of the former principal residence, which is included in the asset test at a capped value of $162,087.20.
There is a question, too, of the interplay of aged care means-testing with age pension eligibility, as this likely affects consumer decision-making and has a bearing on equity considerations. This is particularly the case with the exemption of lump sum accommodation payments from the age pension assets test, which may incentivise some consumers to pay a large lump sum in order to increase their pension entitlement. For example, this might be particularly effective for a person with both a residence and second form of assets, which could otherwise be counted
16 This change was subsequently made for the aged pension income test from 1 January 2017.
38

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
under both the income and assets test, but which could be liquidated to pay a lump sum (whilst the former residence is excluded or capped).
2.5.2 Is the treatment of the former principal residence appropriate?
In addition to combining the income and asset test, the reforms placed a cap on the net value of the former principal residence counted as an assessable asset (where not occupied by a protected person).
Of post-1 July 2014 residents in care on 30 June 2016, approximately 30 per cent own a former principal residence with no protected person. This means that 30 per cent of post-1 July 2014 residents have the net value of their former principal residence included at a capped amount under the aged care means test.
Table 2.1 below shows the proportion of those residents that fall into each of the resident fee paying categories.
Table 2.1 Distribution of post-1 July 2014 residents with unprotected former residence by fee paying status, at 30 June 2016
Fee paying category
Fee paying status of post-1 July 2014
residents with an unprotected
former residenceLow means residentsBasic daily fee only 0%Accommodation contribution 4%
Maximum rate of contribution 1%Means-tested care fee (+ accommodation contribution) 3%
Care fee is capped 0%7%
Non-low means residentsAccommodation payment (no means-tested care fee) 13%
Means-tested care fee (+ accommodation payment) 80%Care fee is capped 4%
93%
See 2.4.3Box 2.1Table 2.1 for an explanation of why a low means resident might pay a means-tested care fee and why a non-low means resident might not.
Of residents with an unprotected former residence, 93 per cent are not low means residents.
13 per cent pay an accommodation payment and basic daily fee, but no means-tested care fee. These are likely to be full pensioners whose former residence is their only asset and who have no other income.
39

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
80 per cent pay an accommodation payment, basic daily fee and a means-tested care fee (either have assets other than former residence and/or income >$26,072.80).
The remaining 7 per cent are low means residents. Some of these residents (e.g. those paying basic daily fee only) would have former residences with net value under the cap. Others (e.g. those paying maximum accommodation contribution and means-tested care fee) were likely the first member of a couple to enter care, whose former residence was therefore initially exempt from the means test, but subsequently lost its protected status.
ACFA notes that the capping of the former principal residence (where not occupied by a protected person) under the combined income and assets test has effectively maintained the pre-1 July 2014 concept that whilst the former principal residence is counted for the purposes of determining a person’s eligibility for assistance with accommodation costs, on its own it would not affect a person’s means-tested care fee.
ACFA notes, however, that the flat cap of $162,087.20 on the value of the former principal residence may be inequitable for residents whose former homes have a lower market value than others. For example, the cap represents 36 per cent of the value of a home worth $450,000, compared with 18 per cent of a home worth $900,000. This differential may be even greater for consumers in rural and regional areas where house prices are generally lower than in metropolitan areas.
Nevertheless, it should be noted that the cap is an effective mechanism in that it does ensure that any consumer with a former principal residence valued above the cap (with no protected person) is required to pay the full cost of their accommodation. They are then required to negotiate an accommodation price with their provider, which may be informed by the value of the former residence. On the other hand it can be argued that preserving the value of the former principal residence at the expense of cost shifting the cost of care to the taxpayer is inequitable.17
The full exemption where a protected person is in the home also can result in a member of a couple with significant housing wealth being treated as a supported resident (subsidised capped accommodation and no means tested care fee) whereas a member of a non-home owning couple with the same wealth will be treated differently and required to pay an accommodation payment and means-tested care fee. It can also result in inequitable treatment compared with a couple who enter residential care at the same time.
2.5.3 Have the means testing reforms contributed to sustainability?
Means testing changes aimed to improve the sustainability of aged care services by increasing contributions from consumers who can afford to contribute to the cost of their aged care, thereby increasing the affordability of government subsidised services.
Changes to the means test – i.e. combining the income and assets tests and capping the value of the former residence – have slightly altered the mix of people receiving government assistance with some or all of their care and/or accommodation costs.18
17 The Productivity Commission discusses this point in Chapter 5 of its report Housing Decisions of Older Australians, pp. 139-140. Available at Productivity Commission report Housing Decisions of Older Australians.
40

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Comparing the fee paying status of residents in care on 30 June 2014, before the reforms commenced, with the fee paying status of post-1 July 2014 residents in care on 30 June 2016 shows that the proportion:
that paid only the basic daily fee was virtually the same for both groups at about a quarter of all residents;
for whom government did not pay any accommodation supplement was the same for both groups at around 60% of all residents;19
that contributed to their care costs was higher for post-1 July 2014 residents in care on 30 June 2016 (44 per cent) than for residents in care immediately before the reforms (34 per cent).
Whilst the proportion of residents contributing to their care costs is higher than for pre-1 July 2014 residents assessed under the previous arrangements, the positive impact on sustainability is limited somewhat as the number of residents paying their full accommodation costs has not increased.
The effect of means-testing changes on the sustainability of residential care can also be assessed by comparing the impact on relative government and consumer contributions when the two different tests (i.e. post-reform means test and the pre-reform income and assets test) are applied to post-1 July 2014 residents.
18 In comparing the fee paying status of pre-1 July and post-1 July 2014 residents, it should be noted that the fee paying categories have changed because of the combination of the income and assets tests. Prior to 1 July 2014, residents could fall into a broader number of fee paying categories, namely:
basic daily fee only; basic daily fee and accommodation contribution; basic daily fee, accommodation contribution and income-tested care fee; basic daily fee and accommodation payment; basic daily fee, accommodation payment and income-tested care fee; and basic daily fee and income-tested care fee.
19 This includes low means residents who are paying the full accommodation contribution.
41

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
That is, if the reforms had not taken place and the pre-reform income and assets test is applied to post 1-July 2014 residents in care during the year ended 30 June 2016 the Government would have borne 68.3 per cent of the cost of the average post 1-July 2014 resident, whereas under the post-reform means test the Government actually only incurred 65.6 per cent of the cost.
The means-testing reforms have therefore improved sustainability by shifting a proportion of the overall average cost per resident per year (including care, accommodation and basic daily living costs) to the consumer.
As might be expected, most of this shift is in relation to care fees:
government care subsidies have reduced as a proportion of the overall average cost20 per resident per year from 59 per cent to 56.6 per cent.
consumer care fees have increased as a proportion of the overall average cost per resident per year from 1.4 per cent to 3.9 per cent.
government accommodation supplements have reduced as a proportion of the overall average cost per resident per year from 8.9 per cent to 8.7 per cent.
consumer contributions toward accommodation have increased as a proportion of the overall average cost per resident per year from 11.7 per cent to 11.9 per cent.
Similarly, means-tested care fees have represented around 6.4% of subsidy payments for post-2014 residents since the new means testing arrangements commenced on 1 July 2014. Under the pre-reform income test, income-tested care fees represented 4.0% of subsidies in 2013-14.
However, it should be noted that the annual and lifetime caps on means-tested care fees (and income-tested care fees in home care) reduce the benefit of the combined means test to government. The cap on the value of the former residence included in the asset test does also limit any benefit from subsidy reductions as a result of means-tested care fees.
2.6 Conclusion
2.6.1 Have the annual and lifetime caps been effective?
ACFA notes that the effect of annual and lifetime caps on care fees cannot be fully assessed, as insufficient time has elapsed since the caps were introduced.
In home care, the annual caps are applied daily, which means that in effect any part pensioners or self-funded retirees paying the maximum income-tested care fee per day ($14.49 and $28.98 respectively) will reach the annual cap.
20 Overall cost includes care, accommodation and basic daily living cost components.
42

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
At 30 June 2016, of all home care package recipients, 17.9 per cent were assessed to be paying an income-tested care fee, of which 2.4 per cent were reaching the first cap and 1.1 per cent were reaching the second cap.
In residential care, an estimated 0.8 per cent of all post-1 July 2014 residents (1.4 per cent of post-1 July 2014 non-low means residents) had reached the annual cap at 30 June 2015, compared with two per cent of post-reform residents (3.6 per cent of post-reform, non-low means residents) at 30 June 2016.
No aged care recipients had reached the lifetime caps at 30 June 2016, as insufficient time had elapsed to enable anyone to reach the lifetime cap, though over time this will change.
In residential care, those benefiting from the annual cap are residents with higher levels of wealth. For example:
A residential care recipient would need to be paying a means-tested care fee of at least $72.30 per day for each day of the year to meet the current annual cap ($26,380.51/365 = $72.27).
The care recipient would need to have assessed assets of more than $1.61 million (and less than $26,072.80 assessed annual income) or assessed annual income of at least $118,812.72 (and less than $47,500 of assessed assets) (or some other combination of income and assets less than these upper limits) to have a daily means-tested care fee of $72.30.
It would take approximately 2.4 years for a person paying a means-tested care fee of $72.27 per day to reach the lifetime cap (although this could take less time if a person had also paid an income-tested care fee in home care).
It is estimated that in around 10 years after the reforms commenced, once all pre-reform residents have left care:
Approximately 5% to 6% of permanent residents will have their means-tested care fee reduced by either the annual or lifetime cap each year;
Most of these (around 4% to 5%) will have reached the lifetime cap.
It is estimated that by this time, the annual and lifetime caps are projected to reduce means-tested care fees by around $0.3 billion per annum, with the annual cap accounting for just over a third of the reduction.21
There remains a question about the equity of the annual and lifetime caps, as they limit the amount that wealthier consumers contribute to their care costs, after which government effectively subsidises the full cost of care for those people.
As the average basic subsidy (i.e. ACFI) for post-1 July 2014 permanent residents is around $156 per day, the annual cap – worked out as a daily amount of $72.27 – limits consumer contributions to around 46 per cent, which is then reduced to zero once the lifetime cap is reached and government fully subsidises the cost of care.
21 Based on income, length of stay, and ACFI level data for current residents and is likely an underestimate of the full impact as: It does not account for the impact on the lifetime cap of residents’ previous home care or respite care fees, No indexation has been applied, dollar amounts are in 2015-16 dollars, and No activity or frailty growth has been applied.
43

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.6.2 Are fees across CHSP, home care and residential care effectively aligned?
The range of services provided within each of the three aged care service types are illustrated in Appendix D.
Whilst the finance and funding changes have improved the alignment of fee arrangements between home and residential care by extending a formalised income-tested care fee to home care packages, the broader alignment of means-testing and fee arrangements between home-based care and residential care is still relatively limited.
For example, whilst care fees in residential care reflect a person’s income and assets, and in some cases can also be capped by care needs, in home care they are only based on income and do not reflect a person’s care needs.
The principles of the Client Contribution Framework (CCF) for the CHSP are consistent with fees policies for home and residential care.22 The CCF:
expects that those who can afford to contribute to the cost of their care will do so whilst providing safeguards for those consumers with limited financial means;
aims to move towards national fairness and consistency in client contributions and to improve the sustainability of CHSP over time; and
expects that, whilst there is no formal means-testing, CHSP providers’ client contribution policies should take into account a clients’ capacity to pay and include arrangements for financial hardship.
However, these principles are not applied uniformly across CHSP.
This raises the broader question of whether fee policies for the respective programs should or could be better integrated. This is not a straightforward or easy question as the types and amounts of care provided range from very small amounts such as Meals on Wheels to very high needs in residential care and some home care packages.
The costs of delivering care in a home setting are also different to those in a residential setting, including the extent of the care provided for people with similar assessed care needs. These factors imply that some differences between fees in different programmes may be appropriate, though there is also a case for exploring the policy basis for the current differences to see whether there is scope to achieve greater integration, consistency and equity in contributions.
The extent to which fees are impacting consumer choice of care types is likely to be clearer in the home and CHSP interactions where some services are interchangeable. Fees are less likely to be driving choice between home care and residential care as entry to residential care is more driven by need than choice, although residential care and higher level packages are considered
22 The CCF was introduced from 1 July 2015 and established a principles-based approach for providers when setting and implementing their own client contribution policy. There is a National Guide to the CCF, intended to help providers with the establishment of client contribution arrangements that align to the CCF. The Guide states that “there is no ‘one size fits all’ approach to client contribution arrangements across the CHSP and providers can flexibly implement the Framework to best meet their clients’ and their organisational needs.”
44

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
equal alternatives by some consumers, especially as more Level 4 packages become available in response to demand.
Table 2.1 Minimum and maximum fees in home-based care and support and residential care (March 2017 rates)
CHSP Home care Residential care
Minimum $0 $10.10 $49.07
Maximum Provider discretion23 $38.98* $349.13^
* Sum of basic daily fee and maximum income-tested care fee.^ Sum of basic daily fee, maximum means-tested care fee (person with HHH ACFI classification plus primary supplements) and an amount equivalent to a maximum accommodation contribution. Means-tested care fee subject to annual and lifetime caps. Accommodation component may be more if price negotiated directly with provider.
ACFA notes that there is limited data available about the range or extent to which CHSP providers charge client contributions. Whilst further information about the implementation of the CCF is expected to be available later in 2017 – including information about the range of client contributions that consumers can expect to pay for different service types in each state and territory – this was unavailable at the time of publication of this report. However it is expected to be available in time to inform the Review.
The data could also inform any future thinking about fees policies in CHSP and the interaction with home care. ACFA observes that options for future reforms in funding and financing will require further analysis and policy development in relation to these alignment issues (including where it may and may not be appropriate) as well as equity considerations.
23 The CCF states that client contributions should not exceed the actual cost of service provision, and should take into account the client’s capacity to pay.
45

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
2.6.3 Have the policy objectives been achieved?
The changes to means testing aimed to: improve equity in the treatment of income and assets; introduce greater consistency in fee arrangements and improve equity in consumer
contributions; improve sustainability by ensuring those who can afford to contribute to the cost of
their care and accommodation; and maintain protection for residents with low means.
ACFA observes that whilst progress has been made in achieving these objectives, aspects of the changes to means testing have not been as effective as they could be, noting that in many cases the reforms that were implemented did not go as far as the Productivity Commission’s recommendations. This is principally the case with regard to improving the sustainability of the
46
Have the changes to means-testing in home and residential care met their policy objectives?
Consumer perspective:
Home care Lower level packages are not attractive, especially to consumers with greater wealth who
would contribute more. There is greater demand for higher level packages, where annual caps on consumer
contributions mean consumers receive comparatively greater value. Confusion about purpose of basic daily fee; perception that fee is too high, especially for
lower level packages. Inconsistent charging of the income-tested care fee and the basic daily fee raises equity
issues.
Residential care Equity in treatment of different forms of wealth has improved, although treatment of former
residence may benefit homeowners over non-homeowners. No impact on access to care for consumers with low means.
Provider perspective:
Some providers are not charging the full basic daily fee and/or full income-tested care fee.
Government perspective
Home care Home care subsidy reductions has not resulted in expected savings, as majority of home care
consumers do not pay any income-tested care fee.Residential care Government share of care costs has reduced marginally, compared with pre-1 July 2014
arrangements

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
aged care system overall, where the changes to means testing and consumer contributions have not resulted in the subsidy reductions expected.
The combination of the income and assets test in residential care has improved equity in the treatment of income and assets and resulting consumer contributions, eliminating the previous situation where people with assets but no income paid for accommodation but nothing for care and those with income but limited assets paid for care costs and not accommodation. The effect of combining the income and assets tests, including the capped value of the former principal residence, ensures that income and assets are treated relatively equally when determining whether someone has sufficient means to be asked to pay the full costs of their accommodation, and thereafter whether they can make a contribution to their care costs. Although, capping the value of the former principle residence benefits homeowners over non-homeowners.
However, the formalisation of income-testing and fee arrangements in home care and associated subsidy reductions have been less successful in improving equity in consumer contributions, or making it easier for consumers to understand and compare fees or improving sustainability. Also, because not all providers are charging allowable fees, different consumers with the same income are paying different fees in some cases. This may be impairing the desired competitive market transition of the industry.
2.6.4 Are there any unintended consequences?
Home care packagesThe limited take-up of Level 1 packages by part-pensioners and self-funded retirees is likely to be at least in part a reflection of the high fees as a proportion of a Level 1 package and the potentially lower fees for similar services available through CHSP.There is anecdotal evidence to suggest that some consumers are not receiving from their provider care and services to the level for which they have been assessed. ACFA does not have any evidence to indicate the extent to which consumers may not be receiving the full package of services. ACFA does note, however, that it may be some consumers’ preference to accept a lower level of services in exchange for either not paying or paying lower than the maximum home care fees and potentially relying instead on informal care arrangements.
Extra Service status
It is likely that the reforms have had some bearing on the ongoing decline (12 per cent in 2014-15 and 23 per cent in 2015-16) in the number of active extra service places. The changes to accommodation payments reduced the need for providers to have extra service status:
lump sums can be accepted from residents regardless of their level of care (whereas accommodation bonds were previously restricted to residents in a low care place or a high care place with extra service status)
market-based prices set by providers apply to all new non-supported residents, thereby allowing additional revenue without needing extra service status
there was a significant increase in the accommodation supplement for residents of new and significantly refurbished homes.
47

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As well, more non-extra service homes are now offering packages of additional care and services for additional fees that apply for the duration of a resident’s stay in the home, similar to what occurs in extra service homes.
This appears to have led some providers to reconsider their extra service status, with some providers either charging for additional care and services or simply increasing their base service offerings (i.e. by building the cost of additional services into the accommodation price). This has the advantage of maintaining their revenue streams while simplifying administration.
ACFA also notes the preference of some providers to maintain regulated extra service status places.
Fees for ‘other care and services’
Whilst providers were permitted to charge fees for other care and services prior to 1 July 2014, there has always been uncertainty about the rules and scope of such fees when compared with the services that are required to be provided under aged care legislation. As a result, the take up of fees for additional services in non-extra service homes prior to July 2014 was limited.
ACFA notes that there has been an increased incidence of fees for additional services since the reforms, partly in response to the removal of retention amounts. The Department of Health issued advice on 2 September 2016 stating that: “providers are not able to charge additional services fees for services or activities that are part of the normal operation of an aged care home, or are required to be delivered as part of a provider’s responsibilities. Fees for ‘other care or services’ can also not be charged unless the resident receives a direct benefit or has the capacity to take up or make use of the services”.
The role and nature of such fees will likely be an ongoing issue with providers looking for options to target different revenue streams, particularly when funding constraints exist in other parts of the system.
The increased incidence of these fees may be impacting affordability of residential care for consumers, particularly those with low means.
There is no data available to allow ACFA to analyse the extent to which providers may be charging additional fees for other care and services or the extent to which consumers are being impacted.
2.6.5 Possible future reform directions
The role and level of consumer contributions in the aged care system will be a key question for future reform. The Aged Care Sector’s Committee’s Roadmap envisages a greater role for consumer contributions in return for greater consumer choice and control and competition in the provision of services.
Having regard to the affordability of a consumer-driven market-based system, the Roadmap suggests that:
all income and assets should be means-tested and treated equally; new financial products (e.g. home equity release) will need to be available; fee arrangements across home care and CHSP should be integrated; and
48

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
consumer subsidies should be aligned across care settings for consumers with the same care needs.
49

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
3 Accommodation payments in residential care
This chapter presents ACFA’s analysis and observations about the effectiveness of changes to accommodation payments, including the effectiveness of the regulation of accommodation prices. These are considered in relation to access to care (consumer perspective), principally in terms of how the new arrangements impact affordability and choice of residential aged care accommodation for consumers, viability (provider perspective) and sustainability (government perspective).
The chapter concludes with an assessment of how well the changes to accommodation payments and associated regulatory measures achieved their objectives, identifies any unintended consequences, and considers how well we are now placed in relation to possible future reform directions.
Supporting data is in Appendix C of Part Two of this report.
3.1 Accommodation payments in residential care
3.1.1 Reforms to accommodation payments
The accommodation payment reforms consisted of:
significant deregulation of accommodation pricing, with previous restrictions such as the types and amounts of payments for high care residents removed;
consumer choice measures such as full consumer choice over accommodation payment type (lump sum or periodic) with the relationship between the lump sum and periodic payment price made ‘equivalent’ by using a standard conversion factor (the maximum permissible interest rate);
consumer protection and competition measures such as requiring publication of accommodation prices on My Aged Care and elsewhere and the introduction of the Aged Care Pricing Commissioner to approve prices over a threshold;
50

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
removing the ability for providers to deduct retention amounts from lump sum payments; and
an increase in the accommodation supplement paid by Government for supported residents in new or significantly refurbished homes.
The reforms to aged care introduced a single accommodation payment system for permanent residential care, regardless of whether residents enter with low or high care needs.
The significant deregulation of accommodation prices as a result of the reforms contrasts with the pricing arrangements that apply for activities of daily living and for personal and nursing care. Prices for the latter continue to be set by government, though there is scope for providers to charge fees with the agreement of the resident for any services that are additional to those specified in legislation.
Resident choice of payment
In conjunction with the removal of the distinction between high and low care places and allowing lump sums to be charged in all places, all permanent residents were given the choice of paying for their accommodation through a refundable lump sum deposit, a rental-style daily payment, or a combination of the two. Refundable deposit balances are fully refundable, less any deductions agreed by the resident. Daily payments are not refundable.
The requirement to leave consumers with the minimum permissible asset value24 after paying a lump sum was maintained. Retention amounts were abolished.
Residents were given 28 days after entry before being required to disclose their preferred payment method, i.e. whether to pay a lump sum or daily payment. Daily payments are paid by default until a lump sum is paid (if any).
Financial equivalence
Financial equivalence between refundable deposits and daily payments was ensured by adapting the pre-reform formula used for determining periodic payments. The MPIR25 was adopted as the interest rate to be used when converting a lump sum deposit into an equivalent daily payment. Prior to the reforms, providers could opt to use a lower interest rate, effectively lowering or ‘discounting’ the periodic payment.
Additional consumer protections
As well as moving to a less regulated accommodation pricing system, the reforms introduced several new measures to improve transparency and protect consumers:
a maximum accommodation payment set by the Minister; appointment of an Aged Care Pricing Commissioner (the Pricing Commissioner); requirement for approval by the Pricing Commissioner of accommodation prices above
the maximum payment set by the Minister;
24 At 1 July 2014 the minimum permissible asset value was $45,000.25 The MPIR is also the rate used to determine the amount of interest to be paid by providers on overdue refund of lump sum accommodation payments.
51

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
requirement to publish accommodation prices on the My Aged Care website and elsewhere.
These additional measures primarily protect non-supported residents paying a market-based accommodation price in a supply constrained environment.
52

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
3.1.2 Key accommodation payments data26
26 Figures shown for payments toward accommodation with equivalent subsidy reduction include an amount equal to the accommodation supplement for non-supported residents as a proxy for the reduction in or avoidance of accommodation supplement for those residents. The latter pay a market-based accommodation payment to the provider, the actual amounts of which are not reflected in these figures.
53
Around three quarters of advertised accommodation prices range between $250,001 and $550,000. The highest concentration (20 per cent) of published accommodation prices is in the $300,001 to $350,000 price band. Six per cent range from $550,001 to over $1 million, whilst 17 per cent of prices are $250,000 or below.
24 per cent of post-1 July 2014 residents are fully supported residents (who do not contribute to their accommodation costs) while 19 per cent are partially supported residents paying an accommodation contribution. Non-supported residents paying a market-based accommodation price represent 56 per cent of post-1 July 2014 residents.
Payments toward accommodation with equivalent reduction in accommodation supplement for post-1 July 2014 residents:
In 2014-15 $152.4 million payable for accommodation by residents with equivalent reduction in accommodation supplement – this compares with total accommodation supplement of $109.5 million.
In 2015-16 $482.8 million payable for accommodation by residents with equivalent reduction in accommodation supplement – this compares with total accommodation supplement of $323.2 million.
In 2015-16 the average accommodation contribution paid by partially supported residents was $13.01, compared with $11.95 for 2014-15.
Lump sum refundable deposits are the preferred payment type for non-low means residents, with over 50 per cent of residents paying by refundable deposit in 2015-16, compared with 22 per cent paying by daily payments and just over 26 per cent paying a combination of both.
In 2015-16, the total pool of lump sums (including both accommodation bonds and refundable deposits) held by approved providers increased to $21.73 billion, up from $15.61 billion in 2013-14.
In 2014-15, provider revenue from resident accommodation payments was $680.7 million (including contributions from partially supported residents and daily payments from non-supported residents who did not pay full lump sums).Total building activity estimated at $4.7 billion in 2015-16, up from $3.8 billion in 2014-15.
At 30 September 2016, an estimated 28.4 per cent of all residential services were eligible or potentially eligible for the higher rate of accommodation supplement of $55.09 (March 2017 rates). This includes significantly refurbished services (23.6 per cent of all services) and newly built services (4.8 per cent of all services).

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
3.2 Analysis and observations
3.2.1 How are consumers exercising choice?
Prior to the reforms, accommodation bonds were the default form of payment for residents in low care and extra service places, although residents were able to negotiate with their provider to pay the bond by periodic payments or a combination of bond and periodic payments.
The impact of residents’ capacity to choose their method of payment – whether a lump sum refundable deposit, daily payments or a combination of both – was a key industry concern in the lead up to the accommodation payment changes. Providers were particularly concerned about the impact on their viability – e.g. the capacity to replace outgoing lump sums – and capacity for investment.
From 1 July 2014 until December 2015, refundable deposits and refundable contributions were the preferred method of payment, with over 40 per cent of residents who pay the full or partial costs of their accommodation choosing this method. This has remained relatively consistent over time, as below demonstrates.
Chart 3.1 Resident choice of accommodation payment, July 2014 to December 2015
Source: ACFA monitoring surveys
However, a different picture emerges when looking at the payment preferences of non-supported residents paying a market-based accommodation prices compared with partially supported residents paying an accommodation contribution.
Data from the Survey of Aged Care Homes (SACH) for 2015-16 (Chart 3.2 below) indicates that refundable deposits are the most common method of payment for non-supported residents, whilst the opposite is true for partially supported residents, who overwhelmingly pay by daily
54

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
contributions.27 For both groups of residents a combination of both lump sum and daily amounts is the second preferred payment method.
Chart 3.2: Resident choice of payment type, 2015-16
Source: Survey of Aged Care Homes 2015-16
Chart 3.2 shows that refundable deposits were the dominant method of payment for non-supported residents in 2015-16, with nearly 52 per cent of non-supported residents paying by lump sum, 22 per cent paying by daily payments and just over 26 per cent paying a combination of a partial refundable deposit and daily payments.
A significant majority (just over 80 per cent) of partially supported residents pay daily contributions only, with nearly 16 per cent paying by a combination of refundable contribution and daily contributions.
It should be noted that the proportion of residents paying by lump sum in Chart 3.2 above may include residents who had previously paid full or partial daily payments, and then paid a lump sum. Similarly, residents paying a daily payment may subsequently pay a lump sum (e.g. once their house is sold).
3.2.2 Is there increased diversity in accommodation prices?
The introduction of accommodation price publishing was designed to provide transparency and competitive market-based pricing rather than pricing based on median house prices or an individual’s wealth. Prices should therefore reflect the diversity of quality and amenity of the accommodation on offer.
27 It should be noted, however, that partially supported residents are advised of their accommodation contribution amounts by the Department of Human Services (based on the person’s means test) as a daily contribution amount. As such, daily contributions could be seen as a ‘default’ form of payment.
55

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Accommodation prices under the reformed accommodation payment arrangements are reasonably diverse. Around three quarters of accommodation prices range between $250,001 and $550,000. The highest concentration of published accommodation prices is in the $300,001 to $350,000 price band (20 per cent). Six per cent range from $550,001 to over $1 million, whilst 17 per cent of prices are $250,000 or below.
Chart 3.1: Spread of published accommodation prices at 1 February 2017
$-
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
$700,000
$800,000
$900,000
$1,000,000 0
200
400
600
800
1000
1200
Published price point
Freq
uenc
y
For-profit services have the most diverse range of accommodation prices, followed by not-for-profit and then government services (see Chart 3.2 in section 3.4 of Appendix C). Services in major cities offer accommodation across the greatest range of price bands, with a greater proportion of services with prices in the higher price bands compared with services in regional and remote areas. Services in regional and remote services offer accommodation across fewer price bands, with a higher proportion of services offering accommodation in the lower price bands.
3.2.3 Have changes to accommodation payments impacted access to care?
There is no evidence to suggest that the changes to accommodation payments have impacted access to care.
Average accommodation prices have increased when compared with the average price of new accommodation bonds prior to 1 July 2014. The average accommodation bond agreed with a new resident in 2013–14 was $296,404, an increase of around eight per cent over 2012-13. The average agreed accommodation price in the September quarter of 2014 (the first quarter after the accommodation payments changes) was $336,000, an increase of around 13 per cent when compared with new bonds in 2013-14 (part of which is most likely in response to the abolition of retention amounts).
56

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
However, although this allows an indicative comparison, changes to the accommodation payment arrangements (e.g. removal of retention amounts) and different data sources mean that these cannot be compared on a like-for-like basis.
Average agreed accommodation prices have gradually increased, from $336,000 in the September quarter 2014 to $377,000 in the December quarter in 2016. On commencement of the reforms, the average published price was around $350,000, which has also gradually increased to $391,000 at 1 February 2017. However, in general, average agreed prices are lower than average published accommodation prices, suggesting that consumers may be negotiating with providers (noting that published prices are the maximum that can be charged). Similarly, providers may be publishing higher prices as a default (as suggested by the cluster of prices published at the $550,000 threshold) to give them flexibility.
Chart 3.1 below shows the average accommodation prices published on the My Aged Care website from July 2014 to February 2017.
Chart 3.1: Average published accommodation prices July 2014 to February 2017
There is a range of accommodation available at different price points, with different options (e.g. private ensuite vs. shared bathroom) influencing advertised prices. This suggests that there is accommodation available for individuals with differing means and preferences, although accommodation for low means residents may be more available in some areas than others and consumer choice may be constrained by supply controls. Sixty-eight per cent of published accommodation prices are equal to or less than $400,000, whilst only seven per cent of published prices are greater than $550,000.
Access to residential accommodation is safeguarded for consumers with low means through the availability of accommodation supplements which, depending on a person’s means, meet all or part of an eligible consumer’s accommodation costs. Access is further safeguarded by discounting the value of the accommodation supplement for those services whose resident profile has fewer than 40 per cent low means residents.
The introduction of choice of payment from 1 July 2014 has provided flexibility for residents in how they pay for their accommodation, with a choice of lump sum, daily payment or a
57

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
combination of the two. Furthermore, if the resident chooses to pay by a combination of lump sum and daily payment, they can choose to draw the daily payment down from the lump sum, providing even greater flexibility and opportunity to access accommodation. However, ACFA understands that choice of payment is not always beneficially available to the resident, with some residents receiving misleading information about their options in this regard or being required to pay in a particular way.
3.2.4 Is the maximum accommodation payment an effective mechanism for regulating accommodation prices?
How has the maximum accommodation payment impacted market prices?
The maximum accommodation payment has had some influence on the way that providers set accommodation prices. The application process requires providers to justify the proposed prices in relation to the quality and amenity of accommodation and value for prospective residents. As the Pricing Commissioner puts it, “the process of making an application requires that providers apply logic to internal pricing structures: to rooms priced above the $550,000 threshold relative to each other, but also to rooms priced above this threshold relative to other rooms in the facility.”28
While the application process leads providers to consider their pricing in a structured way, which along with the publication of accommodation prices may place downward pressure on accommodation prices, the maximum accommodation payment does effectively place an upper threshold on accommodation prices. This is demonstrated by the cluster (about 8 per cent) of accommodation prices published on My Aged Care at $550,000, although there may be several factors at play (e.g. providers may use the maximum as a default price point from which they negotiate down).
Providers appear to be pricing their accommodation appropriately, given that around 87 per cent of applications to the Pricing Commissioner were approved in the first instance, with around 13 per cent withdrawn or substantially re-framed.29
Moreover, it does not appear that the maximum payment amount has adversely impacted lending practices or investment. The Pricing Commissioner has received feedback that lending institutions are often not requiring pre-approvals (i.e. approvals given prior to the completion date for the construction of a new facility, subject to verification).
Does the maximum accommodation payment protect consumers?
A maximum accommodation payment limits the amount that providers can charge for accommodation, unless they seek approval from the Pricing Commissioner and demonstrate that the accommodation price would give value to prospective residents. This ensures that, in an environment where services are rationed, higher accommodation prices reflect the standard of accommodation rather than simply a prospective resident’s capacity to pay.
28 Source: the office of the Aged Care Pricing Commissioner.29 Source: the office of the Aged Care Pricing Commissioner.
58

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
No applications have been refused to date. This reflects the approach taken by the Pricing Commissioner to work with providers to reframe and re-submit applications.
Whilst Pricing Commissioner approval may appear to predominantly protect consumers with higher wealth who can afford to pay an accommodation payment above a refundable deposit of $550,000, the cluster of accommodation prices published at that threshold point does suggest that some providers may have increased their published prices if they were not required to seek approval from the Pricing Commissioner.
3.2.5 Have the changes to accommodation payments improved viability and investment?
The impact of changes to accommodation payments on service viability and investment may be evaluated by considering the level of government funding of accommodation for residents with low means, changes in the pool of lump sum accommodation payments, and changes in building activity.
Accommodation supplement
A comparison of government funding for accommodation for low means residents with the average accommodation prices agreed between non-supported residents and providers since 1 July 2014 shows that the higher accommodation supplement30 of $55.09 paid by government on behalf of supported residents living in homes that are new or significantly refurbished is broadly in line with the average prices paid by non-supported residents.
the overall average agreed accommodation payment of $350,000 RAD (equivalent DAP of $55.23) is broadly equivalent to the higher rate of supplement of $55.09 per day ($349,095 lump sum equivalent).31
approximately 51% of agreed accommodation payments were less than the higher accommodation supplement.
in comparison, approximately 19% of agreed accommodation payments were less than the standard rate of accommodation supplement of $35.90 ($227,491 lump sum equivalent).
This indicates that, on average, the accommodation price the government has set for supported residents is reasonable for generating investment in accommodation. In general, however, market-based published prices for accommodation are higher than government subsidy for accommodation.
30 The higher maximum rate of Accommodation Supplement of $55.09 applies if a service is significantly refurbished or newly built and has more than 40 per cent low means, supported, concessional and assisted residents. The standard maximum rate of $35.90 applies to services that meet specified building standards, but which are not newly built or have not been significantly refurbished.31 This data is indicative only. Agreed accommodation prices are reported by aged care homes through the Aged Care Entry Record (ACER). The ACER must be completed within 28 days of a resident’s entry to permanent residential care. In some instances the provider may complete the ACER before the resident has elected their payment method. The ACER is also completed for supported residents. This means that the data may include prices agreed with supported residents prior to their fee advice letter (and subsequently unpaid).
59

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As at 30 September 2016, an estimated 757 services (28 per cent of all services) were eligible or potentially32 eligible for the higher accommodation supplement.33 This includes 630 services eligible or potentially eligible for significant refurbishment (24 per cent of existing services), and 127 for newly built services (five per cent of existing services).
The estimated completed refurbishment spend per service averages $3.9 million, with a median of $1.7 million and total estimated expenditure of $2.45 billion across the sector.
Lump sum accommodation payments
The overall pool of lump sums has steadily increased since 1 July 2014.
In 2015-16, the total pool of lump sums (including both accommodation bonds and refundable deposits) held by approved providers increased to $21.73 billion, up from $15.61 billion in 2013-14 (Chart 3.1 below).
Chart 3.1: Total pool of lump sums held, 2011-12 to 2015-1634
Source: Annual Prudential Compliance Statements
It is likely that this increase in the lump sum pool held by providers has been driven by three factors:
the larger potential pool of lump sums – an intended outcome of the accommodation payment reforms and removal of the distinction between high and low care;
32 Figures are based on the total number of significantly refurbished services for which standard and conformation of pre-approval applications have been received (excluding withdrawn, incomplete and newly built). ‘Potentially’ includes applications that were not initially successful but may be approved upon review including through the Administrative Appeals Tribunal.33 Based on count of 2,669 operational services nationally at 30 June 2016. Source: Stocktake of Australian Government Subsidised Aged Care Places as at 30 June 2016.34 The figure of $18.2 billion presented for 2014-15 in 3.2.5Box 3.1Chart 3.1 differs from the June 2015 figure of $19.84 billion in Table 3.1 of ACFA’s 2016 annual report because the latter figure from the monitoring surveys includes lump sums held and receivable, whereas figures in 3.2.5Box 3.1Chart 3.1 are sourced from the Annual Prudential Compliance Statement returns of those providers who submitted their GPFRs, and do not include lump sums receivable.
60

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
apparent preference of many non-supported residents to pay for their accommodation by lump sum refundable deposit over daily payments; and
increase in average value of accommodation payments compared with the value of average new accommodation bonds prior to the reforms.
Building activity
Building activity has generally increased since the reforms commenced, suggesting that investors are responding positively to the reforms. The 2016 Survey of Aged Care Homes (SACH) estimates total building activity to the value of $4.7 billion in 2015-16, compared with $3.8 billion in 2014-15 and $3.1 billion in 2013-14. This includes new building, rebuilding and upgrading work both completed during the year and in progress at the end of the year.
Chart 3.2: Residential aged care building activity, 2013-14 to 2015-16
2013–14 2014–15 2015–16$ m
$500 m
$1,000 m
$1,500 m
$2,000 m
$2,500 m
$3,000 m
$3,500 m
$4,000 m
$4,500 m
$5,000 m
New Building Work Rebuilding Work Upgrading Work
It is not possible to determine the extent to which investment and building activity has been driven by increased flexibility to charge lump sums as opposed to the increase in the maximum accommodation supplement.
3.2.6 Is the MPIR appropriate as the rate to be used in calculating equivalence between lump sums and daily amounts?
61

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
ACFA notes that lump sums – including accommodation bonds, refundable deposits and refundable contributions – are an important source of providers’ capital financing and constitute a substantial portion of liabilities in providers’ balance sheets. Under current policy settings, lump sums are the cornerstone of capital financing for residential aged care and the sustainability of the residential sector.
For providers, the key consideration is whether the MPIR results in a daily payment that is sufficient to cover the weighted average cost of capital (WACC), or put another way, to compensate the provider for not receiving capital financing through a lump sum. The WACC will vary for different providers depending on their mix of debt and equity funding. If a development is completely debt-funded, a provider’s cost of debt is likely to be close to the MPIR. If there is significant equity funding a provider’s WACC would likely be greater than the MPIR.
Another consideration is the potential for movement from lump sums to daily payments if the MPIR is set too low. If consumers were to be able to achieve a better return than the MPIR, they may be inclined to invest the lump sum and pay the daily payment out of investment earnings. Given a provider’s higher WACC, the lower daily payment cash flow may not be sufficient to borrow against to replace the lump sum.
Some providers argue that they should be able to set their own policy on the conversion between lump sums and daily payments more broadly (e.g. setting lump sum and daily amounts independently of one another). This may have some benefits for consumers, for example, ‘discounting’ daily payments but would effectively unwind the precise equivalency achieved by MPIR conversion. Anecdotally, ACFA is aware that some providers are negotiating a lower daily amount in order to encourage daily payments, which is not consistent with the legislation.
From a consumer perspective the main issues are transparency – that is, transparency of the rate and equal emphasis on the different forms of payment so it is a ‘true choice’ and not influenced by provider preferences in a supply constrained environment– and consumer understanding. Some residents see daily payments, particularly when paying partial daily payments where only a partial lump sum has been paid, as interest on the outstanding lump sum. From this perspective some residents see the MPIR as a punitively high rate of interest.
While the lump sum form of an accommodation payment is consistently the most common at around 50 per cent of non-supported residents, this means that around half are paying at least part of their agreed accommodation price as a daily payment (either fully by daily payment or a combination of daily payment and lump sum), as shown in 3.2.1Box 3.1Chart 3.2.
While many factors are taken into consideration when determining how to pay the accommodation payment (e.g. expected length of stay and/or personal financial circumstances), this suggests that the MPIR is not overly punitive for consumers given their alternatives.
On balance, ACFA is of the view that under the current policy settings the policy of equivalence between lump sums and daily payments should remain, the MPIR is an appropriate rate to be used to determine equivalency and that lump sums should remain as the anchor point from which to convert to daily payments.
62

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
If conditions in the residential aged care market were to change (for example, a significant change to supply), ACFA suggests that the need for equivalency between lump sums and daily payments could be revisited.
3.2.7 Have the accommodation payment reforms contributed to the sustainability of residential care?
The changes to accommodation payments have improved the sustainability of the residential aged care system by supporting greater investment and development of accommodation capacity.
Enabling lump sum refundable deposits to be accepted across residential care and effectively ‘uncapping’ accommodation charges in high care, has substantially increased the pool of lump sums available to providers for capital financing, supporting investment and increased building activity.
The increase in the maximum accommodation supplement has further supported investment and development of additional residential capacity, as discussed in section 3.2.5.
Of post-reform residents in permanent residential care at 30 June 2016, almost 60 per cent paid the full costs of their accommodation either through a market-based accommodation price (56 per cent) or through the maximum rate of accommodation contribution (3 per cent). Of the remaining residents, around 17 per cent pay an accommodation contribution (with the government paying some accommodation supplement), whilst 24 per cent have their accommodation costs met in full.
As discussed in section 2.5.3, the overall proportion of people paying all of their accommodation costs has not changed significantly, when compared with the fee paying status of residents in care in June 2014. From government’s perspective this means that the proportion of residents for whom it is paying an accommodation supplement has not decreased.
ACFA also notes that to some extent the accommodation supplement replaces the cost of providing other government subsidised housing for individuals receiving those benefits prior to entering aged care.
63

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
3.3 Conclusion
3.3.1 Have the policy objectives been achieved?
The changes to accommodation payments aimed to:
introduce transparency and increase consumer choice; support a more competitive market-based approach to accommodation pricing; encourage investment and development of residential accommodation capacity; improve sector sustainability; and maintain safeguards and access to care for residents with low means.
ACFA observes that these objectives appear to have largely been achieved.
The requirement to publish accommodation prices has achieved greater transparency and price competition. The reforms have also given prospective residents greater choice – by both making different accommodation options and prices more transparent and by requiring that residents be given 28 days after entry to decide their preferred method of payment.
Publication of prices has also established a stronger link between prices and the cost and quality of accommodation. Complemented by choice of payment, transparent market-based pricing supports access to care by making it more difficult for providers to select residents based on means or payment preference.
64
Have the changes to accommodation payments met their policy objectives?
Consumer perspective: Greater transparency of accommodation options, improved quality resulting from increased
investment in refurbishment and greater price competition. Average agreed prices are lower than average published prices, which indicates that consumers are able to negotiate lower amounts than published.
Consumers are exercising greater choice of payment, with more consumers choosing to pay by daily payment or combination, although lump sums are still the preferred payment type for non-supported residents.
Consumers have greater discretion in accommodation choices, because accommodation prices reflect quality and amenity rather than individuals’ net assets.
Provider perspective Pool of lump sums continues to grow. New or significantly refurbished homes receive higher accommodation supplement for low
means residents broadly equivalent to the average market-based accommodation price paid by non-supported residents.
Government perspective Building activity has increased. Liability for guaranteed lump sums has increased.

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
The accommodation payments reforms have supported greater investment and improved sector sustainability by allowing providers to accept market-based lump sum accommodation payments regardless of a resident’s level of care, thereby increasing the potential pool of lump sums available to providers for capital investment and development of additional capacity. The higher accommodation supplement has supported access to care for supported residents.
3.3.2 Issues and potential unintended consequences
Whilst the reforms to accommodation payments have largely achieved the intended outcomes, some issues have arisen which warrant further consideration.
Choice of payment
There is anecdotal evidence that some providers are not allowing true choice of payment, that is, requiring the resident to commit to paying by lump sum in order to gain entry to the facility, or by only admitting those people who the provider feels will pay by lump sum, or providing misleading information to the resident about their options.
This information is anecdotal and difficult to take action on, as residents who were pressured into paying a lump sum in order to gain entry may be less aware of their resident rights and perhaps believe that their continued residence may be put in doubt.
ACFA suggests that this could be addressed by promoting increased awareness of choice of payment and residents’ rights and taking the relevant action where actual evidence does come to light.
Maximum permissible interest rate (MPIR)
ACFA notes that choice of payment method lies with the resident and as a result providers may receive payment for accommodation in a form that is not preferred by them. Overwhelmingly, providers prefer to receive a lump sum and the MPIR has been set at a rate that compensates providers for not receiving that lump sum and having to source that capital from elsewhere at the provider’s weighted average cost of capital.
However, some providers may prefer to receive a daily payment and the relatively high MPIR, from a resident’s point of view, may mean that such a provider is less likely to receive a daily payment. The issue is whether a provider should be able to discount the daily payment to an amount lower than that calculated by the MPIR to encourage that payment choice.
ACFA notes that around half of non-supported residents pay at least part of their agreed accommodation price by daily payment (either fully by daily payment or a combination of daily payment and lump sum), although the proportion is higher for partially supported residents paying an accommodation contribution (as shown in 3.2.1Box 3.1Chart 3.2). It is important to note that residents paying a daily payment may subsequently pay a lump sum, for example if they sell their former home or otherwise acquire additional funds.
This suggests that the MPIR is not acting as a disincentive for residents to pay by daily payments and/or that other considerations are being taken into account when determining the payment method (e.g. expected length of stay and/or personal financial circumstances).
65

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Discounting the daily accommodation payment would remove transparency and comparability that is necessary under the current market conditions. A change in market conditions, such as a significant change to supply, may warrant revisiting the current need for equivalency policy.
Interaction of accommodation pricing and accommodation contributions
ACFA notes that there are several unforeseen scenarios and issues that have arisen in relation to the interaction between the accommodation payments rules for non-supported residents and the accommodation contribution rules for low means residents.
Low means resident paying an accommodation contribution higher than published price
It is possible that a resident classified as low means (partially supported), but whose income and assets means they are paying an accommodation contribution at the mid- to upper end of the scale (e.g. up to $55.09, depending on whether the facility is newly built or significantly refurbished), may be unintendedly worse off in the situation where they are in an aged care home with lower published prices. That is, where they are paying an accommodation contribution amount that is higher than the market-based accommodation price.
ACFA notes that whilst this scenario is possible, analysis shows that this has only occurred in a very small number (less than 0.5 per cent) of cases:
It is estimated that approximately 340 of 96,000 post-1 July 2014 residents (out of 235,000 in total) in care at some point during 2015-16 would have paid an amount of accommodation contribution that was greater than the average accommodation price advertised by their aged care home.
Low means residents unable to pay an accommodation payment
Residents assessed and classified at entry as having low means cannot be asked to pay an accommodation payment. Aged care legislation prohibits providers from accepting an amount for accommodation that is greater than the amount of contribution determined by DHS based on the person’s means-tested amount.
If a resident’s family does contribute an additional amount for accommodation on the person’s behalf (i.e. to secure better quality accommodation), aged care legislation includes that money in the person’s means test.
Because the resident is already classified as low means, the effect is that the person simply pays a higher accommodation contribution, up to the maximum accommodation supplement applicable for the home and so it would be unlikely that the home would move the resident into a higher priced room. The resident may also be liable for a means-tested care fee.
Whilst ACFA notes that there is no data to indicate the extent to which this situation may occur, ACFA observes that this could be perceived as a disincentive to families contributing additional funds to secure higher priced accommodation (which could then lessen the government’s accommodation subsidy for that person).
3.3.3 Possible Future Reform Directions
The reforms to accommodation payments have led the way in moving towards a more market based consumer focused aged care system, by increasing focus on and empowerment of the
66

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
demand side of the marketplace.
The publication of accommodation prices on My Aged Care has achieved market-based pricing for accommodation, improving transparency and enabling consumers to compare and negotiate the accommodation price with their preferred provider. Funds following the consumer and the removal of supply controls would complete the move to a consumer-driven market-based aged care service industry.
As noted in the Aged Care Sector Committee’s Roadmap an important consideration going forward will be that government continues to provide safeguards for consumers with limited means. The Roadmap also envisages that the market will provide an expanded range of financial products to provide flexible ways for people to pay for their aged care.
67

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
4 Access to aged care services
This chapter of the report presents ACFA’s analysis and observations about the effectiveness of funding and financing changes in relation to protecting equity of access to aged care services for different population groups and improving overall access to aged care services.
The chapter focuses on how the availability (e.g. number of aged care places available), affordability (e.g. the cost, funding and price of aged care services) and degree of consumer choice or discretion affects how consumers access aged care services. As such, it focuses on the nexus between issues of supply and demand with aged care funding and pricing (i.e. levels of consumer contributions). Issues related to viability (provider perspective) and sustainability (government perspective) are also considered where relevant.
The chapter concludes with an assessment of how well the funding and financing changes have achieved their objectives in relation to access to care, identifies any unintended consequences, and considers how well we are now placed in relation to the blueprint for aged care contained in the Aged Care Roadmap.
Supporting data is in Appendix D to this report.
Changes related to access to care included:
consumer directed care in home care;
increased supply of home care packages; and
introduction of the Commonwealth Home Support Program.
4.1 Post-1 July 2014 supply of subsidised aged care services
4.1.1 How does supply impact access to care?
Equitable access to care by eligible consumers requires the supply of aged care to reflect and match the need for services and consumer preferences. These are also impacted by cost and affordability – for both consumers and government/taxpayers – and providers’ capacity to earn a return on investment.
Currently the government regulates supply – primarily by limiting the number of subsidised aged care places it releases – and many aspects of pricing. That is, government sets subsidy levels and in most cases determines maximum levels of consumer contributions. The only exception to this is in residential care, where non-supported residents can be asked to pay a market-based accommodation price negotiated directly with the provider.
68

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
The reforms included a substantial but controlled expansion of aged care places, focused on expanding access to home care packages.
Supply planning and operational ratios
The Government uses a population-based planning framework to control supply, which is based on a national provision target ratio for subsidised operational residential and home care places for every 1,000 people aged 70 years or over.
The national provision ratio aims to ensure that the growth in the number of aged care places matches growth in the aged population. The operational provision target for residential care is applied at a regional level and places are allocated to providers based on an annual competitive tender. The allocation of places also has regard to special needs groups.
Since 27 February 2017, a national queue for home care was established to prioritise access to home care packages. The new process allows a fairer allocation of packages nationally, based on the individual needs and circumstances of people, regardless of where they live.
Under the reforms, the overall target operational provision ratio is to increase from 113 per 1,000 people aged 70 and over to 125 by 2021–22.35 The reforms will also change the mix of home and residential care, growing the proportion of home care places by 2021-22 from 27 to 45, reducing the residential target from 86 to 78 and reserving 2 places for short term restorative care.
Since the reforms, the overall operational provision ratio has increased by 0.4 to 113.2 at 30 June 2016 (Chart 4.1. Over that period, the residential operational ratio has reduced to 79.7 and the home care operational provision ratio has increased to 31.9.
Chart 4.1: Aged care operational ratios achieved 2006 to 2016, compared with 2022 target ratio
It should be noted that the supply of home support services through CHSP and WA Home and Community Care (HACC) programs is not regulated in the same way, as these services are
35 2015-16 Report on the Operation of the Aged Care Act 1997, p. 4. Available on the Department of Health website at https://agedcare.health.gov.au/publications-and-articles/reports/report-on-the-operation-of-the-aged-care-act-1997#latest report.
69

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
funded through grant agreements (see section 4.2 in Appendix D for key CHSP data). It should be noted that the availability of services through the CHSP without an access, eligibility and funding regime consistent with home care and residential programs may impair the competitive landscape, especially for home care.
ACFA observes that supply considerations are central to equity of access to care and the effective operation of a consumer-driven market-based aged care sector. Supply limitations and regulation can impact the operation of the market, which in turn can impact how consumers access care, e.g. by impacting competitiveness and pricing, and the ability of the market to respond to specific needs/consumer preferences and consumer choice.
The supply and interplay of home and residential care clearly impacts consumer choice and access to services. For example, the slight downwards trend in occupancy in residential care may be reflective of the increase in the number of higher level home care packages, potentially complemented by the increased use of respite care. This raises the question of whether there are people in residential care who would remain at home if more home care was available.
ACFA notes that data is not systematically collected to allow an estimate of the extent to which supply falls short of total need or whether the reforms have reduced the level of unmet need. Nor is it known whether greater access to home care services would generate demand that would not otherwise exist if only residential care was available, or what might be the impact on demand of changes in consumer contributions. Further investigation of the utilisation of services provided through the private (non-government subsidised) market is warranted, and may provide further insight into supply and demand issues.
ACFA also notes that the change in home care in February 2017 that has seen packages allocated to eligible consumers instead of providers is likely, for the first time, to provide useful data on unmet need and demand for home care packages.
4.1.2 How has the profile of community, home and residential care providers changed since the reforms commenced?
ACFA notes that only a short period of time has elapsed since the reforms commenced and it may be too early to conclude whether the reforms have had a significant effect on the competitive landscape for CHSP, home care and residential care, or on the profile of providers of those services.
The overall profile of providers across the aged care sector has not changed significantly since the reforms commenced, although there has been some further consolidation in the number of providers and services in both the home care and residential care sectors.
70

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Home care
Table 4.1 below shows the number of home care providers, services and places at 30 June 2016.
Table 4.1: Provider numbers, number of services and number of packages, as at 30 June 2016
The number of home care providers and services both decreased in 2015-16, which indicates some consolidation in the home care sector, even though the total number of home care places increased. This is a shift from 2014-15, during which the number of home care services actually increased.
This consolidation occurred at the greatest rate in for-profit providers, the number of which declined by seven per cent. In contrast, the number of government providers increased by three per cent.
The home care market continues to be dominated by not-for-profit providers, which make up 69 per cent of home care providers.
Table 4.2 below shows the proportion of packages held by provider ownership type.
Table 4.2: Home care packages by provider ownership type and package level, 30 June 2016
Level Not-for-profit For profit Government TotalLevel 1 1,590 530 134 2,254Level 2 43,187 4,353 4,875 52,415Level 3 5,762 1,166 441 7,369Level 4 14,130 2,133 655 16,918Total 64,669 8,182 6,105 78,956
Not-for profit providers have the largest share of packages at each level.
For-profit providers have a larger share of the new Level 1 and Level 3 packages than they do of Level 2 and Level 4 packages. However, their share of Level 1 and Level 3 packages has continued to decline as it has done in each of the previous two years.
71

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Table 4.3 shows the annual increase in the number of approved providers of home care. Note that these figures include providers that are approved but not operational, so differ slightly from other data that only includes providers that are operational, e.g. Table 4.1.
Table 4.3 Increase in approved providers of home care
2014-15 2015-16 2016-17*
Increase in APs with home care services 12 16 141
Increase in APs with other aged care services, but no home care
0 0 80
Increase in APs with no services 1 0 84
Total increase in APs approved for home care (#) 13 16 305
* Data for 2016-17 are year-to-date as at March 2017 and are subject to change.^ Providers approved for home care but with no HC services may have other aged care services (e.g. residential care, flexible care).
As can be seen in Table 4.3 above, the number of approved providers approved for home care packages increased significantly in 2016-17 (305), likely in response to the changes to home care commencing in February 2017.
Within that, the number of home care providers with no home care services also increased by a much greater number than in previous years with the increase evenly split between those that have other services (e.g. residential or respite), and those that have no services. This suggests that there is a mixture of new organisations and existing aged care organisations entering the home care market in response to the recent home care reforms.
72

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Residential care
Table 4.4 below shows the number of residential care providers, services and places at 30 June 2016.
Table 4.4: Number of providers, services, places and residents in residential aged care, 30 June 2016
Consolidation in the residential care sector has continued, with a further reduction in the number of providers and services while the total number of respite and permanent residential care places increased.
Consistent with the trend over the last seven years, the overall proportion of places held by for-profit providers has increased. The proportion of places held by government providers has remained stable, whilst the proportion of places held by not-for-profit providers has decreased.
4.2 Have the funding and financing changes impacted consumer access to care?
The shift in the balance of care types within the provision targets in favour of home care has given more consumers the option to access care while continuing to live at home.
Overall, the funding and financing changes have differentially impacted consumer access to care. These are summarised below.
4.2.1 Home care
73

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Whilst overall more people are accessing home care with the release of more home care packages, the income-testing and fee changes in home care have had some impact on the take-up of packages, particularly Level 1 packages, showing a decline in occupancy rates across all levels. As discussed earlier in Chapter 2, perceived inequities in fee arrangements for home care packages have impacted both providers’ fee charging practices and the proportion of part-pensioners and self-funded retirees in receipt of lower level packages. Whilst occupancy rates for Level 4 packages corrected shortly after the reforms were implemented, occupancy rates for the other package levels remained lower than anticipated.
Chart 4.1 below shows the national home care occupancy rates by package level and overall, from August 2013 to September 2016. Occupancy rates can be an indicator of changes in access to care, though occupancy is also influenced by other factors. In particular, the annual allocation of new places to providers, a practice that was followed until the February 2017 changes, resulted in short term drops in occupancy levels until those places are filled.
Chart 4.1: National home care occupancy rates, August 2013 to September 201636
Nevertheless, it is noticeable from the graph above that the more expensive packages tend to have higher occupancy. The occupancy rate for Level 1 packages has generally remained markedly lower than for other packages, at no point achieving an occupancy rate above 72 per cent, as can be seen in Chart 4.1 above.
In comparison, occupancy for Level 4 packages has remained relatively stable at around 92 per cent, whilst occupancy in Level 2 packages has gradually trended downwards, dropping from
36 Occupancy in home care is measured as the total number of days a package was actually being used by a consumer (occupied place) as a proportion of the number of days a package was available to be offered to a consumer by a provider (available/operational place). In this calculation, the numerator is the number of claim days (the days in which a consumer is enrolled in the home care package) during a period of interest, and the denominator is the number of place days (the days over which the package was operational) during that same period. So while this measure of occupancy may not directly reflect the way in which home care is delivered, it does reflect the fact that government pays home care subsidy on a per diem basis is a measure of the proportion of total subsidy revenue the provider could have received for that package over the period.
74

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
around 92 per cent in August 2013 to 81 per cent in September 2016. Occupancy in Level 3 packages has varied, climbing to 87 per cent in November 2014 and 91 per cent in March 2016, followed by sharp declines due to new packages being released, and was trending upwards at 78 per cent in September 2016.
Low occupancy in Level 1 packages could be at least partly explained by anecdotal evidence that the level of consumer contributions make lower level packages unattractive to some consumers. As shown in 2.3.2Box 2.1Table 2.1 in section 2.3.2, a self-funded retiree would have to pay an income tested fee equal to the full amount of a Level 1 package (and therefore received no government subsidy).
4.2.2 Residential care
Overall the funding and financing changes have not negatively impacted consumer access to residential aged care services, although they have impacted the way that people access residential care.
Admissions and occupancy
Impacts on access to care can be evaluated by examining trends in admissions to residential respite and permanent residential care and occupancy.
Admissions and occupancy data for permanent and respite residential care show that there have been some changes in trend since 1 July 2014.
Chart 4.1 below shows the trends in admissions to respite and permanent residential care before and after the 1 July 2014 reforms.
Chart 4.1: Admissions to permanent and respite care, July 2012 to September 2016
75

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As can be seen in the chart above, there was a spike in admissions to permanent residential care immediately prior to the start of changes to residential care on 1 July 2014, followed by a significant drop in July and August 2014, after which admissions started to return to the broad pre-reform trend. This likely reflects uncertainty about the financial implications of the changes to means testing and accommodation payments. Some prospective residents may have entered care before July 2014 in order to ‘lock-in’ the existing fee arrangements.
Admissions to residential respite care, however, increased after 1 July 2014 and have remained higher, both in comparison with pre-reform respite admissions and with post-reform admissions to permanent care. This suggests a change in behaviour that could be partly explained by residents’ and/or providers’ preference for individuals to delay entry into permanent residential care while their financial arrangements are settled, entering respite care in the meantime. Another factor could be that respite care is being used more to complement home care packages.
The increased use of residential respite may warrant a review of current funding and consumer contribution arrangements applying to respite37.
Chart 4.2 below shows the occupancy rate in permanent residential care before and after 1 July 2014.
Chart 4.2: Average number of claim days, place days and occupancy rate, July 2013 to December 2016
Consistent with the trend in admissions, occupancy in permanent residential care increased before 30 June 2014 then decreased in the months immediately following and has slowly trended downwards since then, from 93.2 per cent in June 2014 to just under 92 per cent in
37 Accommodation payments and means tested care fees are not charged for residential respite care, though providers can charge the basic daily fee for living expenses.
76

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
September 2016.38 It is important to note that occupancy varies across different geographical regions, and should be considered both in terms of rural and remote classification and by facility size.39
This longer-term decline in occupancy by permanent residents could be driven by an increase in the supply of available places, noting that between June 2014, when the occupancy peaked at 93.2 per cent, and September 2016, the available places increased by 7,339 compared with an increase of 4,798 residents. Significantly, this decline in occupancy occurred despite a reduction in the residential operational provision ratio from 84.5 per 1,000 people aged 70 and over at 30 June 2013 (i.e. pre-1 July 2014) to 79.7 at 30 June 2016, and coincided with an increase in the operational ratio for home care packages over the same period from 27.2 to 31.9. It may be the case, therefore, that fewer people are seeking permanent residential care relative to supply, and could be an early indicator that the level of unmet demand for residential care is declining.
ACFA suggests that this change in trend of admissions to respite and permanent residential care warrants further investigation to understand the causes of increased respite admissions, including whether the changes to funding and fees in residential care have influenced take-up of residential care. Further investigation is also warranted into whether the increased focus on home care and use of Level 3 and 4 packages are impacting trends in residential care admissions and occupancy.
Flexibility and consumer choice
Changes to accommodation payment arrangements have improved consumer access to residential care. Improving transparency has introduced market elements into accommodation pricing, encouraging competition and diversity, and has enabled consumers to have greater understanding of the range of accommodation options and prices.
Ensuring choice of payment and requiring approval of higher accommodation payments by the Pricing Commissioner have supported improved equity of access to care for residents by reducing the ability for providers to select residents based on wealth and capacity to pay a lump sum and providing an external comparative framework for such pricing.
4.2.3 How is the alignment between home-based care and support and residential care impacting consumer access to care?
While steps have been taken to improve the alignment of CHSP, home care and residential care, e.g. though the introduction of the client contribution framework in CHSP and formal income testing in home care, there are still significant differences and imbalances between them that influence consumer behaviour.
38 92 per cent occupancy would mean that on average a room is vacant for 29 days per year. 39 ACFA’s report Issues affecting the financial performance of rural and remote providers found that residential facilities in rural and remote areas are smaller than those in non-rural and remote locations (rural and remote residential facilities have on average 36 beds per facility compared with 81 in non-rural and remote locations) and that occupancy levels in rural and remote areas (for example 87 per cent in remote and very remote) are lower than in non-rural and remote locations (95%) (see especially pp. 55-56).
77

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
A comparison of home care and CHSP
Whilst there is significant similarity with the services offered in home care and in CHSP (see section 4.3 in Appendix D) they have different access and eligibility arrangements and funding and fee structures.
CHSP clients undergo an assessment by the My Aged Care regional assessment service whereas home care consumers are assessed by an aged care assessment team that includes clinical elements.
The CHSP is a grant-funded program while home care providers are funded on a per package basis. Income-tested care fees are payable by home care consumers, which reduce the Government subsidy payable to home care providers (home care consumers can also be asked to pay the basic daily fee). In contrast, CHSP providers set their own client contribution policy based on principles in the Client Contribution Framework and the extent to which clients are contributing is not known (but will become clearer when data is available later in 2017).
Impact of differences between home care and CHSP
The differences in the access and eligibility arrangements and fees policies between home care and CHSP are likely impacting both the competitiveness of home care and consumer choices in respect of home care and CHSP.
As noted previously, low occupancy in Level 1 packages can be at least partly explained by anecdotal evidence that the level of consumer contributions make lower level packages unattractive to some consumers. As shown in 2.3.2Box 2.1Table 2.1 in Section 2.3.2, a self-funded retiree would have to pay an income-tested fee equal to the full amount of a Level 1 package i.e. receive no government subsidy. Furthermore, a significant amount of that package could be spent on administration amounts and care management charges, rather than services.
There is strong anecdotal evidence to suggest that some consumers may be seeking services through CHSP as client contributions are significantly lower or nil, or remaining in CHSP rather than taking up a Level 1 package. Similarly, it is possible that some consumers may not be accessing any services, whilst others – especially part pensioners or self-funded retirees – might be seeking services outside government funded services.
Low occupancy in lower level packages may also suggest a lower level of demand than expected. However, demand may be impacted by the availability of services through the CHSP at a lower price point, which suggests that the apparent impacts on consumer access to care need to be considered more broadly in terms of the supply and availability of other services and the alignment of charges across these services. For example, consideration could be given to implementing a minimum charge for certain CHSP services and/or means testing for CHSP.
The other relevant issue, which has previously been discussed in Chapter 2, is whether some home care consumers in receipt of a package are not receiving services to the full value of the package (noting that this may be the consumer’s preference). There is insufficient evidence available to indicate the extent to which this may be occurring.
Home care and residential care
Once again, the potentially significant difference in total cost between a home care package and residential care (depending on an individual’s care needs and financial circumstances)
78

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
largely due to the accommodation cost and higher daily living costs (see Table 4.1 in Section 4.3 in Appendix D) may also influence consumers’ decisions about their care, noting that care needs will sometimes be the more significant driver of choice.
Annual consumer contributions to home care packages are capped at $5,276 for full pensioners and $10,552 for self-funded retirees (until lifetime caps are reached), plus the (discretionary) basic daily fee of $3,687. This compares with consumer contributions in residential care of $64,400 per annum comprising living expenses (the basic daily fee) of $17,911 per annum, an accommodation contribution of up to $20,108 per annum or an accommodation payment agreed with the provider, and a means-tested care fee of up to $26,381 per annum (until lifetime caps are reached), and potentially extra service fees and/or additional service fees.
ACFA notes that this differential cost to the resident provides for aged care resident suitable accommodation and increased care and services including daily living and meals on a full time (24/7) basis. It is also a product of different means testing arrangements between the two types of care. That is, in home care only income is subject to an income test whereas income and assets are means tested in residential care. Also, home care has substantially lower caps on care fees. The most a person can pay in care fees in home care is $10,552, which represents 22 per cent of a level four package cost of $48,906 while the cap on care fees in residential care is much higher at $26,381.
ACFA observes that as a whole, the alignment between means testing and charges across home-based care and support and residential care is limited. However, there remains a question about the extent to which they could or should be further aligned, given the fundamental difference in the residential service and nexus between assets that do or have contributed to the housing of a consumer. Further policy investigation and policy development is required on this issue, within the broader context of supply, equity of access to care and equity in consumer contributions to care (reflective of both care needs and capacity to pay) and focus on the fundamental difference between residential care and the home based care provided through home care packages and CHSP.
4.2.4 Has there been any impact on access to care for people with low means?
The changes to means-testing and accommodation payments in residential care have not impaired access to care for people with low means.
There is no clear pattern in the admissions to residential care that would indicate that new means-testing arrangements are impacting on access to care for people in particular income ranges. There has been no substantial change in the average income (in real terms) of new entrants to residential care in the years leading up to the reforms compared with people entering after 1 July 2014 (Chart 4.1).
79

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Chart 4.1: Average income of new entrants to residential care, constant prices (2015-16 dollars)
Source: Income test data for new entrants, Department of Human Services.
Notes: (a) constant 2015-16 prices calculated by indexing against growth in the maximum rate of age pensions, (b) analysis of income only includes residents who have had an income test (i.e. excludes ‘means-not-disclosed’ residents).
Similarly, as shown in Chart 4.2 total admissions by pension status (i.e. full pensioner, part-pensioner, self-funded retiree) over 2014-15 and 2015-16 have not changed significantly compared with admissions for 2012-13 and 2013-14. This also suggests that the means-testing changes have not had any significant impact on access to care by low means residents overall.
80

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Chart 4.2: New permanent admissions to residential care by pension status, 2012-13 to 2015-16
These findings are also supported by data on the average period between ACAT assessment and entry to permanent care, which shows that there is no substantial difference in time for low means residents compared with non-supported residents.
These findings are consistent with ACFA’s January 2017 Report on access to care for supported residents.40 ACFA found that the net impact of the 1 July 2014 reforms do not appear to have adversely affected access to services for supported residents, with the overall proportion of supported residents increasing from 44.4 per cent in 2013-14 to 46.8 per cent in 2015-16. In consultations for that report some anecdotal information was provided to ACFA that some providers were showing a preference for non-supported residents but this does not appear to have led to significant shifts in access.
4.3 Is Consumer Directed Care supporting access to care?
Consumer Directed Care (CDC), which was introduced for all home care packages from 1 July 2015, was a first stage in reforms to home care intended to improve consumer access to preferred services, by giving older people greater flexibility over their health and wellbeing by allowing them to make choices regarding their goals, preferences and assessed needs.
Individual budgets and monthly expenditure statements were introduced as part of CDC to enable consumers to know how their package is funded and decide how their individual budget is spent. Monthly statements of the available funds and expenditure provide regular reports on the status of expenditure to date. This potentially increases the opportunity for consumers to participate in the development of their care plans and, if desired, be involved in the
40 ACFA’s Report on access to care for supported residents is available on the Department of Health website at ACFA's Report on access to care for supported residents.
81

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
management of their package. This supports consumers to exercise greater choice over the services they effectively purchase.
The next step in these reforms commenced in February 2017, with funds attached to the consumer and packages portable between home care service providers.41 This enables consumers to access their preferred service provider.
There is no data available to indicate how well individual budgets, monthly statements and funds following the consumer may be supporting consumers to access care. ACFA notes, however, that comparisons of prices for home care services are difficult because providers are publishing prices in different formats.
Administration and exit amounts
ACFA is aware of anecdotal feedback that indicates that some consumers are concerned about the proportion of package funds allocated to administration fees (administration and case coordination). Some consumer peak bodies have claimed fees equivalent to up to 70 per cent of a consumer’s package are being charged. Proposals have been put to the Government to introduce a cap on the administration fees providers can charge as part of the delivery of home care packages, and for all administration charges to be published on My Aged Care.
ACFA notes that maximum exit amounts have been published on My Aged Care from 2017, and must be included in home care agreements to ensure consumers are aware of the maximum amount they may be asked to agree to when they are choosing a home care provider. A number of providers have decided not to charge exit amounts.
4.3.1 Has Consumer Directed Care impacted provider viability?In considering the impact of CDC on consumer access to care, any impacts on provider viability should also be considered.
The report on Provider and Consumer Research Regarding Recent and Future Changes in Home Care conducted on behalf of the Department of Health found that around three-quarters of providers highlighted challenges associated with the implementation of individual budgets and monthly statements. Around half of providers in the study reported experiencing some difficulty in setting fees.42 According to the report, there was particular confusion around:
how providers should determine administrative fees, particularly because they had previously used unspent funds to cover administrative and operational costs; and
setting price points that were comparable or competitive with those of other organisations (particularly the case for not-for-profit providers, who felt they need to be competitive with for-profit organisations).
41 The Increasing Choice in Home Care reforms also consolidated the suitability criteria for becoming an approved provider into six key areas: the applicant’s experience; understanding of responsibilities as a provider; systems in place to meet its responsibilities; financial management and methods; conduct as a provider; and any other matters.42 See TNS ‘Provider and consumer research regarding recent and future change in home care’ research report, available on the Department of Health website at TNS Provider and consumer research regarding recent and future change in home care research report., especially pp. 33-35.
82

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
ACFA observes that these challenges are likely transitional issues and are not unexpected with such a significant change in business model and associated cultural, systems and procedural issues.
Subsidy reduction
The introduction of the reduction in subsidy equal to a consumer’s income-tested care fee may be impacting on a provider’s viability in circumstances where a provider chooses not to collect the full income-tested care fee, yet is required to provide services to the full value of the package.
Unspent funds
StewartBrown has reported that in the year ending 30 June 2016, home care providers’ revenue utilisation rate was around 80 per cent, equivalent to unspent funds of around 20 per cent.43
From a consumer’s perspective, the reasons for not fully expending the package value include that the consumer’s needs may be less than the full value of the package (but more than the value of a lower level package) or that they are saving for a significant purchase or as a buffer in case care needs increase in the future.
From a provider’s perspective, apart from ensuring that a consumer is receiving the appropriate amount of care, package utilisation has become more important subsequent to the February 2017 changes to home care that require a provider to refund or transfer unspent funds when a consumer leaves their care. Previously, unspent funds were a windfall to the provider. Post February 2017 unspent funds are a liability for the provider, which, if not managed carefully, represent lost revenue and create financial pressure if substantial refunds or transfers are required when a consumer leaves care or moves to another provider.
From a government point of view, significant unspent funds on providers’ balance sheets represent a significant risk that that money may be lost if providers go out of business.
ACFA notes, however, that StewartBrown’s latest survey report indicates that the average unspent funds had dropped to around 8 per cent in December 2016, and suggests that providers are finding ways to increase package utilisation, such as changing their service offerings.44
43 StewartBrown Aged Care Financial Performance Survey – Home Care Report – June 2016, p. 1944 StewartBrown Aged Care Financial Performance Survey – Home Care Report – December 2016, p. 11.
83

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
4.4 Conclusion
4.4.1 Have the policy objectives been achieved?
The overarching objectives of the reforms from an access perspective were to increase consumer access to home care and to give consumers greater choice, control and flexibility when accessing care. To this end, the reforms to means-testing and fee arrangements and the controlled expansion of home based care were the most significant, along with measures to ensure access by consumers with lesser means.
Overall the changes to funding and financing have supported consumer access to care.
84
Have the funding and financing reforms improved accessibility to aged care services for older Australians?
Consumer perspective:Home care: The increase in the operational provision ratio for home care places has given more
consumers the option to access care while continuing to live at home. Consumer directed care, individual budgets and monthly statements have improved
transparency and facilitate consumer choice, although there is some confusion about fees. Low take-up of lower level packages, suggesting fee arrangements have had some impact
and some consumers may be seeking services elsewhere or using informal care arrangements.
Residential care Transparency of accommodation options, quality and prices has improved. There is a diverse range of accommodation options available at different price points. There has been no negative impact on access to residential aged care by low means
consumers.
Provider perspective Some providers do not charge full basic daily and/or income-tested care fees in home care,
depending on financial circumstances.
Government perspectiveHome care Home care recipients predominantly pensioners. Some consumers are choosing to remain on more generous services under the
Commonwealth Home Support Program.
Residential care Building activity has increased. No impact on access to care for residents with low means. Use of respite care has increased.

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
The introduction of individual budgets and monthly statements under CDC in home care and the requirement to publish accommodation prices for residential care have both improved transparency and consumer choice, which are both key in supporting access to care. The increase in the maximum accommodation supplement was also important for ensuring a supply of beds for low means residents, including newly refurbished facilities.
There has not been any differential impact on access to care for people with low means when compared with people with higher means.
ACFA notes that there has been minimal increase in the overall operational provision ratio for subsidised aged care places. ACFA also notes that there is insufficient data to measure the level, if any, of unmet demand for aged care services, or whether the reforms have reduced the level of unmet demand. There is also no data available about aged care services in the private market and the extent to which older Australians – particularly wealthier older Australians – access non-government subsidised services.
However, as noted in the preceding discussion, there are examples where consumers do not appear to be accessing care in the way expected, e.g. higher rates of respite use, slightly lower occupancy in residential care (although arguably this could be expected given the expansion in home care places), lower than expected take-up of lower level home care packages, and potentially greater use of CHSP or private services, or relying on care from family.
4.4.2 Are there any unintended consequences?
As mentioned above, the most significant unintended outcome in relation to access to care is the apparent impact on how consumers are accessing lower level care and services, particularly the relatively low take up of Level 1 packages. Current perceptions that home care fees are too expensive are influencing some consumers’ decisions to not take up a package or to receive a lower level of services that can be purchased with the reduced subsidy only. This can be at least partly attributed to the current settings of the home care fees policy and its relationship with CHSP, where consumers can access similar services for minimal client contributions.
4.4.3 Possible future reform directions
Ensuring access to care will be a key question for future reform, especially in the context of the role of supply restrictions and market operation of the aged care system.
The consumer-driven market-based aged care system envisaged by the Aged Care Roadmap is based on the removal of service rationing, allowing the market to respond to demand (although the Roadmap still see government playing a role in thin markets and access by special needs groups). This would be supported by an independent eligibility and needs assessment process and consumer choice of care setting.
Changes to funding and financing arrangements have better positioned the aged care system for achieving a more market-based, consumer driven system, including since the introduction of funding following the consumer in home care in February 2017. Funds following the consumer is the most significant step taken to date towards achieving a more consumer-driven, flexible and market-based aged care services sector.
85

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As noted previously, changes to means-testing and fee arrangements in home and residential care have somewhat improved the alignment of charges between those two care settings. However, further alignment in both means-testing and fees policies would be required across home-based and residential care to support a more integrated system with greater flexibility of access and movement across care settings.
Similarly, whilst the Client Contribution Framework in CHSP is consistent with the principles of the fees policies in home and residential care, further thought needs to be given to a more integrated care at home system in the future.
In terms of supply and demand, ACFA observes that there is currently insufficient data available to understand the extent, if any, of unmet demand for subsidised aged care services, and that a better understanding of this and the private market would be needed. Monitoring occupancy rates for the different care types as the overall provision ratio is increased and at the same time re-balanced in favour of home care, and monitoring waiting lists through My Aged Care’s national prioritisation process, should shed further light on the level of unmet need and consumer preference.
86

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
5 Aged care workforce
Workforce is the key enabler of aged care service delivery and reform. It is also a significant driver of cost in the aged care system. As workforce costs are such a large component of the overall cost of the aged care system, reform and redesign of workforce roles is becoming increasingly important to support affordable and equitable access to health and aged care services.
As noted in the Introduction, ACFA’s analysis of workforce issues is necessarily limited, as there were few funding and financing changes directly related to the aged care labour market.
Therefore, the discussion related to workforce in this chapter is brief and focussed primarily on the workforce supplement introduced as part of the reforms and subsequently re-directed into generalised funding. It also brings together ACFA’s observations from recent annual reports and study into factors affecting the financial performance of rural, regional and remote providers, including about wage costs and implications for provider viability.
5.1.1 Workforce supplement
The 2012-13 Budget included an allocation of $1.2 billion over five years from 2012-13 (including $471.7 million in 2016-17) to address workforce pressures in aged care. The workforce supplement was paid to aged care providers who met the terms and conditions of the Workforce Compact, which was an attempt to improve wage rates for aged care workers in order to retain workers and also to encourage more workers into the industry.
As part of the 2013-14 Budget, the Government redirected funding from the workforce supplement into the general pool of aged care funding. The offsets included:
Residential, home care and flexible care providers received an increase in funding of 2.4 per cent in their basic care subsidy from 1 July 2014.
Eligible grant programs such as the Commonwealth Home and Community Care Programme received a 2.4 per cent increase in their funding.
Eligible regional, rural and remote providers received a 20 per cent increase to Viability Supplement payments from 1 July 2014.45
5.1.2 Wage costs as a proportion of provider expenses
45 There have also been subsequent increases to the viability supplement.
87

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As ACFA has previously reported in its annual reports on the funding and financing of the aged care sector, wage costs represent the greatest proportion of provider expenditure and have a significant impact on financial performance.
In home care, salaries comprise the greatest proportion of expenditure across all types of provider. In 2014-15 salaries represented 60 per cent of total expenditure.46
Chart 5.1: Proportion of expense types reported by home care providers, 2014-15
Similarly, in residential care employee expenses represent the highest proportion of provider expenditure. In 2014-15, staff costs represented 67 per cent of total expenses (up from 66 per cent in 2013-14), with ‘other’ costs, which include building repairs and maintenance expenses, rent, utilities and costs associated with employment support activities, accounting for 27 per cent. Depreciation and interest costs account for the remaining 4.9 and 0.9 per cent respectively.
Table 5.2 below compares the change in breakdown of expenses between 2013-14 and 2014-15.
46 Source: ACFA annual report 2016. Data sourced from home care financial reports submitted to the Department of Health for 2014-15 in a useable form.
88

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Table 5.2: Summary of expenses for residential care providers 2013-14 to 2014-15
Expenses 2013-14($ million)
2014-15($ million)
Change($ million)
Change(per cent)
Employee expenses $9,313 $9,998 $684 7.3
Depreciation expenses $723 $728 $5 0.7
Interest expenses $147 $140 -$6 -4.3
Other expenses $3,931 $4,037 $106 2.7
Total $14,115 $14,903 $789 5.6
In 2014-15, $10 billion was expended in wages and management fees in residential care, an increase of $684 million from 2013-14. Of this:
$122 million (18 per cent) is attributable to an increase in the number of days of care provided (volume changes);47
$555 million (81 per cent) is attributable to a 6 per cent increase ($8.87 per claim day) in the average amount paid per claim day in wages and management fees. This would reflect a combination of factors including wage increases, increased hours worked per claim day, increased staffing levels and changes in the mix of staff to cater for increased care needs; and
the remaining $7 million (1 per cent) is due to the interaction of price/volume changes.
Table 5.3 below shows the employee expenses as a proportion of total residential service revenue, from 2008-09 to 2014-15.
Table 5.3: Provider expenses as a proportion of total residential service revenue
MeasureExpenses as % of Total Revenue
2008-09 2009-10 2010-11 2011-12 2012-13 2013-14 2014-15Total Revenue $b $10.1b $11.0b $12.0b $13.1b $14.0b $14.8b $15.8b
Employee Expenses 66.6% 65.4% 63.3% 62.3% 63.6% 62.8% 63.2%
$6.7b $7.2b $7.6b $8.1b $8.9b $9.3b $10.0b
As can be seen above, employee expenses as a proportion of total revenue has remained relatively stable over the last five years, averaging around 63 per cent.
47 This broadly reflects increases in resident numbers.
89

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
Chart 5.2 below demonstrates that care income and wages have increased at a similar rate over the last ten years, well in excess of CPI.
Chart 5.1: Cumulative increase in care income and care wages
Source: June 2016 StewartBrown Aged Care Financial Performance Survey
Wage costs in rural, regional and remote areas
ACFA’s 2016 report Financial Issues Affecting Rural and Remote Aged Care Providers found that labour costs are a significant contributor to higher expenses in rural and remote areas.48 Higher labour costs were noticeable for registered nurses and enrolled nurses in particular and also in more general areas such as catering, cleaning and laundry, maintenance and repair.
Financial analysis in this report showed total labour costs in rural and remote areas of $67,770 per resident per annum (prpa) or $185.67 per resident per day (prpd) compared with $51,410 prpa ($140.85 prpd) in non-rural and remote areas. This supports the view that additional labour cost pressures arise in rural and remote areas.
It also found that staff costs accounts for 71 per cent of the expenditure for rural and remote facilities compared with 64 per cent for non-rural and remote facilities.
Consultation conducted as part of this project found that there was a general view that rural and remote aged care providers face a high level of workforce ‘churn’ and challenges in recruiting and retaining staff, both skilled and unskilled. This can lead to difficulties and delays in filling positions and in some cases the need to pay higher wages or offer other additional support such as with accommodation, relocation and travel expenses or through agreeing to provide longer more certain hours to staff. Training and professional development costs for new and existing staff can also be higher.
48 ACFA’s report Financial Issues Affecting Rural and Remote Aged Care Providers is available on the Department of Health website at https://agedcare.health.gov.au/aged-care-reform/aged-care-financing-authority/issues-affecting-the-financial-performance-of-rural-and-remote-providers-both-residential-and-home-care-providers .
90

Aged Care Financing Authority | Report to inform the 2016-17 review of amendments to the Aged Care Act 1997 – Part One – Analysis and Observations
As noted above, a 20 per cent increase to Viability Supplement payments was delivered to eligible providers to help alleviate the higher costs associated with delivering aged care in regional, rural and remote areas.
5.1.3 2016 Aged Care Workforce Census and Survey
According to the 2016 Aged Care Workforce Census and Survey (NACWCS), the overall picture of the size and composition of the aged care workforce is mixed and suggestive of considerable structural change taking place. The overall workforce is estimated to have increased by four per cent as a whole, with direct care workers being five per cent higher in residential care and seven per cent lower in home care and home support (or a three per cent increase and 19 per cent decrease in full-time positions respectively). A considerable shift away from casual or contract employment arrangements has been seen since 2012, particularly within the home care and home support sector.
Job satisfaction is high except in relation to wage rates, with working conditions improving without any major imbalances. However, concerns were raised regarding aged care being considered an unattractive industry by potential employees due to perceptions that it was a low status job which offered poor pay and few career pathways. Future workforce planning and development of the aged care workforce may need to further explore and address these issues.
In summary, the 2016 NACWCS showed that the aged care workforce is both stable and committed. Its workers report relatively high levels of job satisfaction and a large majority wish to stay working in the sector. The overall picture that emerges is that both the retention of current workers and the attraction of new workers to the sector seem to be working well with no major bottlenecks or hurdles that the labour market could not sort out by itself and without intervention.49
49 2016 National Aged Care Workforce Census and Survey – The Aged Care Workforce, 2016, is available on the Department of Health website at 2016 National Aged Care workforce Census and Survey.
91