Embed Size (px)
Citation preview

Goals of CiPA: the Comprehensive In Vitro Proarrhythmia Assay
1 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
Gary Gintant, Ph.D. Dept. Integrative Pharmacology Integrated Sciences and Technology, AbbVie For the CiPA Steering Team Pharm Sci. & Clin. Pharm. Advisory Comm. March 15, 2017
Outline
Background: Cardiac Cellular Electrophysiology Unintended Consequences of focus on hERG/iKr Current CiPA: Goals, Individual Components Ongoing Efforts
2 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Ventricular Repolarization: Integration of Cellular Responses Lead to QT Interval Prolongation, Increased Risk of Proarrhythmia
Repolarization: - the integration of multiple inward and outward currents defines cellular repolarization (action potential) - integration of cellular activity defines QT interval on clinical ECG - repeated with each heartbeat
Net outward (repolarizing) current: - defines repolarization and terminates each cardiac cycle - reduced net outward current leads to delayed repolarization, QT prolongation
- We understand the cellular mechanisms that cause delayed repolarization that lead to proarrhythmia (Torsades-de-Pointes)
3 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
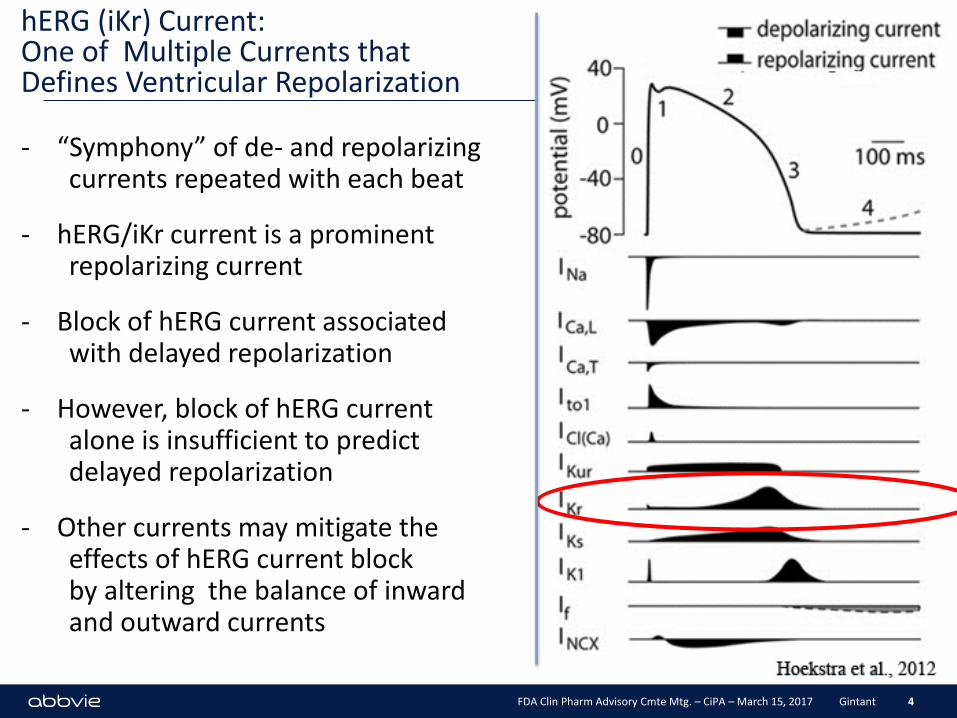
hERG (iKr) Current: One of Multiple Currents that Defines Ventricular Repolarization
4
- “Symphony” of de- and repolarizing currents repeated with each beat
- hERG/iKr current is a prominent repolarizing current
- Block of hERG current associated with delayed repolarization
- However, block of hERG current alone is insufficient to predict delayed repolarization
- Other currents may mitigate the effects of hERG current block by altering the balance of inward and outward currents
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

ICH S7B Guidance: A “hERG-centric” Approach That Impacts Drug Discovery, Approvals
5
ICH S7B Approach “Successful” - No drugs removed from market due
to TdP since 2003
HOWEVER: - hERG not very predictive of QTc effects - Findings of hERG/iKr block in early screening of drug candidates often discourages compound progression,
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
Step 4. 2005
“throwing the baby out with the bathwater” - Triggers additional costly synthetic efforts to remove hERG liability, slowing efforts - Some drugs might not be available today if hERG assay results “enforced” (pentobarbital, verapamil, ranolazine) FINALLY: - Translation of in vivo animal assays to human QT findings imperfect - Binary clinical QT study results do not fully inform on proarrhythmic risk (gradient)

Drugs Block Multiple Cardiac Currents: Inward Currents May Balance Outward Currents
6
More comprehensive mechanistic-based assessment of integrated effects of drug on repolarization is necessary.
Drugs with low torsade risk have balanced block of outward current (hERG/iKr) current and inward current (late sodium or L-type calcium block)
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

CiPA: Comprehensive In Vitro Proarrhythmia Assay
Goal: Develop a new in vitro paradigm for cardiac safety evaluation of new drugs that provides a more accurate and comprehensive mechanistic-based assessment of proarrhythmic potential
- focus on proarrhythmia (not QT prolongation) to improve specificity compared to preclinical hERG and clinical TQT studies
How? - Define drug effects on multiple human cardiac currents, - Characterize integrated electrophysiologic response using in silico reconstructions of human ventricular electrophysiology, - Verify effects on human stem-cell derived ventricular myocytes
7 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
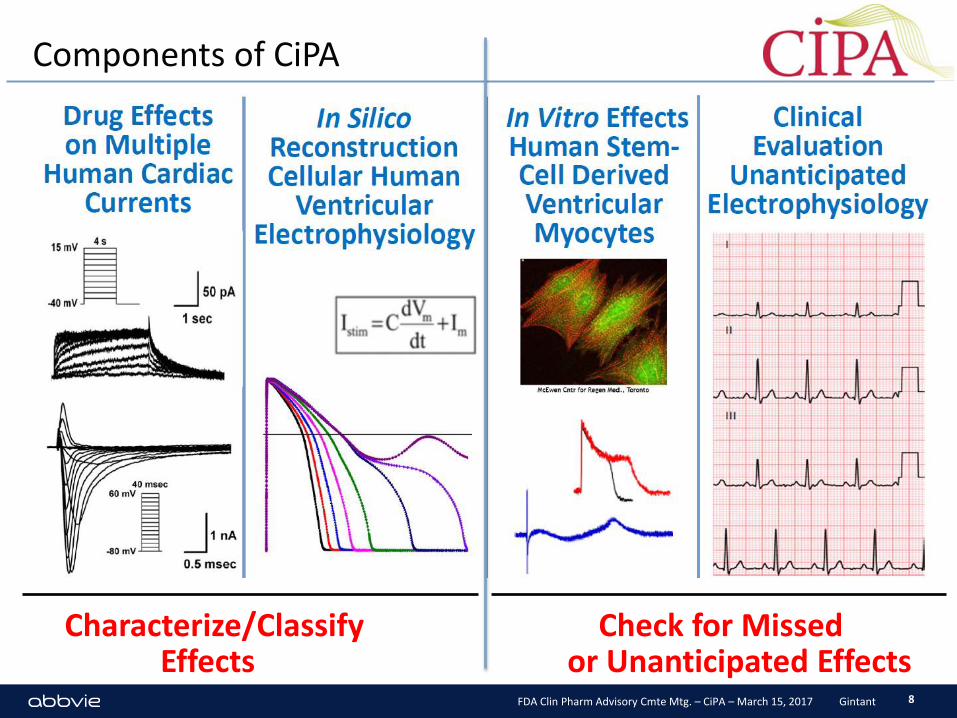
Components of CiPA
Characterize/Classify Check for Missed Effects or Unanticipated Effects
8 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

I. Drug Effects on Human Ionic Currents. Ion Channel Working Group (ICWG)
Goals: characterize effects of drugs on prominent ionic currents that define ventricular repolarization - Reliable and reproducibly characterize block of human cardiac ionic currents in heterologous expression systems - Automated patch platforms for higher throughput, reduced variability - Seven currents selected based on experience of academia, industry, regulators
9
iNa, Fast * iNa, Late
iTo* iCaL* iKr (hERG)
iKsiK1
RED: depolarizing currentGREEN: repolarizing current* most commonly blocked by 12 reference drugs
Ionic CurrentsSelected Cardiac
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Ion Channel Working Group High Throughput System (HTS) Study
HTS study ongoing
- Assess variability and reproducibility of HTS platforms/sites for defining drug effects on cardiac ionic currents across/between platforms and sites using standardized protocols, concentrations
- Generate key ion channel data (IC50 values for current block) for calibration and validation of reconstructions by In Silico Working Group
- hERG current responses to be shared with ISWG for further characterization and modeling of iKr block kinetics
- Phase 1: Blinded “calibration” dataset (12 drugs) due end Q1-2017 Phase 2: Blinded “validation” dataset (16 drugs) due end Q2-2017.
-
10
hERG/iKr current block
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
V
I

II . In Silico Mechanistic Computational Modeling In-Silico Working Group
Goals: - define proarrhythmia risk metric based on drug effects of an in silico model of adult human ventricular cardiomyocyte - metric to be mechanistically related to cellular proarrhythmic effects, experimentally verifiable - O-Hara –Rudy model selected - modified hERG/iKr current Markov model added
- Data from human ionic current assays to be used in model to assess relative Tdp risk - separating reference drugs into three distinct categories (high, intermediate, low/no risk) based on clinical exposure - results to be compared to clinically assigned risk categories
11
More details from Gary Mirams and Zhihua Li FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Proarrhythmic Clinical Risk Categorization: Three-Tier Ranking of TdP Risk (CiPA 28)
Clinical Translational Working Group
High TdP Risk Training Set:
Bepridil Dofetilide Quinidine D,l Sotalol
Validation: Azimilide Ibutilide
Vandetanib Methadone
Intermediate TdP Risk Training Set:
Chlorpromazine Cisapride
Terfenadine Ondansetron
Validation: Astemizole
Clarithromycin Clozapine
Domperidone Droperidol Pimozide
Risperidone
Low TdP Risk Training Set:
Diltiazem Mexiletine Ranolazine Verapamil
Validation: Loratadine Metoprolol Nifedipine
Nitrendipine Tamoxifen
12 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

III. Drug Effects on Stem Cell Derived Cardiomyocytes. CiPA-HESI Myocyte Working Group
Role: to identify potential gaps in cellular electrophysiologic effects (not detected from ionic current/in silico reconstructions) that may impact TdP risk assignment - Relies on ability of myocytes to recapitulate integrated effects of critical systems that influence electrophysiology found in human myocytes Examples: - modulation of channels/currents by receptors, second messengers, additional transporters/exchangers (Na-K pump), (Na-Ca exchange), calcium dysregulation, non-specific” toxicity How: Report drug-induced repolarization abnormalities using induced pluripotent stem cell derived cardiomyocytes
13 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
ww
w.la
broo
ts.c
om

Electrophysiologic Studies of Human Stem Cell-Derived Cardiomyocytes in CiPA
Experimental approaches: higher throughput techniques enable efficient & early assessment of repolarization effects (48/96 well) - Microelectrode arrays: reveal prolongation of field potential duration
(local “ECG” of stem cell cardiomyocytes) - Voltage-sensing dyes: changes in repolarization shape - Other indices: rate, spike amplitude, early after-depolarizations
(EAD’s, triggers for Torsades proarrhythmia) 14
Torsades de Pointes
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Stem-cell Derived Cardiomyocytes: Pilot Study Completed.
• 12 Site Pilot Study (volunteers) - 2 Commercial cell lines, 8 blinded drugs
• 2 approaches - Multi-electrode array (MEA-8 ) - Voltage-sensing optical (VSO-4 sites)
15
Goal: Evaluate ability of stem cell derived cardiomyocytes to detect electrophysiologic effects of select compounds known for single and multiple-channel blocking effects
GRAPHIC HERE
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Validation Study (Ongoing) Stem Cell Derived Cardiomyocytes:
16
FDA Broad Area Announcement (BAA) Award: (9/2015) - Core Group: Blinded evaluation of 28 CiPA drugs (high, intermed., low/no risk) across two different cells and platforms (MEA and VSO) - Focus on delayed repolarization, cellular proarrhythmia (EAD’s) - Input from industry, cell/platform providers, academics - Intermediate Results (drugs unblinded): April 2017
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
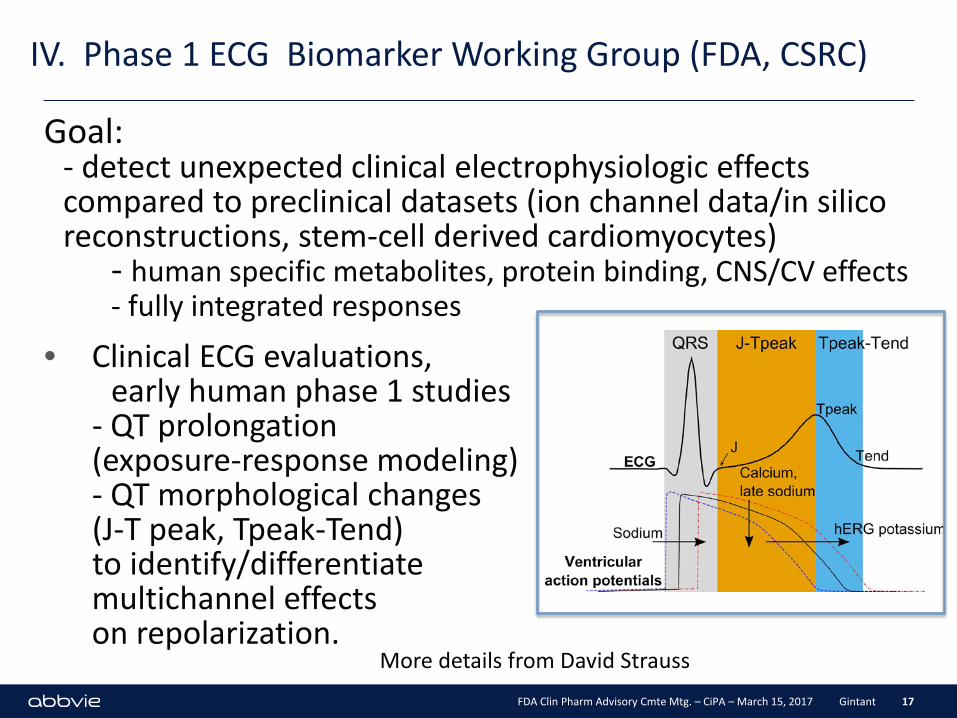
IV. Phase 1 ECG Biomarker Working Group (FDA, CSRC)
Goal: - detect unexpected clinical electrophysiologic effects compared to preclinical datasets (ion channel data/in silico reconstructions, stem-cell derived cardiomyocytes) - human specific metabolites, protein binding, CNS/CV effects - fully integrated responses • Clinical ECG evaluations,
early human phase 1 studies - QT prolongation (exposure-response modeling) - QT morphological changes (J-T peak, Tpeak-Tend) to identify/differentiate multichannel effects on repolarization. 17
More details from David Strauss FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

CiPA: proarrhythmic risk assessment based on mechanistic understanding of integrated, cellular emergent drug effects on multiple human cardiac currents
Present Expectations: - reduce unwarranted attrition early candidates - enable rapid progression of low risk TdP drugs to phase 1 studies (and confirmatory clinical ECG findings) - eliminate need for thorough QT studies in later drug development
Present (and Future) Expectations of Stem-cell derived CM’s - identify potential gaps in cellular electrophysiologic effects (not detected previously from ionic current/in silico reconstructions) that may impact TdP risk assignment -hiPSC-CM’s will eventually replace in silico/computer reconstructions, dedicated animal QT studies
18 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Nonprofits - Public-Private Partnerships • Health and Environmental Sciences Institute (HESI) • Cardiac Safety Research Consortium (CSRC) • Safety Pharmacology Society (SPS) Global Regulatory Agencies • U.S. Food and Drug Administration • European Medicines Agency • Japan Pharmaceuticals and Medical Devices Agency / NIHS • Health Canada Industry / Academia • Numerous Pharmaceutical and Laboratory Device Companies • Contract Research Organizations, Stem Cell Providers • Multiple Academic Groups
19
Acknowledgments
FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

Thank you for your attention.
20 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant

21 FDA Clin Pharm Advisory Cmte Mtg. – CiPA – March 15, 2017 Gintant
12:10 p.m. Presentation #1 Overview of the ICH E14 Guideline and its Implementation within FDA
Christine Garnett, PharmD Clinical Analyst and QT Lead Division of Cardiovascular and Renal Products Office of Drug Evaluation I, Office of New Drugs, CDER, FDA
12:30 p.m. Presentation #2
Goals of CiPA: the Comprehensive In Vitro Proarrhythmia Assay
Gary Gintant, PhD Senior Research Fellow Department of Integrative Pharmacology Abbvie
12:50 p.m. Presentation #3
Background and Rationale for Mechanistic Cardiac Electrophysiology Models
Gary Mirams, PhD Sir Henry Dale Fellow Centre for Mathematical Medicine and Biology University of Nottingham., United Kingdom
1:05 p.m.
Presentation #4 CiPA In Silico Modeling Development Strategy and Results
Zhihua Li, PhD Staff Fellow Division of Applied Regulatory Science OCP, OTS, CDER, FDA
1:20 p.m.
Presentation #5 Phase 1 ECG Analysis under CiPA, Integration of All CiPA Components, and Potential Implementation Strategy
David Strauss, MD, PhD Division Director Division of Applied Regulatory Science OCP, OTS, CDER, FDA
The Next Presentation

Background and rationale for mechanistic cardiac
electrophysiology models
Gary Mirams Centre for Mathematical Medicine & Biology,
University of Nottingham, UK

Why use mathematical models?
“[Mathematical] Models in analytical pharmacology are not meant to be descriptions, pathetic descriptions, of nature; they are designed to be accurate descriptions of our pathetic thinking about nature. They are meant to expose assumptions, define expectations and help us to devise new tests.”
James W. Black Nobel Prize Lecture, 1988
“If people do not believe that mathematics is simple, it is only because they do not realize how complicated life is.”
John von Neumann
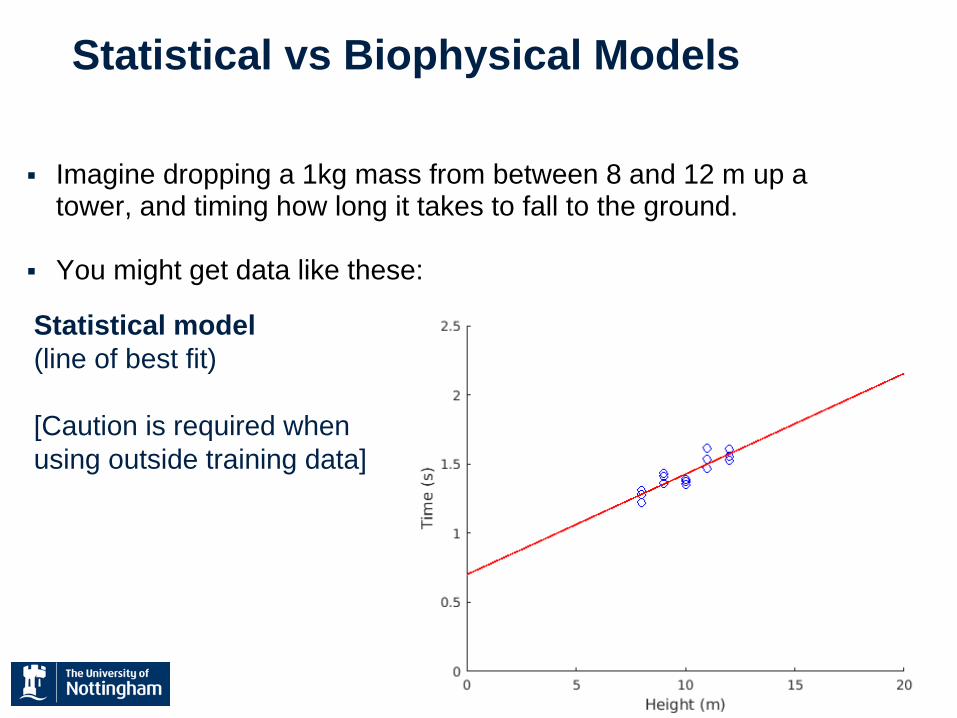
Statistical vs Biophysical Models
Imagine dropping a 1kg mass from between 8 and 12 m up a tower, and timing how long it takes to fall to the ground.
You might get data like these:
Statistical model (line of best fit) [Caution is required when using outside training data]

But if we have a hypothesis for the underlying processes we can make a [bio]physical model.
ℎ = ½𝑔𝑡2
[This is the CiPA approach: reliable for extrapolation if we have captured biophysics well]
Statistical vs Biophysical Models
Imagine dropping a 1kg mass from between 8 and 12 m up a tower, and timing how long it takes to fall to the ground.
You might get data like these:

Biophysical models of electrophysiology Voltage-gated ion
channel currents (& pumps and exchangers)
Cell
Tissue / organ
Body surface markers
Zemzemi et al., British Journal of Pharmacology, 2013
Biophysical Electrophysiology Models
Hodgkin & Huxley, 1952: First applied to cardiac cells by Denis Noble in 1958-60.
First quantitative biophysical model of membrane excitability
Describes dependence of currents on membrane voltage and time. Excitable voltage waveform emerges from interaction of these currents.

Electrophysiology Models
Luo-Rudy 1991
Widely used simple model which includes major ionic currents
Contains a phenomenological description of calcium dynamics

Electrophysiology Models
Noble et al. 1998
Includes the Sarcoplasmic Reticulum (SR) – the cell’s intracellular calcium store
Distinct rapid and slow potassium currents (Ikr/hERG and IKs)

Modern Cardiac Models
O’Hara et al. (2011)
Based on human cell and tissue data
Calcium sub-space gives rise to calcium induced calcium release and afterdepolarisation behaviour
O’Hara et al. (2011). PLoS Comp. Biol. 7: 1002061.

The importance of multi-channel effects
e.g. Simulation of the application of Verapamil up to therapeutic concentrations (hERG and CaL blocker).

Ion Channel In Silico Workflow in CiPA
Clinical Evaluation Unanticipated
EP Effects
Drug Effects on Multiple Human Cardiac Currents
In Silico Reconstruction Human Ventricular
Cellular Electrophysiology
In Vitro Effects Human Stem-Cell
Derived Ventricular Myocytes
a) Obtain patch clamp data on human cardiac ion channels contributing to TdP risk, b) Use these data as inputs to an in silico model of the human ventricular myocyte, c) Run simulations and calculate a metric that classifies the level of TdP risk, d) Check predictions of electrophysiological changes in iPSC-CMs and Phase I ECG.

CiPA modelling flowchart
Comparison with: stem cell; [later in-vivo pre-clinical];
Phase I ECG results
Evaluation of TdP risk metric(s)
Ris
k

In Silico Development Plan
• Training/Calibration phase: assess model performance and modify model as required; identify candidate metrics that can classify TdP risk using a test set of 12 drugs with well characterized clinical profiles
• Validation phase: assess model performance, using a validation set of 16 drugs with well characterized clinical profiles
Acknowledgements
University of Oxford Kylie Beattie, Ross Johnstone, Jonathan
Cooper, Martin Fink, Blanca Rodriguez, David Gavaghan, Denis Noble, Geoff Williams.
Resources Action potential prediction portal:
https://chaste.cs.ox.ac.uk/ActionPotential Cardiac Web Lab for exploring and comparing
action potential models: https://chaste.cs.ox.ac.uk/WebLab

The Next Presentation 12:10 p.m. Presentation #1
Overview of the ICH E14 Guideline and its Implementation within FDA
Christine Garnett, PharmD Clinical Analyst and QT Lead Division of Cardiovascular and Renal Products Office of Drug Evaluation I, Office of New Drugs, CDER, FDA
12:30 p.m. Presentation #2
Goals of CiPA: the Comprehensive In Vitro Proarrhythmia Assay
Gary Gintant, PhD Senior Research Fellow Department of Integrative Pharmacology Abbvie
12:50 p.m. Presentation #3
Background and Rationale for Mechanistic Cardiac Electrophysiology Models
Gary Mirams, PhD Sir Henry Dale Fellow Centre for Mathematical Medicine and Biology University of Nottingham., United Kingdom
1:05 p.m.
Presentation #4 CiPA In Silico Modeling Development Strategy and Results
Zhihua Li, PhD Staff Fellow Division of Applied Regulatory Science OCP, OTS, CDER, FDA
1:20 p.m.
Presentation #5 Phase 1 ECG Analysis under CiPA, Integration of All CiPA Components, and Potential Implementation Strategy
David Strauss, MD, PhD Division Director, Division of Applied Regulatory Science OCP, OTS, CDER, FDA





























