Embed Size (px)
Citation preview

Successes and Evolving Challenges Posed by the Comprehensive In Vitro Proarrhythmia (CiPA) Initiative
Gary Gintant
Dept. Integrative Pharmacology
Integrated Sciences and Technology
AbbVie
For the CiPA Initiative
Outline
• Introduction and Rationale for CiPA Definition and Overarching Goals Scientific Underpinnings
• Components: Progress and Challenges Ionic Currents In Silico Reconstruction Stem-Cell Derived Cardiomyocytes Compound Selection/Regulatory
• Paths Forward and Conclusions
2 CiPA – SPS Webinar April 16, 2015 © 2015
CiPA: Comprehensive In Vitro Proarrhythmia Assay
Goal: Develop a new in vitro paradigm for cardiac safety evaluation of new drugs that provides a more accurate and comprehensive mechanistic-based assessment of proarrhythmic potential
- focus on proarrhythmia (not QT prolongation) to improve specificity compared to preclinical hERG and clinical TQT studies
How? - Define drug effects on multiple human cardiac currents, - Characterize integrated electrophysiologic response using in silico reconstructions of human ventricular electrophysiology, - Verify effects on human stem-cell derived ventricular myocytes
3 CiPA – SPS Webinar April 16, 2015 © 2015
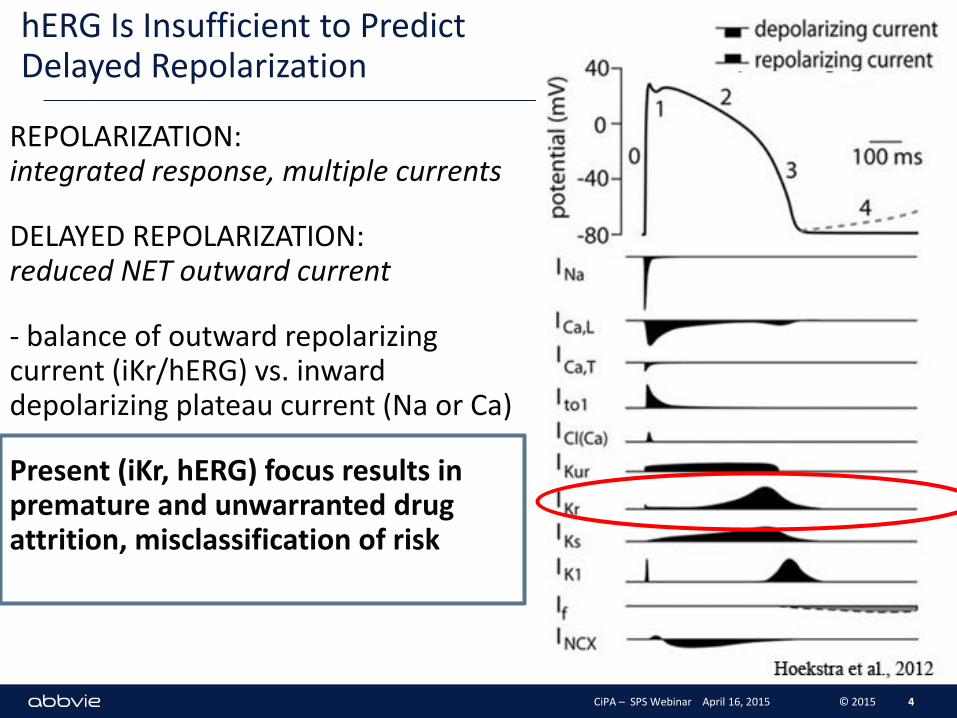
hERG Is Insufficient to Predict Delayed Repolarization
REPOLARIZATION: integrated response, multiple currents
DELAYED REPOLARIZATION: reduced NET outward current
- balance of outward repolarizing current (iKr/hERG) vs. inward depolarizing plateau current (Na or Ca)
Present (iKr, hERG) focus results in premature and unwarranted drug attrition, misclassification of risk
4 CiPA – SPS Webinar April 16, 2015 © 2015
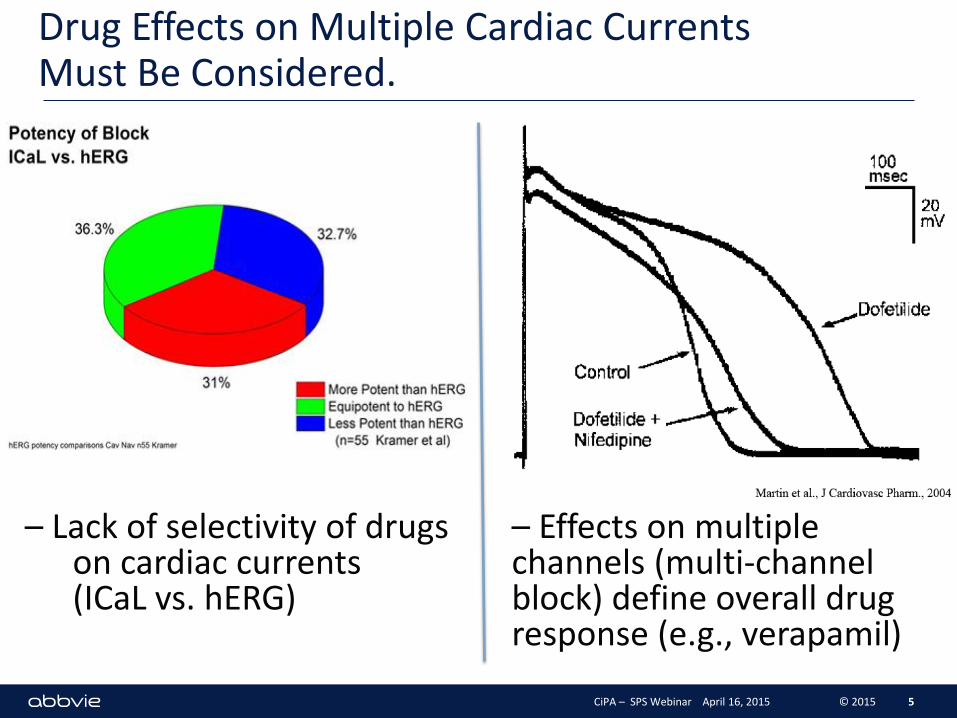
Drug Effects on Multiple Cardiac Currents Must Be Considered.
5
– Lack of selectivity of drugs on cardiac currents (ICaL vs. hERG)
– Effects on multiple channels (multi-channel block) define overall drug response (e.g., verapamil)
CiPA – SPS Webinar April 16, 2015 © 2015
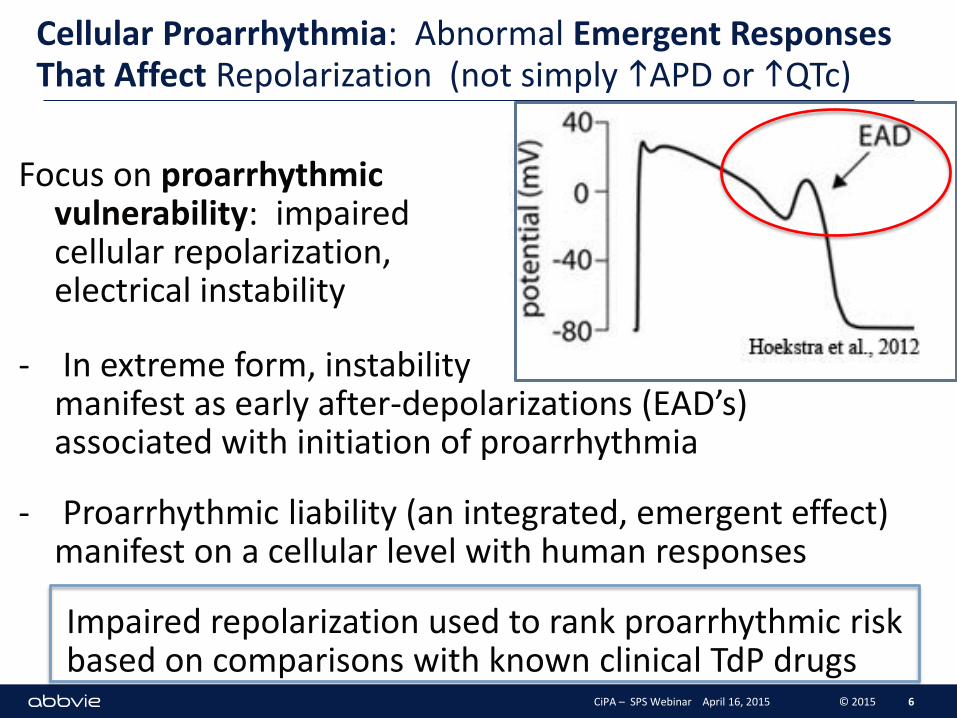
Cellular Proarrhythmia: Abnormal Emergent Responses That Affect Repolarization (not simply hAPD or hQTc)
Focus on proarrhythmic vulnerability: impaired cellular repolarization, electrical instability and l
- In extreme form, instability manifest as early after-depolarizations (EAD’s) associated with initiation of proarrhythmia
- Proarrhythmic liability (an integrated, emergent effect) manifest on a cellular level with human responses
Impaired repolarization used to rank proarrhythmic risk based on comparisons with known clinical TdP drugs
6 CiPA – SPS Webinar April 16, 2015 © 2015
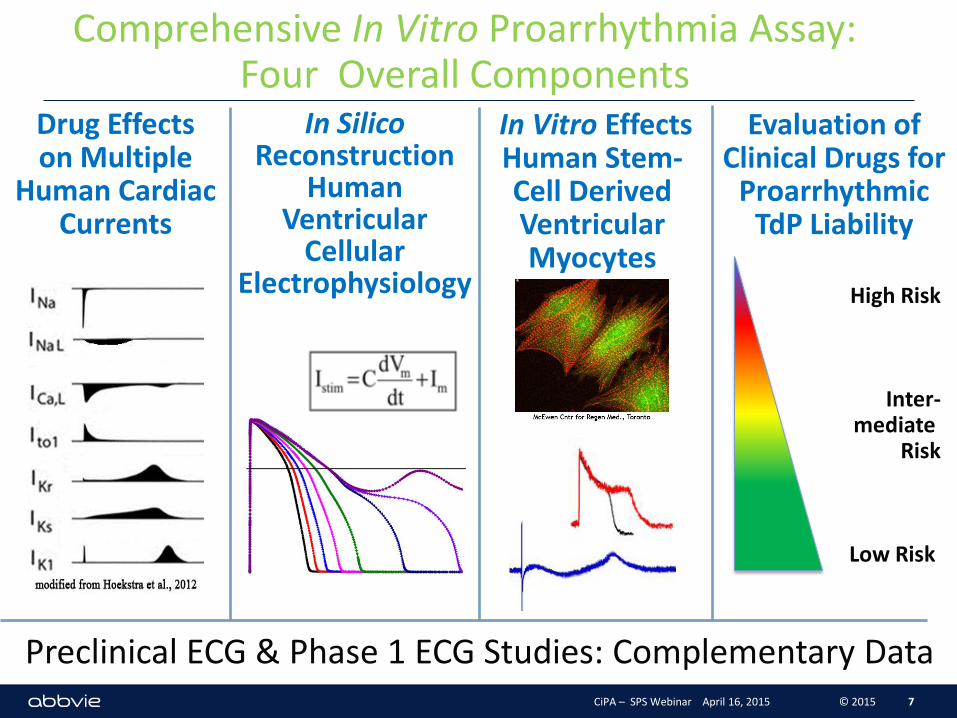
Comprehensive In Vitro Proarrhythmia Assay: Four Overall Components
Evaluation of Clinical Drugs for
Proarrhythmic TdP Liability
7
Drug Effects on Multiple
Human Cardiac Currents
In Silico Reconstruction
Human Ventricular
Cellular Electrophysiology
In Vitro Effects Human Stem-Cell Derived Ventricular Myocytes
High Risk
Inter- mediate
Risk
Low Risk
Preclinical ECG & Phase 1 ECG Studies: Complementary Data CiPA – SPS Webinar April 16, 2015 © 2015
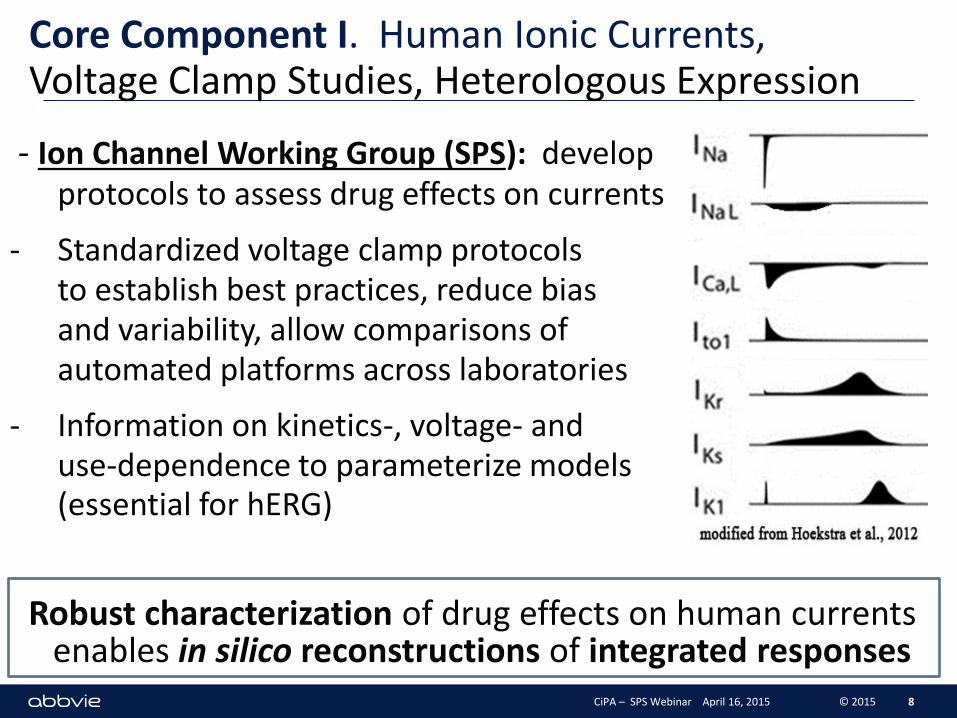
Core Component I. Human Ionic Currents, Voltage Clamp Studies, Heterologous Expression
- Ion Channel Working Group (SPS): develop protocols to assess drug effects on currents
- Standardized voltage clamp protocols to establish best practices, reduce bias and variability, allow comparisons of automated platforms across laboratories
- Information on kinetics-, voltage- and use-dependence to parameterize models for (essential for hERG)
Robust characterization of drug effects on human currents enables in silico reconstructions of integrated responses
8 CiPA – SPS Webinar April 16, 2015 © 2015
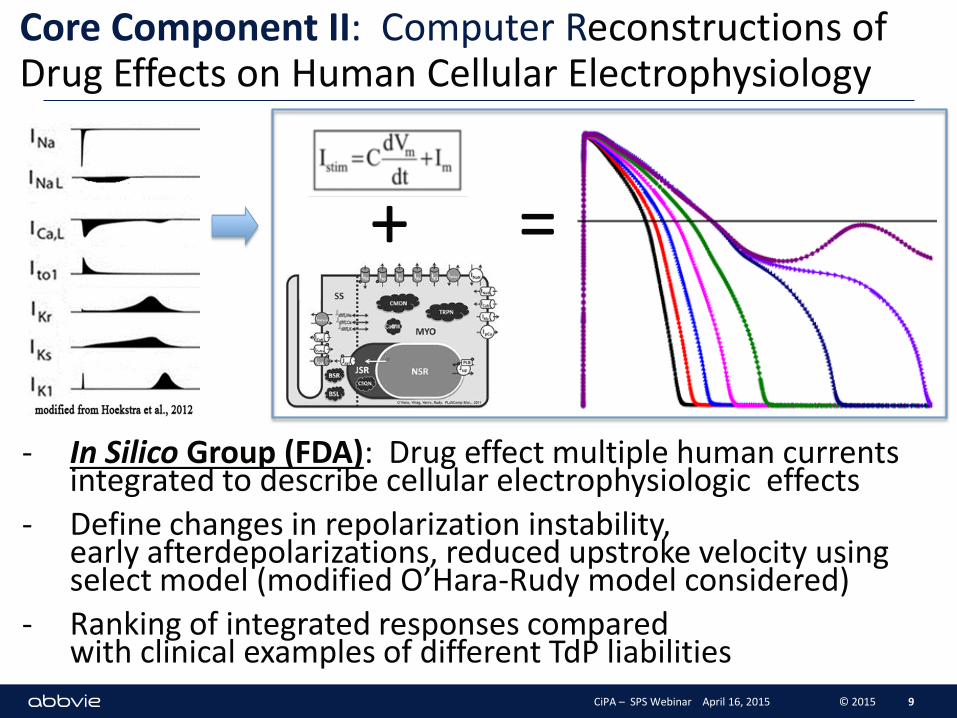
- In Silico Group (FDA): Drug effect multiple human currents integrated to describe cellular electrophysiologic effects
- Define changes in repolarization instability, early afterdepolarizations, reduced upstroke velocity using select model (modified O’Hara-Rudy model considered)
- Ranking of integrated responses compared with clinical examples of different TdP liabilities
Core Component II: Computer Reconstructions of Drug Effects on Human Cellular Electrophysiology
9
+ =
CiPA – SPS Webinar April 16, 2015 © 2015
Core Component II. Computer Reconstructions: Progress (FDA Lead)
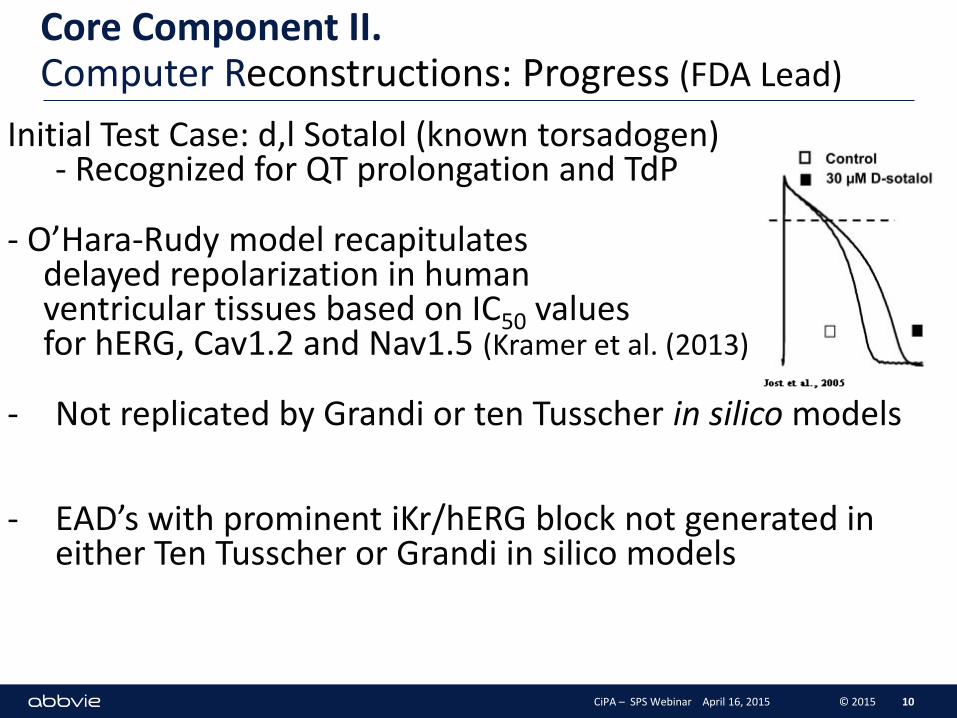
Initial Test Case: d,l Sotalol (known torsadogen) - Recognized for QT prolongation and TdP
- O’Hara-Rudy model recapitulates delayed repolarization in human ventricular tissues based on IC50 values for hERG, Cav1.2 and Nav1.5 (Kramer et al. (2013)
- Not replicated by Grandi or ten Tusscher in silico models
- EAD’s with prominent iKr/hERG block not generated in either Ten Tusscher or Grandi in silico models
10 CiPA – SPS Webinar April 16, 2015 © 2015
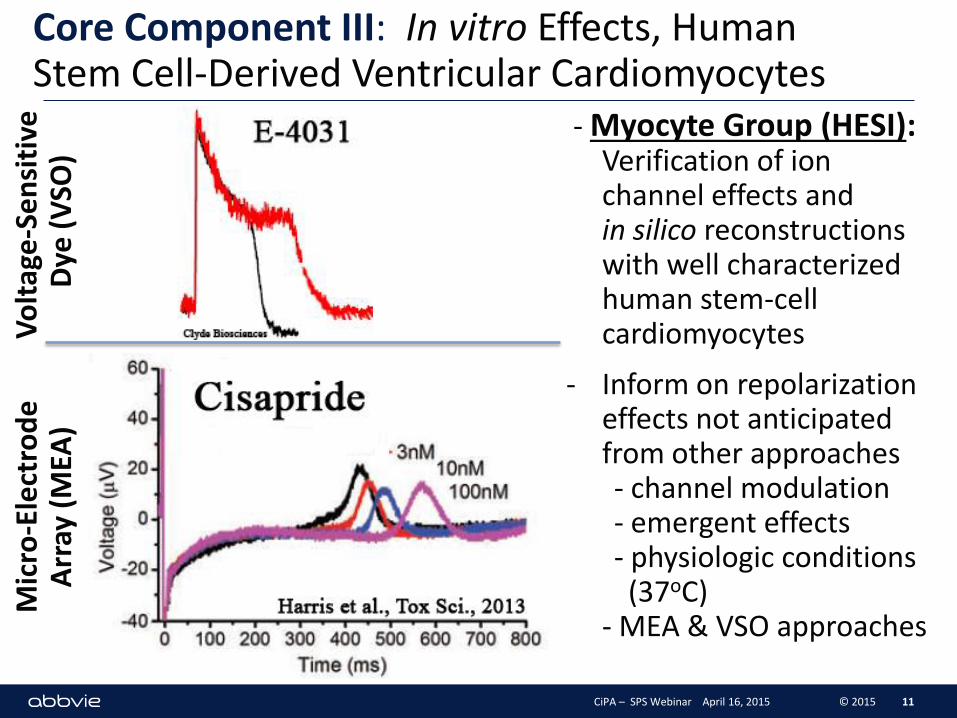
Core Component III: In vitro Effects, Human Stem Cell-Derived Ventricular Cardiomyocytes
- Myocyte Group (HESI): Verification of ion channel effects and in silico reconstructions with well characterized human stem-cell cardiomyocytes
- Inform on repolarization effects not anticipated from other approaches - channel modulation - emergent effects - physiologic conditions (37oC) - MEA & VSO approaches
11
Vo
ltag
e-S
en
siti
ve
Dye
(V
SO)
Mic
ro-E
lect
rod
e
Arr
ay (
MEA
)
CiPA – SPS Webinar April 16, 2015 © 2015
Core Component III. Cardiomyocytes- Microelectrode Array (MEA) Pilot Study
12 CiPA – SPS Webinar April 16, 2015 © 2015
12 site Pilot Study
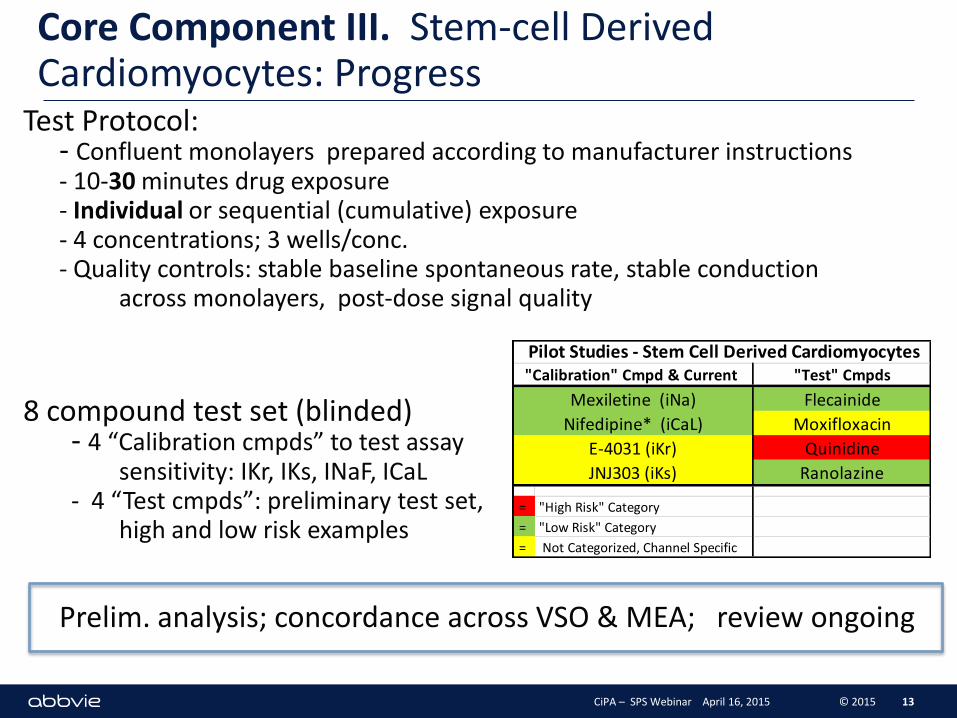
Core Component III. Stem-cell Derived Cardiomyocytes: Progress
Test Protocol: - Confluent monolayers prepared according to manufacturer instructions - 10-30 minutes drug exposure - Individual or sequential (cumulative) exposure - 4 concentrations; 3 wells/conc. - Quality controls: stable baseline spontaneous rate, stable conduction across monolayers, post-dose signal quality
8 compound test set (blinded) - 4 “Calibration cmpds” to test assay sensitivity: IKr, IKs, INaF, ICaL - 4 “Test cmpds”: preliminary test set, high and low risk examples
Prelim. analysis; concordance across VSO & MEA; review ongoing
13
"Test" Cmpds
Flecainide
Moxifloxacin
Quinidine
Ranolazine
= "High Risk" Category
= "Low Risk" Category
= Not Categorized, Channel Specific
Mexiletine (iNa)
Nifedipine* (iCaL)
E-4031 (iKr)
JNJ303 (iKs)
Pilot Studies - Stem Cell Derived Cardiomyocytes"Calibration" Cmpd & Current
CiPA – SPS Webinar April 16, 2015 © 2015
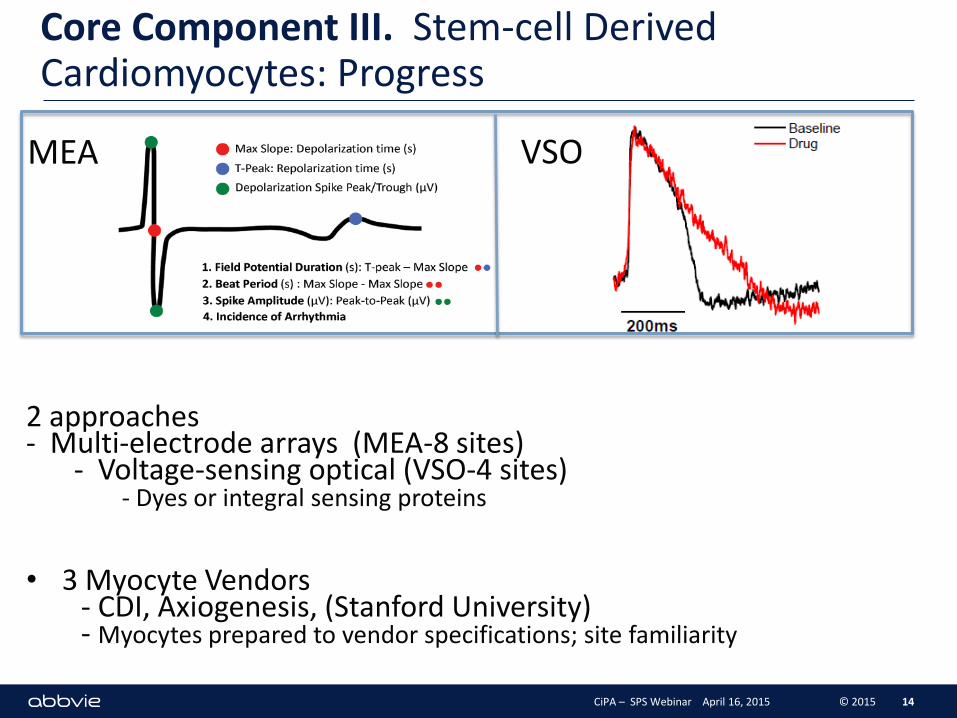
Core Component III. Stem-cell Derived Cardiomyocytes: Progress
2 approaches - Multi-electrode arrays (MEA-8 sites) - Voltage-sensing optical (VSO-4 sites) - Dyes or integral sensing proteins
• 3 Myocyte Vendors - CDI, Axiogenesis, (Stanford University) - Myocytes prepared to vendor specifications; site familiarity
14
MEA VSO
CiPA – SPS Webinar April 16, 2015 © 2015
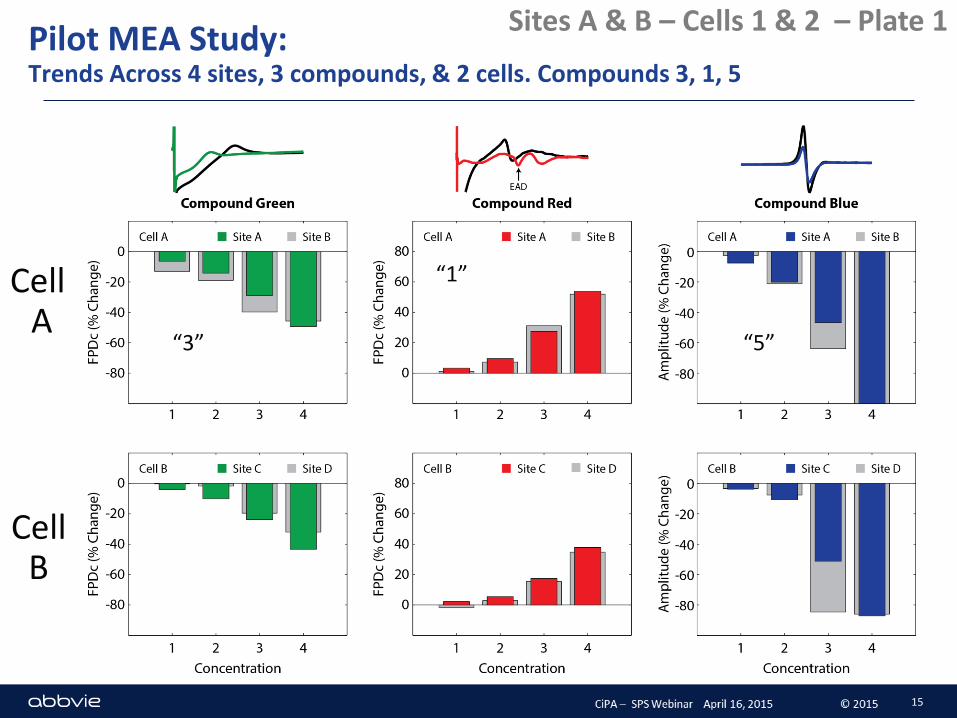
Pilot MEA Study: Trends Across 4 sites, 3 compounds, & 2 cells. Compounds 3, 1, 5
Sites A & B – Cells 1 & 2 – Plate 1
“3”
“1”
“5”
15
Cell A
Cell B
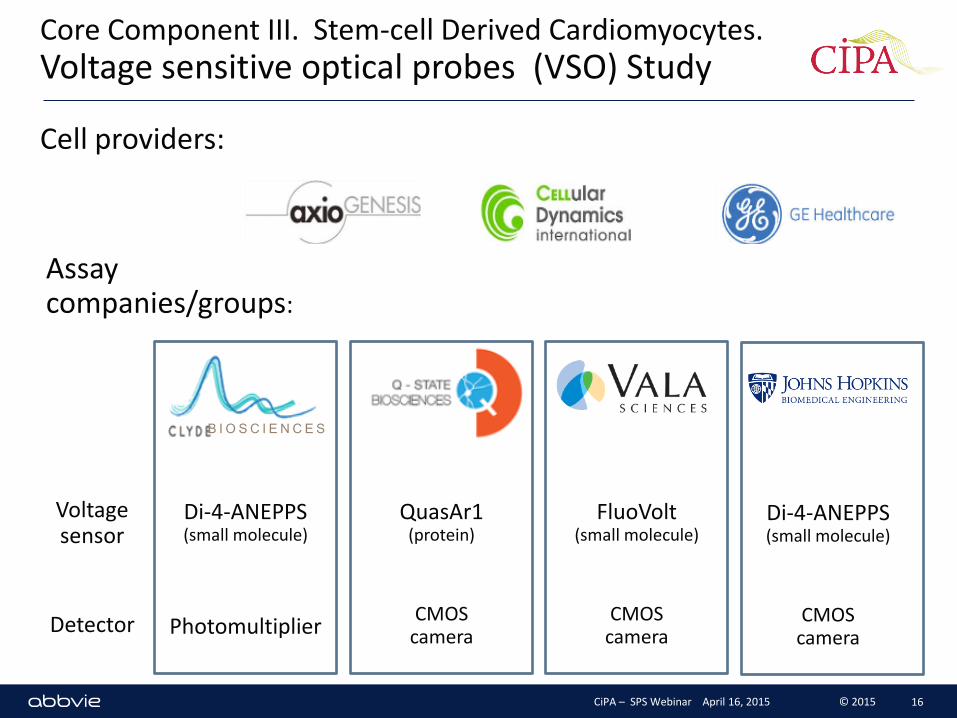
Core Component III. Stem-cell Derived Cardiomyocytes. Voltage sensitive optical probes (VSO) Study
Cell providers:
Assay companies/groups:
Voltage sensor
Detector
QuasAr1 (protein)
CMOS camera
FluoVolt (small molecule)
CMOS camera
Di-4-ANEPPS (small molecule)
CMOS camera
Di-4-ANEPPS (small molecule)
Photomultiplier
B I O S C I E N C E S
CiPA – SPS Webinar April 16, 2015 © 2015 16
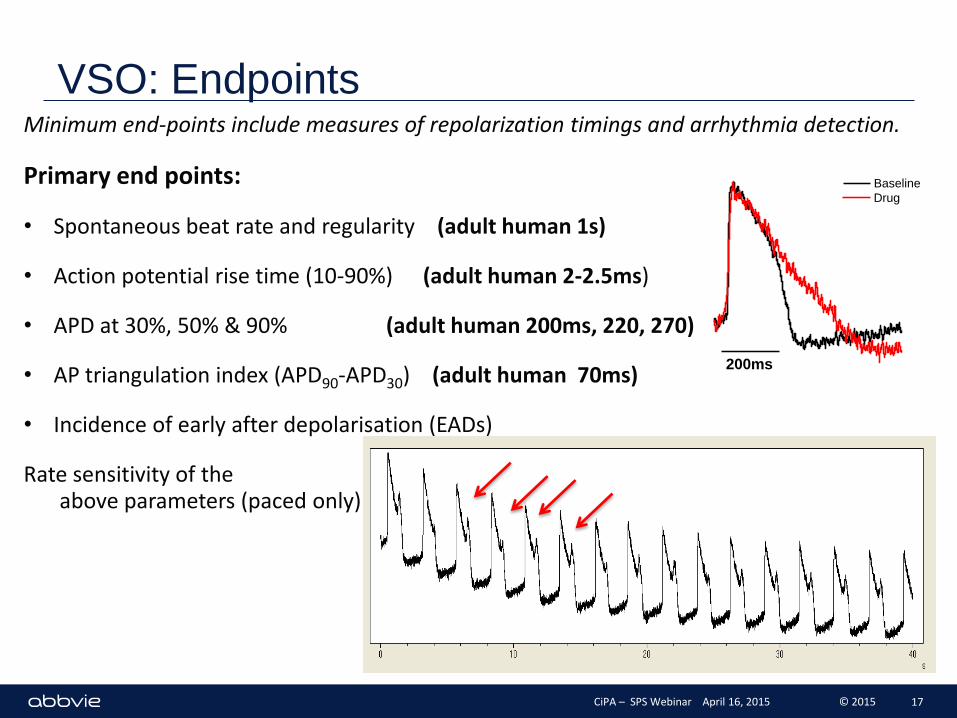
VSO: Endpoints Minimum end-points include measures of repolarization timings and arrhythmia detection.
Primary end points:
• Spontaneous beat rate and regularity (adult human 1s)
• Action potential rise time (10-90%) (adult human 2-2.5ms)
• APD at 30%, 50% & 90% (adult human 200ms, 220, 270)
• AP triangulation index (APD90-APD30) (adult human 70ms)
• Incidence of early after depolarisation (EADs)
Rate sensitivity of the above parameters (paced only)
200ms
Baseline
Drug
CiPA – SPS Webinar April 16, 2015 © 2015 17
C1_Baseline
200ms
C1_Drug
200ms
Baseline
Drug
200ms
Baseline
Drug
200ms
Baseline
Drug
100
200
300
400
500
600
700
AP
D3
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug]
C1 C2 C3 C4
100
200
300
400
500
600
700
*
*
AP
D5
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug] C1 C2 C3 C4
100
200
300
400
500
600
700
***
***
AP
D9
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug] C1 C2 C3 C4
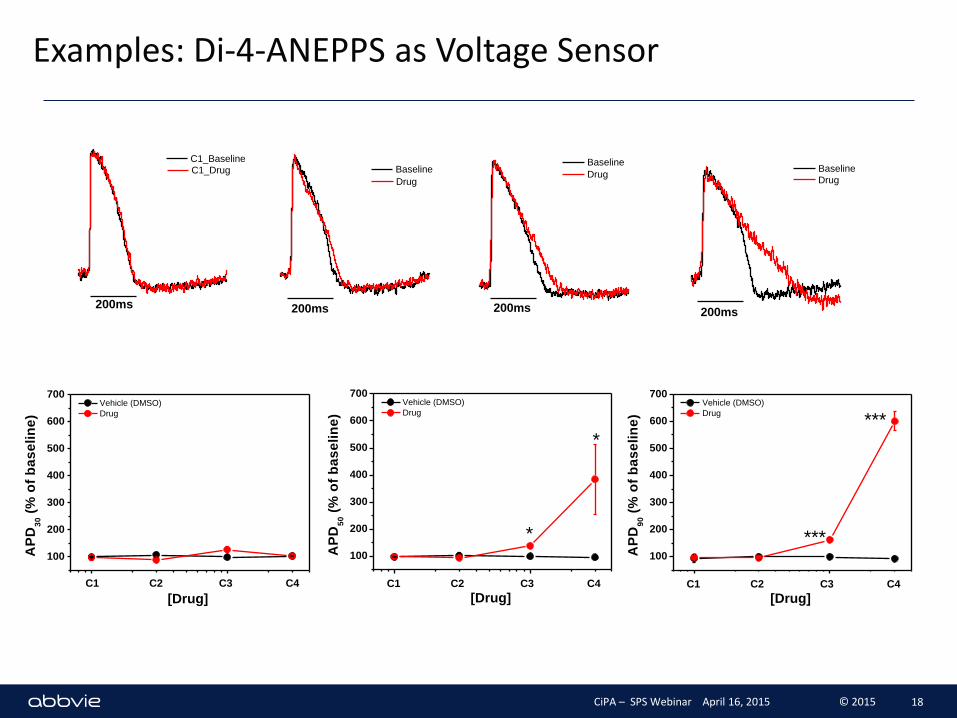
Examples: Di-4-ANEPPS as Voltage Sensor
CiPA – SPS Webinar April 16, 2015 © 2015 18
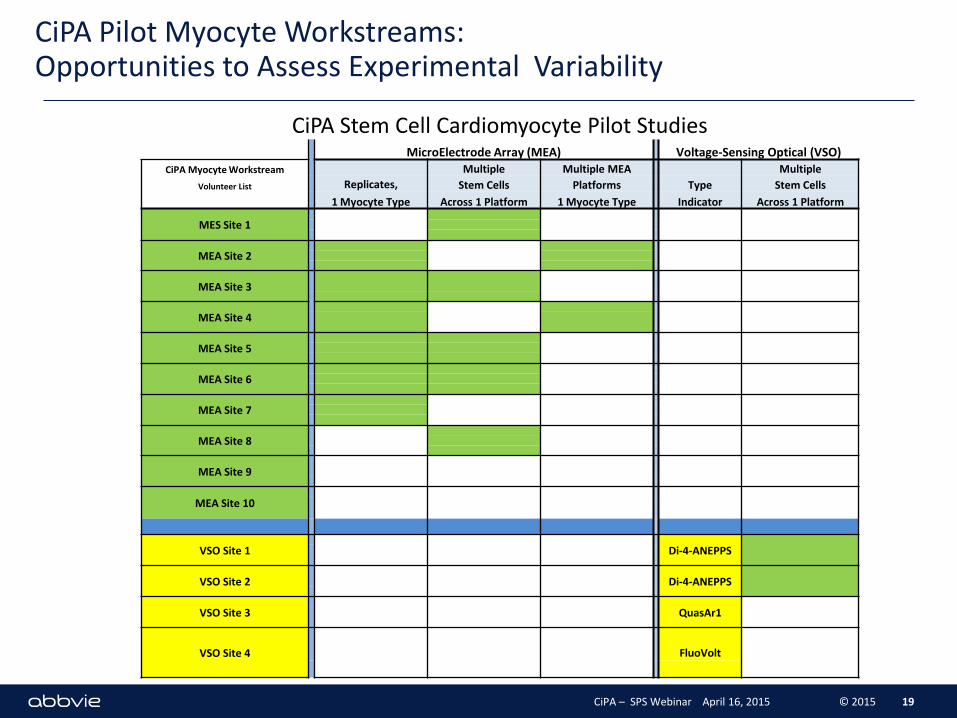
CiPA Pilot Myocyte Workstreams: Opportunities to Assess Experimental Variability
19
CiPA Stem Cell Cardiomyocyte Pilot Studies MicroElectrode Array (MEA) Voltage-Sensing Optical (VSO)
CiPA Myocyte Workstream Multiple Multiple MEA Multiple
Volunteer List Replicates, Stem Cells Platforms Type Stem Cells
1 Myocyte Type Across 1 Platform 1 Myocyte Type Indicator Across 1 Platform
MES Site 1
MEA Site 2
MEA Site 3
MEA Site 4
MEA Site 5
MEA Site 6
MEA Site 7
MEA Site 8
MEA Site 9
MEA Site 10
VSO Site 1
Di-4-ANEPPS
VSO Site 2
Di-4-ANEPPS
VSO Site 3
QuasAr1
VSO Site 4
FluoVolt
CiPA – SPS Webinar April 16, 2015 © 2015
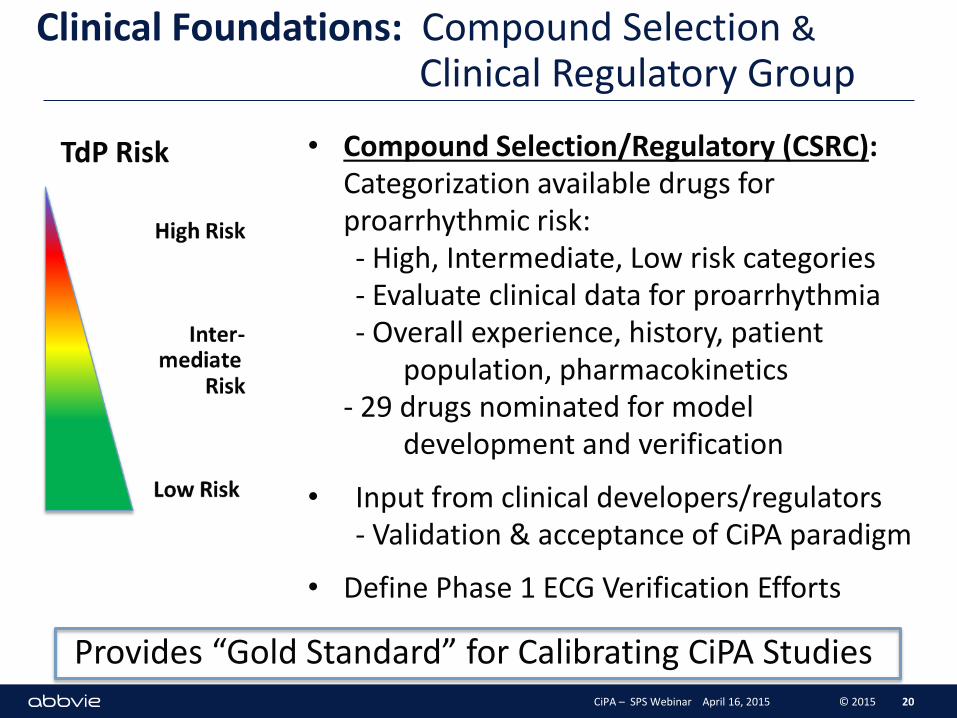
Clinical Foundations: Compound Selection & Clinical Regulatory Group
• Compound Selection/Regulatory (CSRC): Categorization available drugs for proarrhythmic risk: - High, Intermediate, Low risk categories - Evaluate clinical data for proarrhythmia - Overall experience, history, patient population, pharmacokinetics - 29 drugs nominated for model development and verification
• Input from clinical developers/regulators - Validation & acceptance of CiPA paradigm
• Define Phase 1 ECG Verification Efforts
20
TdP Risk
CiPA – SPS Webinar April 16, 2015 © 2015
Provides “Gold Standard” for Calibrating CiPA Studies
Criteria for Compound Selection
- No prominent proarrhythmic / active metabolites
- Good solubility
- Defined cellular electrophysiology
- Ranking compounds based on clinically demonstrated torsadogenic risk and proarrhythmic incidence - published reports, FDA AERS database, additional data sources, expert opinion
- Compounds grouped into ‘high’, ‘intermediate’ and ‘very low’ (i.e., none) risk categories - Intermediate risk compounds grouped into one category - ‘Very low’ risk no discernable risk
- Culled from much larger list of candidates 21 CiPA – SPS Webinar April 16, 2015 © 2015
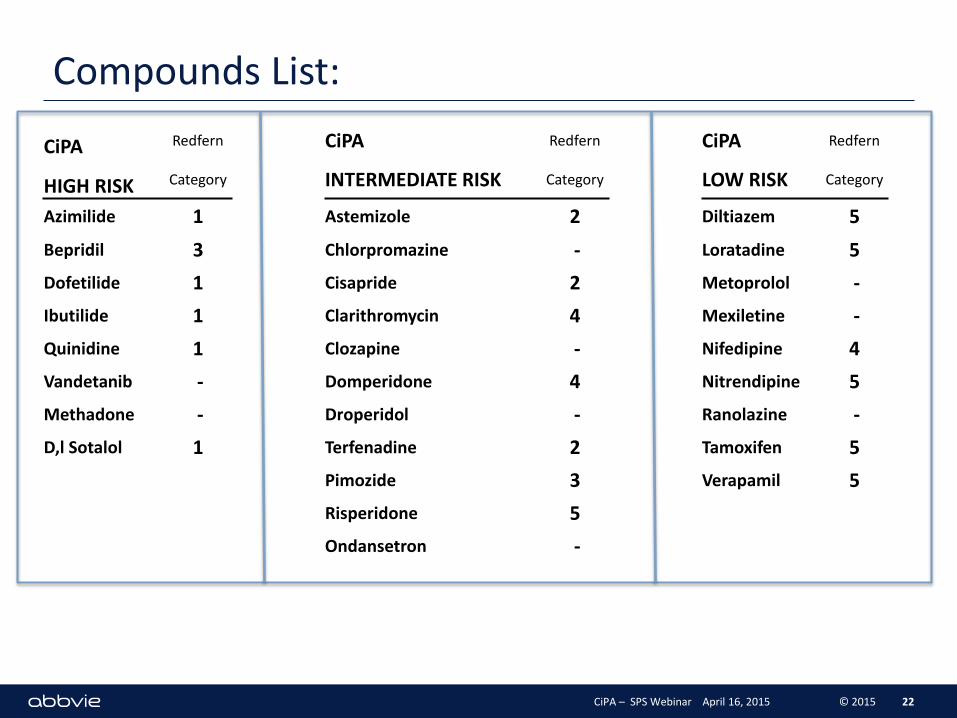
Compounds List:
22
CiPA Redfern CiPA Redfern CiPA Redfern
HIGH RISK Category INTERMEDIATE RISK Category LOW RISK Category
Azimilide 1 Astemizole 2 Diltiazem 5
Bepridil 3 Chlorpromazine - Loratadine 5
Dofetilide 1 Cisapride 2 Metoprolol -
Ibutilide 1 Clarithromycin 4 Mexiletine -
Quinidine 1 Clozapine - Nifedipine 4
Vandetanib - Domperidone 4 Nitrendipine 5
Methadone - Droperidol - Ranolazine -
D,l Sotalol 1 Terfenadine 2 Tamoxifen 5
Pimozide 3 Verapamil 5
Risperidone 5
Ondansetron -
CiPA – SPS Webinar April 16, 2015 © 2015
Group Efforts Against Timelines
Parties Involved:
Cardiac Safety Research Consortium: Cmpd Selection Team FDA: In Silico Working Group ILSI-HESI: Myocyte Stem Cell Working Group Safety Pharm. Society: Ion Channel Working Group
J-iCSA – 2015(?)
Regulators: FDA, Health Canada, EMEA, Japan Japanese Safety Pharmacology Society Academic Contributors Vendors and Suppliers
Timelines: Progress Review: 1Q 2016
23 CiPA – SPS Webinar April 16, 2015 © 2015
Future Activities: CiPA 2015
Refinement-Evaluations of Voltage Clamp Protocols
Preliminary test of In Silico Reconstructions Based on Ionic Current Studies
Assessment of CiPA Stem Cell Cardiomyocyte Pilot Study Results - Planning / Initiation of Validation Studies - Define set of validation compounds - Consult/collaborate/compare with J-iCSA
Further discussion with Regulators - Expectations of CiPA Package of regulators, industry - Relation to eQT Clinical Efforts - How to integrate in vitro/in silico preclinical results with emerging clinical eQT approaches
24 CiPA – SPS Webinar April 16, 2015 © 2015
CiPA: proarrhythmic risk assessment based on mechanistic understanding of integrated, cellular emergent drug effects on multiple human cardiac currents
Expectations: - reduce unwarranted attrition early candidates - enable rapid progression of low risk TdP drugs to phase 1 studies (and confirmatory clinical ECG findings)
25 CiPA – SPS Webinar April 16, 2015 © 2015