Embed Size (px)
Citation preview
Continuing Education
Going Viral: An Overview of Community-
Acquired Respiratory Tract Infections
Authors:
Christopher Whitman, Pharm.D. Harrison School of Pharmacy, Auburn University
Joshua Staples, Pharm.D.
Harrison School of Pharmacy, Auburn University
Samantha Rodriguez, Pharm.D. Harrison School of Pharmacy, Auburn University
Corresponding Author:
Wesley T. Lindsey, Pharm.D. Associate Clinical Professor
Drug Information and Learning Resource Center Harrison School of Pharmacy, Auburn University
Universal Activity #: 0178-0000-19-106-H04-P | 1.75 contact hours (.175 CEUs)
Initial Release Date: December 10, 2019 | Expires: October 1, 2021
Alabama Pharmacy Association | 334.271.4222 | www.aparx.org | [email protected]
4
Objectives After completing this activity, participants
should:
● Describe at least three strategies that can
be used by community pharmacists to
ensure appropriate antibiotic use in
community-acquired respiratory
infections.
● Recognize the consequences of poor
antimicrobial stewardship in the
community setting.
● Given a clinical case, identify the most
common pathogen(s) responsible for the
infection.
● Given a clinical case, identify guideline
recommended treatment strategies
including selection of the most
appropriate antibiotic, dose, and duration.
● Identify patients that qualify for
preventative vaccines.
Introduction Respiratory tract symptoms such as
congestion, sore throat, runny nose, and
cough are the most common reasons that
patients seek out physician care.1,2 Patients
may often perceive that these symptoms are
caused by infectious pathogens requiring
treatment with antibiotics. However, the vast
majority of respiratory infections are caused
by viruses which are innately resistant to
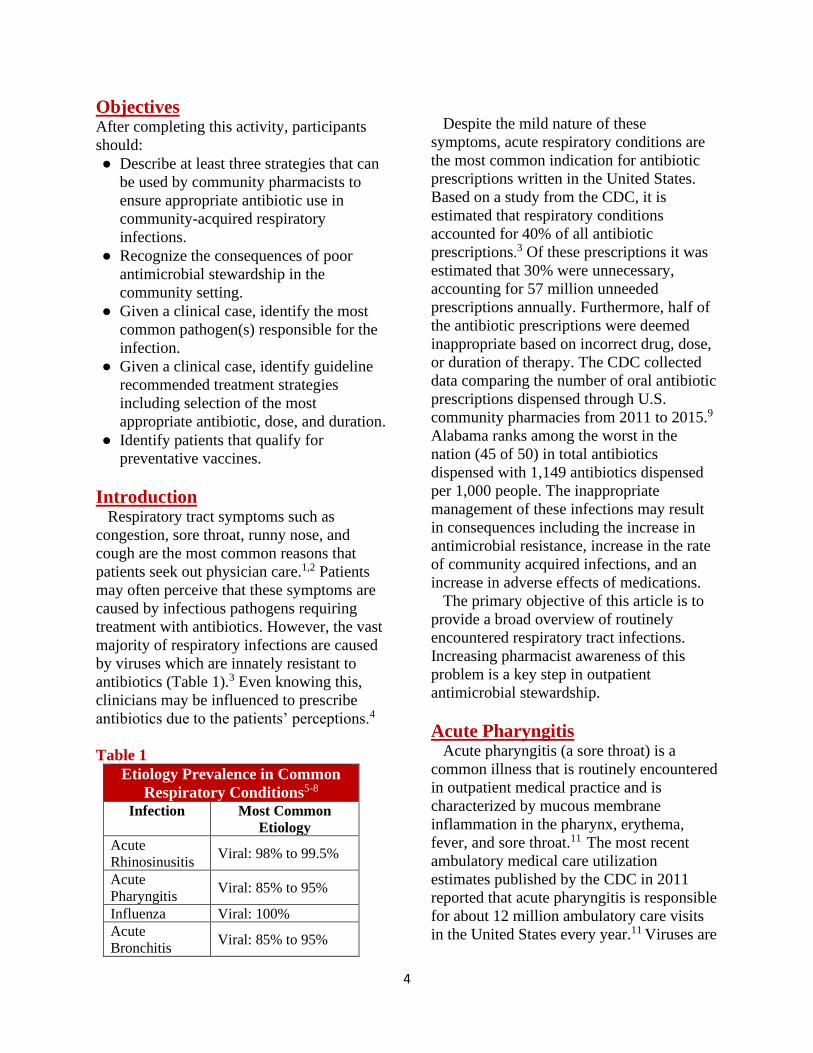
antibiotics (Table 1).3 Even knowing this,
clinicians may be influenced to prescribe
antibiotics due to the patients’ perceptions.4
Table 1
Etiology Prevalence in Common
Respiratory Conditions5-8
Infection Most Common
Etiology
Acute
Rhinosinusitis Viral: 98% to 99.5%
Acute
Pharyngitis Viral: 85% to 95%
Influenza Viral: 100%
Acute
Bronchitis Viral: 85% to 95%
Despite the mild nature of these
symptoms, acute respiratory conditions are
the most common indication for antibiotic
prescriptions written in the United States.
Based on a study from the CDC, it is
estimated that respiratory conditions
accounted for 40% of all antibiotic
prescriptions.3 Of these prescriptions it was
estimated that 30% were unnecessary,
accounting for 57 million unneeded
prescriptions annually. Furthermore, half of
the antibiotic prescriptions were deemed
inappropriate based on incorrect drug, dose,
or duration of therapy. The CDC collected
data comparing the number of oral antibiotic
prescriptions dispensed through U.S.
community pharmacies from 2011 to 2015.9
Alabama ranks among the worst in the
nation (45 of 50) in total antibiotics
dispensed with 1,149 antibiotics dispensed
per 1,000 people. The inappropriate
management of these infections may result
in consequences including the increase in
antimicrobial resistance, increase in the rate
of community acquired infections, and an
increase in adverse effects of medications.
The primary objective of this article is to
provide a broad overview of routinely
encountered respiratory tract infections.
Increasing pharmacist awareness of this
problem is a key step in outpatient
antimicrobial stewardship.
Acute Pharyngitis Acute pharyngitis (a sore throat) is a
common illness that is routinely encountered
in outpatient medical practice and is
characterized by mucous membrane
inflammation in the pharynx, erythema,
fever, and sore throat.11 The most recent
ambulatory medical care utilization
estimates published by the CDC in 2011
reported that acute pharyngitis is responsible
for about 12 million ambulatory care visits
in the United States every year.11 Viruses are
4
the primary causes of a sore throat and are
responsible for up to 95% of cases. Group A
Streptococcus (GAS pharyngitis or “Strep
Throat”) is only responsible for 5% to 15%
of adults presenting with a sore throat.6 The
incidence of GAS pharyngitis is higher in
children (20% to 30%) and is more common
during winter and spring.
Diagnosis
The causes of pharyngitis can be
characterized as either infectious (bacterial
or viral) or noninfectious.12 Physicians have
the difficult responsibility of determining
the underlying etiology of pharyngitis as it is
not possible to differentiate between
bacterial vs viral pharyngitis by simply
examining the back of the throat. The signs
and symptoms overlap between the two
etiologies, but certain clinical findings have
been identified to help distinguish bacterial
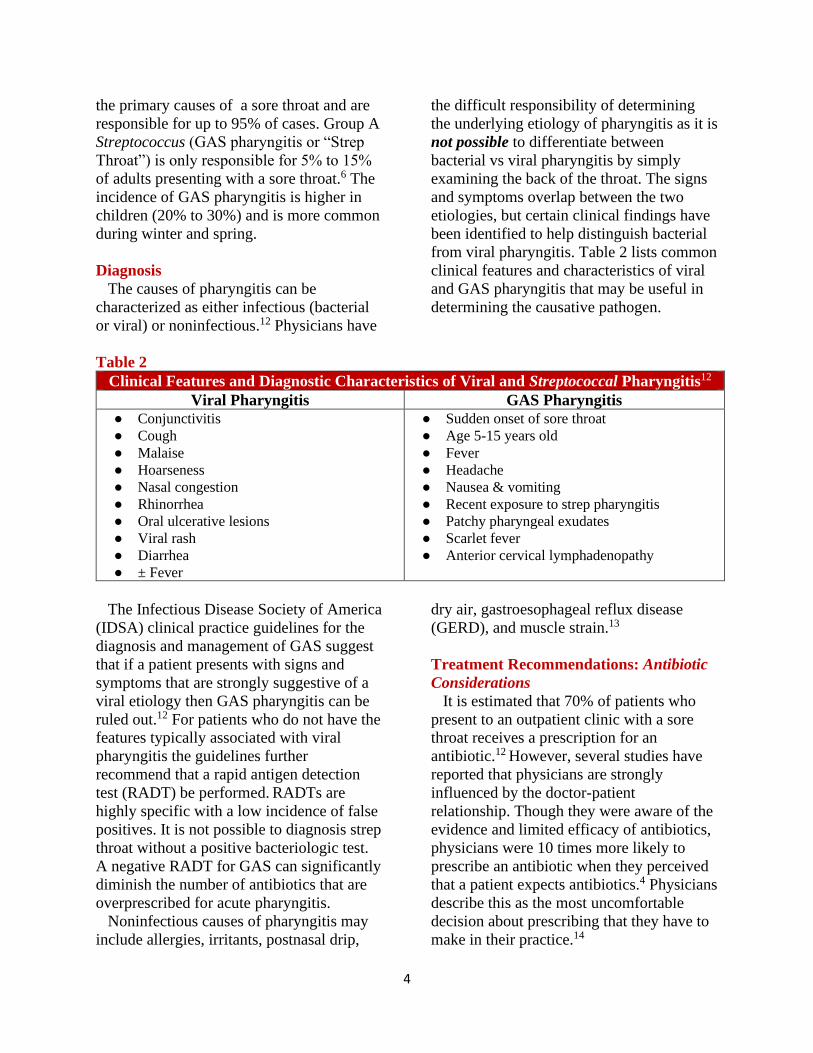
from viral pharyngitis. Table 2 lists common
clinical features and characteristics of viral
and GAS pharyngitis that may be useful in
determining the causative pathogen.
Table 2
Clinical Features and Diagnostic Characteristics of Viral and Streptococcal Pharyngitis12
Viral Pharyngitis GAS Pharyngitis
● Conjunctivitis
● Cough
● Malaise
● Hoarseness
● Nasal congestion
● Rhinorrhea
● Oral ulcerative lesions
● Viral rash
● Diarrhea
● ± Fever
● Sudden onset of sore throat
● Age 5-15 years old
● Fever
● Headache
● Nausea & vomiting
● Recent exposure to strep pharyngitis
● Patchy pharyngeal exudates
● Scarlet fever
● Anterior cervical lymphadenopathy
The Infectious Disease Society of America
(IDSA) clinical practice guidelines for the
diagnosis and management of GAS suggest
that if a patient presents with signs and
symptoms that are strongly suggestive of a
viral etiology then GAS pharyngitis can be
ruled out.12 For patients who do not have the
features typically associated with viral
pharyngitis the guidelines further
recommend that a rapid antigen detection
test (RADT) be performed. RADTs are
highly specific with a low incidence of false
positives. It is not possible to diagnosis strep
throat without a positive bacteriologic test.
A negative RADT for GAS can significantly
diminish the number of antibiotics that are
overprescribed for acute pharyngitis.
Noninfectious causes of pharyngitis may
include allergies, irritants, postnasal drip,
dry air, gastroesophageal reflux disease
(GERD), and muscle strain.13
Treatment Recommendations: Antibiotic
Considerations
It is estimated that 70% of patients who
present to an outpatient clinic with a sore
throat receives a prescription for an
antibiotic.12 However, several studies have
reported that physicians are strongly
influenced by the doctor-patient
relationship. Though they were aware of the
evidence and limited efficacy of antibiotics,
physicians were 10 times more likely to
prescribe an antibiotic when they perceived
that a patient expects antibiotics.4 Physicians
describe this as the most uncomfortable
decision about prescribing that they have to
make in their practice.14
5
The IDSA and the American Heart
Association provide similar
recommendations regarding the treatment of
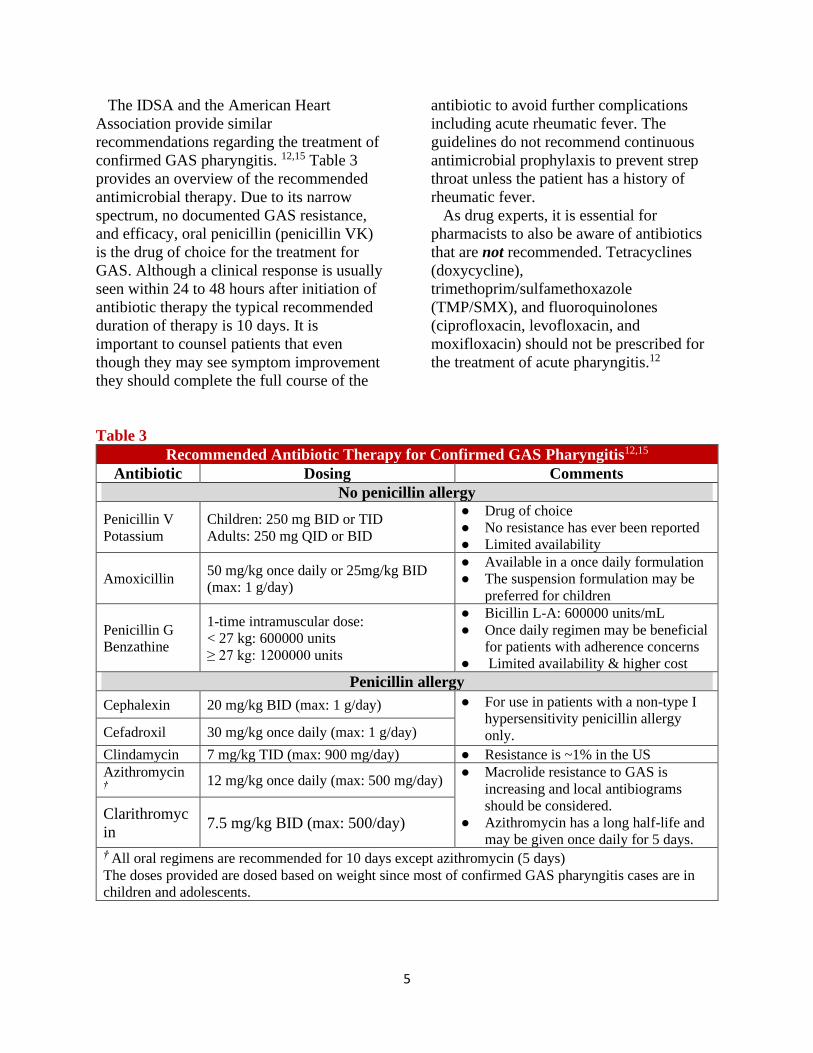
confirmed GAS pharyngitis. 12,15 Table 3
provides an overview of the recommended
antimicrobial therapy. Due to its narrow
spectrum, no documented GAS resistance,
and efficacy, oral penicillin (penicillin VK)
is the drug of choice for the treatment for
GAS. Although a clinical response is usually
seen within 24 to 48 hours after initiation of
antibiotic therapy the typical recommended
duration of therapy is 10 days. It is
important to counsel patients that even
though they may see symptom improvement
they should complete the full course of the
antibiotic to avoid further complications
including acute rheumatic fever. The
guidelines do not recommend continuous
antimicrobial prophylaxis to prevent strep
throat unless the patient has a history of
rheumatic fever.
As drug experts, it is essential for
pharmacists to also be aware of antibiotics
that are not recommended. Tetracyclines
(doxycycline),
trimethoprim/sulfamethoxazole
(TMP/SMX), and fluoroquinolones
(ciprofloxacin, levofloxacin, and
moxifloxacin) should not be prescribed for
the treatment of acute pharyngitis.12
Table 3
Recommended Antibiotic Therapy for Confirmed GAS Pharyngitis12,15
Antibiotic Dosing Comments
No penicillin allergy
Penicillin V
Potassium
Children: 250 mg BID or TID
Adults: 250 mg QID or BID
● Drug of choice
● No resistance has ever been reported
● Limited availability
Amoxicillin 50 mg/kg once daily or 25mg/kg BID
(max: 1 g/day)
● Available in a once daily formulation
● The suspension formulation may be
preferred for children
Penicillin G
Benzathine
1-time intramuscular dose:
< 27 kg: 600000 units
≥ 27 kg: 1200000 units
● Bicillin L-A: 600000 units/mL
● Once daily regimen may be beneficial
for patients with adherence concerns
● Limited availability & higher cost
Penicillin allergy
Cephalexin 20 mg/kg BID (max: 1 g/day) ● For use in patients with a non-type I
hypersensitivity penicillin allergy
only. Cefadroxil 30 mg/kg once daily (max: 1 g/day)
Clindamycin 7 mg/kg TID (max: 900 mg/day) ● Resistance is ~1% in the US
Azithromycin †
12 mg/kg once daily (max: 500 mg/day) ● Macrolide resistance to GAS is
increasing and local antibiograms
should be considered.
● Azithromycin has a long half-life and
may be given once daily for 5 days.
Clarithromyc
in 7.5 mg/kg BID (max: 500/day)
† All oral regimens are recommended for 10 days except azithromycin (5 days)
The doses provided are dosed based on weight since most of confirmed GAS pharyngitis cases are in
children and adolescents.
6
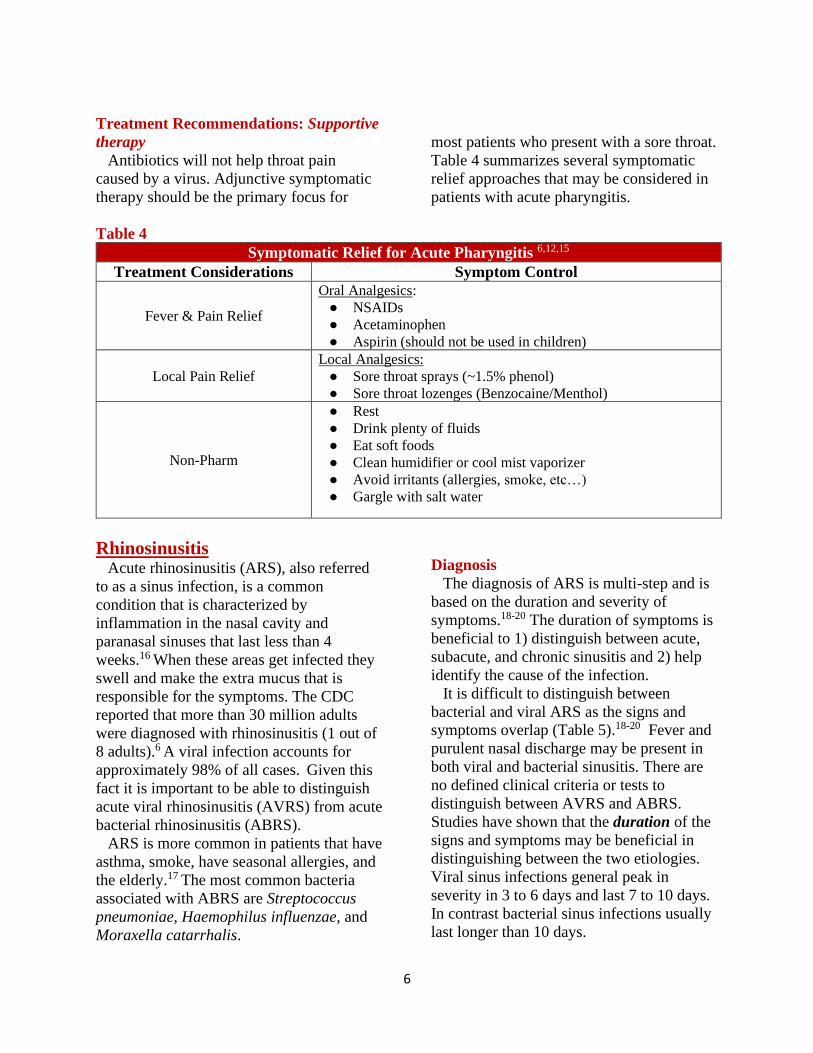
Treatment Recommendations: Supportive
therapy
Antibiotics will not help throat pain
caused by a virus. Adjunctive symptomatic
therapy should be the primary focus for
most patients who present with a sore throat.
Table 4 summarizes several symptomatic
relief approaches that may be considered in
patients with acute pharyngitis.
Table 4
Symptomatic Relief for Acute Pharyngitis 6,12,15
Treatment Considerations Symptom Control
Fever & Pain Relief
Oral Analgesics:
● NSAIDs
● Acetaminophen
● Aspirin (should not be used in children)
Local Pain Relief
Local Analgesics:
● Sore throat sprays (~1.5% phenol)
● Sore throat lozenges (Benzocaine/Menthol)
Non-Pharm
● Rest
● Drink plenty of fluids
● Eat soft foods
● Clean humidifier or cool mist vaporizer
● Avoid irritants (allergies, smoke, etc…)
● Gargle with salt water
Rhinosinusitis Acute rhinosinusitis (ARS), also referred
to as a sinus infection, is a common
condition that is characterized by
inflammation in the nasal cavity and
paranasal sinuses that last less than 4
weeks.16 When these areas get infected they
swell and make the extra mucus that is
responsible for the symptoms. The CDC
reported that more than 30 million adults
were diagnosed with rhinosinusitis (1 out of
8 adults).6 A viral infection accounts for
approximately 98% of all cases. Given this
fact it is important to be able to distinguish
acute viral rhinosinusitis (AVRS) from acute
bacterial rhinosinusitis (ABRS).
ARS is more common in patients that have
asthma, smoke, have seasonal allergies, and
the elderly.17 The most common bacteria
associated with ABRS are Streptococcus
pneumoniae, Haemophilus influenzae, and
Moraxella catarrhalis.
Diagnosis
The diagnosis of ARS is multi-step and is
based on the duration and severity of
symptoms.18-20 The duration of symptoms is
beneficial to 1) distinguish between acute,
subacute, and chronic sinusitis and 2) help
identify the cause of the infection.
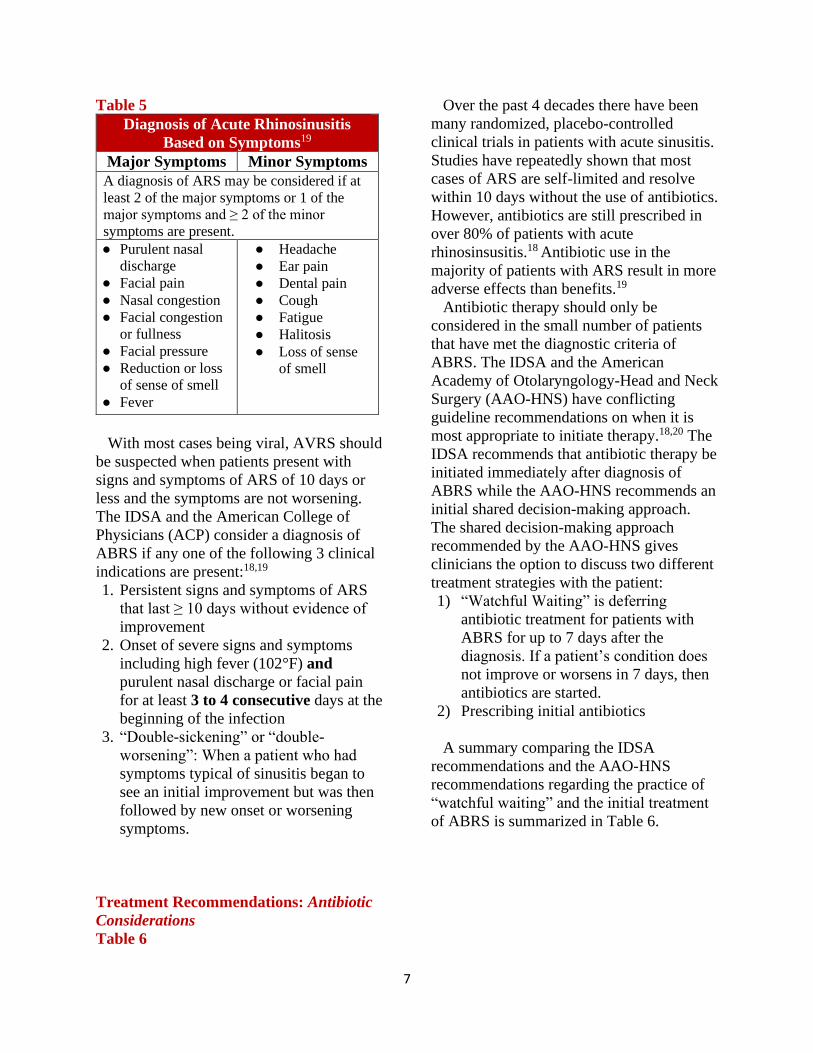
It is difficult to distinguish between
bacterial and viral ARS as the signs and
symptoms overlap (Table 5).18-20 Fever and
purulent nasal discharge may be present in
both viral and bacterial sinusitis. There are
no defined clinical criteria or tests to
distinguish between AVRS and ABRS.
Studies have shown that the duration of the
signs and symptoms may be beneficial in
distinguishing between the two etiologies.
Viral sinus infections general peak in
severity in 3 to 6 days and last 7 to 10 days.
In contrast bacterial sinus infections usually
last longer than 10 days.
7
Table 5
Diagnosis of Acute Rhinosinusitis
Based on Symptoms19
Major Symptoms Minor Symptoms
A diagnosis of ARS may be considered if at
least 2 of the major symptoms or 1 of the
major symptoms and ≥ 2 of the minor
symptoms are present.
● Purulent nasal
discharge
● Facial pain
● Nasal congestion
● Facial congestion
or fullness
● Facial pressure
● Reduction or loss
of sense of smell
● Fever
● Headache
● Ear pain
● Dental pain
● Cough
● Fatigue
● Halitosis
● Loss of sense
of smell
With most cases being viral, AVRS should
be suspected when patients present with
signs and symptoms of ARS of 10 days or
less and the symptoms are not worsening.
The IDSA and the American College of
Physicians (ACP) consider a diagnosis of
ABRS if any one of the following 3 clinical
indications are present:18,19
1. Persistent signs and symptoms of ARS
that last ≥ 10 days without evidence of
improvement
2. Onset of severe signs and symptoms
including high fever (102°F) and
purulent nasal discharge or facial pain
for at least 3 to 4 consecutive days at the
beginning of the infection
3. “Double-sickening” or “double-
worsening”: When a patient who had
symptoms typical of sinusitis began to
see an initial improvement but was then
followed by new onset or worsening
symptoms.
Treatment Recommendations: Antibiotic
Considerations
Over the past 4 decades there have been
many randomized, placebo-controlled
clinical trials in patients with acute sinusitis.
Studies have repeatedly shown that most
cases of ARS are self-limited and resolve
within 10 days without the use of antibiotics.
However, antibiotics are still prescribed in
over 80% of patients with acute
rhinosinsusitis.18 Antibiotic use in the
majority of patients with ARS result in more
adverse effects than benefits.19
Antibiotic therapy should only be
considered in the small number of patients
that have met the diagnostic criteria of
ABRS. The IDSA and the American
Academy of Otolaryngology-Head and Neck
Surgery (AAO-HNS) have conflicting
guideline recommendations on when it is
most appropriate to initiate therapy.18,20 The
IDSA recommends that antibiotic therapy be
initiated immediately after diagnosis of
ABRS while the AAO-HNS recommends an
initial shared decision-making approach.
The shared decision-making approach
recommended by the AAO-HNS gives
clinicians the option to discuss two different
treatment strategies with the patient:
1) “Watchful Waiting” is deferring
antibiotic treatment for patients with
ABRS for up to 7 days after the
diagnosis. If a patient’s condition does
not improve or worsens in 7 days, then
antibiotics are started.
2) Prescribing initial antibiotics
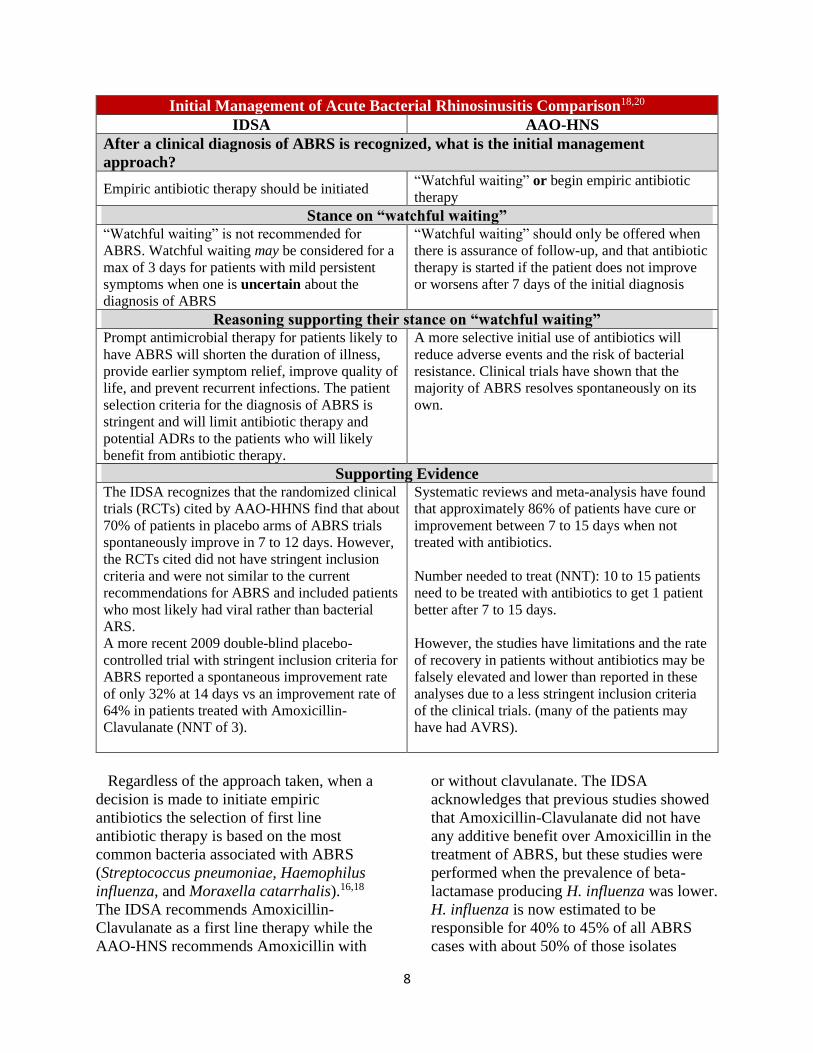
A summary comparing the IDSA
recommendations and the AAO-HNS
recommendations regarding the practice of
“watchful waiting” and the initial treatment
of ABRS is summarized in Table 6.
Table 6
8
Initial Management of Acute Bacterial Rhinosinusitis Comparison18,20
IDSA AAO-HNS
After a clinical diagnosis of ABRS is recognized, what is the initial management
approach?
Empiric antibiotic therapy should be initiated “Watchful waiting” or begin empiric antibiotic
therapy
Stance on “watchful waiting” “Watchful waiting” is not recommended for
ABRS. Watchful waiting may be considered for a
max of 3 days for patients with mild persistent
symptoms when one is uncertain about the
diagnosis of ABRS
“Watchful waiting” should only be offered when
there is assurance of follow-up, and that antibiotic
therapy is started if the patient does not improve
or worsens after 7 days of the initial diagnosis
Reasoning supporting their stance on “watchful waiting” Prompt antimicrobial therapy for patients likely to
have ABRS will shorten the duration of illness,
provide earlier symptom relief, improve quality of
life, and prevent recurrent infections. The patient
selection criteria for the diagnosis of ABRS is
stringent and will limit antibiotic therapy and
potential ADRs to the patients who will likely
benefit from antibiotic therapy.
A more selective initial use of antibiotics will
reduce adverse events and the risk of bacterial
resistance. Clinical trials have shown that the
majority of ABRS resolves spontaneously on its
own.
Supporting Evidence The IDSA recognizes that the randomized clinical
trials (RCTs) cited by AAO-HHNS find that about
70% of patients in placebo arms of ABRS trials
spontaneously improve in 7 to 12 days. However,
the RCTs cited did not have stringent inclusion
criteria and were not similar to the current
recommendations for ABRS and included patients
who most likely had viral rather than bacterial
ARS.
A more recent 2009 double-blind placebo-
controlled trial with stringent inclusion criteria for
ABRS reported a spontaneous improvement rate
of only 32% at 14 days vs an improvement rate of
64% in patients treated with Amoxicillin-
Clavulanate (NNT of 3).
Systematic reviews and meta-analysis have found
that approximately 86% of patients have cure or
improvement between 7 to 15 days when not
treated with antibiotics.
Number needed to treat (NNT): 10 to 15 patients
need to be treated with antibiotics to get 1 patient
better after 7 to 15 days.
However, the studies have limitations and the rate
of recovery in patients without antibiotics may be
falsely elevated and lower than reported in these
analyses due to a less stringent inclusion criteria
of the clinical trials. (many of the patients may
have had AVRS).
Regardless of the approach taken, when a
decision is made to initiate empiric
antibiotics the selection of first line
antibiotic therapy is based on the most
common bacteria associated with ABRS
(Streptococcus pneumoniae, Haemophilus
influenza, and Moraxella catarrhalis).16,18
The IDSA recommends Amoxicillin-
Clavulanate as a first line therapy while the
AAO-HNS recommends Amoxicillin with
or without clavulanate. The IDSA
acknowledges that previous studies showed
that Amoxicillin-Clavulanate did not have
any additive benefit over Amoxicillin in the
treatment of ABRS, but these studies were
performed when the prevalence of beta-
lactamase producing H. influenza was lower.
H. influenza is now estimated to be
responsible for 40% to 45% of all ABRS
cases with about 50% of those isolates
9
producing beta lactamases. Amoxicillin
alone would not be effective compared to a
beta-lactamase producing H. influenza. The
benefit of adding clavulanate provides
greater coverage and efficacy but carries the
risk of increased ADRs.
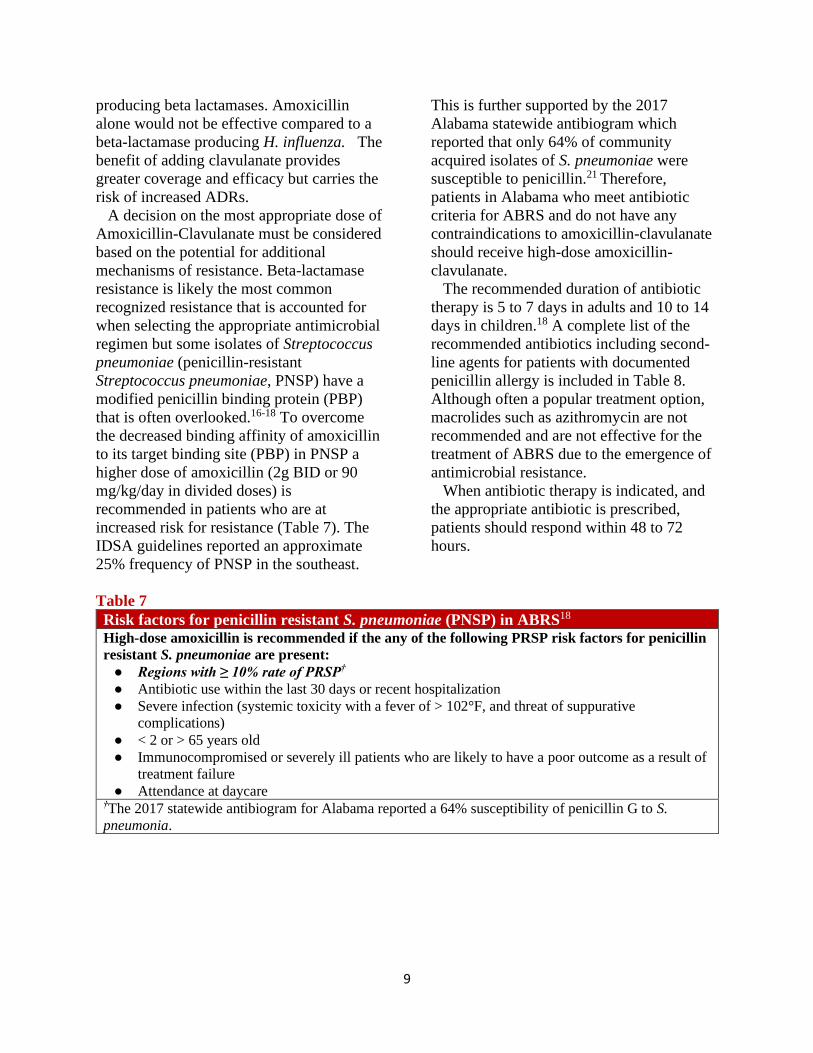
A decision on the most appropriate dose of
Amoxicillin-Clavulanate must be considered
based on the potential for additional
mechanisms of resistance. Beta-lactamase
resistance is likely the most common
recognized resistance that is accounted for
when selecting the appropriate antimicrobial
regimen but some isolates of Streptococcus
pneumoniae (penicillin-resistant
Streptococcus pneumoniae, PNSP) have a
modified penicillin binding protein (PBP)
that is often overlooked.16-18 To overcome
the decreased binding affinity of amoxicillin
to its target binding site (PBP) in PNSP a
higher dose of amoxicillin (2g BID or 90
mg/kg/day in divided doses) is
recommended in patients who are at
increased risk for resistance (Table 7). The
IDSA guidelines reported an approximate
25% frequency of PNSP in the southeast.
This is further supported by the 2017
Alabama statewide antibiogram which
reported that only 64% of community
acquired isolates of S. pneumoniae were
susceptible to penicillin.21 Therefore,
patients in Alabama who meet antibiotic
criteria for ABRS and do not have any
contraindications to amoxicillin-clavulanate
should receive high-dose amoxicillin-
clavulanate.
The recommended duration of antibiotic
therapy is 5 to 7 days in adults and 10 to 14
days in children.18 A complete list of the
recommended antibiotics including second-
line agents for patients with documented
penicillin allergy is included in Table 8.
Although often a popular treatment option,
macrolides such as azithromycin are not
recommended and are not effective for the
treatment of ABRS due to the emergence of
antimicrobial resistance.
When antibiotic therapy is indicated, and
the appropriate antibiotic is prescribed,
patients should respond within 48 to 72
hours.
Table 7
Risk factors for penicillin resistant S. pneumoniae (PNSP) in ABRS18
High-dose amoxicillin is recommended if the any of the following PRSP risk factors for penicillin
resistant S. pneumoniae are present:
● Regions with ≥ 10% rate of PRSP†
● Antibiotic use within the last 30 days or recent hospitalization
● Severe infection (systemic toxicity with a fever of > 102°F, and threat of suppurative
complications)
● < 2 or > 65 years old
● Immunocompromised or severely ill patients who are likely to have a poor outcome as a result of
treatment failure
● Attendance at daycare †The 2017 statewide antibiogram for Alabama reported a 64% susceptibility of penicillin G to S.
pneumonia.
10
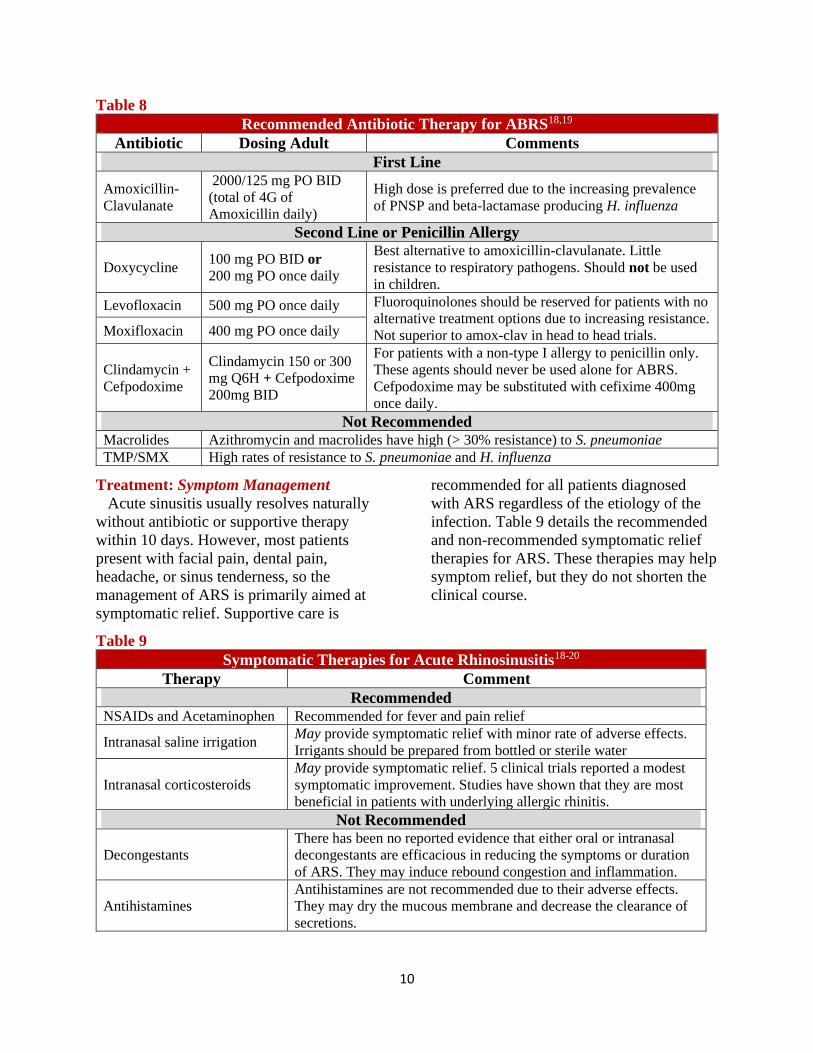
Table 8
Recommended Antibiotic Therapy for ABRS18,19
Antibiotic Dosing Adult Comments
First Line
Amoxicillin-
Clavulanate
2000/125 mg PO BID
(total of 4G of
Amoxicillin daily)
High dose is preferred due to the increasing prevalence
of PNSP and beta-lactamase producing H. influenza
Second Line or Penicillin Allergy
Doxycycline 100 mg PO BID or
200 mg PO once daily
Best alternative to amoxicillin-clavulanate. Little
resistance to respiratory pathogens. Should not be used
in children.
Levofloxacin 500 mg PO once daily Fluoroquinolones should be reserved for patients with no
alternative treatment options due to increasing resistance.
Not superior to amox-clav in head to head trials. Moxifloxacin 400 mg PO once daily
Clindamycin +
Cefpodoxime
Clindamycin 150 or 300
mg Q6H + Cefpodoxime
200mg BID
For patients with a non-type I allergy to penicillin only.
These agents should never be used alone for ABRS.
Cefpodoxime may be substituted with cefixime 400mg
once daily.
Not Recommended Macrolides Azithromycin and macrolides have high (> 30% resistance) to S. pneumoniae
TMP/SMX High rates of resistance to S. pneumoniae and H. influenza
Treatment: Symptom Management
Acute sinusitis usually resolves naturally
without antibiotic or supportive therapy
within 10 days. However, most patients
present with facial pain, dental pain,
headache, or sinus tenderness, so the
management of ARS is primarily aimed at
symptomatic relief. Supportive care is
recommended for all patients diagnosed
with ARS regardless of the etiology of the
infection. Table 9 details the recommended
and non-recommended symptomatic relief
therapies for ARS. These therapies may help
symptom relief, but they do not shorten the
clinical course.
Table 9
Symptomatic Therapies for Acute Rhinosinusitis18-20
Therapy Comment
Recommended
NSAIDs and Acetaminophen Recommended for fever and pain relief
Intranasal saline irrigation May provide symptomatic relief with minor rate of adverse effects.
Irrigants should be prepared from bottled or sterile water
Intranasal corticosteroids
May provide symptomatic relief. 5 clinical trials reported a modest
symptomatic improvement. Studies have shown that they are most
beneficial in patients with underlying allergic rhinitis.
Not Recommended
Decongestants
There has been no reported evidence that either oral or intranasal
decongestants are efficacious in reducing the symptoms or duration
of ARS. They may induce rebound congestion and inflammation.
Antihistamines
Antihistamines are not recommended due to their adverse effects.
They may dry the mucous membrane and decrease the clearance of
secretions.
11
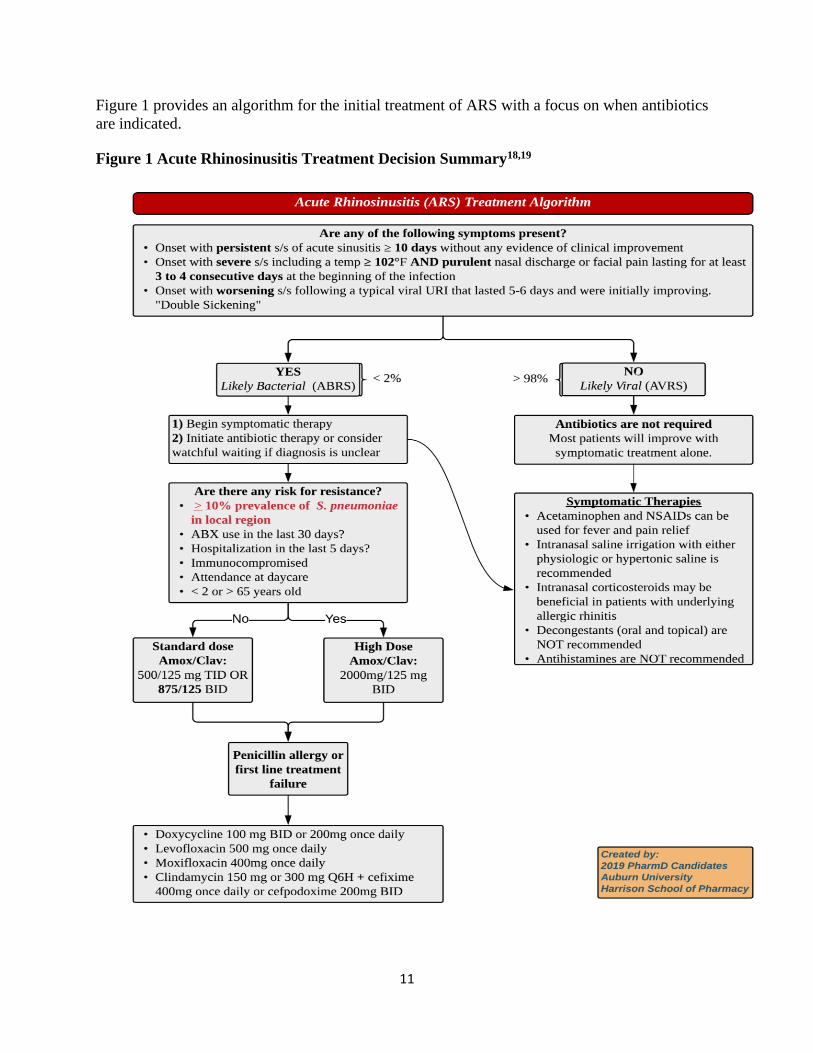
Figure 1 provides an algorithm for the initial treatment of ARS with a focus on when antibiotics
are indicated.
Figure 1 Acute Rhinosinusitis Treatment Decision Summary18,19
12
Community Acquired Pneumonia Overview of Disease State
Pneumonia is an infection of the lung
parenchyma.22 It is one of the most common
causes of severe sepsis and death in the
United States with a mortality rate of 30 to
40%.8 Community acquired pneumonia
(CAP) can be caused by bacterial, viral, or
fungal pathogens. The most common causes
of CAP include the bacteria S. pneumoniae,
the influenza virus, and the respiratory
syncytial virus (RSV).8,23 Other bacteria that
can cause CAP include Haemophilus
influenzae, Mycoplasma pneumoniae, and
Chlamydophila pneumoniae.8 S. pneumoniae
makes up 36% of adult CAP cases. Viral
infections like the flu and RSV can lead to
secondary bacterial pneumonia which is
usually caused by S. pneumoniae.24
Pneumococcal pneumonia leads to
approximately 400,000 hospitalizations in
the United States each year.
Pneumonia is caused by pathogen entry
into the lower respiratory tract.8,22 This can
occur through several mechanisms like
inhalation of aerosolized particles, transport
of pathogens through the bloodstream from
an extrapulmonary site, or aspiration of
oropharyngeal contents. Aspiration is the
most common cause of pneumonia and it
occurs regularly in healthy and sick patients
during sleep. Typically, the lungs protective
mechanisms prevent infection, but these
mechanisms can be impaired or overcome.
For example, in aspiration, if the patient has
factors that promote aspiration like
decreased level of consciousness, the
amount of oropharyngeal contents delivered
to the lungs increases and can overcome the
protective mechanisms. Other risk factors
for development of CAP include age over 65
years old, diabetes mellitus, smoking,
alcohol abuse, asplenia, and chronic
cardiovascular, pulmonary, renal, or liver
disease.8
Clinical presentation of pneumonia usually
involves abrupt onset fever, chills, dyspnea,
tachycardia, tachypnea, and productive
cough.8,22 Typically, the cough produces
rust-colored sputum or hemoptysis. It can
also present with chest pain due to
inflammation of the lining of the lungs.
Diagnosis of pneumonia requires at least one
respiratory symptom as well as a chest
radiograph showing a new infiltrate.
Diagnosis of CAP also requires that patients
have had no contact with a healthcare
facility.8 CAP can affect patients of all ages
and without regard to time of year.
However, it can be more severe in very
young, elderly, or chronically ill patients.
Severity is typically measured using scales
like the CRB65, CURB-65, or PSI.
Treatment Recommendations Overview
Disclaimer: The guidelines for treatment
of community acquired pneumonia
published by the Infectious Diseases Society
of America and the American Thoracic
Society were due to be updated during 2018
but had not been updated at the time of this
writing.
The 2007 Infectious Diseases Society of
America/American Thoracic Society
Consensus Guidelines on the Management
of Community-Acquired Pneumonia in
Adults separates treatment choices by
likelihood of drug resistant pathogens.25 This
overview will focus on outpatient treatment
options for bacterial and viral CAP
infections.
The goal of therapy for CAP is to
eradicate the infecting pathogen which will
result in improved clinical symptoms.25
There is a lack of rapid testing to identify
causative pathogens, so initial treatment will
typically be an empiric antimicrobial
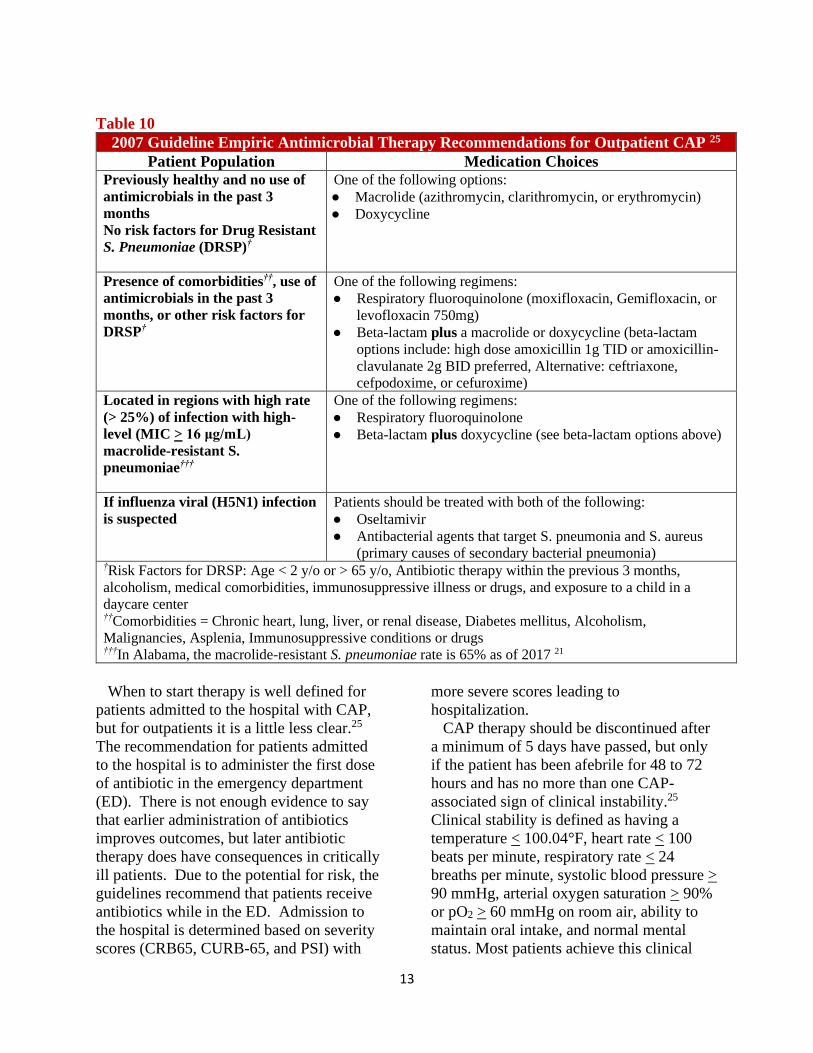
regimen. For outpatient treatment, the risk
for drug resistant pathogens is identified by
presence of risk factors as described in
Table 10).
13
Table 10
2007 Guideline Empiric Antimicrobial Therapy Recommendations for Outpatient CAP 25
Patient Population Medication Choices Previously healthy and no use of
antimicrobials in the past 3
months
No risk factors for Drug Resistant
S. Pneumoniae (DRSP)†
One of the following options:
● Macrolide (azithromycin, clarithromycin, or erythromycin)
● Doxycycline
Presence of comorbidities††, use of
antimicrobials in the past 3
months, or other risk factors for
DRSP†
One of the following regimens:
● Respiratory fluoroquinolone (moxifloxacin, Gemifloxacin, or
levofloxacin 750mg)
● Beta-lactam plus a macrolide or doxycycline (beta-lactam
options include: high dose amoxicillin 1g TID or amoxicillin-
clavulanate 2g BID preferred, Alternative: ceftriaxone,
cefpodoxime, or cefuroxime)
Located in regions with high rate
(> 25%) of infection with high-
level (MIC > 16 μg/mL)
macrolide-resistant S.
pneumoniae†††
One of the following regimens:
● Respiratory fluoroquinolone
● Beta-lactam plus doxycycline (see beta-lactam options above)
If influenza viral (H5N1) infection
is suspected
Patients should be treated with both of the following:
● Oseltamivir
● Antibacterial agents that target S. pneumonia and S. aureus
(primary causes of secondary bacterial pneumonia) †Risk Factors for DRSP: Age < 2 y/o or > 65 y/o, Antibiotic therapy within the previous 3 months,
alcoholism, medical comorbidities, immunosuppressive illness or drugs, and exposure to a child in a
daycare center ††Comorbidities = Chronic heart, lung, liver, or renal disease, Diabetes mellitus, Alcoholism,
Malignancies, Asplenia, Immunosuppressive conditions or drugs †††In Alabama, the macrolide-resistant S. pneumoniae rate is 65% as of 2017 21
When to start therapy is well defined for
patients admitted to the hospital with CAP,
but for outpatients it is a little less clear.25
The recommendation for patients admitted
to the hospital is to administer the first dose
of antibiotic in the emergency department
(ED). There is not enough evidence to say
that earlier administration of antibiotics
improves outcomes, but later antibiotic
therapy does have consequences in critically
ill patients. Due to the potential for risk, the
guidelines recommend that patients receive
antibiotics while in the ED. Admission to
the hospital is determined based on severity
scores (CRB65, CURB-65, and PSI) with
more severe scores leading to
hospitalization.
CAP therapy should be discontinued after
a minimum of 5 days have passed, but only
if the patient has been afebrile for 48 to 72
hours and has no more than one CAP-
associated sign of clinical instability.25
Clinical stability is defined as having a
temperature < 100.04°F, heart rate < 100
beats per minute, respiratory rate < 24
breaths per minute, systolic blood pressure >
90 mmHg, arterial oxygen saturation > 90%
or pO2 > 60 mmHg on room air, ability to
maintain oral intake, and normal mental
status. Most patients achieve this clinical

16
stability after 3 to 7 days of antibiotic
therapy, so longer durations are not typically
necessary. If patients have persistent
symptoms, they should be directed to return
to their primary care physician or the
physician who diagnosed their pneumonia.
Current Prescribing Patterns The current guidelines have very specific
recommendations for outpatient CAP based
on additional patient risk factors. Despite
this, it is not uncommon to see alternative
antibiotics or antibiotics at different doses,
durations, frequencies, and routes of
administration prescribed. There have been
several studies done to address this in
response to the Centers for Medicare and
Medicaid Services (CMS) updated
readmission and reimbursement policy.26
One such study addressed several
prescribing criteria to determine whether
appropriate antibiotic therapy was selected
for patients with CAP. 26 This study was a
retrospective chart review at an outpatient
academic primary care practice. They
assessed appropriateness of antibiotic
therapy based on patient risk factors, drug,
duration, route, dose, and frequency. This
study identified 101 episodes of CAP. Of
those episodes, 49% were treated with an
antibiotic. Twenty-four of those treated
patients were low-risk and only 7 of those
24 patients (29%) were treated appropriately
based on all of the factors reviewed by this
study. For high risk patients the percent was
slightly better, but still of 25 patients only
13 were treated with the appropriate
antibiotic. Two patients were excluded for
lower dose than recommended and one
patient was excluded for shorter duration
than recommended. So, overall, only 40% of
patients in the high-risk group received
appropriate antibiotic therapy. For all 49
patients who received antibiotic therapy,
only 17 (35%) were treated with guideline
directed therapy. This study emphasizes the
importance of addressing all components of
prescribing for antimicrobial stewardship.
Inappropriate duration of antibiotic
therapy has been addressed in several
studies as well. Two studies looked at the
impact of an antimicrobial stewardship
program on duration of antibiotic therapy for
CAP.27,28 Both studies recognized that there
have been improvements in CAP
identification, time to start of antibiotic
therapy, cultures, and assessment of
vaccination needs, but note a lack of
regulation for duration of therapy.
Complications from inappropriate antibiotic
duration include superinfection, readmission
to the hospital with pneumonia, and
antimicrobial resistance. In one study, a
group of 56 patients treated in 2008 before
the stewardship program was implemented
was compared to a group of 63 patients
treated in 2010 after the program was
implemented. 27 In this study, 92% of the
2008 patients and 91% of the 2010 patients
were treated with an appropriate antibiotic,
but median duration of therapy was 3 days
longer in the 2008 group (7 days vs. 10
days; p < 0.001). This study found that after
the program was implemented, there were
148 fewer days of antibiotic therapy. No
significant difference was found between C.
difficile infection, but fewer patients in the
2010 group (1 patient) were infected than
the 2008 group (3 patients). In another
study, 307 control patients treated from
November 2014 to April 2015 before a
stewardship intervention were compared to
293 intervention patients treated from
November 2015 to April 2016 after a
stewardship intervention.28 There was a
significant difference between the median
days of therapy with the intervention group
receiving 6 (5 to 7) days of therapy
compared to 9 (7 to 10) days of therapy in
the control group (p<0.001). Overall, the
control group had a median excess of 3 days
of antibiotic treatment and the intervention
16
group had a median of 1 day of excess
treatment. This intervention prevented 586
days of unnecessary treatment compared
with the control group. This reduction in
excess antibiotic use has the potential to
prevent superinfections and antimicrobial
resistance. However, when evaluated, there
was no significant difference between
readmission to hospital with pneumonia or
mortality, but numeric differences were
found with fewer patients having
complications in the intervention group. No
patients in this study tested positive for C.
difficile.
In conclusion, inappropriate antibiotic use
is very common in the treatment of CAP but
has been improved with the implementation
of antimicrobial stewardship programs.
Pharmacists can play a pivotal role in
preventing inappropriate therapy in the
outpatient setting. Being aware of
prescribing patterns and guideline
recommendations allows pharmacists to
recommend appropriate therapy and prevent
antibiotic side effects and potentially
antimicrobial resistance.
Influenza The influenza virus causes more deaths
each year than any other vaccine-
preventable illness.29 Seasonal epidemics
result in approximately 200,000
hospitalizations and 30,000 deaths each year
in the United States. The groups with the
highest rates of hospitalization, severe
illness and death include: those older than
65 years of age, young children, and those
with underlying medical conditions such as
pregnancy and cardiopulmonary disorders
that may increase the risk of complications.
The complications of influenza most likely
to result in death are secondary bacterial
pneumonia, primary viral pneumonia and
exacerbation of underlying comorbidities.
Influenza virus has the highest rates of
infection during the winter months;
however, infection can occur at any time of
year.29 The flu is contagious and can be
spread from person to person through
inhalation of respiratory droplets when the
infected person coughs or sneezes. Touching
contaminated objects is another route of
possible transmission. Some of the common
signs and symptoms include rapid onset of
fever, myalgia, nonproductive cough and
sore throat. These usually resolve in 3-7
days without intervention but may persist for
several more days. Patients who develop
primary viral pneumonia most often present
with a productive cough with bloody sputum
that will progress to dyspnea and
hypoxemia. Patients who develop secondary
bacterial pneumonia most often present with
a fever, productive cough and radiologic
evidence of consolidation.
Pathogens:
Influenza virus is composed of types A, B
and C which cause disease in many different
species including humans, pigs, horses and
birds; however, humans are only susceptible
to types A and B.29 The annual influenza
outbreaks are associated with the type A
virus; conversely, the sporadic outbreaks are
typically due to type B. The type A virus is
further broken down into subtypes, H1-H16
and N1-N9, with the most common subtypes
affecting humans being H3N2 and H1N1.
The subtypes come from changes in the
surface antigens, hemagglutinin and
neuraminidase. Certain changes, such as
point mutations, produce antigenic variants
that result in a differing immunity profile.
This process is referred to as antigenic drift
and is the reason for the changing annual
influenza vaccine combination.
Treatment Recommendations
There are three antivirals (neuraminidase
inhibitors) currently approved by the FDA
for the prevention and treatment of
influenza: oral oseltamivir, inhaled
16
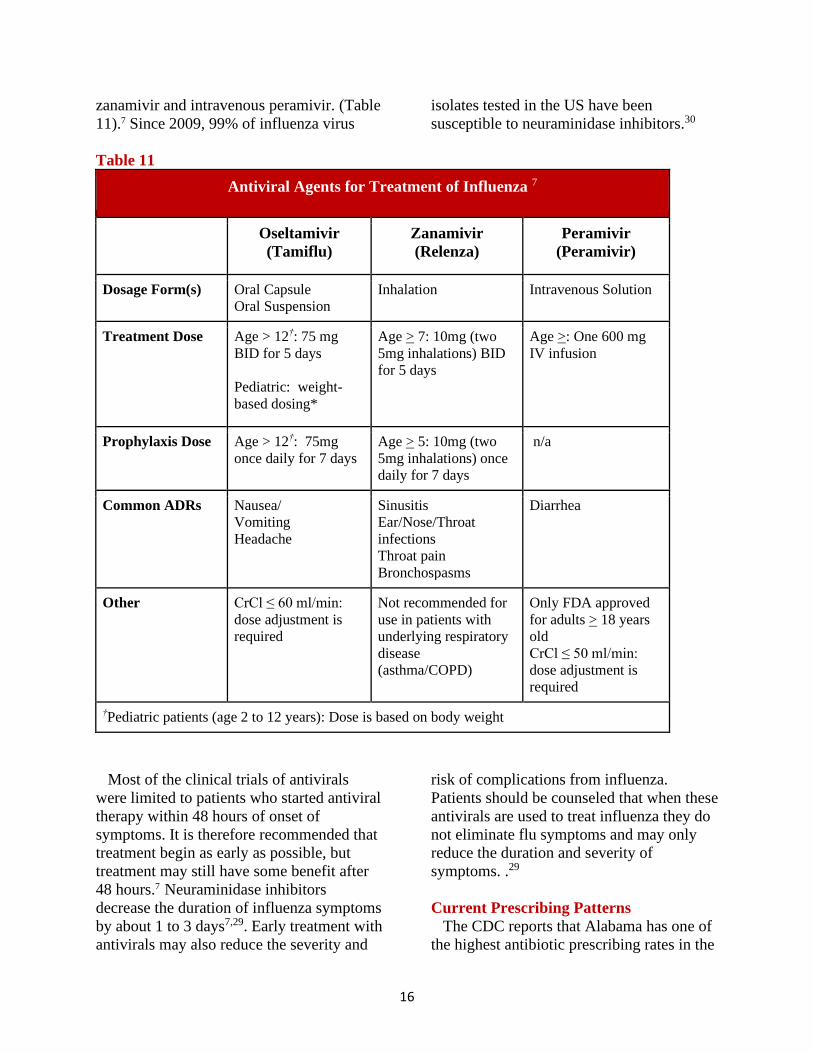
zanamivir and intravenous peramivir. (Table
11).7 Since 2009, 99% of influenza virus
isolates tested in the US have been
susceptible to neuraminidase inhibitors.30
Table 11
Antiviral Agents for Treatment of Influenza 7
Oseltamivir
(Tamiflu)
Zanamivir
(Relenza)
Peramivir
(Peramivir)
Dosage Form(s) Oral Capsule
Oral Suspension
Inhalation Intravenous Solution
Treatment Dose Age > 12†: 75 mg
BID for 5 days
Pediatric: weight-
based dosing*
Age > 7: 10mg (two
5mg inhalations) BID
for 5 days
Age >: One 600 mg
IV infusion
Prophylaxis Dose Age > 12†: 75mg
once daily for 7 days
Age > 5: 10mg (two
5mg inhalations) once
daily for 7 days
n/a
Common ADRs Nausea/
Vomiting
Headache
Sinusitis
Ear/Nose/Throat
infections
Throat pain
Bronchospasms
Diarrhea
Other CrCl ≤ 60 ml/min:
dose adjustment is
required
Not recommended for
use in patients with
underlying respiratory
disease
(asthma/COPD)
Only FDA approved
for adults > 18 years
old
CrCl ≤ 50 ml/min:
dose adjustment is
required
†Pediatric patients (age 2 to 12 years): Dose is based on body weight
Most of the clinical trials of antivirals
were limited to patients who started antiviral
therapy within 48 hours of onset of
symptoms. It is therefore recommended that
treatment begin as early as possible, but
treatment may still have some benefit after
48 hours.7 Neuraminidase inhibitors
decrease the duration of influenza symptoms
by about 1 to 3 days7,29. Early treatment with
antivirals may also reduce the severity and
risk of complications from influenza.
Patients should be counseled that when these
antivirals are used to treat influenza they do
not eliminate flu symptoms and may only
reduce the duration and severity of
symptoms. .29
Current Prescribing Patterns
The CDC reports that Alabama has one of
the highest antibiotic prescribing rates in the
3
country annually with about 1,200
antibiotics being prescribed per 1,000
people.9 The rate is higher in the winter
months due to influenza activity and at least
30% of all antibiotics prescribed are not
appropriate treatment. A recent study has
shown that Alabama prescribes more
antibiotics in response for the flu than
anywhere else in the country.31 The study
also found that the excessive antibiotic
overuse was due to a low prescribing quality
among physicians rather than having a
tendency to prescribe more frequently.
Healthcare providers should be aware of the
efforts that need to be made in the future to
prevent rapidly increasing antimicrobial
resistance.
Acute Bronchitis/COPD
Exacerbations Acute bronchitis is a common lower
respiratory tract infection which is
responsible for about 10 million office visits
annually.8 Similar to the influenza virus,
acute bronchitis can occur at any time of
year but occurs most frequently in the winter
months. Some of the risk factors include
exposure to environmental irritants, prior
acute viral infection and smoking.
Pathologically, acute bronchitis causes
inflammation of the epithelium in the large
airways and increases bronchial secretions.
Prescribers as well as patients should be
aware that this is a self-limiting illness and
unlikely to result in permanent damage. The
most common presenting symptom is a
nonproductive cough which will progress
into a persistent, productive cough as the
illness progresses usually lasting about three
weeks.
Patients with COPD can have
exacerbations and it is important to know
how to differentiate an exacerbation from
other disease states sharing similar symptom
profiles such as acute bronchitis.32A COPD
exacerbation is defined as “an acute
worsening of respiratory symptoms that
result in additional therapy.” Symptoms
typically last between 7 and 10 days and are
often caused by respiratory tract infections.
The key symptom to watch out for is
increased dyspnea but can also include
cough, wheeze, increased sputum production
and sputum purulence.
Pathogens
The major pathogens involved in the
development of acute bronchitis are
predominantly respiratory viruses which
account for roughly 85-95% of cases.29
Infection from a bacterial source is a
possibility but the incidence is rare. Patients
presenting with an antibiotic prescription for
acute bronchitis may be the result of a
prescribing error which creates an important
role for the pharmacist to display
antimicrobial stewardship and confirm the
source of infection.
COPD exacerbations mostly stem from
respiratory viral infections but can also
come from bacterial infections and
environmental factors.32 The common cold,
rhinovirus, is the most common causal
factor and results in more severe
exacerbations compared to other causal
factors.
Treatment Recommendations
The most important recommendation for
the management of acute bronchitis is to
avoid prescribing antibiotics and employ
strategies to reduce antibiotic use.33 The
inappropriate use of antibiotics in this
setting has already lead to increased
antimicrobial resistance. The current
treatment recommendations are mostly over-
the-counter medications emphasizing the
importance of pharmacist knowledge in this
area. Treatment will not necessarily reduce
the duration of illness but rather the goal is
aimed at symptom control. Some of the
common medications used to reduce the
3
severity of cough include guaifenesin,
dextromethorphan and an
antihistamine/decongestant combination.
The 2018 Global Initiative for Chronic
Obstructive Lung Disease (GOLD)
guidelines recommend that “antibiotics,
when indicated, can shorten recovery time,
reduce the risk of early relapse, treatment
failure and hospitalization duration.
Duration of therapy should be 5-7 days.”32
There is still some controversy on the use of
antibiotics for exacerbations, but healthcare
providers should be aware of the specific
signs that are necessary to appropriately
prescribe an antibiotic. Acute bacterial
exacerbations of COPD may warrant
antibiotic therapy if the patient presents with
the following three cardinal symptoms: 1)
increase in dyspnea, 2) sputum volume and
3) sputum purulence. Patients can still
receive antibiotics if they only have two of
the cardinal symptoms as long as one of
them is an increase in sputum purulence.
Additional, COPD patients on mechanical
ventilation or with a history of COPD
exacerbations requiring hospitalization
should also receive antibiotics due to their
increased risk for a pseudomonas infection.
Current Prescribing Patterns
While the overwhelming majority of acute
bronchitis cases are viral in nature,
antibiotics are still commonly being
prescribed. Recent studies have shown that
the antibiotic prescribing rate in this setting
is roughly 70% and that number continues to
rise.33 More specifically, smokers who get
acute bronchitis have been found to receive
a round of antibiotics about 90% of the time.
Clinicians most often use the purulent
sputum sign as indication of infection and
subsequently prescribe antibiotics. However,
there has been shown to be no difference in
outcomes between patients who receive
antibiotics and those who don’t. The
population who receives antibiotics are also
at an increased risk for developing adverse
events such as nausea, diarrhea, headache
and skin rash. Healthcare providers should
all be aware that continued antibiotic use in
the treatment of acute bronchitis will lead to
increased healthcare costs and antimicrobial
resistance.
Recent studies have shown that while
prescription antibiotics are given to patients
with COPD exacerbations the majority of
the time, there is much variability in
prescribing patterns from practice to
practice.34,35 The use of antibiotics for
exacerbations has not been extensively
studied resulting in differing prescribing
patterns site by site depending on their own
opinions and clinical experience with its use.
Prevention of Respiratory Infections There are several methods to prevent
spread of community acquired respiratory
infections. Pharmacists can help prevent the
spread of these infections by identifying
patients that qualify for specific vaccines
and encouraging all patients to practice
preventive measures during times of high
prevalence.
Vaccinations
Influenza Vaccine
The influenza vaccine is recommended to
prevent the flu as well as reduce the
incidence of rhinosinusitis, community
acquired pneumonia, and bronchitis. 23,7,36
There were two distinct categories of
influenza vaccines recommended for the
2017-2018 flu season.7 The two categories
are separated by the number of influenza
strains they cover. The trivalent forms cover
three forms of influenza virus, two influenza
A viruses (H1N1, H3N2) and one influenza
B virus. The quadrivalent forms cover the
same strains as the trivalent plus one more
influenza B virus. Within these two
categories of vaccines, there are two forms
of the influenza vaccine, an inactivated form
3
and a recombinant form. The inactivated
form (IIV) is made using a virus grown in
eggs and the recombinant form (RIV) is not
made with eggs. Influenza vaccines should
be chosen based on age of the patient
receiving the vaccine. Several inactivated
vaccines are approved for use in patients
from 6 months old to over 65 years old, but
recombinant vaccines are only approved in
patients 18 years old or older. High dose
inactivated vaccines are available for
patients aged 65 years or older who are at
greater risk of influenza infection and
complications. The influenza vaccine is
recommended annually for all patients 6
months of age and older. Children between 6
months and 8 years should receive two
doses of influenza vaccine at least four
weeks apart once and then one dose every
year.37,38 The flu vaccine has very mild
adverse effects including soreness, redness,
or swelling at the injection site, low grade
fever, and aches.7 The flu vaccine cannot
cause the flu. Vaccines should be offered by
the end of October and should continue as
long as the influenza virus is a threat.
Haemophilus Influenzae type B (Hib)
Vaccine
The Haemophilus influenzae type B (Hib)
vaccine is recommended to prevent
pneumonia.23 There are several brand names
of Hib vaccines, but all of them are
polysaccharide conjugate vaccines.24 The
Hib vaccine series is recommended for
children at least 6 weeks old.37,38 The four-
dose series (ActHIB, Hiberix, Pentacel)
should occur at 2, 4, 6, and 12-15 months
old and the three-dose series (PedvaxHIB)
should occur at 2, 4, and 12-15 months. Hib
vaccination is not routinely recommended in
adult patients unless they have anatomical or
functional asplenia with no previous
vaccination or they are undergoing
hematopoietic stem cell transplant. This
vaccine is typically well tolerated, but
adverse effects can include swelling,
redness, or pain at injection site, fever, and
irritability.24
Pneumococcal Vaccines
Pneumococcal vaccines are recommended
to prevent pneumonia and rhinosinusitis. 18,23 There are two distinct types of vaccines;
PCV13 (Prevnar 13) and PPSV23
(Pneumovax 23).24 PCV13 is a
pneumococcal conjugate vaccine that covers
13 serotypes of S. pneumoniae. It is 45%
effective in preventing pneumococcal
pneumonia caused by the strains covered in
the vaccine in adults over 65 years old.
PPSV23 is a pneumococcal polysaccharide
vaccine that covers 23 types of
pneumococcal bacteria known to cause 60 to
76% of invasive disease. These vaccinations
are recommended in young children and
elderly adults.37 Children should receive
PCV13 at 2, 4, 6, and 12-15 months. They
must be at least 6 weeks old to get PCV13.
PPSV23 is only indicated for children in
special circumstances like chronic heart
disease, chronic lung disease, diabetes
mellitus, and immunosuppressive disorders.
In these special circumstances, it is better for
patients to receive the PCV13 series first
and then to receive one to two doses of
PPSV23 depending on the conditions the
patient has. Healthy adults aged 65 years old
or older should receive one dose of PCV13
and then one dose of PPSV23 one year later
or if PPSV23 was administered first, PCV13
should be administered one year after
PPSV23.38 There are exceptions where
adults between 19 and 64 years old with
certain conditions should receive
pneumococcal vaccines. The conditions
include chronic heart disease, lung disease,
liver disease, alcoholism, diabetes mellitus,
cigarette smoking, and immunosuppressive
disorders. Indications for when to administer
pneumococcal vaccines to these patients
differ based on which conditions the patient
3
has. As pneumonia is not more prevalent at
any time of year, these should be
administered year-round. 24 These vaccines
can cause a few adverse effects including
local injection site reactions, fever, myalgia,
and serious adverse reactions like
anaphylaxis. PCV13 also has the potential to
cause febrile seizures in children.
Measles Vaccine
The measles vaccine is recommended to
prevent pneumonia, especially in children. 23,24 There is no vaccine for measles
protection alone. 24 The live attenuated
measles vaccine is available combined with
either mumps and rubella vaccines (MMR)
or mumps, rubella, and varicella vaccines
(MMRV). As varicella will be discussed in
another section, this will focus on the MMR
vaccine. As mentioned prior, the measles
induced complication of pneumonia is most
common in children, so vaccination of
children with MMR is very important.
Children should receive a two-dose series of
MMR starting at 12 to 15 months and
completing at 4 to 6 years old.37 In adults,
the main complication of measles infection
is acute encephalitis, not pneumonia.24
However if adults have no evidence of
immunity including being born before 1957,
documentation of vaccination, or positive
titer they should receive a dose of MMR.38
The MMR vaccine can cause some adverse
events like arthralgias in women, and rash,
pruritus, or purpura in all patients.24 It is
important to note that there is no evidence to
suggest that any vaccine, including MMR,
causes autism or autism spectrum disorder.
Pertussis Vaccine
Pertussis vaccination is recommended to
prevent pneumonia.23 Complications of
pertussis include secondary bacterial
pneumonia in children, adolescents, and
adults.24 There is no vaccine that covers
pertussis alone. Two combination vaccines
contain acellular inactivated pertussis as
well as tetanus and diphtheria toxoids; DTaP
and Tdap. Children should receive a five-
dose series of DTaP (diphtheria, tetanus, and
acellular pertussis) at 2, 4, 6, and 15 to 18
months and 4 to 6 years.37 Adults should
receive one dose of Tdap (tetanus,
diphtheria, and pertussis) as an adult or
adolescent (11 to 12 years old) and then
have a booster of Td which excludes
pertussis every ten years.38 Also, pregnant
women should receive a dose of Tdap
during each pregnancy during weeks 27 to
36 of gestation. DTaP can cause a few
adverse reactions like pain, redness, or
swelling at injection site, fever of 101°F,
and rarely more serious adverse reactions
like anaphylaxis.24 Tdap and Td can also
cause pain, redness, or swelling at injection
site, and a fever of 101.4°F or higher.
Varicella Vaccine
Varicella vaccination is recommended to
prevent pneumonia. 23 A common
complication of varicella infection is viral or
bacterial pneumonia.24 More commonly this
pneumonia is caused by viral infections, but
in very young children (< 1 year old)
secondary bacterial infections are more
common. There are three live attenuated
varicella vaccines and one recombinant
vaccine.24,39 The live attenuated vaccines
include one varicella vaccine for children
(Varivax), one combination measles,
mumps, rubella, and varicella (MMRV)
vaccine, and one herpes zoster vaccine for
adults (Zostavax).24 The recombinant
vaccine is also a herpes zoster vaccine for
adults (Shingrix).39 Children should receive
a two-dose series of Varivax or MMRV
starting at 12 to 15 months and completing
at 4 to 6 years old.37 Adults should receive
either a two-dose series of Shingrix
separated by 2 to 6 months starting at age 50
or one dose of Zostavax at age 60.38 If
patients have already received the Zostavax
3
vaccine, they should receive a two-dose
series of Shingrix. Shingrix is preferred as it
has higher efficacy than Zostavax, so if
possible administer Shingrix. Adverse
effects of Varivax and MMRV include pain
and redness at site of injection and
generalized rash.24 Adverse effects of
Zostavax include pain, swelling, and redness
at site of injection. There is also risk of
transmission of varicella virus after
vaccination with live vaccines, and it is
recommended that patients receiving
vaccines should avoid contact with people
who have no evidence of immunity to
varicella. For Shingrix, the adverse effects
are similar, including pain, redness, or
swelling at site of injection, fever, and
headache.39 Without the live component of
varicella in this vaccine, there is no risk of
transmission after receiving this vaccine.
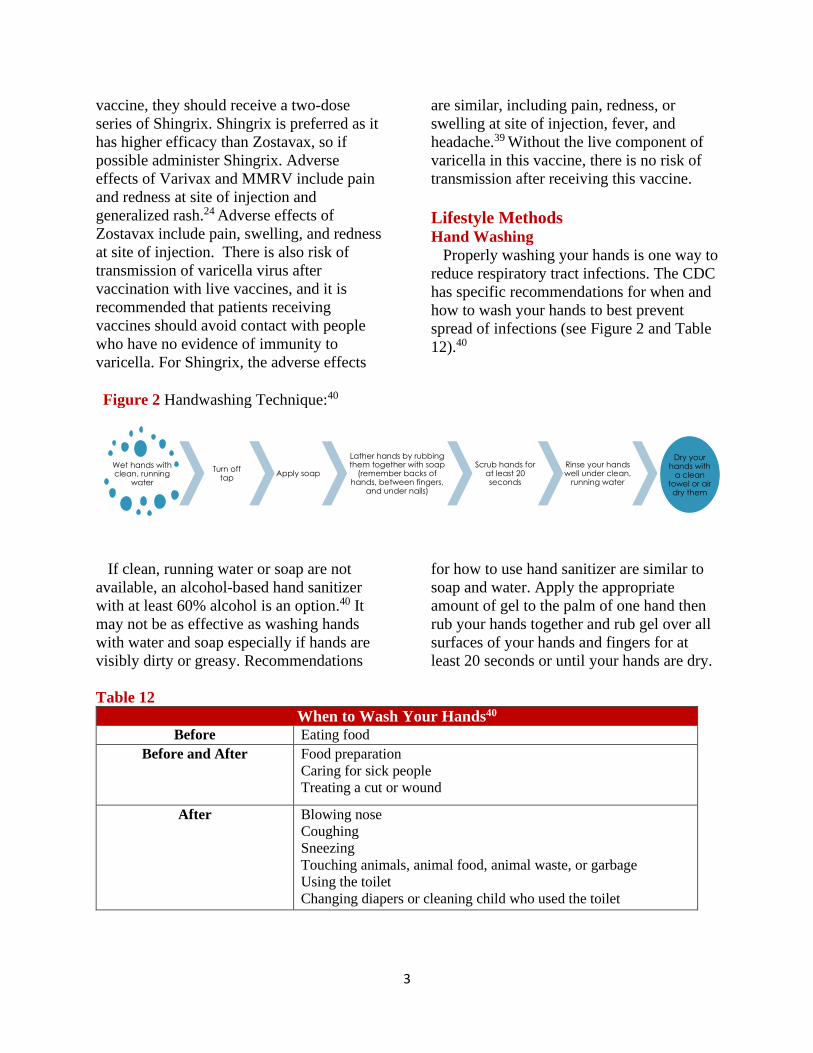
Lifestyle Methods
Hand Washing
Properly washing your hands is one way to
reduce respiratory tract infections. The CDC
has specific recommendations for when and
how to wash your hands to best prevent
spread of infections (see Figure 2 and Table
12).40
Figure 2 Handwashing Technique:40
If clean, running water or soap are not
available, an alcohol-based hand sanitizer
with at least 60% alcohol is an option.40 It
may not be as effective as washing hands
with water and soap especially if hands are
visibly dirty or greasy. Recommendations
for how to use hand sanitizer are similar to
soap and water. Apply the appropriate
amount of gel to the palm of one hand then
rub your hands together and rub gel over all
surfaces of your hands and fingers for at
least 20 seconds or until your hands are dry.
Table 12
When to Wash Your Hands40
Before Eating food
Before and After Food preparation
Caring for sick people
Treating a cut or wound
After Blowing nose
Coughing
Sneezing
Touching animals, animal food, animal waste, or garbage
Using the toilet
Changing diapers or cleaning child who used the toilet
Wet hands with clean, running
water Turn off tap Apply soap
Lather hands by rubbing them together with soap
(remember backs of hands, between fingers,
and under nails)
Scrub hands for at least 20 seconds
Rinse your hands well under clean,
running water
Dry your hands with
a clean towel or air dry them
3
Other Tips for Preventing Infections 6,7,23,36,41,42
• Avoid allergens and irritants
● Avoid people who are sick with respiratory tract infections
● Clean areas that are touched often
● Cover mouth and nose with a tissue, elbow, or sleeve when sneezing, don’t use your hands
● Avoid touching your eyes, nose, or mouth to avoid spreading pathogens to these sensitive
areas
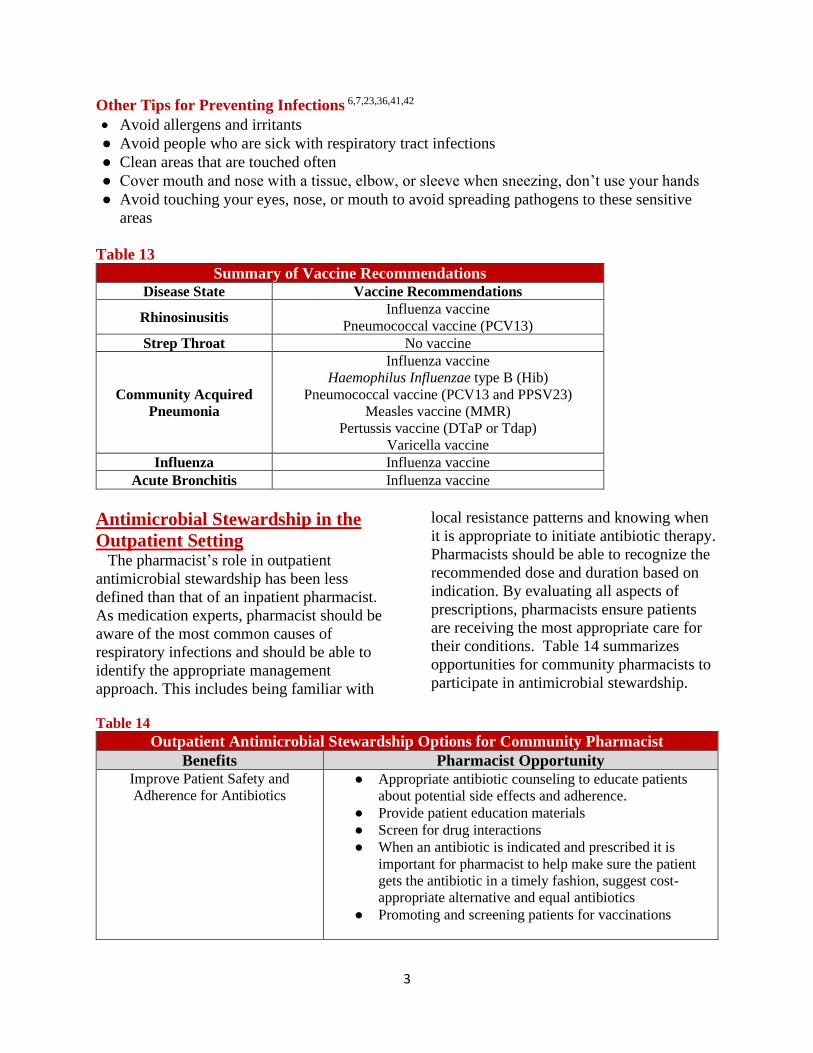
Table 13
Summary of Vaccine Recommendations Disease State Vaccine Recommendations
Rhinosinusitis Influenza vaccine
Pneumococcal vaccine (PCV13)
Strep Throat No vaccine
Community Acquired
Pneumonia
Influenza vaccine
Haemophilus Influenzae type B (Hib)
Pneumococcal vaccine (PCV13 and PPSV23)
Measles vaccine (MMR)
Pertussis vaccine (DTaP or Tdap)
Varicella vaccine
Influenza Influenza vaccine
Acute Bronchitis Influenza vaccine
Antimicrobial Stewardship in the
Outpatient Setting The pharmacist’s role in outpatient
antimicrobial stewardship has been less
defined than that of an inpatient pharmacist.
As medication experts, pharmacist should be
aware of the most common causes of
respiratory infections and should be able to
identify the appropriate management
approach. This includes being familiar with
local resistance patterns and knowing when
it is appropriate to initiate antibiotic therapy.
Pharmacists should be able to recognize the
recommended dose and duration based on
indication. By evaluating all aspects of
prescriptions, pharmacists ensure patients
are receiving the most appropriate care for
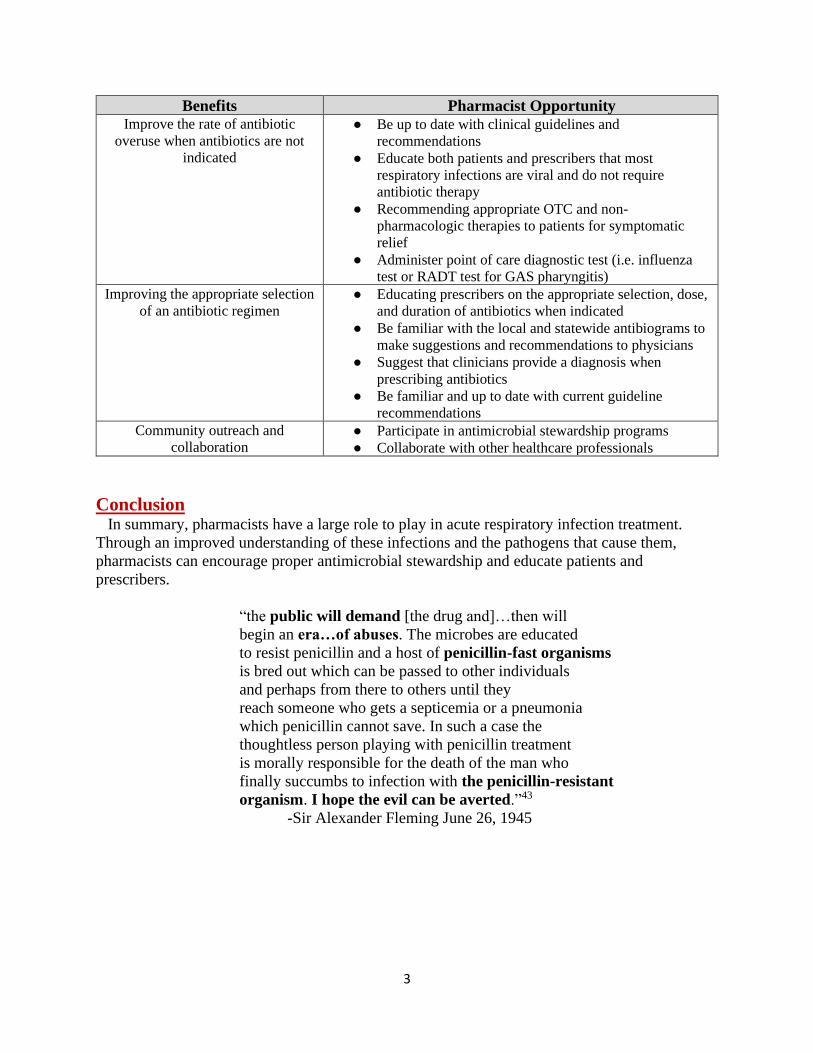
their conditions. Table 14 summarizes
opportunities for community pharmacists to
participate in antimicrobial stewardship.
Table 14
Outpatient Antimicrobial Stewardship Options for Community Pharmacist
Benefits Pharmacist Opportunity Improve Patient Safety and
Adherence for Antibiotics ● Appropriate antibiotic counseling to educate patients
about potential side effects and adherence.
● Provide patient education materials
● Screen for drug interactions
● When an antibiotic is indicated and prescribed it is
important for pharmacist to help make sure the patient
gets the antibiotic in a timely fashion, suggest cost-
appropriate alternative and equal antibiotics
● Promoting and screening patients for vaccinations
3
Benefits Pharmacist Opportunity
Improve the rate of antibiotic
overuse when antibiotics are not
indicated
● Be up to date with clinical guidelines and
recommendations
● Educate both patients and prescribers that most
respiratory infections are viral and do not require
antibiotic therapy
● Recommending appropriate OTC and non-
pharmacologic therapies to patients for symptomatic
relief
● Administer point of care diagnostic test (i.e. influenza
test or RADT test for GAS pharyngitis)
Improving the appropriate selection
of an antibiotic regimen ● Educating prescribers on the appropriate selection, dose,
and duration of antibiotics when indicated
● Be familiar with the local and statewide antibiograms to
make suggestions and recommendations to physicians
● Suggest that clinicians provide a diagnosis when
prescribing antibiotics
● Be familiar and up to date with current guideline
recommendations
Community outreach and
collaboration ● Participate in antimicrobial stewardship programs
● Collaborate with other healthcare professionals
Conclusion
In summary, pharmacists have a large role to play in acute respiratory infection treatment.
Through an improved understanding of these infections and the pathogens that cause them,
pharmacists can encourage proper antimicrobial stewardship and educate patients and
prescribers.
“the public will demand [the drug and]…then will
begin an era…of abuses. The microbes are educated
to resist penicillin and a host of penicillin-fast organisms
is bred out which can be passed to other individuals
and perhaps from there to others until they
reach someone who gets a septicemia or a pneumonia
which penicillin cannot save. In such a case the
thoughtless person playing with penicillin treatment
is morally responsible for the death of the man who
finally succumbs to infection with the penicillin-resistant
organism. I hope the evil can be averted.”43
-Sir Alexander Fleming June 26, 1945
3
References: 1. Harris AM, Hicks LA, Qaseem A. Appropriate Antibiotic Use for Acute Respiratory Tract Infection in
Adults: Advice for High-Value Care from the American College of Physicians and the Centers for Disease
Control and Prevention. Ann Intern Med [Internet]. 2016 Mar 15 [cited 2018 Jul 3];164(6):425. Available
from: http://annals.org/article.aspx?doi=10.7326/M15-1840
2. Renati S, Linder JA. Necessity of office visits for acute respiratory infections in primary care. Fam Pract
[Internet]. 2016 Apr 5 [cited 2018 Jul 16];33(3):312–7. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/27048524
3. Fleming-Dutra KE, Hersh AL, Shapiro DJ, Bartoces M, Enns EA, File TM, et al. Prevalence of
Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010-2011. JAMA [Internet].
2016 May 3 [cited 2018 Jul 1];315(17):1864. Available from:
http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2016.4151
4. Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N. Understanding the culture of prescribing:
qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ
[Internet]. 1998 Sep 5 [cited 2018 Jul 2];317:637-42. Available from:
https://www.bmj.com/content/bmj/317/7159/637.full.pdf
5. Adult Treatment Recommendations. Atlanta, GA, U.S. Department of Health and Human Services. Centers
for Disease Control and Prevention [Internet]. [last updated 2017 Oct 3; accessed 2018 Jul 12]. Available
from: https://www.cdc.gov/antibiotic-use/community/for-hcp/outpatient-hcp/adult-treatment-
rec.html#modalIdString_CDCTable_0
6. Group A Streptococcal (GAS) Disease. Atlanta, GA, U.S. Department of Health and Human Services.
Centers for Disease Control and Prevention. [last updated 2016 Sep 16; accessed 2018 Jul 2] Available
from: https://www.cdc.gov/groupastrep/diseases-public/strep-throat.html
7. Influenza (Flu). Atlanta, GA, U.S. Department of Health and Human Services. Centers for Disease Control
and Prevention. [last updated 2018 Jul 2; accessed 2018 Jul 2] Available from:
https://www.cdc.gov/flu/index.htm
8. Blackford MG, Glover ML, Reed MD. Lower Respiratory Tract Infections. In: Dipiro JT, Talbert RL, Yee
GC, Matzke GR, Wells BG, Posey L. eds Pharmacotherapy: A Pathophysiologic Approach. 10th ed. New
York: McGraw-Hill; Available from:
https://accesspharmacy.mhmedical.com/content.aspx?bookid=1861§ionid=146071234. Accessed June
29, 2018.
9. Outpatient Antibiotic Prescriptions — United States, 2015. Atlanta, GA, U.S. Department of Health and
Human Services. Centers for Disease Control and Prevention. [last updated 2017 Oct 26; accessed 2018
Jul 1] Available from: https://www.cdc.gov/antibiotic-use/community/programs-measurement/state-local-
activities/outpatient-antibiotic-prescriptions-US-2015.html
10. Caserta M, Flores A. Chapter 54: Pharyngitis. In: Mandell G, Bennett J, Dolin R, editors. Mandell,
Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia: Churchill
Livingstone/Elsevier; 2010. p. 815–821.
11. Center for Health Statistics N. Ambulatory medical care utilization estimates for 2007. Vital Heal Stat
[Internet]. 2011 Apr [cited 2018 Jun 29];13(169). Available from:
https://www.cdc.gov/nchs/data/series/sr_13/sr13_169.pdf
12. Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for
the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious
Diseases Society of America. Clin Infect Dis [Internet]. 2012 Nov 15 [cited 2018 Jul 12];55(10):1279–82.
Available from: https://academic.oup.com/cid/article-lookup/doi/10.1093/cid/cis847
13. Sore Throat: Symptoms & Causes. Scottsdale, AZ. Mayo Clinic [last updated 2017 Aug 8; accessed 2018
Jul 5] Available from: https://www.mayoclinic.org/diseases-conditions/sore-throat/symptoms-causes/syc-
20351635
14. Bradley CP. Uncomfortable prescribing decisions: a critical incident study. BMJ [Internet]. 1992 Feb 1
[cited 2018 Jul 2];304(6822):294–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1739831
15. Gerber MA, Baltimore RS, Eaton CB, Gewitz M, Rowley AH, Shulman ST, et al. Prevention of rheumatic
fever and diagnosis and treatment of acute Streptococcal pharyngitis. Circulation [Internet]. 2009 Mar 24
[cited 2018 Jul 2];119(11):1541–51. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19246689
16. Frei C, Frei B. Upper Respiratory Tract Infections. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey L. eds Pharmacotherapy: A Pathophysiologic Approach. 10th ed. New York: McGraw-Hill;
3
Available from: http://accesspharmacy.mhmedical.com/content.aspx?bookid=1861§ionid=146071422.
Accessed July 02, 2018.
17. Turner B. Acute Sinusitis. Ann Intern Med [Internet]. 2010 Sep 7 [cited 2018 Jul 3];153(5):ITC3. Available
from: http://annals.org/article.aspx?doi=10.7326/0003-4819-153-5-201009070-01003
18. Chow AW, Benninger MS, Brook I, Brozek JL, Goldstein EJC, Hicks LA, et al. IDSA clinical practice
guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis [Internet]. 2012 Apr 15
[cited 2018 Jul 12];54(8):e72–112. Available from: https://academic.oup.com/cid/article-
lookup/doi/10.1093/cid/cir1043
19. Aring AM, Chan MM. Current Concepts in Adult Acute Rhinosinusitis. Am Fam Physician [Internet].
2016 Jul 15 [cited 2018 Jul 18];94(2):97–105. Available
from:http://www.ncbi.nlm.nih.gov/pubmed/27419326
20. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, Brook I, Ashok Kumar K, Kramper M, et al. Differences
from Prior Guideline Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol Head Neck Surg
[Internet]. 2015 Apr [cited 2018 Jul 3];152(2S):1–39. Available from:
http://journals.sagepub.com/doi/pdf/10.1177/0194599815572097
21. 2017 State Antibiogram [Internet]. [cited 2018 Jul 12]. Available from:
http://www.alabamapublichealth.gov/hai/assets/2017Antibiogram.pdf
22. Mandell LA, Wunderink RG. Pneumonia. In: Harrison’s Principles of Internal Medicine. 19e New York,
NY; McGraw-Hill; c2015. 803-813 p.
23. Pneumonia Can Be Prevented – Vaccines Can Help. Atlanta, GA, U.S. Department of Health and Human
Services. Centers for Disease Control and Prevention. [last updated 2017 Nov 6; accessed 2018 Jul 2]
Available from: https://www.cdc.gov/Features/Pneumonia/
24. Epidemiology and Prevention of Vaccine-Preventable Diseases. Atlanta, GA, U.S. Department of Health
and Human Services. Centers for Disease Control and Prevention. [last updated 2016 Apr 28; accessed
2018 Jul 2] Available from: https://www.cdc.gov/vaccines/pubs/pinkbook/chapters.html
25. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et. al. Infectious Diseases
Society of America/American Thoracic Society consensus guidelines on the management of community-
acquired pneumonia in adults. Clin Infect Dis [Internet]. 2007 Mar 1 [cited 2018 Jul 2];44 Suppl 2:S27-72.
Available from: https://academic.oup.com/cid/article/44/Supplement_2/S27/372079
26. Thiessen K, Lloyd AE, Miller MJ, Homco J, Gildon B, O’Neal KS. Assessing guideline-concordant
prescribing for community-acquired pneumonia. Int J Clin Pharm [Internet]. 29 May 2017 [cited 2018 Jul
2];39:674-678. Available from: https://link.springer.com/article/10.1007%2Fs11096-017-0489-4
27. Avdic E, Cushinotto LA, Hughes AH, Hansen AR, Efird LE, Bartlett JG. Impact of antimicrobial
stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin
Infect Dis [Internet]. 10 April 2012 [cited 2018 Jul 2];54:1581-1587. Available from:
https://academic.oup.com/cid/article/54/11/1581/322320
28. Foolad F, Huang AM, Nguyen CT, Lim M, Grieger J, Li J, et. al. A multicentre initiative to decrease
excessive duration of antibiotic therapy for the treatment of community-acquired pneumonia. J Antimicrob
Chemother. 16 February 2018 [cited 2018 Jul 2];73:1402-1407. Available from:
https://academic.oup.com/jac/article/73/5/1402/4866116
29. Mary D, Thiman M, Rao SC. Influenza. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey
L. eds. Pharmacotherapy: A Pathophysiologic Approach. 10th ed. New York: McGraw-Hill; Available
from:
https://accesspharmacy.mhmedical.com/content.aspx?bookid=1861§ionid=146071550#1148580263.
Accessed July 2, 2018.
30. Gubareva L V, Besselaar TG, Daniels RS, Fry A, Gregory V, Huang W, et al. Global update on the
susceptibility of human influenza viruses to neuraminidase inhibitors, 2015-2016. Antiviral Res [Internet].
2017 Oct [cited 2018 Jul 5];146:12–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28802866
31. Alsan M, Morden NE, Gottlieb JD, Zhou W, Skinner J. Antibiotic use in cold and flu season and
prescribing quality: a retrospective cohort study. Med Care [Internet]. 2015 Dec [cited 2018 Jul
5];53(12):1066-71. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4829738/.
32. Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management,
and Prevention of Chronic Obstructive Pulmonary Disease (2018 Report). [cited 2018 Jul 5]; Available
from: http://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-
Nov_WMS.pdf
3
33. Kinkade S, Long NA. Acute bronchitis. Am Fam Physician [Internet]. 2016 Oct 1 [cited 2018 Jul
5];94(7):560-565. Available from: https://www.aafp.org/afp/2016/1001/p560.html
34. Boggon R, Hubbard R, Smeeth L, Gulliford M, Cassel J, Eaton S, et. al. Variability of antibiotic
prescribing in patients with chronic obstructive pulmonary disease exacerbations: a cohort study. BMC
Pulm Med [Internet]. 2013 May 31 [cited 2018 Jul 5];13(32):1-8. Available from:
https://bmcpulmmed.biomedcentral.com/articles/10.1186/1471-2466-13-32.
35. Llor C, Bjerrum L, Munck A, et al. Predictors for antibiotic prescribing in patients with exacerbations of
COPD in general practice. Ther Adv Respir Dis [Internet]. 2013 Jan 16 [cited 2018 Jul 5];7(3):131-7.
Available from: http://journals.sagepub.com/doi/abs/10.1177/1753465812472387?url_ver=Z39.88-
2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed
36. Bronchitis. Atlanta, GA, U.S. Department of Health and Human Services. Centers for Disease Control and
Prevention. [last updated 2017 Sep 25; accessed 2018 Jul 2] Available from:
https://www.cdc.gov/antibiotic-use/community/for-patients/common-illnesses/bronchitis.html
37. Advisory Committee on Immunization Practices (ACIP). Recommended Immunization Schedule for Adults
Aged 19 Years or Older, United States, 2018. Centers for Disease Control. 2018 Feb [cited 2018 Jul 2].
Available from: https://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf
38. Advisory Committee on Immunization Practices (ACIP). Recommended Immunization Schedule for
Children and Adolescents Aged 18 years or younger, United States, 2018. Centers for Disease Control.
2018 Jan 1 [cited 2018 Jul 2]. Available from: https://www.cdc.gov/vaccines/schedules/downloads/child/0-
18yrs-child-combined-schedule.pdf
39. Shingrix Recommendations. Atlanta, GA, U.S. Department of Health and Human Services. Centers for
Disease Control and Prevention. [last updated 2018 Jan 25; accessed 2018 Jul 2] Available from:
https://www.cdc.gov/vaccines/vpd/shingles/hcp/shingrix/recommendations.html
40. Wash Your Hands. Atlanta, GA, U.S. Department of Health and Human Services. Centers for Disease
Control and Prevention. [last updated 2018 Apr 2; accessed 2018 Jul 2] Available from:
https://www.cdc.gov/features/handwashing/index.html
41. Acute Sinusitis. Scottsdale, AZ. Mayo Clinic. [last updated 2018 Mar 3; accessed 2018 Jul 2] Available
from: https://www.mayoclinic.org/diseases-conditions/acute-sinusitis/symptoms-causes/syc-20351671
42. Worried your sore throat may be strep? Atlanta, GA, U.S. Department of Health and Human Services.
Centers for Disease Control and Prevention. [last updated 2018 Jan 31; accessed 2018 Jul 2] Available
from: https://www.cdc.gov/features/strepthroat/index.html
43. Bartlett JG, Gilbert DN, Spellberg B. Seven Ways to Preserve the Miracle of Antibiotics. Clin Infect Dis
[Internet]. 2013 May 15 [cited 2018 Jul 13];56(10):1445–50. Available from:
https://academic.oup.com/cid/article/56/10/1445/405531