Embed Size (px)
Citation preview

PATHOPHYSIOLOGY OF VIRAL RESPIRATORY TRACT INFECTIONS
5
Anders Akerlund and Mats Bende
5.1 Introduction 5.2 Applied physiology of the respiratory
tract 5.2.1 Nasal structure 5.2.2 Nasal function
5.3 Pathophysiology of common colds 5.3.1 Epithelial changes 5.3.2 Vascular reactions 5.3.3 Rhinorrhoea 5.3.4 The inflammatory process 5.3.5 Effects on other functions in the
upper airways 5.3.6 Hyperreactivity and viral effects on
the lower airways 5.3.7 Circadian variations
5.4 Pathophysiological aspects of symptomatic treatment 5.4.1 Anti-inflammatory drugs 5.4.2 Anti-mediator drugs 5.4.3 Decongestants
5.5 References
5.1 INTRODUCTION
The common cold is the cause of the great majority of respiratory tract infections. It seems well established that this is a viral infection in the upper airways. In the early 1950s symptoms and signs of a common cold were
Viral and Other Injections oj the Human Respiratory Tract. Edited by S. Myint and D. Taylor-Robinson. Published in 1996 by Chapman & Hall. ISBN 978-94-011-7932-4
induced in isolated healthy individuals for the first time by nasal inoculation of virus cultured in vitro [11]. There is a widespread traditional belief that the symptoms of the common cold are related to cooling of the body. Although cooling, e.g. of the feet, induces physiological alterations in the nasal mucosa [69,82,130], local (or general) cooling has failed to result in disease in volunteers, or even to make them more prone to catch a common cold infection in controlled experiments [10,66]. Common colds are brief, self-limited infections that do not affect the life expectancy of otherwise healthy and well-fed subjects. However, they can be a threat to patients who are immunocompromised, are malnourished or have severe cardiac or pulmonary disease. Malnourishment is a contributing factor in developing countries where the children affected suffer more persistent airway infections and more complications, mainly bronchopneumonia [106], which may lead to considerable mortality [51]. There are vast social, as well as economic consequences, as illustrated by an annual loss of 100 million working days in the USA where each episode of a common cold costs an estimated $15-40 for medications and diagnostic medical consultations [117].
The signs and symptoms of the common cold are the principal tools for identifying clinical infections. The viral aetiology is often verified by virological examinations of the nasal discharge and serological analyses. In practice,

84 Pathophysiology of viral respiratory tract infections
symptom scoring systems have been widely used to monitor the course of the infection [21,106]. Knowledge of the pathophysiology has been further extended by access to increasingly sophisticated objective physiological, biochemical and morphological methods. The nose is the outermost part of the respiratory tract and the port of entry for infective microbes; hence the nose is the part of the airways most frequently affected by viral infections [58]. The reactions in the airway mucosa are to some extent similar throughout the respiratory tract. Hence, nasal mucosal events also reflect the reactions of other parts of the airway mucosa to some extent [142]. The nose is easily accessible and therefore has been studied extensively. This chapter focuses on the nasal physiology and nasal pathophysiology in viral infections.
5.2 APPLIED PHYSIOLOGY OF THE RESPIRATORY TRACT
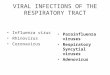
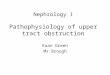
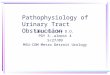
The anatomy and physiology relevant to the pathophysiology here presented is based on an extensive volume of reviews edited by Proctor and Andersen [147]. The air-conditioning function of the nose is essential to the whole of the respiratory system. The respiratory air is modified during its passage through the nose, according to the needs of the lower airways. Humans are exposed to ambient air with extreme temperatures that can range from -40°C to +40°C and humidity extremes that range from dry to saturated moist air. An adult human breathes 400 litres of air every hour at rest and considerably more during physical activity. The upper airways have the capacity to clean, warm and humidify the inspiratory air to 32°C in an ambient temperature of -20°C. The complex split-like lumen in the nose and the narrowing at the nasal valve cause turbulent airflow, which offers the ideal conditions for a high air-conditioning capacity [108] (Figure 5.1).
Figure 5.1 Computed tomographic image (coronal projection) showing a cross-section of the nasal cavity of a normal individual. Note the asymmetry in mucosal swelling which is due to the nasal cycle.
5.2.1 NASAL STRUCTURE
The rigid bony nasal cavity is covered by erectile tissue, the nasal mucosa, which is lined by a ciliated epithelium. This pseudostratified cil~ iated epithelium also lines the paranasal sinuses, the Eustachian tube, the middle ear, the nasopharynx and the larynx (except the vocal cords). In the anterior part of the nose and towards the oropharynx, the epithelium gradually changes to squamous epithelium. The epithelium is covered by a secretion layer, which consists of a low-viscosity periciliary fluid layer under a high-viscosity mucous blanket. The turbulent airflow facilitates the deposition of particles inhaled from the ambient air on the mucous blanket. The latter is the first mechanical barrier which an infective microbe has to overcome. The activity of the epithelial cell cilia is co-ordinated with ciliary beats 10-20 times per second and the cooperation of many cells results in a continuous systematic propulsion of the mucous blanket. The

mucociliary transport system thus clears the airway from dust, pollen and microbes. In the mucus, secretory antibodies - mainly IgA - are present as the first line of immunological defence. The mucus thus has characteristics important for defence against viruses and other microbes deposited in the nose. Additional defence capacity is available in the tissue where inflammatory cells playa major role. The healthy nasal mucosa contains a small number of cells which, if activated, may participate in and escalate an inflammatory reaction. The lymphocyte, the most common cell type, is mainly located in the subepithelial layer. T-cells are the most numerous, T-helper cells outnumbering T -suppressor cells and are, primarily, periglandular. The B-cells are located mainly in the lamina propria, occasionally in clusters [188].
(a)
Applied physiology of the respiratory tract 85
5.2.2 NASAL FUNCTION
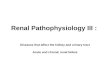
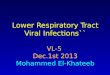
The air-conditioning function of the nose is regulated mainly by adjustments in the vasculature of the nasal mucosa. The abundant veins form networks of large vessels, sinusoids, which can pool considerable volumes of blood and, because of their swelling and shrinkage capacity, can regulate the patency of the nose (Figure 5.2). Under the effect of neurogenic mechanisms, the blood volume in the mucosa can change rapidly, and thereby within minutes adjust the nasal airway resistance and airflow pattern [53,147]. The turbulence of the airflow is essential for bringing the respiratory air into contact with the mucosa.
Nasal blood flow
Arteriovenous shunts allow the mucosa to be heated by blood at core temperature when
(b)
e c
9
s
71lllllllllllll
Figure 5.2 (a) Histopathological view of biopsy from a healthy nasal mucosa and (b) schematic drawing of nasal mucosal vasculature. a, arteries; c, capillaries; e, epithelium; g, submucosal glands; s, sinusoids; v, veins.

86 Pathophysiology of viral respiratory tract infections
required. An extensive system of fenestrated capillaries delivers water to the inspired air. The blood flow in the nasal mucosa, which is regulated by the tone of the arterioles, is about 35 mVmin/l00 g tissue [28]. Such a blood flow, which is 10 times that of the skin, exceeds the nutritive demands of the mucosa. The high blood flow in the nasal mucosa can rapidly activate the humoral systems for defence against viruses and bacteria. To understand the function of the nose it is important to distinguish between blood flow and blood content. Sometimes these parameters change in the same direction: e.g. in the common cold where there is an increase in both the blood flow and the blood content. However, in physiological conditions, blood flow and blood content can change in opposite directions [2,138]. The blood content and the amount of oedema in the nasal mucosa are responsible for the mucosal thickness and thereby regulate nasal patency. This nasal patency is proportional to the nasal airway resistance. Consequently, the blood content of the mucosa can be assessed objectively by rhinomanometry. The temperature of the nasal mucosa is a crucial factor for the regulation of humidity and heat from both inspired and expired air [147]. This is regulated by the blood flow in the mucosa and it is also influenced by the temperature and volume of the airflow through the nose. During normal conditions, the temperature of the nasal mucosa is several degrees below the body core temperature, about 30°C, and about 2°C higher in the expiratory breathing phase [2,69,182].
Nasal patency
Under physiological conditions there exists a circadian variation in nasal secretions [131]. There is, also, a periodic variation in nasal patency, a physiological phenomenon referred to as 'the nasal cycle'. This is regulated by the sympathetic nervous system whereby the blood content in the mucosa
changes asymmetrically, causing cyclical and reciprocal changes in the resistance to airflow every 2-4 hours. This phenomenon is present in about 80% of healthy subjects [81,147]. However, the subjective feeling of nasal patency can be illusory and does not always correspond to the objectively measured nasal airway resistance. It is a common experience, for instance, that the inhalation of cold air causes a sensation of increased patency, while the exposure to heat causes a feeling of stuffiness. Cold sensation in the nose is accompanied by increased airflow sensation [73] although inhalation of cold air actually causes nasal mucosal congestion [25,69].
An increase in sympathetic activity decongests the nasal mucosa by constricting the capacitance vessels [126]. Powerful decongestion - I maximal decongestion' - is achieved after physical exercise at pulse rates over 120 beats/min. This is physiological and supplies a maximally widened airway for the best achievable ventilation. Exercise-induced decongestion can be used to distinguish between nasal obstruction due to structural defects and to obstruction caused by mucosal swelling. Mucosal swelling depends on the body position and increases in the supine position, a phenomenon which is accentuated in infectious rhinitis [54,133,158]. Some of the various reflexes that involve the nasal mucosa have a pathophysiological significance. For example, cooling of the extremities induces a reflectory rapid decrease in the nasal mucosal blood flow, a reflex mediated by sympathetic nerve fibres [134]. Irritants deposited in the nose, e.g. dust in the ambient air, initiate the protective and airway-clearing sneezing reflex.
Sensory function
The senses of smell and hearing and the ability to speak are perceptive and communicative functions associated with the upper airway. Odours are perceived via the olfactory epithe-

lium, which is located in the superior part of the nasal passage. A turbulent airflow through the nose, an adequate nasal patency in the upper nasal cavities and the ability to sniff, are necessary prerequisites for an optimal function of the sense of smell. The sensation of smell can be assessed by the detection of odour intensity - for example, by threshold tests or odour quality - by identification tests.
Speech.
This is executed through the airways where the larynx is the source of sound. During the phonation a pulsating expiratory airstream flows through the oscillating vocal cords, generating the basic sound for speech. The sound is modified by the resonating rooms in the upper airways and by modifications of the tongue and lips to characterize the sophisticated details of speech and the subject's distinctive voice.
The ear.
This converts sound waves to nerve signals which are processed in the central nervous system. The middle ear transfers the sound waves as vibrations to the fluids of the inner ear. Effusion in the middle ear, as in secretory otitis media, leads to a conductive hearing loss. The middle ear and the Eustachian tubes should not be forgotten as parts of the upper respiratory tract. The Eustachian tube maintains a middle ear pressure equivalent to the ambient atmospheric pressure but it is closed to the rapid changes in air pressure in the nasopharynx that are induced by normal breathing. If the closing is suboptimal, a tuba aperta will lead to an inability to close off the sounds of breathing and a disturbed feed-back hearing of the subject's own voice. The Eustachian tube is the common route of entry for the infective microbes that cause acute middle-ear infections.
The paranasal sinuses are anatomical structures of the respiratory tract, which have an
Pathophysiology of common colds 87
obscure function (Figure 5.1). The mucociliary system in the sinus mucosa is similar to that in the nose, but the vascular arrangement in the mucosa is different. There are few, if any, sinusoidal vessels in the sinus mucosa, but the blood flow is as high as that in the nose. The patency of the sinus ostium is essential for adequate sinus ventilation [147]. During nasal breathing, there is a continuous exchange of air in the paranasal sinuses and half of the maxillary sinus volume of air is exchanged in about 30 minutes [137]. The size of the maxillary sinus ostium varies with body posture as in the case of posture effects on the nasal mucosa [15,107,125].
5.3 PATHOPHYSIOLOGY OF COMMON COLDS
The patient history and the clinical investigation form the basis for diagnosing common colds in clinical practice. The signs found in the clinical investigation include changes in the airway mucosa, swelling, reddening and pathological discharge, sometimes antral sinus tenderness, watery eyes, cervical lymphadenitis or secretory otitis media. The symptoms of the common cold are mainly nasal - blockage and discharge (Figure 5.3) [178]. However, symptoms from all parts of the respiratory tract, such as the paranasal sinuses, ears, throat, larynx, trachea and bronchi, are seen. More general symptoms, like headache, malaise, chills and sometimes fever, are also present. The clinical signs and symptoms are not specific for inflammations caused by infections and the patient history is important for distinguishing toxic or allergic inflammation and non-specific hyperreactivity.
5.3.1 EPITHELIAL CHANGES
The viruses mainly infect the ciliated epithelium in the nose. They damage the cells and various viral pathogens are associated with different degrees of destruction of the respiratory epithelium [102]. Histopathological damage to the

88 Pathophysiology of viral respiratory tract infections
80
~ en E .9 60 a. E >. en '0 Q)
g 40 Q) (ij > Q) .... a..
20
0 c: .2 U S IJ)
.0 0
co iii Cl Q) e c: 0 ·N .s:::. :: Q) .... (5 Q)
~ c: C 0 (J) :E (J) a:
Q) .s:::. Q) IJ) IJ) Cl .s:::. IJ) ·ffi :::J 0 Q)
(1j 0 <II c: ::E u "0 Q)
co ~ Q) <II I 0 I
Ui'ill Hev
fI ASV
II HAV
c: .2 19 ·c .~ Q) >. w
IJ) IJ) .!l! Q) Ol
~ (1j >.
:E ::E u
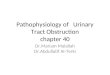
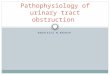
Figure 5.3 The prevalence of symptoms reported after nasal inoculation of virus. The most common are the nasal symptoms and a sore throat; the severity of symptoms is similarly distributed. The error bars indicate the range of the prevalence of symptoms with rhinoviruses types 2, 9 and 14. HRV, rhinovirus; HeV, coronavirus; RSV, respiratory syncytial virus. (From [178] .)
epithelium results from experimental rhinovirus infections [64,103]. Investigations in subjects with natural colds revealed no pathological changes on light microscopy but, with the scanning electron microscope patchy damage to the epithelium was seen [185]. In interpreting these findings it should be held in mind that viral infection has a preference for the nasopharyngeal mucosa but can have a patchy distribution [187] and single biopsies may not be representative for the entire mucosa. Virus-infected epithe-
lial cells are shed during colds [176] but, even if a viral infection causes damage to the epithelium, this may not necessarily be great enough to disturb the epithelial function as a mechanical barrier. This aspect has been investigated in coronavirus colds, when the ability of the mucosa to absorb a luminally deposited macromolecular tracer was not significantly altered [89]. An impaired barrier function certainly cannot be ruled out with infection due to other viruses, bearing in mind the differences between

the effects of various viral pathogens on the morphology of the mucosal epithelium [102].
In colds, the function of the nasal mucociliary clearing system is impaired [86,159,184]. Impairment of this system is significant already when the symptoms begin, and is most pronounced when the symptoms reach peak scores. The impairment lasts for 2-3 weeks, but can persist for several weeks [139]. During common colds, the volume of nasal discharge increases and its composition changes [155]. The composition and viscosity of the mucus and the relation between the volumes of mucus and periciliary fluid are essential to an optimal function of the mucociliary clearing system. Changes during viral infection that affect these factors impair the clearance rate. Besides changes in the mucus there is a loss of ciliated cells in upper respiratory tract infections [176,184]. Also noted during common colds is a reduction in the number of ciliated cells, an asynchronous and reduced ciliary beat frequency, and an increase in the proportion of living ciliated cells with immotile cilia [139].
Lymphocytes, as well as poly- and mononuclear leucocytes increase in numbers in the nasal secretions during upper airway infections and the numbers are directly related to the severity of the symptoms. White cells also increase in the epithelium and in the lamina propria of the mucosa [114,185,186]. In virus infections the peripheral blood leucocyte population is altered, there being an increase in neutrophil granulocytes and a decrease in lymphocyte counts [44,47,65,101] due to a decrease in T-cells [113]. The presence of leucocytes at these sites in the mucosa, and in secretions, indicates that they actively contribute to the local inflammatory process and antiviral defence [95].
5.3.2 VASCULAR REACTIONS
Nasal blockage is the main symptom reported subjectively by patients [178] (Figure 5.3) and an increase in the nasal airway resistance has been confirmed objectively [5,27] (Figure 5.4).
Pathophysiology of common colds 89
60
-1 o 2 3 4 Day
Figure 5.4 Nasal airway resistance changes (v2-values) after inoculation of coronavirus in healthy subjects in relation to symptom scores (shaded). (From [27].)
5
The mechanisms causing nasal blockage in the common cold are multifactorial. There is congestion of blood in the erectile nasal mucosa; the relevance of this pooling of blood in sinusoidal capacitance vessels is illustrated by the prompt decongestant effect produced by vasoconstricting drugs [6]. Interstitial oedema usually explains the cardinal sign of inflammation - tumor. However, no data have been presented that convincingly show oedema in the nasal mucosa during the common cold. Obstruction by a large volume of highly viscous discharge is another obvious cause. The mucosal swelling, although uncomfortable, may be beneficial in the common cold. A reduced airflow, due to nasal obstruction, contributes to an increase in the temperature of the nasal mucosal surface, since it eliminates the cooling effect of the inspiratory nasal airflow (on the nasal mucosa). An increase in the local blood flow is a general phenomenon observed in inflammatory conditions responsible for the cardinal signs, calor and rubor. The nasal mucosal blood flow increases during a common cold [27] (Figure 5.5) and, with the

90 Pathophysiology of viral respiratory tract infections
reduction of airflow, will contribute to an increase in nasal mucosal temperature. The increase in the mucosal surface temperature is 3-5°C, while the increase in body temperature is measured only in tenths of a degree centigrade [2,27] (Figure 5.6). The increase in the local temperature is, theoretically, a defence mechanism per se since the replication rate of many respiratory viruses is reduced above an optimal 33°C [136]. A further potentially beneficial effect is that other defence mechanisms (such as leukotaxis, phagocytosis and the production of interferon) are facilitated at higher temperatures [153]. The facilitation of cell migration is especially relevant because it may counteract the impairment of chemotaxis induced by viral infection [111].
5.3.3 RHINORRHOEA
Rhinorrhoea is another common phenomenon accompanying the common cold [178] (Figure 5.3). The volume of discharge collected in the nose increases due to incapacity of the mucociliary clearance and the discharge accu-
c; o o
60
~ 50 ·e .... E !I: 40 o ;:
"8 :c 30 <ti ~ () ::> E 20 ]i 10 Z
·1 o 1 2 3 4 Day
Figure 5.5 Nasal mucosal blood flow changes (mVmin/lOO g tissue) after inoculation of coron· avirus on day 0 in healthy subjects in relation to symptom scores (shaded). (From [27] .)
5
mulates in the nose and requires clearance in alternative ways (Figure 5.7). The composition of the discharge may differ between individuals and it changes during an infection [104]. Furthermore, the composition and characteristics of the discharge may vary as a result of factors such as biorhythms, climate and the presence of non-specific irritants. Potential sources of the nasal discharge include the water condensed from humid expired air, secretions from serous and seromucous glands, epithelial cells, goblet cells and fluids from the mucosal microcirculation. The origin of the increased nasal discharge in viral infections is still a matter of speculation. There is no reason to believe that the condensation from humidity will increase significantly in the common cold. Active transport of chloride ions causes a flow of water from epithelial cells in response to mediators. The density of goblet cells in the nasal mucosa increases transiently during viral infections [173]. Glandular secretions contribute to the rhinorrhoea stimulated by mediators and neural reflexes [37,104]; these secretions are mainly derived from sero-
35
2: 33 l!!
~ ~ 31 E .!
~ 29 ::> E ]i ~ 27
· 1 o 1 2 3 4 Day
Figure 5.6 Nasal mucosal temperature changes CC) after inoculation of corona virus on day 0 in healthy subjects in relation to symptom scores (shaded). (From [27].)
5

mucous glands in the mucosa, with a minor contribution from intraepithelial and anterior serous glands. The significance of the glandular contribution, however, can be questioned in the common cold, since anticholinergic drugs which block glandular secretion, far from abolish the increased secretion [38,62,68,84]. It seems contradictory that anticholinergics appear to be effective during the first days of infection [38], while the glandular secretory contribution to the rhinorrhoea tends to predominate in a later phase of the infection [104].
The presence of plasma proteins in the discharge during a common cold indicates that the nasal mucosal microcirculation contributes to the discharge in inflammatory conditions [7,40,132,155] and that an inflammatory exudate, rather than a transudate, is the origin of the fluid. Plasma exudation across the endothelial and epithelial barriers is thought to be a specific feature of inflammation [141]. It is a finely regulated and controlled process with a selective outward bulk flux of plasma solutes through morphologically intact barriers. The
10
0;8 ..s Q) Cl (ij 6
.£:. U <J)
'5 g$4 o -E <5 c: :22 oc
0'----'---......... - ....... = -1 o 1 2
Day 3 4 5
Figure 5.7 Rhinorrhoea assessed by weight of used paper handkerchiefs after inoculation of coronavirus on day 0 in healthy subjects in relation to symptom scores (shaded). (From [27].)
Pathophysiology of common colds 91
first barrier is the vascular endothelium. Inflammatory mediators cause endothelial cell contraction in the postcapillary venules, allowing bulk plasma to extravasate through the gaps in the endothelium driven by the hydrostatic pressure [57,121,172]. The second barrier is the airway mucosal epithelium. It has been suggested that the extravasated plasma molecules, via osmotic forces, increase the subepithelial hydrostatic pressure. The pressure forces the epithelium to widen its intracellular spaces and this opens a trans epithelial paracellular route for the flux of macromolecules into the airway lumen. This flux is unidirectional and outwardly directed because of the pressure gradients [140-142] . The exudates in the common cold occur concominantly with the major symptoms and may be a crucial defence mechanism against infection by virtue of providing humoral antibodies and other potent plasma proteins access to the mucosal surface [5]. This mechanism may also be of pathogenic significance, enabling these substances to contribute to symptoms as a result of the induction of inflammatory cascades. Besides the mechanical flushing effect, the non-specific effects of the plasma exudate include inactivation of microbes by enzymatic degradation and binding to plasma proteins. The amount of total protein in nasal secretions has been found to be positively related to resistance to rhinovirus infection [156]. Specific immunity develops and the amounts of secretory IgA and humoral IgG are of importance in mucosal infections [43]. Together with products from the glandular secretions, several molecules with antimicrobial activity are present in human discharges, including glycoproteins showing antiviral activity [123], the antibacterial glandular protein lactoferrin [157] and lysozyme [39,151,154].
5.3.4 THE INFLAMMATORY PROCESS
The inflammatory process in the nasal mucosa that results from a viral infection is complex.

92 Pathophysiology of viral respiratory tract infections
The multiple mechanisms and mediators involved interact in a cascade of events resulting in overt symptomatic disease. Parts of this process are known, but the knowledge is still to some extent incomplete. Specific immunity will not be discussed as it is presented in chapters on individual viruses.
The innate non-specific mechanisms include exudation and binding by plasma proteins. Four distinct enzyme systems participate to modulate the inflammation. These are the clotting and fibrinolytic systems, and the kinin and the complement systems [122]. The prerequisite for their action in the first line of defence is their presence on the mucosal surface, which is achieved through the inflammatory exudation of unfiltered bulk plasma. Fibrinogen is found on the mucosal surface in the common cold [5]. The fibrinopeptides participating in the inflammatory process induce leukotaxis [163]. Fibrin and fibrin-fibronectin gels can repair epithelial damage in the airway. Furthermore, fibrin can facilitate the migration of immunopotent cells by supplying a matrix for inflammatory cell traffic and for re-epithelialization and revascularization of the airway mucosa [59]. The precursor of the kinin system, kininogen, is converted to bradykinin through the enzymatic action of kallikrein. The biological effects of bradykinin include smooth muscle contraction, vasodilatation and an increase in vascular permeability [77,146], and they contribute to nociceptive pain in inflammatory conditions [170]. Characteristic symptoms of the common cold, such as nasal obstruction, rhinorrhoea and sore throat (Figure 5.3), can be induced by nasal bradykinin provocation [150]. Bradykinin is found on the nasal mucosal surface during rhinovirus colds and the concentrations of kinins found in nasal lavages are related to the severity of symptoms [132,149]. Complement factors play an important role in the local inflammatory response. The presence of complement fractions C3b and C5a in lavage fluids has likewise been shown to be related to the symp-
toms encountered with a nasal influenza virus infection [34].
Cytokines.
These are small peptide regulatory molecules that participate in the modulation of inflammation. Interferons (IFNs) are a group of quickly mobilized endogenous proteins and glycoproteins and they are one of the cytokines which participate in modulation of the viral airway inflammation. Interferons also have an immediate inhibitory effect on virus replication. Two types have been identified: type 1 (IFN-a from lymphocytes and macrophages; IFN-13 from fibroblasts and epithelial cells) and type 2 (IFN-'Y from activated T-cells) [18]. Both types are present in nasal lavages from subjects with viral upper airway infections [48,96,109,116,125]. Another multipotent cytokine is interleukin-l (IL-l13), which is also found in nasal lavages during common colds [116,148]. IL-l13 and IFN-'Y are of special significance, since they can up-regulate the cellular surface receptor intercellular adhesion molecule-l (ICAM-l), which is the receptor most rhinoviruses use to adsorb to epithelial cells in order to infect [90,169]. Knowledge of the role of cytokines in viral airway infection remains fragmentary.
Nervous mechanisms
Nervous mechanisms also participate in the pathophysiology of airway inflammation. The airway mucosa is densely innervated by sensory and efferent nerves involved in nociception, protective reflexes and vascular and glandular control. In brief, cholinergic stimulation results in vasodilatation and glandular secretion, and adrenergic stimulation in vasoconstriction and cessation of glandular secretion. Neuropeptides are transmitter substances involved in the control of smooth muscle, blood flow, vascular permeability and glandular secretion in the airways. Tachykinins participate in the neurogenic inflammation, e.g. the

release of the sensory neuronal mediator substance P results in smooth muscle contraction, mucus secretion and increased microvascular permeability [118]. Vasoactive intestinal polypeptide (VIP) in parasympathetic nerves can induce vasodilatation, smooth muscle relaxation and possibly hypersecretion in the airways [17]. Consequently, nervous mechanisms can initiate symptoms indistinguishable from, and possibly be partly responsible for, symptoms of the common cold. Little is known about the role of these transmitters in viral respiratory airway inflammation.
It seems clear that the mediators of a viral infective inflammation differ from those of allergic inflammation, which is orchestrated mainly by mast cells, eosinophilic and basophilic granulocytes and the main mediator, histamine. In viral rhinitis basophils and mast cells do not appear to participate in the inflammatory process [74,132,185].
Inflammatory mediators
Inflammatory mediators are relevant because of their contribution to the development of disease. Histamine concentrations do not increase in rhinoviral rhinitis [132]. However, other viruses (RS virus and parainfluenza virus) seem to be able to induce histamine release in the nasal mucosa [180,181]. The failure of antihistamines alone to counteract the symptoms of viral rhinitis indicates that histamine is of no major significance in this inflammation.
Several arachidonic acid metabolites contribute to the pathogenesis of inflammation. Arachidonic acid can be transformed to bioactive molecules which have implications on inflammatory conditions via two major enzymatic pathways. The cyclooxygenase pathway leads to the formation of prostaglandins and thromboxanes, the lipoxygenase pathway to the formation of leukotrienes, hydroxyeicosatetraenoic acids (HETEs) and lipoxin [115]. Such arachidonic acid derivatives seem to be of no major importance in viral airway
Pathophysiology of common colds 93
inflammation and attempts to identify leukotrienes in nasal lavages from subjects with viral rhinitis have failed [45]. There is no convincing evidence of an active role of prostaglandins in viral rhinitis and furthermore, prostaglandin inhibitors have no obvious effect on the local inflammatory symptoms [87].
5.3.5 EFFECTS ON OTHER FUNCTIONS IN THE UPPER AIRWAYS
Olfaction
Upper respiratory tract infections are often associated with an altered ability to smell and there is an impairment of the ability to detect odours during a common cold. This impairment correlates with the degree of nasal blockage and, to a lesser extent, the volume of nasal discharge, which suggests that the alteration in the characteristics of the mucus and in the pattern of airflow result in an impaired access of the odour to the olfactory sensory epithelium [4]. Some upper airway infections - e.g. influenza - can induce long-lasting, and even permanent anosmia [60,63]. This anosmia is less likely to be due to a persistent nasal congestion, more to a damage of the olfactory epithelium. Moreover, a change in the perception of odours occurs in patients with rhinitis, for example previously pleasant odours being experienced as unpleasant. This phenomenon may be explained by the effects of a viral infection on the nervous system. Related to the impairment of smell is a loss of the appreciation of the taste of food which emphasizes the connection between taste and smell. In terms of food tasting, the olfactory function is of major importance. Only the basic distinguishable taste qualities - sweet, salty, bitter and sour - are identified by the taste buds in the mouth. A normal sense of smell is important for a good quality of life and impairment may be responsible for mood changes, as shown by the increased incidence of mental depression in people who become anosmic [129].

94 Pathophysiology of viral respiratory tract infections
Voice
When the vocal cords are involved in upper airway infections, local inflammatory oedema interferes with the vibratory characteristics of the vocal cords and results in hoarseness. The voice is also changed by alterations in resonance. The resonance of the upper airway is altered in common colds because of mucosal swelling causing nasal obstruction, leading to a hyponasal voice.
Middle ear
Common colds are associated with transient middle ear pressure abnormalities [75,124] and otitis media with effusion [41,174]. The mucosa of the middle ear is subject to infections by respiratory viruses and they can be isolated from this locus [14,50,92]. Pressure abnormalities and otitis media with effusion produce a temporary conductive hearing loss and supposedly predispose to bacterial purulent otitis media [110,161,174]. Acute purulent otitis media is the major complication of the common cold in children.
Paranasal sinuses
Sinus pain is experienced subjectively by one in three subjects with a common cold. Transient sinus mucosal abnormalities are at least as frequent [56,94,175]. Mucosal swelling of the maxillary and ethmoidal sinuses are the most common findings [94]. It must be held in mind, however, that sinus abnormalities are regularly noted on magnetic resonance imaging, and mucosal thickening and sinus fluid are frequent findings in subjects without any symptoms from the upper respiratory tract [56]. In sinusitis, there is viral infection of the sinus mucosa and respiratory viruses can be found in sinus aspirates [78,99]. Viral infection in acute rhinitis frequently affects the patency of the sinus ostium [71], an obstruction of which is considered to predispose to the development of sinusitis [70,189]. Viral infec-
tion of the upper respiratory tract is the principal underlying reason for the development of acute bacterial sinusitis [147].
5.3.6 HYPERREACTIVITY AND VIRAL EFFECTS
ON THE LOWER AIRWAYS
Recurrent colds are related to lower respiratory tract symptoms such as chronic cough, persistent wheezing or asthma in children [19]. Lower airway symptoms do not necessarily indicate an infection of the bronchial mucosa, even if virus can be found at this site [97], but could be induced by an upper air~ ways infection through nervous reflexes or inflammatory mediators. Viral upper airway infections induce hyperreactivity in all parts of the respiratory mucosa. Nasal hyperreactivity is present in viral upper airway infections since the exudative response is enhanced by histamine challenge in coronavirus common colds [89]. In upper airway infections there is also a bronchial hyperreactivity to cold air and exercise [13]. In normal subjects, bronchial reactivity is unchanged during and after rhinovirus infections [171] but it increases temporarily in association with symptomatic viral airway infections [12,76]. Subjects with allergic rhinitis show bronchial hyperreactivity during common colds when this is provoked pharmacologically [42]. When, on the other hand, asymptomatic subjects with an existing bronchial hyperresponsiveness were investigated for a possible viral aetiology, a previous viral infection did not seem to be a likely cause [16]. Viral airway infections can provoke bronchial obstruction, with wheezing in children, as well as obstructive episodes in persons with asthma [33,105,127,128]. The relation between infections and asthma remains controversial [52] and any link between infection and asthma remains speculative. In addition to bronchial hyperreactivity, peripheral pulmonary functions are also affected in viral upper respiratory tract infections [49,145].

Pathophysiological aspects of symptomatic treatment 95
5.3.7 CIRCADIAN VARIATIONS
In viral upper airway infections the most severe symptoms are found in the mornings [165]. This is in accordance with the finding that the most intense inflammatory activity, seen as plasma exudation, occurs during the morning [88]. Other periodic variations include an enhancement of the nasal cycle in the common cold, a greater asymmetry in nasal airway resistance accompanying the increased symptoms [27,183]
5.4 PATHOPHYSIOLOGICAL ASPECTS OF SYMPTOMATIC TREATMENT
Up till now, no drugs have been used regularly in clinical practice to treat the causes of the common cold and only symptomatic treatment is available, many approaches having been tried for generations. High doses of vitamin C have been thought to have a prophylactic effect on the duration of symptoms [100]. However, several investigators have failed to show any positive effect of vitamin C as a means of treating or preventing colds [46,179]. The inhalation of aromatic vapours, such as menthol induces a sensation of increased nasal patency and relief of nasal blockage, even if it has no effect on objective nasal airway resistance in healthy subjects [73] or in subjects with colds [72]. It seems plausible that the temperature of the nasal mucosa is significant for the pathogenesis of colds. Studies of the propagation and basic biology of rhinoviruses reveal that they grow optimally at 33°C and that their growth is impaired at higher temperatures [136]. Consequently, by increasing the nasal mucosal temperature the viral replication can be inhibited and in accordance, inhalation of hot steam seems to decrease the severity and duration of symptoms [120,135,177].
5.4.1 ANTI-INFLAMMATORY DRUGS
Anti-inflammatory drugs, such as glucocorticoids and nedocromil sodium nasal spray, commonly used in treating allergic rhinitis, appear
to improve significantly the symptoms of rhinovirus colds [20,79]. The mechanisms of action of these drugs need further study but effects on cytokines are likely to contribute. Non-steroidal anti-inflammatory drugs (NSAIDs) are frequently used in upper airway infections and can reduce fever, myalgia and malaise [167]. These drugs affect virus shedding and immune system functions in common colds. In one study, aspirin was reported to increase virus-shedding in rhinovirus infec-tions [168] but this could not be confirmed in a study where, on the other hand, aspirin was associated with the suppression of the serum neutralizing antibody response [87]. Although, this suppressed response theoretically may be important, normally aspirin should not have a significant negative clinical effect [87].
5.4.2 ANTI-MEDIATOR DRUGS
Anticholinergic drugs.
These have minor but statistically significant effects on rhinorrhoea [38,62,84]. These will inhibit the glandular secretion from the cholinergically innervated submucous glands but are not likely to affect goblet cells, fenestrated capillaries or plasma exudation. The blocking of glandular secretion could be less favourable for the course of the infection, since the nasal secretions contain components which contribute to the mucosal defence. Such aspects, however, have not been elucidated satisfactorily.
Histamine is not a mediator of viral upper airway inflammation and not surprisingly, antihistamines have little or no effect on symptoms in experimental rhinovirus infections [67,83] and in naturally acquired colds [32,85].
5.4.3 DECONGESTANTS
Oral sympathomimetics.
These have an effect on subjective as well as objectively measured nasal congestion [112], but the effect after a single dose is not sufficient for symptomatic relief in the common

96 Pathophysiology of viral respiratory tract infections
cold [91]. The oral sympathomimetics are often used in combinations with other drugs. However, additive effects by combinations are rarely reported even if the individual effects of the drug combinations together can reduce the total symptoms [93].
Topical nasal decongestants (nosedrops).
These fulfil most of the criteria for an ideal symptomatic treatment, namely that it should be effective, easily accessible, well tolerated, inexpensive and should not counteract the defence mechanism of the host. Decongestive nosedrops fall into two categories - the sympathomimetic amines (e.g. phenylephrine hydrochloride) and the imidazoline derivatives (e.g. oxymetazoline hydrochloride and xylometazoline hydrochloride). Congestion of the nasal mucosa in acute rhinitis is due to vasodilatation of the sinusoids and to interstitial oedema. Nosedrops act by constricting the sinusoids in the nasal mucosa, the onset of action occurs within 10 minutes and the duration of the decongestive effect is about 4-8 hours [6,31,55,98]. These positive effects have led to the widespread use of these drugs, especially since they are accessible as over-thecounter drugs. The proper indication for the use of nosedrops is nasal blockage in the common cold. If the use of nosedrops continues for weeks or even months, a rebound congestion develops [3,35,80,119,152].
Imidazoline derivatives.
These are selective o:z-adrenoceptor agonists, while sympathomimetic amines act on 0:1-
adrenoceptors [8]. This different mode of action may be important because in humans the sinusoids in the nasal mucosa are regulated by 0:1-, as well as o:z-adrenoceptors, while the nasal mucosal blood flow is not significantly affected by O:I-adrenoceptor agonists [9,24]. Along with their desirable decongestive effect, treatment with nasal decongestants of the imidazoline type leads to a decreased blood flow which has a duration of about 6
hours [31]. In clinical doses the reduction in the blood flow after oxymetazoline nosedrops is about 50% in healthy subjects and about 60% of the increased blood flow in patients with the common cold [22]. In common colds the mucociliary function, as previously discussed, is inhibited. Nosedrops can possibly promote [160, 164], as well as inhibit the mucociliary activity and the difference may be due to different effects by different doses [1441 or to added preservatives [61]. An eventual promoting effect does not diminish the impairment of activity seen in common colds [143]. Even protracted use of nosedrops in healthy individuals does not seem to affect mucociliary clearance [143].
Calor and rubor.
These are cardinal signs of infection, caused by an increase in the local blood flow. Drugs interfering with blood flow interfere with the local defence reaction and may counteract an adequate inflammatory response. The basic studies in humans regarding the effects of topical nasal decongestants, other than decongestion, have so far been insufficient. In the rabbit, topical oxymetazoline reduces the nasal mucosal blood flow dose-dependently, with similar effects as in humans [1,30]. Furthermore, the application of oxymetazoline nosedrops in the nasal cavity induces a decrease in the mucosal blood flow in the maxillary sinus [1]. Experiments in this species, however, indicate the existence of less desirable effects on the inflammatory mechanisms. The reduction in blood flow may induce ischaemia in the mucosa, as illustrated by the presence of a microcirculatory phenomenon called vasomotion [30] - i.e. periodic oscillations in blood flow, a mechanism that is thought to optimize tissue perfusion during low-flow conditions. Vasomotion is mobilized when the reduction in local blood flow causes ischaemia in the tissue [36,162]. Nosedrops also inhibit the leucocyte migration during the first 2 hours of a provoked inflammatory reaction but whether

Pathophysiological aspects of symptomatic treatment 97
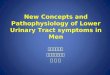
this is due to ischaemia or other causes [23] associated with a reduced vascular permeability [29] is not clear. Oxymetazoline nosedrops seem to prolong the infection in nasal and
(b)
Oxymetazoline
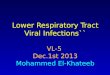
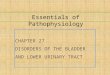
sinus mucosa. In an experimental bilateral bacterial sinusitis nosedrops induce a more pronounced inflammatory reaction 2 days after treatment with oxymetazoline [26] (Figure 5.8).
(c)
Saline
Figure 5.8 (a) Light microscopy of a cross-section through the sinus mucosa of a rabbit 2 days after induction of bilateral sinusitis. (b) One side was treated with topically applied decongestant nosedrops (oxymetazoline) and the other with placebo (saline). Note the increased inflammatory cell invasion on the actively treated side, indicating a more pronounced inflammation due to treatment.

98 Pathophysiology of viral respiratory tract infections
In conclusion, the extensive use of topically administered decongestive nosedrops in upper respiratory tract infections contrasts with the lack of studies concerning the side effects of these drugs [166].
5.5 REFERENCES
1. Akerlund, A., Arfors, K-E., Bende, M. et al. (1993) Effect of oxymetazoline on nasal and sinus mucosal blood flow in the rabbit as measured with laser-Doppler flowmetry. Ann. Otol. Rhinal. Laryngol., 102, 12~.
2. Akerlund, A. and Bende, M. (1989) Nasal mucosal temperature and the effect of acute infective rhinitis. c/in. Otolaryngol., 14, 529-34.
3. Akerlund, A. and Bende, M. (1991) Sustained usage of xylometazoline nose-drops aggravates vasomotor rhinitis. Am. ]. Rhinal., 5, 157-60.
4. Akerlund, A., Bende, M. and Murphy, C. (1994) Olfactory threshold shift during common cold is due to rhinorrhea and nasal blockage. Acta Otolaryngol. (Stockh)., 115, 88-92.
5. Akerlund, A., Greiff, L., Andersson, M. et al. (1993) Mucosal exudation of fibrinogen in coronavirus-induced common colds. Acta Otolaryngol. (Stockh), 113,642-8 .
6. Akerlund, A., Klint, T., Olen, L. et al. (1989) Nasal decongestant effect of oxymetazoline in the common cold: a dose-response study in 106 patients.]. Laryngol. Otol., 103, 743-6.
7. Anderson, T., Riff, L. and Jackson, G. (1962) Immunoelectrophoresis of nasal secretions collected during a common cold: observations which suggest a mechanism of seroimmunity in viral respiratory infections. ]. Immunol., 89, 691-7.
8. Andersson, K-E. (1980) Adrenoceptors - classification, activation and blockade by drugs. Postgrad. Med. ].,56,7-16.
9. Andersson, K-E. and Bende, M. (1984) Adrenoceptors in the control of human nasal mucosal blood flow. Ann. Otol. Rhinal. Laryngol., 93, 179--82.
10. Andrewes, C. (1959) Adventures among viruses. III The puzzle of the common cold. N. Engl. ]. Med., 242, 235-40.
11. Andrewes, c., Chaproniere, D., Gompels, A. et al. (1953). Propagation of common-cold virus in tissue cultures. Lancet, ii, 546-7.
12. Annesi, I., Oryszcyn, M., Neukirch, F. et al. (1992) Relationship of upper airways disorders to FEV1
and bronchial hyperresponsiveness in an epidemiological study. Eur. Respir.]., 5, 1104-10.
13. Aquilina, A., Hall, W., Douglas, G. et al. (1980) Airway reactivity in subjects with viral upper respiratory tract infections: the effects of exercise and cold air. Am. Rev. Respir. Dis., 122, 3-10.
14. Arola, M., Ziegler, T., Lehtonen, O. et al. (1990) Rhinovirus in otitis media with effusion. Ann. Otol. Rhinal. Laryngol., 99, 451-3.
15. Aust, R. and Drettner, B. (1975) The patency of the maxillary ostium in relation to body posture. Acta Otolaryngol. (Stockh), 80, 443-6.
16. Backer, V., Ulrich, c., Bach-Mortensen, N. et al. (1993) Relationship between viral antibodies and bronchial hyperresponsiveness in 495 unselected children and adolescents. Allergy, 48, 240-7.
17. Baraniuk, J., Lundgren, J., Okayama, M. et al. (1990) Vasoactive intestinal peptide in human nasal mucosa.]. c/in. Invest., 86, 825-31.
18. Baron, S., Stanton, G., Fleischmann, W.J. et al. (1987) Introduction: general considerations of the interferon, in The Interferon System. A Current Review to 1987, (eds S. Baron, F. Dianzani, G. Stanton et al.), University of Texas Press, Austin, Texas, pp. 1-17.
19. Barr, M., Weiss, S., Segal, M. et al. (1992) The relationship of nasal disorders to lower respiratory tract symptoms and illness in a random sample of children. Pediatr. Pulmonol., 14, 91--4.
20. Barrow, G., Higgins, P., Al-Nakib, W. et al. (1990) The effect of intranasal nedocromil sodium on viral upper respiratory tract infections in human volunteers. c/in. Exp. Allergy, 20, 45-51.
21. Beare, A. and Reed, S. (1977) The study of antiviral compounds in volunteers, in Chemoprophylaxis and Virus Infections of the Respiratory Tract, (ed. J. Oxford), CRC Press, Cleveland, pp. 27-55.
22. Bende, M. (1983) The effect of topical decongestant on blood flow in normal and infected nasal mucosa. Acta Otolaryngol(Stockh), 96,523-7.
23. Bende, M., Akerlund, A., Intaglietta, M. et al. (1992) The effect of nose drops on an acute sinusitis; an experimental study in the rabbit. Am. ]. Rhinal., 6, 55--8.
24. Bende, M., Andersson, K-E. and Johansson, C. (1985) Vascular effects of phenylpropanolamine on human nasal mucosa. Rhinology, 23, 43--8.
25. Bende, M., Angesjo, P., Hultsten, K et al. (1990) Effect of cold dry air on nasal airway resistance. Am. ]. Rhinal., 4, 65-7.

26. Bende, M., Arfors, K-E., Stierna, P. et al. (1995) Effect of oxymetazoline nose drops on acute sinusitis in the rabbit. Ann. Otol. Rhinol. Laryngol. (In press).
27. Bende, M., Barrow, 1., Heptonstall, J. et al. (1989) Changes in human nasal mucosa during experimental coronavirus common colds. Acta Otolaryngol. (Stockh), 107,262-9.
28. Bende, M., Flisberg, K., Larsson, 1. et al. (1983) A method for determination of blood flow with 133Xe in human nasal mucosa. Acta Otolaryngol. (Stockh), 96,277-85.
29. Bende, M., Hansell, P., Intaglietta, M. et al. (1992) Effect of oxymetazoline nose drops on vascular permeability of the nasal mucosa in the rabbit after provocation with leukotriene B4. J. Otorhinolaryngol., 54, 270-4.
30. Bende, M., Intaglietta, M. and Arfors, K-E. (1993) Nose drops induce vasomotion in the microcirculation of the sinus mucosa of the rabbit. J. Otorhinolaryngol., 55, 110-13.
31. Bende, M. and Loth, S. (1986) Vascular effect of oxymetazoline on human nasal mucosa. J. Laryngol. Otol., 100, 285-8.
32. Berkowitz, R. and Tinkelman, D. (1991) Evaluation of terfenadine for treatment of the common cold. Ann. Allergy, 67, 593-7.
33. Bjornsdottir, U. and Busse, W. (1992) Respiratory infections and asthma. Clin. Allergy, 76, 895-915.
34. Bjornson, A., Mellencamp, M. and Schiff, G. (1991) Complement is activated in the upper respiratory tract during influenza virus infection. Am. Rev. Respir. Dis., 143, 1062-6.
35. Blue, J. (1968) Rhinitis medicamentosa. Ann. Allergy, 26, 425-9.
36. Borgstrom, P., Schmidt, J., Bruttig, S. et al. (1992) Slow-wave flow motion in rabbit skeletal muscle after acute fixed-volume hemorrhage. Circ. Shock, 36, 57-61.
37. Borson, D. and Nadel, J. (1990) Regulation of airway secretions: role of peptides and proteases, in Rhinitis and Asthma: Similarities and Differences, (eds N. Mygind, U. Pipkorn and R. Dahl), Munksgaard, Copenhagen, pp. 76-99.
38. Borum, P., Olsen, L., Winther, B. et al. (1981) Ipratropium nasal spray: a new treatment for rhinorrhea in the common cold. Am. Rev. Respir. Dis., 123, 418-20.
39. Bowes, D., Clark, A. and Corrin, B. (1981) Ultrastructural localization of lactoferrin and
References 99
glycoprotein in human bronchial glands. Thorax, 36, 108-15.
40. Butler, W., Waldmann, T., Rossen, R. et al. (1970) Changes in IgA and IgG concentrations in nasal secretions prior to the appearance of antibody during viral respiratory infection in man. J. Immunol., 105, 584-91.
41. Bylander, A. (1984) Upper respiratory tract infection and Eustachian tube function in children. Acta Otolaryngol. (Stockh), 97,343-9.
42. Calhoun, W., Swenson, c., Dick, E. et al. (1991) Experimental rhinovirus 16 infection potentiates histamine release after antigen bronchoprovocation in allergic subjects. Am. Rev. Respir. Dis., 144, 1267-73.
43. Callow, K (1985) Effect of specific humoral immunity and some non-specific factors on resistance of volunteers to respiratory coronavirus infection. J. Hyg. (Camb), 95, 173-89.
44. Callow, K, Parry, H., Sergeant, M. et al. (1990) The time course of the immune response to experimental coronavirus infection of man. Epidemiol. Infect., 105, 435-46 .
45. Callow, K, Tyrrell, D., Shaw, R. et al. (1988) Influence of atopy on the clinical manifestations of corona virus infection in adult volunteers. Clin. Allergy, 18,119-29.
46. Carson, M., Cox, H., Cobett, M. et al. (1975) Vitamin C and the common cold. J. Soc. Occup. Med., 25, 99-102.
47. Cate, T., Couch, R. and Johnson, K. (1964) Studies with rhinoviruses in volunteers: production of illness, effect of naturally acquired antibody, and demonstration of a protective effect not associated with serum antibody. J. Clin. Invest., 43, 56-67.
48. Cate, T., Douglas, R. Jr and Couch, R. (1969) Interferon and resistance to upper respiratory virus illness. Proc. Soc. Exp. Bioi. Med., 131, 631-6.
49. Cate, T., Roberts, T., Russ, M. et al. (1973) Effect of common cold on pulmonary function. Am. Rev. Respir. Dis., 108, 858-65.
50. Chonmaitree, T., Howie, V. and Truant, A. (1986) Presence of respiratory viruses in middle ear fluids and nasal wash specimens from children with acute otitis media. Pediatrics, 77, 698-702.
51. Chretien, J., Holland, W., Macklem, P. et al. (1984) Acute respiratory infections in children. A global public-health problem. N. Engl. J. Med., 310, 982-4.

100 Pathophysiology of viral respiratory tract infections
52. Clarke, C. (1979) Relationship of bacterial and viral infections to exacerbations of asthma. Thorax, 34, 344-7.
53. Cole, P. (1993) Nasal and oral airflow resistors. Site, function, and assessment. Arch. Otolaryngol. Head Neck Surg., 118, 790-3.
54. Cole, P. and Haight, J. (1984) Posture and nasal patency. Am. Rev. Respir. Dis., 129, 351-4 .
55. Connell, J. (1969) Effectiveness of topical nasal decongestants. Ann. Allergy, 27, 541-6 .
56. Cooke, L. and Hadley, D. (1991) MRI of the paranasal sinuses: incidental abnormalities and their relationship to symptoms. J. Laryngol. Otol., 105, 278-81.
57. Cotran, R. and Majno, G. (1964) The delayed and prolonged vascular leakage in inflammation. I. Topography of the leaking vessels after thermal injury. Am. J. Pathol., 45, 261-81.
58. Couch, R., Cate, T., Douglas, R. et al. (1966) Effect of inoculation on experimental respiratory viral disease in volunteers and evidence for airborne transmission. Bacterial. Rev., 30, 517-27.
59. Crouch, E. (1990) Pathobiology of pulmonary fibrosis. Am. J. Physiol., 259, L159-84.
60. Davidson, T., Jalowayski, A., Murphy, C. et al. (1987) Evaluation and treatment of smell dysfunction. West. J. Med., 146, 434-8.
61. Deitmer, T. and Scheffler, R. (1993) The effect of different preparations of nasal decongestants on ciliary beat frequency in vitro. Rhinology, 31, 151-3.
62. Dockhorn, R., Grossman, J., Posner, M. et al. (1992) A double-blind, placebo controlled study of the safety and efficacy of ipratropium bromide nasal spray versus placebo in patients with the common cold. J. Allergy CZin. Immunol., 90,1076-82.
63. Doty, R. (1979) A review of olfactory dysfunctions in man. Am. J. Otolaryngol., 1, 57-79 .
64. Douglas, R., Alford, B. and Couch, R. (1968) Atraumatic nasal biopsy for studies of respiratory virus infection in volunteers. Antimicrob. Agents Chemother., 8, 340-3.
65. Douglas, R., Alford, R., Cate, T. et al. (1966) The leukocyte response during viral respiratory illness in man. Ann. Intern. Med., 64, 521-30.
66. Dowling, H., Jackson, G., Spiesman, I. et al. (1958) Transmission of the common cold to volunteers under controlled conditions. III. The effect of chilling of the subjects upon susceptibility. Am. J. Hyg., 68, 59-65.
67. Doyle, W., McBride, T., Skoner, D. et al. (1988) A double-blind, placebo controlled clinical trial of the effect of chlorpheniramine on the response of the nasal airway, middle ear and Eustachian tube to provocative rhinovirus challenge. Pediatr. Infect. Dis., 7,229-38.
68. Doyle, W., Riker, D., McBride, T. et al. (1993) Therapeutic effects of an anticholinergic-sympathomimetic combination in induced rhinovirus colds. Ann. OtoI. Rhinal. Laryngol., 102,521-7.
69. Drettner, B. (1961) Vascular reactions of the human nasal mucosa on exposure to cold. Acta Otolaryngol. (Stockh), Suppl., 166.
70. Drettner, B. and Aust, R. (1977) The patency of the maxillary ostium in relation to body posture. Acta Otolaryngol. (Stockh), 83, 16-19.
71. Drettner, B. and Lindholm, C.-E. (1967) The borderline between acute rhinitis and sinusitis. Acta Otolaryngol. (Stockh), 64,508-13.
72. Eccles, R., Jawad, M. and Morris, S. (1990) The effect of oral administration of menthol on nasal resistance to airflow in subjects suffering from nasal congestion associated with the common cold. J. Pharm. Pharmacal., 42, 652-4.
73. Eccles, R. and Jones, A. (1983) The effect of menthol on nasal resistance to air flow. J. Laryngol. Otol., 97, 705-9.
74. Eggleston, P., Hendley, J. and Gwaltney, J. Jr (1984) Mediators of immediate hypersensivity in nasal secretions during natural colds and rhinovirus infection. Acta Otolaryngol. (Stockh), Suppl. 413, 25-35.
75. Elkhatieb, A., Hipskind, G., Woerner, D. et al. (1993) Middle ear abnormalities during natural rhinovirus colds in adults. J. Infect. Dis., 168, 618-21.
76. Empey, D., Laitinen, L., Jacobs, L. et al. (1976) Mechanisms of bronchial hyperreactivity in normal subjects after upper respiratory tract infection. Am. Rev. Respir. Dis., 113, 131-9.
77. Erjefalt, I. and Persson, C. (1991) Allergen, bradykinin, and capsaicin increase outward but not inward macromolecular permeability of guinea-pig tracheobronchial mucosa. CZin. Exp. Allergy, 21, 217-24.
78. Evans, F., Sydnor, J., Moore, W. et al. (1975) Sinusitis of maxillary antrum. N. Engl. J. Med., 293,735-9.
79. Farr, B., Gwaltney, J. Jr, Hendley, J. et al. (1990) A randomized controlled trial of glucocorticoid prophylaxis against experimental rhinovirus infection. J. Infect. Dis., 162, 1173-7.

80. Feinberg, A. and Feinberg, S. (1971) The 'nose drop nose' due to oxymetazoline (Afrin) and other topical vasoconstrictants. Illinois Med. ]., 140,50-2.
81. Fischer, E., Scadding, G. and Lund, V. (1993) The role of acoustic rhinometry in studying the nasal cycle. Rhinology, 31, 57-61.
82. Flisberg, K. and Ingelstedt, S. (1962) Vascular responses to feet cooling in normal and allergic nose. Acta Otolaryngol. (Stockh), 55,457-66.
83. Gaffey, M., Gwaltney, J. Jr, Sastre, A. et al. (1987) Intranasally and orally administered antihistamine treatment of experimental rhinovirus colds. Am. Rev. Respir. Dis., 136, 556-60.
84. Gaffey, M., Hayden, F., Boyd, J. et al. (1988) Ipratropium bromide treatment of experimental rhinovirus infection. Antimicrob. Agents Chemother., 32, 1644-7.
85. Gaffey, M., Kaiser, D. and Hayden, F. (1988) Ineffectiveness of oral terfenadine in natural colds: evidence against histamine as a mediator of common cold symptoms. Pediatr. Infect. Dis., 7,223-8.
86. Ginzel, A. and Iilum, P. (1981) Messung des Schleimtransportes in der Nase an Gesunden und im Anschluss an eine Erkaltung mittels des Saccharin-sky-blue-tests. HNO-Praxis, 6, 31-7.
87. Graham, N., Burrell, c., Douglas, R. et al. (1990) Adverse effects of aspirin, acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. ]. Infect. Dis., 162, 1277-82.
88. Greiff, L., Akerlund, A., Andersson, M. et al. (1994) Day-night differences in mucosal exudation of bulk plasma in corona virus-induced common cold. (submitted).
89. Greiff, L., Andersson, M., Akerlund, A. et al. (1994) Microvascular exudative hyperresponsiveness in human corona virus-induced common cold. Thorax, 49, 121-7.
90. Greve, J., Davis, G., Meyer, A. et al. (1989) The major human rhinovirus receptor is ICAM-1. Cell, 56, 839-47.
91. Groenborg, H., Winther, B., Brofeldt, S. et al. (1983) Effects of oral norephedrine on common cold symptoms. Rhinology, 21, 3-12.
92. Gwaltney, J. (1971) Virology of the middle ear. Ann. Otol., 80, 365-70.
93. Gwaltney, J. (1992) Combined antiviral and antimediator treatment of rhinovirus colds. ]. Infect. Dis., 166, 776-82.
References 101
94. Gwaltney, J., Phillips, c., Miller, R. et al. (1994) Computed tomographic study of the common cold. N. Engl. ]. Med., 330, 25-30.
95. Hackemann, M., Denman, A. and Tyrrell, D. (1974) Inactivation of influenza virus by human lymphocytes. Clin. Exp. Immunol., 16, 583-91.
96. Hall, c., Douglas, R. Jr, Simons, R. et al. (1978) Interferon production in children with respiratory syncytial, influenza, and parainfluenza virus infections. ]. Pediatr., 93, 28-32.
97. Halperin, S., Eggleston, P., Beasley, P. et al. (1985) Exacerbations of asthma in adults during experimental rhinovirus infection. Am. Rev. Respir. Dis., 132, 976-80.
98. Hamilton, L. (1981) Effect of xylometazoline nasal spray on nasal conductance in subjects with coryza. J. Otolaryngol., 10, 109-16.
99. Hamory, B., Sande, M., Sydnor, A. et al. (1979) Etiology and antimicrobial therapy of acute maxillary sinusitis.]. Infect. Dis., 139, 197-202.
100. Hemila, H. (1992) Vitamin C and the common cold. Br.]. Nutr., 67, 3-16.
101. Henderson, F., Dubovi, E., Harder, S. et al. (1988) Experimental rhinovirus infection in human volunteers exposed to ozone. Am. Rev. Respir. Dis., 137, 1124-8.
102. Hoom, B. and Tyrrell, D. (1966) Effects of some viruses on ciliated cells. Am. Rev. Respir. Dis., 93,156-61.
103. Hoom, B. and Tyrrell, D. (1969) Organ cultures in virology. Prog. Med. Virol., 11, 408-50 .
104. Igarashi, Y., Skoner, D., Doyle, W. et al. (1993) Analysis of nasal secretions during experimental rhinovirus upper respiratory infections. ]. Allergy Clin. Immunol., 92, 722-31.
105. Isaacs, D., Clarke, J., Tyrrell, D. et al. (1982) Selective infection of lower respiratory tract by respiratory viruses in children with recurrent respiratory tract infections. Br. Med. ]., 284, 1746-8.
106. Jackson, G., Dowling, H., Spiesman, 1. et al. (1958) Transmission of the common cold to volunteers under controlled conditions. Arch. Intern. Med., 101, 267-78 .
107. James, J. (1972) Longitudinal study of the morbidity of diarrheal and respiratory infections in malnourished children. Am. ]. Clin. Nutr., 25, 690-4.
108. Jannert, M., Andreasson, L., Ivarsson, A. et al. (1984) Patency of the maxillary sinus ostium in healthy individuals. Acta Otolaryngol. (Stockh), 97,137-49.

102 Pathophysiology of viral respiratory tract infections
109. Jao, R, Wheelock, E. and Jackson, G. (1970) Production of interferon in volunteers infected with Asian influenza. J. Infect. Dis., 121, 419-26.
110. Knight, L. and Eccles, R (1993) The relation between nasal airway resistance and middle ear pressure in subjects with acute upper respiratory tract infection. Acta Otolaryngol. (Stockh), 113,196-200.
111. Larson, H., Parry, R and Tyrrell, D. (1980) Impaired polymorphonuclear leucocyte chemotaxis after influenza virus infection. Br. I. Dis. Chest, 74, 56-62.
112. Lea, P. (1984) A double-blind controlled evaluation of the nasal decongestant effect of Day NurseR in the common cold. J. Int. Med. Res., 12, 124--7.
113. Levandowski, R, Ou, D. and Jackson, G. (1986) Acute-phase decrease of T lymphocyte subsets in rhinovirus infection. J. Infect. Dis., 153, 743-8.
114. Levandowski, R., Weaver, C. and Jackson, G. (1988) Nasal-secretion leukocyte populations determined by flow cytometry during acute rhinovirus infection. J. Med. Viral., 25, 423-32.
115. Lewis, R, Austen, K. and Soberman, R (1990) Leukotrienes and other products of the 5-lipoxygenase pathway. Biochemistry and relation to pathobiology in human disease. N. Engl. I. Med., 323, 645-55.
116. Linden, M., Greiff L, Andersson, M. et al. (1995) Nasal cytokines in common cold and allergic rhinitis. CZin. Exp. Allergy, 25, 166-72.
117. Lowenstein, S. and Parrino, T. (1987) Management of the common cold. Adv. Intern. Med., 32,207-34.
118. Lundblad, L. (1990) Neuropeptides and autonomic nervous control of the respiratory mucosa, in Rhinitis and Asthma: Similarities and Differences, (eds N. Mygind, u. Pipkom and R Dahl), Munksgaard, Copenhagen, pp. 65-75.
119. Mabry, R (1982) Rhinitis medicamentosa: the forgotten factor in nasal obstruction. South. Med. /., 75, 817-19.
120. Macknin, M., Mathew, S., vander Brug, S. et al. (1990) Effect of inhaling heated vapor on symptoms of the common cold. JAMA, 264, 989-91.
121. Majno, G., Shea, S. and Leventhal, M. (1969) Endothelial contraction induced by histaminetype mediators. J. Cell BioI., 42, 647-72.
122. Male, D. and Roitt, I. (1989) Adaptive and innate immunity, in Immunology, 2nd edn, (eds I. Roitt, J. Brostoff and D. Male), Gower Medical Publishing, London, pp. 1.1-1.10.
123. Matthews, T., Nair, c., Lawrence, M. et al. (1976) Antiviral activity in milk of possible clinical importance. Lancet, ii, 1387-9.
124. McBride, T., Doyle, W., Hayden, F. et al. (1989) Alterations of the Eustachian tube, middle ear, and nose in rhinovirus infection. Arch. Oto/aryngol. Head Neck Surg., 115, 1054--9.
125. Mcintosh, K. (1978) Interferon in nasal secretions from infants with viral respiratory tract infections. J. Pediatr., 93, 33-6.
126. Melen, I., Andreasson, L., Ivarsson, A. et al. (1986) Effects of phenylpropanolamine on ostial and nasal airway resistance in healthy individuals. Acta Oto/aryngol. (Stockh), 102,99-105.
127. Minor, T., Dick, E., Baker, J. et al. (1976) Rhinovirus and influenza type A infections as precipitants of asthma. Am. Rev. Respir. Dis., 113,149-53.
128. Minor, T., Dick, E., DeMeo, A. et al. (1974) Viruses as precipitants of asthmatic attacks in children. JAMA, 227, 292--8.
129. Moore-Gillon, V. (1989) Olfactometry and the sense of smell, in Rhinitis. Mechanisms and Management, (ed. I. Mackay), Royal Society of Medicine Services Ltd, London, pp. 69-79.
130. Mudd, S., Goldman, A. and Grant, S. (1921) Reactions of the nasal cavity and postnasal space to chilling of the body surface. J. Exp. Med., 34,11-45.
131. Mygind, N. and Thomsen, J. (1976) Diurnal variation of nasal protein concentration. Acta Otolaryngol. (Stockh), 82,219-21.
132. Nacleiro, R, Proud, D., Lichtenstein, L. et al. (1988) Kinins are generated during experimental rhinovirus colds. J. Infect. Dis., 157, 133-42.
133. O'Flynn, P. (1993) Posture and nasal geometry. Acta Oto/aryngol. (Stockh), 113, 530--2 .
134. Olsson, P. and Bende, M. (1987) Sympathetic neurogenic control of blood flow in human nasal mucosa. Acta Otolaryngol. (Stockh), 102, 482-7.
135. Ophir, D. and Elad, Y. (1987) Effects of steam inhalation on nasal patency and nasal symptoms in patients with the common cold. Am. J. Otolaryngol.,3,149-53.
136. Parsons, R and Tyrrell, D. (1961) A plaque method for assaying some viruses isolated from common colds. Nature, 189, 640--2.
137. Paulsson, B., Bende, M., Larsson, I. et al. (1992) Ventilation of paranasal sinuses studied with dynamic emission computer tomography. Laryngoscope, 102, 451-7.

138. Paulsson, B., Bende, M. and Ohlin, P. (1985) Nasal mucosal blood flow at rest and during exercise. Acta Otolaryngol. (Stockh), 99, 140-3.
139. Pedersen, M., Sakakura, Y., Winther, B. et al. (1983) Nasal mucociliary transport, number of ciliated cells, and beating pattern in naturally acquired common colds. Eur. ]. Respir. Dis., 64, 355 ... 64.
140. Persson, C. (1991) Plasma exudation in the airways: mechanisms and function. Eur. Respir. f., 4,1268-74.
141. Persson, c., Erjefalt, I., Alkner, U. et al. (1991) Plasma exudation as a first line respiratory mucosal defence. CZin. Exp. Allergy, 21, 17-24.
142. Persson, c., Svensson, c., Greiff, L. et al. (1992) The use of the nose to study the inflammatory response of the respiratory tract. Thorax, 47, 993-1000.
143. Petruson, B. and Hansson, H.-A. (1982) Function and structure of the nasal mucosa after 6 weeks' use of nose-drops. Acta Otoiaryngoi. (Stockh), 94, 563-9.
144. Phillips, P., McCaffrey, T. and Kern, E. (1990) The in vivo and in vitro effect of phenylephrine (Neo Synephrine) on nasal ciliary beat frequency and mucociliary transport. Otolaryngol. Head Neck Surg., 103, 558-65.
145. Picken, J., Niewoehner, D. and Chester, E. (1972) Prolonged effects of viral infections of the upper respiratory tract upon small airways. Am. ]. Med., 52, 738-46.
146. Polo sa, R. (1993) Role of the kinin-kallikrein pathway in allergic disease. Allergy, 48, 217-25.
147. Proctor, D. and Andersen, I. (1982) The Nose -Upper Airway Physiology and the Atmospheric Environment, Elsevier Biomedical Press, Amsterdam, New York, Oxford.
148. Proud, D., Gwaltney, J., Hendley, J. et al. (1994) Increased levels of interleukin-l are detected in nasal secretions of volunteers during experimental rhinovirus colds.]. Infect. Dis., 169, 1007-13.
149. Proud, D., Nacleiro, R., Gwaltney, J. et ai. (1990) Kinins are generated in nasal secretions during natural rhinovirus colds. ]. Infect. Dis., 161, 120-3.
150. Proud, D., Reynolds, c., Lacapra, S. et al. (1988) Nasal provocation with bradykinin induces symptoms of rhinitis and a sore throat. Am. Rev. Respir. Dis., 137, 613-16.
151. Raphael, G., Jeney, E., Baraniuk, J. ct al. (1989) Pathophysiology of rhinitis. Lactoferrin and lysozyme in nasal secretions. ]. CZin. Invest., 84, 1528-35.
References 103
152. Rijntjes, E. (1985) Nose-drops abuse: a functional and morphological study. (Thesis), University of Leiden.
153. Roberts, N. (1979) Temperature and host defense. Microbiol. Rev., 43, 241-59.
154. Rossen, R., Alford, R., Butler, W. et al. (1966) The separation and characterization of proteins intrinsic to nasal secretion. ]. Immunol., 97, 369-78.
155. Rossen, R., Butler, W., Cate, T. et al. (1965) Protein composition of nasal secretion during respiratory virus infection. Proc. Soc. Exp. BioI. Med. N.Y., 119, 1169-76.
156. Rossen, R., Butler, W., Waldman, R. et ai. (1970) The proteins in nasal secretion. ll. A longitudinal study of IgA and neutralizing antibody levels in nasal washings from men infected with influenza virus. JAMA, 211, 1157--61.
157. Rossen, R., Schade, A., Butler, W. ct al. (1966) The proteins in nasal secretion: a longitudinal study of the gamma-A-globulin, gamma-Gglobulin, albumin, siderophilin and total protein concentrations in nasal washings from adult male volunteers.]. CZin. Invest., 45, 768-76.
158. Rundcrantz, H. (1969) Postural variations of nasal patency. Acta OtoIaryngol. (Stockh), 68,434-43.
159. Sakakura, Y., Sasaki, Y., Togo, Y. et al. (1973) Mucociliary function during experimentally induced rhinovirus infection in man. Ann. Otoi. Rhinol. Laryngol., 82, 203-1l.
160. Saketkhoo, K., Yergin, B., Januszkiewicz, A. et al. (1978) The effect of nasal decongestants on nasal mucus velocity. Am. Rev. Respir. Dis., 118, 251-4.
161. Schilder, A., Zielhuis, G., Straatman, H. et al. (1992) An epidemiological approach to the etiology of middle ear diseases in The Netherlands. Eur. Arch. Otorhinolaryngol., 249, 370-3.
162. Schmidt, J., Borgstrom, P. and Intaglietta, M. (1993) The vascular origin of slow-wave flow motion in skeletal muscle during local hypotension. Int. ]. Microcirc. Clin. Exp., 12, 287-97.
163. Senior, R., Skogen, W., Griffin, G. et al. (1986) Effects of fibrinogen derivatives upon the inflammatory response. Studies with human fibrinopeptide. Br. J. CZin. Invest., 77, 1014-19.
164. Simon, H., Drettner, B. and Jung, B. (1977) Messung des schleimhauttransportes in menschlichen Nase mit SlCr markierten harzkugeln. Acta Otolaryngol. (Stockh), 83,378-90.
165. Smith, A., Tyrrell, D., Coyle, K. ct al. (1988) Diurnal variation in the symptoms of colds and influenza. Chronobiol. Int., 5, 411-16.

104 Pathophysiology of viral respiratory tract infections
166. Smith, M. and Feldman, W. (1993) Over-thecounter cold medications; a critical review of clinical trials between 1950 and 1991. JAMA, 269,2258-63.
167. Sperber, S., Sorrentino, J., Riker, D. et al. (1989) Evaluation of an alpha agonist alone and in combination with a nonsteroidal antiinflammatory agent in the treatment of experimental rhinovirus colds. Bull. N. Y. Acad. Med., 65, 145-60.
168. Stanley, E., Jackson, G., Panusarn, C. et al. (1975) Increasing virus shedding with aspirin treatment of rhinovirus infection. JAMA, 231, 1248-51.
169. Staunton, D., Meriuzzi, V., Rothlein, R. et al. (1989) A cell adhesion molecule, ICAM-1, is the major surface receptor for rhinoviruses. Cell, 56,849-53.
170. Steranka, L., Manning, D. and DeHaas, C. (1988) Bradykinin as a pain mediator: Receptors are localized to sensory neurons, and antagonists have analgesic actions. Proc. NatI Acad. Sci. USA, 85, 3245-9.
171. Summers, Q., Higgins, P., Barrow, I. et al. (1992) Bronchial reactivity to histamine and bradykinin is unchanged after rhinovirus infection in normal subjects. Eur. Respir.]., 5, 313-17.
172. Svensjo, E., Arfors, K.-E., Arturson, G. et al. (1978) The hamster cheek pouch preparation as a model for studies of macromolecular permeability of the microvasculature. Ups. J. Med. Sci., 83,71-9.
173. Tos, M. (1982) Goblet cells and glands in the nose and paranasal sinuses, in The Nose. Upper Airway Physiology and the Atmospheric Environment, (eds D. Proctor and I. Andersen), Elsevier Biomedical Press, Amsterdam, New York, Oxford, pp. 99-144.
174. Tos, M., Poulsen, G. and Borch, J. (1979) Etiologic factors in secretory otitis. Arch. Otolaryngol. Head Neck Surg., 105, 582--8.
175. Turner, B., Cail, W., Hendley, J. et al. (1992) Physiologic abnormalities in the paranasal sinuses during experimental rhinovirus colds. ]. Allergy Clin. Immunol., 90, 474-8 .
176. Turner, R., Hendley, J. and Gwaltney, J. Jr (1982) Shedding of infected ciliated epithelial cells in rhinovirus colds.]. Infect. Dis., 145, 849-53.
177. Tyrrell, D., Barrow, I. and Arthur, J. (1989) Local hyperthermia benefits natural and experimental common colds. Br. Med. ]., 298, 1280-3.
178. Tyrrell, D., Cohen, S. and Schlarb, J. (1993) Signs and symptoms in common colds. Epidemiol. Infect., 111,143-56.
179. Walker, G., Bynoe, M. and Tyrrell, D. (1967) Trial of ascorbic acid in prevention of colds. Br. Med. ]., 1, 603-6.
180. Welliver, R., Wong, D., Middleton, E. et al. (1982) Role of parainfluenza virus-specific IgE in pathogenesis of croup and wheezing subsequent to infection.]. Pediatr., 101, 889-96.
181. Welliver, R., Wong, D., Sun, M. et al. (1981) The development of respiratory syncytial virusspecific IgE and the release of histamine in nasopharyngeal secretions after infection. N. Engl.]. Med., 305, 841-6.
182. Willatt, D. (1993) Continuous infrared thermometry of the nasal mucosa. Rhinology, 31, 63-7.
183. Williams, R. and Eccles, R. (1992) Nasal airflow asymmetry and the effects of a topical nasal decongestant. Rhinology, 30, 277-82.
184. Wilson, R. (1987) Upper respiratory tract viral infection and mucociliary clearance. Eur. ]. Respir. Dis., 70,272--9.
185. Winther, B., Brofeldt, S., Christensen, B. et al. (1984) Light and scanning electron microscopy of nasal biopsy material from patients with naturally acquired common colds. Acta Otolaryngol. (Stockh), 97, 309-18.
186. Winther, B., Farr, B., Turner, R. et al. (1984) Histopathologic examination and enumeration of polymorphonuclear leukocytes in the nasal mucosa during experimental rhinovirus colds. Acta Otolaryngol. (Stockh), Suppl. 413,19-24.
187. Winther, B., Gwaltney, J., Mygind, N. et al. (1986) Sites of rhinovirus recovery after point inoculation of the upper airway. JAMA, 256, 1763-7.
188. Winther, B., Innes, D., Mills, S. et al. (1987) Lymphocyte subsets in normal airway mucosa of the human nose. Arch. Otolaryngol. Head Neck Surg., 113, 59-62.
189. Zeiger, R. (1992) Prospect for ancillary treatment of sinusitis in the 1990s. ]. Allergy Clin. Immunol., 90, 478-95.