Embed Size (px)
Citation preview

Goldenhar syndrome and neuroblastoma: a chance association?
C Michel-Adde1, A Laquerriere2, D Eurin3, V Drouin-Garraud4 and S Marret1
Departments of Neonatal Medicine1; Pathology2; Paediatric Radiology2; Unit of Clinical Genetics4, Rouen University Hospital CharlesNicolle, Rouen, France
Michel-Adde C, Laquerrie`re A, Eurin D, Drouin-Garraud V, Marret S. Goldenhar syndrome andneuroblastoma: a chance association? Acta Pædiatr 2003; 92: 1223–1225. Stockholm. ISSN 0803-5253
Oculoauriculovertebral dysplasia, also called Goldenhar syndrome, includes several anomalies:epibulbar dermoids or lipodermoids, microtia, mandibular hypoplasia, vertebral, skeletal, cardiacand kidney anomalies, among others. Tumours have also been observed in patients with oculo-auriculovertebral dysplasia. We report the first case of oculoauriculovertebral dysplasia associatedwith a neuroblastoma. This tumour consists of cells identical to early migratory neural crest cellsin the embryo. Several theories have been proposed regarding the pathogenetic explanation ofoculoauriculovertebral dysplasia. Currently, some researchers have suggested a deficiency inmesodermal formation or defective interaction between neural crest and mesoderm as a possibleaetiology.
Conclusion: It is suggested that the case reported here is an additional argument for an anomalyin neural crest cell migration or interaction with the mesoderm in the pathogenesis of oculo-auriculovertebral dysplasia.
Key words: Goldenhar syndrome, neural crest cells, neuroblastoma
C Michel-Adde, Department of Neonatal Medicine, Hopital Charles Nicolle, 1 rue de Germont,FR-76031 Rouen cedex, France (Tel. �33 2 3288 8097, fax. �33 2 3288 8633, [email protected])
The term oculoauriculovertebral dysplasia (OAV) wasfirst suggested by Gorlin (1) to describe patients withmicrotia, mandibular hypoplasia, vertebral anomaliesand epibulbar dermoids or lipodermoids, anomalies alsoknown as Goldenhar syndrome. Involvement is notlimited to the facial structure. In fact, skeletal, cardiac,kidney and other anomalies are also features of thissyndrome. The hereditary pattern is mainly sporadic,except for some autosomal, dominant cases. Em-bryologically, OAV has been termed an anomaly ofthe first and second branchial arch (1). More recently,Van Meter and Weaver (2) suggested that theseblastogenesis defects could be linked to a deficiencyin neural crest cells. We report the case of a neonatewith OAV associated with an adrenal neuroblastoma.
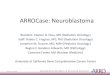
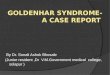
Case reportThe child was born at full term (41 wk) of apparentlyhealthy and non-consanguineous parents. The patientwas the third boy of a 38-y-old, gravida 3, para 3mother, and his brothers were healthy. At 32 wk ofgestation, a left labiomaxillopalatin cleft, a hyper-telorism, a microphthalmia, a tumour on the eyesand a lipoma of the corpus callosum were observed(Figs 1 and 2) but the amniocentesis test was refusedby the parents. Maternal hypertension occurred 3 wk
before birth and a caesarean section was performedbecause of foetal distress, meconial polyhydramniosand dynamic dystocia. The Apgar score at birth was 7 atone min and 10 at 5 min.
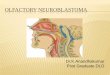
Three hours after birth, the infant was admitted to apaediatric unit because of dysmorphic features. Hisbirthweight was 3775 g, length 50 cm, and headcircumference 35 cm, all parameters being near the50th percentile for age. Clinical examination showedbilateral epibulbar dermoids on the eyelids, bilateralmicrotia, bilateral preauricular fibrochondromas, nasalprobosis and retrognathia with left maxillopalataldefect. All these abnormalities were asymmetrical andmore marked on the left side (Fig. 3). Moderate axialhypotonia was observed. The otorhinolaryngeal exam-ination revealed a severe auditive defect and a PierreRobin sequence with difficulties in feeding caused byproblems with suction-swallowing.
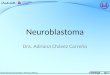
The first morphological examination revealed acomplex embryopathy including an asymmetrical bran-chial arch syndrome and elements of Pierre Robinsequence. Cerebral ultrasonography and a cranial CTscan confirmed a lipoma of the corpus callosum (seeFig. 4). The electroencephalogram was normal. Thehearing tests showed potentials of 5 to 90 decibels waveon the right side and no response on the left side. Furtherexaminations showed a normal karyotype, a normalskeletal radiography with the exception of a left
2003 Taylor & Francis. ISSN 0803-5253
���� ������ �� ���� ���� ����
DOI 10.1080/08035250310005729

mandibular hypoplasia, a normal echocardiography, akidney mass probably due to a lipoma or hamartoma.The epibulbar dermoids were resected at 3 wk and thepathological examination confirmed the diagnosis. Abilateral cataract was discovered after surgery. Duringthe first month of life, difficulty in suction-swallowingpersisted, which required enteral feeding. At one month,respiratory symptoms became increasingly severe withstridor and inspiratory dyspnoea. Severe apnoea withbradycardia and desaturation was observed as early asday 29 but was not related to enteral feeding. The
patient died during an episode of severe distress owingto oesophageal and laryngeal spasms.
An autopsy showed the lipoma of the corpuscallosum, associated with a partial posterior agenesisand a multinodular, necroticohaemorrhagic retroperito-neal tumoral mass. The tumour extended from the leftadrenal gland without macroscopic invasion of thekidney and without extension to the thorax. Onmicroscopic examination, the tumour was composedof neuroblastic atypical cells, situated in a schwannian-poor stroma but with clearly recognizable fibrillar
Fig. 1. Cranial sonography at 32 wk of gestation.
Fig. 2. Left labiomaxillopalatin cleft, hypertelorism and micro-phthalmia.
Fig. 3. Patient morphological characteristics: bilateral epibulbardermoids on the eyelids, microtia, preauricular fibrochondromas,nasal probosis, retrognathia and left maxillopalatal defect.
Fig. 4. Cranial CT scan: lipoma of the corpus callosum, labiomax-illopalatin cleft and retrognathia.
1224 Clinical observations ACTA PÆDIATR 92 (2003)

stroma, resembling a neuropil. Less than 5% ganglioniccells were observed. Rosette formation was noted, aswell as foci of calcification and necrosis. The tumourwas classified as a neuroblastoma, schwannian-poorstroma, poorly differentiated subtype, according to theINPC classification (3) (see Fig. 5). Immunohistochemi-cal studies were performed using various antisera.Diffuse immunoreactivity was noted with antihumanneuroblastoma. Rosettes and fibrillar stroma were posi-tive for synaptophysin. A few cells were positive forchromogranin A. Flow cytometric analysis performedon tumoral cells permitted the detection of DNAtriploidy. The proliferation index of DNA triploid cellsvaried from 13.9% to 24.2%. FISH studies failed todetect any N-myc amplification.
DiscussionTo the best of our knowledge, this is the first case ofOAV associated with neuroblastoma. Lipomas havefrequently been described in association with OAV.Other tumours have also been reported in patients withOAV, i.e. hepatoblastoma, metatarsal and cuneiformchondromyxoid fibroma (4), congenital ameloblasticfibroma of the mandible (5). Neuroblastoma is acommon malignant neoplasm of early life. It is formedby primitive neuroblasts derived from the neural crest.Neuroblastomas usually develop in the adrenal medullaor in the abdominal, thoracic, pelvic or cervical chainsof autonomic ganglia. In its most primitive form, thetumour consists of sheets and nests of cells identical tothe early migratory neural crest cells in the embryo.Maturation or cytodifferentiation can occur as a gang-lioneuroma in its most mature form. OAV contains alarge spectrum of anomalies, suggesting various patho-genetic explanations. Poswillo (6), using an animalmodel, showed that early vascular disruption with
expanding haematoma formationin utero resulted indestruction of differentiating tissues in the region of theear and jaw. Gorlin (1) suggested that vascularanomalies of the neural crest cells could disrupt theembryological development of the branchial arches.Beauchamp and Knepper (7) and Opitz (8) proposedthat OAV could be a neurocristopathy, defined byBolande (9) as a disorder arising from aberrations inneural crest migration, growth and differentiation. Kaye(10) proposed that abnormalities of other cell popula-tions could be involved to encompass the full spectrumof associated malformations (ectodermal placodes,mesoderm and other surface ectoderm). Van Meterand Weaver (2) suggested that deficiency in migrationof neural crest cells, deficiency of mesodermal forma-tion or defective interaction between neural crest cellsand mesoderm may explain the pathogenesis of OAV.The association between OAV and neuroblastomaunderlines the hypothesis of a common origin for bothpathologies and therefore should be considered in theneurocristopathy group. We suggest that the casereported in this paper is an additional argument for ananomaly in neural crest cells migration or interactionwith mesoderm in the pathogenesis of OAV.
Aknowledgements.—We express our thanks to Y. Tallet for technicalassistance, R. Medeiros for his advice in editing the manuscript andC. Leveque for her help with the illustrations.
References1. Gorlin RJ. Oculoauriculovertebral dysplasia. J Pediatr 1963; 63:
991–92. Van Meter TD, Weaver DD. Oculo-auriculo-vertebral spectrum
and the CHARGE association: clinical evidence for a commonpathogenetic mechanism. Clin Dysmorph 1996; 5: 187–96
3. Shimada H, Ambros I, Dehner LP, Hata JI, Joshiv V, Roald B.Cancer 1999; 86: 349–63
4. Goldenhar AS, Neil J, Whittaker S. Chondromyxoı¨d fibroma of ametatarsal and cuneiform. J Am Podiatr Med Assoc 1994; 84:413–5
5. Naidoo LC, Stephen LX. Congenital ameloblastic fibroma inassociation with oculoauriculovertebral spectrum. Int J PediatrOtorhinolaryngol 1998; 43: 283–8
6. Poswillo D. Hemorrhage in development of the face. BDOAS1975; 11: 61–81
7. Beauchamp GR, Knepper PA. Role of the neural crest in anteriorsegment development and disease. J Pediatr OphthalmolStrabismus 1984; 21: 209–14
8. Opitz JM. Developmental field theory and observations-acci-dental progress? Am J Med Genet 1986; 2 Suppl: 1–9
9. Bolande RP. The neurocristopathies: a unifying concept ofdisease arising in neural crest development. Hum Pathol 1974; 5:409–29
10. Kaye CI. Microtia and associated anomalies: statistical analysis.Am J Med Genet 1989; 34: 574–8
Received Nov. 22, 2002; revisions received June 6, 2003; acceptedJuly 10, 2003
Fig. 5. Poorly differentiated neuroblastic proliferation in the leftadrenal gland.
ACTA PÆDIATR 92 (2003) Clinical observations 1225