Embed Size (px)
DESCRIPTION
Good Liver March 2013 Edition, focusing on Liver Transplantation.
Citation preview

The Newsletter of Hepatitis Victoria
March 2013
Good Liver
Applying for a liver –the hows and whys
Julie Pavlovic, Liver Transplant
Coordinator, explains the process
leading to a liver transplant.
Staying well after a liver transplant
It’s vital that post-transplant patients
are engaged in their health care to
make the most of this new opportunity.
Personal stories fromliver transplantees
Frank Carlus and Shane Laffy share
their experiences of having liver trans -
plants and gratitude to their donors.
Liver transplantation

2
Staff contacts:
Melanie EagleCEO
Telephone: 9385 9102
Garry IrvingPrograms Manager
Telephone: 9385 9109
Lisa NultyOffice Coodinator
Telephone: 9380 4644
Alex TaylorPrisons Program
Telephone: 9385 9104
Amy KirwanPrison Project Officer
Telephone: 9385 9108
Isabella NataleYoung People’s Project Officer
Telephone: 9385 9111
Felicity OmarAboriginal Program
Telephone: 9385 9108
Louisa WalshProject Coordinator
Hep C: Take Control Program
Telephone: 9385 9106
Garry SattellCommunity Participation Program
Telephone: 9385 9110
Jessie Di BlasiDevelopment Coordinator
Telephone: 9385 9123
Contact and postal address:
Hepatitis Victoria
Suite 5, 200 Sydney Road,
Brunswick, Victoria. 3056
Telephone: (03) 9380 4644
Facsimile: (03) 9380 4688
Email: [email protected]
Website: www.hepvic.org.au
HepatitisInfoline
1800 703 003
Contents
3 Communiqué
From the desk of the
Chief Executive Officer.
4 In the news
6 Applying for a new liver –
Position description
Julie Pavlovic outlines the process
leading to performing a liver transplant.
8 Liver 2.0: Service and
maintenance guide
It’s vital that post-transplant you are
involved and engaged in your health care
to make the most of this new opportunity.
9 Crunching the numbers –
Liver transplant statistics
Chronic hepatitis C causes more liver
transplants in Australia than any
other condition.
10 A personal story – Frank Carlus
Frank Carlus tells his story – all the
lows and highs of going through a
liver transplant.
12 A personal story – Shane Laffy
With a song in his heart, Shane Laffy tells
of his liver transplant and sings praises
to his organ donor.
13 Fred Negro cartoon
Lily Liver moves into her new home!
14 Organ donation by
people with hepatitis
People with hepatitis can donate their
organs to medicine? Myth or reality?
15 Aboriginal Program report
15 Moving in – Amy Kirwan
Our new Prisons Project Officer
16 Young Blood
17 Hep C Connect – A case study
18 Hep C: Going Viral
19 Hepatitis Victoria membership
20 Liver clinics list
21 Contacts
Good Liver is produced by Hepatitis Victoria.
The opinions and language expressed in
this magazine are not necessarily those
of Hepatitis Victoria or the Department
of Health.
Images used in this newsletter are sourced
from StockXchng stock photo library at:
www.sxc.hu/. Images are used for
illustrative purposes only and have no
connection to hepatitis.
Reader response
Your comments or experiences in regard to
any articles in the Good Liver are welcome.
Call, write or email: [email protected]
Autumn 2013

of Good Liver we pay tribute to the people
who have undergone this life saving
procedure. We also think of the people with
serious liver disease who never get a chance
to access treatments like transplantation, and
that fact that with improvements in treatments
and services end-stage disease in viral
hepatitis is largely preventable. We bear
all this in mind as we strengthen our efforts
to achieve and deliver on our new
strategic goals.
Warm regards
Melanie Eagle
CEO
After concerted advocacy by many
individuals and organisations, including
Hepatitis Victoria, the Federal Government
announced on 19 February, 2013 that two
new treatments for chronic hepatitis C
would be listed on the Pharmaceutical
Benefits Scheme (PBS). This means the
new breakthrough treatments - Boceprevir
and Telaprevir - will be more affordable
and available, and offers new hope for
people with chronic hepatitis who have
not had access to treatments suitable to
their particular condition.
These medicines indeed could double the
cure rate and shorten the treatment duration
by six months - ultimately stopping the
virus from progressing into life-threatening
conditions such as liver failure and liver
cancer. Hepatitis Victoria is delighted with
this development, and would like to thank
all those who joined us in the campaign.
For further information about these new
treatments contact the Hepatitis InfoLine
on 1800 703 003
3
CommuniquéFrom the desk of the Chief Executive Officer
Welcome to the first edition for 2013 of
Good Liver – the quarterly newsletter
of Hepatitis Victoria.
This edition comes at an exciting time. At
the end of last year the Board of Hepatitis
Victoria adopted our Strategic Plan which
will guide the work of the organisation for
the years 2013 to 2017.
Our vision at Hepatitis Victoria is a Victorian
community where there are no new infections
of viral hepatitis, and where those who have
the virus are able to maximise their health
and wellbeing. This vision is underpinned by
our values, namely: Respect; Participation;
Diversity; Excellence; Integrity; Innovation;
Impact and Collaboration.
Further information about this plan, and
the journey we intend to undertake to get
there, can be found on our website at
www.hepvic.org.au/strategicplan.
Another exciting dimension of 2013 is that it
is the year Hepatitis Victoria will celebrate 21
years of service to the Victoria community.
We intend to hold some events to mark our
history and achievements, and also to build
even further on what we have accomplished.
Meanwhile to more sombre matters. For the
first time, Good Liver is dedicating an entire
issue to transplantation.
While fortunate that the medical expertise
exists to provide transplants – and you can
read some positive personal accounts in the
following pages – liver transplants arising
from chronic viral hepatitis is actually some–
thing in theory we should not even need to
discuss. If people with viral hepatitis were
being tested, diagnosed, and able to access
treatment and monitoring early, and if society
invested in new and more effective treat–
ments, fewer people with hepatitis B or C
would reach end stage liver disease, and
we would see a drop in demand for
transplantation for people with viral hepatitis.
But instead the facts are these:
• One third of liver transplants in Australia
are due to chronic hepatitis C, and with the
increasing prevalence of chronic hepatitis
B in our community, the proportion of
transplants being for people with viral
hepatitis (B and C) will only rise.
• While 500 Australians and New
Zealanders die each year from the
complications of viral hepatitis, only 70
people with viral hepatitis were
transplanted in 2011, suggesting many
people with end-stage liver disease are
not connected to transplant services.
• In 2012, Australia performed 230 liver
transplants, however our donor rates are
very low. One in ten people on the
transplant waiting list will die, and many
others die from their viral hepatitis without
even being considered for transplantation.
• Many of these transplants and deaths
are preventable with proper access to
testing, treatment, and monitoring.
With increases in the number of people with
viral hepatitis, and the ageing Australian
population, there is likely to be more demand
for liver transplants into the future. We are
already seeing this occur in the US, and
Australia is likely to follow suit.
Transplantation is an important issue for the
viral hepatitis community, and in this edition
STOP
PRESS!

4
In the newsArticle exerpts and published Letters to the Editor from major newspapers
Demand for livertransplantation set toincrease in the USAn ageing population of adults with hepatitis
C is behind an increasing demand for liver
transplantation in the United States, a new
study reveals.
The findings suggest that the development of
liver cancer in baby boomers with hepatitis C
is spurring the continuing increased demand
for liver transplantation, but that the demand
may decrease as these patients grow older,
the study authors said.
The researchers analysed data from the
Organ Procurement and Transplantation
Network between 1995 and 2010, and found
that nearly 127,000 new candidates for first
liver transplant registered with the network
during that time.
Forty-one percent of those patients had
hepatitis C. People born between 1941 and
1960 accounted for 81 percent of all new
liver transplant registrants infected with the
virus, according to the study in the December
issue of the journal Liver Transplantation.
“The dire projections in [hepatitis C virus]
complications spurred our investigation of
age-specific trends in liver transplantation
demand,” study lead author Dr. Scott
Biggins, of the University of Colorado School
of Medicine, said in a journal news release.
The investigators also found that between
2000 and 2010, rates of new liver transplant
candidates with hepatitis C and liver cancer
quadrupled in those who were born between
1941 and 1960.
Tasmania, Queensland, the Northern
Territory, the Australia Capital Territory and
New South Wales all achieved their highest
ever annual organ donation outcomes in
2012. The breakdown of donors in 2012 was:
New South Wales – 88; Victoria – 92;
Queensland – 78; South Australia – 29;
Western Australia – 32; Tasmania – 15;
Northern Territory – 8 and ACT – 12.
Pioneering surgery usingcow heart tissue saveswoman with incurable liver cancerA team of British doctors has managed
to save the life of a woman in Liverpool
suffering from an incurable liver cancer
thanks to a pioneering surgery through
which they rebuilt her liver by using cow’s
heart tissue.
Michelle Morgan-Grainger was diagnosed
with a rare and incurable form of liver cancer
back in October 2010. While she was initially
told by doctors that the cancer could not be
cured, she underwent a pioneering form of
surgery at the Aintree University Hospitals
NHS Foundation Trust where the doctors
removed the tumor along with a large portion
of her Inferior Vena Cava (IVC) and went on
to reconstruct the major blood vessel by
using tissue, known as bovine pericardium,
from a cow’s heart.
“This was a long and complex procedure and
is offered only in a handful of places around
the world. There are only five centres in
Europe with experience in such cases. To
date about 150 patients have been treated
worldwide. The bovine patch has been used
in heart surgery for a while but employed in
just six liver surgery cases, four of which
we’ve performed”, the consultant
hepatobiliary surgeon, Hassan Malik said.
“Over the coming decade, the ageing of those
infected with [hepatitis C virus] will challenge
the transplant community to reconsider
current treatment plans given the projected
increase in liver transplantation demand,
particularly from patients with [hepatitis C
virus] and liver cancer,” Biggins said.
“Many of these patients may not be healthy
enough for transplantation, and the number
of liver transplants in patients with [hepatitis
C virus] may decrease,” he added.
Organ donation andtransplantation report shows steady progress Australian families are being urged to decide
and discuss their donation decisions in an
effort to build on the generosity of those
families who in 2012 agreed to their loved
one becoming an organ and tissue donor.
A total of 354 Australians became organ
donors in 2012, representing a 5% increase
above the 2011 outcome of 337, and a 43%
increase since 2009. The 2012 outcome of
1,052 transplant recipients from deceased
donors represents a 4% increase (or addi–
tional 43 recipients) above the 2011 outcome
of 1,009, and a 30% increase since 2009.
Associate Professor Stephen McDonald
said, “Australia achieved its highest ever
number of liver transplant recipients at 230,
compared to the 213 recipients in 2011. This
represents an 8% increase over 2011 and a
24% increase since 2009.

5
equipment in service stations, in late-night
convenience stores because the primary
needle and syringe programs are open only
from nine to five and that’s limiting access
and service,’’ he said.
‘’So we need expansion of outlets, we need
more distribution machines - vending
machines and the like. Overall, we need a
proper official look at what the impact of the
drug laws in Australia is on blood-borne
virus transmission.’’
The ACT government has proposed a
needle-exchange program for Canberra’s jail
but other states have not taken such action.
“It is something that we believe is absolutely
essential to reduce the transmission of
blood-borne viruses, particularly hepatitis C.
Prisons are a hotbed of hepatitis C trans-
mission, they are a hotbed or a powerhouse
of the hepatitis C epidemic,’’ he said.
Hepatitis C was spread between prisoners
and then into the general community when
detainees were released, Mr Loveday said.
It could damage the liver for decades before
symptoms appeared and led to cirrhosis and
Hep C: call for more actionNeedle exchange services should be
provided in late-night convenience stores,
petrol stations and in all Australian prisons
to help stop the spread of hepatitis C,
according a public health group.
A report by the Economist Intelligence Unit in
London warns hepatitis C has become a
‘silent pandemic’ that kills 350,000 people
each year.
The impact of the disease was likely to
increase as many people who were infected
with the blood-borne virus before it was
discovered in 1989 reach the end stages
of associated medical conditions.
Commenting on the report, Hepatitis
Australia president Stuart Loveday said
Australian health authorities were doing a
good job to combat the disease but more
action was needed, including stepped-up
preventive measures.
Mr Loveday said better access to clean
injecting equipment for intravenous drug
users should be considered.
“We would dearly love to see injecting
liver cancer. ‘’The need for a prison-based
needle exchange is not just necessary in the
Alexander Maconochie Centre [in the ACT],
it is necessary in every prison,’’ he said.
,
Hepatitis Victoria calls foraccess to new therapies
On 2 February, 2013, Hepatitis Victoria
hosted a roundtable at St Vincent’s Hepatitis
Clinic in Werribee Mercy Hospital on the
need to urgently improve treatment options
for people living with Hepatitis C in Western
Melbourne.
Hepatitis Victoria CEO, Melanie Eagle, said
that hepatitis C is an urgent health concern
needing immediate action to prevent new
infections and to limit the rising burden of
cirrhosis, liver cancer and avoidable deaths.
“With more than 225,000 Australians living
with chronic hepatitis C, successive national
hepatitis strategies have pointed out the
need to improve access to new therapies
which lead to increased cure rates.
The new drugs, telaprevir and boceprevir,
were recommended for listing under the
Pharmaceutical Benefits Scheme (PBS),
by the Pharmaceutical Benefits Advisory
Committee in July 2012, and are already
available in 25 countries.
Editor’s note: These two treatments were
approved on the 19 February 2013.
Please see Communique on page 3.

radiological scans and procedures, heart
tests, endoscopic procedures) and interviews
with members of the multidisciplinary
transplant team. The assessment usually
takes 5-8 days as an outpatient or it can be
undertaken as an inpatient if the patient is
unwell. The purpose of the assessment is to
assess the extent of the liver disease and to
identify any associated problems with other
organs that may make the liver transplant too
risky. Associated problems may be corrected
if possible.
Patients and family get
to know the LTU team,
which consists of
medical staff, surgical
staff, transplant coord -
inators, allied health
staff- dietician, physio -
therapist, psychiatrist,
pastoral care, occu -
pational therapist and
social work. Patients
and family are encour -
aged to ask questions
and learn about trans -
plantation and its
risks. At the end of the
assessment process
all results are
Transplantation has become an accept -
able form of treatment for many liver
related diseases. With improvements in
knowledge, surgical skill and immunosup -
pressive medication the success rate and
long term survival of transplant recipients
has greatly improved and the patient
population continues to grow.
The Liver Transplant Unit (LTU) at the Austin
Hospital, is a unique service to Victoria and
Tasmania. It is the only liver transplant unit in
Victoria and Tasmania and receives referrals
state wide. Each year approximately 120
patients are referred for liver transplant ation
assessment. At least 70 of these are admitted
for a formal assessment to determine their
suitability for placement
onto the transplant waiting list.
The conditions that can lead to liver transplant
are very varied. Hepatitis B and C used to be
unsuitable for transplantation, but now with
the development of anti-viral medication,
transplantation is an option for people with
viral hepatitis.
Patients are referred to the Austin LTU usually
via specialists, GPs or other Hospitals. The
majority of patients referred to LTU have either
a confirmed diagnosis or at least a suspected
diagnosis. The diagnosis is confirmed with
patient interview, blood tests, radiological
procedures and physical assess–ment.
Once the results are collaborated a plan for
assessment, treatment and care can be made.
Patients are reviewed by the liver specialist in
either the outpatient clinic or as an inpatient if
they are unwell. Depending on the review, the
patient is either referred for liver transplant
assessment or they will be treated and
monitored as an outpatient (deferred). These
patients may very well be referred for liver
transplant assessment at a later time.
However some patients are deemed unsuitable
for liver transplantation due to extensive liver
disease or other health problems.
The liver transplant assessment consists of
a variety of medical tests (blood tests,
6
collaborated and discussed within the team
as to whether the patient is suitable for liver
transplantation. Those patients who are not
suitable for liver transplantation are either
referred back to their specialist for continuing
care or are monitored by the liver specialists .
Those patients who are suitable for liver
transplantation are placed onto the Liver
Transplant Waiting List. They have regular
contact with the liver transplant coordinator,
medical staff and allied health staff, to ensure
optimal health prior to liver transplantation.
Applying for a new liver - position descriptionThe who, what, where, why and how of liver transplantation
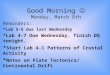
A diagram of a diseased liver (A) and a transplanted liver(B) showing the vessels that are joined (anastomosed).
Still waiting
Die on waiting list
DelistedAssessed
Rejected
Deferred
Patient andGraft surviving
Died post-transplantation
What happens...
Activated
Referred
Waiting
Graft failed
Transplanted
Diseased liver removed
Anastomoses
Hepatic artery
Common bile duct
Portalvein
Inf.venacava
A.
B. Donor liver transplanted

7
Waiting for a liver transplant can be taxing on
patients, the constant wondering “when is a
liver going to become available” often puts
lives and dreams on hold. Family relation -
ships are often tested, as the focus is on
keeping the patient in optimal health. Waiting
times for a liver can be as little as a
few days or as long as 3 years.
During this time all patients on the
liver transplant waiting list are
regularly reviewed by the LTU, and
the patients and their families are
asked to participate in a support
group program.
Unfortunately not all patients make it to
transplantation. Some patients become too
sick whilst on the waiting list and their other
organs start to fail. These patients are
removed from the waiting list – they are
delisted and deemed too sick for transplant.
Some patients need to go on hold – to treat
an infection or stabilize their liver disease.
Once treated or stabilized they are then re-
activated onto the waiting list. Some patients
however, die on the waiting list as a suitable
organ has not been found.
DonationWhen a potential donor has been identified
and the donor family has expressed the wish
to donate their loved one’s organs, the organ
donor coordinator is contacted by the
hospital. The donor coordinator discusses at
length with the family and investigates the
donor’s medical and social history to ensure
the suitability for organ donation. Once all
information has been obtained, the organ
donor coordinator contacts the liver
transplant coordinator and relays the
information. The liver transplant
coordinators discuss the potential offer with
the liver transplant surgeon and physician.
The potential recipient is chosen based on:
• Same blood group;
• Similar size- based on height, weight
and girth measurement;
• Priority within that blood group (the
sickest patients get top priority).
On certain occasions the liver is able to be
split into 2 halves. A child and adult are then
able to be transplanted, however this is
dependent on the anatomy of the liver and is
not suitable for all livers. Wherever possible,
if the liver is able to be split, this
is undertaken.
The liver recipient is then notified
that a potential liver has been
offered for them and they are
advised to come to the hospital
urgently for preparation for liver
transplant ation. Preparation for
liver trans plantation can take up to
12 hours – blood tests, chest x-ray,
antibac terial body wash. During this
time a retrieval team has been sent
to the donor hospital to view and
retrieve the liver. Once the liver has been
viewed by the lead surgeon a go ahead is
given to the liver transplant coordinator, and
the recipient operation can commence. The
liver transplant surgery takes 6 –12 hours
and the patient is taken to the intensive care
unit (ICU) immediately after the transplant to
recover. On some occasions the liver is
deemed untrans plantable when viewed by
the lead surgeon, the liver transplant
coordinator is then notified and the recipient
surgery is cancelled.
After as little as a few hours or a number of
days in the ICU, depending on how the
transplant surgery went or how sick the
patient was prior to the transplant. The patient
is then transferred to the ward where they
usually stay for 7–10 days. Prior to
discharge the patient and their family
receive education on medications –
why they are taking particular
medication and how and when to take
them, outpatient clinics, infection
prophylaxis and general health care.
They are given the direct phone
number to the liver transplant coordinator for
any questions or concerns. The patient is
discharged home or to the hospital flats
depending on how far they live from the
hospital. The patients attend post liver
transplant clinic initially twice weekly. As they
improve the clinic visits are extended out to
monthly, bi-monthly and then every 3 – 6
months. The LTU at the Austin sees all post
transplant patients at least once every six
months no matter how long post transplant.
Post transplant patients are with us for life
and a bond is created between the patient
and the unit.
Liver transplantation requires an extra -
ordinary multidisciplinary team to manage
and support the patient from the initial
referral through the transplant procedure,
post operatively, and beyond. The Liver
Transplant Unit relies on every department
in the hospital for their expertise to ensure
a successful outcome for our patients.
Julie Pavlovic,
Liver Transplant Coordinator, CNC
Liver Transplant Unit, Austin Health
References:
Gow, P.J., D. Mutimer. Liver Transplantation.
Indications and outcomes at the start of the 21st
century. CME Gastroenterology 2001;
4: 17-20.
Liver Transplant Unit, Austin Hospital, Liver
Transplant Unit Website 2012, Liver Transplant
Unit Protocols and Clinician Information.
Manzarbeiria, C. & Smith, S .L, Liver
Transplantation, viewed 13/5/10
www.medscape.com/viewarticle/451209_print>
The Liver Transplant Unit relies on everydepartment in the hospital for theirexpertise to ensure a successful
outcome for our patients.

Aliver transplant is a life changing event,
and can restore health to people with
hepatitis B or hepatitis C who are in end-stage
liver disease. It has usually come after a long
time spent on a waiting list, with lots of
contact with both gastroenterology specialists
and transplant specialists. It can be an
overwhelming time, and may also seem like
your medical care is out of your control.
However, it is vital that post-transplant you
are involved and engaged in your health care
to make the most of this new opportunity.
So how can you keepyourself healthy after a liver transplant?
Take all medications as
prescribed, keep all doctor
appointments and get all
recommended tests. Medications
post transplant help the body to
accept the new organ, as well as
assist with fighting infections. You may
also be on specific treatment for your
viral hepatitis. All of these medications
need to be taken regularly, without
skipped doses, to be effective.
You will also have lots of medical
appointments in the months after your
transplant, and contact with the clinic
for the rest of your life. It is important
to keep these appointments so any
problems with your new liver can be
picked up quickly and managed
effectively.
Monitor your health. Your doctor
or nurse may have instructed you to
monitor some aspects of your health,
such as blood pressure, temperature
and weight. It is important that you do
this as directed by your doctors and
nurses and report back any changes
or problems. Similarly, if you start
having any unusual symptoms, issues
with pain or fatigue, or you become ill,
you should contact the transplant clinic.
8
Liver 2.0: Service and maintenance guideStaying well after a liver transplant
Know your medications. It is
important that you know the
medications you are on, doses and
what they do. This can be quite
challenging initially because there
may be a lot of medications and a big
change from your previous regime.
Tell your doctor about any other
medications (even over-the-
counter) you are taking. Transplant
medications can interact with a lot of
different medications and drugs – it is
important to check with your doctor
before taking anything new.
Eat a healthy diet. A diet low in fat
and salt, and high in fruits, vegetables,
whole grains and fibre is essential for
whole body health. Many people with
advanced liver disease require fluid-
restrictions, but this can change after
transplant – ask your doctor. After the
transplant you will speak to a dietitian
who can guide you on the types and
amounts of food to eat, and what to
avoid, to maintain good health.
Avoid alcohol and smoking.
Smoking and alcohol can both do
damage to your new liver, and should
be avoided post-transplant.
Exercise. Ask your doctor or
physiotherapist about exercise post-
transplant. You should be able to
make a gradual return to exercise, but
this will need to be done in
consultation with your treating team.
Regular exercise can help you to
maintain a healthy weight – it is not
uncommon to put on a few kilograms
after transplant.
Avoid infection. The transplant
drugs need to alter the function of your
immune system so your body won’t
reject your new liver. Unfortunately
this means that you are more
susceptible to all sorts of infections.
Try to avoid people who are sick,
practice good handwashing, avoid
crowded spaces like public transport
at peak hour, and talk to your doctor
about regular vaccinations you may
need. Some foods which put you at
higher risk of food poisoning (such as
sushi, shellfish, food in bain-maries
and buffets, processed meats) may
need to be avoided post-transplant.
Speak to your doctor or dietitian to find
out more about food safety.
Be sun smart. Many transplant
medications make you more likely to
tan or burn, and they also make your
immune system less able to get rid of
pre-cancerous cells. Both of these
things means you are more
susceptible to skin cancers, so slip,
slop, slap, seek and slide to stay sun
safe when outdoors.
A transplant is a wonderful, life-saving
operation for people who develop end-stage
liver disease, but it is definitely not the end of
the story. Good self management and working
closely with your treating team are the keys
to a long and healthy life with your new liver.
People with viral hepatitis who have had a
transplant are welcome to be part of our self
management programs at Hepatitis Victoria.
If you’re interested, contact Louisa
([email protected]) or the Infoline
1800 703 003 to find out more.
Reference
Australian National Liver Transplant Unit.
Information Manual for Liver Transplant
Recipients and Their Families. January 2009.
Louisa Walsh
Take Control Coordinator
Hepatitis Victoria
4
4
4
4
4
4
4
4
4

9
With over 200,000 Australians currently
living with hepatitis C and 11,000 new
infections each year, chronic hepatitis C
causes more liver transplants in Australia
than any other condition.i Around one-third of
liver transplants performed in Australia are
due to liver damage caused by the virusii,
however transplants generally only occur
when liver disease would lead to death within
two years without a transplant or if other life-
threatening complications have occurrediii.
Despite hepatitis C being the leading cause of
liver transplantation in Australia, the chance
of developing severe liver complications with
hepatitis C is quite low. After 40 years of living
with the virus, the chance of developing liver
failure or liver cancer for which the only
treatment option is transplantation is only
around 4%iv. However, when approximately
1 in 100 people in Australia has the virus,
this can lead to quite a high demand for liver
transplants.
A recent US studyv found that untreated virus
in an ageing population was contributing to a
greater demand for liver transplant relating to
hepatitis C. More than three quarters of new
patients on the liver transplant register in the
US between 1995 and 2010 had hepatitis C
and were born between 1941 and 1960. This
figure quadrupled between 2000 and 2010,
indicating a sharp increase in demand for liver
transplant among older patients with hepatitis
C. This is a trend likely to be mirrored in
Australia and New Zealand where demand for
liver transplants outweighs their availability.
The Australasian Viral Hepatitis Conference
draws together professionals and community
members on an annual basis to discuss new
developments in viral hepatitis from both
research and practice. In 2012, this
conference revealed that around 500
Australians and New Zealanders die each
year from complications relating to viral
hepatitis, however only 70 of 250 liver
transplants performed in the two countries
are in individuals with chronic viral hepatitisvi.
Approximately one in ten people on the
waiting list for a liver transplant will pass
away before one becomes availablevii.
One drug company (Janssen) that manufac -
tures treatment drugs for hepatitis C has
commissioned a study which found that
widely available anti-viral treatment could
prevent 2,200 deaths from virus-related
complications and around 10,000 people
could be prevented from having serious
liver disease developing after living with
hepatitis Cviii.
Extremely low treatment rates amongst
those with chronic hepatitis C (less than 2%)
increases the likelihood of individuals
progressing to more serious liver disease.
Without significant scale-up in treatment
provision in Australia, demand for liver
transplant will only rise, as it has done in
the US. This will particularly happen as
those with hepatitis C age and the disease
progresses. If treatment is scaled up to
reach a much larger proportion of those with
chronic hepatitis C, particularly in light of new
and more effective treatment regimens, the
need for transplants amongst this group
could potentially decline.
Similarly, the increasing prevalence of
chronic hepatitis B in our community brings
with it an elevated demand for liver
transplants. If not monitored and treated,
chronic hepatitis B can lead to life-
threatening complications in 30% of cases.
With adequate monitoring and treatment
when needed, people with chronic hepatitis B
will not need liver transplants.
With both hepatitis B and C having poor
treatment uptake in our community and
untreated disease potentially leading to
severe complications that may require liver
transplants, the importance of increasing
treatment rates cannot be underestimated
Amy Kirwan
Prison Project Officer
Hepatitis Victoria
References
i. McDonald, T. (2012) PBS decision on Hepatitis
C drugs looms ABC News
www.abc.net.au/news/2012-08-23/hepatitis-c-
treatment-decision-looms/4218946
ii. Hepatitis Australia (2012) A guide to current
and emerging hepatitis C treatments , Hepatitis
Australia, Woden
www.hepatitisaustralia.com/__data/assets/pdf_fi
le/0010/2350/Guide-to-hepatitis-C
treatments.pdf
iii. The Transplantation Society of Australia and
New Zealand (2012) Organ transplantation from
deceased donors: Consensus statement on
eligibility criteria and allocation protocols,
Australian Government Organ and Tissue
Authority, Canberra
www.donatelife.gov.au/media/docs/TSANZ_Con
sensus_Statement_V1.2.pdf
iv. Hepatitis Victoria (2012) Impact: Information
about hepatitis C, Hepatitis Victoria, Melbourne
www.hepvic.org.au/sites/default/files/Impact%20
2012.pdf
v. Batey, R. (2006) Managing hepatitis C in the
community Australian Prescriber, 29
www.australianprescriber.com/magazine/29/2/3
6/9/
vi. Australasian Viral Hepatitis Conference
(2012) Key facts and figures, published online
www.hepatitis.org.au/Key-facts-and-figures
vii. Australasian Viral Hepatitis Conference
(2012) Key facts and figures, published online
www.hepatitis.org.au/Key-facts-and-figures
viii. McDonald, T. (2012) “PBS decision on
Hepatitis C drugs looms” ABC News
www.abc.net.au/news/2012-08-23/hepatitis-c-
treatment-decision-looms/4218946
Crunching the numbersAustralian liver transplant statistics
Extremely low treatment rates amongst those with chronichepatitis C ( less than 2% ) increases the likelihood ofindividuals progressing to more serious liver disease

From
the DonateLife Book of
Life:
http://www.donatelife.gov.au/resources/book-of-
life/read-the-book-of-life#/page/405
Reprinted with permission from the author and DonateLife
10
Frank Carlus was surprised tofind out he had hepatitis C.Moving on with his busy lifehe soon realised there weremore surprises in store.
My Hep C diagnosis came about quite
by chance, long before I started to
suffer it’s worst effects, and was not
something that I initially attached a lot of
importance to.
It was a chance visit to my GP during a quiet
summer afternoon, a routine blood test to
check the speed of my blood clotting. Then
a referral to a Gastroenterologist and I was
told that I had Hep C.
“So, how do I get rid of it”, I asked. You don’t
get rid of it, there is no cure at the moment,
she responded. Some further questioning
and a passing reference was made to the
possibility of a liver transplant, should I ever
need it in the future.
I was in my very early 30’s, fit and living an
active lifestyle. So life went on, there was a
career to pursue, overseas travel, family,
sport. I wouldn’t say the issue was fully
forgotten, but it was certainly pushed to
the back of my mind.
My only ‘risk factor’ appeared to be the fact
that I was born and immunised overseas, in
Spain. Consequently I told my family of my
diagnosis and suggested that they get tested.
I sensed some skepticism, after all what
might have I got up to while living away and
at university? Had I been using drugs?
Eventually they all got tested and
unfortunately I was not alone. My mother
and younger sister tested positive for chronic
Hep C, and one of my older sisters carries
the antibodies as evidence of contact with
the virus. My mother would eventually die as
a direct result of liver failure. My younger
sister continues in the quest to find a cure
to this insidious bug.
Initially life went on for me, but more
concerning symptoms would inevitably
appear and start to undermine my general
health. By the late 1990’s, some 7– 8 years
after my original diagnosis, the tell tale
symptoms started to take their toll and I was
referred to the Alfred’s Liver Clinic.
A year or so of close monitoring, a short
course of interferon, all my body could take at
that point, and soon I was fully in the grip of
Hep C. It’s worst damage done. My liver was
cirrhotic and there was no going back. Soon
enough the subject of transplantation came
up again.
The formal referral to the Austin’s Liver
Transplant Unit came as a bit of a shock at
first. Surely there would be other solutions to
help me beat this. Apparently not! I was
placed on the liver transplant waiting list.
By mid 1999 I was down for the count. No
longer able to drive or do any thing involving
even minor exertion. I managed to stay at
work for a few more months thanks to the
strong support of my wife, employer and work
colleagues. My wife would have rather I’d
stayed home, but I wasn’t prepared to give
up, not just yet.
By then I had become used to short hospital
stays at the Austin, to undergo tests and
minor procedures and fight off infections.
I got to know the staff and the routines and
developed a great respect and confidence in
their work. My work was in the health field
and I knew the pressures that health services
work under.
Mid November, helplessly waiting, feeling my
self get weaker and sicker by the day, I got
the call – my turn had come up. With great
excitement and some trepidation my wife,
daughter and I made our way to the Austin
and the pre-op process started, but within a
few hours, by now the middle of the night, the
bad news came. Some issues with the donor
liver meant it was not suitable for me and we
were sent home, disappointed but not
dejected. My confidence in the process and
the staff kept me in a positive state of mind –
well mostly!
Many weeks would pass, my health fast
deteriorating, my mood and confidence
dropping. I suffered terrible leg cramps, poor
digestion, esophageal varices, internal
bleeding, constipation and terrible
Personal storyFrank Carlus
My sense of gratitude to my donor and his family continues to be overwhelming, and I doubt it will ever wear off.
Frank Carlus

From
the DonateLife Book of
Life:
http://www.donatelife.gov.au/resources/book-of-
life/read-the-book-of-life#/page/405
Reprinted with permission from the author and DonateLife
encephalopathy. I was on my last legs.
January 2000 was terrible, I hadn’t lost hope
or patience, but I was just hanging in there by
the barest of threads. Another false alarm
was shortly followed by the real thing early
in February. I was euphoric on my way to
theatre – I thought that one way or the other
my suffering was coming to an end.
The transplant procedure was long but
successful. The 36 long hours in Intensive
Care, not knowing where I was and what was
happening to me, were terrible. It was not
what I had expected. Beam me up Scotty!
Soon enough I was moved out to the ward,
in total isolation initially to prevent infections,
and I started to get my bearings, although I
was still connected to a central line and
several beeping machines. Better times were
around the corner. Soon I had a ravenous
appetite and I was up and about, ready to
take on the world and make up on lost
ground, or so I thought!
The transplant had not removed Hep C from
my body and the immune suppressed state of
my body immediately post transplant was its
perfect playground. The virus was having a
ball and playing merry hell with my new liver,
it tested not just my reserves but the know–
ledge and resolve of the liver transplant and
other specialists at the Austin and beyond.
11
We beat the bugger – well, not really, but we
won the first decisive battle, but not before my
new liver had been severely damaged, a ten
day long bout of prednisolone psychosis and
a few other minor complications. By week six
post transplant I was on my way home with
my new liver and a new sense of hope – a
rare second chance in life.
My sense of gratitude to my donor and his
family continues to be overwhelming, and I
doubt it will ever wear off. Importantly my
wife, family and many friends share in that
sense. The journey would never have been
possible without their firm support
The last 13 years have been relatively
smooth sailing. I was able to resume work
and a healthy active life, just like I had hoped.
I could say I am a model post transplant
patient, although unfortunately there is
probably no such thing. Everyone is different;
we all face different issues at different times.
Sadly many still die waiting for a transplant,
others recover but are not necessarily able
to resume their earlier activities and remain
challenged by their health and scarred by the
pre transplant experience of ill health and
near misses. Some of my contemporaries
have sadly passed on.
Post transplant I’ve continued to pursue a
lifestyle that would honor my donor, the
transplant team, and all of those who have
supported and encouraged me throughout
the ordeal. But don’t get me wrong, I am not
up for sainthood just yet.
Life is meant to be lived, challenges need to
be confronted, some risks need to be taken.
One does not need to be reckless to enjoy
all that life has to offer.
Post transplant cycling has become my
physical activity of choice. I am no Lance
Armstrong and I can freely admit to being on
drugs, immune suppressants mostly. I have
competed in two Australian Transplant
games, completed 6 Round The Bay in a Day
rides, and later this year I hope to complete
my tenth Murray to Moyne cycle relay from
Echuca to Port Fairy through which my work
based team, sponsored by the Better Health
Channel, has raised over $100,000 for a
number of health related organizations.
It would be wrong to present my Hep C and
transplant journey as straight forward or
easy. It has had many ups and downs, but I
look forward to every new day with a sense
of optimism. I have been given a great gift
which I respect not by attempting super -
natural feats but by doing simple every day
things as well as I can and contributing
to my community and the lives of others.
Frank Carlus
16 January 2013

12
At Hepatitis Victoria’s AnnualGeneral Meeting in 2009,musician, Shane Laffy spokeof his discovery that he hadhepatitis C and his subsequentliver transplant. Shane’s livertransplant story is told herefor Good liver readers.
Ihad my liver transplant on 31 July 2004.
I was discharged home in 13 days. I had
my birthday and wrote 30 songs. I wrote a
song and a poem for the family of the donor.
It was passed on to them. I do think about the
donor from time to time. He was a young guy
who died in a car accident. I don’t dwell on
it though, or have any guilt. I’m just lucky to
get another chance. I’ve always been a
happy-go-lucky type.
When you have your liver transplant and then
get discharged home, there’s a euphoria that
happens. Mine hasn’t gone away yet. I still
think it’s just amazing. Before the transplant,
I’d thought I was gone, and I’ve had seven
plus years of good heath now. I have a great
life. I’ve worked for community television for
ten years, I write songs, perform, I’ve got into
film editing. I’ve started learning new things
and doing things since I got my health back.
It’s been a long road but I got there in the end.
I haven’t really felt the stigma of having hep C.
Most of my friends are artists or musicians
from a certain era, and a lot of that crowd
have hep C. I know lots of people who have
died from liver failure or liver cancer and
usually it’s a result of hep C. Outside that
community of course, there’s a lot of stigma
about drug use and hepatitis. I’m not shy
about talking about it, and I’m not shy about
showing my scars.
Life afterdeath, Shane’sstory now
It’s eight years 6 months
after my transplant.
Amazing, I’m still here
enjoying life. Playing rock
& roll, writing, performing,
meeting new friends and
generally having a very
nice time of it. It’s fine to
say that I am having a
Personal storyShane Laffy
wonderful time, but the truth is, it’s the people
I have around me that make it so special. I’m
about to celebrate my 12th anniversary with
my partner. If I didn’t have that strong relation -
ship with her, I may well be gone by now.
Paulie Stewart (The Liver Brother), my old
friend from the band Painters and Dockers,
is also part of The Transplants. Paulie is
now into his 5th year of transplantation.
You couldn’t work with a better person.
Always up and at em’, eccentric to the 9’s,
and just an amazing artist, and the best PR
guy you could want. Last year we put on a
show for Donate Life Week at the Caravan
Club in Oakleigh. We had some refugee boys
from Africa, “The Flybeez” Hip Hoppin’ their
way through the afternoon. Paulie works with
these guys through The Brosnan Centre
Brunswick, and they are just fantastic people.
Paulie got the Human headline, Derryn Hinch
to give a talk and he also did his Joe Cocker
When you have your liver transplant and then get discharged home, there’s a euphoriathat happens . Mine hasn’t gone away yet.
I still think it’s just amazing.
...with Derryn Hinch.
Jo Fraser
Steve Dagg
Paul Stewart
Shane Laffy

13
impersonation You are so beautiful.
(Apparently it’s one of his old party tricks). He
then did a Painters and Dockers song with
us Your going home in the back of a divi van
and it was hilarious. I interviewed Derryn for
ASYLUM TV and he was great. His presence
also got all free to air channels to show up,
which gave us national coverage on the news
that evening. We had over 400 attend the
show, which is still a record for the venue.
Thank you Paulie, you’re a legend mate.
We lost our little mate Shaun Miller just
after the show. He was 17 and had 2 heart
transplants. His book has been published and
it looks like a movie is in the wind. Shaun was
to give a talk on the day for Heart Kids, but
was unable to attend. We miss you mate.
‘The Transplants’ are doing Donate Life Week
again this year, and will be performing in
Lygon Street, Carlton on the 3 March. We
have a couple of new members who
performed with us last year. Jo’ Fraser on
vocals and Steve Dagg on Sax, They are both
double liver transplant patients and are just
great performers, as well as John Grant (keys)
Bob Cary (drums) Colin and Michael Badger
The Transplants
(guitar and bass). Also Derryn Hinch is
coming along with Judith Durham (the
seekers) who will be reading some poetry
that she has written about organ donation,
it should be a great day.
So, it’s fine to be alive, but without all these
people, it would be a very lonely existence.
I’m a very, very lucky boy.
Shane Laffy
Musician
Shane Laffy, 56, is a 35 year veteran of the
music industry, performing with bands such as
20 Flight Rock, Man Friday, and most recently
with the Transplants and his original band
‘RUMBLE’. He spent the past decade working
in community television in Victoria.

VOILA!OILA!VOILA!
14
Organ donationCan people with hepatitis be organ donors?
To learn more about organ donation visit
www.donatelife.gov.au and discover the facts,
decide if you wish to be a donor, and discuss
the issue with your family and friends.
Article supplied by DonateLife
Ed’s note: We often talk about organ
donation in Hep C: Take Control, and
sometimes I get asked if signing up to the
organ donor register means you have to
disclose your health status to your family.
Your family knowing your medical history may
make parts of the donation assessment
process quicker, however, if someone is
identified as a potential organ or tissue donor,
they will have lots of tests done to determine
their health status, and their medical records
will be retrieved and read. A decision will then
be made by the medical team as to whether
the organs and tissue are suitable for
being transplanted into a recipient.
Part of this testing involves looking
for blood borne viruses, which
means that your family does not
have to be able to inform the
doctors of your full medical
history for a decision to be
made.
Illustra
tion
by S
wiv
el D
esig
n
In recent years the number of organ donors
and transplant recipients has increased
steadily, however, there is still more than
1,500 Australians waiting for an organ
transplant.
Although 80 percent of Australians support
donation, many Australians have still not
discussed their wishes with their families, or
are unsure if they would be able to donate.
A common myth is that you are not eligible to
donate if you have been diagnosed with
transmissible diseases, like chronic hepatitis
B or C.
This is a myth. People can be an organ
donor and have acute or even chronic viral
hepatitis (hepatitis B or hepatitis C).
Very few people die in such a way
that organ donation is possible, so
every potential organ donor is critical.
People with hepatitis are able to donate
their organs and every effort is made
to find a suitably matched recipient.
Often an organ from a donor with
hepatitis will save the life of a
potential recipient with hepatitis or a
person with only days or hours to
live without a transplant.
Organs from donors with chronic
hepatitis B can also be donated
to recipients who have already
been immunised against
hepatitis B.
DonateLife Victoria’s Organ Donor Coordinator,
Hayley Furniss.
One donor can transformthe lives of up to 10 peopleand significantly improve thelives of many more.
Last year 92 Victorians gave life-changing transplants to
267 Australians.
Many Australians do not know that less
than two percent of people will die in
hospital in the specific circumstances
where organ donation is even possible.
Every donation counts and it is
important for everyone to discuss their
wishes regarding organ donation with
their loved ones, as they will be asked
to give the final OK.
DonateLife Victoria’s
State Operations Manager,
Kelly Rogerson.

15
Ph
oto
Mic
k T
sik
as
. S
MH
.
Young BloodFor young people with hepatitis. Personal story... Imagine
Imagine you’re 13 and someone said your
mum was dying. Without a liver transplant
she wouldn’t survive till Christmas. Imagine
knowing that to save your mum, someone
would have to give the ultimate gift of life.
This was my family’s reality some years ago.
As Mum’s condition grew worse, she clung to
the life she had left, but slowly it was slipping
away. Then at midnight we received a call
that changed our family forever as a donor
liver had been found. Mum went straight into
surgery and it went well. While there were still
many post-transplant challenges, Mum met
them all and returned to near perfect health.
This moment forever changed my life.
Between the dedication of Mum’s medical
team and the courageous and selfless gift
of life from the donor family, I wanted to
give something back.
In 2005 at age 15, I saw the Tour de France
and an idea hit me—a ride to raise awareness
and get people talking about organ and tissue
donation. Two years later I completed the
inaugural Awareness Ride during Australian
Organ Donor Awareness Week, cycling
over 1,800km and raising much needed
awareness. Then in 2009 another cycle ride
took me from Cairns to Brisbane, helping to
further spread the word about organ donation.
Recently Mum needed another transplant,
and again thanks to a kind selfless donor,
one was found. They say each donor can
help the lives of up to ten people and I knew
that if I could change one person’s perspec -
tive on organ donation, then indirectly, I might
improve the lives of ten.
I encourage everyone to think about organ
donation and talk about it with your family.
Imagine if your discussion or decision resulted
in saving one life, or even ten. To you, I’d be
forever grateful.*
Josh
E H T Y I F O A H Y C F M R S Y T S E D
K D Y A P N Y C F C S O E K L Y R L N E
K K O D I Y T X Y S N C R I F X A A A C
T Y F C A L F E E C I L M N L N N T B I
X E N O T R A N S P L A N T E K S I S D
S F M T Z O E R I T F O T A P A P P I E
E G X E Y R R E T I I T S Q N R L S R L
S O D Z A O N S I S S N A P J P A O B E
R Y S W X T B Z A V U F E R O R N H Y S
U R A M S T N E M E G A G N E R T K C T
N C O M M U N I T Y R D F T Y C I L N E
D E S A E C E D R E I C S W O O I N H C
S H O R T A G E S S L I N R O N O D E H
E U S S I T V N C E G P G A I S L L K N
B J K K I I G U F E V A O C P E U R X I
I O B O L V S Z R Y N I A E S N N O P Q
Y E W B J S H E A R T L L K P T G W M U
E K K E E Z X T F V K K I D N E Y C W E
F O F Y L R H W T J Z N L F P R L H O P
S P K X I H T T M G B M O L O F U M I P
AUSTRALIA
AWARENESS
BOWEL
BRISBANE
CLINICAL
COMMUNITY
CONSENT
CORNEA
CYCLOSPORINE
DECEASED
DECIDE
DISCUSS
DOCTORS
DONOR
ENGAGEMENT
FAMILY
HEART
HOSPITALS
INTESTINE
KIDNEY
LIVER
LIVES
LUNG
NURSES
ORGAN
PANCREAS
PEOPLE
RECIPIENTS
REGISTER
SHORTAGE
SKIN
TECHNIQUE
TISSUE
TRANSPLANT
WORLD
XENOTRANSPLANT
FIND-A-WORD by Lauren Proudfoot
* From the DonateLife, Book of Life:
www.donatelife.gov.au/resources/book-of-
life/read-the-book-of-life#/page/405
Reprinted with permission from the author
and DonateLife

16
Moving inAmy Kirwan
After a very productive 2012, I am
excited and looking forward to the
New Year. Of note from last year were two
important projects that I worked on:
Firstly, I attended the Mob in the Margins
Forum – Ararat, Warrnambool, Swan Hill
and Cobram.
This Forum was to open high level
discussions with CEO’s and Aboriginal
Community Controlled Health Organisation
(ACCHO) board members on Viral Hepatitis
prevention in Victorian Aboriginal
communities. As Hepatitis C rates are 6 times
higher in Aboriginal Communities, over 80%
of new hepatitis C (HCV) infections are from
injecting drug use. Needle Syringe Program
(NSP) services are proven to reduce HCV
and HIV transmission and increase support to
a vulnerable group in the Aboriginal
population. The Yiaga ba Wadamba Report
recommendations show that Aboriginal
people who inject drugs want NSP services
from ACCHO and culturally competent
mainstream services. I accompanied
VACCHO staff and we were fortunate to
spend a day at the people at Lake Condah
Mission who were holding their annual
Strengthening Community Day.
Secondly, VACCHO Chronic Disease and
Health Lifestyle Forum was held late
November and Hepatitis Victoria’s Aboriginal
Program had a stall. This State-wide event
was aimed at health care professionals
working in the Aboriginal Health Sector and
focused on chronic conditions, such as:
• smoking cessation and control;
• nutrition and physical activity;
• sexual health and blood borne viruses;
• general health promotion.
This was a great opportunity for Hepatitis
Victoria to network with other organisations,
government departments and ACCHO’s from
rural, urban and regional Victoria. It was
also an excellent chance to develop
networks and partnerships with other
Aboriginal organisations and communities.
2013 began with the Hepatitis Victoria
Aboriginal Program participating in theYoung
Aboriginal and Torres Strait Islander National
Sexual Health Survey on Survival Day,
26 January.
This iniative involved developing and
conducting the first Australia-wide study
describing levels of knowledge, risk practices
and access to health services in relation to
sexually transmitted infections (STI’s) and
blood borne viral infections (BBV’s) among
young Aboriginal and Torres Strait Islander
(TSI) people aged 16 to 29 years.
Another exciting project is our multi–
organisational partnership with the Aboriginal
Community Development Workers from the
Melbourne Sexual Health Centre; Konnect -
Jesuit Social Services; Cancer Council
Victoria; Victorian Aboriginal Health Service
(VAHS); to deliver educational sessions to
the Aboriginal prison population.
I am looking forward to working with and
developing further strong partnerships with
other Aboriginal Organisations and the
community around the state as well as
working with the Aboriginal Liaison Prison
Officers.
Felicity Omar
Health Educator
Aboriginal Program
Aboriginal Program
Hi, I’m Amy Kirwan, the new Prisons
Project Officer at Hepatitis Victoria.
My focus will be on exploring how particularly
marginalised prisoners (young people in the
adult prison system, women and prisoners
from non-English speaking backgrounds)
can be better served by the organisation
and their opportunities to become educated
about viral hepatitis can be improved.
I have spent the past nine years working in
public health in Victoria. My early beginnings
were in community health over on the
Richmond public housing estate working to
assist health service providers to respond
to the needs of culturally and linguistically
diverse communities. For the last five years I
have worked in the harm reduction field with
a range of roles across policy advocacy,
research and frontline service delivery. It is
in this field that I feel I have found my niche,
particularly through my work with prisoners
and injecting drug users, two of Hepatitis
Victoria’s key population target groups. I am
also a qualified social worker.
Each person has a story. While these
stories may have common themes, such as
disadvan tage and poor physical and mental
health, each person has had their own
journey. Sometimes the most important
thing anyone can do is listen and just treat
them as another human being, as this is
often missing from people’s experiences.
I hope to work with a range of stakeholders
to ensure that these individuals are given the
opportunity to make informed choices about
their health.
Amy Kirwan
Prisons Project Officer

17
Last issue we told you about our new
service Hep Connect, which provides an
opportunity for people with hepatitis C to
mutually discuss their experience with a trained
peer volunteer over the telephone. All peer
volunteers have experience of living with
hepatitis C and have undertaken hepatitis C
treatment or are living with cirrhosis. Hep
Connect is a free and confidential service.
Read below to find out how it’s going from an
Infoline caller and the corresponding Hep
Connect volunteer.
Background
Sophia’s partner was about to start treatment
for hepatitis C and Sophia wanted to learn
more about what that would be like for him.
She wanted to understand what he might go
through so she was able to provide him with
the support he needed. Hepatitis Victoria
Infoline staff connected Sophia to a male
volunteer who has been through treatment.
Sophia – Infoline callerSometimes, your partner doesn’t tell you
everything. Maybe he just doesn’t know and
doesn’t want to ask the question. I spoke
with David and he covered everything I
needed to know.
“He made me see reality”
It was very good to hear what going through
12 months of treatment was like for David, as
I want to be there for my partner and now I
know it’s going to be difficult, I can prepare
for it. I can work out how I will cope. I would
definitely recommend Hep Connect to other
people and might use it again in the future.
It would be great to talk to other partners of
people who have been through treatment.
David – Hep Connect Volunteer
Recently I received my first request
through the Hep Connect program to speak
to somebody about my experience of going
on hepatitis C treatment.
We were able to cover a lot of topics during
our chat. These topics included preparation
for treatment (or, in some cases, my lack of
preparation) and understanding how and
when to administer the drugs and be
educated about their possible side effects.
We also discussed in detail having support
from family, friends and the relevant
medical professionals. Clearly these
support networks weren’t great for me at
the time, but I would say that was largely
owing to my own stubbornness.
I tried to relate as best I possibly could
about my thoughts and emotions while on
the interferon/ribavirin medication. I have to
say that a lot of my thoughts and feelings
during the treatment were quite negative.
Largely owing to this often negative
experience, I cautioned against rushing
onto treatment unless it really is an urgent
matter. Perhaps the fact that I didn’t clear
the virus has tended to make me view my
story in a poor light.
As for Hep Connect, I think these contacts
can be very beneficial, for both the caller
and the called. It’s not always easy for an
individual to seek a counselling or support
service face to face and this could be due
to different factors. They may be shy, they
may live in a remote area or it could be
something else I haven’t thought of.
Overall, I enjoyed sharing my experience in
the hope that it can assist somebody else
in their journey.
Call for Hep Connect
volunteers:
Are you the partner of someone who
has been through treatment?
Are you interested in supporting
other people like yourself?
For more information contact
Garry Sattell on the
Hepatitis Infoline 1800 703 003
Hep ConnectA case study

18
We need YOUR help!Making a donation to Hepatitis Victoria helps us to help others.
I would like to make a donation of $
q Please find my cheque/money order enclosed.
Please debit my: q Visa q Mastercard q American Express q Diner
Club
Name on card: Signature:
Title: First name: Surname:
Address:
Postcode: Email: Phone: ( )
Expiry date:
In the first half of 2013 HepatitisVictoria is running the popular andsuccessful Hep C: Take Control as an Internet-based program.
We are currently looking for people with hepatitis
C, or who have had hepatitis C in the past,
to help us trial our Internet-based group.
Hep C: Going Viral will be a six week online
group program with a focus on health education
around hepatitis C, and learning the skills for
setting goals around health and well-being.
The online group will be made up of between
5 and 10 people, and will consist of a weekly
one hour online (typed) chat session with the
whole group, plus some modules you can work
on in your own time, for your own learning.
The commitment will be around one and a half – two
hours (one hour group chat, 30 mins to one hour module
activities) per week for six weeks. The modules will be
tailored to your health needs and interests. Multiple
groups will be running (including outside work hours),
so we should be able to find a day and time to suit
your needs.
Previous participants in Hep C: Take Control are also
welcome, and this will be great way to refresh some of
those self management skills, and get your health back
on track if you’ve had a few slips recently.
If you are interested in being part ofHep C: Going Viral, or would like more information, please contactLouisa Walsh at Hepatitis Victoria on1800 703 003 or [email protected]
HepC:Going ViralDo you have, or have you ever had, hepatitis C?
Would you like to connect with other people with hepatitis C?
Face-to-face not your style?

19
JOIN BEFORE THEPRICE RISE IN JULY,(currently $77 for organisations)
WITH NO RENEWALUNTIL JULY 2014!
Having remained unchanged for several years, the
Hepatitis Victoria membership fee is set to rise
on 1 July, 2013
We are committed to growing our organisational
capacities and will be able to provide our members
with the best possible tools, services and resources.
2013 will see the addition of new resources, new
programs, new services, and a dedicated approach to
providing a flow-on of valuable benefits to our members.
As an organisation we are constantly striving to raise
awareness and support for those affected by viral
hepatitis. Unfortunately much of the community see
hepatitis as a 'dirty word' rather than a chronic disease
that 400 million people worldwide are living with at
this very moment (over 400,000 Australians – 2% of
our population!)
By becoming a member you are also providing a voice for people living with viral hepatitis.
Hepatitis Victoria membershipMake a difference. Become a member of Hepatitis Victoria.
Fees from 1 July, 2013
• Organisations $150
• Individuals $40
• Concession (student, pensioner, unemployed) $15
• People living with viral hepatitis $0 (or by donation)
To join please email Lisa Nulty: [email protected]
PROMOTIONAL OFFER!

20
Liver clinics and liver specialistsTo access public hepatitis C treatment
services a referral from a GP is needed.
In most cases a referral is faxed to the
hepatitis treatment service. The hepatitis
treatment services will generally not discuss
your treatment options with you until after
they have received a referral from your GP.
This list of hepatitis treatment services
includes clinics that are known to Hepatitis
Victoria. Not all possible services are listed
and there may be others in your local area.
ALBURYAlbury Community Health – Hepatitis Clinic
Suite 3, Albury Wodonga Specialist Centre
2 Ramsey Place, West Albury.
Contact: (02) 6058 1800
Fax: (02) 6058 1801
BAIRNSDALEBairnsdale Regional Hospital
Bairnsdale Regional Health Service
Specialist Consulting Rooms.
Princes Hwy, Bairnsdale.
Contact: 5150 3478
Fax: 5150 3404
BALLARATBallarat Base Hospital
Drummond Street, Ballarat
Contact: 5320 4211
Fax: 5320 4472
BALLARATBallarat Community Health
210 Stuart Street, Ballarat
Contact: 5338 4500 or 5320 7500
Fax:5339 3044
BENDIGOBendigo Health
Cnr Arnold and Lucas Streets, Bendigo
Contact: 5454 8422
Fax: 5454 8419
BOX HILLBox Hill Hospital
16 Arnold Street, Box Hill
Contact: 9895 3333 (ask for OPD)
Fax: 9895 4852
CLAYTONSouthern Health Monash Medical Centre
246 Clayton Road, Clayton
Contact: 9594 6035
Fax: 9594 6925
CRANBOURNESouthern Health Monash Medical Centre
Contact: 95943177
Fax: 9594 6245
EPPINGNorthern Hospital
185 Cooper Street,
Contact: 8405 8000
Fax: 8405 8761
FITZROYSt Vincents Hospital
35 Victoria Parade, Fitzroy
Contact; 9288 3771
Fax: 9288 3489
FOOTSCRAYWestern Hospital
Eleanor Street, Footscray
Contact: 8345 6291
GEELONGGeelong Hospital
Ryrie Steet, Geelong
Contact: 5246 5117
Fax: 5221 3429
GIPPSLANDCentral Gippsland Health Service
Guthridge Parade, Sale.
Contact: 5143 8600
Email: [email protected]
HEIDELBERGAustin Hospital
145 Studley Road, Hiedelberg
Contact: 9496 2787
Fax: 9496 7232
MAROONDAHMaroondah Hospital (Eastern Health)
Out-Patients, Ground Floor, Davey Drive,
Ringwood East
Contact: 9895 3333
Fax: 9871 3202
MOORABBINBayside Liver Clinic (Alfred Hospital)
999 Nepean Highway, Moorabbin
Contact: 9276 2223
Fax: 9276 2194
MILDURAMildara
234 Thirteenth Street, Mildura
Contact: 0408 581 781
PARKVILLERoyal Melbourne Hospital
Corner Royal Parade and Grattan Streets,
Parkville
Contact: 9342 7212
Fax: 9342 7277
PRAHRANAlfred Hospital
Gastroenterology Department
55 Commercial Road, Prahran
Contact: 9076 2223
Fax: 9276 2194
Alfred Hospital
Infectious Diseases Unit
55 Commercial Road, Prahran
Contact; 9076 6081
Fax: 9076 6578
SHEPPARTONGoulburn Valley Health
50 Graham Street, Shepparton
Telephone: 03) 5832 3600
SPRINGVALESpringvale Community Health
55 Buckingham Street, Springvale
Contact: 9594 3088
TRARALGONLatrobe Regional Hospital
Private Consulting Suites 3 and 4
Princes Highway, Traralgon West.
Contact: 5173 8111
WARRNAMBOOLWestern Region Alcohol and Drug Centre
(limited hepatitis treatment services)
172 Merri Street, Warrnambool
Contact: 1300 009 723
WODONGAMurray Valley (Private) Hospital
(Dr Tim Shanahan – Gastroenterologist)
Nordsvan Drive, Wodonga. Vic.
Contact: (02) 6056 3366
WODONGAWodonga Regional Hospital
Vermont Street. Wodonga
Contact: (02) 6051 7413
Liver clinics

21
Contacts
Community-based hepatitis C treatment servicesCommunity based treatment clinics have
been developed to enable more people to
access treatment in their local communities.
Living Room
7 – 9 Hosier Lane, Melbourne
Contact: 9945 2100
Health Works
4 –12 Buckley Street, Footscray
Contact: 9362 8100
Barkley Street Medical Centre
Dr Elizabeth Leder
Monthly visiting Gastroenterologist
and hep C Nurse
60 Buckley Street, St. Kilda
Contact: (03) 9534 0531 or (03) 9288 2259
Greater Dandenong
Community Health Service
Hepatitis C outreach treatment clinic
229 Thomas Street, Dandenong
Contact: 9594 3089
Cranbourne Integrated Care Centre
Hepatitis C outreach treatment clinic
as part of Southern Health Services
140–154 Sladen Street, Cranbourne
Contact: 9594 3089
North Richmond
Community Health
Dr John Furler
Weekly visiting Hep C Nurse
23 Lennox Street, Richmond
Contact: (03) 9418 9800 or (03) 9288 2259
St. Kyrollos Family Clinic
Dr Ashraf Saddik
Monthly visiting Hep C Nurse
2A Moore Street, Coburg
Contact: 9386 0900 or 9288 2259
Werribee Mercy Hospital
Consulting Suites
300 Princess Hwy, Werribee
Contact: 9386 2259
Fax: 9288 3596
North Yarra Community
Health
Dr Ohnmar John
Weekly visiting Hep C Nurse
75 Brunswick St, Fitzroy
Contact: 9411 3555 or 9288 2259
Dr John Sherman
GP who does hepatitis C treatment
Also opiate replacement therapy
131b Hopkins Street (rear)
(entry via Chambers Street), Footscray
Contact: 96891602
Primary health carecentres (for people who use drugs) Primary Needle Syringe Programs
Living Room
Primary healthcare and needle
syringe program
Hepatitis C information, support
and treatment services
7–9 Hosier Lane (off Flinders Lane),
Melbourne
Contact: 9662 4488
www.youthprojects.org.au
Access Health
Primary healthcare and needle syringe
program for marginalised/street based
injecting drug users, street sex workers and
people experiencing homelessness.
Hepatitis C information, support and
treatment
31 Grey Street, St. Kilda
Contact: 9536 7780
Inner Space
Primary healthcare and needle
syringe program
Hepatitis C information, support
and treatment.
4 Johnson Street, Collingwood
Contact: 9468 2800
www.nych.org.au/services/drug.html
South East Alcohol and
Drug Service (Forster Street)
Primary healthcare and needle syringe
program
84 – 85 Forster Street
Dandenong
Contact: 9794 7895
Health Works
Primary healthcare and needle
syringe program
Hepatitis C information, support
and treatment
4-12 Buckley Street
Footscray
Contact: (03) 9362 8100
www.wrhc.com.au/Services_HEALTH.html
Services-Metro/statewideCOMPLEMENTARY MEDICINESNational Herbalist Association
of Australia
Peak body of accredited herbalist
and naturopaths
Contact: (02) 8765 0071
www.nhaa.org.au
Professor Jerry Zhang (Jiansheng)
Chinese Medical Service, specialising in
Chinese Immunology, internal medicine
and dermatology
Suite 9, 2nd floor, 517 St. Kilda Road,
Melbourne
Contact: 9820 4462
Jenny Adams
Naturopath
Wellness Medicine Centre.
Integrating western medicine with
complementary and alternative medicine
41 Queens Parade, Clifton Hill
Contact: 9489 7955
www.wellnessmedicine.com.au
Gill Stannard
Herbalist and Naturopath
City Natural Therapies
510/220 Collins Street, Melbourne
Contact: (03) 9650 3419
gillstannard.com.au
Kundalini House
Wide range of complementary therapies
1/391 St Georges Road, Fitzroy North
Contact: 9482 4325
www.kundalinihouse.com.au

22
COUNSELLING SERVICESCaraniche
Free Counselling
Community Alcohol and Other Drug Services
Craigieburn Office – 8339 6800
Whittlesea Office – 0429 855 673
Positive Health
(Hep C) Counseling
Victorian AIDS Council
6 Clarendon Street, South Yarra.
Telephone: 9865 6700
1800 134 840 (freecall for country callers)
Direct Line
(Drug and alcohol counselling and NSP info)
Free call: 1800 888 236
Margie Fry
Psychologist, Nexus Psychology
Balwyn Road Medical
353 Balwyn Road, Balwyn North
Telephone: 9500 0751
www.nexuspsychology.com.au/
MEDICAL SERVICESRoyal District Nursing Service
Telephone: 9536 5222
Email: [email protected]
Indigenous HealthNgwala Willumbong Co-op Limited
93 Wellington Street, St Kilda
Indigenous drug and alcohol service
Telephone: 9510 3233
Email: [email protected]
VACCHO (Victorian Aboriginal Community
Controlled Health Organisation)
17 – 23 Sackville Street, Collingwood.
Telephone: 9411 9411
Email: [email protected]
Web: www.vaccho.org.au
Victorian Aboriginal Health Service
186 Nicholson Street, Fitzroy
Telephone: 9419 3000
Fax:9417 3897
Sexual HealthMelbourne Sexual Health Centre
580 Swanston Street, City
Telephone: 9347 0244
Free call: 1800 032 017
Multicultural Health and
Support Service, Carlton
81 – 85 Barry Street, Carlton.
HIV, hepatitis C and sexually
transmissible infections
Telephone: 9342 9720
Go to: www.ceh.org.au/mhss.aspx
MISCELLANEOUS SERVICESANEX (Association of
Needle Exchanges)
Suite 1 Level 2, 600 Nicholson Street,
North Fitzroy
Telephone: 9486 6399
Email: [email protected]
HIV/Hepatitis/STI Education and
Resource Centre at the Alfred
Moubray Street, Prahran
Statewide resource centre on HIV/AIDS,
Hepatitis and Sexually Transmissible
Infections
Telephone: 9276 6993
Email: [email protected]
Web: www.hivhepsti.info
Turning Point Alcohol
and Drug Centre, Fitzroy
54-62 Gertrude Street
Telephone: 8413 8413
Email: [email protected]
Web: www.turningpoint.org.au
Victorian Equal Opportunity and
Human Rights Commission
Level 3, 380 Lonsdale Street, City
Information on state and federal equal
opportunity laws and programs
Telephone 9281 7111
Freecall: 1800 134 142
Email: [email protected]
Web: www.humanrightscommission
.vic.gov.au
Haemophilia Foundation Victoria,
13 Keith Street, Hampton East
Bleeding disorders and hepatitis C.
Telephone:9555 7595
Hepatitis Australia
Web forum for professionals in the hepatitis C
sector.www.hepatitisaustralia.com/
forum/publicaccess/
Office of the Health Services Commissioner
30th Floor, 570 Bourke Street, City
Telephone: 8601 5222
Complaints: 8601 5200
Freecall: 1800 136 066
Victorian Viral Hepatitis Educator
Training for Doctors, Nurses and
other health professionals
Telephone 9288 3586
Mobile 0407 865 140
Harm Reduction Victoria (HRV)
128 Peel Street, North Melbourne
Telephone: 9329 1500
Email: [email protected]
Website: www.hrvic.org.au
Multilingual Hepatitis C Resources
This website has over 400 pages of hepatitis C
and HIV information in 18 languages.
www.multiculturalhivhepc.net.au
Services - RegionalThese contacts are able to provide
information about local viral hepatitis related
services as well as active support groups.
Ballarat Community Health
Contact: Marg Stangl
Telephone: (03) 5338 4500
Barwon - Surf Coast Health Service
Telephone: 03) 5261 1100
Barwon Health Drug and Alcohol Services
Telephone: (03) 5273 4000
Bendigo Health Care Group
Contact: Catina Eyres
Telephone: 5454 8414
Camperdown Hepatitis C Support worker
Contact: Jo Sloetjes
Telephone: 5593 3415
Email: [email protected]
CAN (Country Awareness Network),
Bendigo
Information, education, support, referrals
and advocacy to Victorian rural/regional
communities regarding HIV/AIDS, Hepatitis C,
other Blood Borne Viruses and Sexually
Transmitted Infections
Telephone: 5443 8355
Email: [email protected]
Web: www.can.org.au

HEPATITISVICTORIASUPPORT GROUP
Meets monthly on a Sunday
between 2.00pm – 4.00pm
The Hepatitis Support Group meets
at the office of Hepatitis Victoria,
Suite 5, 200 Sydney Road, Brunswick.
The meetings are a great place to meet
other people who are also living with
hepatitis. The group is friendly and
welcoming and comprises people from
various backgrounds who come together
once a month to talk about their
experiences of living with hepatitis.
One aspect of the group is support while
another is socialising regularly with
people who are going through the same
sorts of challenges as you. It’s a great
way to deal with those feelings of
isolation and aloneness.
You can call Garry on the Hepatitis Infoline
1800 703 003 if you want to either attend
a meeting or would like to learn more
about how the support group works.
Garry Sattell
Community Participation Coordinator
(Support Group Facilitator)
Upcoming Support Group dates in 2013
March 17
April 21
May 19
June 16
July 21
23
Jigsaw Youth Health Service
Contact: Rochelle Hamilton
Telephone: 5279 2754
Latrobe - Mobile Drug Safety Worker
Helen Warner
Mobile: 0438 128 919
Mildura - Sunraysia Community Health
Contact: Anne Watts
Telephone: 5023 7511
Moe Community Health Centre
Telephone: 5127 5555
Portland - Glenelg Southern Grampians
Drug Treatment Service
Contact: Bev McIlroy
Telephone: 5521 0350
Shepparton Community Health
Telephone: 5823 3200
Wangaratta - Ovens and King
Community Health Centre
Contact: Diane Hourigan
Telephone: 5723 2000
Warrnambool - Western Region
Alcohol and Drug Centre (WRAD)
Dr Brough is offering limited specialist
services from the WRAD centre on the
2nd Thursday of each month.
Telephone: 1300 009 723
Wimmera (East) Region
(Birchip, Wycheproof, St Arnaud)
Phil Blackwood (Naturopath/Psychologist)
Mobile telephone: 0403 625 526
Wodonga Community Health
Contact: Jenny Horan/Anita
Telephone: (02) 6022 8888
Yarra Valley Community Health Service
Contact: Debra Cahill
Telephone: 1300 130 381
Yarrawonga Community Health
Contact: Cherie McQualter Whyte
Telephone: 5744 1324
Hepatitis C support on the InternetAustralia Hepatitis C Support (AHCS)
A community-based information resource,
providing support and assistance to people
from Australia and around the world.
www.hepcaustralia.com.au
Hep C Australasia Forum
A community based internet discussion
forum which aims to empower people
affected by hepatitis C by providing a place
to share ideas, opinions and support
www.hepcaustralasia.org/
'Our C-ciety' Hepatitis C Support Website
This is a hepatitis C support web site with an
injecting drug use focus. It is for those who are
interested in hepatitis C, injecting drug use and
pharmacotherapy, regardless of hepatitis C
status or history of injecting drug use.
‘Our C-ciety’ still has a separate peer
support closed section for people who are
living with hepatitis C and have a history
of injecting drug use and/or are on a
pharmacotherapy program.
http://c-ciety.ning.com/
Hepatitis B support on the InternetHepatitis B Support List
A worldwide information and support group,
dedicated to providing timely resource
information and support to all those
involved with Hepatitis B.
www.hblist.org/
Hepatitis C support/discussion groupsBrunswick Hepatitis C Support Group
Group meets monthly. (See advertisement
at right side of this page)
Frankston Hep C Discussion Group
SHARPS
20 Young Street, Frankston
Hep C Nurse visits weekly on Tuesdays
10.00am – 1.00pm
Call Melissa 9781 1622

Chinese
Amharic
Khmer
Vietnamese
Farsi
Arabic
EnglishHepatitis C Information Line. To use an interpreter withthis service first call 131 450
Hepatitis InfolineCall to talk to an Educator about hepatitis.
Information: We can answer questions
and mail information to you.
Support: We can provide support for a range
of issues and concerns.
Referral: We can refer you to other
organisations and services.
The Hepatitis Infoline is a free
and confidential service
for all Victorians.
1800 703 003
www.hepvic.org.au
Your donations help us to provide information, services,
advocacy, resources and support for people affected by
hepatitis C, health profess ionals and members of the general
Your donations make a difference!
I would like to donate the following amount:
■ $20 ■ $50 ■ $100 $_____ (Your choice)
I have enclosed my cheque/money order/cash or
Please debit my credit card for $______
Type of card: Visa/MasterCard
Name on Card
Card number:
■■■■ ■■■■ ■■■■ ■■■■Expiry Date
Please send my receipt to:
Name
Address
Suburb/City
Postcode State
Send to: Hepatitis Victoria
Suite 5, 200 Sydney Road
Brunswick, Victoria. 3056
public. All donations of $2 or more are tax deductible.
If you do not receive your receipt promptly, then please call
Halo Jones on 03 9380 4644.