Embed Size (px)
Citation preview
GRACE(Geriatric Rapid Acute Care Evaluation)
2NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
NSW Department of Health73 Miller StreetNORTH SYDNEY 2060Tel: (02) 9391 9000Fax: (02) 9424 5994www.health.nsw.gov.au
This work is copyright. It may be reproduced inwhole or in part for study training purposes subjectto the inclusion of an acknowledgement of thesource. It may not be reproduced for commercialusage or sale. Reproduction for purposes other thanthose indicated above, requires written permissionfrom the NSW Department of Health.
© NSW Department of Health
SHPN (HP) 060088ISBN 0 7347 3954 0
For further copies of this document please contact:Better Health Care Centre - Publications WarehouseLocked Mail Bag 5003Gladesville NSW 2111
Tel: (02) 9879 0443Fax: (02) 9879 0994
Further copies of this document can be downloadedfrom the Australian Resource Centre for Hospital Innovations(ARCHI) website: http://www.archi.net.au/e-library/build/moc
Model of Care concept Angela Littleford and Judith Carll
Design by Elisabeth Sampson (02) 4968 1337
June 2006
3NSW HealthClinical Services Redesign ProgramTransitional Aged Care
Acknowledgments 4
Executive Summary 5
Section One: The need for change
Lilly’s Story Prior to GRACE 6
Background to the Model 8
Hornsby Ku-ring-gai Health Service 9
Section Two: Geriatric Rapid Acute Care Evaluation (GRACE)
Lilly’s Story Under GRACE 10
What is GRACE? 12
Aims 12
Benefits 13
GRACE Flowchart 14
How Does GRACE Work? 16
GRACE Emergency Department Flow 18
GRACE Success Stories 20
Establishing and Maintaining GRACE 22
Staffing 24
Section Three: Resources
Resources 25
Implementing GRACE 26
Table of Contents
4NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
Acknowledgments
Acknowledgments and AdvisorsThis model of care has been developedby the Hornsby Ku-ring-gai HealthService.
NSW Health would like to acknowledgethe contribution of the following people atHornsby Ku-ring-gai Health Service(HKHS) who assisted in the developmentof this model.
Associate Professor Susan KurrleClinical DirectorSenior Staff SpecialistRehabilitation and Aged Care
Dr Brett Gardiner, Director MedicalServices.
Ms Jenny Houston, GRACE ProjectLeader.
Ms Anne Bruce, Clinical Nurse Consultant,GRACE Project.
Ms Rosalyn Ferguson, Emergency NursingUnit Manager.
Mr Danny Mayor, Emergency Medical UnitManager.
Ms Alison Powis, Nursing Manager,Rehabilitation and Aged Care Service.
Ms Sharon Strahand, Clinical NurseConsultant, Aged Care Services inEmergency Team.
Marion Harris, Aged Care Liaison Nurse.
After Hours GRACE/ASET nurses - Felicity Hollins- Makasini Kaho- Pamela Lee-Chue- Nadia Yazdani
Ms Deborah Mayall, Bed Manager.
Trish Price, Leighton Lodge Nursing Home
Narrelle Bath, Waldergrave House
Ines Vansevenant, Masonic Towers Hostel
Dr Angus Cottee, GP representative
Dr Magda Campbell, General PracticeLiaison Officer
Mary Potter, Hornsby Ku-ring-gai RydeDivision of General Practice
Staff at the Northern Sydney HomeNursing Service
Staff at the Northern Sydney CentralCoast Acute Post Acute Care Service
Ms Kerry Robinson, Aged Care EarlyIntervention and Management ProjectOfficer, Gold Coast District, QueenslandHealth Department
The Directors of Nursing and CareManagers of aged care facilities.
EndorsementsNSW Health would like to thank thefollowing people for their extensivecomments and endorsement of this model of care.
Jean McCoy, Care Services Manager,Christian Brethren Community Services
Dr Stephen Christley, Chief Executive,Northern Sydney Central Coast AreaHealth Service.
5NSW HealthClinical Services Redesign ProgramTransitional Aged Care
The number of aged care facility residentsbeing admitted to hospital has beenincreasing over the past decade. Thepopulation is ageing and demanding morefrom current services.
New models of care are required to meetthese increasing expectations anddemand for services.
Hospital admissions for aged care facilityresidents are often physically andemotionally disruptive. In hospital, olderpatients have higher rates of adverseevents and are more likely to becomedeconditioned.
There is strong evidence that treatingnursing home and hostel residents in thehome improves outcomes for thesepatients. While the benefits of caring forresidents in an aged care facility ratherthan in hospital are increasinglyrecognised, these facilities are oftenchallenged in managing acute and sub-acute illness.
This model of care has been developed bythe Hornsby Ku-ring-gai Health Service(HKHS).
Under the Rapid Evaluation and AcuteCare for Aged Care Residents Model ofCare (hereafter referred to as GRACE),hospital staff work in collaboration withgeneral practitioners and aged carefacilities to improve the journey of agedcare facility residents. Enhanced hospitalresources support general practitionersand aged care facility staff to care forresidents at home, avoiding hospitaladmissions.
At the centre of the model is the GRACEClinicial Nurse Consultant (CNC). ThisCNC, along with other hospital staff,manages a single entry, 7 day per week,telephone triage service for aged carefacilities and their general practitioners.The GRACE team also provides support,education and training to staff of the agedcare facilities.
When hospital admission is required, careis case managed by the GRACE CNC tofacilitate rapid treatment and ensure thepatient’s stay in hospital is as short aspossible.
The success of GRACE relies onpartnerships between the hospital, agedcare facilities and their residents’ generalpractitioners. It also requires enhancedcollaboration between GRACE and otherclinical, nursing, community health andadministrative staff.
Initial data indicates that GRACE hascontributed to high levels of avoidedhospital admissions, reduced accessblock for older patients and reducedaverage length of stay at HKHS. TheGRACE project has enhanced the journeyof aged care facility residents and helpedto improve communication and trustbetween the hospital, general practitionersand the aged care facilities.
Executive Summary
6NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
Lilly’s Story Prior to GRACE
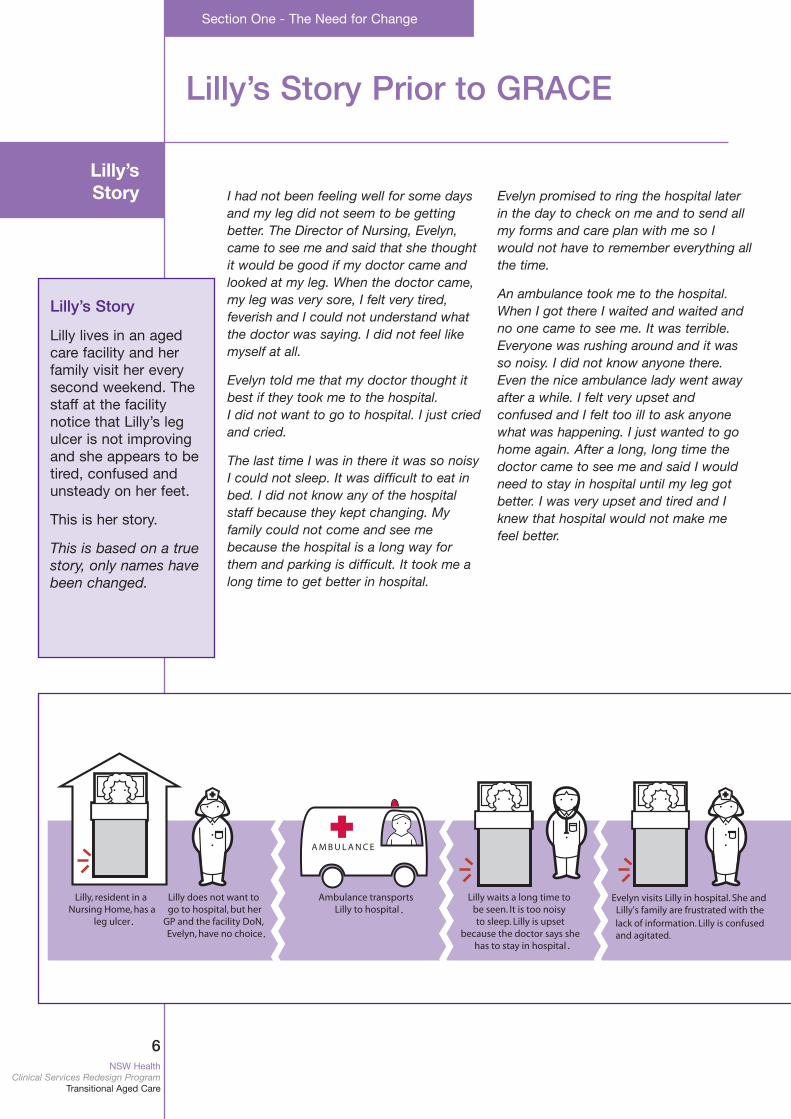
I had not been feeling well for some daysand my leg did not seem to be gettingbetter. The Director of Nursing, Evelyn,came to see me and said that she thoughtit would be good if my doctor came andlooked at my leg. When the doctor came,my leg was very sore, I felt very tired,feverish and I could not understand whatthe doctor was saying. I did not feel likemyself at all.
Evelyn told me that my doctor thought itbest if they took me to the hospital. I did not want to go to hospital. I just criedand cried.
The last time I was in there it was so noisyI could not sleep. It was difficult to eat inbed. I did not know any of the hospitalstaff because they kept changing. Myfamily could not come and see mebecause the hospital is a long way forthem and parking is difficult. It took me along time to get better in hospital.
Evelyn promised to ring the hospital laterin the day to check on me and to send allmy forms and care plan with me so Iwould not have to remember everything allthe time.
An ambulance took me to the hospital.When I got there I waited and waited andno one came to see me. It was terrible.Everyone was rushing around and it wasso noisy. I did not know anyone there.Even the nice ambulance lady went awayafter a while. I felt very upset andconfused and I felt too ill to ask anyonewhat was happening. I just wanted to gohome again. After a long, long time thedoctor came to see me and said I wouldneed to stay in hospital until my leg gotbetter. I was very upset and tired and Iknew that hospital would not make mefeel better.
..
.
.
lack of information. Lilly is confused and agitated.
Section One - The Need for Change
Lilly’s Story
Lilly lives in an agedcare facility and herfamily visit her everysecond weekend. Thestaff at the facilitynotice that Lilly’s legulcer is not improvingand she appears to betired, confused andunsteady on her feet.
This is her story.
This is based on a truestory, only names havebeen changed.
Lilly’s Story
7NSW HealthClinical Services Redesign ProgramTransitional Aged Care
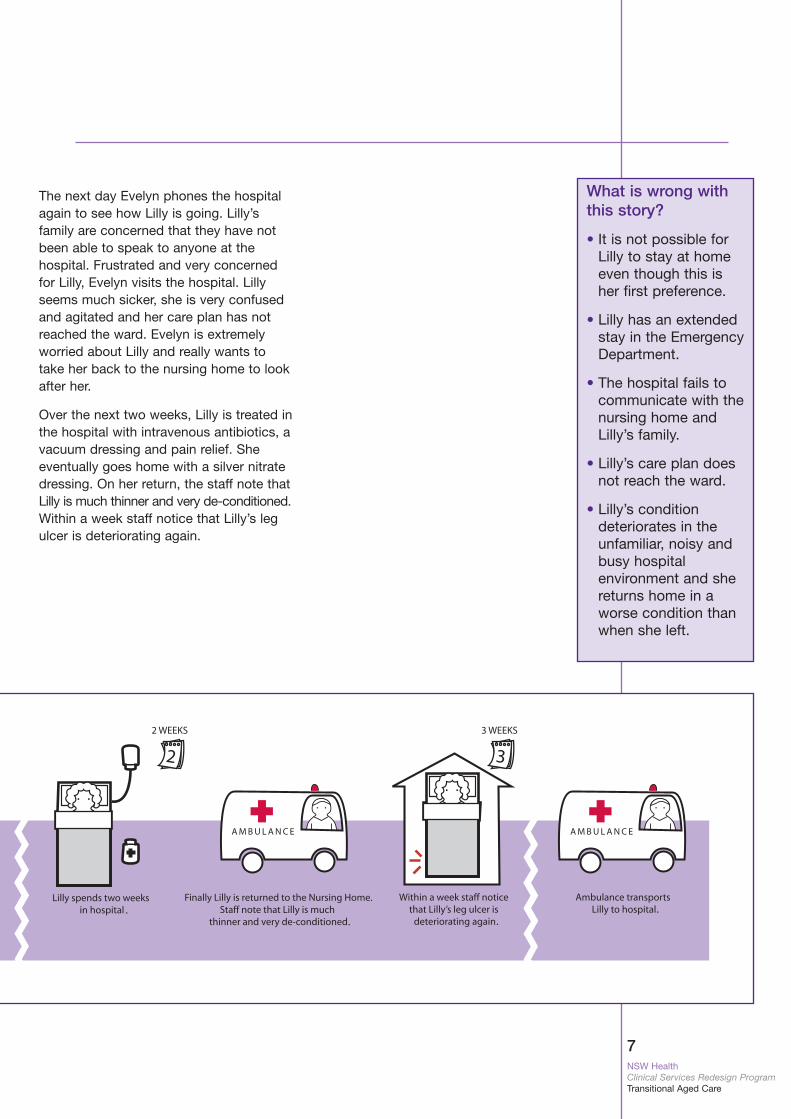
What is wrong withthis story?
• It is not possible forLilly to stay at homeeven though this isher first preference.
• Lilly has an extendedstay in the EmergencyDepartment.
• The hospital fails tocommunicate with thenursing home andLilly’s family.
• Lilly’s care plan doesnot reach the ward.
• Lilly’s condition deteriorates in theunfamiliar, noisy andbusy hospital environment and shereturns home in aworse condition thanwhen she left.
The next day Evelyn phones the hospitalagain to see how Lilly is going. Lilly’sfamily are concerned that they have notbeen able to speak to anyone at thehospital. Frustrated and very concernedfor Lilly, Evelyn visits the hospital. Lillyseems much sicker, she is very confusedand agitated and her care plan has notreached the ward. Evelyn is extremelyworried about Lilly and really wants totake her back to the nursing home to lookafter her.
Over the next two weeks, Lilly is treated inthe hospital with intravenous antibiotics, avacuum dressing and pain relief. Sheeventually goes home with a silver nitratedressing. On her return, the staff note thatLilly is much thinner and very de-conditioned.Within a week staff notice that Lilly’s legulcer is deteriorating again.
.. .
.
8NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
Background to the Model
The population is ageing and older people, including thosefrom aged carefacilites, represent asignificant and increasing proportion ofEmergency Departmentpatients.
Hospital admissions foraged care facility residents are oftenphysically and emotionally disruptive.In hospital, olderpatients have higherrates of adverse eventsand are more likely tobecome deconditioned.
While the benefits ofcaring for residents inan aged care facilityrather than in hospitalare increasingly recognised, these facilities are often challenged to manageacute and sub-acute illness.
The Ageing PopulationThe World Health Organisation statespeople aged over 80 years are the fastestgrowing age group in the western world.
As our population is ageing and patientsand carers are demanding greaterflexibility and choice of services, it isimperative that we improve our models ofaged care to effectively meet the growingdemands and expectations of this agegroup and the wider community.
In NSW, an elderly person presenting atan Emergency Department (ED) is farmore likely to experience a stay of greaterthan eight hours (access block),regardless of their admission status, thanany other age group. Between July 2004and March 2005, 40% of patients aged 65years and over admitted to a NSW publichospital ward or Intensive Care Unitexperienced access block in the EDcompared with only 23% for all other ages.
Hospital admissions for aged care facilityresidents are often physically andemotionally disruptive and fraught with thepotential for iatrogenic illnesses(Ouslander, 1989). Hospitals are busy,noisy, confusing places for elderly people.
Residences and staff, routines, as well asfriends are both familiar and comforting,even more so during a time of illness.Aged care facility staff are familiar withtheir residents and able to notice subtlechanges in their health and wellbeing.
Inappropriate transfers to hospital arepotentially a large problem for aged carefacilities. A study carried out in the UnitedStates (Saliba, 2000) has shown thatstructured review can help reduceinappropriate transfer.
There is evidence that treating residents intheir nursing home or hostel improvespatient outcomes (Ackerman aet. al.,1998). Elderly patients who are treated athome do not have to change theirenvironment or routine and do not need toadapt to the sociological culture of thehospital.
Once hospitalised, older people havehigher rates of adverse events (falls,medication errors, infections andulcerations) and are more likely to becomede-conditioned.
A study of nursing home residents in theUnited States (Zimmer et al., 1997) hasfound that patients treated in the nursinghome or hostel, experienced less confusionand other geriatric complications and haddecreased mortality during the acutephase or in the two months following theacute episode, compared with thosetreated in hospital. McCusker et al. (2001)showed that ED screening, standardisednursing assessment and referral toprimary and home care services cansignificantly reduce the rate of subsequentfunctional decline in older people.
While the benefits of caring for residentsin an aged care facility rather than inhospital are increasingly recognised, thereality is that most aged care facilities donot have on-site physicians or the readyavailability of diagnostic and therapeuticservices. Factors such as rapidly changingtechnology, limited availability of hospitalsupport and the ageing nursing workforcemakes it difficult for aged care facilities tomanage acute and sub-acute illness.
9NSW HealthClinical Services Redesign ProgramTransitional Aged Care
HKHS is a major metropolitan hospital inSydney’s north serving more than 250,000people.
Population projections indicate that in2006 there will be more than 20,000residents aged over 75 years in thehospital’s catchment area. Patients over70 years of age already occupy 70% ofthe bed days (2002 data).
In 2003/04 patients admitted to HKHSfrom aged care facilities accounted for:
• approximately 11,000 bed days (30 beds)
• approximately 10% of acute admissionsand 19% of acute hospital bed days
• 9,630 Emergency Department bed daysor 26 beds.
In 2003/04 patients admitted to HKHS from:
• nursing homes had an average length ofstay (LOS) of six days
• other aged care facilities (hostels) had aLOS of seven days.
Despite the introduction of innovative careprograms at the hospital and in thecommunity, more had to be done toaddress the above issues.
A 2004 survey of local aged care facilitiesby the Hornsby Ku-ring-gai Ryde Divisionof General Practice identified that staffwere very supportive of initiatives toreduce hospital admission for residentsand, where hospitalisation was required,stays should be as short as possible. Staffalso felt enhanced communication andcloser relationships with HKHS and localarea general practitioners would reduceproblems like the discharge of residentsfrom hospital at difficult times such as lateafternoon/evening.
Hornsby Ku-ring-gai Health Service
GRACE began operation at HKHS inAugust 2005.
It developed out ofrecognition of theincreasing needs of theageing population andthe desire to improvecare for those people living in aged care facilities.
5.30 amVera, a resident in a nursing home, istaken to hospital by ambulance afterbecoming unwell.
6 amThe Emergency Department isexperiencing very high demand forservices. There are several significanttrauma cases. Vera waits on a trolleyto be transferred from the ambulanceto the Emergency Department.
11 amVera is transferred to an EmergencyDepartment Bay where she waits formedical assessment.
NoonVera is assessed. An x-ray andpathology is ordered. Vera isbecoming increasingly uncomfortableand disoriented.
2 pmVera has the tests.
4 pmVera’s tests are reviewed. She has aurinary tract infection. An ambulanceis ordered to take Vera home.
5 pmFreda is one of two registered nursesworking at the nursing home. She isabout to go home late, aftercompleting a nine hour shift, when shegets a call from the hospital. They aredischarging Vera.
5.30 pmFreda calls home. She has peoplecoming for dinner at 6pm.
6 pmVera arrives at the nursing homewithout medication or a script.
7.30 pmFreda drives to Vera’s GP to obtain ascript and drives to a pharmacy to fill it.
8.30 pmFreda administers the medication. Theenrolled nurses do not have authorityto do so.
9 pmFreda arrives home to her dinner guests.
A familiar story?

10NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
Lilly’s Story Under GRACE
Lilly is a resident of a nursing home. Shereturned home yesterday after a two weekhospital stay for her leg ulcer.
The general practitioner reviews Lilly andis concerned that she may need to goback into hospital. He and the aged carefacility Director of Nursing agree toexplore the option of GRACE to try andavoid hospital admission. The Director ofNursing contacts the GRACE CNC.
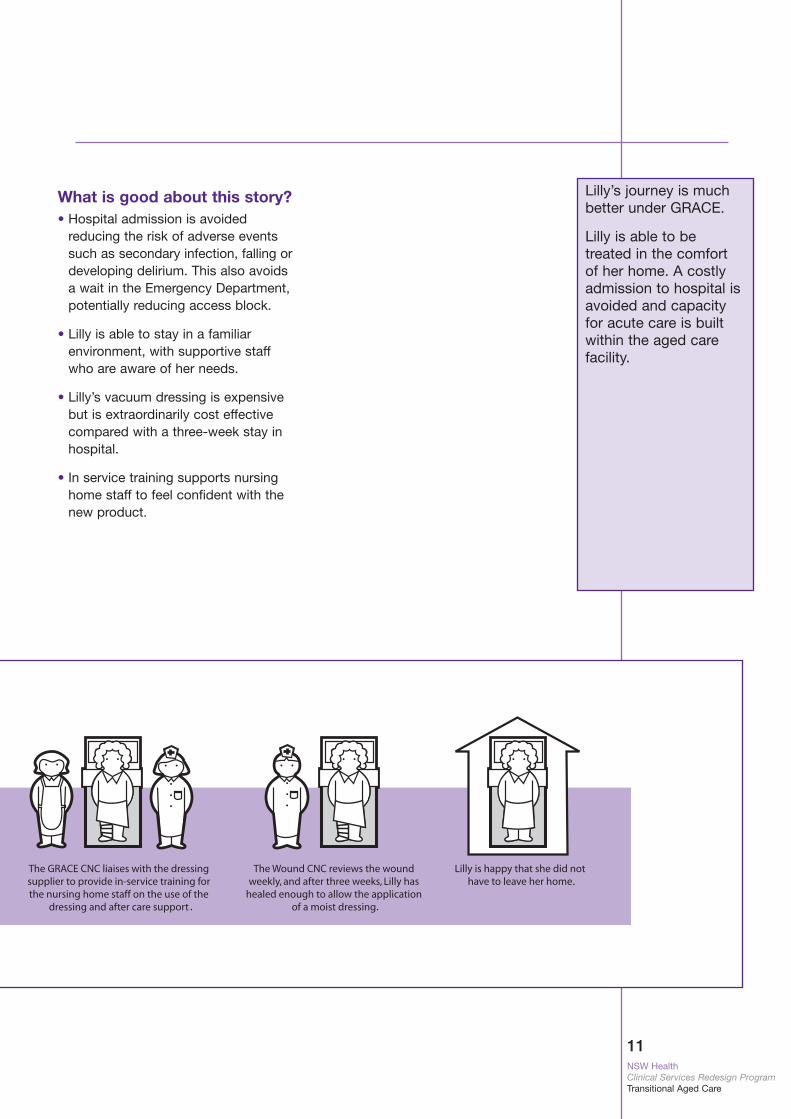
The GRACE CNC completes a TriageAssessment Form with the Director ofNursing over the phone. This assessmenthelps the GRACE CNC to determine sheneeds to refer Lilly to the hospital’s WoundCNC. The Wound CNC visits the nursinghome and quickly establishes that a three-week vacuum dressing is required.
Approval is obtained from the hospital’sDirector of Medical Services to proceedwith treatment. The GRACE CNCorganises the vacuum dressing andsupporting machinery. She liaises with thedressing company representative toprovide in-service training for the nursinghome staff as they have not previouslyused this type of equipment. Thecompany representative agrees to be aresource to assist in managing the use ofthe new equipment for the vacuumdressing.
The Wound CNC reviews the woundweekly. The GRACE CNC and other staffare available seven days a week if thenursing home staff have any concernsabout Lilly’s progress. Within three weeksLilly’s wound has healed sufficiently toapply a moist dressing.
Lilly’s new story
Lilly is back in her nursing home afterbeing in hospital fortwo weeks with aninfected leg ulcer. Thenursing home staffnotice that her legulcer is deteriorating.
This is her story underGRACE.
Section Two - Rapid Evaluation and Acute Care for Aged Care Residents (GRACE)
. ..
Lilly’s new Story
11NSW HealthClinical Services Redesign ProgramTransitional Aged Care
Lilly’s journey is muchbetter under GRACE.
Lilly is able to be treated in the comfortof her home. A costlyadmission to hospital isavoided and capacityfor acute care is builtwithin the aged carefacility.
What is good about this story?• Hospital admission is avoided
reducing the risk of adverse eventssuch as secondary infection, falling ordeveloping delirium. This also avoidsa wait in the Emergency Department,potentially reducing access block.
• Lilly is able to stay in a familiarenvironment, with supportive staffwho are aware of her needs.
• Lilly’s vacuum dressing is expensivebut is extraordinarily cost effectivecompared with a three-week stay inhospital.
• In service training supports nursinghome staff to feel confident with thenew product.
. .
.
12NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
What is GRACE?
What is GRACE?
Under GRACE hospitalstaff work in collaboration with general practitionersand aged care facilitystaff to provideenhanced care “athome” for aged carefacility residents. Thereis provision of hospitalresources not traditionally available toaged care facilities.
When hospital admission is necessary,GRACE patients aregiven access to rapid treatment to ensuretheir hospital stay is asshort as possible.
GRACE Aims
• To reduce hospital access block by supporting generalpractitioners and aged care facilities with enhanced hospitalresources to provide care “at home”. This avoids anunnecessary hospital admission (pre-hospital).
• To reduce the Average Length of Stay (ALOS) of aged carefacility residents in the ED and the hospital.
• To collaborate with the general practitioners and aged carefacilities to develop a model of care that:
- provides a decision support system
- provides hospital resources to assist with assessment andcare provision
- provides coordinated management plans.
• Increase the profile and uptake of Advance Care Directives inaged care facilities.
13NSW HealthClinical Services Redesign ProgramTransitional Aged Care
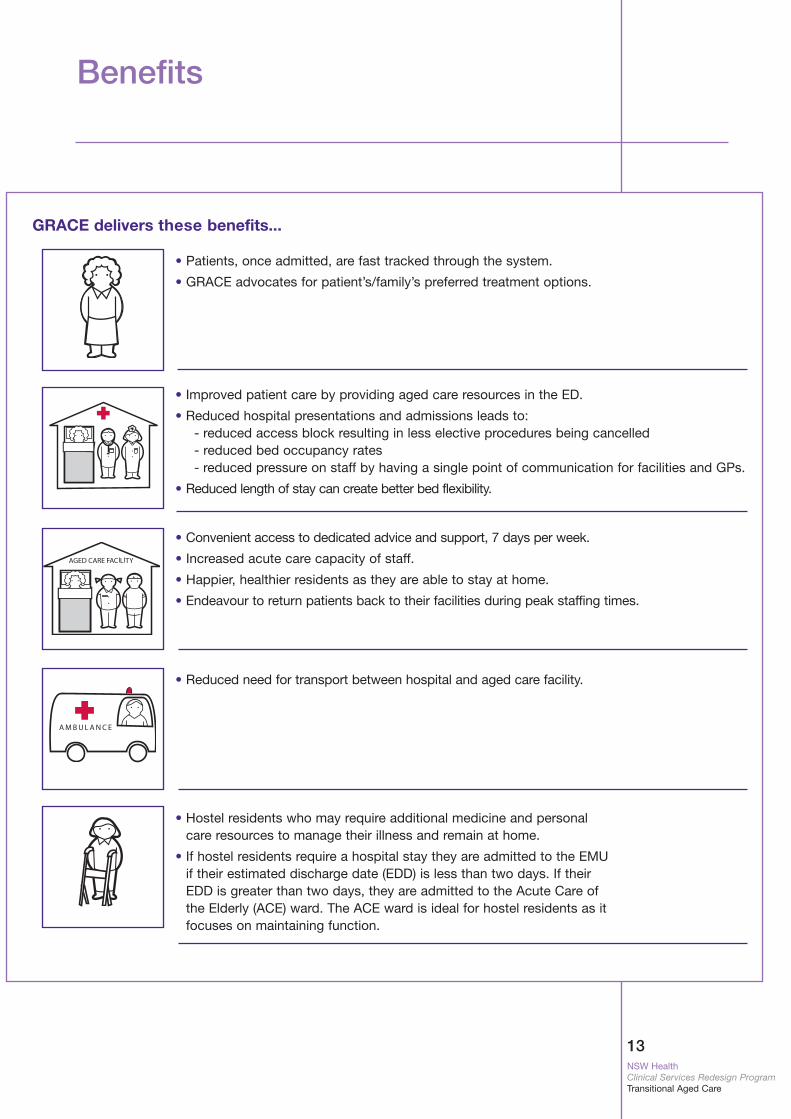
GRACE delivers these benefits...
• Patients, once admitted, are fast tracked through the system.
• GRACE advocates for patient’s/family’s preferred treatment options.
• Improved patient care by providing aged care resources in the ED.
• Reduced hospital presentations and admissions leads to:- reduced access block resulting in less elective procedures being cancelled- reduced bed occupancy rates- reduced pressure on staff by having a single point of communication for facilities and GPs.
• Reduced length of stay can create better bed flexibility.
• Convenient access to dedicated advice and support, 7 days per week.
• Increased acute care capacity of staff.
• Happier, healthier residents as they are able to stay at home.
• Endeavour to return patients back to their facilities during peak staffing times.
• Reduced need for transport between hospital and aged care facility.
• Hostel residents who may require additional medicine and personalcare resources to manage their illness and remain at home.
• If hostel residents require a hospital stay they are admitted to the EMUif their estimated discharge date (EDD) is less than two days. If theirEDD is greater than two days, they are admitted to the Acute Care ofthe Elderly (ACE) ward. The ACE ward is ideal for hostel residents as itfocuses on maintaining function.
Benefits
14NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
staff staff
staff
.
.
.
.
.
.
.
.
.
.
.
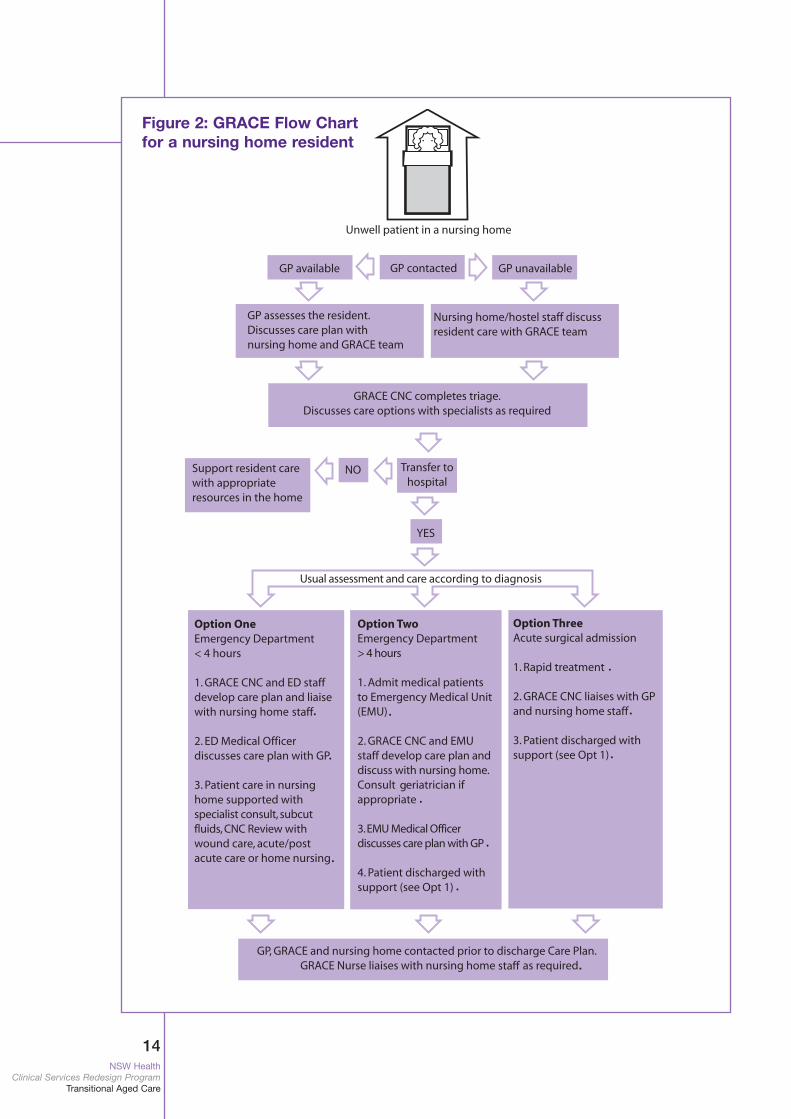
Figure 2: GRACE Flow Chartfor a nursing home resident
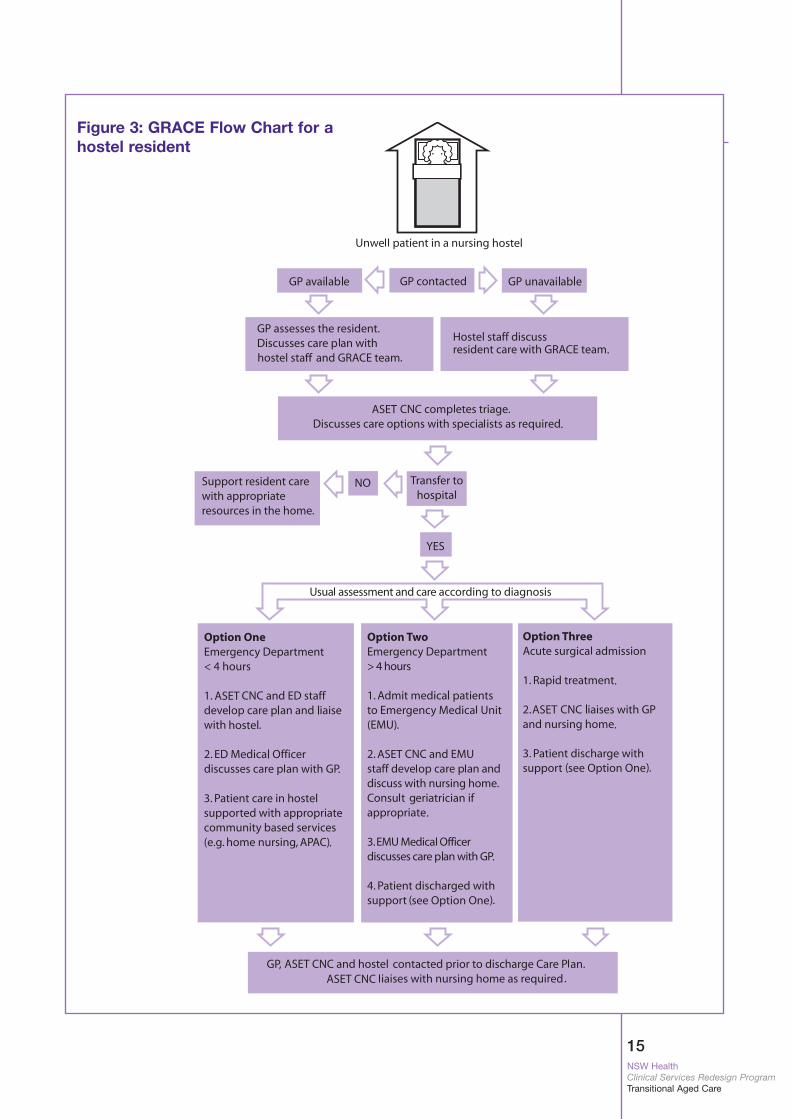
15NSW HealthClinical Services Redesign ProgramTransitional Aged Care
g
16NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
How Does GRACE Work?
Aged care facilities and GPs caring fortheir residents have a single entry pointfor advice and hospital services.
They are able to access hospitalservices that are usually only availableto in-patients. These can includediagnostic specialist medical review aswell as clinical nurse consultant review.
Telephone triage service Rapid treatment
Emergency Department medical staffreview the patient in collaboration withthe treating team with geriatriciansupport as required. The GRACE team,along with the GP, follows up any healthconcerns that aged care facility staffmay have expressed about the patient.
Comprehensive treatment of underlying health issues
When Emergency Departmentpresentations are required the acutecare patients are fast tracked throughthe Emergency Department. If admittedtheir stay is kept as short as possible toreduce the risk of adverse events suchas pressure areas and delirium.
The GRACE CNC and other nursingstaff offer support that includeseducation sessions at aged carefacilities on the use of new equipment,infection control and wound care.
This cost effective support to thefacilities has reduced EmergencyDepartment presentations as well asaverage length of stay for aged carefacility residents at HKHS.
Visits to residential aged care facilities
GRACE CNC inaction
The GRACE Team iscontacted by an agedcare facility about apatient.
• Uses triage checklist toidentify the presentingproblem and the natureof the illness.
• In collaboration withaged care facility staff,and the GP, determinesthe action required.
• Liaises with hospital orcommunity based nursing personnel toassist with specialisedfunctions. Eg, the GRACE team may referpatient to the hospital’s WoundCare CNC. Alternatively, theymay visit the facility andprovide demonstrations andassistance with subcutaneousfluid packs or the use of a newvacuum dressing system.
• Makes targeted referrals to specialistservices such as geriatricians or external serviceproviders.
• Liaises directly withthe patient’s GP andfamily to discuss treatment plans.
• In consultation withthe GP, GRACE maysupply someconsumables such asfluids or silver basedwound dressings toprevent hospitaladmission.
17NSW HealthClinical Services Redesign ProgramTransitional Aged Care
Comprehensivetreatment
A nursing home resident with a historyof dementia presentswith delirium, low albumin levels andfever. It is quicklyestablished that a urinary tract infection ispresent and IV antibiotics are administered.
The aged care facilityDirector of Nursing orthe nurse in chargerequests that theGRACE team investigate the patient’sdietary needs as thepatient’s swallowingability and physical condition has recentlydeteriorated.
A Dietitian visits thepatient during her two-day stay and anew dietary regime isestablished. Thepatient’s delirium isresolved with theantibiotic therapy andshe is discharged homewith oral antibiotics andhigh protein thickenedfluids.
Dedicated GRACE short stay beds
The GRACE CNC actively works toincrease the profile and use of advancecare planning within aged carefacilities.
GRACE can discuss palliative caretreatment options and support generalpractitioners with linkages to outreachpalliative care services. This reducesthe number of aged care facilityresidents transferring to hospital forend of life care.
The GRACE CNC should also workwith the Divisions of General Practiceto identify needs of local GPs andsupport their applications for palliativecare funding grants.
HKHS has targeted that at the end ofone year, 10% of GRACE patients willhave Advance Care Directives/Planningin place.
Advance care planning
Takes responsibility for the telephonetriage service and case manages allGRACE patients.
Ensures specialist, holistic, care isprovided to the patient and that agedcare facilities and the patient’s GPhave a clear and consistent channel ofcommunication.
Provides outreach advice, support andtraining to aged care facilities.
Works in partnership with other staffparticularly the Agedcare Services inEmergency Team (ASET) CNC andAged Care Liaison Nurse.
GRACE CNC
Dedicated GRACE beds in the EMU havemodified criteria that allow for a short stayover the normal 48 hours.
The GRACE CNC, with assistance from theGRACE registrar, case manages the shortstay beds in the EMU to ensurecomprehensive care is provided within thecontext of a short stay admission.
Four beds in HKHS EMU have beenassigned as ‘GRACE’ beds.
18NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
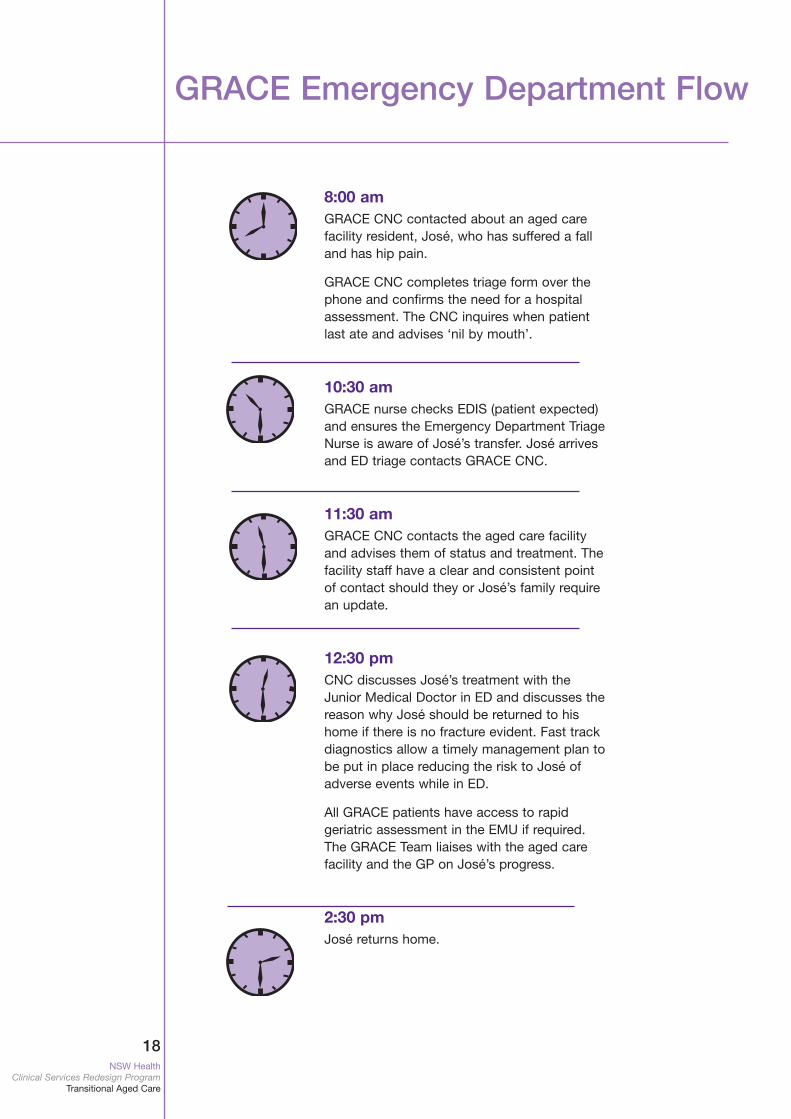
GRACE Emergency Department Flow
8:00 amGRACE CNC contacted about an aged carefacility resident, José, who has suffered a falland has hip pain.
GRACE CNC completes triage form over thephone and confirms the need for a hospitalassessment. The CNC inquires when patientlast ate and advises ‘nil by mouth’.
10:30 amGRACE nurse checks EDIS (patient expected)and ensures the Emergency Department TriageNurse is aware of José’s transfer. José arrivesand ED triage contacts GRACE CNC.
11:30 amGRACE CNC contacts the aged care facilityand advises them of status and treatment. Thefacility staff have a clear and consistent pointof contact should they or José’s family requirean update.
12:30 pmCNC discusses José’s treatment with theJunior Medical Doctor in ED and discusses thereason why José should be returned to hishome if there is no fracture evident. Fast trackdiagnostics allow a timely management plan tobe put in place reducing the risk to José ofadverse events while in ED.
All GRACE patients have access to rapidgeriatric assessment in the EMU if required.The GRACE Team liaises with the aged carefacility and the GP on José’s progress.
2:30 pmJosé returns home.
19NSW HealthClinical Services Redesign ProgramTransitional Aged Care
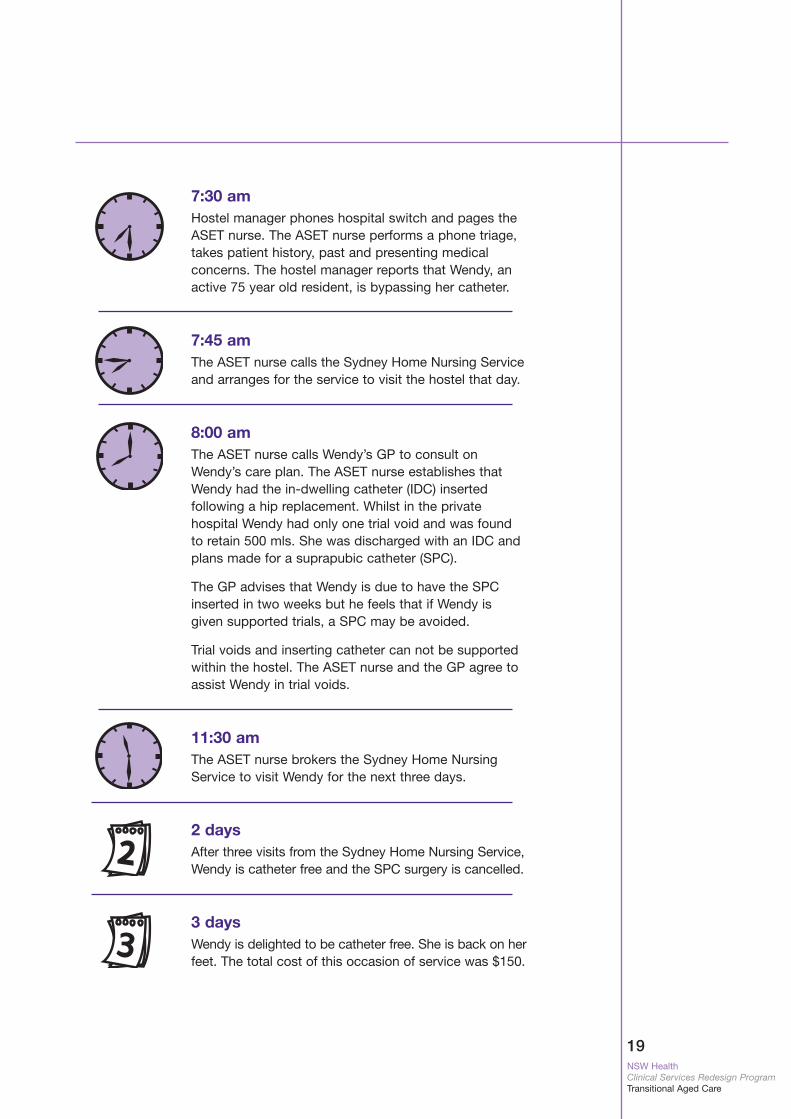
7:30 amHostel manager phones hospital switch and pages theASET nurse. The ASET nurse performs a phone triage,takes patient history, past and presenting medicalconcerns. The hostel manager reports that Wendy, anactive 75 year old resident, is bypassing her catheter.
7:45 amThe ASET nurse calls the Sydney Home Nursing Serviceand arranges for the service to visit the hostel that day.
8:00 amThe ASET nurse calls Wendy’s GP to consult onWendy’s care plan. The ASET nurse establishes thatWendy had the in-dwelling catheter (IDC) insertedfollowing a hip replacement. Whilst in the privatehospital Wendy had only one trial void and was foundto retain 500 mls. She was discharged with an IDC andplans made for a suprapubic catheter (SPC).
The GP advises that Wendy is due to have the SPCinserted in two weeks but he feels that if Wendy isgiven supported trials, a SPC may be avoided.
Trial voids and inserting catheter can not be supportedwithin the hostel. The ASET nurse and the GP agree toassist Wendy in trial voids.
11:30 amThe ASET nurse brokers the Sydney Home NursingService to visit Wendy for the next three days.
2 daysAfter three visits from the Sydney Home Nursing Service,Wendy is catheter free and the SPC surgery is cancelled.
3 daysWendy is delighted to be catheter free. She is back on herfeet. The total cost of this occasion of service was $150.
20NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
GRACE Success Stories
Josie, the Director of Nursing at Pinedale,a local nursing home, phones the GRACECNC to advise she has six nursing homeresidents and seven hostel residents withgastroenteritis. Many of these 13 residentsare starting to show signs of dehydrationand have the potential to present at theED.
After discussion with the EmergencyDepartment physician it is agreed that theprovision of subcutaneous fluids at thenursing home would assist both thenursing home and the hospital toeffectively manage the outbreak. TheGRACE CNC and another registered nursetake 13 three-day subcutaneous fluidpacks to Pinedale.
At Pinedale, the CNC discusses infectioncontrol and subcutaneous fluid pack usewith the registered and enrolled nurses.The nurses are then able to provide in-service training to other staff. The Directorof Nursing also contacts each resident’sgeneral practitioner to inform them of thecare plan that has been established fortheir patient. Pinedale staff use half of thesubcutaneous packs for the patients whoare dehydrated.
None of the Pinedale residents requirehospitalisation. As a result, the chance ofadverse events such as falls, medicationerrors, and the development of pressureareas is reduced.
These are true storiesthat show how GRACEcan provide better carefor older patients in thehome, avoiding theneed for Ambulancetravel, treatment at anEmergency Departmentand hospitalisation.
What’s good aboutthese stories?
• Residents are caredfor in the comfort oftheir home ratherthan coming to hospital.
• The capacity of theaged care facility staffis enhanced.
• Access block isreduced.
Betty is a 76 year old nursing home resident.
Staff notice Betty has a blockedPEG tube.
The GRACE CNC gives adviceover the phone which allowsnursing home staff to unblockthe PEG tube.
Hospital admission is avoidedand Betty remains comfortable athome.
Van is a 90 year old womanin a nursing home.
She has a left CVA, and isaphasic with intermittentwheezing. She hasn’t passedurine for 17 hours.
The GP wants to treat her at herhome but Van’s daughter wantsher mum to be treated in hospital.
The GRACE CNC telephonesVan’s daughter and discussestreatment choices.
With input from GRACE Van istreated at the nursing home.
Franco is an 89 year old nursing home resident withcellulitis.
He is admitted to hospitalovernight, returning to the nursinghome with an IV in-situ for twicedaily antibiotics.
The GRACE CNC arranges for theCommunity Acute and Post AcuteCare team to assist with themanagement of the IV antibiotics.
GRACE sends a medication sheetand the required amount ofantibiotics with Franco’sdischarge letter to the nursinghome and Franco is able tocontinue to be treated at home.
GRACE avoids 13 Emergency Department presentations

21NSW HealthClinical Services Redesign ProgramTransitional Aged Care
2005 2006
Source: Hornsby Ku-ring-gai Health Service
Graph 2 shows theeffectiveness of theGRACE project in maintaining residents intheir facility. SinceAugust 2005 the number of GRACEpatients who haveavoided presentationhas risen from twopatients per month toten patients per monthin January 2006.
Before GRACE wasimplemented aged carefacility residents had anaverage length of stayof six days. GRACE hashelped to reduce lengthof stay, freeing up beddays. (See Toolkit forother performance indicators showing thesuccess of GRACE).
Graph 2: GRACE - ED Avoidable Presentations by Month
No.
of
pat
ient
s
Louise is a 83 year old hostelresident.
Louise has COPD and becameincreasingly breathless throughthe night. After a GP visit it isdetermined that Louise needs IVantibiotics.
The hostel manager calls theASET CNC, who arranges for theAPAC service to visit the hosteland deliver a care plan. TheAPAC team liaises with Louise’sGP and respiratory physician.
After seven days of regularantibiotics injections,physiotherapy and social workvisits, Louise is back on her feet.
22NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
Establishing and Maintaining GRACE
Partnerships between thehospital, residential aged carefacilities and general practitionersare essential.
Visit each aged care facility andGP Division meetings to explainGRACE.
Find clinical, senior management,and nursing champions in thehospital and ED that will assiststaff to work collaboratively. LocalGP and aged care facilitychampions like directors ofnursing are also critical.
Establish Steering Committee.(See Toolkit for more information.)
A project officer can pull peopletogether, document, plan, monitor,report on targets and “put the legson the ideas”.
Create a project plan that staff own.Involve them in the development butdon’t make it hard or timeconsuming. The plan should set out:• the burning platform for change -
evidence about the current patientjourney problems
• the vision and ideal patient journey• objectives and strategies• roles and responsibilities• baseline data and key performance
indicators.
Set firm but realistic timeframes forimplementation and stick to them.Allow time for obtaining staffsupport, orientation to processmapping, developing the model ofcare as well as documenting KPIsand baseline data.
Key performance indicators needto be developed and strictlymonitored. These may include:• hospital admissions avoided• reduced length of stay in hospital
and ED• reduced access block• increased patient, hospital staff,
aged care facility, and GPsatisfaction
• decreased adverse events.
Talk up the need for changeacross all facets of the hospital,aged care facilities and amongGPs. Create a folder of evidencethat can be reviewed at any time.Describe the current patientjourney.
Take the time to educate andinform people, particularly the keyopinion leaders and the ‘naysayers’, about the benefits to thepatient, aged care facility,ambulance service and hospitalof caring for residents ‘in thehome’.
23NSW HealthClinical Services Redesign ProgramTransitional Aged Care
Define key GRACE teammembers*.
Appoint a GRACE CNC and basethem in or near the ED.
Interdisciplinary team work isessential.
Continue visits to aged carefacilities and GPs.
Hold regular team meetings andreview individual patient journeys.
* see section on Staffing.
This is a critical role for the ProjectOfficer/Steering Committee/CNC.
Foster good communication throughinformal and formal means. • Produce information sheets,
newsletters and presentations forgeneral practitioners, thecommunity, patients and theirfamilies, hospital and aged carefacility staff.
• Informal sessions over coffee cancreate the incentive for people totake time from their busyschedules to listen in a non-threatening and collaborativemanner.
• Establish methods for rapidfeedback from patients and staff inaddition to patient surveys.Respond directly to feedback.
Celebrate and communicate everytangible achievement of the projectthrough a variety of means includingmorning teas, awards, mentions atstaff meetings.
Nominate your model, championsand teams for internal and externalawards.
Steering Committee and GRACEproject team review initial dataresults, including results ofpatient, hospital staff, GP andaged care facility surveys.
Refine model as required.
24NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
These estimates are for the establishmentof GRACE within a metropolitan generalhospital. They also take into account theneed for enhanced collaborativerelationships between GRACE and otherclinical, nursing, community health andadministrative staff.
• 1.0 FTE GRACE CNC.
• 0.5 FTE Geriatric Registrar. At HKHS afull time Geriatric Registrar has beenemployed to build capacity within theorganisation. A key role of the registrarat HKHS will be to spend time with theGRACE project and the AgedcareServices in Emergency Team.
• 0.5 FTE Project Officer (Clinical NurseConsultant).
• An Agedcare Services in EmergencyTeam to assess and quickly identifyelderly patients, provide support to theGRACE CNC and enhance the ability ofthe hospital to provide a seven day aweek service to the aged care facilities.
• A staffing profile in the EmergencyMedical Unit that allows additionalnursing care for elderly patients.
Staffing
Agedcare Services inEmergency Team (ASET)The ASET assesses elderly patientsand provides rapid identification ofthose whose journey will beenhanced by GRACE. Duringweekends, the ASET and GRACECNC roles can combine to providea comprehensive and extendedservice to aged care facilities.
Emergency Department nursesThe GRACE project has also increased thecapacity of Emergency Department nursesby cultivating aged care skills in interestednurses. At HKHS, five ED nurses havecompleted the GRACE/ASET preceptership.These nurses now have an increasedawareness of aged care issues andcommunity resources, which in turn assistswith discharge planning. In the ED, theGRACE and ASET nurses prioritise theirpatients. When the GRACE/ASETpresentations are low these nurses assistthe ED staff, allowing full utilisation of theirtime. After hours the GRACE and ASETteams combine.
Community NursingService and CommunityAcute/Post Care Team The Community Nursing Serviceand the Community Acute/PostCare Team provide expertmultidisciplinary care to patientswith complex needs once theyhave been discharged home toan aged care facility.
Registered and enrolled nursesAt HKHS, the Nurse Unit Manager of theEmergency Medical Unit altered thestaffing profile to increase the numbers ofenrolled nurses to look after GRACEpatients. Aged care facility residents oftenhave eating difficulties and, because oftheir frailty, require regular repositioning ina gentle manner to prevent skin tears andpressure areas developing. Many elderlypatients become disorientated to person,time and place in the unfamiliarenvironment of the hospital and mobilisingthem requires additional time and expertiseand therefore additional nursing care.
Aged Care Liaison Nurse(ACLN)If an aged care facility patient isadmitted to the EMU, the ACLN isable to follow up and identifyissues with the patient and has anessential role in ensuring that theyhave a smooth transition back totheir home.
It has also been identified at HKHS that a Geriatric Registrar is required to build capacity within the organisation.
Staffing levels willdepend on the size ofthe hospital and thenumber of aged carefacility residents withinthe hospital catchmentarea.
25NSW HealthClinical Services Redesign ProgramTransitional Aged Care
Resources
Section Three - Resources
Ackerman, R.J. and Kemle, K.A. The Effect of a Physician Assistant on theHospitalisation of Nursing Home Residents. Journal of the American Geriatric Society,1998; 46:610-614.
Boockvar, S., Gruber-Baldini, A.L., Burton, L., Zimmerman, S., May, C. and Magaziner,J. Outcomes of Infection in Nursing Home Residents with and without Early HospitalTransfer. Journal of the American Geriatric Society, 2005; Vol 53:4, 590-596.
Caplan, G.A., Ward, J.A., Brennan, N.J., Coconis, J., Board, N. and Brown, A. Hospitalin the home; a randomised controlled trial. Medical Journal of Australia, 1999; 170:156-160.
Finucane, P.M., Wundke, R., Whitehead, C., Williamson, L. and Baggoley, C.J.Profile ofpeople referred to an emergency medical department from residential care. AustraliaNew Zealand Journal of Medicine,1999; 29:494-499.
McCusker, J., Verdon, J., Tousignant, P., de Courval, L., Dendukuri, N. and Belzile, E.Rapid emergency department intervention for older people reduced risk of functionaldecline: results of a randomized trial. Journal of the American Geriatrics Society 2001;49(10):1272-1281.
Ouslander, J.G. Medical Care in the Nursing Home. Journal of the American MedicalAssociation, 1989; 262:18, 2582-2590.
Saliba, D., Kington, R., Buchanan, J., Bell, R., Wang, M., Lee, M., Herbst, M., Lee, D.,Sur, D. and Rubenstein, L. Appropriateness of the decision to transfer nursing homefacility residents to the hospital. Journal of the American Geriatrics Society, 2000;48(2):154-163.
Zimmer, J.G. Needed: acute care in the nursing home. Patient Care 1993; 27(19):59-62,65-68.
Zimmer, J.G. and Hall, W.J. Nursing Home Acquired Pneumonia: Avoiding the Hospital.Journal of the American Geriatrics Society 1997; 45(3):380-381.
For more informationabout GRACE visit theModels of Care section of the ARCHIwebsite
www.archi.net.au
Here you will find anelectronic copy of thisdocument, a resourcetoolkit and have theopportunity to participate in online discussion groups.
26NSW Health
Clinical Services Redesign ProgramTransitional Aged Care
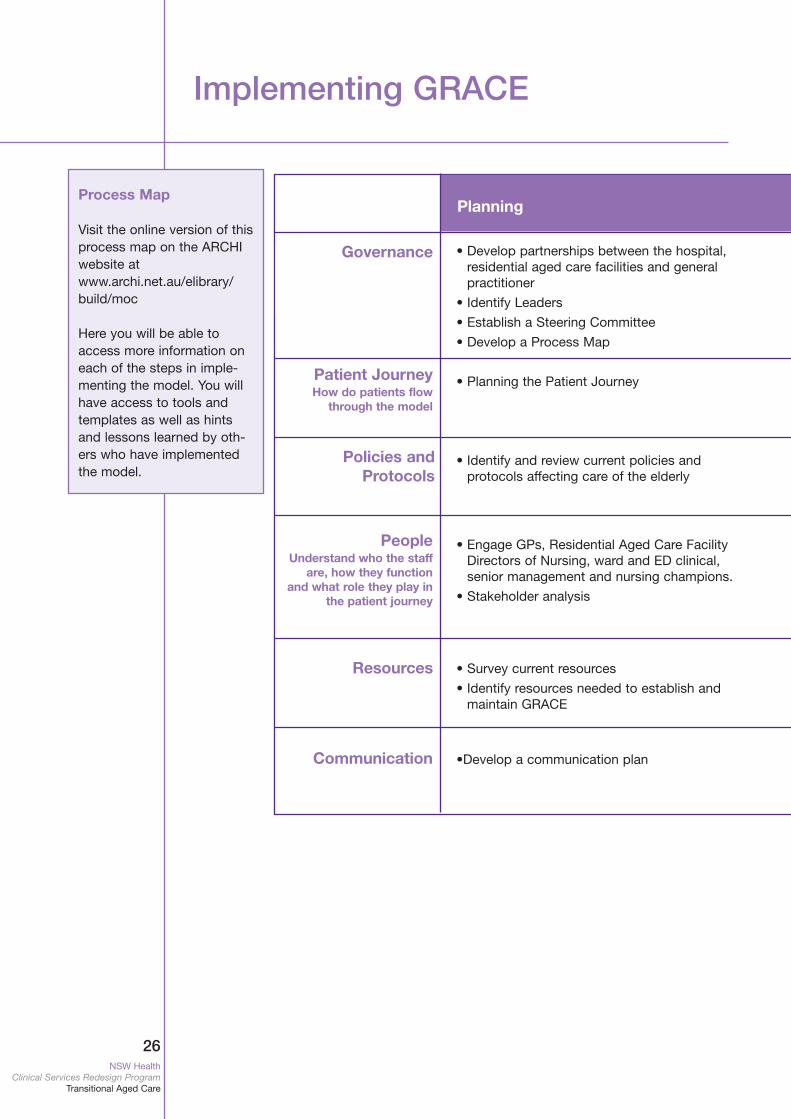
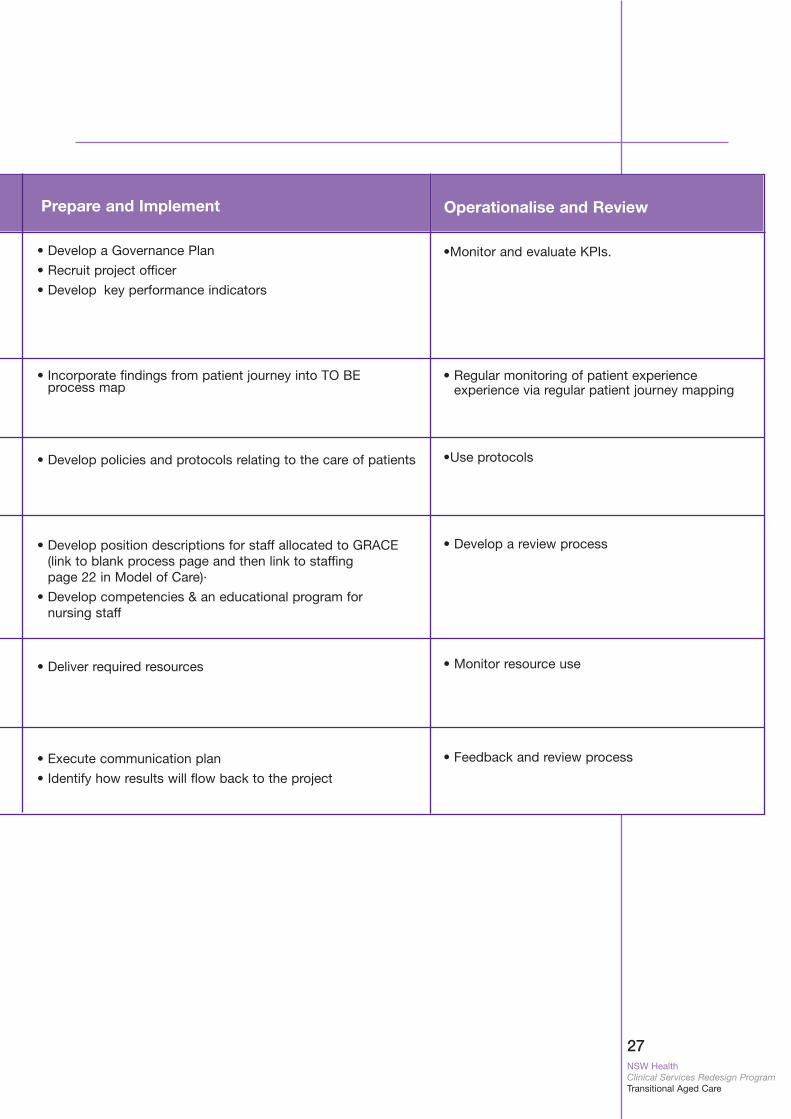
Process Map
Visit the online version of thisprocess map on the ARCHIwebsite atwww.archi.net.au/elibrary/build/moc
Here you will be able toaccess more information oneach of the steps in imple-menting the model. You willhave access to tools andtemplates as well as hintsand lessons learned by oth-ers who have implementedthe model.
Governance • Develop partnerships between the hospital,residential aged care facilities and generalpractitioner
• Identify Leaders
• Establish a Steering Committee
• Develop a Process Map
• Planning the Patient Journey
• Identify and review current policies and protocols affecting care of the elderly
• Engage GPs, Residential Aged Care FacilityDirectors of Nursing, ward and ED clinical, senior management and nursing champions.
• Stakeholder analysis
• Survey current resources
• Identify resources needed to establish and maintain GRACE
•Develop a communication plan
Patient JourneyHow do patients flow
through the model
Policies andProtocols
PeopleUnderstand who the staff
are, how they functionand what role they play in
the patient journey
Resources
Communication
Planning
Implementing GRACE
27NSW HealthClinical Services Redesign ProgramTransitional Aged Care
•Monitor and evaluate KPIs.
• Regular monitoring of patient experience experience via regular patient journey mapping
•Use protocols
• Develop a review process
• Monitor resource use
• Feedback and review process
Prepare and Implement Operationalise and Review
• Develop a Governance Plan
• Recruit project officer
• Develop key performance indicators
• Incorporate findings from patient journey into TO BE process map
• Develop policies and protocols relating to the care of patients
• Develop position descriptions for staff allocated to GRACE (link to blank process page and then link to staffing page 22 in Model of Care)·
• Develop competencies & an educational program for nursing staff
• Deliver required resources
• Execute communication plan
• Identify how results will flow back to the project






























