Embed Size (px)
Citation preview

Guidance for the Safeguarding Process Prior
To and Immediately After The Birth Of A Baby
Where There May Be Risks of Significant Harm
January 2016

January 2016 1 | P a g e
Contents Page
1. Introduction 2
2. Purpose of the guidance 2
3. Target Audience 2
4. Equality, Human Rights and Disability
Discrimination Act 2
5. Alternative Formats 3
Sources of Advice in relation to this guidance 3
7. The Pre-Birth Referral Pathway 3
8. The Pre-Birth Assessment and Planning Process 4
9. The Pre Birth Planning Meeting 6
10. Completion of the Pre-Birth Risk Assessment &
Pre-Birth Child Protection Report 6
11. The Pre Birth Child Protection Conference 7
12. Actions to be Taken Upon the Birth of the Baby 7
Appendices
Appendix 1: Referral for Expectant Mother 10
Appendix 2: Exemplar of Significant Event 13
Appendix 3: Guidance to Completing a Pre-Birth
Risk Assessment 16
Appendix 4: Pre-Birth Child Protection
Conference Report 29
Figure 1
Pre Birth Assessment Pathway 8

January 2016 2 | P a g e
Regional Guidance for the Safeguarding Process Prior To and Immediately After The Birth
Of A Baby Where There May Be Risks of Significant Harm.
Name Date Reason For Changes Version
Claire Fulton 30.10.13 Original Document 1.0
Claire Fulton 07.11.13 Updates after meeting with Workstream 1 UNOCINI
Development Group 07.11.13
1.1
Claire Fulton 10.06.14 Update after Regional CSI Co-ordinators Meeting 1.2
Claire Fulton 03.07.14 Update after Regional CSI Co-ordinators Meeting
(01.07.14) and Workstream 1 UNOCINI Development
Group (03.07.14)
1.3
Claire Fulton 25.07.14 Update further to additional feedback from Southern
and South Eastern Trusts
1.4
Claire Fulton 05.08.14 Update after Regional CSI Co-ordinators Meeting 1.5
Claire Fulton 03.12.14 Update after CSI Co-ordinators Meeting further to
WHSCT and NHSCT requests 1.6
Claire Fulton 08.01.14 Update after feedback from BHSCT 1.7
Claire Fulton 14.01.14 Update after CSIB Implementation Group Meeting 1.8
Claire Fulton 11.02.14 Revision of referral further to CSIB Implementation
Group Meeting 1.9
Claire Fulton 10.12.15 Revision of guidance following post-implementation
issues being raised. Agreed changes at CSIB
Implementation Group Meeting 09.12.15
2.0
January 2016 3 | P a g e
1.0 Introduction
1.1 A pre-birth assessment is essentially defined as ‘an assessment of the risk to the
future safety of the unborn child with a view to making informed decisions about the
child and family’s future’.
1.2 Research indicates that young babies are particularly vulnerable to abuse but
that work carried out in the ante-natal period can help minimise harm if there is early
assessment, intervention and support. The main purpose of a pre-birth risk
assessment is to identify what the risks to the new born child may be, whether the
parent(s) have the capacity to change so that the risk can be reduced and, if so,
what supports will be required.
2.0 Purpose of the Guidance
2.1 The guidance will provide clarity to staff in relation to the pre-birth risk
assessment pathway, the assessment process and their individual and collective
roles and responsibilities within the process
3.0 Target Audience
3.1 Whilst this guidance has been developed to assist Social Workers in their
recording of safeguarding issues and the ante-natal period, this guidance is also
relevant to those professionals who are involved with families about whom there are
concerns in the antenatal period such as Midwives, Health Visitors, General
Practitioners, Paediatric and Obstetric Medical Staff and Children’s Social Workers.
3.2 The guidance is appropriate for professionals such as those from Adult Mental
Health, or Learning Disability Services or Community Addiction Services who may
be/have been involved with families because of particular needs which the
parent/proposed carer may have.
4.0 Equality, Human Rights and Disability Discrimination Act
4.1 This guidance has been drawn up and reviewed in light of Section 75 of The
Northern Ireland Act (1998) which requires the Trust to have due regard to the need
to promote equality of opportunity. It has been screened to identify any adverse
impact on the 9 equality categories and no significant differential impact was
identified. Therefore an Equality Impact Assessment is not required.

January 2016 4 | P a g e
5.0 Alternative Formats
5.1 This document can be made available on request on disc, larger font, Braille,
audio-cassette and in other minority languages to meet the needs of those who are
not fluent in English.
6.0 Sources of advice in relation to this document
6.1 The Author of the guidance, responsible Assistant Director or Director as detailed
on the title page of the document should be contacted with regard to any queries on
its’ content.
7.0 The Pre-Birth Referral Pathway
7.1 When a safeguarding concern is identified in the ante natal period by any
professional involved with the client/family a referral (Appendix 1) should be made to
the appropriate children’s social work team.
7.2 Referrals about unborn babies should be made by the 18th week of the
pregnancy, unless it has not been possible to meet this timescale, for example,
because the pregnancy has been concealed. Referring at this time:
• Provides sufficient time for a full and informed assessment;
• Avoids initial approaches to parents in the latter stages of pregnancy, as this
is already an emotionally charged time;
• Enables parents to have more time to contribute their own ideas and solutions
to concerns and increases the likelihood of a positive outcome;
• Enables the provision of support services so as to facilitate optimum home
circumstances prior to the birth;
• Provides sufficient time to make adequate plans for the baby's protection,
where this is necessary.
7.3 New referrals (where mother is not known to Social Services) for expectant
mothers should be submitted to the Single Point of Entry (Duty) Gateway Team with
responsibility for the area in which the client resides.

January 2016 5 | P a g e
7.4 The Expectant Mother Referral (Appendix 1) should be used for any mother aged
over 18 years of age. For mothers aged under 18 years, a UNOCINI referral should
be completed instead.
7.5 New referrals received at Single Point of Entry will be passed to the Locality
Gateway Team for completion of an initial assessment.
7.6 If the referrer is aware that social services are already involved with the client/
family in any capacity, for example, Family Intervention Team, Looked After Child
Team, 16 + Team, Young People’s Partnership or the Team for Children with
Disabilities, telephone contact should be made with the case co-ordinator in that
team to discuss the administration of the case. The relevant Social Worker will
record the information shared as a Significant Event (REC 4).
7.7 In circumstances where it is identified that a pre-birth risk assessment should be
commenced and the expectant mother is already known to the Family Intervention
Service or the Looked After Children Service, the pre-birth assessment should be
completed by the current social worker. Onward transfer to another social work
team will be determined by the outcome of the pre-birth assessment and as per the
criteria outlined above. Where it is assessed that on-going social work involvement
is required, case transfer will be progressed where appropriate at the pre-birth case
conference or case planning meeting.
7.8 Where a young person currently receiving support from 16 Plus Service
becomes pregnant and there are child care/ child protection concerns, the
responsible social worker will liaise with the relevant Family Intervention Team and
forward an initial assessment, recorded on a REC4, with recommendations in
respect of the unborn baby.
7.9 This referral is entered as a ‘pre-birth safeguarding concern’ against the mother
and the detail of the referral is captured on a REC4 (Significant Event) within the
mother’s record.

January 2016 6 | P a g e
8.0 The Pre-Birth Assessment and Planning Process
8.1 When a social worker in any social work team receives a referral identifying a
concern in relation to the future care which an ante natal mother may give to either
her unborn child and/or to her new born child, it is a social work responsibility to
undertake an initial assessment. The purpose of this will be to clarify the
information provided at point of referral and to ascertain if threshold of risk is
met. This process will involve engagement with the multi-disciplinary team.
Whilst this initial contact is held within the mother’s record (as she is the only one at
this point that has parental responsibility) it should include any concerns pertaining to
both parents, if known. As a concern in pregnancy is significant, this will be recorded
as a Significant Event (REC 4) and will be completed within 10 working days.
Within this, the Social Worker should include:
An outline of previous Social Work involvement (if applicable)
Any initial information pertaining to early ante-natal care and an expected
date of confinement (EDC) – this allows for robust planning and timescales
Current family relationships
Extended family supports
Brief outline of the risks apparent, if relevant
An exemplar of the Significant Event can be found in Appendix 2.
8.2 For new referrals (no current Social Work involvement) and, if the initial
assessment identifies risk factors as outlined in ACPC Regional Child Protection
Policy and Procedures ref. 6.10, the Social Worker will liaise with the Senior Social
Worker in order to arrange the transfer of the case to the appropriate receiving team,
taking cognisance of Trusts’ transfer processes from Gateway to Family Support and
Intervention.
8.3 This transfer will comprise the Pre-Birth Planning Meeting.
8.4 Note: Where a pregnancy has been concealed and the referral is made post 35
weeks gestation, the procedures cannot be followed due to timescale restraints. The
case should remain with the appropriate team and a proportionate pre-birth risk
assessment, using the format in Appendix 4 should be completed and the case

January 2016 7 | P a g e
progressed pending the outcome of the risk assessment, for example, pre-birth child
protection conference or family support meeting.
9.0 The Pre Birth Planning Meeting
9.1 The meeting will:
Include the parent(s), relevant Team Manager/s and Social Worker/s (as per
Transfer Policy), referrer (if appropriate), Health Visiting, Midwifery, and any
other key professionals.
Parents should be invited, unless there is a valid reason to exclude them.
Identify clearly the causes for concern in terms of the ante natal mother, and
any potential risks for the unborn child and the new born child.
Decide whether or not a full pre-birth risk assessment is required, having
considered the information known alongside the Threshold of Needs.
Decide whether the matter should be referred for a Pre-Birth Child Protection
Conference. The earliest date for this is 24 weeks gestation of the unborn
child.
Identify the specific areas requiring assessment, which professional is
responsible for each aspect and determine the timeframe for the assessment
Establish the date of the next multi-disciplinary meeting.
9.2 Where the meeting decides not to proceed to a full pre-birth risk assessment,
consideration should be given to developing a Pre-Birth Family Support Plan.
10.0 Completion of the Pre Birth Risk Assessment and Pre-Birth Child
Protection Conference Report
10.1 The detail of the pre-birth risk assessment described at Appendix 3 has been
developed from the work of Martin Calder (2008). This should ordinarily take place
between 14 and 24 weeks gestation, however time may be limited if a pregnancy is
concealed. Each professional identified at the Pre-Birth Planning Meeting as needing
to contribute to the assessment will individually collate, record and analyse
information about the aspect of the family for which they have professional expertise.
10.2 The detail of the assessment will be recorded in the Pre-Birth Risk Assessment
Report (Appendix 4) and held against the mother’s record. This risk assessment
report will become the Report for the Family Support meeting or the pre-birth Child
Protection Conference, dependent on its outcome. The domains are not mutually

January 2016 8 | P a g e
exclusive and it will require a high level of effective multi-disciplinary communication,
facilitated by the Case Co-ordinator, to ensure that the maximum amount of
information is available to facilitate the pre-birth planning process. This will ensure
the best outcomes for the child and his parents/ carers.
10.3 The ACPC Regional Policy and Procedures does not provide specific guidance
on when to commence a Pre Birth Risk Assessment but does state that a Pre Birth
Initial Child Protection Case Conference should not be held before 24 weeks
gestation of the unborn child.
11.0 The Pre-Birth Child Protection Conference
11.1 The aim of the Pre-Birth Child Protection Conference is to enable professionals
with particular expertise (even if they are not currently involved with the family),
those most involved with the family, and the family itself to assess all relevant
information and plan how to safeguard the unborn child and promote his or her
welfare. There must be representation from the midwifery services, health visiting
and other professionals as appropriate.
11.2 At this meeting, agreement will be sought regarding the Parental Plan; and the
Proposed Child Protection Plan and the need for agreement regarding categories of
registration, if appropriate, at birth.
11.3 The discussion from the Pre-birth Child Protection Conference will be recorded
at the end of the report, alongside the Parental Plan and Proposed Child Protection
Plan.
12.0 Actions To Be Taken Upon Birth Of The Baby
12.1 Upon the birth of the baby, it is the co-ordinating Social Worker’s responsibility
to enter the child as ‘potential at risk’ referral and ensure registration is updated,
further to the outcome of the Pre-Birth Child Protection Conference.
12.2 It is important to remember to update the child’s religion and ethnicity as this
information is required for quarterly reporting and Corporate Parenting.

January 2016 9 | P a g e
12. 3 The Proposed Child Protection Plan will be used to begin the UNOCINI Child
Protection process.
0 | P a g e
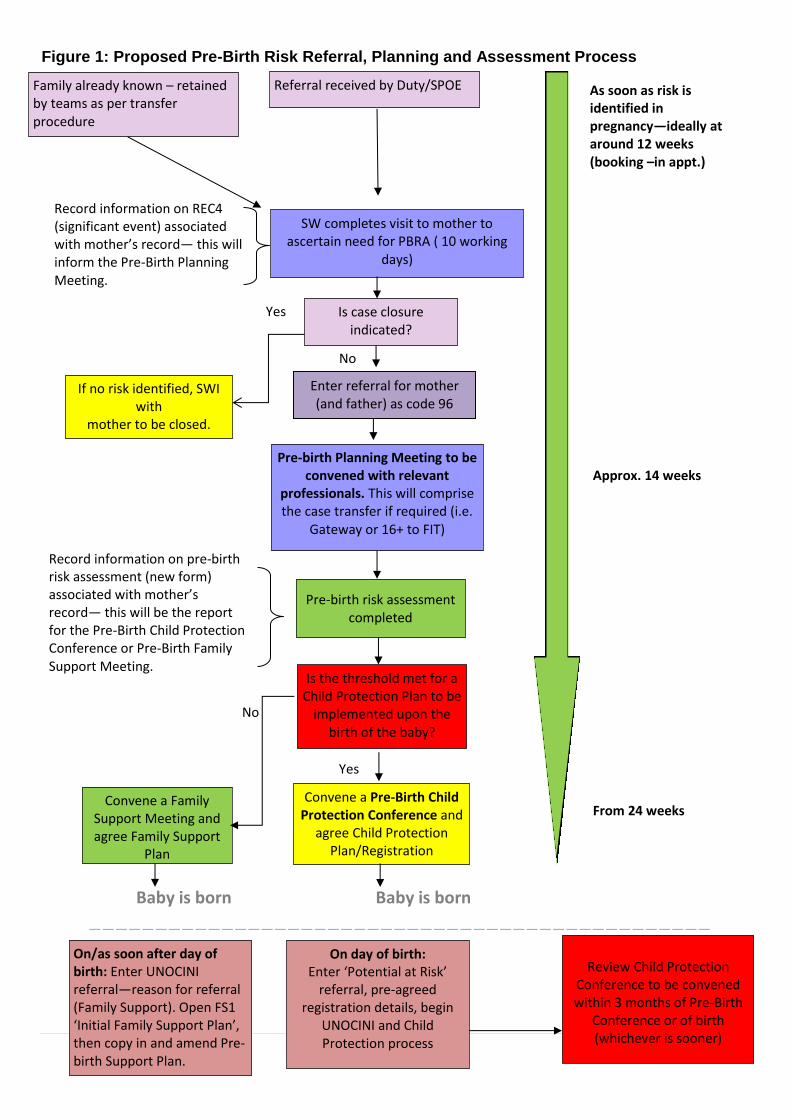
Figure 1: Proposed Pre-Birth Risk Referral, Planning and Assessment Process
Yes
Referral received by Duty/SPOE
Record information on REC4 (significant event) associated with mother’s record— this will inform the Pre-Birth Planning Meeting.
SW completes visit to mother to ascertain need for PBRA ( 10 working
days)
Is case closure indicated?
If no risk identified, SWI with
mother to be closed.
No
Pre-birth Planning Meeting to be convened with relevant
professionals. This will comprise the case transfer if required (i.e.
Gateway or 16+ to FIT)
Pre-birth risk assessment completed
Is the threshold met for a Child Protection Plan to be
implemented upon the birth of the baby?
Convene a Family Support Meeting and agree Family Support
Plan
Convene a Pre-Birth Child Protection Conference and
agree Child Protection Plan/Registration
Categories.
No
On day of birth: Enter ‘Potential at Risk’
referral, pre-agreed registration details, begin
UNOCINI and Child Protection process
Yes
Record information on pre-birth risk assessment (new form) associated with mother’s record— this will be the report for the Pre-Birth Child Protection Conference or Pre-Birth Family Support Meeting.
On/as soon after day of birth: Enter UNOCINI referral—reason for referral (Family Support). Open FS1 ‘Initial Family Support Plan’, then copy in and amend Pre-birth Support Plan.
Review Child Protection
Conference to be convened within 3 months of Pre-Birth
Conference or of birth (whichever is sooner)
Approx. 14 weeks
From 24 weeks
As soon as risk is identified in pregnancy—ideally at around 12 weeks (booking –in appt.)
Baby is born Baby is born
———————————————————————————————————————————————
—————-
Family already known – retained by teams as per transfer procedure
Enter referral for mother (and father) as code 96

9 | P a g e
References
Calder, M.C. (2003) Unborn Children: A Framework for Assessment and Intervention. In:
Calder, M.C. and Hackett, S., eds. Assessment in Child Care Using and Developing
Frameworks for Practice. Dorset: Russell House Publishing
Corner, R. (1997) Pre-Birth Risk Assessment in Child Protection. Social Work
Monographs, Norwich: University of East Anglia
Hart, D. (2010) Assessment Prior to Birth. In: Horwath, J., ed. The Child’s World,
Assessing Children in Need. London: Jessica Kingsley Publishers
http://www.communitycare.co.uk/articles/11/09/2012/118486/how-research-on-pre-birth-
assessments-should-affect-practice.htm

January 2016 10 | P a g e
Expectant Mother Referral
Section 1: Expectant Mothers Details
Surname: EDC (if known):
ID No.
Forename:
Known As: HCN:
Referral Code: 96
Address:
Previous Address:
Postcode:
Telephone No: Previous Postcode:
Mobile No: Locality:
Date of Birth: Gender
GP Name: GP Tel No:
GP Address:
GP Email Address:
GP Postcode:
Does the Expectant
mother have a Disability?
If Yes, What Disability:
(& source of diagnosis)
Other Special Needs:
Nationality: Ethnic Origin:
Religion: Country of Origin:
Language Spoken:
Communication
Support:
Interpreter Signer Document Translator

January 2016 11 | P a g e
Section 2a: Referrer’s Details
Name of Referrer: Designation:
Address:
Date of Referral:
Postcode: Contact Details:
Section 2b: Reason for Referral
Section 2c: Immediate Actions
Are Immediate /Actions necessary?
January 2016 12 | P a g e
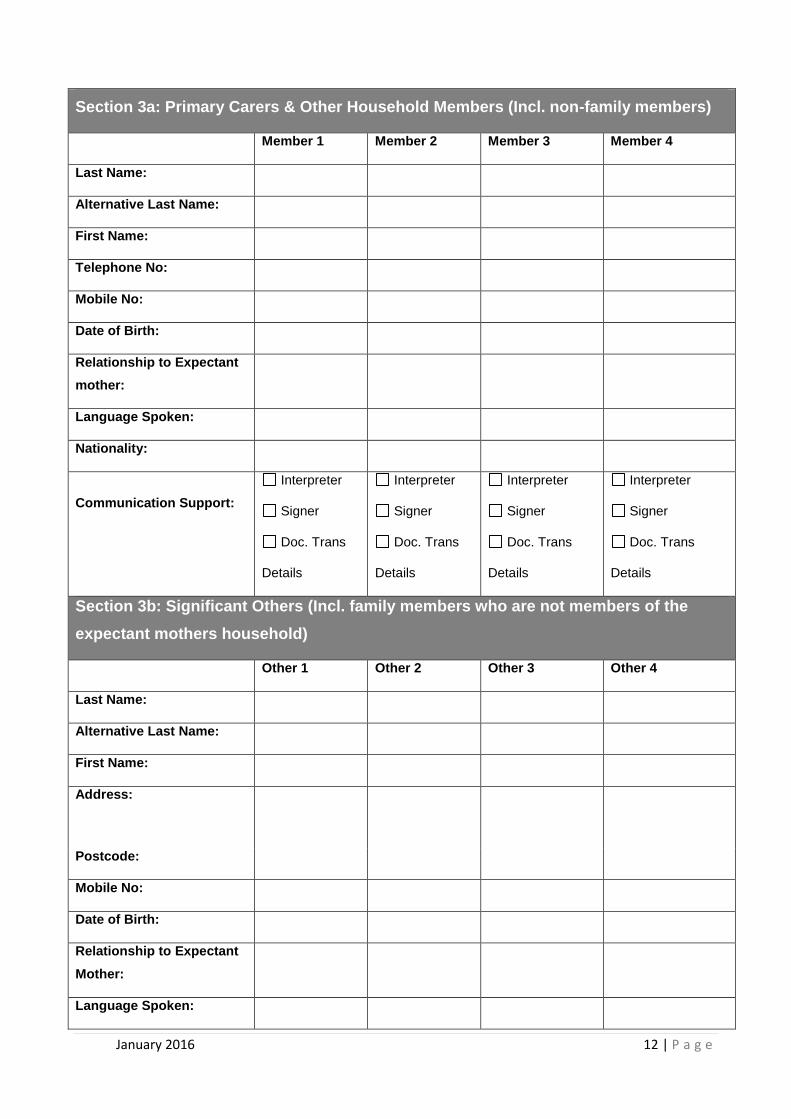
Section 3a: Primary Carers & Other Household Members (Incl. non-family members)
Member 1 Member 2 Member 3 Member 4
Last Name:
Alternative Last Name:
First Name:
Telephone No:
Mobile No:
Date of Birth:
Relationship to Expectant
mother:
Language Spoken:
Nationality:
Communication Support:
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Section 3b: Significant Others (Incl. family members who are not members of the
expectant mothers household)
Other 1 Other 2 Other 3 Other 4
Last Name:
Alternative Last Name:
First Name:
Address:
Postcode:
Mobile No:
Date of Birth:
Relationship to Expectant
Mother:
Language Spoken:

January 2016 13 | P a g e
Nationality:
Communication Support:
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Interpreter
Signer
Doc. Trans
Details
Section 4a: Summary of Referrer’s Previous Involvement
Section 4b: Referral Consent
Is the expectant mother aware the referral is
being made?
Yes No
Does the expectant mother consent to the
referral?
Yes No
If NO, please explain

January 2016 14 | P a g e
Section 5: Additional Information: Agencies Currently Working with the Expectant
Mother
Agency and Contact Details
Name:
Role:
Tel No:
Email:
Name:
Role:
Tel No:
Email:
Name:
Role:
Tel No:
Email:
Name:
Role:
Tel No:
Email:
Name:
Role:
Tel No:
Email:
Name:
Role:
Tel No:
Email:
January 2016 15 | P a g e
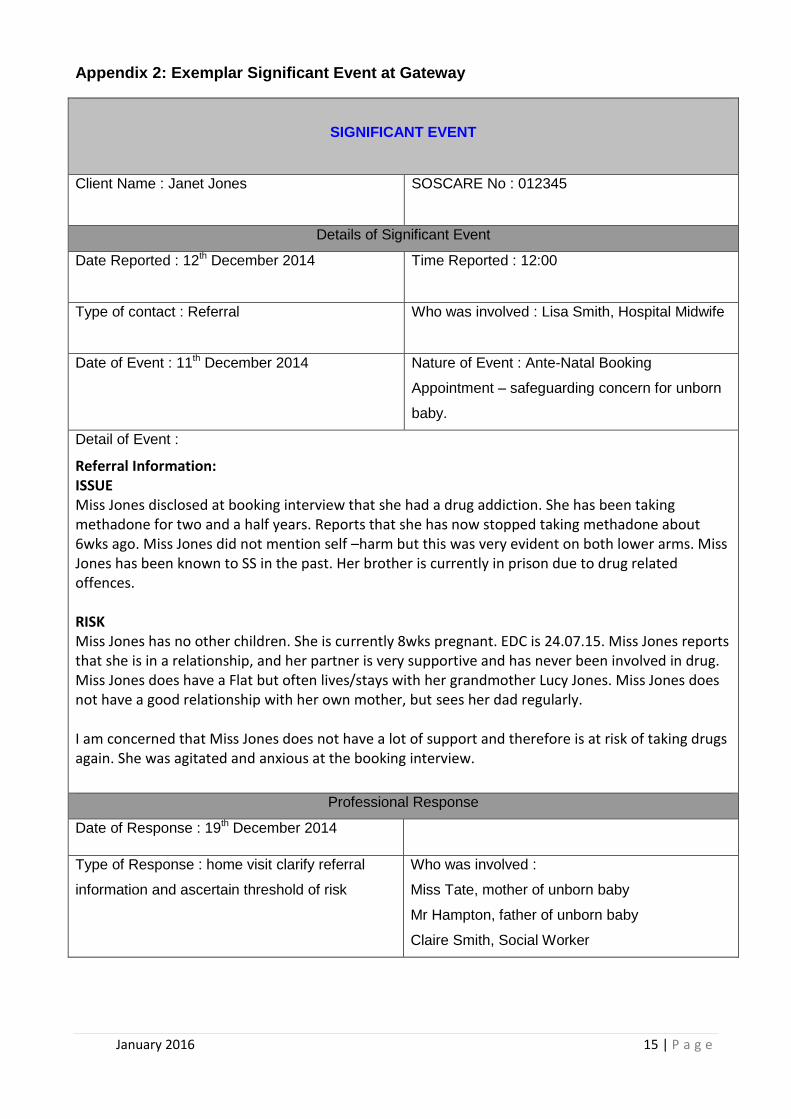
Appendix 2: Exemplar Significant Event at Gateway
SIGNIFICANT EVENT
Client Name : Janet Jones
SOSCARE No : 012345
Details of Significant Event
Date Reported : 12th December 2014
Time Reported : 12:00
Type of contact : Referral
Who was involved : Lisa Smith, Hospital Midwife
Date of Event : 11th December 2014
Nature of Event : Ante-Natal Booking
Appointment – safeguarding concern for unborn
baby.
Detail of Event :
Referral Information: ISSUE
Miss Jones disclosed at booking interview that she had a drug addiction. She has been taking methadone for two and a half years. Reports that she has now stopped taking methadone about 6wks ago. Miss Jones did not mention self –harm but this was very evident on both lower arms. Miss Jones has been known to SS in the past. Her brother is currently in prison due to drug related offences. RISK
Miss Jones has no other children. She is currently 8wks pregnant. EDC is 24.07.15. Miss Jones reports that she is in a relationship, and her partner is very supportive and has never been involved in drug. Miss Jones does have a Flat but often lives/stays with her grandmother Lucy Jones. Miss Jones does not have a good relationship with her own mother, but sees her dad regularly. I am concerned that Miss Jones does not have a lot of support and therefore is at risk of taking drugs again. She was agitated and anxious at the booking interview.
Professional Response
Date of Response : 19th December 2014
Type of Response : home visit clarify referral
information and ascertain threshold of risk
Who was involved :
Miss Tate, mother of unborn baby
Mr Hampton, father of unborn baby
Claire Smith, Social Worker

January 2016 16 | P a g e
Details:
Child’s Needs Health and Development
Ms Jones has been attending her antenatal appointments appropriately. She disclosed to the midwife at the antenatal booking appointment that she had been addicted to methadone for 2 1/2 years. She ceased when she found out she was pregnant and appears to be doing well. Expected due date is 24
th July 2015. The GP advised that Ms Jones is attending her
antenatal appointments appropriately and agreed that she appears to be doing well in terms of refraining from substance misuse. He agreed to make a referral to Social Services if he has reason to believe that Ms Jones is using illegal substances in the future. Education and Learning
Ms Jones and Mr Hampton have been buying items to promote the baby's learning. They will endeavour to stimulate the baby appropriately and the health visitor will provide advice about same. Identity, self-esteem, and self-care
Baby Jones will rely on her parents for her care needs to be met. The health visitor will provide advice about good care routines. Mr Hampton is a Roman Catholic and Ms Jones is of Church of Ireland faith. The advice that they will give consideration to the baby's religion but that it is not an issue. Ms Jones is considering living with her mother when the baby is born but Mr Hampton will be greatly involved. Family Relationships
Ms Jones and Mr Hampton report a good relationship. The both advise that they were initially shocked about the pregnancy but have now come to terms with the news and are looking forward to the baby's arrival and are making preparations. Parent/Carer’s Capacity Basic Care and Ensuring Safety
Ms Jones has advised that she no longer uses illicit drugs. She advised that she found it easier to cease the substance misuse than she had envisaged. She currently resides in supported living and staff there monitor and support her progress. Ms Jones's key worker advised that she is attending her appointments appropriately and is not using drugs. He advised that she is making preparations in terms of buying essential items for the baby. Mr Hampton had been addicted to cannabis and had previously used extensively. Mr Hampton advised that he weaned himself off cannabis and that he did not feel the need to attend addiction support services. The key worker in the supported housing complex advised that Mr Hampton very rarely uses cannabis and has distanced himself from friends and relatives who continue to misuse substances. The Social Worker advised Ms Jones and Mr Hampton that he is not to be in contact with the baby if ever under the influence of cannabis. Ms Jones advised that she no longer self-harms and attended a self-harm group in Craigavon Hospital for support to address these behaviours. Ms Jones is considering moving in with her mother when she has to leave the supported housing - one month before the birth of the baby. A previous Social Services assessment indicates that Ms Jones’ mother was deemed to be appropriate and protective of her younger daughter when Ms Jones was using drugs. Emotional Warmth
Both parents appear to be looking forward to the birth of their first baby. Ms Jones had informed the health visitor that she was beginning to feel anxious about the birth and she has subsequently been attending antenatal breathing classes. Guidance, Boundaries and Stimulation
The health visitor will advise the couple about appropriate routines. Ms Jones's grandmother Lucy Jones is supportive. Ms Jones is considering living with her mother in preparation for the birth of the baby. These extended family members will provide guidance and support to the new parents. Stability
Ms Jones had previous difficulties with substance misuse and self-harming. She appears to have ceased using mephodrone since becoming pregnant and attended a self-help group in her local Hospital for support in relation to self-harming. Environmental Factors Family History, Functioning and Well-Being
Previous referrals in relation to Ms Jones are when she was a minor:-
19/01/2006 referred by relative - reason - other. closed 21/01/06 31/01/07 referred by police - reason - child care problem. Closed 13/02/07 - Closed file indicates that Ms Jones was referred by PSNI after witnessing an older male exposing himself from an upstairs window.
Referrals in relation to Ms Jones since becoming an adult:-
22/09/11 referral from hospital nurse - re. hospital referral. case closed 30/09/11
January 2016 17 | P a g e
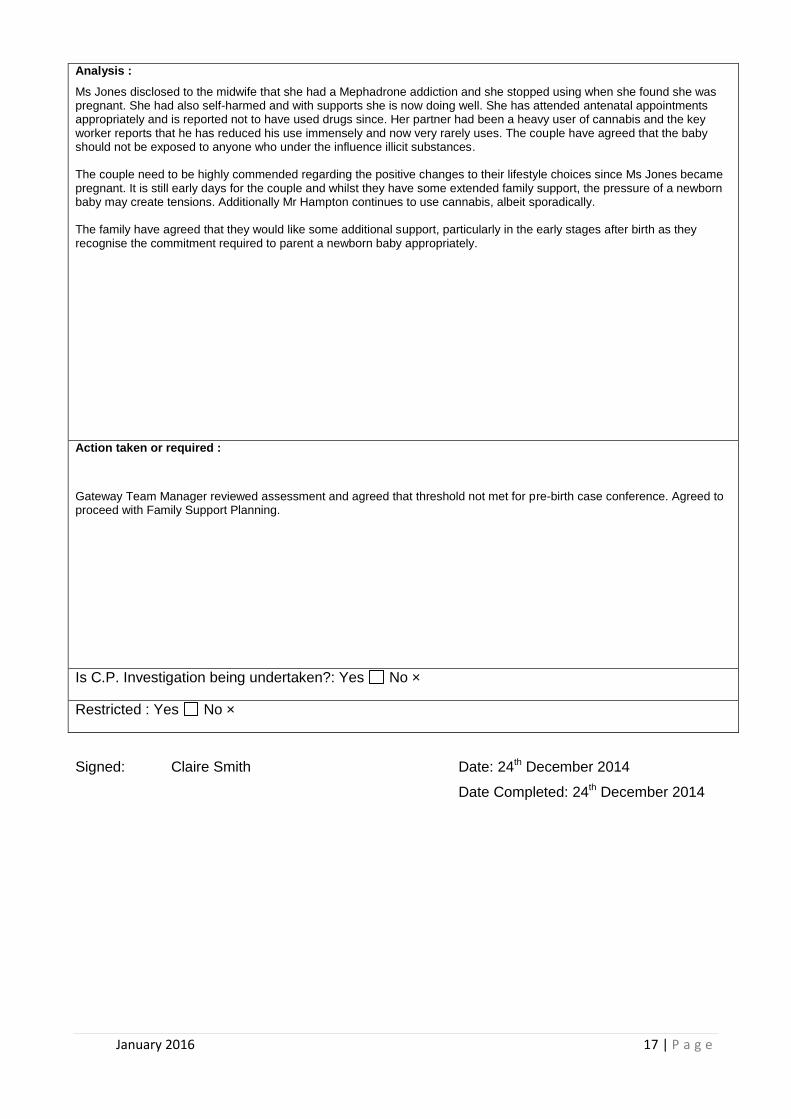
Analysis :
Ms Jones disclosed to the midwife that she had a Mephadrone addiction and she stopped using when she found she was pregnant. She had also self-harmed and with supports she is now doing well. She has attended antenatal appointments appropriately and is reported not to have used drugs since. Her partner had been a heavy user of cannabis and the key worker reports that he has reduced his use immensely and now very rarely uses. The couple have agreed that the baby should not be exposed to anyone who under the influence illicit substances. The couple need to be highly commended regarding the positive changes to their lifestyle choices since Ms Jones became pregnant. It is still early days for the couple and whilst they have some extended family support, the pressure of a newborn baby may create tensions. Additionally Mr Hampton continues to use cannabis, albeit sporadically. The family have agreed that they would like some additional support, particularly in the early stages after birth as they recognise the commitment required to parent a newborn baby appropriately.
Action taken or required :
Gateway Team Manager reviewed assessment and agreed that threshold not met for pre-birth case conference. Agreed to proceed with Family Support Planning.
Is C.P. Investigation being undertaken?: Yes No ×
Restricted : Yes No ×
Signed: Claire Smith Date: 24th December 2014
Date Completed: 24th December 2014

January 2016 18 | P a g e
Appendix 3: Guidance to Completing a Pre-Birth Risk Assessment
Antenatal Care: Medical and Obstetric History.
When considering these issues it is important to be aware that the named lead midwife will
have provided the expectant mother with choices about the place of birth and type of care
they would like to receive. A booking interview is carried out at around 8-12 weeks of
pregnancy.
During the interview the lead midwife, responsible for the patients care, collects
information which will build into a full medical and social history. When all the data is
collated the midwife is able to assist the women in making informed choices about the care
she receives and advises on the suitability of her choices. The midwife will discuss with the
women the pattern of care which is most suited to her needs. A holistic approach, taking
into account the women’s social history will be provided. This needs to be incorporated
into the pre-birth assessment.
In accordance with ‘Healthy Child, Healthy Futures’, the midwife and health visitor will be
involved during the pregnancy. They will advise the parents about keeping the baby
healthy and well. Together they will assess any specific needs and will commence the
family health assessment. This will inform the pre-birth risk assessment.
Social History
When planning a pre-birth assessment it is vital to review any previous history. This will
include; the quality of their parenting; their early life experiences; social, educational,
medical, marital, occupational, criminal (and sexual) history. Consideration should be
given to any complications during the pregnancy and birth; any developmental issues and
milestones; peer and sibling relationships; school performance; family relationships; drug
and alcohol abuse; general impulsivity; anger levels; self-esteem; social skills and
competence; and past psychiatric history.
This will entail reading the case files on any siblings/children including those any have
been removed from the parents care. In addition searches must be done on any new
partners in the household or those who are playing a significant role in the life of the
family, particularly checking if they have children with whom they no longer live with
and/or have contact to ascertain the reasons for this.

January 2016 19 | P a g e
A chronology of significant events must be included within the Pre Birth Safeguarding
Report.
Practitioners must be mindful that repeated serious case reviews point to failures in
drawing information together, analysing it and identifying patterns that, when seen
together, actually changes the perspective of the case. It is essential that agency
colleagues contribute fully to this process.
Reder and Duncan (1999) propose that maltreating parents may experience "care" and/or
"control" conflicts in which the parents' own experiences of adverse parenting left them
with unresolved tensions that spilled over into their adult relationships: Care conflicts arise
out of experiences of abandonment, neglect or rejection as a child, or feeling unloved by
parents. They show in later life as excessive reliance on others and fear of being left by
them; or by the adult distancing themselves from others; being intolerant of a partner's or
child's dependency; unwillingness to prepare antenatally for an infant's dependency
needs; or declining to respond to the needs when the child is born.
Control conflicts are based on childhood experiences of feeling helpless in the face of
sexual or physical abuse or neglect, or inappropriate limit setting. In adult life they may be
enacted through: violence; low frustration tolerance; suspiciousness; threats of violence; or
other attempts to assert power over others. Violence or control issues can become part of
their relationship with partners, children, professionals or society in general.
Unresolved conflicts can influence the meaning that a child has for its carer. For example:
the child's birth may have coincided with a major life crisis e.g. as a consequence of the
mother being raped, being abandoned by a partner, or a child born of incest, following
which the child becomes a constant reminder of the associated feelings. The child may be
blamed for problems in the parent's life or expected to help resolve them.
The Social Worker should attempt to build up a clear history from the parents of their
previous experiences in order to ascertain whether there are any unresolved conflicts and
also to identify the meaning any previous children had for them.
Area’s for enquiry when completing a social history should include;

January 2016 20 | P a g e
Family of origin
Both parent’s culture of origin.
Parental criminal/ ante-social behaviour
The extent of any parental alcohol and substance misuse and it’s consequences for
them and their family.
Presence and degree of any parental conflict including physical violence.
What caused this violence? Who was it directed towards?,
What were the consequences of that violence then and now?
What did their parents enjoy doing together?
Extent of parental separations and family bereavements?
Family interests and activities?
Allocation of roles and responsibilities?
Family demonstration of feelings?
Childhood
The nature and quality of family relationships and the type and adequacy of role
modelling.
What was it like to be a child in their family home?
Who was special to them and who cared for them the most?
What was their place in the family?
Were they abused or neglected, if so, who by, for how long?
What was the emotional and behavioural consequence for them?
Had there been any referrals to professional agencies?
Any periods of time in local authority care?
School
Mainstream or special schooling?
Subject to any statement of special educational needs?
Any academic difficulties, behaviour or attainment issues?
School achievements, aptitude, abilities and qualifications?
Existence of any attendance issues?
Reasons for any changes in schooling, moves or exclusions etc?
Any other significant events?
January 2016 21 | P a g e
Occupational/social/recreational history
Degree of success in establishing adult relationships, social, intimate, employment
and the degree of satisfaction with these?
Employment history, evidence of any dismissal and extent to which this may
indicate social incompetence, problems with authority or substance misuse?
Types of jobs, performance, satisfaction and level of responsibility and
dependability.
Types of leisure activities/hobbies/clubs etc and extent to which these reflect their
social skills and self image?
Criminal history
Number of previous offences? (one of the best predictors of future abuse is the
number of previous offences)
Are the offences against people or property, social rule violations e.g. drink driving?
What is the frequency, circumstances and motivation of the offending behaviour?
When did they become know to the Police/other criminal agencies? What were the
circumstances?
Details of previous disposals and the responses to these?
Are they entrenched in their behaviour and what does this mean for the expectant
baby?
Is their evidence of escalation in criminal behaviour?
What were their modus operandi and antecedent conditions or behaviours?
Details of victim; ages, offences and consequences for the adult/child?
Current Family Structure and Sources of Support
It is essential to establish the full details of the immediate and extended family and that
relevant child protection checks are completed as a means of aiding the assessment and
future care planning, if required.
It is important that consideration is given to the family strengths and their potential ability to
harness these to produce positive change for the unborn child, as well as the risks that
may be prevalent within the household. Examples of relevant questions would include
What is the family’s culture now and that of their origin?

January 2016 22 | P a g e
How the parents met?
Why they stay together?
How their relationship has developed and changed?
The positive and negative attributes that exist within the relationship?
Individual parents physical/emotional/intellectual abilities?
Previous parental experiences i.e. number of children?
Extent of disputes and violence in previous relationships?
Extent of abuse substance misuse in previous relationship?
Potential impact of previous problematic adult relationships on couple?
Parents hopes, aspirations, strengths and talents?
Parents range of support networks?
Extent to which parents engage with professional agencies?
Parent’s ability to use family strengths to produce positive change?
Attitudes to Previous Interventions
It is particularly important to ascertain the parent(s) views and attitudes towards any
previous children who have been removed from their care, or where there have been
serious concerns about the parenting practices. Examples of relevant questions would
include:
Do the parent(s) understand and give a clear explanation of the circumstances in
which the abuse occurred?
Do they accept responsibility for their role in the abuse?
Do they blame others?
Do they blame the child?
Do they acknowledge the seriousness of the abuse?
Did they accept any treatment/counselling?
What was their response to previous interventions? E.g. genuinely attempting about
that child now?
What has changed for each parent since the child was abused or removed?
It is important to ascertain the parents’ feelings towards the current pregnancy and the
new baby including:
Is the pregnancy wanted or not?
Is the pregnancy planned or unplanned?
January 2016 23 | P a g e
Is this pregnancy the result of sexual assault?
Is domestic abuse an issue in the parents' relationship?
Is the perception of the unborn baby different/abnormal? Are they trying to replace
any previous children?
Have they sought appropriate ante-natal care?
Are they aware of the unborn baby's needs and able to prioritise them?
Do they have realistic plans in relation to the birth and their care of the baby?
Existence of Previous Abuse and Acceptance of Responsibility
In cases where a child has been removed from a parent's care because of abuse there are
some additional factors which should be considered. These include:
The ability of the perpetrator to accept responsibility for the abuse although this
should not be seen as lessening the risk for additional children.
The ability of the non-abusing parent to protect. The fact that the child has been
removed from their care suggests that there have been significant problems in
these areas and pre-birth assessment will need to focus on what has changed and
the prospective parent(s) current ability to protect.
Relevant questions when undertaking a pre-birth assessment when previous abuse has
been the issue include:
The circumstances of the abuse: e.g. was the perpetrator in the household?
Was the non-abusing parent present?
What relationship/contact does the mother have with the perpetrator (Assuming the
man as perpetrator - however, this is not always the case)
How did the abuse come to light? E.g. did the non-abusing parent disclose or
conceal? Did the child tell? Did professionals suspect? Did the non-abusing parent
believe the child? Did they need help and support to do this?.
What are current attitudes towards the abuse? Do the parents blame the child/see it
as her/his fault?
Has the perpetrator accepted full responsibility for the abuse? How is this
demonstrated? What treatment did he/she have?
Who else in the family/community network could help protect the new baby?
How did the parent(s) relate to professionals? What is their current attitude?

January 2016 24 | P a g e
In circumstances where the perpetrator is the prospective father or is living in the
household, where there is no acknowledgement of responsibility, where the non-
abusing parent blames the child and there is no prospect of effective intervention
within the appropriate timescale, then confidence in the safety of the newborn baby
and subsequent child will be poor.
Circumstances where the perpetrator is convicted of posing a risk to children and is
already living in a family with other children, (albeit with social work involvement), should
not detract from the need for a pre-birth assessment. In all assessments it is important to
maintain the focus on both prospective parents, and any other adults living in the
household and not to concentrate solely on the mother.
Non-Abusing Parents Ability to Protect
When considering capacity of non-abusing parents to protect it is important to assess their
own personal history and particularly their understanding in and perception as regards the
abuse perpetrated by the partner. Smith, 1994 cited from Calder (2003) poses a number
of relevant questions including:
How critical or uncritical are they regarding their partner’s abusive behaviour?
To what extent were they party to or aware of their partner’s abusive behaviour?
What has changed regarding their understanding of past abuse
To what extent to they accept responsibility for failure to protect or collusion with the
abuse?
What is the non-abusing parent's position regarding the abuse/conviction both at
the time and now?
What information do they have regarding the abuse and who provided it?
Can additional information be provided to move the parent from any disbelieving
position?
What feelings do they have to the child? E.g. anger, sympathy, blame?
To what extent does the non-abusing partner accept that their partner was
responsible for the abuse?
To what extent can the non-abusing partner work with Children’s Social Care and
other agencies?
Could/can they choose their unborn child over abusing partner?
To what extent is the non-abusing partner dependent on the abuser?
January 2016 25 | P a g e
How vulnerable is the non-abusing partner?
Do they have a history of violent or abusive relationships?
Does the non-abusive partner have other vulnerabilities i.e. disability, ill health, or
other condition that isolates them from help?
To what extent do they recognise the existence of future risk to the unborn child
What is their ability to manage this?
What level of knowledge do they have re the impact sexual offending behaviour in
general and specific to partner?
Understanding Of Expectant Baby’s Needs And Ability To Meet Them
When looking at the parents capacity to understand and meet their new born baby’s
needs. Consideration should be given to the expertise of Health Visiting and Midwifery in
carrying out this task and those relating to practical preparation for the baby and parental
insight into the development of routines and baby’s basic needs.
Other relevant questions would include:
What are the social and cultural expectations of the family?
What are the ethnic expectations of the family role and interventions?
What are the family roles for women, children, men and elders?
What is the response to ethnic history?
What is the impact of any racism?
What is the impact of class and social position?
Is the family integrated/marginalised/powerful/powerless?
What belief systems and values influence role expectations, define and set limits of
acceptable behaviour?
What are the key support structures?
Which are the key relationships within the immediate and extended family?
What life cycle stage are the family at/ what are the risks and challenges?
What solutions are used to manage family conflict?
How have the parents both individually and together responded to their expected
baby?
To what extent are the parents developing a sense of attachment to their expected
baby?
How do the parents build relationships and whose responsibility to they feel it is?

January 2016 26 | P a g e
What understanding do the parents have of their expected baby’s basic needs?
Do the expectant parents have the capacity to provide ‘good enough parenting’ to
the expected baby?
Contributing Risk Factors
Mental Health Problems
Although most parents with mental health needs are able to care for their children
appropriately, research has indicated that child-maltreating parents are often shown to
have mental health problems e.g. depression, history of attempted suicide, schizophrenia
etc. Non- compliance with medication without medical supervision is a cause for concern.
Children are at increased risk of abuse by psychotic parents when incorporated into their
delusional thinking e.g. "(the baby) is trying to punish me for my sins".
Calder (2003) notes that the practitioner needs to be aware that:
Parental illness affects children, but not necessarily adversely.
Mental illness can affect the capacity of parents to parent and the resulting
parent/child relationship.
Parents may not be able to address the needs of their newborn child safely or
adequately as a result of their illness.
Caring for children affects the mental health of the parent. The challenges of
parenting can precipitate and influence parental mental illness.
Children’s mental health and development needs have an impact on parental
mental health.
If mental health is likely to be a significant issue, more detailed assessment should be
sought from professionals with relevant expertise. While the practitioner will need to obtain
a mental health assessment in these cases it is important not to become "paralysed" if that
is not forthcoming. It is essential to continue the assessment based on the behaviour of
the parent(s), not the diagnosis, and the potential risk of that behaviour to the need to
include the risk to unborn to new-born child. In addition, where there are mental health risk
factors identified, on-going revaluation of risk is essential.
There it is suspected that a prospective parent may have a learning difficulty that may
result in significant harm to the new born child a more detailed assessment should also be
sought from professionals with the relevant experience.

January 2016 27 | P a g e
Substance and Alcohol Misuse
Social workers must always use the expertise with community alcohol and substance
misuse teams as well as other relevant health professionals when considering the
implications of drug and alcohol misuse on the unborn child and the impact post-delivery.
‘While drug or alcohol misuse is not in itself a contra-indication that the parent(s) will
be unable to care safely for the baby, excessive parental substance and alcohol
misuse is likely to have a detrimental impact on the unborn child’. Cleaver et al
(1999).
The Social Worker will need to give consideration to the following:
What type of substances is the prospective parent/s dependent upon?
What is the route/amount/duration/pattern of the substance misuse?
The consequences for the baby of the mother's substance misuse
during pregnancy e.g. withdrawal symptoms, and for the parenting of any other
children in the household.
The history of parental substance misuse, current dependency.
Any evidence of being incapacitated/comatose or paranoid/overtly psychotic?
Is the prospective parent engaged with drug and alcohol services?
Motivation to engage with drug and alcohol services?
What is the prospective parent/s understanding of the potential effects of their
substance misuse on the unborn and new born child?
Can parental substance misuse be managed compatibly with the demands of a
new-born child?
What has been the impact of parental substance misuse been on other
children/sibling within the household?
Domestic abuse and other violent behaviours
A current and/or previous history of domestic abuse and or violent behaviour should be
carefully evaluated. When addressing these issues it is recommended that Maddie
Bell’s Domestic Violence Risk Assessment model is used.
Detail should be obtained about:
The nature of violent incidents
January 2016 28 | P a g e
Their frequency and severity
Information on what triggers violent incidents.
The non-abusing/non-violent parent’s recognition of the potential risks as a result of
the history of or current domestic abuse/ violent behaviour see ‘Domestic Abuse
assessment’ in tools.
Some babies may be more difficult to care for than others (Reder and Duncan, 1995, p.49;
Reder and Duncan, 1999, pp. 62-71). Research has indicated that the risks are greater
when a parent with unresolved care and control conflicts is caring for a baby with particular
characteristics which may make him/her harder to care for e.g. a poor feeder or sleeper,
constant crying, a disabled child etc.
During the pre-birth assessment increased risk factors may be prevalent for example:-
Domestic abuse incidents in the pregnancy
Parent/s may exhibit aggressive behaviour
There may be pregnancy complications that could lead to e.g. pre-term delivery with
the result of a baby that will require a higher level of care
It is essential that there is close liaison with the midwives and obstetricians in relation to
these factors .It is also important to examine the history of previous children who have
been removed from the parent(s) care. This will indicate if there were particular
characteristics which made that child harder to care for. It is essential to find out from the
parent(s) what problems, if any/they identified in caring for that child.
Home Environment
Current living arrangements, including amenities and facilities and the impact mental
health and or substance misuse may have upon this; type of accommodation, including
owner occupier, tenant (consider rent arrears), temporary; the exterior of the
accommodation and immediate surroundings; the interior of the accommodation with
specific reference to the child’s individual living arrangements; water, heating, sanitation,
cooking facilities, sleeping arrangements, cleanliness, hygiene, safety; or if homeless,
reasons for this.
Support Networks

January 2016 29 | P a g e
Caring for a new born baby is difficult enough for any parent but can be particularly
stressful if the parent(s) are isolated and do not have a network of support. It is important
to identify whether partners are going to share responsibility or whether it will fall to one,
usually the mother.
Research has indicated that when children have been abused the trigger may often be a
family crisis e.g. loss of home or job, marital problems or upheavals, physical exhaustion
etc (Reder and Duncan, 1999, p.69). However, there are many other triggers and factors
that will need to be considered within an assessment.
It is therefore important to identify the support networks that the parent(s) have, their
financial and housing position. Clear guidelines are outlined in the Framework for
Assessment of Children in Need and their Families.
Parent’s potential for and motivation for change
Future plans of the parent(s)
This will include the degree of realism of the parents’ plans for the future; have they
considered the impact of a future child on their relationship/ lifestyle? Is it safe for the child
to be placed with the parents?
Parental capacity and motivation for change is a critical part of the pre-birth assessment
and is critical to future care planning.
Analysis/Conclusion
Once the information has been gathered through the pre-birth assessment process it
needs to be written up in a final report on the template found at Appendix 4 of this
document.
Critical to the final report is a detailed and robust analysis. It is important to recognise that
analysis is far more than a description or summary of the assessment. The aim of the
assessment is to accurately identify the level of anticipated risk and look at whether this
risk is manageable or not. (Calder, p. 82 2008).
The analysis needs to be logical, evidenced based and must focus on the impact of
parental capacity and environmental factors on the unborn child. It needs to consider both
January 2016 30 | P a g e
parental strengths and weaknesses and any reoccurring patterns of parental behaviour.
The analysis should draw some conclusions as to the parents motivation to change and
what actions need to be taken to either safeguard the child or provide the necessary levels
of support to enable the unborn child to thrive once born and fulfil their full potential.
Finally the Pre-Birth Safeguarding Report should make clear recommendations to aid
future planning. This will be captured in the Proposed Safeguarding Plan. It is these
recommendations that will be considered post birth by a Child Protection Case Conference
and subsequent Core Group Meetings, a Child in Need Meeting or the Court.
The outcome of the Pre-Birth Risk Assessment should be shared with parents and all
agencies involved with the assessment.

January 2016 31 | P a g e
Appendix 3: Pre-Birth Child Protection Conference Report
PBRA
UNOCINI
Understanding the Needs of Children in Northern Ireland
PRE-BIRTH CHILD PROTECTION CONFERENCE REPORT
Child Protection Conference Date:
Unborn Child/ren Details
Proposed Surname at Birth
EDD Ethnic Origin Home Address (at birth)
Family Composition
Name DOB Relationship
to Unborn
Child
PR? Address
Significant Others
Name DOB Relationship
to Unborn
Child
PR? Address

January 2016 32 | P a g e
Family GP:
Family Midwife:
Family Health Visitor:
Dates Parents/Carers Seen for Completion of Pre-Birth Assessment
Name: Date(s) seen:
Multi-Agency Involvement
Agency: Person:
Specialist Assessment(s)
Agency: Purpose of Assessment:
Significant Events
Date Event
Pre-Birth Risk Assessment
Ante Natal Medical And Obstetric History
Social History
Current Family Structure And Sources Of Support
Attitude To Previous Intervention (If Appropriate)
Attitude To Current Pregnancy

January 2016 33 | P a g e
Existence Of Previous Abuse And Acceptance Of Responsibility
Non-Abusing Parent’s Ability To Protect
Understanding of Expectant Baby’s Needs and Ability to Meet Them
Contributing Risk Factors
Home Environment
Support Networks
Parents’ Potential And Motivation To Change
Analysis
What needs have you identified?
What strengths have you identified?
What existing and/or potential risks have you identified?
What resilience and protective factors have you identified?
Conclusions
What are your conclusions?

January 2016 34 | P a g e
____________________________________________________________________
PRE BIRTH CHILD PROTECTION CONFERENCE MEETING OUTCOME
Areas of Discussion

January 2016 35 | P a g e
Agreed Parental Plan The baby will have a Child in Need Plan / Child Protection Plan (delete as appropriate) ( see below) due to risk of ................................ Risk issues for: mother C baby C staff C during hospital stay C on return home C
Little / no extra support or observation required
Mother and baby to be placed together on Post Natal Ward.
Observation, assessment and support required with caring for baby
Mother and baby to be placed together on Transitional Care Unit/Mother & Baby Unit for a maximum of 5-7 days
Baby to be placed on Transitional Care Unit or Neo-natal Unit and all contact for ………….. ……………………………………………………..to be arranged / supervised by
Children's Services
It is proposed to place Baby with alternative carers/ Foster Carers as soon as possible once medically fit for discharge from hospital and any legal process has been completed
Other relevant information A brief history of issues to include eg proposed legal status of baby, risk of aggression or violence, restricted contact for family members etc Specific discharge details Please inform Children’s Services /RESWS prior to discharge Should any emergency situation arise contact Police by dialling 101 or 999 Date: Signature:
Copies to Parents, Social Worker, Regional Emergency Social Work Service, Midwife,
Liaison Midwife, Ambulance Service and Police in child protection cases.
January 2016 36 | P a g e
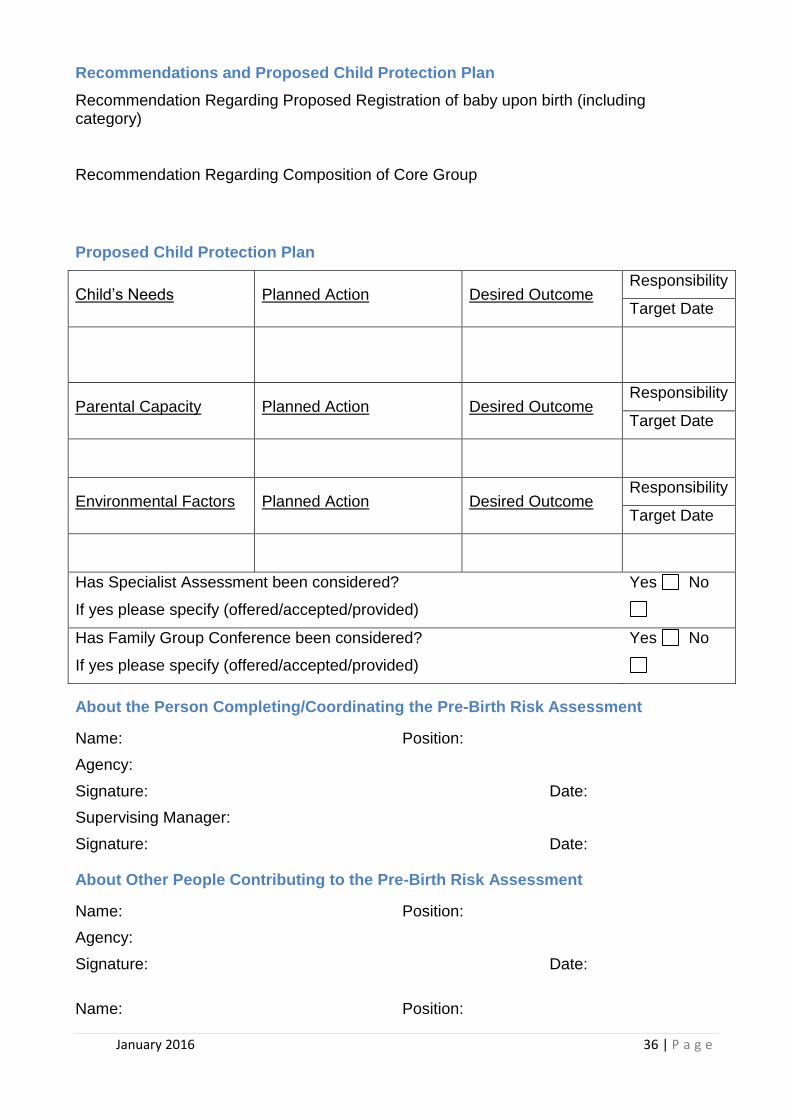
Recommendations and Proposed Child Protection Plan
Recommendation Regarding Proposed Registration of baby upon birth (including category)
Recommendation Regarding Composition of Core Group
Proposed Child Protection Plan
Child’s Needs Planned Action Desired Outcome Responsibility
Target Date
Parental Capacity Planned Action Desired Outcome Responsibility
Target Date
Environmental Factors Planned Action Desired Outcome Responsibility
Target Date
Has Specialist Assessment been considered?
If yes please specify (offered/accepted/provided)
Yes No
Has Family Group Conference been considered?
If yes please specify (offered/accepted/provided)
Yes No
About the Person Completing/Coordinating the Pre-Birth Risk Assessment
Name: Position:
Agency:
Signature: Date:
Supervising Manager:
Signature: Date:
About Other People Contributing to the Pre-Birth Risk Assessment
Name: Position:
Agency:
Signature: Date:
Name: Position:

January 2016 37 | P a g e
Agency:
Signature: Date:
Name: Position:
Agency :
Signature: Date:
Name: Position:
Agency:
Signature: Date: