Embed Size (px)
Citation preview

Guide to intracranial cysts: A “Cyst-o-matic” approach
Bryan Foley MD, Jennifer Becker MD, Rihan Khan,MD

Control #: 680Title: Intracranial cystic lesions: A “cyst-o-matic” approach to identification with pathologic correlationeEdE#: eEdE-63

None
DISCLOSURES

Purpose:The purpose of this exhibit is to provide an
interactive case based review of intracranial cystic lesions with a focus on CT and MR, while discussing the etiologies and diff erential diagnostic considerations.
Approach/Methods:We present a spectrum of intracranial cystic lesions
and interesting variants from cases collected over the last 3 years from everyday neuroradiology practice at a university medical center.

CHARACTERIZING AN INTRACRANIAL CYST
Location CT or MR imaging features+
= Diagnosis or short Differential Diagnosis

ANATOMIC LOCATION
Intra-axial
Extra-axial
Midline
Off-Midline
Supra or infratentorial

Findings/Discussion: Cases will be presented demonstrating common and uncommon intracranial cysts and cystic lesions. First you will see the images, next an image description locating the cyst, then a summary slide with key facts and differential diagnosis.

THE MOST COMMON EXTRA-AXIAL CYST
Extra-axial, supratentorial, off-midlinecyst that follows CSF signal, no restricted diffusion Arachnoid Cyst

ARACHNOID CYST
•Benign congenital lesion, lined by arachnoid cell single layer•Extraaxial, conforms around brain parenchyma•Most are supratentorial and off-midline•Contain clear fluid that follows CSF signal•Uniclocular, smooth wall, can remodel the calvarium•No restricted diffusion, No enhancement•Typically supratentorial, middle cranial fossa ~65%•Posterior fossa ~10%•Treatment options: observe, resection, shunting•Hemorrhage into cyst can rarely occur
DDXEpidermoid cyst (+DWI)Porencephalic cyst (communicates with ventricle)Chronic subdural hematoma (old blood products GRE or SWI)
Classic
Uncommon

ARACHNOID CYST
Rare midline arachnoid cyst assumed in the velum interpositum

EPIDERMOID CYST
Extra-axial, basal cistern, para-midline cystic mass, CT hypodense, MR restricted diffusion and incomplete FLAIR suppression

EPIDERMOID CYST
•Congenital •Squamous epithelium wall with internal keratin and cholesterol•Location: Extra-axial, paramidline, basal cisternsCerebellopontine angle CPA cistern ~50%•Fill cisterns, surround vessels and cranial nerves•CT: hypodense similar to CSF•MR: + DWI restriction, T1 T2 iso to hyperintense, mild heterogeneity, incomplete FLAIR suppression , minimal–no enhancement
DDXArachnoid cyst, (no DWI, CSF signal)Dermoid cyst, (midline, less common, fat T1 signal)

EPIDERMOID CYST
Incidental finding of an intracranial extra-axial, lesion just above the right foramen ovale that is consistent with an incidental epidermoid cyst.

DERMOID CYST
Extra-axial, suprasellar, midline cystic massT1 hyperintense (fat) , FLAIR intense, +DWI

DERMOID CYST
•Benign, congenital•Keratin + cholesterol + hair, fat, oil•Midline, suprasellar cistern location most common•Rare, younger age than epidermoid•Can rupture, chemical meningitis•CT: hypodense•MR: fat T1 signal, +DWI, FLAIR intense
DDXEpidermoid cyst, (no fat signal)Lipoma (homogeneous)Craniopharyngioma (multicystic, enhancement)

ENLARGED PERIVASCULAR SPACE
T2 cyst
Intra-axial, supratentorial, follows CSF signal, no enhancement, No restricted diffusion

ENLARGED PERIVASCULAR SPACE
•AKA “Virchow-Robin space•Most common intra-axial cyst•Anatomic variant, nonneoplastic•Dilated pia lined spaces along arterioles into brain parenchyma (intra-axial)•Follow CSF signal•Classic located near the anterior commisure in basal ganglia•Also common in white matter, midbrain, and cerebellum dentate nuclei (*infratentorial)•Incidental, usually asymptomatic
DDXLacunar infarctNeurocysticercosis

NEUROGLIAL CYST
There is no restricted diffusion, internal or peripheral enhancement, solid components, or surrounding vasogenic edema. The cyst does not communicate with the adjacent right lateral ventricle or extend to the right frontal cortex.
Imaging findings are consistent with a Neuroglial cyst
Intra-axial, supratentorial, follows CSF signal, no enhancement, No restricted diffusion

NEUROGLIAL CYST
Companion case of a left temporal lobe Neuroglial cyst
•Benign congenital lesion•Uncommon•Intra-axial•Clear CSF like cyst lined by epithelium•Typically intraparenchymal in the frontal lobe•Round, smooth, no enhancement,•Does not communicate with the ventricle
DDXEnlarged perivascular spaceInfectious cystArachnoid cystCystic neoplasm

CHOROID PLEXUS CYST
Intra-axial, intra-ventricular subtle CSF density and T2 hyperintense cystic masses with peripheral enhancement in the choroid plexus glomi in the lateral ventricle atria.

CHOROID PLEXUS CYST
•Benign, congenital and acquired•Location: intraventricular, choroid glomus in atrium•Usually asymptomatic and incidental, rarely can cause hydrocephalus obstruction with large size•Cyst contains protein; CT and MR signal vary iso to hyper T1 and T2, variable enhancement•~75% bright on DWI•enhancement
Acute stroke workup demonstrating incidental choroid plexus cysts on DWI
DDXEpendymal cystChoroid plexus papilloma (child, avid enhancement)

COLLOID CYST
Intra-axial, intra-ventricular unilocular hyperdense cyst at the upper 3rd ventricle/foramen of Monroe area. MR demonstrates isointense T2 signal and nonenhancment. No acute hydrocephalus.

COLLOID CYST
•Unilocular 3rd ventricle mucin containing cyst derived from endoderm•Characteristic location: antero-superior aspect of the third ventricle, adjacent to the Foramen on Monro and between the fornices•Symptoms asymptomatic/incidental to headache and obstructive hydrocephalus •CT majority are hyperdense•MR signal variable depending on protein and water content, No restricted diffusion• Size subcentimeter – 3 cm Treatment: surgical excision
Notify physician about findings b/c risk of hydrocephalus and death
DDX Characteristic location limited differentialIntraventricular metastasisAstrocytoma

PINEAL CYST
Etra-axial, supratentorial, midline cyst in pineal gland

PINEAL CYST
•Benign, fluid cyst in pineal gland•Etiology unknown•Incidental finding, relatively common ~25% of adults•Usually asymptomatic•Large cyst can compress cerebral aqueduct and cause hydrocephalus or compress midbrain tectum (Perinaud syndrome)•Rarely hemorrhage complication•Small <1 cm•Signal intensity variable but usually iso to hyperintense to CSF
DDXPineocytoma (solid, enhancement)

RATHKE CLEFT CYST
Extra-axial, supratentorial, midline T2 hyperintese cyst in the sella

RATHKE CLEFT CYST
•Congenital lesion of residual Rathke’s pouch between the anterior and intermediate pituitary lobes•Usually incidental and asymptomatic•Hemorrhage complication is rare•Sellar and suprasellar mass effect •Symptoms: asymptomatic or related to mass effect, headache, pituitary dysfunction, visual field deficits•Well circumscribed sellar based cyst usually T2 hyperintense based on protein content• No enhancement, peripheral enhancement represents compressed pituitaryDDX
CraniopharyngiomaPituitary adenomaArachnoid cyst

PORENCEPHALIC CYST
•Congenital or acquired CSF cystic cavity that communicates with the ventricles•Follow CSF signal and density
Intra-axial, supratentorial, off-midline CSF cystic cavity that communicates with the ventricles

PORENCEPHALIC CYST
•CSF filled cavity in the brain parenchyma•Majority are acquired from prior insultbut can be congenital•Communicate with or adjacent to the ventricle •Follow CSF signal, sharp margins, No restricted diffusion
DDXArachnoid cyst (extraaxial)Cystic encephalomalacia

INTRACRANIAL ABSCESS
Intra-axial, supratentorial, off-midline frontal lobe low density ring enhancing mass with restricted diffusion,
surrounding vasogenic edema ,and mass effect . Findings consistent with …

INTRACRANIAL ABSCESS
•Rare •Appearance of infection depends on stage-early/late cerebritis stage, early/late capsule stage•Commonly supratentorial at grey-white junction•Restricted diffusion (+DWI) and presentation (headache, fever) •Etiology depends on age and immune status, most are hematogenous and pyogenic•Treatment: surgical excision and drainage + antibiotics
DDX “Ring-enhancing mass”Cystic neoplasm 1° or metastaticSubacute hematoma or infarctionDemyelinating process

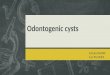
NEUROCYSTICERCOSIS
Extra-axial, supratentorial, off-midline temporal lobe T2 hyperintense cyst with central enhancing scolex, thin
enhancing wall, and absent surrounding vasogenic edema

NEUROCYSTICERCOSIS
•Most common CNS parasitic infection• Caused by the encysted larva of the tapewormTaenia solium•Common worldwide and the Southwest United States•Extraaxial, cyst actually in the subarachnoid space but can appear intraparenchymal•Multiple stages: vesicular, colloid, granular, calcified•Early vesicular stage can present as an intracranial cystDDX
Malignancy, cystic metastasisEnlarged perivascular space
Left temporal lobe vesicular stage cyst with scolex

CRANIOPHARYNGIOMA
Extra-axial, suprasellar, midline T2 hyperintense cystic sella/suprasellar mass causing obstructive hydrocephalus

CRANIOPHARYNGIOMA
•Benign, WHO 1 epithelial tumor from Rathke pouch•Extra-cranial cystic suprasellar mass •Usually T2 hyperintense•Wall and solid components enhance•Look for a calcification•Bimodal distribution children, adults•2 types - Adamantinomatous: cystic pediatric type - Papillary: solid adult type•Treatment: resection, radiation
DDXDermoid (T1 fat signal, +DWI, no enhancement)Rathke cleft cyst

CYSTIC BRAIN METASTASISCOLON ADENOCARCINOMA

HEMANGIOBLASTOMA

CYSTIC SCHWANNOMA

We reviewed common and uncommon intracranial cysts.
1. Start with anatomic localization of a cyst first (intra/extra axial, midline, intraventricular?)
2. CT and MR imaging features (CSF signal, diffusion, enhancement)
3. Combine location and appearance to make diagnosis or form a short differential.
SUMMARY/CONCLUSION:

REFERENCES
•Osborn AG, Preece MT. Intracranial Cysts: Radiologic-Pathologic Correlation and Imaging Approach.Radiology 2006:239:650-664
•Lerner A, Shiroisho MS, Zee C, Law M, et al. Imaging of Neurocysticercosis. Neuroimaging Clin N Am 2012:22:659-76
•Armao D, Castillo M, Chen H, et al. Colloid Cyst of the Third Ventricle:Imaging-pathologic Correlation. AJNR Am J Neuroradiol 2000:21:1470–77
•Salzman KL, Osborn AG, House P et-al. Giant tumefactive perivascular spaces. AJNR Am J Neuroradiol. 2005:26:298-305
•Harrison MJ, Morgella S, Post KD. Epithelial cystic lesions of the sellar and parasellarregion: a continuum of ectodermal derivatives? J Neurosurg 1994:80:I018-25
•Osborn, AG Intracranial Cysts In: Diagnostic Imaging Brain. Salt Lake City, Utah: Amrsys, 2013; 773-808.