-
8/18/2019 Guideline Pancreatite 2013 AJG
1/127
00 PRACTICE GUIDELINES nature publishing group
ME
American College of Gastroenterology Guideline:
Management of Acute Pancreatitiscott Tenner, MD, MPH, ACG!, "ohn
#aillie, M#, Ch#, $CP, ACG% , "ohn De&itt, MD,
ACG' and Santhi S(aroop )ege, MD, ACG*
his guideline presents rec!!end"tins #r the !"n"ge!ent #
p"tients $ith "cute p"ncre"titis %AP&' During the p"st
ec"de( there h")e *een ne$ underst"ndings "nd de)elp!ents in the
di"gnsis( etilg+( "nd e"rl+ "nd l"te !"n"ge!ent
the dise"se' As the di"gnsis # AP is !st #ten est"*lished *+
clinic"l s+!pt!s "nd l"*r"tr+ testing( cntr"st,
nh"nced c!puted t!gr"ph+ %CECT& "nd- r !"gnetic resn"nce
i!"ging %MRI& # the p"ncre"s shuld *e reser)ed #r
"tients in $h! the di"gnsis is uncle"r r $h #"il t i!pr)e
clinic"ll+' .e!d+n"!ic st"tus shuld *e "ssessed
!!edi"tel+ upn present"tin "nd resuscit"ti)e !e"sures *egun
s needed' P"tients $ith rg"n #"ilure "nd- r the s+ste!ic in#l
"!!"tr+ respnse s+ndr!e %SIRS& shuld *e "d!itted
"n intensi)e c"re unit r inter!edi"r+ c"re setting $hene)er
pssi*le' Aggressi)e h+dr"tin shuld *e pr)ided t "ll
"tients( unless c"rdi)"scul"r "nd- r ren"l c!r*idites preclude
it' E"rl+ "ggressi)e intr")enus h+dr"tin is !st
ene#i ci"l $ithin the #i rst 1//4 h( "nd !"+ h")e little *ene#i
t *e+nd' P"tients $ith AP "nd cncurrent "cute
hl"ngitis shuld underg endscpic retrgr"de chl"ngip"ncre"tgr"ph+
%ERCP& $ithin /4 h # "d!issin'
"ncre"tic duct stents "nd- r pstprcedure rect"l nnsterid"l
"nti,in#l "!!"tr+ drug %NSAID& suppsitries shuld
e utilied t l$er the ris2 # se)ere pst,ERCP p"ncre"titis in
high,ris2 p"tients' Rutine use # prph+l"ctic
nti*itics in p"tients $ith se)ere AP "nd- r sterile necrsis is
nt rec!!ended' In p"tients $ith in#ected necrsis(
nti*itics 2n$n t penetr"te p"ncre"tic necrsis !"+ *e use#ul in
del"+ing inter)entin( thus decre"sing !r*idit+
nd !rt"lit+' In !ild AP( r"l #eedings c"n *e st"rted i!!edi"tel+
i# there is n n"use" "nd )!iting' In se)ere AP(
nter"l nutritin is rec!!ended t pre)ent in#ectius c!plic"tins(
$here"s p"renter"l nutritin shuld *e ")ided'
s+!pt!"tic p"ncre"tic "nd- r e3tr"p"ncre"tic necrsis "nd- r
pseudc+sts d nt $"rr"nt inter)entin reg"rdless
# sie( lc"tin( "nd- r e3tensin' In st"*le p"tients $ith in#ected
necrsis( surgic"l( r"dilgic( "nd- r endscpic
r"in"ge shuld *e del"+ed( pre#er"*l+ #r 4 $ee2s( t "ll$ the
de)elp!ent # " $"ll "rund the necrsis'
m J Gastroenterol %+!' !+-:!*++.!*!/ doi:!+0!+'-1a2g0%+!'0%!-
published online '+ "uly %+!'
cute pancreatitis 3AP4 is one of the most common diseases
of
e gastrointestinal tract, leading to tremendous emotion5al,
hysical, and 6 nancial human burden 3!,%40 7n the 8nited
States,
%++9, AP (as the most common gastroenterology discharge
agnosis (ith a cost of %0 billion dollars 3%40 $ecent
studies
o( the incidence of AP ;aries bet(een *09 and
-
8/18/2019 Guideline Pancreatite 2013 AJG
2/127
-
8/18/2019 Guideline Pancreatite 2013 AJG
3/127
0/ Tenner et al.
T"*le /' Su!!"r+ # rec!!end"tins
Diagnosis
!0 The diagnosis of AP is most often established by the presence
of t(o of the three follo(ing criteria: 3i4 abdominal pain
consistent (ith the disease,3ii4 serum amylase and1or lipase
greater than three times the upper limit of normal, and1or 3iii4
characteristic fi ndings from abdominal imaging3strong
recommendation, moderate Ouality of e;idence40
%0 Contrast5enhanced computed tomographic 3C=CT4 and1or magnetic
resonance imaging 3M$74 of the pancreas should be reser;ed for
patients in(hom the diagnosis is unclear or (ho fail to impro;e
clinically (ithin the fi rst *-.A should be gi;en 3strong
recommendation, lo( Ouality of e;idence40
Table % continued on the follo(ing page
The A!eric"n 8urn"l # GAST$I=>T=$IIG )I8M= !+-
J S=PT=M#=$ %+!' $$$'"!9g"str'c!
-
8/18/2019 Guideline Pancreatite 2013 AJG
4/127
-
8/18/2019 Guideline Pancreatite 2013 AJG
5/127
04 Tenner et al.
rt
i
s
e
3
c
o
n
d
iti
o
n
a
l
r
e
c
o
m
m
en
d
a
ti
o
n
,
l
o
(
O
ua
li
t
y
o
f
e
;
i
d
e
nc
e
40
0Genetictestingmay beconsidered inyoungpatient
s 3 L
'+
-
8/18/2019 Guideline Pancreatite 2013 AJG
6/127
ye
ar
s
ol
d4
if
no
ca
us
eis
e;
id
en
t
an
d
a
fa
mi
ly
hi
st
or
y
of
pa
nc
re
ati
c
di
seas
e
is
pr
es
en
t
3c
on
dit
io
na
l
re
co
m
m
en
da
tio
n,
lo
(Ou
ali
ty
of
e;i
de
nc
e40
=T7I
IG:GASTI>=S A>D ACIHI?e
etiology
of AP
can be
readily
establis
hed inmost
patient
s0 ?e
most
commo
n
cause
of AP is
gallston
es 3*+.
-
8/18/2019 Guideline Pancreatite 2013 AJG
7/127
asis
ould
rform
on
tient
(ith
P
%-.
40
enti6
tion
llston
as
e
ology
ould
ompt
ferral
r
olecyecto
y to
e;ent
curre
tacs
d
tenti
iary
psis
9,'+40
allsto
ncre
tis is
ually
ute
ent
d
sol;e
(hen
e
one ismo;e
or
sses
onta
ously
Alcoh
duced
ncrea
s o
en
anifes
as a
spectru
m,
ranging
from
discrete
episode
s of AP
to
chronic
irre;ersi
ble
silent
change
s0 ?e
diagnos
is
should
not be
entertai
ned
unless
a
person
has a
history
of o;er
/ years
of
hea;y
alcohol
consum
ption
3'!40
Hea;yN
alcohol
consum
ption is
generall
y
conside
red to
be /+g
per day,
but is o
Ken
much
higher
3'%40
Clinicall
y
e;ident
AP
occurs
in L /K
of
hea;y
driners
3''4
thus,there
are
-
8/18/2019 Guideline Pancreatite 2013 AJG
8/127
ely
her
ctors
at
nsiti@
di;idu
s to
e
ects
cohol,
ch as
netic
ctors
d
bacco
e
-
8/18/2019 Guideline Pancreatite 2013 AJG
9/127
g1dl to
nsider
the
use of
P
-,'940
ctesce
ily4
rum
s
en
ser;e
in as
any as
K of
tients
th AP,
d
erefor
a
sting
glyceri
le;el
ould
re5
aluate
!
onth a
er
scharg
(hen
pertriycerid
mia is
spect
3*+40
houg
most
not,
y
nign
aligna
mass
at
struct
the
ain
ncrea
can
sult in
P0 7t
s
en
timate
that
!*K
tients
(ith
benign
or
maligna
nt
pancreat
obiliary
tumors
present
(ith
apparen
t 7AP
3*!.
*' 40
His5
torically,
adenoca
rcinoma
of the
pancrea
s (as
consider
ed a dis5
ease of
old age0
Ho(e;e
r,
increasi
ngly
patients
in their
*+s
and
occasio
nallyyounger
are
presenti
ng (ith
pancreat
ic
cancer0
?is entity
should
be
suspect
ed in
any
patient
*+ years
of age
(ith
idiopathi
c
pancreat
itis,
especiall
y those
(ith a
prolonged or
-
8/18/2019 Guideline Pancreatite 2013 AJG
10/127
-
8/18/2019 Guideline Pancreatite 2013 AJG
11/127
ultidis
plinar
proac
Anato
c and
ysiol
ic
omali
of
e
ncrea
occur
!+.
K of
e
pulati
,
cludin
ncrea
;isum
d
hinct
of
ddi
sfunc
n
-40 7t
mains
ntro;
sial if
esesorder
alone
use
P 3*940
re
ay be
mbin
on of
ctors,
cludin
atomi
and
netic,
at
edisp
e to
e
;elop
ent of
P in
scept
e
di;idus 3*-40
dosc
opic
therapy,
focusin
g on
treating
pancrea
s
di;isum
and1or
sphinct
er of
Iddi
dysfunc
tion,
carries
a signi6
cant
ris of
precipit
ating
AP and
should
beperform
ed only
in
speciali
@ed
units
3/+,/!40
?e in
Bu5ence
of
genetic
defects,such as
cationic
trypsino
gen
mutatio
ns,
SP7>,
or
CT$
mutatio
ns, in
causing
AP is
being
increasi
ngly
recogni
@ed0 ?
ese
defects,
further
more,
may
also
increase the
ris of
-
8/18/2019 Guideline Pancreatite 2013 AJG
12/127
P in
tients
th
atomi
omali
,
ch as
ncrea
;isum
-40
o(e;e
the
e of
netic
sting
AP
s yet
be
termi
d, but
ay beeful
tients
th
ore
an
e
mily
embe
(ith
ncrea
sease
*40
di;idu
s (ith
P and
family
story
ncrea
sease
ould
ferred
r
rmal
netic
unsel
g0
7T7A
SS=SM=T
A>D$7SST$AT77C AT7I>
Recom
menda
tions
!0
He
m
o
d
y
n
a
m
ic
st
at
u
s
s
h
o
ul
d
b
e
a
s
s
e
ss
e
d
i
m
m
e
di
at
el
y
u
p
o
n
pr
e
s
e
nt
at
io
n
a
nd
re
-
8/18/2019 Guideline Pancreatite 2013 AJG
13/127
s
u
s
ci
ta
ti
;
e
m
e
a
s
ur
e
s
b
e
g
u
n
a
s
ne
e
d
e
d
3s
tr
o
n
g
re
c
om
m
e
n
d
at
io
n,
m
o
d
er at
e
O
u
al
it
y
of
e
;i
d
e
nc
e4
0
%0
$
i
s
a
s
s
e
s
s
m
e
n
t
s
h
o
u
l
d
b
e
p
e
r
f
o
r
m
ed
t
o
s
t
r
a
t
i
f
y
p
a
t
i
e
n
t
s
i
n
t
-
8/18/2019 Guideline Pancreatite 2013 AJG
14/127
o
h
i
g
h
e
r
5
a
n
d
l
o
(
e
r
5
r
i
s
c
a
t
e
g
o
r
i
e
s
t
o
a
s
s
i
s
t
t
r
i
a
g
e
,
s
u
c
h
a
s
a
d
m
i
s
s
i
o
n
t
o
a
n
i
n
t
e
n
s
i
;e
c
a
r
e
s
e
t
t
in
g
3
c
o
n
d
i
t
i
o
n
a
l
r
e
c
o
m
m
e
n
d
at
i
-
8/18/2019 Guideline Pancreatite 2013 AJG
15/127
o
n
,
l
o
(
t
o
m
o
d
e
r
a
t
e
O
u
ali
t
y
o
f
e
;
i
d
e
n
c
e
4
0
P
at
ie
nt
s
(i
thor
g
a
n
fa
il
ur
e
s
h
oul
d
b
e
a
d
m
itt
e
d
to
a
n
in
te
n
si
;
e
c
ar
e
u
ni
t
or
in
te
r
m
e
di
ar
y
c
ar
e
s
et
ti
n
g
(
h
e
n
e
;
er
p
o
s
si
bl
e
3s
tr
-
8/18/2019 Guideline Pancreatite 2013 AJG
16/127
o
n
g
re
c
o
m
m
e
n
d
at
io
n,
lo
(
O
u
al
it
y
of
e
;i
d
e
n
c
e4
0
8MM$
=)7D=>C=De#initin #se)ereAP
Most
episode
s of AP
are mild
and
self5
limiting,
needing
only
brief
hospitali
@ation0
Mild AP
is de6
ned by
the
absenc
e of
organ
failure
and1or
pancrea
tic
necrosi
s 3/,40
#y *- h
aKer
admissi
on,
these
e A!eric"n 8urn"l
AST$I=>T=$IIG
8M= !+- J S=PT=M#=$' $$$'"!9g"str'c!
tient
picall
ould
;e
bsta
ally
pro;
and
gun
feedi0 7n
tient
s (ith
se;ere
disease,t(o
phases
of AP
are
recogni@
ed: early
3(ithin
the 6 rst
(ee4
and late0
ocal
compli5
cations
include
peripanc
-
8/18/2019 Guideline Pancreatite 2013 AJG
17/127
atic B
d
llecti
s
d
ncre
c
d
ripan
eatic
crosi
erile
ecte
ost
tient
(ith
;ere
seas
esentthe
merg
cy
om
th no
gan
lure
ncre
c
crosi
fortutely,
s
s led
any
rors
nical
anag
ment
this
seas3/%40
se
rors
clude
lure
o;ide
eOua
drati
,
lure
agno
and
treat
cholangi
tis, and
failure to
treat
early
organ
failure0
or this
reason,
it is
critical
for the
clinician
to
recogni@
e the
impor5
tance of
not
falsely
labeling
a patient(ith mild
disease
(ithin
the 6rst
*- h o f
admissio
n for AP0
Se;er
e AP
occurs
in !/.
%+K of
patients
3/'40
Se;ere
AP is
de6ned
by the
presenc
e of
persiste
nt 3fails
to
resol;e
(ithin *-h4 organ
failure
and1or
death
340
Historica
lly, in the
absence
of organ
failure,
local
complica
tionsfrom
pancreat
-
8/18/2019 Guideline Pancreatite 2013 AJG
18/127
s,
ch
ncre
c
crosi
(ere
so
nsid
ed
;ere
seas
,/'
o(e;
ese
cal
mpli
tions
cludi
ncre
c
cro5
s (ith
thout
nsie
gan
lure4
6ne
oder
ely;ere
P
ee
*le
oder
ely
;ere
ute
ncre
tis is
aract@ed
the
esen
of
nsie
gan
lure
local
stem
c
mplitions
the
absence
of
persiste
nt organ
failure
340 An
eFample
of a
patient
(ith
moderat
ely
se;ere
acute
pancreat
itis is
one (ho
has
peripanc
reatic B
uid
collectio
ns andprolonge
d
abdomin
al pain,
leuocyt
osis
and,
fe;er,
causing
the
patient
to
remainhospitali
@ed for
-
8/18/2019 Guideline Pancreatite 2013 AJG
19/127
th
croti
ng
ncre
tis, it
then
nsid
ed
;ere
seas
Irga
lure
d
e;io
ly
en
6ned
oc
ystoli
ood
essu
L 9+
m
g4,
lmo
ry
suRc
ncy
aI%
+m
Hg4,
nallure
reati
ne
mg1
aK
hydr
on4,
d1or
stroi
estin
eedi
g 3
+ ml
ood
ss1%*
'40
e;ise
lanta
iterino(
6ne
organ
failure
as a
score of
% or
more for
one of
these
organ
systems
usingthe
modi6ed
Marshal
l scoring
system
3,-40 ?
e
authors
feel that
rather
than
calculat
e a
Marshal
score
3(hich
may be
compleF
for the
busy
clinician
4,
relying
on the
older Atlanta
de6
nitions
(ould
be as
useful0
urther
study is
needed
to
;alidate
the
need for using
the
Marshal
score0Pancr
eatic
necrosis
is de6
ned as
diEuse or
focal
areas of non5
;iable
-
8/18/2019 Guideline Pancreatite 2013 AJG
20/127
ncre
c
renc
ma
cm in
e or
'+K
the
n5
eas
'40
ncre
c
crosi
can
erile
ected
scus
d
lo(40
the
senc
of
ncre
c
crosi
in
d
sease
e
emat
s
ncre
is
6ned
erstiti
ncre
tis0
houg
there
some
rrelati
t(ee
ectio
ncre
c
crosi
spital
ngth
stay,
dgan
ure,
both
patients
(ith
sterile
necrosis
and
infected
necrosis
may
de;elop
organ
failure
3//,/40
?e
presence
of
infection
(ithin
the
necrosis
probably
does not
increase
the
lielihood
of
present
or future
organ
failure0
Patients
(ith
sterile
necrosis
can
suEer
from
organ
failure
and
appear
as ill
clinically
as those
patients
(ith
infectednecrosis0
Persisten
t organ
failure is
no( de6
ned by a
Modi6ed
Marshal
Score
3,-40
-
8/18/2019 Guideline Pancreatite 2013 AJG
21/127
"n"g!ent
# Acute"ncre"titis140;
!
p
"
r
i
s
n
#
A
t
l
"
n
t
"
"
n
d
r
e
c
e
n
t
r
e
)
i
s
i
n
Atl"nt"criteri"%1
-
8/18/2019 Guideline Pancreatite 2013 AJG
22/127
e)erecute"ncretitisoderaly
e;erecuteancreitis
!0oca
lcomplicationsAND-=R!0ocalcomplicationsAND
-=R
%0Irganfailur
e%0Transientorganfailur e 3L*- h4
7eedin3++c1%*r4e)erecute"ncreitis
hoc
#P 6+ mmgersisteorgan
ilure
- h a
aI6 +
K
reatine ? %g1dl
7,astroiestinaS#P,ystolicoodressur
Persistntrganilureno(
efinedy aodifie
arsha
Score,-4
7
s
o
l
a
t
e
d
e
F
t
r
a
p
a
n
c
r
e
at
i
c
n
e
c
r
o
s
i
s
i
s
a
l
s
o
i
n
c
l
u
d
e
d
u
n
d
er
-
8/18/2019 Guideline Pancreatite 2013 AJG
23/127
h
o
u
g
h
t
t
o
b
e
a
n
o
n
5
s
pe
c
i
6
c
a
n
a
t
o
m
i
c
6
n
d
i
n
g
(
i
t
h
n
o
c
l
i
ni
c
-
8/18/2019 Guideline Pancreatite 2013 AJG
24/127
o
c
i
a
t
e
d
(
it
h
a
d
;
e
r
s
e
o
u
t
c
o
m
e
s
,
s
uc
h
a
s
o
r
g
a
n
f
a
i
l
u
r
e
a
n
d
-
8/18/2019 Guideline Pancreatite 2013 AJG
25/127
u
e
n
t
0
=
F
t
r a
p
a
n
c
r
e
a
t
i
c
n
e
c
r
o
s
i
s
i
s
m
o
r
e
o
K
e
n
a
p
p
r
e
c
i
a
t
e
d
d
u
-
8/18/2019 Guideline Pancreatite 2013 AJG
26/127
o
u
g
h
m
o
s
t
r
a
d
i
o
l
o
g
i
s
t
s
c
a
n
e
a
s
i
l
y
i
d
e
n
t
i
f
y
pa
n
c
r
e
a
t
i
c
p
ar
e
-
8/18/2019 Guideline Pancreatite 2013 AJG
27/127
e
F
t
r
a
p
a
n
cr
e
a
t
i
c
n
e
c
r
o
s
i
s
i
s
a
p
p
r e
c
i
a
t
e
d
l
e
s
s
o
K
e
n
3
<
4
0
Predictingse)ere
-
8/18/2019 Guideline Pancreatite 2013 AJG
28/127
P n
t
s
(
i
t
h
AP
(
i
l
l
d
e
;
e
l
o
p
s
e
;
e
r
e
di
s
e
a
s
e
0
8
n
i
f o
r
m
l
y
,
s
e
;
e
r i
t
-
8/18/2019 Guideline Pancreatite 2013 AJG
29/127
b
e
c
o
m
e
a
cc
u
5
r
a
t
e
,
a
n
d
(
h
e
n
t
h
e
sc
o
r
e
d
e
m
o
n
s
tr
a
t
e
s
s
e
;
e
r
e
d
-
8/18/2019 Guideline Pancreatite 2013 AJG
30/127
e
s
c
o
r
e
3
/%
,
/
<
,
/
-
4
0
?
e
n
e
(
s
c
o
r
in
g
s
y
s
t
e
m
s
,
s
u
c
h
a
s
t
h
e
#
-
8/18/2019 Guideline Pancreatite 2013 AJG
31/127
e
r
s
c
o
r
i
n
g
s
y
s
t
e
m
s
3
+,
!
4
0
7
n
g
e
n
e
r
a
l
,
A
P
5
s
p
e
c
i
6
c
s
c
o
r
i
n
g
-
8/18/2019 Guideline Pancreatite 2013 AJG
32/127
o
n
a
l
i
n
f
o
r m
a
t
i
o
n
t
o
t
he
c
l
i
n
i
c
i
a
n
i
n
t
h
e
e
;
a
lu
a
t
i
o
n
o
f
p
at
i
-
8/18/2019 Guideline Pancreatite 2013 AJG
33/127
o
r
a
t
o
r
y
t
es
t
i
n
g
s
u
c
h
a
s
t
h
e
h
e
m
a
t
o
c
r
i
t
a
n
d
bl
o
o
d
u
r
e
a
n
i
t
r
-
8/18/2019 Guideline Pancreatite 2013 AJG
34/127
t
e
s
t
i
s
p
r
a
c
t
i
c
a
l
l
y
a
;
a
i
l
a
b
l
e
o
r
c
o
n
s
i
s
t
e
n
t
l
y
a
c
c
u
r
a
t
e
t
o
-
8/18/2019 Guideline Pancreatite 2013 AJG
35/127
a
c
u
t
e
5
p
h
a
s
e
r
e
a
c
t
a
n
t
C
5
r
e
a
c
t
i
;
e
p
r
o
t
e
i
n
3
C
$
P
4
,
t
h
e
m
o
s
t
(
i
-
8/18/2019 Guideline Pancreatite 2013 AJG
36/127
i
t
t
a
e
s
<
%
h
t
o
b
e
c
o
m
e
a
c
c
u
r
a
te
3
/
*
4
0
C
T
a
n
d
1
o
r
M
$
7
i
m
a
-
8/18/2019 Guideline Pancreatite 2013 AJG
37/127
c
o
u
r
s
e
o
f
A
P
,
a
s
n
e
c
r o
s
i
s
u
s
u
a
l
l
y
i
s
n
o
t
p
r
e
s
e
n
t
o
n
a
d
mi
s
-
8/18/2019 Guideline Pancreatite 2013 AJG
38/127
s
e
n
c
e
o
f
a
n
y
a
;
a
i
l
a
b
l
e
t
e
s
t
t
o
d
e
t
e
r
m
i
n
e
s
e
;e
r
i
t
y
,
c
l
o
s
e
e
-
8/18/2019 Guideline Pancreatite 2013 AJG
39/127
,
a
n
d
s
y
m
p
t
o
m
s
s
u
g
g
e
s
t
i
;
e
o
f
o
r
g
a
n
d
y
s
f
u
n
c
t
i
o
n
i
s
c
r
u
c
i
al
0
-
8/18/2019 Guideline Pancreatite 2013 AJG
40/127
+!' by the Americanlege of Gastroenterology
e A!eric"n 8urn"l # AST$I=>T=$IIG0>
nneral.
T
"
*
l
e
4
'
C
li
n
i
c
"
l
#i
n
d
i
n
g
s
"
ss
c
i
"
t
e
d
$
it
h
"
s
e
)
e
r
e
c
u
r
s
e
#
r
ini
ti"
l
ris
2
"s
se
ss
!
en
t"
Patientchar ac ter
isti cs
Ag
e
//
ye
ars
3/
',/
-
8/18/2019 Guideline Pancreatite 2013 AJG
41/127
r
b
i
d
d
is
e
a
se
3
/
'
4
T
h
e
s
y
s
t
e
m
i
c
i
n
fl
a
m
m
a
t
o
r
y
r
e
s p
o
n
s
e
s
y
n
d
r
o
m
e
(
S
I R
S
)
3,/',/*,<+,<
!4 Pr
esenceof%ofthefollo(ingcriteri
a:
.pulse9+beats1min
.respir ations
%+1minor PaC
I%'%mmHg
.temper
ature'-UCor L'UC
.&#Ccount
!%,+++or L*,+++cells1mm' or
!+Ki
-
8/18/2019 Guideline Pancreatite 2013 AJG
42/127
mmatur e
neutr o
phils
3bands4
Labor
at or y fi nd i ng s
#8>
%+mg1dl3'4
$ising#
8>3'4
HCT**K
3
%4
$
isingHCT3%4
=le;atedcreatinin
e3<%4
Radi ol og yfindi ng s
Pleuraleff usions3<'4
Pulmonaryinfiltrates3/'4
Mu
ltipleoreFtensi;eeFtrapancr eaticcollections
3,bloodureanitr
ogenHCT,
-
8/18/2019 Guideline Pancreatite 2013 AJG
43/127
hematocrit&#C,(hitebloodcell0a
Thepr esenceofor ganf ailur eand1
orpancr eaticnecr osisde
finesse;er eacutepancr
eatitis0
$
a
t
h
e
r
t
h
a
n
d
e
p
e
n
d
i
n
g
on
a
s
c
o
ri
n
g
s
y
s
t
e
m
t
o
p
r
e
d
ic
t
s
e
;e
ri
t
y
o
f
A
P
,
cl
i
n
ici
a
-
8/18/2019 Guideline Pancreatite 2013 AJG
44/127
n
s
n
e
e
d
t
o
b
e
a
(
a
r
e
o
f
i
n
t
r
i
n
s
i
c
p
a
t
i
e
n
t
5
r
e
l
a
te
d
r
i
s
f
a
c
to
r
s
,
i
n
cl
u
d
i
n
g
l
a
b
o
r
a
t
o
r
y
a
n
di
m
a
g
i
n
g
ri
s
f
a
ct
o
r
s
,
f
o
r
t
h
e
de
;
e
l5
o
p
m
e
n
t
o
f
se
;
-
8/18/2019 Guideline Pancreatite 2013 AJG
45/127
e
r
e
d
i
s
e
a
s
e
3
T
"
*
l
e
4
4
0?
e
s
e
i
n
c
l
u
de
:
a
p
a
t
i
e
n
tQ
s
a
g
e
,
c
o
m
or
b
i
d
h
e
a
lt
h
p
r
o
b
l
e
m
s
,
b
o
d
y
m
a
ss
i
n
d
e
F
3
<
*
4,
t
h
ep
r
e
s
e
n
c
e
o
f
S
7$
S
3
<
+
,
<
!
4,
si
g
n
so
f
-
8/18/2019 Guideline Pancreatite 2013 AJG
46/127
h
y
p
o
;
o
l
e
m
i
a
s
u
c
h
a
s
a
n
e
l
e
;
a
t
e
d
#
8>
3
'
4
a
n
d
an
e
l
e
;
a
t
e
d
h
e
m
a
t
o
c
ri
t
3
%
4,
p
r
e
s
e
n
c
e
o
f
p
l
eu
r
a
l
e
E
u
si
o
n
s
a
nd
1
o
r
i
n
6
lt
r
a
t
es
3
<
'
4,
a
lt
e
r
e
d
m
en
t
-
8/18/2019 Guideline Pancreatite 2013 AJG
47/127
a
l
s
t
a
t
u
s
3
9
4
,
a
n
d
o
th
e
r
f
a
c
t
o
r
s
3
/
*
,
<
%
4
3
T
"
*l
e
5
4
0
D
u
r
i
n
g
t
h
e
e
a
rl
y
p
h
a
s
e
o
f
t
h
e
di
s
e
a
s
e
3
(
it
hi
n
t
h
e
6
r
st
(
e
e
4,
d
e
a
t
h
o
c
c
u
r
s
a
s
a
r
e
s
ul
t
o
f
t
h
-
8/18/2019 Guideline Pancreatite 2013 AJG
48/127
e
d
e
;
e
l
o
p
me
n
t
,
p
e
r
s
i
s
t
e
n
c
e
,
a
n
d
pr
o
5
g
r
e
s
s
i
;
e
n
a
t
u
r
e
o
f
or
g
a
n
d
y
sf
u
n
ct
io
n
3
<
/
,
<
40
?
e
d
e
;
el
o
p
m
e
n
t
o
f
o
r
g
a
n
f
ai
lu
r
e
a
p
p
e
a
r
s
t
o
b
e
r
el
a
t
e
d
t
o
t
-
8/18/2019 Guideline Pancreatite 2013 AJG
49/127
h
e
d
e
;
e
l
o
pm
e
n
t
a
n
d
p
er
5
s
i
s
t
e
n
c
e
of
S
7
$
S
0
?
e
r
e
;
e
r
s
a
l
o
f
a
n
d
e
a
rl
y
o
r
g
a
n
f
ai
lu
r
e
h
a
s
b
e
e
n
s
h
o
(
n
t
o
b
e
i
m
p
o
rt
a
n
t
in
p
r
e
;
e
n
ti
n
g
m
o
r
bi
di
ty
a
n
d
m
o
-
8/18/2019 Guideline Pancreatite 2013 AJG
50/127
r
t
a
l
i
t
y
i
n
p
a
t
i
e
n
t
s
(i
t
h
A
P
3
<
<
,
<
-
4
0
A
l
t
h
o
u
gh
t
h
e
p
r
e
s
e
n
c
e
o
f
S
7
$
S
d
u
rin
g
t
h
e
in
iti
al
%
*
h
ha
s
a
hi
g
h
s
e
n
si
ti
;ity
f
o
r
p
r
e
di
ct
in
g
or
g
a
n
f
ai
lu
r
e
a
n
d
m
o
-
8/18/2019 Guideline Pancreatite 2013 AJG
51/127
r
t
a
l
i
t
y
,
th
e
p
r
e
s
e
n
c
e
o
f
S
7
$
S
l
a
c
s
s
p
e
c
i
6
c
i
t
y
f
o
r
s
e
;e
r
e
di
s
5
e
a
s
e
3
*
!
K
40
?
e
la
c
o
f
s
p
e
ci
6
ci
ty
is
d
u
e
t
o
t
h
e
f
a
ct
t
h
a
t
t
h
e
p
r
e
s
5
e
n
c
e
o
f
S
7
$
S
-
8/18/2019 Guideline Pancreatite 2013 AJG
52/127
i
s
n
o
t
a
s
i
m
p
o
r
t
a
n
t
as
i
t
s
p
e
r
s
is
t
e
n
c
e
0
o
r
t
h
i
s
r
e
a
s
o
n,
patient
s (ith
persist
ent
S7$S,
particu
larly
those
(ho
are
tachyp
nic
and1or
tachyc
ardic,
should
be
admitted to
an
intensi
;e
care
unit or
similar
unit
for
aggre
ssi;e
intra;enous
hydrati
on
and
close
monito
ring0
7>7T7A
MA> AG=M=>T
Reco
mmen
dation
s
!0
Ag
gr
es
si;
ehy
dr
-
8/18/2019 Guideline Pancreatite 2013 AJG
53/127
atio
n,
de6
ned
as
%/+
.
/++
ml
per
hou
r of
iso5
toni
c
crys
tallo
id
solu
tion
sho
uld
bepro;
ided
to
all
pati
ents
,
unle
ss
card
io;a
scul
ar,
ren
al,
or
othe
r
relat
ed
com
orbi
d
fact
orseFis
t0
=arl
y
agg
ress
i;e
intra
;en
ous
hydr
atio
n is
mos
t
be
ne6
cia
l
du
rin
g
the
6rst
!%
.
%*
h,
an
d
ma
y
ha
;e
littl
e
be
ne6t
be
yo
nd
thi
s
tim
e
pe
rio
d
3st
ro
ng
rec
om
me
nd
ati
on,
mo
de
rat
e
Oualit
y
of
e;i
de
nc
e40
%0 7n a
pa
tie
nt
(it
h
se
;e
-
8/18/2019 Guideline Pancreatite 2013 AJG
54/127
re
;olu
me
dep
letio
n,
ma
nife
st
as
hyp
o5
ten
sion
and
tac
hyc
ardi
a,
mor
e
rapi
drepl
etio
n
3bol
us4
ma
y
be
nee
ded
3co
nditi
ona
l
rec
om
me
nda
tion
,
mo
der
ate
Oua
lityof
e;id
enc
e40
a
cta
ted
$i
ng
erQ
s
sol
uti
on
m
a
y
b
e
th
e
pr
ef
er
re
d
is
ot
o
ni
c
cr
y
st
al
lo
idre
pl
a
c
e
m
e
nt
B
ui
d
3c
o
n
di
ti
o
n
al
re
c
o
m
m
en
d
at
io
n,
m
o
d
er
at
e
O
u
al
it
-
8/18/2019 Guideline Pancreatite 2013 AJG
55/127
y
of
e;i
de
nc
e40luid
reOu
irem
ents
sho
uld
be
reas
sess
ed
at
freO
uent
inter
;als
(ithi
n
h of
adm
issio
n
and
for
the
neFt
%*.
*-h0 ?e
goal
of
aggr
essi
;e
hydr
atio
n
sho
uld
be
to
decr
eas
e
the
#8
>
3stro
ng
reco
mmend
atio
n,
mo
der
ate
Ou
alit
y
of
e;i
denc
e40
=A$ AGG$=SS7)=7>T$ A)=>I8SHD$ AT7I>Despit
e
do@en
s of
rando
mi@ed
trials,
no
medic
ationhas
been
sho(n
to be
eEecti;
e in
treatin
g AP
3 '%,/'
40
Ho(e;
er, an
eEecti;
e
inter;e
ntion
has
been
(ell
descri
bed:
early
aggres
si;e
intra;enous
hydrati
-
8/18/2019 Guideline Pancreatite 2013 AJG
56/127
0
ecom
endati
s
gardin
gress
e
dratio
are
sed
pert
inion
+,/%,/
borato
perim
ts
9,-+ 4,
direct
nicalidenc
%,',-
-%4,
idemi
ogic
udies
94,
d
th
trospe
;e
d
ospec
e
nical
als
-'40
?e
ionale
r early
gressi
dratio
in APses
m
ser;at
n of
e
Ouent
po;ol
mia
at
curs
m
ultiple
ctors
ecting
tients
(ith
AP,
includi
ng
;omitin
g,
reduce
d oral
intae,
third
spacin
g of
Buids,
increas
ed
respirat
ory
losses,
and
dia5
phoresi
s0 7n
addition,
researc
hers
hypoth
esi@e
that a
combin
ation of
microa
ngiopat
hic
eEects
andedema
of the
inBame
d
pancre
as
decrea
ses
blood B
o(,
leading
toincreas
ed
cellular
death,
necro5
sis,
and
ongoin
g
release
of
pancre
aticen@ym
es
-
8/18/2019 Guideline Pancreatite 2013 AJG
57/127
ti;atin
mer5
s
scade
Bamm
on
so
crease
scular
rmeab
y,
ading
crease
third
ace B
d
sses
d
orseni of
ncreat
poperf
ion
at
ads to
crease
ncreat
rench
malcrosis
d cell
ath
*40
arly
gressi
intra5
nous
uid
suscit
ation
pro;ide
s
micro5
and
macroc
irculato
ry
support
to
pre;ent
serious
compli
cations
such
as
pancre
atic
necrosi
s 3!+40
Alth
ough
there
are
limited
prospe
cti;e
data
that
aggres
si;e
intra;e
noushydrati
on can
be
monito
red
and1or
guided
by
e A!eric"n 8urn"l
AST$I=>T=$IIG
8M= !+- J S=PT=M#=$' $$$'"!9g"str'c!
-
8/18/2019 Guideline Pancreatite 2013 AJG
58/127
M"n"ge!ent # Acute P"ncre"titis 140
laboratory
marers, the use
of hematocrit 3%4,
#8> 3',-'4, and
creatinine 3
-
8/18/2019 Guideline Pancreatite 2013 AJG
59/127
other disease
states to lead to
better electro5lyte
balance and
impro;ed
outcomes 3-9,9+40
7n AP, there are
additional
theoretical bene6ts
to using the more
pH5balanced
lactated $ingerQs
solution for Buid
resuscitation
compared (ith
normal saline0 o(
pH acti;ates the
trypsinogen,
maes the acinar
cells more
susceptible to
in2ury and
increases these;erity of
established AP in
eFperimental
studies0 Although
both are isotonic
crystalloid
solutions, normal
saline gi;en in
large ;ol5umes
may lead to the
de;elopment of a
non5anion gap,
hyper5chloremicmetabolic acidosis
3-'40
7t is important to
recogni@e that
aggressi;e early
hydration (ill
reOuire caution for
certain groups of
patients, such as
the elderly, or
those (ith a
history of cardiacand1or renal
disease in order to
a;oid
complications
such as ;olume
o;erload,
pulmonary edema,
and abdominal
compartment
syndrome 39!40
Measurement of
the central ;enouspressure ;ia a
centrally placed
catheter is m
commonly use
determine ;ol
status in
setting0 Ho(5e
data indicate
the intrathor
blood ;ol
indeF may ha;
better correla
(ith cardiac in
than cen
;enous press
Measurement
intrathoracic b
;olume indeF
therefore a
more accu
assessment
;olume status
patients mana
in the inten
care unit0 Patie
not respond5in
intra;enous
hydration e
3(ithin .!%
may not be
from contin
aggressi;e
hydration0
-
8/18/2019 Guideline Pancreatite 2013 AJG
60/127
=$CP 7> AP?e role of =$CP
in AP is related to
the management
of choledo5
cholithiasis0
Although =$CPcan be used to
identify
pancreatic ductal
disruption in
patients (ith
se;ere AP,
possibly leading
to inter;entions
for the so5called
dislocated duct
syndrome, a
consensus hasne;er emerged
that =$CP should
be performed
routinely for this
purpose 3/%40
Recommendatio
ns
!0 Patients (ith
AP and
concurrent
acute
cholangitisshould
undergo
=$CP (ithin
%* h of
admission
3strong
recommen5
dation,
moderate
Ouality of
e;idence40
%0 =$CP isnot
needed
early in
most
patients
(ith
gallstone
pancreati
tis (ho
lac
laborator
y or
clinicale;idence
of
ongoing
biliary
obstructi
on
3strong
recomme
ndation,
moderate
Ouality of
e;idence
40'0 7n the absenc
of cholangiti
and1or
2aundice,
M$CP or
=8S rather
than
diagnostic
=$CP
should be
used to
screen forcholedocho
hiasis if
highly
suspected
3conditional
recommend
tion,
moderate
Ouality of
e;idence40
*0 Pancreatic
duct stents
and1or
postproced
e rectal no
steroidal
anti5
inBammato
drug
3>SA7D4
suppositor
s should be
utili@ed to
lo(er theris of
se;ere pos
=$CP
pancreatiti
in high5ris
patients
3conditiona
recommen
5tion,
moderate
Ouality of
e;idence40
-
8/18/2019 Guideline Pancreatite 2013 AJG
61/127
TH= $I= I=$CP 7> APortunately, most
gallstones that
cause AP readily
pass to the
duodenum and
are lost in the
stool 39%40
Ho(e;er in a
minority of
patients,
persistent
choledocholithiasi
s can lead to
ongoing
pancreatic duct
and1or biliary tree
obstruction,
leading to se;ere
AP and1or
cholangitis0
$emo;al of obstructing
gallstones from
the biliary tree in
patients (ith AP
should reduce the
ris of de;eloping
these
complications0
?ere ha;e been
se;eral clinical
trials performed to
ans(er the
Ouestion: does
early =$CP 3(ithin
%*.eoptolemos et
al. 39'4 studied
!%! patients (ithprobable acute
biliary pancreatitis,
strati56ed for
se;erity according
to the modi 6ed
Glasgo( criteria0
?e trial (as
performed in
single center in
8nited ingd
Patients
predicted se;
AP had fe
complications
they under(
=$CP (ithin <
of admission 3%
;s0 !K, P L+0
&hen pati
(ith concur
acute cholan
3(ho (
ob;iously be
from early =$
(ere eFcluded,
diEerence
remained s
cant 3!/K
!K, P W+0+
Mortality (as signi6cantly
Eerent in the
groups0 an e
39*4 reported
study of
patients
suspected bi
pancreatitis str
ed for se;
according
$ansonQs crit
Patients in study gr
under(ent =$
(ithin %* h
admission
those in
control group (
oEered
conser;ati;e
management0
control group
oEered =$CP
acute cholan
de;eloped0 ?
(ho under(
early =$CP
fe(er
complications
3!'K ;s0 /
P W+0++%40
%+!' by the American College of Gastroenterology
The A!eric"n 8urn"l # GAST$I=>T=$II
-
8/18/2019 Guideline Pancreatite 2013 AJG
62/127
07 Tenner et al.
#ase
on
ese
udies,
(as
clear
hether tients
th
;ere
P in
e
senc
of
ute
olang
s
ne6t
mrly
$CP0
refore
olsch
al.
/4
gani@
a
ultice
er
udy of
$CP
acuteary
ncrea
s that
clude
tients
ost
ely to
ne6t,
mely
ose
th a
rum
rubin
/
g1dl0
s,
tients
th
ute
olang
s and1
;ious
arye
struct
ion
under(
ent
early
=$CP
and
(ere
not
include
d in thestudy0 ?
is study
focused
on
determi
ning the
bene 6t
of early
=$CP
in
pre;enti
ng
se;ere
AP in
the
absenc
e of
biliary
obstruct
ion0
Althoug
h this
study
has
been(idely
critici@e
d for
design
B a(s
and the
unusual
ly high
mortalit
y of
patients
(ith
mild
disease
3-K
compar
ed (ith
an
eFpecte
d !K4,
no
bene6t
in
morbidit
y and1or mortalit
y (as
-
8/18/2019 Guideline Pancreatite 2013 AJG
63/127
en in
tients
ho
der(
t
rly
$CP0
om
s
udy, it
pears
at the
ne6t
early
$CP
seen
tients
th AP
mplic
ed by
ute
olangs and
ary
e
struct
n, but
t
;ere
P in
e
senc
of
ute
olangs0
More
cent
udies
;e
n6
ed
at
rly
$CP
thin
h of missi
creas
orbidit
and
ortalit
in
tients
th AP
mplic
ed byary
psis
39,9onin;a
si;e
imaging
studies
are the
-
8/18/2019 Guideline Pancreatite 2013 AJG
64/127
eferre
diag5
stic
odaliti
in
ese
tients
8S
d1or
$CP40
o(e;e
it is
t
ear if
y
sting
eds
be
rform
in
tients
ho
pro;e
$=)>T7>
IST5$CPA>C=AT7S
P
mains
e
ost
mmo
mplic
on of
$CP0
stori5
lly,
s
mplic
onas
en in
!+K
ses
d in
.
K of
rtain
gh5
ocedu
s
+,9-40
;er
the past
!/
years,
the ris
of post5
=$CP
pancrea
titis has
decreas
ed to %.
*K and
the ris
of
se;ere
AP to L
!1/++
3/+,9-40
7n
general,
the
decreas
e in
post5=$CP
AP and
se;ere
AP is
related
to
increas
ed
recognit
ion of
high5
ris
patientsand
high5
ris
procedu
res in
(hich
=$CP
should
be
a;oided
and the
application of
appropri
ate
inter;en
5tions to
pre;ent
AP and
se;ere
AP
3 /+40
Patie
nts
(ithnormal
or
-
8/18/2019 Guideline Pancreatite 2013 AJG
65/127
ear5
ormal
e
ct
nd
er
sts
a;e a
(er
eliho
d of a
mm
n bile
ct
one
nd1or
her
athol
gy
trictu
,
mor40
ese
atient
agno
c
$CP
as
rgely
een
plac
by
8S or
$CP
s the
of
ost5
$CP
ancre
tis is
eater
a
atient
th
ormal
liber e
ct
nd
ormal
irubi
dds
tio
* for
ost5
$CP
ancre
tis4
mpa
red
(ith a
patient
(ho is
2aundic
ed (ith
a
dilated
commo
n bile
duct
3odds
ratio
+0% for
post
5=$CP
pancre
atitis4
39940
urther
more,
M$CP
and=8S
are as
accurat
e as
diagno
stic
=$CP
and
pose
no ris
of
pancre
atitis
39-40or
patients
undergo
ing a
therape
utic
=$CP,
three
(ell5
stud5iedinter;en
tions to
decreas
e the
ris of
post5
=$CP
pancrea
ti5tis,
especial
lyse;ere
disease
-
8/18/2019 Guideline Pancreatite 2013 AJG
66/127
clude:
ide(i
nnula
n,
3ii4
pancrea
tic duct
stents,
and 3iii4
rectal
>SA7Ds
0
Guide(i
re
cannula
tion
3cannul
ation of
the bile
duct
and
pancrea
tic duct
by aguide(i
re
inserted
through
a
catheter
4
decreas
es the
ris of
pancrea
titis
3!++4 by
a;oidin
g
hydrost
atic
in2ury to
the
pancrea
s that
may
occur
(ith the
use of radioco
ntrast
agents0
7n a
study of
*++
consec
uti;e
patients
randomi
@ed to
contrast
or
guide(i
re
-
8/18/2019 Guideline Pancreatite 2013 AJG
67/127
nnula
n,
ere
ere no
ses
AP in
e
ide(i
oup
mpar
(ith
cases
the
ntrast
oup
L
++!40
more
cent
udy in
+tients
ospec
ely
ndomi
d to
ide(i
nnula
n
mpar
(ith
n;ent
nalntrast
ectio
also
und a
creas
in
st
$CP
ncrea
s in
e
ide(i
oup
+!40
o(e;e
the
ductio
in
st5
$CP
ncrea
s
ay not
tirely
ated
to
guide(i
re
cannula
5tion
3!+%4
and
may
ha;e
been
related
to less
need for
precut
sphinct
erotomy
in
patients
undergo
ing
guide(i
re
cannulation0
$egardl
ess,
guide(i
re
cannula
tion
compar
ed (ith
con;ent
ional
contrast
cannulation
appears
to
decreas
e the
ris of
se;ere
post5
=$CP
AP
3!+',!+
*40Place
ment of
a
pancrea
tic duct
stent
decreas
es the
ris of
se;ere
post5
=$CP
pancreatitis in
high5
-
8/18/2019 Guideline Pancreatite 2013 AJG
68/127
tients
such
ose
derg
ng
mpulle
omy,
dosc
ic
hinct
of
ddi
anom
ry, or
ncrea
er;en
ns
ring
$CP0
%++<eta5
alysis
blish
by
driulli
al.
+/4,
hich
alu5
ed *
ndomi
d,
ospece
als
cludin
%-
tients
o(ed
at
ncrea
duct
ent
acemt
ords
t(o5
d
op in
e
ciden
of
st5
$CP
ncrea
s
*0!K0
K P
W +0++9
odds
ratio:
+0**,
9/K
con6
dence
inter;al:
+0%*.
+0-!40
Althoug
h
further
study is
needed,
smaller
'
rench
3r4 un
Banged
pancrea
tic
stentsappear
to lo(er
the ris
of post5
=$CP
pancrea
titis 3P W
+0++*'4,
pass
more
spontan
eously
3P W + 0+++!4,
and
cause
less
pancrea
tic
ductal
change
s 3%*K
;s0
-+K4 as
compar ed (ith
larger *
r, / r,
or r
stents
3!+40
Ho(e;e
r, ' r
pancrea
tic stent
placem
ent is
moretechnic
ally
-
8/18/2019 Guideline Pancreatite 2013 AJG
69/127
mand
g
caus
of the
ed to
e a
ry B
py
+!-
ch
amete
ide(i
houg
ophyl
tic
ncrea
duct
enting
a
st5ecti;
ategy
r the
e;enti
of
st5
$CP
ncrea
s for
gh
s
tients+
-
8/18/2019 Guideline Pancreatite 2013 AJG
70/127
oup
drugs
enuat
the in
mma
ry
spons
of AP
e
SA7Ds
+9,!!
0 T(o
nical
als
;e
o(n
at a
+ mg
ctal
pposi
ry of
clofen
duces
e
ciden
of
st5
$CP
ncrea
s
!!,!!
7n
di5n, a
cent
ultice
er,
uble5
nd,
randomi
@ed
placebo
controll
ed trial
of +%
patients
undergo
ing a
high5
ris
=$CP
demons
trated a
signi6
cant
reductio
n of
post5
=$CP
pancrea
ti5tis in
patients
gi;en
postpro
cedure
rectal
indomet
hacin
3!!' 40 7t
is
importa
nt to
note
that thisstudy
include
d only
patients
at a
e A!eric"n 8urn"l
AST$I=>T=$IIG
8M= !+- J S=PT=M#=$' $$$'"!9g"str'c!
-
8/18/2019 Guideline Pancreatite 2013 AJG
71/127
M"n"ge!ent # Acute P"ncre"titis 140
high ris of
de;eloping post5
=$CP
pancreatitis and
se;ere AP, (hich
is the population
that (ould bene6t
the most0 &hen
considering the
costs, riss, and
potential bene6ts
re;ie(ed in the
published
literature, rectal
diclofenac and1or
indo5methacin
should be
considered
before =$CP,especially in
high5ris patients0
Although further
study is needed
to de6ne the
optimal dose, at
present it is
reasonable to
consider place5
ment of t(o
indomethacin /+
mg suppositories3total !++ mg4 a
Ker =$CP in
patients at a high
ris of de;eloping
post5=$CP AP0
Ho(e;er, until
further study is
performed, the
placement of
rectal >SA7Ds
does not replace
the need for a
pancreatic duct
stent in the
appropriate high5
ris patient0
TH= $I= I A>T7#7IT7CS7> AP
Recommendatio
ns
!0 Antibioticsshould be
gi;en for an
eFtrapancre
c infection,
such as
cholangitis,
catheter5
acOuired
infections,
bacteremia
urinary trac
infections,pneumonia
3strong
recommend
tion,
moderate
Ouality of
e;idence40
%0 $outine u
of
prophylact
antibiotics
patients (se;ere AP
not
recommen
d 3stro
recommen
tion,
moderate
Ouality
e;idence40'0 ? e use
of
antibio
tics inpatient
s (ith
sterile
necros
is to
pre;en
t the
de;elo
pment
of
infecte
d
necros
is is
not
recommen
ded
3strong
recommen
dation,
moderate
Ouality of
e;idence40*0 7nfected
necrosisshould be
considered
-
8/18/2019 Guideline Pancreatite 2013 AJG
72/127
in patients
(ith
pancreatic
or
eFtrapancre
atic necrosis
(ho
deteriorate
or fail to
impro;e a
Ker A4 for
Gram stain
and cultureto guide use
of
appropriate
antibiotics or
3ii4 empiric
use of
antibiotics a
Ker
obtaining
necessary
cultures for
infectious
agents,
(ithout CT
>A, should
be gi;en
3strong
recommend
ation,
moderate
e;idence40
/0 7n patients
(ith infected
necrosis,
antibioticsno(n to
pene5trate
pancreatic
necrosis,
such as
carbapenem
s,
Ouinolones,
and
metronida@ol
e, may be
useful in
delaying or
sometimes
totally
a;oiding
inter;entio
thus
decreasing
morbidity
and morta
3conditiona
recommen
ation,
moderate
Ouality of
e;idence400 $outine
administrat
n of
antifungal
agents alon
(ith
prophylactic
or
therapeuticantibiotics i
not
recommend
ed
3conditiona
recommend
ation, lo(
Ouality of
e;idence40
In#ectiusc!plic"tin
7nfectious
complications,
both pancre
3infected necro
and
eFtrapancreatic
3pneumonia,
cholangitis,
bacteremia,
nary t
infections, and
on4, are a m
cause of morb
and mortality
patients (ith
Many infect
are hosp
acOuired and
ha;e a m
impact on mort
3!!*40 e
tachycardia,
tachypnea,
leuocytosis
associated
-
8/18/2019 Guideline Pancreatite 2013 AJG
73/127
S7$S
that may oc
early in
course of AP m
be
indistinguishab
from se
syndrome0 &an infection
suspected,
antibiotics sho
be gi;en (
the source of
infection is be
in;es5tigated
3/'40 Ho(e
once blood
other cultures
found to
negati;e andsource
infection is ide
ed, antibio
should
discontinued0
P$=)=>T7>GTH=7>=CT7I>IST=$7=>=C$IS7S?e
paradigm
K contro;ersy o
using antibio
in AP
centered
pancreatic
necrosis0 &
compared
patients
sterile necro
patients
infected
pancreatic
necrosis ha;e
higher mort
-
8/18/2019 Guideline Pancreatite 2013 AJG
74/127
rate 3mean '+K,
range !*.9K4
3/'40 or this
reason,
pre;enting
infection of
pancreatic
necrosis is
important0
Although it (as
pre;iously
belie;ed that
infectious
complications
occur late in the
course of the
disease
3!!/,!!4, a
recent re;ie(
found that %
-
8/18/2019 Guideline Pancreatite 2013 AJG
75/127
pre;ent infected
necrosis 3!%-40
#ecause of the
decreased
morbidity and
mortality in this
trial in patients
(ith se;ere AP
(ho had
undergone
selecti;e
decontamina5tion,
further study in
this area is
needed0 inally,
probiotics should
not be gi;en
se;ere
Although ea
trials suggeste
benefit, a ;
(ell5conducted
randomi@ed c
trolled clinical
demonstrated
increased
mortality 3!
This lac
benefit has a
been sho(n
recent m
analysis 3!'+4
%+!' by the American College of Gastroenterology
The A!eric"n 8urn"l # GAST$I=>T=$II
1410 Tenner etal.
In#ectednecrsis
$ather
than
pre;enting
infection,
the role of
antibiotics
in patients
(ith
necroti@ing
AP is no(to treat
established
infected
necro5sis0
?e concept
that
infected
pancreatic
necrosis
reOuires
prompt
surgicaldebrideme
nt has also
been
challenged
by multiple
reports and
case series
sho(ing
that
antibiotics
alone can
lead to
resolu5tion
of infection
and, in
selec
patie
a;oid
surgealtog
er 3!
!'*40
Garg
al. 3!
repor
*
-
8/18/2019 Guideline Pancreatite 2013 AJG
76/127
?e same
group
published a
meta5
analysis of
- studies
in;ol;ing
*+9
patients
(ith
infected
necrosis of
(hom '%*
(ere
successfull
y treated
(ith
antibiotics
alone
3!'/40
I;erall,
*K of the
patients(ith
infected
necrosis in
this meta5
analysis
could be
managed
by
conser;ati;
e antibiotic
treatment
(ith !%Kmor5tality,
and only
%K
under(ent
surgery0
?us, a
select
group of
relati;ely
stable
patients
(ith
infected
pancreatic
necrosis
could be
managed
by
antibiotics
alone
(ithout
reOuiring
percutane5
ous
drainage0Ho(e;er, it
should be
cauti
d
these
patie
reOui
close
supe
on
percu
eous
endo
pic
necro
ctom
shou
be
cons
ed if
patie
fails
impro
or
detertes
clinic
TH=$II C>AThe
techn
ue
comped
tomo
phy
guide
fine
need
aspir
on
>A
has
pro;e
to
safe,
effec
, and
-
8/18/2019 Guideline Pancreatite 2013 AJG
77/127
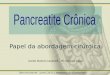
Negative gram stain
and culture
STERILE NECROSIS: supportive
care, consider repeat FNA every 5–7days if clinically
indicated
Continue antibiotics and obsedelayed minimally invasive su
endoscopic, or radiologic debridif asymptomatic: consider no
debr
@igure 1'
Management
of pancreatic
necrosis
(hen
infection is
suspected0
7nfected
necrosis
should be
considered in
patients (ith
pancreatic or
eFtrapancreat
ic necrosis
(ho
deteriorate or
fail to
impro;e after
A4 for
Gram stain
and culture to
guide use of
appropriate
antibiotics or
3ii4 empiric
use of
antibiotics
(ithout CT
>A should
be gi;en0 7n
patients (ith
infectednecrosis,
antibiotics
no(n to
penetrate
pancreatic
necrosis may
be useful in
delaying
inter;ention,
thus
decreasing
morbidity and
mortality0 7n
stable
patients (ithinfected
necrosis,
surgical,
radiolo
and1o
endos
c drain
should
delaye
by
prefer
* (ee
allo( t
de;elo
ent of
(all
aroun
necro
3(alle
pancr
necro
-
8/18/2019 Guideline Pancreatite 2013 AJG
78/127
accurate in
distinguishing
infected and sterile
necrosis 3/',!' 40
As patients (ith
infected necrosis
and sterilenecrosis may
appear similar (ith
leuocytosis, fe;er,
and organ failure
3!'A
should be
considered (hen
an infection is
suspected0 An
immediate re;ie(
of the Gram stain
(ill often establish
a diagnosis0Ho(e;er, it may
be prudent to
begin antibiotics
(hile a(aiting
microbiologic
confirmation0 7f
culture reports are
negati;e, the
antibiotics can be
discontinued0
?ere is some
contro;ersy as to(hether a CT >A
is neces5sary in all
patients 3 @igure
140 7n many
patients, the CT
>A (ould not
inBuence the
management
3!'-40 7ncreased
use of
conser;ati;e
management and
minimally in;asi;e
drainage ha;e
decreased
use of >A
the diagnosi
infected
necrosis 3
Many patie
(ith sterile
infected
necrosis ei
impro;e Oui
or beco
unstable,
decisions
inter;ention
a minim
in;asi;e ro
(ill not be i
enced by
results of
aspiration0
consensus
conference c
cluded that should only
used in se
situations (h
there is
clinical respo
to antibio
such as (he
fungal infec
is suspec
3/*40
>8T$7T7I>7> AP
Recommend
ons
!0 7n mild AP
oral
feedings
can be
started
immediat
y if there
no nauseand
;omiting,
and the
abdomina
pain has
resol;ed
3condition
l
recomme
dation,
moderate
Ouality ofe;idence
%0 7n mild AP
-
8/18/2019 Guideline Pancreatite 2013 AJG
79/127
initiation of
feeding (ith
a lo(5fat
solid diet
appears as
safe as a
clear liOuid
diet
3conditional
recommen5
dations,
moderate
Ouality of
e;idence40'0 7n se;ere AP,
enteral
nutrition is
recommend
ed to
pre;ent
infectious
complication
s0 Parenteralnutrition
should
be
a;oide
d,
unless
the
enteral
route
is not
a;aila
ble,
not
tolerat
ed, or
not
meetin
g
caloric
reOuir
ement
s
3stron
g
recommenda
tion,
high
Ouality
of
e;iden
ce40
*0 >asogastric
deli;ery
and
naso2e2una
l deli;ery
of
enteral
feeding
appear
compar
able in
eRcacy
and
safety
3strong
recomm
endatio
n,
moderat
e Ouality
of
e;idenc
e40
S8MMA$I=)7D=>C=Nutritin in!ild AP
Historically,
despite
absence
clinical d
patients (ith
(ere ept >
3nothing
mouth4 to rest
pancreas 3
Most guidel
in the
recommended
>PI
resolution of
and so
suggested
a(aiting
normali@ation
pancre5atic
en@ymes or e
imaging e;ide
of resolution
inBam5mation
before resum
oral feed
3/'40 ? e nee
place
pancreas at
until comp
resolution of
no longer
The A!eric"n 8urn"l #
-
8/18/2019 Guideline Pancreatite 2013 AJG
80/127
GAST$I=>T=$IIG)I8M= !+- J S=PT=M#=$ %+!'
$$$'"!9g"str'c!
-
8/18/2019 Guideline Pancreatite 2013 AJG
81/127
M"n"ge!ent # Acute P"ncre"titis 141
seems
imperati;e0 ?e
long5 held
assumption that
the in Bamed
pancreas
reOuiresprolonged rest by
fasting does not
appear to be
supported by
laboratory and
clinical
obser;ation
3!'940 Clini5cal
and eFperimental
studies sho(ed
that bo(el rest is
associated (ithintestinal mucosal
atrophy and
increased
infectious compli5
cations because
of bacterial
translocation from
the gut0 Multiple
studies ha;e
sho(n that
patients pro;ided
oral feeding early
in the course of AP ha;e a
shorter hospital
stay, decreased
infec5tious
complications,
decreased
morbidity, and
decreased
mortal5ity
3!!
-
8/18/2019 Guideline Pancreatite 2013 AJG
82/127
controlled clinical
trials in;ol;5ing '-!
patients found a
decrease in
infectious
complications,
organ failure, and
mortality in patients
(ith se;ere AP (ho
(ere pro;ided
enteral nutrition as
compared (ith total
parenteral nutri5tion
3!*'40 Although
further study is
needed, continuous
infusion is preferred
o;er cyclic or bolus
administration0
Although the use
of a naso2e2unal
route has been
traditionallypreferred to a;oid
the gastric phase of
stimulation,
nasogastric enteral
nutrition appears as
safe0 A systematic
re;ie( describ5ing
9% patients from *
studies on
nasogastric tube
feeding found that
nasogastric feeding(as safe and (ell
tolerated in patients
(ith predicted
se;ere AP 3!!aso2e2
tube placem
reOuires
inter;entional
radiology
endoscopy and
can be eFpens
or these reas
nasogastric
feeding should
preferred 3!*<
large multice
trial sponsored
the >ational 7
tutes of He
3>7H4 is curre
being performe
in;estigate (he
nasogastric
naso2e2unal
feedings
preferred in thes
-
8/18/2019 Guideline Pancreatite 2013 AJG
83/127
patients because
of signi6cant
eFperimental and
some human
e;idence of
superiority of
distal 2e2unal
feeding in AP0
TH= $I= IS8$G=$ 7> AP
Recommendatio
ns
!0 7n patients
(ith mild
AP, foundto ha;e
gallstones
in the
gallbladder,
a
cholecyste
ctomy
should be
performed
before
discharge
to pre;ent
a
recurrence
of AP
3moderate
recommen
dation,
moderate
Ouality of
e;idence40
%0 7n a patient
(ith
necroti@ing
biliary AP, inorder to
pre;ent
infection,
cholecystect
omy is to be
deferred
until acti;e
inBammatio
n subsides
and Buid
collections
resol;e orstabili@e
3strong
recommend
ation,
moderate
e;idence40
'0
Asymptom
ic
pseudocys
and
pancreatic
and1or eFt
pancreatic
necrosis d
not (arran
inter;entio
regardless
of si@e,
location,
and1or
eFtension
3moderate
recommen
ation, highOuality of
e;idence4
*0 7n stable
patients
(ith
infected
necrosis,
surgical,
radiologic,
and1or
endoscopi
drainage
should be
delayed
preferably
for more
than *
(ees to
allo( liOue
cation of th
contents
and the
de;elopme
t of a 6brou
(all arounthe necros
3(alled5oE
necrosis4
3strong
recommen
ation, lo(
Ouality of
e;idence4/0 7n symptomat
patients (ith
infected
necrosis,minimally
in;asi;e
-
8/18/2019 Guideline Pancreatite 2013 AJG
84/127
methods of
necrosectomy
are preferred to
open necro5
sectomy 3strong
recommendatio
n, lo( Ouality of
e;idence40
S8MMA$ I=)7D=>C=Chlec+stect!+
7n patients (ith
mild gallstone
pancreatitis,
cholecystectomy
should be
performed during
the indeF
hospitali@ation0 ?e
cur5rent literature,
(hich includes -
cohort studies and
one rando5mi@ed
trial describing 99-
patients (ho had
and (ho had not
undergone
cholecystectomy
for biliary
pancreatitis, 9/
3!-K4 (ere
readmitted for
recurrent biliary
e;ents (ithin 9+
days of discharge
3+K ;s0 !-K, P L
+0+++!4, including
recurrent biliary
pancreatitis 3 n W
*', -K4 3!*-40
Some of the cases
(ere found to be
se;ere0 #ased on
this eFperience,there is a need for
early
cholecystectomy
during the same
hospitali@ation,
the attac is m
Patients (ho h
se;ere
especially
pancre5atic
necrosis,
reOuire com
decision ma
bet(een
surgeon
gastroenterolog
7n these patie
cholecystec5tom
is typically dela
until 3i4 a later t
in the typic
prolonged
hospitali@ation,
as part of
management
the pancre
necrosis if presor 3iii4 a
discharge
3!*-,!*940 =a
guidelines
recommended
cholecystectom
Ker % attacs
7AP, (ith
presumption
many such ca
might be beca
of microlithiaHo(e;er,
population5bas
study found
cholecystectom
performed
recurrent atta
of AP (ith
stones1sludge
ultrasound and
signi6cant
ele;ation of
tests during
attac of AP
associated (it
/+K recurre
of AP 3!/+40
%+!' by the American College of Gastroenterology
The A!eric"n 8urn"l # GAST$I=>T=$II
-
8/18/2019 Guideline Pancreatite 2013 AJG
85/127
/ Tenner et al.
7n the
a2ority
tients
h
llston
ncrea
s, the
mmon
e duct
one
sses
the
oden
m0
outine
$CP is
t
propri
e
less
ere is
high
spicio
of a
rsis5
nt
mmon
e duct
one,anifest
by an
e;atio
n the
rubin
/!40
tients
h
d AP,
h
rmal
rubin,n
dergo
prosco
c
olecy
ectom
(ith
raope
i;e
olangi
raphy,
d any
mainin
bile
duct
stones
can be
dealt
(ith by
postoper
ati;e or
intraope
rati;e
=$CP0
7n
patients
(ith lo(
to
moderat
e ris,
M$CP
or =8S
can be
used
preoper
ati;ely,but
routine
use of
M$CP
is
unneces
sary0 7n
patients
(ith mild
AP (ho
cannot
undergosurgery,
such as
the frail
elderly
and1or
those
(ith
se;ere
comorbi
d
disease,
biliarysphincte
rotomy
alone
may be
an
eEecti;e
(ay to
reduce
further
attacs
of AP,
although
attacs
of
-
8/18/2019 Guideline Pancreatite 2013 AJG
86/127
olecy
tis
ay still
cur
'40
=#$7=M=T I
=C$S7Sstoric
y,
en
crose
omy1d
ridem
t (as
e
atme
of
oice
r
ected
crosi
and
mpto
atic
erile
crosi
ecade
ago,
tients
therile
crosi
der(
t
rly
bri5
ment
at
sulted
creas
ortalit
or
s
ason,
rly
en
bride
ent
r
erile
crosi
(asando
d
3'%40
Ho(5
e;er,
debride
ment for
sterile
necrosi
s is
recomm
ended if
associ5
ated
(ith
gastric
outlet
obstruct
ion
and1or
bile
duct
obstruct
ion0 7n
patient