Embed Size (px)
Citation preview
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
The Essentials
Canadian Diabetes Association 2013 Clinical Practice Guidelines
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Learning Objectives
By the end of this session, participants will be able to:
1. Understand the major changes within the 2013 CDA clinical practice guidelines
2. Understand the rationale behind these changes
3. Apply the recommendations in clinical practice
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Faculty for slide deck development
• Jonathan Dawrant, BSc, MSc, MD, FRCPC• Zoe Lysy, MDCM, FRCPC• Geetha Mukerji, MD, FACP, FRCPC• Dina Reiss, MD, FACP, FRCPC• Steven Sovran, BSc, MD, MA, FRCPC
• Alice Y.Y. Cheng, MD, FRCPC• Peter J. Lin, MD, CCFP• Catherine Yu, MD, FRCPC, MHSc
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
www.guidelines.diabetes.ca
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
guidelines.diabetes.ca
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
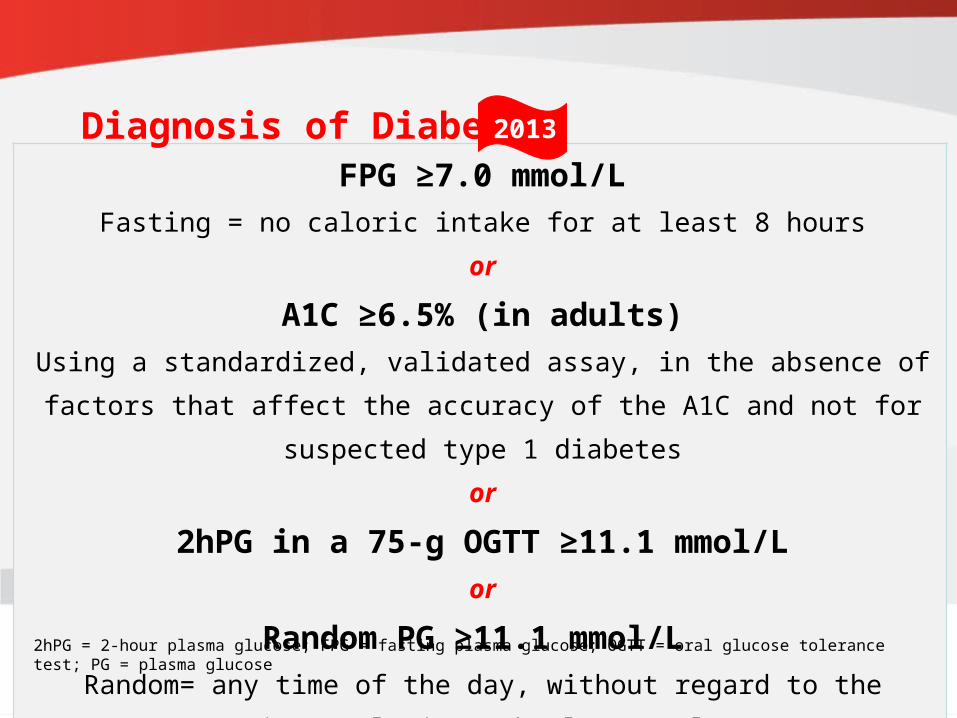
FPG ≥7.0 mmol/LFasting = no caloric intake for at least 8 hours
or
A1C ≥6.5% (in adults)Using a standardized, validated assay, in the absence of factors that affect the
accuracy of the A1C and not for suspected type 1 diabetesor
2hPG in a 75-g OGTT ≥11.1 mmol/Lor
Random PG ≥11.1 mmol/L Random= any time of the day, without regard to the interval since the last meal
2hPG = 2-hour plasma glucose; FPG = fasting plasma glucose; OGTT = oral glucose tolerance test; PG = plasma glucose
Diagnosis of Diabetes 2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
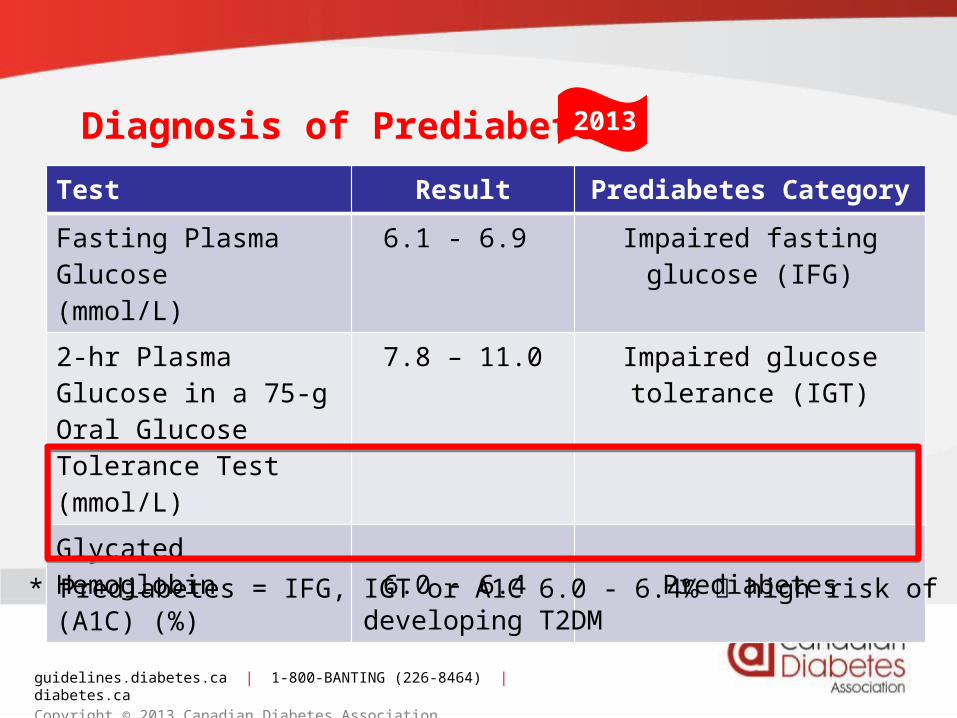
Diagnosis of Prediabetes*
Test Result Prediabetes Category
Fasting Plasma Glucose(mmol/L)
6.1 - 6.9
Impaired fasting glucose (IFG)
2-hr Plasma Glucose in a 75-g Oral Glucose Tolerance Test (mmol/L)
7.8 – 11.0 Impaired glucose tolerance (IGT)
GlycatedHemoglobin(A1C) (%)
6.0 - 6.4 Prediabetes
* Prediabetes = IFG, IGT or A1C 6.0 - 6.4% high risk of developing T2DM
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
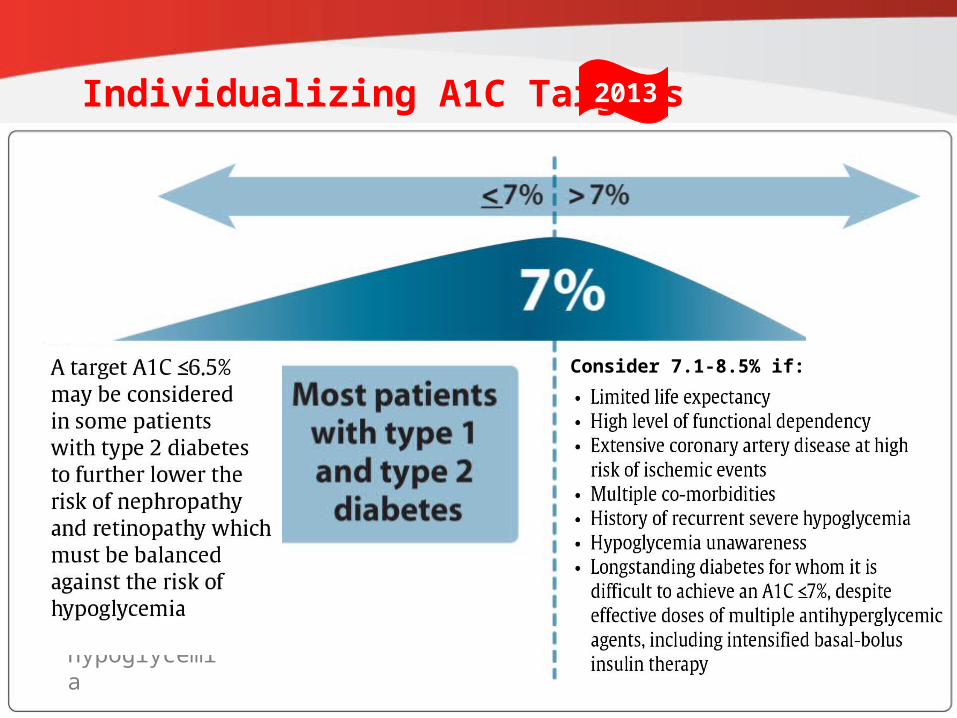
Individualizing A1C Targets
which must be balanced against the risk of hypoglycemia
Consider 7.1-8.5% if:
2013
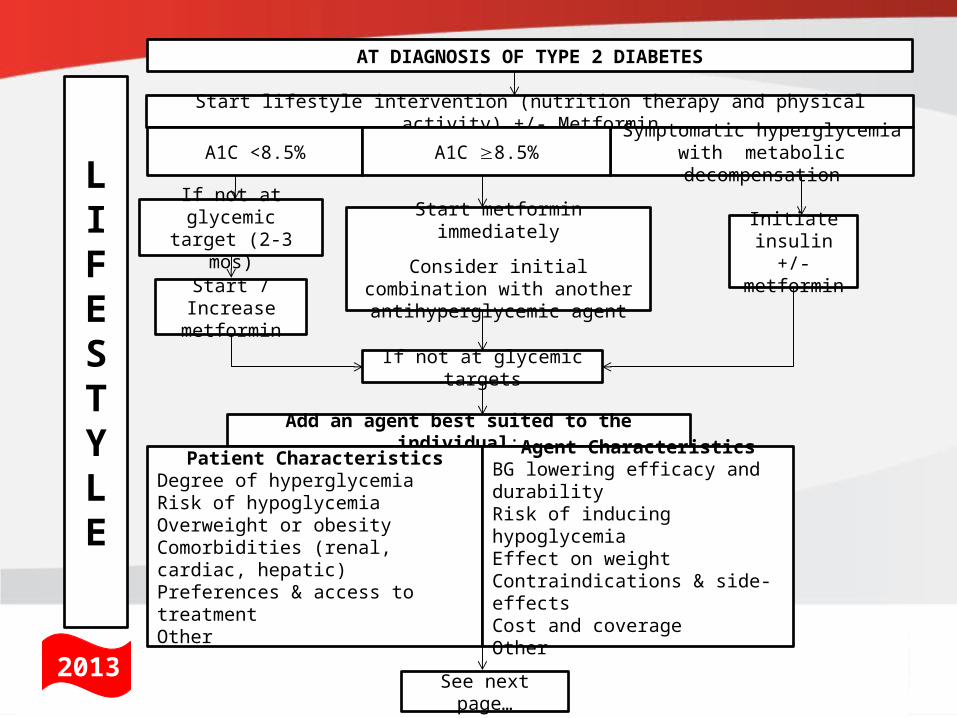
Start metformin immediately
Consider initial combination with another antihyperglycemic agent
Start lifestyle intervention (nutrition therapy and physical activity) +/- Metformin
A1C <8.5%Symptomatic hyperglycemia with
metabolic decompensationA1C 8.5%
Initiate insulin +/-metformin
If not at glycemic target (2-3 mos)
Start / Increase metformin
If not at glycemic targets
LIFESTYLE
Add an agent best suited to the individual:
Patient CharacteristicsDegree of hyperglycemiaRisk of hypoglycemiaOverweight or obesityComorbidities (renal, cardiac, hepatic)Preferences & access to treatmentOther
See next page…
AT DIAGNOSIS OF TYPE 2 DIABETES
Agent CharacteristicsBG lowering efficacy and durabilityRisk of inducing hypoglycemiaEffect on weightContraindications & side-effectsCost and coverageOther
2013
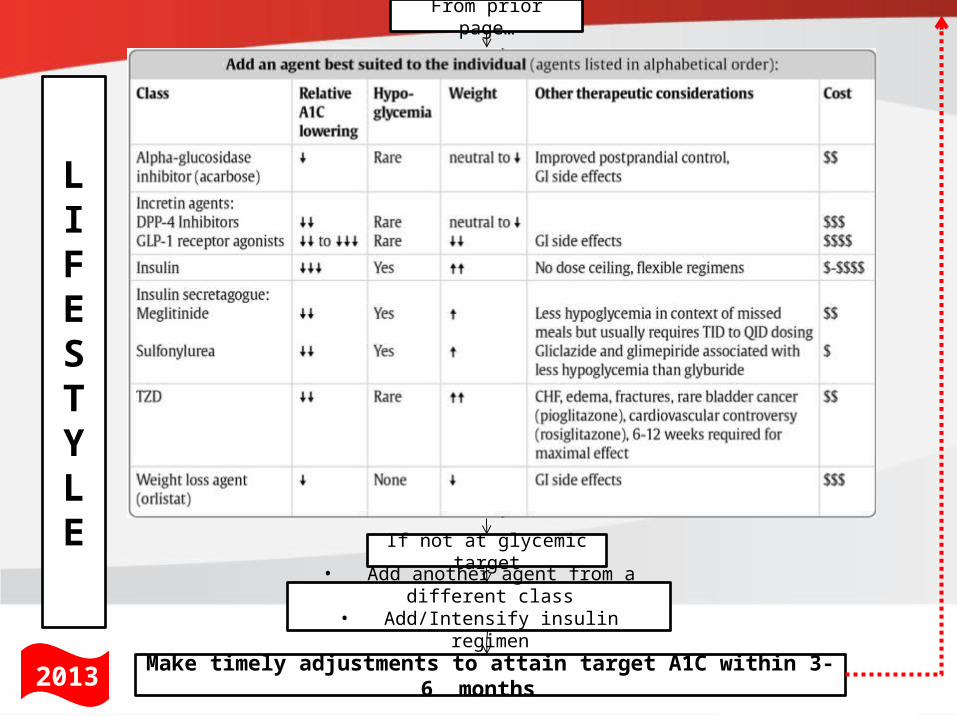
If not at glycemic target
From prior page…
• Add another agent from a different class
• Add/Intensify insulin regimen
Make timely adjustments to attain target A1C within 3-6 months 2013
LIFESTYLE
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
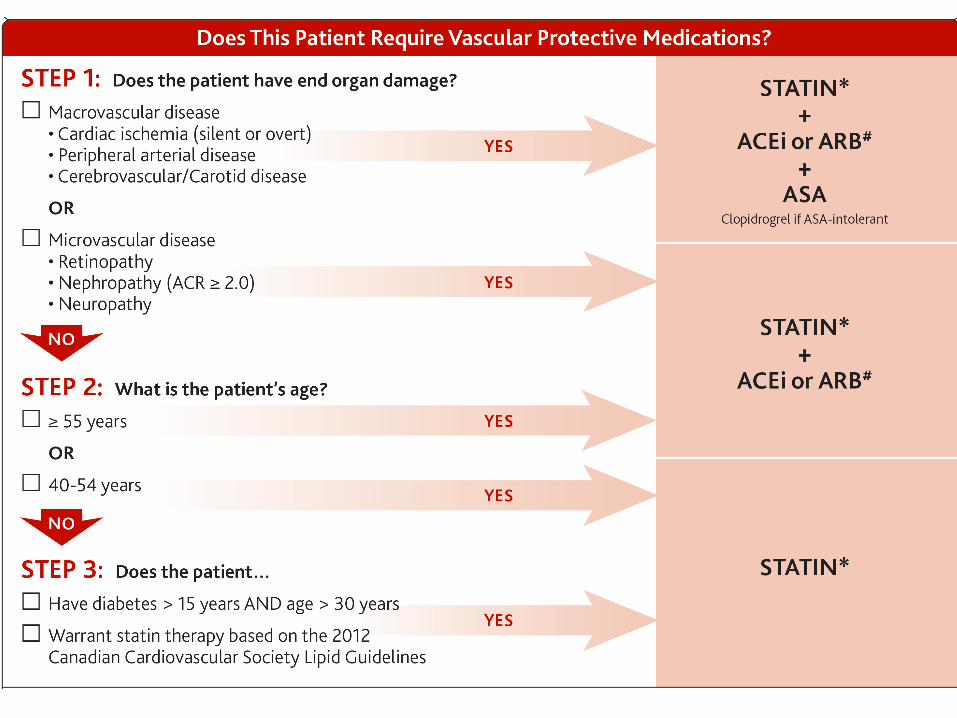
Vascular Protection Checklist 2013
A • A1C – optimal glycemic control (usually ≤7%)
B • BP – optimal blood pressure control (<130/80)
C • Cholesterol – LDL ≤2.0 mmol/L if decided to treat
D • Drugs to protect the heart (regardless of baseline BP or LDL)
A – ACEi or ARB │ S – Statin │ A – ASA if indicated
E • Exercise / Eating healthily – regular physical
activity, achieve and maintain healthy body weight
S • Smoking cessation
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
• ≥40 yrs old or • Macrovascular disease or• Microvascular disease or• DM >15 yrs duration and age >30 years or• Warrants therapy based on the 2012 Canadian
Cardiovascular Society lipid guidelines
Among women with childbearing potential, statins should only be used in the presence of proper preconception counseling &
reliable contraception. Stop statins prior to conception.
2013Who Should Receive Statins? (regardless of baseline LDL-C)
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
What if baseline LDL-C ≤2.0 mmol/L?
• Within CARDS and HPS, the subgroups that started
with lower baseline LDL-C still benefited to the same
degree as the whole population
• If the patient qualifies for statin therapy based on the
algorithm, use the statin regardless of the baseline
LDL-C and then target an LDL reduction of ≥50%
HPS Lancet 2002;360:7-22 Colhoun HM, et al. Lancet 2004;364:685.
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Who Should Receive ACEi or ARB Therapy?(regardless of baseline blood pressure)
• ≥55 years of age or • Macrovascular disease or • Microvascular disease
At doses that have shown vascular protection [perindopril 8 mg daily (EUROPA), ramipril 10 mg daily
(HOPE), telmisartan 80 mg daily (ONTARGET)]
Among women with childbearing potential, ACEi or ARB should only be used in the presence of proper preconception
counseling & reliable contraception. Stop ACEi or ARB either prior to conception or immediately upon detection of pregnancy
2013
EUROPA Investigators, Lancet 2003;362(9386):782-788.HOPE study investigators. Lancet. 2000;355:253-59.
ONTARGET study investigators. NEJM. 2008:358:1547-59
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation
ASA should not be routinely used for the primary
prevention of cardiovascular disease in people with
diabetes [Grade B, Level 2]
ASA may be used in the presence of additional cardiovascular risk factors [Grade D, Consensus]
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Chronic Kidney Disease (CKD) Checklist
SCREEN regularly with random urine albumin creatinine ratio
(ACR) and serum creatinine for estimated glomerular filtration
rate (eGFR)
DIAGNOSE with repeat confirmed ACR ≥ 2.0 mg/mmol and/or
eGFR < 60 mL/min
DELAY onset and/or progression with glycemic and blood
pressure control and ACE inhibitor or angiotensin receptor
blocker (ARB)
PREVENT complications with “sick day management”
counselling and referral when appropriate
2013
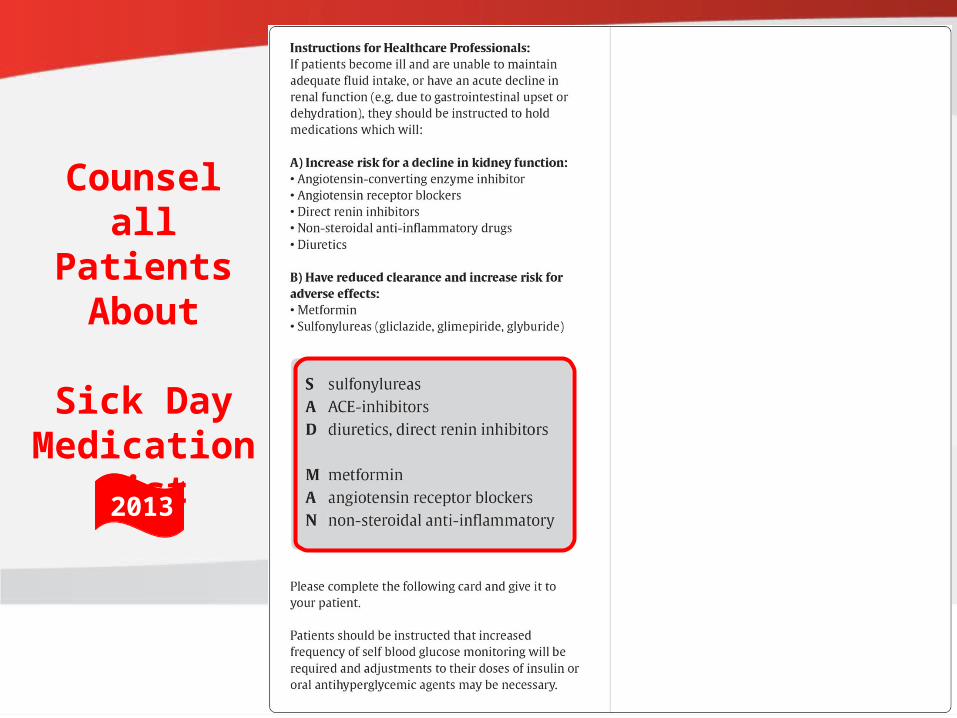
Counsel all Patients About
Sick Day Medication
List
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Diabetes in the Elderly Checklist ASSESS for level of functional dependency (frailty)
INDIVIDUALIZE glycemic targets based on the above (A1C ≤ 8.5% for frail elderly) but if otherwise healthy, use the same targets as younger people
AVOID hypoglycemia in cognitive impairment
SELECT antihyperglycemic therapy carefully caution with sulfonylureas or thiazolidinediones Basal analogues instead of NPH or human 30/70
insulin Premixed insulins instead of mixing insulins separately
GIVE regular diets instead of “diabetic diets” or nutritional formulas in nursing homes
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Need a preconception checklist for women with pre-existing diabetes
1. Attain a preconception A1C of ≤ 7.0% (if safe)
2. Assess for and manage any complications
3. Switch to insulin if on oral agents
4. Folic Acid 5 mg/d: 3 mo pre-conception to 12 weeks post-conception
5. Discontinue potential embryopathic meds: Ace-inhibitors/ARB (prior to or upon detection of pregnancy) Statin therapy
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
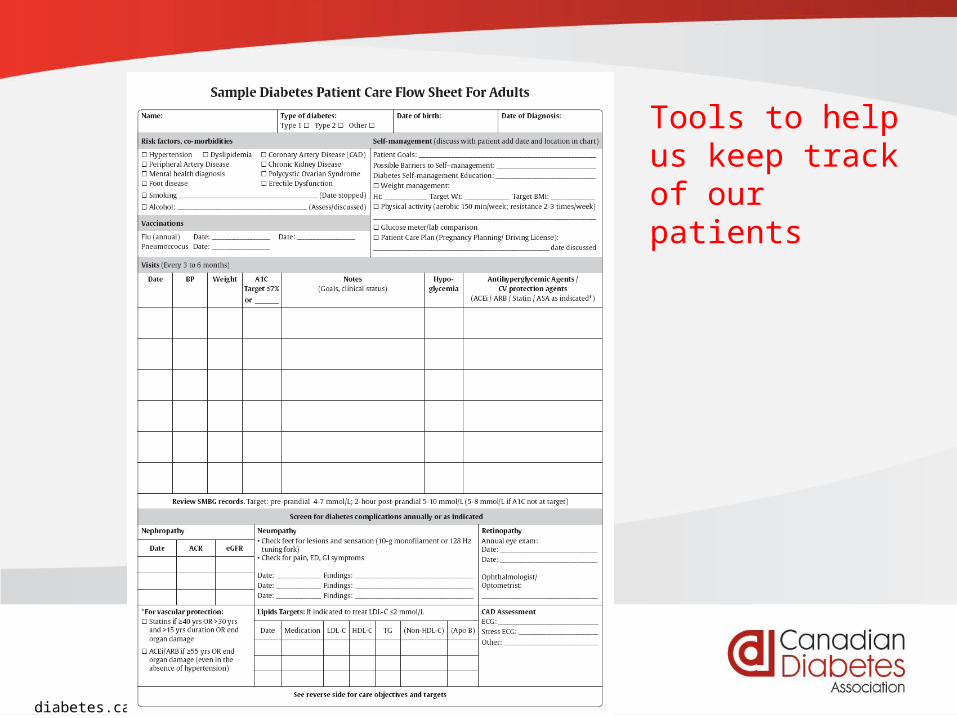
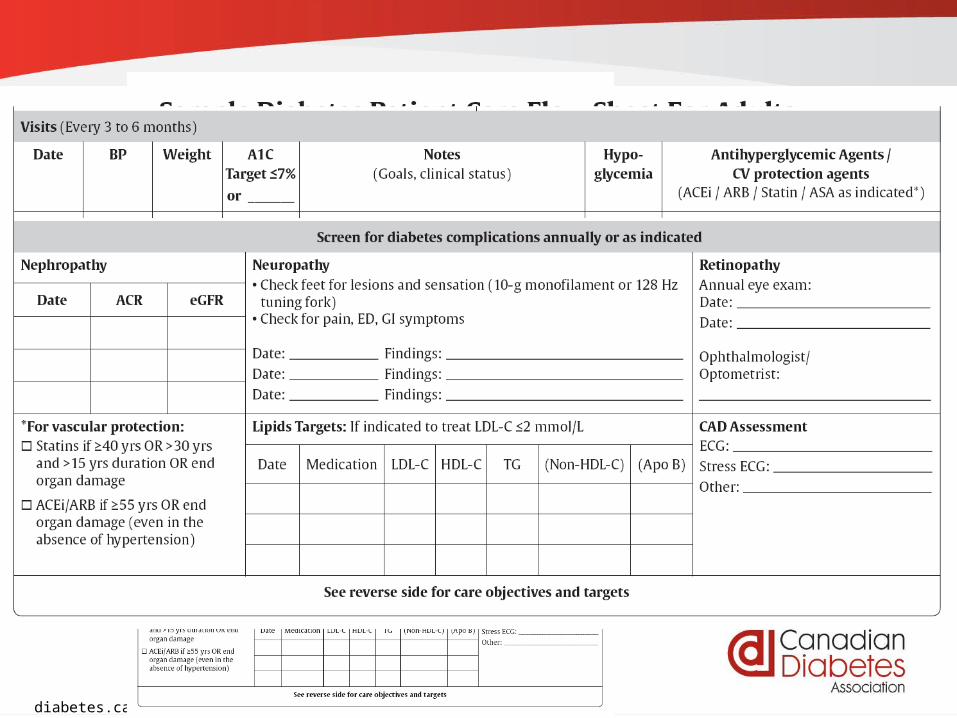
Tools to help us keep track of our patients
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Tools to help us keep track of our patients
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
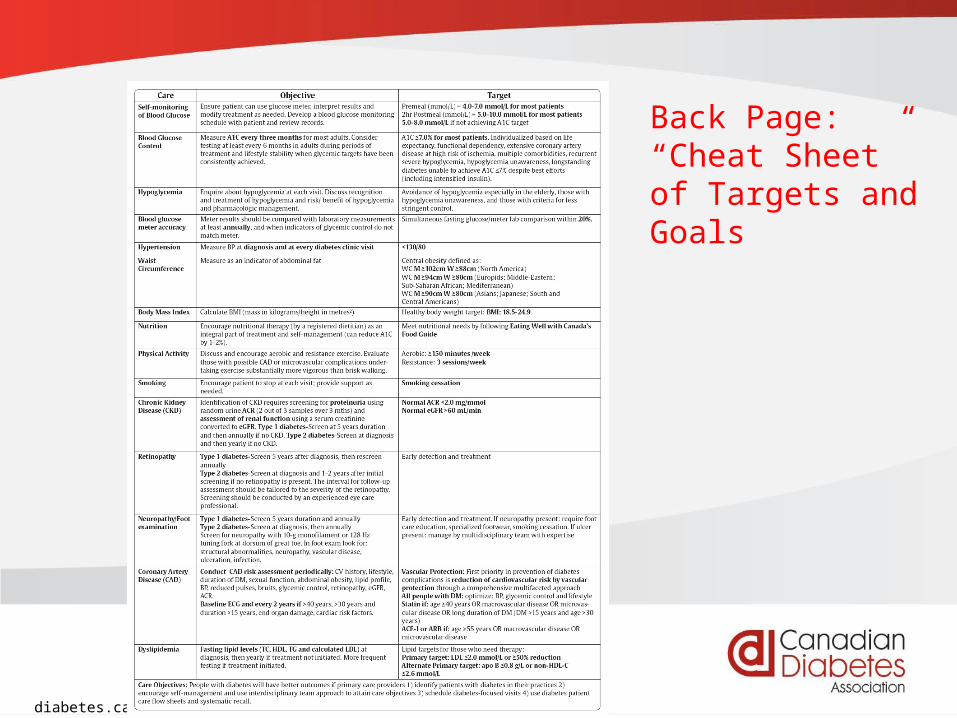
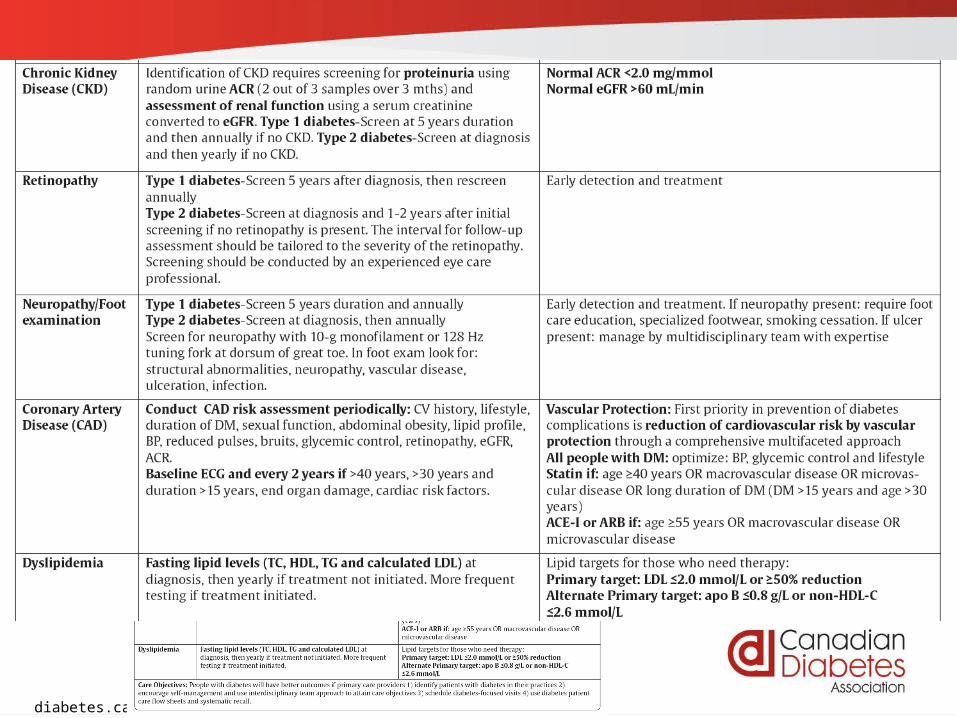
Back Page:“Cheat Sheet” of Targets and Goals
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Back Page:“Cheat Sheet” of Targets and Goals
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
New resources
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Download the App Today!
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
“Neither evidence nor clinical judgment alone is sufficient.
Evidence without judgment can be applied by a technician.
Judgment without evidence can be applied by a friend.
But the integration of evidence and judgment is what the healthcare provider does in order to dispense the best clinical care.”
(Hertzel Gerstein, 2012)





























