Embed Size (px)
Citation preview

Gut 1995; 36: 183-188
Relation between gastric emptying rate and energy
intake in children compared with adults
B D Maes, Y F Ghoos, B J Geypens, M I Hiele, P J Rutgeerts
AbstractMeasurement of gastric emptying rate ofsolids in children is difficult because theavailable methods are either invasive orinduce a substantial radiation burden.In this study the newly developed 13Coctanoic acid breath test was used toexamine the gastric emptying rate ofsolids and milk in healthy children and tocompare gastric emptying in childrenand adults. Fifteen healthy children andthree groups of nine healthy adults werestudied, using three different test mealslabelled with 50 mg of 13C octanoic acid: alow caloric pancake (150 kcal), a highcaloric pancake (250 kcal), and 210 ml ofmilk (134 kcal). Breath samples weretaken before and at regular intervals afteringestion of the test meal, and analysedby isotope ratio mass spectrometry. Thegastric emptying parameters were derivedfrom the 13C02 excretion curves by non-
linear regression analysis. No significantdifference was found between childrenand adults in the emptying rate of the lowcaloric solid test meal. In children as wellas in adults, increasing the energy contentofthe solid meal resulted in a significantlyslower emptying rate. The milk test meal,however, was emptied at a faster ratein adults and at slower rate in childrencompared with the low caloric solid testmeal. Moreover, the emptying rate ofmilk in children was significantly slowerthan in adults. In conclusion, a similargastric emptying rate of solids but aslower emptying of full cream milk wasshown in children ofschool age comparedwith adults, using the non-radioactive 13Coctanoic acid breath test.(Gut 1995; 36: 183-188)
Keywords: gastric emptying, energy intake.
gastric emptying rate in symptoms such aschronic abdominal pain, nausea, and vomitingare largely unexamined in children. -5
Recently, we developed a carbon labelledbreath test to measure gastric emptying rate ofsolids, based on the characteristics of octanoicacid.6 Using a solid standard test meal of 250kcal consisting of a labelled egg and two slicesof white bread, an excellent correlationbetween the gastric emptying results of theradioscintigraphic method (lag phase, halfemptying time) and those of the breath test(gastric emptying coefficient, lag phase, andhalf emptying time) could be shown in adults.6It was also shown that day to day variability ofgastric emptying rate of solids, obtained by thecarbon labelled octanoic acid breath test iscomparable with data obtained by radioscinti-graphy,6 and that the breath test was sensitiveenough to detect pharmacological influences oferythromycin and propantheline on gastricemptying rate of solids.7The aim of this study was to evaluate the
gastric emptying rate in children using 13Coctanoic acid labelled test meals and tocompare gastric emptying in children withgastric emptying in adults.
Methods
SUBJECTSFifteen healthy children performed threegastric emptying studies using three differenttest meals within one month in a randomlyallocated sequence. Nine of the children weregirls, six were boys; the mean age was 9 years,ranging from 4 to 15. The mean weight was31 kg, ranging from 17 to 65 and the mean
height was 135 cm, ranging from 105 to 165.Table I gives detailed description of thechildren. Twenty seven adults, divided into
Department ofMedicine, Division ofGastroenterology andGastrointestinalResearch Centre,University HospitalGasthuisberg, Leuven,BelgiumB D MaesY F GhoosB J GeypensM I HieleP J Rutgeerts
Correspondence to:Professor Dr P J Rutgeerts,Department of Medicine andMedical Research, UniversityHospital Gasthuisberg,B-3000 Leuven, Belgium.Accepted for publication9 June 1994
Gastric emptying in children is difficult toevaluate properly. The main reason is the lackof safe and non-invasive methods to measuregastric emptying rate in children. All methodsused until now have some disadvantages forroutine gastric emptying studies in children:intubation studies are invasive and time con-
suming, radioscintigraphic methods cause a
substantial radiation burden to the patient,ultrasonographic evaluation of gastric empty-ing rate can only be applied to liquid test mealsand is largely dependent on the experience ofthe investigator. Therefore the impact ofdelayed gastric emptying rate on nutrientassimilation and nutritional state or the role of
TABLE I Characteristics of the examined children
Weight Height Age BSAChild (kg) (cm) (y) Sex (m2)
Cl 32 143 11 M 1-12C2 36 147 11 M 1-21C3 38 143 10 F 1-23C4 41 163 14 F 1-35C5 17 105 4 M 0.70C6 27 141 9 F 1.02C7 20 123 6 F 0-82C8 24 122 6 M 090C9 28 134 9 F 1.01ClO 65 165 15 F 1-73Cli 39 142 10 F 1-24C12 20 116 7 M 0-80C13 37 133 10 F 1-18C14 25 132 7 F 0.95C15 21 115 5 M 0-82
BSA: body surface area.
183
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from
Maes, Ghoos, Geypens, Hiele, Rutgeerts
TABLE II Characteristics of the examined adults, according to the ingested test meal (meanand interquartile range)
Test meal Femaldmale Weight (kg) Height (cm) Age (y) BSA (m2)
150 kcal 5/4 61(60-78) 177 (168-182) 23 (21-24) 1-70 (1.69-2-00)250kcal 5/4 62 (57-74) 168(168-172) 22(19-23) 1-66(1-56-1-77)Milk 5/4 60 (57-76) 167 (162-176) 20 (18-22) 1.63 (156-1 91)
BSA: body surface area.
three groups of five women and four men, eachperformed one gastric emptying study usingone of the three test meals. Table IIsummarises the characteristics of the adultgroups. The test meal of each adult group wasallocated at random. None of the childrenor adults had gastrointestinal complaints, a
medical or surgical gastrointestinal history or
was taking any drugs. The study protocol was
approved by the ethics committee of theUniversity of Leuven. Informed consent was
obtained from all the subjects or their parents.
MATERIALSAll gastric emptying studies were performedafter an overnight fast at 8 am with the childrenquietly seated in front of a video tape, andthree children, who could not eat the test mealwithin 10 minutes, were excluded.The low caloric solid test meal was based on
a pancake made of 5 g of sugar, 12.5 g of flour,10 g of full cream milk, and one egg. Half ofthe egg yolk was baked separately after 50 mgof 13C octanoic acid (Isotec, Ohio, USA) was
solubilised in the yolk by mixing. The pastewas baked around the labelled half of theegg yolk. Total energy content of the testmeal was 150 kcal (9 g of proteins, 13 g ofcarbohydrates, and 7 g of fat).The high caloric solid test meal consisted
of two pancakes; one was a labelled pancakeas described above (150 kcal) and one was
an unlabelled pancake baked with the same
ingredients apart from the separately bakedhalf egg yolk (100 kcal). Total energy contentwas 250 kcal (14 g of proteins, 26 g of carbo-hydrates, and 10 g of fat). Both solid test mealswere consumed within a 10 minute period.The subjects were allowed to drink 150 ml ofwater during the test meal.The liquid test meal used in the third study
consisted of 210 ml of full cream milk in which50 mg of 13C octanoic acid was solubilised.The energy content of this liquid test meal was
134 kcal, containing 7 g of proteins, 10 g ofcarbohydrates, and 7 g of fat. The liquid testmeal was consumed within five minutes.
MEASURING TECHNIQUESBreath samples were taken before intake of thetest meal and every 15 minutes after ingestionofthe meal up to four hours to study the gastricemptying rate of the solid test meals. Thegastric emptying rate of the liquid test mealwas examined by taking breath samples beforethe meal and every 10 minutes during a threehour period for children and during a twohour period for adults. Breath was collectedin a 3 litre aluminium coated plastic bag
(Tesseraux, Burstadt, Germany), from whichaliquots were taken to determine 13C enrich-ment with an isotope ratio mass spectrometer(model 250, Finigan MAT, Bremen, Germanyand ABCA, Europa Scientific, Lowe,England). The results were expressed as thepercentage of '3C recovery per hour. Thecarbon dioxide production was assumed to be300 mmollm2 body surface area per hour.Body surface area was calculated by theweight-height formula of Haycock et al.8
MATHEMATICAL ANALYSISThe 13C02 excretion in breath, expressedas percentage dose per hour was furthermathematically analysed using two non-linearregression equations (SAS: PROC NLIN9 orwith a home made program written forEXCEL 4.0 (G Mys, personal communica-tion)) to find the best fitting curve through themeasured data points. The first formula isgiven by:
(I) y=atbe-ctwhere y is the percentage of 13C02 excretion inbreath per hour; t is time in hours; and a, b,and c are constants. The second formula isexpressed as:
(II) y=mke-kt(l-e-kt)I-1
where y is the percentage of 13C excretion inbreath per hour; t is time; m, k, and P areconstants and m is the total cumulative '3Crecovery when time is infinite. This formula isthe first derivative of the modified power expo-nential formula of Siegel et al10 with a correc-tion factor m. Three parameters of gastricemptying were derived from these formulas,based on regression models obtained by simul-taneous radioscintigraphic and breath testmeasurements6:
(1) The gastric emptying coefficient(GEC), corresponding to ln(a) of the firstformula and a global index for the gastricemptying rate.
(2) T112, the breath test determined gastrichalf emptying time (in minutes), by the follow-ing equation derived from the first formula:
t1/2= [60(gamma inv (0-5;b+ 1;1/c)-66]/1112
or by the following equation using the secondformula:
t112= [60(- 1/k)ln(1 -2 l/c).-6.66]/1 v12(3) The lag phase. The lag phase is defined
as was done by Siegel et al," as the time (inminutes) at the point of inflection of the curveafter mathematical integration - that is, thetime of maximal 13C02 excretion of the fittedcurve, calculated by the following equationderived from the first formula:
tmax= [60(b/c-66]/0*94or by the following equation using the secondformula:
tm. = [60(In,B)/k- 66]/0.94
184
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from
Relation between gastric emptying rate and energy intake in children compared with adults
The gastric half emptying time and the lagphase are - by the nature of their mathematicaldefinition - completely determined by theshape of the curve and thus independent of theendogenous carbon dioxide production.
W-(wSTATISTICAL EVALUATIONGastric emptying parameters of the threeseries of studies in children and in adultswere analysed by descriptive statisticalmethods (SAS: PROC UNIVARIATE9).Because of a skew distribution, median andinterquartile range are given. The gastricemptying parameters of each child were com-pared in a non-parametrical paired way forthe low and high energy solid test meal, andfor the low energy solid test meal and theliquid test meal using the signed rank test(SAS: PROC UNIVARIATE). The gastricemptying parameters of the three adult groupswere compared using the non-parametricMann-Whitney-Wilcoxon test (SAS: PROCNPAR1WAY). Non-parametric methods(SAS: PROC NPAR1WAY: Mann-Whitney-Wilcoxon) were also used to compare thegastric emptying parameters in children andadults for the meals with the same energy load.
5.OOT
4.00t
3.00t
2.00+
1.00+
u0.u
240.
180
c
E 1201-
604.
A
A
AA
AaAA
A
A
A
A
AAA
A
Milk 150 kcal 250 kcal
A A
AA
A
AA
AA
A
AA
Milk 150 kcal 250 kcal
Results
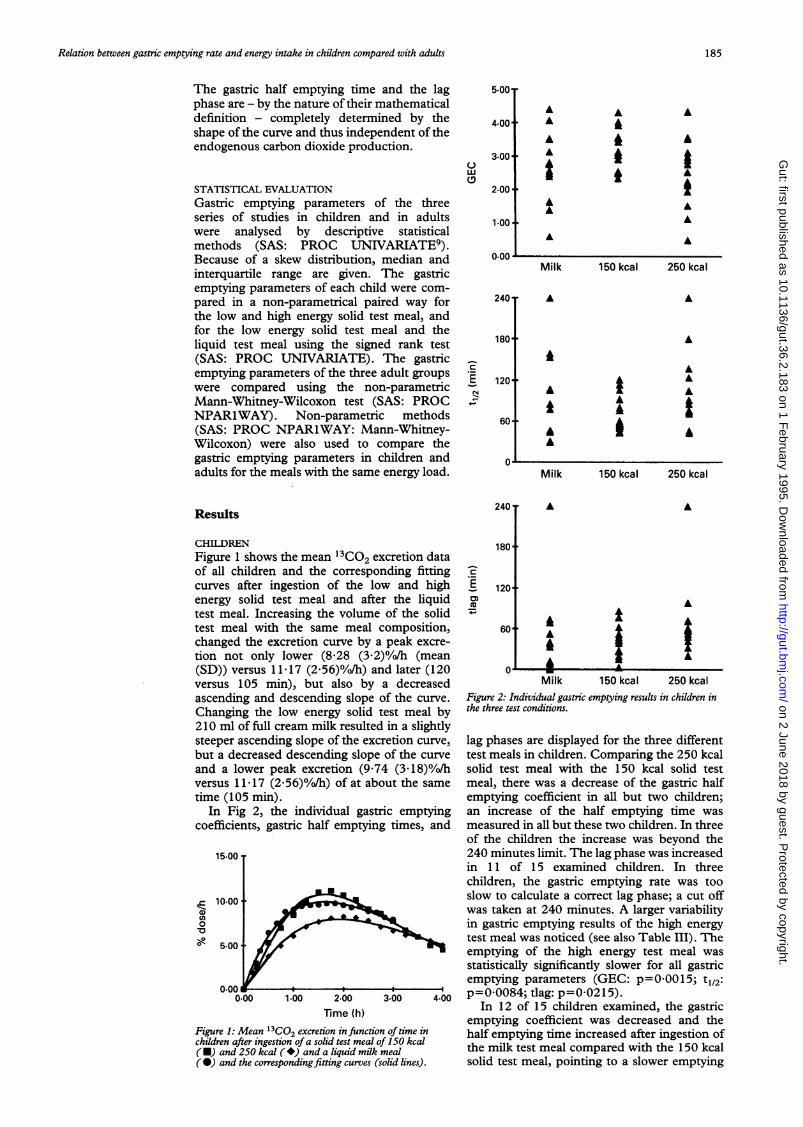
CHILDRENFigure 1 shows the mean 13CO2 excretion dataof all children and the corresponding fittingcurves after ingestion of the low and highenergy solid test meal and after the liquidtest meal. Increasing the volume of the solidtest meal with the same meal composition,changed the excretion curve by a peak excre-tion not only lower (8.28 (3.2)0/o/h (mean(SD)) versus 11.17 (2.56)0/o/h) and later (120versus 105 min), but also by a decreasedascending and descending slope of the curve.Changing the low energy solid test meal by210 ml of full cream milk resulted in a slightlysteeper ascending slope of the excretion curve,but a decreased descending slope of the curveand a lower peak excretion (9.74 (3-1 8)0//hversus 1 1 c17 (2.56)0/o/h) of at about the sametime (105 min).
In Fig 2, the individual gastric emptyingcoefficients, gastric half emptying times, and
15.00.
0n,.c 10.00
0.00 1.00 2.00 3.00
Time (h)Figure 1: Mean 13C02 excretion in function of time inchildren after ingestion ofa solid test meal of 150 kcal(E) and 250 kcal ( *) and a liquid milk meal(@) and the corresponding fitting curves (solid lines).
240T A
180'
10120
60 At A
A
a~~IMilk 150 kcal 250 kcal
Figure 2: Individual gastric emptying results in children inthe three test conditions.
lag phases are displayed for the three differenttest meals in children. Comparing the 250 kcalsolid test meal with the 150 kcal solid testmeal, there was a decrease of the gastric halfemptying coefficient in all but two children;an increase of the half emptying time wasmeasured in all but these two children. In threeof the children the increase was beyond the240 minutes limit. The lag phase was increasedin 1 1 of 15 examined children. In threechildren, the gastric emptying rate was tooslow to calculate a correct lag phase; a cut offwas taken at 240 minutes. A larger variabilityin gastric emptying results of the high energytest meal was noticed (see also Table III). Theemptying of the high energy test meal wasstatistically significantly slower for all gastricemptying parameters (GEC: p=00015; t112:p=00084; tlag: p=0.0215).
In 12 of 15 children examined, the gastricemptying coefficient was decreased and thehalf emptying time increased after ingestion ofthe milk test meal compared with the 150 kcalsolid test meal, pointing to a slower emptying
U
185
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from

186 ~~~~~~~~~~~~~~~~~~~~~~~~~Maes,Ghoos, Geypens, Hiele, Rutgeerts
TABLE iii Gastric emptying results in children and adults (median and interquartilerange)
GEC tl/2 (min) tiag (min)
Median Q3-Q1 Median Q3-QJ Median Q3-Q1
Children 150 kcal 3.12 0.69 58 39 39 26250 kcal 2.54 1.18 91 105 60 50Milk 2.76 1.12 86 112 40 64
Adults 150 kcal 3.40 0.38 55 21 20 33250 kcal 2.81 0.30 94 29 50 22Milk 3.94 0.54 35 31 16 23
5.OOT
4.00.
3.001W(D
AA
AAA
kAAA
2.004-
1.-00
rate of the first meal (Fig 2). In three children,the decrease of the gastric emptying coefficientand the increase of the gastric half emptyingtime was remarkably large. The lag phase,however, was only increased in eight of theinvestigated children. Again, the variability ofthe emptying results in the milk test meal wasvery large compared with the low energy solidtest meal. Paired comparison showed thatthe differences between the two meals werestatistically significant for the gastric emptyingcoefficient (p=0.0366) and the half emptyingtime (p=0.Ol5 1), but the lag phase was similar(p=0.5245).Comparing the milk and high energy solid
test meal, a globally similar emptying rate withan equally high variability was seen in children(see Table III). No gastric emptying parametershowed a statistical difference for these twomeals (GEC: p=0.488'7; t112: p=l1; tlag:p=0.2958).
ADULTS
Figure 3 shows the mean 13C02 excretiondata of the three groups of adults and thecorresponding fitting curves after ingestion ofthe corresponding test meal. The results aresimilar to those obtained in children for the150 kcal and 250 kcal solid test meal, but amuch faster pattern of 13C02 excretion andcorresponding gastric emptying is seen afteringestion of the milk test meal. The peakexcretion of the curves was 13.25 (2.58)0/o/h at105 minutes, 10.94 (1.75)0/o/h at 120 minutes,and 13.48 (3.42)07oTh at 60 minutes for the lowenergy, high energy, and milk test meal,respectively.
In Fig 4, the individual gastric emptyingvalues for the three different test mealsexamined in adults are given. A gradualincrease of the energy content of the meal
15.00..
.~10.00-
0-0
5f00l
0.00 1.00 2.00 3.00
Time (h)
Figure 3: M~an 3C02 excretion in function of time in
adults after ingestion of a solid test meal of 150 kcal (UM)and 250 kcal (*) and a liquid milk meal (@0) and the
corresponding fitting curves (solid lines).
100
n.nn'a
1801CEE 1201
60
Milk 150 kcal 250 kcal
AA
A
Milk
A
AAA
150 kcal 250 kcal
240T
180+
0)E) 120+
60 + AA
A
AAAA
Mil71k 150 kcal1 250 kcalFigure 4: Individual gastric emptying results in adults inthe three test conditions.
(milk, 150 kcal pancake, 250 kcal pancake)resulted in a gradual increase of the halfemptying time and the lag phase and in agradual decrease of the gastric emptyingcoefficient. There is an almost equal variabilityin emptying results for the three different testmeals (see Table III). The differences ingastric emptying results for the low energy andhigh energy solid meal (GEC: p=O0l036;p=0.0171; tlag: p=0.0212) and for the liquidmilk and high energy solid meal (GEC:p=0.0040; t112: p=0.0041; tlag: p=0.0010)are statistically significant; the differencesbetween the milk and 150 kcal solid test meal,however, are not significantly different (GEC:p=0.1255; tl/2: p=0.0638; tlag: p=0.1632).
CHILDREN VERSUS ADULTSTable III shows that.gastric emptying of thelow (GEC: p=0.1286; t112: p=0.23'72; tlag:p=0.0851) and high energy solid test meal(GEC: p=0-ll65; t112: p=0.2751; tlag:p=0.0604) in children and adults is very
0 1
fl .
186
240T
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from

Relation between gastric emptying rate and energy intake in children compared with adults
similar. In contrast with solids, the emptyingrate of the liquid milk test meal is significantlyslower in children than in adults (GEC:p=0.0048; tl12: p=00052; tlag: p=0.0180). Agreater variability in gastric emptying rate,however, was seen in children compared withadults in the liquid milk and the high energysolid test meal (Figs 2 and 4).
DiscussionThe gastric emptying rate of solids in childrenis difficult to evaluate. From the age of threeyears, all children are receiving an 'adult' diet,consisting of solids as an important energysource. Therefore, an accurate evaluation ofthe gastric motor function (that is, the abilityto mix, grind, and evacuate the ingested meal)of children of school age should be performedusing a solid test meal. However, there are twoimportant problems.
Firstly, the volume/energy content of thesolid test meal should be adjusted to the bodysurface area or lean body weight, not onlyfor children but also for adults. As, from thepractical view point, this correction is difficultto perform for solid test meals, the use ofstandard solid test meals is widespread, bothin adults and children of school age.1' 12 Inthis study, the emptying rate of two standard-ised solid test meals and one standardisedliquid test meal was evaluated in children ofschool age, and compared with the emptyingrate of the same meals in adults. Secondly,until now, the radioscintigraphic techniqueis the only available method to measureaccurately the gastric emptying rate of solidsin children despite the radiation hazard. Inthis study gastric emptying rate was measuredusing the newly developed 13C labelledoctanoic acid breath test, inducing noradiation at all.The second technique can describe gastric
emptying rate of a standard solid test meal inan accurate and reliable way, including thebiphasic nature of gastric emptying of solids.6 7However, some additional methodologicalconsiderations have to be made for this study.The solid test meal used in this study consistedof a pancake to ameliorate the palatability ofthe meal for children. Despite the labellingtechnique (a labelled egg yolk, which is bakedseparately) and a meal composition thatremained unchanged, the viscosity of the testmeal was not the same as the meal describedearlier.6 7 Furthermore, the 13C octanoic acidbreath test is an indirect method to measuregastric emptying of solids. Although directmeasurements on metabolism of octanoic acidhave never been done in infants, several reportsshowed that the oxidation rate of trioctanoin issimilar in children and adults.13 14
Moreover, as the gastric half emptying timeand the lag phase are independent of endo-genous carbon dioxide production, differencesin basal metabolism between children andadults have no influence on these results.Also, other external influences were excluded.Day to day variability in gastric emptyingrate is very well known in adults (similar in
scintigraphic and breath test technology6), buthas never been examined in children with noneof the existing methods. As we did not studythe children at different times using the sametest meal, intrasubject variability of test resultsin children could also not be evaluated; butconfounding by day to day variability waseliminated as much as possible by randomisingthe sequence of test meal administration.
Concerning the adult groups, the threegastric emptying parameters described,changed unidirectly with increasing energyload of the test meal. This further validatesthe breath test for measurement of gastricemptying of solids. A larger variability ingastric emptying results was seen with theliquid milk test meal of 134 kcal.
In children, the gastric emptying resultsobtained with the low energy solid test mealare comparable with those obtained in adults,however, with a larger variability of results.Increasing the energy content of the mealresulted in a slower gastric emptying patternsimilar to adult gastric emptying in 12 of 15children examined. Three of the childrenshowed an extremely delayed gastric emptying,which seemed to be blocked once a certainplateau of energy load is reached. No relationwith age, weight, length, body surface area orsex, however, could be found.
Changing the low energy solid test meal by aliquid fat emulsion with less energy valueresulted in children in a slower gastric emptyingof the test meal, apart from the lag phase(Table III). The reason for a slower gastricemptying of milk in children is not very clear.No difference in emptying results of the milktest meal were obtained if the calculations werebased on the 13C02 excretion data of the firsttwo hours, as performed in adults. Milk leads tothe formation of separate gastric food phasesbecause casein is precipitated below a pH of 4. 1to form curds,'1'7 which are probably emptiedas solid particles. A similar finding has beenmade in gastrostomy fed patients with spasticquadriplegia, in which whey based milk for-mulas showed a significantly shorter emptyingtime than a casein based formula.'8 However,curd formation of casein in the stomach alsooccurs in adults. The emptying rate of milk hasnever been compared between children andadults. A factor of unknown influence, is theeffect of liberated opioid peptides duringdigestion of casein19-21 on gastric motility bydirect action with gut opiate receptors. It ispossible that the gut is more sensitive to theinhibitory action of these opioid peptides duringchildhood. Or the role of cholecystokinin inthe regulation of gastric emptying22 may bedifferent in children compared with adults. Itis known that casein induces a considerablerelease of cholecystokinin, at least in animalexperiments.2324 The release of cholecystokininin response to casein may vary differentially inadults and children or the receptor density maybe different in children. Further validation onthis point will be necessary.The 13C octanoic acid breath test to measure
gastric emptying in children has some importantadvantages over other existing techniques: it is
187
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from

188 Maes, Ghoos, Geypens, Hiele, Rutgeerts
non-invasive, causing no radiation at all, thetest can be performed in a place and at a timecausing a minimum of stress for the child, as thecarbon dioxide samples can be collected awayfrom the analytical unit and the test can even berepeated several times within a short period oftime.We conclude that the 13C labelled octanoic
acid breath test is a comfortable and promisingtechnique to evaluate gastric emptying inchildren. Further studies will be necessary toinvestigate (a) intraindividual variability of testresults in children and (b) the best test meal foraccurate discrimination between normal anddelayed gastric emptying.
1 Gryboski JD, Burger JA, McCallum R, Lange R. Gastricemptying in childhood inflammatory bowel disease: nutri-tional and pathological correlates. Gastroenterology 1992;87: 1148-53.
2 Kelts DG, Grand RJ, Shen G, Watkins JB, Werlin SL,Bochme C. Nutritional basis of growth failure in childrenand adolescents with Crohn's disease. Gastroenterology1979; 76: 720-7.
3 Franco VH, Collares EF, Troncon LE. Gastric emptyingin children. Studies on kwashiorkor and on marasmickwashiorkor. Arquivos de Gastroenterologia 1986; 23:42-6.
4 Papaila JG, Wilmot D, Grosfeld JL, Rescorla FJ, West KW,Vana DW. Increased incidence of delayed gastric empty-ing in children with gastroesophageal reflux. A prospectiveevaluation. Arch Surg 1989; 124: 933-6.
5 Woolridge MW, Fisher C. Colic, 'overfeeding', and symp-toms of lactose malabsorption in the breast-fed baby: apossible artefact of feed management? Lancet 1988; ii:382-4.
6 Ghoos Y, Maes B, Geypens B, Mys G, Hiele M, RutgeertsP, et al. Measurement of gastric emptying rate of solids bymeans of a carbon labelled octanoic acid breath test.Gastroenterology 1993; 104: 1640-7.
7 Maes B, Hiele M, Geypens B, Rutgeerts P, Ghoos Y,Vantrappen G. Pharmacological modulation of gastricemptying rate of solids as measured by the carbon labelledoctanoic acid breath test: influence of erythromycin andpropantheline. Gut 1994; 35: 333-7.
8 Haycock G, Schwartz G, Wisotsky D. Geometric methodfor measuring body surface area: a height-weight formula
validated in infants, children and adults. Jf Pediatr 1978;93: 62-6.
9 SAS Institute Inc. SAS/STAT User's Guide. Release 6.03Edition 1. Raleigh, NC: SAS Institute, 1988.
10 Siegel JA, Urbain JLC, Adler LP, Charkes ND, MaurerAH, Krevsky B, et al. Biphasic nature of gastric emptying.Gut 1988; 29: 85-9.
11 Scarpignato C. Gastric emptying measurement in man. In:Scarpignato C, Bianchi Porro G, eds. Frontiers ofGastrointestinal Research. Basel: Karger, 1990: 198-246.
12 Grill BB, Lange R, Markowitz R, Hillemeier AC,McCallum RW, Gryboski JD. Delayed gastric emptyingin children with Crohn's disease. Jf Clin Gastroenterol1985; 7: 216-26.
13 Metges C, Wolfram G, Schmidt H-L. Oxidation rate of13C-labelled medium chain triglycerides administeredenterally or parenterally. Clin Nutr 1985; 4 (suppl): 83.
14 Paust H, Keles T, Park W, Knoblach G. Fatty acid metab-olism in infants. In: Chapman TE, Berger R, ReijngoudDJ, Okken A, eds. Stable isotopes in paediatric nutritionaland metabolic research. Andover: Intercept, 1990:1-22.
15 Dagleish DG. Denaturation and aggregation of serum pro-teins and caseins in heated milk. Journal ofAgricultural andFood Chemis"y 1990; 38: 1995-9.
16 Scanff P, Savalle B, Miranda G, Pelissier JP, Guilloteau P,Toullec R. In vivo gastric digestion of milk proteins. Effectof technological treatments. Journal of Agricultural andFood Chemistry 1990; 38: 1623-9.
17 Nakai S, Li-Chan E. Effect of clotting in stomachs of infantson protein digestibility of milk. Food Microstructure 1987;6: 161-70.
18 Frie MD, Khoshoo V, Secker DJ, Gilday DL, Ash JM,Pencharz PB. Decrease in gastric emptying time andepisodes of regurgitation in children with spastic quadri-plegia fed a whey-based formula. Jf Pediatr 1992; 120:569-72.
19 Sturner RA, Chang KJ. Opioid peptide content ofpredigested infant formulas. Pediatr Res 1991; 29: A670.
20 Daniel H, Vohwinkel M, Rehner G. Effect of casein and,-casomorphins on gastrointestinal motility in rats. Jf Nutr1990; 120: 252-7.
21 Miller MJ, Witherly SA, Clark DA. Casein: a milk proteinwith diverse biologic consequences. Exp Biol Med 1990:143-59.
22 Meyer BM, Beglinger C, Jansen JB, Rovati LC, Werth BA,Hildebrand P, et al. Role of cholecystokinin in regulationof gastrointestinal motor functions. Lancet 1989; ii: 12-4.
23 Cuber JC, Bernard C, Levenez F, Chayvialle JA. Leslipides, proteines et glucides stimulent la secretion decholecystolinine intestinale chez le porc. Gastroenterol Jf1990; 30: 267-75.
24 Lewis LD, Williams JA. Regulation of cholecystokininsecretion by food, hormones, and pathways in the rat. AnAcad Bras Cienc 1990; 258: G512-8.
on 2 June 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.36.2.183 on 1 February 1995. D
ownloaded from





























