Embed Size (px)
Citation preview
1
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
(GYNE 1) Abortion Incomplete Abortion: Clinical features:
• Vaginal Bleeding with passage of products of gestation • Pain lower abdomen • Vitals -‐ disturbed according to the blood loss • Vaginal examination: Cervix is dilated with hanging of
fetal products and uterus size will be lesser than amenorrhea
Diagnosis: • Ultrasound
Treatment:
• Stabilize vitals and Suction evacuation / curettage • After 12 weeks – Under GA and IV oxytocin drip products
are removed by ovum forceps / Curettage.
Complete Abortion:
Clinical features:
• Vaginal Bleeding with passage of products of gestation • Pain may be less or absent • Vitals -‐ disturbed according to the blood loss • Vaginal examination: Cervix is closed and uterus size is
lesser than amenorrhea
Diagnosis: • Ultrasound
Treatment:
• No active intervention
2
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
Septic Abortion: Any abortion associated with evidence of infection in the uterus and its contents. Clinical features: � Temperature – 100.4 degree F for 24 hrs or more � Offensive or purulent vaginal discharge � Lower abdominal pain and tenderness � This is mostly due to incomplete and illegal abortions or
also following spontaneous abortion
Investigations: � Endo cervical swab for culture & sensitivity � High vaginal swab for culture & Sensitivity � CBC � DIC profile if required � Blood culture � Urine Culture � Ultrasound
Treatment: � IV Antibiotics – for aerobic, anaerobic organisms – IV
Ampicillin, Gentamycina and Metronidazole � Anti Gas Gangrene serum � Treatment of complications
� Surgery – Evacuation of uterus and Laparotomy if
necessary depending on peritonitis features
Cervical Incompetence: Causes:
• Congenital • Iatrogenic – Dilatation and Curettage, Amputation of the
cervix, cone biopsy
Clinical features: History of recurrent mid trimester abortions where leaking followed by painless expulsion of fetus
Diagnosis:
� Ultrasound – Cervical length less than 2.5 cm and cervical dilatation more than 1.5 cm with funneling of cervix and bulging of membranes
� Periodic per speculum examination Treatment:
� Cervical Circlage with Merseline tape at 16 – 18 weeks (Mc Donald operation)
� Shiridkar’s operation
3
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
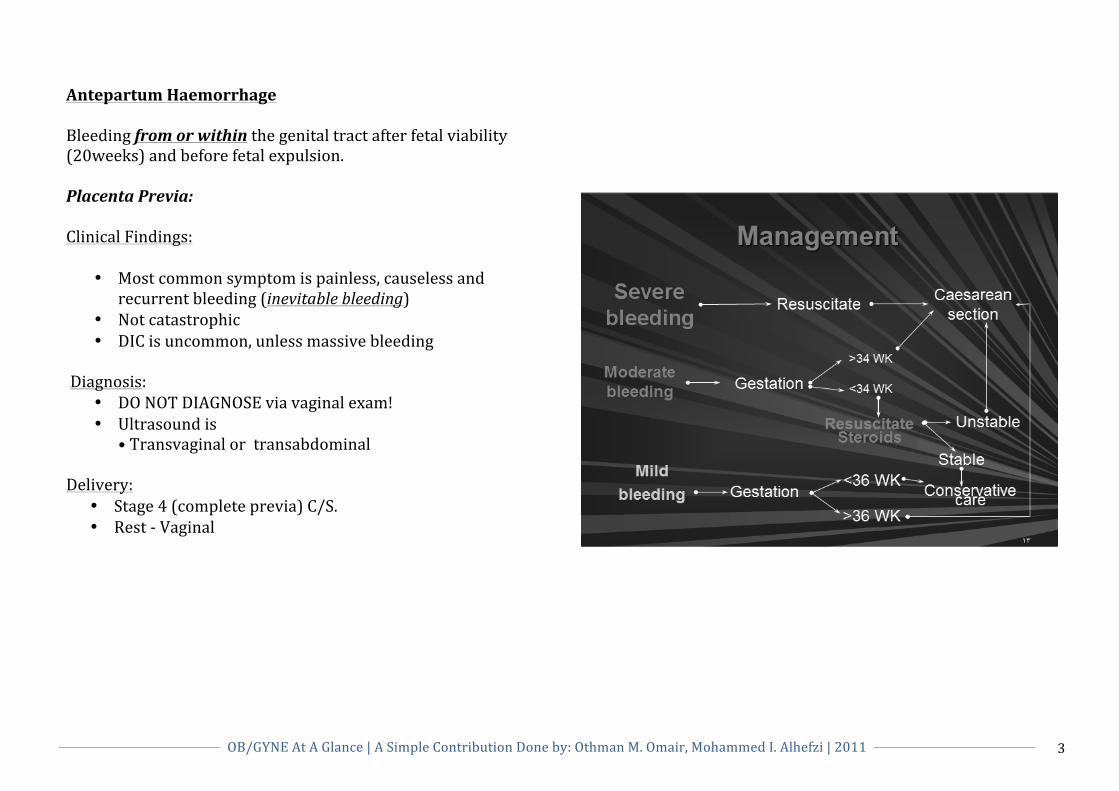
Antepartum Haemorrhage Bleeding from or within the genital tract after fetal viability (20weeks) and before fetal expulsion. Placenta Previa: Clinical Findings:
• Most common symptom is painless, causeless and recurrent bleeding (inevitable bleeding)
• Not catastrophic • DIC is uncommon, unless massive bleeding
Diagnosis:
• DO NOT DIAGNOSE via vaginal exam! • Ultrasound is
• Transvaginal or transabdominal
Delivery: • Stage 4 (complete previa) C/S. • Rest -‐ Vaginal
4
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
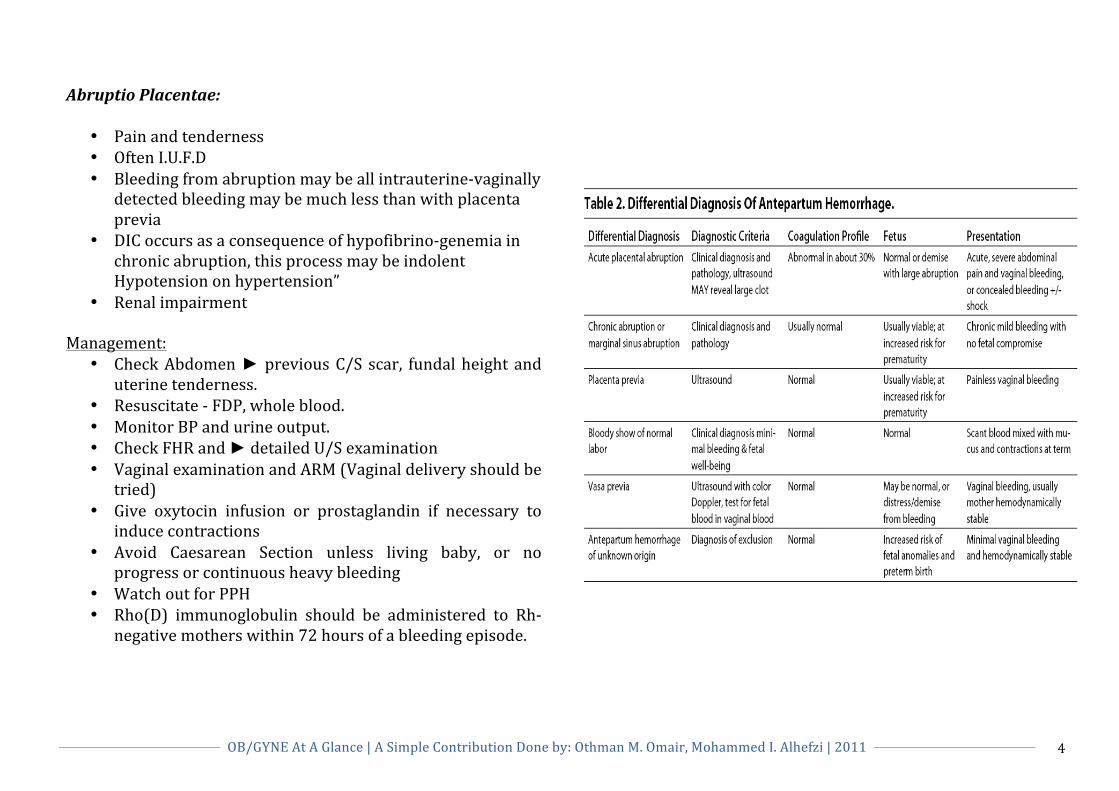
Abruptio Placentae:
• Pain and tenderness • Often I.U.F.D • Bleeding from abruption may be all intrauterine-‐vaginally
detected bleeding may be much less than with placenta previa
• DIC occurs as a consequence of hypofibrino-‐genemia in chronic abruption, this process may be indolent Hypotension on hypertension”
• Renal impairment Management:
• Check Abdomen ► previous C/S scar, fundal height and uterine tenderness.
• Resuscitate -‐ FDP, whole blood. • Monitor BP and urine output. • Check FHR and ► detailed U/S examination • Vaginal examination and ARM (Vaginal delivery should be
tried) • Give oxytocin infusion or prostaglandin if necessary to
induce contractions • Avoid Caesarean Section unless living baby, or no
progress or continuous heavy bleeding • Watch out for PPH • Rho(D) immunoglobulin should be administered to Rh-‐
negative mothers within 72 hours of a bleeding episode.
5
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
PreTerm Labor (PTL) Prediction: The 2 most important tests up to date are:
1. Fetal fibronectin 2. Cervical length measurement by TVUS
Risk Factors:
• Race. • Age: <17 yo >35 yo • Low socioeconomic status. • Poor/over weight. • Smoking • Previous hx of PTL • Multiple Gestation • Polyhydrominos. • Abdominal surgery. • Asymptomatic Bacteriuria • Systemic Infection • Medical condition complicate pregnancy
Management:
• Admission • Bed rest • Hydration / sedation • Progesterone • Tocolytics • Antibiotics • Steroids
PROM: Before onset of delivery, after 37wks. Diagnosed by: speculum vaginal examination of the cervix and vaginal cavity
1. Pooling of fluid in the vagina or leakage of fluid from the cervix
2. Ferning of the dried fluid under microscopic examination 3. Alkalinity of the fluid as determined by Nitrazine paper 4. A new product, AmniSure
Management:
• Wait for spontaneous delivery for 12-‐24hours. • Induction of labor after 24 hours.
PPROM: Occurs 24-‐34wks of gestation. Management:
• Avoid digital examination • Admission • Bed rest • Antibiotics • Corticosteroids
* Delivery according to maternal and fetal states.
6
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
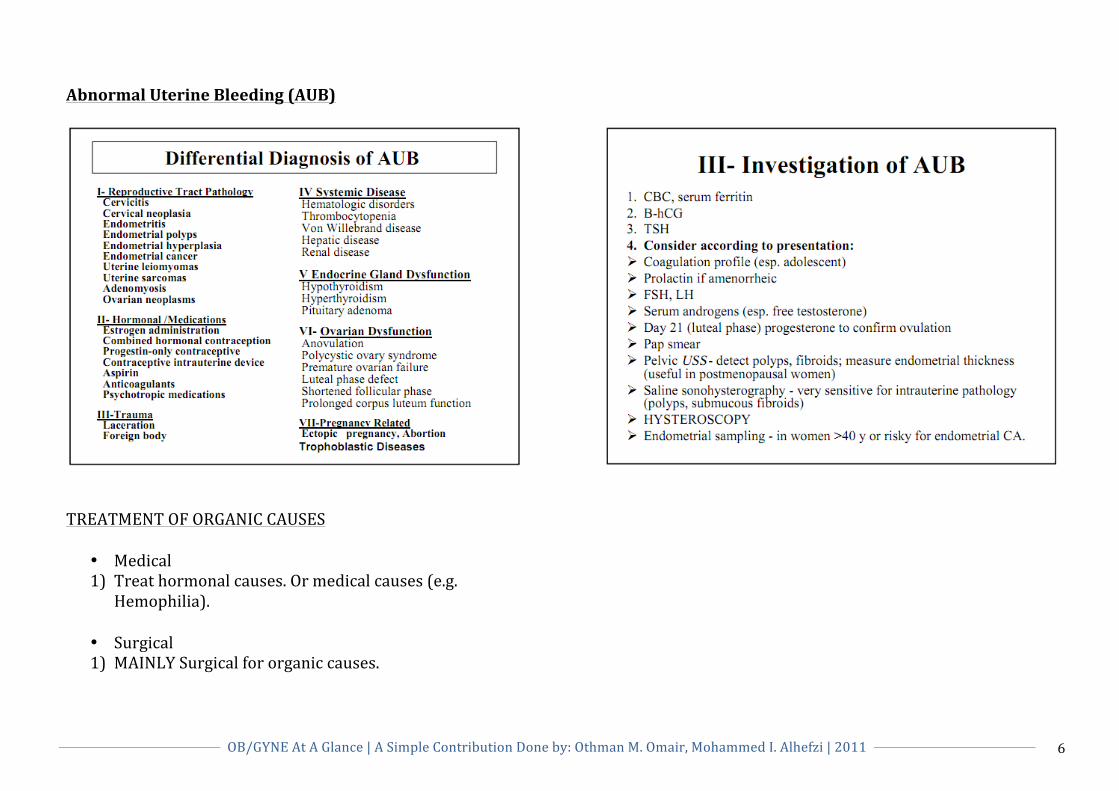
Abnormal Uterine Bleeding (AUB)
TREATMENT OF ORGANIC CAUSES
• Medical 1) Treat hormonal causes. Or medical causes (e.g.
Hemophilia).
• Surgical 1) MAINLY Surgical for organic causes.
7
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
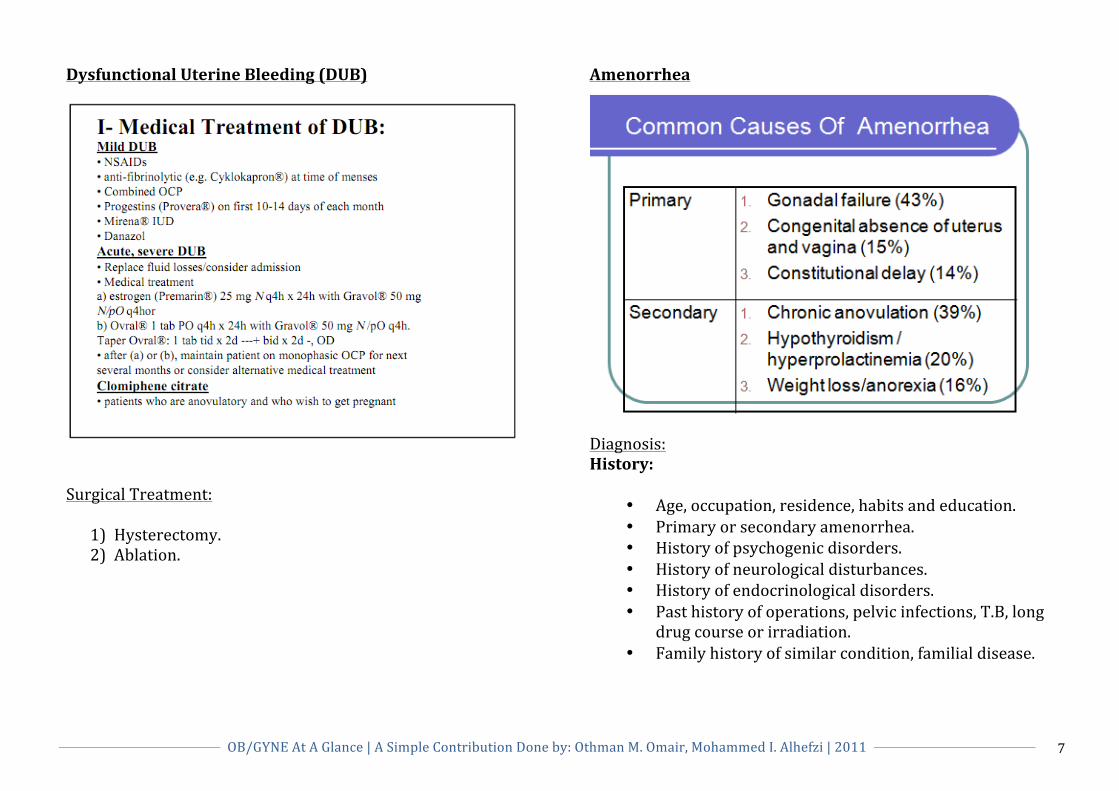
Dysfunctional Uterine Bleeding (DUB)
Surgical Treatment:
1) Hysterectomy. 2) Ablation.
Amenorrhea
Diagnosis: History:
• Age, occupation, residence, habits and education. • Primary or secondary amenorrhea. • History of psychogenic disorders. • History of neurological disturbances. • History of endocrinological disorders. • Past history of operations, pelvic infections, T.B, long
drug course or irradiation. • Family history of similar condition, familial disease.
8
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
Amenorrhea (C’ntd) Physical Exam:
• Psyche, height, weight and span measure. Nutritional status should be also evaluated.
• Secondary sexual characters. • Evidence of neurological disorders specially central lesions.
• Evidence of endocrinological disorders with special reference to galactorrhea and hirsutism.
• Evidence of general disease as heart, chest, renal or hepatic disorder.
• Abdominal masses (ovarian, adrenal, renal hepatosplenomegaly or ascites).
• External genital anomaly or hypoplasia. • Pelvic examination (PV or PR) for uterine and ovarian abnormalities.
INVESTIGATIONS:
• Special investigations – Step I: a. Search for specific disease if suspected. b. Pregnancy test. c. TSH assay. d. Prolactin assay. e. Progesterone challenge test:
1) If (+)ve withdrawal → Normal outflow tract and well estrogenized cases → The cause is anovulation.
2) If (-‐)ve withdrawal → Hypoestrogenic state or uterine cause → step II
• Special investigations – Step II:
a. Give estrogen + Progesterone:
1) If (+)ve withdrawal → Normal outflow tract and uterus, and there is ovarian failure → Step III
2) If (-‐)ve withdrawal → Uterine cause.
• Special investigations – Step III: a. Measure FSH:
1) If high → Ovarian cause. 2) If low → Central cause.
Treatment:
• Treat the cause.
9
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
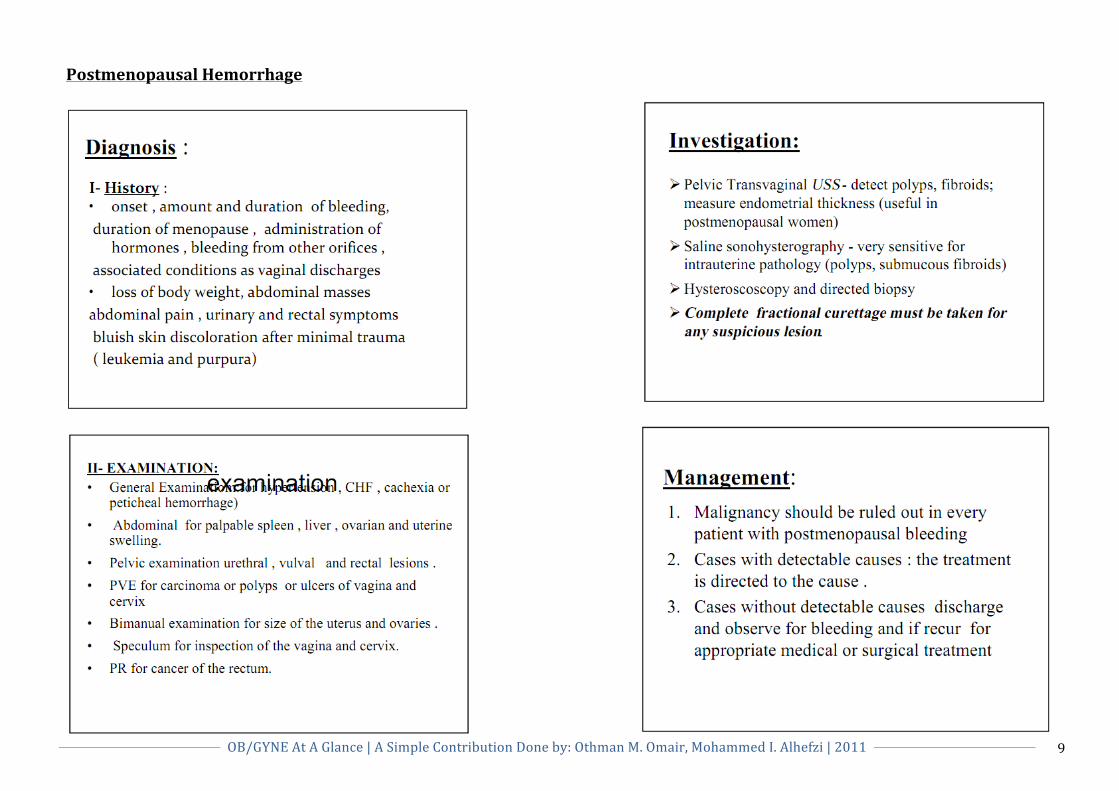
Postmenopausal Hemorrhage
10
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
(GYNE 2) HTN (Pre-‐eclampsia) RISK FACTORS:
1) +ve family history in the first–degree relatives. Increase the risk of PET 4 – 8 fold.
2) Prime Parity 3) Medical disorders as:
a. History of PET. b. Chronic hypertension. c. Diabetes. d. Obesity. e. Antiphospholipid syndrome. f. Molar pregnancy. g. Multiple pregnancy. h. Hydrops Fetalis.
Diagnosis:
(1) US (2) Biochemical tests
a) Hb, and Hematocrit concentrations. b) CBC with platelets count. c) Serum uric acid . d) Endothelial activation markers are increased. e) Urinary excretion of Ca and microalbuminuria f) Urine analysis. g) 24h urine for protein, creatinine clearance,
Catecholamine metabolites and free cortisol. h) Blood Urea and electrolytes as Na & K. i) Lupus anticoagulant and anticardiolipin in APS. j) Serum lipids.
(3) Fundoscopy. (4) ECG & ECHO. (5) X ray chest. Signs & Symptoms: Weight gain + HTN + Edema. Criteria of Severe Preeclampsia:
(1) Blood Pressure: o > 160 mmHg Systolic or o > 110 mm Hg Diastolic
(2) Proteinuria: > 3g in 24 hours. (3) Persistent and Severe cerebral or visual disturbances
o Headache o Blurred vision
(4) Persistent and Severe epigastric pain or RUQ pain. (5) Pulmonary edema or cyanosis. (6) Oliguria (< 500 ml urine / 24 hours). (7) Eclampsia (Grand Mal Seizures). (8) HELLP syndrome.
Management:
A. PET Remote from Term
1) Placental insufficiency: a) Monitoring of fetal movements. b) Serial symphesis-‐Fundal Height . c) Serial US.
2) Involvement of other organ systems: a) Serial platelets count. b) Hematocrit values c) Clotting abnormalities d) Raised uric acid e) Severe proteinuria f) HELLP syndrome
11
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
HTN (C’ntd) Indications of termination of pregnancy in PET:
1. Uncontrollable hypertension. 2. Deteriorating liver or renal function. 3. Progressive fall in platelets. 4. Neurological complications as cerebral Hge. 5. Deteriorating fetal condition as non-‐reactive CTG.
B. PET near term a) Antihypertensive b) Low dose aspirin c) For prophylaxis:
a. Ca b. Fish oil c. Antioxidants d. Vit. C e. Vit. E
C. Severe cases: 1) IV antihypertensive 2) Anticonvulsant therapy
a. Magnesium Sulfate. 3) Fluid management.
Diabetes In Pregnancy
RISK FACTORS: 1) Diabetes in 1st degree relatives. 2) Maternal obesity. Wt.90kg. 3) Persistent glycosuria. 4) Previous hx. Of large baby. 5) Previous hx. Of unexplained still birth. 6) Previous birth of congenitally malformed baby. 7) Polyhydramnios/Macrosomia in current Pregnancy.
Diagnosis:
1) Random glucose Test. • Cut of value 6.4 mmol/l with in 2 hrs & 5.8mmol/l
after 2 hrs of meal -‐-‐-‐-‐-‐ OGTT. 2) Fasting glucose Test.
• Cut of value 4.8mmol/l -‐-‐-‐-‐-‐OGTT. 3) Glucose challenge Test: At 28wks.
• 50g glucose given. • 1hr later blood taken -‐-‐ if >7.8mmol/l -‐-‐-‐-‐ OGTT.
Treatment: • Insulin + Diet. • Antenatal care. • DELIVERY:
a) Time of Delivery: 1) Well controlled DM -‐-‐-‐ 39-‐40 weeks 2) Uncontrolled DM -‐-‐-‐-‐-‐ 38 weeks
b) Mode of Delivery: 1) Vaginal delivery is mode of choice 2) Low threshold for C-‐ section
c) Management During Labour: • Insulin therapy: Give I/V insulin 1 unit/h
12
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
Benign Ovarian Tumors Presentation:
• Asymptomatic • Pain • Abdominal swelling • Pressure effects • Menstrual disturbances • Hormonal effects • Abnormal cervical smear
Follicular cyst • During treatment with clomiphene or gonadotropin
Lutein cyst • Amenorrhea or delayed onset of menstruation.
Hemorrhagic cyst • Haemoperitoneum.
Theca–lutein cyst • high levels of hCG; a) Ovulation induction with gonadotropins or clomiphene b) Are usually bilateral
Surgical intervention if there is haemorrhage. Granulosa–theca cell tumor
• precocious menarche • irregular and prolonged vaginal bleeding. • Postmenopausal bleeding
Sertoli-‐Leydig cell tumor
• Hirsutism, deepening of the voice, clitoromegaly and defeminizing change in body habitus to a muscular build.
Ovarian fibroma
• Meigs' syndrome (ascites and hydrothorax in association with an ovarian fibroma).
Investigations:
• Bimanual examination • Pelvic ultrasonography • Tumor markers, such as Serum CA 125, may help to
distinguish between benign and malignant masses • Laparoscopy • Laparotomy
Treatment:
• Surgery.
13
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
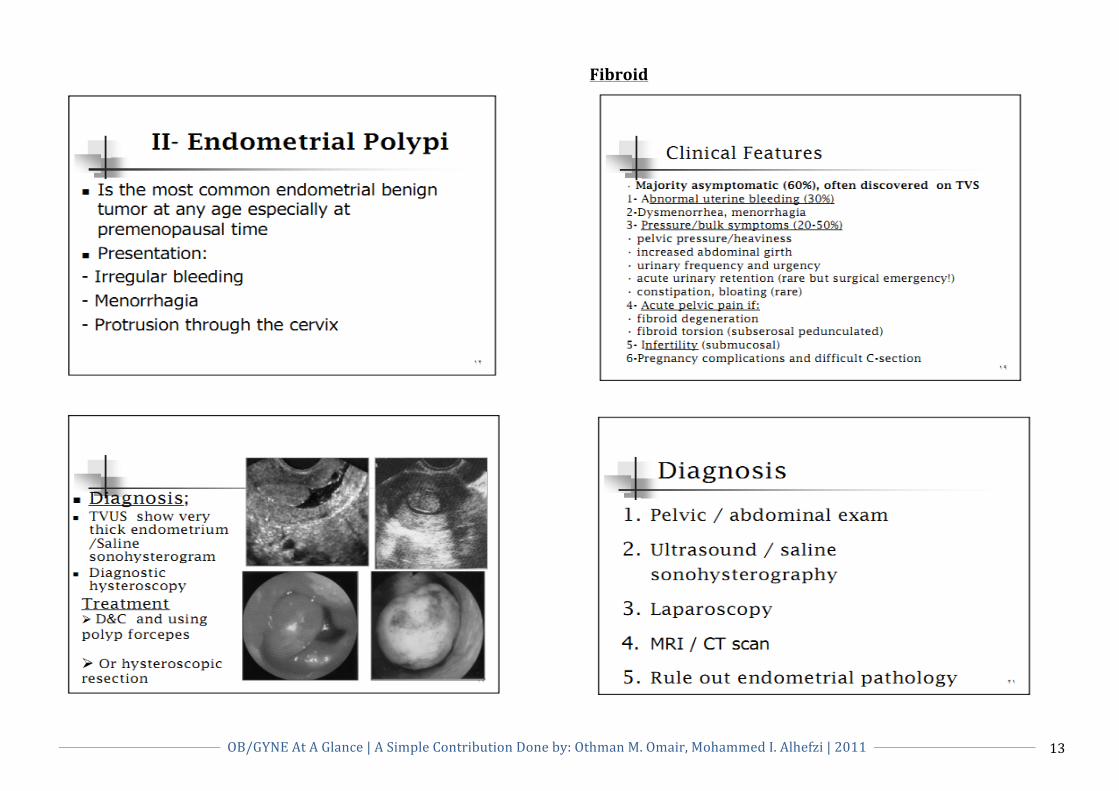
Fibroid

14
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
Fibroid (C’ntd)
Conservative Treatment; if:
• Less than 6-‐8cm. • Mild symptoms. • Not Sub-‐Mucosal. • Not Postmenopausal.
15
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
Urinary Tract Infection (UTI)
• Pyelonephritis is a bacterial infection of the renal–parenchyma and the renal pelvicaliceal system.
• Acute pyelonephritis is commonly associated with chills
and fever, flank pain, costovertebral tenderness, urinary frequency, urgency and dysuria.
• Cystitis is an inflammation of the urinary bladder.
Patients with cystitis usually have symptoms of lower urinary tract irritation (dysuria, frequency, urgency, suprapubic discomfort, hematuria).
ü Recurrent UTI is diagnosed when two UTIs occur within
6 months or 3 or more occur during a single year.
Investigations:
ü Urinalysis • Microscopic examination • Pyuria
ü Urine Culture and Microbiology
ü Radiologic Studies
• Intravenous pyelography • Computed tomographic urography • Cystography and voiding urethrocystography
ü Endoscopic Studies • Urethroscopy • Cystoscopy
ü Renal Function Test
• Urea nitrogen • Serum creatinine
Management:
1) Rest and hydration
2) Acidification of the urine • Ascorbic acid (500 mg twice daily) • Ammonium
3) Urinary analgesics • Phenazo–pyridine hydrochlorid (Pyridium), 100 mg
twice daily for 2 to 3 days
4) Antimicrobial therapy • Nitrofurantoin • Cephalosporins (e.g., Keflex, Duricef) • Antibiotics such as ampicillin, tetracycline, and
trimethoprim–sulfamethoxazole (e.g., Septra, Bactrim)

16
OB/GYNE At A Glance | A Simple Contribution Done by: Othman M. Omair, Mohammed I. Alhefzi | 2011
This Document has been done by: Othman M. Omair & Mohammed I. Alhefzi It does highlight on important topics at both Gyne I and Gyne II which are needed in Final OSCE Exam
Infertility, Isoimmunization lectures are not in this document as they were not completed by the time we made this. Sorry for any inconvinence that this may cause you
However, most information were collected from lectures, powerpoint slides and PDFs We hope you find this helpful
Please Don’t forget to pray for us both!
Best of Luck,
Othman M. Omair Mohammed I. Alhefzi
OB/GYN II | 2011